brain function monitoring and itʼs role in anesthetic...
TRANSCRIPT

086-0092 1.01 1
Brain Function Monitoring and it’s Role
in Anesthetic Management
Michael Geisler, CRNA, BSN
Private Anesthesia Practitioner
Ponte Vedra Beach, Florida
Learning Objectives • Explore the rationale for monitoring brain function
• Review Bispectral Index™ (BIS) fundamentals
• Examine evidence-based results of BIS monitoring
• Provide an update on Intraoperative Awareness
• Using case studies, illustrate BIS responses during anesthesia
• Discuss clinical applications and benefits of BIS monitoring
Why Monitor Consciousness?
Side-effects Costs Adverse Outcomes
Complications Adverse Outcomes
ANESTHETIC DEPTH
OVERDOSING UNDERDOSING ADEQUATE/OPTIMAL
BEST OUTCOMES Quality + Safety
Anesthetic Effect Management
086-0092 1.01 2
100
80
60
40
20
0
BIS
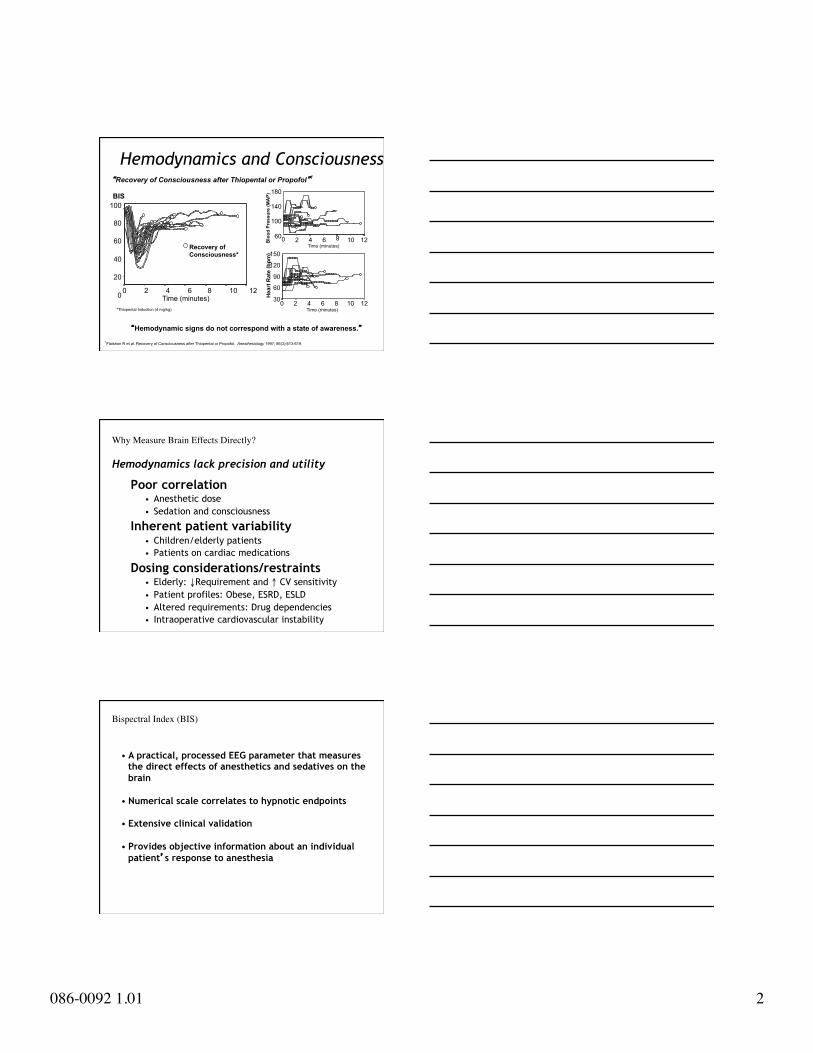
Recovery of Consciousness*
0 2 4 6 8 10 12
*Thiopental Induction (4 mg/kg)
Time (minutes)
Blo
od P
ress
ure
(MA
P) 180
140
100
60 12 10
8
6 4 2 0 Time (minutes)
Hea
rt R
ate
(bpm
)
150
120
90
60
30 12 10 8 6 4 2 0 Time (minutes)
“Hemodynamic signs do not correspond with a state of awareness.” 1Flaishon R et al. Recovery of Consciousness after Thiopental or Propofol. Anesthesiology 1997; 86(3):613-619.
