biostatistics biostatistics is statistics applied to biology design of experiments the limitations...
Post on 20-Dec-2015
224 views
TRANSCRIPT

Biostatistics
• Biostatistics is statistics applied to biology
• Design of experiments
• The limitations when working with human subjects
• Non-normality

Biostatistics
text topics
Bland, Ch. 2A short historical review
Design of experiments
Bland, Ch. 13 Contingency tables
Dawson and Trapp, Ch.9 Survival analysis
Logistic regression
ROC analysis

Proofs
• Mathematical proofs:
• Emperical proofs:
F = m*a
2xe

Medical research
• Experimental studies– Clinical trials
• Observational studies– Cohort study
• Longitudinal, and prospective, time and patient consuming– Case-control study
• Can be applied with low sampling number, difficult to choose the control
– Cross-sectional study / survey• Inexpensive, historical, provides the current
– Case-series study• Usually reports unexpected clinical observations
• Meta-analysis• Reviews

Comparing Treatments
• The treatments must be: – Applied concurrently– Treated by the same investigator– Random allocation into treatment groups– Avoid cheating (investigator bias)– Volunteer bias– Intention to treat– Use cross-over design if possible– Double blinded– Ethically solid

Comparing Treatments
• The treatments must be: – Applied concurrently– Treated by the same investigator– Random allocation into treatment groups– Avoid cheating (investigator bias)– Volunteer bias– Intention to treat– Use cross-over design if possible– Double blinded– Ethically solid

Concurrent treatment
• The wonders of the CT scanner– Patients treated in 1978 for stroke scanned by
CT scanner– Patched paired with stroke patients from 1974
(before the scanner)
C-T scan in 1978
Pairs with 1978 better than 1974 9 (31%)
Pairs with same outscome 18 (62%)
Pairs with 1978 worse than 1974 2 (7%)

Concurrent treatment
• The wonders of the CT scanner– Patients treated in 1978 for stroke NOT
scanned by CT scanner– Matched paired with stroke patients from 1974
(before the scanner)
C-T scan in 1978 No C-T scan in 1978
Pairs with 1978 better than 1974 9 (31%) 34 (38%)
Pairs with same outscome 18 (62%) 38 (43%)
Pairs with 1978 worse than 1974 2 (7%) 17 (19%)

Comparing Treatments
• The treatments must be: – Applied concurrently– Treated by the same investigator– Random allocation into treatment groups– Avoid cheating (investigator bias)– Volunteer bias– Intention to treat– Use cross-over design if possible– Double blinded– Ethically solid

Comparing Treatments
• The treatments must be: – Applied concurrently– Treated by the same investigator– Random allocation into treatment groups– Avoid cheating (investigator bias)– Volunteer bias– Intention to treat– Use cross-over design if possible– Double blinded– Ethically solid

Random allocation
• Doctors chose for them self if tuberculosis should receive a BCG vaccine or be in the control group
No. of children
deaths from TB
# visits to the clinic
cooperation
1927-32
Selected allocation
BCG 445 3 (0.67%) 3.6 43%
Control 545 18 (3.30%) 1.7 24%

Random allocation
• Tuberculosis patients were allocated randomly to receive BCG vaccine or to be in the control group
No. of children
deaths from TB
# visits to the clinic
cooperation
1927-32
Selected allocation
BCG 445 3 (0.67%) 3.6 43%
Control 545 18 (3.30%) 1.7 24%
1933-44
Random allocation
BCG 566 8 (1.41%) 2.8 40%
Control 528 8 (1.52%) 2.4 34%

Random allocation
• OK:– Toss a coin – Throw dices– Computer programs – http://www.random.org/
• Not OK– Alternation– By date

Comparing Treatments
• The treatments must be: – Applied concurrently– Treated by the same investigator– Random allocation into treatment groups– Avoid cheating (investigator bias)– Volunteer bias– Intention to treat– Use cross-over design if possible– Double blinded– Ethically solid

Investigator Bias
• Do not allocate by date of arrival:– Patients arriving at even days should be
treated, and patients arriving at odd days should act as control.
Comparing Treatments
• The treatments must be: – Applied concurrently– Treated by the same investigator– Random allocation into treatment groups– Avoid cheating (investigator bias)– Volunteer bias– Intention to treat– Use cross-over design if possible– Double blinded– Ethically solid

Volunteer Bias
• People volunteering for experiments differs form the general population – Obviously more compliant – Volunteers for experiments at AAU?

