bleeding in congenital hemangiomas: crusting as a clinical predictive sign and usefulness of...
TRANSCRIPT
Bleeding in Congenital Hemangiomas: Crustingas a Clinical Predictive Sign and Usefulness
of Tranexamic Acid
Julie Powell, M.D., F.R.C.P.C.,* Marie-Michele Blouin, M.D.,� Michele David, M.D.,
M.R.C.P.C.,� and Josee Dubois, M.D., F.R.C.P.C.§
*Division of Pediatric Dermatology, Department of Pediatrics, CHU Sainte-Justine, University of Montreal,Montreal, Quebec Canada, �Division of Dermatology, Centre Hospitalier Universitaire de Quebec, Laval
University, Quebec City, Montreal, Canada, �Division of Pediatric Hematology-Oncology, CHU Sainte-Justine,University of Montreal, Montreal, Quebec, Canada, §Department of Medical Imaging, CHU Sainte-Justine,
University of Montreal, Montreal, Quebec Canada
Abstract: We present two case reports of CH in which severe bleedingepisodes occurred during the first weeks of life and report the use of topicaltranexamic acid to control bleeding in this setting. Patient 1 was a full-termfemale infant who presented at birth with a large 7- by 6-cm CH of the fore-head showing a few millimeter-sized crusts. No active treatment except closefollow-up was advised. At 10 weeks of age, the size of the lesion havingspontaneously decreased more than 50%, she presented with severebleeding from a small crusted area. The bleeding was controlled using top-ical tranexamic acid, and except for a few minor, easily controlled bleedingepisodes in the following weeks, the lesion regressed more than 80%. Patient2 was a full-term male infant seen at 1 day of life for a 14- by 10-cm CH of theright knee with a few small, dark, superficial crusts. At 3 weeks of age, hewas hospitalized after severe bleeding from one of the crusted areas, with adrop in hemoglobin from 131 to 114 g ⁄ L. Bleeding was controlled usingtopical tranexamic acid, and compressive dressing. Because the lesion wasclinically a rapidly involuting CH, there was no need for embolization orsurgery. The presence of crusting in CH, even in the absence of frankulceration, is an ominous sign and can precede serious bleeding. Tranexa-mic acid, an antifibrinolytic agent that helps stabilize the clot, has proveduseful topically in controlling bleeding in CH.
Congenital hemangioma (CH) is a term that Boonet al introduced in 1996 to describe a group of vasculartumors that differ clinically and histopathologically fromthe common infantile hemangiomas (IH) (1–5).
Congenital hemangiomas are fully formed at birth,having undergone their proliferative phase in utero, donot undergo the typical postnatal evolutive patternof IH, and can be diagnosed prenatally using
Address correspondence to Julie Powell, M.D., Department ofPediatrics, Division of Dermatology, CHU Sainte-Justine, 3175chemin de la Cote Sainte-Catherine, Montreal (Quebec) H3T 1C5,Canada, or e-mail: [email protected].
DOI: 10.1111/j.1525-1470.2011.01517.x
182 � 2011 Wiley Periodicals, Inc.
Pediatric Dermatology Vol. 29 No. 2 182–185, 2012

ultrasonography (6). These tumors are rare, with anincidence of less than 3% of all hemangiomas (7). Theextensive work of the Boston and Paris vascular anom-alies teams led to the subdivision of CH into two groups(5): rapidly involuting CH (RICH), which regress muchmore rapidly than IH during the first year of life, andnoninvoluting CH (NICH), which persist lifelong, usu-ally requiring surgical excision. RICH and NICH sharesimilar clinical features; they have an almost equal sexdistribution, are usually solitary, have a similar averagediameter (£10 cm), and have a predilection for the samecutaneous locations (head or limbs near a joint). Color isviolaceous, with variable telangiectasia and a typicalsurrounding pale halo. Those CH rapidly involute andhave or develop central depression or rarely ulceration.Superficial bleeding is a frequent feature of ulceratedCHand generally involves small capillaries, but severebleeding has been reported in only four infants withRICH due to ulceration involving large vessels (4, 6, 8–10). Histopathologically, RICH and NICH differ fromIH by being uniformly glucose transporter (GLUT)1negative (1). In most infants with RICH, involution iscomplete, leaving anetodermic skin within the first 6–14 months of life, whereas NICH grow proportionallywith the child’s growth and never disappear. We reporttwo cases of CH that presented with significant bleedingfrom superficial areas of crusting in the neonatal period.Management was conservative in both cases, becausefeatures of RICH were present, and bleeding stoppedwith topical care. Topical tranexamic acid was used tocontrol any recurrent bleeding.
