blood component therapy
DESCRIPTION
paediatric guidelinesTRANSCRIPT
BLOOD AND BLOOD COMPONENT
THERAPY Dr Rakesh Verma
Guided by
Dr Santosh Singh 1
Nelson
Cloherty handbook
Ghai Essential Paediatrics
Meherban Singh Care of Newborn
AIIMS Newborn protocol
Nathan and Oski children and infant Haematology
-
• The routine separation of donor blood intocomponents and plasma fraction has made itpossible for blood banks to provide thespecialized blood products required for thesupport of patients in multiple treatmentmodalities.
• The infusion of blood component is called component transfusion or blood component therapy.
2

However, in most cases blood components arepreferred because each component has specificoptimal storage conditions and component therapymaximizes the use of blood donations.
Removal of 10 ml from 1500gm neonate equals400ml of adult (= 8% blood volume)
As many as 70% - 80% LBW require atleast 1transfusion
3

Fresh Whole Blood
Packed Red Cells
Light spin, 22oC(within 8 hrs)
Platelet Rich Plasma
Platelet Concentrate Fresh Plasma
Store at 22oC Freeze(FFP)
Heavy spin,22oC
4

TYPESBlood-
• Fresh Whole Blood
• Reconstituted whole blood
• From one unit of whole blood
one can make = Blood components
• PRBC
• Platelet pack(random donor)
• Fresh plasma
• Granulocyte pack
• Fresh plasma →frozen at -30°C→FFP
• Pooled plasma→ components
Cryoprecipitate
Albumin
Immunoglobulins
5
Before transfusion consider
Whether required
How much required
Actual component required
Time of duration of transfusion
WHOLE BLOOD
Duration of preservation varies according to preservative (CPD,CPDA, SAGM)
Reconstituted whole blood lacks significant quantities of platelets and clotting factors
1 unit increases Hgb 1 g/dL and Hct 3%
Indications.• Exchange transfusions.
• Surgery
• Acute blood loss (>20% blood volume)
• Can be used as a substitute for blood components.
6

Packed Red Blood Cells (PRBCs)
After centrifugation of 350 ml whole blood, the RBC component has a volume of about 200 ml and Hct of about 80 %.
Genarally 100 to 110 mL of a nutrient additive solution is added back to the packed RBCs, creating an “additive RBC” product that has a final hematocritof 55% to 60%.
These solutions prolong the shelf life of the RBC product from 21 days (packed RBCs in CPD) to 35 days in (CPDA) to 42 days (additive RBCs).
• Once the unit is “opened” it has a to be used in 24 hours
7

ABO group selection for RBC Transfusion
Recipient ABOGroup
Component ABO Group
1st Choice 2nd Choice 3rd Choice 4thChoice
A A O None None
B B O None None
AB AB A B O
O O None None None
8

Available forms of RCCs
• RBC concentrates.
• RBC concentrates deprived of the buffy coat.
• RBC concentrates with additive solutions.
• Washed RBC.
• Leucodepleted RBC.
• Frozen RBC.
• Apheretic RBC.
• Irradiated RBC.
9

1. Leucodepleted/ Leucoreduced RCCs
Most plasma & 70-80% WBC(buffy coat) removed & 100 ml of Additive Solution added.
Indications• Prevention of febrile non-haemolytic
transfusion reactions (FNHTRs) • - patients with recurrent FNHTR;• - patients who need prolonged
transfusion support.• Reduction of the incidence of CMV
infections and other leukotrophic viruses• Intrauterine transfusions and transfusions
to premature babies, neonates, and infants up to 1 year.
• Candidates for renal transplantation.10

2. Washed RCC
RBC washed with Normal SalineWashing eliminates antibodies & other plasma
constituents reduce potassium• recommended for intrauterine transfusions, • exchange transfusion and • large volume transfusions
Indication• Patients with IgA deficiency (presence of
anti-IgA).• Paroxysmal nocturnal hemoglobinuria• Allogeneic bone marrow transplant
11