Volunteer Bias
• Salk poliomyelitis with two different designs:– Randomized controls
2nd grades were invited to participate and randomized to either vaccine or saline injection
– Observed controls
2nd graters was offered vaccine. 1st and 3rd graders were unvaccinated controls

Volunteer Bias
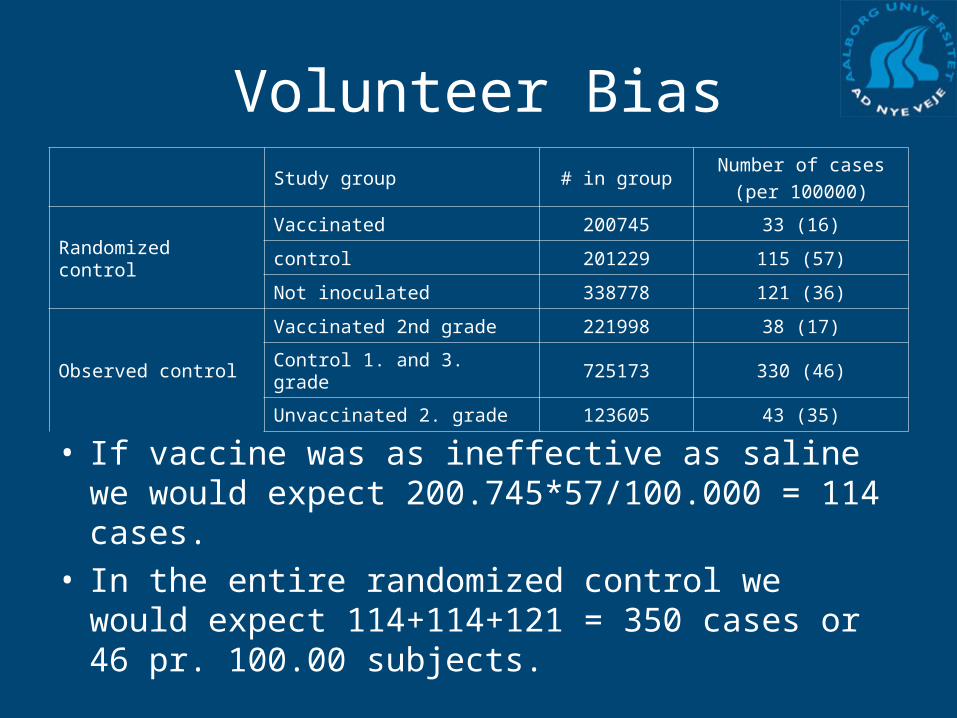
Study group # in groupNumber of cases
(per 100000)
Randomized control
Vaccinated 200745 33 (16)
control 201229 115 (57)
Not inoculated 338778 121 (36)
Observed control
Vaccinated 2nd grade 221998 38 (17)
Control 1. and 3. grade 725173 330 (46)
Unvaccinated 2. grade 123605 43 (35)
Volunteer Bias
• If vaccine was as ineffective as saline we would expect 200.745*57/100.000 = 114 cases.
• In the entire randomized control we would expect 114+114+121 = 350 cases or 46 pr. 100.00 subjects.
Study group # in groupNumber of cases
(per 100000)
Randomized control
Vaccinated 200745 33 (16)
control 201229 115 (57)
Not inoculated 338778 121 (36)
Observed control
Vaccinated 2nd grade 221998 38 (17)
Control 1. and 3. grade 725173 330 (46)
Unvaccinated 2. grade 123605 43 (35)

Selection of subjects
• Low variability makes it easier to detect differences in the treatments
• Inclusion and exclusion criterions – Acute bilateral pulmonary tuberculosis– Bacteriologically proved– Between 15 and 30 years – Unsuitable for other treatment
• Narrow inclusion criterion makes it difficult to conclude on the general population

Prevalence
What if patients die before inclusion?