CASE 1
J.F. was a girl referred to us at 1 week of life for a largecongenital vascular tumor of the forehead that hadbeen noted prenatally on ultrasound (US). She was theproduct of a normal full-term pregnancy, and deliverywas uncomplicated. On physical examination, a 7- by6-cm violaceous tumor with peripheral pallor of the leftforehead was noted (Fig. 1), causing slight ptosis, butophthalmologic evaluation was normal. A few pinpointcrusts were noted on the lesion. Complete blood countwas normal. Ultrasound revealed a highly vascularizedlesion with arterial and venous components and int-ralesional arteriovenous microfistulae, suggestive ofRICH. At 10 weeks of age, although the lesion hadspontaneously regressed approximately 50% (Fig. 2),the infant was hospitalized after several episodes ofpulsatile bleeding from a tiny crusted area that she hadscratched, causing a drop in hemoglobin from 113 to90 g ⁄L within a few hours, with normal platelet countand coagulation profile. Because compression alone
was ineffective in controlling the bleeding, topical tra-nexamic acid was used. In the month after her hospi-talization, a few minor bleeding episodes were similarlyrapidly controlled using topical tranexamic acid used athome by her parents, and the lesion continued to re-gress. A biopsy performed at a later stage showedGLUT1-negative lobular capillary proliferation, com-patible with RICH. Now at age 2.5 years, the lesionhas continued to involute, but incompletely, suggestinga RICH ⁄NICH overlap (11).
Figure 1. Patient 1 (1 week of age). Large vascular tumor ofthe forehead with typical grayish halo and dark bluish areas atsuperior pole of the lesion.
