board of directors – session in public meeting to be held ... public papers 30 november 2… ·...
TRANSCRIPT

Board of Directors – session in public Meeting to be held on Thursday 30 November 2017 from 13:30 to 15:40
at the Elisabeth Room, Endeavour House, Russell Road, Ipswich, IP1 2BX
AGENDA Time Item No
13:30 17.181 Chair’s welcome, apologies for absence and notification of any urgent business Apologies:
13:35 17.182 Standing Item: Declarations of Interest
13:40 17.183 To approve the minutes of the previous meeting in public, held on 26 October 2017
Attachment A
i. To approve the release of the minutes under the Freedom of Information Act
13:45 ii. To note the minutes of the AGM held on 10 October 2017
Attachment B
13:50 17.184 Matters arising from the meeting in public held on 26 October 2017
Attachment C
13:55 17.185 Chair’s Report (Gary Page) Attachment D
14:00 17.186 CEO’s Report (Julie Cave) Attachment E
17.187 Items for Approval
14:05 i. CQC Improvement Plan including Quality Programme Board ToR.(Julie Cave)
Attachment F
14:25 ii. Quarterly Patient Safety and Quality report (Dawn Collins)
Attachment G
14:35 iii. Finance Report M07 (Daryl Chapman)
Attachment H
14:40 iv. Business Performance Report (Daryl Chapman)
Attachment I
14:50 v. Finance Committee Chair’s Report for 21 November 2017 (Tim Newcomb)
Attachment J
14:55 vi. CoG/BoD joint working agreement (Robert Nesbitt)
Attachment K
Board of Directors - Public 30November2017 - Agenda
Version 1.0 Author: Kate Hope Department: Corporate
Page 1 of 2 Date produced: 2November2017 Retention period: 20 years

Time Item No
17.188 Items for Assurance
15:00 i. Review committee structure (Robert Nesbitt) Attachment L
15:05 ii. Freedom to Speak Up Annual Report (Liz Keay)
Attachment M
15:15 Committee Meeting Chairs’ Reports
iii. Quality Governance Chair’s Report for 14 November 2017 (Gary Page)
Attachment N
iv. Charitable Funds Committee Chair’s Report for 26 October 2017 (Tim Stevens)
Attachment O
v. Organisational Development and Workforce Committee Chair’s Report for 14 November 2017
Attachment P
15:20
17.189
Questions from the public in relation to the papers
15:30 17.190 Any other urgent business, previously notified to the Chair
15:35
17.191 Date, time and location of next meeting
The next meeting of the Board of Directors will be held in public on Thursday 25 January 2018 at the King’s Centre, 63-67 King Street, Norwich NR1 1PH.
15:40 17.192 Motion to exclude public and press from confidential part of the meeting on 25 January 2018
CLOSE
Board of Directors - Public 30November2017 - Agenda
Version 1.0 Author: Kate Hope Department: Corporate
Page 2 of 2 Date produced: 2November2017 Retention period: 20 years

Unconfirmed
Minutes of the Board of Directors – Public Session
Held on Thursday 26 October 2017 from 13.30 at Conference Room 1, King Centre, 63–67 Kings Street, Norwich NR1 1PH
Present: Julie Cave: CEO Daryl Chapman: Interim Director of Finance Dawn Collins: Interim Director of Nursing and Patient Safety Gary Page (Chair) Bohdan Solomka: Medical Director Debbie White: Director of Operations Ian Brookman: Non-Executive Director Adrian Matthews: Non-Executive Director Jill Robinson: Non-Executive Director Marion Saunders: Non-Executive Director Tim Stevens: Non-Executive Director
In attendance:
Robert Nesbitt: Company Secretary Kate Hope: Assistant Company Secretary Lisa Mungham-Gray: Head of Communications
There were 5 governors, 1 staff member and 10 members of the public present.
Meeting commenced at: 13.29
17.162 Chair’s welcome, apologies for absence and notification of any urgent business
The Chair (Gary Page) greeted the Board of Directors, governors, staff and the public. The Chair welcomed new board members Pete Devlin, Dawn Collins and Daryl Chapman.
The Chair informed those present that questions from the public gallery would be taken at the end of the agenda.
Date: 30 November 2017 A Item: 17.183i
BoD Public – 26 October 2017 Unconfirmed minutes
Version 1.0 Author: Kate Hope Department: Corporate
Page 1 of 12 Date produced 30 October 2017 Retention period: 20 years

There was one item of urgent business to discuss at 17.170.
17.163 Standing Item: Declarations of Interest
None
17.164 To approve the minutes of the previous meeting in public, held on 28 September 2017
The minutes were approved, by the Board as an accurate record of the meeting of 28 September 2017 subject to the following amendments:-
Item 17.146 – Matters Arising
Jill Robinson will check the date provided of May 2019 for mandatory training and appraisals and will confirm the position to Board members after the meeting.
Item 17.150vii – Organisational Development and Workforce (OD&W) Committee Chair’s Report
Paragraph 4 should be amended to ‘Sickness level rates are improving across NSFT which is positive and improvement in feedback from undergraduate medical students has been sustained’.
Action 17.164 The date provided for mandatory training and appraisals at 17.146 will be clarified following the meeting (Jill Robinson)
17.165 Matters arising from the meeting in public held on 28 September 2017
All matters were noted as complete save for action 17.149ic which is on the agenda for the Board meeting on 30 November 2017.
17.166 Chair’s Report
The report was taken as read and noted by the Board.
17.167 CEO’s Report
The report was taken as read and Julie Cave updated the Board as follows:-
1. The Care Quality Commission (CQC) Report was published on 13 October 2017 and a number of media statements were released to the press. Julie Cave took part in a live broadcast to staff where 750 staff engaged and fielded 143 questions for Julie Cave to answer. This was a helpful method of reaching staff and received positive
BoD Public – 26 October 2017 Unconfirmed minutes
Version 1.0 Author: Kate Hope Department: Corporate
Page 2 of 12 Date produced 30 October 2017 Retention period: 20 years

feedback. Future broadcasts have been planned on a monthly basis to keep staff fully briefed.
2. Julie Cave highlighted her visit to the Dragonfly Unit which was rated as outstanding by the CQC. She discussed best practice with the ward manager and lead consultant and how this process could be duplicated throughout NSFT. The Board noted the contents of the report.
17.168 Main Agenda Items
i. CQC inspection report response
Julie Cave confirmed that the Board’s focus is on addressing the concerns raised by the CQC in their Section 29a Regulatory letter and achieving significant improvement by the end of March 2018. The whole of NSFT is involved with this work and staff engagement is the key to achieving improvement. All requirements in the letter have been planned and key themes have been developed throughout the action plan, adopting a service line approach.
Robert Nesbitt explained how the approach would work and that the emphasis will be on accountability. A compliance audit is being developed and each member of the executive team will take the lead for different areas throughout the Trust.
Debbie White confirmed that she is taking the lead for the adult community service. A workshop took place for this area on Friday 20 October 2017. 60 people attended from both counties including staff from corporate services, human resources, IT and physical health colleagues. Staff left the meeting with a clear set of agreed actions. There will be a monthly meeting of the adult community forum to make sure that the agreed actions are taken forward. Workshops are also planned in Suffolk to review processes for service delivery and make them as effective as possible.
The Transformation Change team will meet weekly and will include the Heads of Estates, IT and HR to ensure momentum is kept going.
Accountability Review meetings will continue and as changes are made to the programme board work this should show in the feedback from the Accountability Review meetings.
Monthly meetings will take place with NHS Improvement to review the Trust’s progress and assurance meetings are planned to keep stakeholders, governors, Healthwatch members and unions updated and informed as to what steps they can take to support the Trust.
NHSI have appointed Philippa Slinger as NSFT Improvement Director and she has already met with some Board members and started to visit services in Norfolk and
BoD Public – 26 October 2017 Unconfirmed minutes
Version 1.0 Author: Kate Hope Department: Corporate
Page 3 of 12 Date produced 30 October 2017 Retention period: 20 years

Suffolk. In addition, a ‘buddy’ Trust will be appointed and the Board expect this to be announced by NHSI on 31 October 2017.
Changes already implemented include the deployment of defibrillators in community teams and sourcing additional administration staff to support Clinical Team Leaders and Ward Managers in having more time to do clinical work. In addition, investment will be made in pharmacy support for community services.
In relation to ligature points, 1004 had been identified for work. All in Suffolk have been resolved and Norfolk is 98% completed. NHSI Estates Team are visiting the Trust today to assist the NSFT Estates Team in completing this work.
The quality of the data NSFT produces and uses is being examined and reviewed. Abacus 2.0 is due to be launched for clinicians to use during week commencing 30 October 2017.
Gary Page confirmed that the Non-Executive Directors met on 23 October 2017 and agreed that they would align themselves to service lines to enable them to have oversight of the CQC action plan and give them an opportunity to gain assurance that things are happening on the front line as reported.
Assurance was requested on how the Board would ensure compliance continued throughout NSFT. This will be conducted through the peer review process so that the Executive Team can be confident that care delivery is what it should be. This will also be informed through methods such as the Friends and Family Test and the Staff Survey. NSFT is also signing up to accreditation with the Royal College of Nursing which will provide a useful framework to follow.
ii. Quality Improvement Plan Progress Report
The report was taken as read and Julie Cave confirmed that the current Cost Improvement Plans (CIPs) and Quality Improvement Plans (QIPs) would now change following the CQC report.
Clinical supervision and statutory and mandatory training were issues that were raised in the CQC report and will form part of the action plan.
Assurance was requested that the Trust-wide Central Bed Administration initiative would have a positive impact on out of area placements. Debbie White confirmed that the initiative would provide a Trust-wide, accurate view of bed availability on an hourly basis. Bohdan Solomka added that work is also taking place on the gatekeeping process with workshops taking place over the next month and this should have a positive impact in the out of area placements from November 2017.
The Board noted the report.
BoD Public – 26 October 2017 Unconfirmed minutes
Version 1.0 Author: Kate Hope Department: Corporate
Page 4 of 12 Date produced 30 October 2017 Retention period: 20 years

iii. Quality Account Report
Dawn Collins presented an update on progress for the Quality Account for 2017/18.
The focus is on three main areas, patient safety, patient experience and clinical effectiveness. Significant progress has been made on improving the recording of capacity and Section 17 leave.
Work continues on care planning to ensure that everyone has a care plan that is of good quality and co-produced with the service user. Extra clinical and administrative staff resource is being put in place to assist with the completion and monitoring of the care planning process. Daryl Chapman confirmed that throughout Norfolk and Suffolk there would be 40 full time administrative staff deployed to assist with this and clear plans are in place for how clinical staff are expected to use the additional time they will have as a result. There will be £1m of new expenditure invested in this initiative.
The report was noted by the Board.
17.169 Items for approval or assurance that have already been review at committee or executive team meeting
i. Finance Report M06
Daryl Chapman presented the report to the Board and highlighted the following points:-
1. Month 6 provides an opportunity to re-forecast the Trust’s position. This has improved by £200,000 taking the Trust to a £1.2m deficit by the end of the financial year.
2. The CIP forecast will be delivered in full.
3. The Trust’s cash position is £9.1m and ahead of forecast.
Assurance was requested that the additional expenditure required, following the recent CQC report, was contained in the plan for 2017/2018. It was confirmed that it was included and the Trust would be re-phasing its capital as only a third had been spent so far. In addition, NHSI provide additional funding for advice and support when an NHS Trust is placed in special measures. It was agreed that this additional expenditure should be included in the ‘Risks’ section of the Finance Report.
The Board noted the contents of the report.
ii Business Performance Report
Daryl Chapman confirmed that the CQC report and the associated actions will have a direct impact on many of the indicators included in the Business Performance Report such as supervision, appraisals and CPA compliance. The Executive Team are
BoD Public – 26 October 2017 Unconfirmed minutes
Version 1.0 Author: Kate Hope Department: Corporate
Page 5 of 12 Date produced 30 October 2017 Retention period: 20 years

reviewing which of the metrics should be the focus for the Board over the next six months.
It was noted that recovery rates within Wellbeing between May to August 2017 had not made any progress. Assurance was requested that the Executive Team were aware of the cause behind this lack of progress and that improvements were taking place which would achieve the 50% target. Debbie White confirmed that this was a changing pathway which was offering too much choice. In addition, there were a lot of counsellors involved in the commissioned model. Those interventions are not measured in relation to recovery. Changes will be made to this approach which will mean the trajectory will get worse before it gets better but Debbie White is confident that the 50% target will be met.
Concern was expressed at the low level of referrals to secure services. Debbie White confirmed that the Trust was in contact with NHS England on the issue of demand. This is a national issue and the teams involved are conducting a review of options available to them.
It was noted that for item 4, CPA patients having formal review within 12 months, no narrative was provided to explain why the localities had not achieved the target. It was confirmed that this was a data quality issue. The figures for September are much higher at 95%.
The Board noted the remainder of the Business Performance Report.
iii. Performance and Finance Committee Chair’s Report for 17 October 2017
Ian Brookman presented the report to the Board and highlighted that the Non-Executive Directors who attend the Performance and Finance Committee spend a great deal of time going through the information provided in the Business Performance Report each month.
A large portion of the meeting on 17 October 2017 was spent prioritising the metrics the Committee needed to focus on following the CQC report and the resources available for the resulting work.
Financial performance was rated as green.
An update was provided to the Committee on plans for ICT and the Committee was encouraged by the work that has been undertaken there to make sure the ICT infrastructure was resilient for the future.
The report was noted by the Board.
BoD Public – 26 October 2017 Unconfirmed minutes
Version 1.0 Author: Kate Hope Department: Corporate
Page 6 of 12 Date produced 30 October 2017 Retention period: 20 years

iv. Medical Education Report
Bohdan Solomka highlighted that medical undergraduate satisfaction has maintained the recent improvement. This appears to be a result of clearer organisation of the welcome procedure and structural changes in the way funding is delivered. Medical student numbers are expanding.
There is due to be a General Medical Council (GMC) education visit in November to inspect the training provision the Trust offers trainees and doctors. There are particular issues around inductions and workloads that are currently being addressed in West Suffolk. Bohdan Solomka will be spending the afternoon in West Suffolk on 27 October 2017 to monitor this.
v. Equality Objectives Report
Robert Nesbitt took the report as read.
The Equality and Diversity Group (EDG) have agreed to provide support for localities by working with managers via local coordinators for Equality Leads to put together smart action plans to get teams back on track to completing their assessments. This was approved by the Executive Team on 25 October 2017.
A query regarding safe domain/patient care/care planning was raised and specifically, where these issues are examined in detail. Robert Nesbitt confirmed that these issues were reported to the EDG who in turn reports to the Quality Governance Committee.
In relation to objective 3, workplace disability equality scheme, there are areas of the estate at Hellesdon which are not accessible to all. A question was raised whether the Trust has annual accessibility check of all premises. Robert Nesbitt will check with the Estates Team whether checks are performed annually and will report back to the Board. He explained that where possible, the Trust had utilised rooms on the ground floor, near disabled parking spaces for accessible meeting rooms.
It was noted that indicator 8 on page 17 shows an increasing number of BME staff experiencing discrimination at work. Robert Nesbitt confirmed that better training is being rolled out for leaders and managers in emotional intelligence. Where issues are raised they are reviewed and examined thoroughly to see what changes can be made to lead to positive outcomes.
Action 17.169 Check the frequency of accessibility inspections of Trust premises and report back to the Board (Robert Nesbitt)
BoD Public – 26 October 2017 Unconfirmed minutes
Version 1.0 Author: Kate Hope Department: Corporate
Page 7 of 12 Date produced 30 October 2017 Retention period: 20 years

vi. Complaints Annual Report
Dawn Collins presented the annual Complaints Report to the Board.
The report provides a summary of complaints received over the last year, examines the process around the complaints procedure and identifies learning opportunities to improve the process.
Julie Cave confirmed that communication is a recurring theme and she has met with the Communications Team to examine the best way to apply the learning we have from previous complaints and how best to communicate this throughout the organisation. This will also be picked up as part of the CQC action plan work.
A discussion took place on the benchmarking figures provided on page 2 and whether this was actually helpful. It was requested that this part of the report was re-examined and presented in a more useful format.
There is a lack of consistency in the Trust’s approach to complaints throughout the organisation. The process should be the same throughout the Trust and this was identified by the CQC in their recent inspection report.
It would be useful and more beneficial for staff if the report gave details of the compliments at the beginning. This is the approach used by Northumberland, Tyne and Wear NHS Foundation Trust.
It was noted that the Patient Advice and Liaison Service (PALs) should be a source of information on patient experiences and does not seem to be included in the report. Dawn Collins confirmed that she would liaise with PALs to access the information they have available.
A number of complaints have been raised against individual members of staff and there appears to be a disconnect with the number of complaints about staff behaviours and what is feeding through the disciplinary system. Assurance was requested on how aligned the figures were with the disciplinary system and how effective the system was. Bohdan Solomka confirmed that in relation to doctors, complaints are usually dealt with locally and any associated learning following a complaint is utilised in the appraisal process to demonstrate learning.
It was agreed that assurance was needed that every effort was made to meet with and discuss complaints with complainants. The Board would like to see evidence that this is taking place throughout the organisation.
The report was noted by the Board.
Action 17.169vi a. PALs to be contacted to access information they have on service user
BoD Public – 26 October 2017 Unconfirmed minutes
Version 1.0 Author: Kate Hope Department: Corporate
Page 8 of 12 Date produced 30 October 2017 Retention period: 20 years

experiences of the Trust (Dawn Collins) b. Evidence to be circulated to the Board that efforts have been made in
all cases to meet and discuss complaints with complainants (Dawn Collins)
Committee Chair’s Reports
vii. Service User and Carer Trust Partnership Chair’s Report for 3 October 2017
Gary Page confirmed that he had met with the Council of Governors yesterday who were concerned that the implementation of locality hubs and the Involvement Strategy had made it more difficult for the voice of the service user and carers to be heard and their views are not being taken up by the Trust. It was agreed that this must be addressed and it was agreed that Gary Page and Dawn Collins would liaise with the governors on this issue and report back to the Service User and Carer Trust Partnership on their findings.
The Board noted the contents of the report.
viii. Quality Governance Committee Chair’s Report for 10 October 2017
The report was taken as read and noted by the Board.
The Terms of Reference had been revised following feedback from staff on the duplication of some of the issues that are covered in Performance Review meetings and Quality Governance meetings. As a result, the Quality Governance Committee was to be a smaller assurance meeting. However, following the CQC inspection it was felt that reducing the number of meetings was not appropriate so this element of the proposed changes was suspended and would be reviewed following the next CQC inspection.
It was noted that the report stated that the Quality Governance Committee reported to the Audit and Risk Committed. This is incorrect and will be amended.
It was requested that patient safety was referred to specifically in the objectives.
The report was noted and subject to the changes requested above, the Terms of Reference were approved. These will be amended and re-circulated to the Board.
Action 17.169viii QGC Terms of Reference to be amended as agreed and re-circulated to the Board (Gary Page)
BoD Public – 26 October 2017 Unconfirmed minutes
Version 1.0 Author: Kate Hope Department: Corporate
Page 9 of 12 Date produced 30 October 2017 Retention period: 20 years

17.170 Any other urgent business, previously notified to the Chair
There had been one notification of urgent business.
NSFT will be agreeing to join the initiative led by Norman Lamb promoting the Zero Suicide ambition. There has been some debate amongst clinicians about this but this initiative is one that the Trust should support as an ambition. The Board approved the endorsement of the initiative.
17.171 Questions from the public in relation to the papers
The meeting took questions from members of the public and the following questions were put to the Board:-
A Suffolk public governor asked for the CQC presentation to be amended to remove the acronyms and uploaded onto the NSFT website. It was agreed that this would be done.
A Suffolk public governor noted that the Performance and Finance Committee Report rated the ICT update provided as green. Her experience is that staff continue to have problems with ICT with ESR not recording correctly, lack of roll out of mobile phones and continuing problems with Lorenzo.
Ian Brookman clarified that the update was a strategic update provided to the committee on the infrastructure for the data centre rather than specific software used.
Bohdan Solomka added that a Chief Clinical Information Officer has been appointed for NSFT to provide a bridge between digital technology and clinicians to help benefit patient experiences. The idea being that no technology is implemented without demonstrating benefits for patient care. Other factors introduced are a Lorenzo users group and a clinical content assurance group to help form Lorenzo into something that will be more useful going forward.
A Norfolk public governor highlighted that there were many concerning issues arising in Central Norfolk such as levels of staff sickness, complaints and targets not being met.
Debbie White confirmed that this was due to lack of resource and lack of funding. The staff in that area do a fantastic job but the area is the least well resourced for the population it serves. Norwich City has a high level of morbidity. Additional funding has therefore been requested from Norwich CCGs to fund an enhanced community team in Norwich to try and combat these issues.
A member of the public echoed the concerns already highlighted about Central Norfolk. Next year Universal Credit will be rolled out in Norfolk. Is the Trust prepared for the effect this new system may have on service users and carers?
Debbie White confirmed that staff at the Trust were prepared as best we can and had knowledge on how to obtain food parcels from food banks. The changes have the potential
BoD Public – 26 October 2017 Unconfirmed minutes
Version 1.0 Author: Kate Hope Department: Corporate
Page 10 of 12 Date produced 30 October 2017 Retention period: 20 years

to have a challenging impact on Trust referrals as we saw before with the introduction of the bedroom tax.
A member of the public asked if the Trust had any update on the Ashcroft Unit closing?
Debbie White confirmed no further information had been forthcoming but she would investigate and provide an update.
A member of the public asked about the Zero Suicide initiative and who was involved with it.
Gary Page confirmed that Joe Rafferty, CEO of Mersey Care was leading on the initiative and NSFT is in discussions with him on the approach which, is not a target but an aspiration the Trust should be aiming for. A launch will take place in November 2017 involving service users, carers and families.
A public governor for Norfolk highlighted the thread of lack of resources and staffing which negatively impacts service delivery. Is there any possibility of using the additional funds from NHSI to recruit new staff?
Julie Cave confirmed that NHSI are very specific that the additional funding is to provide support whilst in special measures rather than for operational needs. In terms of recruitment other methods of recruitment have been rolled out and some areas are using social media to recruit staff. To combat the difficulties experienced in recruiting to Churchill Ward the Trust has been able to offer accommodation for staff at the Queen Elizabeth Hospital and this has been popular and the Trust has the best staffing on Churchill Ward than in any other inpatient area in the Trust.
A Norfolk public governor confirmed he was encouraged by the contents of the CQC presentation and asked what the presentation would mean in practice for the Executive Team.
Julie Cave confirmed that there would be an Executive Team lead and Non-Executive lead attached to all service lines. Their job would be to ensure that the action plan for that service line was being delivered in full and any obstacles to delivery were removed. The Non-Executive lead would provide a more independent oversight to the process. All information then feeds back to the Programme Board which is chaired by the CEO. By way of example, Debbie White is working with locality leads in Adult Community to ensure that the Section 29a Regulatory letter imperatives are carried out. This is done via weekly meetings, workshops and clinical engagement. They are also working to Royal College accreditation. Debbie White can visit the community teams to check progress against the CQC action plan and a monthly adult community forum starts next week to bring all the actions together. Bohan Solomka will be checking her progress to ensure actions are reached. The Non-Executive Directors will then visit services as part of a triangulation exercise so they can be personally assured that work is being done and actions achieved. Adrian Matthews (NED) is sitting on the weekly Programme Board meetings to provide
BoD Public – 26 October 2017 Unconfirmed minutes
Version 1.0 Author: Kate Hope Department: Corporate
Page 11 of 12 Date produced 30 October 2017 Retention period: 20 years

feedback from the NEDs. Overarching the whole process is a central access database where actions and progress can be monitored at all times.
A member of the Campaign to Save Mental Health Services in Norfolk and Suffolk made reference to the consequences of a radical re-design which took place at NSFT back in 2013/2014. The group warned about losing staff and beds as a result. His view is that members of the Board should stand down. Another member of the public confirmed she supported his views.
Gary Page confirmed that the Board’s entire focus was on addressing the issues that CQC have raised in their report.
A member of the public who was a previous employee confirmed that she can see from the information provided in the CQC report that a great deal of work is needed following the CQC inspection. Radical changes need to take place to ensure change takes place.
Julie Cave confirmed that there is an element of supervision for the Board of Directors as it reports to regulators. Front line staff will be involved in the process as the Board will not always have the answers at the table. Therefore, staff views and input are fundamental to the changes that need to be made.
Action 17.171 a. CQC presentation to be amended to remove acronyms and uploaded to
the NSFT website (Julie Cave)
b. Update on the closure of the Ashcroft Unit to be circulated to the Board (Debbie White)
17.172 Date, time and location of next meeting
The next meeting of the Board of Directors will be held in public on Thursday 30 November 2017 at the Elisabeth Room, Endeavour House, Russell Road, Ipswich, IP1 2BX.
The meeting closed at 15.26
Chair: ……...…..…………………………
Date: ……....…………………………….
BoD Public – 26 October 2017 Unconfirmed minutes
Version 1.0 Author: Kate Hope Department: Corporate
Page 12 of 12 Date produced 30 October 2017 Retention period: 20 years

Unconfirmed
Minutes of the Annual General Members’ Meeting held on Tuesday 10 October 2017
The King’s Centre, 63-75 King Street, Norwich NR1 1PH Present: Gary Page: Chair Tim Newcomb: Non-Executive Director Brian Parrott: Non-Executive Director Julie Cave: CEO Leigh Howlett: Director of Strategy and Performance Dr Jane Sayer, Director of Nursing, Governance and Performance Daryl Chapman: Director of Finance Debbie White: Director of Operations – Norfolk and Waveney Pete Devlin: Director of Operations – Suffolk Robert Nesbitt: Company Secretary Dr Bohdan Solomka: Medical Director Tim Newcomb: Non-Executive Director Ian Brookman: Non-Executive Director Jill Robinson: Non-Executive Director Marion Saunders: Non-Executive Director (SID)
Guenever Pachent: Public Governor – Suffolk Sheila Preston: Norfolk Public Governor Anne Humphrys: Carer Governor Nigel Boldero: Norfolk Public Governor Hilary Hanbury: Norfolk Public Governor Howard Tidman: Staff Governor Malcolm Blowers: Service User Governor, Suffolk Stephen Fletcher: Norfolk Public Governor Catherine Wells: Public Governor, Norfolk (Lead Governor) Martin Wright: Suffolk Public Governor Ron French: Norfolk Public Governor Marcus Hayward: Staff Governor
In attendance Kate Hope: Assistant Company Secretary (minutes)
There were 17 members of the public, staff and press were present.
Meeting commenced at: 14:30
A17.01 Chair’s welcome, notification of any urgent business and apologies for absence Gary Page welcomed everyone to the meeting and thanked members of the public and staff for their continued interest in the Trust’s work. The purpose of the AGM is to formally present the NSFT accounts and annual report to the public.
Date: 30 November 2017 B Item: 17.183ii
AGM – 10Oct 2017 – Minutes Unconfirmed
Version 0.1 Author: Kate Hope Department: Corporate
Page 1 of 6 Date produced: 11 Oct2017
Retention period: 20 years

Gary Page extended his thanks to Michael Scott for his hard work and dedication to NSFT over the last few years and wished him well with his retirement. Julie Cave is in attendance as Chief Executive Officer (CEO). The Board of Directors have agreed that Julie Cave should take on the CEO role with immediate effect pending the recruitment of a substantive CEO, to allow the Board to focus on the challenges ahead. This proposal will be put to the Council of Governors, for approval, at their meeting on 12 October 2017. Apologies were received from: Tim Stevens, Non-Executive Director, Paul Gaffney: Suffolk Service User Governor, Sian Coker: UEA Partner Governor, Andrew Good: Suffolk Public Governor, Kathleen Ben Rabha: Suffolk Public Governor: Jane Millar: Suffolk Public Governor, Paddy Fielder: Suffolk Public Governor, Heather Rugg: UOS Partner Governor, Dr Richard Gorrod: Norfolk Service User Governor.
A17.02 To approve the minutes of the Norfolk & Suffolk NHS Foundation Trust Annual General Meeting held on 20 October 2017
The minutes were approved as accurate.
i. To approve the release of the minutes in accordance with the Freedom of Information Act
The minutes were approved for release in accordance with the Freedom of Information Act.
A17.03 To address any Matters Arising from the minutes of the previous meeting, not covered by the Agenda There were no matters arising.
A17.04 To receive the 2016-2017 Annual Report and Annual Accounts Julie Cave presented the 2016-2017 Annual Report and Accounts starting with a review of 2016- 2017. Following the Care Quality Commission (CQC) inspection in July 2016 immediate work took place on actions to address issues raised by the CQC. This work continues. NSFT commissioned an independent review of unexpected deaths in the Trust which was carried out by Verita. The Trust continues to work on the learning opportunities arising from that review. One of the key points from the report is that rates of suicide at NSFT are no higher than in the rest of the UK. However, learning continues through the work of the Mortality Review Group and the implementation of our Suicide Strategy which Dr Jane Sayer leads on. As we implement the service user and carer and involvement strategy, a number of improvements have been rolled out over the last year. One of these improvements is the Green Light Toolkit, dedicated to improving mental health services to meet the needs of people with learning disabilities and autism.
AGM – 10Oct 2017 – Minutes Unconfirmed
Version 0.1 Author: Kate Hope Department: Corporate
Page 2 of 6 Date produced: 11 Oct2017
Retention period: 20 years

