board of directors meeting€¦ · pg/sh . 18 april 2019 . dear colleague . a meeting of the board...
TRANSCRIPT

Board of Directors Meeting
Thursday, 25 April 2019 at 1:00 pm
Boardroom
University Hospital of Hartlepool

Glossary of Terms
Strategic Aims and Objectives Putting Patients First
• Improve outcomes, achieve performance targets • Effective planning • Develop new approaches that support recovery and wellbeing • Develop new services to meet peoples’ needs • Focus on research to improve services
Valuing Our People
• Promote and ‘live’ the NHS values within a healthy organisational culture • Develop, train and retrain our staff • Ensure a healthy work environment • Listen to the ‘experts’ • Encourage the future leaders
Transforming Our Services
• Deliver cost effective and efficient services, maintaining financial stability • Make better use of information systems and technology • Provide services that are fit for purpose and delivered from cost effective buildings • Ensure future clinical sustainability of services
Health and Wellbeing
• Promote and improve the health of the population • Promote health services through full range of clinical activity • Increase health life expectancy in collaboration with partners • Promote self-care

PG/SH 18 April 2019 Dear Colleague A meeting of the Board of Directors will be held on Thursday, 25 April 2019 at 1:00 pm in the Boardroom, University Hospital of Hartlepool. Yours sincerely
Paul Garvin Chairman
Agenda
Led by
1. (1.00pm) Apologies for absence Chairman 2. (1.00pm) Declaration of Interest Chairman 3. (1.00pm) Minutes of the meeting held on, 28 March 2019 (enclosed) Chairman 4. (1.05pm) Matters Arising Chairman Items for Information 5. (1.10pm) Chairman’s Report (enclosed) Chairman 6. (1.20pm) Chief Executive’s Report (enclosed) J Gillon 7. (1.30pm) Retrospective Approval of Documents Executed Under Seal (enclosed) J Gillon Strategic Management 8. (1.40pm) Capital Programme Performance 2018/19 (enclosed) N Atkinson

Performance Management 9. (1.50pm) Integrated Compliance and Performance Report (enclosed) L Taylor, J Lane A Sheppard & N Atkinson 10. (2.10pm) Integrated Compliance and Performance Year End
Report 2018/19 (enclosed) L Taylor 11. (2.20pm NHS Access Standards Gap Analysis (enclosed) L Taylor 12. (2.30pm) Gram Negative Bacteraemia Update Report (enclosed) J Lane 13. (2.40pm) Draft Revenue and Capital Budgets 2019/20 (enclosed) N Atkinson 14. (2.50pm) NHS National Staff Survey Results 2018 (enclosed) A Sheppard Governance 15. (3.00pm) Learning from Deaths Report (enclosed) D Dwarakanath
16. (3.10pm) Any Other Notified Business Chairman 17. Date of Next Meeting (Thursday, 30 May 2019, Boardroom, University Hospital of North Tees)

____________________ * voting member
North Tees and Hartlepool NHS Foundation Trust
Minutes of a meeting of the Board of Directors held on Thursday, 25 April 2019 at 1.00 pm
at the University Hospital of Hartlepool Present: Paul Garvin, Chairman* Chairman Brian Dinsdale, Vice-Chair / Non-Executive Director* BD Jonathan Erskine, Non-Executive Director* JE Steve Hall, Non-Executive Director* SH Kevin Robinson, Non-Executive Director* KR Rita Taylor, Non-Executive Director* RT Julie Gillon, Chief Executive* CE Neil Atkinson, Director of Finance* DoF Barbara Bright, Director of Corporate Affairs and Chief of Staff DoCA&CoS Deepak Dwarakanath, Medical Director* MD Graham Evans, Chief Information & Technology Officer CI&TO Julie Lane, Director of Nursing, Patient Safety and Quality* DoN,PS&Q Alan Sheppard, Director of Workforce DoW Lynne Taylor, Director of Performance and Planning DoP&P In attendance: Samantha Sharp, Personal Assistant (note taker) Posmyk Boleslaw, Chair, Hartlepool and Stockton CCG Judith Donkin, Non-Executive Director of Governing Body, Hartlepool and Stockton CCG / GP Peter Wilkinson, Hospital User Group (HUG) Representative Ruth Dalton, Head of Communications and Marketing Alan Smith, Elected Governor for Hartlepool BoD/3942 Apologies for Absence Apologies for absence were noted from Julie Parkes, DoO. The Chairman welcomed Peter Wilkinson to this meeting as the new Chair for the Hospital User Group. BoD/3943 Declaration of Interests There were no declarations of interest on open agenda items. BoD/3944 Minutes of the meeting held on Thursday, 28 March 2019
Resolved: that the minutes of the meeting held on Thursday, 28 March 2019 be confirmed as an accurate record.
BoD/3945 Matters Arising
a. BoD/3856a Healthcare User Group (HUG) Visits The DoN,PS&Q provided an update in respect to a visit by the Hospital User Group (HUG) to audiology and explained that she had escalated the concerns raised to the Director of Nursing at South Tees Hospitals NHS FT, who run the service. Once clarification and the current position was known, the DoN,PS&Q would attend a HUG meeting to provide an

2
update.
Resolved: (i) that, the verbal update be noted; and (ii) that, the DoN,PS&Q meet with HUG representatives following
clarification in respect to concerns raised regarding audiology. BoD/3946 Report of the Chairman A summary of the Report of the Chairman included:-
Consultant appointments: Dr Helen White, Consultant in Elderly Care; Dr Vineeth Cheruvalli, Consultant Paediatrician and Dr Madhu Podalakur, Consultant Paediatrician;
Discussions had taken place between the three Chairs from the Trust, County Durham and Darlington NHS FT and South Tees Hospitals NHS FT concerning the South Integrated Care Partnership and the role to be undertaken by the Integration and Transformation Director to examine potential organisational forms for the South. It had been agreed that each of the three Trusts would contribute 20% to the salary with NHS Improvement (NHSI) and the Integrated Care System (ICS) providing the remaining 40%. A Memorandum of Understanding would be drawn up between the Trusts, NHSI and ICS;
The Chairman had met with the new Regional Director for NHS Improvement and NHS England, Richard Barker to emphasise the good work being undertaken by the Trust and the commitment to wider system working. Resolved: that, the information be noted.
BoD/3947 Report of the Chief Executive A summary of the Report of the Chief Executive included:-
The Terms of Reference for the Tees Valley Health and Care Partnership had been agreed and key stakeholders were being briefed;
NHS Improvement and NHS England had appointed Prerana Issar to the role of Chief People Officer to ensure that the NHS in England had enough people, with the right skills and experience to deliver the improvements for patients set out in the Long Term Plan;
NHS England had launched the NHS Parliamentary Awards for 2019 with nominations closing on 26 April 2019. Local MPs were being encouraged to nominate individuals or organisations for an award;
A team from the Trust spoke at a National Maternity and Neonatal Health Safety Collaborative Learning Event where they presented findings surrounding their quality improvement achievements and work with local partners in developing a bespoke MatNeo Local Learning System to support the ambitions of maternity outcomes across the region;
The Trust was one of three organisations that had come together to launch an innovative apprenticeship programme to support better outcomes for residents across the region. The Integrated Health and Social Care Apprenticeship would focus on offering students the opportunity to develop their knowledge in a range of healthcare environments;
In response to a query raised by JE, Non-Executive Director, the CE explained that she was part of a national workforce group which would give her the opportunity to influence and raise the national profile of initiatives undertaken by the Trust. The Chairman highlighted that the Trust had provided a case study on its successful
3
recruitment of nurses which was included in a national publication and the DoN,PS&Q advised that a number of Trusts had been in touch to discuss this. The Chairman wished all potential nominees for a parliamentary award the very best of luck and highlighted that the Trust had its annual Shining Stars awards ceremony in June which gave the Trust the opportunity to acknowledge and reward staff for the work they do.
Resolved: that, the information be noted. BoD/3948 Retrospective Approval of Documents Executed Under Seal The CE requested retrospective approval for the sealing of the following document:
Document Date Sealed By
Licence to Assign Between:
1) North Tees and Hartlepool NHS Foundation Trust
And
2) Gentian (North Tees) Limited
And
3) Gentian Holdings Limited
In respect of Entrance Concourse Units, University Hospital of North Tees
3 April 2019
Mr N Atkinson, Director of Finance
Mrs B Bright,
Director of Corporate Affairs and Chief of Staff
(witness)
Resolved: that, the retrospective approval of the sealing of documents be granted.
BoD/3949 Capital Programme Performance 2018/19 The DoF provided an update in respect of the Capital Programme Performance for Quarter 4 2018/19. The allocation agreed for 2018/19 was £22.06m, which included a £8.82m internally generated depreciation, £12.7m loan for the major engineering infrastructure replacement scheme, £1.08m loan payback reduction to internally generated depreciation, £2.4m Public Dividend Capital (PDC) for Global Digital Exemplar Fast Follower, £0.92m energy centre retention spend anticipated in 2019/20 and £150k donated funds. NHS Improvement‟s compliance framework required Trusts to spend between 85% and 115% of the capital allocation on a monthly basis. At the end of Quarter 4, expenditure was £17.43m which was 79% of the Trust‟s planned spend. Provision had been made in the 2019/20 programme to recover this shortfall. The Major Engineering Infrastructure Replacement Scheme was now complete and costs remained below budget allocation with minimal disruption to clinical services. Work to replace the fire alarm system on the North Tees was slightly ahead of plan. In Quarter 4 work had commenced on site to refurbish lifts throughout the Trust. To address high backlog maintenance levels, a revised five year backlog maintenance plan had been developed. The revised plan was based on a £3.7m annual backlog allocation.

4
The four main workstreams; Medical Equipment, Digital/ICT, Service Development, and Estates Backlog Maintenance were performing to plan and the DoF provided an overview of each. The CI&TO provided an update in respect of ICT projects and recent developments to ensure that the Trust safeguards itself against potential threats. BD, Chair of the Audit Committee sought assurance that the programme to address backlog maintenance would consider identified risks and schedule maintenance as appropriate. The DoF confirmed that this was the case and would provide further detail and assurance at a future meeting. In response to a concern raised by the Chairman, the DoF confirmed that £3.7m was enough to keep pace with backlog maintenance requirements over the next five years but advised that there would always be a residual amount of backlog maintenance. RT, Non-Executive Director commended the work of the Trust in respect to technological advances and asked how engaged staff were with this. The CI&TO and MD both highlighted the positive engagement of staff and medics and explained how mind sets had changed over the past couple of years. The Chairman raised concern in respect to the amount of PDC drawn down linked to the Global Digital Exemplar Fast Follower Programme (£1.5m) and asked what the revenue consequence of this would be. The CI&TO explained that the business itself owned that part of the business case and that it was their responsibility to look at whether there were any revenue consequences.
Resolved: that, the position on capital schemes up to 31 March 2019 be noted. BoD/3950 Integrated Compliance and Performance Report BoD/3951 Integrated Compliance and Performance Year-End Report 2018/19 The DoP&P presented the Integrated Compliance and Performance Report for the month of March 2019 and Quarter 4 2018/19. As part of the update the key points of the year-end position were also included. Key points were:-
Single Oversight Framework: The majority of key access standards had been achieved in March and Quarter 4 and the Trust had performed relatively well against all national and local key indicators throughout 2018/19. Pressures remained around the cancer 62 day standards, however, provisional March and Quarter 4 reported a positive position. The aggregate provisional year-end position indicated that the Trust had narrowly underachieved against this standard reporting a year-end position of 84.53%. The Trust had exceeded the Emergency Care four hour standard, reporting in 1st position (March) nationally, one of only thirteen Trusts to achieve the standard. The Trust had regularly reported within the top ten nationally throughout 2018/19. The year-end position reported at 97.18%. The Trust under-achieved against the 99% diagnostic national standard reporting a year-end position of 98.69%, due to in year capacity issues, however the position was recovered in Quarter 4. All referral to treatment standards had been met;
Efficiency and Productivity: Readmissions, outpatient DNA rates and theatre productivity measures were the key areas of focus going into 2019/20. Extended stay patients had reduced though further work was required to reduce emergency readmissions to prevent potential avoidable readmissions;
Quality and Safety: Both HSMR and SHMI mortality rates remained within the expected range. Two cases of Clostridium Difficile (C-Diff) infection were reported for March which had reduced from the previously reported five cases in February. For Quarter 4, the Trust reported 12 cases of C-Diff with a total of 31 cases over 2018/19, which had decreased from 35 cases in 2017/18. 100% compliance with dementia standards had been maintained. There was on-going focus around pressure ulcers and falls;

5
Workforce: Overall sickness absence had decreased in February (latest available position) when compared to the previous month. Long-term sickness had seen a reduction whilst short-term sickness had increased. Turnover had slightly increased from the previous month and the attrition rate had reduced. Mandatory training compliance had improved since the previous month with 89% of staff being compliant. Appraisal compliance was reported at 84% which was unchanged from the previous month. The time on average that internal volunteers contribute per week equates to 911 hours. Volunteers had been recruited via a successful open day on 6 March. Helpforce were supporting the Trust, following its successful bid for national funding, to develop new and innovative ideas to support volunteering services;
Financial position: The Group reported a year-end deficit of £(17.4)m which was £2.6m ahead of the Group plan. The Trust had met its CIP requirements for 2018/19 and focus was now shifting to converting non-recurrent to recurrent savings and identifying schemes for 2019/20. Cash levels stood at £12.8m at the end of March. Creditor and debtor performance had both improved in recent months.
Assurance was sought in relation to sickness absence and the DoW explained that a „deep dive‟ into absence management had been undertaken and findings on sickness absence related to levels of deprivation would be presented at a Board Seminar in May. The Chairman and Non-Executive Directors commended the Trust on turning around the Trust‟s financial performance in year.
Resolved: (i) that, the performance against the key operational, quality, finance and workforce standards during March and Quarter 4 be noted;
(ii) that, the positive year-end position for 2018/19 be noted; and (iii) that, the on-going financial pressures be recognised; and (iv) that, the on-going operational performance and system risks to
regulatory key performance indicators and the intense mitigation work that is being undertaken to address these going forward be noted; and
(v) that, the Trusts participation to be a pilot site testing the new proposed access standards from 1 May 2019 be noted; and
(vi) that, the findings on sickness absence related to levels of deprivation be presented at a Board Seminar in May; and
(vii) that, the Trust be commended on turning around its financial performance in year.
BoD/3952 NHS Access Standards Gap Analysis The DoP&P reported that the Trust had been chosen as one of fourteen organisations to field test proposed new standards over the next six months and provided an update in relation to the Trust‟s position and development plans to support the pilot of the proposed revised „Access Standards‟. The DoP&P outlined the proposed standards demonstrating the Trust‟s current position against the revised standards and highlighted that an initial gap analysis showed the Trust in a generally positive position. The Trust had commenced data collection against the proposed standards alongside the Integrated Performance Dashboard and would feedback issues to the national team. Final recommendations were expected in Spring 2020 and a public consultation was anticipated. In response to a query from RT, Non-Executive Director, the DoP&P explained that information on clinical outcomes and patient experience would also be collated as part of the new access standards. KR, Non-Executive Director raised concerns that the Trust would be removed from the BBC healthcare tracker which was an indicator to the public on how well a Trust was performing.

6
The CE explained that the Trust would continue to report internally on the current standards and would ensure media representation continued in respect to how the Trust continued to meet and exceed targets. Following a concern raised by the Chairman in respect to elective care patients waiting over 26 weeks, the DoP&P agreed to analyse data and bring back the key themes to a future Board meeting.
Resolved: (i) that, the content of Professor Powis‟ proposal and the associated revised standards be noted; and
(ii) that, the initial gap analysis against the proposed standards be noted; and
(iii) that, the Trust‟s current position against proposed measures be noted; and
(iv) that, the Trust‟s position in supporting the pilot of the proposed revised indicators be noted.; and
(v) that, data be analysed in respect to elective care patients waiting over 26 weeks and that key themes be brought back to a future Board meeting.
BoD/3953 Gram-Negative Bacteraemia Update Report The DoN,PS&Q provided an update on the Trust‟s position against the Gram-Negative Bloodstream Infection (GNBSI) self-assessment and reported on actions identified. The Trust had a total of 455 GNBSI to 27 March 2019. Of these cases 68 were hospital onset and 377 were community onset. The Trust had achieved a score of 18 out of a possible 21 points following self-assessment and an action plan to address areas for improvement would be presented at the Infection Control Committee in April 2019. The estimated cost to the Trust and mortality associated with E-coli blood stream infections was £455,000 in 2017/18 and was noted in 44 deaths. There was no similar tool to calculate the cost of Klebsiella and Pseudomonas bacteraemia. Following discussions with commissioners, it had been agreed that a quality review group would be implemented to enable organisations across the Tees Valley to share quality improvements and learning.
Resolved: (i) that, the content of the report be noted; and (ii) that, the current position and actions planned to achieve further
improvements in 2019/20 be noted. BoD/3954 Draft Revenue and Capital Budgets 2019/20 The DoF provided an overview of the Trust‟s approach to financial planning and the draft capital and revenue budgets for 2019/20. A key risk was the delivery of the Cost Improvement Plan (CIP) with £2m remaining unidentified. CIP delivery had been phased in equal twelfths. This financial plan was in keeping with the Trusts ambition to return to surplus as outlined in its five-year financial strategy. This plan enabled the Trust to sign up to the 2019/20 Control Total (c£10.2m deficit excluding non-recurrent FRF, PSF and MRET funding) which reinforced the Trusts commitment to returning to recurrent financial balance. In the event the Trust meets the control total set by NHSI, the Trust would receive c£10.2m of non-recurrent PSF, FRF and MRET funding which would result in the Trust reporting a financially balanced position in 2019/20.

7
The capital programme was funded through a combination of internally generated depreciation, cash carried forward from 2018/19 and external funding associated with specific programmes of work. The DoF outlined the capital plan for 2019/20 and beyond and explained that this had been split into internally generated and externally generated funds. The Trust had submitted its Annual Operating Plan to NHSI and confirmed acceptance of the overall control total. Draft control totals had been distributed to directorates and were in the process of being signed-off. Revenue budgets by directorates and capital budgets had been produced and were summarised by the DoF. BD, Chair of the Finance Committee confirmed that the draft budgets had been presented to and approved by the Finance Committee. Following a query from JE, Non-Executive Director, the Chairman explained that NHSI would be reviewing the Trust segmentation position at the end of quarter 1.
Resolved: (i) that, the requirements of the Annual Operating Planning for 2019/20,
including system wide delivery of clinical and financial recovery be noted; and
(ii) that, the draft revenue and capital budgets for 2019/20 be approved. BoD/3955 NHS National Staff Survey Results 2018 The DoW presented the outcomes of the NHS National Staff Survey 2018. A total of 1,250 questionnaires had been issued to staff with 565 completed, which was a response rate of 45% which was above average when compared to similar Trusts nationally (41%). The Trust reported above the national average on eight of the ten indicators and scored average in the remaining two. The DoW provided a summary of the key findings, highlighting that the Trust had been rated in the upper outer quadrant of the most recent NHS staff survey. JE, Non-Executive Director sought clarity in relation to violence and aggression towards staff and the DoW explained that this part of the survey relied on what staff perceived to be violence and aggression against them and did not differentiate between that inflicted by patients, their family or visitors
Resolved: (i) that, the content of the report be noted; and (ii) that, the on-going activity relating to analysing the information
presented within the NHS staff survey and continued use of action planning going forward be noted.
BoD/3956 Learning from Deaths Report The MD provided an update in respect of Learning from Deaths, in line with guidance published in March 2017 by the National Quality Board “Learning from Deaths: A Framework for NHS Trust and NHS Foundation Trusts on Identifying, Reporting, Investigating and Learning from Deaths in Care”. Key points included:
Mortality: The Trust‟s HSMR value had decreased to 96.17 (February 2018 to January 2019), the SHMI was currently 100.72 (October 2017 to September 2018) both were within the „as expected‟ range;
Compulsory case reviews: To date 78% of the cases identified in the Trust‟s policy had been reviewed during 2018/19 with 16 cases identified as serious incidents, prior to case review. Of these, 11 had been reviewed and none were identified as being avoidable. There were a further five cases where the investigations were incomplete and updates would be provided in the next report.

8
Suitably trained Senior Nurses, Clinical Nurse Specialists and Allied HealthcareProfessionals (AHP‟s) were now able to complete Do Not Attempt Cardio PulmonaryResuscitation (DNACPR) forms;
The Trust were planning to hold a “Sepsis” week in September to coincide with WorldSepsis Day;
The Trust was taking part in a trial regarding antibiotic prescribing which wouldaddress issues of antibiotic stewardship and help to promote the early cessation ofantibiotic use.
RT, Non-Executive Director sought an update in respect to the Medical Examiners Role. The MD explained that Medical Examiners would be responsible for reviewing deaths and speaking with families in relation to any concerns they may have. Although clarity around the funding of a Medical Examiners team was needed, the Trust felt that it should proceed to develop this role in order to improve quality of death certification and to improve liaison with the bereaved. A business case was being developed to support the introduction of a Medical Examiners role.
Resolved: (i) that, the content of the report be noted; and (ii) that, the on-going work to maintain mortality rates within the
expected range be noted.
BoD/3957 Any Other Notified Business
a. Healthcare User Group (HUG) Visits
Peter Wilkinson, Healthcare User Group representative provided generally positive feedback following a visit to Ward 33. Concerns had been raised regarding a rise in the number of patients with damaged veins due to substance misuse which caused difficulty when inserting cannulas, etc. The MD advised that there was now a specialist venous access team who used lasers to identify veins in those patients whose veins were difficult to find.
BoD/3958 Date and Time of Next Meeting
Resolved: that, the next meeting be held on Thursday, 30 May 2019 at 1.00 pm in the Boardroom, University Hospital of North Tees.
BoD/3959 Exclusion of Press and Public
Resolved: that, representatives of the press and other members of the public be excluded for the remainder of the meeting having regard to the confidential nature of the business to be transacted, publicity on which would be prejudicial to the public interest (Section 1(2), Public Bodies (Admission to Meetings) Act 1960).
Signed: Date:
The meeting closed at 3:10 pm
30 May 2019

1
North Tees and Hartlepool NHS Foundation Trust
Meeting of the Board of Directors
25 April 2019
Report of the Chairman
Strategic Aim (The full set of Trust Aims can be found at the beginning of the Board Reports) Putting Patients First; Valuing our People; Transforming our Services; Health and Wellbeing. 1. Introduction
1.1 The Chairman’s Report aims to provide information to the Board of Directors on key local, regional and national issues.
2. Key Issues and Planned Actions
2.1 Consultant Appointments:
The following consultant appointments have been made since the last meeting: Dr Helen White – Elderly Care Dr Vineeth Cheruvalli – Paeds Dr Madhu Podalakur – Paeds
2.2 South Integrated Care Partnership
There have been several meetings between the three chairs from County Durham and Darlington NHS Foundation Trust, our Trust and South Tees Hospitals NHS Foundation Trust concerning the South Integrated Care Partnership and the role to be undertaken by the Transition Director to examine potential organisational forms for the South. The new Regional Director for NHS Improvement and NHS England, Richard Barker, and Alan Foster the lead for the North East and Cumbria Integrated Care System will join with the three trusts in sponsoring and funding this work.
2.3 Chairs Meetings
I have taken the opportunity of having a 1:1 meeting with Richard Barker, the new Regional Director for NHS Improvement and NHS England to emphasise the good work being undertaken by the Trust and highlight some of the progressive ways of working across our locality. I also took the opportunity of emphasising our commitment to wider system working.
3. Recommendations
3.1 The Board of Directors is asked to note the content of this report.
Paul Garvin Chairman

1
Board of Directors
Date: 25 April 2019
Prepared by: Barbara Bright, Director of Corporate Affairs and Chief of Staff
Executive Sponsor: Julie Gillon, Chief Executive
Purpose of the report
This purpose of the report is to provide information to the Board of Directors on key local, regional and national issues.
Action required: Approve Assurance Discuss X Information X
Strategic Objectives supported by this paper:
Putting Patients First
X Valuing our People
X Transforming our Services
X Health and Wellbeing
X
Which CQC Standards apply to this report
Safe X Caring X Effective X Responsive X Well Led
X
Executive Summary and the key issues for consideration/ decision:
The report provides an overview of the health related news and issues that feature at a national, regional and local level from the main statutory and regulatory organisations of NHS Improvement, NHS England, Care Quality Commission and the Department of Health and Social Care. In addition, information is provided on strategic and operational issues not covered elsewhere in the agenda. Key issues for information: Update on Integrated Care System and Integrated Care Partnership The Trust is one of fourteen hospitals involved in a pilot of new performance measures
which could lead to changes in the 4-hour emergency care standard Plans are announced on the introduction of three new Care Groups, Healthy Lives:
Responsive Care; and Collaborative Care with the appointment of Deputy Chief Executive, Care Group Directors and Care Group Clinical Leads.
Nominations for NHS Parliamentary Awards Success of Elective Care 100-day challenge The Trust is working collaboratively with Hartlepool Borough Council and Hartlepool
College to launch a dedicated apprenticeship scheme.
How this report impacts on current risks or highlights new risks:
Consideration will be given to the information contained within this report as to the potential impact on existing or new risks.
Committees/groups where this item has been discussed
Items contained in this report will be discussed at Executive Team and other relevant Committees.
Recommendation
The Board of Directors is asked to receive and note the content of this report.

2
North Tees and Hartlepool NHS Foundation Trust
Meeting of the Board of Directors
25 April 2019
Report of the Chief Executive Strategic Aim (The full set of Trust Aims can be found at the beginning of the Board of Directors Reports) Putting Patients First; Valuing our People; Transforming our Services; Health and Wellbeing. 1. Introduction
This report provides information to the Board of Directors on key local, regional and national issues. 2. Key Issues and Planned Actions 2.1 Integrated Care System/Integrated Care Partnership Update The ICS continues to focus on improving health outcomes and to better manage the ‘here and now’ operational challenges to achieve sustainability, with a number of pivotal work streams. The Tees Valley Health and Care Partnership is evolving with terms of reference agreed and liaison with key stakeholders now taking place. The Clinical Services Strategy is work in progress with an additional finance work stream now part of the overall programme of work across the local system. 2.2 Pilot of new Urgent and Emergency Care Standards This year the NHS National Medical Director, Professor Stephen Powis, working with leading clinicians is reviewing the access targets currently in place. An interim report included proposals to update these targets in line with advances in clinical practice, and what patients say matters most to them. This report included several proposed standards to be tested in urgent and emergency care services, potentially in place of the existing 4-hour standard. The Trust is one of the leading performing organisations in England regarding achievement of the A&E four-hour target with success due to continuous improvement, innovation and development of services to meet the ever changing demands of our communities. As a result, the Trust has agreed to be one of fourteen hospitals chosen to pilot and test the proposed new ways to measure performance which could lead to changes to the four-hour A&E target. It is expected that field testing of the proposed standards will commence in May 2019 and until field testing starts existing clinical standards and processes remain in place. The focus throughout the trial remains firmly on delivering safe, excellent, clinically appropriate patient care and experience. 2.3 Introduction of Care Groups
The Trust has recently announced plans to deliver its strategic direction with the introduction of three new Care Groups, which will focus on Healthy Lives: Responsive Care; and Collaborative Care. This is an exciting and innovative evolvement from the more traditional hospital model which will look to future-proof healthcare for our communities. In order to deliver this vision which will focus on population health, transformation of services and dynamic local partnerships, three Care Group Directors and Clinical Leads have been appointed to drive the ambition.

3
2.4 NHS Providers Visit Chris Hopson, Chief Executive of NHS Providers visited the Trust on Friday, 12 April 2019. During his visit he gave a presentation to the Executive Team and Trust Directors Group on national policy, enabling debate and discussion. The Trust demonstrated its achievements and successes in performance and quality by showcasing the Frailty Pathway; Improving the Patient Journey; the Integrated Discharge Team; getting patients home safer, sooner; the Urgent and Emergency Care Service and the Single Point of Access, the successful integration of Health and Social Care. 2.5 NHS Chief People Officer Role NHS Improvement and NHS England have appointed Prerana Issar to the role of chief people officer. This new position is part of the NHS Executive Group and will play a leading role in ensuring that NHS in England has enough people, with the right skills and experience to deliver the improvements for patients set out in the long term plan. The Chief People Officer will take over from Julian Hartley and lead the development of the workforce implementation plan, working closely with organisations across the NHS, including NHS England regional teams, local systems, national bodies and trade unions.
2.6 NHS Parliamentary Awards NHS England has launched the NHS Parliamentary Awards 2019 with nominations closing on 26 April 2019. Last year over 250 Members of Parliament nominated an individual or organisation for an award with over 750 nominations from MPs. This year, it is hoped even more MPs get involved and show their local NHS staff, volunteers and carers what they mean to them and the communities they serve each day. MP nominations open on 5 March 2019 and close on 26 April 2019. The winners will be presented with their awards in parliament on 10 July 2019. 2.7 Local Elections: Purdah considerations Due to local elections taking place on 2 May 2019, the Board of Directors should be aware of the pre-election ‘purdah’ period. This is the period of time immediately before elections when announcements from and activities by public bodies which could influence or be seen to influence the election are restricted. This period is designed to avoid the actions of public bodies distracting from or having influence on election campaigns. The ‘purdah’ period typically will be six weeks before the election and NHS Providers has published national guidance for organisations. 2.8 Elective Care 100-day challenge A Project team has helped to successfully bring about changes (in a 100-day challenge) to improve care for patients having surgery at the University Hospital of Hartlepool. The challenge was to focus on improving better utilisation of surgery at Hartlepool. The aims being to reduce the number of cancelled operations and to increase the amount of elective procedures carried out, with the ultimate aim to improve patient care. The project involved excellent engagement and involvement from clinical teams and successfully delivered on its objectives in increasing the number of elective procedures at Hartlepool, preventing cancellations of surgery due to bed pressures, and providing a better patient experience. 2.9 Making a Difference in Maternity Care A Trust team was invited to speak at a National Maternity and Neonatal Health Safety Collaborative Learning Event in London for a second successive year where they presented findings surrounding their quality improvement achievements and work with local partners in developing a bespoke MatNeo Local Learning System to support the ambitions of maternity outcomes across the region.

