bleeding disorders / orthodontic courses by indian dental academy
TRANSCRIPT
Introduction
Bleeding disorders is a general term for a wide range of medical problems that lead to poor blood clotting and continuous bleeding. Doctors also call them with such terms as coagulopathy, abnormal bleeding and clotting disorders.
When someone has a bleeding disorder they have a tendency to bleed longer. The disorders can result from defects in the blood vessels or from abnormalities in the blood itself. The abnormalities may be in blood clotting factors or in platelets.
Blood clotting, or coagulation, is the process that controls bleeding. It changes blood from a liquid to a solid. It's a complex process involving as many as 20 different plasma proteins, or blood clotting factors. Normally, a complex chemical process occurs using these clotting factors to form a substance called fibrin that stops bleeding. When certain coagulation factors are deficient or missing, the process doesn't occur normally.
HistoryBleeding disorders have been recognized all the way back to ancient times. Though not named, they were referenced extensively. In the Talmud, a collection of Jewish Rabbinical writings from the 2nd century AD, it was written that male babies did not have to be circumcised if two brothers had already died from the procedure. A 12th century Arab physician named Albucasis also wrote about a family in which males died of excessive bleeding from minor injuries. Bleeding disorders like hemophilia have been recognized for hundreds of years to "run in" families.In the U.S., the transmission of hemophilia from mothers to sons was first described in the early 1800s. In 1803, a Philadelphia physician named Dr. John Conrad Otto wrote an account of "a hemorrhagic disposition existing in certain families." He recognized that a particular bleeding condition was hereditary and affected males. He traced the disease back through three generations to a woman who had settled near Plymouth, New Hampshire, in 1720. The word "Hemophilia" first appeared in a description of a bleeding disorder condition at the University of Zurich in 1828.
A Royal Disease
Hemophilia has often been called the "Royal Disease." This is because Queen Victoria, Queen of England from 1837 to 1901, was a carrier. She passed the disease on to several royal families. Her eighth child, Leopold, had hemophilia and suffered from frequent hemorrhages, which were reported in the British Medical Journal in 1868. Leopold died of a brain hemorrhage at the age of 31, but not before he had children. His daughter, Alice, was a carrier and her son, Viscount Trematon, also died of a brain hemorrhage in 1928.
Nicholas and Alexandra Hemophilia played an important role in the Russian Royal family, as well. Two of Queen Victoria's daughters, Alice and Beatrice, were carriers of hemophilia. They passed the disease on to the Spanish, German and Russian royal families. Alexandra, Queen Victoria's granddaughter, married Nicholas, the Tsar of Russia in the early 1900's. Alexandra was a carrier of hemophilia. Her first son,
1
Alexei, was a hemophiliac. Nicholas and Alexandra were pre-occupied by the health problems of their son at a time when Russia was in turmoil. A monk, Rasputin, gained great influence in the Russian court, partly because he was the only one able to help the young Tsarevich Alexei. He used hypnosis to relieve Alexei's pain. The use of hypnosis not only relieved pain, but may have also helped slow or stop the boy's hemorrhages. The illness of the heir to the Tsar's throne, the strain it placed on the Royal family, and the power wielded by the mad monk Rasputin were all factors leading to the Russian Revolution of 1917. In 1916, the 45-year old faith-healer Rasputin was killed at Petrograd at the hands of a group of noblemen bent on ridding Russia of the monk's corrupting influence on Nicholas II and Alexandra.
Finding the Cause
In the 20th century doctors looked for the cause of excessive bleeding. Until then, they had believed that the blood vessels of hemophiliacs were simply more fragile.
1925 Although it is probably the most common hereditary bleeding disorder (affecting approximately 1% to 2% of the population), von Willebrand disease was not recognized until 1925.
1930s Doctors looked at defective platelets as the likely cause of bleeding disorders and hemophilia. Then in 1937, Patek and Taylor, two doctors at Harvard, found they could correct the clotting problem by adding a substance which came from the plasma in blood. They called it "anti-hemophilic globulin."
1944 Pavlosky, a doctor from Buenos Aires, Argentina, did a lab test which showed that blood from one hemophilic patient could correct the clotting problem in a second and vice-versa. He had stumbled upon two persons with hemophilia each with a deficiency in different proteins - factor VIII and factor IX. This led to the recognition in 1952 of hemophilia A and hemophilia B as two distinct diseases.
Identifying Clotting Factors
1960s In the 1960s the clotting factors were identified and named. An article in Nature in 1964 described the clotting process in detail. The interaction of the different factors in blood clotting was named the "coagulation cascade."
In the 1950s and early 1960s, hemophilia and other bleeding problems were treated with whole blood or fresh plasma. Unfortunately, there wasn't enough of the factor VIII or IX proteins in these blood products to stop serious internal bleeding. Most people with severe hemophilia and some people with mild or moderate hemophilia died in childhood or early adulthood. The most common causes of death were bleeding in vital organs, especially the brain, and bleeding after minor surgery or after an injury.
2

Those who survived were usually crippled by the long-term effects of repeated hemorrhages into the joints. The pressure of massive bleeding into joints and muscles made hemophilia one of the most painful diseases known to medicine.
Then, in the 1960s, cryoprecipitate was discovered by Dr. Judith Pool. Cryoprecipitate is the factor-rich component of blood, containing concentrated factor VIII. Dr. Pool found that the sludge on top of thawing plasma was rich in factor VIII. For the first time, enough factor VIII clotting factor could be infused to control serious bleeding. Even surgery became possible. This medical breakthrough ended the need for high-volume whole plasma transfusions for persons with hemophilia
1970s Then, later in the 1960s and early 1970s, concentrates containing factor VIII and IX began to be available. These freeze-dried powdered concentrates could be kept at home and used as needed. They revolutionized hemophilia care. Persons with hemophilia were now independent of hospitals. They could travel, hold steady jobs and hope to lead normal lives. Tragically, these same blood products carried blood-borne viruses like hepatitis C and HIV. Many persons with hemophilia were infected.
1990s In the 1990s, modern treatment, using safer factor concentrates, has again improved the outlook. Most children born with hemophilia today can look forward to long, healthy, active and productive lives. Recent progress includes: • New clotting factor products and drugs such as desmopressin acetate (also known as DDAVP, used to treat mild-to-moderate hemophilia A and von Willebrand disease)
• New, synthetic (not derived from plasma) clotting products that take advantage of recombinant technologies
• Better screening methods to detect and remove viruses and other agents from factor concentrates and blood products
• Improved surgical options
• Advanced genetic testing methods
• Medically supervised home-infusion therapy
• Prophylactic treatment
HEMOSTASISI. PLATELETS:Origin:
Platelets are developed in bone marrow from megakaryocyte.
3

Pluripotent stem cellPromegakaryoblastMegakaryoblastMegakaryocytePlatelets 1. FUNCTIONS :1. Damage to vessel releases 5HT, TXA2 2. Platelet adhesion, platelet aggregation and platelet plug formation. 3. PF3 - which helps in clotting. 4. Helps in clot retraction5. PDGF - Helps in growth and multiplication of vascular endothelial cells, vascular submucosal cells and
fibroblasts required for repair of damaged walls.
Life span: 7-14 daysSite of destruction : SpleenNormal count : 1.5 - 4.5 lacks / ccIncrease in count: ThrombocytosisDecrease in count: Thrombocytopenia Decrease in platelet count below 40,000is associated with hemorrhagic disorders.
2 a) Physiological Variations :1. Seasonal - Count is more during winter season. 2. Pregnancy - Count decrease3. Exercise, excitement, injection of adrenaline, high altitude - Increased count.
b. Pathological Variations :1. Increased platelet count seen after splenectomy idiopathic. 2. Decreased platelet count is seen in - Viral infection- Idiopathic- Aplastic anaemia
II. COAGULATION : Primary hemostasis is platelet plug formation. Secondary hemostasis is coagulation. Coagulation
is the convertion of fibrinogen to fibrin in the presence of thrombin.
4