“Recovery of Consciousness after Thiopental or Propofol”1
Hemodynamics and Consciousness
Poor correlation • Anesthetic dose • Sedation and consciousness
Inherent patient variability • Children/elderly patients • Patients on cardiac medications
Dosing considerations/restraints • Elderly: ↓Requirement and ↑ CV sensitivity • Patient profiles: Obese, ESRD, ESLD • Altered requirements: Drug dependencies • Intraoperative cardiovascular instability
Hemodynamics lack precision and utility
Why Measure Brain Effects Directly?
• A practical, processed EEG parameter that measures the direct effects of anesthetics and sedatives on the brain
• Numerical scale correlates to hypnotic endpoints
• Extensive clinical validation
• Provides objective information about an individual patient’s response to anesthesia
Bispectral Index (BIS)
086-0092 1.01 3
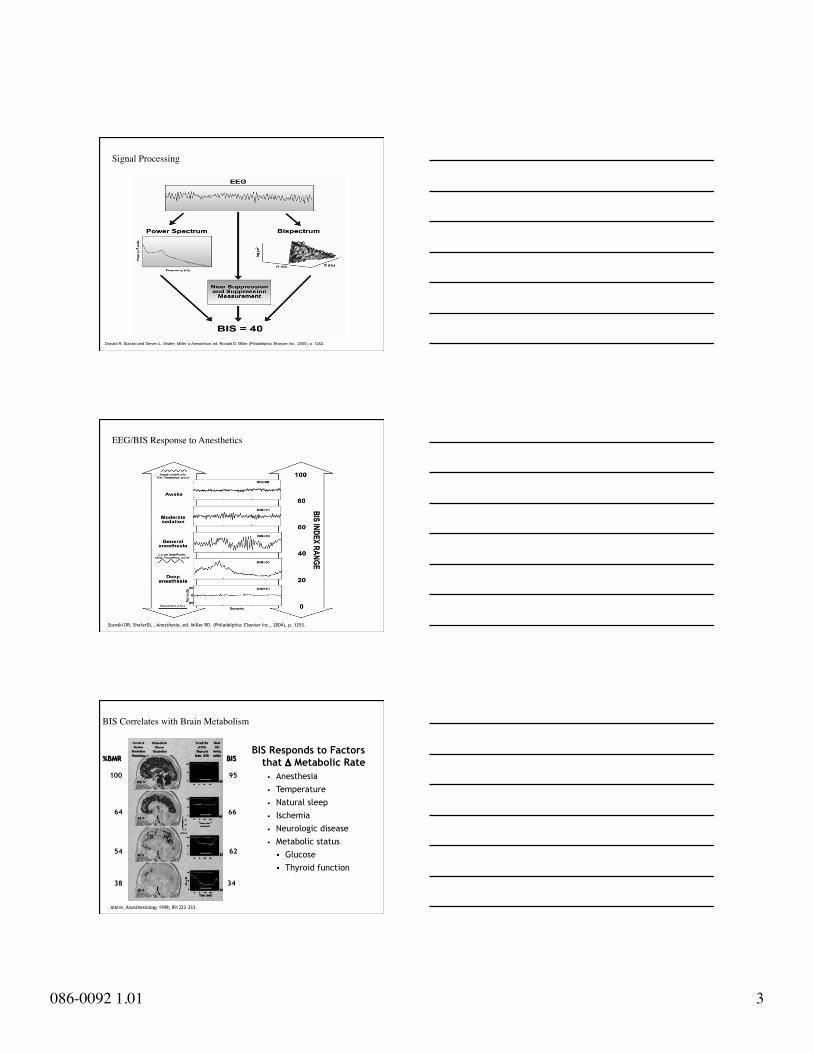
Donald R. Stanski and Steven L. Shafer, Miller’s Anesthesia, ed. Ronald D. Miller (Philadelphia: Elsevier Inc., 2005), p. 1252.