Figure 2. Patient 1 (10 weeks of age). Appearance of thetumor at the time of bleeding, with pinpoint areas of crustingwithout frank ulceration.
Powell et al: Tranexamic Acid in Bleeding CH 183
CASE 2
F.D., a 1-day-old boy, was referred to our institution fora large congenital vascular tumor of the right knee thathad been diagnosed prenatally onUS as a probable CH.The baby was full term but was delivered by cesareansection because of breech presentation.
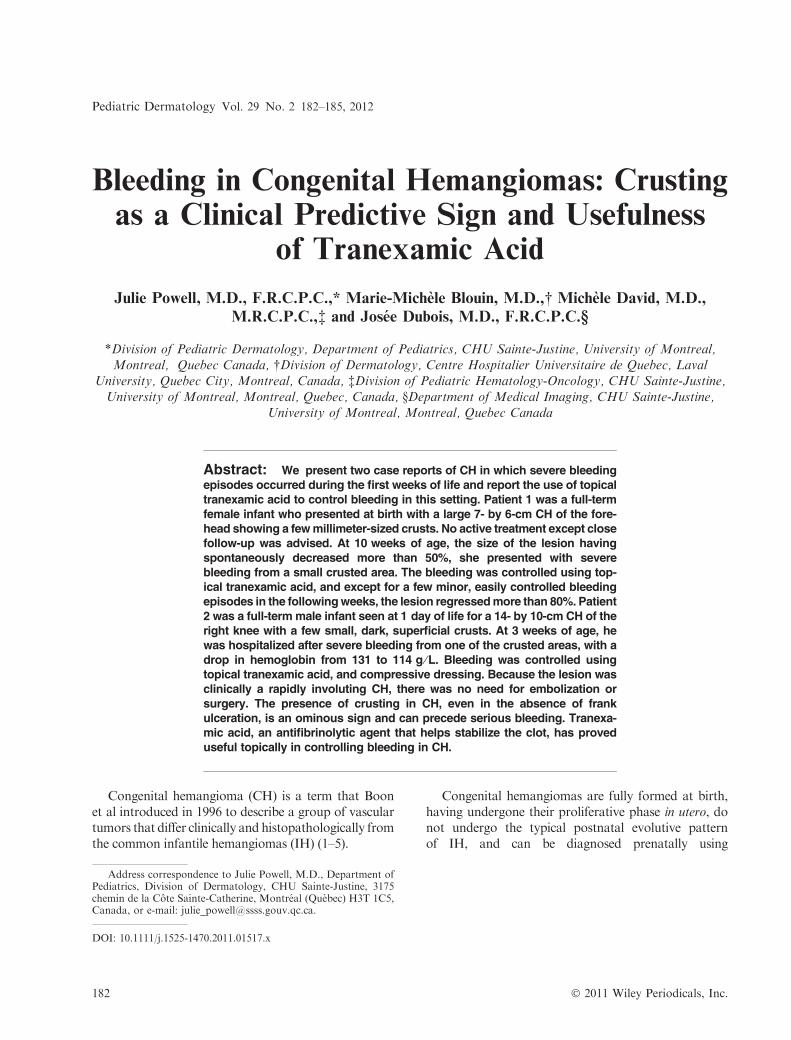
Physical examination revealed a large 14- by 10-cmviolaceous tumorwith a pale grayish peripheral halo anda few dark superficial crusted areas but no frank ulcer-ation (Fig. 3). Doppler US showed a richly vascularizedlesion with high systolic peaks and large venous andarterial vessels, compatiblewith aCH.At 3 weeks of age,he was hospitalized after a serious bleeding episodecaused a drop in hemoglobin from 131 to 114 g ⁄Lwithina few hours; platelets and coagulation profile were nor-mal. The tumor had regressed slightly since birth but stillhad superficial crusts but no frank ulceration. Com-pression alone failed to control the bleeding, bleeding
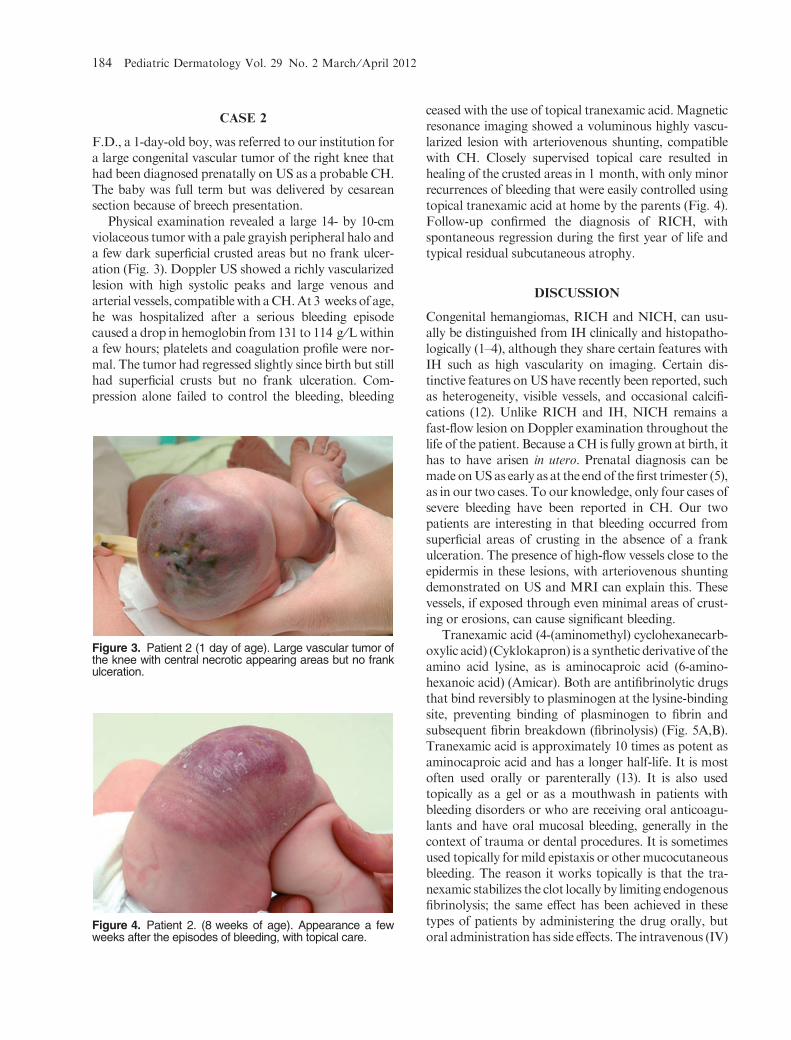
ceased with the use of topical tranexamic acid.Magneticresonance imaging showed a voluminous highly vascu-larized lesion with arteriovenous shunting, compatiblewith CH. Closely supervised topical care resulted inhealing of the crusted areas in 1 month, with only minorrecurrences of bleeding that were easily controlled usingtopical tranexamic acid at home by the parents (Fig. 4).Follow-up confirmed the diagnosis of RICH, withspontaneous regression during the first year of life andtypical residual subcutaneous atrophy.
