biopharmaceutical aspects of exploratory microdose … stevens.pdf · exploratory microdose and...
TRANSCRIPT
1
Biopharmaceutical aspects of exploratory microdose
and microtracer
clinical studies
Lloyd Stevens PhD
Senior Research Fellow
Quotient Clinical
Nottingham, UK
2
Scope
• What is a microdose
and....what is a microtracer
• Walk through “fit-for-purpose”
IV product manufacture
• Microdose
and microtracer
study designs
• Examine the biopharmaceutical outcomes from various microdose
and microtracer
study designs
• Utility and caveats
• Summary and take home messages
3
Microdosing...... Phase 0 Generation of human pharmacokinetic and ADME profile data to support candidate selection
4
What is a microdose?
Exploratory PK and ADME profiling study ........ Regulatory guidance given in ICH M3 (R2) Issued in June 2009 for implementation Jan 2010http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2009/09/WC500002720.pdf
• Reduced toxicology package to support microdoses
in healthy
male subjects•
A microdose
defined as a total dose ≤
100 μg
AND •
Total dose ≤
1/100th NOAEL and ≤1/100th pharmacologically
active dose (scaled on mg/kg) •
IV/PO 2-way crossover = 50μg IV and 50μg PO... Usually 14C-API
5
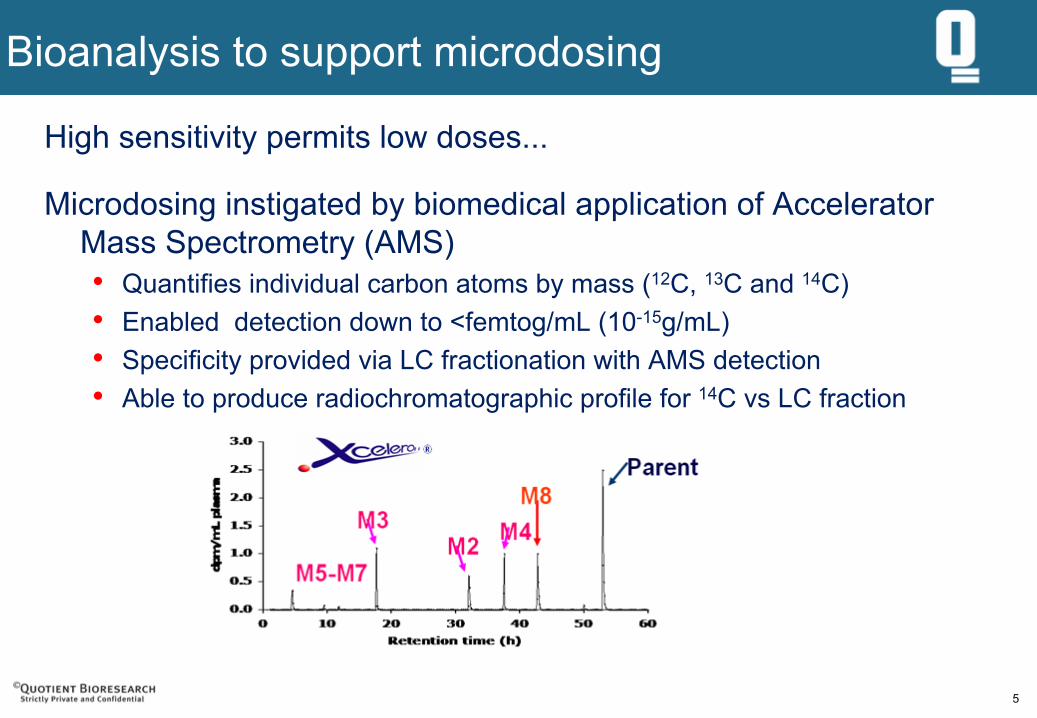
Bioanalysis to support microdosing
High sensitivity permits low doses...
Microdosing instigated by biomedical application of Accelerator
Mass Spectrometry (AMS)•
Quantifies individual carbon atoms by mass (12C, 13C and 14C)
• Enabled detection down to <femtog/mL
(10-15g/mL)•
Specificity provided via LC fractionation with AMS detection
• Able to produce radiochromatographic
profile for 14C vs
LC fraction
622 June 2011
Bringing it all together...... Established practices
14C-API &Product
ManufacturingUnder GMP
Regulatoryframework
LC-AMS and
LC-MS/MS
Clinical and logistics
know-howICH M3
7
Utility and perspectives....