3. Irradiated RCCs
• Irradiation, at the dose of 25–50 Gy Gamma radiation, is for preventing transfusion-related GvHD. Radiation damages T cells
• Shelf life of RBC decrease to 28 days, hyperkalaemia is risk
Donor units from a blood relative (Directed Donations)
Intrauterine transfusion
Immunodeficiency
Premature newborns, recommended <1200gm baby
Preferable for any transfusions till 4 months of age.
Chemo or Radiotherapy
Solid organ transplant, Bone marrow transplant
12
4. Frozen RCCsGlycerol is used as preservativeStored for 10 years, Once thawed should be used in 24 hours
Autologous transfusion Preservation of rare blood group

Choice of blood in Emergency need• Patient should receive type specific blood
• Time not permissible, then O –ve RBC and AB plasma can be given
• In males when there is shortage of blood then O +ve RBC can be given
Choice of blood in Massive transfusion
• Greater than 1 blood volume within 24 hours
• For alloimmunised tested patients, blood not tested for antigen may be used during an acute bleeding period and antigen negative blood reserved for late transfusion
13
Autologous blood transfusion • For autologous blood transfusion children should have Hb >11gm%, and
Hct >33%.
• Collection before 4-5 weeks before surgery.
• Oral iron supplement
• Erythropoietin may be used
Choice of blood for fetus
• For intrauterine transfusion group O Rh(D-) should be used
• To prevent GVHD blood is irradiated and to prevent CMV; CMV antibody negative blood or leukocyte reduced blood should be used
14

Choice of blood for neonate• CMV antibody negative blood or leukocyte reduced blood should be used especially
in less than 1200gm
• Leukocyte reduced blood also prevent GVHD which is more common in low birth weight babies
• For exchange transfusion for HDN, RBC must be negative for implicated antibody
• In term of ABO group selection, group O RBC and plasma of infant’s ABO are used
15
Directed DonationsA directed donation occurs when a patient's family or friends donate blood for their childrenTransfusion-associated GVHD can occur in these recieversIt can also occur in situations in which the blood donor is homozygous and the recipientis heterozygous for an HLA haplotype. It is associated with higher mortality (80-90%). It is almost entirely preventable by controlled irradiation of blood products

Choice of blood in Sickle cell anemia
• PRINCIPLE ARE1. Avoidance of excessive viscosity:
• PRBC of high haematocrit should be used cautiously;
• Cautious transfusion when haematocrit is >30%
2. Prevention of sensitization of Red cell antigen
Approach Antigens matched
1. Provide fully antigen matched blood before patient makes antibodies
Matched for D, C, E, c, e, K, Fy, Jkantigens
2. Provide partially antigen matched blood
Matched for D, C, E, K antigen
3. Treat like other patient Avoid antigens to which patient has made antibody
16

In sickle cell anemia Hb should be maintained at 10-12 gm/dl with <30% Hb S
Transfusion therapy is not normally indicated in patients with Hb values > 7 g/dL
• Type of blood transfusion
1. erythrocytapheresis,
2. manual exchange transfusions
3. simple transfusion.
17

Choice of blood in Thalassemia
• Goal of therapy are • Prevention of anemia
• Maintenance of Hb level sufficient to supress endogenous erythropoiesis
• Maintenance of pretransfusion level of 9-10g% is sufficient
• Red cell alloantibodies are not a significant problem in most cases, probably because transfusion is usually initiated at early age when tolerance may develop
18

Choice of blood transfusion in allogeneic marrow transplant
Major ABO incompatibility Minor ABO incompatibility
Recipient has antibody against donor RBC Donor has antibody against recipient RBC
Recipient Donor Red cell
A O O
A B O
A AB O or A
B O O
B A O
B AB O or B
Recipient Donor Red cell
AB O O
AB B O or B
AB A O or A
O A O
O B O
O AB O
In minor ABO incompatibility plasma is removed before infusion
When there is major ABO incompatibility
19
Factors other than hemoglobin concentration to beconsidered in the decision to transfuse RBCs include:
• Patient's symptoms, signs, and functional capacities,
• The presence of cardiorespiratory, vascular, andcentral nervous system disease
• The cause and anticipated course of the anemia
• Alternative therapies, such as recombinant humanerythropoietin (EPO) therapy, which is known toreduce the need for RBC transfusions and to improvethe overall condition of children with chronic renalinsufficiency and preterm infants.
20