NSFT is one of only 3 Trusts in the Country with this dedicated resource available to drive this work forward. The National Staff Survey was launched this week. There is further work to be done on improving staff satisfaction but significant improvements have been made in terms of staff wellbeing and this work will continue. A new financial regime had been implemented where financial control totals were issued to all Trusts. NSFT was issued with a control total for £4.8m deficit. This meant achieving a 50% reduction on the deficit the previous year. A £3.3m deficit was achieved with the assistance of additional funds from the Government as part of the Sustainability and Transformation Plan (STP) funding. The Trust’s cash position for the year improved and stands at £9.8m and this is sufficient to maintain operations. Therefore Trust has a Financial Sustainability Rating of 3. Capital expenditure for the year was £5.4m. Julie Cave outlined the sources of NSFTs income and outlined where the funds were allocated. Challenges to NSFT finances include the upkeep of increasingly old buildings and estates. To offset this, the Trust’s estates have, where possible, sold to raise funds. Placing service users out of Trust when there are no available beds remains a challenge to resources. This year the CCGs have provided support and have funded these placements. The level of Agency staff spend continues to be high and is the case across the UK. Despite this challenge, NSFT stayed within the agency staff spending cap set in the last financial year. The Board of Directors has fought hard for parity of esteem for mental health funding over the last year and will continue to do so when negotiating with CCGs over the coming year. Capital has been invested in projects such as the Dragonfly Unit which provides a light and airy unit for children and young people. New facilities are being provided for the Trusts Secure Services totalling an investment of £1.1m. In addition routine maintenance in the form of IT investment and ward upgrades has continued to keep services working efficiently. As part of the STP and Five Year Forward View the Trust has secured £4m to invest in a new ward for West Norfolk. NSFT is also proud to be providing new services such as the mother and baby unit in Hellesdon and new perinatal community services in Norfolk and Suffolk. The motion to approve the Annual Report and Accounts, already presented to Parliament, was proposed by Stephen Fletcher (Norfolk Public Governor) and seconded by Ron French.
The motion was approved unanimously.
A17.05 Constitution Changes 2016/2017
AGM – 10Oct 2017 – Minutes Unconfirmed
Version 0.1 Author: Kate Hope Department: Corporate
Page 3 of 6 Date produced: 11 Oct2017
Retention period: 20 years

Robert Nesbitt outlined the proposed changes to the NSFT Constitution as follows:-
• Consolidating partner governor seats.
• The closing date for new members during an election period to be the same date as nominations open.
• Specifying the number of meetings that can be missed by governors without permission before triggering the exclusion process from the Council of Governors.
• Miscellaneous references to ‘Board’ of Governors to be amended to ‘Council’ of Governors.
The motion to approve the amendments to the Constitution was proposed by Anne Humphrys (Suffolk Carer Governor) and seconded by Hilary Hanbury (Norfolk Public Governor). The motion was approved unanimously.
A17.06 Chair’s reflection and summary
Gary Page confirmed that following the latest inspection, the CQC report would be published on Friday 13 October 2017. Until that time the Board were under embargo not to release any details of the contents of the report.
There is still a great deal of work for the Board of Directors to do to ensure improvement in services throughout Norfolk and Suffolk whilst continuing to operate in a challenging environment. The demand for mental health services is increasing across the Country with a rise in the complexity of cases against a backdrop of continuing pressure on finances. Over the last few years the Trust has been required to work to reduce the deficit to return to surplus in the next financial year. It is challenging to deal with such an increase in demand and provide the services required whilst being expected to save money. There has been a historic underfunding of mental health services in Norfolk and Suffolk coupled with a shortage of staff levels. The accounts for 2016/2017 demonstrate that there has been some new investment in services and today, on 10 October 2017 it has been announced that the pay cap has been lifted for the NHS. This is welcome news and it is the Board’s hope that this will translate into further funding that can be passed on to staff to give them the recognition they deserve.
Work continues to alleviate the pressure on bed numbers. The Board believes it is not acceptable for any service user to be placed out of area. Therefore 7 new step down beds are to be introduced in Norfolk. Further work needs to be done in conjunction with both Norfolk and Suffolk County Councils on delayed transfers of care. There are currently 20 patients in beds at NSFT in Norfolk who are able to be safely discharged but there is no suitable accommodation to discharge them into. Therefore we have 23 service users staying in the commissioned service at Mundesley Hospital to keep service users in Norfolk and close by their families. In the meantime regular checks are made to ensure that service users staying in the commissioned service are well cared for and safe. It was to try and resolve these issues that Debbie White and Gary
AGM – 10Oct 2017 – Minutes Unconfirmed
Version 0.1 Author: Kate Hope Department: Corporate
Page 4 of 6 Date produced: 11 Oct2017
Retention period: 20 years

Page met with the CEO of Norfolk County Council and the Director of Adult Social Care at Suffolk County Council last week.
Finally, Gary Page paid tribute to the amazing staff at NSFT who carry out their work in very difficult circumstances and do and incredible job. The Board would like to put on record, their appreciation for everything that they do.
A17.07 Questions from the floor to Directors and Governors
Are there any other sites at NSFT that could be sold?
Julie Cave confirmed that a site review was being undertaken and it is planned to dispose of the upper plateau site at Hellesdon in Norwich over the next few years.
Has NSFT consulted with service users and staff on ensuring that steps are taken to deliver a multi-agency approach to service delivery?
Dr Jane Sayer stated that the planned Crisis Café service in Norwich would be a service that had mulita agency involvement. In addition the Trust has weekly meetings about bed management which involves social care to work together to try and resolve bed management issues at NSFT.
The service at Ashcroft, providing services for women with severe mental health issues, is due to be closed due to lack of funding. This will have a negative impact on services. Is NSFT involved in trying to save the unit?
Debbie White confirmed that one of the locality managers in Norfolk was working closely with colleagues at Norfolk County Council and with Julian Support who currently provide the services at Ashcroft. Nothing has been agreed yet but NSFT is involved in the dialogue.
The unexpected death rate has risen. What is the Trust doing to try to address this? In particular, for those service users, dying unexpectedly of physical ailments?
Dr Jane Sayer replied that this is a priority concern for the Board at NSFT. A Mortality Review Group has been set up which examines the figures in detail to assess whether there are any emerging themes. The Trust continues to work with Mazars on the reporting of mortality and they have compared NSFT with other mental health Trusts around the Country to see where issues are emerging and where the Trust is an outlier. One element that has been identified is the frequency of cardiac events. The Trust is therefore working alongside other agencies to ensure service users can access the services that they need at all times to try and prevent any further deaths. In addition, Dr Bohdan Solomka confirmed that from 1 April 2018 the Trust will be completely smoke free and will be promoting vaping instead of allowing service users and staff to smoke on Trust properties.
Audits are taking place on how well the Trust is giving advice on health promotion and wherever possible staff are signposting other services and helping service users with information on diet and exercise. This will go some way to reduce mortality rates in the future.
AGM – 10Oct 2017 – Minutes Unconfirmed
Version 0.1 Author: Kate Hope Department: Corporate
Page 5 of 6 Date produced: 11 Oct2017
Retention period: 20 years

Work continues between NSFT and local GPs. Education sessions have been set up in Norfolk and Suffolk involving 150 GPs and Trust consultants to share concerns and help build better relationships within the system.
How does the Board see NSFT’s role in Sustainability and Transformation Plans (STPs)?
Julie Cave confirmed that work on STP planning process was vital and the Trust was fully involved in mental health work-streams in both Norfolk and Suffolk resulting in services such as the Crisis Café, step down beds, psychiatric liaison and intervention in psychosis.
What work is the Trust doing to help those who develop mental ill health as the result of a physical illness?
Dr Bohdan Solomka said that in such circumstances a holistic approach should be taken with a quality handover between services with a handover to a community mental health team where appropriate with regular contact with a patient’s GP.
What work is being done to improve crisis services for children and young people in Norfolk and Suffolk?
Pete Devlin confirmed that through the STP planning process in Suffolk, NSFT has an allocation of funds, specifically for children. Current services on offer are very adult focused and the plan is to resolve that through the use of the additional income, working in partnership with children, young people, parent networks and CCGs to ensure that children and young people have the crisis service and support needed.
Debbie White provided details of the new Norfolk and Waveney Crisis Team for children and young people in Norfolk. There were no further questions or comments.
A17.07 Closing remarks Gary Page thanked attendees for coming and thanked NSFT Governors for the work that they have done for the Trust over the course of the year.
Meeting closed at: 15:11
Chair: ……...…..…………………………
Date: ……....…………………………….
AGM – 10Oct 2017 – Minutes Unconfirmed
Version 0.1 Author: Kate Hope Department: Corporate
Page 6 of 6 Date produced: 11 Oct2017
Retention period: 20 years

Matters arising from Board of Directors’ meeting - public 26 October 2017
Action 17.164 – Minutes of the meeting held on 28 September 2017 The date provided for mandatory training and appraisals at 17.146 will be clarified following the meeting (Jill Robinson)
Completed. Clarification circulated via email from Kate Hope on 30 October 2017
Action 17.169v - Equality Objectives Report Check the frequency of accessibility inspections of Trust premises and report back to the Board (Robert Nesbitt)
Completed. Update circulated via email 1 November 2017
Action 17.169vi - Complaints Annual Report
a. PALs to be contacted to access information they have on service user experiences of the Trust (Dawn Collins)
b. Evidence to be circulated to the Board that efforts have
been made in all cases to meet and discuss complaints with complainants (Dawn Collins)
Completed. This is covered in Section 8 of the Patient Safety and Quality Report. Completed. Circulated via email on 23 November 2017
Action 17.169viii – Quality Governance Chair’s Report for 10 October 2017 QGC Terms of Reference to be amended as agreed and re-circulated to the Board (Gary Page)
ToR amended and due to be circulated shortly
Action 17.171 - Questions from the public in relation to the papers a. CQC presentation to be amended to remove acronyms
and uploaded to the NSFT website (Julie Cave) b. Update on the closure of the Ashcroft Unit to be circulated
to the Board (Debbie White)
Completed.
Completed. Update circulated
on 10 November 2017
Date: 30 November 2017 C Item: 17.184
Board of Directors Meeting - public 30Nov2017 Matters Arising from 26Oct2017 BoD
Version 1.0 Author: Kate Hope Department: Trust Secretariat
Page 1 of 1 Date produced: 31Oct2017 Retention period: 20 years

Report To: Board of Directors – Public
Meeting Date: 30 November 2017
Title of Report: Chair’s Report
Action Sought: For Information
Estimated time: 5 minutes
Author: Gary Page: NSFT Chair Executive Summary: This report highlights some themes following the meetings that have taken place over the last month. I also include at the end of report a list of the key meetings that I have had.
1.0 Key observation from the month:
1.1 One of the real highlights for me this month was the opening of the Trusts dedicated purpose designed Recovery College building in Bury. The enthusiasm of the staff, peer tutors, service users and carers was magical. It was also great to meet up again with the tutors who led the first Recovery College course I attended. The work on Recovery is one of the many great achievements of the Trust in recent years and I was reminded again when talking to service users who it has transformed the lives of so many people.
2.0 Key Meetings
2.1 Staff and Services: • I had a monthly teleconference with the Non-Executive Directors (NEDs). • I opened the new dedicated Recovery College building in Bury St Edmunds. • Our new Improvement Director Philippa Slinger has started work within the Trust and
I have had two meetings with her in the last month. • I conducted interim appraisals for several of the NEDs. • I chaired a phone call involving the NEDs, Julie Cave and our Improvement Director
Philippa Slinger to sign off the CQC action plan. • I met with Mark Gammage who is supporting the Trust on OD and HR matters. • I attended the Nominations Committee. • I chaired the monthly Quality Governance Committee. • I chaired the Men’s Mental Health Conference held at the Kings Centre on
23rd November 2017. • I participated in a development day for the Board. • I chaired a Hospital Managers Hearing. • I had a one to one with Marion Saunders, Senior Independent Director • I met with Marcus Hayward, Head of Participation and Recovery
Date: 30 November 2017 D Item: 17.185
Public Board of Directors, 30 November 2017, Chair’s Report
Version 1.0
Author: Gary Page Department: Trust Mgmt
Page 1 of 2 Date produced: 15th Nov 2017 Retention period: 20 years

• I met with Debbie White and Gill Morshead who are leading on our improvement work
for the Adult Community Teams in my capacity as NED lead for this service Line.
2.2 Service Users and Carers and Governors: • I attended an informal Council of Governors meeting to discuss the CQC Report and
subsequently chaired a Council of Governors Meeting • A Governor public event was held in Ipswich on the subject of Talking Therapies and I
co- chaired the event • I had a one to one with Catherine Wells, Lead Governor. • I met with a service user to discuss the volunteering work they do for the Trust. • I attended the Governors Planning & Performance subgroup to present on the CQC
Action Plan . • Myself and our Youth Participation Lead met with our new Youth Governors.
2.3 External Organisations: • NHSI held a Special Measures Conference in London and myself and Julie Cave
attended. • Along with Julie Cave I met with the Norfolk and Suffolk MPs to update them on the
work of the Trust and plans following the CQC report. • Robert Rowland-Smith is working with the Trust on Board development and I had a
teleconference with him on this subject to prepare for the Board Development Day. • I had a telephone call with Jim Mackey, Chief executive of NHSI • I met with Councillor Michael Chenery Chair of the Norfolk Health Overview and
Scrutiny Committee. • I spoke to the Chief Executive of Merseycare regarding the national Zero Suicide
initiative. • I met with the Chief Executive of The Grow Organisation. • I met with Sheila Childerhouse, the STP Chair for Suffolk and North Essex. • The Suffolk and North Essex STP held an event for Chairs, NEDs and governors
which I attended and was part of a Chairs Panel. • Myself and the Executive members of the Board attended a Progress Review Meeting
with NHSI and subsequently attended the Overview and Assurance Group meeting with NHSI and our key stakeholders to present our CQC Action Plan.
• Myself and Julie Cave had a telephone call with the Chair and Chief executive of our buddy Trust, the East London NHS Foundation Trust and subsequently spent some time with their Chief Executive and Chair at their Head Office in Tower Hamlets
• In order to start the recruitment process for our Executive Board level vacancies I chaired a panel to select a recruitment agency to work with us.
3.0 Recommendations
3.1 The Board is asked to note the report. Gary Page Chair
Public Board of Directors, 30 November 2017, Chair’s Report
Version 1.0
Author: Gary Page Department: Trust Mgmt
Page 2 of 2 Date produced: 15th Nov 2017 Retention period: 20 years

Report To: Board of Directors Meeting Date: 30 November 2017 Title of Report: Chief Executive’s Update Action Sought: For Assurance Estimated time: 10 minutes Author: Julie Cave, CEO Director: Julie Cave, CEO Executive Summary: The purpose of this report is to provide the Trust Board with the Chief Executive Officer’s update on significant developments and key issues over the past month. 1.0 Norfolk and Waveney STP Chair visit: 1.1 Patricia Hewitt, the chair of the Norfolk and Waveney STP, and Antek Lejk, the
lead Executive for the STP, visited the Trust on 3rd November to discuss mental health and the issues facing the Trust and to consider how the STP can support the Trust over the next few months.
1.2 Ms Hewitt and Mr Lejk met with a number of members of staff, including the
Recovery College team, Wellbeing teams and visited the wards on the Hellesdon Hospital site.
1.3 Following the visit Ms Hewitt said she was very impressed by ‘the dedication,
enthusiasm and compassion’ of everyone she met. 2.0 Care Quality Commission: 2.1 The summary report of actions was submitted to the CQC on 14th November. The
report was presented at the Oversight and Assurance meeting on 15th November where stakeholders from a number of organisations were represented. This includes the CQC, NHS Improvement, NHS England, Suffolk CCGs, Norfolk and Waveney CCGs, the County Council, Health Overview and Scrutiny Committee, Healthwatch, representatives of Service Users and Carers, Staffside, the GMC and Trust Governors.
2.2 Monthly calls have been established with the Head of Inspection to discuss
progress against the plan and to discuss any issues or concerns.
Date: 30 November 2017 E Item: 17.186
Board of Directors 30 November 2017, CEO’s Update
Version: 0.1 Author: Carol Carter Department: Corporate
Page 1 of 3 Date produced: 161117 Retention period: 20 years

3.0 New appointments: 3.1 You will be aware that interim appointments have been made namely Daryl
Chapman, Director of Finance and Dawn Collins, Director of Nursing. 3.2 In addition to these roles we have appointed Dearden HR to provide external
advice to the Board of Directors on workforce issues. Mark Gammage of Dearden HR will be with us over the next few months.
4.0 Communications: 4.1 The second live broadcast to staff took place on 16th November. This takes the
form of a brief introduction and then is open to questions from staff. We plan to do this on a monthly basis.
4.2 The Senior Management Engagement Forum took place on 14th November with
discussions on the key themes within our CQC improvement plan: leadership, staff engagement and culture.
5.0 East London NHS Foundation Trust (ELFT) 5.1 ELFT has been appointed as our ‘buddy trust’ as part of the special measures
package of support. Jonathan Warren (Director of Nursing) and Richard Evans (Medical Director) have spent some time with us, meeting the teams and assessing the ward environments.
5.2 We have agreed that ELFT will work with us on the following areas:
• Nursing structures and practice • Governance arrangements • Service user and carer involvement • Clinical leadership • Quality Improvement • Estates strategy and processes, including clinical ownership
6.0 CEO visits: 6.1 In the past month the following visits have taken place to:
• The Coastal IDT team at Walker Close in Ipswich where they explained about the service they provide, what they are proud of, some of the frustrations and where we can make things easier for staff.
• The Crisis Team at Hellesdon Hospital in Norwich where I listened to their plans for their services and discussed how we can improve the environment in which they work.
• The team at Wedgewood House, Bury St Edmunds, to tour the wards and talk to staff about their concerns and achievements.
Board of Directors 30 November 2017, CEO’s Update
Version: 0.1 Author: Carol Carter Department: Corporate
Page 2 of 3 Date produced: 161117 Retention period: 20 years

7.0 Environment Scan August/September 2017
Environmental Scan November 2017
External
National Local System • NHSE putting pressure on
government re funding ahead of Budget (22 Nov)
• Plan for MH Trusts to face regulatory action over out of area placements
• Carter Review suggests mental and community health services could save £181m through combining corporate services.
• Norfolk and Suffolk STPs told to increase GP WTEs by 174 by 2020
• Carnall Farrar appointed by Suffolk STP to develop an Accountable Care System bid.
Internal
Trust-wide Locality/Service-specific
• Action plans underway across the
Trust to meet CQC requirements.
• Senior operational managers seconded to lead CQC action plan service lines across the Trust
• CGL (Care Grow Live) have been awarded the Norfolk Alcohol and Drug Behaviour Change Service contract, which will replace NRP from April.
Julie Cave Chief Executive
Board of Directors 30 November 2017, CEO’s Update
Version: 0.1 Author: Carol Carter Department: Corporate
Page 3 of 3 Date produced: 161117 Retention period: 20 years

Report To: Board of Directors [Public] Meeting Date: 30th November 2017 Title of Report: Programme Management Office Progress Report Action Sought: For Assurance Estimated time: 15 mins Author: Stuart Clifton, Head of PMO Director: Julie Cave Executive Summary: As part of the ongoing CQC improvement plan initiative, the focus for the Programme Management Office has been on supporting the immediate actions as well as the longer term improvements required. A system of governance has been established to track and deliver the progress against the plan. This has included the set-up of the Quality Performance Board. The plans have been developed on a service line basis to match the approach taken by the CQC. The improvement plan is being monitored by the Quality Programme Board on a weekly basis, with the agenda planned so that each service line is reviewed every two weeks. CQC Service Line Reports “must and should dos” have been cross-referenced into individual actions. Peer Reviews have been established and staff trained. These check that the actions are taking place and outcomes being delivered. The master action plan is available to Service Line Leads, and the Executive Team via the Trust’s SharePoint system. Any projects that do not support the CQC action plan or are not essential projects will be paused or put in a slow stream until April 2018 to release capacity to support the CQC must-dos action plan. One of the challenges has been the scale of change activity being planned. There are 25 generic CQC “must / should dos” which translate to approximately 400 internal actions.
Overview of Progress:
1. Work began on the CQC actions as soon as the draft report was received in early September 2017. In parallel with this the focus has been on creating a robust governance and organisational structure including “agile” decision-making, the ability to challenge in a supportive way, and clarity on roles and responsibilities.
Date: 30 November 2017 F Item: 17.187i
Board of Directors PMO Programme Progress Report
Version 1.1
Author: Stuart Clifton Department: PMO
Page 1 of 2 Date produced: 23/11//2017 Retention period: 20 years

2. CQC Service Line reports have been cross-referenced to specific actions within the
internal plans. Where no CQC observations were noted for a specific team, the Service Line Lead has been challenged to ensure compliance across the Trust.
3. The detailed plans are owned by the Service Line Lead and disaggregated into local area plans. As part of the lean governance arrangements, the executive oversight comes from the weekly Quality Programme Board [QPB] where issues and exception reporting are discussed and resolved.
4. The internal actions plans have identified the required outcome and measures and there is further work to refine these. Milestones have been assigned to keep momentum and help with interdependency mapping. The action plan is available to each Service Line via the organisations SharePoint; this is a live data base with regular updates. During the next reporting period, modifications are planned to enhance the functionality, reporting and search / filtering capabilities of the data base.
5. The Head of Governance has scheduled 70+ Peer Reviews to take place prior to March 2018 re-inspection. The Peer Review Team will visit sites as if in the role of a CQC inspector and look for ways in which the evidence could be found lacking. The findings are detailed within an individual report and summarised as part of a generic Heatmap which is reviewed at QPB. The detailed report is given to local management for resolution with outcomes and assurance being given to QPB via Service Line leads.
6. Any projects that are not mission critical will be paused or put in a slow stream until April 2018 to release capacity to support the CQC must-dos action plan. The role of the Programme Manger is to:
a. work with the named responsible Service Lead to understand the action and how this relates to the CQC recommendation
b. agree reporting milestones c. agree measurement and outcome d. manage synergies across the service lines and to ensure consistency in
approach e. report progress against milestones.
7. One of the challenges has been the scale of change activity being planned. A key
focus for the coming weeks is to prioritise the key critical actions and to learn from good practices.
8. There are 25 generic CQC “must / should dos” which translate to approx 400 internal actions split across 11 service lines (including Trustwide enablers). These have been distilled into an abridged document “Summary of the CQC Improvement Plan” which will be available monthly to evidence overall progress.
Recommendations: The Board is asked to note this report.
Stuart Clifton Head of Programme Management Office.
Board of Directors PMO Programme Progress Report
Version 1.1
Author: Stuart Clifton Department: PMO
Page 2 of 2 Date produced: 23/11//2017 Retention period: 20 years

Summary of the CQC Improvement Plan
Version 1.10
21 Nov 2017
Board assessment that action is on track to deliver outcome Key: Delivered On track to deliver Some issues – narrative disclosure Not on track to deliver
1

Norfolk and Suffolk NHS Foundation Trust – our improvement plan and our progress
What are we doing?
• The Trust was rated as ‘Inadequate’ and placed into ‘special measures’ following an inspection by the Chief Inspector of Hospitals (CQC) in July 2017.
• The Chief Inspector made 25 recommendations in total, 21 of which the Trust must undertake and 4 of which the Trust should undertake. All 25 recommendations are included in our CQC Improvement Plan. The key themes of these recommendations are summarised below:
• Improving safety • Improving staffing • Improving service access / capacity • Improving data / performance (Quality) • Improving compliance
• The plan is iterative and will include a governance review to be commissioned by NHS Improvement which will add to the improvement learning.
• The Trust Board has approved the CQC Improvement Plan which has been designed to deliver the immediate actions required as well as the longer term improvements needed. Support and engagement of our staff and our stakeholders will be fundamental to making the sustainable changes that are required for the benefit of everyone who uses our services.
• A robust system of governance has been established to track and deliver the progress against the plan. The plans have been developed on a service line basis to match the approach taken by the CQC. Service Line Leads have been appointed to implement the plans and Operational Leads have been allocated to ensure actions are implemented quickly and effectively and to unblock any obstacles that might prevent completion of the actions. There is Executive and Non-Executive oversight against all service lines plans and further independent review will be provided through a clinically-led Peer Review and Audit process. Performance will be monitored through our Quality Programme Board and reported to the Quality Governance Committee and to the Trust Board. Further oversight will be provided to our stakeholders through a monthly Oversight and Assurance meeting.
• The improvement plan will be monitored by the Quality Programme Board on a weekly basis, with each service line being reviewed on a fortnightly basis. This document shows our plan for making these improvements and will demonstrate our progression against the plan.
• The CQC Improvement Plan was signed off by the Board on 13 November 2017. The plan ensures that the format and content align to the CQC reporting domains and that there is further clarity of the intended outcomes and key performance indicators across the programme of improvement. This will assist in the process to ensure that improvement actions align with the improvement recommendations.
2

Who is responsible?
• Our actions to address the recommendations have been agreed by the Trust Board.
• Our Chief Executive, Julie Cave, is ultimately responsible for implementing actions in this document. Other executive directors are responsible for ensuring the plan is implemented as they provide the executive leadership for quality, patient safety and workforce: Debbie White (Director of Ops – Norfolk & Waveney), Pete Devlin (Director of Ops – Suffolk), Dawn Collins (Director of Nursing), Bohdan Solomka (Medical Director), Daryl Chapman (Director of Finance). Mark Gammage is the external advisor to the Board on HR/OD issues. Non-executive directors are responsible for testing and challenging the executive on the robustness of the plan, triangulating board reports with experience of front line staff and service users & carers.
• Philippa Slinger has been appointed as our Improvement Director and she will support our progress by challenging our approach to ensure we deliver the most effective service to our patients. The Improvement Director acts on behalf of NHS Improvement and works with the Trust to ensure delivery of the improvements and to oversee the implementation of the action plan.
• Ultimately, our success in implementing the recommendations of the CQC Improvement Plan will be assessed by the Chief Inspector of Hospitals, who will re-inspect our Trust in 2018.
• If you have any questions about the work we are doing you may contact our Head of Governance, Sue Barrett, [email protected].
The format of this plan…
• This summary document begins with the longer term changes that we need to make. We recognise that sustainable improvement requires cultural changes which will take longer than our immediate action plans. We need to build a culture that empowers colleagues, that instills ownership and accountability for quality and which ensures that we deliver our promises. We have called these long term themes our systemic issues and they focus on leadership and medical and staff engagement.
• The pages that follow the systemic issues cover our required actions. These are our immediate responses to the Chief Inspector’s 25 ‘must dos’ and ‘should dos’. Although we have shown these on a calendar going up to April 2018 this does not mean that our work will stop in April. There will be more work to do on some actions and where we have made changes we will continue to check that the improvements have been sustained.
• This is a summary document and behind each of the actions there are detailed service line plans that are not shown here. These include milestones to measure progress and the names of individuals who are accountable for delivering the improvements.
• We have rated the actions as “green” at this stage in our planning. This is because we believe that the plan is realistic and is on track. We recognise that as time goes on, some actions may not go to plan and if this happens they will then change to ‘amber’ which means that there are reasons to be concerned that the action will not deliver the outcome or timescale or ‘red’ if we now believe that the action is not on track to deliver. There are some actions where important aspects are not under our control and so we have used ‘amber’ to show that we have less certainty.
• The “amber” and “red” ratings make sure that we focus our attention on the important actions to get them back on track.
3

How we will communicate our progress to you?
• We will provide a progress report every month, which will be monitored by the Quality Programme Board and reviewed by the Trust Board.
• The progress report will be published on the Trust website, and subsequent longer term actions may be included as part of a continuous process of improvement. Each month we will let all staff, governors and stakeholders know our progress.
• We will write to all FT members via our newsletters letting them know more about the inspection outcome and describing the improvement plan, where members can access the action plan and how and when we will update it.
• We will present updates on progress at our scheduled Council of Governor meetings which are held in public.
• We will provide staff with an update on progress at our monthly broadcasts and communications to staff.
• We will provide updates to our stakeholders through the oversight and assurance meetings which will be held on a monthly basis.
Chair / Chief Executive Approval (on behalf of the Board):
Chair Name: Gary Page Signature: Date:
Chief Executive Name: Julie Cave Signature: Date:
4

OUR IMPROVEMENT PLAN - SYSTEMIC ISSUES
Leadership
Leadership is a core theme to our improvement. It shapes our culture, promotes engagement and creates an environment open to learning and quality improvement. Whilst some work has started on building emotional intelligence we need to ensure our staff are equipped with the right skills to lead their teams in delivering excellent care to our service users. To do this we need to engage everyone in the organisation so that we have compassionate, inclusive and effective leaders at all levels. To do this we must:
• Agree what good leadership looks like at different levels to include knowledge, skills, attitudes and behaviours. • Ensure that our staff receive appropriate skills development, including feedback and support. • Ensure a system is in place to recognize talent and to attract, identify and develop people with good leadership potential.
We will work with East London NHS Foundation Trust to develop some aspects of this core theme, learning from their approach to leadership. Another important feature of our work will be as part of the Norfolk and Waveney and the Suffolk and North East Essex Sustainability and Transformation Plans. This work will focus on the long term sustainability of the health systems across our counties.
Summary of key actions Oct Nov Dec Jan Feb Mar Apr &
beyond Strategic actions Trust Board to review Executive roles and ensure appropriate structure is in place Trust Board to develop a revised Organisational Development Strategy and agree an implementation plan
Trust Board agree and adopt improvement methodology to drive forward a high quality, high performing organisation based on continuous improvement
Executive Team to adopt the ‘Developing People – Improving Care’ Framework Trust Board to participate in and develop the ‘Leadership for Improvement’ programme
Executive Team to agree and develop leadership programmes for all levels CEO to introduce a ‘coaching for performance’ scheme for managers Operational actions
Executive Team to communicate clear plans for addressing CQC issues and progress
Visibility of the Board (Executives and Non-Executive Directors (NEDs)) – to include the CEO monthly broadcast, weekly/monthly planned visits to each area, partnered
5

up with corporate heads HR lead to introduce a team briefing process Chair to lead on substantive appointments to Board vacancies (including recruitment process)
CEO to ensure regular Senior Leadership Group (SLG) meetings HR lead to formalise 360 appraisal process for Senior Leadership Team HR lead to introduce mentoring network Executive Team to renew approach to Executive oversight and performance management of appraisal, supervision and mandatory training compliance (see separate plan NSFT15)
Evidence/Assurance Regular and consistent messaging of plans for addressing CQC issues through a variety of mechanisms (Julie’s Monday Message, Team Brief, SLGs) Plan in place for regular Board visits; visits undertaken; feedback from visits shared with Board colleagues Team briefing process implemented Executive positions appointed substantively Regular SLG meetings held Leading in Care Programme delivered Managers held to account for performance at every level Early Intervention (EI) programme for staff cohorts at Bands 4, 5 and 6 completed Staff survey engagement scores for 2018
6