• ~25-30 NCE studies/programs undertaken to date•
First study undertaken in 2004/5
• Significant initial scientific scepticism•
Linearity (transporters, clearance, solubility) and extrapolation to therapeutic doses
• Additive cost (time and money)
• Now starting to see changes in the marketplace•
Design is dictated by the questions to be answered
• Back-up programs may be the most useful application
8
Scientific and commercial drivers for exploratory microdose
studies
• Bioavailability for investor confidence IV/PO
• Oral bioavailability IV/PO
• Half-life determination and oral bioavailability IV/PO
• Human metabolite hunt IV/PO
• Lead candidate selection from 3 IV/PO
• PK characterisation of lead compound IV/PO
• Back-up candidate selection from 4 + lead IV/PO (LC-MS/MS)
• Clearance and Abs Bio single compound IV/PO (LC-MS/MS)
• Exposure to potential carcinogenic metabolite PO
9
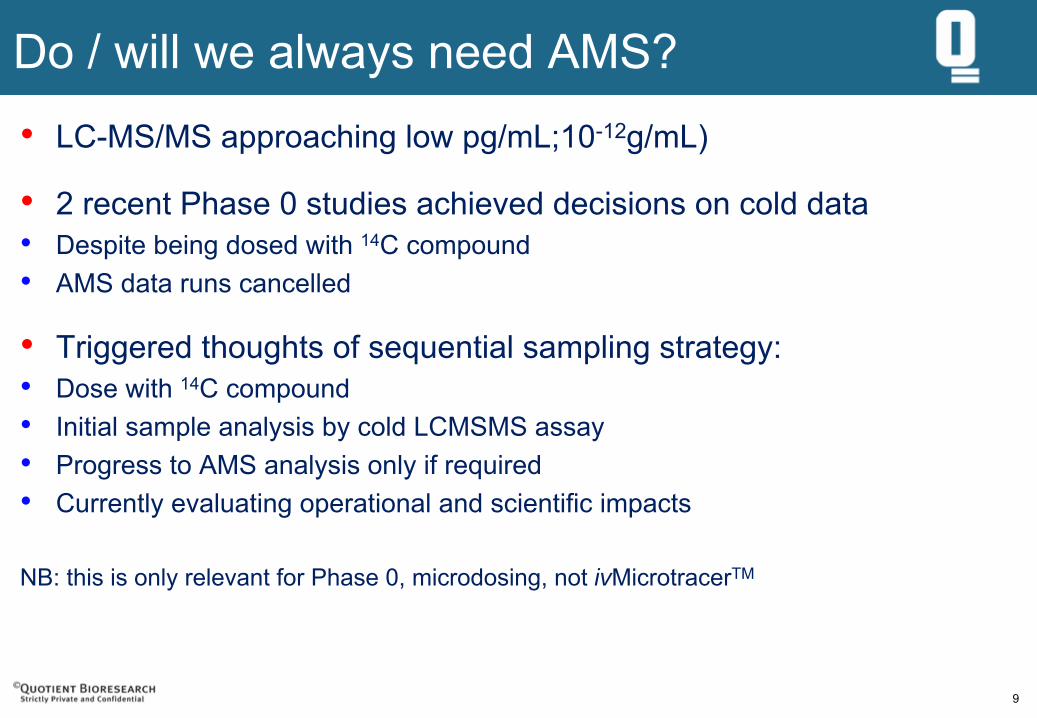
Do / will we always need AMS?•
LC-MS/MS approaching low pg/mL;10-12g/mL)
• 2 recent Phase 0 studies achieved decisions on cold data
•
Despite being dosed with 14C compound•
AMS data runs cancelled
• Triggered thoughts of sequential sampling strategy:
•
Dose with 14C compound•