4
The Trust was one of the first 44 organisations in England to sign up to the collaborative when it was launched in 2017; a three year programme that supports improvement in the quality and safety of maternity and neonatal units across England. The Trust will contribute to the national ambition of reducing the rates of maternal and neonatal deaths, stillbirths and brain injuries that occur during or soon after birth by 20% by 2020’. The Trust is working closely with the Academic Health Science Network for the North East and North Cumbria with the aim of promoting engagement, collaboration and innovation in ways that benefit patients and public. The MatNeo Local Learning System is now established in the region and holds quarterly learning events with providers from across the area, to share findings and best practice surrounding key developments within maternity and neonatal teams. 2.9 Collaborative working – Apprenticeship programme The Trust is one of three organisations that have come together to launch an innovative apprenticeship programme to support better outcomes for residents across the region. Hartlepool Borough Council, Hartlepool College of Further Education and the Trust have launched a dedicated apprenticeship scheme. The Integrated Health and Social Care Apprenticeship will focus on offering students the opportunity to develop their knowledge in a range of healthcare environments, building upon understanding to date and providing wider comprehension of service provision. The hope is that this new way of learning will lead to a more personalised health and care model to reflect the changing needs of the region. The pilot for the first cohort of students will launch in April 2019. 3. Recommendations
The Board of Directors is asked to note the content of this report. Julie Gillon Chief Executive

North Tees and Hartlepool NHS Foundation Trust
Meeting of the Board of Directors
25 April 2019
Report of the Chief Executive
Retrospective Approval of Documents Executed Under Seal
Strategic Aim (The full set of Trust Aims can be found at the beginning of the Board Reports)
Transforming our Services The following documents have been executed under the Common Seal of the Trust.
Document Date Sealed By
Licence to Assign Between:
1) North Tees and Hartlepool NHS Foundation Trust
And
2) Gentian (North Tees) Limited
And
3) Gentian Holdings Limited
In respect of Entrance Concourse Units, University Hospital of North Tees
3 April 2019
Mr N Atkinson Mrs B Bright
(witness)
The Board is requested to grant retrospective approval for the sealing of these documents.
Julie Gillon Chief Executive

1
Board of Directors
Title: Capital Programme Performance 2018/19
Date: 25 April 2019
Prepared by: Steve Taylor, Associate Director, Estates and Capital, NTH Solutions LLP
Executive Sponsor: Neil Atkinson, Director of Finance
Purpose of the report
To provide an update as at 31 March 2019 (Quarter 4) on the progress of delivering the 2018/19 capital programme.
Action required: Approve Assurance x Discuss x Information x
Strategic Objectives supported by this paper:
Putting Patients First
Valuing our People
Transforming our Services
x Health and Wellbeing
Which CQC Standards apply to this report
Safe x Caring Effective Responsive Well Led
x
Executive Summary and the key issues for consideration/ decision:
The four work streams of Medical Equipment, Digital/ICT, Service Development and Estates Backlog Maintenance have performed as forecast in Quarter 4.
The Energy Centre project is complete with the contractor demobilizing the site accommodation at the end of March 2019. The overall major engineering infrastructure replacement project costs are anticipated to be under the DH approved OBC cost plan of £26m and within the actual funding award, which was limited to £25m. Certainty has increased in Q4 that the project will be completed £1m under the overall budget. This provides the Trust with an opportunity to invest the money elsewhere.
To manage down the current £45.5m of backlog maintenance a revised detailed 5 year backlog maintenance plan has been developed to address the high backlog maintenance levels within the Trust Estates. The revised plan is based on a £3.7m annual backlog allocation.
How this report impacts on current risks or highlights new risks:
No new risks are identified in this report.
Committees/groups where this item has been discussed
Capital Planning Group
Recommendation
The Board is requested to receive this report and note the position on capital schemes.

1
North Tees and Hartlepool NHS Foundation Trust
Meeting of the Board of Directors
25 April 2019
Capital Programme Performance 2018/19
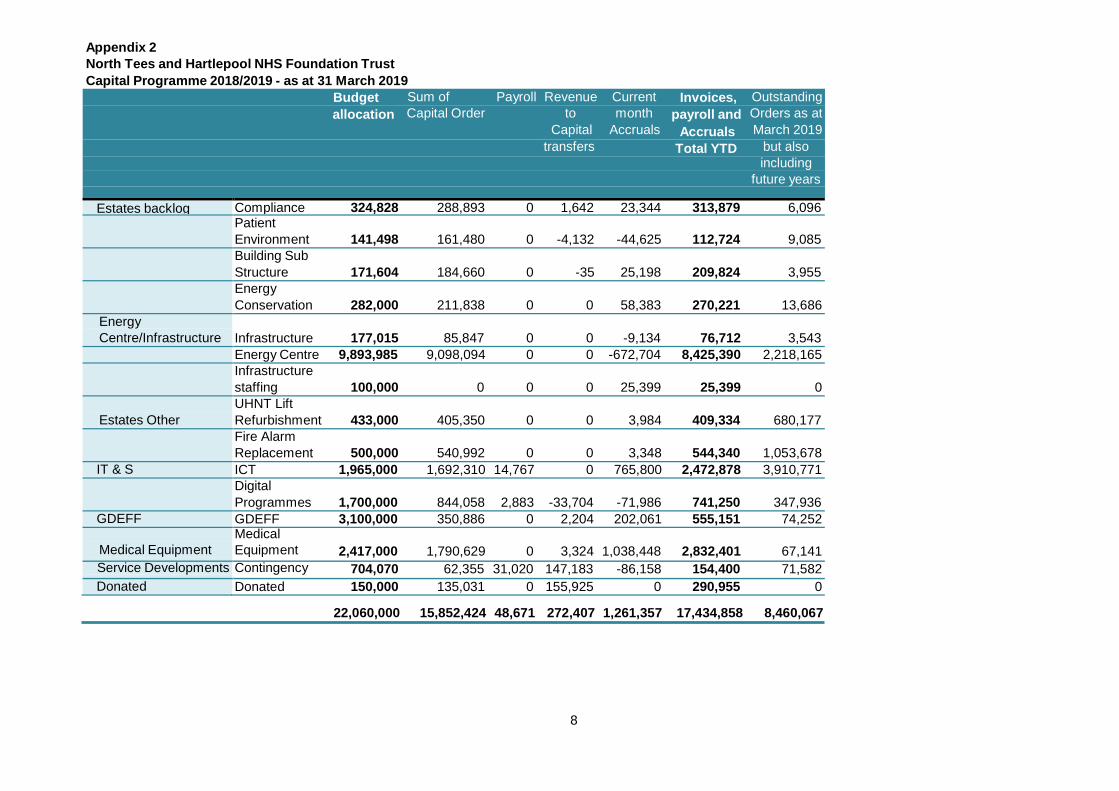
Report of the Director of Finance 1. Introduction/Background 1.1 The 2018/19 capital programme allocation was agreed at £22.06m comprising
£8.82m internally generated depreciation, £12.7m loan for the Major Engineering Infrastructure Replacement Scheme, £1.08m loan payback reduction to internally generated depreciation, £2.4m Public Dividend Capital (PDC) for Global Digital Exemplar Fast Follower (GDE FF), £0.92m Energy Centre retention spend anticipated in 2019/20, and £150K Donated Funds. The NHS Improvement Compliance Framework requires that a minimum of 85% and a maximum of 115% of the original capital allocation should be spent on a monthly basis. Only goods and services that have been received or invoiced may be counted as expenditure. At the end of Q4, expenditure (invoices and accruals) was £17.43m, which is 79% of the Trust’s planned spend.
2. Main content of report 2.1 The major engineering infrastructure replacement scheme is now complete and costs
remain below budget allocation. There remains a small on site contractor presence to complete the defects / snagging issues and to complete the remaining electrical changeovers. The first phase to construct and make operational the new electrical substations is complete. The second phase of work concerns the construction of a new energy centre. A recommendation was made to the Project Board in March 2017 to award the contract to NG Bailey Limited. Following expiry of the compulsory standstill period, NG Bailey Limited was appointed as principal contractor, and construction work commenced in July 2017. The project has been completed under budget and in a safe manner with minimal disruption to clinical services. Of the 70 non-essential and essential cables to be transferred, 65 have now been successfully completed. The last 5 electrical changeovers are associated with substation 6. These changeovers have been delayed due to a failure of an existing electrical switch within substation 6. A new switch has been ordered and will be installed in mid-April 2019 to allow the remaining changeovers to be completed by the end of April 2019. The complex electrical changeovers have successfully been carried out in a manner to minimise disruption to fully operational clinical services. This has inevitably delayed the project. The contract will be applied but at this stage it is unlikely that any costs could be successfully levied against NG Bailey Limited for the delay. The current financial year spend for the project is forecast to be under the planned capital forecast expenditure of £10.17m.
2.2 Work continues to progress slightly ahead of programme to replace the fire alarm
system on the UHNT site. This project is anticipated to be completed by Q4 of 2019/20 and is expected to be delivered for the approved sum of £1.68m.
The work continues to be planned carefully with Infection Control and clinical departments. A significant ward decant programme is required during the 2019/20 financial year to allow access to complete this project. The decant programme will be carefully planned and co-ordinated with the General Manager / Senior Clinical Matron Group (GM/SCM Group).

2
2.3 The replacement and refurbishment of lifts on the UHNT site is anticipated to be
delivered for the approved sum of £1.155m and phased over the 2018/19 and 2019/20 and into Q1 of the 2020/21 financial year to minimise disruption to clinical services and due to the long lead time associated with lifts. The scope includes 2 x bed evacuation lifts within the Tower block.
The lift refurbishment project continues to progress carefully to prevent disruption to clinical services. In Q4 work has commenced on site to refurbish the West wing, South Wing and Tower block lift No. 1. The West wing lift is anticipated to be brought into operational use by the end of May 2019 and the first bed evacuation lift on Tower block is anticipated to be brought into operation use by the end of June 2019.
2.4 To manage down the current £45.5m of backlog maintenance a revised detailed 5
year backlog maintenance plan has been developed to address the high backlog maintenance levels within the Trust Estates. The revised plan is based on a £3.7m annual backlog allocation.
2.5 The significant elements of the programme to comment upon are:
• Financial expenditure is aligned to the annual programme and capital cash flow
projections/expenditure is on plan in relation to the annual financial forecast. • Completed schemes have been achieved within the overall planned programme
timescales and budget allocations, with good outcomes and positive feedback. The overall financial summary for the period to 31 March 2019 is presented at
Appendix 2.
3. Recommendation
3.1 The Board is requested to receive this report and note the position on capital schemes up to 31 March 2019.
Neil Atkinson Director of Finance

3
Appendix 1 - Work Stream Reports 1. Medical Equipment As part of the Medical Equipment Capital Programme the following equipment has been purchased: 1.1 7 replacement CTG machines (Foetal monitors) have been delivered and are
currently being commissioned for use for Maternity. 1.2 A total of 7 Non-invasive ventilators have been purchased for A&E, EAU and the
respiratory wards this completes the rolling NIV replacement programme
1.3 A Gamma camera has been installed to replace the aging and failing Gamma camera on the UHH site. The new machine is currently being commissioned.
1.4 A new static x-ray system has been ordered to replace a current x-ray system on the
UHH site. The new machine has now been installed and is fully operational. 1.5 10 new hoists have been delivered to replace start to replace current stock some of
which are 18 years old. 1.6 20 New patient monitors have been commissioned and are in use within A&E,
Surgical Decisions Unit (SDU) and the Surgical Observations unit 1.7 A new MRI compatible anaesthetics machine and integrated ventilator has been
ordered for the MRI suite. The new machine has been delivered and is currently being commissioned.
1.8 A new Endoscopy stack was purchased for the bowel screening programme using
additional money from NHS England for use in Cancer treatment. 1.9 A new Ultrasound machine has been installed in the Coronary Care Unit. The new
machine provides a much improved image quality than the one it replaces and also has Cardio Echo facilities.
1.10 The mortuary has been updated by replacing fridge doors; the temporary body
storage has been replaced by a permanent facility with Bariatric storage. Two new mortuary tables are being installed which are variable height and a new concealment trolley has been purchased.
2. Information Communication & Technology 2.1 Additional fibre and network cabling is currently being installed at both UHH and
UHNT, this is a continuation of the successful programme of work to increase wireless coverage and access, especially to support the expansion and rollout of both Electronic Prescribing and Medicines Administration (EPMA) and the Vocera, communication and collaboration platform.
2.2 The rollout of the new desktop computer estate, with updated operating and security
systems continues to plan, this also include a mechanism for NHS Digital to remotely monitor the Trust Active Threat Prevention (ATP) defence systems automatically.
Currently all clinical areas have been completed, delivering some 1200 units.

4
3. Digital Strategy – Electronic Patient Record 3.1 The Trusts Digital programme continues to progress well against plan. Paediatric
services including; Accident and Emergency (A&E) Paediatrics, successfully went live with TrakCare electronic observation (PEWS, fluid balance, pain assessment and sepsis screening) in February, the changes have been well received and feedback has been very positive.
Electronic NEWS2 roll out across all inpatient areas will commence May 2019. To support the roll out and adoption of functionality a Business Case has been prepared to purchase smart mobile blood pressure devices that will interface into TrakCare, negating any need for manual intervention, the business case will be presented for approval at Deputy Executive Team (DET) team in April 2019.
3.2 A&E went live with TrakCare Active Clinical Notes (ACN) on 5th March 2019 which
has allowed the CAS card to be removed from operation; all information is now recorded directly into TrakCare, making information available at the right time, in the right place to the right clinical staff. The feedback from the service has been extremely positive with all staff adapting to the new process with ease. The next steps are to work with the Emergency Assessment Unit (EAU) to review all of their paper processes with a view to moving them across to ACN, estimated timescales are Q2 of 2019/20.
Furthermore, external agencies are also now able to use ACN – 50% of TEWV staff have access to TrakCare. The team continue to work with Human Resources (HR) and other external agencies to ensure that relevant and legitimate access is granted to TrakCare where necessary and staff receive sufficient training.
3.3 Outpatient (clinical letters) – the templates required to submit data electronically are
being prepared in readiness of going live with all outpatient clinic letters directly to GPs. Communications are being drafted for all stakeholders and will be circulated imminently.
3.4 Dawn (Anticoagulation) – is a system currently being used for noting, referring to
notes, dosing (warfarin) and producing and printing letters. Going forward this is to be completed within TrakCare. A number of efficiencies and benefits have been identified and being worked up with the service.
3.5 Hospital @ Night – A new virtual ward has been set up in TrakCare to identify and
monitor clinical tasks associated with patient care that requires escalation, a new team established from 8/4/19 covering 8pm-8am will run for a period of four weeks to assess its effectiveness.
3.6 Antibiotic Review – TrakCare has been set up to help with the Antibiotic review
process, waiting for a trial to be initiated on the wards. 3.7 Dispensing Robot – A Business Case for a pharmacy dispensing robot is currently
being refreshed; this will be scheduled for review at DET in May 2019. 3.8 CareScan+ - the areas to pilot will be Model Ward and ACU. The formal process has
commenced with GS1 to obtain accreditation for CareScan+ and present at GS1 conference in April 2019. A scoping exercise carried out in theatres (UHNT) and ACU is on-going. The product upload process has also now commenced.
3.9 Approval in February 2019 to draw down the next milestone payment of £1.5m Public
Dividend Capital (PDC) funding, linked to the Global Digital Exemplar Fast Follower (GDE FF) programme was given by NHS Digital, this affirms their continued support of the programme.

5
4. Service Developments 4.1 The Trust currently provides Community Services from 71 external premises and is
currently working in collaboration with Hartlepool and Stockton CCG, NHS Property Services and other landlords to explore the potential to rationalize the use of external premises to achieve cost savings for the health economy. NT&HS LLP continues to support the Trust to carry out a review of these leases. The review has now commenced, with the arrival of the new Capital Planning and Property Manager on the 1 March 2019. Recommendations are anticipated to be made within Q2 of 2019/20.
4.2 NT&HS LLP will continue to work with the Trust to develop a clinical use for the area that fits with the STP / ICS plan and wider clinical strategy and update as developments occur.
4.3 NT&HS LLP continue to support the Trust to provide options to explore the future use and ownership of the Peterlee Community hospital building.
4.4 The CCG has contacted North Tees and Hartlepool Solutions LLP and are keen to
build on the collaborative success of the Urgent Care project and relocate 2 local GP practices onto the UHH site. The CCG’s preferred option is to enter into a 25 year lease arrangement with the Trust to develop the former Rainbow Nursery at the front of the Hospital site for this purpose. The existing building would be redeveloped and substantially enlarged, creating a footprint of approximately 1350sq.m. using adjoining land. A dedicated car park and access road would be created. The CCG have applied to the Estates Technology and Transformational fund (ETTF) for 100% Public Dividend Capital (PDC) to fund the work, with the Trust benefitting from the potential lease income. The CCG has requested that North Tees and Hartlepool Solutions LLP provide a capital cost estimate to assist the CCG with its bid for funding. Should the bid be successful, the CCG proposes that North Tees and Hartlepool Solutions LLP further develop this solution and manage the scheme through design development, procurement through the execution phase to completion on site. If this projects proceeds, it will strengthen the health provision of the UHH site. A decision from the ETTF Fund on the bid is has still not been made by the end of Q4. It is understood that the project is one of three still under consideration. The CCG and the Trust will continue to press for a decision in Q1 or 2019/20.
4.5 NT&HS LLP are working to facilitate the sale of the surplus land on the UHH site.
The proposal is a tier 4 Hospital for service veterans suffering from PTSD. A heads of terms for the land sale has now been negotiated by the LLP in Q4, and subject to Trust approval, will allow the sale of the first 3 acres tranche with options on the remainder of the land. The sale is subject to the purchaser receiving satisfactory planning permission within 18 months of submission of planning application. The purchase price of first tranche is agreed at £548,781.
If the purchaser proceeds with the purchase of the remaining tranches, this will allow the Trust to realise the overall land sale value of £1,500,000 for the full 8.2 acre site.
Alice House hospice is also interested in a potential leasing solution for 1-2 acres of the 8.2 acre site to extend the services that they offer.
4.6 The Trust is currently working in collaboration with Hartlepool and Stockton CCG,
NHS Property Services and other landlords to explore the potential to rationalize the use of external premises by the Trust and to achieve cost savings for the health economy. A team of Speech and Language Therapy (SALT) staff are planned to move from Fairfield Clinic to Newtown Neighbourhood Centre. The estates enabling works are now complete. This allows the Trust to withdraw from a long term lease for
6
Fairfield Clinic and relocate into a much larger and more cost effective premises where, not only could the SALT team be accommodated, but there is also adequate space to accommodate another service. Wheelchair Services are also planned to relocate to Newtown Neighbourhood Centre to free up much needed space to address future requirements (e.g. potential expansion of Rapid Access Lounge and provision of additional CT scanning facilities).
5. Estates Programme 5.1 The Energy Centre project is complete with the contractor demobilizing the site
accommodation at the end of March. There remains a small on site contractor presence to complete the defects / snagging issues and to complete the remaining mechanical and electrical changeovers. The overall major engineering infrastructure replacement project costs are anticipated to be under the DH approved OBC cost plan of £26m and within the actual funding award, which was limited to £25m. Certainty has increased in Q4 that the project will be completed £1m under the overall budget. This provides the Trust with an opportunity to invest the money elsewhere.
5.2 The electrical changeovers to migrate departmental power supplies from old substations onto the new substations are now 92 % complete. Of the 70 non-essential and essential cables to be transferred, 65 have now been successfully completed. The last 5 electrical changeovers are associated with substation 6. These changeovers have been delayed due to a failure of an existing electrical switch within substation 6. A new switch has been ordered and will be installed in mid-April to allow the remaining changeovers to be completed by the end of April.
5.3 The new Medium Combustion Plant Directive (MCPD) came into law in January
2019. The Energy Centre is designed to meet the latest emissions standards associated with this Directive. A significant modeling exercise has been undertaken to demonstrate compliance with this new standard. A permit application has now been made to the Environment Agency to comply with these standards. The latest position is that the Environment Agency is reviewing the application and a formal response is anticipated by May. This does not affect or prevent the operation of the Energy Centre.
5.4 Backlog maintenance 5.4.1 A revised detailed 5 year backlog maintenance plan has been developed to address
the high backlog maintenance levels within the Trust Estates. The revised plan is based on a £3.7m annual backlog allocation.
The Fire alarm replacement project on the UHNT site is now 35% complete and the project continues slightly ahead of programme. The current work areas are within North Wing, plant rooms and other non-clinical areas within the lower ground floor areas. The network cabling between the new fire alarm panel positions around site are now 100% complete. The work continues to be planned carefully with Infection Control and clinical departments. A significant ward decant programme is required during the 2019/20 financial year to allow access to complete this project. The decant programme will be carefully planned and co-ordinated with the General Manager / Senior Clinical Matron Group (GM/SCM Group). The lift refurbishment project continues to progress carefully to prevent disruption to clinical services. The progress by lift is detailed below:-

7
1. The end of life West wing lift has now been stripped out. The new lift cab has been delivered to site and the installation of the new lift has commenced. This lift is anticipated to be completed and back in service by the end of May.
2. Tower block lift No. 1 strip out has commenced, its replacement lift will be the
first bed evacuation lift. This lift is anticipated to be completed and back in service by the end of June 2019.
3. Tower block Lift No. 2, which is to be the second bed evacuation lift, is now
being manufactured off site. Work will not start on site to install this lift until lift No. 1 is fully operational. Only 1 Tower block lift will be taken out of use at any one time to minimise disruption to clinical services.
4. The end of life South Wing lift has now started to be stripped out.
The LED lighting replacement works within the 2018/19 financial year has been completed spending the 100K 2018/19 allocation to replace existing lighting with LED equivalents on the UHNT site within the main hospital corridors, main outpatients department and within the medical records area. The project will continue into the 2019/20 financial year to complete the overall project to replace the majority of lighting with LED equivalents. This includes £300K of grant funding from NHSI. The anticipated energy saving at project completion is £100K / annum. The replacement of R22 air conditioning plant planned works within the 2018/19 financial year have been completed spending the 150K 2018/19 allocation. The project will continue to meet mandatory compliance standards to remove Ozone depleting R22 gases from the Trust in the 2019/20 financial year. The anticipated energy savings at project completion are £40K / annum. The planned building management system replacement works within the 2018/19 financial year have been completed spending the 162K 2018/19 allocation. The project will continue into the 2019/20 financial year to complete the overall project.
The planned Medical air plant replacement works on the UHNT site was completed on the 26th March. The solution replaces the existing end of life duplex plant with a HTM 02 compliant triplex plant with an increased backup manifold system.
8
Appendix 2 North Tees and Hartlepool NHS Foundation Trust Capital Programme 2018/2019 - as at 31 March 2019
Budget Sum of Payroll Revenue Current Invoices, Outstanding allocation Capital Order to month payroll and Orders as at
Capital Accruals Accruals March 2019 transfers Total YTD but also
including future years
Estates backlog Compliance 324,828 288,893 0 1,642 23,344 313,879 6,096 Patient
Environment 141,498 161,480 0 -4,132 -44,625 112,724 9,085 Building Sub
Structure 171,604 184,660 0 -35 25,198 209,824 3,955 Energy
Conservation 282,000 211,838 0 0 58,383 270,221 13,686 Energy Centre/Infrastructure
Infrastructure 177,015 85,847 0 0 -9,134 76,712 3,543
Energy Centre 9,893,985 9,098,094 0 0 -672,704 8,425,390 2,218,165 Infrastructure
staffing 100,000 0 0 0 25,399 25,399 0
Estates Other UHNT Lift Refurbishment 433,000 405,350 0 0 3,984 409,334 680,177
Fire Alarm Replacement 500,000 540,992 0 0 3,348 544,340 1,053,678
IT & S ICT 1,965,000 1,692,310 14,767 0 765,800 2,472,878 3,910,771 Digital
Programmes 1,700,000 844,058 2,883 -33,704 -71,986 741,250 347,936 GDEFF GDEFF 3,100,000 350,886 0 2,204 202,061 555,151 74,252
Medical Equipment
Medical Equipment 2,417,000 1,790,629 0 3,324 1,038,448 2,832,401 67,141
Service Developments Contingency 704,070 62,355 31,020 147,183 -86,158 154,400 71,582 Donated Donated 150,000 135,031 0 155,925 0 290,955 0
22,060,000 15,852,424 48,671 272,407 1,261,357 17,434,858 8,460,067

1
Board of Directors
Title: Integrated Compliance and Performance Report
Date: 25 April 2019
Prepared by: Lindsey Wallace, Head of Planning, Performance and Development
Executive Sponsor: Lynne Taylor, Director Planning and Peformance
Purpose of the report
To provide an overview of the integrated performance for compliance, quality, workforce and finance for Quarter 4 and year end.
Action required: Approve Assurance x Discuss x Information x
Strategic Objectives supported by this paper:
Putting Patients First
x Valuing our People
x Transforming our Services
Health and Wellbeing
x
Which CQC Standards apply to this report
Safe x Caring x Effective x Responsive x Well Led
x
Executive Summary and the key issues for consideration/ decision:
Compliance against key access standards including quality and workforce in accordance with the Single Oversight Framework for March and Quarter 4 period.
Overall the Trust has performed well against national and local indicators, achieving compliance against the majority of the key standards in March and Quarter 4, though pressures remain around the cancer 62 day standards.
Operational efficiency standards indicate improvement, however with further work required across readmission rates, DNA rates and theatre utilisation.
Quality standards indicate positive performance against a number of key indicators, including HSMR/SHMI, C-difficile and Dementia standards.
Sickness absence remains the key pressure within Workforce, however with multiple actions implemented to understand the underlying reasons, including the Trust Stress group and a pilot of the ‘Tackling Stress in the Northern Region’ survey planned to commence in April 2019.
Financial recovery is on track, with the month 12 position reporting within plan and full delivery of the 2018/19 CIP.
How this report impacts on current risks or highlights new risks:
Continuous and sustainable achievement of key access standards across elective, emergency and cancer pathways, alongside a number of variables outside of the control of the Trust within the context of system pressures and financial constraints. Financial recovery continues to be the Trust’s key challenge. Compliance for sickness absence continues to be a key pressure. Continuous and sustainable achievement of key quality indicators including Healthcare Acquired Infections.
Committees/groups where this item has been discussed
Executive Management Team and Performance, Planning and Compliance Committee.
2
Recommendation
The Board of Directors are asked to note: The performance against the key operational, quality and
workforce standards during March and Q4. Recognise the on-going financial pressures. The on-going operational performance and system risks to
regulatory key performance indicators and the intense mitigation work that is being undertaken to address these going forward.
Note the Trusts participation to be a pilot site testing the new proposed access standards from 1 April 2019.

1
North Tees and Hartlepool NHS Foundation Trust
Meeting of the Board of Directors
25 April 2019
Integrated Compliance and Performance Report Report of the Director of Planning and Performance, Director of Nursing, Patient Safety and Quality, Director of Workforce and Director of Finance
Strategic Aim and Strategic Objective: Putting Patients First 1. Introduction/Purpose
1.1 The Integrated Compliance and Performance Report highlights performance against a range of indicators against the Single Oversight Framework (SOF) and the Foundation Trust terms of licence for the month of March and Q4 2018/19. Due consideration has been given to both positive and negative variances and progress against monthly, annual and in year improvement targets.
1.2 The Integrated Dashboard is attached in Appendix 1- 5, with additional commentary provided against key metrics, providing month on month trend analysis. Appendix 1 outlines the trend analysis against the key Compliance indicators, Appendix 2 outlines Operational Efficiency and Productivity, Appendix 3 demonstrates Quality metrics, Appendix 4 Workforce and Appendix 5 relates to Finance.
2. Performance Overview
2.1 Overall the Trust has performed well against national and local indicators, achieving compliance against the majority of the key standards in March and Q4, though pressures remain around the cancer 62 day standards. However, provisional March and Q4 performance reports a positive position against the 62 day standard, despite pressures seen in February, reporting at 78.9%, which had an unusually low number of overall patients, which subsequently impacted upon performance. The Trust continues to consistently deliver against the Emergency 4 hour standard, reporting in top position nationally in March, with the RTT standard also reporting above the 92% target.
2.2 Emergency activity across the organisation has seen an increase of 9.24% (n=1041) in Q4 compared to the same time last year with emergency activity including 946 patients who were treated via Ambulatory Care, equating to 23.76% of the total emergency admissions.
2.3 The report indicates the Trust has performed above or within expected for the majority
of efficiency and productivity indicators, demonstrating performance above the national average, as outlined within the main report, with a positive position evident against pathway indicators including Delayed Transfers of Care (DToC) and bed utilisation.
2.4 Readmissions, Outpatient DNA rates and Theatre productivity measures are the key areas of focus going into 2019/20.

2
2.5 NHS England has pledged a review, clinically led, of all appropriate access standards to test against quality outcomes. The Trust has been chosen as one of fourteen organisations to test the proposed standards over the next 6 months, with the aim of identifying the appropriateness, or not, of the individual standards, the potential impact of the standards on improved patient care and any significant gaps in both the availability of the data and the criteria set to record, monitor and report the revised indicators (See Board Agenda item 11 for detail).
2.6 The Trust continues to remain within the expected range for both HSMR and SHMI values. The latest data for HSMR is 96.17 reducing from 97.79, with SHMI quarterly end position seeing a reduction to 100.72 from the previously reported 103.02.
2.7 The Trust has seen a financial year improvement of 11.43% in C difficile rates compared to 2017/18 when the Trust reported 35 cases, against the 31 for 2018/19.
2.8 The Trust continues with its excellent performance in relation to dementia standards maintaining 100% compliance.
2.9 The sickness absence rate for February 2019 is reported at 5.01% against the Trust target of 3.5%. When comparing February 2019 to the previous months’ sickness absence rate, there has been a decrease of 0.42%.
2.10 Long term sickness absence rate reported at 2.68%, a decrease of 0.72% when
compared to the previous month (3.40%). Short-term sickness absence rate reported at 2.34%, an increase of 0.46% when compared to the previous month (1.88%).
2.11 The cost of sickness absence is reported as £498,750 for the month of February 2019. Anxiety/stress/depression/other psychiatric illnesses’ continues to account for the highest proportion of all sickness absence reasons at 28%. The Trust Stress group has commenced with a pilot of the ‘Tackling Stress in the Northern Region’ survey planned to commence April 2019.
2.12 A further step to understand directorate sickness will include senior managers
attending deputy ETM when their respective areas continually under achieve against the sickness absence target. The new approach will focus attention on proactively managing absence within directorate areas, reinforcing ownership, responsibility and accountability of managers for absence review and management.
2.13 The turnover rate for March 2019 is reported at 8.70%, an increase of 0.37% when compared to the previous month (8.33%). The Top 3 ‘Reasons for Leaving’ attributed to the Trust’s Turnover rate are; ‘Voluntary Resignation – Unknown’ (36.09%), ‘Voluntary Resignation – Work Life Balance’ (16.04%) and ‘Retirement Age’ (12.78%).
2.14 In comparison, an attrition figure has been calculated which includes those employees who have left the organisation for ‘involuntary’ reasons, for example due to dismissal, employee transfers, redundancy and end of fixed term contact. The attrition figure for March 2019 is reported at 2.77%, a decrease of 1.85% when compared to the previous month (4.62%).
2.15 The overall compliance for mandatory training for March 2019 is 89%, 1% greater than in the previous month.
2.16 Appraisal compliance is reported at 84% for March 2019, this figure is unchanged from the previous month.