Disease requiring intermittent or chronic blood transfusion in childhood
• Thalassemia
• Sickle cell disease
• Aplastic anaemia
• Chronic renal dysfunction
21
Guideline for chronic transfusion
• Aggressive management of the underlying diseasedialysis or erythropoietin therapy for renalimpairment
• Leukocyte reduced RBC (to prevent FNHTR)
• PRBC in such amount to prevent symptomaticanaemia and allow normal growth
• Monitor iron, ferritin, TIBC, liver iron store
22
Chronic Anaemia
• Transfusion should be considered in a asymptomatic child with a Hb level of less than 4 g/dL.
• Transfusion should be considered in a child with a Hb level of less than 5 g/dL with clinical signs of cardiac or respiratory distress.
• Children with a Hb level of 5 g/dL or greater should NOT be transfused indiscriminately, but the cause of their anaemia should be investigated.
• Transfusions must be given slowly (over a 4 hour period. At the rate of 2-3 ml/kg/hr).
23
Patients with iron-deficiency anemia are often treated successfully with oral iron alone, even at hemoglobin levels of <5 g/dL.
Treat the cause as infection, nutritional and mild blood loss anaemia with specific therapeutic agents as indicated (iron, folic acid, B12).
• Premature babies are comfortable at Hb 6.5 - 7
gm%.
• Healthy asymptomatic neonate will self correct
anemia, provided iron should be adequate
• BT in neonate when asymptomatic Hct <21% or
reticulocyte count < 2%
24

CHILDREN AND ADOLESCENTS
• Acute loss of >25% at circulating blood volume
• Hemoglobin of <8.0 g/dL in the perioperative period
• Hemoglobin of <13.0 g/dL and severe cardiopulmonary disease
• Hemoglobin of <8.0 g/dL and symptomatic chronic anemia
• Hemoglobin of <8.0 g/dL and marrow failure
(Nelson)
25
INFANTS WITHIN THE FIRST 4 MO OF LIFE
Hemoglobin of <13.0 g/dL and severe pulmonary disease
Hemoglobin of <10.0 g/dL and moderate pulmonary disease
Hemoglobin of <13.0 g/dL and severe cardiac disease
Hemoglobin of <10.0 g/dL and major surgery
Hemoglobin of <8.0 g/dL and symptomatic anemia
26

Blood component therapy in newborn
• The total blood volume of neonates is small, although the volume is higher per kg of body weight than that of older children or adults. (85 ml/kg for full-term and 100 to 105 ml/kg for pre-term). .
27
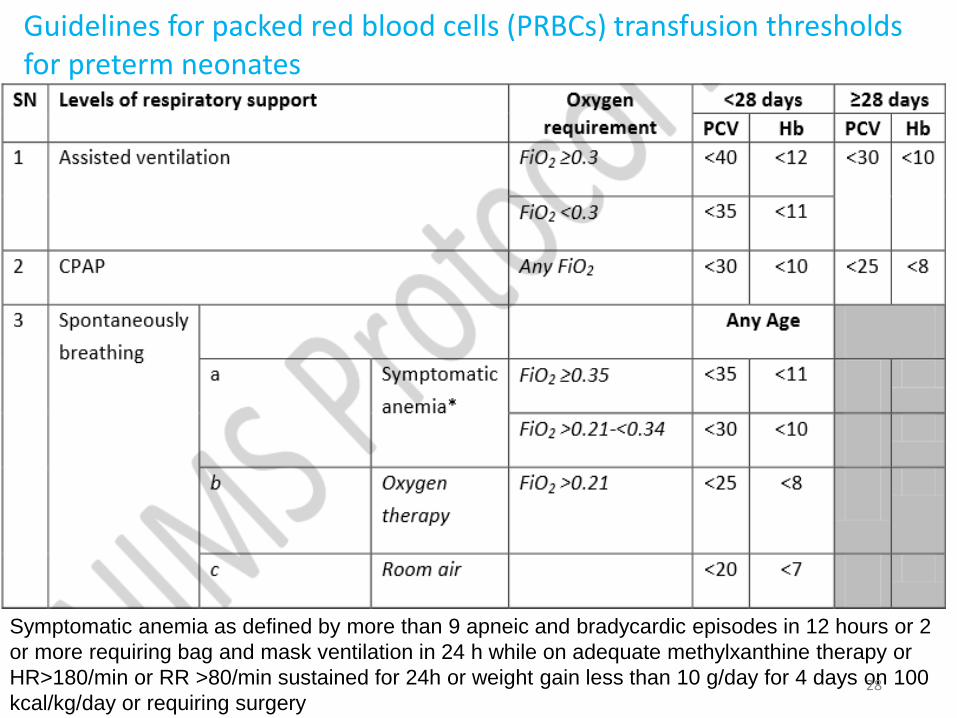
Guidelines for packed red blood cells (PRBCs) transfusion thresholds for preterm neonates
Symptomatic anemia as defined by more than 9 apneic and bradycardic episodes in 12 hours or 2
or more requiring bag and mask ventilation in 24 h while on adequate methylxanthine therapy or
HR>180/min or RR >80/min sustained for 24h or weight gain less than 10 g/day for 4 days on 100
kcal/kg/day or requiring surgery28

