blue cross blue shield of georgia - h9947 cy 2013 medicare ... · tagalog: mayroon kaming libreng...
TRANSCRIPT

• How our members rate our plan's services and care;
• How well our doctors detect illnesses and keep members healthy;
• How well our plan helps our members use recommended and safe prescription medications
Plan too new to be measured
Image description. 5 stars End of image description.
Image description. 4 stars End of image description.
Image description. 3 stars End of image description.
Image description. 2 stars End of image description.
Image description. 1 star End of image description.
The number of stars shows how well our plan performs.
excellent above average average below average poor
Blue Cross Blue Shield of Georgia - H9947
CY 2013 Medicare Plan Ratings
The Medicare Program rates all health and prescription drug plans each year, based on a plan's quality andperformance. Medicare Plan Ratings help you know how good a job our plan is doing. You can use this Plan Ratingto compare our plan's performance to other plans. Examples of the areas covered by this rating include:
For 2013, Blue Cross Blue Shield of Georgia received the following overall Plan Rating from Medicare.
Learn more about our plan and how we are different from other plans at www.medicare.gov.
You may also contact us Sunday, Monday, Tuesday, Wednesday, Thursday, Friday, Saturday, 8:00 a.m. - 8:00p.m. Eastern at 800-797-1769 (toll-free) or 711 (TTY/TDD).
Current members please call 866-438-9968 (toll-free) or 711 (TTY/TDD).
Y0071_13_16160_U CMS Accepted 33587GASENBGA
Multi-language Interpreter Services
English: We have free interpreter services to answer any questions you may have about our health or drug plan. To get an interpreter, just call us at 1-866-438-9968. Someone who speaks English/ Language can help you. This is a free service.
Spanish: Tenemos servicios de intérprete sin costo alguno para responder cualquier pregunta que pueda tener sobre nuestro plan de salud o medicamentos. Para hablar con un intérprete, por favor llame al 1-866-438-9968. Alguien que hable español le podrá ayudar. Este es un servicio gratuito.
Chinese Mandarin: 我们提供免费的翻译服务,帮助您解答关于健康或药物保险的任何疑问。如果 您需要此翻译服务,请致电 1-866-438-9968。我们的中文工作人员很乐意帮助您。 这是一项免费服 务。
Chinese Cantonese: 您對我們的健康或藥物保險可能存有疑問,為此我們提供免費的翻譯服務。如 需翻譯服務,請致電1-866-438-9968。我們講中文的人員將樂意為您提供幫助。這是一項免費服務。
Tagalog: Mayroon kaming libreng serbisyo sa pagsasaling-wika upang masagot ang anumang mga katanungan ninyo hinggil sa aming planong pangkalusugan o panggamot. Upang makakuha ng tagasaling-wika, tawagan lamang kami sa 1-866-438-9968. Maaari kayong tulungan ng isang nakakapagsalita ng Tagalog. Ito ay libreng serbisyo.
French: Nous proposons des services gratuits d'interprétation pour répondre à toutes vos questions relatives à notre régime de santé ou d'assurance-médicaments. Pour accéder au service d'interprétation, il vous suffit de nous appeler au 1-866-438-9968. Un interlocuteur parlant Français pourra vous aider. Ce service est gratuit.
Vietnamese: Chúng tôi có dịch vụ thông dịch miễn phí để trả lời các câu hỏi về chương sức khỏe và chương trình thuốc men. Nếu quí vị cần thông dịch viên xin gọi 1-866-438-9968 sẽ có nhân viên nói tiếng Việt giúp đỡ quí vị. Đây là dịch vụ miễn phí.
German: Unser kostenloser Dolmetscherservice beantwortet Ihren Fragen zu unserem Gesundheits- und Arzneimittelplan. Unsere Dolmetscher erreichen Sie unter 1-866-438-9968. Man wird Ihnen dort auf Deutsch weiterhelfen. Dieser Service ist kostenlos.
Korean: 당사는 의료 보험 또는 약품 보험에 관한 질문에 답해 드리고자 무료 통역 서비스를 제공하 고 있습니다. 통역 서비스를 이용하려면 전화 1-866-438-9968 번으로 문의해 주십시오. 한국어를 하 는 담당자가 도와 드릴 것입니다. 이 서비스는 무료로 운영됩니다.
Russian: Если у вас возникнут вопросы относительно страхового или медикаментного плана, вы можете воспользоваться нашими бесплатными услугами переводчиков. Чтобы воспользоваться услугами переводчика, позвоните нам по телефону 1-866-438-9968. Вам окажет помощь сотрудник, который говорит по-pусски. Данная услуга бесплатная.
Arabic:إننا نقدم خدمات المترجم الفوري المجانية لإلجابة عن أي أسئلة تتعلق بالصحة أو جدول األدوية لدينا .
سيقوم شخص1-668-834-8699.للحصول على مترجم فوري، ليس عليك سوى االتصال بنا على. ما يتحدث العربية بمساعدتك. هذه خدمة مجانية
Hindi: हमार ेसवासथय या दवा की योजना क ेबार ेमे ंआपक ेिकसी भी पशन क ेजवाब देन ेक ेिलए हमार ेपास मुफत दुभािषया सेवाए ँउपलबध हैं. एक दुभाियषा परापत करन ेक ेिलए, बस हमे ं1-866-438-9968 पर फोन करें. कोई वयिकत जो िहनदी बोलता ह ैआपकी मदद कर सकता है. यह एक मुफत सेवा है.
Italian: È disponibile un servizio di interpretariato gratuito per rispondere a eventuali domande sul nostro piano sanitario e farmaceutico. Per un interprete, contattare il numero 1-866-438-9968. Un nostro incaricato che parla Italianovi fornirà l'assistenza necessaria. È un servizio gratuito.
Portugués: Dispomos de serviços de interpretação gratuitos para responder a qualquer questão que tenha acerca do nosso plano de saúde ou de medicação. Para obter um intérprete, contacte-nos através do número 1-866-438-9968. Irá encontrar alguém que fale o idioma Português para o ajudar. Este serviço é gratuito.
French Creole: Nou genyen sèvis entèprèt gratis pou reponn tout kesyon ou ta genyen konsènan plan medikal oswa dwòg nou an. Pou jwenn yon entèprèt, jis rele nou nan 1-866-438-9968. Yon moun ki pale Kreyòl kapab ede w. Sa a se yon sèvis ki gratis.
Polish: Umożliwiamy bezpłatne skorzystanie z usług tłumacza ustnego, który pomoże w uzyskaniu odpowiedzi na temat planu zdrowotnego lub dawkowania leków. Aby skorzystać z pomocy tłumacza znającego język polski, należy zadzwonić pod numer 1-866-438-9968. Ta usługa jest bezpłatna.
Japanese: 当社の健康 健康保険と薬品 処方薬プランに関するご質問にお答えするために、無料の 通訳サービスがありますございます。通訳をご用命になるには、1-866-438-9968 にお電話くださ い。日本語を話す人 者 が支援いたします。これは無料のサービスです。
Y0071_14_18283_U_012 CMS Accepted 30879MUSMLMUB_012
Summary of Benefitsfor Medicare Preferred Core (PPO)
Available in Bibb, DeKalb, Forsyth, Fulton, Harris, Jones, Liberty, Meriwether,Muscogee, Newton, Peach, Rockdale, Talbot, Toombs, and Twiggs Counties,GA
Blue Cross and Blue Shield of Georgia, Inc. is an LPPO plan with a Medicare contract. Enrollment inBlue Cross and Blue Shield of Georgia, Inc. depends on contract renewal. Blue Cross and Blue Shield ofGeorgia, Inc. is an independent licensee of the Blue Cross and Blue Shield Association. The Blue Crossand Blue Shield names and symbols are registered marks of the Blue Cross and Blue Shield Association.
Y0071_14_17593_U_053 CMS Accepted 10/01/2013 38887WPSENMUB_053H9947_001_GA_LPPO
Section I:
Introduction to Summary of BenefitsThank you for your interest in Medicare Preferred Core (PPO). Our plan is offered by Blue Cross Blue Shield ofGeorgia, Inc. which is also called Blue Cross Blue Shield of Georgia, a Medicare Advantage Preferred ProviderOrganization (PPO) that contracts with the Federal government. This Summary of Benefits tells you some featuresof our plan. It doesn't list every service that we cover or list every limitation or exclusion. To get a complete list of ourbenefits, please call Medicare Preferred Core (PPO) and ask for the "Evidence of Coverage."
You have choices in your health careAs a Medicare beneficiary, you can choose from differentMedicare options. One option is the Original(Fee-for-Service) Medicare Plan. Another option is aMedicare health plan, like Medicare Preferred Core(PPO). You may have other options too. You make thechoice. No matter what you decide, you are still in theMedicare Program.
You may be able to join or leave a plan only at certaintimes. Please call Medicare Preferred Core (PPO) at thenumber listed at the end of this introduction or1-800-MEDICARE (1-800-633-4227) for moreinformation. TTY/TDD users should call1-877-486-2048. You can call this number 24 hours aday, 7 days a week.
How can I compare my options?You can compare Medicare Preferred Core (PPO) andthe Original Medicare Plan using this Summary ofBenefits. The charts in this booklet list some importanthealth benefits. For each benefit, you can see what ourplan covers and what the Original Medicare Plan covers.
Our members receive all of the benefits that the OriginalMedicare Plan offers. We also offer more benefits, whichmay change from year to year.
Where is Medicare Preferred Core(PPO) available?The service area for this plan includes:
Bibb, DeKalb, Forsyth, Fulton, Harris, Jones, Liberty,Meriwether, Muscogee, Newton, Peach, Rockdale,Talbot, Toombs, Twiggs Counties, GA.
You must live in one of these areas to join the plan.
Who is eligible to join MedicarePreferred Core (PPO)?You can join Medicare Preferred Core (PPO) if you areentitled to Medicare Part A and enrolled in MedicarePart B and live in the service area. However, individualswith End-Stage Renal Disease generally are not eligibleto enroll in Medicare Preferred Core (PPO) unless theyare members of our organization and have been sincetheir dialysis began.
Can I choose my doctors?Medicare Preferred Core (PPO) has formed a networkof doctors, specialists, and hospitals. You can use anydoctor who is part of our network. You may also go todoctors outside of our network. The health providers inour network can change at any time.
You can ask for a current provider directory. For anupdated list, visit us athttp://www.bcbsga.com/medicare. Our customer servicenumber is listed at the end of this introduction.
What happens if I go to a doctor who'snot in your network?You can go to doctors, specialists, or hospitals in or outof network. You may have to pay more for the servicesyou receive outside the network, and you may have tofollow special rules prior to getting services in and/or outof network. For more information, please call thecustomer service number at the end of this introduction.
Page 2 – Medicare Preferred Core (PPO)
Where can I get my prescriptions if Ijoin this plan?Medicare Preferred Core (PPO) has formed a networkof pharmacies. You must use a network pharmacy toreceive plan benefits. We may not pay for yourprescriptions if you use an out-of-network pharmacy,except in certain cases. The pharmacies in our networkcan change at any time. You can ask for a pharmacydirectory or visit us athttp://www.bcbsga.com/medicare. Our customer servicenumber is listed at the end of this introduction.
Medicare Preferred Core (PPO) has a list of preferredpharmacies. At these pharmacies, you may get your drugsat a lower co-pay or co-insurance. You may go to anon-preferred pharmacy, but you may have to pay morefor your prescription drugs.
What if my doctor prescribes less thana month's supply?In consultation with your doctor or pharmacist, you mayreceive less than a month's supply of certain drugs. Also,if you live in a long-term care facility, you will receiveless than a month's supply of certain brand and genericdrugs. Dispensing fewer drugs at a time can help reducecost and waste in the Medicare Part D program, whenthis is medically appropriate.
The amount you pay in these circumstances will dependon whether you are responsible for paying coinsurance(a percentage of the cost of the drug) or a copay (a flatdollar amount for the drug). If you are responsible forcoinsurance for the drug, you will continue to pay theapplicable percentage of the drug cost. If you areresponsible for a copay for the drug, a "daily cost-sharingrate" will be applied. If your doctor decides to continuethe drug after a trial period, you should not pay more fora month's supply than you otherwise would have paid.Contact your plan if you have questions aboutcost-sharing when less than a one-month supply isdispensed.
Does my plan cover Medicare Part Bor Part D drugs?Medicare Preferred Core (PPO) does cover both MedicarePart B prescription drugs and Medicare Part Dprescription drugs.
What is a prescription drug formulary?Medicare Preferred Core (PPO) uses a formulary. Aformulary is a list of drugs covered by your plan to meetpatient needs. We may periodically add, remove, or makechanges to coverage limitations on certain drugs or changehow much you pay for a drug. If we make any formularychange that limits our members' ability to fill theirprescriptions, we will notify the affected members beforethe change is made. We will send a formulary to you andyou can see our complete formulary on our Web site athttp://www.bcbsga.com/medicare.
If you are currently taking a drug that is not on ourformulary or subject to additional requirements or limits,you may be able to get a temporary supply of the drug.You can contact us to request an exception or switch toan alternative drug listed on our formulary with yourphysician's help. Call us to see if you can get a temporarysupply of the drug or for more details about our drugtransition policy.
How can I get extra help with myprescription drug plan costs or getextra help with other Medicare costs?You may be able to get extra help to pay for yourprescription drug premiums and costs as well as get helpwith other Medicare costs. To see if you qualify forgetting extra help, call:
* 1-800-MEDICARE (1-800-633-4227). TTY/TDDusers should call 1-877-486-2048, 24 hours a day/7 daysa week; and see http://www.medicare.gov 'Programsfor People with Limited Income and Resources' in thepublication Medicare & You.
* The Social Security Administration at 1-800-772-1213between 7 a.m. and 7 p.m., Monday through Friday.TTY/TDD users should call 1-800-325-0778; or
* Your State Medicaid Office.
Page 3 – Medicare Preferred Core (PPO)

What are my protections in this plan?All Medicare Advantage Plans agree to stay in theprogram for a full calendar year at a time. Plan benefitsand cost-sharing may change from calendar year tocalendar year. Each year, plans can decide whether tocontinue to participate with Medicare Advantage. A planmay continue in their entire service area (geographic areawhere the plan accepts members) or choose to continueonly in certain areas. Also, Medicare may decide to enda contract with a plan. Even if your Medicare AdvantagePlan leaves the program, you will not lose Medicarecoverage. If a plan decides not to continue for anadditional calendar year, it must send you a letter at least90 days before your coverage will end. The letter willexplain your options for Medicare coverage in your area.
As a member of Medicare Preferred Core (PPO), youhave the right to request an organization determination,which includes the right to file an appeal if we denycoverage for an item or service, and the right to file agrievance. You have the right to request an organizationdetermination if you want us to provide or pay for anitem or service that you believe should be covered. If wedeny coverage for your requested item or service, youhave the right to appeal and ask us to review our decision.You may ask us for an expedited (fast) coveragedetermination or appeal if you believe that waiting for adecision could seriously put your life or health at risk, oraffect your ability to regain maximum function. If yourdoctor makes or supports the expedited request, we mustexpedite our decision. Finally, you have the right to filea grievance with us if you have any type of problem withus or one of our network providers that does not involvecoverage for an item or service. If your problem involvesquality of care, you also have the right to file a grievancewith the Quality Improvement Organization (QIO) foryour state. Please refer to the Evidence of Coverage(EOC) for the QIO contact information.