3
2.17 At 31 March 2019, the Trust has 170 internal volunteers and 150 volunteers provided by external organisations such as Royal Voluntary Service (RVS), Radio Stitch, Bookbase and League of Friends. The time on average that internal volunteers contribute per week equates to 911 hours, which is the equivalent of 24.3 WTE. Work is on-going to promote volunteering opportunities and recruitment centres are held on a monthly basis for candidates.
2.18 The Trust is an early adopter, (one of only four across the country), to roll out the Helpforce and Daily Mail volunteer initiative at pace. An ‘Open Day’ was arranged for 6 March 2019 for the first cohort of people who have pledged their support. The day was successful in recruiting volunteers. In addition, Helpforce are supporting the Trust, following its successful bid for national funding, to develop new and innovative ideas to support volunteering services. Work is progressing at pace in developing the project and implementation plan, working with all interested parties both internally and externally including local authorities, the voluntary sector and Helpforce. The aim is to pilot work across EAU and Wards 26/27 in order to develop processes and test the proof of concept, with a view to scaling up when appropriate.
3. Finance Overview
3.1 The year-end position is a deficit of (£17.4m). This compares to a planned deficit of (£20.0m). The Group is therefore finished the year £2.6m ahead of plan. The year-end position included an impairment of £1.2m. The deficit before impairment was £16.2m, £3.8m ahead of plan.
3.2 The Trust met the 2018/19 CIP requirements through a combination of corporate,
directorate and non recurrent schemes. Focus of the programme has shifted to converting non recurrent to recurrent savings and 2019/20 scheme identification.
3.3 Cash levels stand at £12.8m at the end of March. Creditor metrics have improved in
recent months, and operational issues have reduced substantially consequently. Similarly, debtor performance has improved.
4. Key Challenges 4.1 Continuous and sustainable achievement of key access standards across elective,
emergency and cancer pathways. 4.2 Delivery against the Lord Carter operational efficiency recommendations and
associated cash releasing savings. 4.3 Continuous and sustainable achievement of key quality indicators including Healthcare
Acquired Infections which is reflected within the Board Assurance Framework. 4.4 Compliance for appraisal and sickness absence continues to be significantly adrift from
the target position. Plans are in place to monitor and improve percentage compliance. 4.5 Financial recovery continues to be the Trust’s key challenge. 5. Conclusion/Summary
5.1 The Trust has performed well against the majority of key operational national and local standards within March and Q4 2018/19, notwithstanding the on-going financial pressures. The Trust continues to develop the performance reporting framework to

4
ensure it meets the needs of both corporate and directorate level delivery, reflecting the multiple internal and external performance requirements.
5.2 The Trust continues to work closely with NHSI colleagues to deliver robust financial
recovery plans. 6. Recommendations
The Board of Directors are asked to note:
The performance against the key operational, quality, finance and workforce standards during March and Q4.
Recognise the on-going financial pressures. The on-going operational performance and system risks to regulatory key
performance indicators and the intense mitigation work that is being undertaken to address these going forward.
Note the Trusts participation to be a pilot site testing the new proposed access standards from 1 April 2019.
Lynne Taylor, Director of Planning and Performance Julie Lane, Director of Nursing, Patient Safety and Quality Alan Sheppard, Director of Workforce Neil Atkinson, Director of Finance

Integrated Performance and Compliance Report
March 2019
Developed by: Performance TeamDevelopment lead: Lindsey Wallace

Measure (click on
measure for trend graphs)
Reporting
periodTarget Actual Q4 Trend Details
Emergency Care 4 hr standard Mar-19 95.00% 97.77% 96.22%
The Trust’s Integrated Urgent and Emergency Care service reported a positive position against the four hour standard for the month of March, Q4 and year end (97.18%). The NHS England published statistical report for the A&E 4 hour standard indicates that only 13 out of the 130 acute providers achieved the standard with the Trust reporting in 1st position (March 2019). The England average reported at 86.6% with the North East position reporting at 93.1%.
On aggregate, the overall IUC activity (Type 1 and Type 3) during Q4 indicates the Trust has seen a net increase of 9.85% (n=3999) compared to the same period last year, with admissions increasing by 8.13% (n=524).
Streaming continues to prove successful with A&E streaming 210 patients into the Urgent Care Centre, 5.55% of the overall patients whopresented at the Type 1 facility.
Emergency activity across the organisation has seen an increase of 9.24% (n=1041) in Q4 compared to the same time last year with emergency activity including 946 patients who were treated via Ambulatory Care, equating to 23.76% of the total emergency admissions.
New Cancer 31 days subsequent Treatment (Drug Therapy) Mar-19 98.0% 100.0% 100.0% The Trust achieved against this standard for Q4 (Latest unvalidated position)
New Cancer 31 days subsequent Treatment (Surgery) Mar-19 94.0% 100.0% 100.0% The Trust achieved against this standard for the month of March and Q4 (Latest unvalidated position)
New Cancer 62 days (consultant upgrade) Mar-19 85.0% 93.3% 95.0%
New Cancer 62 days (screening) Mar-19 90.0% 100.0% 94.6%
New Cancer GP 62 Day (New Rules) Mar-19 85.0% 85.8% 85.6%
Whilst the Trust has achieved against this standard for the month of March pressures persist across most tumour groups with close monitoring on a daily basis. Patient choice, complex pathways and some elective capacity pressures accross the region continue to present a risk to compliance, therefore this standard is highlighted within the Board Assurance Framework. February saw an unusually low number of patients which adversely affected performance (reporting 78.9%), however recovered the position in March and Q4. The year end position is reporting a provisional position of 84.57%.
New Cancer Current 31 Day (New Rules) Mar-19 96.0% 99.1% 99.4%
New Cancer Two week Rule (New Rules) Mar-19 93.0% 94.1% 94.4%
Integrated Performance and Compliance Dashboard - March 2019
SINGLE OVERSIGHT FRAMEWORK
The Trust achieved against this standard for the month of March and Q4 (unvalidated)
The Trust achieved against this standard for the month of March and Q4 (Latest unvalidated position)
Page 2 of 39

Measure (click on
measure for trend graphs)
Reporting
periodTarget Actual Q4 Trend Details
Integrated Performance and Compliance Dashboard - March 2019
SINGLE OVERSIGHT FRAMEWORK
Breast Symptomatic Two week Rule (New Rules) Mar-19 93.0% 94.4% 95.3%
The Trust achieved against this standard for the month of March and Q4 (unvalidated)
Page 3 of 39

Measure (click on
measure for trend graphs)
Reporting
periodTarget Actual Q4 Trend Details
Integrated Performance and Compliance Dashboard - March 2019
SINGLE OVERSIGHT FRAMEWORK
RTT incomplete pathways wait (92%) Mar-19 92.00% 94.43% 94.28%
RTT incomplete pathways wait (92nd percentile) Mar-19 28.00 15.90 16.00
RTT incomplete pathways wait (Median) Mar-19 7.20 4.70 4.90
RTT incomplete pathways >52 week wait Mar-19 0 0 0 No patients waited longer than 52 weeks
Number of patients waiting less than 6 weeks for diagnostic procedures
Mar-19 99.00% 99.51% 99.69% The Trust has sustained recovery against this standard. Actions against this standard in relation to the risk register have now been closed.
CIDs -Referral information Feb-19 50.00% 98.79% -
CIDs- Referral to Treatment information Feb-19 50.00% 96.13% -
CIDs- Treatment Activity Information Feb-19 50.00% 96.44% -
The Trust continues to perform well against the Community Information Datasets, with all standards reporting above the 50% targets.
The Trust reported compliance against the incomplete RTT standard for Q4 and year end. The Trust has achieved the national directive to reduce the overall incomplete waiting list size by March 2019 with a reduction of 1.51% (n=168) decrease against the end of March 2018 position with 10984 patients on the active incomplete waiting list in comparison to March 2018 when 11,152 patients were waiting achieveing the national directive to reduce waiting lists.
Page 4 of 39
Measure (click on
measure for trend graphs)
Reporting
periodTarget Actual Q4 Trend Details
Integrated Performance and Compliance Dashboard - March 2019
SINGLE OVERSIGHT FRAMEWORK
Performance Overview / Key
Highlights
Conclusion and recommendation
The Trust has performed well against a number of standards however on-going pressures remain against the cancer 62 day referral to treatment. The Trust is prepared to pilot NHS Englands new proposed access standards from April 2019.
Whilst the Trust has robust governance processes in place for the monitoring and management of all performance standards there is recognition that current pressures across the whole health economy may ultimately impact on consistent delivery, therefore presents an on-going risk. This risk is outlined within the Trust’s Risk Register and Board Assurance Framework, with supporting mitigation and recovery plans, alongside internal and external governance assurance processes.
Please note:• The positive performance against the key operational, quality and workforce standards.• Recognise the on-going financial and operational pressures.• The detailed review of performance against the Single Oversight Framework requirements and the key national indicators including compliance, workforce, quality and finance.• The on-going operational performance and system risks to regulatory key performance indicators and the intense mitigation work that is being undertaken to address these going forward.Acknowledge the Trusts participation in the national pilot to test the new proposed access standards.
Page 5 of 39

Measure (click on
measure for trend graphs)
Reporting
periodTarget Actual Q4 Trend Details
New to Review ratio (cons led) Feb-19 1.45 1.49 -Aggregate New to Review shows a positive performance against the current target of 1.45 and below peers (latest available data). Consideration for reduction in reviews will be considered by the Transformation and Improvement Committee.
Outpatient DNA (new) Mar-19 5.40% 7.96% 7.93%
Outpatient DNA (review) Mar-19 9.00% 10.49% 10.28%
Average depth of coding Feb-19 3.01 6.60 -
Average depth of coding is reporting in a positive position reflecting the significant work being carried out within the Data Quality Improvement Programme (DQIP). This project is clinically led and focussing on accurate documentation to assist clinical coding processes and delivering subsequent data quality and financial improvements.
Length of Stay Elective Dec-18 3.26 1.68 - The Trust is reporting within target and significantly below the peer target.
Length of Stay Emergency Dec-18 4.17 3.57 - The Trust is reporting within target (includes Ambulatory Care activity).
Day case Rate Dec-18 76.65% 76.51% - No exceptions to report.
Pre - Op Stays Mar-19 4.50% 2.19% 1.76% The internal pre-op stay data indicates the Trust is reporting in a very positive position keeping pre op stays to a minimum.
Integrated Performance and Compliance Dashboard - March 2019
EFFICIENCY AND PRODUCTIVITY
DNA rates continue on a downward trend as a result of the work within the DPP. DNA’s have improved overall by 0.80%, meaning 1478 more patients attended their appointment in 2018/19 improving efficiency.
Page 6 of 39
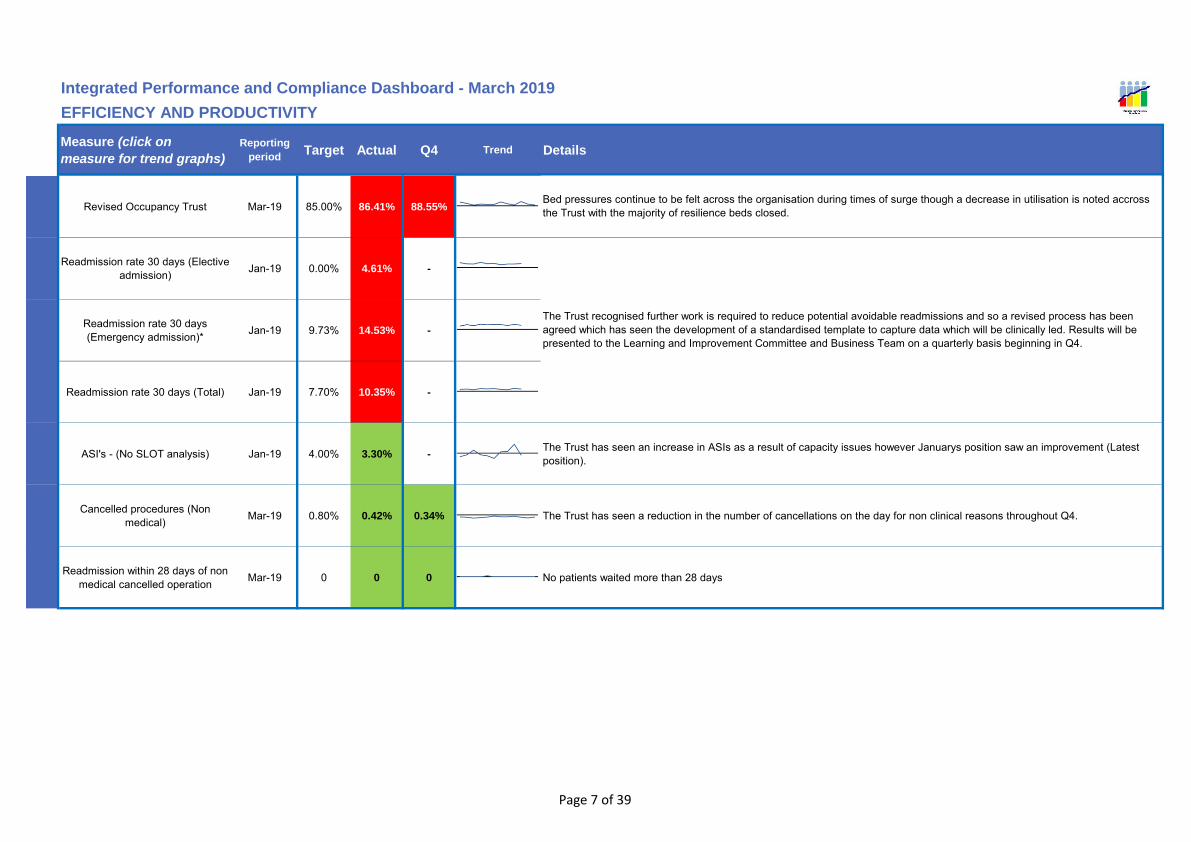
Measure (click on
measure for trend graphs)
Reporting
periodTarget Actual Q4 Trend Details
Integrated Performance and Compliance Dashboard - March 2019
EFFICIENCY AND PRODUCTIVITY
Revised Occupancy Trust Mar-19 85.00% 86.41% 88.55%
Readmission rate 30 days (Elective admission) Jan-19 0.00% 4.61% -
Readmission rate 30 days (Emergency admission)* Jan-19 9.73% 14.53% -
Readmission rate 30 days (Total) Jan-19 7.70% 10.35% -
ASI's - (No SLOT analysis) Jan-19 4.00% 3.30% -The Trust has seen an increase in ASIs as a result of capacity issues however Januarys position saw an improvement (Latest position).
Cancelled procedures (Non medical) Mar-19 0.80% 0.42% 0.34% The Trust has seen a reduction in the number of cancellations on the day for non clinical reasons throughout Q4.
Readmission within 28 days of non medical cancelled operation Mar-19 0 0 0 No patients waited more than 28 days
Bed pressures continue to be felt across the organisation during times of surge though a decrease in utilisation is noted accross the Trust with the majority of resilience beds closed.
The Trust recognised further work is required to reduce potential avoidable readmissions and so a revised process has been agreed which has seen the development of a standardised template to capture data which will be clinically led. Results will be presented to the Learning and Improvement Committee and Business Team on a quarterly basis beginning in Q4.
Page 7 of 39

Measure (click on
measure for trend graphs)
Reporting
periodTarget Actual Q4 Trend Details
Integrated Performance and Compliance Dashboard - March 2019
EFFICIENCY AND PRODUCTIVITY
Number of ambulance handovers between ambulance and A&E
waiting more than 30 minutes *Mar-19 0 8 42
In March the Trust reported 8 ambulance handover greater than 30 minutes. In comparison, the North East average handovers greater than 30 minutes reported at 100 (range 11 – 267).
The Trust’s overall performance in March indicated 73.87% of ambulance handovers (valid) within 15 minutes.
Number of ambulance handovers between ambulance and A&E waiting more than 60 minutes
Mar-19 0 0 4The Trust reported zero validated ambulance handover delay greater than 60 minutes. The North East average over 60 minutes reported at 7 (range 0 – 29).
TCS 19 - % of Community Patients that have had an unplanned
admission LOS <=2 days (Defined set of conditions)
Mar-19 17.00% 14.97% 15.31%
TCS 19 is used to monitor the progress being made in reducing avoidable emergency admissions for patients on a community case load, covering a defined set of conditions : Diabetes complications, Nutritional deficiencies, Iron deficiency anaemia, Hypertension, Congestive heart failure, Angina, Chronic obstructive pulmonary disease and Asthma. No exceptions to report.
TCS 24 - % of Patients achieving improvement using a EQ5 validated assessment tool
Mar-19 93.50% 100.00% 100.00%
TCS 24 - The percentage of patients on a community caseload achieving improvement, as measured using a validated assessment tool appropriate to the scope of the practice, is used by the Community Integrated Assessment Team (CIAT) to monitor progress during/post treatment. No exceptions to report.
TCS 35 - % of standard wheelchair referrals completed within five days Mar-19 90.00% 87.73% 81.24%
Key reason for delay is a result of lack of wheelchair availability due to issues with orders from the company. The service are looking into other providers with a view to trialling a service to ensure comparability of service needs and patient requirements whilst ensuring quality.
Delayed Transfers of Care Mar-19 3.50% 2.11% 2.04%
Super Stranded Reduction (per day average) Mar-19 60 62 62
NHSI have set a trajectory to reduce the number of 'super stranded' patients by an average of 21 per day resulting in a target of 68 by December 2018. This was achieved. A slight increase has been noted in March however significant progress can be seen.
Page 8 of 39

Measure (click on
measure for trend graphs)
Reporting
periodTarget Actual Q4 Trend Details
Integrated Performance and Compliance Dashboard - March 2019
EFFICIENCY AND PRODUCTIVITY
Performance Overview / Key
Highlights
Conclusion and recommendation
* In January the number of ambulance handovers between ambulance and A&E waiting more than 30 minutes was reported at 5. After revalidation the actual number is 23.
The Hospital Evaluation Data (HED) within the main report provides a summary of the Trusts benchmark position against a number of performance indicators covering clinical quality, operational efficiency, patient safety and finance. Success against the reduction in super stranded patients.
The Trust has demonstrated a positive performance against a number of the key operational indicators, supported by the Health Evaluation Data (HED) benchmarking data available in the main menu. The report indicates the Trust is performing above or within expected for the majority of indicators and also demonstrates improvement in indicators where performance has previously been below the national average.
Page 9 of 39

Measure (click on
measure for trend graphs)
Reporting
periodTarget Actual Trend Details
HSMR Mortality Rates(Rolling 12 month value) Jan-19 109.00 96.17
The latest HSMR value is now 96.17 (February 2018 to January 2019), this has decreased from the previously reported 97.79 (January 2018 to December 2018). The value of 96.17 continues to remain inside the ‘as expected’ range; the national mean is 100.
When benchmarked against the same period last year (February 2017 to January 2018) this has decreased from 103.12 to 96.17.
HSMR Crude mortality Rate (Rolling 12 month value) Jan-19 3.46% 3.45%
The Trust crude mortality rate for HSMR has decreased to 3.45% (February 2018 to January 2019) from 3.54% (January 2018 to December 2018).
When benchmarked against the same period last year (February 2017 to January 2018) this has decreased from 3.46% to 3.45%.
SHMI Mortality rate(Rolling 12 month value) Sep-18 111.43 100.72
The latest SHMI value is now 100.72 (October 2017 to September 2018), this has decreased from 101.64 (September 2017 to August 2018).
Trusts SHMI which is released each quarter has seen a reduction from the previously reported Q1 2018/19 position of 103.02 to 100.72 in Q2 2018/19.
SHMI Crude mortality Rate (Rolling 12 month value) Sep-18 3.50% 3.49%
The Trust crude mortality rate for SHMI has decreased to 3.49% (October 2017 to September 2018) from 3.54% (September 2017 to August 2018).
When benchmarked against the same period last year (October 2016 to September 2017) this has decreased from 3.50% to 3.49%.
Dementia - % of patients aged 75 and over, admitted as emergencies,
stayed more than 72 hours and were asked the dementia case
finding question
Feb-19 90.00% 100.00%The Trust is reporting that 100% of patients aged 75 and over, who were admitted as emergencies, stayed more than 72 hours were asked the dementia case finding question.
Dementia - % of patients undergone a diagnostic assessment Feb-19 90.00% 100.00% The Trust is reporting that 100% of patients identified as potentially having dementia underwent a diagnostic assessment.
Integrated Performance and Compliance Dashboard - March 2019
QUALITY AND SAFETY
Page 10 of 39

Measure (click on
measure for trend graphs)
Reporting
periodTarget Actual Trend Details
Integrated Performance and Compliance Dashboard - March 2019
QUALITY AND SAFETY
Dementia - % of those that received a diagnostic assessment that were
referred onto another service or back to GP
Feb-19 90.00% 100.00% The Trust is reporting that 100% of those that received a diagnostic assessment were referred onto another service or back to GP.
Page 11 of 39

Measure (click on
measure for trend graphs)
Reporting
periodTarget Actual Trend Details
Integrated Performance and Compliance Dashboard - March 2019
QUALITY AND SAFETY
Complaint Stage 1 - Informal Mar-19 59 60
The Trust is reporting 60 stage 1 complaints for March 2019. This has decreased from the 64 stage 1 complaints in February 2019.
When benchmarked against the same period last year (March 18) this has increased from 59 to 60.
For quarter 4, there were 197 stage 1 complaints, compared with 193 from quarter 4 2017/18.
For 2018/19, there were 725 stage 1 complaints compared with 822 for 2017/18.
Complaint Stage 2 - Formal Meeting Mar-19 8 8
The Trust is reporting 8 stage 2 complaints for March 2019. This has decreased from the 13 stage 2 complaints in February 2019.
When benchmarked against the same period last year (March 18) this has remained the same at 8.
For quarter 4, there were 26 stage 2 complaints, compared with 28 from quarter 4 2017/18.
For 2018/19, there were 100 stage 2 complaints compared with 104 for 2017/18.
Complaint Stage 3 - Formal Chief Executive Letter Mar-19 7 10
The Trust is reporting 10 stage 3 complaints for March 2019. This has decreased from the 30 stage 3 complaints in February 2019.
When benchmarked against the same period last year (March 18) this has increased from 7 to 10.
For quarter 4, there were 54 stage 3 complaints, compared with 44 from quarter 4 2017/18.
For 2018/19, there were 192 stage 3 complaints compared with 183 for 2017/18.
Complaint response times % (25 days) Feb-19 85.00% 93.00% The Trusts response rate for Formal - Stage 3 complaints for February 2019 was 93%.
Never Events Mar-19 0 0 There have been no Never Events in the reporting period.
Page 12 of 39

Measure (click on
measure for trend graphs)
Reporting
periodTarget Actual Trend Details
Integrated Performance and Compliance Dashboard - March 2019
QUALITY AND SAFETY
Grade 2 Pressure Ulcers (In-Hospital) Feb-19 20 28
The Trust is reporting 28 grade 2 pressure ulcers for February 2019. This has increased from the 15 grade 2 ulcers reported for January 2019.
When benchmarked against the same period last year (February 18) this has increased from 20 to 28.
Grade 3 Pressure Ulcers (In-Hospital) Feb-19 1 4
The Trust is reporting 4 grade 3 pressure ulcers for February 2019. This has increased from the 3 grade 3 ulcers reported for January 2019.
When benchmarked against the same period last year (February 18) this has increased from 1 to 4.
Grade 4 Pressure Ulcers (In-Hospital) Feb-19 0 1
The Trust is reporting 1 grade 4 pressure ulcer for February 2019. This has increased from the zero grade 4 ulcers reported for January 2019.
When benchmarked against the same period last year (February 18) this has increased from 0 to 1.
Page 13 of 39
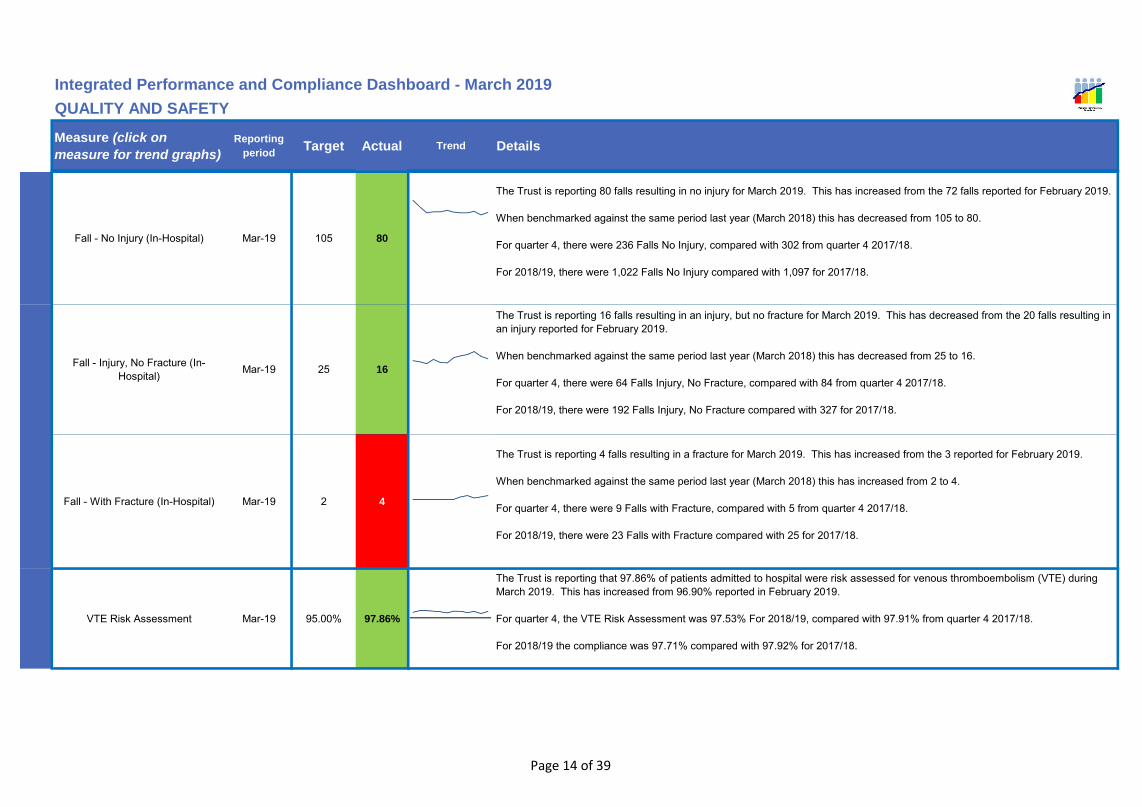
Measure (click on
measure for trend graphs)
Reporting
periodTarget Actual Trend Details
Integrated Performance and Compliance Dashboard - March 2019
QUALITY AND SAFETY
Fall - No Injury (In-Hospital) Mar-19 105 80
The Trust is reporting 80 falls resulting in no injury for March 2019. This has increased from the 72 falls reported for February 2019.
When benchmarked against the same period last year (March 2018) this has decreased from 105 to 80.
For quarter 4, there were 236 Falls No Injury, compared with 302 from quarter 4 2017/18.
For 2018/19, there were 1,022 Falls No Injury compared with 1,097 for 2017/18.
Fall - Injury, No Fracture (In-Hospital) Mar-19 25 16
The Trust is reporting 16 falls resulting in an injury, but no fracture for March 2019. This has decreased from the 20 falls resulting in an injury reported for February 2019.
When benchmarked against the same period last year (March 2018) this has decreased from 25 to 16.
For quarter 4, there were 64 Falls Injury, No Fracture, compared with 84 from quarter 4 2017/18.
For 2018/19, there were 192 Falls Injury, No Fracture compared with 327 for 2017/18.
Fall - With Fracture (In-Hospital) Mar-19 2 4
The Trust is reporting 4 falls resulting in a fracture for March 2019. This has increased from the 3 reported for February 2019.
When benchmarked against the same period last year (March 2018) this has increased from 2 to 4.
For quarter 4, there were 9 Falls with Fracture, compared with 5 from quarter 4 2017/18.
For 2018/19, there were 23 Falls with Fracture compared with 25 for 2017/18.
VTE Risk Assessment Mar-19 95.00% 97.86%
The Trust is reporting that 97.86% of patients admitted to hospital were risk assessed for venous thromboembolism (VTE) during March 2019. This has increased from 96.90% reported in February 2019.
For quarter 4, the VTE Risk Assessment was 97.53% For 2018/19, compared with 97.91% from quarter 4 2017/18.
For 2018/19 the compliance was 97.71% compared with 97.92% for 2017/18.
Page 14 of 39

Measure (click on
measure for trend graphs)
Reporting
periodTarget Actual Trend Details
Integrated Performance and Compliance Dashboard - March 2019
QUALITY AND SAFETY
Hand Hygiene Compliance Mar-19 95.00% 97.00%
The overall Trust compliance score for hand hygiene is 97% for March 2019; this has increased from 96% reported in February 2019.
For quarter 4, the hand hygiene compliance was 96% For 2018/19, compared with 97% from quarter 4 2017/18.
For 2018/19 the compliance was 97% compared with 97% for 2017/18.
Page 15 of 39