• Blood transfusion in pre-term infants, is often given for the anaemia of prematurity, associated with delayed renal production of erythropoietin due to decreased sensitivity to lower haematocrit levels.
• These neonates may require multiple transfusions, increasing the risk of infectious disease transmission, through multiple donor exposures alloimmunization
• Studies have shown that multiple transfusion from multiple donor in preterms is associated with increased risk of ROP and BPD.
• Multiple donor exposures in small and sick neonates can be prevented by reserving a bag of fresh PRBC for up to 7 days for a newborn and withdrawing small aliquots required as and when needed
29

Choosing the blood group for neonatal transfusions
• Mother’s sample should be tested for blood group and for any atypical red cell antibodies.
• ABO compatibility.
Though ABO antigens may be expressed only weakly on neonatal erythrocytes, neonate’s serum may contain transplacentally acquired maternal IgG anti-A and/or anti-B.
30

Choosing the blood group for neonatal transfusions.
c. Blood should be of newborn’s ABO and Rh group.
It should be compatible with any ABO or atypical red cell antibody present in the maternal serum.
d. In exchange transfusions for hemolytic disease of newborn-, blood transfused should be compatible with mother’s serum.
If the mother’s and the baby’s blood groups are the same, use Rh negative blood of baby’s ABO group.
In case mother’s and baby’s blood group is not compatible, use group O and Rh negative blood for exchange transfusion.
31
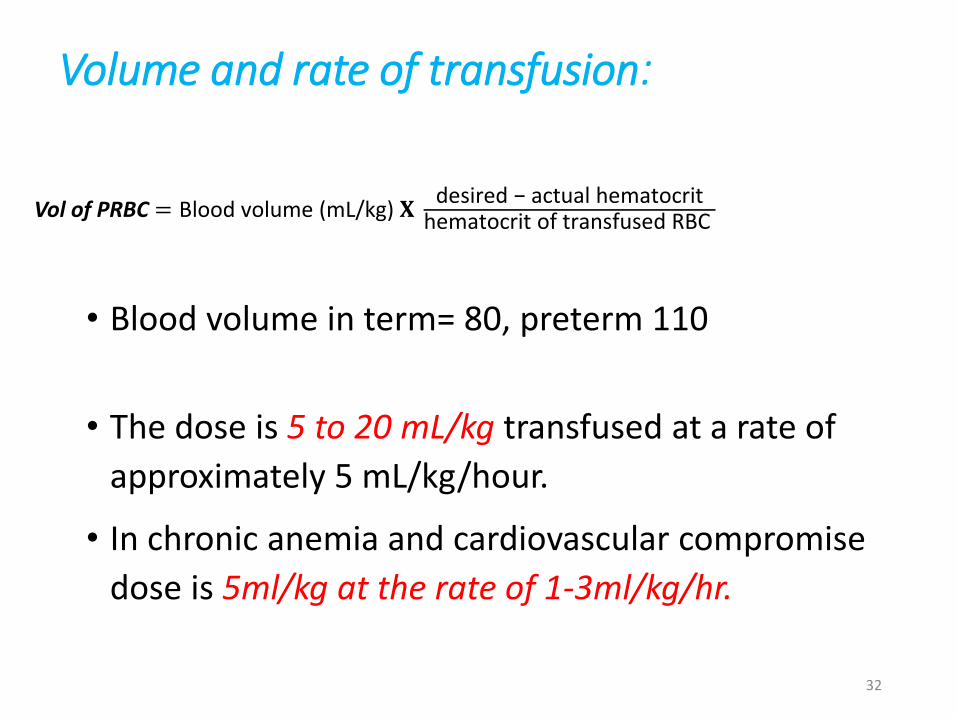
Volume and rate of transfusion:
• Blood volume in term= 80, preterm 110
• The dose is 5 to 20 mL/kg transfused at a rate of
approximately 5 mL/kg/hour.
• In chronic anemia and cardiovascular compromise
dose is 5ml/kg at the rate of 1-3ml/kg/hr.
Vol of PRBC = Blood volume (mL/kg) 𝐗desired − actual hematocrit
hematocrit of transfused RBC
32