Clotting Factors: I. FibrinogenII. ProthrombinIII. Tissue thromboplastinIV. CalciumV. Labile factor - ProaccelerinVI. Does not existVII. Stable factor - ProconvertinVIII. AIIG or AHFIX. Christmas factorX. Stuart Prower factor XI. PTA - Plasma thromboplastin antecedentXII. Hageman factor XIII. Fibrin stabilizing factor
The coagulation proteins are divided into 3 groups on the basis of their biochemical properties and function. I. Vitamin K dependent coagulation proteinsII. Contact proteinsIII. Thrombin sensitive proteins
I. These are prothrombin, factor VII, factor IX, and Factor X. These are synthesized in liver. II. These are XII, prekallikrein, factor XI and HMWC. They are produce in liver. III. They are fibrinogen, V, VIII, XIII. 2) There are 3 essential steps in coagulation. 1. Formation of prothrombin activator in response to vessel or tissue damage. 2. Conversion of prothrombin to thrombin3. Conversion of fibrinogen to fibrin SYNTHESIS OF PROTHROMBIN ACTIVATOR:2 mechanisms. 1. Extrinsic mechanism2. Intrinsic mechanism 3) EXTRINSIC MECHANISM:
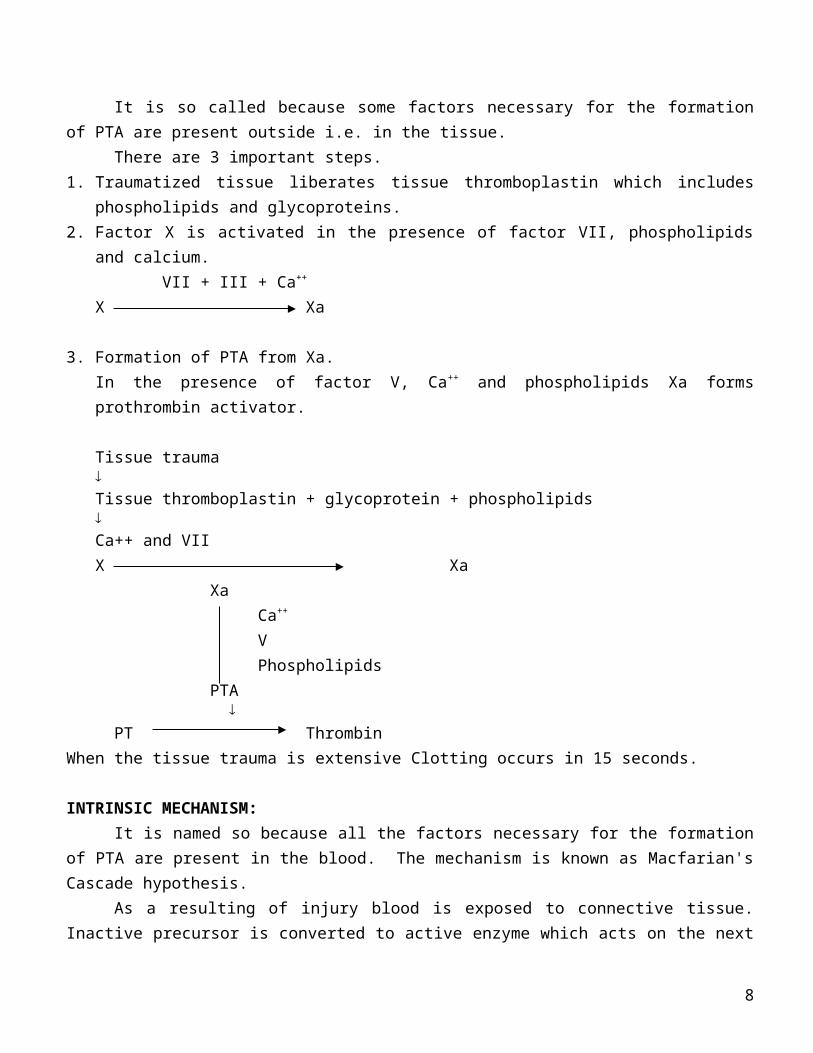
It is so called because some factors necessary for the formation of PTA are present outside i.e. in the tissue.
There are 3 important steps. 1. Traumatized tissue liberates tissue thromboplastin which includes phospholipids and glycoproteins. 2. Factor X is activated in the presence of factor VII, phospholipids and calcium.
VII + III + Ca++ X Xa
5

3. Formation of PTA from Xa. In the presence of factor V, Ca++ and phospholipids Xa forms prothrombin activator.
Tissue traumaTissue thromboplastin + glycoprotein + phospholipidsCa++ and VII X Xa
Xa Ca++ VPhospholipids
PTA
PT ThrombinWhen the tissue trauma is extensive Clotting occurs in 15 seconds.
INTRINSIC MECHANISM:It is named so because all the factors necessary for the formation of PTA are present in the blood.
The mechanism is known as Macfarian's Cascade hypothesis. As a resulting of injury blood is exposed to connective tissue. Inactive precursor is converted to
active enzyme which acts on the next precursor to form next active enzyme and thus so on. Thus sequence of changes occurs. 1. Trauma to vessel wall causes factor XII. HMWK and PK to form a complex with vascular and
subendothelial collagen. After binding to HMWK inactive factor XII is converted to active XII (XIIa). XIIa converts PK to kallikrein activates conversion of XII to XIIa. This is positive feed back mechanism.
2. XIIa activates XI to XI a3. XIa activates IX to IXa in presence of calcium. 4. IXa along with VII, Ca++, platelet phospholipids converts X to Xa.5. Xa in the presence V Ca+2 and platelet phospholipid forms PTA. 6. Except in the first two steps Ca is necessary for clotting. Formation of PTA by intrinsic mechanism
occurs in 4-8 minutes. Once PTA formed clot is formed in 10-30 seconds.
Fibrin monomer forms the fibrin threads, these threads are not cross linked. Hence clot is weak. In the presence of factor XIII a firm polymer is formed.
INTRINSIC EXTRINSICSurface contact Tissue damage
6

XII XIIa
XI XIa Tissue factor
IX IXa Ca++
Ca++ VIIVIII
Phospholipid X Xa
Ca++ Phospholipid V
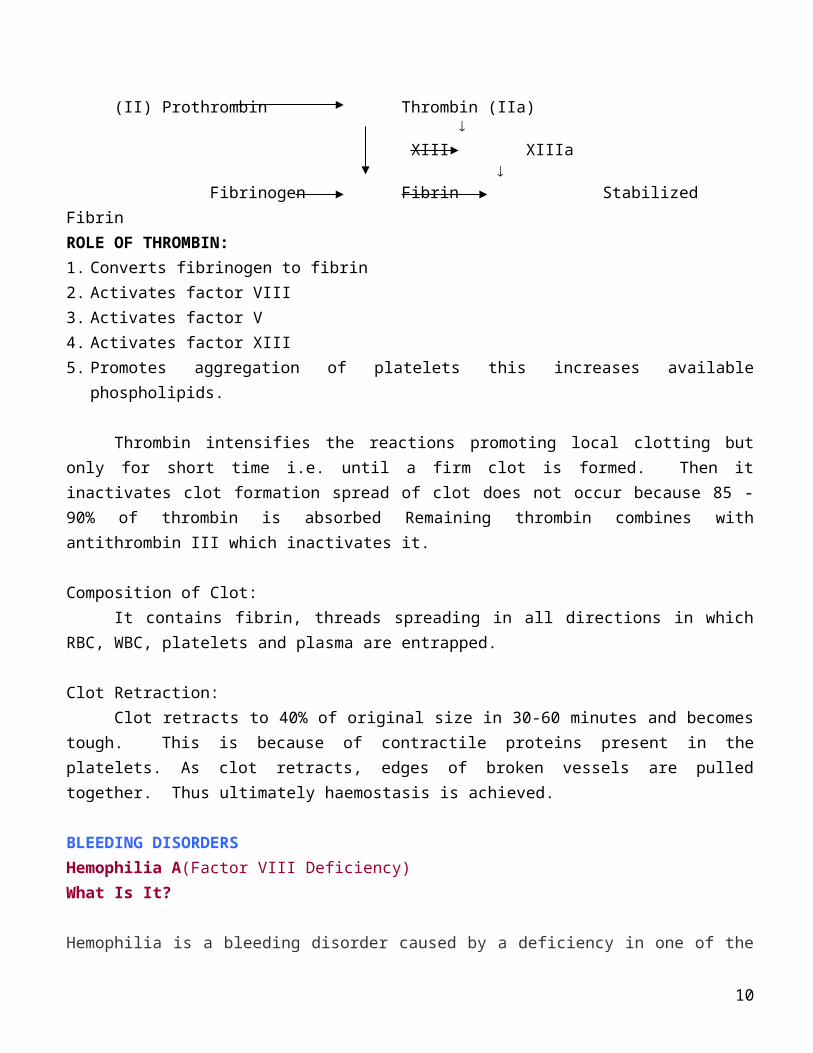
(II) Prothrombin Thrombin (IIa)
XIII XIIIa
Fibrinogen Fibrin StabilizedFibrin ROLE OF THROMBIN: 1. Converts fibrinogen to fibrin 2. Activates factor VIII3. Activates factor V4. Activates factor XIII5. Promotes aggregation of platelets this increases available phospholipids.
Thrombin intensifies the reactions promoting local clotting but only for short time i.e. until a firm clot is formed. Then it inactivates clot formation spread of clot does not occur because 85 - 90% of thrombin is absorbed Remaining thrombin combines with antithrombin III which inactivates it.
Composition of Clot: It contains fibrin, threads spreading in all directions in which RBC, WBC, platelets and plasma are
entrapped.
Clot Retraction:Clot retracts to 40% of original size in 30-60 minutes and becomes tough. This is because of
contractile proteins present in the platelets. As clot retracts, edges of broken vessels are pulled together. Thus ultimately haemostasis is achieved.
BLEEDING DISORDERSHemophilia A(Factor VIII Deficiency)
7
What Is It?
Hemophilia is a bleeding disorder caused by a deficiency in one of the blood clotting factors. Hemophilia A (often called classic hemophilia) accounts for about 80% of all hemophilia cases. It is a deficiency in clotting factor VIII.Hemophilia A is a hereditary disorder in which the clotting ability of the blood is impaired and excessive bleeding results. Small wounds and punctures are usually not a problem, but uncontrolled internal bleeding can result in pain and swelling and permanent damage, especially to joints and muscles.
Severity of symptoms can vary and severe forms become apparent early on. Prolonged bleeding is the hallmark of hemophilia A and typically occurs when an infant is circumcised. Additional bleeding manifestations make their appearance when the infant becomes mobile. Mild cases may go unnoticed until later in life when there is excessive bleeding and clotting problems in response to surgery or trauma. Internal bleeding may happen anywhere, and bleeding into joints is common. The incidence of hemophilia A is one in 10,000 live male births. About 17,000 Americans have hemophilia. Women may have it, but it's very rare. With treatment and management, the outcome is good. Most men with hemophilia are able to lead relatively normal lives.
Inheritance Pattern Hemophilia A is caused by an inherited sex-linked recessive trait with the defective gene located on the X chromosome. Females are carriers of this trait. Fifty percent of the male offspring of female carriers have the disease, and 50% of their female offspring are carriers. All female children of a male with hemophilia are carriers of the trait. One third of all cases of hemophilia A occur when there is no family history of the disorder. In these cases, hemophilia develops as the result of a new or spontaneous gene mutation.Genetic counseling may be advised for carriers. Female carriers can be identified by testing.A woman is definitely a hemophilia carrier if she is: • the biological daughter of a man with hemophilia; • the biological mother of more than one son with hemophilia;• the biological mother of one hemophilic son who has at least one other blood relative with hemophilia. A woman may or may not be a hemophilia carrier if she is: • the biological mother of one son with hemophilia;• the sister of a male with hemophilia; • an aunt, cousin or niece of an affected male related through maternal ties; • the biological grandmother of one grandson with hemophilia.The only way a woman could ever have hemophilia is if her father has it and her mother carries the gene. Women who are carriers can also be symptomatic carriers, whereby they do experience factor deficiencies.
Symptoms & Diagnosis
8

