brain infections3
TRANSCRIPT

Infections of the Brain and
Meninges
Mohamed SamirAssist. Lecturer

Acquired:♣ Non-Specific:
1- Meningitis.
2- Pyogenic Parenchymal Infections.
3- Encephalitis.
♣ Specific:
1- TB & Fungal Infections.
2- Parasitic Infections.

1. Acquired:♣ Specific:
Fungal Infections.
Parasitic Infestations.
TB.

Fungal Infections

Fungal Infect ions
Immunicompetent:• Histoplasmosis.
• Blastomycosis.
• Coccidioidomycosis.
• Aspegillosis (Rare).
Immunocompromized:• Aspergillosis.
• Candidiasis.
• Cryptococcosis.

Fungal Infections
• Direct extension (Fungal Sinusitis).
• Hematogenous.

Fungal Infections
• Granulomatous Reaction.• Aspergillosis → invades blood vessels-Hgic infarcts.
• Cryptococcosis → gelatinous perivascular space
pseudocysts.
• Coccidioidomycosis → meningitis – caseating
granulomas

Fungal Infections

Fungal Infections

Fungal Infections

Parasitic Infestations

Parasitic Infestations
• Toxoplasmosis.
• Cysticercosis.


Toxoplasmosis
• Toxoplasma gondii
• Intracellular protozoal parasite
• Human infection usually occurs via the oral or
transplacental route.
• Most T gondii infections are subclinical, but
severe infection can occur in patients who are
immunocompromised

Toxoplasmosis
• In immunocompetent hosts, cysts containing live T
gondii organisms cause no harm; most patients remain
asymptomatic but seropositive.
• However, if the immune system of the host declines, the
cysts may reactivate, causing disseminated infection that
manifests as encephalitis, myocarditis, or chorioretinitis.
• In immunocompromised patients, T gondii infection is
potentially fatal. If seronegative, these patients can be
infected via the usual oral route or via transplantation of
an organ. More commonly, infection results from
reactivation of latent tissue cysts.

Toxoplasmosis
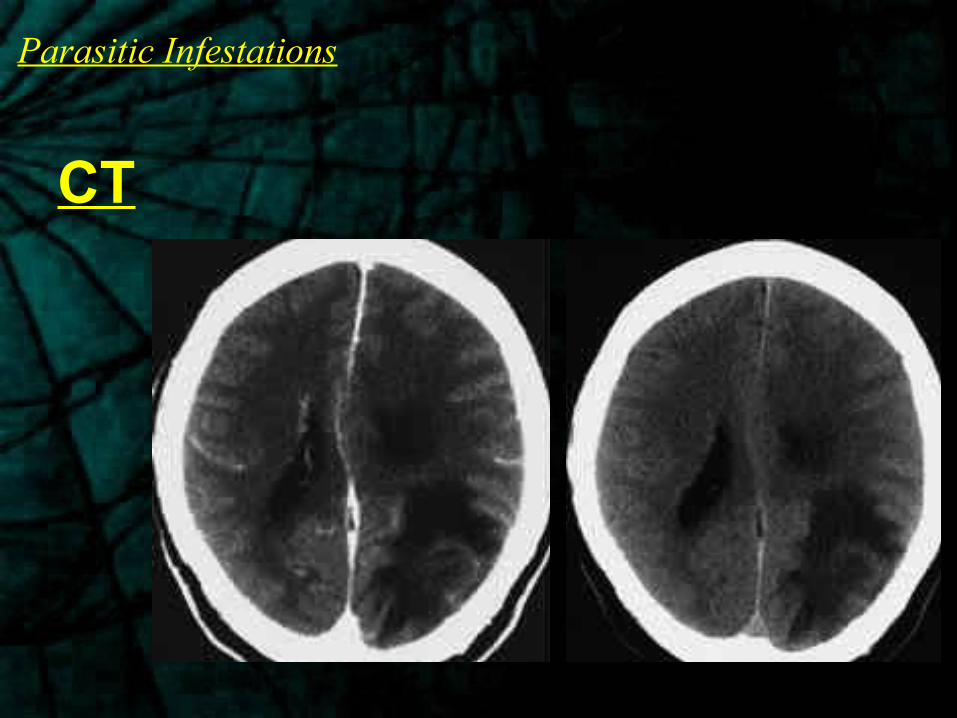
• CT scans of the brain may show
single (30%) or multiple
nodular/Ring enhancing lesions.
• Edema of the surrounding white
matter is often depicted.
CT
Parasitic Infestations
CT

Toxoplasmosis
•Approximately 75% of the nodules are
located in the basal ganglia, but others are
scattered throughout the brain at the gray
matter–white matter junction.