Comparing Treatments
• The treatments must be: – Applied concurrently– Treated by the same investigator– Random allocation into treatment groups– Avoid cheating (investigator bias)– Volunteer bias– Intention to treat– Use cross-over design if possible– Double blinded– Ethically solid
Intention to treat
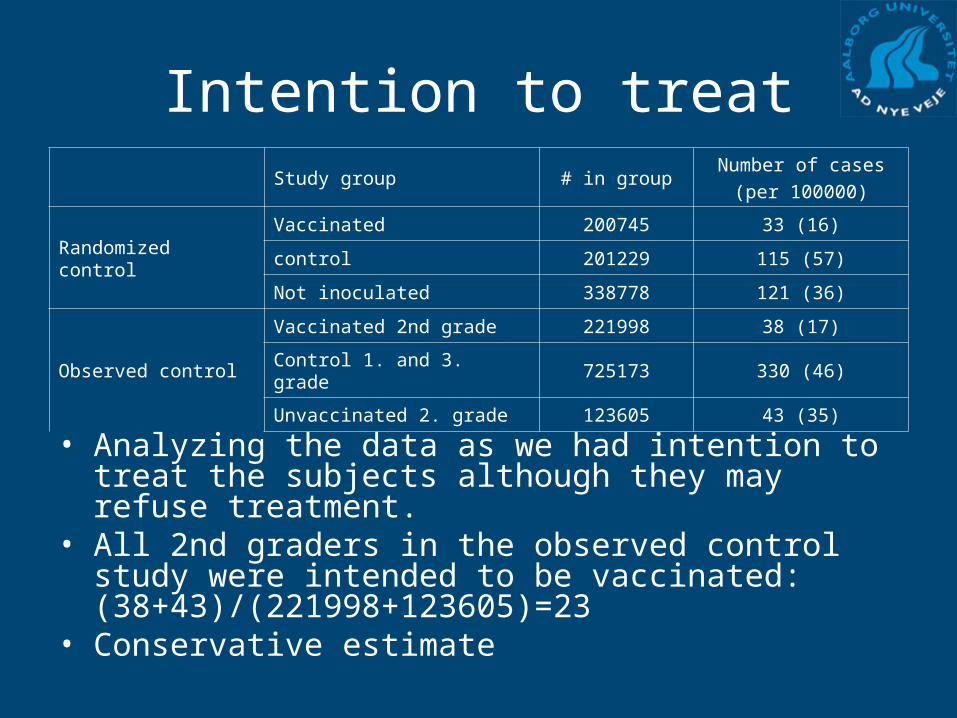
• Analyzing the data as we had intention to treat the subjects although they may refuse treatment.
• All 2nd graders in the observed control study were intended to be vaccinated: (38+43)/(221998+123605)=23
• Conservative estimate
Study group # in groupNumber of cases
(per 100000)
Randomized control
Vaccinated 200745 33 (16)
control 201229 115 (57)
Not inoculated 338778 121 (36)
Observed control
Vaccinated 2nd grade 221998 38 (17)
Control 1. and 3. grade 725173 330 (46)
Unvaccinated 2. grade 123605 43 (35)

Subject flow

Comparing Treatments
• The treatments must be: – Applied concurrently– Treated by the same investigator– Random allocation into treatment groups– Avoid cheating (investigator bias)– Volunteer bias– Intention to treat– Use cross-over design if possible– Double blinded– Ethically solid

Cross-over design
Patient number
# attack on
placebo Pronethaol
1 71 29
2 323 348
3 8 1
4 14 7
5 23 16
6 34 25
7 79 65
8 60 41
9 2 0
10 3 0
11 17 15
12 7 2
ANOVA
num_attack
352.667 1 352.667 .041 .842
191161.2 22 8689.144
191513.8 23
Between Groups
Within Groups
Total
Sum ofSquares df Mean Square F Sig.