Hemophilia is caused by several different gene abnormalities. The severity of the symptoms of hemophilia A depends on how a particular gene abnormality affects the activity of factor VIII. When the activity is less than 1 percent of normal, episodes of severe bleeding occur and recur for no apparent reason.
Symptoms include:• Bruising• Spontaneous bleeding• Bleeding into joints and associated pain and swelling• Gastrointestinal tract and urinary tract hemorrhage• Blood in the urine or stool • Prolonged bleeding from cuts, tooth extraction, and surgery People whose clotting activity is 5 percent of normal may have only mild hemophilia. They rarely have unprovoked bleeding episodes, but surgery or injury may cause uncontrolled bleeding, which can be fatal. Milder hemophilia may not be diagnosed at all, although some people whose clotting activity is 10 to 25 percent of normal may have prolonged bleeding after surgery, dental extractions, or a major injury.Generally, the first bleeding episode occurs before 18 months of age, often after a minor injury. A child who has hemophilia bruises easily. Even an injection into a muscle can cause bleeding that results in a large bruise (hematoma). Recurring bleeding into the joints and muscles can ultimately lead to crippling deformities. Bleeding can swell the base of the tongue until it blocks the airway, making breathing difficult. A slight bump on the head can trigger substantial bleeding in the skull, causing brain damage and death. A doctor may suspect hemophilia in a child whose bleeding is unusual. A laboratory analysis of blood samples can determine whether the child's clotting is abnormally slow. If it is, the doctor can confirm the diagnosis of hemophilia A and can determine the severity by testing the activity of factor VIII. Treatments Hemophilia is treated by infusing the missing clotting factor. The amount infused depends upon the severity of bleeding, the site of the bleeding, and the size of the patient. In the past, mild hemophilia A was typically treated with infusion of cryoprecipitate or desmopressin acetate (DDAVP), which causes release of factor VIII that, is stored within the body on the lining of blood vessels. Today, experts recommend desmopressin injection or Stimate nasal spray. Clotting factors are found in plasma and, to a greater extent, in plasma concentrates. Some plasma concentrates are intended for home use and can be self-administered, either on a regular basis to prevent bleeding or at the first sign of bleeding. More often, they are administered three times a day, but both the dose and frequency depend on the severity of the bleeding problem. The dose is adjusted according to the results of periodic blood tests. During a bleeding episode, more clotting factors are needed. To prevent a bleeding crisis, people with hemophilia and their families can be taught to administer factor VIII concentrates at home at the first signs of bleeding. People with severe forms of the disease may need regular prophylactic infusions, which bring factor levels higher than 1% to prevent bleeds.
Depending on the severity of the disease, DDAVP or factor VIII concentrate may be given prior to dental
9
extractions and surgery to prevent bleeding. Immunization with hepatitis B vaccine is necessary because of the increased risk of exposure to hepatitis due to frequent infusions of blood products.Gene therapy and fetal tissue implant techniques are under study as possible treatments.People who have hemophilia should avoid situations that might cause bleeding. They should be conscientious about dental care so they won't need to have teeth extracted. People who have hemophilia should also avoid certain drugs that can aggravate bleeding problems:• Aspirin • Heparin • Warfarin • Certain analgesics such as nonsteroidal anti-inflammatory drugs Treatment should be coordinated by a healthcare practitioner who is expert in the field, such as a hematologist of hemophilia treatment center nurse. The National Hemophilia Foundation's Medical and Scientific Advisory Council (MASAC) made recommendations for treatment of hemophilia in November of 1999. They include: • Factor VIII products for patients who are HIV seronegative, including Recombinant factor VIII, especially for young and newly diagnosed patients who have not received any blood or plasma-derived products. • Immunoaffinity purified factor VIII concentrates for patients who are HIV seropositive. • Cryoprecipitate is not recommended because of the risk of HIV and hepatitis infection. Despite greatly improved screening and purification for viral inactivation in blood products, cryoprecipitate can still contain viruses. • Mild hemophilia A should be treated with desmopressin, in a DDAVP injection or Stimate nasal spray.
Complications • Chronic joint deformities, caused by recurrent bleeding into the joint, may be managed by an orthopedic specialist• Intracerebral hemorrhage is another possible complication.
Some persons with hemophilia develop antibodies to transfused factor VIII. As a result, the transfusions are ineffective. If antibodies are detected in blood samples, the dosage of the plasma concentrates may be increased, or different types of clotting factors or drugs to reduce the antibody levels may be used. In the past, the plasma concentrates carried the risk of transmitting blood-borne diseases such as hepatitis and AIDS. About 60 percent of persons with hemophilia who were treated with plasma concentrates in the early 1980s were infected with HIV. However, the risk of transmitting HIV infection through plasma concentrates has been virtually eliminated by today's use of screened and processed blood and a genetically engineered factor VIII (Recombinant).
Hemophilia B (Factor IX Deficiency)What Is It?
10
Hemophilia is a bleeding disorder caused by a deficiency in one of the blood clotting factors. Hemophilia B (also called "Christmas disease" after Stephen Christmas, a British boy in the 20th century who was first diagnosed with it) is a deficiency in clotting factor IX. Hemophilia A is seven times more common than hemophilia B. The incidence of hemophilia B is one in 34,500 men. Hemophilia B is a hereditary disorder in which the clotting ability of the blood is impaired and prolonged bleeding results. Small wounds and punctures are usually not a problem. But uncontrolled internal bleeding can result in pain, swelling and permanent damage, especially to joints and muscles. The outcome is good with treatment and management. Most people with hemophilia B are able to lead relatively normal lives.
Inheritance PatternHemophilia B is caused by an inherited sex-linked recessive trait with the defective gene located on the X chromosome. Females are carriers of this trait. Fifty percent of the male offspring of female carriers will have the disease, and 50% of their female offspring will be carriers. All female children of a male with hemophilia will be carriers of the trait. One fifth of all cases of hemophilia B occur when there is no family history of the disorder. In these cases, hemophilia develops as the result of a new or spontaneous gene mutation. Genetic counseling may be advised for carriers. Female carriers can be identified by testing. A woman is definitely a hemophilia carrier if she is: • the biological daughter of a man with hemophilia; • the biological mother of more than one son with hemophilia; • theBiological mother of one son with hemophilia and has at least one otherblood relative with hemophilia.A woman may or may not be a hemophilia carrier if she is:• the biological mother of one son with hemophilia; • the sister of a male with hemophilia;• an aunt, cousin or niece of an affected male related through maternal ties;• the biological grandmother of one grandson with hemophilia.Symptoms and Diagnosis Hemophilia is caused by several different gene abnormalities. The severity of hemophilia B symptoms depends on how a particular gene abnormality affects the activity of factor IX. When the activity is less than 1% of normal, episodes of prolonged bleeding may occur for no apparent reason. Severity of symptoms can vary, but severe forms become apparent early on. Prolonged bleeding is the disease's hallmark and typically manifests itself when an infant is circumcised. Additional bleeding manifestations make their appearance when the infant becomes mobile. Mild cases may go unnoticed until later in life, when they occur in response to surgery or trauma. Internal bleeding may occur anywhere and bleeding into joints is common. Risk factors are a family history of bleeding and being male. The incidence of hemophilia B is one in 34,500 men. Symptoms include:
11