Toxoplasmosis
Calcification may occur following
medical treatment.
Toxoplasmosis
MRI
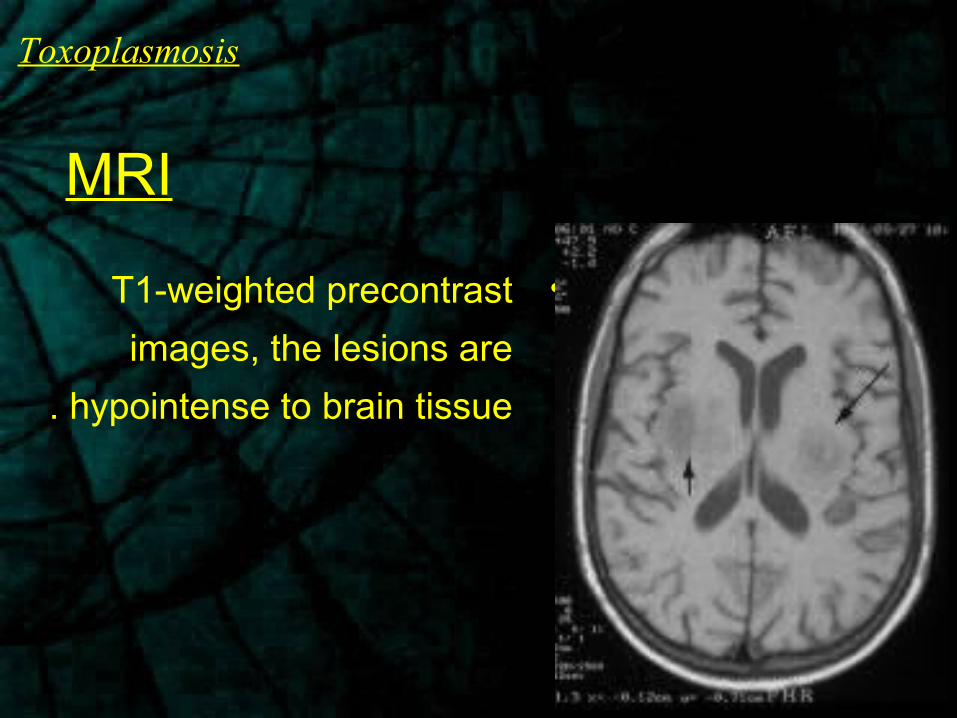
•T1-weighted precontrast
images, the lesions are
hypointense to brain tissue.

Toxoplasmosis
MRI
• T2-weighted MRI, the foci of
infection are usually
hyperintense, but they can
occasionally be isointense to
hypointense.

Toxoplasmosis
MRI
• Focal nodular or ring
enhancement occurs in
approximately 70% of
patients after gadolinium
enhancement.

Toxoplasmosis
MRI
• Active lesions often are
surrounded by edema.

Toxoplasmosis
• The characteristic sign of CNS toxoplasmosis is the
asymmetric target sign, which is detectable on both CT
scans and MRI, though MRI is more sensitive. The
asymmetric target sign represents a ring-enhancing
abscess, which contains similar ring-enhancing abscesses,
which contain similarly enhancing, eccentric nodules in the
abscess cavity.

Toxoplasmosis

Toxoplasmosis
• Lesions of CNS lymphoma often are solitary, whereas
nodules of CNS toxoplasmosis are more often multiple.
• A diagnosis of toxoplasmosis is favored over a diagnosis of
lymphoma when more than 3 lesions or slender, ring-
enhancing foci are seen or when marked edema is present.
In addition, toxoplasmosis is more common subcortically
than lymphoma and seldom affects the corpus callosum

Toxoplasmosis
MRI
Disease CT T1-weighted T2-weighted ContrastEnhancement
MRSpectroscopy
Toxoplasmosis Hypodense masses with
ring enhancement
Hypointense lesions.
Discrete hyperintense foci
– moderate edema
Ring enhancement
Markedly elevated lactate and lipids with
depleted metabolites.
Lymphoma Hyperdense masses with solid or ring
enhancement
Hypointense. Iso to Hyperintense
masses – moderate edema
Homogeneous or ring
enhancement
Elevated choline with
mildly to moderately
elevated lactate and lipids.