• It has been seen that transfusion with PRBC at a dose of 20 mL/kg is well tolerated and results in an overall decrease in number of transfusions compared to transfusions done at 10 mL/kg in preterm and VLBW infants.
• In Infants and newborn, one unit of RCC( 10 ml/kg) increases Hb by 3g/dl.
• In children, the transfusion of RCC 10 mL/kg increases the Hb concentration by about 2 g/dL.
33

PLATELET TRANSFUSION
• Platelets are stored at 20°C to 24°C using continuous gentle horizontal agitation in storage bags specifically designed to permit O2 and CO2 exchange to optimize platelet quality.
• It should be transported quickly and infused rapidly over 20-30minutes to prevent loss of platelets due to aggregation.
• Should use only ABO/Rh identical compatible donor.
• In emergency one can use incompatible donors though the efficacy may be less than expected
34

• Types – SDP and RDP
• The storage time from collection to transfusion of platelets (RDPs) is 5 days.
• SDPs can be stored for up to 7 days.
Random donor platelet (RDP)
Platelet atleast5.5x1010
1unit/10kgRaise 30,000-50,000/cumm
Single donor platelet (SDP) Platelet atleast3x1011
1 collection equals 6RDP
35

Types of platelets
• RANDOM DONOR
• SINGLE DONOR
• PLASMA DEPLETED PLATELETS
• WASHED PLATELETS
• WBC FILTERED
• UV OR GAMMA IRRADIATED
• PLATELETS FROM SPECIFIC DONOR:
CMV NEGATIVE OR HLA-MATCHED DONOR.
36
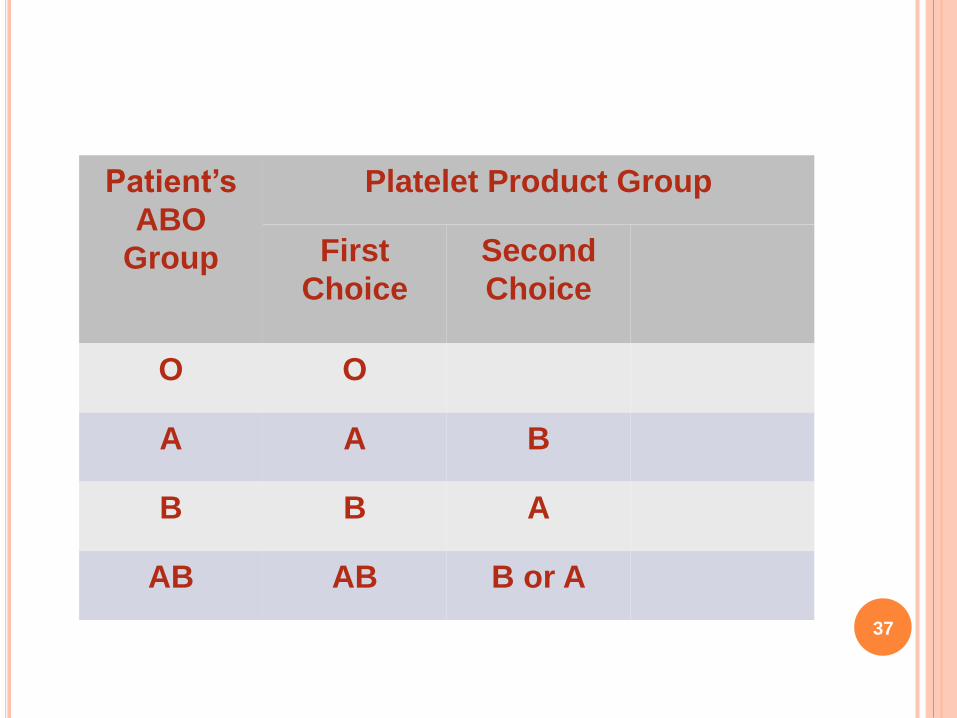
Patient’s
ABO
Group
Platelet Product Group
First
Choice
Second
Choice
O O
A A B
B B A
AB AB B or A
37