Measure (click on
measure for trend graphs)
Reporting
periodTarget Actual Trend Details
Integrated Performance and Compliance Dashboard - March 2019
QUALITY AND SAFETY
Clostridium difficile (C.diff) Mar-19 1 2
The Trust is reporting 2 Trust attributed cases of Clostridium difficile infection for March 2019. This has reduced from the previously reported 5 cases in February 2019.
When benchmarked against the same reporting period last year (March 2018) this has decreased from 4 to 2 cases.
For quarter 4, the Trust reported 12 Trust attributed cases of Clostridium difficile, with a total of 31 cases over 2018/19, this has decreased from 35 cases in 2017/18.
Methicillin-Resistant Staphylococcus Aureus (MRSA) bacteraemia Mar-19 0 0
The Trust is reporting zero Trust attributed cases of MRSA bacteraemia in March 2019. This remains the same from previous reporting period and the target of zero cases.
For quarter 4, the Trust reported zero Trust attributed cases of MRSA, with a total of zero cases over 2018/19, this has decreased from 4 cases in 2017/18.
Methicillin-Sensitive Staphylococcus Aureus (MSSA) bacteraemia Mar-19 4 1
The Trust is reporting 1 Trust attributed case of MSSA bacteraemia for March 2019. This has decreased from the 3 reported cases in February 2019.
When benchmarked against the same period last year (March 2018) this has decreased from 4 to 1 case.
For quarter 4, the Trust reported 5 Trust attributed cases of MSSA, with a total of 21 cases over 2018/19, this has decreased from 25 cases in 2017/18.
Escherichia coli (E.coli) Mar-19 1 3
The Trust is reporting 3 Trust attributed cases of E coli bacteraemia in March 2019. This has increased from the 1 reported case in February 2019.
The Trust has set a target of 10% reduction throughout the year; to achieve this, the Trust is participating in a Tees-wide collaborative project.
When benchmarked against the same period last year (March 2018) this has increased from 1 to 3.
For quarter 4, the Trust reported 6 Trust attributed cases of E.coli, with a total of 39 cases over 2018/19, this has decreased from 43 cases in 2017/18. Therefore achieving the target.
Page 16 of 39

Measure (click on
measure for trend graphs)
Reporting
periodTarget Actual Trend Details
Integrated Performance and Compliance Dashboard - March 2019
QUALITY AND SAFETY
Klebsiella species bacteraemia (Kleb sp) Mar-19 2 1
The Trust has reported 1 Trust attributed case of Klebsiella species bacteraemia in March 2019. This has decreased from the 2 reported cases in February 2019.
The Trust has set a target of 10% reduction throughout the year.
When benchmarked against the same period last year (March 2018) this has decreased from 2 to 1.
For quarter 4, the Trust reported 4 Trust attributed cases of Klebsiella species bacteraemia, with a total of 20 cases over 2018/19, this has decreased from 29 cases in 2017/18. Therefore exceeding the reduction target.
Pseudomonas aeruginosa bacteraemia (Ps a) Mar-19 0 0
The Trust has reported zero Trust attributed cases of Pseudomonas aeruginosa bacteraemia in March 2019. This has decreased from the 1 cases previously reported in February 2019.
The Trust has set a target of 10% reduction throughout the year.
When benchmarked against the same period last year (March 2018) this has remained the same at zero cases.For quarter 4, the Trust reported 1 Trust attributed cases of Pseudomonas aeruginosa bacteraemia, with a total of 9 cases over 2018/19, this has increased from 5 cases in 2017/18. Therefore, not achieving the target for this HCAI.
Page 17 of 39

Measure (click on
measure for trend graphs)
Reporting
periodTarget Actual Trend Details
Integrated Performance and Compliance Dashboard - March 2019
QUALITY AND SAFETY
Friends & Family - (Ward) [National Score based on % ‘extremely likely’
& 'Likely' to recommend to F&F]Mar-19 70.00% 98%
The in-patient position for Friends and Family for ‘Would Recommend’ was 98% for March 2019; this increased from the previously reported 97% in February 2019.
Friends & Family - (A&E)[National Score based on % ‘extremely likely’ & 'Likely' to
recommend to F&F]
Mar-19 70.00% 88%The A&E position for Friends and Family for ‘Would Recommend’ was 88% for March 2019; this has decreased from the reported 89% in February 2019.
Friends & Family - (Birth)[National Score based on % ‘extremely likely’ & 'Likely' to
recommend to F&F]
Mar-19 70.00% 98%For maternity – (Question 2 – birth) the Friends and Family ‘Would Recommend’ is 98% for March 2019; this has decreased from the reported 100% in February 2019.
Patient and Staff Experience Score (100% max) Mar-19 90.00% 96.41%
For the month of March 2019 the patient and staff experience score was 96.41%, this has increased from 94.33% in February 2019.
For quarter 4, the patient and Staff experience score was 94.23%. For 2018/19 the overall patient and staff experience score was 93.91%.
Patient and Staff Experience Survey Number of surveys undertaken Mar-19 20 19
For the month of March 2019, there were a total of 19 Patient and Staff audits conducted. This has increased from the previous month when 15 audits were carried out. A continued effort is being made by the department to ensure that the audits are carried out in a timely manner.
For quarter 4, there were 56 audits carried out and throughout 2018/19, 249 audits were conducted.
Registered Nurse/Midwife day shift fill rates Mar-19 >=80% and
<=109.99% 84.82%Registered Nurse/Midwife day shift fill rates across inpatient areas for the month of March 2019 is 84.82%, down from 85.38% in February 2019.
Registered Nurse/Midwife Night shift fill rates Mar-19 >=80% and
<=109.99% 91.32%Registered Nurse/Midwife night shift fill rates across inpatient areas for the month of March 2019 is 91.32% down from 93.56% in February 2019.
Page 18 of 39

Measure (click on
measure for trend graphs)
Reporting
periodTarget Actual Trend Details
Integrated Performance and Compliance Dashboard - March 2019
QUALITY AND SAFETY
Care Staff day shift fill rates Mar-19 >=80% and <=109.99% 92.55% Care Staff day shift fill rates across inpatient areas for the month of March 2019 is 92.55% up from 89.11% in February 2019.
Care Staff Night shift fill rates Mar-19 >=80% and <=109.99% 119.03% Care Staff night shift fill rates across inpatient areas for the month of March 2019 is 119.03% up from 117.87% in February 2019.
Trust - Harm Free Care % Mar-19 97.84% 98.49% The Trusts overall Harm Free care in March 2019 was 98.49% this has decreased from 98.75% in February 2019.
Deep Dive Visits Mar-19 90.00% 90.28%The Trust conducts monthly deep dive visits within areas of the Trust. For the month of March 2019, the deep dive audit scored 90.28%. This has decreased from the previous reported audit score of 94.81% in February 2019.
Performance Overview / Key
Highlights
Conclusion and recommendationThe Board of Directors is asked to note the content of the report; current performance and work to continuously improve. The Board are asked to note the excellent HSMR and SHMI values which continue to remain within the expected range and the continued improvement in HCAI despite the disappointing pseudomonas performance.
The latest data for the Trusts HSMR is 96.17, this has decreased from the previously reported 97.79 and the Trusts SHMI which is released each quarter has seen a month on month reduction from 101.64 to 100.72, with a reduction from the previously reported Q4 2017/18 position of 103.02 to 100.72.
The Trust has seen a financial year improvement of 11.43% in C difficile rates compared to 2017/18, when the Trust reported 35 cases, against the 31 for 2018/19. Whilst the pseudomonas target has not been achieved this year, the target for e coli and Klebsiella has been exceeded. Route Cause Analysis of the Pseudomonas cases has not identified any themes or trends.
Page 19 of 39
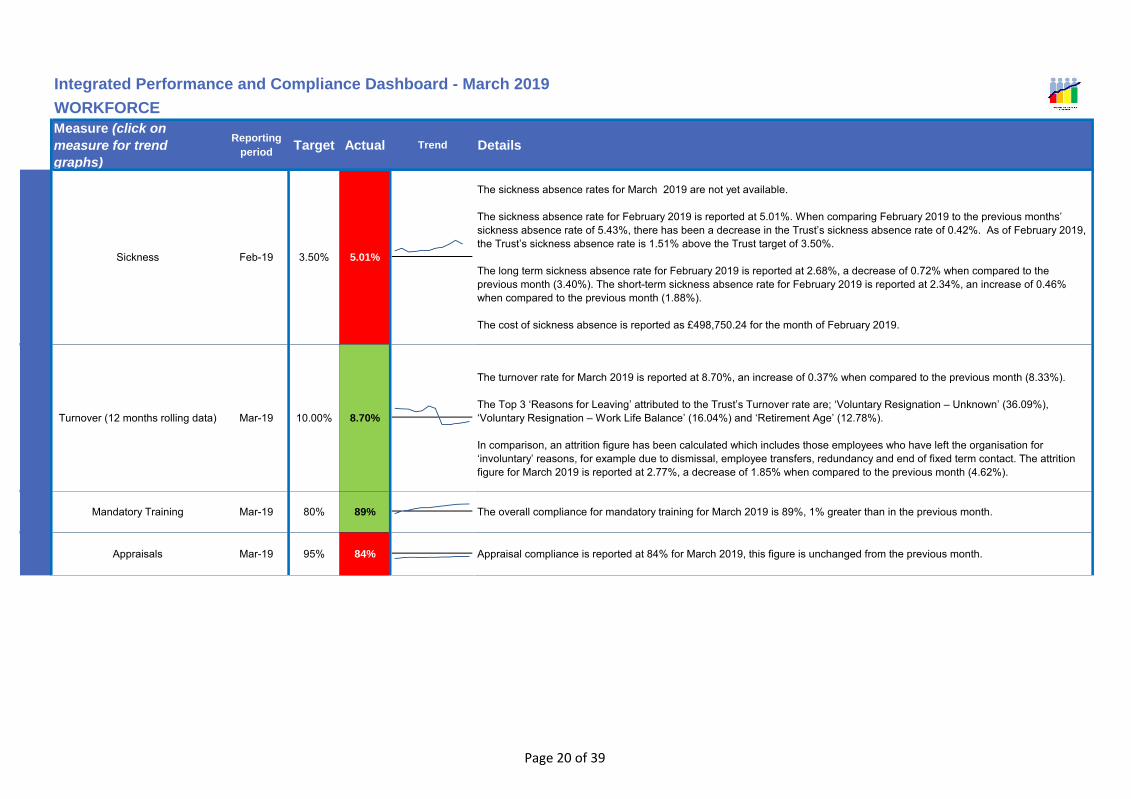
Measure (click on
measure for trend
graphs)
Reporting
periodTarget Actual Trend Details
Sickness Feb-19 3.50% 5.01%
The sickness absence rates for March 2019 are not yet available.
The sickness absence rate for February 2019 is reported at 5.01%. When comparing February 2019 to the previous months’ sickness absence rate of 5.43%, there has been a decrease in the Trust’s sickness absence rate of 0.42%. As of February 2019, the Trust’s sickness absence rate is 1.51% above the Trust target of 3.50%.
The long term sickness absence rate for February 2019 is reported at 2.68%, a decrease of 0.72% when compared to the previous month (3.40%). The short-term sickness absence rate for February 2019 is reported at 2.34%, an increase of 0.46% when compared to the previous month (1.88%).
The cost of sickness absence is reported as £498,750.24 for the month of February 2019.
Turnover (12 months rolling data) Mar-19 10.00% 8.70%
The turnover rate for March 2019 is reported at 8.70%, an increase of 0.37% when compared to the previous month (8.33%).
The Top 3 ‘Reasons for Leaving’ attributed to the Trust’s Turnover rate are; ‘Voluntary Resignation – Unknown’ (36.09%), ‘Voluntary Resignation – Work Life Balance’ (16.04%) and ‘Retirement Age’ (12.78%).
In comparison, an attrition figure has been calculated which includes those employees who have left the organisation for ‘involuntary’ reasons, for example due to dismissal, employee transfers, redundancy and end of fixed term contact. The attrition figure for March 2019 is reported at 2.77%, a decrease of 1.85% when compared to the previous month (4.62%).
Mandatory Training Mar-19 80% 89% The overall compliance for mandatory training for March 2019 is 89%, 1% greater than in the previous month.
Appraisals Mar-19 95% 84% Appraisal compliance is reported at 84% for March 2019, this figure is unchanged from the previous month.
WORKFORCE
Integrated Performance and Compliance Dashboard - March 2019
Page 20 of 39

Measure (click on
measure for trend
graphs)
Reporting
periodTarget Actual Trend Details
WORKFORCE
Integrated Performance and Compliance Dashboard - March 2019
Page 21 of 39

Measure (click on
measure for trend
graphs)
Reporting
periodTarget Actual Trend Details
WORKFORCE
Integrated Performance and Compliance Dashboard - March 2019
Performance Overview / Key
Highlights
Conclusion and recommendation
North Tees & Hartlepool NHS Foundation Trust
‘Anxiety/stress/depression/other psychiatric illnesses’ continues to account for the highest proportion of all sickness absence reasons at 28%.
The Trust Stress group has met a number of times with a pilot of the ‘Tackling Stress in the Northern Region’ survey planned to commence April 2019; in partnership with staff side.
It was agreed at Trust ETM in March 2019 that a new absence management process be implemented; whereby senior managers within directorates will be required to attend DET when they continually fail to achieve the sickness absence target. The new approach will intentionally focus directorates’ attention on proactively managing absence within their area; reinforcing ownership, responsibility and accountability of managers for absence.
The Board is asked to note the contents within the workforce report and positive performance against standards together with the on-going work to integrate performance reporting.
Page 22 of 39

Measure KPI Period Apr-18 May-18 Jun-18 Q1 Jul-18 Aug-18 Sep-18 Q2 Oct-18 Nov-18 Dec-18 Q3 Jan-19 Feb-19 Mar-19 Q4
AE Target Mar-19 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00%
AE Emergency Care 4 hr standard Mar-19 97.75% 97.64% 98.06% 97.81% 97.71% 97.73% 97.26% 97.57% 96.73% 97.65% 97.09% 97.14% 95.38% 95.54% 97.77% 96.22%
Target Mar-19 98.0% 98.0% 98.0% 98.0% 98.0% 98.0% 98.0% 98.0% 98.0% 98.0% 98.0% 98.0% 98.0% 98.0% 98.0% 98.0%
Cancer *New Cancer 31 days subsequent Treatment (Drug Therapy) Mar-19 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%
Target Mar-19 94.0% 94.0% 94.0% 94.0% 94.0% 94.0% 94.0% 94.0% 94.0% 94.0% 94.0% 94.0% 94.0% 94.0% 94.0% 94.0%
CancerNew Cancer 31 days subsequent Treatment (Surgery) Mar-19 100.0% 94.7% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 94.7% 100.0% 97.9% 100.0% 100.0% 100.0% 100.0%
Target Mar-19 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0%
New Cancer 62 days (consultant upgrade) Mar-19 33.3% 90.9% No
patients70.6% 100.0% 100.0% 100.0% 100.0% No
patients 100.0% 100.0% 100.0% 93.3% 100.0% 93.3% 95.0%
Target Mar-19 90.0% 90.0% 90.0% 90.0% 90.0% 90.0% 90.0% 90.0% 90.0% 90.0% 90.0% 90.0% 90.0% 90.0% 90.0% 90.0%
Cancer New Cancer 62 days (screening) Mar-19 94.1% 94.8% 96.8% 95.4% 97.6% 100.0% 96.1% 97.5% 96.1% 98.6% 95.9% 96.9% 90.9% 93.5% 100.0% 94.6%
Target Mar-19 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0%
New Cancer GP 62 Day (New Rules) Mar-19 86.5% 85.0% 76.7% 83.4% 84.4% 82.1% 87.0% 84.7% 82.7% 89.9% 82.1% 85.0% 90.5% 78.9% 85.8% 85.6%
Target Mar-19 96.0% 96.0% 96.0% 96.0% 96.0% 96.0% 96.0% 96.0% 96.0% 96.0% 96.0% 96.0% 96.0% 96.0% 96.0% 96.0%
Cancer New Cancer Current 31 Day (New Rules) Mar-19 99.2% 99.3% 100.0% 99.5% 99.3% 97.4% 100.0% 99.0% 100.0% 99.2% 100.0% 99.7% 99.2% 100.0% 99.1% 99.4%
Target Mar-19 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0%
New Cancer Two week Rule (New Rules) Mar-19 93.6% 93.6% 93.0% 93.4% 94.0% 93.6% 93.5% 93.7% 95.6% 94.6% 94.3% 94.8% 94.7% 94.6% 94.1% 94.4%
Target Mar-19 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0% 93.0%
Cancer Breast Symptomatic Two week Rule (New Rules) Mar-19 94.7% 96.9% 94.4% 95.4% 97.7% 99.2% 98.5% 98.5% 98.9% 95.5% 93.1% 95.8% 95.3% 96.6% 94.4% 95.3%
Integrated Performance and Compliance Dashboard - March 2019
APPENDIX 1 - SINGLE OVERSIGHT FRAMEWORK
Page 23 of 39

Measure KPI Period Apr-18 May-18 Jun-18 Q1 Jul-18 Aug-18 Sep-18 Q2 Oct-18 Nov-18 Dec-18 Q3 Jan-19 Feb-19 Mar-19 Q4
Integrated Performance and Compliance Dashboard - March 2019
APPENDIX 1 - SINGLE OVERSIGHT FRAMEWORK
Target Mar-19 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00%
RTT RTT incomplete pathways wait (92%) Mar-19 93.66% 94.43% 94.25% 94.12% 94.48% 94.06% 93.83% 94.13% 94.14% 94.63% 93.64% 94.15% 93.85% 94.54% 94.43% 94.28%
Target Mar-19 28.00 28.00 28.00 28.00 28.00 28.00 28.00 28.00 28.00 28.00 28.00 28.00 28.00 28.00 28.00 28.00
RTT RTT incomplete pathways wait (92nd percentile) Mar-19 15.90 15.90 16.10 15.90 15.60 16.00 16.30 16.00 16.30 15.60 16.40 16.10 16.30 15.90 15.90 16.00
Target Mar-19 7.20 7.20 7.20 7.20 7.20 7.20 7.20 7.20 7.20 7.20 7.20 7.20 7.20 7.20 7.20 7.20
RTT RTT incomplete pathways wait (Median) Mar-19 5.00 5.40 5.40 5.40 5.40 5.40 5.70 5.60 5.00 4.40 5.70 5.10 4.90 4.90 4.70 4.90
Target Mar-19 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
RTT RTT incomplete pathways >52 week wait Mar-19 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Target Mar-19 99.00% 99.00% 99.00% 99.00% 99.00% 99.00% 99.00% 99.00% 99.00% 99.00% 99.00% 99.00% 99.00% 99.00% 99.00% 99.00%
DiagnosticsNumber of patients waiting less than 6 weeks for diagnostic procedures Mar-19 96.22% 97.24% 98.39% 97.30% 98.97% 96.22% 99.25% 98.16% 99.38% 99.86% 99.92% 99.72% 99.73% 99.82% 99.51% 99.69%
Target Feb-19 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00%
CIDS CIDs -Referral information Feb-19 96.44% 96.89% 96.67% 96.67% 96.82% 96.03% 96.72% 96.52% 96.57% 96.47% 96.74% 96.59% 95.59% 98.79% 0.00%
Target Feb-19 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00%
CIDS CIDs- Referral to Treatment information Feb-19 96.54% 96.05% 96.55% 96.57% 96.00% 96.22% 96.20% 96.14% 95.38% 96.09% 96.06% 95.85% 96.06% 96.13% 0.00%
Target Feb-19 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00%
CIDS CIDs- Treatment Activity Information Feb-19 97.15% 98.62% 96.56% 97.46% 96.54% 96.59% 97.40% 96.83% 95.72% 96.26% 97.64% 96.49% 96.94% 96.44% 0.00%
* Unvalidated position
Page 24 of 39

Measure KPI Period Apr-18 May-18 Jun-18 Q1 Jul-18 Aug-18 Sep-18 Q2 Oct-18 Nov-18 Dec-18 Q3 Jan-19 Feb-19 Mar-19 Q4
New to review Target Feb-19 1.45 1.45 1.45 1.45 1.45 1.45 1.45 1.45 1.45 1.45 1.45 1.45 1.45 1.45 1.45
New to review New to Review ratio (cons led) Feb-19 1.22 1.20 1.24 1.24 1.24 1.19 1.31 1.25 1.25 1.34 1.21 1.27 1.28 1.49 0.00
Target Mar-19 5.40% 5.40% 5.40% 5.40% 5.40% 5.40% 5.40% 5.40% 5.40% 5.40% 5.40% 5.40% 5.40% 5.40% 5.40% 5.40%
DNA Outpatient DNA (new) Mar-19 7.53% 7.50% 7.38% 7.17% 7.67% 8.69% 7.66% 8.06% 8.76% 7.82% 8.49% 8.28% 8.00% 7.75% 7.96% 7.93%
Target Mar-19 9.00% 9.00% 9.00% 9.00% 9.00% 9.00% 9.00% 9.00% 9.00% 9.00% 9.00% 9.00% 9.00% 9.00% 9.00% 9.00%
Outpatient DNA (review) Mar-19 9.08% 9.02% 9.55% 9.60% 9.97% 10.10% 9.84% 9.92% 10.08% 9.53% 9.91% 9.83% 10.32% 9.95% 10.49% 10.28%
Target Feb-19 3.01 3.01 3.01 3.01 3.01 3.01 3.01 3.01 3.01 3.01 3.01 3.01 3.01 3.01 3.01
Coding Average depth of coding Feb-19 6.16 5.51 6.25 6.25 6.36 6.43 6.49 6.49 6.55 6.59 6.60 6.60 6.60 6.60 0.00
Target Dec-18 3.30 3.30 3.29 3.30 3.27 3.26 3.26 3.26 3.25 3.25 3.26 3.25
LOS Length of Stay Elective Dec-18 1.84 1.82 1.70 1.70 1.72 1.65 1.62 1.62 1.63 1.64 1.68 1.68 0.00
Target Dec-18 4.29 4.28 4.06 4.21 4.24 4.23 4.21 4.23 4.20 4.19 4.17 4.19
Length of Stay Emergency Dec-18 3.77 3.73 3.72 3.72 3.73 3.70 3.66 3.66 3.64 3.61 3.57 3.57 0.00
Target Dec-18 76.30% 76.47% 76.11% 76.29% 76.38% 76.47% 76.76% 76.54% 76.65% 76.60% 76.65% 76.63%
Day case Day case Rate Dec-18 76.45% 77.10% 77.25% 77.25% 77.57% 77.41% 76.77% 76.77% 76.21% 76.20% 76.51% 76.51% 0.00%
Target Mar-19 4.50% 4.50% 4.50% 4.50% 4.50% 4.50% 4.50% 4.50% 4.50% 4.50% 4.50% 4.50% 4.50% 4.50% 4.50% 4.50%
Pre - Op Stays Mar-19 1.88% 1.30% 2.74% 2.75% 2.02% 1.46% 1.87% 2.09% 1.32% 1.32% 3.48% 2.24% 1.15% 0.59% 2.19% 1.76%
Target Mar-19 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00%
Occupancy Revised Occupancy North Tees Mar-19 92.64% 90.46% 88.48% 90.56% 90.72% 90.36% 89.96% 90.35% 92.02% 89.35% 87.77% 89.55% 92.59% 88.84% 87.75% 89.78%
Target Mar-19 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00%
Revised Occupancy Hartlepool Mar-19 68.48% 71.55% 62.63% 67.58% 57.29% 53.42% 53.73% 54.87% 75.48% 70.83% 62.08% 69.59% 75.15% 70.77% 67.19% 71.09%
Target Mar-19 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00%
Revised Occupancy Trust Mar-19 90.59% 88.78% 86.13% 88.53% 87.70% 87.05% 87.08% 87.28% 90.85% 88.08% 86.40% 88.27% 91.45% 87.63% 86.41% 88.55%
Integrated Performance and Compliance Dashboard - March 2019 (2018-2019 against target)
APPENDIX 2 - EFFICIENCY AND PRODUCTIVITY
Page 25 of 39

Measure KPI Period Apr-18 May-18 Jun-18 Q1 Jul-18 Aug-18 Sep-18 Q2 Oct-18 Nov-18 Dec-18 Q3 Jan-19 Feb-19 Mar-19 Q4
Integrated Performance and Compliance Dashboard - March 2019 (2018-2019 against target)
APPENDIX 2 - EFFICIENCY AND PRODUCTIVITY
Target Feb-19 972 972 998 2942 998 965 998 2961 998 998 998 2994 998 998 998
Bed days Excess bed days Feb-19 514 742 718 1974 466 550 432 1448 335 358 230 923 399 289 0
Target Mar-19 668 753 535 1956 535 535 535 1605 535 535 535 1605 535 535 535 1605
Delayed bed days Mar-19 619 575 753 1947 704 434 296 1437 342 377 383* 1098 383* 250* 322 955
Target Jan-19 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00%
Readmissions * Readmission rate 30 days (Elective admission) Jan-19 5.69% 4.21% 3.99% 4.92% 5.95% 4.51% 4.88% 5.22% 3.40% 4.07% 4.13% 3.80% 4.61% 0.00%
Target Jan-19 9.73% 9.73% 9.73% 9.73% 9.73% 9.73% 9.73% 9.73% 9.73% 9.73% 9.73% 9.73% 9.73% 9.73% 9.73%
Readmission rate 30 days (Emergency admission)* Jan-19 13.55% 15.08% 14.01% 16.46% 15.65% 14.87% 15.35% 15.29% 15.22% 14.29% 15.38% 15.19% 14.53% 0.00%
Target Jan-19 7.70% 7.70% 7.70% 7.70% 7.70% 7.70% 7.70% 7.70% 7.70% 7.70% 7.70% 7.70% 7.70% 7.70% 7.70%
Readmission rate 30 days (Total) Jan-19 9.92% 10.29% 9.52% 10.96% 10.78% 10.46% 10.82% 10.69% 9.82% 9.46% 10.96% 10.15% 10.35% 0.00%
Target Mar-1995.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00%
EDSElectronic Discharge Summaries within 24 hours (incl. A&E) Mar-19 69.42% 88.72% 87.28% 82.20% 87.46% 87.85% 89.33% 88.21% 90.30% 90.69% 88.26% 89.78% 90.90% 88.96% 89.17% 89.73%
Target Mar-19 15.60% 15.60% 15.60% 15.60% 15.60% 15.60% 15.60% 15.60% 15.60% 15.60% 15.60% 15.60% 15.60% 15.60% 15.60% 15.60%
C-sections Emergency c-section rates Mar-19 11.57% 8.82% 9.00% 12.43% 9.02% 12.05% 17.78% 12.84% 10.80% 11.11% 13.33% 11.74% 13.07% 13.00% 18.57% 15.76%
Target Jan-19 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00%
ASI's ASI's - (No SLOT analysis) Jan-19 2.70% 3.40% 5.10% 3.74% 3.40% 3.00% 2.10% 2.80% 4.50% 4.60% 7.30% 5.30% 3.30% 0.00%
Target Mar-19 72.86% 72.86% 72.86% 72.86% 72.86% 72.86% 72.86% 72.86% 72.86% 72.86% 72.86% 72.86% 72.86% 72.86% 72.86% 72.86%
Theatres Operation Time Utilisation Mar-19 85.12% 75.15% 72.90% 73.16% 75.91% 75.33% 75.58% 75.56% 75.73% 75.83% 74.66% 75.52% 73.64% 73.55% 76.70% 74.57%
Target Mar-19 87.07% 87.07% 87.07% 87.07% 87.07% 87.07% 87.07% 87.07% 87.07% 87.07% 87.07% 87.07% 87.07% 87.07% 87.07% 87.07%
Run Time Utilisation Mar-19 86.08% 88.83% 87.82% 87.33% 91.60% 91.19% 89.91% 90.84% 89.86% 90.12% 88.61% 89.72% 88.50% 87.71% 90.16% 88.68%
Target Mar-19 92.50% 92.50% 92.50% 92.50% 92.50% 92.50% 92.50% 92.50% 92.50% 92.50% 92.50% 92.50% 92.50% 92.50% 92.50% 92.50%
Planned Session Utilisation Mar-19 95.41% 96.81% 94.98% 95.87% 96.40% 93.85% 94.48% 94.31% 93.51% 93.53% 90.26% 92.50% 95.02% 88.46% 89.73% 91.26%
Page 26 of 39

Measure KPI Period Apr-18 May-18 Jun-18 Q1 Jul-18 Aug-18 Sep-18 Q2 Oct-18 Nov-18 Dec-18 Q3 Jan-19 Feb-19 Mar-19 Q4
Integrated Performance and Compliance Dashboard - March 2019 (2018-2019 against target)
APPENDIX 2 - EFFICIENCY AND PRODUCTIVITY
Target Mar-19 0.80% 0.80% 0.80% 0.80% 0.80% 0.80% 0.80% 0.80% 0.80% 0.80% 0.80% 0.80% 0.80% 0.80% 0.80% 0.80%
Cancelled procedures (Non medical) Mar-19 0.43% 0.38% 0.23% 0.34% 0.32% 0.41% 0.58% 0.47% 0.46% 0.48% 0.55% 0.49% 0.36% 0.25% 0.42% 0.34%
Target Mar-19 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Readmission within 28 days of non medical cancelled operation Mar-19 0 0 0 0 0 1 0 1 0 0 0 0 0 0 0 0
Target Mar-19 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Cancelled Urgent Operations for second time Mar-19 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Target Mar-19 8.80% 8.80% 8.80% 8.80% 8.80% 8.80% 8.80% 8.80% 8.80% 8.80% 8.80% 8.80% 8.80% 8.80% 8.80% 8.80%
Cancelled on day of operation Mar-19 7.65% 7.02% 6.14% 7.03% 7.28% 7.26% 8.19% 7.85% 8.37% 8.23% 9.20% 8.51% 7.52% 8.25% 6.73% 7.77%
Target Mar-19 33.11% 33.11% 33.11% 33.11% 33.11% 33.11% 33.11% 33.11% 33.11% 33.11% 33.11% 33.11% 33.11% 33.11% 33.11% 33.11%
Late Start % Mar-19 35.00% 34.45% 40.86% 36.76% 32.26% 38.93% 32.73% 34.50% 33.44% 36.36% 39.82% 37.28% 40.86% 33.46% 31.18% 35.44%
Target Mar-19 46.13% 46.13% 46.13% 46.13% 46.13% 46.13% 46.13% 46.13% 46.13% 46.13% 46.13% 46.13% 46.13% 46.13% 46.13% 46.13%
Early Finishes % Mar-19 56.68% 42.38% 49.17% 47.13% 38.35% 43.03% 40.36% 40.53% 42.90% 42.74% 44.69% 43.26% 49.83% 48.85% 41.83% 46.97%
Target Mar-19 12.89% 12.89% 12.89% 12.89% 12.89% 12.89% 12.89% 12.89% 12.89% 12.89% 12.89% 12.89% 12.89% 12.89% 12.89% 12.89%
Session overruns (>30 minutes) Mar-19 11.67% 13.72% 13.95% 13.14% 16.85% 14.75% 17.82% 16.56% 16.40% 16.11% 14.60% 15.71% 13.62% 16.92% 14.83% 15.05%
Target Mar-19 00:15 00:15 00:15 00:15 00:15 00:15 00:15 00:15 00:15 00:15 00:15 00:15 00:15 00:15 00:15 00:15
A&EA&E Time to Initial Assessment -Ambulance arrivals (95th percentile) - Type 1 Mar-19 00:39 00:37 00:37 00:38 00:40 00:41 00:43 00:41 00:42 00:43 00:45 00:43 00:41 00:52 00:42 00:44
Target Mar-19 01:00 01:00 01:00 01:00 01:00 01:00 01:00 01:00 01:00 01:00 01:00 01:00 01:00 01:00 01:00 01:00
A&E Time to Initial Treatment (Median) - Type 1 Mar-19 00:51 00:59 00:53 00:54 01:01 00:55 01:07 01:01 01:06 01:08 01:06 01:07 01:20 01:17 01:03 01:13
Target Mar-19 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00%
A&E unplanned returns within 7 days - Type 1 Mar-19 1.79% 1.87% 1.55% 1.74% 2.00% 1.91% 1.83% 1.92% 1.62% 2.47% 1.80% 1.95% 1.69% 1.92% 1.70% 1.77%
Target Mar-19 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00% 5.00%
A&E left without being seen - Type 1 Mar-19 2.95% 3.10% 2.89% 2.98% 2.98% 3.17% 3.94% 3.39% 3.13% 3.43% 2.71% 3.09% 3.54% 4.74% 2.99% 3.63%
Page 27 of 39