OUR IMPROVEMENT PLAN - SYSTEMIC ISSUES (continued)
Medical Engagement
The link between doctors and management is an important one and one on which we need to make significant improvement. Medical leaders have a key role in driving quality improvement which is fundamental to our future success. We aim to have a culture whereby managers and clinicians work in partnership to deliver high quality care. To do this we have to be clear on our vision and values, working together to achieve a common objective with an absolute commitment to quality, safety, improvement and engagement. This is not a short term goal: it needs to be embedded and sustainable. We aim to be a Trust with high levels of medical engagement which possesses:
• Understanding, trust and respect between doctors and managers • Clear expectations, professional behaviour and firm decision-making • Clarity of roles and responsibilities and empowerment • A culture focused on quality improvement and safety
We will be supported by East London NHS Foundation Trust in this work.
Summary of key actions Oct Nov Dec Jan Feb Mar Apr &
beyond Strategic actions HR lead to establish a values and competency based selection process for all consultants
Medical director to develop a leadership programme for consultants Medical director and CEO to assess medical engagement through the Medical Engagement Scale, resulting in plans to address the identified issues.
CEO to establish a programme of learning from other high-performing organisations world-wide
Medical director to establish key roles for medical leadership Operational actions
Medical director to organise GMC Regional Liaison service workshops CEO to meet individual consultants and consultant groups on a regular basis HR lead to formalise 360 appraisal process for consultants HR lead to introduce mentoring network Medical Director to develop the clinical strategy implementation with clinical leads
7

OUR IMPROVEMENT PLAN - SYSTEMIC ISSUES (continued)
Staff Engagement
Staff engagement is critical to our approach to improvement. There is evidence to show that engaged staff are more likely to show empathy and compassion. Trusts with engaged staff have higher patient satisfaction levels, with more patients reporting that they are treated with dignity and respect. Staff are more enthusiastic about their work and collaborate more effectively, ultimately delivering better performance. Staff are more engaged if they have responsibility for their work and influence over their working environment. Just as importantly staff must feel able to raise concerns and to identify opportunities for improvement – and for these to be considered fairly. Our aim is to be inclusive, to promote collaboration, involve staff in decisions, to encourage and coach staff and support staff in addressing organisational challenges. We want to be a learning organisation where staff participate at all levels and feel able to deliver staff-led improvements. The focus must be on developing frontline staff and creating a culture that promotes innovation.
Summary of key actions Oct Nov Dec Jan Feb Mar Apr & beyond
Strategic actions To build on the development of our values in developing our approach to improvement through engagement (e.g. Listening into Action)
Executive Team to analyse the results from the Staff Survey for 2017 and establish actions to address the issues.
CEO to promote a more-accessible organisation to deliver a better relationship with the local population and the media
Operational actions
CEO-led communications in a variety of channels: live broadcasts, blogs, social media, newsletters, magazines
Executive/NED walk arounds for visibility and to operate with purpose, with NEDs feedback to impact on changes and opportunities for improvement. All feedback to be included in the programme governance.
CEO to continue ‘You said we did’ Executives to establish drop in sessions for staff
8

OUR IMPROVEMENT PLAN - SYSTEMIC ISSUES (continued)
Culture
Whilst we have worked to develop our vision and values and start to transform the organisational culture we have more to do to ensure that: • Organisational culture helps to maintain high levels of staff engagement and underpins safe, high quality patient care. • It is critically important that leaders are seen to act authentically and that organisations live by their values they promote. • Developing effective procedures to address behaviours that are consistent with our values is a priority. That means addressing negative
behaviours of aggression, bullying, harassment and rudeness. • Staff are more engaged when they feel valued by the organisational leaders and operate within a supportive environment.
We need to build on and progress with the work on our values to ensure that we adopt professional behaviours associated with high-performing organisations in that we take responsibility for our actions, we are accountable and hold people to account for delivery.
Summary of key actions Oct Nov Dec Jan Feb Mar Apr & beyond
Strategic actions The Board to consider its approach to learning with a focus on learning from mistakes and what has worked well.
The Board to emphasise and re-state a clear direction and priorities based on empowerment/ deliverability/ accountability.
Operational actions
HR lead to ensure our values are embedded in our recruitment and appraisal processes
Executive team to agree on its approach to performance management and the consequences of inappropriate behaviours and performance.
The Board of Directors to publicly celebrate the success of its staff in delivering results, including against the CQC plan
9

Our CQC Improvement Plan
to address S29A issues:
Required Actions
10

OUR CQC IMPROVEMENT PLAN – REQUIRED ACTIONS
NSFT20 Exec lead: Julie Cave
The Trust must ensure that they fully address all areas of previous breach of regulation.
PLAN ON TRACK: RAG
RATING
Summary of actions Oct Nov Dec Jan Feb Mar Apr & beyond
The Head of Governance confirms completion of review of 2014/2016/2017 reviews to ensure all must dos/should dos are covered
The Board of Directors agrees the governance structure to monitor the plan
The executive team agree leads at all levels The Quality Programme Board (QPB) agrees and implements an escalation process
The Trust’s compliance functions report to the QPB that processes are embedded and sustainable.
OUTCOME: Regulators are assured that all breaches have been addressed.
Evidence/Assurance Governance structure in place Progress is made with the plans and evidence is provided Processes are embedded and sustainable Peer Reviews
11

NSFT02 Exec lead:
Julie Cave
The Trust must ensure that action is taken to remove identified ligature anchor points and to mitigate risks where there are poor lines of sight.
PLAN ON TRACK: RAG
RATING
Summary of actions Oct Nov Dec Jan Feb Mar Apr &
beyond The Head of Estates ensures that site specific risk assessments are published on the intranet. Matrons confirm that risk assessments are accessible to ward staff
Community toilet area risk assessments complete Head of Estates sign off that original work plan complete Matrons confirm that they have reviewed risk assessments with ward managers including all relational management arrangements. Ward managers confirm that they have reviewed risk assessments with ward staff including all relational management arrangements. Matrons escalate any issues immediately to locality managers for intervention
Head of Estates to complete further potential work plan Board agrees additional work and funding Head of Estates to confirm that the work plan is in place and has been signed off by ward managers
Every month, matrons to report outcomes of audits to locality governance groups. Locality manager confirms that there are SMART actions in place for all issues identified. Improvements are evidenced and reported via Locality Governance Group minutes. Both environmental and relational aspects are covered
Matron audits confirm that operational policies are complied with in all areas and relational approaches are working
Head of Estates signs off that work is complete OUTCOME: The board is assured that patient safety is protected as ligatures have been removed or the board has agreed that there are robust local arrangements which all local staff work to.
12

Evidence/Assurance Monthly matron audits Peer Review process Exec and Non-Exec visits Photographs of completed work Further reviews of existing areas to check risk assessments are comprehensive and complete
13

NSFT17 Exec leads:
Debbie White /Pete Devlin
The Trust must ensure that people receive the right care at the right time by placing them in suitable placements that meet their needs and give them access to 24 hour crisis services.
PLAN ON TRACK: RAG
RATING
Summary of actions Oct Nov Dec Jan Feb Mar Apr & beyond
Locality Managers develop capacity business cases where appropriate for discussion with Commissioners
The Director of Operations for Norfolk &Waveney to confirm that if Out of Area (OOA) placements are required then appropriate monitoring is in place to return the patients to the Trust asap (to include Length of Stay)
The executive team approve acceptable staffing levels for Section 136 suite (Health Based Place of Safety) has been agreed or alternative actions taken
Directors of Operations agree position with Commissioners on crisis services for dementia
Directors of Operations agree performance and waiting time management plans for all areas that are not delivering waiting time standards
Head of Estates confirms disabled access assessments have been completed
Directors of Operations agree Delayed Transfer of Care (DToC) plans with local stakeholders
Directors of Operations N&W confirms that the Crisis Hub has been established
OUTCOME: Patient safety is protected by access to appropriate services that meet their needs.
Evidence/Assurance Service user survey Reduction in complaints S136 compliance monitored through audits/Peer Review Waiting time performance improvement
14

Reduced OOA patients Reduced DToC
NSFT18 Exec leads: Debbie White /Pete Devlin
The Trust must minimise disruption to patients during their episode of care and ensure that discharge arrangements are fully effective.
PLAN ON TRACK: RAG
RATING
Summary of actions Oct Nov Dec Jan Feb Mar Apr & beyond
Directors of Operations to confirm that a protocol has been established to minimise risk of out of hours transfers.
The Patient Safety & Complaints Lead reviews readmissions to identify learning and address review outcomes
The executive team monitors progress against the OOA Trust/Commissioners action plan
Directors of Operations confirm implementation of ‘Red-to-Green’ process and ‘Purposeful admission’. This to include all aspects of effective discharge.
OUTCOME: Patient admission, transfer and discharge arrangements promote recovery.
Evidence/Assurance Monitor performance on number of readmissions within 28 days Monitor the number of OOA placements (and bed days) Monitor DToC Monitor LOS for acute wards Peer Review
15

NSFT07 Exec leads:
Pete Devlin/ Debbie White
The Trust must ensure there are enough personal alarms for staff and that patients have a means to summon assistance when required.
PLAN ON TRACK: RAG
RATING
Summary of actions Oct Nov Dec Jan Feb Mar Apr & beyond
Locality managers sign off confirmation that all staff have access to personal alarms
The Associate Director of Operations (Norfolk & Waveney) / Chair of Acute Services Forum confirms that procedures on what to do in the event of an alarm have been reviewed (including Lone Worker Policy). Ward managers and community team managers confirm that amended procedures have been communicated to staff
Ward managers and community team managers to confirm that a programme of practice drills is in place.
Ward managers and community team managers confirm that any malfunctioning alarm systems have been identified by local testing. Ward managers and community team managers confirm that they have tested their local arrangements and that staff know what to do if alarm sounds. Head of Estates confirms that any faulty alarm systems have been repaired
Peer reviews confirm that alarm systems are effective. OUTCOME: Staff and patients can summon effective help if they need it urgently.
Evidence/Assurance Sign off by team leaders that sufficient personal alarms are in place and their areas are functioning satisfactorily Peer Reviews Compliance checks Matrons and team leaders monthly checks and reporting Environmental risk assessments
16

NSFT01 Exec
lead: Dr Bohdan Solomka
The Trust must ensure that all services have access to a defibrillator and that staff are aware of arrangements for life support in the event of an emergency. The Trust must ensure all clinic rooms are equipped with emergency medication for use on site and in the community. The Trust must ensure that alternative procedures are in place for staff to follow in the event of a medical emergency.
PLAN ON TRACK: RAG
RATING
Summary of actions Oct Nov Dec Jan Feb Mar Apr &
beyond Physical health lead to review requirements for access to emergency equipment and provide a case for change.
Executive decision to purchase defibrillator packs for all community bases (oxygen & adrenalin available in packs).
Physical health lead signs off that that packs are in place for areas requiring defibrillators. Physical health lead signs off that the protocol is in place and that training has been provided to all areas where defibrillators are not appropriate.
Senior Maintenance Services Manager to sign off that defibrillator calibration and maintenance schedule is in place.
OUTCOME: Arrangements are in place to minimise risk to people experiencing a medical emergency in that all Trust services either have trained staff with access to a defibrillator or have alternative procedures in place
Evidence/Assurance Protocol approved and published on intranet Training sign off by all relevant individuals Compliance checks that equipment is in place Peer review on operational safety Matrons audits
17

NSFT06 Exec
lead: Dawn Collins
The Trust must fully implement guidance in relation to restrictive practices and reduce the number of Restrictive Interventions (RI).
PLAN ON TRACK: RAG
RATING
Summary of actions Oct Nov Dec Jan Feb Mar Apr & beyond
Trust lead on RIs completes review of Trust practice versus national guidance to identify weaknesses
Trust lead on RIs identifies best practice organisations and arranges visits/discussions
Executive team agree revised policy, including performance metrics
Executive team agrees preventative measures plan including training. Head of Training and Prevention and Management of Aggression (PMA) lead implements plan
Monthly data in the form of a balanced scorecard will be provided to each ward to enable the ward manager to take action to address any shortcomings. The data will be overseen by the patient safety and complaints lead and reported to Quality Governance Committee (QGC).
OUTCOME: Patient safety and recovery is promoted by minimal use of restrictive interventions.
Evidence/Assurance Performance improvement is seen (data shows a reduction in the number of restrictive practices). Multi-Disciplinary Team (MDT) review of older people restraints, to include Root Cause Analysis (RCA) and actions to address weaknesses. All patients who have a history of aggression or who have been secluded have a Positive Behavioural Support Plan.
18

NSFT04 Exec
lead: Julie Cave
The Trust must review the continued use of bed bays in the acute wards and work with commissioners to provide single room accommodation.
PLAN ON TRACK: RAG
RATING
Summary of actions Oct Nov Dec Jan Feb Mar Apr & beyond
Business case to address single room issues at Hellesdon Hospital (Glaven and Waveney wards) agreed by Finance Committee
Executive team review options for and patient care implications of removing bays.
If bays continue in short term, Matrons to review use of management of bed bays with ward managers to maximise privacy and dignity until works completed. Peer reviews confirm effectiveness of measures.
Head of Estates signs off that work is complete Business case for West Norfolk beds agreed in July 2017 and work is underway. Head of Estates signs off works as complete December 2018
OUTCOME: Patient privacy and dignity is protected by the provision of single room accommodation.
Evidence/Assurance New facilities are open and in use No shared rooms available in Trust
19

NSFT03 Exec
leads: Pete Devlin / Debbie White
The Trust must ensure that all mixed sex accommodation meets Department of Health and Mental Health Act code of practice guidance and promotes safety and dignity.
PLAN ON TRACK: RAG
RATING
Summary of actions Oct Nov Dec Jan Feb Mar Apr & beyond
Head of Governance to confirm that all ward areas have been assessed against Department of Health (DoH) guidelines
Locality managers to confirm that all inpatient areas have zoned sleeping areas so that male/female sleeping areas are clearly boundaried
Head of Governance to confirm that the Single Sex Trust Procedure has been reviewed and updated
Performance data is reviewed weekly by Directors of Ops and areas of non-compliance escalated to Executives
Locality Managers sign off that poor performance has been addressed with the local team and plan implemented.
OUTCOME: Patient safety and dignity are protected because ward areas are gender boundaried.
Evidence/Assurance CCG Quality Leads to review areas with Matrons Peer Review Matrons audits Compliance team checks
20

NSFT05 Exec
leads: Pete Devlin / Debbie White
The Trust must ensure that seclusion facilities are safe and appropriate and that seclusion and restraint are managed within the safeguards of national guidance and the Mental Health Act Code of Practice.
PLAN ON TRACK: RAG
RATING
Summary of actions Oct Nov Dec Jan Feb Mar Apr & beyond
Work for seclusion rooms is complete Compliance checks against standards complete Matrons review areas every month and sign off confirmation of operational compliance, or, if there are issues, make recommendations to the Clinical Team Leader (CTL) and Locality Manager to address these. Confirmation that compliance issues have been addressed are signed off by the Locality Manager via the Senior Operational Team (SOT) minutes and re-checked the following month by the Matron. Compliance includes physical environment, recording and care planning which promotes wellbeing of patients.
OUTCOME: Patients’ safety and dignity is protected because seclusion and restraint are only used within national standards.
Evidence/Assurance Peer Review Compliance Team checks Matrons audits Compliance check against the standards was completed in week commencing 23rd Oct. Operational issues identified e.g.cleaning. Compliance checks to be undertaken at random times.
21

NSFT16 Exec lead:
Robert Nesbitt The Trust must ensure that patients are only restricted within appropriate legal frameworks.
PLAN ON TRACK: RAG
RATING
Summary of actions Oct Nov Dec Jan Feb Mar Apr & beyond
The Company Secretary identifies those teams that are below training performance standards and locality managers implement a targeted 4-week turnaround process
Ward managers report progress on a weekly basis to Operational Teams
Where training performance is <50% teams to be escalated to QPB
The Company Secretary has strengthened the section reminder system (date that an authority is due to expire).
The Company Secretary ensures revised systems are in place to provide clarity on medication chart recording and consent form reporting.
OUTCOME: Patients’ human rights are protected.
Evidence/Assurance Peer Reviews Improved CQC Mental Health Act (MHA) assessments Compliance assurance results show documentation is correct Improved performance Random audits to check compliance with documentation and timescales
22

NSFT10 Exec
lead: Dr Bohdan Solomka
The Trust must ensure that all risk assessments, crisis plans and care plans are in place, updated consistently in line with multidisciplinary reviews and incidents and reflect the full and meaningful involvement of patients.
PLAN ON TRACK: RAG
RATING
Summary of actions Oct Nov Dec Jan Feb Mar Apr & beyond
The Medical Director signs off the co-produced work of the CPA Task & Finish Group to include risk assessments as well as care plans and trajectories for monitoring.
Additional admin resource is in place (NSFT08) to support improvement in recording.
Locality managers sign off to confirm that their staff are clear on Trust expectations and implement training plans accordingly, including DICES training, Lorenzo training
BSMs provide monthly or more frequent reporting to team leaders and managers and escalation of implementation issues through to execs for resolution.
OUTCOME: There is effective care planning including risk management that meaningfully involves service users and carers.
Evidence/Assurance Random audit of care plans Peer Review Performance monitoring improvement against trajectory Link with NSFT13
23

NSFT13 Exec
lead: Daryl Chapman
The Trust must ensure that all staff have access to clinical records and should further review the performance of the electronic system.
PLAN ON TRACK: RAG
RATING
Summary of actions Oct Nov Dec Jan Feb Mar Apr & beyond
Locality managers identify any areas where paper records continue to be used and address with ICT.
Head of ICT confirms that there is on-site support for clinical teams designed to increase the knowledge of staff and the efficiency with which they use the patient record management system (Lorenzo). Clinical teams to identify those that want and require support.
Head of ICT confirms that there is additional support to ‘super-users’ (to be identified by clinical teams) so that there is a local resource for clinical teams
The Head of ICT confirms that system performance issues have escalated to the system provider (DXC) and that there is at least monthly progress chasing: the contract for Lorenzo is between DXC and NHS Digital. High risk of issues at NSFT not being resolved
OUTCOME: Staff have access to a reliable health records system.
Evidence/Assurance Improved staff satisfaction with the system in surveys Link with NSFT10 – improved performance in CPA & risk assessments Improved timeliness and accuracy of system reporting Peer Reviews Functional improvements in the system are delivered by DXC/NHS Digital (dashboard)
24

NSFT21 Exec
lead: Daryl Chapman
The Trust must ensure that data is being turned into performance information and used to inform practices and policies that bring about improvement and ensure that lessons are learned.
PLAN ON TRACK: RAG
RATING
Summary of actions Oct Nov Dec Jan Feb Mar Apr & beyond
The Director of Finance establishes the Digital Information Improvement Group with the following work streams: Skills & capability, System performance, Data quality, Reporting,
Clinical Information Officer appointed Quality Programme Board reviews and agrees process for data and information sent to external organisations
Execs review quality standards and agree set of metrics to improve performance
The Director of Finance confirms that a work plan is in place for all work streams so that performance against clear milestones to improve data and information can be reported on a monthly basis
Review performance targets with Commissioners: what’s relevant & appropriate
Director of Finance agrees communication strategy on why data is important for Trust-wide dissemination
Director of Finance completes a review of performance management processes with Locality Managers and Directors of Ops
OUTCOME: Reliable data is used to improve quality. Evidence/Assurance Revised set of quality & workforce standards to monitor performance against Performance improves Protocols are in place for how we manage performance standards Workforce performance is recognised and owned Peer Reviews
25

NSFT22 Exec
lead: Dr Bohdan Solomka
The Trust should ensure that the work undertaken in relation to deaths is learnt from to ensure that there are not missed opportunities that would prevent serious incidents (SIs).
PLAN ON TRACK: RAG
RATING
Summary of actions Oct Nov Dec Jan Feb Mar Apr & beyond
The Medical Director (through the Mortality Review Group) to develop a work plan in relation to deaths with SMART actions
Patient Safety & Complaints Lead benchmarks position against other organisations
The Head of Governance to ensure all staff are aware of and understand the SI Policy and how it relates to their practice and responsibilities
Patient Safety & Complaints Lead provides feedback to teams on lessons and learning from incidents to ensure reflective learning and practice change
Medical Director reports to the Board on learning from the best in the world
OUTCOME: We can demonstrate that we improve quality by learning from deaths.
Evidence/Assurance Team meeting minutes show that learning has been communicated. Staff can describe how they learn from SIs including unexpected deaths Reduction in serious incidents
26

NSFT08 Exec
lead: Dawn Collins
The Trust must ensure there are sufficient staff at all times, including medical staff and other healthcare professionals, to provide care to meet patients’ needs.
PLAN ON TRACK: RAG
RATING
Summary of actions Oct Nov Dec Jan Feb Mar Apr & beyond
Executive agreement to increase admin resource to release clinicians for patient care in return for increased performance (specifics agreed with ward managers). HR recruitment team to place adverts and organise interviews.
Locality Managers (LMs) develop business cases to increase capacity where demand has increased and is evidenced (for CCG support)
HR Lead carries out review of recruitment and retention strategy and leads on executive agreed actions to address shortcomings
Business Support Managers (BSMs) provide daily roster reporting to local managers so that staff pressure hot spots can be mitigated by CTLs.
Community team managers confirm that daily ‘huddles’ in community teams established
OUTCOME: Patients have their needs met.
Evidence/Assurance Time to hire performance is reduced Level of vacancies is reduced Reduction in number of Datix incidents for staff shortages Reduced sickness levels for work-related stress Peer Review
27

NSFT19 Exec lead:
Pete Devlin / Debbie White
The Trust must ensure that there are clear targets for assessment and that targets for waiting times are met. The Trust must ensure that people have an allocated care co-ordinator.
PLAN ON TRACK: RAG
RATING
Summary of actions Oct Nov Dec Jan Feb Mar Apr & beyond
Directors of Operations confirm that Demand and capacity reviews for services (in conjunction with waiting time performance) have been completed
Directors of Operations confirm that consistent business approach to record unallocated cases has been agreed and implemented
Directors of Operations confirm that the Caseload Weighting Tool is in place across the Trust and review current position: agreeing actions to address concerns
See NSFT17: Directors of Operationss agree performance and waiting time management plans for all areas that are not delivering waiting time standards
Directors of Operations confirm that Standardised documentation is in use across Trust
Medical Director confirms that referrals from GPs (Sustainability and Transformation Plans (STP) work programme) have been reviewed and learning fed back to STP
OUTCOME: Patients receive timely care.
Evidence/Assurance Peer Review Line management supervision improvement Consistent caseloads in line with agreed thresholds Staff survey improvements Waiting time performance improvements Service User survey feedback shows that people know who their care coordinator is.
28

NSFT15 Exec leads:
Pete Devlin / Debbie White
The Trust must ensure that all staff receive regular supervision and annual appraisals and that the system for recording levels of supervision is effective and provides full assurance to the trust board.
PLAN ON TRACK: RAG
RATING
Summary of actions Oct Nov Dec Jan Feb Mar Apr & beyond
Human Resources Business Partners (HRBPs) ensure that there is monthly reporting to service managers and through to Accountability Review meetings
Executives agree appropriate performance target % Line Managers confirm that ‘supervision trees’ are in place to ensure everyone is clear who is providing and receiving supervision.
See NSFT10 additional admin to support recording The HR Lead completes a review of the appraisal process to ensure it is simple and effective, including recording to demonstrate compliance. HRBPs work with outlier teams. Performance Accountability meetings follow up actions to green.
OUTCOME: The board is assured that staff receive regular supervision and annual appraisals.
Evidence/Assurance Performance improvement Staff satisfaction (survey in 2018) Increased training need identification Peer Reviews
29

NSFT09 Exec lead:
Dawn Collins
The Trust must ensure all relevant staff have completed statutory, mandatory and where relevant specialist training, particularly in suicide prevention and life support.
PLAN ON TRACK: RAG
RATING
Summary of actions Oct Nov Dec Jan Feb Mar Apr & beyond
HRBPs provide managers and team leaders with compliance reports on a weekly basis
The Trust Education Lead to review access to training and increases this where necessary (flexibility in provision of training (e.g. locally) is required).
The Trust Education Lead provides monthly reporting to execs on individuals <50% and executive leads confirm that there are plans in place to reach the compliance targets for each Statutory or Mandatory training area.
The Trust Education Lead to carry out a review of rationale for mandatory training and targets, and reports to the executive team which approves any updated targets based on patient and staff priorities.
Team leaders report through to Executive directors on reasons why compliance has not improved and provides actions to address at team or individual level as appropriate.
OUTCOME: Our staff are competent to provide safe and effective care.
Evidence/Assurance Performance on mandatory training improves Increased training courses filled Peer review process
30

NSFT14 Exec
lead: Dr Bohdan Solomka
The Trust must ensure that there is full and clear physical healthcare information and that patients’ physical healthcare needs are met.
PLAN ON TRACK: RAG
RATING
Summary of actions Oct Nov Dec Jan Feb Mar Apr & beyond
Physical Healthcare Lead to confirm that the Physical Healthcare Policy review is complete and that the user guide/quick action guide has been developed.
Physical Healthcare Lead to confirm that reporting on compliance system has been established
Line managers monitor application of the policy through management supervision
Physical Health Lead attends ward meetings in each locality to assess / address barriers to compliance
OUTCOME: Patients’ physical healthcare needs are appropriately assessed and addressed.
Evidence/Assurance Matrons audits Peer Review Line management supervision Compliance reporting improvement
31

NSFT23 Exec
lead: Dr Bohdan Solomka
The Trust should review the audit trail for medicines held at community clinics for administration or supply to service users.
PLAN ON TRACK: RAG
RATING
Summary of actions Oct Nov Dec Jan Feb Mar Apr & beyond
Head of Maintenance confirms Backtraq (medical devices inventory) system is operational
CTLs to ensure weekly checks on equipment and report issues Head of Pharmacy confirms medical competencies check with staff is complete and any shortfalls are addressed
Head of Pharmacy to confirm pharmacy team provides supervised drug rounds to improve practice
OUTCOME: Management of medication in community services is consistent with best practice.
Evidence/Assurance Peer Review Local audits
32

NSFT12 Exec
lead: Dr Bohdan Solomka
The Trust must ensure that the temperature of medicines storage areas is maintained within a suitable range, and that the impact on medicines subject to temperatures outside the recommended range is assessed and acted on.
PLAN ON TRACK: RAG
RATING
Summary of actions Oct Nov Dec Jan Feb Mar Apr & beyond
Increased resource agreed for Pharmacy to support community teams
Matrons confirm that electronic systems for monitoring fridge temperatures are in place and working. Issues are escalated to the pharmacy team and maintenance team.
The Head of Pharmacy reviews medicines management competencies within teams
Matrons/Pharmacy Leads confirm that all staff are clear on the operational procedures to support the system
OUTCOME: Medication is properly stored.
Evidence/Assurance Matrons audits Central fridge monitoring (to Pharmacy) Peer Reviews
33

NSFT11
Exec lead: Dr Bohdan Solomka
The Trust must ensure that the prescribing, administration and monitoring of vital signs of patients are completed as detailed in the NICE guidelines [NG10] on violence and aggression: short-term management in mental health, health and community settings.
PLAN ON TRACK: RAG
RATING
Summary of actions Oct Nov Dec Jan Feb Mar Apr & beyond
Minutes demonstrate that governance meetings in localities consider their local compliance.
The Lead Clinician establishes a system to ensure that there is team discussion for reflective practice after any event.
The Physical Health Team Lead reviews Trust procedure against NICE guidelines and makes amendments if necessary
The head of Training signs off that training is compliant with NICE and training delivered.
OUTCOME: Violence and aggression is managed effectively in line with NICE guidelines.
Evidence/Assurance Performance will improve Matron and clinical audits No of incidents reported on Datix will decrease Peer review
34

NSFT24 Exec
lead: Dr Bohdan Solomka
The Trust should review the arrangements to support people in the rehabilitation and recovery service to manage their own medicines in preparation for discharge.
PLAN ON TRACK: RAG
RATING
Summary of actions Oct Nov Dec Jan Feb Mar Apr & beyond
Associate Director of Operations/Head of Pharmacy confirm the policy for self-administration of medication is agreed
Associate Director of Operations to establish protocols for discharge of patients with suitably packaged medication
OUTCOME: People in rehabilitation services are supported to live independently by promotion of self-management of medication.
Evidence/Assurance Peer Review
35

NSFT25 Exec
lead: Dr Bohdan Solomka
The Trust should review the training provided to staff in St Catherine’s who handle medicines.
PLAN ON TRACK: RAG
RATING
Summary of actions Oct Nov Dec Jan Feb Mar Apr & beyond
Associate Director of Operations for Norfolk to provide case on the long term use of St Catherine’s under consideration to Executives
Local training package to be developed between matron and pharmacy
OUTCOME: Staff at St Catherine’s manage medication safely.
Evidence/Assurance Audit of training records Peer Review
36