Signal Processing
Stanski DR, ShaferDL , Anesthesia, ed. Miller RD. (Philadelphia: Elsevier Inc., 2004), p. 1253.
EEG/BIS Response to Anesthetics
Alkire, Anesthesiology 1998; 89:323-333.
BIS Responds to Factors that Δ Metabolic Rate
• Anesthesia • Temperature • Natural sleep • Ischemia • Neurologic disease • Metabolic status
Glucose Thyroid function
34
95
62
66
38
54
64
100
BIS %BMR
BIS Correlates with Brain Metabolism

086-0092 1.01 4
Meta-analysis to examine the clinical impact of BIS monitoring on anesthetic use, incidence of PONV, duration of PACU stay and time to discharge in ambulatory anesthesia.
• 11 randomized controlled trials enrolling 1,380 subjects • Comparison of BIS monitoring to standard practice (sp)
Key Results BIS monitoring:
• Significantly reduced anesthetic use by 19% compared to sp • Reduced the incidence of PONV by 16% • Reduced PACU time by 4 minutes
Author estimated net cost of $5.55 per patient
Liu SS. Effects of Bispectral Index Monitoring on Ambulatory Anesthesia: A Meta-analysis of Randomized Controlled Trials and a Cost Analysis. Anesthesiology 2004; 101(2):311-315.
Clinical Impact of BIS Monitoring
Meta-analysis
Drug Savings (Gan, 1997; Bannister, 2001; Wong 2002; White 2004; Liu ,2004)
Isoflurane Propofol Sevoflurane Desflurane
Decreased PONV (Nelskya, 2001; Luginbühl, 2003)
Control BIS Titrated
Faster Wake-Ups (Gan, 1997)
Standard Practice BIS-Titrated
Shorter PACU Stays (White, 2004)
Standard Practice BIS-Titrated
Documented Anesthesia Benefit Summary
%
%
%
Min
utes
Denman WT et al. Anesthesia & Analgesia 2000; 90 (4): 872-877. Degoute CS et al. British Journal of Anaesthesia 2001; 86(2): 209-212. Davidson AJ et al. Anesthesia & Analgesia 2001; 93 (2): 326-330. Laussen PC et al. Paediatric Anaesthesia 2001; 11 (5): 567-573. Bannister CF et al. Anesthesia & Analgesia 2001; 92 (4):877-881. Johansen JW. Anesthesia & Analgesia 1998; 86: S406.
BIS-guided titration during general anesthesia: • Correlates with the hypnotic component of anesthetics
accurately reflecting level of consciousness
• Improves titration of general anesthetics
• 25-40% reduction in measured recovery times
• Useful during pediatric anesthesia, including cardiac
Documented Benefits in Children

086-0092 1.01 5
• General Incidence: 0.1-0.2% Sandin, Lancet 2001; Sebel, Anesth Analg 2004
• Preoperatively, many patients are concerned
Royston & Cox, Lancet 2003;362:1648-58
• Patients would pay $35 to prevent awareness Gan, J Clin Anesth 2003; 15:108-12
• Highest risk factor for patient dissatisfaction Myles et al. BJA 2000; 84: 6-10
• 65% of patients do not tell their anesthetist Moerman et al. Anesthesiology 1993; 79:454-464
Is Intraoperative Awareness a Problem?