Measure KPI Period Apr-18 May-18 Jun-18 Q1 Jul-18 Aug-18 Sep-18 Q2 Oct-18 Nov-18 Dec-18 Q3 Jan-19 Feb-19 Mar-19 Q4
Integrated Performance and Compliance Dashboard - March 2019 (2018-2019 against target)
APPENDIX 2 - EFFICIENCY AND PRODUCTIVITY
Target Mar-19 04:00 04:00 04:00 04:00 04:00 04:00 04:00 04:00 04:00 04:00 04:00 04:00 04:00 04:00 04:00 04:00
A&E Time to departure (95th percentile) - Type 1 Mar-19 05:03 05:19 05:03 05:09 05:18 05:31 05:29 05:27 05:53 05:19 05:41 05:38 06:35 06:37 05:24 06:17
Target Mar-19 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Number of ambulance handovers between ambulance and A&E waiting more than 30 minutes * Mar-19 13 21 1 35 10 13 11 34 17 15 10 42 23 11 8 42
Target Mar-19 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Number of ambulance handovers between ambulance and A&E waiting more than 60 minutes Mar-19 0 1 1 1 1 0 0 1 0 0 1 1 1 3 0 4
Target Mar-19 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
A&E 12 Hour Trolley waits - Type 1 Mar-19 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Target Mar-19 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00%
Screening Diabetic Retinopathy Screening Mar-19 98.46% 98.35% 98.35% 98.39% 98.32% 98.11% 98.25% 98.23% 98.45% 98.40% 98.47% 98.44% 98.41% 98.46% 98.56% 98.47%
Target Mar-19 17.00% 17.00% 17.00% 17.00% 17.00% 17.00% 17.00% 17.00% 17.00% 17.00% 17.00% 17.00% 17.00% 17.00% 17.00% 17.00%
TCS
TCS 19 - % of Community Patients that have had an unplanned admission LOS <=2 days (Defined set of conditions)
Mar-19 14.61% 16.67% 19.77% 15.23% 15.48% 20.62% 13.97% 19.10% 12.50% 16.67% 21.21% 16.01% 17.33% 16.44% 14.97% 15.31%
Target Mar-19 93.50% 93.50% 93.50% 93.50% 93.50% 93.50% 93.50% 93.50% 93.50% 93.50% 93.50% 93.50% 93.50% 93.50% 93.50% 93.50%
TCS 24 - % of Patients achieving improvement using a EQ5 validated assessment tool Mar-19 96.29% 98.57% 95.70% 97.70% 100.00% 100.00% 100.00% 100.00% 95.00% 100.00% 98.60% 97.87% 100.00% 100.00% 100.00% 100.00%
Target Mar-19 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00%
TCS 35 - % of standard wheelchair referrals completed within five days Mar-19 85.63% 87.38% 88.89% 87.34% 87.98% 90.36% 93.40% 90.66% 85.31% 79.84% 73.68% 80.18% 74.50% 83.33% 87.73% 81.24%
Target Mar-19 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00%
AudiologyThe % patients treated within 18 weeks of referral to audiology (Hpool site) Mar-19 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00%
Target Mar-19 18.30 18.30 18.30 18.30 18.30 18.30 18.30 18.30 18.30 18.30 18.30 18.30 18.30 18.30 18.30 18.30
Audiology non admitted wait (92nd percentile) Mar-19 4.00 5.00 5.00 5.00 5.00 5.00 5.00 5.00 5.00 4.00 5.00 5.00 4.00 5.00 4.00 4.00
Target Feb-19 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00%
Patient identifier Patient Identifier Indicator Feb-19 97.15% 98.62% 96.56% 97.46% 96.54% 96.59% 97.40% 96.83% 95.72% 96.26% 97.64% 96.49% 96.94% 96.44% 0.00%
Page 28 of 39

Measure KPI Period Apr-18 May-18 Jun-18 Q1 Jul-18 Aug-18 Sep-18 Q2 Oct-18 Nov-18 Dec-18 Q3 Jan-19 Feb-19 Mar-19 Q4
Integrated Performance and Compliance Dashboard - March 2019 (2018-2019 against target)
APPENDIX 2 - EFFICIENCY AND PRODUCTIVITY
Target Feb-19 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00% 50.00%
EOL End of Life measure Feb-19 85.34% 85.82% 86.49% 85.93% 82.00% 84.09% 89.86% 85.35% 83.80% 80.21% 84.12% 82.54% 76.97% 87.70% 0.00%
Target Mar-19 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50%
DTOC Delayed Transfers of Care Mar-19 3.94% 3.83% 4.93% 4.22% 4.85% 2.88% 2.06% 3.26% 2.21% 2.57% 2.70% 2.48% 2.28% 1.70% 2.11% 2.04%
Target Mar-19 83 81 78 76 73 71 68 65 63 60
Super Stranded Super Stranded Reduction (per day average) Mar-19 83 83 0 72 63 64 67 73 60 56 64 65 58 62 62
Readmissions * Data refresed for April-Nov to report new methodology in reporting information
Page 29 of 39

Measure KPI Period Apr-18 May-18 Jun-18 Q1 Jul-18 Aug-18 Sep-18 Q2 Oct-18 Nov-18 Dec-18 Q3 Jan-19 Feb-19 Mar-19 Q4
Unplanned Target Feb-19 152.3 158.4 176.7 181.1 147.7 143.0 139.5 157.8 181.9 172.9 149.3 0.0
UnplannedEmergency admissions for acute conditions that should not usually require hospital admission Feb-19 175.9 136.4 177.0 184.9 198.9 143.3 146.8 0.0 152.1 169.3 173.2 0.0 226.8 199.2 0.0
Target Feb-19 22.25 25.58 18.91 18.91 13.35 32.26 26.70 28.92 13.35 28.92 11.12 0.00
Unplanned hospitalisation for asthma, diabetes and epilepsy in under 19s Feb-19 16.69 27.81 26.70 32.26 24.47 16.69 28.92 0.00 36.71 17.80 26.70 0.00 25.58 15.57 0.00
Target Feb-19 63.3 69.3 60.8 61.6 52.3 64.9 66.8 62.5 86.8 79.7 58.1 0.0
Unplanned hospitalisation for chronic ambulatory care sensitive conditions (adults) Feb-19 71.8 66.3 55.3 79.5 81.1 75.6 75.1 0.0 83.0 79.7 81.1 0.0 104.9 86.0 0.0
Target Feb-19 13.35 20.02 6.67 5.56 1.11 12.24 14.46 62.29 83.43 51.17 26.70 0.00
Unplanned hospitalisation for respiratory tract infections in under 19s Feb-19 22.25 26.70 15.57 20.02 11.12 11.12 21.13 0.00 97.89 127.92 90.10 0.00 46.72 45.61 0.00
Target Feb-19 80.00% 80.00% 80.00% 80.00% 80.00% 80.00% 80.00% 80.00% 80.00% 80.00% 80.00% 80.00% 80.00% 80.00% 80.00%
StrokeStroke admissions 90% of time spent on dedicated Stroke unit Feb-19 85.71% 90.48% 94.23% 89.81% 89.47% 95.56% 90.32% 91.72% 94.59% 92.86% 93.02% 93.44% 89.80% 100.00% 0.00%
Target Feb-19 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00%
High risk TIAs assessed and treated within 24 hours Feb-19 90.00% 86.67% 100.00% 91.43% 100.00% 80.00% 100.00% 95.24% 100.00% 100.00% 80.00% 92.31% 80.00% 100.00% 0.00%
Integrated Performance and Compliance Dashboard - March 2019 (2018-2019 against target)
APPENDIX 2 - EFFICIENCY AND PRODUCTIVITY
Page 30 of 39

Measure KPI Period Apr-18 May-18 Jun-18 Q1 Jul-18 Aug-18 Sep-18 Q2 Oct-18 Nov-18 Dec-18 Q3 Jan-19 Feb-19 Mar-19 Q4
HMSR Target Jan-19 110.00 110.00 110.00 110.00 110.00 110.00 110.00 110.00 110.00 110.00 110.00 110.00 109.00 109.00 109.00
HMSRHSMR Mortality Rates(Rolling 12 month value) Jan-19 104.41 104.02 104.33 104.33 102.58 102.20 102.29 102.29 101.49 100.37 97.79 97.79 96.17 96.17
Target Jan-19 #DIV/0! #DIV/0! #DIV/0!
HMSRHSMR Crude mortality Rate (Rolling 12 month value) Jan-19 3.72% 3.66% 3.68% 3.68% 3.63% 3.60% 3.59% 3.59% 3.59% 3.63% 3.54% 3.54% 3.45% 3.45%
Target Sep-18 111.43 111.43 111.43 111.43 111.43 111.43 111.43 111.43 111.43 111.43 111.43 110.00 110.00 110.00
SHMISHMI Mortality rate(Rolling 12 month value) Sep-18 104.22 103.00 103.02 105.91 103.02 101.64 100.72 100.72 - -
Target Sep-18 #DIV/0! #DIV/0!
SHMISHMI Crude mortality Rate (Rolling 12 month value) Sep-18 3.67% 3.59% 3.58% 3.50% 3.60% 3.54% 3.49% 3.49% - -
Target Feb-19 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00%
Dementia
Dementia - % of patients aged 75 and over, admitted as emergencies, stayed more than 72 hours and were asked the dementia case finding question
Feb-19 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00%
Target Feb-19 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00%
DementiaDementia - % of patients undergone a diagnostic assessment Feb-19 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00%
Target Feb-19 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00%
Dementia
Dementia - % of those that received a diagnostic assessment that were referred onto another service or back to GP
Feb-19 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00%
Target Mar-19 #DIV/0! #DIV/0! #DIV/0! #DIV/0!
Complaints Complaint Stage 1 - Informal Mar-19 57 42 55 154 63 78 70 211 64 49 50 163 73 64 60 197
Target Mar-19 #DIV/0! #DIV/0! #DIV/0! #DIV/0!
Complaints Complaint Stage 2 - Formal Meeting Mar-19 7 9 6 22 14 8 8 30 7 9 6 22 5 13 8 26
Target Mar-19 #DIV/0! #DIV/0! #DIV/0! #DIV/0!
Complaints Complaint Stage 3 - Formal Chief Executive Letter Mar-19 18 6 10 34 16 16 12 44 28 20 12 60 14 30 10 54
Target Feb-19 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00%
Complaints Complaint response times % (25 days) Feb-19 93.00% 93.00% 85.00% 90.00% 80.00% 83.00% 100.00% 88.00% 84.00% 100.00% 91.00% 92.00% 82.00% 93.00% 82.00%
APPENDIX 3 - QUALITY AND SAFETY
Integrated Performance and Compliance Dashboard - March 2019 (2018-2019 against target)
Page 31 of 39

Measure KPI Period Apr-18 May-18 Jun-18 Q1 Jul-18 Aug-18 Sep-18 Q2 Oct-18 Nov-18 Dec-18 Q3 Jan-19 Feb-19 Mar-19 Q4
APPENDIX 3 - QUALITY AND SAFETY
Integrated Performance and Compliance Dashboard - March 2019 (2018-2019 against target)
Target Mar-19 #DIV/0! #DIV/0! #DIV/0! #DIV/0!
Risks Corporate & Departmental Risks (Red) Mar-19 3 3 3 9 6 9 8 23 8 10 8 26 9 7 7 23
Target Mar-19 #DIV/0! #DIV/0! #DIV/0! #DIV/0!
Never Events Never Events Mar-19 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Target Feb-19 5 6 7 6 6 2 4 4 2 1 0 1 0 3 3
Pressure Ulcers Grade 1 Pressure Ulcers (In-Hospital) Feb-19 0 2 2 4 3 4 3 10 4 6 8 18 8 6 14
Target Feb-19 10 11 10 10 13 10 7 10 6 6 7 6 13 19 16
Pressure Ulcers Grade 2 Pressure Ulcers (In-Hospital) Feb-19 13 26 13 52 14 17 14 45 9 19 15 43 15 28 43
Target Feb-190 2 0 1 2 0 0 1 1 0 1 1 1 2 0
Pressure Ulcers Grade 3 Pressure Ulcers (In-Hospital) Feb-19 5 5 1 11 0 2 4 6 3 2 1 6 3 4 7
Target Feb-19 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0
Pressure Ulcers Grade 4 Pressure Ulcers (In-Hospital) Feb-19 0 1 0 1 0 0 0 0 0 0 0 0 0 1 1
Target Mar-19 #DIV/0! #DIV/0! #DIV/0! #DIV/0!
Falls Fall - No Injury (In-Hospital) Mar-19 119 98 79 296 82 82 87 251 81 79 79 239 84 72 80 236
Target Mar-19 #DIV/0! #DIV/0! #DIV/0! #DIV/0!
Falls Fall - Injury, No Fracture (In-Hospital) Mar-19 13 11 8 32 15 10 9 34 18 21 23 62 28 20 16 64
Target Mar-19 #DIV/0! #DIV/0! #DIV/0! #DIV/0!
Falls Fall - With Fracture (In-Hospital) Mar-19 1 1 1 3 1 1 1 3 1 3 4 8 2 3 4 9
Target Mar-19 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00%
VTE VTE Risk Assessment Mar-19 97.51% 98.17% 98.12% 97.93% 97.99% 97.66% 97.23% 97.63% 97.99% 97.88% 97.37% 97.75% 97.83% 96.90% 97.86% 97.53%
Page 32 of 39

Measure KPI Period Apr-18 May-18 Jun-18 Q1 Jul-18 Aug-18 Sep-18 Q2 Oct-18 Nov-18 Dec-18 Q3 Jan-19 Feb-19 Mar-19 Q4
APPENDIX 3 - QUALITY AND SAFETY
Integrated Performance and Compliance Dashboard - March 2019 (2018-2019 against target)
Target Mar-19 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00%
Hand Hygiene
ComplianceHand Hygiene Compliance Mar-19 98.00% 95.00% 96.00% 96.00% 94.00% 97.00% 95.00% 95.00% 97.00% 97.00% 99.00% 97.00% 96.00% 96.00% 97.00% 96.00%
Target Mar-19 1 1 1 3 1 1 1 1 1 1 1 1 1 1 1 1
Infections Clostridium difficile (C.diff) Mar-19 4 2 1 7 1 4 2 7 2 2 1 5 5 5 2 12
Target Mar-19 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
InfectionsMethicillin-Resistant Staphylococcus Aureus (MRSA) bacteraemia Mar-19 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Target Mar-19 #DIV/0! #DIV/0! #DIV/0! #DIV/0!
InfectionsMethicillin-Sensitive Staphylococcus Aureus (MSSA) bacteraemia Mar-19 1 2 1 4 0 2 2 4 3 1 4 8 1 3 1 5
Target Mar-19 #DIV/0! #DIV/0! #DIV/0! #DIV/0!
Infections Escherichia coli (E.coli) Mar-19 4 3 3 10 8 2 3 13 5 3 2 10 2 1 3 6
Target Mar-19 #DIV/0! #DIV/0! #DIV/0! #DIV/0!
Infections Klebsiella species bacteraemia (Kleb sp) Mar-19 1 2 3 5 2 2 2 4 0 3 1 4 1 2 1 4
Target Mar-19 #DIV/0! #DIV/0! #DIV/0! #DIV/0!
Infections Pseudomonas aeruginosa bacteraemia (Ps a) Mar-19 0 1 2 2 0 0 1 1 1 1 2 4 1 0 0 1
Target Mar-19 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00%
FFTFriends & Family - (Ward) [National Score based on % ‘extremely likely’ & 'Likely' to recommend to F&F] Mar-19 97.00% 97.00% 97.00% 97.00% 98.00% 97.00% 97.00% 97.00% 96.00% 98.00% 96.00% 96.00% 97.00% 97.00% 98.00% 97.00%
Target Mar-19 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00%
FFT
Friends & Family - (A&E)[National Score based on % ‘extremely likely’ & 'Likely' to recommend to F&F]
Mar-19 93.00% 95.00% 95.00% 94.00% 94.00% 96.00% 96.00% 95.00% 96.00% 92.00% 94.00% 94.00% 91.00% 89.00% 88.00% 89.00%
Target Mar-19 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00% 70.00%
FFT
Friends & Family - (Birth)[National Score based on % ‘extremely likely’ & 'Likely' to recommend to F&F]
Mar-19 100.00% 98.00% 100.00% 99.00% 100.00% 99.00% 96.00% 98.00% 90.00% 95.00% 100.00% 95.00% 100.00% 100.00% 98.00% 99.00%
Page 33 of 39

Measure KPI Period Apr-18 May-18 Jun-18 Q1 Jul-18 Aug-18 Sep-18 Q2 Oct-18 Nov-18 Dec-18 Q3 Jan-19 Feb-19 Mar-19 Q4
APPENDIX 3 - QUALITY AND SAFETY
Integrated Performance and Compliance Dashboard - March 2019 (2018-2019 against target)
Target Mar-19 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00%
Experience
SurveyPatient Experience Survey Score (100% max) Mar-19 95.98% 96.62% 95.88% 96.16% 93.10% 96.02% 97.61% 95.58% 94.57% 97.29% 95.66% 95.84% 94.09% 93.39% 98.15% 95.21%
Target Mar-19 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00%
Experience
SurveyStaff Experience Survey (100% max) Mar-19 84.64% 89.95% 94.74% 89.78% 92.40% 88.49% 92.89% 91.26% 88.98% 94.44% 86.71% 90.04% 88.36% 96.13% 93.63% 92.71%
Target Mar-19 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00%
Experience
SurveyPatient and Staff Experience Score (100% max) Mar-19 91.50% 94.02% 95.51% 93.68% 92.87% 93.12% 95.85% 93.95% 92.58% 96.40% 92.32% 93.77% 91.95% 94.33% 96.41% 94.23%
Target Mar-19 20 20 20 60 20 20 20 60 20 20 20 60 20 20 20 20
Experience
Survey
Patient and Staff Experience Survey Number of surveys undertaken Mar-19 27 20 17 64 16 24 21 61 22 25 21 68 22 15 19 56
Target Mar-19>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
Workforce Registered Nurse/Midwife day shift fill rates Mar-19 83.13% 82.99% 81.42% 82.51% 82.16% 81.36% 83.64% 82.39% 83.92% 87.88% 84.46% 85.42% 90.33% 85.38% 84.82% 86.84%
Target Mar-19>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
Workforce Registered Nurse/Midwife Night shift fill rates Mar-19 93.39% 92.08% 90.49% 91.99% 89.50% 89.47% 91.10% 90.02% 90.52% 93.56% 92.38% 92.15% 96.42% 93.56% 91.32% 93.77%
Target Mar-19>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
Workforce Care Staff day shift fill rates Mar-19 91.61% 70.45% 86.61% 82.89% 89.08% 88.76% 86.90% 88.25% 81.30% 76.55% 87.90% 81.92% 88.71% 89.11% 92.55% 90.12%
Target Mar-19>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
>=80% and <=109.99%
Workforce Care Staff Night shift fill rates Mar-19 108.36% 89.04% 108.13% 101.84% 103.01% 103.82% 105.54% 104.12% 103.53% 90.51% 117.91% 103.98% 129.77% 117.87% 119.03% 122.22%
Target Mar-19 97.79% 97.84% 97.84% 97.82% 97.84% 97.84% 97.84% 97.84% 97.84% 97.84% 97.84% 97.84% 97.84% 97.84% 97.84% 97.84%
Safety
ThermometerTrust - Harm Free Care % Mar-19 98.66% 98.12% 97.37% 98.05% 98.55% 98.42% 98.57% 98.51% 98.13% 98.47% 98.14% 98.25% 97.86% 98.75% 98.49% 98.37%
Target Mar-19 2.21% 2.16% 2.16% 2.18% 2.16% 2.16% 2.16% 2.16% 2.16% 2.16% 2.16% 2.16% 2.16% 2.16% 2.16% 2.16%
Safety
ThermometerTrust - New Harm % Mar-19 1.34% 1.88% 2.63% 1.95% 1.45% 1.58% 1.43% 1.49% 1.87% 1.53% 1.86% 1.75% 2.14% 1.25% 1.51% 1.63%
Target Mar-19 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00%
Experience
SurveyDeep Dive Visits Mar-19 86.10% 86.10% 88.46% 88.53% 88.49% 88.48% 84.27% 88.54% 87.10% 96.76% 94.81% 90.28% 93.95%
Page 34 of 39

Measure KPI Period Apr-18 May-18 Jun-18 Q1 Jul-18 Aug-18 Sep-18 Q2 Oct-18 Nov-18 Dec-18 Q3 Jan-19 Feb-19 Mar-19 Q4
Staff Target Feb-19 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50%
Staff Sickness Feb-19 4.17% 4.49% 4.05% 4.12% 4.10% 4.23% 4.20% 4.09% 4.48% 4.58% 4.96% 4.57% 5.43% 5.01% 0.00%
Target Mar-19 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00%
StaffTurnover (12 months rolling data) - revised methodology from Nov-18 * Mar-19 12.49% 12.36% 12.27% 12.41% 11.57% 11.79% 13.22% 13.22% 12.51% 7.76% 7.83% 7.83% 8.08% 8.33% 8.70% 8.70%
Target Mar-19 80% 80% 80% 80% 80% 80% 80% 80% 80% 80% 80% 80% 80% 80% 80.00% 80.00%
Staff Mandatory Training Mar-19 77% 80% 81% 81% 83% 84% 84% 84% 85% 86% 87% 87% 88% 88% 88.61% 88.61%
Target Mar-19 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95.00% 95.00%
Staff Appraisals Mar-19 77% 79% 81% 81% 81% 80% 81% 81% 81% 82% 82% 82% 83% 84% 84% 84%
Target Feb-19 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50% 3.50%
Staff NTH Solutions Sickness Feb-19 4.25% 3.83% 4.41% 4.09% 5.83% 4.89% 4.77% 4.77% 5.16% 4.65% 5.73% 5.19% 5.56% 5.43% 0.00%
Target Mar-19 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00% 10.00%
Staff NTH Solutions Turnover Mar-19 1.21% 1.36% 1.51% 1.51% 2.56% 3.32% 4.22% 4.22% 4.63% 5.85% 6.32% 6.32% 7.09% 7.21% 7.22% 7.22%
Target Mar-19 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95.00% 95.00%
Staff NTH Solutions Mandatory Training Mar-19 84% 84% 84% 84% 85% 84% 84% 84% 87% 89% 88% 88% 88% 88% 89% 89%
Target Mar-19 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95.00% 95.00%
Staff NTH Solutions Appraisals Mar-19 93% 90% 88% 88% 87% 86% 87% 87% 88% 86% 86% 86% 89% 88% 85% 85%
Integrated Performance and Compliance Dashboard - March 2019 (2018-2019 against target)
APPENDIX 4 - WORKFORCE
* This figure has been calculated using a revised methodology (from November) to include those employees who have left the organisation on a voluntary basis, for example Resignation (due to Relocation, Health reasons, Promotion etc.)
and Retirement.
Page 35 of 39

Measure National North EastNorth Tees &
HartlepoolS Tyneside Sunderland N Cumbria Gateshead Newcastle Northumbria S Tees
Durham &
Darlington
RTT - February 19
Incomplete Pathways waiting <18 weeks 87.0% 94.5% 95.4% 92.6% 78.0% 92.2% 93.0% 92.3% 88.8% 90.4%
Half of patients wait less than 7 5 5 5 10 6 6 6 7 5
Half of admitted patients wait less than 11 5 5 12 16 13 9 9 7 10
19 out of 20 patients wait less than 37 25 19 30 48 31 30 26 34 34
Half of Non admitted Pathways waited less than 6 2 5 5 8 4 7 5 4 4
19 out of 20 patients wait less than 26 16 16 20 33 21 20 22 20 18
A&E - March 19 National North EastNorth Tees &
HartlepoolS Tyneside Sunderland N Cumbria Gateshead Newcastle Northumbria S Tees
Durham &
Darlington
A&E 4 hour target 86.6% 93.1% 97.8% 92.9% 85.3% 86.8% 93.5% 96.2% 95.2% 96.0% 90.6%
Cancer 62 Day Standard - February 19 National North EastNorth Tees &
HartlepoolS Tyneside Sunderland N Cumbria Gateshead Newcastle Northumbria S Tees
Durham &
Darlington
Breast 92.11 (70/76) 100 (8/8) 0 (0/0) 100 (0.5/0.5) 87.5 (7/8) 89.19 (16.5/18.5) 66.67 (4/6) 100 (13/13) 100 (9/9) 92.31 (12/13)
Lung 67.29 (72/107) 81.82 (9/11) 85.71 (3/3.5) 100 (9.5/9.5) 47.62 (5/10.5) 62.5 (2.5/4) 65.71 (11.5/17.5) 70.27 (13/18.5) 70 (10.5/15) 45.71 (8/17.5)
Gynae 82.5 (33/40) 33.33 (0.5/1.5) 0 (0/0) 77.78 (3.5/4.5) 100 (5.5/5.5) 100 (5.5/5.5) 66.67 (2/3) 88.89 (4/4.5) 73.91 (8.5/11.5) 87.5 (3.5/4)
Upper GI 58.82 (35/59.5) 100 (1/1) 100 (1/1) 76.92 (5/6.5) 50 (2/4) 87.5 (3.5/4) 51.52 (8.5/16.5) 63.16 (6/9.5) 57.69 (7.5/13) 12.5 (0.5/4)
Lower GI 73.61 (53/72) 40 (2/5) 100 (4/4) 71.43 (5/7) 41.67 (5/12) 85.71 (3/3.5) 70 (7/10) 94.74 (9/9.5) 82.61 (9.5/11.5) 89.47 (8.5/9.5)
Uro (incl testes) 65.14 (128/196.5) 78.95 (15/19) 0 (0/0) 68.63 (35/51) 66.67 (9/13.5) 41.67 (2.5/6) 42.65 (14.5/34) 61.54 (20/32.5) 80 (32/40) 0 (0/0.5)
Haem (incl AL) 81.63 (40/49) 100 (2/2) 100 (0.5/0.5) 93.75 (7.5/8) 83.33 (5/6) 80 (4/5) 55.56 (2.5/4.5) 100 (4.5/4.5) 77.78 (7/9) 73.68 (7/9.5)
Head & Neck 62.16 (23/37) 0 (0/0) 0 (0/0) 69.23 (4.5/6.5) 83.33 (5/6) 0 (0/0) 76.47 (6.5/8.5) 0 (0/0) 44 (5.5/12.5) 42.86 (1.5/3.5)
Skin 93.33 (126/135) 0 (0/0) 0 (0/0) 75 (3/4) 92.86 (13/14) 0 (0/0) 95.65 (44/46) 100 (6/6) 91.23 (26/28.5) 93.15 (34/36.5)
Sarcoma 66.67 (2/3) 0 (0/0) 0 (0/0) 0 (0/0) 0 (0/0) 100 (0.5/0.5) 75 (1.5/2) 0 (0/0) 0 (0/0.5) 0 (0/0)
Brain/CNS 0 (0/0) 0 (0/0) 0 (0/0) 0 (0/0) 0 (0/0) 0 (0/0) 0 (0/0) 0 (0/0) 0 (0/0) 0 (0/0)
Children's 0 (0/0) 0 (0/0) 0 (0/0) 0 (0/0) 0 (0/0) 0 (0/0) 0 (0/0) 0 (0/0) 0 (0/0) 0 (0/0)
Other 90 (9/10) 0 (0/0) 100 (1/1) 100 (4/4) 0 (0/0) 100 (1/1) 50 (1/2) 100 (1/1) 100 (1/1) 0 (0/0)
All 75.29 (591/785) 78.95 (37.5/47.5) 95 (9.5/10) 76.35 (77.5/101.5) 71.07 (56.5/79.5) 81.25 (39/48) 68.67 (103/150) 77.27 (76.5/99) 76.9 (116.5/151.5) 76.53 (75/98)
Integrated Performance and Compliance Dashboard - March 2019 Benchmark Regional
Data not
available
Page 36 of 39

Integrated Performance and Compliance Dashboard - March 2019 Benchmark HED
Page 37 of 39

Integrated Performance and Compliance Dashboard - March 2019 Benchmark HED
Page 38 of 39

Integrated Performance and Compliance Dashboard - March 2019 Finance
APPENDIX 5 - FINANCE
Page 39 of 39

1
Board of Directors
Title: Integrated Compliance and Performance Year End Report 2018/19
Date: 25 April 2019
Prepared by: Lindsey Wallace, Head of Planning, Performance and Development
Executive Sponsor: Lynne Taylor, Director of Planning and Performance
Purpose of the report To provide an overview of the integrated performance for compliance, quality and workforce during 2018/19
Action required: Approve Assurance x Discuss x Information x
Strategic Objectives supported by this paper:
Putting Patients First
x Valuing our People
x Transforming our Services
x Health and Wellbeing
x
Which CQC Standards apply to this report
Safe x Caring x Effective x Responsive x Well Led x
Executive Summary and the key issues for consideration/ decision:
Compliance against key access standards including quality and workforce in accordance with the Single Oversight Framework for 2018/19 period.
Activity indicates an increase across both emergency and elective pathways.
Despite these pressures, overall the Trust has performed well against national and local indicators, achieving compliance against the majority of the key standards during 2018/19, reporting within the top percentile on a regular basis, however recognising pressures remain around the cancer 62 day standards.
Seasonal pressures were managed well, supported by robust planning in-year, with reductions in bed occupancy, super stranded and DToCs evident throughout the year.
Operational efficiency standards indicate improvement, however with further work required across readmission rates, DNA rates and theatre utilisation.
Quality standards indicate positive performance against a number of key indicators, including HSMR/SHMI, C-difficile and Dementia standards.
Sickness absence remained the key pressure within Workforce.
How this report impacts on current risks or highlights new risks:
Robust emergency and elective care management has reduced the inherent risk of non -compliance against the key standards during 2018/19, however with key risks remaining across a number of standards going into 2019/20. Mitigation and recovery plans will be developed to reduce these risks,
Committees/groups where this item has been discussed
Performance, Planning and Compliance Committee.
Recommendation
The Board of Directors are asked to note:
The performance against the key operational, quality and workforce standards during 2018/19.
The continuous in-year planning and pathway reviews which have contributed to the successful delivery of the quality and operational standards
The on-going collaborative operational management across the system to support improved pathway development going into 2019/20.