Quality Programme Board governance structure and systems
1.0 Purpose of the governance structure
The purpose of this structure is to deliver the CQC inspection ‘must-dos’ before March 2018. To be fit for purpose the structure must be:
a) As simple as possible. b) Clear about roles and responsibilities for delivery of the changes, with
everyone named in the plan fully accepting the part they play. c) Accepted as the only way of coordinating the work of everyone involved.
There can be no parallel or alternative arrangements. There can be no opting out.
d) A source of timely and accurate assurance / early warnings to the executive team and the board of directors.
e) Resourced appropriately.
2.0 Quality Programme Board
2.1 Purpose
The overall purpose of the QPB is, “the management authority for the CQC programme ensuring that the day-to-day management is geared to the achievement of the objectives, benefits and outcomes.”
This section sets out how the QPB will function on a day to day basis.
2.2 What we mean by accountability for delivery
The QPB oversees the allocation of CQC actions and delegates the allocation of specific tasks to the named responsible Service Line Leads.
Accountability for delivery means that everyone, at every level, who accepts an action or task agrees to complete that task within the required timescale and quality standard.
Not delivering a task on time because of being ‘too busy’ is unacceptable. Similarly, offering to ‘try’ is unacceptable. In order for the action plan to be implemented there has to be a high degree of confidence that tasks will be delivered on time and to the required standard.
If the person allocated a task thinks they may not be able to do so because they are too busy then it is their responsibility to flag this before accepting it. It will then
QPB Governance Structure Version 0.9
Author: Robert Nesbitt based on PMO work Department: Corporate
Page 1 of 6 Date produced: 13/112017 Retention period: 20 years

be possible to re-prioritise their work, allocate extra resources or allocate the task to someone else. The focus is on finding a way to deliver the action not on explaining why it is difficult to do so.
If an unforeseeable change does takes place which jeopardises the delivery of the action then the owner must escalate this immediately. It is not acceptable to wait until the next meeting / QPB. Maintaining speedy implementation which is based on the action plan imperatives and not the meetings cycle is essential in order to deliver the CQC actions by 11 March 2018.
2.3 Sign off of evidence for milestones and outcomes
We learned from our last CQC inspection that actions that we thought were complete, on testing, were not. We have therefore changed our approach to rectify this problem. The person responsible for delivery will sign off the evidence that a milestone has been completed and later that the overall action has been delivered.
To minimise the burden on managers, the evidence that they submit is simply the same material as they used to satisfy themselves. For example, if they visited a ward to see for themselves that estates work was complete then a photograph is the evidence. If the evidence is an audit that shows compliance then that is all that is required.
The evidence that an action is complete will vary but will be set out in the CQC action plan and will so far as possible be in the form of an objective measure, photograph, or document which demonstrates the outcome.
We learned from our last inspection that it is sometimes possible for all the actions to be complete but the outcome not delivered. The Service Line Lead will be responsible for confirming to their Operational Lead that the outcome has been delivered as well as the actions.
The Compliance Team will provide an objective ‘stress-test’ the evidence to provide assurance to the QPB that the changes are robust and sustainable.
3.0 Understanding the delivery structure
The S.29a warning notice has 10 themes and the actions within these must be delivered by 11 March 2018. These include rectifying outstanding actions from the 2014 and 2016 inspections.
The S.29a actions are a subset of the full CQC inspection report ‘must and should’ dos which fall into 25 elements. All of these actions are cross referenced into the themes set out below.
3.1 Themes
The action plan covers a wide range of actions from discrete tasks (such as building changes) to system-wide requirements (such as safe staffing levels).
QPB Governance Structure Version 0.9
Author: Robert Nesbitt based on PMO work Department: Corporate
Page 2 of 6 Date produced: 13/112017 Retention period: 20 years

In order to make this manageable, these are themed with a programme manager allocated to each and each linked to a board committee:
Action plan theme Programme manager Committee 1. Environment / risk /
safety Matt Wilson QGC (ARC for some risk
elements) 2. Staffing Denise Zandbergen ODWF 3. Data / Performance
(Quality) Isabel Pollock Performance and Finance
4. Access / Capacity John Devenney Performance and Finance 5. Compliance /Audit Matt Wilson Audit and Risk
Programme Managers will primarily work with named responsible Service Line Leads. So, for example, Matt Wilson will work with Gary Hazelden in relation to seclusion room environmental actions.
3.2 Roles and responsibilities
Core Service Operational Lead Service Line Leads responsible for specific CQC actions plans
Monitoring Executive Oversight
NEDs oversight
Adult Wards Veno Sunghuttee/ Margaret Little
Gary Hazelden, Denise Grimes 2 weekly Dawn Collins Jill Robinson
Rehabilitation Wards Veno Sunghuttee/ Margaret Little
Gary Hazelden, Denise Grimes 2 weekly Dawn Collins Tim Newcomb
Adult Community Debbie White Gill Morshead 2 weekly Bohdan Solomka Gary Page
Older People’s Wards Michele Allott / Margaret Little
Micki Munro 2 weekly Dawn Collins Tim Stevens
Older People’s Community
Margaret Little, Veno Sunghuttee
Michele Allott 2 weekly Daryl Chapman Ian Brookman
Crisis and HBPoS (including Mental Health Liaison Services)
Margaret Little, Veno Sunghuttee
Ian Young 2 weekly Bohdan Solomka Adrian Matthews
LD Wards Margaret Little Sue Bridges 2 weekly Pete Devlin Marion Saunders
LD Community Margaret Little Sue Bridges 2 weekly Pete Devlin Marion Saunders
CAMHS Community (CAMHS Ward need to be included)
Veno Sunghutte, Margaret Little
Andy Goff 2 weekly Debbie White Marion Saunders
Secure Ian Young Karen Clements 2 weekly Robert Nesbitt Tim Newcomb
Corporate (Enabler) Daryl ChapmanThe appropriate Corporate Head of Department 2 weeks Robert Nesbitt
3.2.1 Operational Lead
The Operational Lead role is primarily coordination and problem solving. They are responsible for ensuring that the action plans for their core services are implemented quickly and effectively. This means that they:
• Check that the action plans for their Core Services are properly formulated and understood by everyone involved.
QPB Governance Structure Version 0.9
Author: Robert Nesbitt based on PMO work Department: Corporate
Page 3 of 6 Date produced: 13/112017 Retention period: 20 years

• Coordinate the work of the named responsible Service Line Leads across and between action plans intervening where efforts are not aligned or where there is scope for misunderstandings / duplication.
• Provide day to day support and act quickly to resolve issues that named responsible Service Line Leads cannot address or to escalate these to the appropriate director.
• Provide exception reporting to the QPB on their Core Service action plans. • Ensure that the QPB is aware of risks to delivery as soon as they are
identified. • Satisfy themselves that evidence signed off by Service Line Leads is robust
and sustainable (e.g. part of business as usual rather than the result of a special effort for an audit).
3.2.2 Service Line Lead responsible for the delivery of the CQC internal actions
The named Service Line Lead role is primarily about making actions happen, for the avoidance of doubt, the service line leads are empowered to operate across locality boundaries. They are responsible for implementing the action plan elements allocated to them. This means that they:
• Allocate SMART tasks to named staff. • Confirm that these staff have the resources (including time) to deliver the
tasks within the deadline. • Draw up plans / action lists proportionate to the task (if the CQC must-do
action plan does not provide sufficient detail). • Provide close monitoring of the implementation of the actions, intervening to
keep the plan on trajectory. • Escalate decisions / issues that they cannot resolve to their Operational Lead
without delay. • Keep their elements of the CQC ‘must do’ action plan up to date by
submitting reports (kept as concise as possible) to the CQC action plan administrator.
• Signing off evidence for milestones and outcomes. • Monitor focus of work to avoid ‘creep’. • Mobilise resources where an action plan is at risk of falling behind trajectory
(for example through staff sickness). • Report to the QPB on the progress of the identified actions within the Service
Line implementation plan including but limited to :- any actions that are slipping or at risk of slipping and plans to get back
on track specific proposals of any support identification of any Trust-wide learning from their work identification of any key risks resolution and evidencing Peer Reviews finding
3.2.3 Executive oversight lead
The Executive oversight lead provides a support and compliance function. The role complements the Compliance Manager role. This means that they: • Act as an arm’s length questioner of the robustness of progress / evidence.
QPB Governance Structure Version 0.9
Author: Robert Nesbitt based on PMO work Department: Corporate
Page 4 of 6 Date produced: 13/112017 Retention period: 20 years

• Triangulate sources of information and focus on weaknesses that might be identified by CQC on re-inspection.
• Step in to support the Operational Lead where an inter-director issue becomes stuck or is at risk of being overlooked.
3.2.4 Non-executive director
The non-executive director monitors, supports and challenges the work of the QPB in order to provide an independent source of assurance to the board of directors.
3.2.5 Improvement director [ID]
The ID reports to NHSI. In relation to the QPB, the ID monitors, supports and challenges the work of the QPB in order to provide an independent source of assurance and performance monitoring to the board of directors especially in relationship to the delivery of the most effective service to our patients.
3.2.6 Compliance Function
The compliance function works from the CQC ‘must dos’ recommendations. They visit sites as if in the role of a CQC inspector (Peer Reviews) and look for ways in which the evidence could be found lacking. For example, in testing knowledge about local ligature management arrangements on a ward they would ask questions of an NHSP member of staff. The findings are detailed within an individual report and summarised as part of a generic Heatmap which is reviewed at QPB. The detailed report is given to local management for resolution with outcomes and assurance being given to QPB via Service Line leads.
3.2.7 CQC action plan administrator
The CQC action plan administrator is responsible for maintaining the database with evidence, requesting evidence updates from Service Line Leads, and exporting extracts.
3.2.8 Heads of service / function enablers
The focus of the QPB’s work is on speedy, proactive change. The purpose of the heads of service / functions is to resolve problems and remove obstacles for Service Line Leads. In between QPB meetings, heads of service / function must make themselves available to Service Line Leads and Operational Leads to resolve problems. The expectation is that only significant deviations from policy, intractable issues, or those with complex interdependencies should come to the QPB for resolution.
4.0 Meeting structure and reporting structure 4.1 Meeting ‘A’ / ‘B’ pattern and focus
Each service line is reviewed every two weeks. Some service lines have many more actions than others and so they are divided into two roughly equal sets which
QPB Governance Structure Version 0.9
Author: Robert Nesbitt based on PMO work Department: Corporate
Page 5 of 6 Date produced: 13/112017 Retention period: 20 years

form model agenda ‘A’ and model agenda ‘B’. The QPB may decide to re-balance service lines between ‘A’ and ‘B’ as the programme develops. The meeting focus is on the action milestones and in particular on getting late milestones, or those at risk, back on trajectory (see also 3.2.8). However, as well as addressing ‘red’ and ‘amber’ milestones, the robustness of a sample of ‘greens’ will also be tested (and any problems reported to the QPB) by the compliance team function.
4.2 Reporting
The QPB reports to the Board of Directors each month, providing assurance where evidence is robust and flagging risk areas and remedial action plans.
5.0 Evidence 5.1 The named responsible Service Line lead implements the action plan with support
from the Operational Lead. They arrange for the database to be updated OR forward evidence of progress and completion to the CQC action plan administrator (proactively or by request) who updates the spreadsheet.
5.1 There is a programme of Peer Review visits by trained assessors who check that
actions are embedded and looking at the bigger picture of the 25 must dos. Their evidence for compliance / evidenced of gaps is owned by the local teams and forwarded to the named responsible service lead and PMO.
6.0 PMO interdependencies and effective use of time
6.1 Where a current PMO project is required to achieve an element of the CQC must-do action plan, reporting will be via the QPB meeting to avoid duplication.
6.2 Any PMO projects that sit outside the CQC action plan which the executive team agree need to continue will either report to a specific programme board (such as for the Mother and Baby Unit) or, for less complex programmes, on an exception basis to executive team meetings.
6.3 Any PMO projects that are not mission critical will be moth-balled or put in a slow stream until April 2018 to release capacity to support the CQC must-dos action plan.
6.4 The role of the Programme Manger is to a) work with the named responsible Service Lead to understand the action and how this relates to the CQC recommendation b) agree reporting milestones c) agree measurement and outcome d) manage synergies across the service lines and to ensure consistency in approach e) report progress against milestones.
QPB Governance Structure Version 0.9
Author: Robert Nesbitt based on PMO work Department: Corporate
Page 6 of 6 Date produced: 13/112017 Retention period: 20 years

Report To: Board of Directors
Meeting Date: 30 November 2017
Title of Report: Quality; Patient safety and Safeguarding.
Action Sought: For Information and assurance.
Estimated time: 10 minutes
Author: Saranna Burgess. Head of Patient Safety and Safeguarding
Director: Dawn Collins. Interim Director of Nursing, Patient Safety and Quality.
Executive Summary:
Patient safety and safeguarding are core business for the organisation. This report provides data analysis and comparison plus a narrative for the overarching themes within the different sectors; serious incidents including unexplained deaths, complaints, the risk register, safeguarding activity, raising concerns, restrictive interventions, infection control and service user and carer experience.
Serious incident numbers and themes remain consistent whilst this is reassuring in that there is not an increase it demonstrates that there is still work to do in ensuring that learning from serious incidents is embedded within operational teams. Accepting that not all risks for our service users, their families and our staff can be wholly eradicated striving to improve quality and hence outcomes for all are one of the organisations priority objectives.
Complaints remain of concern highlighting issues of poor communication, delayed or lack of access to services and attitude of staff. However, ‘poor attitude’ is off set by the feedback received through the Friends and Family Test, which are generally positive (88%) particularly in relation to ‘care’ and ‘attitude’.
The risk register further evidences the pressure on services and workload across the organisation due to vacancy rates, skill mix and capacity within service lines.
Safeguarding within the organisation continues to work well the activity within the team is indicative of the awareness throughout the organisation no doubt this is in part at least as a result of the high level of compliance in training.
The Flu jab campaign is progressing well and the organisation is aligned to the UNICEF “Have a jab, give a jab” incentive scheme.
Date: 30 November 2017 G Item: 17.187ii
Board of Directors 30th November 2017
Version: 2
Author: Saranna Burgess Head of patient safety and safeguarding
Page 1 of 18 Date produced: 20th
November 2017 Retention period: 20 years

1.0 REPORT CONTENTS
Control Section for detail
Comments
Patient safety including serious incidents of moderate/severe harm
2.1 There are no significant variations during this reporting period. The number of unexpected deaths continues to be within normal variation; the highest number is within our community services.
Complaints 2.2 There are no significant variations during this
reporting period. The highest reporting areas are; Suffolk Access and Assessment team, Central Norfolk, East Suffolk inpatient and Central Norfolk Youth team.
Risk Register 2.3 Risk linked to staffing, service demand and service capability continue to be of high concern to the Trust.
Suicide prevention strategy
2.4 Strategic and practice initiatives including; joint working, A&E follow up, crisis cafes, letter of hope and staying alive smart phone app are all on course.
Safeguarding 3 The number of contacts to the duty team remains
high indicating a healthy level of awareness and professional curiosity. Safeguarding training compliance rates are high generally across the organisation.
Raising Concerns 4 Number of concerns raised increased by one on the
previous quarter.
Restrictive Interventions
5 The draft strategy has been approved and implementation plan is in progress. Available figures on reducing restrictive interventions are disappointing however; work is ongoing to enhance data analysis and collection.
Safety Thermometer 6 Safety Thermometer; compliance target met in one month out of three.
IPAC 6 Flu vaccination programme is progressing well.
Further initiatives are under way to improve water safety.
Service User and Carer Experience
7 A range of strategies is underway to help improve service user and carer experience of services. Feedback shows that there is much work to do to reduce the proportion of people who report a negative experience, particularly in online posted comments, and the experience of those referred to community services.
Patient Advice and Liaison Service
8 PALS continues to be a busy service providing a valuable liaison and information resource.
Board of Directors 30th November 2017
Version: 2
Author: Saranna Burgess Head of patient safety and safeguarding
Page 2 of 18 Date produced: 20th
November 2017 Retention period: 20 years

2.0 PATIENT SAFETY 2.1 Serious Incidents.
The chart below shows that the Trust reported fifty-four serious incidents in this period. The monthly number sits within the variation shown over the past five years. More recently for comparison in the last reporting period, the figure was forty-five and in the previous reporting period to that, the figure was sixty. The fifty-four SIs cases include; allegation of abuse (5), injury (3), homicide (2), disruptive behaviour (3), near miss (1), pressure ulcer at grade 3 (2), under 18 admission (3) and, sadly, thirty-five relate to unexpected deaths. This includes three inpatient deaths; one due to cardiac disease within Central Norfolk Older Person’s Services, one due to respiratory disease in Great Yarmouth and Waveney Services and one due to what appears to be self-harm within the Central Norfolk Adult Service. Investigations are ongoing and, to date, sixteen reports have been completed. Emergent themes are non-adherence to policy, poor communication, lack of management supervision and physical health issues.
Avg=16.9
UCL=29.3
LCL=4.6
0
5
10
15
20
25
30
Serious Incidents (c Chart)
Board of Directors 30th November 2017
Version: 2
Author: Saranna Burgess Head of patient safety and safeguarding
Page 3 of 18 Date produced: 20th
November 2017 Retention period: 20 years

The chart below shows the unexpected deaths by service. As in previous periods, community services experienced the highest number of deaths (thirty-two); these deaths are broken down as follows:
11 in Norfolk Community Services 7 in Suffolk Community Services 5 in Norfolk Recovery Partnership 5 in Wellbeing 4 in Great Yarmouth and Waveney
At the time of writing, six deaths have been confirmed as being due to natural causes, the organisation is waiting for the cause of death in two cases, and three remain ‘unascertained’. The organisation awaits Coroner’s verdicts to affirm whether or not the remaining cohort took their own lives.
Avg=11.3
UCL=21.3
LCL=1.2 0
5
10
15
20
25
30Unexpected deaths reported as a SI (c Chart)
0 2 4 6 8 10 12 14
Older people's community services
DIST
Liaison services
Youth
Inpatient services
Norfolk Recovery Partnership
CRHT
Wellbeing
Community Services
Unexpected death reported as a SI by service in quarter two
Board of Directors 30th November 2017
Version: 2
Author: Saranna Burgess Head of patient safety and safeguarding
Page 4 of 18 Date produced: 20th
November 2017 Retention period: 20 years

The chart below shows the number of serious incidents that resulted in an inquest verdict of suicide / “took own life” up until April 2017. Due to timescales for Coroner’s hearings, the outcomes are updated as inquests are concluded which does not always align to the organisation’s reporting periods. For comparison, the data across the year 2016/2017 (table below) indicates that the variation experienced to date is within that seen previously.
During this reporting period there have been no Regulation 28; Prevention of Future Death reports received from the Coroner.
2.2 Complaints. 2.2.1 Summary of complaints in the period July – September 2017
During this quarter, 155 complaints were received. The chart below provides the totals per month, showing that this period was within the variation experienced over the past three years.
Avg=3.5
UCL=9.1
05
1015202530
Apr-
12Ju
n-12
Aug-
12O
ct-1
2De
c-12
Feb-
13Ap
r-13
Jun-
13Au
g-13
Oct
-13
Dec-
13Fe
b-14
Apr-
14Ju
n-14
Aug-
14O
ct-1
4De
c-14
Feb-
15Ap
r-15
Jun-
15Au
g-15
Oct
-15
Dec-
15Fe
b-16
Apr-
16Ju
n-16
Aug-
16O
ct-1
6De
c-16
Feb-
17Ap
r-17
SIs with Suicide/ Took own life verdict by month reported (c Chart)
Avg=51.4
UCL=72.9
LCL=29.9
0
10
20
30
40
50
60
70
Complaints (c chart)
Board of Directors 30th November 2017
Version: 2
Author: Saranna Burgess Head of patient safety and safeguarding
Page 5 of 18 Date produced: 20th
November 2017 Retention period: 20 years

The chart below shows the teams which received three or more complaints during this reporting period. The four teams which received the highest numbers of complaints, (Suffolk Access and Assessment Team, Central City 2 Adult Community, Poppy Ward (East Suffolk) and the Adult Central Youth Service) continue a longer term trend and are noted to have risks recorded on the risk register linked to staffing and capacity concerns. Whilst actions to address the risks are in motion, this is not currently reflected by a reduction in the number of complaints to date.
Information explaining the content of the complaints received by these four teams has been summarised below: Central City Community Services: Of the seven complaints received within this reporting period, six referenced values and behaviours of staff members. Specifically, this was reporting as either failing to follow through on promised actions (such as onward referral) or, more frequently, appearing dismissive towards their concerns or issues regarding their mental state. Whilst in many cases it is not possible to conclude exactly what happened during the interaction without being there, one of these complainants recorded their interaction and the staff member accepted the assertions and apologised unreservedly, explaining they knew it was wrong as soon as they had said the remark in question.
Board of Directors 30th November 2017
Version: 2
Author: Saranna Burgess Head of patient safety and safeguarding
Page 6 of 18 Date produced: 20th
November 2017 Retention period: 20 years

This suggests on balance that the perception of some that staff members’ behaviour was “rude” or “dismissive” in manner is likely to reflect the experience of the complainants accurately. In consideration of the complaints, it is likely that such behaviour is as a result, in some cases, of balancing a heavy workload alongside systems and human factors which do not always allow time to stop and reflect on the impact of our behaviour on others. Adult Central Youth Service: Of the six complaints received within this reporting period by Adult Central Youth Service, three cited the failure of staff to follow through on promised actions. These included a failure to organise timely CPA meetings, arrange appointments or make onward referrals in a timely fashion. One complainant also commented that it was their perception that the service had shown itself to be “intolerant and dismissive”. Complaints also highlighted experiences of poor quality of assessment, incorrect information recorded and poor continuity of care (regular staff). The majority of these complaints were not upheld; however one complaint established that inaccurate information had been recorded and this was duly corrected and an apology issued. Poppy Ward (East Suffolk): Of the six complaints received within this reporting period by Poppy Ward, five included concerns regarding service users’ experience of clinical treatment:
• inaccurate information being recorded within the health record leading to an incorrect diagnosis
• not having basic health need met • the treatment of other service users noted during a witnessed restraint • the ability of a detained service user to gain access to the roof via a
smoking shelter.
Access to the roof via the smoking shelter has been rectified as an immediate action and the incident subject to a serious incident investigation. The other concerns appear to have been due to the perception of the service user at the time, influenced by ill health. Suffolk Access and Assessment Complaints analysed over the reporting period cite issues around communication within the team. These have been unreturned phone calls, delays and cancellations with appointments. Some of these errors have been due to poor administration and staff have been reminded of the importance of completing this correctly.
Board of Directors 30th November 2017
Version: 2
Author: Saranna Burgess Head of patient safety and safeguarding
Page 7 of 18 Date produced: 20th
November 2017 Retention period: 20 years

One such complaint provided a timely learning opportunity establishing better links between the Access and Assessment Team and the Suffolk Wellbeing Service. GPs also raised concern over the referral processes. On one occasion, the GP raised an issue with a service user passed between services. In response, a new forum has been set up for Trust managers to discuss cases to avoid this in the future. Another GP highlighted the Trust’s failure to refer for a Mental Health Act assessment, instead asking the GP to do this. Staff have been reminded about the need for the Trust to have made the referral in this instance. Parliamentary and Health Service Ombudsman The Parliamentary and Health Service Ombudsman reached a final decision regarding two complaints as outlined below:
1. The Ombudsman found the organisation did not follow the NICE guidance relating to the care and treatment of service users with a diagnosis of Borderline Personality Disorder (QS88); the organisation should not have discharged the service user as their condition required secondary mental health services at that time. The discharge caused a three-month delay in receiving appropriate treatment. Furthermore, the organisation delayed telling the service user that there was a working diagnosis of personality disorder for two and a half months, which caused frustration. The Ombudsman also found the Trust did not organise a care coordinator for the service user for nine months.
An action plan is in production to address these identified issues and an apology has been extended to the person affected. A local review is underway which aims to fully understand the issues around the delay in the allocation of a worker and how the organisation can address this.
2. The Ombudsman found both the local council and the Trust failed to
ensure adequate aftercare planning for a service user. The Trust also failed to offer therapy during this time. A full apology and small payment, as recommended, has been extended to the service user.
2.3 Risk Register.
Linked to the narrative theme of pressure on capacity due to workload and low staffing highlighted within complaints, high level risks with origins in staffing shortage, service demand and service capability remain the greatest concern to the organisation. Most of the current risks impact on the quality of service provision. There are currently six “high” level risks: • Three are in West Norfolk (Fermoy unit staffing, community workload and
psychology staffing) • One is in Central Norfolk (psychology service demands in the city)
Board of Directors 30th November 2017
Version: 2
Author: Saranna Burgess Head of patient safety and safeguarding
Page 8 of 18 Date produced: 20th
November 2017 Retention period: 20 years

• One is in Secure Services (recruitment on Yare and Whitlingham wards- including medical cover)
• One is Suffolk Access and Assessment Team (low staffing). West Norfolk holds five risks with staffing implications. Three of these rate as “high” at 20, 15 and 16. The East Suffolk IDTs have six staffing-associated risks. Three are rated at 12, with the rest at 9 or less. A suite of actions is being employed to respond to these risks including an ongoing recruitment strategy, using opportunities such as job fairs and social media and reviewing the skill mix within the service.
2.4 Suicide Prevention Strategy and Mortality Review Board Updates.
Clinical Pathways Work continues to understand the most effective clinical pathways that support suicide prevention, including the internal pathways of the organisation, third sector and other external organisations. The objective is to understand which pathways are most helpful, and where most risk and/or gaps lie.
Safer Prescribing An opportunity for a secondment or fixed term role for a Consultant Psychiatrist to explore safe prescribing for people in need is currently out to advert. Whilst this process is ongoing, the Suicide Prevention Lead, Liz Howlett, plans to explore the confidence of non-medical prescribers to prescribe to someone experiencing suicidal ideation. To this end, Liz will present the Suicide Prevention Strategy to the Non-Medical Prescribing Forum in January 2018. Focusing on male suicide The Patient Safety Managers’ Bulletin August 2017 asked teams to consider four questions related to the practice of caring for males. The response rate was low but replies highlighted a need to focus on males with ASD and those who have difficulty managing transitions. It is hoped that this work will be taken forward by a Consultant Psychologist - yet to be finalised.
Young People Like many mental health organisations nationally, concerns about the mental health of young people in Norfolk and Suffolk is growing within the organisation. In response to this perceived decline in young people’s wellbeing, an external review of the serious incidents involving young people between April 2015 and May 2017 has been undertaken. As a result practice, knowledge and system factors have been identified as the overarching themes; in particular communication with GPs, information sharing with families and other agencies, assessments which are not age/development appropriate,
Board of Directors 30th November 2017
Version: 2
Author: Saranna Burgess Head of patient safety and safeguarding
Page 9 of 18 Date produced: 20th
November 2017 Retention period: 20 years

problems accessing patient systems and management of waiting lists are highlighted as influencing factors. Next steps will be for the Suicide Prevention Lead to share the report and findings with the Mortality Review Board and to facilitate a learning event for the relevant services in the organisation, inviting partner agencies to participate. Working with Families and Carers Co-working with the Recovery College and service users’ forums has commenced to develop a strategy to incorporate service users/carers. A support resource for families and carers to advise how to access services in times of crisis is now on the organisations public website. A pilot scheme has been planned with Great Yarmouth & Waveney Locality to develop a crisis / safety plan to assist carers managing a loved one in crisis. This is due to commence by January 2018.
Supporting staff with up to date skills and knowledge The Recovery College and NSFT Training Department have been engaged to review and develop co-produced suicide training in the organisation. Innovations A support package for patients following attendance at A&E in East Suffolk is due to begin, in line with the current model in Norfolk where 48 hour follow up contact is provided by MIND. Plans for crisis cafes in Norwich and Suffolk (location to be identified) are continuing. The letter of hope initiative has been completed and is awaiting publication. A trial of a “Staying Alive” app for use in times of crisis has been planned to commence in the Spring of 2018.
3.0 Safeguarding.
There are two recently completed safeguarding reviews, which the organisation has participated in alongside other partners. The first is an adult case; the review was commissioned by the Norfolk Safeguarding Adult Board (NSAB) and concerned a person who survived a serious self-harm event. The report will not be published publically due to the need to keep the identity of the subject confidential. Learning from the review will be shared and agencies required to implement actions have been notified. The NSAB will monitor compliance. The second case is a child review commissioned by the Suffolk Safeguarding Children Board (SSCB). The case relates to induced illness and will not be published publically to maintain the child’s confidentiality. However, findings from the review will be shared and actions implemented; these will be monitored through the SSCB. The number of contacts (referrals and consultations) received by the team, by email or by advice form, reached a peak for 2017 in July of 311, dropping to 239 in August and increasing again to 290 in September; however outstanding referrals for September will add to this total.
Board of Directors 30th November 2017
Version: 2
Author: Saranna Burgess Head of patient safety and safeguarding
Page 10 of 18 Date produced: 20th
November 2017 Retention period: 20 years

There were seven allegations against staff in the current reporting period, three in July and September and one in August. The Trust is working closely with Suffolk MASH to improve notification from the MASH to the Trust of concerns raised related to NSFT staff or services. Safeguarding training compliance rates across NSFT have remained constant or increased across the reporting period with the exception of DOLS, which reduced slightly in September.
The level 3 safeguarding children figure is of concern as this is a contractual and statutory requirement the total splits into: 89% in Norfolk and 84% in Suffolk. The compliance target is 90%. To address the shortfall the safeguarding team continue to offer additional training within areas with low numbers of compliance. The level 3 adult safeguarding training is being significantly updated to improve the domestic abuse content. The new course will go live in January 2018. The Trust has a target of 80% compliance for this training by April 2019.
4.0 Raising concerns.
There were eight concerns raised to the Freedom to Speak Up Guardian in the period July – September 2017, an increase of one case from the previous quarter.
Common themes, as in previous periods, were patient safety concerns, attitudes of staff and patient experience with a further two concerns relating to leadership and management (workload of part time staff) and perceived lack of action in addressing low
MONTH NSFT L1
Adult
NSFT L3
Adult
NSFT L1
Child
NSFT L3
Child
NSFT Preven
t
NSFT DOLS
MCA
MHA
Jul-17 97% 53% 97% 84% 79% 82% 83% 82%
Aug-17 97% 56% 97% 84% 80% 82% 84% 83%
Sept 17 97% 57% 97% 84% 80% 79% 84% 83%
Attitudes and
behaviours Staffing levels
Patient safety and
quality Patient
experience Leadership and
management TOTAL Central Norfolk 0 0 0 1 1 2 West Norfolk 1 0 0 0 0 1 GY&W 0 0 1 0 0 1 East Suffolk 1 1 0 1 0 3 Wellbeing 0 0 1 0 0 1 Total 2 1 2 2 1 8
Board of Directors 30th November 2017
Version: 2
Author: Saranna Burgess Head of patient safety and safeguarding
Page 11 of 18 Date produced: 20th
November 2017 Retention period: 20 years

staffing numbers. Advice was given, senior staff were informed, work has been undertaken with teams and investigations have taken place as appropriate.
5.0 Restrictive interventions. 5.1 Strategy update
The draft strategy for Promoting Positive Practice and Reducing Restrictive Interventions has been approved by the Executive Committee and will be published following agreement by the Quality Governance Committee. There is a detailed implementation plan accompanying the strategy and this is already in progress. A pilot project on Rollesby Ward will roll out positive behaviour support plans (PBS) on that ward for the first time. The goal is that, by March 2018, at least 80% of people who have experienced restraint, seclusion or rapid tranquilisation will have a PBS within 7 days of the incident.
• Matrons and ward managers have started work on collaborative annual safety
plans for each ward. • An e-learning package to complement PMA training has been planned and will
include a film of service users talking about their experiences of restrictive practices.
• The Executive Committee will receive proposals later this month for a structured executive safety walk round which will connect ward to Board on developing a positive safety culture.
• Datix reports are being used to design dashboards for the wards to help them and the executives to understand the impact of safety initiatives.
5.2 Data and targets
Analysis of Datix reports shows that reductions in restrictive interventions in some areas have been offset by increases elsewhere. Abbeygate, Northgate and Waveney wards have all reported significant increases in the use of restrictive interventions in the physical assaults sub-category, with Abbeygate Ward becoming the largest reporter of such incidents this year. Waveney Ward is now the highest reporter of restraint and rapid tranquilisation incidents; further analysis will be undertaken to understand the causation of this. This type of analysis forms part of the ongoing priorities for the Restrictive Interventions Lead. Avocet, Thurne and Yare wards have all reduced their reporting of restrictive interventions compared to 2016-17. All of the top 10 wards reporting prone and supine restraint are PICUs or adult acute wards, with the exception of the Dragonfly Unit, which is the 7th highest reporter. Seclusion rates on Abbeygate Ward have reduced and the seclusion room has now been decommissioned. Seclusion rates have increased on both Glaven and Waveney wards.
6.0 Safety thermometer and IPAC. 6.1 Safety Thermometer
The National Safety Thermometer tool provides monthly point prevalence data that measures the proportion of patients who are free from harm and who were residing on
Board of Directors 30th November 2017
Version: 2
Author: Saranna Burgess Head of patient safety and safeguarding
Page 12 of 18 Date produced: 20th
November 2017 Retention period: 20 years