Recommandation for platelets use
• Platelets should never be filtered through a micropore blood filter before transfusion.
• Should be ABO compatible.
• The usual recommended dose of platelets for neonates is 1 unit of platelets per 10 kg body weight, which amounts to 5 mL/kg.
• The predicted rise in platelet count from a 5-mL/kg dose would be 20 to 60,000/cubic mm.
38

CHILDREN AND ADOLESCENTS
• PLTs < 50 × 109/L and bleeding
• PLTs < 50 × 109/L and an invasive procedure
• PLTs < 20 × 109/L and marrow failure with hemorrhagic risk factors
• PLTs < 10 × 109/L and marrow failure without hemorrhagic risk factors
• PLTs at any count, but with PLT dysfunction plus bleeding or an invasive procedure
39

INFANTS WITHIN THE FIRST 4 MO OF LIFE
oPLTs < 100 × 109/L and bleeding on ECMO
oPLTs < 50 × 109/L and an invasive procedure
oPLTs < 50 × 109/L and clinically unstable
oPLTs < 20 × 109/L and clinically stable
oPLTs at any count, but with PLT dysfunction plus bleeding or an invasive procedure
40

Indications for platelet transfusion in nonimmunethrombocytopenia in newborn: AIIMS
1. Platelet count less than 30,000/cubic mm: transfuse all neonates, even if asymptomatic
2. Platelet count 30,000 to 50,000/cubic mm: consider transfusion in
a. Sick or bleeding newbornsb. ELBW or less than 1 week of agec. Previous major bleeding tendencyd. Newborns with concurrent coagulopathye. Requiring surgery or exchange transfusion
3. Platelet count more than 50,000 to 99,000/cubic mm: transfuse only if actively bleeding
41

Plasma-Derived Blood Components
FFPPlasma separated from a unit of whole blood and
frozen within 8 h of collection is designated fresh frozen plasma (FFP) .
The usual volume of FFP is about 225 ml. FFP supplies all of the constituents of fresh plasma, including the labile coagulation factors, albumin and globulin.
Plasma contains about 1 unit/mL of each of the coagulation factors
42
Indications
• Severe clotting factor deficiency (including DIC) withbleeding
• Severe clotting factor deficiency patient undergoingan invasive procedure
• Vitamin K deficiency with bleeding
• Dilutional coagulopathy with bleeding
• Severe anticoagulant protein deficiency
• Reconstitution of packed RBC for exchangetransfusion
44

FFP use in newborn
• Plasma should be transfused only after reference to normal values adjusted for the birthweight and age of the infant
• 1. Sick neonate with unspecified coagulation disorder due to sepsis, DIC, NEC etc.
• 2. Vitamin K deficiency bleeding
• 3. Inherited deficiencies of coagulation factors
It should not be used for prevention of intraventricularhemorrhage, and in supportive treatment of sepsis
45

It is prepared from FFP by thawing at 2 – 4C.
Contains approximately 100 u of factor VIII and von Willebrand factor,
75 u of factor XIII, and
250mg of fibrinogen
in a volume of 20 ml.
It is transfused usually at 5ml/kg over 30 min.
Cryoprecipitate:
46