Initial sample analysis by cold LCMSMS assay
•
Progress to AMS analysis only if required•
Currently evaluating operational and scientific impacts
NB: this is only relevant for Phase 0, microdosing, not ivMicrotracerTM
10
‘Phase 0’ Microdose
case study
Selection of lead candidate from three
Poster: AAPS Conference 2009, Los Angeles, CA
11
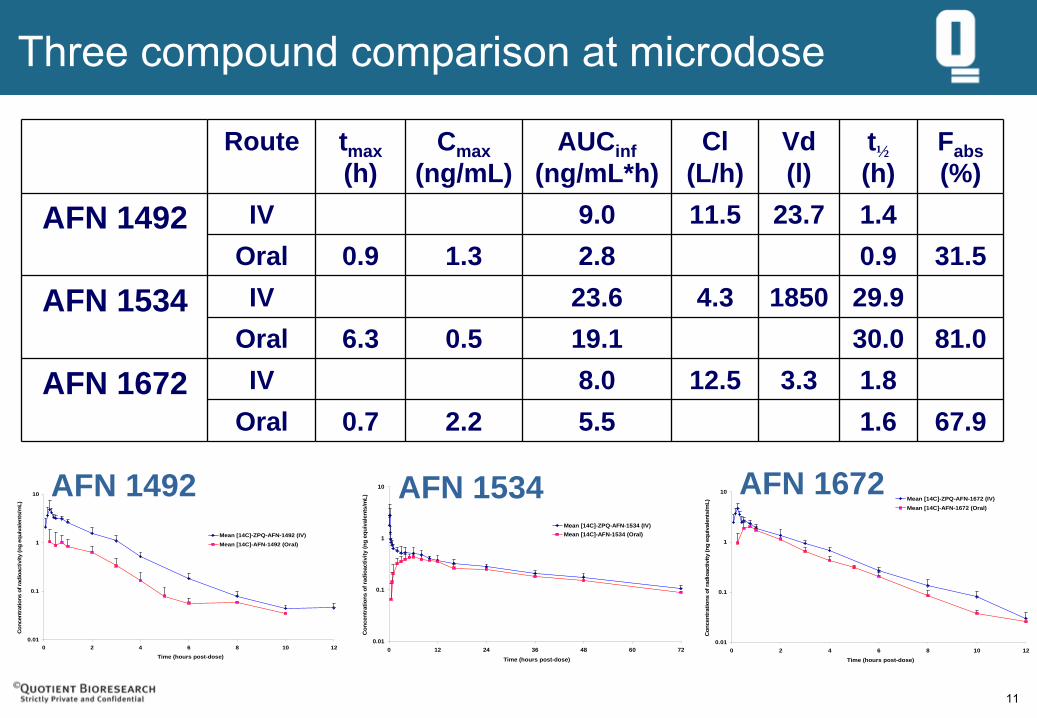
Three compound comparison at microdose
0.01
0.1
1
10
0 2 4 6 8 10 12Time (hours post-dose)
Con
cent
ratio
ns o
f rad
ioac
tivity
(ng
equi
vale
nts/
mL)
Mean [14C]-ZPQ-AFN-1492 (IV)Mean [14C]-AFN-1492 (Oral)
0.01
0.1
1
10
0 12 24 36 48 60 72Time (hours post-dose)
Con
cent
ratio
ns o
f rad
ioac
tivity
(ng
equi
vale
nts/
mL)
Mean [14C]-ZPQ-AFN-1534 (IV)Mean [14C]-AFN-1534 (Oral)
0.01
0.1
1
10
0 2 4 6 8 10 12Time (hours post-dose)
Con
cent
ratio
ns o
f rad
ioac
tivity
(ng
equi
vale
nts/
mL)
Mean [14C]-ZPQ-AFN-1672 (IV)Mean [14C]-AFN-1672 (Oral)
Route tmax(h)
Cmax(ng/mL)
AUCinf(ng/mL*h)
Cl(L/h)
Vd(l)
t½(h)
Fabs(%)
AFN 1492 IV 9.0 11.5 23.7 1.4Oral 0.9 1.3 2.8 0.9 31.5
AFN 1534 IV 23.6 4.3 1850 29.9Oral 6.3 0.5 19.1 30.0 81.0
AFN 1672 IV 8.0 12.5 3.3 1.8Oral 0.7 2.2 5.5 1.6 67.9
AFN 1672AFN 1534AFN 1492
12
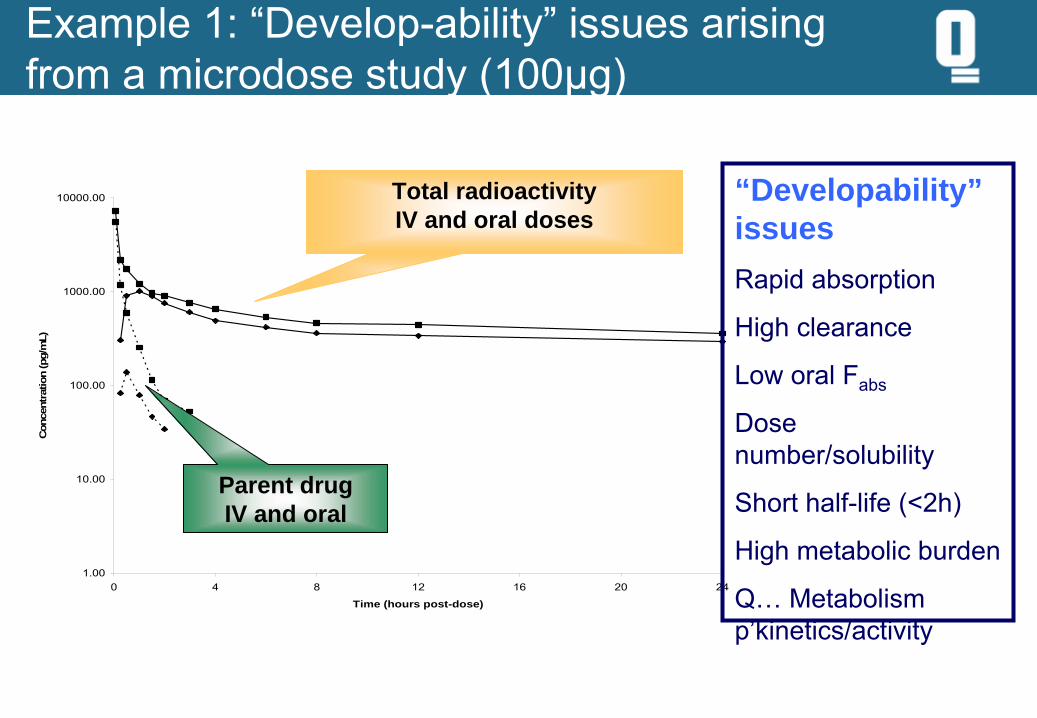