N Death Awareness Pain PONV
382 23% 19% 5% 6%
100 15% 15% - - 5%
129 54% 4.5% - - 22%
800 37% 24% 34% 22%
166 43% 52% 38% - -
132 19% - - 39% - -
1216 12% 20% 9% 12%
Royston & Cox, Anesthesia: the patient’s point of view. The Lancet 2003;362:1648-58
Patient Concerns Before Anesthesia
• Large, prospective, multicenter study • 19,576 Patients interviewed • Postoperatively and after one week • Convenience sampling of all patients types
0
0.05
0.1
0.15
0.2
0.25
Site 1
Site 2
Site 3
Site 4
Site 5
Site 6
Site 7
Tota
l
Awareness Incidence by Site
Aw
aren
ess
Inci
denc
e %
1 case per 1000
1 case per 500
Sebel et al Anesth Analg 2004; 99:833-9
Awareness in the United States

086-0092 1.01 6
Ghoneim MM, Awareness During Anesthesia. Anesthesiology 2000; 92:597-602
Selection of inadequate anesthetic
dose
Resistance to anesthetics
Mechanical malfunction or
misuse of anesthetic machine
INADEQUATE ANESTHETIC
EFFECT
CONSCIOUSNESS EXPLICIT RECALL
Why Does Awareness Occur?
• Definition, Role of NMB • Patient Experience & Sequelae • Incidence (0.1-0.2%) • “High risk” Scenarios • Current Monitoring Limitations • Brain monitoring devices • Anesthesia Challenge:
Balance psychological risk vs. physiologic risk • Recommendation: Develop Awareness Policy
JCAHO Sentinel Event Alert · Issue 32 ���Preventing, and managing the impact of, anesthesia awareness ��� http://www.jcaho.org/about+us/news+letters/sentinel+event+alert/sea_32.htm
Practice Advisory for Intraoperative Awareness and Brain Function Monitoring
A Report by the American Society of Anesthesiologists Task Force
on Intraoperative Awareness
Adopted by ASA House of Delegates, October 2005. http://www.asahq.org
• Not routinely indicated for general anesthesia patients • The decision to use a brain function monitor should be
made on a case-by-case basis by the individual practitioner for selected patients
Brain Function Monitoring in Anesthesia Practice

086-0092 1.01 7
Strongly Agree
Agree
Uncertain
Disagree
Strongly Disagree
“Brain function monitors are valuable and should be used to reduce the risk of intraoperative awareness for patients with conditions that may place them at risk for intraoperative awareness”.
http://www.asahq.org
ASA Practice Advisory Member Survey
Emerging Role of Brain Monitors
Avoiding Awareness Algorithm
1. Assess Individual Risk 2. Change Care Appropriate to Risk 3. Use Multiple Modalities
BIS Monitoring
Patients Elderly Obese Medically-compromised
Pediatric Labile Organ dysfunction
Procedures Outpatient procedures Cardiac surgery Neurosurgery Office procedures
Increased awareness risk cardiac, trauma, obstetric, expected hypotension, airway surgery, limited cardiac reserve
Techniques Volatile-based anesthesia IV-based anesthesia Combined regional-general Muscle relaxant use
MAC & Procedural Sedation Perioperative Adjuvant therapy
Beta-blockers, Alpha-2 agonists Closed loop anesthesia
Broad Clinical Applications

086-0092 1.01 8
BIS Sample Profile: GA
Strategy for intraoperative management based on integration of BIS index value with observed clinical response. Patient management should never be based on BIS monitoring information alone.
Physical signs
Clinical profile
BIS Index*
Management strategy
Desired range (45-60)
Hypertension Tachycardia Movement Autonomic responses
Light
High value
Low Value • Consider antihypertensive administration • Assess level of surgical stimulation • Consider ↓ hypnotic / ↑ analgesic dosing
• Assess level of surgical stimulation • Consider ↑ analgesic dosing • Consider antihypertensive administration
• Assess level of surgical stimulation • Confirm delivery of hypnotics/analgesics • Consider ↑ hypnotic / ↑ analgesic dosing • Consider antihypertensive administration
*Potential impact of artifact should be considered when interpreting BIS values.
Patient Management Table
Adapted from Stanski DR, Shafer DL. Anesthesia, ed. Miller RD. (Philadelphia: Elsevier Inc., 2004) p. 1257.