Indications for use of cryoprecipitate:
• Afibrinogenemia,
• Von Willebrand factor deficiency,
• Congenital antithrombin III deficiency, hemophilia.
• It is also used for reconstitution of blood for exchange transfusion.
47
Granulocyte Transfusions
Granulocyte concentrates are collected from single donors by use of a blood cell separator.
Each concentrate contains approximately 1010
granulocytes.
Granulocytes has to transfused as soon as possible no longer than 24 h.
When needed give 1000-2000 granulocytes/kg in volume of 15-20ml/kg.
The desired count must be maintained for 48 hours for therapeutic benefits
48
Guidelines for Pediatric Granulocyte Transfusions
CHILDREN AND ADOLESCENTS
• Neutrophils of <0.5 × 109/L and bacterial infection unresponsive to appropriate antimicrobial therapy
• Qualitative neutrophil defect and infection (bacterial or fungal) unresponsive to appropriate antimicrobial therapy
INFANTS WITHIN THE FIRST 4 MO OF LIFE
• Neutrophils of <3000/cumm (1st wk of life) or <1000 cumm (> 1st wk of life)
• Bone marrow having <10% nucleated neutrophils or peripheral blood having >70% immature polymorphs
49
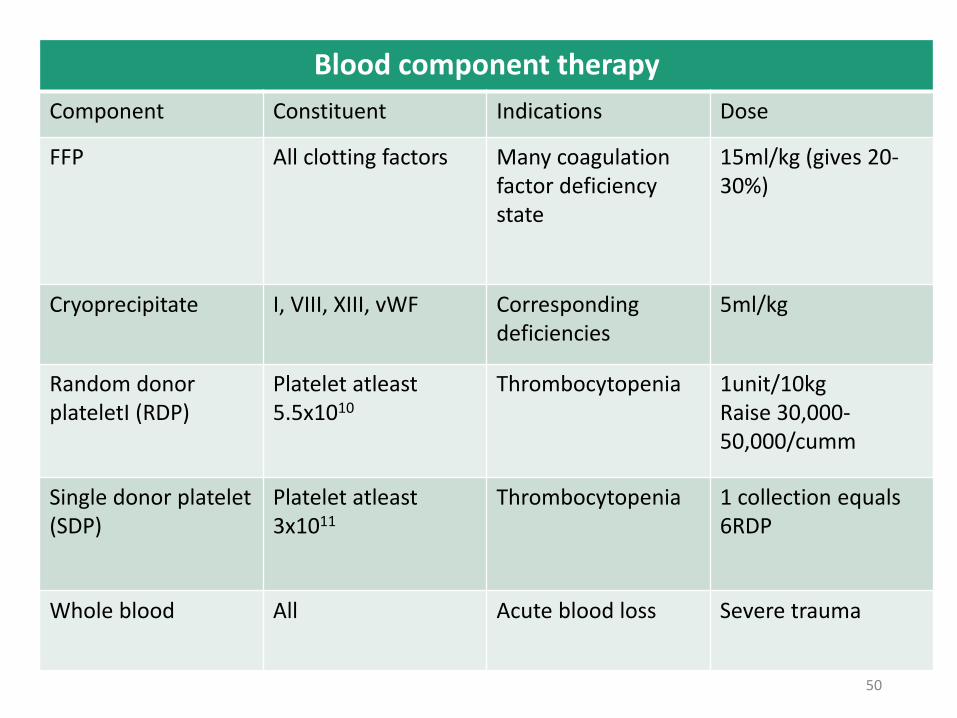
Blood component therapy
Component Constituent Indications Dose
FFP All clotting factors Many coagulationfactor deficiency state
15ml/kg (gives 20-30%)
Cryoprecipitate I, VIII, XIII, vWF Corresponding deficiencies
5ml/kg
Random donor plateletI (RDP)
Platelet atleast5.5x1010
Thrombocytopenia 1unit/10kgRaise 30,000-50,000/cumm
Single donor platelet (SDP)
Platelet atleast3x1011
Thrombocytopenia 1 collection equals 6RDP
Whole blood All Acute blood loss Severe trauma
50

51