DISCUSSION
Congenital hemangiomas, RICH and NICH, can usu-ally be distinguished from IH clinically and histopatho-logically (1–4), although they share certain features withIH such as high vascularity on imaging. Certain dis-tinctive features onUS have recently been reported, suchas heterogeneity, visible vessels, and occasional calcifi-cations (12). Unlike RICH and IH, NICH remains afast-flow lesion on Doppler examination throughout thelife of the patient. Because aCH is fully grown at birth, ithas to have arisen in utero. Prenatal diagnosis can bemadeonUSas early as at the endof the first trimester (5),as in our two cases. To our knowledge, only four cases ofsevere bleeding have been reported in CH. Our twopatients are interesting in that bleeding occurred fromsuperficial areas of crusting in the absence of a frankulceration. The presence of high-flow vessels close to theepidermis in these lesions, with arteriovenous shuntingdemonstrated on US and MRI can explain this. Thesevessels, if exposed through even minimal areas of crust-ing or erosions, can cause significant bleeding.
Tranexamic acid (4-(aminomethyl) cyclohexanecarb-oxylic acid) (Cyklokapron) is a synthetic derivative of theamino acid lysine, as is aminocaproic acid (6-amino-hexanoic acid) (Amicar). Both are antifibrinolytic drugsthat bind reversibly to plasminogen at the lysine-bindingsite, preventing binding of plasminogen to fibrin andsubsequent fibrin breakdown (fibrinolysis) (Fig. 5A,B).Tranexamic acid is approximately 10 times as potent asaminocaproic acid and has a longer half-life. It is mostoften used orally or parenterally (13). It is also usedtopically as a gel or as a mouthwash in patients withbleeding disorders or who are receiving oral anticoagu-lants and have oral mucosal bleeding, generally in thecontext of trauma or dental procedures. It is sometimesused topically formild epistaxis or othermucocutaneousbleeding. The reason it works topically is that the tra-nexamic stabilizes the clot locally by limiting endogenousfibrinolysis; the same effect has been achieved in thesetypes of patients by administering the drug orally, butoral administration has side effects. The intravenous (IV)
Figure 3. Patient 2 (1 day of age). Large vascular tumor ofthe knee with central necrotic appearing areas but no frankulceration.
Figure 4. Patient 2. (8 weeks of age). Appearance a fewweeks after the episodes of bleeding, with topical care.
184 Pediatric Dermatology Vol. 29 No. 2 March ⁄April 2012

preparation or a gel preparedwith crushed tablets can beused. In our patients, we used the IV preparation, undi-luted, on a compress for bleeding unresponsive to com-pression alone. Tranexamic acid also has had a goodefficacy and safety profile in treating severe Kasabach-Merritt syndrome in newborns (14–17). Although alsoreportedly effective in infantile hemangiomas, the casesdescribed in these referencesweremore likelykaposiformhemangioendotheliomas. In our cases, the favorablecontrol of bleeding with compression and topical tra-nexamic acid, together with the rapid healing of thecrusted eroded areas in tumors that had already startedto involute, allowed us to avoid embolization or emer-gency surgical excision.