Example 1: “Develop-ability” issues arising
from a microdose study (100µg)
1.00
10.00
100.00
1000.00
10000.00
0 4 8 12 16 20 24
Time (hours post-dose)
Con
cent
ratio
n (p
g/m
L)
total 14C (oral)ONO-8539 (oral)total 14C (IV)ONO-8539 (IV)
Total radioactivityIV and oral doses
Parent drug IV and oral
“Developability” issuesRapid absorption
High clearance
Low oral Fabs
Dose number/solubility
Short half-life (<2h)
High metabolic burden
Q…
Metabolism p’kinetics/activity
13
Biopharmaceutical outcomes from intravenous and oral microdose
studies in compound selection (Phase 0)
Utility and caveats
14
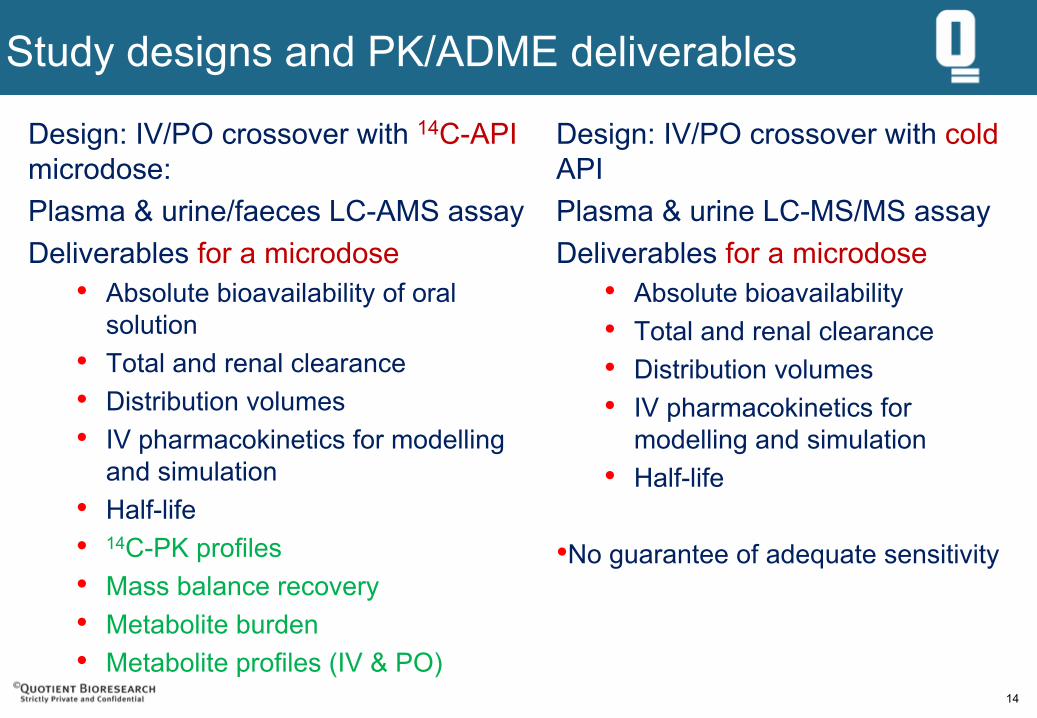
Study designs and PK/ADME deliverables
Design: IV/PO crossover with 14C-API microdose:
Plasma & urine/faeces LC-AMS assayDeliverables for a microdose
• Absolute bioavailability of oral solution
• Total and renal clearance
• Distribution volumes
• IV pharmacokinetics for modelling and simulation
• Half-life
•
14C-PK profiles•
Mass balance recovery
• Metabolite burden
• Metabolite profiles (IV & PO)
Design: IV/PO crossover with cold API
Plasma & urine LC-MS/MS assayDeliverables for a microdose
• Absolute bioavailability
• Total and renal clearance
• Distribution volumes