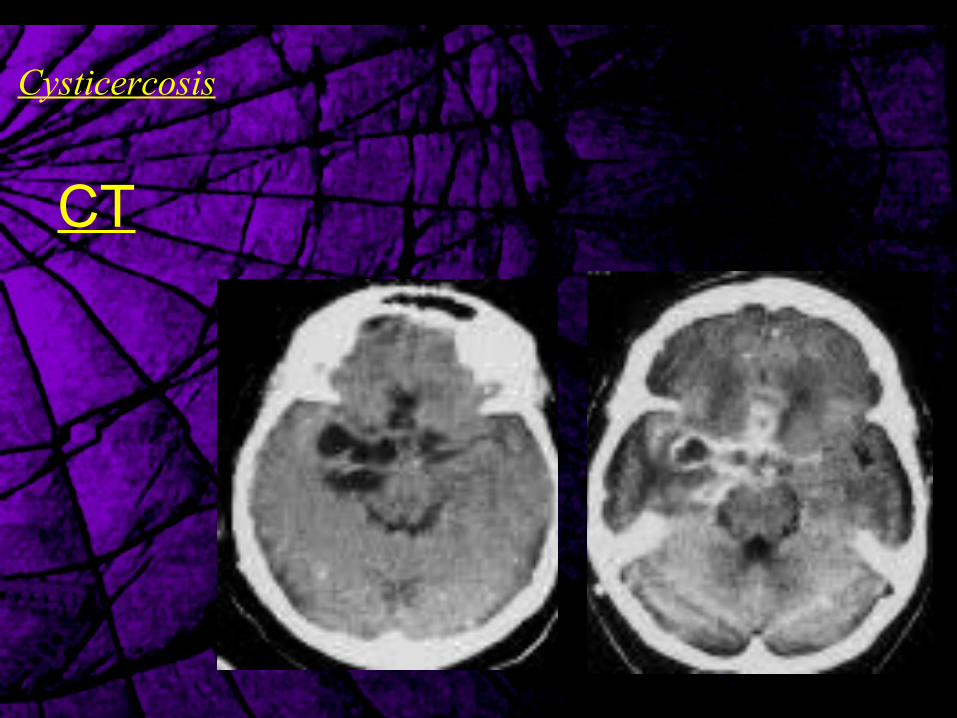
Cysticercosis

Cysticercosis
• Cysticercosis is the most common
parasitic infestation affecting the central
nervous system.
• Taenia solium.

Cysticercosis
CNS cysts are encountered in 4 types in NCC:
(1) Meningeal (racemose variety).
(2) Parenchymal (solitary or multiple cysts).
(3) Ventricular (usually solitary).
(4) Mixed.

Stages of NCC:
• The host can tolerate the worm as long as the
embryo is alive. Viable cysticerci are associated
with minimal inflammation (vesicular stage).
Cysticercosis

Stages of NCC:
• The worm usually dies 2-6 years after infection, and
the disintegration of the parasite triggers a vigorous
tissue reaction, the cyst wall is infiltrated and
surrounded by predominantly mononuclear cells.
Inflammatory cells enter the cyst fluid (colloid stage).
Cysticercosis

Stages of NCC:
• As the host's immune response progresses,
fibrosis encompasses the cysticercus, with
collapse of the cyst cavity (granular-nodular
stage). The dead parasite decays into an
eosinophilic desiccated material.
Cysticercosis

Stages of NCC:
• The final stage is a calcified nodule, presumably
the result of dystrophic calcification of the
necrotic larva (calcific stage).
Cysticercosis

Cysticercosis
The various pathologic states that may be seen in NCC include the following:
(1) Meningoencephalitis
(2) Granulomatous meningitis.
(3) Focal granuloma.
(4) Focal or diffuse multiple cysts.
(5) Hydrocephalus.
(6) Intraventricular cysts.
(7) Ependymitis.
(8) Arteritis.

Cysticercosis
The viable cyst appears as a thin-walled fluid-filled
cyst with a mural nodule (live scolex).
The cyst causes no inflammatory reaction or edema,
and it does not enhance
CT

Cysticercosis
In the colloid stage, the cyst is encapsulated, it
contains a high-protein fluid, and it demonstrates
ring enhancement. Often, associated edema or
enhancement is noted in the brain parenchyma
CT

Cysticercosis
CT

Cysticercosis
As the cysticercus becomes fibrotic or
collapses, a focal area of enhancement
suggestive of granuloma is seen
(granular-nodular stage)
CT