1
North Tees and Hartlepool NHS Foundation Trust
Meeting of the Board of Directors
25 April 2019
Integrated Compliance and Performance - Year End Report 2018/19
1. Introduction/ Purpose
1.1 This Integrated Compliance and Performance Report highlights performance against a range of indicators against the Single Oversight Framework (SOF) and the Foundation Trust terms of licence for the year end period, 2018/19.
1.2 It comprises a year-end summary report including Compliance and Performance,
Quality and Workforce, as received in-year by the Board, with a summary of key areas of action during 2018/19.
1.3 Appendix 1 details compliance and performance against the SOF standards. 2. Summary 2.1 The Trust has performed well against national and local key indicators throughout
2018/19 despite considerable challenges associated with on-going operational, clinical, financial and system wide pressures. This report indicates the Trust has performed above or within expected for the majority of indicators, as outlined in Appendix 1.
2.2 The table below provides a summary of activity, by point of delivery, in comparison to the same period 2017/18. Overall emergency activity indicates an increase across both inpatient and ambulatory care activity, evidence of the on-going pressures across the Trust. Elective activity has seen a further shift to daycase delivery, with a decrease in inpatient activity, however an overall increase across elective care. This has supported the reduction of the overall RTT waiting list, a key NHSI requirement for 2018/19. Increased daycase procedures and ambulatory care delivery has supported improved pathway management, releasing base ward beds to absorb the increasing pressures.
2.3 Despite increased emergency demand this year with surges in activity, high bed
occupancy rates on both base wards and critical care, the Trust managed the seasonal pressures well. Robust and effective winter planning supported delivery, demonstrated by the decrease in the number of cancelled elective procedures over the winter period with only 6 elective operations cancelled due to bed pressures, a significant reduction on the previous year.
2.4 The NHSI Model Hospital dashboard has made a number of updates in year to include additional reports across specialties and directorates, which have been utilised to identify efficiency and productivity opportunities. The Trust has embraced
2018-19
Point of Delivery 2017-18 Actual 2018-19 Actual
Variance 2018-19
against 2017-18
% Variance 2018-19
against 2017-18
A&E Attendances 161,123 175,584 14,461 8.98%
Day Case Admissions 35,340 36,530 1,190 3.37%
Inpatient Planned Admissions 4,951 4,711 -240 -4.85%
Inpatient Emergency Admissions 41,689 43,383 1,694 4.06%
Ambulatory Care Attendances 9,973 10,824 851 8.53%
Outpatient Attendances (New and Review)
Provisional 180,362 180,631 269 0.15%
Ward Attenders 34,808 37,065 2,257 6.48%

2
Lord Carter’s recommendations and continues to explore productivity, quality, efficiency and responsiveness, to provide a clearer view of improvement opportunities through the ‘Delivering Productivity Programme’.
2.5 NHS Improvement has recognised, on the whole, the excellent performance of the
Trust with regard to quality of care, operational and financial delivery and strengthens the Trust’s credibility in meeting the challenges moving forward.
2.6 The success of the Integrated Urgent Care Centre has seen sustained achievement
of the Emergency 4-hour standard throughout the year, regularly reporting in the top 10 nationally and at times best in class. Year-end position reported at 97.18% in comparison to 97.24% last year.
2.7 Delivery against the 62-day referral to treatment cancer standard has continued to be
a challenge both nationally and locally, with varied performance throughout the year, impacted on by a number of variables including patient choice, complex pathways, capacity and system wide issues. Despite these challenges, the aggregate provisional year end position indicates the Trust has just missed achievement of the 62-day standard, reporting a year end position of 84.53% however has remained above the national and regional position. In context, this stand was last achieved nationally in December 2015, demonstrating the difficulty in managing the variables associated with cancer pathway delivery.
2.8 Seasonal challenges inevitably impact on the management of the Referral to
Treatment standard; however, with improved management the Trust consistently performed above the 92% standard, achieving 94.21% for the year end position, an improvement on last year when the Trust reported 93.63%. No patients waited more than 52 weeks in comparison to the national position which reported 1936 patients waiting greater than 52 weeks (validated data February 2019).
2.9 During 2018-19, the Trust has continued to review and re-model its services to
meet the needs of the population. The Trust’s bed base has been re-aligned to meet the increasing emergency activity coming into the organisation, providing resilience for the periods of seasonal demand and flexibility within service delivery. The elective bed base has been re-configured, providing a flexible week day and weekend resource to achieve maximum operational efficiency, including improved use of the Hartlepool site, supported by the NHSI 100-day challenge. There is a commitment to the continued review and improvement of patient pathways, through integrated acute and community care and collaborative working with social care and Tertiary centres where appropriate.
2.10 The Trust under-achieved against the 99% Diagnostic national standard reporting a
year end position of 98.69%, due it in year capacity issues, however recovered the position in Q4. Diagnostic pathways continue to be monitored closely to ensure maximum contribution to RTT pathway management and to reduce waiting times.
2.11 Delayed Transfers of Care (DTOC) have reported a significant reduction in 2018/19
reporting at 2.99% with a gradual reduction noted throughout the year. A similar picture has been seen with the reduction of super stranded patients with the Trust achieving NHSI’s directive of less than 68 average per day by December 2018. The Trust recognises readmissions as an area requiring further work, in line with national drivers to reduce avoidable admissions and reviews where clinically appropriate with focused project work planned for 2019/20.
2.12 Whilst DNA rates report above the Trust’s internal target considerable improvements
have been noted throughout the year with achievement against the 10% reduction planned at the beginning of the year.
2.13 Performance against indicators for Community Information Dataset indicators has
remained complaint throughout 2018/19 with a positive year end position against all indicators.

3
2.14 The Trust continues to remain within the expected range for both HSMR and SHMI values. The latest data for HSMR is 96.17 reducing from 97.79, with SHMI quarterly end position seeing a reduction to 100.72 from the previously reported 103.02.
2.15 The Trust has seen a financial year improvement of 11.43% in C difficile rates
compared to 2017/18, which reported 35 cases, against the 31 for 2018/19.
2.16 Whilst the pseudomonas target has not been achieved this year, the target for E coli and Klebsiella has been exceeded.
2.17 Route Cause Analysis of the Pseudomonas cases has not identified any themes or
trends. The Trust continues to closely monitor all incidences of Health Care Associated infection.
2.18 The increase in pressure ulcers over the reporting period is currently being investigated with validation being undertaken by the Tissue Viability Team.
2.19 There have been 212 less falls over the last financial year compared to the previous year. The Trust has developed a falls strategy outlining key priorities for the next 3 years.
2.20 The Trust continues with its excellent performance in relation to dementia standards maintaining 100% compliance.
2.21 The sickness absence data is the year to date figure (up to 28 February 2019) and is reporting as 4.39%, a decrease of 0.14% when compared to the previous year (4.53%).
2.22 The Trust’s Turnover rate at the end of 2018/19 was 8.70% against a target of 10%.
Turnover has been calculated using a revised methodology to include those employees who have left the organisation on a voluntary basis, for example Resignation (due to relocation, health reasons, promotion etc.) and retirement.
2.23 Staff Engagement Score, as reported by the annual NHS Staff Survey (2018), is 3.87
out of a total score of 5. There has been a steady increase in the engagement score over the previous years, which is in recognition of the impact of the enhanced engagement activities which have taken place.
3. Conclusion/Summary
3.1 The Trust has performed well against the majority of key operational national and local standards throughout 2018/19, despite the considerable challenges associated with on-going operational, clinical, financial and system wide pressures. The Trust continues to develop the performance reporting framework to ensure it meets the needs of both corporate and directorate level delivery, reflecting the multiple internal and external performance requirements.
4. Recommendations
The Board of Directors are asked to note:
The performance against the key operational, quality and workforce standards during 2018/19.
The continuous in-year planning and pathway reviews which have contributed to the successful delivery of the quality and operational standards
The on-going collaborative operational management across the system to support improved pathway development going into 2019/20.
Lynne Taylor, Director of Planning and Performance Julie Lane, Director of Nursing and Infection Prevention and Control Alan Sheppard, Director of Human Resources and Organisational Development

4
Appendix 1 – Year end position 2018-19
Single Oversight Framework Indicators Standard/Trajectory 2018-19 Performance
2017-18 Performance
Achieved (cumulative)
A&E: maximum waiting time of 4 hours from arrival to admission/transfer/discharge (Apr 18 – Mar 19) 95% 97.18% 97.24% ✔
Cancer 31 day wait for second or subsequent treatment – surgery (Apr 18 – Mar 19 Provisional) 94% 98.84% 98.29% ✔
Cancer 31 day wait for second or subsequent treatment – anti cancer drug treatments (Apr 18 – Mar 19 Provisional) 98% 100.00% 99.87% ✔
Cancer 31 day wait for second or subsequent treatment – radiotherapy
94% N/A N/A N/A
Cancer 62 Day Waits for first treatment (urgent GP referral for suspected cancer) (Apr 18 – Mar 19 Provisional)
85% 84.53% 85.83% ᵡ
Cancer 62 Day Waits for first treatment (from NHS cancer screening service referral) (Apr 18 – Mar 19 Provisional) 90% 96.25% 97.02% ✔
Cancer 31 day wait from diagnosis to first treatment (Apr 18 – Mar 19 Provisional) 96% 99.38% 98.55% ✔
Cancer 2 week wait from referral to date first seen, all urgent referrals (cancer suspected) (Apr 18 – Mar 19 Provisional)
93% 94.11% 93.82% ✔
Cancer 2 week wait from referral to date first seen, symptomatic breast patients (cancer not initially suspected) (Apr 18 – Mar 19 Provisional)
93% 96.16% 96.64% ✔
Maximum time of 18 weeks from point of referral to treatment in aggregate, patients on incomplete pathways (Apr 18 – Mar 19)
92% 94.21% 93.63% ✔
Referral to Treatment 52 Week Waits (Apr 18 – Mar 19) 0 0 0 ✔
Number of Diagnostic waiters over 6 weeks (Apr 18 – Feb 19) 99% 98.69% 99.56% ᵡCommunity care data completeness – referral to treatment information completeness (Apr 18 – Feb 19) 50% 96.14% 96.81% ✔
Community care data completeness – referral information completeness (Apr 18 – Feb 19) 50% 96.67% 96.47% ✔
Community care data completeness – activity information completeness (Apr 18 – Feb 19) 50% 96.90% 95.70% ✔
Community care data completeness – patient identifier information completeness (Shadow Monitoring) (Apr 18 – Feb 19)
50% 96.90% 95.70% ✔
Community care data completeness – End of life patients deaths at home information completeness (Shadow Monitoring) (Apr 18 – Feb 19)
50% 83.88% 85.70% ✔
Compliance with access to healthcare for patients with learning disabilities
100% Full compliance Full compliance ✔
Other National and Contract Indicators 2018-19 Target 2018-19 Performance
2017-18 Performance Achieved
Cancelled Procedures for non-medical reasons on the day of op (Apr 18 – Mar 19) 0.80% 0.41% 0.72% ✔
Cancelled Procedures reappointed within 28 days (Apr 18 – Feb 19) 100% 99.41% 94.84% ᵡ
Eliminating Mixed Sex Accommodation (Apr 18 – Mar 19) Zero cases 0 0 ✔
A&E Trolley waits > 12 hours (Apr 18 – Mar 19) Zero cases 0 1 ✔
Stroke – 90% of time on dedicated Stroke unit (Apr 18 – Feb 19) 80% 92.12% 93.49% ✔
Stroke – TIA assessment within 24 hours (Apr 18 – Feb 19) 75% 91.92% 96.59% ✔
Delayed transfers of care (Apr 18 – Mar 19) <3.5% 2.99% 3.42% ✔
VTE Risk Assessment (Apr 18 – Mar 19) 95% 97.72% 97.89% ✔
Sickness Absence Rate (2018/19)Year to Date Figure (28 Feb 2019) 3.5% 4.39% 4.53% ᵡ
Mandatory Training Compliance (2018/19) 80% 89.00% 84.00% ✔
Turnover Rate (2018/19) 10.0% 8.70% 14.80% ✔
Operational Efficiency Indicators 2018-19 Target 2018-19 Performance
2017-18 Performance Achieved
New to Review Ratio (Apr 18 – Feb 19) 1.45 1.26 1.18 ✔
Outpatient DNA (new) (Apr 18 – Mar 19) 5.40% 7.97% 8.67% ᵡOutpatient DNA (review) (Apr 18 – Mar 19) 9.00% 9.76% 10.61% ᵡLength of Stay Elective (Jan 18 – Dec 18) 3.26 1.68 1.86 ✔
Length of Stay Emergency (Jan 18 – Dec 18) 4.17 3.57 3.76 ✔
Readmission Elective (Apr 18 to Jan 19) 0.00% 4.61% 4.17% ᵡReadmission Emergency (Apr 18 to Jan 19) 9.37% 14.53% 14.60% ᵡOccupancy (Trust) (2018-19) 85% 90.06% 90.97% ᵡ
Quality Indicators Standard/Trajectory 2018-19 Performance
2017-18 Performance Achieved
Clostridium Difficile – meeting the C.Diff objective (Apr 18 – Mar 19) 12 31 35 ᵡMethicillin-Resistant Staphylococcus Aureus (MRSA) bacteraemia (Apr 18 – Mar 19) 0 0 4 ✔
Methicillin-Sensitive Staphylococcus Aureus (MSSA) bacteraemia (Apr 18 – Mar 19) 21 21 25 ✔
Escherichia coli (E.coli) (Apr 18 – Mar 19) 50 39 43 ✔
Klebsiella species (Kleb sp) bacteraemia (Apr 18 – Mar 19) N/A 20 29 N/A
Pseudomonas aeruginosa (Ps a) bacteraemia (Apr 18 – Mar 19)
N/A 9 5 N/A
Trust Complaints - Formal CE Letter (Stage 3)(Apr 18 – Mar 19)
<270 192 183 ✔
Trust Complaints Compliance within 25days (Apr 18 – Feb 19) 95% 89.45% 96.00% ᵡTrust Falls with Fracture (Apr 18 – Mar 19) <20 23 26 ᵡIn Hospital Pressure Ulcers Grade 4 (Apr 18 – Feb 19) 2 2 2 ✔
Friends and Family Test - Would Recommend(Apr 18 – Mar 19) 95% 96.00% 95.10% ✔
Never Events (Apr 18 – Mar 19) 0% 0.00% 100.00% ✔
Hand Hygiene (Apr 18 – Mar 19) 95% 97.00% 97.00% ✔
HSMR (Feb 18 – Jan 19) 100 - 102 96.17 101.32 ✔
SHMI (Oct 17 – Sep 18) 100 - 106 100.72 105.91 ✔
SPEQS (Apr 18 – Mar 19) 90% 96.41% 92.23% ✔

1
Board of Directors
Title: NHS Access Standards Gap Analysis
Date: 25 April 2019
Prepared by: Lindsey Wallace, Head of Planning, Performance and Development
Executive Sponsor: Lynne Taylor, Director of Planning and Performance
Purpose of the report
To provide a gap analysis against the proposed pilot to test the NHS access standards and provide the Trusts position against performance.
Action required: Approve Assurance x Discuss x Information x
Strategic Objectives supported by this paper:
Putting Patients First
x Valuing our People
x Transforming our Services
Health and Wellbeing
Which CQC Standards apply to this report
Safe x Caring x Effective x Responsive x Well Led
x
Executive Summary and the key issues for consideration/ decision:
The attached report provides an overview of the proposed new access standards, post the review of current standards by Professor Stephen Powis, NHS National Medical Director. The report provides a gap analysis against the proposed standards, where available, providing the Board with a first stage review of the Trust’s position.
The Trust has been chosen as one of fourteen organisations to pilot the proposed standards over the next 6 months, with the aim of identifying the appropriateness, or not, of the individual standards, the potential impact of the standards on improved patient care and any significant gaps in both the availability of the data and the criteria set to record, monitor and report the revised indicators.
How this report impacts on current risks or highlights new risks:
No additional risk at the point in time.
The revised standards could potentially result in under-achievement of key compliance indicators in the future, if the appropriate pathways, recording, reporting and monitoring processes are not in place to deliver the new standards.
Appropriate action plans and mitigation will be developed as part of the pilot process to reduce any future risk.
Committees/groups where this item has been discussed
Executive Management Team, Planning, Performance and Compliance Committee.
Recommendation
The Board of Directors is asked to receive and note: The content of the Professor Powis proposal and the associated
revised standards; The initial gap analysis against the proposed standards, contained
within this report; The Trust’s current position against the proposed measures; and The Trust’s position in supporting the pilot of the proposed revised
indicators.

1
North Tees and Hartlepool NHS Foundation Trust
Meeting of the Board of Directors
25 April 2019
NHS Access Standards Gap Analysis
Report of the Director of Planning and Performance 1. Introduction/Purpose
1.1 The purpose of this report is to provide the Board of Directors with an update in
relation to the Trust’s position and development plans to support the pilot of the proposed revised ‘Access Standards’ on behalf of NHS England.
1.2 The history of the National Health Service is one of evolution and innovation, with each generation using the latest technology and treatments to meet the changing needs of patients and the public. It is well documented that standards and performance targets have incentivised and encouraged improvements in care and outcomes, and provided assurance on quality and availability of care when people need it. It is also recognised that in some cases the same targets can restrict the ability to innovate or result in other unintended consequences.
1.3 With this in mind, Professor Stephen Powis, the NHS National Medical Director, was
tasked in June 2018 to review the core set of NHS access standards, in the context of the model of service described in the NHS Long Term Plan, informed by the latest clinical and operational evidence, with the aim to provide recommendations to support the review and re-development of access and quality outcome standards.
1.4 The attached proposal sets out a review to consider what is already known, map
current standards against the revised standards and test and evaluate the proposed standards, with the aim of updating several of the existing standards, as set out in the NHS Constitution, including mental health, cancer, urgent and emergency care services and elective care, which will be clinically led.
1.5 It is envisaged that outcomes from the new standards will reduce waiting times across elective and emergency care services, improve clinical quality outcomes and encourage the modernisation of care pathways.
1.6 North Tees and Hartlepool has been identified as one of fourteen providers who will pilot and test the proposed access standards during 2019, which will then feed into the final review and potential implementation of the standards.
1.7 Appendix 1 details the proposed standards with Appendix 2 demonstrating the Trust’s current position against the revised standards, where available.
2. Cancer Standards
2.1 There are currently nine specific cancer standards, which have been in place in their current form since 2009, covering Two week GP referral to assessment, 31 day diagnosis to treatment and 62 day referral to treatment. The NHS Long Term plan is to improve early detection of cancer and improve cancer survival rates.

2
2.2 The proposal sets out to offer a faster diagnosis standard (within 28 days) and merge
together existing 31 day diagnosis to treatment standards and the 62 day referral to treatment standards. The review also proposes to remove the two week wait to first appointment standard. Combining the nine existing standards and one new standard into three.
2.3 No ‘targets’ have been specified however the initial information suggests the 28 day standard will be set at 85% of patients to have received a diagnosis (definitive cancer or not) within 28 days, including screening. The review is yet to determine how the new standards will be tested and evaluated but is expected to be rolled out from April 2020.
2.4 Based on these principles, the Trust is currently reporting an average of 83% for the 28 day standard (3 months data), 88.5% for 62 days and 99.5% against 31 day.
3. Urgent and Emergency Care Standards 3.1 The four hour waiting time standard has been in place since 2004, however historical
and on-going evidence suggests this is now out of date following various reviews across urgent and emergency care services over the past 15 years. Criticism of the four hour standards suggest it only measures a point in time, does not take into consideration the severity of a patient’s condition or quality outcomes and drives hospitals to look at ‘processes’ rather than clinical judgement.
3.2 The review recommends the following standards, however further guidance is required to enable providers to measure comparatively and include the correct denominators/ numerators, to ensure consistency of measurement and reporting;
3.3 The baseline performance has been measured using the average over the 2018/19 year to date period.
i. Time to initial clinical assessment in Emergency Departments and Urgent
Treatment Centres (Type 1 and 3 departments) - This information is currently available, with the Trust 2018/19 average reporting a ‘mean time’ of 11 minutes based on the provisional guidance. There is a further proposal to monitor this split by ‘admitted’ and ‘non admitted’ pathways. Based on this principle the Trust is reporting an average of 11 minutes for non-admitted and 13 minutes for admitted.
ii. Time to emergency treatment for critically ill and injured patients. The Trust is currently unable to measure against this proposed standard as further guidance is required to define the ‘critically ill and injured’ criteria. The standard also refers to a ‘complete package of treatment’ within the first hour for condition such as stroke, heart attack, major trauma, sepsis, acute severe asthma, mental health, which again requires further detailed criteria before a clear measurement can be monitored. Clarity will be sought during the pilot to ensure the Trust is able to capture this level of data at source.
iii. Total time in A&E (based on mean for Type 1 and Type 3) – The Trust
currently reports at 1 hour 27 minutes.
iv. Utilisation of same day emergency care (SDEC) – The Trust currently reports an 33.95% of emergency admission discharged with no overnight stay, with 23.1% equating to Ambulatory Care pathways.

3
v. The proposed Mental Health standards include a new measure of ‘Access to liaison psychiatry services within 1 hour for A&E departments. The Trust currently has support from both Adult (Tees Esk and Wear Valley Mental Health) and Children’s (Children’s and Adolescent Mental Health) within the A&E department, however at this point in time there is no data available to support this measure. Further work will be required on this indicator.
3.3 The pilot sites will be exempt from reporting against the Emergency 4-hour standard
during the testing period to ensure the participating organisations can test pathway changes without the influence of hitting current national access requirements.
4. Elective Care
4.1 There are currently three standards relating to elective care which addresses how quickly a patient can expect treatment against the 18 week referral to treatment standard, the six week diagnostic standard and short notice cancelled operations.
4.2 The NHS Long Term plan stipulate a zero tolerance approach to no patients waiting
over 52 weeks for an operation with recommendations to redesign outpatient and diagnostic services over the next five years.
4.3 The review sets out the following standards again with no targets specified for the new standards at this stage; Maximum wait of six weeks from referral to test for a diagnostic test to remain –
the Trust currently reports at 99.51% (March 2019) with a yearend position averaging of 98.69% (Performance impacted on by capacity issues in the first part of the year).
The defined maximum weeks wait for incomplete pathways (current target 92% within 18 weeks). This standard will be reviewed for on-going relevance. This may be replaced with the average wait target for incomplete pathways. The Trust is currently reporting at 94.45% within 18 weeks, with an average in-year compliance position of 94.12%, and an average 7 weeks wait. The new standard requires further clarification.
26 week patient choice offer. Patients are to be ‘offered’ alternative provider for
treatment if their treatment cannot be accommodated within 26 weeks. The Trust is reported an average of 185 patients waiting over 26 weeks during 2018/19, 2.01% of its overall RTT waiting list; however validation is on-going to understand the impact of patient choice to delay treatment and outstanding delays in documentation to support the stopping of RTT clocks on the long waiters. All remaining 26 week waiters will be prioritised and offered booked dates.
52 week treatment guarantee – the Trust has no patients waiting more than 52
weeks and remains compliant against this standard.
5 Next Steps
5.1 The proposal will pilot data collection against each distinct service area and during the test phase NHS England and NHS Improvement will engage with sites. The timeframe broadly sets six months for testing with roll out in the autumn. This will take the format of 6 weeks of testing, review and feedback, then another round of

4
testing. Final recommendations are expected in spring 2020. A public consultation is anticipated.
5.2 The first stage will include the release of baseline data for validation in April/May.
Webinar’s are currently being set up for key organisational leads to discuss the next steps.
5.3 The Trust will commence data collection against the proposed standards, alongside the Integrated Performance Dashboard, to fully engage in the pilot, identifying any gaps during the pilot stage, feeding back issues to the national team and addressing process changes internally where necessary.
6. Summary 6.1 The key NHS access standards and targets have played a pivotal and valuable role
in improving access to care in a timely manner and have become widely recognised as indicators of performance, however clinical practice has moved on, questioning relevance and best practice. NHS England has therefore pledged a review, clinically led, of all appropriate access standards to test against quality outcomes, with evidence evaluated to ascertain best clinical practice in the best interest of service users and patients.
6.2 As the Trust is one of the leading performing organisations for a number of national
standards, our successes are owing to the ability to innovate, reflect and develop services to represent the ever-changing demands of the population and, as a result of this, the Trust has been chosen to test the proposed standards in collaboration with NHS England and NHS Improvement.
8. Recommendations
The Board of Directors are asked to note:
The content of the Professor Powis proposal and the associated revised
standards; The initial gap analysis against the proposed standards, contained within this
report; The Trust’s current position against proposed measures; and The Trust’s position in supporting the pilot of the proposed revised indicators.
Lynne Taylor, Director of Planning and Performance

5
Appendix 1 – Proposed Standards
Cancer Standards

6
Urgent and Emergency Care Standards

7
Elective Care Standards

8

9
Appendix 2 – Trust Position against proposed standards
Cancer Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19 Average
Access Standards
1Faster Diagnosis Standard: Maximum 28-day wait to communication of definitive cancer / not cancer diagnosis for patients referred urgently (including those with breast symptoms) and from NHS cancer screening
79.00% 85.00% 87.00% 83.00%
2Maximum two-month (62-day) wait to first treatment from urgent GP referral (includes standard, screening and upgrade) 87.10% 87.71% 83.61% 89.57% 87.43% 91.44% 85.99% 93.10% 88.02% 90.83% 84.77% 90.71% 88.50%
3Maximum one-month (31-day) wait from decision to treat to any cancer treatment for all cancer patients (includes standard, surgery and drug) 99.49% 99.06% 100.00% 99.58% 98.36% 100.00% 100.00% 98.80% 100.00% 99.51% 100% 99.39% 99.51%
Urgent and Emergency Care Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19 Average
Access Standards
1Time to initial clinical assessment in Emergency Departments and Urgent Treatment Centres (mean includes Type 1 and 3) 00:11:59 00:11:46 00:10:56 00:11:21 00:10:36 00:11:19 00:10:57 00:11:20 00:12:26 00:13:37 00:14:46 00:11:25 00:11
1Time to initial clinical assessment in Emergency Departments and Urgent Treatment Centres for Non Admitted 00:11:48 00:11:30 00:10:35 00:11:09 00:10:13 00:10:55 00:10:36 00:10:59 00:11:46 00:13:34 00:14:51 00:11:00 00:11
1Time to initial clinical assessment in Emergency Departments and Urgent Treatment Centres for Admitted Patients 00:15:41 00:13:15 00:12:57 00:12:24 00:12:47 00:13:24 00:12:55 00:13:13 00:13:34 00:13:53 00:14:23 00:13:44 00:13
3 Total Time in A&E (mean Type 1 and Type 3) 01:25 01:25 01:23 01:25 01:21 01:25 01:28 01:27 01:29 01:37 01:37 01:27 01:27
Utilisation of Same day Emergency Care (Ambulatory Care) 22.60% 24.12% 23.78% 23.96% 24.01% 21.92% 22.09% 22.82% 21.45% 24.78% 22.88% 23.78% 23.10%
Utilisation of Same day Emergency Care (All emergency admissions) 34.38% 35.59% 35.78% 35.75% 33.85% 31.92% 32.28% 33.13% 32.98% 34.13% 33.24% 34.41% 33.95%
Elective Care Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19 Average
Access Standards
96.22% 97.24% 98.39% 98.97% 96.22% 99.25% 99.38% 99.86% 99.92% 99.73% 99.82% 99.51% 98.69%
93.66% 94.43% 94.25% 94.48% 94.06% 93.83% 94.14% 94.63% 93.64% 93.85% 94.54% 94.45% 94.12%
Supporting indicator
3 Average wait target for incomplete pathways (weeks) 7 7 7 7 7 7 7 7 7 7 7 7 7
26-week patient choice offer (Total patients > 26 weeks) 231 212 196 195 196 216 191 143 164 185 143 149 185
Total number of Incomplete waiting list 8301 9564 9801 9381 8401 9325 9833 9288 8931 8897 9277 9303 9191
% of patients > 26 weeks against total patients in period 2.8% 2.2% 2.0% 2.1% 2.3% 2.3% 1.9% 1.5% 1.8% 2.1% 1.5% 1.60% 2.01%
5 52-week treatment guarantee 0 0 0 0 0 0 0 0 0 0 0 0 0
Where cell is grey - data is not availableProvisional Data
4
Defined number of maximum weeks wait for incomplete pathways, with percentage threshold
Maximum wait of six weeks from referral to test, for diagnostic tests.1
2
4

Board of Directors
Date: 25 April 2019
Prepared by: Julie Lane, Director of Nursing, Patient Safety & Quality
Executive Sponsor: Julie Lane, Director of Nursing, Patient Safety & Quality
Purpose of the report
The report provides an update on the Trust position against the gram negative blood stream infection (GNBSI) self-assessment, and actions identified from the assessment
Action required: Approve Assurance Discuss Information
Strategic Objectives supported by this paper:
Putting Patients First
Valuing our People
Transforming our Services
Health and Wellbeing
Which CQC Standards apply to this report
Safe Caring Effective Responsive Well Led
Executive Summary and the key issues for consideration/ decision:
The Trust has reported a total of 455 GNBSI to 27 March 2019. Of these cases 68 are hospital onset and 377 are community onset. The GNBSI cases include E coli, Klebsiella and Pseudomonas all of which are included in the mandatory surveillance programme facilitated by Public Health England. The Secretary of State for Health announced a GNBSI reduction ‘ambition’ as part of the CCG Quality Premium programme in 2016. The ambition was to reduce GNBSI by 50% by 2021. In the recent 5-year Antimicrobial Resistance Action Plan this ambition has been amended to delivering a 25% reduction by 2021-22 with the full 50% by 2023-24. A self-assessment tool was published by NHS Improvement in January 2019 to enable organisations or systems to self assess against standards and identify areas for improvement. The self-assessment has been completed by the Trust and achieved a score of 18 out of a possible 21 points. The IPC annual programme and improvement plan to be approved at the Infection Control Committee in April 2019 will address the areas for improvement identified. A tool to calculate the estimated cost and mortality associated with E coli blood stream infections is available from NHSI and has been used to calculate that in 2017-18 E coli blood stream infections cost £455,000 in excess bed days and A&E costs and contributed to 44 excess deaths. There is no similar tool to calculate the cost of Klebsiella or Pseudomonas bacteraemia.
How this report impacts on current risks or highlights new risks:
Risk to reduction and management of Healthcare Associated Infections with consequent impact on Patient experience, clinical outcomes and finance
Committees/groups where this item has been discussed
Health Care Associated Infection Committee
Recommendation
The Board of Directors is asked to note the content of this report, the current position and the actions planned to achieve further improvements in 2019-20.