• IV pharmacokinetics for modelling and simulation
• Half-life
•No guarantee of adequate sensitivity
15
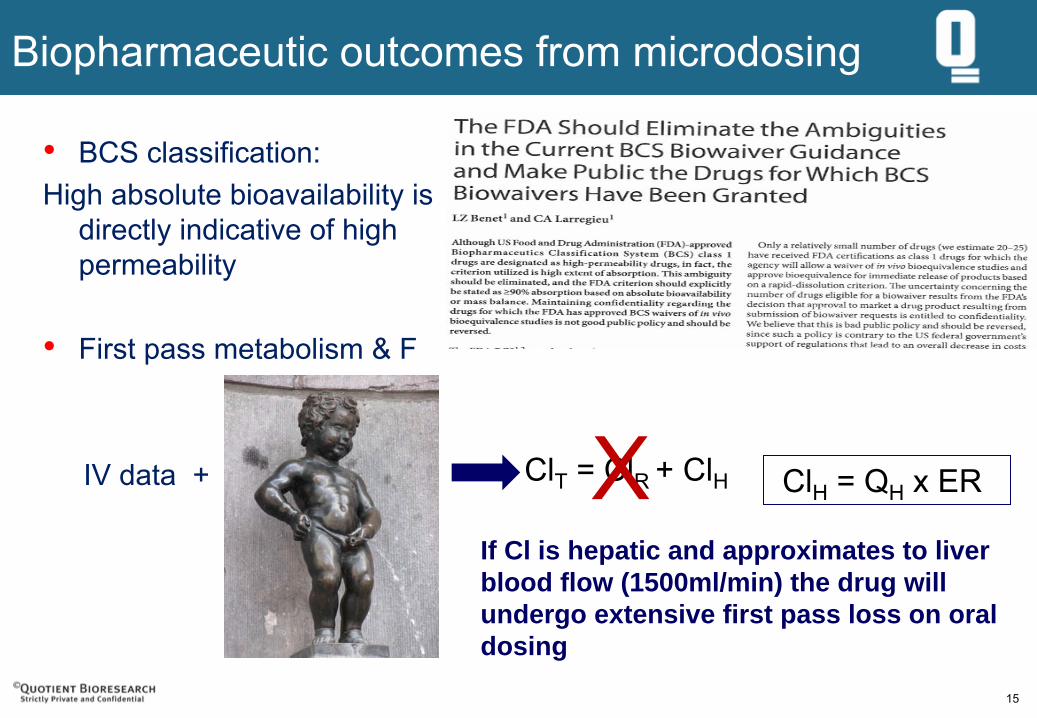
Biopharmaceutic outcomes from microdosing
• BCS classification:
High absolute bioavailability is directly indicative of high permeability
• First pass metabolism & F
IV data + ClT
= ClR
+ ClH
If Cl is hepatic and approximates to liver blood flow (1500ml/min) the drug will undergo extensive first pass loss on oral dosing
ClH
= QH
x ERX
16
Microdosing: Biopharmaceutical outcomes
Microdose to therapeutic dose extrapolation
•
Pharmacokinetic derived non-linearities: •
capacity limited clearance
• transporter
capacity (P-gP, OAT, OATP)
• Physicochemical non-linearities•
Solubility
• Biopharmaceutical challenges identified•
Absolute bioavailability ... Inferences regarding permeability
• Clearance.... Implications regarding first pass metabolism
• PK characteristics will not support QD dosing
• Modified delivery required to alter PK profile
17
ivMicrotracer
Generating IV pharmacokinetic data for oral drugs in early development
18
ivMicrotracer
Imagine having IV PK data for every molecule coming through into clinical development
19
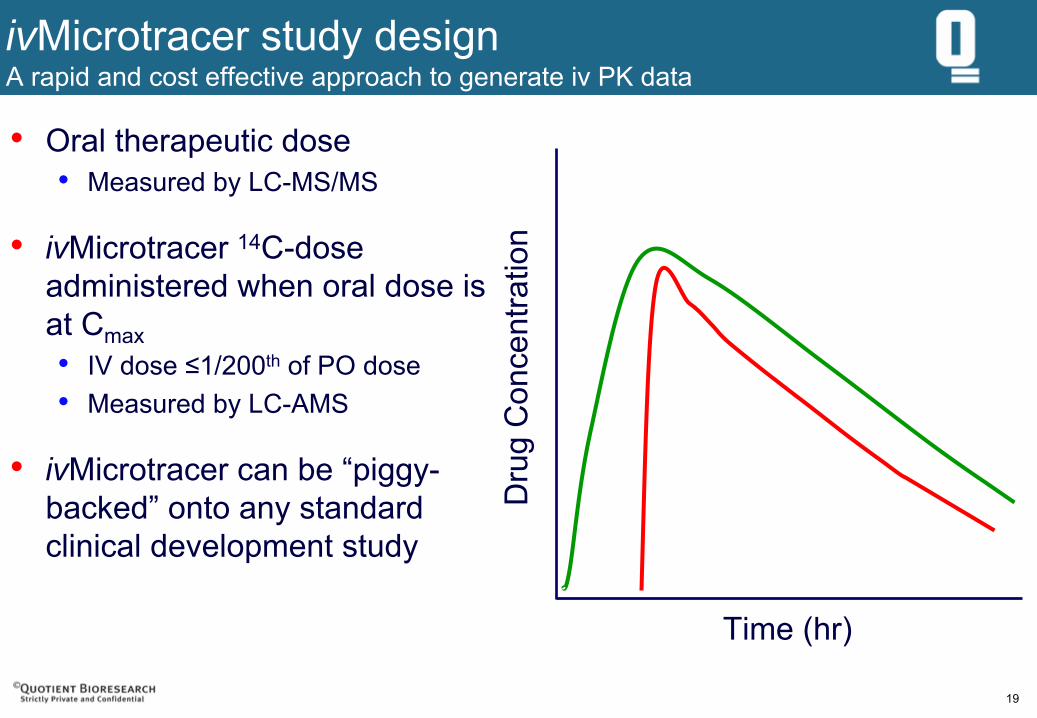
ivMicrotracer study design
A rapid and cost effective approach to generate iv PK data
Time (hr)
Dru
g C
once
ntra
tion
• Oral therapeutic dose•
Measured by LC-MS/MS
• ivMicrotracer
14C-dose administered when oral dose is at Cmax•
IV dose ≤1/200th
of PO dose•
Measured by LC-AMS
• ivMicrotracer
can be “piggy-
backed” onto any standard
clinical development study
20
Why is IV data only accessible now and not in the past?
Historical barriers for access to IV data•
Cost and time for IV toxicity testing and human safety, tolerability assessments
ICH M3 (R2) •
“In some situations it could be appropriate to carry out a clinical microdose
study using the i.v. route on a product intended for oral administration and for which an oral nonclinical
toxicology package already exists. In this case the i.v. microdose can be qualified by the existing oral toxicity studies as described in Table 1 or Table 3, Approach 3, where adequate exposure margins have been achieved. It is not recommended to investigate i.v. local tolerance of the drug substance in this situation because the administered dose is very low (100 μg
maximum). If a novel i.v. vehicle is being employed then local tolerance of the vehicle should be assessed.”