• Nose bleeds • Bruising • spontaneous bleeding• bleeding into joints and associated pain and swelling• Gastrointestinal tract and urinary tract hemorrhage • Blood in the urine or stool• prolonged bleeding from cuts, tooth extraction and surgery• prolonged bleeding following circumcision
People whose clotting activity is 5% of normal may have only mild hemophilia. They rarely have unprovoked bleeding episodes, but surgery or injury may cause uncontrolled bleeding, which can be fatal. Milder hemophilia may not be diagnosed at all, although some people whose clotting activity is 10% to 25% of normal may bleed excessively after surgery, dental extractions or a major injury.
Generally, the first bleeding episode occurs before 18 months of age, often after a minor injury. A child who has hemophilia bruises easily. Even an injection into a muscle can cause bleeding that results in a large bruise (hematoma). Continuous bleeding into the joints and muscles can ultimately lead to crippling deformities. Bleeding can swell the base of the tongue until it blocks the airway, making breathing difficult. A slight bump on the head can trigger substantial bleeding in the skull, causing brain damage and death.
A doctor may suspect hemophilia in a child whose bleeding is unusual. A laboratory analysis of blood samples can determine whether the child's clotting is abnormally slow. If it is, the doctor can confirm the diagnosis of hemophilia and determine the severity by testing the activity of factor IX. Coagulation studies involving many tests are performed if the person tested is the first one in the family to have the bleeding disorder. Once the defect has been identified, other family members will need less testing to diagnose the disorder.
Treatments Like hemophilia A, hemophilia B is typically treated by infusing the missing clotting factor. The amount infused depends upon the severity of bleeding, the site of the bleeding and the size of the patient. A hepatitis B vaccine is recommended for individuals with hemophilia B because they are at increased risk of developing hepatitis due to exposure to blood products. Clotting factors are found in plasma and, to a greater extent, in plasma concentrates. Some plasma concentrates are intended for home use and can be self-administered, either on a regular basis to prevent bleeding or at the first sign of bleeding. More often, they are administered three times a week (prophylaxis), but both the dose and frequency depend on the severity of the bleeding problem. The dose is adjusted according to the results of periodic blood tests. During a bleeding episode, more clotting factors are needed. Treatment should be coordinated by a healthcare practitioner who is an expert on the disease.
To prevent a bleeding crisis, people with hemophilia and their families can be taught to administer factor
12

IX concentrates at home at the first signs of bleeding. People with severe forms of the disease may need regular prophylaxis infusions two to three times a week. Depending on the severity of the disease, factor IX concentrate may be given prior to dental extractions and surgery to prevent bleeding.
Gene therapy and fetal tissue implant techniques are under study as possible treatments.
People who have hemophilia should avoid situations that might provoke bleeding. They should be conscientious about dental care so they won't need to have teeth extracted. If people who have milder forms of hemophilia need to have dental or other surgery, the drug desmopressin acetate (DDAVP) may be given to improve clotting temporarily so that transfusions can be avoided.
People who have hemophilia should also avoid certain drugs that can aggravate bleeding problems:• aspirin • heparin • warfarin • certain analgesics, such as nonsteroidal antiinflammatory drugsThe National Hemophilia Foundation's Medical and Scientific Advisory Council (MASAC) made recommendations for treatment of hemophilia B inNovember of 1999. They include• Recombinant factor IX products for patients who are HIV seronegative, especially for young and newly diagnosed patients who have not received any blood or plasma-derived products.
• Today, plasma-derived factor IX products offer greatly reduced risk for HIV and hepatitis B and C transmission, but there is still some risk. Dry heating, solvent-detergent treatment, vapor treatment and sodium thiocyanate plus ultrafiltration and are all effective purification steps, but there remains a slight possibility of viral transmission. • Patients who are HIV-seropositive should also be treated with high purity products such as immunoaffinity purified and recombinant factor VIII products. • For patients with inhibitors to factors VIII and IX, there is Recombinant Factor VIIa (NovoSeven). Produced by baby hamster kidney cells, no human albumin or other proteins are used in its production, reducing virus risk. There is also Porcine factor VIII (Hyate C) and activated prothrombin complex concentrates.
Complications • Chronic joint deformities, caused by recurrent bleeding into the joint, may be managed by an orthopedic specialist. • Intracerebral hemorrhage may also occur. • Thrombosis may occur following use of factor IX concentrate.
Some persons with hemophilia develop antibodies to transfused factor IX. As a result, transfusions become
13
ineffective. If antibodies are detected in blood samples, the dosage of the plasma concentrates may be increased, or different types of clotting factors or drugs to reduce the antibody levels may be used.
In the past, plasma concentrates carried the risk of transmitting blood-borne diseases such as hepatitis and AIDS. About 60% of persons with hemophilia who were treated with plasma concentrates in the early 1980s were infected with HIV. However, the risk of transmitting HIV infection through plasma concentrates has been virtually eliminated by today's use of screened and processed blood.
Von Willebrand DiseaseWhat Is It? Von Willebrand disease is a hereditary deficiency or abnormality of the von Willebrand factor in the blood, a protein that affects platelet function. It's the most common hereditary disorder of platelet function, affecting both women and men. The disease is estimated to occur in 1% to 2% of the population. The disease was first described by Erik von Willebrand, a Finnish physician who reported a new type of bleeding disorder among island people in Sweden and Finland. In von Willebrand disease, blood platelets don't stick to holes in blood vessel walls. Platelets are tiny particles in the blood that clump together at the site of an injury to prepare for the formation of a blood clot. Von Willebrand factor causes them to bind to areas of a blood vessel that are damaged. If there is too little von Willebrand factor or the factor is defective, platelets do not gather properly when a blood vessel is injured. Von Willebrand factor is found in plasma, platelets and blood vessel walls. When the factor is missing or defective, the first step in plugging a blood vessel injury (platelets adhere to the vessel wall at the site of the injury) doesn't take place. As a result, bleeding doesn't stop as quickly as it should, although it usually stops eventually. There are no racial or ethnic associations with the disorder. A family history of a bleeding disorder is the primary risk factor. Researchers have identified many variations of the disease, but most fall into the following classifications
• Type I: This is the most common and mildest form of von Willebrand disease. Levels of von Willebrand factor are lower than normal, and levels of factor VIII may also be reduced. • Type II: In these people, the von Willebrand factor itself has an abnormality. Depending on the abnormality, they may be classified as having Type IIa or Type IIb. In Type IIa, the level of von Willebrand factor is reduced, as is the ability of platelets to clump together. In Type IIb, although the factor itself is defective, the ability of platelets to clump together is actually increased.
• Type III: This is severe von Willebrand disease. These people may have a total absence of von Willebrand factor, and factor VIII levels are often less than 10%.• Pseudo (or platelet-type) von Willebrand disease: This disorder resembles Type IIb von Willebrand disease, but the defects appear to be in the platelets, rather than the von Willebrand factor.
14

Once in a while, people develop what appears to be von Willebrand disease later in life. When this occurs in those who have no family history of the disease, it is thought that they're probably producing antibodies that destroy or decrease the amount of von Willebrand factor. Some other people have "acquired" a form of the disease in association with another disorder, such as rheumatoid arthritis, systemic lupus erythematosus, kidney disease and certain cancers. The life span of patients is usually normal length. Since the disease is genetically transmitted, genetic counseling may be recommended for parents. Von Willebrand disease can be more complicated for women because of obstetric and gynecological issues.
Inheritance PatternLike hemophilia, the disease is passed down through the genes. But unlike hemophilia, which usually affects only males, von Willebrand disease occurs in men and women equally.
A man or woman with the disease has a 50% chance of passing the gene on to his or her child. Types I and II are usually inherited in what is known as a "dominant" pattern. This means that if even one parent has the gene and passes it to a child, the child gets the disease. Whether the child has no symptoms, mild symptoms or, less commonly, severe symptoms, he or she definitely has the disease. Regardless of severity of the symptoms, the child can still pass the gene to his or her own offspring.
Type III von Willebrand disease, however, is usually inherited in a "recessive" pattern. This type occurs when the child inherits the gene from both parents. Even if both parents have mild or asymptomatic disease, their children are likely to be severely affected.
These patterns of inheritance differ from hemophilia, which is caused by a defect in one of the "sex-linked" chromosomes. A man with hemophilia cannot pass the gene on to a son, because the abnormality is carried on the X chromosome and a man contributes only a Y chromosome to his male offspring. von Willebrand disease is found on the autosomal chromosomes and therefore can be inherited by either males or females. von Willebrand disease can often be traced through several generations in a family. Some have symptoms while others just carry the gene.
Symptoms and Diagnosis Diagnosis can be difficult. When a healthcare practitioner hears of recurrent nosebleeds, easy bruising, heavy menstrual periods or longer than usual bleeding after such routine operations as tonsillectomies or tooth extractions, diagnostic tests should be performed to rule out the possibility of von Willebrand disease.
Usually, a person with von Willebrand disease has a parent with a history of bleeding problems. Typically, a child bruises easily or has bleeds excessively after a skin cut, tooth extraction, tonsillectomy or other surgery. A woman may have increased menstrual bleeding. Bleeding may worsen at times. On the other hand, hormonal changes, stress, pregnancy, inflammation and infections may stimulate the body to increase production of the von Willebrand factor and temporarily improve clot formation.
15