Cysticercosis
CT
Cysticercosis
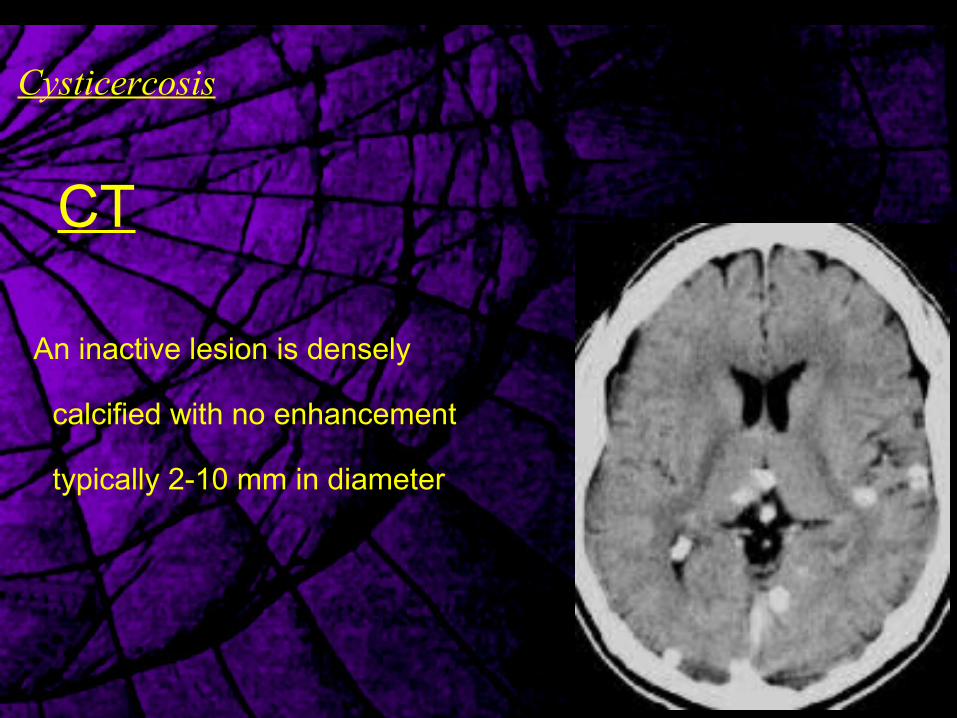
An inactive lesion is densely
calcified with no enhancement
typically 2-10 mm in diameter
CT
Cysticercosis
• Intraventricular cysts result in obstructive hydrocephalus.
• Cysticerci can be seen in any of the ventricles.
• CT scans may reveal evidence of obstructive hydrocephalus or
dilatation or distortion of the involved ventricle.
CT

Cysticercosis
CT
CT scans obtained after the
intraventricular administration of
contrast material delineate the cyst
and the site of the obstruction

Cysticercosis
CTSubarachnoid NCC is described in 3 subtypes as follows:
(1) If it is located in the gyri of the cerebral convexities.
(2) When cysticerci are found in the fissures (eg, Sylvian fissure).
(3) Cysticercosis of the basal cisterns is characterized by arachnoiditis and
seen as focal or diffuse meningeal enhancement or vasculitis with stroke.
Patients often develop communicating hydrocephalus.
Cysticercosis
CT

Cysticercosis
MRI
T1WIs clearly show an eccentric,
hyperintense, 2- to 5-mm scolex
The demonstration of a scolex is
pathognomonic for NCC.

Cysticercosis
MRI
When the larva begins to die (colloid stage), the fluid in the
cyst becomes more turbid, and it is mildly hyperintense to
CSF on both T1WIs and T2WIs. The surrounding edema
is hypointense on T1WIs and hyperintense on T2WI.

Cysticercosis
MRI
The hypointense cyst wall stands out
between the hyperintense cyst fluid
and edema on T2WI.
The cyst wall may be enhancing in the
granular-nodular stage.

Cysticercosis
MRI

Cysticercosis
MRI

Tuberculosis

Tuberculosis
• Mycobacterium Tuberculosis.
• Hematogenous.

Tuberculosis
• CNS TB affects the brain and meninges.
• Infection starts in a subpial or subependymal cortical
focus (ie, Rich focus), resulting in a granuloma that
erodes into the subarachnoid space causing basal
leptomeningitis.
Pathophysiology:

Tuberculosis
• The meningitis usually causes communicating
hydrocephalus, but it may also cause obstruction of
the foramina of Luschka and Magendie, resulting in
obstructive hydrocephalus.
• Vasculitis involving the lenticulostriate and
thalamoperforatoring arteries may occur and cause
small infarcts in the deep gray nuclei and deep white
matter.
Pathophysiology:
Tuberculosis
• Tuberculous meningitis.
• Focal parenchymal granulomas (e.g. tuberculomas).
• Tuberculous abscesses.
• Tuberculous cerebritis.