........ together with GMP product manufacture
21
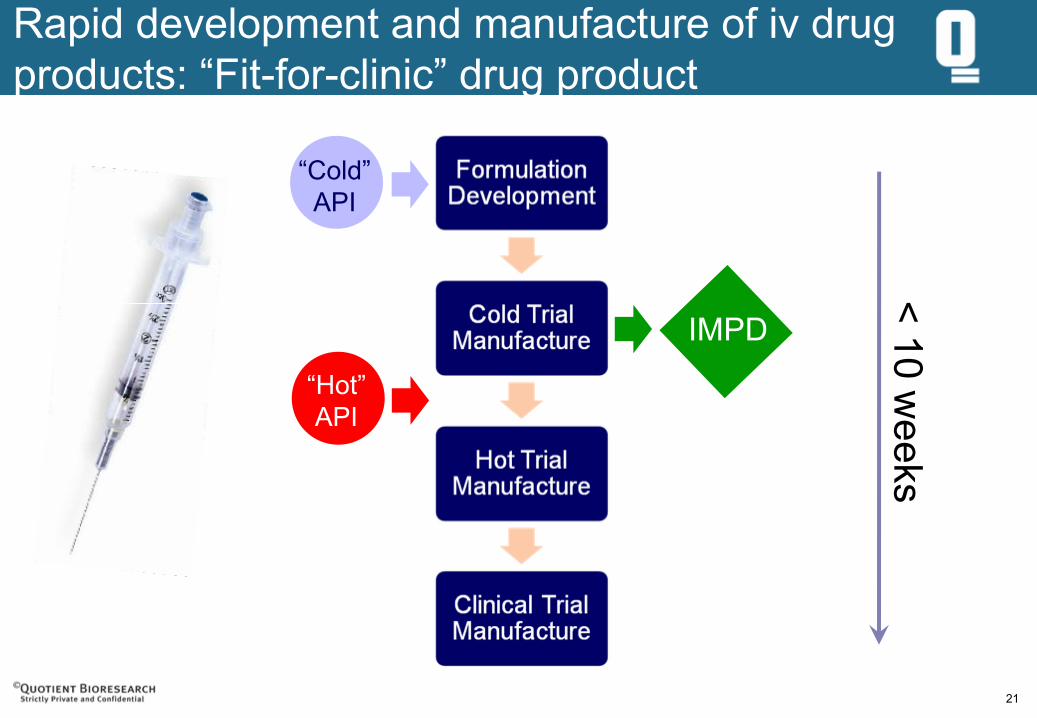
Rapid development and manufacture of iv drug products: “Fit-for-clinic”
drug product
“Cold”API
“Hot”API
IMPD
< 10 weeks
22
“Piggy-back” IVmicrotracers
• IV Microtracers
are incorporated into any other bioavailability or
PK study•
Food interaction
• Drug-drug interaction (victim drug before and after perpetrator)
• Bioavailability or bioequivalence for formulation change
• Effect of age and gender
• Dose proportionality; particularly in cases of non-linear PK
• SAD and MAD (1st
and at steady state)
• Regional absorption study
• Human ADME (14C oral with piggy-back 13C IV microtracer)
• Pro-drug PO plus “piggyback”
IV parent pro-drug and/or active moeity
• Not just “piggy-back”
on oral dosing
• Non-oral routes: inhaled, nasal, rectal, dermal plus ANOther
routes
23
Biopharmaceutical outcomes from exploratory IV microtracer
studies
Utility and caveats
24
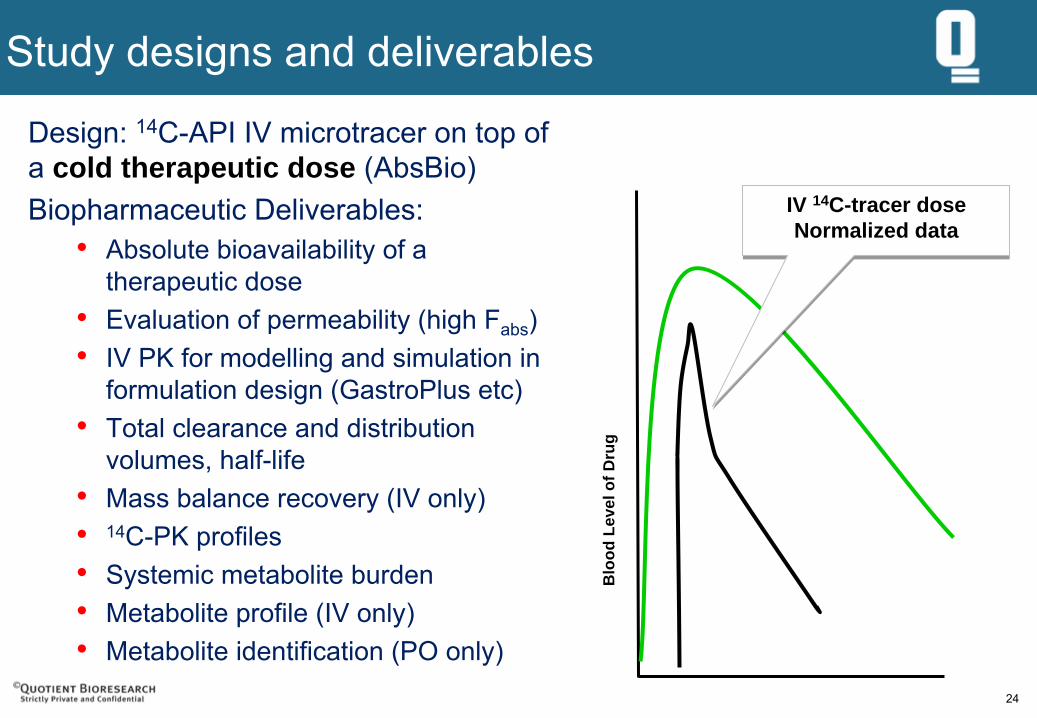
Study designs and deliverables
Design: 14C-API IV microtracer on top of
a cold therapeutic dose (AbsBio)Biopharmaceutic
Deliverables:
• Absolute bioavailability of a therapeutic dose
• Evaluation of permeability (high Fabs
)•
IV PK for modelling and simulation in formulation design (GastroPlus
etc)•
Total clearance and distribution volumes, half-life
• Mass balance recovery (IV only)
•