As a member of Medicare Preferred Core (PPO), youhave the right to request a coverage determination, whichincludes the right to request an exception, the right tofile an appeal if we deny coverage for a prescription drug,and the right to file a grievance. You have the right torequest a coverage determination if you want us to covera Part D drug that you believe should be covered. Anexception is a type of coverage determination. You mayask us for an exception if you believe you need a drug
that is not on our list of covered drugs or believe youshould get a non-preferred drug at a lower out-of-pocketcost. You can also ask for an exception to cost utilizationrules, such as a limit on the quantity of a drug. If youthink you need an exception, you should contact usbefore you try to fill your prescription at a pharmacy.Your doctor must provide a statement to support yourexception request. If we deny coverage for yourprescription drug(s), you have the right to appeal and askus to review our decision. Finally, you have the right tofile a grievance if you have any type of problem with usor one of our network pharmacies that does not involvecoverage for a prescription drug. If your problem involvesquality of care, you also have the right to file a grievancewith the Quality Improvement Organization (QIO) foryour state. Please refer to the Evidence of Coverage(EOC) for the QIO contact information.
What is a Medication TherapyManagement (MTM) Program?A Medication Therapy Management (MTM) Programis a free service we offer. You may be invited to participatein a program designed for your specific health andpharmacy needs. You may decide not to participate butit is recommended that you take full advantage of thiscovered service if you are selected. Contact MedicarePreferred Core (PPO) for more details.
What types of drugs may be coveredunder Medicare Part B?Some outpatient prescription drugs may be covered underMedicare Part B. These may include, but are not limitedto, the following types of drugs. Contact MedicarePreferred Core (PPO) for more details.
Some Antigens: If they are prepared by a doctor andadministered by a properly instructed person (whocould be the patient) under doctor supervision.Osteoporosis Drugs: Injectable osteoporosis drugs forsome women.Erythropoietin: By injection if you have end-stagerenal disease (permanent kidney failure requiringeither dialysis or transplantation) and need this drugto treat anemia.Hemophilia Clotting Factors: Self-administeredclotting factors if you have hemophilia.
Page 4 – Medicare Preferred Core (PPO)
Injectable Drugs: Most injectable drugs administeredincident to a physician's service.Immunosuppressive Drugs: Immunosuppressive drugtherapy for transplant patients if the transplant tookplace in a Medicare-certified facility and was paid forby Medicare or by a private insurance company thatwas the primary payer for Medicare Part A coverage.Some Oral Cancer Drugs: If the same drug is availablein injectable form.Oral Anti-Nausea Drugs: If you are part of ananti-cancer chemotherapeutic regimen.Inhalation and Infusion Drugs administered throughDurable Medical Equipment.
Where can I find information on planratings?The Medicare program rates how well plans perform indifferent categories (for example, detecting and preventingillness, ratings from patients and customer service). Ifyou have access to the web, you can find the Plan Ratingsinformation by using the “Find health & drug plans”web tool on http://www.medicare.gov to compare theplan ratings for Medicare plans in your area. You canalso call us directly to obtain a copy of the Plan Ratingsfor this plan. Our customer service number is listedbelow.
Please call Blue Cross Blue Shield of Georgia for more information aboutMedicare Preferred Core (PPO) Visit us at http://www.bcbsga.com/medicare or, call us:
Customer Service Hours for October 1 – February 14: Sunday, Monday, Tuesday,Wednesday, Thursday, Friday, Saturday, 8:00 a.m. - 8:00 p.m. Eastern Customer Service Hours for February 15 – September 30: Monday, Tuesday,Wednesday, Thursday, Friday, 8:00 a.m. - 8:00 p.m. Eastern Current members should call toll-free 1-866-438-9968 for questions related to theMedicare Advantage and Medicare Part D Prescription Drug Program. (TTY/TDD 711) Prospective members should call toll-free 1-800-797-1769 for questions related tothe Medicare Advantage and Medicare Part D Prescription Drug Program. (TTY/TDD711) Current members should call locally 1-866-438-9968 for questions related to theMedicare Advantage and Medicare Part D Prescription Drug Program. (TTY/TDD 711) Prospective members should call locally 1-800-797-1769 for questions related tothe Medicare Advantage and Medicare Part D Prescription Drug Program. (TTY/TDD711)
Page 5 – Medicare Preferred Core (PPO)
For more information about Medicare, please call Medicare at 1-800-MEDICARE(1-800-633-4227). TTY users should call 1-877-486-2048. You can call 24 hours aday, 7 days a week. Or, visit http://www.medicare.gov on the web.
This document may be available in other formats such as Braille, large print or otheralternate formats.
This document may be available in a non-English language. For additional information,call customer service at the phone number listed above.
Este documento podría estar disponible en otros formatos como Braille, textos conletras grandes u otros formatos. Este documento podría estar disponible en idiomas distintos del inglés. Comuníquesecon el número de nuestro Servicio de Atención al Cliente, indicado anteriormente,para obtener más información
Page 6 – Medicare Preferred Core (PPO)

Medicare Preferred Core (PPO)Original MedicareBenefit
IMPORTANT INFORMATION
General$35 monthly plan premium in addition toyour monthly Medicare Part B premium.
In 2013 the monthly Part B Premium was$104.90 and may change for 2014 and theannual Part B deductible amount was $147and may change for 2014.
1 Premium andOther ImportantInformation
Most people will pay the standard monthlyPart B premium in addition to their MA planIf a doctor or supplier does not accept
assignment, their costs are often higher, whichmeans you pay more.
premium. However, some people will payhigher Part B and Part D premiums becauseof their yearly income (over $85,000 forMost people will pay the standard monthly
Part B premium. However, some people will singles, $170,000 for married couples). Formore information about Part B and Part Dpay a higher premium because of their yearlypremiums based on income, call Medicare atincome (over $85,000 for singles, $170,0001-800-MEDICARE (1-800-633-4227). TTYfor married couples). For more informationusers should call 1-877-486-2048. You mayabout Part B premiums based on income, callalso call Social Security at 1-800-772-1213.TTY users should call 1-800-325-0778.
Medicare at 1-800-MEDICARE(1-800-633-4227). TTY users should call1-877-486-2048. You may also call Social Some physicians, providers and suppliers that
are out of a plan's network (i.e.,Security at 1-800-772-1213. TTY usersshould call 1-800-325-0778. out-of-network) accept "assignment" from
Medicare and will only charge up to aMedicare-approved amount. If you choose tosee an out-of-network physician who doesNOT accept Medicare "assignment," yourcoinsurance can be based on theMedicare-approved amount plus an additionalamount up to a higher Medicare "limitingcharge." If you are a member of a plan thatcharges a copay for out-of-network physicianservices, the higher Medicare "limiting charge"does not apply. See the publications Medicare& You or Your Medicare Benefits availableon http://www.medicare.gov for a full listingof benefits under Original Medicare, as wellas for explanations of the rules related to
If you have any questions about this plan's benefits or costs, please contactBlue Cross Blue Shield of Georgia for details
Section II:
Summary of Benefits
Page 7 – Medicare Preferred Core (PPO)
Medicare Preferred Core (PPO)Original MedicareBenefit
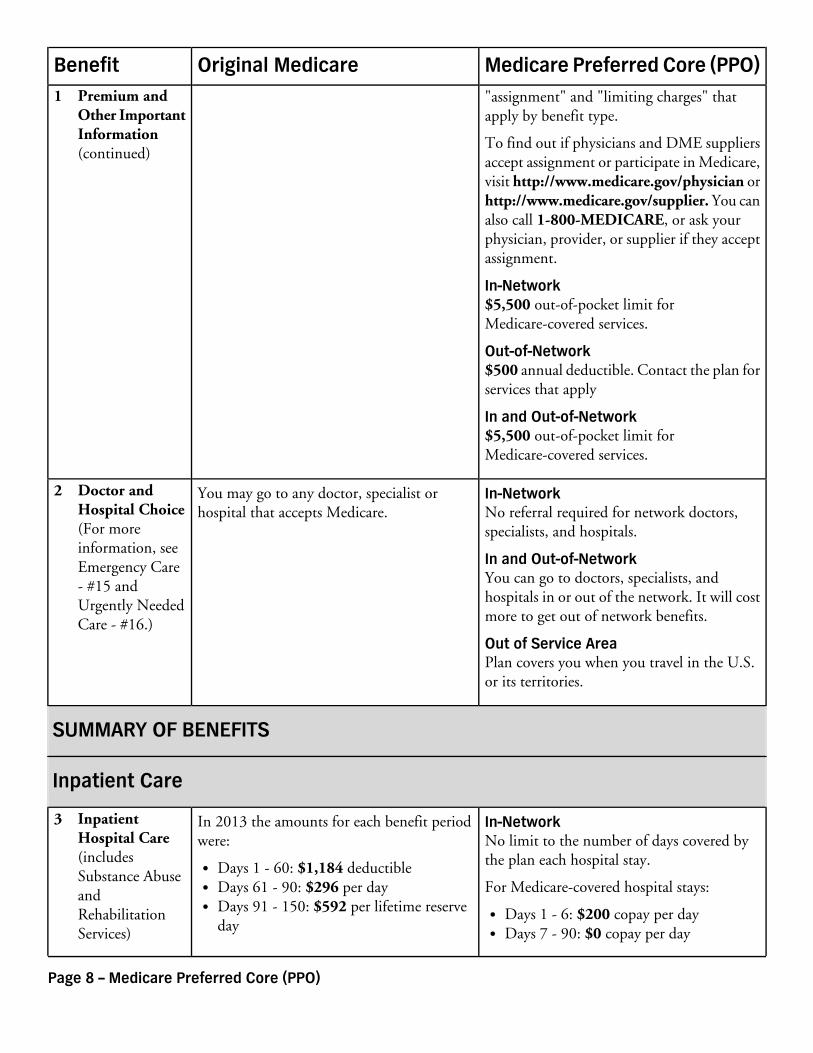
"assignment" and "limiting charges" thatapply by benefit type.
To find out if physicians and DME suppliersaccept assignment or participate in Medicare,visit http://www.medicare.gov/physician orhttp://www.medicare.gov/supplier. You canalso call 1-800-MEDICARE, or ask yourphysician, provider, or supplier if they acceptassignment.
In-Network$5,500 out-of-pocket limit forMedicare-covered services.
Out-of-Network$500 annual deductible. Contact the plan forservices that apply
In and Out-of-Network$5,500 out-of-pocket limit forMedicare-covered services.
In-NetworkNo referral required for network doctors,specialists, and hospitals.
You may go to any doctor, specialist orhospital that accepts Medicare.
2 Doctor andHospital Choice(For moreinformation, seeEmergency Care- #15 andUrgently NeededCare - #16.)
In and Out-of-NetworkYou can go to doctors, specialists, andhospitals in or out of the network. It will costmore to get out of network benefits.
Out of Service AreaPlan covers you when you travel in the U.S.or its territories.
SUMMARY OF BENEFITS
Inpatient Care
In-NetworkNo limit to the number of days covered bythe plan each hospital stay.
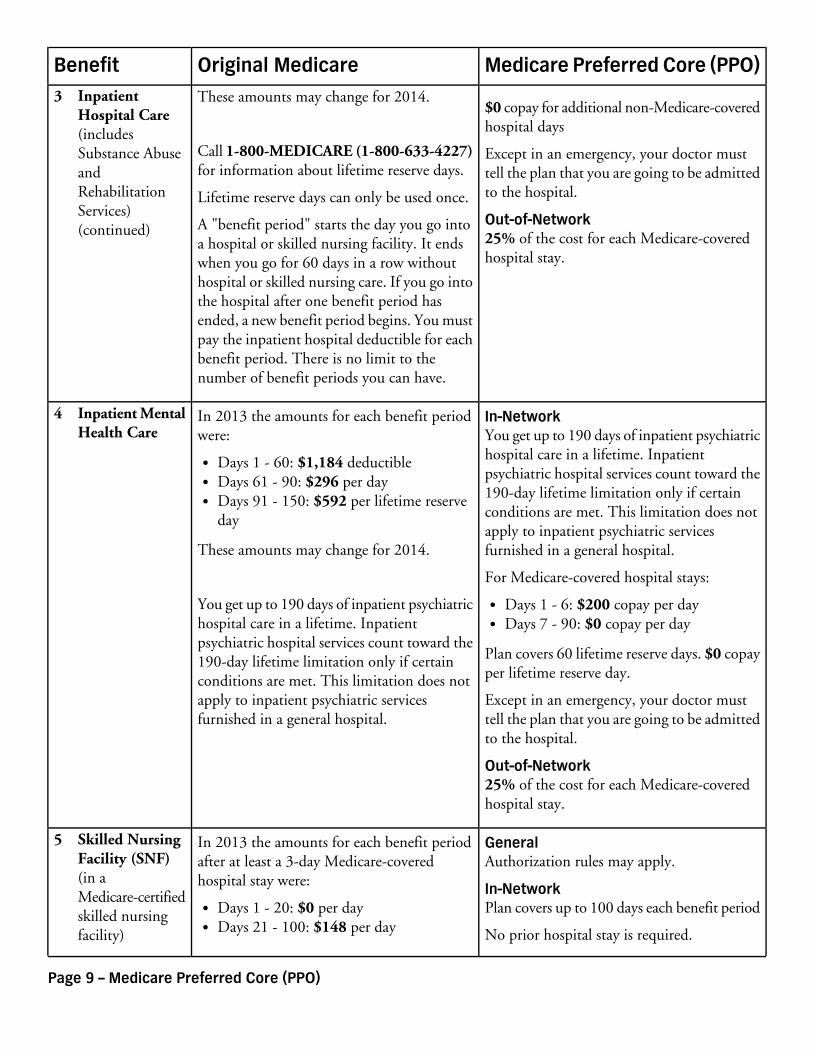
In 2013 the amounts for each benefit periodwere:
3 InpatientHospital Care(includesSubstance AbuseandRehabilitationServices)
Days 1 - 60: $1,184 deductibleFor Medicare-covered hospital stays:Days 61 - 90: $296 per day
Days 91 - 150: $592 per lifetime reserveday
Days 1 - 6: $200 copay per dayDays 7 - 90: $0 copay per day
1 Premium andOther ImportantInformation(continued)
Page 8 – Medicare Preferred Core (PPO)
Medicare Preferred Core (PPO)Original MedicareBenefit
These amounts may change for 2014.$0 copay for additional non-Medicare-coveredhospital days
Call 1-800-MEDICARE (1-800-633-4227)for information about lifetime reserve days.
Except in an emergency, your doctor musttell the plan that you are going to be admittedto the hospital.Lifetime reserve days can only be used once.Out-of-Network25% of the cost for each Medicare-coveredhospital stay.
A "benefit period" starts the day you go intoa hospital or skilled nursing facility. It endswhen you go for 60 days in a row withouthospital or skilled nursing care. If you go intothe hospital after one benefit period hasended, a new benefit period begins. You mustpay the inpatient hospital deductible for eachbenefit period. There is no limit to thenumber of benefit periods you can have.
In-NetworkYou get up to 190 days of inpatient psychiatrichospital care in a lifetime. Inpatient
In 2013 the amounts for each benefit periodwere:
4 Inpatient MentalHealth Care
Days 1 - 60: $1,184 deductiblepsychiatric hospital services count toward theDays 61 - 90: $296 per day190-day lifetime limitation only if certainDays 91 - 150: $592 per lifetime reserve
day conditions are met. This limitation does notapply to inpatient psychiatric servicesfurnished in a general hospital.These amounts may change for 2014.