Tuberculosis
• CECT of the brain depicts prominent
leptomeningeal and basal cistern
enhancement.
• Ventricular dilatation (eg, dilatation of the
third and fourth ventricles) due to
hydrocephalus is usually seen.
CT
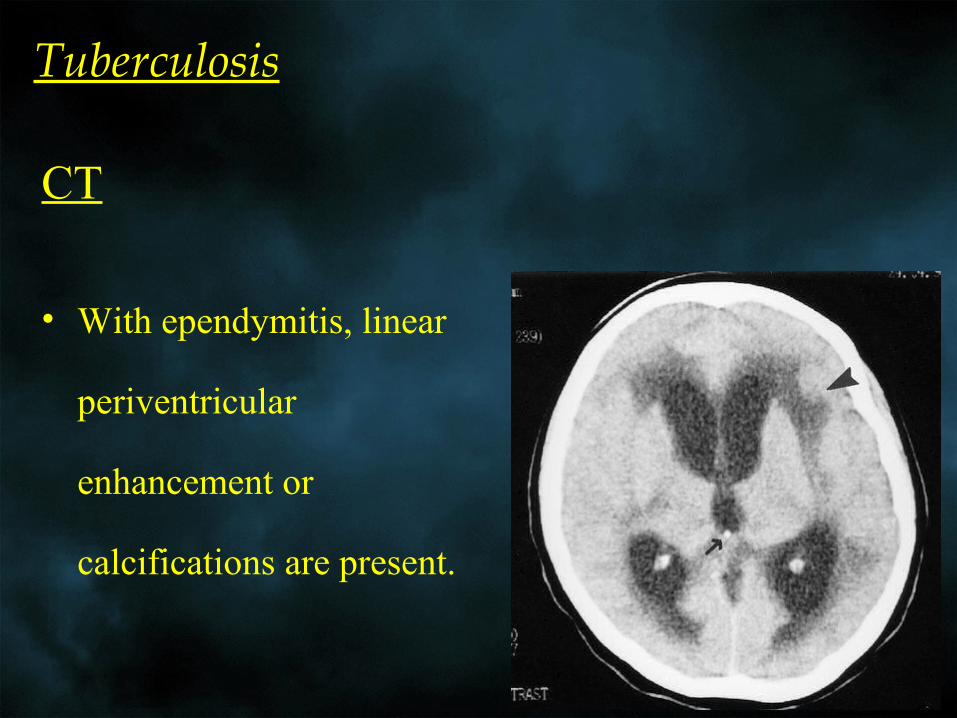
Tuberculosis
• With ependymitis, linear
periventricular
enhancement or
calcifications are present.
CT

Tuberculosis
• Often, low-attenuating
focal infarcts are seen in
the deep gray matter nuclei,
deep white matter, and
pons; these infarcts result
from associated vasculitis.
CT

Tuberculosis
Parenchymal tuberculomas demonstrate various patterns:
• Noncaseating granulomas are homogeneously enhancing lesions.
• Caseating granulomas are rim enhancing; if these have a central
calcific focus, they may form a target-like lesion.
• Granulomas may also form a miliary pattern with multiple tiny
nodules scattered throughout the brain.
CT

Tuberculosis
CT

Tuberculosis
CT

Tuberculosis
• Gadolinium-enhanced T1-
weighted images demonstrate
prominent leptomeningeal and
basal cistern enhancement.
MRI

Tuberculosis
• With ependymitis, linear
periventricular enhancement is
present. Ventricular dilatation due to
hydrocephalus is usually seen.
• Deep gray matter nuclei, deep white
matter, and pontine infarctions.
MRI

Tuberculosis
Parenchymal tuberculomas demonstrate various patterns:
• They are typically hypointense on T2-weighted images, but they
may be hyperintense as well.
• Noncaseating granulomas are homogeneously enhancing lesions.
• Caseating granulomas are rim enhancing.
• Granulomas may also form a miliary pattern
• Lesions are typically surrounded by hyperintense edema.
MRI

Tuberculosis
MRI

Tuberculosis
MRI

Tuberculosis
• MR spectroscopy can be used to characterize
tuberculomas and differentiate them from neoplasms.
• Tuberculomas show elevated fatty-acid spectra.
MRI

THANK YOU