Laboratory tests may determine that the number of platelets is normal but bleeding time is abnormally long. Bleeding time is the amount of time that elapses before bleeding stops after a small cut is made on the forearm. To make the diagnosis, doctors may order tests that measure the amount of von Willebrand factor in the blood. Because the von Willebrand factor is the protein that carries factor VIII in the blood, the blood level of factor VIII may also be decreased.
Diagnostic signs can include: • normal platelet count• prolonged bleeding time• reduced von Willebrand factor level • reduced platelet adhesion may occur • reduced or increased platelet aggregation (platelet aggregation test) • ristocetin cofactor is reduced
Treatments There are a range of treatment choices that depend on whether the illness is mild or severe. Many people with von Willebrand disease never even need treatment.Stimate, desmopressin acetate (DDAVP), a drug sprayed into the nose, is the treatment of choice for mild von Willebrand disease. Bleeding is usually controlled in individuals with mild von Willebrand disease by using this nasal spray to boost their own factor VIII and von Willebrand levels. DDAVP may be given to increase the amount of the von Willebrand factor long enough for surgery or dental procedures to be performed. DDAVP is a synthetic product that carries no risk of infectious disease.
For excessive bleeding, infusions of a viral inactivated factor VIII product rich in von Willebrand factor, such as Humate-P, Alphanate and Koate DVI, may be required. If trauma occurs or surgery is scheduled, desmopressin acetate can be given to raise the levels of von Willebrand factor, which will decrease the tendency toward bleeding. Fresh plasma may also be used to decrease bleeding but the risk of viral infection can be high. Children with von Willaebrand disease should avoid unnecessary trauma, and those with severe disease should avoid certain contact sports. During menstruation, adolescent females may want to take extra precautions to avoid accidents. During bleeding episodes, they can elevate and apply cold compresses and gentle pressure to the area. During nosebleeds, they can apply pressure over the bridge of the nose lean forward to prevent blood running down the back of the throat and being swallowed. Aspirin and many of the drugs used for arthritis can aggravate bleeding because they interfere with platelet function. People who have von Willebrand disease can take acetaminophen for pain relief because it doesn't inhibit platelet function. The National Hemophilia Foundation's Medical and Scientific Advisory Council (MASAC) made recommendations for treatment of von Willebrand disease in November of 1999. They include: • Stimate, desmopressin acetate (DDAVP), a nasal spray or injection. • For patients who have become unresponsive to DDAVP or need surgical procedures, viral-inactivated factor VIII preparations rich in von Willebrand factor, such as Alphanate, Humate-P and Koate DVI, are
16

recommended. • Cryoprecipitate is not recommended except in life-threatening emergencies because of the risk of HIV and hepatitis infection. Despite greatly improved screening and purification for viral inactivation in blood products, cryoprecipitate can still be infectious.
Complications After any kind of surgery, hemorrhaging may occur. The condition is worsened by the use of aspirin and other nonsteroidal anti-inflammatory drugs. Women may have heavy menstrual periods as well as risks during pregnancy and childbirth. . Those who have this disorder and are scheduled for surgery or are in an accident, should be sure to notify healthcare providers about the condition.
Factor I Deficiency (Afibrinogenemia)What Is It? Fibrinogen, also known as factor I, is needed for most types of platelet aggregation. It's the last step in the clotting process—the "glue" that holds the clot together. People who have a factor I deficiency have a combined bleeding and clotting disorder, meaning that both platelets and clotting are abnormal. Since its discovery in 1920, there have only been about 200 cases of this disorder. Included under factor I deficiency are several rare coagulation disorders known as congenital fibrinogen defects. They include:• afibrinogenemia• hypofibrinogenemia• dysfibrinogenemia The first two are called quantitative abnormalities because they have to do with an absent or low quantity of fibrinogen. The third is called a qualitative abnormality because the fibrinogen does not work well.
Afibrinogenemia is the complete absence of fibrinogen. Hypofibrinogenemia is a low level of fibrinogen—less than 100mg in 1dL of blood. Both conditions are inherited in an autosomal fashion and can affect males and females.The severity of the disorder is related to the amount of fibrinogen. Afibrinogenemia is usually discovered in newborns and can cause bleeding from the umbilical cord, genitourinary tract or central nervous system. People with hypofibrinogenemia may have little, moderate or severe bleeding.Dysfibrinogenemias are due to variations in the factor I molecule. More than 70 different types of dysfibrinogenemia have been identified.
Inheritance Pattern The disorder is not sex-linked as is hemophilia. It affects both males and females with equal frequency. It is autosomal recessive, which means that if the clotting defect is inherited from a parent, the child will be a genetic carrier of the condition, but may or may not have symptoms.
17

Symptoms and Diagnosis Few people who have any of these disorders suffer symptoms, although some are predisposed to form blood clots (thrombosis). Treatments Many people with hypofibrinogenemia or dysfibrinogenemia need no treatment. Those who require treatment may be given cryoprecipitate or fresh frozen plasma. Anticoagulants are sometimes prescribed to reduce the risk of thrombosis. The goal of treatment is to raise the patient's fibrinogen level to 100 mg/dL for minor bleeding and up to 200 mg/dL for surgery or severe bleeding. (One unit of fresh frozen plasma has about 450 mg of fibrinogen.)
Complications Plasma levels of fibrinogen exceeding 1,000 mg/dL have been reported to possibly increase the risk of thrombosis. In women, menstrual bleeding can be a severe problem and must be controlled
Factor II Deficiency (Prothrombin)What Is It? Prothrombin is a vitamin K-dependent proenzyme that functions in coagulation. There are two types of this deficiency, a congenital version called hypoprothrombinemia, and an acquired version called dyspothrombinemia. A life-long bleeding disorder when congenital, factor II deficiency is extremely rare. In fact, only 30 cases of this hereditary clotting factor defect have been identified in the whole world. Acquired factor II deficiency is more common. It results from vitamin K deficiency, severe liver disease and therapeutic use of anticoagulant drugs. Risk factors for vitamin K deficiency are prolonged use of antibiotics, bile duct obstruction and intestinal malabsorption (inadequate absorption of nutrients from the intestinal tract) disorders. Some newborns are born with vitamin K deficiencyIf the deficiency is caused by liver disease, the outcome depends on control of the liver problem. Vitamin K administration will correct vitamin K deficiency. Either form may lead to severe bruising, excessive menstrual bleeding, postoperative hemorrhage or occasional muscle bleeds.Inheritance Pattern A congenital factor II deficiency is a very rare inherited disorder that results in deficient blood clotting. The disorder is not sex-linked as is hemophilia. It affects both males and females with equal frequency. It is autosomal recessive, which means that if the clotting defect is inherited from a parent, the child will be a genetic carrier of the condition, but may or may not have symptoms. A family history of bleeding disorder is a risk factor. Symptoms and DiagnosisSigns and symptoms vary with the level of prothrombin. Patients with levels greater than 50% of normal have no bleeding problems, whereas people with levels from 2% to 50% may easily bruise or suffer from epistaxis, menorrhagia, muscle hemorrhages, postpartum hemorrhages and hemorrhage following surgery and trauma.
18
Symptoms include: • umbilical cord bleeding at birth • nose bleeds• abnormal menstrual bleeding • abnormal bleeding after delivery• bleeding after trauma• bleeding after surgery• easy bruising
Signs and Tests: • prolonged prothrombin time • prolonged partial thromboplastin time • factor II assay showing decreased activity• levels of prothrombin ranging from 2% to 50% of normal
Treatments Treatment depends on the severity of the disorder and the type of bleeding. Mild cases may be treated with plasma infusion. Loss of blood can be controlled by infusions of fresh frozen plasma. Severe factor II deficiencies may be treated with prothrombin complex concentrates (PCCs). When necessary, it can be treated with plasma replacement therapy. Effective control of a hemorrhage is achieved when prothrombin levels are at 30% to 50% of normal.
Genetic counseling may be helpful in the case of congenital disorders. The use of vitamin K in malabsorption and long-term antibiotic use may be preventative. If the disorder is caused by vitamin K deficiency, then vitamin K is prescribed. Diagnosis of a bleeding disorder is important so that precautionary measures can be taken if surgery is needed or anticipated. The National Hemophilia Foundation's Medical and Scientific Advisory Council (MASAC) made recommendations for treatment of factor II deficiency in November of 1999. They include:• Prothrombin complex concentrates (PCCs) can be used, but these products vary considerably in the amount of factors they contain.• Fresh frozen plasma can be used as along as it is processed to reduce the risk of viral infection.
Complications Bleeding has to be controlled in instances of trauma or surgery, or else bleeding into the brain or skull can occur.
Factor V Deficiency (Parahemophilia, Labile factor or Proaccelerin Deficiency)What Is It?
19