For Medicare-covered hospital stays:
You get up to 190 days of inpatient psychiatrichospital care in a lifetime. Inpatient
Days 1 - 6: $200 copay per dayDays 7 - 90: $0 copay per day
psychiatric hospital services count toward thePlan covers 60 lifetime reserve days. $0 copayper lifetime reserve day.
190-day lifetime limitation only if certainconditions are met. This limitation does notapply to inpatient psychiatric servicesfurnished in a general hospital.
Except in an emergency, your doctor musttell the plan that you are going to be admittedto the hospital.
Out-of-Network25% of the cost for each Medicare-coveredhospital stay.
GeneralAuthorization rules may apply.
In 2013 the amounts for each benefit periodafter at least a 3-day Medicare-coveredhospital stay were:
5 Skilled NursingFacility (SNF)(in aMedicare-certifiedskilled nursingfacility)
In-NetworkPlan covers up to 100 days each benefit period
No prior hospital stay is required.
Days 1 - 20: $0 per dayDays 21 - 100: $148 per day
3 InpatientHospital Care(includesSubstance AbuseandRehabilitationServices)(continued)
Page 9 – Medicare Preferred Core (PPO)
Medicare Preferred Core (PPO)Original MedicareBenefit
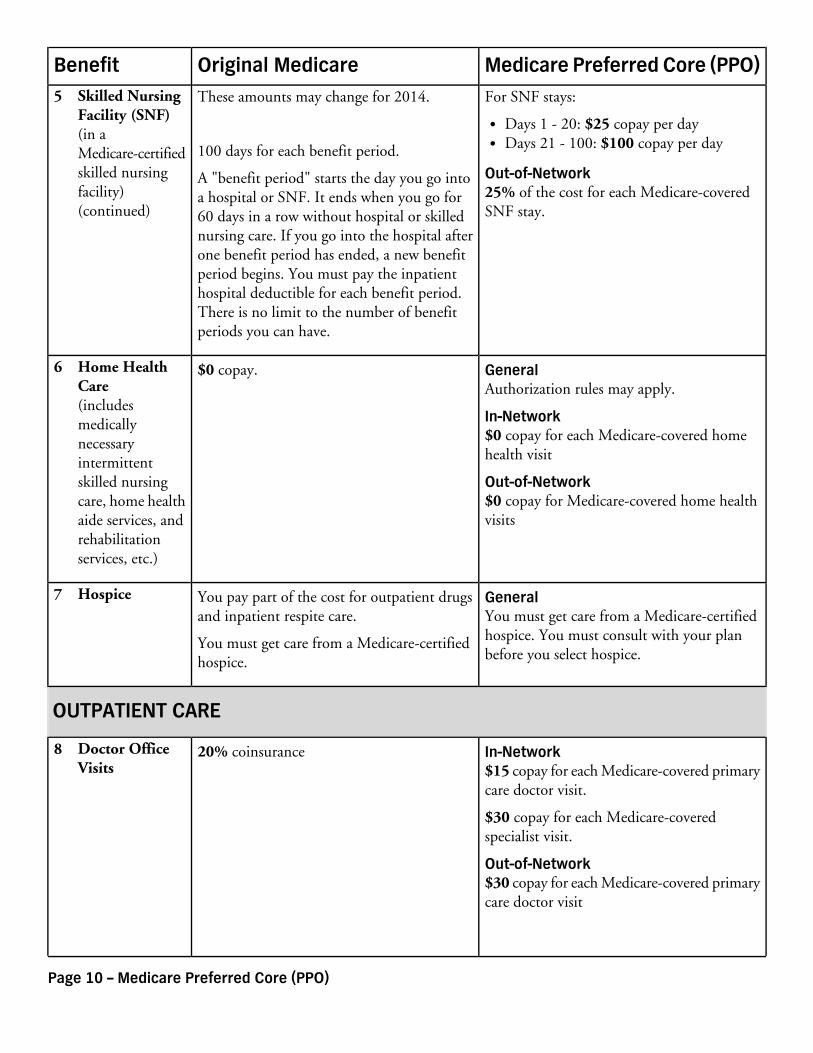
These amounts may change for 2014. For SNF stays:
Days 1 - 20: $25 copay per dayDays 21 - 100: $100 copay per day100 days for each benefit period.
Out-of-Network25% of the cost for each Medicare-coveredSNF stay.
A "benefit period" starts the day you go intoa hospital or SNF. It ends when you go for60 days in a row without hospital or skillednursing care. If you go into the hospital afterone benefit period has ended, a new benefitperiod begins. You must pay the inpatienthospital deductible for each benefit period.There is no limit to the number of benefitperiods you can have.
GeneralAuthorization rules may apply.
$0 copay.6 Home HealthCare(includesmedicallynecessaryintermittentskilled nursingcare, home healthaide services, andrehabilitationservices, etc.)
In-Network$0 copay for each Medicare-covered homehealth visit
Out-of-Network$0 copay for Medicare-covered home healthvisits
GeneralYou must get care from a Medicare-certifiedhospice. You must consult with your planbefore you select hospice.
You pay part of the cost for outpatient drugsand inpatient respite care.
You must get care from a Medicare-certifiedhospice.
7 Hospice
OUTPATIENT CARE
In-Network$15 copay for each Medicare-covered primarycare doctor visit.
20% coinsurance8 Doctor OfficeVisits
$30 copay for each Medicare-coveredspecialist visit.
Out-of-Network$30 copay for each Medicare-covered primarycare doctor visit
5 Skilled NursingFacility (SNF)(in aMedicare-certifiedskilled nursingfacility)(continued)
Page 10 – Medicare Preferred Core (PPO)
Medicare Preferred Core (PPO)Original MedicareBenefit
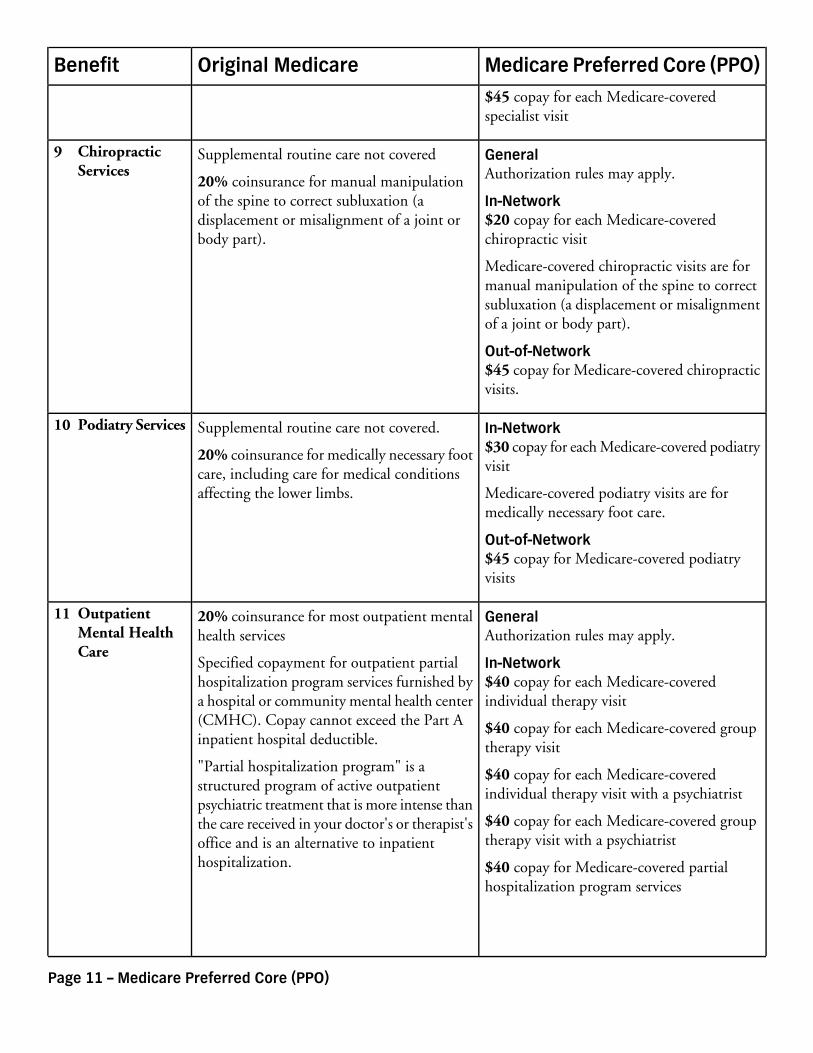
$45 copay for each Medicare-coveredspecialist visit
GeneralAuthorization rules may apply.
Supplemental routine care not covered
20% coinsurance for manual manipulationof the spine to correct subluxation (a
9 ChiropracticServices
In-Network$20 copay for each Medicare-coveredchiropractic visit
displacement or misalignment of a joint orbody part).
Medicare-covered chiropractic visits are formanual manipulation of the spine to correctsubluxation (a displacement or misalignmentof a joint or body part).
Out-of-Network$45 copay for Medicare-covered chiropracticvisits.
In-Network$30 copay for each Medicare-covered podiatryvisit
Supplemental routine care not covered.
20% coinsurance for medically necessary footcare, including care for medical conditionsaffecting the lower limbs.
10 Podiatry Services
Medicare-covered podiatry visits are formedically necessary foot care.
Out-of-Network$45 copay for Medicare-covered podiatryvisits
GeneralAuthorization rules may apply.
20% coinsurance for most outpatient mentalhealth services
11 OutpatientMental HealthCare
In-Network$40 copay for each Medicare-coveredindividual therapy visit
Specified copayment for outpatient partialhospitalization program services furnished bya hospital or community mental health center(CMHC). Copay cannot exceed the Part Ainpatient hospital deductible.
$40 copay for each Medicare-covered grouptherapy visit
"Partial hospitalization program" is astructured program of active outpatient
$40 copay for each Medicare-coveredindividual therapy visit with a psychiatrist
psychiatric treatment that is more intense than$40 copay for each Medicare-covered grouptherapy visit with a psychiatrist
the care received in your doctor's or therapist'soffice and is an alternative to inpatienthospitalization. $40 copay for Medicare-covered partial
hospitalization program services
Page 11 – Medicare Preferred Core (PPO)
Medicare Preferred Core (PPO)Original MedicareBenefit
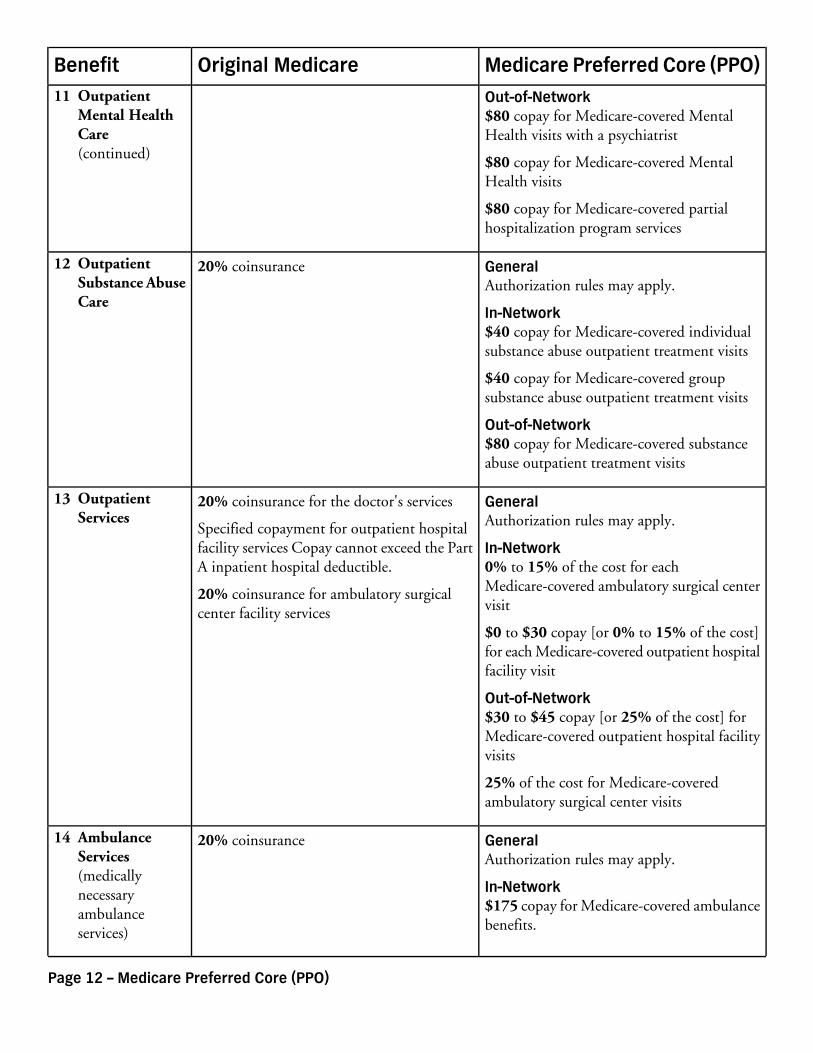
Out-of-Network$80 copay for Medicare-covered MentalHealth visits with a psychiatrist
$80 copay for Medicare-covered MentalHealth visits
$80 copay for Medicare-covered partialhospitalization program services
GeneralAuthorization rules may apply.
20% coinsurance12 OutpatientSubstance AbuseCare
In-Network$40 copay for Medicare-covered individualsubstance abuse outpatient treatment visits
$40 copay for Medicare-covered groupsubstance abuse outpatient treatment visits
Out-of-Network$80 copay for Medicare-covered substanceabuse outpatient treatment visits
GeneralAuthorization rules may apply.
20% coinsurance for the doctor's services
Specified copayment for outpatient hospitalfacility services Copay cannot exceed the PartA inpatient hospital deductible.
13 OutpatientServices
In-Network0% to 15% of the cost for eachMedicare-covered ambulatory surgical centervisit
20% coinsurance for ambulatory surgicalcenter facility services
$0 to $30 copay [or 0% to 15% of the cost]for each Medicare-covered outpatient hospitalfacility visit
Out-of-Network$30 to $45 copay [or 25% of the cost] forMedicare-covered outpatient hospital facilityvisits
25% of the cost for Medicare-coveredambulatory surgical center visits
GeneralAuthorization rules may apply.
20% coinsurance14 AmbulanceServices(medicallynecessaryambulanceservices)
In-Network$175 copay for Medicare-covered ambulancebenefits.
11 OutpatientMental HealthCare(continued)
Page 12 – Medicare Preferred Core (PPO)
Medicare Preferred Core (PPO)Original MedicareBenefit
Out-of-Network$175 copay for Medicare-covered ambulancebenefits.