Later Life wards within NSFT. The compliance target of 95% was achieved in one month during this reporting period:
Month July 2017 August 2017 September 2017 Compliance achieved 94.17% 96.19% 94.55%
The harms reported affecting the overall score were: grade 2 pressure ulcers in July, August and one sacral wound. All falls reported were graded as ‘low harm’.
6.2 Infection Prevention and Control
6.3.1 Flu Vaccination Programme The seasonal flu vaccination programme commenced on the 9th October 2017 with various approaches to encourage and enable staff to receive the vaccination. These include:
• A dedicated flu nurse to deliver vaccinations • A flu crew of 20 who are supporting vaccination in the workplace • The provision of 28 drop-in or booked appointment clinics run by
Occupational Health and NRP
In addition, a communication strategy is in progress and a Trust intranet site for flu-related information has been set up. An incentive scheme to encourage staff to take up the offer of a Flu vaccination has been put in place; this entails the organisation making a charitable donation to UNICEF to vaccinate children against Tetanus in high risk regions known as “Have a jab, give a jab”. Other incentives are available through UNICEF dependent on staff uptake, e.g. water purifying tablets. Our Communications Department is working with the Infection Prevention and Control Team to raise awareness of the scheme and encourage staff to have their Flu jab. The vaccination uptake on 24th October 2017 (day 15 of the campaign) was as follows:
Total Trust 801 19.82% Direct Care ( Frontline staff) 503 17.34%
The campaign, with its associated CQUIN, will end on 28th February 28th 2018.
6.3.2 Infection Surveillance
In the last quarter there have been no confirmed outbreaks of gastrointestinal infections. There have been no confirmed cases of Meticillin-resistant Staphylococcus aureus (MRSA) blood stream infection and no reportable cases of Clostridium difficile infection (denoted by toxin detected in laboratory specimen or evidence of infection documented on pathology report).
Board of Directors 30th November 2017
Version: 2
Author: Saranna Burgess Head of patient safety and safeguarding
Page 13 of 18 Date produced: 20th
November 2017 Retention period: 20 years

Review of the risk relating to the lack of provision of an infection control doctor service is continuing and discussions have been planned with a potential provider.
6.3.3 Cleanliness
The Infection Prevention and Control Team is supporting ISS to implement revised operational practices in the Julian and Hellesdon sites, following the model of service provision used in the Suffolk inpatient sites.
6.34 Water Safety A range of initiatives is underway regarding water safety in the Trust:
• A Water Safety Operational Group has been formed to continue to review the Water Safety Plan and oversee the operational aspects of water safety in the Trust.
• There remains a number of faults to be rectified from risk assessments. Safety controls are in place as interim measures in affected sites.
• The Water Safety Group is reviewing electronic systems for purchase by the Trust to improve recording and reporting, and to facilitate a water safety ‘dashboard’.
• Suffolk sites have been externally audited and a plan of action has been developed to address the findings.
• The rollout of a project involving flushing of low use outlets continues. 7.0 Service user and carer experience.
Feedback regarding service users’ and carers’ experience of the Trust is collected via the Friends and Family Test (FFT), NHS Choices and Healthwatch online posts, and Quality Health surveys. A summary of the results is shown below:
• Friends and Family Test
Recent work to improve participation rates in the Friends and Family Test (FFT) has improved the number of teams participating and the number of returns received. However, increasing the number of actual returns per month from its current level of 165 to a target of over 300 by the end of 2017-18 will require substantial support to the clinical teams. To this end leaflets and return boxes are being consistently replenished, teams are looking at different ways of alerting service users to the opportunity to comment, and the awareness of staff is being championed through the internal communications systems. Comments in FFT returns are allocated to categories by our FFT provider and identified as “positive” or “negative”. The proportion of positive comments compared to negative is generally commensurate with our overall FFT score (averaging in the region of 88% positive). The percentage of positive to negative comments by theme is shown below, with negative comments tending to reflect themes around facilities and punctuality (which includes waiting times and delays) and high percentages of positive comments around quality of care and attitude.
Board of Directors 30th November 2017
Version: 2
Author: Saranna Burgess Head of patient safety and safeguarding
Page 14 of 18 Date produced: 20th
November 2017 Retention period: 20 years

• NHS Choices and Healthwatch posts Further service user and carer feedback is obtained from posts logged on NHS Choices and Healthwatch websites. During the 10-month period January 2017 – October 2017, there were 175 comments posted about NSFT on these sites.
The profile of ratings for NSFT services is as follows:
The themes that receive the most frequent comments in online posts are, in order of frequency, quality of care, access, communication and waiting times. As with FFT returns, the online posts also show the category of “quality of care” as receiving a high frequency of comments and a high rating. “Punctuality / waiting times” was a negative theme in FFT and online postings. Overall, the ratings suggest that the demand on services and workload pressures are negatively impacting on people’s experience of using services which is resulting in the negative picture this profile shows, particularly within secondary community services.
• The Community Service Users’ Survey 2017 This survey breakdown so far has demonstrated an improvement in the organisations results; these are to be presented fully to the Executive team alongside a formal action plan as soon as practicable and later presented at Board in January 2018 (see appendix 1).
0
20
40
60
80
1 Star 2 Stars 3 Stars 4 Stars 5 Stars
Wellbeing Service Community Teams
Inpatient Wards
Board of Directors 30th November 2017
Version: 2
Author: Saranna Burgess Head of patient safety and safeguarding
Page 15 of 18 Date produced: 20th
November 2017 Retention period: 20 years

In the interim, the priority actions that have been recommended by the survey have been picked up in the CQC “must do” action list, covering crisis care, treatments and therapies, and support and wellbeing. Priorities cover three overarching areas: 1. Overall scores: breakdown results to locality level and focus on ‘bottom scores’ to
be shared with local teams. Undertake an Always Event pilot project within the Central Norfolk locality exploring the community care pathway.
2. Care and treatment: formulation implementation, contact business cards for all community staff, Central Norfolk Crisis Hub.
3. Treatment and therapies: involve pharmacy and medics in improving information for service users and carers. Support and wellbeing; focus on support with physical health needs and gaining/returning to employment.
An update on key strategies and initiatives to improve service user and carer experience overall is provided below: • Triangle of Care
Stage 2 of Triangle of Care began this year and the required self-assessments from all secondary community teams have been completed. In addition, a survey of carers has been set up to provide further information which will be triangulated with the results of the self-assessments to identify the priority areas requiring improvement.
• Improving Services Together
The locality service user and carer hub meetings and reporting structure has been implemented across all 5 NSFT localities. The focus is now on the content of reports and on ensuring that more service users and carers can have their say and contribute to improvements.
• The Recovery Strategy
The recovery strategy was launched in Ipswich on 22nd September, following a successful launch event in Norfolk in June. Work will focus on those aspects of the strategy that closely align with the CQC “must do” list, in particular reducing restrictive interventions and improved personalisation in the assessment and care planning process.
8.0 Patient Advice and Liaison Service. 8.1 During the 6-month period from 1st April to 30th September 2017, PALS received a total of
731 separate enquires, 448 from people in Norfolk and Waveney and 283 from people in Suffolk. 52.4% of enquirers were from service users and carers, and 21.4% NSFT staff. 25.1% enquired were from people in neither category with 1.1% unknown.
8.2 PALS enquiries are categories into the following eight main themes used nationally by MH
PALS: Access, Waiting (delays), Relationship (attitudes and behaviour); Information; Communication; Environment; Quality of Care; and, Other.
The breakdown of enquires by theme is as follows:
Board of Directors 30th November 2017
Version: 2
Author: Saranna Burgess Head of patient safety and safeguarding
Page 16 of 18 Date produced: 20th
November 2017 Retention period: 20 years

. 42% of calls to PALS in the reporting period were issues related to communication and
35% information. Only 8% of calls received were allocated to the 3rd most common theme, Access. An analysis of the sub-categories for communication and information provides further useful information.
8.3 Communication by sub-category
8.4 Information by sub-category
9.0 Equality implications. 9.1 This report highlights an overarching risk in relation to timely access to services for both
those within protected characteristic cohorts and for the wider population. Much work is
020406080
100120
N&W
Suf
0102030405060
N&W
Suf
Board of Directors 30th November 2017
Version: 2
Author: Saranna Burgess Head of patient safety and safeguarding
Page 17 of 18 Date produced: 20th
November 2017 Retention period: 20 years

underway to enhance skill mix within services and address the running vacancy risks that the organisation is facing. The review of service pathways and many of the actions within the CQC action plan address this theme.
10.0 Risks to the organisation aligned to the Trust objectives. 10.1 The dominant risk remains against ‘improving quality’; as demonstrated through the
narrative of complaints and the detail available via the risk register. The difference that the organisation is able to make in terms of improving outcomes (quality) for service users in relation to their mental health is hampered in some areas due to the national issue of a lack of nurses, commissioning and financial disparities within mental health and more locally due to workload pressures and a lack of managerial oversight.
S.Burgess Head of Patient Safety and Safeguarding.
Board of Directors 30th November 2017
Version: 2
Author: Saranna Burgess Head of patient safety and safeguarding
Page 18 of 18 Date produced: 20th
November 2017 Retention period: 20 years

• Analysis of results by Locality, informed locality based remedial planning workshops (x5) in January / February 2017
• Introduced the Team Recovery Implementation Plan (TRIP) within community teams
• Other remedial actions taken including by pharmacy team to improve access to medication information
• Localities took ownership of local remedial plans
• Recovery College developed courses in partnership with Equal Lives providing benefits and employment advice (now scheduled into recovery college timetable).
• Our Recovery Strategy 2017-2022 (launched in Sept 2017, informed by learning from 2016 survey)
Actions we took in 2016
1.4 SU Survey 2017 Results (1)

-18.0%
-15.0%
-12.0%
-9.0%
-6.0%
-3.0%
0.0%
3.0%
6.0%
9.0%
12.0%
15.0%
18.0%
Q3
Q4
Q5
Q6
Q7
Q9
Q10
Q11
Q12
Q13
Q14
Q15
Q16
Q18
Q19
Q20
Q21
Q23
Q25
Q27
Q29
Q31
Q32
Q33
Q34
Q35
Q36
Q37
Q38
Q39
Q40
Q41
Heal
th &
Soc
ial c
are
Wor
ker
Org
anizi
ng c
are
Plan
ning
Car
e
Revi
ewin
g Ca
re
Chan
ges i
n w
ho y
ou se
e
Crise
s Ca
re
Trea
tmen
ts
Supp
ort &
Wel
lbei
ng
Ove
rall
1.4 SU Survey 2017 Results (2) Percentage change by question compared to 2016
Ca
re &
Tre
atm
ent

In comparison with other mental health trusts, most scores are in the intermediate 60% range. However there are some scores in the bottom 20% of all Trusts. We will be focusing on these areas to increase overall scores while continuing to improve
all categories.
OVERALL What: Focus on the ‘bottom’ scores, but also ensure the improving trend between 2016 and 2017 continues in 2018 and at a greater rate than other Mental Health Trusts to initially move the Trust out of the bottom 20% and continue progress over subsequent years to above average. How: 1) When available (expected mid-November), breakdown results by Locality and present to localities and community teams (17/18 Q4); 2) Undertake an Always Event pilot project within Central Norfolk to explore the community care pathway with service users and carers, with the outputs shared with all localities to inform subsequent actions (17/18 Q4 onwards).
Issues for priority action 1/3
1.4 SU Survey 2017 Results (3)

CARE AND TREATMENT
What: Not seen often enough to meet needs (Q3).
How: NSFT.08; NSFT.10; NSFT.19; Formulation implementation.
ORGANISING CARE
What: Knowing how to contact and care poorly organised care (Q9,10)
How: Business Cards for all community practitioners; Formulation implementation (also Q4); Always Event project (also Q4).
CRISIS CARE What: How to make out of hours contact and the right response (Q21, 23) How: NSFT.17; Central Norfolk Crises Hub development (N&W STP Plan)
Issues for priority action 2/3 1.4 SU Survey 2017 Results (4)

TREATMENTS AND THERAPIES What: Ensure involvement in deciding treatments and understanding about them (Q31,32) How: Share results with all teams, with focus on prescribing staff and all doctors; Formulation implementation; Always Event.
SUPPORT AND WELLBEING What: Ensure support with physical health needs, finding work, and what is important to the service user (Q33,35,39). How: NSFT.14; NSFT.10; Formulation implementation; Always Event to inform further actions; introducing Dialog+ PROM; develop more partnerships with employment support agencies
Issues for priority action 3/3
1.4 SU Survey 2017 Results (5)

Report To: Board of Directors
Meeting Date: 30 November 2017
Title of Report: 2017/18 Financial Performance Report - Month 7 (October)
Action Sought: For Assurance
Estimated time: 10 minutes
Author: Simon Ledger, Head of Financial Management
Director: Daryl Chapman, Interim Director of Finance
Date: 30 November 2017 H Item: 17.187iii
Executive Summary: The purpose of the report is to inform the Board of the Trust’s financial performance as at 31st October 2017.
• The year-end forecast deficit is £0.9m which is £0.2m favourable to our £1.1m financial control total.
• The financial performance of the Trust is assessed by NHS Improvement through the Finance and Use of Resources metric. Both our Plan and our performance against the Plan are rated at a ‘3’.
• Out of Trust (OOT) placements expenditure was £0.5m in October.
• Secondary commissioned placements expenditure was £0.3m in October.
• The spending on agency staffing was within the NHS Improvement agency cap for the
month and is expected to remain within the cap for the year.
• The 2017/18 CIP target of £10m is forecast to be delivered in full. • Cash held by the Trust at 31st October was £9.4m.
• The full finance report was discussed at the Performance and Finance Committee on
21st November 2017.
30th November Board of Directors Financial Performance Report
Version 1.1
Author: Simon Ledger Department: Finance
Page 1 of 4 Date produced: 14th November 2017 Retention period: 30 years

1.0 FINANCIAL ANALYSIS Our financial position is as follows:
2.0 FINANCIAL COMMENTARY OUT OF TRUST (OOT) PLACEMENTS Total bed days increased from 744 in September to 874 in October. Total expenditure for the month was £0.5m. The year to date overspend of £2.8m will be funded by the CCGs.
SECONDARY COMMISSIONED PLACEMENTS There were three admissions and three discharges during October. Total expenditure for the month was £0.3m, an overspend of £0.1m. The year to date overspend of £0.8m will be funded by the CCGs.
Statement of Comprehensive Income (SOCI)-Year to Date Full Year
Annual Actual Variance Annual
Plan Plan
£'000 £'000 £'000 £'000
Operating Income (127,672) (127,171) (501) (220,122)
Pay Costs (Substantive, Bank & Overtime) 88,401 87,816 585 144,369
Agency & Locum Costs 5,853 5,078 775 9,781
Drugs Costs 1,775 1,519 256 3,040
Other Costs 26,517 28,166 (1,649) 52,192
EBITDA 5,126 4,592 (534) 10,740
Depreciation 4,285 4,389 (104) 7,323
Non Operating Income (15) (65) 50 (28)
Non Operating Expenses 2,682 2,065 617 4,592
Net surplus / (deficit) (1,826) (1,798) 28 (1,147)
EBITDA margin 4% 4% 5%
OOT PLACEMENTS
Bed Days APR MAY JUN JUL AUG SEP OCT NOV DEC JAN FEB MAR YTDMundesley 559 456 583 422 533 450 294 3,297Ellingham 27 91 150 193 461OOA 63 77 195 458 411 144 387 1,735TOTAL 622 533 778 907 1,035 744 874 0 0 0 0 0 5,493
Total spend £'000s 466 322 551 574 574 423 510 3,420Budget £'000s 83 83 83 83 83 83 83 583Variance (383) (239) (468) (491) (491) (340) (427) 0 0 0 0 0 (2,837)
12 MONTHS ACTUALS TO MARCH 2018
30th November Board of Directors Financial Performance Report
Version 1.1
Author: Simon Ledger Department: Finance
Page 2 of 4 Date produced: 14th November 2017 Retention period: 30 years

TEMPORARY STAFFING NHS Improvement (NHSI) has set the Trust an agency spending cap of £10.783m, the same cap as 2016/17. This has been phased in the annual plan to produce a reduction each month. Within this agency spending cap is a specific saving requirement of £0.4m of Medical Locum spend against 2016/17 spend levels The following table provides a summary on overall temporary staffing spend. The key booking reason for agency for qualified nursing and medical staff is unfilled vacancies.
CIP The agreed CIP target for 2017/18 submitted in the Annual Plan was £10.0m and this is forecast be to achieved in full. CASH FLOW As at the end of October, the Trust held cash and cash equivalents of £9.4m. This is ahead of the Annual Plan figure of £8.3m by £1.1m.
ACTUAL SPEND £'000s ACTUAL SPEND £'000sAgency Bank Total Agency Bank Total
Medical 324 324 Medical 2,122 2,122Qualified nursing 267 132 399 Qualified nursing 1,972 931 2,903Unqualified nursing 37 527 564 Unqualified nursing 272 3,825 4,097Clinical a&c 34 16 50 Clinical a&c 307 115 422Scientific & Therapeutic 4 4 Scientific & Therapeutic 150 150Corporate 28 28 Corporate 255 255
694 675 1,369 5,078 4,871 9,949NHS Improvement Spending Cap 875 NHS Improvement Spending Cap 6,645
OCTOBER YTD
30th November Board of Directors Financial Performance Report
Version 1.1
Author: Simon Ledger Department: Finance
Page 3 of 4 Date produced: 14th November 2017 Retention period: 30 years

BALANCE SHEET Non-current assets and funds employed are showing significant adverse variations, due to the revaluation exercise carried out in 2016/17 financial year not being reflected in current annual plan.
The total capital spend YTD is £4.5m against the revised annual capital plan of £9.6m.
3.0 QUALITY IMPLICATIONS Adherence to our financial plan and compliance with Standing Financial Instructions enables the Trust to improve its service quality within the financial resources available. 4.0 RISKS Based upon current performance and in order to achieve the Trust forecast financial deficit of £0.9m, the following areas need to be closely monitored and controlled.
(i) Out of Trust Placements and Secondary Commissioned Placements. (ii) Agency and locum spend. (iii) Financial impact of CQC recommendations and requirements.
5.0 RECOMMENDATION The Board is asked to review and note the report. Daryl Chapman Interim Director of Finance November 2017
30th November Board of Directors Financial Performance Report
Version 1.1
Author: Simon Ledger Department: Finance
Page 4 of 4 Date produced: 14th November 2017 Retention period: 30 years

Report To: Board of Directors – Public
Meeting Date: 30 November 2017
Title of Report: Business Performance Report - September 2017 Performance
Action Sought: For Information
Estimated time: 10 Minutes
Author: Karen Rix, Deputy Director Contracts, Performance and Information
Directors: Daryl Chapman, Interim Director of Finance Debbie White, Director of Operations (Norfolk) Peter Devlin, Director of Operations (Suffolk)
Executive Summary:
The purpose of this report is to provide information on Trust wide performance against a range of key performance indicators and assurance on the indicators which are not meeting the required standard for the period to 31 October 2017. The following information is provided: Section A: Summary Dashboards for Performance Section B: Commentary on Indicators Appendices with historic trends and activity.
The report was discussed at the Performance and Finance Committee on 21st October 2017.
Date: 30 November 2017 I Item: 17.187iv
Board of Directors – Public –30th Nov 2017 Business Performance Report
Version 1.0 Authors: Karen Rix Department: Contracts Performance Information
Page 1 of 15 Date produced: 21st November 2017 Retention period: 20 years

Section A (i): Summary Performance Dashboard September 2017
ACTUAL TARGET CHANGE ACTUAL TARGET CHANGE ACTUAL TARGET CHANGE
97.8% 95% -0.1% Admissions to inpatient services had access to CRHT teams 8.38% 2.50%
IAPT patients who have depression and/or anxiety disorders who receive psychological therapy
# 96.9% 95% -0.6% CPA patients receiving follow up within 7 days of discharge
67.5% 50% 1.4%Referrals with suspected FEP start NICE-recommended care within 2 weeks1 115.2% 95% -1.9%
Meeting commitment to serve new psychosis cases by early intervention teams2 # 92.3% 95% -1.2% CPA patients having formal review
within 12 months
100.0% 97% -0.01% Data Completeness: Identifiers 92.9% 95% -0.4% % of qualifying patients with a MHCT cluster
# 6.3% 7.5% 0.3% Minimising delayed transfers of care
93.8% 75% -0.3% People referred to the IAPT programme will be treated within 6 weeks of referral 98.0% 90% 1.8% Medium Secure Bed Occupancy Rate
(including leave)# 118 0 -5.9% Waiting Times - Number of incomplete
pathways waiting > 18 weeks
99.9% 95% -0.1% People referred to the IAPT programme will be treated within 18 weeks of referral 89.2% 90% -7.3% Low Secure Bed Occupancy Rate
(including leave)# 95.6% 80.0% -1.7% Waiting Times - % of CAMHS patients
seen within standard
43.6% 50.0% 1.2% IAPT patients who complete treatment and 'move to recovery' 57.1% 90% -11.3% MS/LS Blended Bed Occupancy Rate
(including leave)# 94.6% 95% -2.6% Patient Safety Thermometer
90%Ensure that cardio-metabolic assessment and treatment for people with psychosis is delivered routinely in inpatient wards
34.31 28 -2.03 Average Length of Stay - Adult Acute Service
# 100.0% 100% 1.4% Long-term (> 12 months) inpatients have received an annual health check
90%
Ensure that cardio-metabolic assessment and treatment for people with psychosis is delivered routinely in Early intervention in psychosis services
#
65%
Ensure that cardio-metabolic assessment and treatment for people with psychosis is delivered routinely in Community mental health services (people on CPA)
#
85% Data Completeness : Priority Metrics #
Notes 1) Only reporting on referrals to existing (a) 14-35 year old early intervention services in Suffolk, and (b) 14-65 year old early intervention services in Norfolk & Waveney. No NSFT early intervention services currently commissioned to triage, assess and treat people with an at-risk mental state2) The number of new psychosis cases accepted by either (a) 14-35 year old early intervention services in Suffolk, or (b) 14-65 year old early intervention services in Norfolk & Waveney
NHS IMPROVEMENT (SINGLE OVERSIGHT FRAMEWORK)
ORGANISATIONAL DELIVERY QUALITY, SAFETY & EXPERIENCE
Awai
ting
Info
rmat
ion
Board of Directors – Public –30th Nov 2017 Business Performance Report
Version 1.0 Authors: Karen Rix Department: Contracts Performance Information
Page 2 of 15 Date produced: 21st November 2017 Retention period: 20 years

Section A (ii): Summary Workforce Performance Dashboard September 2017
Engaged Workforce KPI Mar-17 Apr May Jun Jul Aug SepAnnualised Sickness absence % 4.63% 4.76% 4.93% 4.89% 4.86% 4.78% 4.75% 4.79% 4.76%Monthly Sickness absence % 4.63% 4.34% 5.32% 4.81% 5.22% 4.28% 4.41% 4.87% 4.34%Staff recommending as place to work 56% - 80.0% - - 52.0% 0.0% 0.0% 0.0%Survey Response Rate 52% - 44.2% - - 37.7% 0.0% 0.0% 0.0%
Skilled Workforce KPI Mar-17 Apr May Jun Jul Aug SepVacancy Rate - All Staff 13.7% 10.9% 10.4% 11.8% 11.3% 11.6% 11.5% 11.0% 10.9%
Of which Clinical Vacancies 13.7% 11.7% 11.0% 12.6% 12.0% 12.3% 12.4% 12.1% 11.7%Of Which Non-Clinical Vacancies 13.7% 8.6% 8.8% 9.5% 9.0% 9.2% 8.8% 7.9% 8.6%
All Turnover 13.0% 14.0% 14.1% 14.5% 15.0% 15.0% 14.7% 14.5% 14.0%Voluntary Turnover 10.0% 9.0% 9.3% 10.4% 10.5% 9.7% 9.6% 9.4% 9.0%
Of which Clinical Turnover 10.0% 8.7% 0.0% 9.5% 8.7% 9.3% 9.5% 9.2% 8.7%Of which Non-Clinical Turnover 10.0% 9.7% 0.0% 10.7% 12.2% 10.8% 10.1% 10.2% 9.7%
Stability Index 87.0% 89.4% 88.9% 88.8% 88.9% 88.7% 88.9% 89.2% 89.4%Time to Hire (Days) 75.0 87.5 82.8 76.1 76.4 69.0 80.5 80.7 87.5Management Supervision % - Non Medical 89.0% 27.4% 0.0% 0.0% 22.4% 32.4% 29.3% 27.4% 27.4%Management Supervision % - Medical 89.0% 9.9% 0.0% 0.0% 4.1% 9.6% 8.1% 28.0% 9.9%Appraisal % - Non Medical 89.0% 73.7% 62.0% 64.0% 66.4% 70.6% 73.5% 74.4% 73.7%Appraisal % - Medical 89.0% 81.8% 86.0% 80.7% 62.1% 54.5% 65.2% 84.2% 81.8%Mandatory Training % 90.0% 84.8% 84.8% 84.9% 84.9% 86.8% 86.8% 86.9% 84.8%
Responsive Workforce KPI Mar-17 Apr May Jun Jul Aug SepTotal Agency spend £k 970.0 694 984 742 818 771 744 665 694Temp Nursing Demand ('000's hrs) N/A 58 N/A 58 58 54 57 63 64 58
Temp Nursing fill rate# 90.0% 85.8% 89.8% 88.3% 92.7% 91.2% 87.3% 86.4% 85.8%Net Nurse Contracted Hrs Worked (%)^ 0.0% 1.1% 2.5% 2.2% 2.2% 1.4% 2.1% 1.0% 1.1%% of Approved Job Plans 89.0% 84.0% 87% 79% 87% 88% 88% 82% 84%Notes: * Represents 12 month rolling trend/performance# This is a management performance indicator, not a contract based KPI
Performance Tracker*
Performance Tracker* Trend*
Represents performance in 4 week rolling rostering period. Current month reflects 'planned roster', previous months reflect 'actual roster'
Performance Tracker*
Trend*
Trend*
Benchmark Target
Currrent Performance
Benchmark Target
Currrent Performance
Benchmark Target
Currrent Performance
Trend data not available
Trend data not available
Board of Directors – Public –30th Nov 2017 Business Performance Report
Version 1.0 Authors: Karen Rix Department: Contracts Performance Information
Page 3 of 15 Date produced: 21st November 2017 Retention period: 20 years

Section B (i): Indicators not achieved in the period
Table 1 summarises the indicators which were not achieved in the period. A commentary is provided on these indicators
Table 1
Indicator Target Actual Change from
previous month
IAPT patients who complete treatment and 'move to recovery' 50% 43.6% 1.2%
% of qualifying patients with a MHCT cluster 95% 92.9% 0.4%
Average Length of Stay - Adult Acute Service 28 34.3 2.0
CPA patients having formal review within 12 months 95% 92.3% 1.2%
Waiting Times - Number of incomplete pathways waiting > 18 weeks 0 118 7
Patient Safety Thermometer 95.0% 94.6% 2.6%
Low Secure Bed Occupancy Rate (including leave) 90% 89.2% 7.3%
MS/LS Blended Bed Occupancy Rate (including leave) 90% 57.1% 11.3%
Annualised Sickness absence % 4.69% 4.76% 0.03%
All Turnover 13.0% 14.0% 0.43%
Time to Hire (Days) 75.0 87.5 6.8
Management Supervision % - Non Medical 89.0% 27.4% 0.05%
Management Supervision % - Medical 89.0% 9.9% 18.15%
Appraisal % - Non Medical 89.0% 73.7% 0.64%
Appraisal % - Medical 89.0% 81.8% 2.34%
Mandatory Training % 90.0% 84.8% 2.07%
Net Nurse Contracted Hrs Worked (%) 0.0% 1.1% 0.03%
% of Approved Job Plans 89.0% 82.0% 2.00%
Board of Directors – Public –30th Nov 2017 Business Performance Report
Version 1.0 Authors: Karen Rix Department: Contracts Performance Information
Page 4 of 15 Date produced: 21st November 2017 Retention period: 20 years