Factor V deficiency is also known as Owren's disease or parahemophilia. This deficit was identified in Norway in 1943. Since then about 150 cases have been reported, occurring in both men and women. The exact frequency of this rare disorder is unknown, but is estimated to be one per 1 million. The role of factor V is to accelerate the activity of thrombin. When levels of factor V are low, blood clotting is delayed or it progresses slowly. People with this deficiency may have occasional nosebleeds, excessive menstrual bleeding and bruising; although, many have no symptoms. The first sign of this condition may be bleeding following surgery. In this disorder, bleeding ranges from mild to severe. The disease is similar to hemophilia, except that bleeding into joints is uncommon. Bleeding can occur almost anywhere in the body, and death from hemorrhage has occurred with this disorder. Excessive bleeding with menstrual periods and postpartum hemorrhage occurs frequently. A family history of a bleeding disorder is a risk factor. Men and women are affected equally.The probable outcome is good with proper diagnosis and treatment.
Inheritance Pattern The disorder is not sex-linked as is hemophilia. It affects both males and females with equal frequency. It is autosomal recessive, which means that if the clotting defect is inherited from a parent, the child will be a genetic carrier of the condition, but may or may not have symptoms. Several families with combined deficiencies of factors V and VIII have been reported.
Symptoms and Diagnosis Symptoms include: • bleeding into the skin• excessive bruising with minor injuries • nose bleeds • bleeding of the gums • excessive menstrual bleeding• prolonged or excessive loss of blood with surgery or trauma
Diagnosing the deficiency involves tests and signs such as:• factor V assay showing decreased activity• slightly prolonged bleeding time (in some people) • prolonged partial thromboplastin time• prolonged prothrombin time
Treatments There are no commercially available concentrates of factor V, so fresh plasma or fresh frozen plasma infusions are used to correct the deficiency temporarily and should be given daily during a bleeding episode. Other plasma is not given because factor V deteriorates very rapidly. The half-life of factor V is 24 hours. This is an inherited disorder; there is no known prevention.
20
Complications Dangerous hemorrhaging can occur if bleeding isn't controlled quickly. If platelets are used as a source of factor V, antiplatelet antibodies can be induced.
Factor VII Deficiency (Proconvertin or Stable Factor)What Is It? This extremely rare disorder can be inherited or acquired by people who do not have hemophilia who take Coumadin, a drug used to inhibit blood clotting. With this disorder, bleeding can vary from mild to severe within the same person over time. Bleeding doesn't always correspond with the severity of the deficiency shown in blood tests. A history of bleeding may occur in infancy or childhood. Gastrointestinal and central nervous system bleeding can also occur. This disorder occurs in one in 500,000 males and females. Congenital factor VII deficiency should be distinguished from acquired factor VII deficiency, which may result from liver disease, vitamin K deficiency or other malabsorption conditions. When levels of the factor are less than 1% of normal, bleeding can be severe. The trauma of birth may cause bleeding in the head of a newborn. Circumcision may cause prolonged bleeding. Children and adults may suffer bleeding from nose, gums or gastrointestinal tract, and women may suffer excessive menstrual bleeding.The probable outcome is good with proper treatment.
Inheritance PatternThe disorder is not sex-linked as is hemophilia. It affects both males and females with equal frequency. It is also autosomal recessive, which means that if the clotting defect is inherited from a parent, the child will be a genetic carrier of the condition, but may or may not have symptoms. Those who have inherited a defective factor VII gene from only one parent will usually have only moderate levels of the factor but no symptoms.
Symptoms and Diagnosis Severity of bleeding episodes depends on the degree of the severity of the defect. Symptoms include: • bleeding of mucous membranes • spontaneous nosebleeds• excessive bruising• prolonged menstrual bleeding• bleeding into muscles• bleeding into joints
Diagnosis is made by testing for factor VII in the blood. Signs and tests include: • prolonged prothrombin time • normal partial thromboplastin time • decreased factor VII assay
21

Treatments Bleeding episodes can be controlled with normal plasma or concentrates containing factor VII. Severe bleeding may be treated with fresh frozen plasma or Prothrombin complex concentrates (PCCs). Because the life span of infused factor VII is very short (two to four hours), patients may require treatment every two to six hours for severe bleeding or surgery. Menstrual bleeding can be controlled by the use of oral contraceptives.
Note that factor VII concentrate is sold only in Europe, but is available in the US on a compassionate basis from the manufacturer (Immuno Ag).
The National Hemophilia Foundation's Medical and Scientific Advisory Council (MASAC) made recommendations for treatment of Factor VII deficiency in November of 1999. They include: • Recombinant factor VIIa (NovoSeven), which was recently licensed in the US and is produced by baby hamster kidney cells. No human albumin is used.• Prothrombin complex concentrates (PCCs) can be used, but these products vary considerably in the amount of factors they contain.• Fresh frozen plasma can be used as along as it is processed to reduce the risk of viral infection. Complications These can include hemorrhages, strokes or other neurological problems related to central nervous system bleeding. Fatal intracranial bleeding caused by birth trauma has occurred. Menstrual bleeding may also be severe.
THROMBOCYTOPENIA
Definition
Thrombocytopenia is any disorder in which there are not enough platelets. Platelets are cells in the blood that help blood to clot. This condition is sometimes associated with abnormal bleeding.
Causes, incidence, and risk factors
Thrombocytopenia is often divided into three major causes of low platelets:
1. Low production of platelets in the bone marrow 2. Increased breakdown of platelets in the bloodstream (called intravascular) 3. Increased breakdown of platelets in the spleen or liver (called extravascular )
Disorders that involve low production in the bone marrow include:
22

Aplastic anemia Cancer in the bone marrow Infections in the bone marrow (rare) Drugs (very rare)
Disorders that involve the breakdown of platelets include:
Immune thrombocytopenic purpura (ITP) Drug-induced immune thrombocytopenia Drug-induced nonimmune thrombocytopenia Thrombotic thrombocytopenic purpura Primary thrombocythemia Disseminated intravascular coagulation (DIC) Hypersplenism (an enlarged spleen)
Symptoms
Bruising Nosebleeds or bleeding in the mouth Rash (pinpoint red spots)
Other symptoms may be present as well, depending on the cause of the condition. Mild thrombocytopenia can occur without symptoms.
Signs and tests
CBC shows low platelets Bone marrow aspiration or biopsy may be normal or may show low megakaryocytes (platelet
precursors) or an infiltrating disease. PTT clotting study is normal PT clotting study is normal Platelet associated antibodies may be present
Treatment
Treatment depends on the cause of the condition. In some cases, a transfusion of platelets may be required to stop or prevent bleeding.
Expectations (prognosis)
The outcome depends on the disorder causing the low platelet counts.
23
Complications
Hemorrhage Gastrointestinal bleeding (vomiting blood or blood in the stools) Bleeding in the brain (intracranial hemorrhage)
Calling your health care provider
Call your healthcare provider if you experience unexplained bleeding or bruising.
Prevention
Prevention depends on the specific cause.
DISSEMINATED INTRAVASCULAR COAGULATION DIC is a syndrome arising as a complication of many different serious and life-threatening illnesses. In its acute (overt) form it is a hemorrhagic disorder, characterized by multiple ecchymoses, mucosal bleeding, and depletion of platelets and clotting factors in the blood. Chronic (nonovert) DIC, on the other hand, is more subtle and involves thromboembolism accompanied by evidence of activation of the coagulation system. With chronic DIC, coagulation factors may be normal, increased, or moderately decreased, as may the platelet counts. Successful management of acute DIC depends almost entirely on prompt, effective control of the underlying disease. Chronic DIC usually can be treated with heparin or low-molecular-weight heparin, but warfarin is sometimes ineffective for long-term control. Successful treatment of the underlying disease is necessary to eliminate DIC, whether it is acute or chronic.
Pathogenesis of DIC DIC occurs when monocytes and endothelial cells are activated or injured by toxic substances elaborated in the course of certain diseases. The response of monocytes and endothelial cells to injury is to generate tissue factor on the cell surface, activating the coagulation cascade (figure 1). In acute DIC, an explosive generation of thrombin depletes clotting factors and platelets and activates the fibrinolytic system. Bleeding into the subcutaneous tissues, skin, and mucous membranes occurs, along with occlusion of blood vessels caused by fibrin in the microcirculation. In chronic DIC, the process is the same, but it is less explosive. Usually there is time for compensatory responses to take place, which diminish the likelihood of bleeding but give rise to a hypercoagulable state. These changes in the blood can be detected by testing the coagulation system.1-4 Thromboembolism occurs in this setting, and when oral anticoagulants are given following heparin therapy, there is a tendency for it to recur. Long-term therapy with low-molecular-weight heparin may be a solution to this problem until the underlying cause can be brought under control. Conditions associated with DIC: The conditions that regularly give rise to the DIC syndrome are outlined in table 1 (1,5-8). Knowledge of this association is helpful to the physician, who may then anticipate onset and intervene in a timely manner.
Table 1. Conditions underlying DIC syndrome
24