General$65 copay for Medicare-covered emergencyroom visits
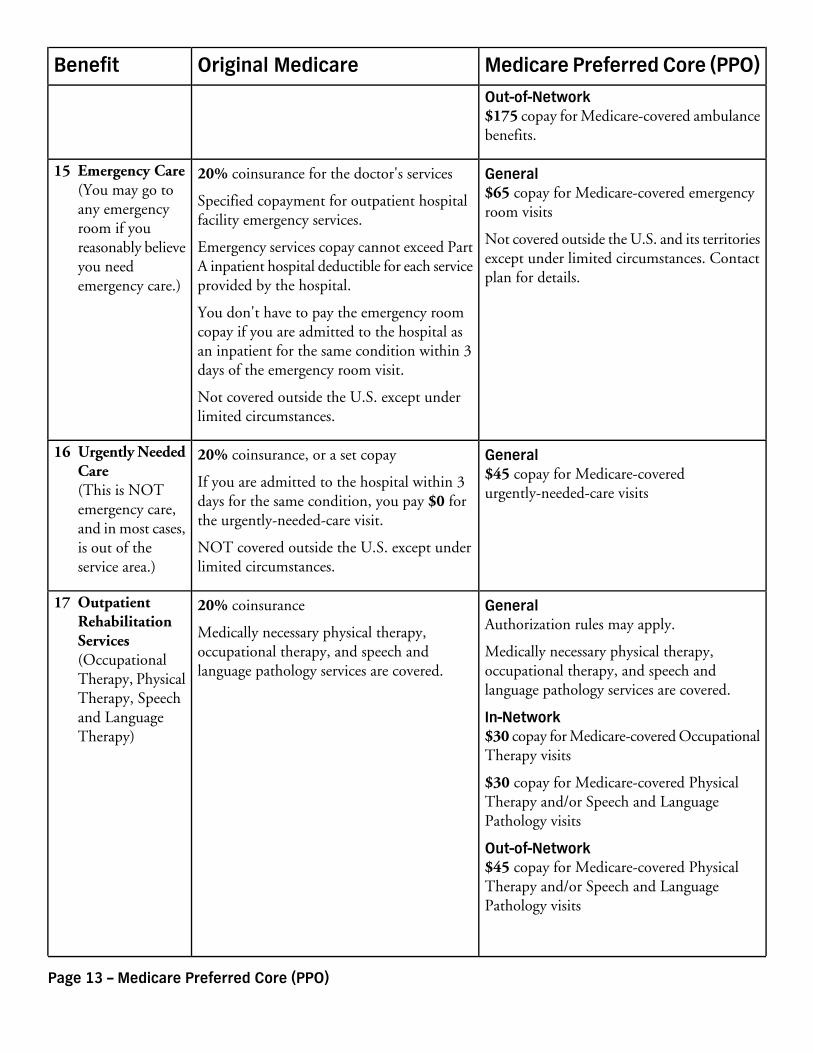
20% coinsurance for the doctor's services
Specified copayment for outpatient hospitalfacility emergency services.
15 Emergency Care(You may go toany emergencyroom if youreasonably believeyou needemergency care.)
Not covered outside the U.S. and its territoriesexcept under limited circumstances. Contactplan for details.
Emergency services copay cannot exceed PartA inpatient hospital deductible for each serviceprovided by the hospital.
You don't have to pay the emergency roomcopay if you are admitted to the hospital asan inpatient for the same condition within 3days of the emergency room visit.
Not covered outside the U.S. except underlimited circumstances.
General$45 copay for Medicare-coveredurgently-needed-care visits
20% coinsurance, or a set copay
If you are admitted to the hospital within 3days for the same condition, you pay $0 forthe urgently-needed-care visit.
16 Urgently NeededCare(This is NOTemergency care,and in most cases,is out of theservice area.)
NOT covered outside the U.S. except underlimited circumstances.
GeneralAuthorization rules may apply.
20% coinsurance
Medically necessary physical therapy,occupational therapy, and speech andlanguage pathology services are covered.
17 OutpatientRehabilitationServices(OccupationalTherapy, PhysicalTherapy, Speechand LanguageTherapy)
Medically necessary physical therapy,occupational therapy, and speech andlanguage pathology services are covered.
In-Network$30 copay for Medicare-covered OccupationalTherapy visits
$30 copay for Medicare-covered PhysicalTherapy and/or Speech and LanguagePathology visits
Out-of-Network$45 copay for Medicare-covered PhysicalTherapy and/or Speech and LanguagePathology visits
Page 13 – Medicare Preferred Core (PPO)
Medicare Preferred Core (PPO)Original MedicareBenefit
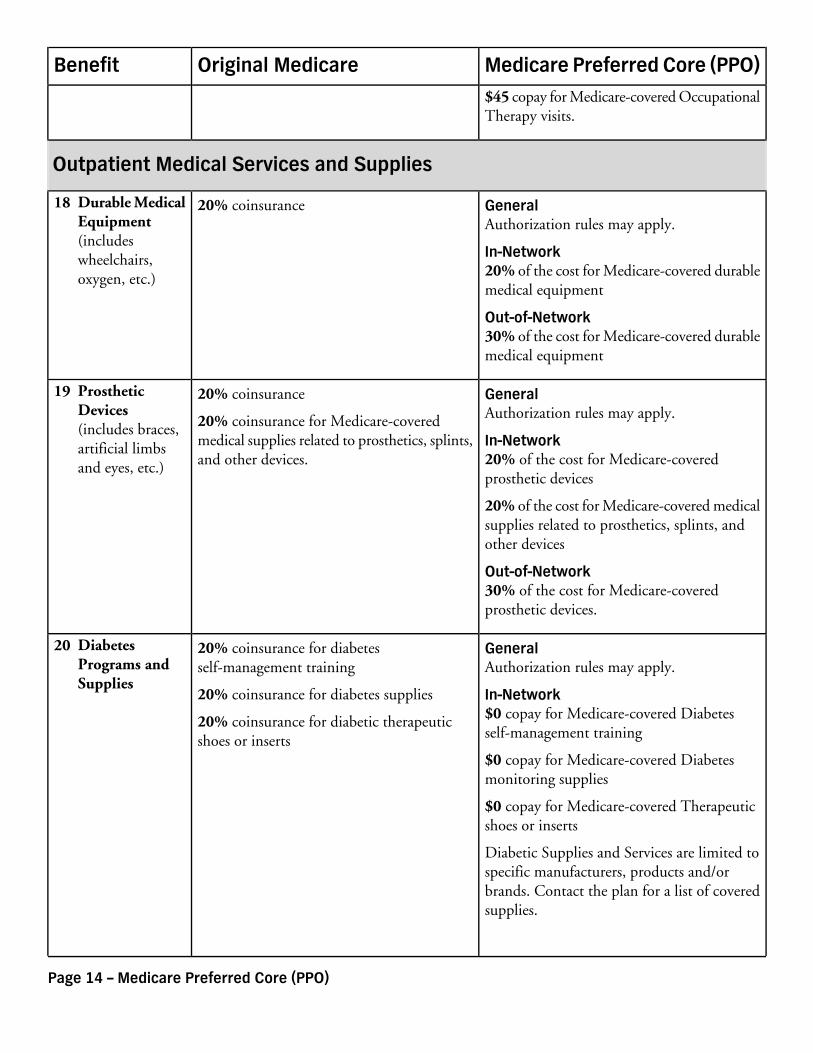
$45 copay for Medicare-covered OccupationalTherapy visits.
Outpatient Medical Services and Supplies
GeneralAuthorization rules may apply.
20% coinsurance18 Durable MedicalEquipment(includeswheelchairs,oxygen, etc.)
In-Network20% of the cost for Medicare-covered durablemedical equipment
Out-of-Network30% of the cost for Medicare-covered durablemedical equipment
GeneralAuthorization rules may apply.
20% coinsurance
20% coinsurance for Medicare-coveredmedical supplies related to prosthetics, splints,and other devices.
19 ProstheticDevices(includes braces,artificial limbsand eyes, etc.)
In-Network20% of the cost for Medicare-coveredprosthetic devices
20% of the cost for Medicare-covered medicalsupplies related to prosthetics, splints, andother devices
Out-of-Network30% of the cost for Medicare-coveredprosthetic devices.
GeneralAuthorization rules may apply.
20% coinsurance for diabetesself-management training
20 DiabetesPrograms andSupplies
In-Network$0 copay for Medicare-covered Diabetesself-management training
20% coinsurance for diabetes supplies
20% coinsurance for diabetic therapeuticshoes or inserts
$0 copay for Medicare-covered Diabetesmonitoring supplies
$0 copay for Medicare-covered Therapeuticshoes or inserts
Diabetic Supplies and Services are limited tospecific manufacturers, products and/orbrands. Contact the plan for a list of coveredsupplies.
Page 14 – Medicare Preferred Core (PPO)
Medicare Preferred Core (PPO)Original MedicareBenefit
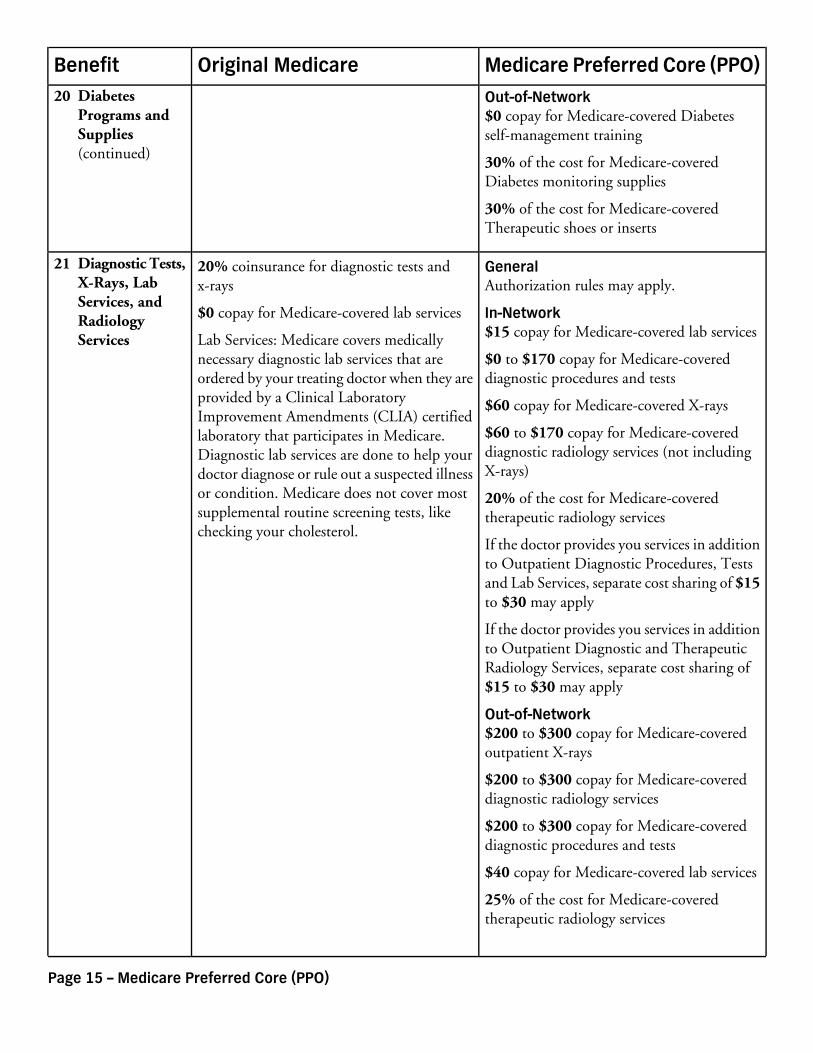
Out-of-Network$0 copay for Medicare-covered Diabetesself-management training
30% of the cost for Medicare-coveredDiabetes monitoring supplies
30% of the cost for Medicare-coveredTherapeutic shoes or inserts
GeneralAuthorization rules may apply.
20% coinsurance for diagnostic tests andx-rays
21 Diagnostic Tests,X-Rays, LabServices, andRadiologyServices
In-Network$15 copay for Medicare-covered lab services
$0 to $170 copay for Medicare-covereddiagnostic procedures and tests
$0 copay for Medicare-covered lab services
Lab Services: Medicare covers medicallynecessary diagnostic lab services that areordered by your treating doctor when they areprovided by a Clinical Laboratory $60 copay for Medicare-covered X-raysImprovement Amendments (CLIA) certified
$60 to $170 copay for Medicare-covereddiagnostic radiology services (not includingX-rays)
laboratory that participates in Medicare.Diagnostic lab services are done to help yourdoctor diagnose or rule out a suspected illnessor condition. Medicare does not cover most 20% of the cost for Medicare-covered
therapeutic radiology servicessupplemental routine screening tests, likechecking your cholesterol.
If the doctor provides you services in additionto Outpatient Diagnostic Procedures, Testsand Lab Services, separate cost sharing of $15to $30 may apply
If the doctor provides you services in additionto Outpatient Diagnostic and TherapeuticRadiology Services, separate cost sharing of$15 to $30 may apply
Out-of-Network$200 to $300 copay for Medicare-coveredoutpatient X-rays
$200 to $300 copay for Medicare-covereddiagnostic radiology services
$200 to $300 copay for Medicare-covereddiagnostic procedures and tests
$40 copay for Medicare-covered lab services
25% of the cost for Medicare-coveredtherapeutic radiology services
20 DiabetesPrograms andSupplies(continued)
Page 15 – Medicare Preferred Core (PPO)
Medicare Preferred Core (PPO)Original MedicareBenefit
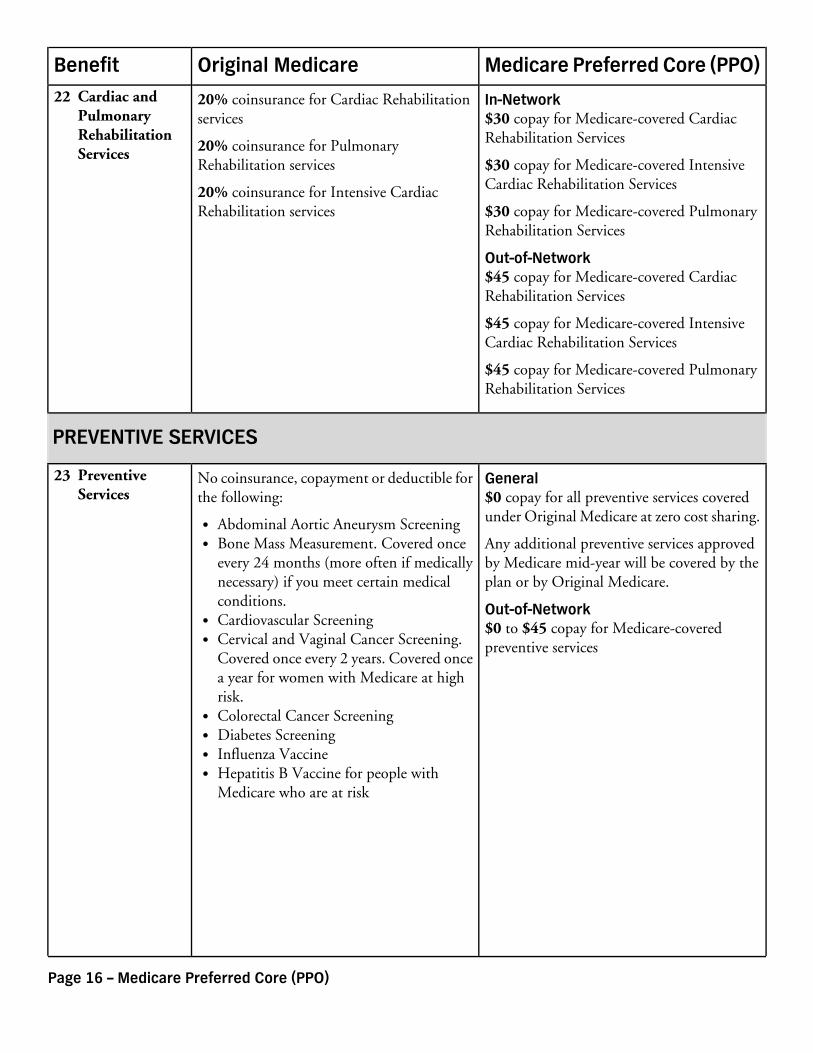
In-Network$30 copay for Medicare-covered CardiacRehabilitation Services
20% coinsurance for Cardiac Rehabilitationservices
20% coinsurance for PulmonaryRehabilitation services
22 Cardiac andPulmonaryRehabilitationServices
$30 copay for Medicare-covered IntensiveCardiac Rehabilitation Services20% coinsurance for Intensive Cardiac
Rehabilitation services $30 copay for Medicare-covered PulmonaryRehabilitation Services
Out-of-Network$45 copay for Medicare-covered CardiacRehabilitation Services
$45 copay for Medicare-covered IntensiveCardiac Rehabilitation Services
$45 copay for Medicare-covered PulmonaryRehabilitation Services
PREVENTIVE SERVICES
General$0 copay for all preventive services coveredunder Original Medicare at zero cost sharing.