Cross-over design
Patient number
# attack on difference
placebo Pronethaol Placebo-Pronetahol
1 71 29 42 +
2 323 348 -25 -
3 8 1 7 +
4 14 7 7 +
5 23 16 7 +
6 34 25 9 +
7 79 65 14 +
8 60 41 19 +
9 2 0 2 +
10 3 0 3 +
11 17 15 2 +
12 7 2 5 +

Cross-over design
• Each subject acts as his/hers own control
• Randomization
• Carry-over effect of treatment or testing
• Treating ‘symptoms’
• Better than case-control (The healthy worker)

Comparing Treatments
• The treatments must be: – Applied concurrently– Treated by the same investigator– Random allocation into treatment groups– Avoid cheating (investigator bias)– Volunteer bias– Intention to treat– Use cross-over design if possible– Double blinded– Ethically solid

Placebo (response bias)
• Any treatment may help• The subject should be
blinded to the kind of treatment
• Effective treatment should be better than a sham treatment
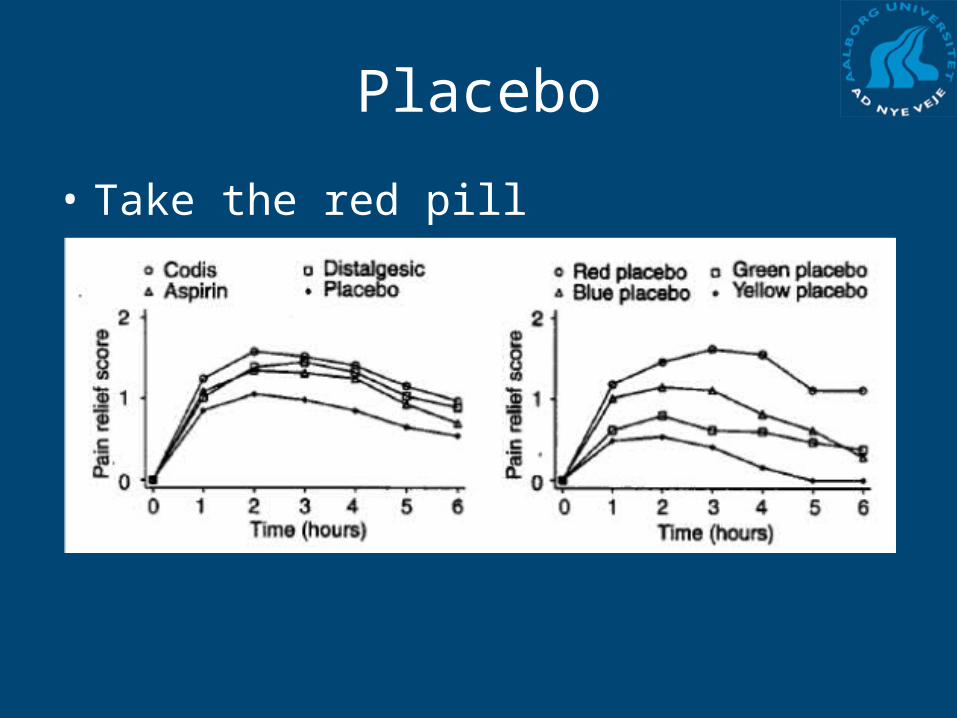
Placebo
• Take the red pill

Double blind studies
• When the assessment is made the investigator should be blind to the treatment.
• Can all studies be blinded?
• Communication between subjects

Comparing Treatments
• The treatments must be: – Applied concurrently– Treated by the same investigator– Random allocation into treatment groups– Avoid cheating (investigator bias)– Volunteer bias– Intention to treat– Use cross-over design if possible– Double blinded– Ethically solid

Ethical considerations
• The Declaration of Helsinki– Reduce suffering of the subjects
• Local ethics comity– Den videnskabsetiske kommité consists of
both experts and laymen. – Secures that the rights of the subjects are
being followed, especially as to the information given to the subjects.

Ethical considerations
• Informed Consent – Subjects must be informed about the nature,
purpose, risks etc. in the study. – The subjects should give their consent before
being enrolled and have the right to withdraw from the study at any time.

Stanley Milgrams "watershed" experiment

Comparing Treatments
• The treatments must be: – Applied concurrently– Treated by the same investigator– Random allocation into treatment groups– Avoid cheating (investigator bias)– Volunteer bias– Intention to treat– Use cross-over design if possible– Double blinded– Ethically solid