1
North Tees and Hartlepool NHS Foundation Trust
Meeting of the Board of Directors
25 April 2019
Gram Negative Bacteraemia Update Report
Report of the Director of Nursing, Patient Safety and Quality
1. Introduction/Background 1.1 The purpose of this report is to provide an update on healthcare associated infection
performance, specifically gram negative bacteraemia. 1.1 The national ambition is to reduce GNBSI by 25% by 2021-22 and by 50% by 2023-24.
This ambition applies to all reported cases. The organisation has set an internal reduction target of 10% for hospital onset cases since 2017-18. E coli has been chosen by NHS Improvement as the priority for action as this infection accounts for the largest proportion of reported GNBSI annually.
Safe
2. Gram Negative Bloodstream Infection
2.1 The GNBSI cases include E coli, Klebsiella and Pseudomonas blood cultures, all of which are included in the mandatory surveillance programme facilitated by Public Health England. Trust data is entered by the Infection Prevention and Control Team and signed off monthly by the Chief Executive.
2.2 In 2017 -18 the Trust achieved the 10% reduction target for E coli bacteraemia
reporting 16% fewer hospital onset cases than the previous year. However, community onset cases have continued to increase, making it important that we work with commissioners and local authorities to target actions at those patients who develop the bacteraemia outside of the hospital setting. To this end a Teeswide GNBSI Collaborative Forum was established. This is led by the CCG and reports into a Cumbria and North East HCAI Improvement Forum chaired by NHS England.
2.3 In 2018-19 to date a total of 39 hospital onset cases have been reported by the Trust.
This represents a 9.3% reduction on the previous year. Community cases are showing an increase with 317 cases reported to date. This represents a 4.2 % increase.
3. GNBSI Self-assessment
3.1 In January 2019 NHS Improvement, as part of the national improvement programme, published a self-assessment tool to allow an organisation or system to assess its overall approach to reducing E coli blood stream infections and the engagement with the wider health and social care sector in delivering a reduction together.
3.2 The assessment is split into sections headed leadership, infection prevention & control/patient safety and clinical staff and each question links to the Health and Social Care Act 2008 Code of Practice. Under these headings are seven subheadings with up to three points scored for each depending on the level of assurance selected. The Trust self-assessment scored 18 points with full marks in the leadership section, 4 out of 6 in the IPC/Patient safety section and 2 out of 3 in the Clinical staff section. A summary of the assessment can be found at Appendix 1

2
3.3 Where areas for improvement have been identified from the self-assessment these will be integrated into the IPC annual programme for 2019-20 and the HCAI Improvement Plan for 2019-20, both of which will be presented to the Infection Control Committee in April 2019.
3.4 Specific actions will include the implementation of a process to review a selection of community onset cases with commissioners, review of the Trust catheter passport and compliance with its use and reviewing the training on antimicrobial stewardship and its availability to staff. No major gaps were identified from the self-assessment and the participation in collaborative work already underway across Teesside and wider across the ICS has put the Trust in a good position.
4. GNBSI associated costs and mortality
4.1 Appendix 2 shows the calculation applied to demonstrate the estimated cost and
mortality associated with E coli bacteraemia cases for the Trust in 2017-18. It is estimated that the cost of the E coli blood cultures is £455,000 including excess bed days and A&E costs, and associated deaths is 44. This is an increase in both cost (£410,000) and associated deaths (40) from 2016-17.
5. Recommendation 5.1 The Board of Directors is asked to note the content of this report, the current position
and the actions planned to achieve further improvements in 2019-20.
Julie Lane Director of Nursing, Patient Safety and Quality

3
Appendix 1

4
Appendix 2

North Tees and Hartlepool NHS Foundation Trust
Board of Directors Meeting
Title: Draft Revenue and Capital Budgets 2019/20
Date: 25 April 2019
Prepared by: Kevin Scollay
Executive Sponsor: Neil Atkinson
Purpose of the report
To provide an overview of the Trusts approach to financial planning and the draft Capital and Revenue Budgets for 2019/20.
Action required: Approve x Assurance x Discuss Information x
Strategic Objectives supported by this paper:
Putting Patients First
Valuing our People
Transforming our Services
x Health and Wellbeing
Which CQC Standards apply to this report
Safe Caring Effective Responsive Well Led
x
Executive Summary and the key issues for consideration/ decision:
The paper outlines the process and assumptions used in arriving at the annual plan. It alsoprovides the draft revenue budgets by directorate and the 5 year capital plan (bothinternally and externally funded)
The Board of Directors are asked to approve the draft budgets included in the report.
How this report impacts on current risks or highlights new risks:
No new risks are identified in this report.
Committees/groups where this item has been discussed
Finance Committee.
Recommendation The Board of Directors is asked to:
Note the requirements of the AnnualOperational Planning for 2019/20, includingsystem wide delivery of clinical and financialrecovery;
Approve the draft revenue and capital budgetsas outlined in this paper.

1
North Tees & Hartlepool NHS Foundation Trust
Meeting of the Board of Directors
25 April 2019
Financial Planning - 2019/20
Report of the Director of Finance Strategic Aim and Objectives (the full set of Trust Aims can be found at the beginning of the Board of Directors Reports) Putting Patients First; Transforming our Services 1. Introduction/Background 1.1 The NHS Operational and Contracting Planning Guidance was released in January
2019, outlining the annual planning requirements for 2019/20.
1.2 This report provides an overview of the Trusts approach to financial planning and the draft Capital and Revenue Budgets for 2019/20.
2. Main content of report
Key Priorities and Overall Approach
2.1 The Trust has prepared a financial plan which is consistent with current financial
performance and run rate expenditure with realistic, but challenging, estimates for cost improvement, which are consistent with historic performance.
2.2 This plan is in keeping with the Trusts ambition to return to surplus as outlined in its 5-year financial strategy. This plan enables the Trust to sign up to the 2019/20 Control Total (c£10.2m deficit excluding non recurrent FRF, PSF and MRET funding) which reinforces the Trusts commitment to returning to recurrent financial balance. In the event the Trust meets the control total set by NHSI, the trust will receive c£10.2m of non recurrent PSF, FRF and MRET funding which will result in the Trust reporting a financially balanced position in 2019/20.
2.3 The submitted plan is aligned with commissioner assumptions. Like most health economies, significant financial challenges are faced by the local NHS. The Trust and the Commissioner have agreed to work closely to identify system solutions that will enable both provider and commissioner to meet their financial obligations for 2019/20. The contract form for 2019/20 reflects this commitment through the use of an Aligned Incentive Contract (AIC). This demonstrates the commitment of the Trust to work collaboratively in the ICP. The Trust is confident that it can support the system in this manner and continue to subscribe to its financial control total for 2019/20.

2
Modelling assumptions Income
2.4 Current run rates for activity have been used to produce a forecast of activity levels for the 2018/19 financial year. These forecasts have been normalised and used to establish baselines for activity trajectories. Activity trajectories are based on bottom up plans agreed by services and therefore reflect realistic levels of growth and therefore achievable income projections.
2.5 Income figures include a benefit from changes in contract form with commissioners. The aligned gain share (marginal rate) agreement has substantially benefitted the commissioner in 2018/19 as both case mix and activity has grown beyond planning expectations. This benefit is priced into the Trust contract position for 2019/20. The commissioner has accepted these assumptions into the contract baseline for 2019/20.
2.6 The Trust and the CCG have established closer working relationships to jointly manage financial risk across the local health economy. Joint working groups have been established to manage these risks. This will enable the Trust to influence and plan for the impact of QIPP in a more structured manner and ensures that incentives are aligned across both commissioner and provider.
2.7 Where services have been transferred to other providers such as Neo-Natal and Durham Community Services, these have been factored into the income projections for 2019/20.
Pay
2.8 Pay costs and establishments have been set for the 2019/20 financial year based on established run rates – including agency and bank costs. This approach has enabled the Trust to establish a realistic assessment of baseline costs for 2019/20.
2.9 Pay expenditure has been uplifted for specific items such as Agenda for Change pay awards, pay progression and the consultant pay award. Where CIP has been identified in 2018, but delivered non-recurrently, this has been reflected in the planning assumptions to ensure the CIP for 2019/20 realistically communicates the size of the challenge required to meet the Trusts Control Total. One off payments made to top of scale agenda for change staff in April 2019 have been included in the pay expenditure plan.
2.10 Pension contributions are rising in 2019. The Trust has been advised by NHSI not to include a pressure in our plan and that these contributions will be paid centrally by NHSE/NHSI in 2019. The Trust is expected to make payments for the increased level of contributions from April 2020 onwards and a commensurate increase in tariff income is expected. The trust has made provision in the budget for anticipated increases in agency and bank costs.
Non Pay
2.11 Baseline operating costs associated with non-pay expenditure have been set based on a normalised forecast for 2018/19. This has enabled the Trust to set a baseline commensurate with the current expenditure run rate.
2.12 Inflation has been included as well as an adjustment for increased activity levels assumed in the income plan.

3
Table 1: Financial Planning - Key Assumptions
Category Assumption
Income
Contract income Contract income has been uplifted in line with the 2019/20 tariffs at an HRG level. Activity levels have been set at realistic levels with the Trusts commissioners. Aligned incentive contract (AIC) (block with a risk share) is accepted as the contract form. The impact of transfer of Neo Natal and DDES community services to other providers has been included within the Income and the Expenditure figures.
Winter Pressures Included in the contract baseline.
Drugs/Other Pass though Costs
Pass through costs have been reflected for income and expenditure equally – Adulimumab price reductions have been applied to income.
Expenditure
Pay
WTEs have been aligned to pay budgets based on detail directorate plans which are triangulated with activity and pay expenditure plans. This is supplemented by inclusion of bank and agency budgets. Pay Inflation has been calculated based on the Agenda for Change and Consultant pay awards. General and winter contingency exists within the plan. The Trust has assumed activity growth arising from population and demographic changes will be absorbed within the existing budgeted establishment. Value of growth is split by both increased activity and continuous coding improvement to regional levels.
Non pay Inflationary uplift applied to non-pay expenditure as per national guidance with some pressures funded which are unavoidable (e.g. licencing costs)
Marginal cost of activity rises is included in the figures.
Efficiencies Cost Improvement Programme
c£15m efficiency target has been included (including system risks). The Trust is working towards fully identifying programmes to meet this target.
Capital and Cash Planning
2.13 The capital programme is funded through a combination of internally generated depreciation, cash carried forward from 2018/19 and external funding associated with specific programmes of work – specifically HSLA (Carescan+ and Digital radiology) and GDEFF. The capital plan for 2019/20 and beyond has therefore been split into internally generated and externally generated funds. This is outlined in the tables below.

4
Table 2 – Internally Generated Capital Plan
INTERNALLY GENERATED AND DONATED CAPITAL PLAN
2019/20 2020/21 2021/22 2022/23 2023/24
£'000 £'000 £'000 £'000 £'000
FUNDING DETAIL
Internally Generated Depreciation (now includes
estimate for GDEFF from 19/20)
9,139 9,439 9,729 9,729 9,729
Energy Centre Loan payback - reduction to internally
generated depreciation
1,089- 1,089- 1,089- 1,089- 1,089-
Other - donated assets estimate 204 204 204 204 204
Total internally generated and donated funding 8,254 8,554 8,843 8,843 8,843
PLANNED SPEND ( based on depreciation split)
Estates Total 3,680 3,680 3,680 3,680 3,680
Medical Equipment Total 2,499 2,199 2,199 2,199 2,199
I&TS Total 2,171 2,471 2,761 2,761 2,761
Contingency and donated assets Total 204 204 204 204 204
Total Capital Expenditure from internally generated
and donated funding
8,554 8,554 8,844 8,844 8,844
Surplus / (Shortfall) in Funding (300) (0) (0) (0) (0)
Table 3 – Externally Generated Capital Plan
EXTERNALLY FUNDED CAPITAL PLAN2019/20 2020/21 2021/22 2022/23 2023/24
£'000 £'000 £'000 £'000 £'000
FUNDING DETAIL
PDC for Digital Exemplar (GDEFF) 1,500 - - - -
PDC for Care scan plus 250 250 - - -
C/fwd Digital Radiology HSLI 50 - - - -
C/fwd PDC Digital Pathology 2,035 - - - -
C/fwd PDC Cancer Transformation 550 - - - -
C/fwd PDC for Digital Exemplar (GDEFF) 400 2,700 - - -
C/fwd PDC for Care scan plus 268 -
C/fwd PDC for Energy Centre 920 420 - - -
Total external funding 5,973 3,370 - - -
PLANNED SPEND
Estates Total 920 420 - - -
Digital GDEFF Total 1,900 2,700 - - -
Care scan plus Total 518 250 - - -
Cancer Transformation Total 550 - - - -
Digital Radiology HSLI Total 50 - - - -
Digital Pathology Total 2,035 - - - -
Total Capital Expenditure from external funding 5,973 3,370 - - -
Surplus / (Shortfall) in Funding 0 0 0 0 0
2.14 The Trust is required to repay ITFF loans associated with the development of the energy central and has made provision from a cash planning perspective to be able to fund this. From a cash perspective, the Trust does not expect to require interim revenue support for 2019/20 and has repaid outstanding interim support loans in full during 2018/19.

5
Risk
2.15 The plan currently contains some risk associated with delivery of CIP. The Trust expects to be in a position to have this fully identified and delivered to support delivery of the Control Total for 2019/20 – this will be delivered via the Programme Management and Improvement Office.
Internal financial management and budget setting
2.16 Control totals were initially issued to Directorates in August 2018. These have been updated in March 2019 to take into account;
Uplift in tariff income; Agreed unavoidable pressures via Executive Team; Virements (budget transfers between directorates); Redefined CIP allocation to take into account opportunity for delivery based on
reference cost data, and; A reward to directorates based on 2018/19 over-performance across the Trust.
2.17 Draft control totals have been distributed to directorates and a sign off process is
currently underway. These control totals are shown in the table below. Control totals include income associated with the service lines. This income is presented as a negative value (in brackets) and therefore some control totals are negative. No material issues have been identified in the engagement with directorates to date.
Table 4 – Proposed Directorate Control Totals
Directorate Revised CT
Accident And Emergency (153,325)
Anaesthetics 13,670,498
Eau & Ambulatory Care (976,268)
Endoscopy (3,759,393)
In Hospital Care (42,670,043)
Obs And Gynae (7,139,332)
Orthopaedics (13,305,888)
Out Of Hospital Care 1,218,363
Outpatients 2,670,318
Paediatrics (2,708,979)
Pathology 6,075,290
Pharmacy 2,587,973
Radiology 3,233,494
Research And Development 87,400
Surgery And Urology (10,465,857)
Urgent Care Services (2,273,247)
Winter 515,559
Chief Executive 1,992,807
Finance 2,879,071
I&Ts 7,893,684
Medical Director 523,560
Nursing And Patient Safety 4,120,307
Strategy, Operations & Performance 2,579,282
Workforce 5,197,039 3. Conclusion/Summary 3.1 The Trust has submitted its annual operating plan to NHSI and confirmed
acceptance of the control total. 3.2 Revenue budgets by directorate and capital budgets have been produced and
are summarised in this paper.

6
4. Recommendations 4.1 The Board of Directors is asked to:
Note the requirements of the Annual Operational Planning for 2019/20, including system wide delivery of clinical and financial recovery;
Approve the draft revenue and capital budgets.
Neil Atkinson Director of Finance

Board of Directors
Date: 25 April 2019
Prepared by: Gary Wright, Deputy Director of Workforce
Executive Sponsor: Alan Sheppard, Director of Workforce
Purpose of the report
To provide Board of Directors an update on NHS National Staff Survey results 2018 and associated actions.
Action required: Approve Assurance Discuss Information X
Strategic Objectives supported by this paper:
Putting Patients First
Valuing our People
X Transforming our Services
Health and Wellbeing
X
Which CQC Standards apply to this report
Safe Caring Effective Responsive Well Led
X
Executive Summary and the key issues for consideration/ decision:
High level summary of the 2018 National Staff Survey results showing that the Trust is above national average on eight of the ten indicators and scores average in the remaining two.
How this report impacts on current risks or highlights new risks:
Positive staff survey results enable the Trust to attract, develop and retain the best staff to deliver our strategic objectives.
Committees/groups where this item has been discussed
Culture Group Workforce & OD Committee
Recommendation
The Board is asked to acknowledge detail contained within the report and agree actions are appropriate.

1
North Tees and Hartlepool NHS Foundation Trust
Meeting of the Board of Directors
25 April 2019
NHS National Staff Survey Results 2018
1. Introduction
This report provides detail relating to the 2018 staff survey results; specifically in relation to the benchmarked report produced by the Survey Co-ordination Centre on behalf of the Department of Health. These reports provide the Trust with a national view on the staff survey responses and highlights areas of good practice and also those areas where focus may be required when compared against other similar Trusts.
A sample of 1250 staff were selected to participate in the survey, with 565 surveys completed. This gives a response rate of 45% which is above average when compared to similar Trusts nationally (41%).
2. Trust Results 2018
It is positive to note that of the ten themes covered in the 2018 staff survey, the Trust scored above average for eight themes and average for the remaining two themes.
The scores contained within this report range from 1 to 10, with 1 being the worst and 10 being the best score. As a Trust, it is important that we do not compare the scores across the themes and instead we are required to focus on the score in comparison with best/worst and average scores within that particular theme. Therefore, whilst Quality of Appraisals may seem to be low in comparison with the other themes, the Trust is performing well in this area when compared with other Trusts and we rank as above average in this area. The Trust’s highlights from the staff survey results (2018) show that almost three quarters of staff feel enthusiastic about their job. More than seven out of ten staff would recommend the organisation to family and friends for treatment and even more staff this year were satisfied with the recognition that they receive as a result of their good work. Nationally, the Trust scored the highest within the benchmarking group for taking positive action on the health and wellbeing of staff. This is an increase on our previous score and goes against the national benchmarking trend which has seen an overall and significant decline for 2018 (a reduction from 32.5% to 27.8%, as compared to the Trust’s response of 39.9%, increasing to 40.2% in 2018).
This is a direct result of the commitment of our award winning health and wellbeing team and the way in which we take a proactive approach to looking after our staff which in turn, enables staff to deliver better care to patients.
It is important that we consider the Trust’s position from a national perspective. ‘Listening into Action’ (LIA) have analysed the results of the national staff survey and they have created, for the 8th year running, the LIA Scatter Map. This provides a ‘helicopter view’ of how staff across the 230 NHS Providers rate their Trust leaders and culture. A copy of the LIA Scatter Map is contained at Appendix 1 of this paper and plots the Trust’s position on a 52 by 44 scale matrix against a performance axis and a trend axis. By reviewing staff responses to the 52 questions and comparing the results with those from the previous year, each trust has a grid co-ordinate for how staff rate their trust leadership and

2
culture against their peer group, and whether they are more or less positive than this time last year. The Map places each provider into one of four quadrants, with the top right quadrant being the best position. We are delighted that the Trust is placed within the top right quadrant which acknowledges an above average performance and a positive improvement on previous years. It is noted that our local Trusts are not performing as well and are are placed within the bottom left quadrant of the map. This is regarded as the worst position to be placed, with staff views on leadership and culture reported as resoundingly negative. We recognise that such an achievement for this Trust does not happen accidentally and it is important that we highlight that our performance in this area is testament to the way in which we invest in our staff and value the contribution that they make. We continuously strive to be an employer of choice - to attract and retain quality staff and support them with continued development throughout their employment with us. By enhancing our staff engagement function and continuing to invest in organisational development activities, we believe that this has had a significant impact on our performance, which is reflected in numerous areas including our band 5 nursing vacancy rate, which currently sits at below 1.5%. 3. Detailed Results The following section of the report reflects the detail of the Trust’s responses, broken down by each of the ten themes. 3.1 Staff Engagement The Staff Engagement indicator considers the ability of staff to contribute to improvements at work; a willingness to recommend the Trust as a place to work or receive treatment and; the extent to which staff feel motivated and engaged in their work. The Trust’s score of 7.2 shows a continued and sustained positive trend. The Trust’s score in relation to this theme is above average when compared to other similar Trusts within the benchmark (7.0).
2014 2015 2016 2017 2018 6.6 6.9 7.1 7.0 7.2
It is positive to note a steady improvement in the Trust’s engagement score over the previous years which is a reflection on the activities developed and implemented with the 4 key priority areas in mind:
Increasing compliance and quality of performance appraisals across the Trust; Ensuring all staff know how they can (and do) make a positive impact on patient care; Recognising and celebrating good practice; Communicating the strategic vision and the part we all play in making the vision a
reality.
3.2 Equality, diversity and inclusion The Trust scored a positive 9.2 in this theme, which is reflective of the national benchmarked average. Responses were extremely positive in relation to acting fairly on career progression and promotion, and also the low number of people who have experienced discrimination at work from their manager or colleagues.

3
2014 2015 2016 2017 2018 9.3 9.4 9.4 9.4 9.2
3.3 Health and wellbeing The Trust’s score of 6.2 is above the national benchmarked average of 5.9. This theme considers opportunities for flexible working (the Trust scored higher than average); whether individuals have suffered MSK problems or stress as a result of work (the Trust scored lower than average) and how positive the Trust is in relation to health and wellbeing – the Trust achieved the best national score within the benchmarking group for this key finding.
2014 2015 2016 2017 2018 N/A 6.0 6.2 6.3 6.2
3.4 Immediate Managers This theme considers staff experience in relation to support, involvement and feedback provided by line managers across the Trust. With a score of 7.0, the Trust rates higher than the national benchmarked average (6.8) with positive outcomes highlighted relating to feedback, interest in health and wellbeing, managers valuing their staff and supporting staff in their learning, training and development.
2014 2015 2016 2017 2018 N/A 6.6 6.9 6.8 7.0
3.5 Morale Staff morale is a new theme for 2018 and as a result, there is no historical data for us to compare against. The Trust’s score of 6.3 is above the national average for similar Trusts (6.2). The Trust rated most positive in relation to the respect shown to staff from their colleagues; encouragement received from managers, and; the low number of people thinking about leaving the Trust. 3.6 Quality of Appraisal The Trust’s score of 5.6 is above the national average for similar Trusts (5.4). There was positive feedback in this category, with a high number of staff reporting that the appraisal had helped them to do their job and also helped them to agree clear objectives. We achieved the highest score within the national benchmark for the number of staff reporting that their appraisal had made them feel valued by the Trust (38% as compared to the average of 31.1%).
2014 2015 2016 2017 2018 N/A 4.7 5.4 5.2 5.6
3.7 Quality of Care A consistently high score has been achieved in relation to the theme of quality of care over previous years and the Trust continues to score above average when compared to other Trusts nationally (7.7 compared to 7.4). It is pleasing to note particularly positive responses relating to satisfaction of the quality of care given to patients, and staff being able to deliver the quality of care that they aspire to.

4
2014 2015 2016 2017 2018 N/A 7.4 7.6 7.7 7.7
3.8 Safe environment – bullying and harassment The Trust continues to achieve a positive trend for this theme, particularly in relation to the number of times staff have experienced harassment, bullying or abuse from managers or colleague, with scores in this area reported as below the national benchmarked average. Whilst seeing a decline in the number of staff experiencing this type of behaviour from patients, relatives or other members of the public since the 2017 survey, the Trust score is above the national benchmarked average in this area and has therefore been identified as a continued area of priority. This will be taken forward by the Trust’s Keeping Staff Safe group and a number of actions have been identified, some of which have already been implemented in 2018, i.e. the Respect Campaign
2014 2015 2016 2017 2018 N/A 8.0 8.2 8.0 8.2
3.9 Safe environment – violence Despite seeing a positive trend over the previous 3 years, the Trust’s score of 9.5 for 2018 is comparable to the national benchmarked average. The Trust scored 0% in relation to the number of staff experiencing violence from managers and was below the national benchmarked average when considering violence from other colleagues (1.2% compared to the average of 1.5%). When considering violence from patients, relatives or other members of the public the Trust score remains static and is above the national benchmarked average (14.9% compared to the average of 12.6%). As with 3.8 above, this action will be taken forward by the Trust’s Keeping Staff Safe group.
2014 2015 2016 2017 2018 N/A 9.4 9.2 9.4 9.5
3.10 Safety culture The Trust has reported a positive increase in relation to the safety culture within the organisation, which supports the Trust’s objective of putting patients at the centre of all we do. We achieved a significantly above average score in the number of staff who would feel secure in raising concerns about unsafe clinical practice and staff having confidence that the Trust would address and act upon those concerns. There were also positive trends in relation to reporting errors, near missed or incidents. Our improved performance within this theme can be attributed to the appointment of the Trust’s Freedom To Speak Up Guardian in 2018, which is now an independent role with dedicated time commitment to act upon the concerns raised by staff.

5
2014 2015 2016 2017 2018 N/A 6.6 6.8 6.8 7.0
4. Taking things forward It is right to that we celebrate the areas of good practice that are clearly demonstrated throughout the 2018 staff survey results. These achievements are a product of the dedicated focus provided across the Trust in relation to improving engagement, recognition, values and behaviours, equality, diversity and inclusion, and many other cultural related elements that can be measured through the staff survey. A priority of the Trust going forward continues to be our journey to outstanding; with positive correlation evidenced between excellent leadership, engagement and quality and being an Outstanding Trust from a CQC rating perspective. As a result, focus and priority will be given to those elements contained within the staff survey that are linked to engagement, leadership and quality. 4.1 Engagement . Although the Trust rates as above average when compared to other similar Trusts, it is important that we aim to achieve the best score in the benchmark group. The key activities that have been identified and are planned to support this aim include: Develop robust mechanisms that empower staff to make a difference in their area of
work/across the Trust; Improved communication and feedback in relation to responding to staff comments and
suggestions; Develop robust mechanisms to share best practice across Trust/System; Increase participation/response rate of the National NHS Staff Survey; Ensure engagement/communication takes into account generational differences; Undertake greater utilisation of pulse surveys with action taken in response, as
appropriate. 4.2 Leadership
Engagement Score
Trust 7.2, Best 7.4 Staff recommending
the organisation as a place to work
Staff ability to contribute
towards improvements
at work
Staff motivation at
work
Leadership Score Trust 7.0, Best
7.3
Team Management
Development
& Support
Senior
Leadership

6
Having leaders that demonstrate the appropriate skills, behaviours and values on a daily basis are crucial to the successful future of the Trust. Whilst ‘recruiting the correct leaders’ plays a vital part in this (i.e. recruiting for values), this should also be continuously tested and further developed throughout the period of employment. The key activities that have been identified and are planned to support this aim include: Commit to ensuring leaders are visible at all levels of the Organisation; Revise recruitment practices to mirror a Recruitment Centre approach; where values
and behaviours are observed and always include service users at interview; Challenge leaders that do not display the values and behaviours that we aspire to and
take action where necessary (support or otherwise); Promote good practice; Improve links from staff appraisal to targeted development; By working with our partners, utilise the apprentice levy to develop current and future
leaders; Encourage and promote role modelling; Provide the right environment of support, to stretch and grow our leaders – celebrate
success and learn from mistakes. 4.3 Quality Again, whilst scoring positively in the quality related aspects of the NHS staff survey, it is appropriate that we continue to strive for improvement with a view to being the best in the benchmarking group. The key activities that have been identified and are planned to support this aim include: Develop Business Intelligence (BI) across Care Groups and Systems; Commission Life QI as an agreed platform to collate Improvements; Agree QI methodology and introduce QI at induction at all levels; Agree Education across Care Groups, including understanding change and normal
variance; Develop ‘Quality Summit’ across Care Groups for all; Embed Just Culture across Care Groups; Develop strategies to engage and co-produce/improve services with the people who
use them; Equip staff to engage, listen and act on behalf of the people who use services and not
to welcome feedback.
Quality Score
Trust 7.7, Best 7.9
Safety
Culture
Effective
Patient
Experience

7
5. Recommendation The Trust Board is requested to note the content of this paper; noting in particular the on-going activity relating to analysing the information presented within the NHS staff survey and continued use of action planning going forward. Alan Sheppard Director of Workforce

1
Appendix 1

Board of Directors
Date: 25 April 2019
Prepared by: Prof Jane Metcalf and Janet Alderton
Executive Sponsor: Medical Director
Purpose of the report
To provide an overview of the learning obtained through the review of deaths that occur within the organisation. Also, to provide details from the clinical teams around actions that have been implemented as a result of the overall learning and, where available, to provide an evaluation of the impact of these.
Action required: Approve X Assurance X Discuss Information
Strategic Objectives supported by this paper:
Putting Patients First
X Valuing our People
Transforming our Services
Health and Wellbeing
X
Which CQC Standards apply to this report
Safe X Caring X Effective X Responsive X Well Led
X
Executive Summary and the key issues for consideration/ decision:
1. The Trusts HSMR value in the latest period has decreased to 96.17 (February 2018 to January 2019), the SHMI is currently 100.72 (October 2017 to September 2018).
2. There has been a sustained improvement in the level of care being documented which has helped sustain the current reported national mortality statistics.
3. During 2018-19, 78% of the compulsory mortality reviews identified using the Trust Learning from Deaths policy have been reviewed.
4. There are a number of workstreams in place, to support ongoing clinical and service improvements. There is an updated from several of these within this report.
How this report impacts on current risks or highlights new risks:
Any new risks identified through mortality review processes are assessed and added to the risk register as needed.
Committees/groups where this item has been discussed
Trust Outcome Performance, Delivery and Operational Group
Recommendation
1. The Board of Directors is asked to note the content of this report and to derive assurance that there is continued focus to ensure in depth multidisciplinary learning being is obtained from mortality review processes.
2. The Board is asked to recognise the continued sustained improvement in the national mortality statistics.