No coinsurance, copayment or deductible forthe following:
23 PreventiveServices
Abdominal Aortic Aneurysm ScreeningAny additional preventive services approvedby Medicare mid-year will be covered by theplan or by Original Medicare.
Bone Mass Measurement. Covered onceevery 24 months (more often if medicallynecessary) if you meet certain medicalconditions. Out-of-Network
$0 to $45 copay for Medicare-coveredpreventive services
Cardiovascular ScreeningCervical and Vaginal Cancer Screening.Covered once every 2 years. Covered oncea year for women with Medicare at highrisk.Colorectal Cancer ScreeningDiabetes ScreeningInfluenza VaccineHepatitis B Vaccine for people withMedicare who are at risk
Page 16 – Medicare Preferred Core (PPO)
Medicare Preferred Core (PPO)Original MedicareBenefit
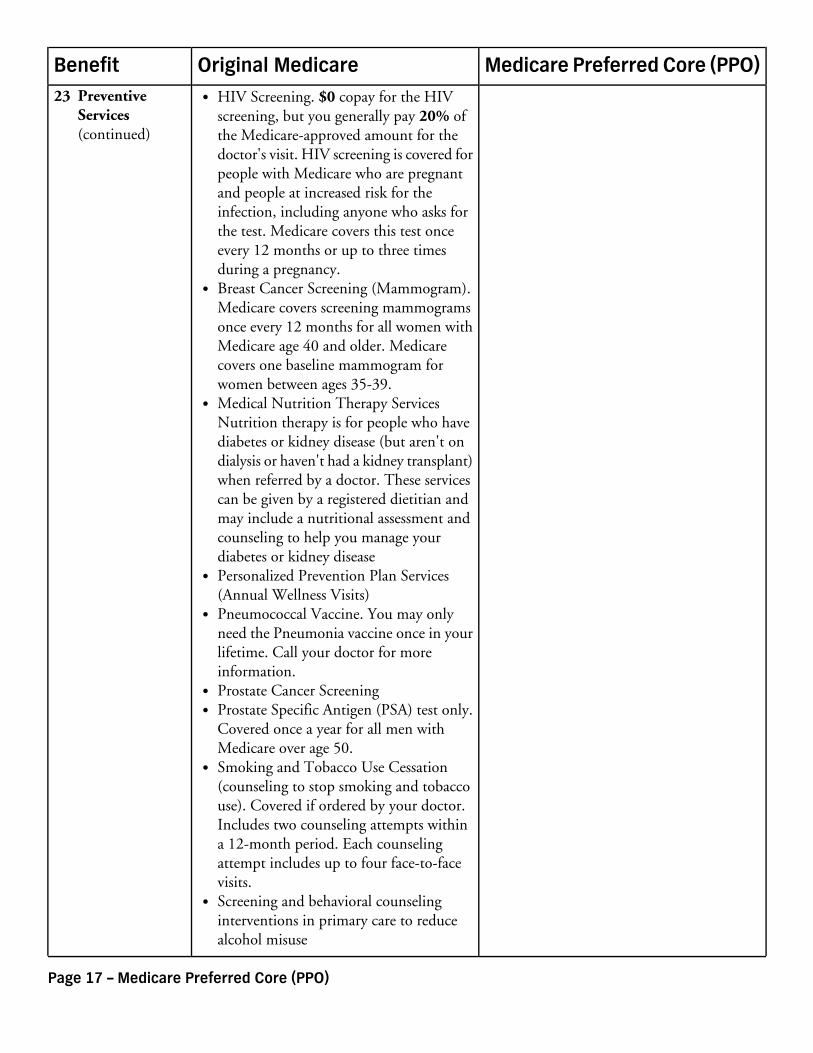
HIV Screening. $0 copay for the HIVscreening, but you generally pay 20% ofthe Medicare-approved amount for thedoctor's visit. HIV screening is covered forpeople with Medicare who are pregnantand people at increased risk for theinfection, including anyone who asks forthe test. Medicare covers this test onceevery 12 months or up to three timesduring a pregnancy.Breast Cancer Screening (Mammogram).Medicare covers screening mammogramsonce every 12 months for all women withMedicare age 40 and older. Medicarecovers one baseline mammogram forwomen between ages 35-39.Medical Nutrition Therapy ServicesNutrition therapy is for people who havediabetes or kidney disease (but aren't ondialysis or haven't had a kidney transplant)when referred by a doctor. These servicescan be given by a registered dietitian andmay include a nutritional assessment andcounseling to help you manage yourdiabetes or kidney diseasePersonalized Prevention Plan Services(Annual Wellness Visits)Pneumococcal Vaccine. You may onlyneed the Pneumonia vaccine once in yourlifetime. Call your doctor for moreinformation.Prostate Cancer ScreeningProstate Specific Antigen (PSA) test only.Covered once a year for all men withMedicare over age 50.Smoking and Tobacco Use Cessation(counseling to stop smoking and tobaccouse). Covered if ordered by your doctor.Includes two counseling attempts withina 12-month period. Each counselingattempt includes up to four face-to-facevisits.Screening and behavioral counselinginterventions in primary care to reducealcohol misuse
23 PreventiveServices(continued)
Page 17 – Medicare Preferred Core (PPO)
Medicare Preferred Core (PPO)Original MedicareBenefit
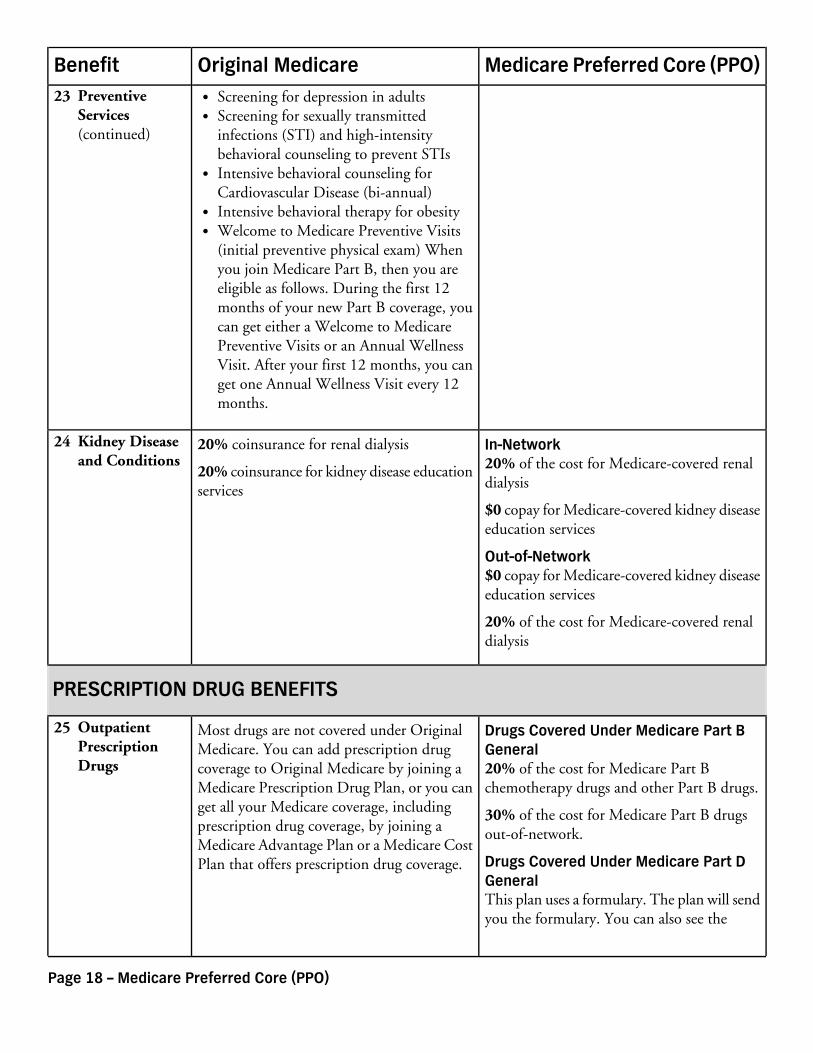
Screening for depression in adultsScreening for sexually transmittedinfections (STI) and high-intensitybehavioral counseling to prevent STIsIntensive behavioral counseling forCardiovascular Disease (bi-annual)Intensive behavioral therapy for obesityWelcome to Medicare Preventive Visits(initial preventive physical exam) Whenyou join Medicare Part B, then you areeligible as follows. During the first 12months of your new Part B coverage, youcan get either a Welcome to MedicarePreventive Visits or an Annual WellnessVisit. After your first 12 months, you canget one Annual Wellness Visit every 12months.
In-Network20% of the cost for Medicare-covered renaldialysis
20% coinsurance for renal dialysis
20% coinsurance for kidney disease educationservices
24 Kidney Diseaseand Conditions
$0 copay for Medicare-covered kidney diseaseeducation services
Out-of-Network$0 copay for Medicare-covered kidney diseaseeducation services
20% of the cost for Medicare-covered renaldialysis
PRESCRIPTION DRUG BENEFITS
Drugs Covered Under Medicare Part BGeneral20% of the cost for Medicare Part Bchemotherapy drugs and other Part B drugs.
Most drugs are not covered under OriginalMedicare. You can add prescription drugcoverage to Original Medicare by joining aMedicare Prescription Drug Plan, or you canget all your Medicare coverage, including
25 OutpatientPrescriptionDrugs
30% of the cost for Medicare Part B drugsout-of-network.prescription drug coverage, by joining a
Medicare Advantage Plan or a Medicare CostPlan that offers prescription drug coverage. Drugs Covered Under Medicare Part D
GeneralThis plan uses a formulary. The plan will sendyou the formulary. You can also see the
23 PreventiveServices(continued)
Page 18 – Medicare Preferred Core (PPO)

Medicare Preferred Core (PPO)Original MedicareBenefit
formulary at http://www.bcbsga.com/medicare on the web.
Different out-of-pocket costs may apply forpeople who
have limited incomes,live in long term care facilities, orhave access to Indian/Tribal/Urban (IndianHealth Service) providers.
The plan offers national in-networkprescription coverage (i.e., this would include50 states and the District of Columbia). Thismeans that you will pay the same cost-sharingamount for your prescription drugs if you getthem at an in-network pharmacy outside ofthe plan's service area (for instance when youtravel).
Total yearly drug costs are the total drug costspaid by both you and a Part D plan.
The plan may require you to first try one drugto treat your condition before it will coveranother drug for that condition.
Some drugs have quantity limits.
Your provider must get prior authorizationfrom Medicare Preferred Core (PPO) forcertain drugs.
You must go to certain pharmacies for a verylimited number of drugs, due to specialhandling, provider coordination, or patienteducation requirements that cannot be metby most pharmacies in your network. Thesedrugs are listed on the plan's website,formulary, printed materials, as well as on theMedicare Prescription Drug Plan Finder onMedicare.gov.
If the actual cost of a drug is less than thenormal cost-sharing amount for that drug,you will pay the actual cost, not the highercost-sharing amount.
If you request a formulary exception for a drugand Medicare Preferred Core (PPO) approves
25 OutpatientPrescriptionDrugs(continued)
Page 19 – Medicare Preferred Core (PPO)
Medicare Preferred Core (PPO)Original MedicareBenefit
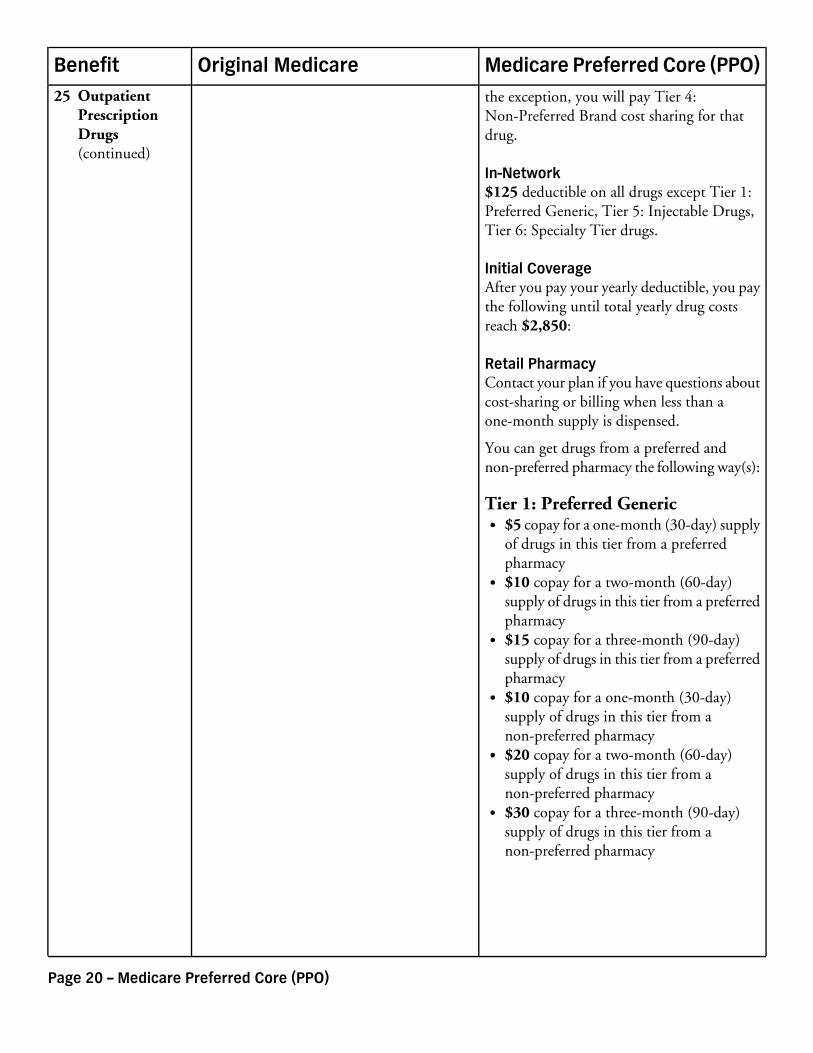
the exception, you will pay Tier 4:Non-Preferred Brand cost sharing for thatdrug.
In-Network$125 deductible on all drugs except Tier 1:Preferred Generic, Tier 5: Injectable Drugs,Tier 6: Specialty Tier drugs.
Initial CoverageAfter you pay your yearly deductible, you paythe following until total yearly drug costsreach $2,850:
Retail PharmacyContact your plan if you have questions aboutcost-sharing or billing when less than aone-month supply is dispensed.