Section B (ii): Commentary: Indicators not achieved in the period
The report continues to use the format of the Single Oversight Framework (SOF). The cardio-metabolic assessment in inpatient and community based mental health services for people with psychosis will be included in the report once the detail of the metric is provided by NHS Improvement (NHSI). NHSI are proposing to replace the data completeness ‘Identifiers’ and ‘priority’ measures with a Data Quality Maturity Index (DQMI) Mental Health Services Data Set (MHSDS) Data Score. The change will be implemented once NHSI publish the updated SOF for 2017/2018.
The following indicators did not achieve the set target in September 2017.
1. Improving Access to Psychological Therapies – patients who complete and ‘move to recovery’
Performance by localities that did not achieve the target is as follows:
Jul Aug Sep Target Central Norfolk 36.0% (578) 34.2% (471) 37.0% (497) 50%
West Norfolk 46.0% (127) 42.8% (152) 40.2% (132) 50% Suffolk East 52.0% (191) 50.9% (232) 49.8% (219) 50%
Note: For reference denominator total shown in brackets In Suffolk East the recovery standard has been met for the previous two reporting months and if one more service user who completed treatment in September had moved to recovery the standard would have been met. In Norfolk and Waveney the service remains under a Contract Performance Notice (CPN). Following the review by the NHS Intensive Support team (IST) the service is in the process of implementing a wide range of recommendations that will support delivery of a revised trajectory to meet the recovery target by June 2018. The trajectory is based on a number of service improvements that are fully evidenced within the project documentation which has been shared with the Wellbeing Service Improvement Group of which the CCGs are stakeholders. This includes a predicted detrimental impact on recovery as the backlog of service users experiencing long waits is cleared. The service improvements are being managed by the Trust’s Project Management Office (PMO) who will report monthly to the Trust’s Executive. Issues as agreed with IST and Norfolk and Waveney CCGs that need resolution:
• The service was initially commissioned to deliver a 60:40 access ratio. This means that 60% of people accessing the service were expected to access direct workshops and not be individually assessed prior to attendance at a workshop. Analysis of the direct workshops has identified that people are accessing treatments that are NICE recommended but not always appropriate for their clinical presentation, thereby not contributing to their recovery.
• The original service model design had locally commissioned waiting targets for 1st and 2nd appointments (15 and 28 days wait for treatment) which has led to the front loading of the service delivery in terms of 1st and 2nd contacts and resulted in the service having significant waits for subsequent treatment, negatively impacting on recovery
Actions to provide resolution:
• To move to a 100% 1:1 initial assessment model that goes ‘live’ in January 2018 so that: o the service user is assessed by an appropriately trained clinician o the presenting diagnosis will be captured at assessment by the clinician o the clinical diagnosis will be used to determine appropriate treatment based on NICE
guidance
Board of Directors – Public –30th Nov 2017 Business Performance Report
Version 1.0 Authors: Karen Rix Department: Contracts Performance Information
Page 5 of 15 Date produced: 21st November 2017 Retention period: 20 years

• To eradicate the current long waits by: o implementing a simplified clinical pathway o replacing locally commissioned waiting time standards to concentrate service delivery
against national waiting time targets o undertaking a review of waiting list management processes to develop more
sophisticated means of care pathway monitoring and waiting times reporting • Norfolk and Waveney CCG support is required to deliver the contractual changes; the joint CCG
and NSFT Wellbeing Service Improvement Group continues to work through the action plan.
2. Qualifying patients with a MHCT cluster
Performance by localities that did not achieve the target is as follows:
July Aug Sep Target Central Norfolk Adult 89.4% (2832) 88.8% (2861) 88.7% (2858) 95%
Central Norfolk CFYP 90.5% (535) 90.0% (528) 88.2% (541) 95% Great Yarmouth & Waveney Adult & DCLL 93.9% (2165) 92.8% (2206) 91.6% (2222) 95%
Great Yarmouth & Waveney CFYP 80.5% (318) 79.9% (324) 77.0% (335) 95% Suffolk West 94.4% (1702) 93.7% (1677) 93.7% (1644) 95%
Note: For reference denominator total shown in brackets The overall trend this year is of deterioration against the target. Actions:
• The appropriateness of reporting this metric is currently under review, previous actions include; the recognition for continued discussion and agreement with Commissioners
• A clearer understanding of the use of SNOMED as an alternative and how this will be implemented nationally.
3. Average Length of Stay - Adult Acute Service
Performance by localities that did not achieve the target from the dashboard is as follows:
Jul Aug Sep Target Central Norfolk 43 (34) 65 (48) 48 (36) 28
West Norfolk 37 (18) 21 (16) 58 (11) 28 Suffolk East 43 (29) 44 (41) 37 (35) 28
Note: Average length of stay shown in days. For reference total discharges shown in brackets
Across the trust 147 service users were discharged in September 2017 (33 less than August 2017) and their total Length of Stay (LOS) was 5,044 days. Of 168 service users occupying a bed at the end of 31st October 2017, the total LOS is 10,545 days. The following table demonstrates these service users by a range of days:
Board of Directors – Public –30th Nov 2017 Business Performance Report
Version 1.0 Authors: Karen Rix Department: Contracts Performance Information
Page 6 of 15 Date produced: 21st November 2017 Retention period: 20 years

Banding Central West
Great Yarmouth &
Waveney Suffolk East Suffolk
West Grand Total
Non DToC DToC Non
DToC DToC Non DToC DToC Non
DToC DToC Non DToC DToC Non
DToC DToC
0-28 days 22 0 7 0 15 0 21 0 18 0 83 0 29-62 days 15 0 4 0 3 0 12 0 9 0 43 0 63-100 days 9 1 1 0 0 0 7 0 0 0 17 1 100+ days 7 3 2 2 0 0 4 0 5 1 18 6 Note: DToC category denotes the service user was recorded as a Delayed Transfer of Care at the end of 31st October 2017
• Comparing those active at the end of September to the end of October there has been an overall
increase in the numbers occupying a bed for 100+ days by 6 service users
• 25% of the Trust total service users active at the end of with 100+ days LOS are flagged as Delayed Transfers of Care (DToC)
Actions: • Weekly discharge meetings discuss service users with longer length of stays with a view to
facilitating discharge. This meeting considers service users in Trust beds and out of Trust beds
• The Daily Silver Calls are an inter-ward teleconference between all inpatient wards to discuss all delays, and to get an update on proposed discharged patient movements
• Issues are escalated to the Senior Operational Team for senior management action
In addition please refer to actions listed below at section 8 a, Minimising delayed transfers of care.
4. CPA patients having formal review within 12 months
Performance by localities that did not achieve the target is as follows:
Jul Aug Sep Target Central Norfolk Adult 90.6% (550) 86.6% (546) 85.1% (538) 95%
Central Norfolk CFYP 96.4% (55) 88.1% (59) 90.9% (77) 95% Great Yarmouth & Waveney Adult & DCLL 95.6% (206) 95.1% (203) 94.1% (219) 95%
Great Yarmouth & Waveney CFYP 92.3% (69) 95.6% (68) 94.4% (72) 95% Suffolk East 95.9% (614) 94.8% (615) 93.1% (639) 95%
Note: For reference denominator total shown in brackets
The Norfolk and Waveney Commissioners issued a Contract Performance Notice (CPN) in relation to this measure. In response to this the services have written a comprehensive action plan and committed to a trajectory to meet the target across Norfolk and Waveney by January 2018. Performance against the revised trajectory for the month is as follows:
September Trajectory Actual Variance
Norfolk and Waveney CCGs 91.2% 90.8% -0.4%
Board of Directors – Public –30th Nov 2017 Business Performance Report
Version 1.0 Authors: Karen Rix Department: Contracts Performance Information
Page 7 of 15 Date produced: 21st November 2017 Retention period: 20 years

The table below demonstrates the remaining trajectory targets up to attainment of the standard:
Oct-17 Nov-17 Dec-17 Jan-18 Norfolk and Waveney CCGs 93.0% 93.5% 94.2% 95.2%
Actions:
• Service users without a diarised CPA review date will be raised within local governance meetings and deputy service managers will be provided with a breakdown on the clinicians in question
• Reports are being shared with clinical team leads highlighting upcoming breaches which includes those due within 6 months to ensure appointments are scheduled prior to the 12 months elapsing
5. Waiting times – number of incomplete pathways waiting over 18 weeks
Performance by localities that did not achieve the target is as follows:
Note: %’s shown in brackets represent number incomplete pathways waiting over 18 weeks as a % of the total number of incomplete pathways at month end In the Central Norfolk Adult service line 22 referrals breached the 18 week standard a reduction of 4 from August, of which:
• 8 are awaiting appointments to adult community services • The remaining breaches have subsequently been treated or are delays caused by service users
not attending scheduled appointments In Central Norfolk CFYP service line 19 referrals breached the 18 week standard, there is no change from the August) of which:
• 12 were on a Youth waiting list, these cases were assessed and then referred internally from the Wellbeing service and put straight on waiting list for treatment where an issue with capacity has caused the delay. The referral process from Wellbeing is being redesigned to ensure future delays do not occur as a result of any transfers
• 5 were within the Neuro Developmental Disorder team waiting list for treatment • The remaining 2 breaches were either discharged or seen in October
In Central Norfolk Later Life service line 10 referrals breached the 18 week standard, this is an increase of 8 from August. The breaches were either; discharged, seen in October, as a result of appointment cancellations or put on hold due to physical health problems. In Suffolk Countywide locality 32 referrals breached the 18 week standard, an increase of 24 from August but a reduction of 5 from July. This fluctuation will be monitored. Breaches are attributable to the Access & Assessment team of which:
• 13 were delays caused by waits for Connors reviews. These are attributable to either a delay in sending the forms to the schools or families to complete or a wait for the review to be completed within the service
• 5 relate to delays caused by service users not responding to opt-in letters
Jul Aug Sep Central Norfolk Adult 25 (12%) 26 (13%) 22 (11%)
Central Norfolk CFYP 15 (7%) 19 (9%) 19 (10%) Central Norfolk Later Life 3 (0.8%) 2 (0.4%) 10 (6%)
Gt Yarmouth & Waveney Adult & DCLL 2 (1.0%) 5 (2%) 3 (1%) East Suffolk 22 (28%) 27 (31%) 28 (28%)
West Suffolk 39 (37%) 39 (36%) 46 (22%) Suffolk Countywide 37 (4%) 7 (0.8%) 32 (3%)
Board of Directors – Public –30th Nov 2017 Business Performance Report
Version 1.0 Authors: Karen Rix Department: Contracts Performance Information
Page 8 of 15 Date produced: 21st November 2017 Retention period: 20 years

• The remaining breaches have either been subsequently treated, have appointments scheduled or were either data quality issues which have now been addressed or delays relating to awaiting further information
In East Suffolk locality 23 of the 28 referrals breaching the 18 week standard were in the CFYP pathway relating to ADHD. There remain vacancies for ADHD nurses and clinicians in the locality to serve the Children and Youth pathways. The remaining breaches were either data quality issues which have now been addressed or are scheduled to be seen or have been subsequently discharged. In West Suffolk locality 42 of the 46 referrals breaching the 18 week standard were in the CFYP pathway also relating to ADHD. Recruitment is still in progress for the Children’s ADHD Service. The remaining breaches were either data quality issues which have now been addressed or are scheduled to be seen. The numbers of incomplete waits in Great Yarmouth and Waveney remain at 1% of the total number of service users waiting and West Norfolk continues to report no breaches.
Actions:
• Clinical priority is being given to service users based on risk and complexity; those not deemed clinically urgent are seen based on those waiting longest are seen first
• Breach reports are sent to team managers to review and to follow up with clinical teams
• Business Support Managers are working with staff to identify and correct data entry issues
• In Suffolk the locality is currently in the process of recruiting to ADHD posts in the new service model commissioned by CCGs
• Suffolk Countywide team are working to address capacity issues which are currently impacting
on Connors Reviews through the use of NHSP staff in the short term whilst recruitment is underway. Monitoring will continue of delays attributable to this issue within AAT
6. Patient Safety Thermometer
Performance by localities that did not achieve the target is as follows:
Aug Sep Target Central Later Life 96.3% 94.3% 95%
GY&W Adult & DCLL 84.6% 88.9% 95%
Suffolk West 100.0% 93.8% 95%
• In Central Later Life services: 3 incidents have been reported, 2 incidents relate to falls and 1 incident relates to a new category 2 pressure ulcer
• In Great Yarmouth and Waveney Adult and DCLL services: 1 incident was reported relating to a new category 2 pressure ulcer
• In West Suffolk: 1 incident was reported, relating to a fall where no harm was reported
Actions: • Pressure ulcers are regularly reviewed and management plans are in place
7. Low Secure Bed Occupancy Rate (including leave)
Performance is as follows:
Board of Directors – Public –30th Nov 2017 Business Performance Report
Version 1.0 Authors: Karen Rix Department: Contracts Performance Information
Page 9 of 15 Date produced: 21st November 2017 Retention period: 20 years

Jul Aug Sep Target
Low Secure Bed Occupancy Rate (including leave)
93.9% 96.5% 89.2% 90%
As part of a planned restructure three additional beds were opened on Foxhall Ward during September, this increased the number of available bed days for low secure services from 740 in August to 807 in September. Lower incoming referrals for this service area in September coupled with the increase in available beds has contributed to the decrease in occupancy rates.
Actions: • The rate of incoming referrals to the service to be monitored weekly and raised as appropriate
in management and referral meetings
8. MS/LS Blended Bed Occupancy Rate (including leave)
Performance is as follows:
Jul Aug Sep Target
MS/LS Blended Bed Occupancy Rate (including leave)
73.6% 68.4% 57.1% 90%
In August the service did not receive the required number of new referrals to meet the commissioned levels.
Actions: • The issue of a low level of referrals was raised with NHS England at a contractual level
whereby it was recognised by NHS England representatives as a national issue. Dialogue is ongoing with NHSE Commissioners
9. Other performance related issues
a. Minimising delayed transfers of care
Performance by localities that did not achieve the target is as follows:
Jul Aug Sep Target Central Later Life 4.2% 4.5% 8.01% 7.5% GY&W Adult & DCLL 10.6% 10.6% 10.2% 7.5% Suffolk West 10.8% 10.3% 9.1% 7.5%
The following tables provide a summary position on formal delayed transfers of care (DToC) for adult acute and DCLL beds reported for September at a countywide and trust wide level:
Norfolk and Waveney - September 2017
Ward Type
DToC
NHS Social Care Both Total
No. SU's
No. Days
No. SU's
No. Days
No. SU's
No. Days
No. SU's
No. Days
Adult acute 0 30 3 33 1 0 4 63
DCLL 2 104 7 216 0 0 9 320 Total 2 134 10 249 1 0 13 383
Board of Directors – Public –30th Nov 2017 Business Performance Report
Version 1.0 Authors: Karen Rix Department: Contracts Performance Information
Page 10 of 15 Date produced: 21st November 2017 Retention period: 20 years

Suffolk - September 2017
Ward Type
DToC NHS Social Care Both Total
No. SU's
No. Days
No. SU's
No. Days
No. SU's
No. Days
No. SU's
No. Days
Adult acute 3 45 5 51 0 0 8 96
DCLL 0 0 4 36 1 24 5 60 Total 3 45 9 87 1 24 13 156
Trust Total - September 2017
Ward Type
DToC NHS Social Care Both Total
No. SU's
No. Days
No. SU's
No. Days
No. SU's
No. Days
No. SU's
No. Days
Adult acute 3 75 8 84 1 0 12 159
DCLL 2 104 11 252 1 24 14 380 Total 5 179 19 336 2 24 26 539 Note: Excludes Learning Disability, Secure Services and Continuing Care Inpatient Wards
September figures continue to show that “Social Care Only” delays are negatively impacting on NSFT wards:
• For DCLL wards “Social Care Only” delays account for 68% (216 of 320) of Norfolk and Waveney and 60% (36 of 60) of Suffolk DToCs (66% Trust wide)
• For Adult wards “Social Care Only” delays account for 52% (33 of 63) of Norfolk and Waveney and 53% (36 of 60) of Suffolk DToCs (53% Trust wide).
Actions: Norfolk and Waveney
• The service is in frequent contact with social care to progress those with social needs delays
• All delays are discussed at the weekly service meeting to resolve issues and to facilitate discharge, also see narrative for lengths of stay
• Review of the NCC DToC performance levels agreements for NSFT patients • Review of NSFT discharge processes using a Quality Improvement methodology to identify
delays while focusing on quality and safety • Four new supported housing flats have been jointly commissioned between NSFT and Norfolk
County Council with Evolve to provide step down accommodation, with an option of commissioning a further 3 units
Suffolk
• NSFT DToC numbers to be reported in Suffolk Adult Social Care Directorate Management Team on a monthly basis to agree remedial actions required by the Area Teams
• The staff model element of the Adult Community Services restructure will have dedicated social work capacity to expedite hospital discharge planning for adults with learning disabilities
Board of Directors – Public –30th Nov 2017 Business Performance Report
Version 1.0 Authors: Karen Rix Department: Contracts Performance Information
Page 11 of 15 Date produced: 21st November 2017 Retention period: 20 years

• Mental Health Supported Housing resource to be reviewed ensuring that admission prevention placements are utilised to facilitate a stepdown pathway
• Review of NSFT discharge processes to ensure robust management oversight and inclusion of
Clinical Commissioning Group and Adult Community Services personnel
b. Meeting commitment to serve new psychosis cases by early intervention teams
Performance by localities that did not achieve the pro rata monthly target when applied to the commissioned levels is as follows:
September Target Actual Variance
Suffolk West 13 10 -3
Provisional figures for October show an improvement in performance against this measure.
c. Bed Occupancy
Adult Continuing Support The admission protocol for St Catherine’s Way ward in the Great Yarmouth and Waveney locality has been robustly reviewed and recently updated. All service users transferred to the unit are risk assessed to ensure suitability based on the new criteria. This has led to a lower number of admissions resulting in a lower bed occupancy level for September of 62%
Section B (iii): Workforce
This section presents analysis against workforce performance indicators aligned to our Workforce and Organisational Development Strategy where targets based on regional mental health benchmarks have not been achieved. The indicators have been broken into 3 key areas of focus:
• Engaged Workforce • Skilled Workforce • Responsive Workforce.
Improved performance in these areas will support the delivery of our Trust goals, in particular, improving quality and achieving financial sustainability and ‘working as one Trust'. It should be noted that for some indicators that have an overall satisfactory performance at a Trust level, there are significant variances across localities (e.g. vacancy rates). These variances, and action being taken, are monitored at a detailed level by the Workforce and Organisational Development Committee and additionally through locality Performance, Accountability and Review meetings. HR Locality Plans highlight corrective action required and commit to a timescale for achievement.
1. Annualised sickness absence rate
The Trust’s 12 month annualised sickness absence rate to end September 2017 has decreased to 4.76%, 0.13% points above the 4.63% target. Should the average rate of reduction over the last six months continue over the next six months, the target will be achieved and exceeded by the end of the financial year (4.59% by end of March 2018). This does not, however, factor in seasonal variations associated with colds and ‘flu. Our annual ‘flu campaign started on 9 October 2017. In light of a warning from NHS England of increased cases of ‘flu this winter, a ‘flu fighter nurse has been appointed to provide easy access to vaccinations across the Trust. The strategy is to try and beat last year’s position where 46% of staff received a vaccination.
Board of Directors – Public –30th Nov 2017 Business Performance Report
Version 1.0 Authors: Karen Rix Department: Contracts Performance Information
Page 12 of 15 Date produced: 21st November 2017 Retention period: 20 years

2. Vacancy Rate
The Trust’s vacancy rate decreased at the end of September 2017, to 10.9%, below the target of 13% (the target being set in line with the average for Mental Health Trusts in the region). Clinical vacancies decreased to 11.7%. A range of new services and the development of existing services (and other organisational change) will mean that the overall staff in post and vacancy rate will fluctuate over the next year. Recruitment is active for the new mother and baby unit and developments relating to the Tier 4 CAMHS unit. Additional capacity has been brought in to support this activity and a partner has been engaged to support us in taking forward our social media in recruitment strategy. This will largely focus on registered nurse band 5 and medical recruitment, with some targeted focus on hard to fill areas.
3. Turnover
Total turnover is just above the target of 13% at 14%. This includes all leavers, including staff finishing fixed-term contracts, dismissals or ending training programmes. Voluntary turnover, which is a better indicator of workforce churn, is, however, below the Trust target of 10% at 9%. Clinical turnover is 8.7% compared to non-clinical at 9.7%. There is, however, variation across localities. Voluntary turnover within the Norfolk Recovery Partnership at 17.72% is particularly notable. This is linked with staff uncertainty relating to the forthcoming transfer of services. Career discussions have been offered to all affected staff.
4. Time to hire
Time to hire for new starters in September averaged at 87.5 days. This is 7.5 days above the target of 75 days. The increase is due to the high volume of adverts and appointment activity in the period coupled with the peak holiday period. Activity is likely to remain high over coming months to support the new service developments. A number of changes have been agreed by the Executive Team to be trialled to help support getting new starters in post quicker.
5. Supervision
Supervision is now reported through the Workforce Dashboard. The recorded management supervision rate for non-medical staff is 27.4% and 9.85% for medical staff. Compliance is poor across all localities. To support improved recording, 40 wte admin staff are being recruited across the Trust to assist Clinical Team Leaders in the management administration elements of their roles. Additionally, an HR Business Partner has been realigned to provide additional support to managers and administrators on how to record supervision and appraisals and how they can monitor performance at team level through their business intelligence dashboard available on the Electronic Staff Record.
6. Appraisals
The Trust’s appraisal rate is currently 73.7% for non-medical staff and 81.8% for medical. Since April 2017, when reporting via ESR commenced, the non-medical rate has increased from 64%, whereas the medical rate has remained fairly static (80.7% in April). Performance with appraisals and supervisions requires significant improvement in line with the Care Quality Commission’s improvement notification.
7. Mandatory Training
The Trust’s mandatory training compliance rate is 84.8%. This has decreased by 2.43% since August 2017. This decrease is largely due to a large number of staff not completing health and safety refresher training by the end of September 2017. This was added to the mandatory training requirements in September 2015 with staff given 2 years to undertake the refresher training. Actions to improve mandatory training compliance have been presented to the Organisational Development and Workforce Committee.
Board of Directors – Public –30th Nov 2017 Business Performance Report
Version 1.0 Authors: Karen Rix Department: Contracts Performance Information
Page 13 of 15 Date produced: 21st November 2017 Retention period: 20 years

This table reports the current activity and Indicative Activity Plan (IAP) levels across the Trust by specific service lines.
Appendix 1: KPI – Activity Table 2017/18
2016/2017
Service Line1 Annual TrendEstimated Year
End Outturn3 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17
Access and AssessmentActuals 42,498 42,368 2,900 3,945 3,847 3,664 3,332 3,496
Indicative Activity Plan Levels 41,310 3,443 3,443 3,443 3,443 3,443 3,443Actuals 20,314 21,936 1,678 1,893 1,943 1,956 1,800 1,698
Indicative Activity Plan Levels 19,385 1,615 1,615 1,615 1,615 1,615 1,615Crisis
Actuals 47,431 46,420 3,779 4,136 3,991 3,929 3,842 3,533Indicative Activity Plan Levels 50,192 4,183 4,183 4,183 4,183 4,183 4,183
Actuals 10,189 10,894 768 952 927 992 949 859Indicative Activity Plan Levels 9,352 779 779 779 779 779 779
Adult CommunityActuals 9,012 9,629 9,529 9,663 9,696 9,630 9,607 9,651
Indicative Activity Plan Levels 9,352 9,352 9,352 9,352 9,352 9,352 9,352Actuals 147,297 144,912 10,698 12,642 12,947 12,220 12,316 11,633
Indicative Activity Plan Levels 155,105 12,925 12,925 12,925 12,925 12,925 12,925CAMHS / Youth
Actuals 6,243 5,693 5,927 5,857 5,769 5,731 5,443 5,433Indicative Activity Plan Levels 5,765 5,765 5,765 5,765 5,765 5,765 5,765
Actuals 81,289 70,588 5,235 6,447 6,085 6,090 5,768 5,669Indicative Activity Plan Levels 71,105 5,925 5,925 5,925 5,925 5,925 5,925
Dementia and Complexity in Later Life2
Actuals 4,353 4,373 4,364 4,353 4,297 4,381 4,373 4,470Indicative Activity Plan Levels 4,578 4,578 4,578 4,578 4,578 4,578 4,578
Actuals 77,881 70,796 5,415 6,166 6,228 6,028 6,033 5,528Indicative Activity Plan Levels 77,612 6,468 6,468 6,468 6,468 6,468 6,468
NeurodevelopmentalActuals 1,309 1,264 1,272 1,285 1,263 1,254 1,253 1,257
Indicative Activity Plan Levels 1,319 1,319 1,319 1,319 1,319 1,319 1,319Actuals 17,993 18,146 1,312 1,628 1,609 1,582 1,572 1,370
Indicative Activity Plan Levels 17,299 1,442 1,442 1,442 1,442 1,442 1,442
2017/2018
Key:1 Activity relates to secondary care services only excluding NRP/secure services, in Norfolk and Suffolk CCG Areas Only2 Excludes Suffolk Community Memory Asessment Service3 Estimate based on year to date average extrapolated to year end= Exceeds 2017/2018 Indicative Activity Plan (IAP) levels= Below 2017/2018 Indicative Activity Plan (IAP) levels
Number new referrals receive
Number open referrals
Number contacts delivered
Number open referrals
Number contacts delivered
Number open referrals
Number contacts delivered
Number open referrals
Number contacts delivered
Discharged after two or less co
Number contacts delivered
Number new referrals receive
Board of Directors – Public –30th Nov 2017 Business Performance Report
Version 1.0 Authors: Karen Rix Department: Contracts Performance Information
Page 14 of 15 Date produced: 21st November 2017 Retention period: 20 years
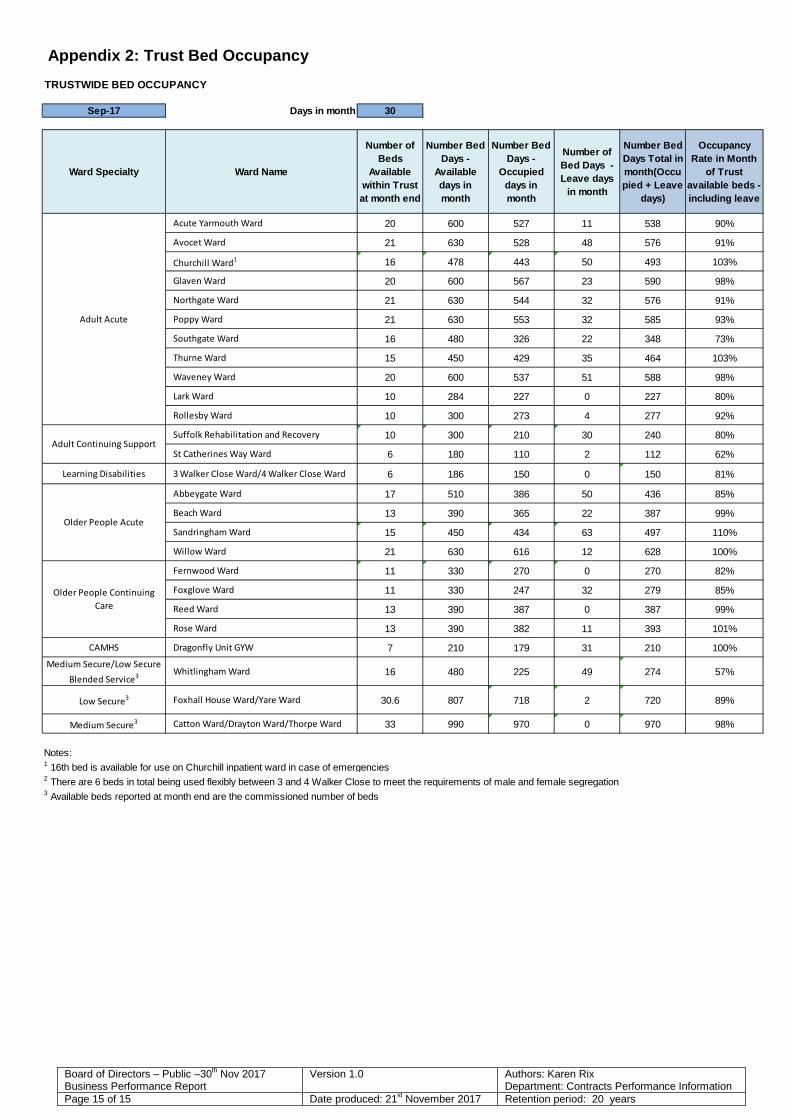
Appendix 2: Trust Bed Occupancy
TRUSTWIDE BED OCCUPANCY
Sep-17 Days in month 30Y N
Ward Specialty Ward Name
Number of Beds
Available within Trust at month end
Number Bed Days -
Available days in month
Number Bed Days -
Occupied days in month
Number of Bed Days - Leave days
in month
Number Bed Days Total in month(Occupied + Leave
days)
Occupancy Rate in Month
of Trust available beds - including leave
Acute Yarmouth Ward 20 600 527 11 538 90%
Avocet Ward 21 630 528 48 576 91%
Churchill Ward1 16 478 443 50 493 103%
Glaven Ward 20 600 567 23 590 98%
Northgate Ward 21 630 544 32 576 91%
Poppy Ward 21 630 553 32 585 93%
Southgate Ward 16 480 326 22 348 73%
Thurne Ward 15 450 429 35 464 103%
Waveney Ward 20 600 537 51 588 98%
Lark Ward 10 284 227 0 227 80%
Rollesby Ward 10 300 273 4 277 92%
Suffolk Rehabilitation and Recovery 10 300 210 30 240 80%
St Catherines Way Ward 6 180 110 2 112 62%
Learning Disabilities 3 Walker Close Ward/4 Walker Close Ward 6 186 150 0 150 81%
Abbeygate Ward 17 510 386 50 436 85%
Beach Ward 13 390 365 22 387 99%
Sandringham Ward 15 450 434 63 497 110%
Willow Ward 21 630 616 12 628 100%
Fernwood Ward 11 330 270 0 270 82%
Foxglove Ward 11 330 247 32 279 85%
Reed Ward 13 390 387 0 387 99%
Rose Ward 13 390 382 11 393 101%
CAMHS Dragonfly Unit GYW 7 210 179 31 210 100%Medium Secure/Low Secure
Blended Service3 Whitlingham Ward 16 480 225 49 274 57%
Low Secure3 Foxhall House Ward/Yare Ward 30.6 807 718 2 720 89%
Medium Secure3 Catton Ward/Drayton Ward/Thorpe Ward 33 990 970 0 970 98%
Notes:1 16th bed is available for use on Churchill inpatient ward in case of emergencies2 There are 6 beds in total being used flexibly between 3 and 4 Walker Close to meet the requirements of male and female segregation3 Available beds reported at month end are the commissioned number of beds
Adult Acute
Adult Continuing Support
Older People Acute
Older People Continuing Care
Board of Directors – Public –30th Nov 2017 Business Performance Report
Version 1.0 Authors: Karen Rix Department: Contracts Performance Information
Page 15 of 15 Date produced: 21st November 2017 Retention period: 20 years