1
North Tees and Hartlepool NHS Foundation Trust
Meeting of the Board of Directors
25 April 2019
Learning from Deaths Report
Report of the Medical Director
1. Introduction/Background 1.1 In March 2017, the National Quality Board (NQB) published national guidance “Learning from
Deaths: A Framework for NHS Trust and NHS Foundation Trusts on Identifying, Reporting, Investigating and Learning from Deaths in Care”. The guidance provide requirements for Trust to implement as a minimum in order ensure there is a focused approach towards responding to and learning from deaths of patients in our care.
1.2 The Trust strives to improve the care provided to all of our patients; the overall aim is to identify,
understand and implement improvements where any issues are related to the provision of safe and effective quality care. It is considered that if such safety and quality improvements are initiated effectively and embedded, then the mortality statistics will naturally show improvement.
1.3 The information presented in this report provides an overview of learning from deaths that has
been obtained from mortality reviews undertaken by the Trust. The Trust policy identifies some key areas where all deaths will be reviewed and also identifies additional randomly selected cases will also be included in the review process. Some compulsory review areas have small numbers; therefore learning is presented as a summation of all reviews to reduce the risk of identifying cases directly.
2. Mortality Data
2.1 Information related to mortality is gathered from data provided routinely by the Trust to a national system where all hospital episode statistics (HES Data) is collated. Hospital Standardised Mortality Ratio (HSMR) examines information covering 56 diagnostic groups that are identified as accounting for 80% of hospital deaths nationally. This information is used to calculate an overall HSMR taking into account, gender of the patient, age, how the patient was admitted (emergency or elective), levels of deprivation, how many times they have been admitted as an emergency in the last year, if palliative care was provided and various details relating to presenting complaint on admission.
2.2 This calculation is undertaken nationally and provides the Trusts overall HSMR. The latest HSMR value is 96.17 (February 2018 to January 2019) which represents a continued decrease. This new value continues to ensure the Trust remains in the „as expected‟ range.
2.3 The Trust currently has the 44th lowest HSMR value from the 137 Trusts nationally, and the lowest value out of the 8 North East Trusts.
2.4 The Summary Hospital-level Mortality Indicator (SHMI) is a ratio between the number of actual (observed) deaths to the “expected” number of deaths for an individual Trust, including deaths in hospital and up to 30 days following discharge. The ratio is calculated with consideration of gender, age, admission method, admissions in the last year and diagnosis being treated for the last admission.
2.5 The ratio is calculated nationally and provides the trusts overall SHMI. The latest SHMI value is 100.72 (October 2017 to September 2018); this also represents a continued decrease. The value continues to ensure the Trust remains in the „as expected‟ range.

2
2.6 The Trust currently has the 70th lowest SHMI value from the 137 Trusts nationally, and 3rd
lowest value out of the 8 North East Trusts.
2.7 There continues to be an ongoing focus on ensuring there is accurate documentation of the diagnosis and co-morbidities; this information is required to ensure there is clear clinical communication between healthcare professionals who are caring for the patients.
2.8 The increased focus on this should allow the Trust to maintain clearer clinical records but also maintain the current statistical mortality rates over the winter period when there are nationally more deaths occurring.
3. Mortality reviews 3.1 The Trust uses an electronic system to record mortality case reviews that are undertaken; this
system is also used by other trusts in the region and is based on the “PRISM” methodology, one of the review tools recommended in the national guidance. This is a structured review of a case record, carried out by clinicians not involved in the patient‟s care, to determine whether there were any problems in care. Case record review is undertaken routinely to learn and improve in the absence of any concerns, with all directorates undertaking their own specialty based mortality and morbidity meetings. This is because it can help identify issues where there are no initial concerns. It is also used where concerns exist, such as when bereaved families or members of staff raise issues about care.
3.2 The Trust policy identifies that all in-patient deaths and those in the Accident and Emergency department are included in the scope of the mortality reviews. Since April 2017 the Trust has reported the following deaths:
The following chart shows the overall numbers of deaths in the Trust since April 2016:

3
3.3 The Trust policy identifies specific cases where a compulsory review is required; these include:
• Where requests are made by families to undertake a case review.
• Where staff request a case review.
• All deaths in the Intensive Care Unit (ICU).
• All deaths linked to complaints about significant concerns in relation to clinical care.
• All deaths linked to Serious Incident investigations.
• All deaths where the patient was admitted for elective treatment.
Compulsory case reviews are also undertaken for the following cases, which are linked to specific national review processes, some of these reviews are not yet recorded in the Trust mortality system and this is an area of ongoing development:
• All deaths where a patient has a registered Learning Disability (LD) – in conjunction with the Learning Disability Mortality Review Programme (LeDER).
• All maternal deaths – in conjunction with M-BRRACE-UK.
• All deaths where the patient has a severe mental illness – in conjunction with local Mental Health Trusts as required.
• All child deaths (up to 18th birthday) – in conjunction with the Child Death Overview Panel (CDOP) process.
• All stillbirths – in conjunction with nationally agreed Perinatal Mortality Review tool.
There are also additional reviews that are undertaken either as a random selection or in response to requests internal or external to the Trust.
3.4 Where a patient‟s death immediately raises concern this should be reported and escalated through the Trusts incident reporting process, implementing Duty of Candour procedures as required. This includes informing senior staff of the case and the identified concerns; the details of the case will then be considered in line with the national Serious Incident framework and reported to the Trusts commissioners. A case record review is completed as part of the investigation process. In all cases investigated as serious incidents Duty of Candour has been considered and applied appropriately.
From April 2018 to date there have been 16 cases reported and investigated as serious
incidents, all of these were identified prior to mortality reviews being completed. Of these cases 11 have been investigated and reviewed, none of the cases were considered to be avoidable deaths (judged to be more likely than not to have been due to problems in the care provided to the patient). The remaining 5 investigations are currently being completed and the overall outcome will be reported in future reports.
3.5 The data presented in the appendix provides detail of all case reviews undertaken since April 2018. There are cases that may not have been identified immediately but have come to light as a result of the receipt of complaints and family requests through the Trust Bereavement survey; as a result there are some reviews pending completion and details may change slightly for each report.

4
3.6 The following table provides a summary of the data by financial quarters, to date, for 2018-19; a more detailed monthly breakdown is included in appendix 1.
2018-19 Q1 Q2 Q3 Q4 Total
Total deaths in scope 342 317 406 397 1462
Deaths in compulsory criteria 45 44 41 41 171
Compulsory case reviews completed (no.) 43 41 32 17 133
Compulsory case reviews completed (%) 97% 93% 78% 41% 78%
Compulsory reviews pending 2 3 9 24 38
Additional reviews completed 21 10 13 17 61
Total of reviews completed (no.) 64 51 45 34 194
Total of reviews completed (%) 19% 16% 11% 8% 13%
Reviewed Deaths considered avoidable (no.) 0 0 0 0 0
Reviewed Deaths considered avoidable (%) 0% 0% 0% 0% 0%
Reviewed Deaths considered not preventable (no.) 64 51 45 34 194
Reviewed Deaths considered not preventable (%) 100% 100% 100% 100% 100%
3.7 Medical Examiners
Over recent years a national Coronial review has been completed; this review identified a variety of recommendations one of which relates to the introduction of a “Medical Examiners” (ME) role that is responsible for reviewing deaths and speaking with families in relation to any concerns they may have. The role of the ME has been extensively discussed at the Regional Mortality meeting, which the Trust is part of, however, no consensus has been reached. A neighbouring Trust has already successfully implemented a ME team; some Trust are not planning on developing this role until there is clarity around funding or if it is mandated. The Trust feels that we should develop this role in order to improve quality of death certification and also improve liaison with the bereaved.
At this time a business case to support implementation over the next year is currently being
developed for consideration through the normal Trust procedures. It is envisaged that as this role is implemented, there will be changes to the mortality review processes already in place; however it is considered that this will only improve the overall analysis of mortalities.
4. Learning and actions from reviews 4.1 Learning Disabilities
The Trust has continued to be involved in the national Learning Disabilities Mortality Review (LeDeR) process specifically looking at all deaths of people with a learning disability, these reviews are comprehensive, looking at the full life span of the person and identifying areas where care could be improved to enable the person to live a longer life, we also identify good practice.
Nationally these reviews have been scrutinised and four areas for development have been
identified with actions being developed regionally and nationally. The areas are: • aspiration pneumonia • easy read health promotion • constipation • carers recognising the deteriorating patient.
Fact sheets have been developed by LeDeR for these four areas and are available on the
national LeDeR website. Regionally, the Learning Disability team have developed a STOP and WAIT tool to work with non-hospital carers to help identify deteriorating patients to then ensure appropriate and timely access health care.

5
Within the Trust reviews we have identified good practice, including evidence of multi-agency work to reduce the risk of self-neglect behaviour with good effect and excellent evidence of using community services to help complex patients avoid a hospital admission. We have identified one area for action, which was the follow up treatment and advice for someone who was obese and presenting to hospital. As a result of looking at this from a multi-agency point of view, we have identified that North of Tees Learning Disability Community Team does not have a specialist dietician where equivalent regional teams have this provision.
In order to encourage people with a learning disability to access bowel screening, the Trust
bowel screening team have completed a refresh of their website which includes easy read information and accessible information. This has been shared with community learning disability teams, local carers groups and local Learning Disability Partnership boards for information and feedback.
In order to increase overall knowledge and awareness the Trust is also including Learning
Disability and Autism awareness sessions as part of the mandatory training for all staff groups during 2019-20.
4.2 End of Life care
Subsequent to learning from mortality reviews, end of life care planning across the organisation, supported by the Specialist Palliative Care Team (SPCT) as a part of the Out of Hospital Care Directorate (OOHC) has continued to develop and progress.
This has included work undertaken to update the Trust Resuscitation policy; with an addendum
now added to enable suitably trained Senior Nurses, Clinical Nurse Specialists and Allied Healthcare Professionals (AHP‟s) to be able to complete regional Do Not Attempt Cardio Pulmonary Resuscitation (DNACPR) forms. Advance Care Planning remains a priority topic in teaching across the organisation and beyond and is now delivered to nurses, medics and students across the disciplines. This includes the proposed trust-wide rollout of the AMBER Care Bundle.
Changes to the way we use our IT Systems has enabled integration into the Trust SystmOne
modules, the ability to pass “Special Patient Notes” directly to the North East Ambulance Service (NEAS) Control Room via secure electronic system. This is promoting greater partnership working and also improved patient experience should our emergency service colleagues need to attend the patient in their place of residence.
To enable and empower patients and those close to them to tell of their experience around
palliative and end of life care, the Trust continues to be part of the Palliative & End of Life Project (PEOLC) run by Care Opinion/Hospice UK, supported by the Scottish Government. The project is supporting 12 clinical teams, selected through an application process and representing a diversity of hospice, hospital and community care services in different parts of the UK, with North Tees & Hartlepool NHS Foundation Trust being one of the 12.
The Care Opinion project has encouraged patients, and those close to them, to share their
stories of palliative and end of life care. Whilst there are only few stories to date, they have started to tell us what we do well and what could be done better. Reviewing this information is such a timely manner has enabled us to look at making improvements quickly as issues come to light.
To ensure there is additional resilience in the Specialist Palliative Care Team to be able to
support clinical teams with end of life care, we developed an innovative approach of a Specialist Palliative Care Nursing Bank. We have become the first Trust regionally to establish Specialist Bank staffing in partnership with NHS Professionals.

6
Greater work on pathway design and strategic development around palliative and end of life care services continues to be ongoing between the organisation and strategic stakeholders across the North Tees & Hartlepool NHS Foundation Trust geographical footprint.
The introduction of the “e-observations” module as part of the electronic patient record will
support improvements in the identification and monitoring of the deteriorating patient. This will potentially highlight patients who may then be identified as approaching end of life care, through the decision to stop routine clinical physiological observation. We are looking to work with IT colleagues to introduce monitoring of „Comfort Observations‟ at that time; these observations will look at comfort, symptoms and care of the patient and family, in accordance with the regional „Caring for a Dying Patient Document (CDP).
There are further plans to enhance the collaborative working between the specialist palliative
and end of life care team (SPCT) and Critical Care Outreach Team (CCOT), this is in order to improve and support smoother transition of care, ceilings of treatment, management planning and identification of patients with uncertain recovery. This will be developed alongside the planned stratified introduction of the AMBER Care Bundle across the inpatient areas of the organisation.
The development of an End of Life Forum within the organisation has been identified as a key
priority for the coming year; this work will be led by the Macmillan Lead Nurse for End of Life Care & the Lead Chaplin. This will support the development of „Role Champions‟ across all clinical areas to raise the profile of Palliative and End of Life care which is also planned across the coming year.
In a drive to improve awareness around the importance of palliative and end of life care, in
conjunction with our communications team colleagues, the SPCT will be developing a strategy to improve public facing information around palliative care, end of life care, Advance Care Planning and Priorities of Care. This will include the development of a „Care Opinion Wall‟, social media campaign and events in the annual „Dying Matters Week‟.
The Trust will be continuing its on-going commitment to supporting national developments
around uncertain recovery, palliative care and end of life care with representation in the AMBER Care Bundle Strategic Network, along with a clinical advisor representative in the national EOLC Practitioners Network, being developed by NHS Improvement. Education of staff across all professional groups will continue to remain a high priority around end of life care, with study days and opportunities planned throughout the coming year, including a Collaborative GP/Consultant event.
4.3 Engagement with families / carers
The Trust has for the last 2 years actively encouraged feedback from families and carers in relation to how they feel bereavement is handled. All families are provided with a “bereavement survey” to complete, when they feel ready, to provide information on their experiences and if they think there is something staff can do to improve care and communication at such a difficult time.
Since the introduction of the survey there have been 151 completed and returned to date. The
majority of these provide very positive feedback about the care provided and this is passed on to the relevant ward and staff involved. There are others where concerns have been identified; these have been shared with the relevant areas and also the Trusts Patient Experience team, a number of these have been handled through the Trusts complaints process. Many of the issues raised through the survey relate to communication and compassion; these are disseminated across the organisation for overall learning but are also taken into account through the updates and training provided by the SPCT as described in the previous section.

7
The survey also gives families an opportunity to request that a mortality review is completed by the Trust; families are asked to supply the details of the patient to support this. To date in 2018-19, 20 such requests have been made. Many of the requests for reviews are made despite positive feedback being provided on the survey; there are also a significant number of surveys returned where concerns are raised but no details are given to support identifying the patient involved. As a result the trust is looking at changing the wording on the survey to help support families and carers. All requests for reviews are followed up and completed; to date none have had to be escalated as a result of possibly being preventable.
4.4 Perinatal Mortality Review Tool
In response to the recommendations of the MBRRACE-UK (Mothers and Babies: Reducing Risk through Audits and Confidential Enquiries in the UK) reports, the Department of Health on December 2017 issued guidance that all Trusts should ensure that all stillbirths and neonatal deaths are reviewed by an appropriate multidisciplinary team using a standardised mortality review tool and process. Recommending that MBRRACE-UK should work closely with Trusts in order to build on the skills and experience developed through stillbirth audit to establish a process for ongoing quality assurance of local mortality to identify learning from cases.
The standardised Perinatal Mortality Review tool (PMRT) has been introduced to support this
work and the Trust has implemented the use of this tool to support the completion of high quality reviews of stillbirths and neonatal deaths. The PMRT is designed to facilitate robust, systematic, multidisciplinary reviews with parental involvement and come to a clear understanding of why each baby died and whether with different actions the death of their baby might have been prevented. The tool development is an iterative process with on-going opportunities to develop and improve the tool during the two-year pilot 2018/2020.
The overall aim of the clinical review process for stillbirths is to try to explain to parents why
their baby may have died and secondly, to support the Trust to identify areas for learning. The use of tools such as PMRT, as a framework to support case review, is standardising processes and preventing conclusions being drawn without full analysis of the facts.
However, the value of multi-professional, cross organisational discussions is central to good
review of care. External review to provide objectivity undoubtedly has a role to play in quality assuring processes, and also demonstrating transparency to families and the wider public. It is necessary that only those staff with in-depth local knowledge of systems, processes and culture will be able to provide the appropriate context and understanding required to identify and solve problems. Relevant clinical staff may benefit from additional training to lead and/or participate in reviews and this will be examined as this work progresses.
As a result of undertaking these reviews the Obstetric team have identified two areas for action:
Risk Assessments: Good antenatal care in preventing complications and in optimising both maternal and fetal outcomes, by the management of risk, are seen as central to the entire pathway so that women who have pre-existing conditions, risks associated with a higher incidence of stillbirth or those that develop complications during pregnancy are managed appropriately. It should be clear what type of care a woman is receiving and the rationale for such. Any changes to the pathway should also be clearly documented; a common theme was lack of clarity on referrals to consultant care, management plans and incomplete risk assessment both at booking and where there was a change to a woman‟s risk profile during pregnancy. Current risk assessments are in line with national guidance, however the team have made some changes to the documentation and staff who complete the risk assessments are having updates within mandatory training sessions. There is also collaboration with neighbouring Trusts in relation to the management of women across boundaries.

8
A number of communication issues were highlighted in the reviews which related to interactions with families and other stakeholders; these resulted in a detrimental impact on the family experience. Communication issues were also noted in relation to the management of complex pregnancies resulting in inadequate sharing of information/management plan between professionals. The team have included communication within the mandatory training for maternity staff and also included this as part of the simulation training exercises.
4.5 Sepsis diagnosis and management
As a result of undertaking mortality reviews, the Trusts Sepsis group have further enhanced multiprofessional education and training in relation to sepsis screening, supporting rapid recognition and management. The Sepsis guidance is being reviewed; this is based on the regional guidance. Across the Trust there are “Sepsis Champions” identified to support application of these guidelines; however the Trust recognises the importance of this being a multidisciplinary approach and that all staff have responsibility for this.
Part of the ongoing work in relation to sepsis is to examine ways of promoting early recognition
of sepsis. The Trust will be continuing engagement with primary care professional teams and NEAS to support this, alongside the work being undertaken by the Alliance as described earlier.
The Trust are planning to hold a “Sepsis” week in September, this is being timed to coincide
with World Sepsis Day. On this day the Trust will be focussing on raising awareness with patients, the public and staff. A specific multiprofessional Sepsis training day is also being planned to include awareness/teaching sessions and clinical simulation opportunities.
4.6 Intensive Treatment Unit
The Intensive Treatment Unit (ITU) team undertake mortality reviews for all patients that pass away in the department; these form the larger part of the Trusts agreed mandatory reviews. Many of the patients who die on ITU are there for short periods, often being admitted to the trust in a critical condition with a high risk of a poor outcome. However, there are a small number of patients who have a prolonged stay on the unit having active treatments for their illness.
As a result of undertaking the mortality reviews, the ITU team have identified that there were
occasionally inconsistent management plans and communication in relation to patients who had prolonged stays in the unit. In order to impact upon this the team have introduced the need for a multidisciplinary team (MDT) planning meeting for all of these patients to occur every Wednesday. This MDT planning meeting includes an update on progress, details of what has been discussed with the patients‟ family, agreement in relation to MDT decision making and agreements about the levels of care to be offered / provided.
The current evaluation from staff involved in these MDT planning meetings is that these are
having a positive impact and that the team approach has led to fewer isolated decisions being made. There has been suggestion made by the team that a fixed proforma to record the discussion should be developed to reduce discussion duplication and confirm previous agreed action points. It is hoped that this approach will support the families and carers of the patient during this time by ensuring there is consistent communication during this difficult period of time and also allowing them to feel they have been included in planning. Currently the evaluation has been from staff as the process has been developed; the feedback from families will be reviewed over the coming year.
4.7 Urinary Tract Infections
Over the last 2-3 years the Trust has completed record reviews where patients had been admitted and diagnosed with urinary tract infections (UTI). Following analysis of the reviews completed it was identified that all of the patients involved were frail and elderly; and in around

9
50% of cases the diagnosis of a UTI had not been confirmed and it was possible that some of these patients may not have needed admission into hospital.
Part of the improvements suggested from the reviews was for the Trust to examine ways of
improving the diagnosis and management of UTI in the elderly. The Trust participated in a UTI Collaborative facilitated by NHS Improvement, with the outcomes of two change projects presented in January 2019.
The initial projects related to care home and in-patient ward settings. A reduction in
inappropriate urine samples and an 81% reduction in treatment for UTI in the pilot care home were noted. In January 2019, the project was extended to a further 3 care homes, with support from the community dementia nurse. Other homes are also independently implementing aspects of the project to improve hydration in their residents and increase awareness of recognition and diagnosis of UTI. The hospital based project saw a 70% reduction in catheter associated UTI on a pilot ward, comparing a 3 month baseline period with October – December 2018. This project has now been extended to a second ward and once data collection is complete a cost benefit analysis will be undertaken prior to a decision on further rollout.
The quality of diagnosis and management of suspected UTIs continues to be a high priority for
the Trust, and is subjected to regular audit against NICE standards (Quality Standard 90). The latest audit was completed in 2018, and overall showed several areas of improvement compared to the previous audit. These overall results were presented to a general medical audience in July 2018 where areas requiring further improvement were also highlighted.
The Trust is also taking part in a trial regarding antibiotic prescription, the ARK (Antibiotic
Review Kit) trial. This trial addresses the issue of antibiotic stewardship, with the intention of promoting effective antibiotic prescription and the empowerment of clinicians to stop antibiotics when appropriate. While relevant to all antibiotic prescriptions, this is of direct relevance to those with suspected UTI. The results of this trial will inform changes in practice as they are identified.
4.8 Acute Kidney Injury
As part of another focused review of deaths where the patients had been recorded as being admitted with acute kidney injury (AKI, also referred to as acute renal failure); it was identified that the group of patients represent a population of frail, elderly patients with multiple significant co-morbidities including for many of them, chronic kidney disease. Analysis of the review findings identified that many of the patients may have had renal failure when they were admitted into the trust; this was treated appropriately and the patients later died as a result of one of their other long term co-morbidities or a secondary illness.
The Trust has undertaken a programme of quality improvement over the last 2-3 years in
relation to effectively identifying patients with AKI; which as a result has impacted on the overall management of this. A number of clinical audits undertaken over this time have shown key areas of improvement that have been supported by a statistical reduction in deaths of patients who were admitted with AKI. The quality improvement work in relation to AKI is to continue however this repeat focused case review has assisted in the positive evaluation of the work being undertaken across the Trust.
4.9 Clinical documentation and coding
The overall focus of all of the mortality reviews is to support the Trust in identifying areas where clinical practice or services can be changed to enhance the overall quality and safety of the care given to patients anywhere in the Trust and to also support patients, carers and staff when managing care when the overall outcome of their illness may be uncertain.
The Trust has in the past been reported as having increased Hospital Standardised Mortality
Rates (HSMR) and Standardised Hospital Mortality Indices. These are both nationally agreed

10
figures that use some areas of healthcare data (Charlson co-morbidities) to assist in benchmarking Trusts nationally. By examining ways of making improvements, in these nationally published measures, the Trust feels that it has not only improved quality and safety, but has also helped to allay some concerns patients, families and carers may have as a result of media coverage, during times of critical illness.
As a result of the mortality reviews it has been identified that records made may not fully reflect
all health problems (co-morbidities) an individual patient has or that the records may not clearly identify the diagnosis of the problems being treated. This impacts on communication of management plans between healthcare professionals providing care across primary and secondary areas, but can also impact on the healthcare data collected for national statistical analysis.
In order to improve the records made and to support clearer communication a number of
teaching sessions have been held with various clinical teams. The sessions are multi-disciplinary and raise awareness around the importance of accurately and comprehensively recording co-morbidities. They cover the mortality indicators and demonstrate the positive impact it has on trust HSMR and SHMI rates when the coding gives an accurate clinical picture of the patients who are treated in hospital.
The depth (number of codes for each patient) of coding of co-morbidities is monitored on a
monthly basis, with particular emphasis being placed on the depth of coding for Charlson co-morbidities. Following regional benchmarking it showed the Trust was falling behind in the recording of chronic kidney disease (CKD), metastatic cancer and hemiplegia. The Trust has implemented some remedial actions to resolve the issues identified and the impact of these will be monitored closely.
Following various internal focused reviews of groups of cases where there has been a clinical
diagnosis linked to senility, pneumonia or stroke; audits have been completed around to ensure all conditions documented within the case notes have been coded. Following the coding review clinician validation has been introduced to ensure all relevant co-morbidities and conditions have been documented. A recent analysis has shown the average Charlson co-morbidity score for pneumonia patients has increased from 12.2 to 13.3. For stroke patients the average Charlson co-morbidity score has increased from 10.1 to 14.5. Also any patient who dies in hospital, who has a primary diagnosis of delirium or dementia assigned, the coding will be sent to be validated by a clinician.
As a result of the ongoing work examining areas where quality and safety of care can be
enhanced; and also because of the improvements in clinical documentation and consequently the clinical coding; the Trusts HSMR and SHMI rates have been within the national “as expected” range for the last 12 consecutive quarters.
5. Conclusion/Summary 5.1 The Trusts HSMR value in the latest period has decreased to 96.17 (February 2018 to January
2019), the SHMI is currently 100.72 (October 2017 to September 2018). 5.2 There has been a sustained improvement in clinical documentation to support multidisciplinary
working but also to support the increased data the Trust are able code and subsequently provide for the national mortality statistics.
5.3 Of the compulsory case reviews identified in the Trusts policy 78% have been reviewed during
2018-19 to date; overall to date the Trust has reviewed 13% of all deaths. 5.4 During 2018-19 to date 16 cases have been identified as serious incidents, prior to case review.
Of these, 11 have been reviewed and none were identified as being avoidable (judged to be more likely than not, to have been due to problems in the care provided to the patient). There

11
are 5 further cases where the investigations are incomplete and updates will be provided in the next report. In all cases investigated as serious incidents Duty of Candour has been considered and applied appropriately.
5.5 Learning from the Trust Learning Disabilities mortality reviews is being shared regionally as part
of an overall collaborative approach. The multidisciplinary review enables shared learning across all care sectors involved in a patients care. There are some excellent examples of good quality supportive care being provided.
5.6 There is a significant amount of work ongoing in relation to the provision of end of life care; both
in the hospital and community areas. This will continue to support our staff providing consistently high quality end of life care but also to support patients and families in preparing for the end of life.
5.7 The Trust continues to focus on gathering information from patients and families about the care
provided; the Trust bereavement survey and Family Voice continue to provide a wealth of information that is being used to help improve our care; but also they continue to provide positive feedback to our staff.
5.8 The maternity team have over this last year embedded the use of the Perinatal Mortality review
tool. This is a nationally developed tool that supports the review of stillbirths to gain the maximum learning; the investigation tool also enhances family involvement.
5.9 The Trust is developing a business case to support the introduction of the Medical Examiners
role; this role is recommended from a recent national Coronial review. 5.10 There are areas where continued improvements are needed; these have been identified and
each has ongoing monitoring in place. The Trust Outcome, Performance, Delivery Operational Group and the Patient Safety and Quality Standards Committee seek further assurance in relation to these areas in line with their terms of reference. The group also proactively seeks to identify other areas in care and service provision where improvements may be required.
6. Recommendations 6.1 The Board of Directors are asked to note the content of this report and the information provided
in relation to the identification of trends to assist in learning lessons from the mortality reviews in order to maintain the reduction in the Trusts mortality rates.
6.2 The Board are asked to note the on-going work programme to maintain the mortality rates
within the expected range for the organisation. Dr D Dwarakanath Medical Director

12
Appendix 1
Pending
Review
Additional
ReviewsTotal Reviewed
Overall %
Reviewed
No. No. No. No. % No. % No. %
Apr 18 13 1 13 26 19% 0 0% 26 100%
May-18 18 0 2 20 19% 0 0% 20 100%
Jun-18 12 1 6 18 18% 0 0% 18 100%
Quarter 1 43 2 21 64 19% 0 0% 64 100%
Jul-18 14 2 8 22 19% 0 0% 22 100%
Aug-18 12 0 2 14 15% 0 0% 14 100%
Sep-18 15 1 0 15 14% 0 0% 15 100%
Quarter 2 41 3 10 51 16% 0 0% 51 100%
Oct-18 15 4 1 16 12% 0 0% 16 100%
Nov-18 10 3 7 17 13% 0 0% 17 100%
Dec-18 7 2 5 12 9% 0 0% 12 100%
Quarter 3 32 9 13 45 11% 0 0% 45 100%
Jan-19 6 6 9 15 10% 0 0% 15 100%
Feb-19 7 11 8 15 11% 0 0% 15 100%
Mar-19 4 7 0 4 4% 0 0% 2 100%
Quarter 4 17 24 17 34 9% 0 0% 32 100%
Totals 133 38 61 194 13% 0 0% 194 100%1462 171 78%
114 11 36%
397 41 41%
149 12 50%
134 18 39%
132 9 78%
406 41 78%
139 19 79%
135 13 77%
109 16 94%
317 44 93%
114 16 88%
94 12 100%
102 13 92%
342 45 96%
135 14 93%
105 18 100%
North Tees and Hartlepool NHS Foundation Trust Mortality Review Data 2018-19
Month of death Total No of deaths
Deaths meeting
inclusion criteria
Deaths reviewed meeting inclusion
criteria
Death judged as
avoidable (>50%
liklihood of avoidability)
Deaths reviewed judged as
not preventable
No. %