You can get drugs from a preferred andnon-preferred pharmacy the following way(s):
Tier 1: Preferred Generic$5 copay for a one-month (30-day) supplyof drugs in this tier from a preferredpharmacy$10 copay for a two-month (60-day)supply of drugs in this tier from a preferredpharmacy$15 copay for a three-month (90-day)supply of drugs in this tier from a preferredpharmacy$10 copay for a one-month (30-day)supply of drugs in this tier from anon-preferred pharmacy$20 copay for a two-month (60-day)supply of drugs in this tier from anon-preferred pharmacy$30 copay for a three-month (90-day)supply of drugs in this tier from anon-preferred pharmacy
25 OutpatientPrescriptionDrugs(continued)
Page 20 – Medicare Preferred Core (PPO)
Medicare Preferred Core (PPO)Original MedicareBenefit
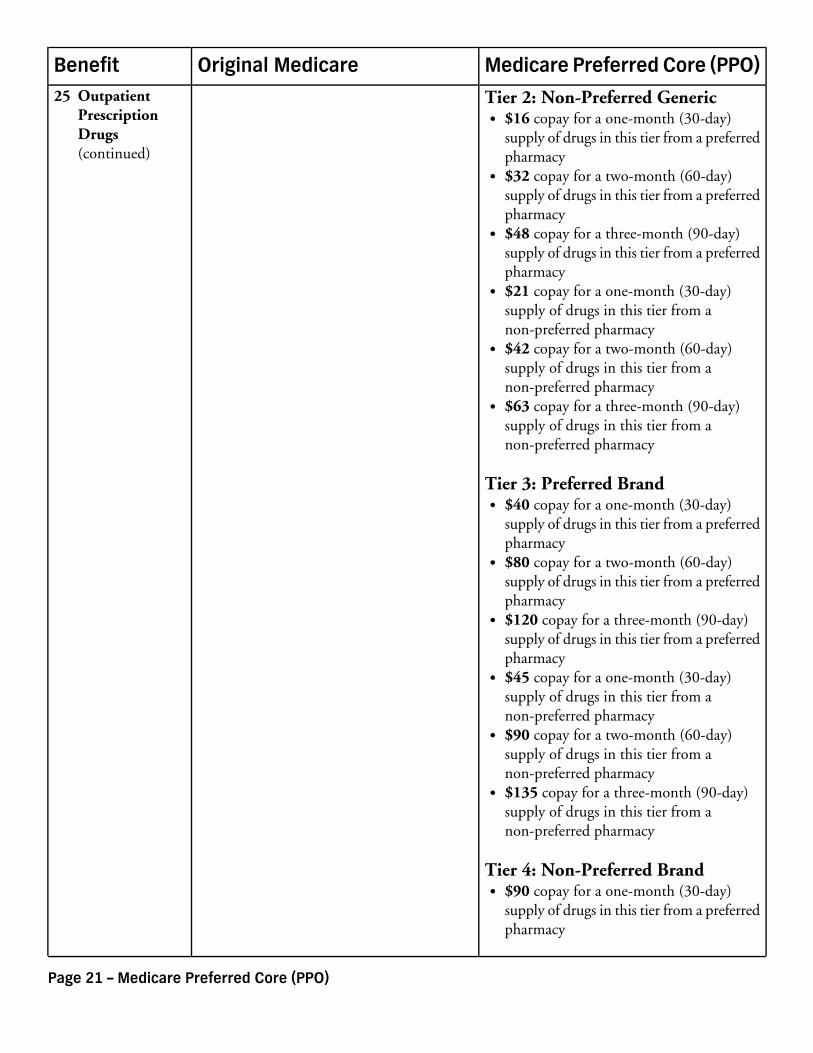
Tier 2: Non-Preferred Generic$16 copay for a one-month (30-day)supply of drugs in this tier from a preferredpharmacy$32 copay for a two-month (60-day)supply of drugs in this tier from a preferredpharmacy$48 copay for a three-month (90-day)supply of drugs in this tier from a preferredpharmacy$21 copay for a one-month (30-day)supply of drugs in this tier from anon-preferred pharmacy$42 copay for a two-month (60-day)supply of drugs in this tier from anon-preferred pharmacy$63 copay for a three-month (90-day)supply of drugs in this tier from anon-preferred pharmacy
Tier 3: Preferred Brand$40 copay for a one-month (30-day)supply of drugs in this tier from a preferredpharmacy$80 copay for a two-month (60-day)supply of drugs in this tier from a preferredpharmacy$120 copay for a three-month (90-day)supply of drugs in this tier from a preferredpharmacy$45 copay for a one-month (30-day)supply of drugs in this tier from anon-preferred pharmacy$90 copay for a two-month (60-day)supply of drugs in this tier from anon-preferred pharmacy$135 copay for a three-month (90-day)supply of drugs in this tier from anon-preferred pharmacy
Tier 4: Non-Preferred Brand$90 copay for a one-month (30-day)supply of drugs in this tier from a preferredpharmacy
25 OutpatientPrescriptionDrugs(continued)
Page 21 – Medicare Preferred Core (PPO)
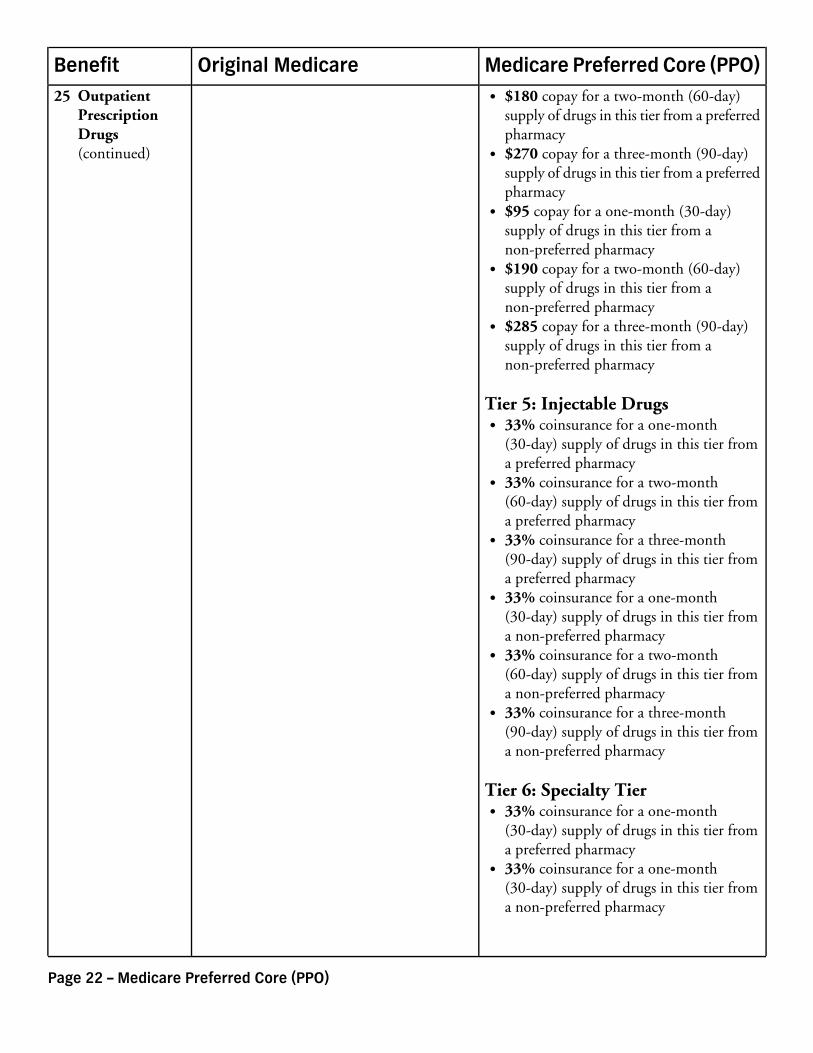
Medicare Preferred Core (PPO)Original MedicareBenefit$180 copay for a two-month (60-day)supply of drugs in this tier from a preferredpharmacy$270 copay for a three-month (90-day)supply of drugs in this tier from a preferredpharmacy$95 copay for a one-month (30-day)supply of drugs in this tier from anon-preferred pharmacy$190 copay for a two-month (60-day)supply of drugs in this tier from anon-preferred pharmacy$285 copay for a three-month (90-day)supply of drugs in this tier from anon-preferred pharmacy
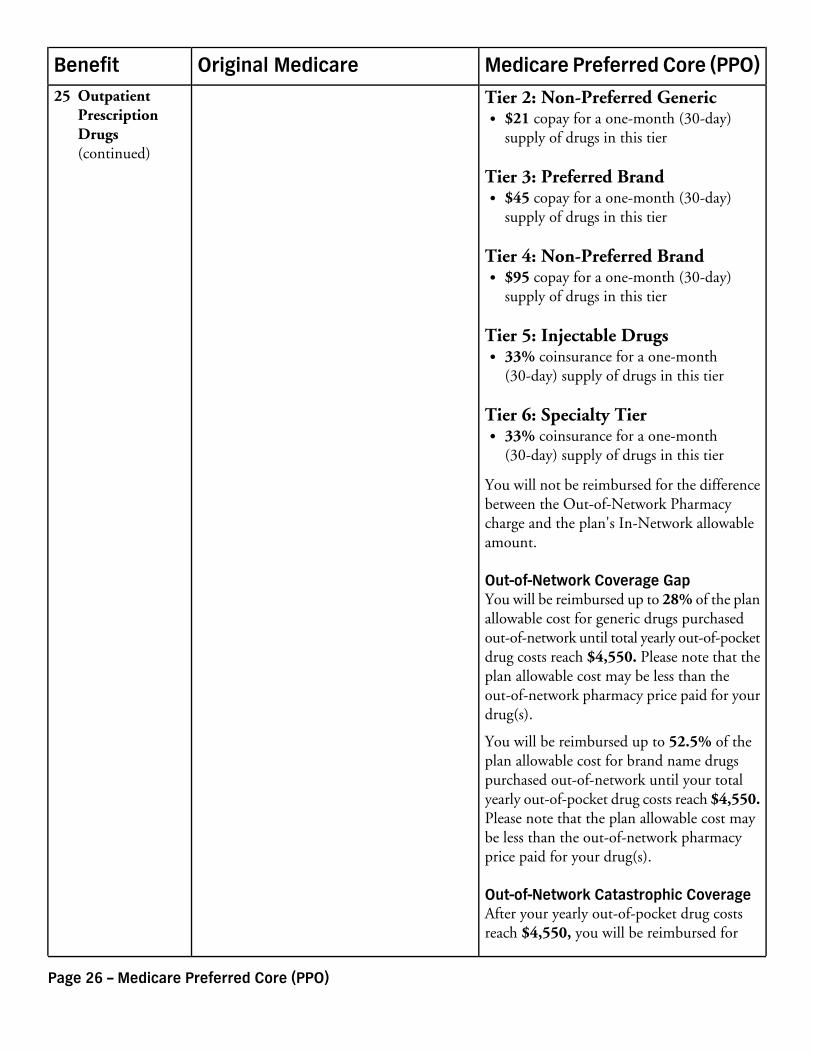
Tier 5: Injectable Drugs33% coinsurance for a one-month(30-day) supply of drugs in this tier froma preferred pharmacy33% coinsurance for a two-month(60-day) supply of drugs in this tier froma preferred pharmacy33% coinsurance for a three-month(90-day) supply of drugs in this tier froma preferred pharmacy33% coinsurance for a one-month(30-day) supply of drugs in this tier froma non-preferred pharmacy33% coinsurance for a two-month(60-day) supply of drugs in this tier froma non-preferred pharmacy33% coinsurance for a three-month(90-day) supply of drugs in this tier froma non-preferred pharmacy
Tier 6: Specialty Tier33% coinsurance for a one-month(30-day) supply of drugs in this tier froma preferred pharmacy33% coinsurance for a one-month(30-day) supply of drugs in this tier froma non-preferred pharmacy
25 OutpatientPrescriptionDrugs(continued)
Page 22 – Medicare Preferred Core (PPO)
Medicare Preferred Core (PPO)Original MedicareBenefit
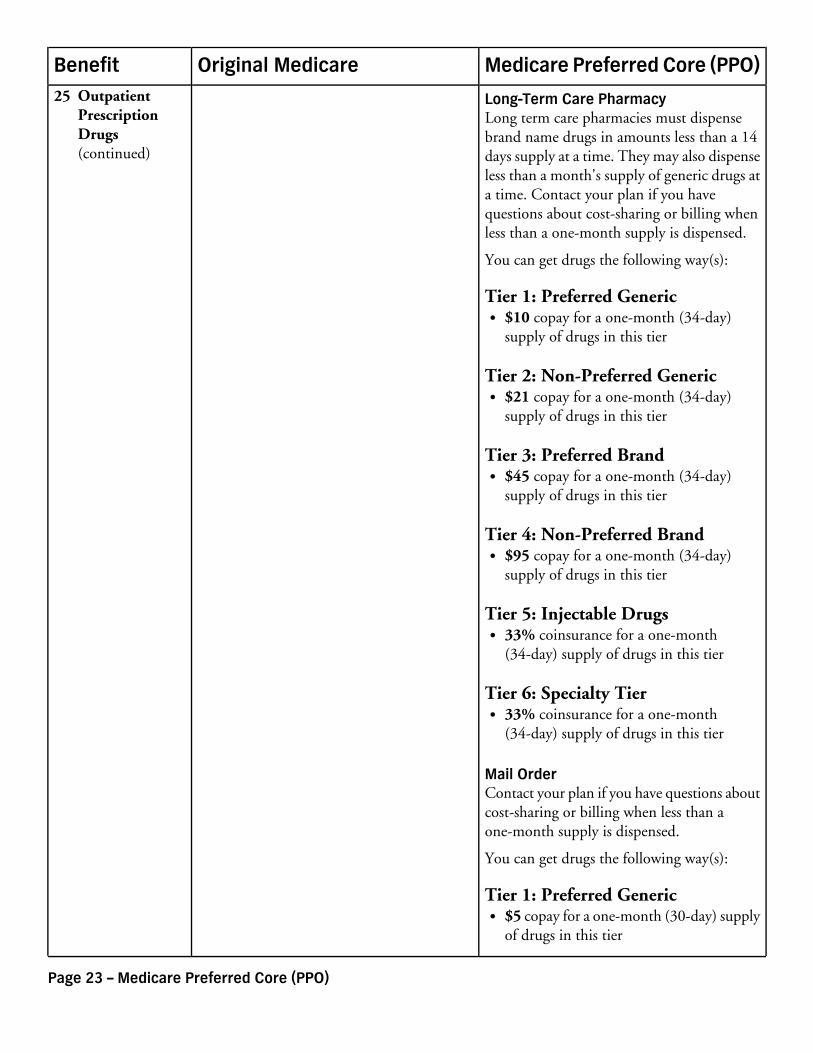
Long-Term Care PharmacyLong term care pharmacies must dispensebrand name drugs in amounts less than a 14days supply at a time. They may also dispenseless than a month's supply of generic drugs ata time. Contact your plan if you havequestions about cost-sharing or billing whenless than a one-month supply is dispensed.
You can get drugs the following way(s):
Tier 1: Preferred Generic$10 copay for a one-month (34-day)supply of drugs in this tier
Tier 2: Non-Preferred Generic$21 copay for a one-month (34-day)supply of drugs in this tier
Tier 3: Preferred Brand$45 copay for a one-month (34-day)supply of drugs in this tier
Tier 4: Non-Preferred Brand$95 copay for a one-month (34-day)supply of drugs in this tier
Tier 5: Injectable Drugs33% coinsurance for a one-month(34-day) supply of drugs in this tier
Tier 6: Specialty Tier33% coinsurance for a one-month(34-day) supply of drugs in this tier
Mail OrderContact your plan if you have questions aboutcost-sharing or billing when less than aone-month supply is dispensed.