Report To: Board of Directors – Public
Meeting Date: 30 November 2017
Title of Report: Chair’s report of Performance & Finance Committee on 21 November 2017
Action Sought: For Assurance
Estimated time: 10 minutes
Author: Daryl Chapman – Interim Director of Finance
Director: Tim Newcomb – Non-Executive Director Executive Summary: The report provides an update to the Board on issues reviewed by the Trust’s Performance and Finance Committee November Assurance review Issue reviewed by
committee Commentary (including actions where required) Level of
assurance Business
Performance Report
The Committee noted the performance report. The rating of the key metrics has remained largely unchanged since the previous month. The Committee noted the paper on options that are presently being reviewed in respect of a refresh of the KPIs that are reported, and the process that will be followed to ensure areas of non-achievement are addressed with meaningful action plans. The Committee noted that further work is ongoing with a broad stakeholder base to review the report contents and further updates are expected. The Committee noted that the Performance and Accountability Review Meetings are to be used to focus on performance against CQC identified risk areas, where measurable.
Amber
Financial Performance
The Committee noted the financial position at the end of October, being in line with plan. Green
Date: 30 November 2017 J Item: 17.187v
Board of Directors – Chair’s report on Finance Committee
Version 1.0
Author Daryl Chapman/Tim Newcomb Department: Corporate
Page 1 of 2 Date produced: 21 November 2017 Retention period: 20 years RED = significant gaps and not assured on adequacy of action plans
AMBER = Gaps in assurance but assured appropriate plans in place to address
GREEN = No gaps in assurance

Items for ratification The Committee ratified the following items: • Norfolk recovery Partnership contract
extensions with partner organisations • Laundry and linen contract award • Suffolk Emotional Wellbeing Hub service
Green
Risk Register The Committee noted the overall status of the risk register and the process of managing the risks. A new style report will be developed for the next review which will focus more on risk mitigation and management rather than risk analysis.
Amber
Commercial Update
The Committee noted the commercial opportunities presented. Agreement that the Trust should only explore opportunities if they are complimentary with our approach to exit Special Measures.
Green
Recommendations The Board is asked to note the highlighted issues within the Committee. Tim Newcomb Chair of Finance Committee 21 November 2017
Board of Directors – Chair’s report on Finance Committee
Version 1.0
Author Daryl Chapman/Tim Newcomb Department: Corporate
Page 2 of 2 Date produced: 21 November 2017 Retention period: 20 years RED = significant gaps and not assured on adequacy of action plans
AMBER = Gaps in assurance but assured appropriate plans in place to address
GREEN = No gaps in assurance

Joint working agreement for governors, non-executive directors and the wider Trust
30 November 2017 (for BoD approval) 11 January 2018 (for CoG approval)
Date: 30 November 2017 K Item: 17.187vi

Norfolk and Suffolk NHS Foundation Trust Joint working agreement for governors, non-executive directors
and the wider Trust
1. Purpose and status.......................................................................................................................... 1
2. Legal and governance framework ................................................................................................... 2
3. Structures, functions and the flow of information ......................................................................... 3
I. The relationship between the Council of Governors and its subgroups .................................... 3
II. Performance monitoring functions ............................................................................................. 3
III. Planning functions................................................................................................................... 4
IV. Trust Member and Governor Development Subgroup ........................................................... 5
V. Governor attendance at BoD meetings in public ........................................................................ 6
VI. Governor attendance at other BoD committee meetings ...................................................... 6
VII. Governor attendance at Trust operational / management meetings and visiting services ... 7
VIII. Director attendance at CoG meetings .................................................................................... 7
IX. Governor requests for information ........................................................................................ 7
4. Working relationships and behaviours ........................................................................................... 8
i. Support for governors to carry out their role ............................................................................. 8
ii. Objective setting and appraisals ................................................................................................. 9
iii. Promoting good relationships ..................................................................................................... 9
iv. Resolving disagreements between the Board of Directors and the Council of Governors ...... 10
v. The role of the lead governor ................................................................................................... 10
1. Purpose and status
The FT code of governance recommends that the roles and responsibilities of the Council of Governors should be set out in a written document and should establish an engagement policy with the Board of Directors. The purpose of this document is therefore to fulfil these functions by clarifying expectations for governors, non-executive directors, and for the wider Trust in order to promote effective and efficient accountability to the people we serve.
Although the governors’ duty to ‘hold to account’ is set out in law, it is not defined anywhere. NHS Improvement (previously known as Monitor) acknowledges that there is no ‘right way’ to hold non-executive directors to account and it recommends that a jointly agreed process be developed.
The document sets out the structures, flows of information, relationships and behaviours that underpin good governance for governors and non-executive directors working together.
Page 1 of 12

Once agreed by governors and directors it is intended to complement and put into practice the legal and governance framework.
2. Legal and governance framework
Foundation Trust governance is based on accountability of Boards of Directors to the local population through the Council of Governors. This is reflected in the powers of governors for the appointment and removal of NEDs and the Chair, the appointment of the external auditors, the approval of the appointment of the CEO and the approval of the forward plan.
The Health and Social Care Act (2012) strengthened the role of governors by placing a two-fold duty upon them;
S.151 (4)
“The general duties of the council of governors are—
(a) to hold the non-executive directors individually and collectively to account for the performance of the board of directors, and
(b) to represent the interests of the members of the corporation as a whole and the interests of the public.”
For its part the FT, under S.151 (5);
“…must take steps to secure that the governors are equipped with the skills and knowledge they require in their capacity as such.”
In addition to the legal powers and duties, Monitor’s Code of Governance and the publication, “Your statutory duties: a reference guide for NHS foundation trust governors (Aug 2013)” provide further guidance on joint working arrangements.
NHS Providers offer this definition of accountability:
“To be accountable is:
• To be responsible for the delivery of a specific task or outcome, • To be liable to explain and justify to another party, • To be subject to judgement and possible sanction or reward. • To hold to account is to receive the explanation or justification, to test it through
questioning, to form a judgement and to feed back.”
For their part, governors must understand the role of non-executive directors, the importance of their independence and the distinction between non-executive and executive directors in order to carry out their role. Non-executive directors maintain their independence partly in order to be able to test the evidence provided by executives and where appropriate to provide assurance that the governance systems are working effectively. Where assurance is lacking then they check what the significance is of this and where the testing identifies weaknesses then they require changes to address these.
Page 2 of 12

3. Structures, functions and the flow of information
I. The relationship between the Council of Governors and its subgroups The formal exercise of governors’ duties is carried out at the Council of Governors’ (CoG) general meetings as set out in the Constitution. The Council of Governors meets across the two counties six times a year. Four of these meetings deal with Council of Governor formal business. Two of these meetings have a smaller business component and focus on member engagement. Governors need to commit to attend these meetings which usually include a development session. Each meeting normally lasts a full day (c. 10:00 to 16:00). In order to ensure that the meetings are accessible to members and the public, venues usually have microphones and are accessible by public transport. Whilst these meetings are sufficient to make appointments and receive reports, this is not frequent enough to fulfil an effective scrutiny role nor to capture the interests of the wider public. The CoG therefore delegates some functions to subgroups which are empowered by their approved terms of reference to act on behalf of the full CoG. The CoG has approved meeting standards which also apply to its subgroups. Final decisions in relation to the CoG’s legal powers and duties can only be made at a general meeting. Although the subgroups are an important way in which detailed work can take place, governors remain collectively responsible for the delegated functions. For example, every governor must individually engage with members and the wider public. This role cannot be left to the Trust Governor and Member Development Subgroup. Similarly, every governor must take individual responsibility for monitoring the performance of the board – this role cannot be left solely to the Planning and Performance Subgroup.
II. Performance monitoring functions Consideration of performance information takes place at the Planning and Performance Subgroup and is in the context of assessing the performance of the board of directors (BoD). The purpose of this scrutiny is not to duplicate the work of the BoD in challenging information, but to gain assurance on the performance of the board in doing so. The focus of questions from governors should therefore be “What have NEDs done to examine this issue and to ensure that the board addresses it?”, and not “How can this performance be improved by governors?” In order for governors to be able to fulfil their role the Trust must supply subgroup members with information that is up-to-date, accurate, relevant and timely (i.e. received in sufficient time for governors to read and consider). At least two non-
Page 3 of 12

executive directors will normally attend each Planning and Performance Subgroup meeting with NED attendance varying over the course of the year. Their purpose is to answer questions put by the subgroup, either at the meeting or in writing within a given timescale. As this subgroup primarily looks into the organisation it provides a valuable opportunity for governors to hold NEDs to account. This does not mean that governors need to see all reports or to question every line of information that they receive. To do so would risk getting lost in the detail of Key Performance Indicator definitions and measurement problems instead of taking a wider view of board performance. Governors will normally therefore question a small selection of measures or reports which reflect issues of concern. These concerns could include incongruence between the data and other sources of information or a theme emerging from complaints made by patients or the wider public. For the period when the Trust was in special measures, an additional subgroup operated (the Improvement Plan Coordination (IPC) subgroup). It is proposed that this will continue in modified form following the Trust’s exit from special measures. The IPC will meet prior to each P&P subgroup meeting and review post-inspection action plan progress and feedback from committee observations. The Improvement Plan Coordination subgroup (IPC) was set up by governors when the Trust entered special measures in 2015. The IPC continued after the Trust left special measures in 2016 and the role of the subgroup will be reviewed to consider the response to the Trust re-entering special measures in 2017.
III. Planning functions In order for governors to contribute effectively to forward planning they need to have an understanding of members’ and the public’s views, and have a clear mechanism through which to feed these views into the process. Engaging with members and the wider public is led by with the work of the Trust Member and Governor Development Subgroup (see 3.IV below). The Council of Governors express a view on the Board of Directors’ forward plans. Governors should be involved through-out the planning cycle and should not be presented with plans as a ‘fait accompli’. The Planning and Performance Subgroup informs and tracks the development of the plan and has been delegated authority to lead on the forward plan to ensure that it receives appropriate attention. The subgroup also leads on the CoG role in relation to the Quality Account. The CoG can influence the direction of the organisation through the selection of the Chair and NEDs, but responsibility for setting the Trust’s strategy sits solely with BoD. The CoG does not set the strategy of the Trust.
Page 4 of 12

In setting the strategy and the forward plan that flows from it, the BoD should be able to demonstrate how they have taken account of governor views, particularly in so far as they flow from S.151 (4)b whereby governors represent “the interests of the members of the corporation as a whole and the interests of the public.” This does not mean that the CoG and BoD will necessarily agree. The BoD have to take into account their formal obligations (such as to operate the Trust as a going concern) and a divergence of views may simply reflect the different responsibilities of governors and directors. It is for this reason that the CoG cannot veto the forward plan.
IV. Trust Member and Governor Development Subgroup Elected governors are accountable to their members and should report to them on work undertaken. To some extent this function is fulfilled by the publication of the minutes of CoG meetings on the public website, but this is a narrow format and few members are likely to read these documents. The governors’ document Governor engagement with members and the public: our approach, sets out how governors approach engagement with members and the public. The main methods of communicating with members and the public are through the Trust’s Insight Magazine and via email. Governors can communicate directly with their constituents by submitting material for articles in Insight. The communications team can assist by drafting text based on these materials. The current Trust membership totals around 16,000 (including staff) of whom around 3,500 public, service user and carers have email addresses. The Trust’s Governor and Membership Development (TMGD) sub group leads on reviewing the Trust’s Membership Strategy, including what is expected of members and what they are offered, how they are communicated with and engaged. Current communication methods include the Trust’s Insight Magazine, email newsletters, member events and forums. Coordination of membership recruitment, and member and public engagement takes place through the Trust Member and Governor Development Subgroup. This group also oversees preparation of election materials. The Chair of the Trust is the lead as far as Trust membership and governor development is concerned. Regular contact between the Chair of the TMGD sub Group, Trust Chair and Lead Governor on membership and governor development matters and occasional attendance by the former two at TMGD sub Group meetings will ensure ownership of membership and governor development matters by the Board and their coordination with other Trust strategies. Members can contact their governors through a general email address [email protected] which is monitored by the Trust Secretariat. Member queries will be forwarded to the relevant governor, usually the Lead Governor, with advice and support on options for responding. A summary of the issue raised by the
Page 5 of 12

member will then be shared, by the Secretariat, with the CoG maintaining the confidentiality of the matter.
V. Governor attendance at BoD meetings in public There are ten BoD meetings in public a year. These are normally held in public in Ipswich and Norwich. For governors, these meetings provide an important opportunity to assess the performance of the BoD, to consider how the NEDs fulfil their functions within it, and to gain understanding of the BoD’s decisions for onward sharing with service users, carers, staff and stakeholders as appropriate when out and about. The role of the governor at a BoD is therefore as an observer. Whilst the Chair may invite questions and comments from governors, the function of these is to assist governors in their role rather than for governors to act as an additional member of the BoD. In order to fulfil their general duty to hold the NEDs to account for the performance of the BoD, governors should therefore aim to attend several BoD meetings a year. To facilitate governors in doing this, the BoD needs to ensure that governors and the public can hear what the directors are saying. This may require the use of microphones, or excellent acoustics. The BoD conducts a small amount of confidential (in that it relates to individual staff or service users) or commercially sensitive business in private. There is a requirement for FTs to share the agenda and minutes from these meetings with governors., but NSFT goes further and shares all private board papers with those governors who have signed a special confidentiality form. This form deals with the handling and disposal of the private papers as well as the protection of the information they contain. Governors can return papers to the Trust Secretariat for secure disposal.
VI. Governor attendance at other BoD committee meetings Governors are also welcome to attend BoD committee meetings, in the role of observer, by prior arrangement with the Chair of the committee. BoD committee meetings are chaired by NEDs. Following the learning from the experience of monitoring the Trust exiting special measures (through the IPC subgroup), Ggovernors have developed a process in which identified governors who are members of the IPC observe the committee meetings (see 3.ii above). It is important to be clear as to the rationale for attending BoD committee meetings since the governors’ role can usually be assured by the committee reports that come to the BoD. The advantage of governors observing committee meetings is that it can contribute to governor insights into the performance of the non-executive directors they appoint. For this to be effective, governors observing committees must have a
Page 6 of 12

sound understanding of the role of non-executive directors and what effective committee governance consists of. Most committee agendas are very full and it would impede the work of the committee if time was spent explaining the background to papers or answering governor questions. There may be value, however, in governors attending as ad hoc observers to understand the role of the committee and the work of the NED in more detail. A briefing before or after the meeting with the NED may also be useful. Guidance on observing committee meetings is available from the Company Secretary.
VII. Governor attendance at Trust operational / management meetings and visiting services There are a small number of operational meetings that NEDs attend (but do not chair). For the most part governors would not attend operational meetings since this is not part of their role (and, if the limited time available to governors was spent in this way, it would be time lost to fulfilling their core duties). When visiting services it is important for governors to bear in mind that they are not in the role of inspector, regulator or auditor. The purpose of a governor visit to a service is to understand what the service is for and how it works. In talking to service users (say on a visit to a ward) governors may gather insights that help in their role of representing the interests of members and the wider public. In order to avoid slipping into an inspector role, governors should not normally visit the same team more than once. The value of service visits for governors is that it enables them to gain a broad understanding of how care pathways and the whole work of the Trust operates and so visits should reflect this. Separate guidance for governors on visiting services is available.
VIII. Director attendance at CoG meetings For directors, the CoG provides a good opportunity to meet governors and to listen to their priorities and concerns; this is particularly important for NEDs who are directly accountable to governors. The expectation therefore is that NEDs will try to attend CoG meetings where practicable and that EDs will make reasonable efforts to attend when the agenda is relevant to their responsibilities.
IX. Governor requests for information
Page 7 of 12

Governors cannot fulfil their role unless they can ask questions and request information and the Trust must try to provide up-to-date, accurate replies to fulfil its accountability to local people.
There are several ways to request information.
The first is informally through a discussion with a board member or the Company Secretary about why the information is needed. This is helpful because it may be that the information sought would not meet the need, but that there is another way of addressing the same question. A meeting or telephone discussion with a manager may be more useful than a table of figures.
Where appropriate, governors can also request information through the ‘issues registerrepresenting interests register’ section in each Council of Governors meeting. The issues representing interests register also provides a way for governors to flag issues as part of their ‘representing interests’ role and has a ‘holding to account’ function in consideration of the responses received.
Any governor can ask that an item be put on the CoG agenda, giving two weeks’ notice. This right is set out in the Constitution and would generally be used when the other methods have proved ineffective.
If the information is already collected it will be shared as soon as practical.
If the information is not already collected then a discussion will take place about the benefits and costs of retrieving it. Normally this will resolve the matter to everyone’s satisfaction but if agreement cannot be reached the Chair will be asked to adjudicate.
X Governor feedback on services
Governors frequently hear feedback about services not working quite as they should, or indeed about them working exceptionally well. Governors should normally report such feedback to the Directors of Operations (Norfolk & Waveney or Suffolk) so that they can take appropriate action.
4. Working relationships and behaviours
i. Support for governors to carry out their role
The TMGD sub group produces an Annual Training Plan for governors largely based on an annual self-evaluation of governors, alongside governor evaluations by Service Users and Carer members and Trust directors. This includes annual induction sessions for all governors. NSFT has a legal duty to ensure that governors are equipped with the skills and knowledge that they need to discharge their duties. The training and development needs of governors are overseen by the Trust Member and Governor Development Subgroup.
Page 8 of 12

The Trust organises annual induction sessions for all new governors and arranges development sessions for all governors throughout the year on specific topics. So far as possible these are held on CoG days. Additional sessions between CoG days can also be arranged at the request of the Trust Member and Governor Development Subgroup. Ways to support governors are continually being refined and improved. Currently, elected governors are paired with a director who can act as an initial contact for queries and exchange of ideas. Partner governors can also request to be paired. This informal relationship can be used in whatever way is most useful to the governor. Governors also elect a Lead Governor from among their number, normally for a three two year period. The Lead Governor is available for conversation and advice. The Chair of the Council of Governors, who is also Chair of the Board of Directors is available for one to one conversations, and holds regular meetings with relevant governors to discuss matters of interest or concern in Norfolk and Suffolk, respectively. Any governor is also welcome to contact the Trust’s Company Secretary for informal information or advice about any aspect of the work of the Trust, the Constitution, the role of governors or wider corporate governance queries.
ii. Objective setting and appraisals
The role of the CoG is first to define the process for objective setting and evaluating the performance of the Chair and, in consultation with the Chair, the NEDs and second, to be assured that it has been followed. The Nominations Committee oversees this on behalf of the CoG and reports the outcomes of the appraisals to the full CoG for approval. In line with NHSI’s Code of Governance, the Senior Independent Director carries out the Chair’s appraisal and the Chair carries out the NEDs’ appraisals. The process followed is overseen by the Nominations Committee in both cases. As part of the appraisal process, governors are invited to provide confidential feedback on the performance of the Chair and NEDs. This is the formal point at which governors reflect on the performance of the Chair and NEDs as they have seen them operate during the year, for example at the meetings of the CoG, the BoD and its committees or the P&P Subgroup, and provide their feedback on their performance.
iii. Promoting good relationships
Effective relationships between governors and directors are promoted by all parties:
Page 9 of 12

• Acknowledging that governors and directors have the same goals but
different responsibilities.
• Accepting that constructive tension is required in any accountability structure and that an effective relationship is neither cosy nor adversarial.
• Fulfilling but not exceeding their remits.
• Working to common solutions rather than insisting on a single answer.
iv. Resolving disagreements between the Board of Directors and the Council of Governors The Chair, in liaison with the Lead Governor and the Senior Independent Director, will facilitate discussions between the two Boards to resolve any disagreements. An informal approach to resolving disagreements will usually be sufficient and the requirements will depend on the matter under consideration. It may consist of ensuring that further information is made available (for example, where there is a disagreement over the basis for a decision) or taking legal advice where there is a question over interpretation of responsibilities. Where an informal approach does not resolve the matter to the satisfaction of the governors and a motion is passed by two thirds of the Council of Governors to call a Resolution Meeting then this will be arranged as soon as practical, but no later than 20 working days after the motion. A Resolution Meeting is a joint meeting (of the CoG and BoD) held in private. The agenda and papers will be issued in line with the Trust Constitution and quoracy requirements for both Boards apply. The Chair may choose to invite a facilitator to the meeting. All participants will make every effort to resolve the matter, but if the issues cannot be resolved to the satisfaction of both boards (by a simple majority vote of those present from each board separately) then the final decision rests with the Board of Directors. The Council of Governors may then decide to escalate the matter to the Panel for Advising Governors (established by the Health and Social Care Act (2012)) or through the lead governor to Monitor in relation to a potential breach of the terms of its licence.
v. The role of the lead governor The lead governor is the main contact point for NHSI (although any governor may contact NHSI if they feel this is appropriate). The lead is elected by governors through a secret ballot. The role is set out in full in the role profile (available separately).
Page 10 of 12

Robert Nesbitt
Company Secretary 13.11.17
Page 11 of 12

Local People
Quality Governance Ctte
KEY
Board of Directors
Council of Governors
Performance and Finance Ctte
MHA Hosp Mgrs Ctte
Nominations Ctte Planning & Performance
Trust Governor and Member Development
SU & Carer Trust Partnership
Drugs and Therapeutics Grp
Research Governance Grp
Infection Prev. & Control Ctte
Safeguarding Group
MH Law Forum
H&S Grp
Clinical Effectiveness &
Policy Group
Equality and Diversity Group
Locality / Service Governance
Groups
Executive Team Information Gov Sub-Ctte
Trust Partnership Meeting / LNC
Clinical Cabinet CoG Group
BoD Ctte
Operational
bod cog ctte and subgroup structure 12nov2017.docx
Reporting
Consulting / Liaising
Professional education groups
Remuneration Ctte
Audit & Risk Ctte
OD and Workforce Ctte
Charitable funds
Committee structure at Nov 2017
Medical Staff Ctte
Improvement Plan Coordination Subgroup
Physical Health Strategy Group
Mortality Review Group Preventing death
by suicide
Perf Accountability Review Meeting
Programmes (e.g. MBU)
Quality Programme Board

Guide to committee and group governance structure diagram (November 2017)
Name of group Notes Council of Governors Constituencies (elected governors): Public Suffolk (5), Public
Norfolk (6), Staff (4), Service User Suffolk (2), Service User Norfolk (2), Carer Suffolk (1), Carer Norfolk (1). Partner governors include Suffolk and Norfolk County Councils.
Council of Governor Subgroups and Committees: Nominations Committee NED / Chair appointment, remuneration and appraisal
oversight. Planning and Performance Subgroup
Bi-monthly holding NEDs to account subgroup of governors meeting.
Trust governors and member development subgroup
Quarterly subgroup of governors meeting to assess governors’ training needs, plan training and development, and plan member recruitment and engagement events.
Improvement Plan Subgroup (from Feb 2017)
Subgroup of the Planning and Performance Subgroup, meeting prior to the P&P meeting from Feb 2017. Main focus is on quality improvement plans and committee observations.
Name of group Notes Board of Directors Meets in public 10 times a year (not August or December). Remuneration Committee Quarterly NED committee with CEO makes executive director
appointments, sets remuneration for exec and senior management, keeps oversight of appraisals.
Performance and Finance Committee
10 times a year (not August or December) committee with delegated authority for investment appraisal and financial monitoring and assurance.
Quality Governance Committee 10 times a year (not August or December) committee oversees all aspects of quality aligned to safe, effective, responsive, caring, well-led.
Organisational Development and Workforce Committee
Quarterly committee oversees leadership and culture, resourcing / flexible workforce, workforce development
Audit and Risk Committee Quarterly NED meeting oversees governance, risk management, financial and quality accounts, internal and external audit and system controls.
Hospital Managers Committee Quarterly meeting of MHA hospital managers, oversees practice, quality, recruitment of HMS and training and development. Produces annual report on its work to the BoD.
Charitable Funds Committee Twice yearly meeting. Oversees stewardship of funds and allocation in line with delegated authority.

Reporting operational groups
Name of group Notes Executive Team Meeting Weekly executive meeting which oversees performance,
strategy and policy matters. Performance Accountability Review Group
Monthly meetings chaired by the Director of Finance / Deputy CEO with locality managers to review KPI performance issues and identify plans to address where appropriate.
Trust Partnership Meeting / Local Negotiation Council
Staff / management consultative meetings. Monthly.
Information Gov Sub-Group Oversees and coordinates all aspects of information governance including data protection and IG toolkit requirements. Meets quarterly.
SU & Carer Trust Partnership Monthly coordinating umbrella group for service user and carer involvement local forums.
Clinical Cabinet Monthly meeting providing clinical review and oversight of Trust policy and initiatives as requested by the Executive Team and Board of Directors.
Quality Programme Board Weekly meeting for the delivery of the quality improvement plan.
Specific programmes Any programmes which do not report into the QPB (for example the Mother and Baby Unit) report directly to the executive team.
Medical Staff Ctte Reviews and oversees working conditions including training for doctors. Meets three times per year.
Locality / Service Governance Groups
Locally based quality groups that oversee and address quality issues aligned to safe, effective, responsive, well-led and caring.
Equality and Diversity Group Bi-monthly group with oversight of Equality Delivery Scheme (EDS). Include both service and workforce aspects.
Drugs and Therapeutics Committee
Clinically led group that reviews implementation of NICE guidance, alerts, best practice. Bi-monthly.
Clinical Effectiveness & Policy Group
Reviews and approves clinical policies including related documents such as leaflets. Monthly.
Health and Safety Group Quarterly meeting overseeing H&S concerns including incidents, themes, relevant CAS alerts.
Research Governance Group Carries out governance reviews each month to quality check proposals and approve / feedback for improvements. Meets monthly.
Infection Control and Prevention Group
Meets three times a year. Reviews and approves related policies and monitors compliance / safety issues.
Safeguarding Group Oversees Trust responsibilities for child and adult safeguarding. Meets quarterly.
Mental Health Law Forum Bi-monthly inter-agency forum that reviews and approves policy and monitors compliance with MHA administration requirements as well as MHA activity.
Physical Health Strategy Group Bi-monthly meetings progresses physical health strategy. Oversees compliance through audits including flu vaccination programme. Approves relevant policies.
Mortality Review Group Quarterly review of all deaths to identify themes and any causes

for concern. Preventing Death by Suicide Group
Bi-monthly to oversees development and delivery of the Trust’s internal suicide prevention strategy.