• Clinical judgment should always be used when interpreting BIS in conjunction with other available clinical signs.
• Reliance on the BIS alone for intraoperative anesthetic management is not recommended.
• As with any monitored parameter, artifacts and poor signal quality may lead to inappropriate BIS values.
• BIS values should be interpreted cautiously in patients: with known neurological disorders taking psychoactive medications in children below the age of one
Important Information about Using BIS Monitoring
086-0092 1.01 9
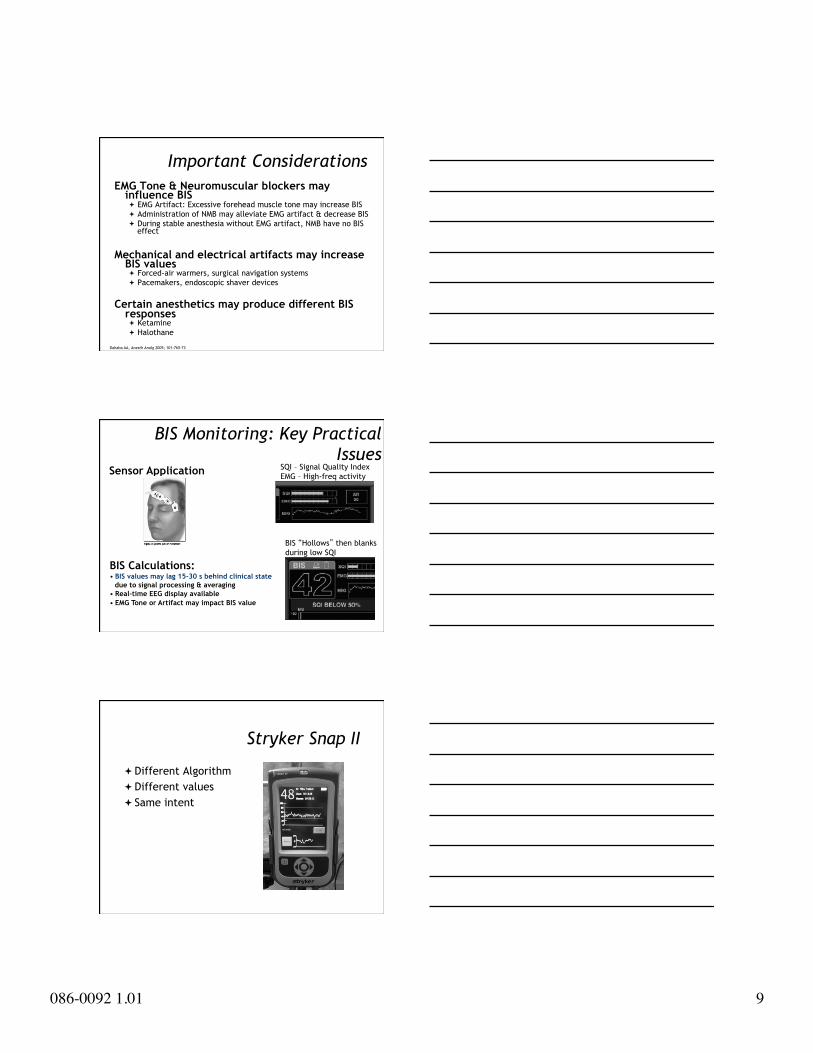
EMG Tone & Neuromuscular blockers may influence BIS EMG Artifact: Excessive forehead muscle tone may increase BIS Administration of NMB may alleviate EMG artifact & decrease BIS During stable anesthesia without EMG artifact, NMB have no BIS
effect
Mechanical and electrical artifacts may increase BIS values Forced-air warmers, surgical navigation systems Pacemakers, endoscopic shaver devices
Certain anesthetics may produce different BIS responses Ketamine Halothane
Dahaba AA, Anesth Analg 2005; 101:765-73
Important Considerations
SQI – Signal Quality Index EMG – High-freq activity
BIS “Hollows” then blanks during low SQI
BIS Monitoring: Key Practical Issues
BIS Calculations: • BIS values may lag 15-30 s behind clinical state
due to signal processing & averaging • Real-time EEG display available • EMG Tone or Artifact may impact BIS value
Sensor Application
Stryker Snap II
Different Algorithm Different values Same intent

086-0092 1.01 10
• EMG tone & neuromuscular blockers may influence BIS
• Mechanical and electrical artifacts may increase BIS values
• Certain serious clinical conditions have been associated with low BIS values intraoperatively • Hypovolemia, hypoglycemia, hypothermia, cerebral ischemia
• Certain anesthetics may produce different BIS responses
Dahaba AA, Anesth Analg 2005; 101:765-73
Important Considerations