You can get drugs the following way(s):
Tier 1: Preferred Generic$5 copay for a one-month (30-day) supplyof drugs in this tier
25 OutpatientPrescriptionDrugs(continued)
Page 23 – Medicare Preferred Core (PPO)
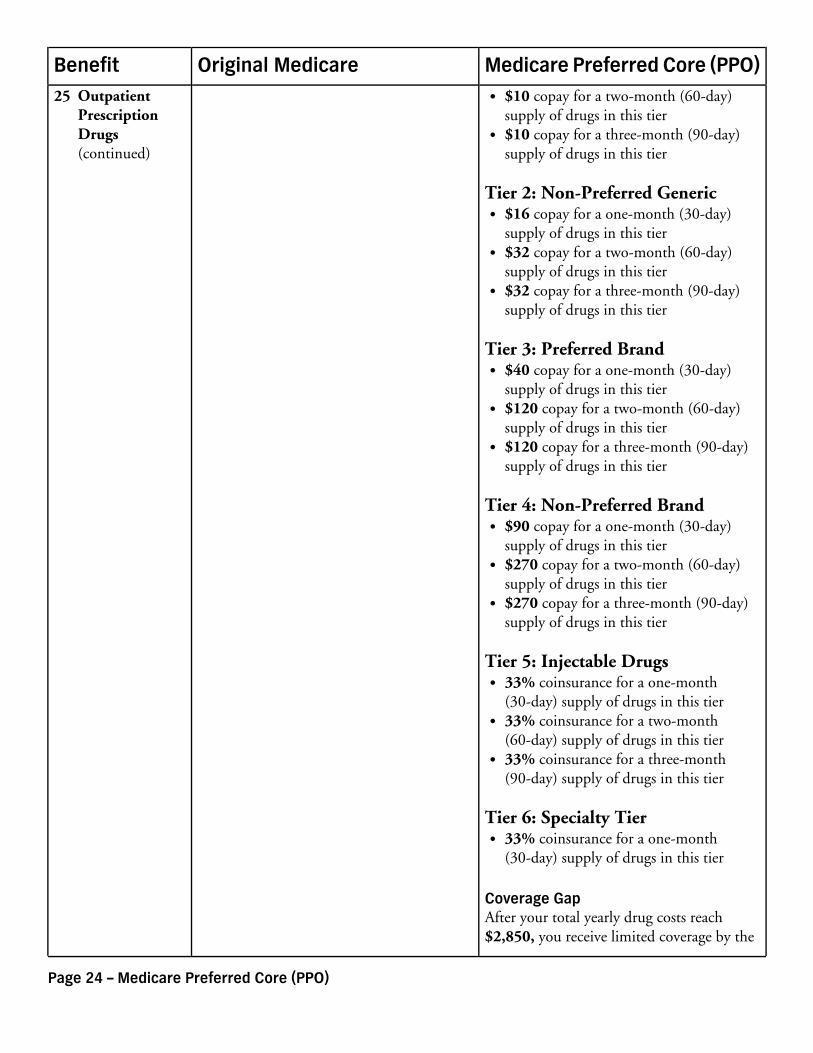
Medicare Preferred Core (PPO)Original MedicareBenefit$10 copay for a two-month (60-day)supply of drugs in this tier$10 copay for a three-month (90-day)supply of drugs in this tier
Tier 2: Non-Preferred Generic$16 copay for a one-month (30-day)supply of drugs in this tier$32 copay for a two-month (60-day)supply of drugs in this tier$32 copay for a three-month (90-day)supply of drugs in this tier
Tier 3: Preferred Brand$40 copay for a one-month (30-day)supply of drugs in this tier$120 copay for a two-month (60-day)supply of drugs in this tier$120 copay for a three-month (90-day)supply of drugs in this tier
Tier 4: Non-Preferred Brand$90 copay for a one-month (30-day)supply of drugs in this tier$270 copay for a two-month (60-day)supply of drugs in this tier$270 copay for a three-month (90-day)supply of drugs in this tier
Tier 5: Injectable Drugs33% coinsurance for a one-month(30-day) supply of drugs in this tier33% coinsurance for a two-month(60-day) supply of drugs in this tier33% coinsurance for a three-month(90-day) supply of drugs in this tier
Tier 6: Specialty Tier33% coinsurance for a one-month(30-day) supply of drugs in this tier
Coverage GapAfter your total yearly drug costs reach$2,850, you receive limited coverage by the
25 OutpatientPrescriptionDrugs(continued)
Page 24 – Medicare Preferred Core (PPO)
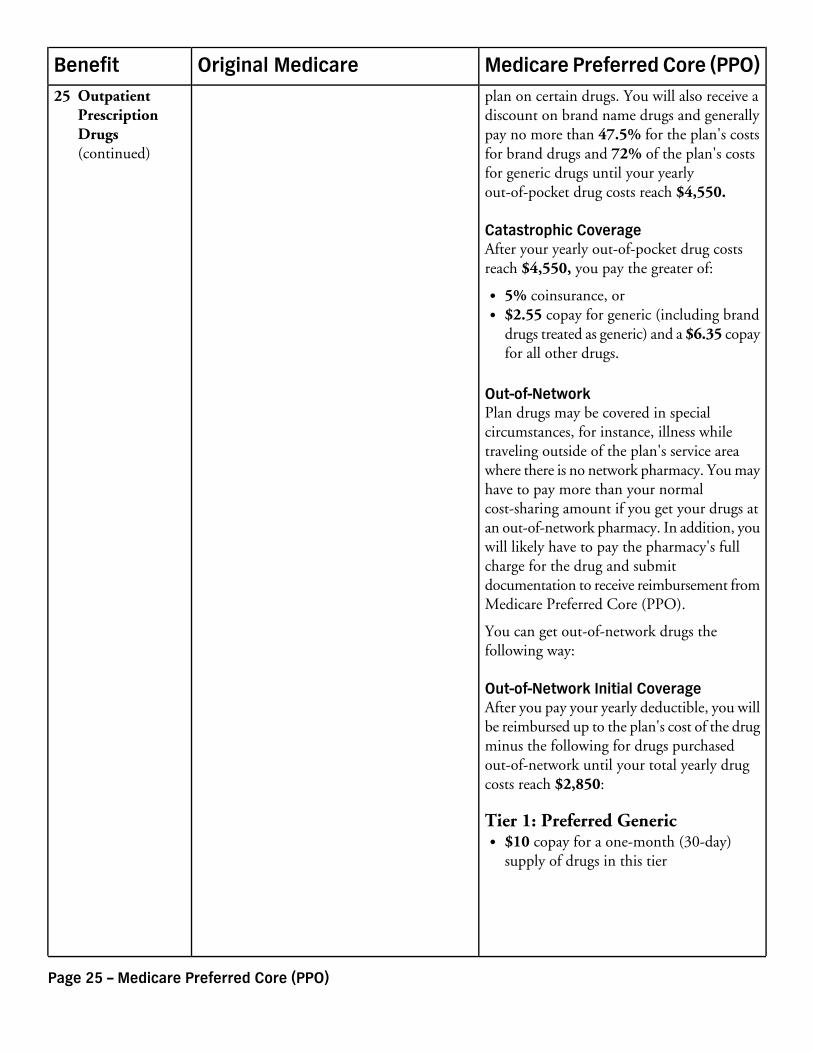
Medicare Preferred Core (PPO)Original MedicareBenefitplan on certain drugs. You will also receive adiscount on brand name drugs and generallypay no more than 47.5% for the plan's costsfor brand drugs and 72% of the plan's costsfor generic drugs until your yearlyout-of-pocket drug costs reach $4,550.
Catastrophic CoverageAfter your yearly out-of-pocket drug costsreach $4,550, you pay the greater of:
5% coinsurance, or$2.55 copay for generic (including branddrugs treated as generic) and a $6.35 copayfor all other drugs.
Out-of-NetworkPlan drugs may be covered in specialcircumstances, for instance, illness whiletraveling outside of the plan's service areawhere there is no network pharmacy. You mayhave to pay more than your normalcost-sharing amount if you get your drugs atan out-of-network pharmacy. In addition, youwill likely have to pay the pharmacy's fullcharge for the drug and submitdocumentation to receive reimbursement fromMedicare Preferred Core (PPO).
You can get out-of-network drugs thefollowing way:
Out-of-Network Initial CoverageAfter you pay your yearly deductible, you willbe reimbursed up to the plan's cost of the drugminus the following for drugs purchasedout-of-network until your total yearly drugcosts reach $2,850:
Tier 1: Preferred Generic$10 copay for a one-month (30-day)supply of drugs in this tier
25 OutpatientPrescriptionDrugs(continued)
Page 25 – Medicare Preferred Core (PPO)
Medicare Preferred Core (PPO)Original MedicareBenefit
Tier 2: Non-Preferred Generic$21 copay for a one-month (30-day)supply of drugs in this tier
Tier 3: Preferred Brand$45 copay for a one-month (30-day)supply of drugs in this tier
Tier 4: Non-Preferred Brand$95 copay for a one-month (30-day)supply of drugs in this tier
Tier 5: Injectable Drugs33% coinsurance for a one-month(30-day) supply of drugs in this tier
Tier 6: Specialty Tier33% coinsurance for a one-month(30-day) supply of drugs in this tier
You will not be reimbursed for the differencebetween the Out-of-Network Pharmacycharge and the plan's In-Network allowableamount.
Out-of-Network Coverage GapYou will be reimbursed up to 28% of the planallowable cost for generic drugs purchasedout-of-network until total yearly out-of-pocketdrug costs reach $4,550. Please note that theplan allowable cost may be less than theout-of-network pharmacy price paid for yourdrug(s).
You will be reimbursed up to 52.5% of theplan allowable cost for brand name drugspurchased out-of-network until your totalyearly out-of-pocket drug costs reach $4,550.Please note that the plan allowable cost maybe less than the out-of-network pharmacyprice paid for your drug(s).
Out-of-Network Catastrophic CoverageAfter your yearly out-of-pocket drug costsreach $4,550, you will be reimbursed for
25 OutpatientPrescriptionDrugs(continued)
Page 26 – Medicare Preferred Core (PPO)
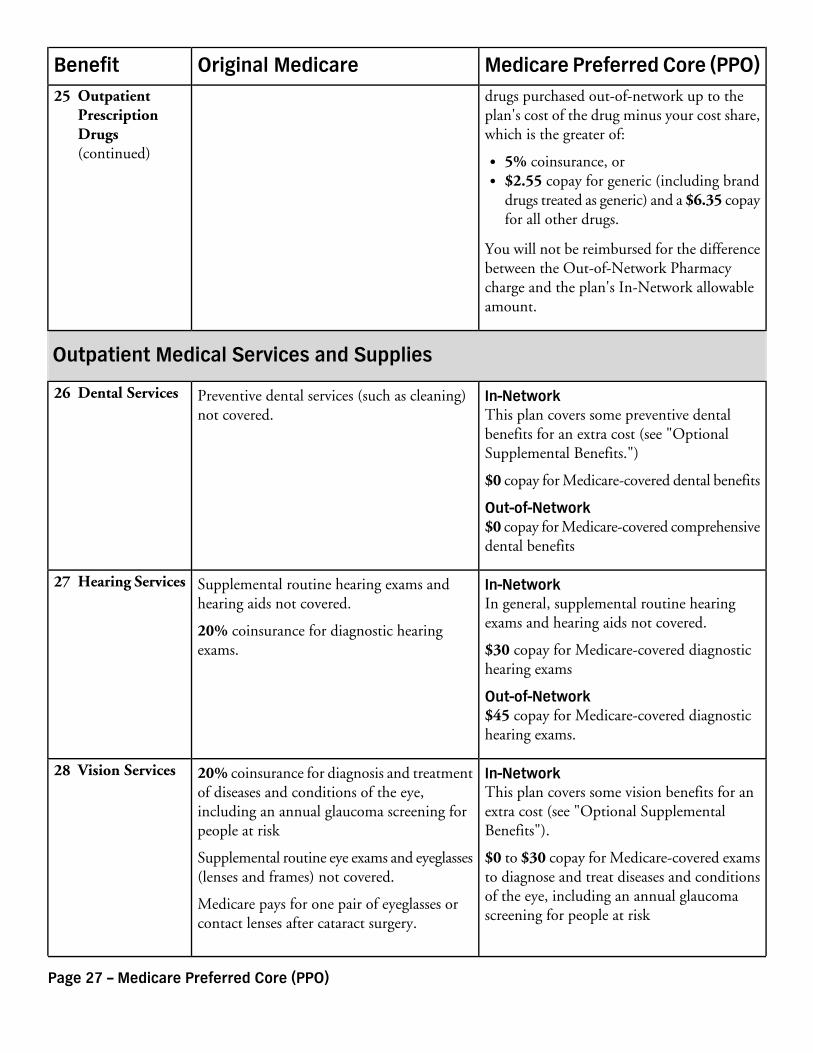
Medicare Preferred Core (PPO)Original MedicareBenefitdrugs purchased out-of-network up to theplan's cost of the drug minus your cost share,which is the greater of:
5% coinsurance, or$2.55 copay for generic (including branddrugs treated as generic) and a $6.35 copayfor all other drugs.
You will not be reimbursed for the differencebetween the Out-of-Network Pharmacycharge and the plan's In-Network allowableamount.
Outpatient Medical Services and Supplies
In-NetworkThis plan covers some preventive dentalbenefits for an extra cost (see "OptionalSupplemental Benefits.")
Preventive dental services (such as cleaning)not covered.
26 Dental Services
$0 copay for Medicare-covered dental benefits
Out-of-Network$0 copay for Medicare-covered comprehensivedental benefits
In-NetworkIn general, supplemental routine hearingexams and hearing aids not covered.
Supplemental routine hearing exams andhearing aids not covered.
20% coinsurance for diagnostic hearingexams.
27 Hearing Services
$30 copay for Medicare-covered diagnostichearing exams
Out-of-Network$45 copay for Medicare-covered diagnostichearing exams.
In-NetworkThis plan covers some vision benefits for anextra cost (see "Optional SupplementalBenefits").
20% coinsurance for diagnosis and treatmentof diseases and conditions of the eye,including an annual glaucoma screening forpeople at risk
28 Vision Services
$0 to $30 copay for Medicare-covered examsto diagnose and treat diseases and conditions
Supplemental routine eye exams and eyeglasses(lenses and frames) not covered.
of the eye, including an annual glaucomascreening for people at risk
Medicare pays for one pair of eyeglasses orcontact lenses after cataract surgery.