InfectionsAcute DIC: Bacteria and their toxins, fungi, viruses, rickettsiaeChronic DIC: Any chronic infection (eg, tuberculosis, abscesses, osteomyelitis)
Noninfectious inflammatory diseases Inflammatory bowel disease: Crohn's disease and similar disorders
Obstetrical complications Acute DIC: Abruptio placentae, abortions (especially therapeutic abortions), amniotic fluid embolism, hemorrhagic shockChronic DIC: Dead fetus syndrome
Malignancy Acute DIC: Acute promyelocytic leukemia, acute myelomonocytic or monocytic leukemia, disseminated prostatic carcinomaChronic DIC: Lung, breast, gastrointestinal malignancy
Vascular disease Acute DIC: Brain infarction or hemorrhageChronic DIC: Aortic aneurysm, giant hemangioma
Venoms Acute DIC: Snake, spider (rare)
Trauma ;Acute DIC: Massive tissue destruction, brain damage
Others Acute DIC: Heparin-induced thrombocytopenia with thrombosis (HITT), purpura fulminans in newborns (homozygous protein C deficiency)zDIC, disseminated intravascular coagulation.
It is well known that Trousseau described an association between cancer and venous thromboembolism. However, it is less well known that half of his patients did not have cancer but rather had tuberculosis (9). Other inflammatory diseases are also often associated with thromboembolism. Patients with these conditions have the hypercoagulable state known as chronic DIC. Nonbacterial thrombotic endocarditis and arterial thromboembolism constitute "arterial Trousseau's syndrome."
Diagnosis of DIC
Diagnostic findings in DIC are outlined in table 2. The clinical and laboratory features of acute DIC differ from those of chronic DIC. This is only a general rule, however, in that chronic DIC in dead fetus syndrome and in certain vascular disorders (eg, aortic aneurysm) may show coagulation abnormalities similar to those found in acute DIC (10,11).
Table 2. Clinical and laboratory findings in DIC Acute DICClinical findings
Multiple bleeding sites
25
Ecchymoses of skin, mucous membranes Visceral hemorrhage Ischemic tissue
Laboratory abnormalities Coagulation abnormalities: prolonged prothrombin time, activated partial thromboplastin time, thrombin time; decreased fibrinogen levels; increased levels of FDP (eg, on testing for FDP, D dimer) Platelet count decreased as a rule but may be falling from a higher level yet still be normal. Schistocytes on peripheral smear
Chronic DICClinical findings
Signs of deep venous or arterial thrombosis or embolism Superficial venous thrombosis, especially without varicose veins Multiple thrombotic sites at the same time Serial thrombotic episodes
Laboratory abnormalities
Modestly increased prothrombin time in some patients Shortened or lengthened partial thromboplastin time Normal thrombin time in most patients High, normal, or low fibrinogen level High, normal, or low platelet count Increased levels of FDP (eg, on testing for FDP, D dimer) Evidence of molecular markers* (eg, thrombin-antithrombin complexes, activation markers on
platelet membranes, prothrombin fragment F1+2)
DIC, disseminated intravascular coagulation; FDP, fibrin-fibrinogen degradation products. *These tests are used primarily in research.
Diagnosis of acute DIC can be established without performing all of the laboratory tests we know to have abnormal findings in most cases of this syndrome. This is especially true when the clinical setting is consistent with DIC and results of routine tests (eg, platelet count, prothrombin time, partial thromboplastin time, fibrinogen level) are all abnormal (table 2). Disorders such as hepatic insufficiency, hepatic necrosis, anticoagulant overdose, and the presence of certain circulating anticoagulants should also be considered in the differential diagnosis, particularly when there is no obvious underlying disease to account for DIC (10-13). A number of other laboratory markers are associated with DIC, including prolonged thrombin time and decreased levels of antithrombin III, protein C, plasminogen, and alpha2-antiplasmin. However, these same abnomalities may be seen in severe liver disease and in severe hemorrhage caused by plasma loss. The one coagulation system test that helps distinguish between DIC and liver disease is D dimer. This test
26
is usually negative in liver disease unless there is massive necrosis, which can cause DIC. Another laboratory clue to chronic DIC is a shortened activated partial thromboplastin time (14,15). Platelet counts may be normal, high, or moderately low. In addition, platelet counts may rise with heparin therapy and fall when heparin is stopped in the presence of a hypercoagulable state or chronic DIC.
Management of DIC: Treatment of the underlying disease is the mainstay of management of either acute or chronic DIC (table 3). Additionally, acute DIC is treated with blood products that control bleeding if necessary. Experimental drugs (eg, concentrate of the tissue factor pathway inhibitors antithrombin III, protein C, or thrombomodulin) are currently undergoing clinical trials (5,16).
Table 3. Treatment options for DIC syndrome Treat the underlying diseaseAvoid delayTreat vigorously (eg, shock, sepsis, obstetrical problems)
Manage the DICAcute DIC Without bleeding or evidence of ischemia No treatment With bleeding Blood components as needed Fresh frozen plasma Cryoprecipitate Platelet transfusions With ischemia Anticoagulants (see "with thromboembolism" below) after bleeding risk is corrected with blood productsChronic DIC Without thromboembolism No specific therapy needed but prophylactic drugs (eg, low-dose heparin, low-molecular-weight heparin) may be used for patients at high risk of thrombosis With thromboembolism Heparin or low-molecular-weight heparin, trial of warfarin sodium (Coumadin). (If warfarin is unsuccessful, long-term use of low-molecular-weight heparin may be helpful.)*
27

DIC, disseminated intravascular coagulation.
*Some patients respond to warfarin, others do not. Use of low-molecular-weight heparin for prolonged periods has potential hazards and is expensive but can be useful when warfarin therapy fails despite good control (international normalized ratio [INR], 2-3).
When there is no serious hemorrhage or unusual risk of bleeding or thromboembolism in acute DIC, it is appropriate to observe rather than treat. As Milton stated in On His Blindness, "They also serve who only stand and wait."
Chronic DIC is primarily a hypercoagulable state that may result in venous or arterial thrombosis. In some vascular and obstetrical disorders, chronic DIC manifests primarily by consumption coagulopathy of mild to modest degree. Standard treatment of thromboembolism with heparin or low-molecular-weight heparin is appropriate, although it is important to be aware of warfarin resistance. Should thrombosis recur while a patient is receiving warfarin, it is advisable to use heparin or low-molecular-weight heparin until the underlying disease is fully controlled or cured.
IDIOPATHIC THROMBOCYTOPENIC PURPURA
What is ITP?
ITP stands for idiopathic thrombocytopenic purpura. "Idiopathic" means that the cause is unknown. "Thrombocytopenic" means the blood doesn't have enough platelets. "Purpura" means a person has excessive bruising. You may also hear ITP called "immune thrombocytopenic purpura."
In people with ITP, all of the blood cells are normal except for the blood platelets. Platelets are the tiny cells that seal minor cuts and wounds and form blood clots. A person with too few platelets bruises easily and bleeds for a long time after being injured. Tiny red dots on the skin, called petechiae (say "pe-TEEK-ee-ay") might also appear. When the platelet count is very low, the person with ITP might have nosebleeds that are hard to stop, or might have bleeding in the intestines.
What causes ITP?
The cause of ITP is not known. People with ITP form antibodies that destroy their blood platelets. Normally, antibodies are a healthy response to bacteria or viruses. In people with ITP, however, the antibodies attack the body's own blood platelets.
Who gets ITP?
28