CONCLUSION
The presence of crusting or erosions in congenital vas-cular tumors suspected of being RICH or NICH is anominous sign that can precede episodes of severe bleed-ing. Early US evaluation is warranted to identify asso-ciated large fast-flow vessels. Close follow-up ismandatory, as is supervised wound care. Topicaltranexamic acid can be a useful and safe adjunct incontrolling the bleeding from these lesions and inavoidingmore aggressive treatment, especially in RICH.
REFERENCES
1. North PE,WanerM, James CA et al. Congenital nonpro-gressive hemangioma: a distinct clinicopathologic entityunlike infantile hemangioma. Arch Dermatol 2001;137:1607–1620.
2. Berenguer B, Mulliken JB, Enjolras O et al. Rapidlyinvoluting congenital hemangioma: clinical and histopath-ologic features. Pediatr Dev Pathol 2003;6:495–510.
3. North PE, Waner M, Buckmiller L et al. Vascular tumorsof infancy and childhood: beyond capillary hemangioma.Cardiovasc Pathol 2006;15:303–317.
4. Enjolras O, Picard A, Soupre V. Hemangiomes congenit-aux et autre tumeurs vasculaires infantiles rares (Congen-ital hemangiomas and other rare infantile vasculartumors). Ann Chir Plast Esthet 2006;51:339–346.
5. Boon LM, Enjolras O, Mulliken JB. Congenital heman-gioma: evidence of accelerated involution. J Pediatr 1996;128:329–335.
6. Brix M, Soupre V, Enjolras O et al. Diagnostic antenataldes RICH (rapidly involuting congenital hemangiomas).Antenatal diagnosis of rapidly involuting congenitalhemangiomas (RICH). Rev Stomatol Chir Maxillofac2007;108:109–114.
7. North PE, Waner M, Mizeracki A et al. GLUT1: a newlydiscovered immunohistochemical marker for juvenilehemangiomas. Hum Pathol 2000;31:11–22.
8. Konez O, Burrows PE, Mulliken JB et al. Angiographicfeatures of rapidly involuting congenital hemangioma(RICH). Pediatr Radiol 2003;33:15–19.
9. Agesta N, Boralevi F, Sarlangue J et al. Life-threateninghaemorrhage as a complication of a congenital haemang-ioma. Acta Paediatr 2003;92:1216–1218.
10. Nakada K, Kawada T, Fujioka T et al. Hemangioma ofthe upper arm associated with massive hemorrhage in aneonate. Surg Today 1993;23:273–276.
11. Mulliken JB, Enjolras O. Congenital hemangiomas andinfantile hemangioma:missing links. JAmAcadDermatol2004;50:875–882.
12. Gorincour G, Kokta V, Rypens F et al. Imaging charac-teristics of two subtypes of congenital hemangiomas:rapidly involuting congenital hemangiomas and non-involuting congenital hemangiomas. Pediatr Radiol2005;35:1178–1185.
13. Mannucci PM. Hemostatic drugs. N Engl J Med 1998;339:245–253.
14. HannaBD,BernsteinM.Tranexamic acid in the treatmentof Kasabach-Merritt syndrome in infants. Am J PediatrHematol Oncol 1989;11:191–195.
15. Morad AB, McClain KL, Ogden AK. The role oftranexamic acid in the treatment of giant hemangiomasin newborns. Am J Pediatr Hematol Oncol 1993;15:383–385.
16. Smith SW, Carruthers JD. Intractable periocular heman-gioma of infancy. Can J Ophthalmol 1985;20:220–224.
17. Bell AJ, Chisholm M, Hickton M. Reversal of coagulop-athy in Kasabach-Merritt syndrome with tranexamic acid.Scand J Haematol 1986;37:248–252.
A
B
Figure 5. (A) Mechanism of action of tranexamic acid withactivation of plasminogen on the fibrin surface by binding tolysine-binding site, which changes plasminogen in plasmin,its activated form. Plasmin then degrades fibrin into fibrin-degradation products. (B) Tranexamic acid blocks the lysine-binding site on plasminogen, preventing the activation ofplasminogen, although some plasmin generation occurs.(Adapted with permission from Mannucci PM. Hemostaticdrugs. N Engl J Med 1998;339:245–253).
Powell et al: Tranexamic Acid in Bleeding CH 185