• Examine for presence of artifacts (e.g., EMG, electrocautery or high frequency signals) • Ensure anesthetic delivery systems are operating properly • Ensure that the anesthetic dose is sufficient • Assess current level of surgical stimulation • Additional patient parameters (e.g., hemodynamics)
Responding to a Sudden BIS Increase
• Assess for new pharmacologic changes • Assess current level of surgical stimulation • Assess for other potential physiologic changes • Assess raw EEG for large delta waves (paradoxical delta)
Responding to a Sudden BIS Decrease
086-0092 1.01 11
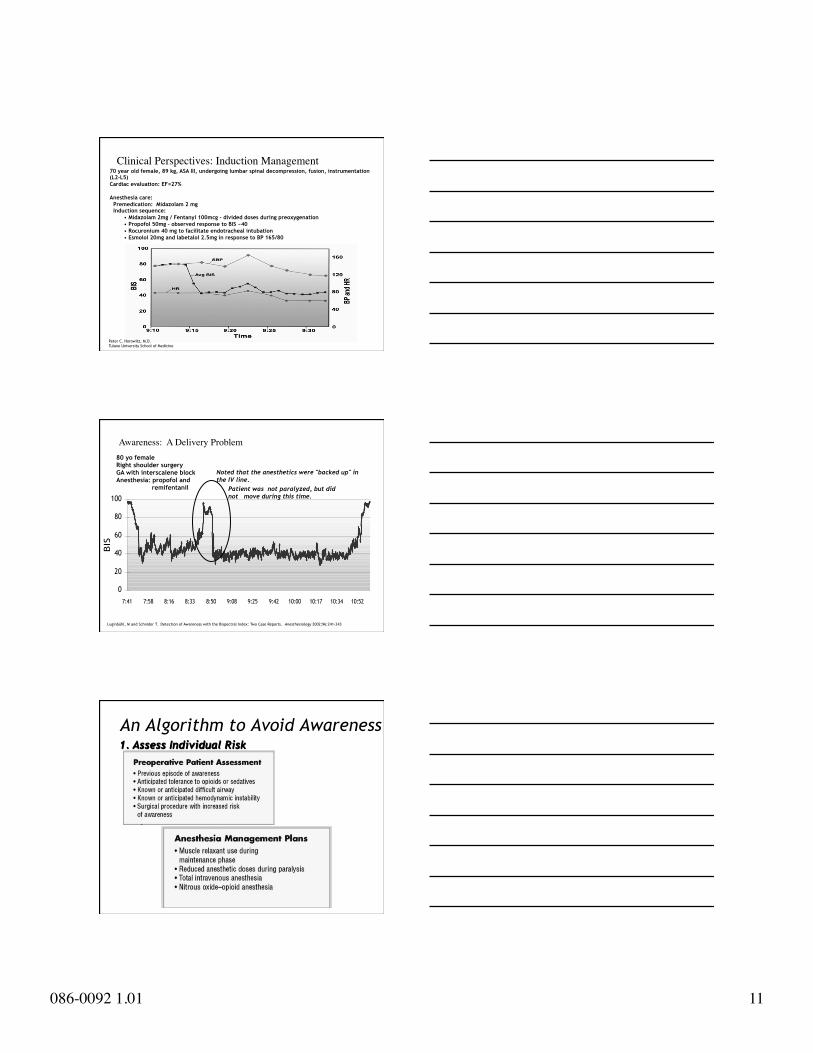
70 year old female, 89 kg, ASA III, undergoing lumbar spinal decompression, fusion, instrumentation (L2-L5) Cardiac evaluation: EF=27% Anesthesia care: Premedication: Midazolam 2 mg Induction sequence:
• Midazolam 2mg / Fentanyl 100mcg – divided doses during preoxygenation • Propofol 50mg – observed response to BIS ~40 • Rocuronium 40 mg to facilitate endotracheal intubation • Esmolol 20mg and labetalol 2.5mg in response to BP 165/80
Peter C. Horowitz, M.D. Tulane University School of Medicine
Clinical Perspectives: Induction Management
0
20
40
60
80
100
7:41 7:58 8:16 8:33 8:50 9:08 9:25 9:42 10:00 10:17 10:34 10:52
Time
BIS
Luginbühl, M and Schnider T. Detection of Awareness with the Bispectral Index: Two Case Reports. Anesthesiology 2002;96:241-243
Noted that the anesthetics were "backed up" in the IV line.
Awareness: A Delivery Problem
Patient was not paralyzed, but did not move during this time.
80 yo female Right shoulder surgery GA with interscalene block Anesthesia: propofol and
remifentanil
An Algorithm to Avoid Awareness 1. Assess Individual Risk
086-0092 1.01 12
An Algorithm to Avoid Awareness
2. Change Care Appropriate to Risk
An Algorithm to Avoid Awareness
3. Use Multiple Modalities
Summary • BIS measures the hypnotic effects of anesthetics and
sedatives on the brain.
• Substantial evidence demonstrates the impact of BIS-guided anesthesia care:
• Drug use • Speed and quality of recovery • Safety