Report To: Board of Directors
Meeting Date: 30 November 2017
Title of Report: Freedom to Speak up – Year 1 review
Action Sought: For Assurance
Estimated time: 10 minutes
Author: Liz Keay: PPF Freedom to Speak up Guardian
Director: Dawn Collins: Director of Nursing, Quality and Patient Safety Executive Summary:
• This paper is an annual review of the Putting People First Freedom to Speak up Guardian role (FTSUG). It will provide members of the Board of Directors assurance that concerns raised are robustly managed in line with current best practice.
• It is also to benchmark our organisation against the principle recommendations set
out in Sir Robert Francis’ report in 2014 and the findings of the Freedom to Speak up Guardians National Survey
1.0 Background
1.1 The Freedom to Speak up Review undertaken by Sir Robert Francis was a result of the failings at Mid Staffordshire. The aim of this report was to provide advice and recommendations to ensure that NHS staff feel safe to raise concerns, be confident that they will be listened to and that concerns will be acted upon. The review concluded that there is a culture within many parts of the NHS which deters staff from raising serious and sensitive concerns and which has negative consequences for some of those who do raise them.
2.0 Management of FTSU cases
2.1 Employees can raise their concerns in person, by phone or in writing. Their concerns can be handled confidentially or openly depending on their preference. Anonymously raised concerns will be dealt with in the same manner as any other concern however there will be no feedback possible to the originator. All concerns are recorded on a password protected spreadsheet which includes actions and updates as appropriate. Formal guidance as to the process of raising a concern
Date: 30 November 2017 M Item: 17.188ii
Board of Directors - 30th November 2017 Freedom to Speak up Guardian’s Report
Version 0.1
Author: Liz Keay Department: Governance / HR
Page 1 of 9 Date produced: 16/10/17 Retention period: 20 years

can be found in the Speak up Safely policy. There is also an information leaflet for those wanting to raise a concern and one in the process of being written as guidance for those receiving a concern via the FTSUG.
2.2 The FTSUG will guide staff to existing internal processes and/or mechanisms such as the Resolution Policy or the Dignity and Respect policy for matters around employee relations
2.3 Since the pilot and subsequent substantive appointment of the FTSUG, Liz Keay there have been 42 concerns raised, ranging from ones which involved a single conversation after which the individual felt they could take the matter forward themselves to ones involving more lengthy, formal investigation.
2.4 Central Norfolk staff have raised the highest number of concerns, 14. It is felt that this is because the FTSUG is located in Norwich and will see people on a more regular basis which might prompt them to report more frequently. Whilst there has been communications and visits undertaken, more needs to be done to inform staff of this role. There is an ongoing plan in place for the FTSUG to visit different locations to continue to raise awareness of the role
2.5 Staff have raised 19 concerns in confidence and openly raised concerns are slightly higher at 20. This would indicate that confidence to report concerns safely is sound however we should continue measures to assure staff that they will not suffer detriment for doing so.
2.6 The themes of concerns raised are:
Attitudes and behaviours 12 Infrastructure and environment 0 Staffing levels 6 Staff Safety 0 Bullying and harassment 5 Systems, procedures and processes 2 Patient safety and quality 7 Patient experience 5 Performance capability 3 Service change 0 Leadership and management issues 1 Other 1
Informally it feels like there is a lot of talk around how we work together which feeds into the OD work that sits alongside the Guardian work. It is encouraging that people feel they can raise patient experience/safety issues and have the confidence that they will be listened to and acted upon
Board of Directors - 30th November 2017 Freedom to Speak up Guardian’s Report
Version 0.1
Author: Liz Keay Department: Governance / HR
Page 2 of 9 Date produced: 16/10/17 Retention period: 20 years

2.7 Feedback from people using the FTSUG service has been positive however more
formal feedback will be sought once the standard questions set has been received from the national office
“As you know I raised a concern, not only did I feel listened to, Liz communicated with me at all the stages.” “Thank you so much for all your support, it has been invaluable.” “From personal experience it’s probably one of the first times I`ve felt listened too so thank you” “Just seen your official appointment to post, well done definitely a good choice by the Trust”
3.0 Benchmarking against the principles raised in Sir Robert Frances’ Report
3.1 The review created 20 principles under 5 overarching themes with actions for NHS organisations locally and nationally to help foster a culture of safety and learning in which all staff feel safe to raise a concern. The 5 themes are:
• Culture change • Improved handling of cases • Measures to support good practice • Particular measures for vulnerable staff groups • Extending the legal protection
3.2 Of the 20 principles, 13 are specifically related to our Trust. The following table benchmarks us against these recommendations and identifies further actions/next steps.
Principle Recommendation from Francis report
What NSFT has in place
Further action/next steps
Culture Change
1. Culture of Safety
Every organisation involved in providing NHS Healthcare should actively foster a culture of safety and learning in which all staff feel safe to raise concerns
Datix entries FTSUG in post Risk Register Dignity and Respect policy Speak out Safely policy
2. Culture of raising concerns
Raising concerns should be part of the normal routine business of any well-led NHS organisation
Michael’s listening Roadshow Dignity and Respect policy Speak out Safely policy
Further listening sessions Continue communications encouraging speaking up
3. Culture free from bullying
Freedom to speak up about concerns depends on staff being
Dignity and Respect policy
Implementation and education of refreshed policies
Board of Directors - 30th November 2017 Freedom to Speak up Guardian’s Report
Version 0.1
Author: Liz Keay Department: Governance / HR
Page 3 of 9 Date produced: 16/10/17 Retention period: 20 years

able to work in a culture which is free form bullying and other oppressive behaviours
4. Culture of visible leadership
All NHS should demonstrate, through visible leadership at all levels in the organisation, that they welcome and encourage the raising of concerns by staff
Exec visits to teams and localities MMM and Julie’s Journal Email Michael and Ask Julie
CEO weekly blog CEO monthly live webinars Team visits by Execs and senior managers
5. Culture of valuing staff
Employers should show that they value staff who raise concerns and celebrate the benefits for patients and the public from the improvements made in response to issues raised
Datix system Publicising a summary of action taken following concerns that have been raised, subject to confidentiality
6. Culture of reflective practice
There should be opportunities for all staff to engage in regular reflection of concerns in their work
Reflective practice is already an integral part of revalidation for registered healthcare professionals
Ensure all staff have supervision and the opportunity to participate in reflective practice in a team or individual environment
Handling Cases
7. Raising and reporting concerns
All NHS organisations should have structures to facilitate both informal and formal raising and resolution of concerns
MDT meetings Speak out Safely policy Supervision
Further communications about speaking out safely with reinforced messages from managers
8. Investigations When a formal concern has been raised, there should be prompt, swift, proportionate, fair and blame free investigations to establish the facts
Investigation procedure is set out in the Speak out Safely policy Investigation training for staff
Ensure internal investigations are undertaken promptly and swiftly. Feedback should be given to the individual raising the concern
9. Mediation and dispute resolution
Consideration should be given at an early stage to the use of expert interventions to resolve conflicts, rebuild trust or support staff who have raised concerns
Internal facility for mediation
Consider training more staff in mediation
Measures to Support Good Practice
Board of Directors - 30th November 2017 Freedom to Speak up Guardian’s Report
Version 0.1
Author: Liz Keay Department: Governance / HR
Page 4 of 9 Date produced: 16/10/17 Retention period: 20 years

10. Training Every member of staff should receive training in their organisation’s approach to raising concerns and in receiving and acting on them
FTSU principles are introduced to all new staff at induction Staff are made aware of the FTSUG role in both Safeguarding and Equality and Diversity training
Consider FTSUG input into the leadership and investigation training
11. Support All NHS organisations should ensure there is a range of persons to whom concerns can be reported easily and without formality. They should provide staff who raise concerns with ready access to mentoring, advocacy, advice and counselling
The Speak up Safely policy identifies a number of individuals and organisation with whom concerns can be raised
Republish contact details in Trust Update and other newsletters
13. Transparency All NHS organisations should be transparent in the way they exercise their responsibilities in relation to raising concerns, including the use of settlement agreements
Trust values and behaviours
Publish qualitative and quantitative data about formally raised concerns in the Quality Account
14. Accountability Everyone should expect to be held accountable for adopting fair, honest and open behaviours and practices when raising or receiving and handling concerns
Trust values and behaviours Values based recruitment
Continue to embed the values across the Trust
4.0 Freedom to Speak up Guardians’ National Survey
See appendix 1 for full report on the results of the survey. The following is a high level summary of the results. The observations are based on a national results and the recommendation relate to our Trust
4.1 Who is in the role?
Most FTSUGs do this role alongside another and the staff group most represented is nurses at 23% although there is a broad range of professional backgrounds. Currently FTSUGs are predominantly middle aged, white, heterosexual females without a disability
Observations Board of Directors - 30th November 2017 Freedom to Speak up Guardian’s Report
Version 0.1
Author: Liz Keay Department: Governance / HR
Page 5 of 9 Date produced: 16/10/17 Retention period: 20 years

• The variety of professional backgrounds and banding is a strength • Having another role brings the potential for conflict and may be a barrier to
people speaking up • The lack of demographic diversity may also present a barrier to people
speaking up and does not provide assurance that the needs of black, minority or ethnic staff or vulnerable groups are catered for
Recommendations • Be aware of potential conflicts • Develop working relationships with local diversity groups • Appointment to the guardian role should be done in an open and transparent
way
4.2 Activity
88% of FTSUGs have measures in place to communicate about their role internally to their organisation. The focus for most, NSFT included, is around involvement in the induction and training processes and attending team meetings. Feedback is currently obtained informally for those who have used the service.
Observations • FTSUGs are involved in a wide variety of communication, training and other
activities, and developing a broad range of partnerships • Gathering feedback is not universal
Recommendations • The next challenge will be keeping momentum and keeping messages fresh • Ensure messages and language are consistent • Gather feedback from those who are speaking up to you, your senior team,
your partners, and others • When gathering feedback from people who speak up use the standard
question set out by the NGO (Awaiting receipt of these)
4.3 Implementation - time
51% of guardians don’t have any ring fenced time to perform this role and whilst 38% of guardians feel they have enough time to perform their duties the higher the proportion of time allocated sees an increase in the confidence they are meeting the needs of their organisation
Observations Board of Directors - 30th November 2017 Freedom to Speak up Guardian’s Report
Version 0.1
Author: Liz Keay Department: Governance / HR
Page 6 of 9 Date produced: 16/10/17 Retention period: 20 years

• The guardian job is a big one and time is needed to do it • Ring-fenced time gives confidence to guardians and champions that they can
meet the need of their staff • The amount of time should be driven by the needs of your staff and needs of
your trust
Recommendations • Guardians need ring-fenced time for the role – For our Trust the way the role is
structured alongside organisational development work is allowing for the flexibility to be reactive to concerns raised
4.4 Implementation - budget
The vast majority of guardians do not hold, or have access to, a specific budget. Whilst our Trust also doesn’t have a specific budget, access to funds is through the HR department subject to approval of spend.
Observations • Many communications and other activities can probably be undertaken without
a specific budget • Guardians should be able to work with other teams to promote and embed
Freedom to Speak Up • Guardians should also be able to bid for funding locally for particular work that
they wish to undertake
Recommendations • Trusts need to provide guardians with access to the budget they need to
address the needs of workers in their trust
4.5 Support
There has been excellent support for guardians from CEOs and senior management which is also true for our organisation.
Observations • There is widespread support from senior leaders for Freedom to Speak Up
Recommendations • Support should continue, with leaders role-modelling their commitment to
Freedom to Speak Up
Board of Directors - 30th November 2017 Freedom to Speak up Guardian’s Report
Version 0.1
Author: Liz Keay Department: Governance / HR
Page 7 of 9 Date produced: 16/10/17 Retention period: 20 years

• Guardians should meet with their chief executive and responsible non-
executive director regularly • Guardians should report to their board regularly, in person
4.6 Perceptions
Results indicate that the level of perception that an organisation is open to people speaking up is in direct correlation with the CQC rating of that organisation.
Observations • The perceptions of guardians and champions are a valuable insight into
Freedom to Speak Up culture • The apparent correlation between Care Quality Commission rating and
respondents’ answers is interesting but not conclusive
Recommendations • Overall, these responses indicate that there is a way to go before speaking up
becomes business as usual
5.0 Financial implications (including workforce effects)
5.1 There are no financial implications from this report
6.0 Quality implications
6.1 By implementing a continuing communications and engagement plan, staff will become more familiar with the service and more inclined to report concerns with the ultimate aim of making speaking up business as usual and maintaining/improving the quality of the service we offer our patients, families and carers
7.0 Equality implications / summary of consultation
7.1 It is noted that statistically BME staff members are particularly vulnerable to suffering detriment after speaking up. The FTSUG attends the Equality Leads meeting and BME network meetings on a regular basis. Further work to engage these members of staff is required
8.0 Risks / mitigation in relation to the Trust objectives
8.1 Strategic Objectives 1. Improving quality and achieving financial stability
• Delivering a reliable data set to monitor performance and give assurance
Board of Directors - 30th November 2017 Freedom to Speak up Guardian’s Report
Version 0.1
Author: Liz Keay Department: Governance / HR
Page 8 of 9 Date produced: 16/10/17 Retention period: 20 years

8.2 Board Assurance Framework
1a.1 The inability to recruit sufficient staff with appropriate qualifications could affect staff morale and patient care. • When staff feel listened to a safe to raise concerns within the organisation,
retention rates will improve, response rates to staff survey and FFT will increase and word of mouth encouragement to join the organisation is more prevalent
9.0 Recommendations
9.1 That members of the Board of Directors note the contents of this report
Liz Keay Freedom to Speak up Guardian Background Papers / Information Appendix 1. Results of the National Guardian’s office survey
Board of Directors - 30th November 2017 Freedom to Speak up Guardian’s Report
Version 0.1
Author: Liz Keay Department: Governance / HR
Page 9 of 9 Date produced: 16/10/17 Retention period: 20 years

National Guardian Freedom to Speak Up
What are Freedom to Speak up Guardians?
Russell Parkinson
2017 Freedom to Speak Up Guardian Survey Recommendations

Today’s webinar
1. First ever Freedom to Speak Up Guardian Survey – its key findings
2. How the National Guardian’s Office is responding to them
3. What implications will the recommendations have?
4. Answering your questions

2017 Freedom to Speak Up Guardian Survey
Took place 12 – 30 June 2017
493 requests sent 234 responses received 47% response rate
Anonymous (cannot identify individuals / trusts) Sent to guardians / ambassadors / champions – no distinguishing between these groups No statistical analysis of
the results has taken place Some potential trends indicated but numbers of responses in some groups involved are small

Who is in the guardian role?
Professional background % respondents
Nurse 23%
Corporate Services 18%
Allied Healthcare Professional 11%
Administrative / Clerical 7%
Human Resources 6%
Organisational Development 6%
Governor 6%
Doctor 5%
Safety 4%
Midwife 2%
Chaplaincy 2%
Healthcare Assistant 1%
Therapist 1%
Maintenance / Ancillary 0.5%
Other* 28%
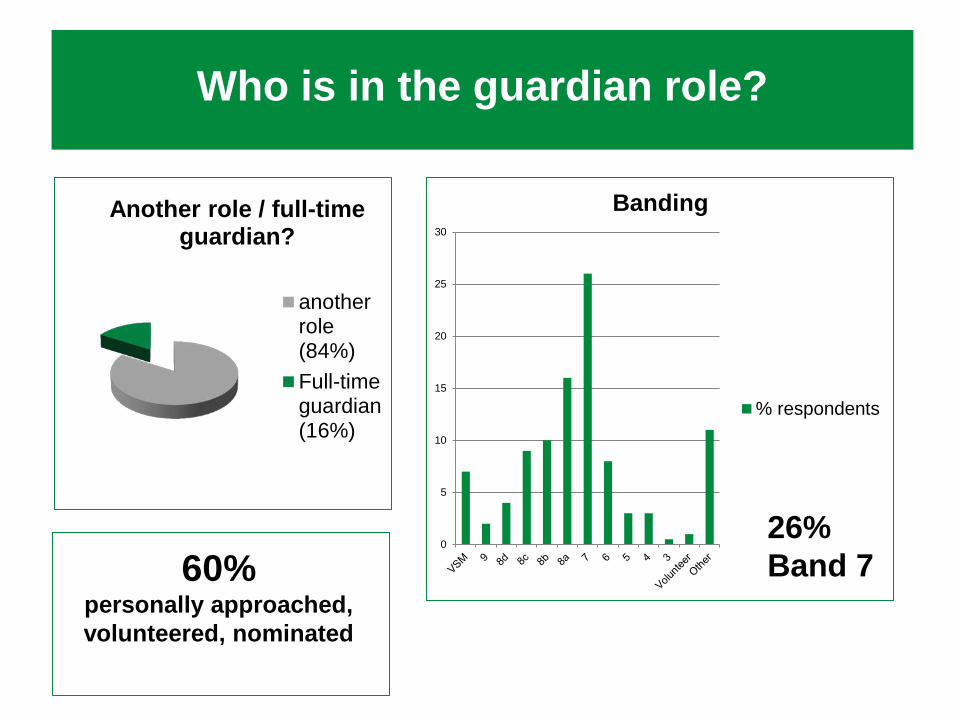
Who is in the guardian role?
Another role / full-time guardian?
anotherrole(84%)Full-timeguardian(16%)
0
5
10
15
20
25
30
Banding
% respondents
60% personally approached, volunteered, nominated
26% Band 7

Demographics
79% female 91%
white
91% do not consider themselves to
have a disability
44% Aged
45 – 54
88% Straight /
heterosexual

Who is in the role - conclusions
Observations • The variety of professional backgrounds and banding is a strength • Having another role brings the potential for conflict and may be a barrier
to people speaking up • The lack of demographic diversity may also present a barrier to people
speaking up and does not provide assurance that the needs of black, minority or ethnic staff or vulnerable groups are catered for
Recommendations • Be aware of potential conflicts • Develop local networks or other means to help navigate around
conflicts, introduce diversity, and extend ‘reach’ • Develop working relationships with local diversity groups • Appointment to the guardian role should be done in an open and
transparent way

Who is in the role - conclusions

What you are doing
Activity % respondents Communication of role internally 88% Communication of role externally 11% Involvement in staff induction 62% Involvement in other staff training 52% Attending team meetings 65% Carrying out surveys 16% Other* 25%
Partnership % respondents Senior leaders / the board 83% HR 82% Organisational development teams / similar 50% Communications teams 73% Training and development teams 49% Unions / staff-side 54% Staff diversity networks 36% Patient representative groups 18% Internal audit 15% Other* 15%
A broad range of activities and partnerships
46% Gathered
feedback on their performance

What you are doing
Observation • You are involved in a wide variety of communication,
training and other activities, and developing a broad range of partnerships
• Gathering feedback is not universal
Recommendations • Keep it up • The next challenge will be keeping momentum and
keeping messages fresh • Ensure messages and language are consistent • Gather feedback from those who are speaking up to you,
your senior team, your partners, and others • When gathering feedback from people who speak up use
the standard question set out by the NGO

What you are doing

Implementation - time
0
10
20
30
40
50
60
None 0.5 days 1 day 2 days 3 days 4 days 5 days
Ring-fenced time
% respondents
Sufficient time to carry out the role appropriately for my organisation
% respondents
Strongly agree 12% Agree 26% Neither agree nor disagree 25% Disagree 30% Strongly disagree 8%
51% No ring-fenced
time

Implementation - time
Ring-fenced time for guardian role
Sufficient time to carry out the role appropriately for my organisation (agree/strongly agree)
None 26% Up to 0.5 days per week 38% Up to 1 day a week 32% Up to 2 days a week 47% Up to 3 days a week 48% Up to 4 days a week 100% Up to 5 days a week 100%
Ring-fenced time for guardian role
Confident I meet the needs of staff in my trust (agree/strongly agree)
None 36% Up to 0.5 days per week 31% Up to 1 day a week 36% Up to 2 days a week 43% Up to 3 days a week 50% Up to 4 days a week 100% Up to 5 days a week 64%

Implementation - time
Observations • The guardian job is a big one and time
is needed to do it • Ring-fenced time gives confidence to
guardians and champions that they can meet the need of their staff
• The amount of time should be driven by the needs of your staff and needs of your trust
Recommendation • Guardians need ring-fenced time for
the role

Implementation - budget
Budget for Freedom to Speak Up activities % respondents
There is no specific budget set aside 67% Less than £500 1% Over £500 but less than £1,000 1% Over £1,000 but less than £2,000 1% Over £2,000 but less than £5,000 3% Over £5,000 but less than £10,000 2% Over £10,000 1% Don’t know 24%
I have access to the budget I need % respondents
Strongly agree 8% Agree 20% Neither agree nor disagree 44% Disagree 21% Strongly disagree 8%

Implementation - budget
Observations • Many communications and other activities can probably be
undertaken without a specific budget • Guardians should be able to work with other teams to
promote and embed Freedom to Speak Up • Guardians should also be able to bid for funding locally for
particular work that they wish to undertake
Recommendation • Trusts need to provide guardians with access to the budget
they need to address the needs of workers in their trust

Support
“My senior management team supports me”
“My chief executive supports me”
Agree / strongly agree 81% 85%
Neither agree nor disagree 16% 12%
Disagree / strongly disagree 3% 3%
‘I have access to the support I need’ % respondents
Strongly agree 34% Agree 44% Neither agree nor disagree 15% Disagree 8% Strongly disagree 0%

Support
CQC rating “My senior management team supports me” (agree / strongly agree)
“My chief executive supports me” (agree / strongly agree)
Outstanding 92% 92% Good 84% 89% Requires improvement 83% 84% Inadequate 54% 64%
CQC rating “I have access to the support I need” (agree/strongly agree)
Outstanding 92% Good 77% Requires Improvement 77% Inadequate 72%
55% present board reports in person

Support
Observation • There is widespread support from senior leaders for
Freedom to Speak Up
Recommendations • Support should continue, with leaders role-modelling their
commitment to Freedom to Speak Up • Guardians should meet with their chief executive and
responsible non-executive director regularly • Guardians should report to their board regularly, in person

Support

Perceptions
• most likely to respond positively : • ‘My organisation sees speaking up as an opportunity to learn and
improve’ (75% agreed) • ‘There are significant barriers to speaking up in my organisation’ (only
25% agreed) • least likely to respond positively :
• ‘Managers support staff to speak up’ (41% agreed)
• more positively responses from trusts with higher CQC ratings • most marked difference between higher and lower rated trusts:
• ‘Managers support staff to speak up’ (59 percentage point difference between outstanding and inadequate trusts (77% vs 18%))
• mental health services tended to be the most positive • ambulance trusts tended to be the least positive.

Perceptions
0 20 40 60 80
My organisation sees speaking up as anopportunity to learn and improve
My organisation has a positive culture ofspeaking up
Managers support staff to speak up
There are significant barriers to speaking up inmy organisation
% agree

Perceptions
0 5 10 15 20 25 30 35 40 45 50
Outstanding
Good
Requires improvement
Inadequate
Significant barriers to speaking up in my organisation?
% agree
0 20 40 60 80 100
Outstanding
Good
Requires improvement
Inadequate
Managers support staff to speak up
% agree

Perceptions
Managers may be a particular
barrier
Apparent correlation between Care Quality
Commission rating and respondents’ answers is
interesting but not conclusive
These results act as a baseline and our ambition
is that responses will improve overtime

Perceptions
Observations • The perceptions of guardians and champions are a valuable insight into
Freedom to Speak Up culture • There were some positive responses, and some less positive • It may be too early in the journey for guardians and champions to have a
definite opinion about some of the questions we asked • Managers may be a particular barrier • The apparent correlation between Care Quality Commission rating and
respondents’ answers is interesting but not conclusive
Recommendations • The opinions of guardians and champions are important and we will
continue to ask for your thoughts on Freedom to Speak Up culture • These results act as a baseline and our ambition is that responses will
improve overtime • Overall, these responses indicate that there is a way to go before
speaking up becomes business as usual

National Guardian’s Office
0 5 10
How do guardians rate the support provided by the
office (out of 10)? 5.7 (average)

Further support requirements
More training
More networking and other events
Greater clarity about the guardian role,
more standardisation
Guidance about particular
aspects of the role
Easier contact with the National Guardian’s
Office, swifter responses

Summary of our recommendations

Report To: Board of Directors – Public
Meeting Date: 30 November 2017
Title of Report: Quality Governance Committee Chairs report - 14th November 2017
Action Sought: For Assurance
Estimated time: 10 minutes
Author: Gary Page – Non-Executive Director Executive Summary: The report provides an update to the Board on issues reviewed by the Trust’s Quality Governance Committee on 14th November 2017. Assurance review
Issue reviewed by committee
Commentary (including actions where required) Level of assurance
Quality Dashboard The Dashboard was reviewed. A discussion took place on Long Term Segregation and Seclusion and the Committee was advised that a Revised proposal would be made on how Long Term Segregation is recorded given the lack of clarity in the guidelines. It was emphasized that this needed to also provide assurance that our recording of seclusion met guidelines. Work is underway on a revised Quality dashboard which will come to the December meeting. Concern was expressed at the continuing findings around the inadequacy of Care Plans following CQC MHA visits. This issue was acknowledged and assurance provided that it would be addressed as part of the CQC Action Plan.
AMBER
Restrictive interventions Strategy
A revised Restrictive Interventions strategy has been discussed by the Executive but it was agreed prior to the QGC meeting that it would not come for formal sign off as there was still work to do. The Committee requested greater clarity around what was being measured in which service line and for baseline data to be available so it was clear what the trend was and also what our targets
RED
Date: 30 November 2017 N Item: 17.188iii
Board of Directors – Chair’s report on QG Committee
Version 1.0
Author Gary Page Department: Corporate
Page 1 of 3 Date produced: 20th Nov 2017 Retention period: 20 years RED = significant gaps and not assured on adequacy of action plans
AMBER = Gaps in assurance but assured appropriate plans in place to address
GREEN = No gaps in assurance

should be. Lorenzo We were advised that the next release (v2.12)
would fix 50 of our known performance issues. This led to a discussion on the remaining number of performance issues that exist which are outside of our Control. After the meeting I was advised that there are 135 outstanding issues on the national dashboard, 23 of which were fixed in the 2.11 release but 62 will remain outstanding after the 2.12 release. This was raised with NHSI in the Performance Meeting and assistance was requested.
RED
Physical Health Update
We received the quarterly Update. A discussion took place about the fact that some clinicians felt the recently agreed Physical health strategy was too ambitious because we did not have the resources to deliver and that it could jeopardise the improvements required by the CQC in this area. The Medical Director was asked to follow this up outside of the meeting and report back to the next meeting.
RED
Themed Learning A paper was received outlining a move towards themed learning from Serious Incidents. This is based on best practice and how many Safeguarding Boards seek to learn from incidents. It was emphasized that the responsibility for embedding Learning has to sit with the front Line. This will go live from December 1.
AMBER
NICE Annual report We received the NICE Annual Report. Reference was made to the process whereby Clinical Cabinet determines what guidelines apply to NSFT but locally Lead Clinicians can decide what is locally appropriate and prioritise accordingly. This appeared in conflict with good practice and the One Trust strategy. This will be followed up by the Chair and Medical Director outside of the Meeting.
AMBER
Service User Experience Report
The Report included the results of the 2017 Community Survey which showed continued improvement year on year with only 2 of the 32 measures showing a deterioration. Full analysis will come to the Board in due course. The report triangulated data from various sources and issues with Access to Services, especially at times of crisis features prominently.
AMBER
Research Report An Internal Audit Report on the Research Department concluded that there was significant assurance around the processes and controls used in the day to day management of Research projects. There were some low rated recommendations around frequency of reporting to the Board and how activities are coordinated to
GREEN
Board of Directors – Chair’s report on QG Committee
Version 1.0
Author Gary Page Department: Corporate
Page 2 of 3 Date produced: 20th Nov 2017 Retention period: 20 years RED = significant gaps and not assured on adequacy of action plans
AMBER = Gaps in assurance but assured appropriate plans in place to address
GREEN = No gaps in assurance

maximise benefits Recommendations The Board is asked to note the highlighted issues. It has also been agreed that following the adoption of the new Terms of Reference Marion Saunders will replace me as Chair of the Committee from the next meeting. As previously advised Tim Newcomb will also be joining the Committee as from January ensuring that we will continue to have three NEDS in attendance. Gary Page Chair of Finance Committee 20 November 2017
Board of Directors – Chair’s report on QG Committee
Version 1.0
Author Gary Page Department: Corporate
Page 3 of 3 Date produced: 20th Nov 2017 Retention period: 20 years RED = significant gaps and not assured on adequacy of action plans
AMBER = Gaps in assurance but assured appropriate plans in place to address
GREEN = No gaps in assurance

Report To: Board of Directors – Public
Meeting Date: 30 November 2017
Title of Report: Chair’s report of Charitable Funds Committee
Action Sought: For Assurance
Estimated time: 5 Mins
Author: Tim Stevens, Chair of Committee and Non-Executive Director
Director: Tim Stevens, Chair of Committee and Non-Executive Director Executive Summary: The Trust’s Charitable Funds Committee met on 26 October 2017 and agreed a number of matters for reporting to the Board: Assurance review
Issue reviewed by committee
Commentary (including actions where required) Level of assurance
Norfolk and Suffolk NHS Foundation Trust Charitable Funds the
2016-17 Annual Report and Accounts
The 2016-17 Annual Report and Accounts were approved by the Committee. These will be formally submitted to the Board for approval by the Director of Finance on 25 January 2018.
N/A
Investment Opportunities
The Committee agreed that there were no agreeable investment opportunities to consider. N/A
Terms of Reference The Terms of Reference were reviewed and it was agreed that the quorum should be amended from two to three Committee members. Subject to the amendment above, the Terms of Reference were approved by the Committee.
N/A
Recommendations The Board of Directors is asked to note the report Tim Stevens: Chair, Charitable Funds Committee 22 November 2017
Date: 30 November 2017 O Item: 17.188iv
BoD - 30 November 2017 CF Committee Chair’s Report
Version 1.0 Author: Tim Stevens Department: Corporate
Page 1 of 1 Date produced: 22 November 2017 Retention period: 20 years

Report To: Board of Directors – Public
Meeting Date: 30 November 2017
Title of Report: Chair’s report OD&W Committee 13 November 2017
Action Sought: For Assurance
Estimated time: 5 minutes
Author: Jill Robinson: Non-Executive Director
Director: Assurance review Issue reviewed by
committee Commentary (including actions where required) Level of
assurance Risk Register Concern was expressed that the report accompanying
the risk register spreadsheet had not changed since the last committee and did not provide the right information to assist the committee in prioritising risks for consideration. The committee again asked for a narrative report on high risks, and an evaluative commentary on mitigations, including other risks by exception e.g. where deteriorations is evident, with appropriate explanation and plans. The committee made clear it required the spreadsheet to be up to date and expected EDs to be well prepared to answer questions on the risks they own. The committee is not assured that the risk register is being used effectively.
RED
Appraisal rates Appraisals remain below target with some services below 70% completed. Where this is due to inadequate reporting, additional clerical support may improve performance.
RED
Supervision rates No additional assurance was provided in support of the theory that supervision was being undertaken but not recorded, although we heard some anecdotal examples of difficulties in recording. Unverified October data suggested rates had risen to 36% but the committee agreed that progress was inadequate. Appointment of clerical support for CTLs was in progress and it was expected that significant improvement would be seen by January 2018.
RED
Mandatory training Deterioration evident overall but of concern is the deterioration in most localities across 4 of the 6 areas considered crucial for patient safety. The committee
RED
Date: 30 November 2017 P Item: 17.188v
BoD 30 November 2017 OD&W Chair’s Report
Version 1.0
Author: Jill Robinson Department: Corporate
Page 1 of 2 Date produced: 14 November 2017 Retention period: 20 years RED = significant gaps and not assured on adequacy of action plans
AMBER = Gaps in assurance but assured appropriate plans in place to address
GREEN = No gaps in assurance

expressed concern that the strategy for offering block training had been shelved owing to lack of support from managers and staff. The committee report described actions already seen by the committee in the past and presented no new strategy for improving performance. The Committee was therefore not assured that appropriate actions were in place to improve performance. The committee urged the team to consider adding the option of block training to increase opportunities and flexibility and pressed the importance of consequences for non-compliance.
Safe Staffing A safer staffing report was received which included data on fill rates drawing attention to areas where registered nurse fill rates fell below 70% in September. A verbal report of unverified data for October suggested fill rates had improved. In the absence of a better indicator, the committee agreed that registered nurse fill-rates would return to the dashboard. Several actions were in progress to improve recruitment including the use of an external partner to improve social media presence particularly targeted at registered band 5 staff and medical vacancies. The committee gained partial assurance from these actions and examples of impact but remain concerned about the continuing impact of vacancies and availability of temporary staffing.
AMBER
Staff retention The committee received a full report on staff retention. Generally staff retention is above average for the sector and a number of initiatives have been recognised externally as good practice. It was noted that our lowest retention rates were for some of our hardest to recruit roles e.g. Bands 5 and 6 but the committee was assured that the Trust’s retention strategy was effective.
GREEN
PG Medical Education
The committee was concerned that following a series of trainee complaints, the PG Deanery were not satisfied with arrangements for trainees in West Suffolk, and will re-visit on 16th November to review viability of the training rotation in that area. The DME assured the committee of the actions taken to improve the trainee experience in West Suffolk and has liaised with Deputy PG Dean at HEE regarding improvements made. The DME also reported worsening vacancy rates for CTs and predicts 10 vacancies out of 29 for February 2018. Several options for making up this shortfall are being actively considered.
AMBER
Author: Jill Robinson Title: Non-Executive Director Date: 14 November 2017
BoD 30 November 2017 OD&W Chair’s Report
Version 1.0
Author: Jill Robinson Department: Corporate
Page 2 of 2 Date produced: 14 November 2017 Retention period: 20 years RED = significant gaps and not assured on adequacy of action plans
AMBER = Gaps in assurance but assured appropriate plans in place to address
GREEN = No gaps in assurance