There are 2 types of ITP. One type affects children, and the other type affects adults. In children, the usual age for getting ITP is 2 to 4 years of age. Most adults with ITP are young women, but it can occur in anyone. ITP does not run in families.
How does ITP affect children?
ITP is different in children than in adults. Most children with ITP have a very low platelet count that causes sudden bleeding. The usual symptoms are bruises and the tiny red dots on the skin. Nosebleeds and bleeding gums are also common.
How is ITP diagnosed?
Your doctor can diagnose ITP by asking questions about your health and doing a physical exam. Your doctor may take a blood sample and look at it under a microscope.
How is ITP treated in children?
Because most children recover with no treatment, many doctors recommend just watching them carefully and taking care of the bleeding symptoms. Children don't have to go to the hospital if good care is available at home. However, some doctors recommend a short treatment with prednisone pills or intravenous infusions (given in a vein) of gamma globulin to increase the platelet count more quickly. Both medicines have some side effects.
How does ITP affect adults?
In most adults, ITP lasts much longer than it does in children. At the time of diagnosis, most adults have noticed increased bleeding and easy bruising for several weeks, or even months. In women, increased menstrual blood flow is a major sign.
Many adults have only mild thrombocytopenia. In fact, quite a few people have no bleeding symptoms. They are only diagnosed with ITP when their blood is checked for another reason and a low blood platelet count is found.
How is ITP treated in adults?
Treatment of ITP in adults is aimed at increasing the blood platelet count. This is not the same as curing the disease. Patients may take prednisone for several weeks, even a month or longer. However, when the medicine is stopped, the platelet counts may get low again.
If prednisone doesn't help enough, the spleen can be removed. The spleen makes most of the antibodies that destroy the blood platelets. It also destroys old or damaged blood cells. In an otherwise healthy young person, removal of the spleen is not a serious operation.
29

What about ITP in pregnant women?
Diagnosing ITP during pregnancy can be difficult, because platelet counts may be low for other reasons. About 5% of women have mildly low platelet counts at the end of a normal pregnancy. The cause of this is unknown. The platelet count goes back to normal right after delivery.
A baby born to a mother with ITP may have a low blood platelet count a few days to a few weeks after birth. These babies are usually kept in the hospital for several days for observation (watching to make sure they are ok) before they go can home.
Thrombotic thrombocytopenic purpura
What is thrombotic thrombocytopenic purpura?
Thrombotic thrombocytopenic purpura (TTP) is a rare blood condition characterised by the formation of small clots (thrombi) within the circulation, which results in the consumption of platelets and thus a low platelet count (thrombocytopenia).
What causes TTP?
Until recently the cause of TTP remained elusive. However, recent research points to the involvement of a protein in the plasma called von Willebrand factor (vWF).
DRUG-INDUCED IMMUNE THROMBOCYTOPENIA
DRUG-INDUCED IMMUNE THROMBOCYTOPENIA is a condition where the use of certain drugs leads to the formation of antibodies against platelets. These antibodies can cause a low platelet count, which make bleeding more likely. If these antibodies are formed during pregnancy, they may pass from the mother to the fetus.
Thrombocytopenia (nonimmune) drug-induced; Nonimmune thrombocytopenia - drug-induced
Drug-induced nonimmune thrombocytopenia is a reduction in normally functioning platelets that can be caused by certain drugs.Platelets are important in forming blood clots. Certain drugs may decrease the number of platelets by damaging the bone marrow where platelets are made. Decreased platelets may cause easy bruising or abnormal bleeding. Bleeding can be life-threatening if it occurs in the brain or other vital organ. Other drugs can increase the risk of bleeding by preventing platelets from working normally. A common example of this is aspirin
PRIMARY THROMBOCYTHEMIA
Essential thrombocythemia; Essential thrombocytosis
30

Primary thrombocythemia is a condition of overproduction of platelets without a recognizable cause.
Causes, incidence, and risk factors
Primary thrombocythemia is a slowly progressing disorder caused by overgrowth of a type of cell that is a precursor of blood cells. Although the platelets are primarily affected, the red blood cells and white blood cells are also involved.The disease has similarities to polycythemia vera, chronic myelogenous leukemia, and myelofibrosis. Usually it affects people in middle age. Bleeding can occur from the gastrointestinal tract, respiratory system, urinary tract, or skin. The formation of blood clots, called thrombosis, may coincide with bleeding episodes. It may even cause strokes in some people. Risk factors are unknown. The incidence is about 3 out of 100,000 people.
Symptoms
Nosebleeds (epistaxis ) Bleeding from the gums Bleeding from the gastrointestinal tract Easy bruising Prolonged bleeding from surgical procedures or tooth extraction Enlarged lymph nodes (rare) Bloody stools Headache Numbness of hands or feet Dizziness Ulcers on fingers or toes
Signs and tests
Bone marrow aspiration.
CBC that shows elevated platelet count. Uric acid level may be elevated. Physical examination may show enlarged spleen or liver.
Treatment
If a patient is having life-threatening complications, rapid decrease of the platelet count may be achieved through platelet pheresis, a procedure to remove platelets from the blood directly. Long-term decrease of the platelet count using medications can reduce both bleeding and clotting complications. Most common medications include hydroxyurea, interferon-alpha, or anagrelide. For patients with a known clotting tendency, aspirin may help decrease clotting episodes. Some patients do not need any treatment.
31

Expectations (prognosis) The outcome varies with reports ranging from prolonged periods without complications in some people, to fatalities from complications related to hemorrhage and thrombosis in others.
Complications
Severe hemorrhage Thrombotic episodes (stroke, heart attack, or blood clots in extremities) Acute leukemia or myelofibrosis can develop in some patients
Calling your health care provider
If unexplained or prolonged bleeding occurs. If chest pain, leg pain, confusion, weakness, numbness, or other new symptoms develop
HYPERSPLENISM
Hypersplenism is increased activity of the spleen caused by tumors, anemia, malaria, tuberculosis, and various connective tissue and inflammatory diseases.
An enlarged spleen is often accompanied by a low level of one or more types of blood cells. The enlarged spleen can cause stomach pain on the left side, as well as feeling full prematurely after eating
DENTAL EVALUATION
good thorough medical history a physical examination
screening clinical lab tests
excessive bleeding following surgical procedure
good thorough history
Family HX Personal HX
Medications
Past & Present Illness
Spontaneous Bleeding
32

REVIEW PATIENT’S MEDS
FIVE DRUGS THAT INTERFERE WITH HEMOSTASIS
ASPIRIN ANTICOAGULANTS
ANTIBIOTICS
ALCOHOL
ANTICANCER
ORAL MANIFESTATIONS
Petechiae & Ecchymosis Gingival Hyperplasia
Spontaneous Gingival Bleeding
Ulceration of Oral Mucosa
Lymphadenopathy
DENTAL PATIENTS
LOW RISK Patients with No Hx of Bleeding Disorders
Normal Laboratory Results
MODERATE RISK
Patients on Chronic Oral Anticoagulant
Therapy. PT is 1.5 - 2 Times Control Range
Patients on Chronic Aspirin Therapy
DENTAL PATIENTS
HIGH RISK Patients with Known Bleeding Disorders
33

Patients without Known Bleeding Disorders Who Have Abnormal Laboratory Results
DENTAL MANAGEMENT
LOW RISK PATIENTS Normal Protocol
MODERATE RISK PATIENTS
Anticoagulants - Consult Physician
Aspirin Therapy - BT, Consult Physician
HIGH RISK PATIENTS
Close Coordination with Physician
Hospitalization (Platelet Transfusion) (Factor Replacement)(Vit K Therapy)(Dialysis)
CONCLUSIONS
The history (medical /family history) is extremely important in evaluating patients with disorders of hemostasis.The duration of the bleeding disorder must be determined, since many of these disorders are inherited. Careful questioning may be necessary to reveal a life long history of bleeding and bruising a family history of bleeding may be elicited with a carefully taken history.
Dental extractions are a very common major stresses of the haemostatic mechanism, and a prior history of excessive bleeding following an extraction is important. In evaluating this history, one must consider the number of teeth extracted, the location of teeth that were extracted, the time of onset and duration of the hemorrhage, and the extent of blood loss. Bleeding brought on by platelet abnormalities is likely to be immediate and to respond readily to direct pressure. While bleeding secondary to coagulation factor disorders may be delayed a few hours in onset and last for many days, often with recurrences.
So, thorough understanding and knowledge about bleeding disorders is very much needed for dental professionals to minimize the complications of many treatment procedures.
Human gene for factor VIII isolated.
1. B-domain removed from factor VIII gene. 2. B-domain-deleted (BDD) gene inserted into the production cells (Chinese hamster ovary cells).
34

3. BDD production cells grown in culture media that contain small amounts of human serum albumin. 4. BDD recombinant factor VIII (BDDrFVIII) production cells are frozen and stored. 5. BDDrFVIII production cells are obtained from the cell bank and thawed. 6. BDDrFVIII production cells grow inside bioreactors with human serum albumin in the culture
medium. 7. ReFacto is filtered away from production cells and purified and concentrated by a chromatography
step. 8. ReFacto is processed through a viral solvent-detergent step. 9. ReFacto is processed through monoclonal antibody purification and three additional
chromatography steps. 10. No albumin is added to the final formulation.
35