25 OutpatientPrescriptionDrugs(continued)
Page 27 – Medicare Preferred Core (PPO)
Medicare Preferred Core (PPO)Original MedicareBenefit
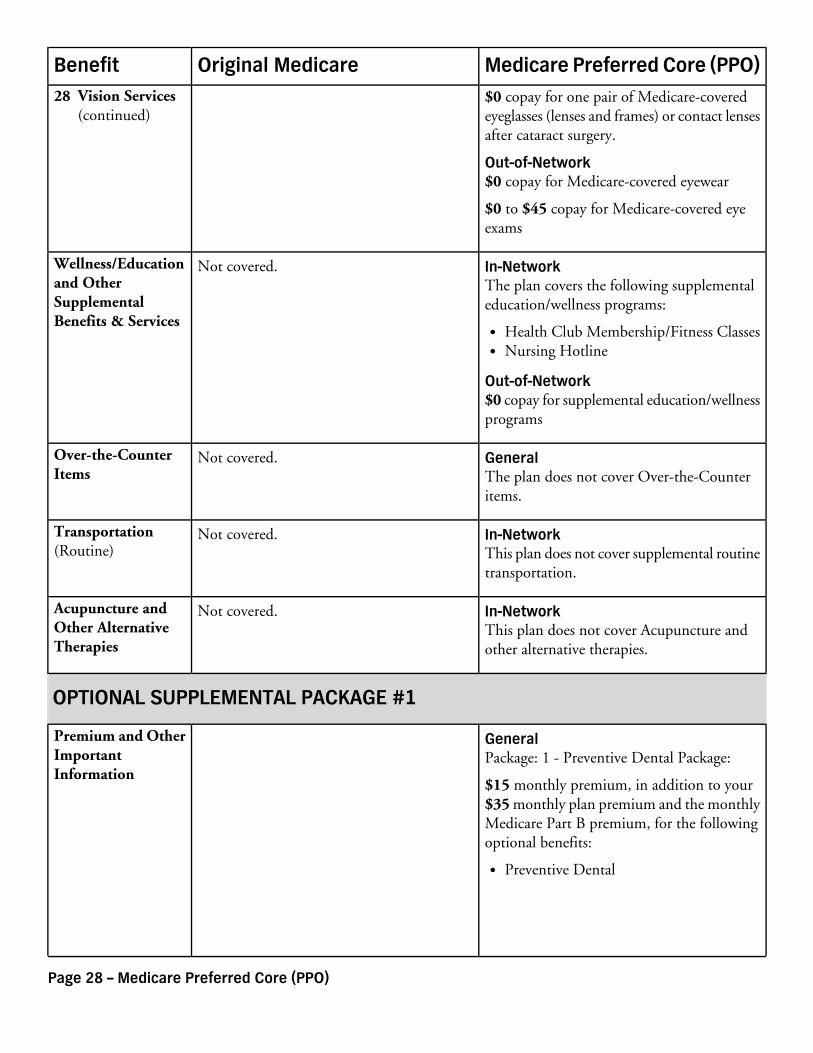
$0 copay for one pair of Medicare-coveredeyeglasses (lenses and frames) or contact lensesafter cataract surgery.
Out-of-Network$0 copay for Medicare-covered eyewear
$0 to $45 copay for Medicare-covered eyeexams
In-NetworkThe plan covers the following supplementaleducation/wellness programs:
Not covered.Wellness/Educationand OtherSupplementalBenefits & Services
Health Club Membership/Fitness ClassesNursing Hotline
Out-of-Network$0 copay for supplemental education/wellnessprograms
GeneralThe plan does not cover Over-the-Counteritems.
Not covered.Over-the-CounterItems
In-NetworkThis plan does not cover supplemental routinetransportation.
Not covered.Transportation(Routine)
In-NetworkThis plan does not cover Acupuncture andother alternative therapies.
Not covered.Acupuncture andOther AlternativeTherapies
OPTIONAL SUPPLEMENTAL PACKAGE #1
GeneralPackage: 1 - Preventive Dental Package:
Premium and OtherImportantInformation
$15 monthly premium, in addition to your$35 monthly plan premium and the monthlyMedicare Part B premium, for the followingoptional benefits:
Preventive Dental
28 Vision Services(continued)
Page 28 – Medicare Preferred Core (PPO)
Medicare Preferred Core (PPO)Original MedicareBenefit
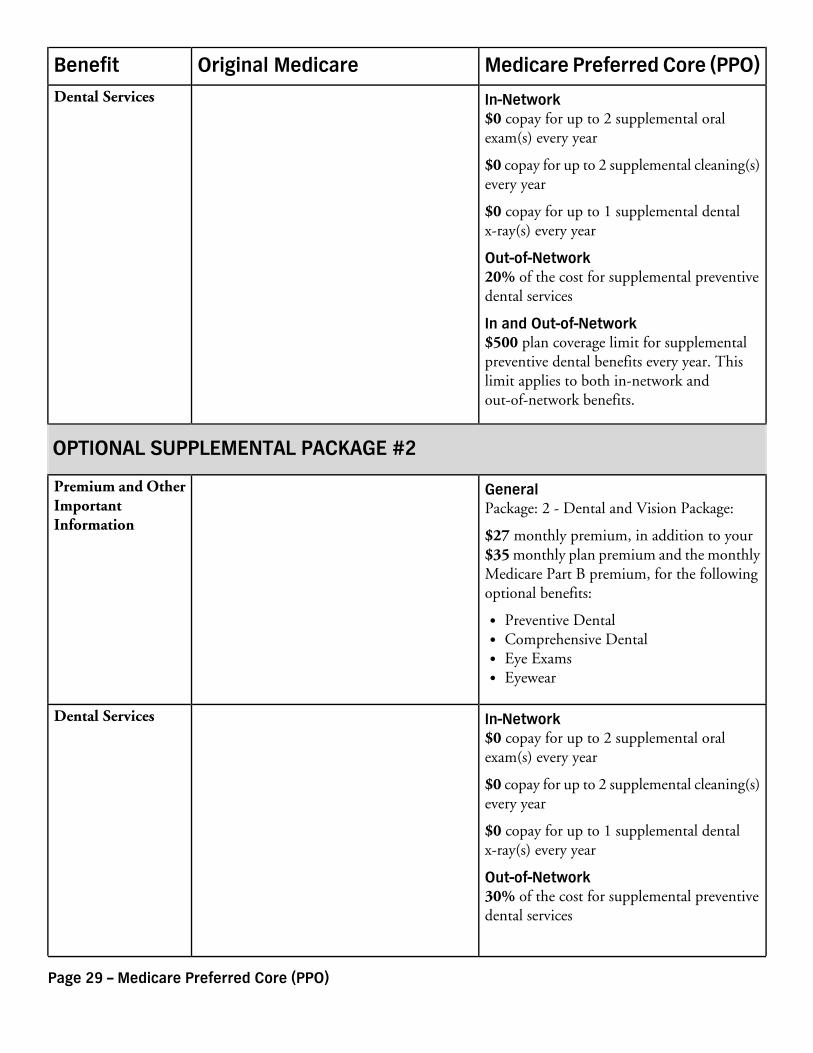
In-Network$0 copay for up to 2 supplemental oralexam(s) every year
Dental Services
$0 copay for up to 2 supplemental cleaning(s)every year
$0 copay for up to 1 supplemental dentalx-ray(s) every year
Out-of-Network20% of the cost for supplemental preventivedental services
In and Out-of-Network$500 plan coverage limit for supplementalpreventive dental benefits every year. Thislimit applies to both in-network andout-of-network benefits.
OPTIONAL SUPPLEMENTAL PACKAGE #2
GeneralPackage: 2 - Dental and Vision Package:
Premium and OtherImportantInformation
$27 monthly premium, in addition to your$35 monthly plan premium and the monthlyMedicare Part B premium, for the followingoptional benefits:
Preventive DentalComprehensive DentalEye ExamsEyewear
In-Network$0 copay for up to 2 supplemental oralexam(s) every year
Dental Services
$0 copay for up to 2 supplemental cleaning(s)every year
$0 copay for up to 1 supplemental dentalx-ray(s) every year
Out-of-Network30% of the cost for supplemental preventivedental services
Page 29 – Medicare Preferred Core (PPO)

Medicare Preferred Core (PPO)Original MedicareBenefit
30% to 75% of the cost for supplementalcomprehensive dental services
In and Out-of-NetworkContact the plan for availability of additionalsupplemental in-network and out-of-networkcomprehensive dental benefits.
$1,000 plan coverage limit for supplementaldental benefits every year. This limit appliesto both in-network and out-of-networkbenefits.
In-Network$0 copay for up to 1 pair(s) of contact lensesevery year
Vision Services
$0 copay for up to 1 pair(s) of eyeglasses(lenses and frames) every year
$0 copay for up to 1 supplemental routineeye exam(s) every year
Out-of-Network$0 copay for supplemental routine eye exams
$0 copay for supplemental eyewear
In and Out-of-Network$69 plan coverage limit for supplementalroutine eye exams every year. This limitapplies to both in-network andout-of-network benefits.
$130 plan coverage limit for eyeglasses (lensesand frames) every year. This limit applies toboth in-network and out-of-network benefits.
$80 plan coverage limit for contact lensesevery year. This limit applies to bothin-network and out-of-network benefits.
OPTIONAL SUPPLEMENTAL PACKAGE #3
GeneralPackage: 3 - Enhanced Dental and VisionPackage:
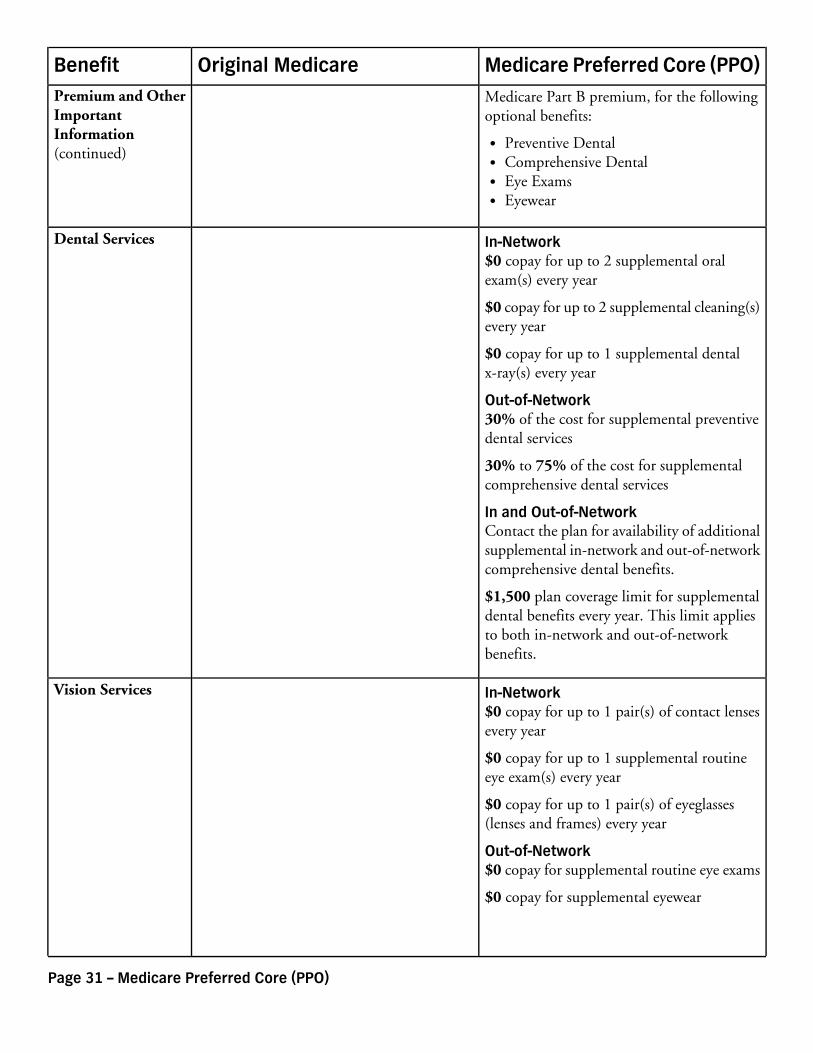
Premium and OtherImportantInformation
$38 monthly premium, in addition to your$35 monthly plan premium and the monthly
Dental Services(continued)
Page 30 – Medicare Preferred Core (PPO)
Medicare Preferred Core (PPO)Original MedicareBenefit
Medicare Part B premium, for the followingoptional benefits:
Preventive DentalComprehensive DentalEye ExamsEyewear
In-Network$0 copay for up to 2 supplemental oralexam(s) every year
Dental Services
$0 copay for up to 2 supplemental cleaning(s)every year
$0 copay for up to 1 supplemental dentalx-ray(s) every year
Out-of-Network30% of the cost for supplemental preventivedental services
30% to 75% of the cost for supplementalcomprehensive dental services
In and Out-of-NetworkContact the plan for availability of additionalsupplemental in-network and out-of-networkcomprehensive dental benefits.
$1,500 plan coverage limit for supplementaldental benefits every year. This limit appliesto both in-network and out-of-networkbenefits.
In-Network$0 copay for up to 1 pair(s) of contact lensesevery year
Vision Services
$0 copay for up to 1 supplemental routineeye exam(s) every year
$0 copay for up to 1 pair(s) of eyeglasses(lenses and frames) every year
Out-of-Network$0 copay for supplemental routine eye exams
$0 copay for supplemental eyewear
Premium and OtherImportantInformation(continued)
Page 31 – Medicare Preferred Core (PPO)
Medicare Preferred Core (PPO)Original MedicareBenefit
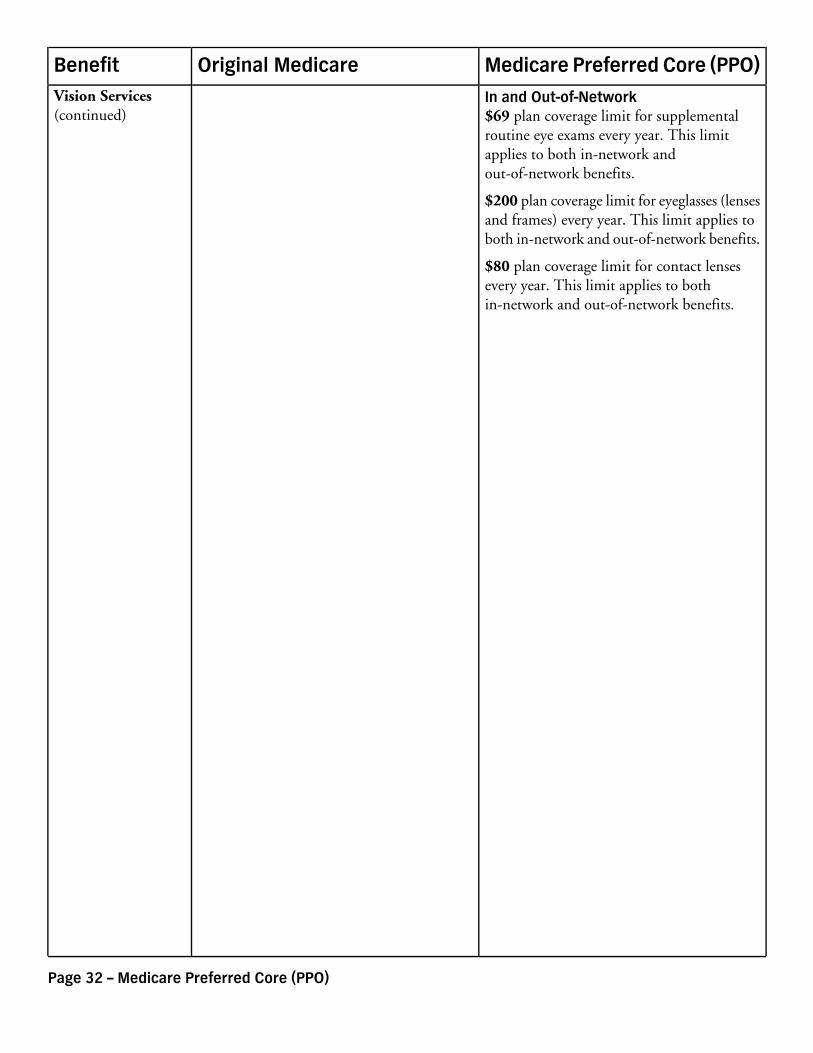
In and Out-of-Network$69 plan coverage limit for supplementalroutine eye exams every year. This limitapplies to both in-network andout-of-network benefits.
$200 plan coverage limit for eyeglasses (lensesand frames) every year. This limit applies toboth in-network and out-of-network benefits.
$80 plan coverage limit for contact lensesevery year. This limit applies to bothin-network and out-of-network benefits.
Vision Services(continued)
Page 32 – Medicare Preferred Core (PPO)