• New ASA Practice Advisory provides guidance on awareness & brain function monitoring role.
• BIS monitoring can facilitate decision-making and patient management.

086-0092 1.01 13
Aver
age
Isof
lura
ne (
% in
spir
ed)
Clinical Utility in Elderly Patients
Standard Practice
BIS Titrated
27%
Faster Time to Orientation
Min
utes
Reduced Anesthetic Dosing
1%
0
.5%
1%
0.7%
Standard Practice
BIS Titrated
30%
Wong. Canadian Journal of Anesthesia 2002;49:13-18.
13.1 9.5
Organ Transplantation
Mayo Clinic, Jacksonville Florida Largest liver transplant program 50% of patients extubated in OR 30% bypass ICU to floor BIS very important part of anesthetic
plan
New Generation Medications
Precedex (dexmedetomidine) Significant decrease in narcotics Significant decrease in volatile agent Bradycardia, hypotension masks depth of
anesthesia

086-0092 1.01 14
BIS Monitoring Adoption Published Scientific Literature
• > 2,200 published studies
Broad clinical experience • Over 13 million patients monitored to date
Significant BIS adoption • Over 29,000 monitors & modules installed worldwide • BIS monitoring available in 68% of “best” US hospitals
B-Unaware Trial
First large independently funded evaluation of the technology
Reports that BIS provides no greater reduction of anesthesia awareness than a protocol guided by levels of end-tidal anesthetic gases
New England Journal of Medicine (2008;358:1097-1108
B-Unaware Trial
Critics say marketing and public demand, not science drove hospitals to adopt the monitor
Looked at BIS vs. End Tidal Anesthetic Gas ETAG - 0.7 - 1.3 MAC BIS 40-60 target range N= 950+ in both groups
086-0092 1.01 15
B-Unaware Trial
Two patients in each high risk group had awareness
Aspect defended their studies Rate of awareness was 80% lower with the
BIS than in expected in high risk patients Did not look at TIVA
Legal Aspects
Washington v. Washington What is standard of care for patients
How will this change your practice
Questions?
Thank you for your attention