14C-PK profiles•
Systemic metabolite burden
• Metabolite profile (IV only)
• Metabolite identification (PO only)
Blo
od L
evel
of D
rug
IV 14C-tracer doseNormalized data
IV 14C-tracer doseNormalized data
25
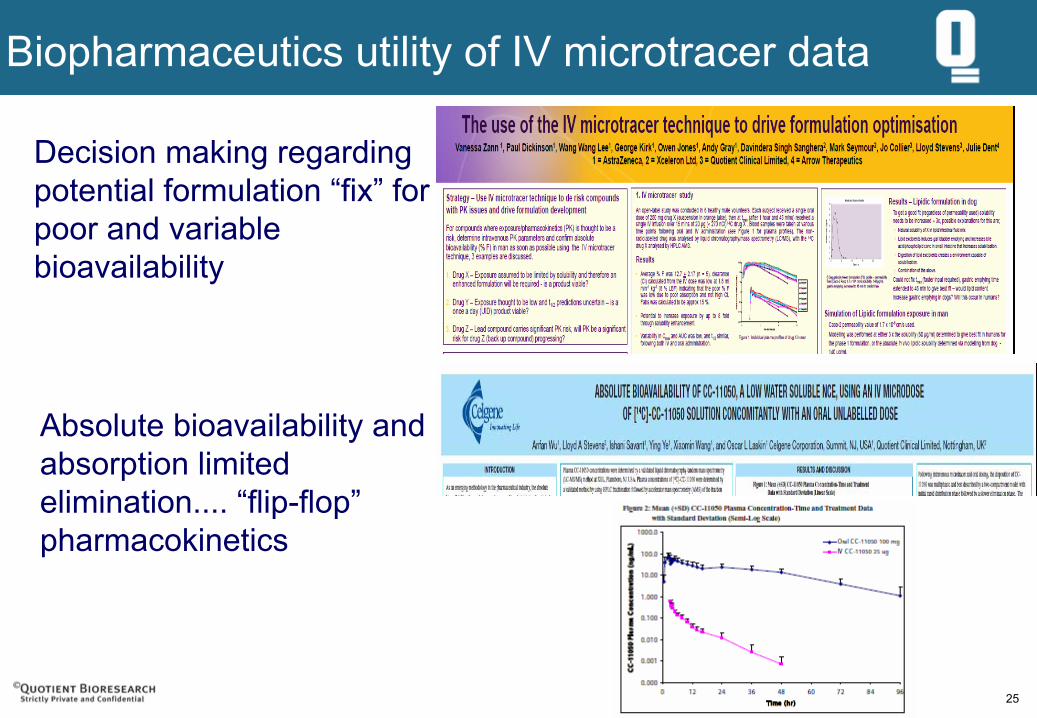
Biopharmaceutics utility of IV microtracer
data
Decision making regarding potential formulation “fix”
for
poor and variable bioavailability
Absolute bioavailability and absorption limited elimination.... “flip-flop”
pharmacokinetics
26
Summary and take home messages
27
Summary and take home messages
MicrodosingCompound selection and characterisation:•
Identification of potential “develop-ability”
issues•
Bioavailability and variability
• Shape of PK profile
• Indication of potential need for MR delivery at therapeutic doses
•
Assessment of permeability from Fabs
•
Contribution of FPM to poor bioavailability•
Feed real human IV and oral PK data into “bottom up”
modelling tools•
Symcyp, Cyprotex, GastroPlus
•
Exercise caution in extrapolating bioavailability and oral PK for drugs with likely solubility limitations
•
Be aware of potential capacity limitations for transporters and metabolism
28
Summary and take home messages
IV MicrotracerIV PK and AbsBio:•
IV PK desirable for MR formulation definition, modelling & IVIVC
•
Assessment of the pharmaceutical challenge (Fabs
)•
Assessment of permeability....... BCS
•
Access to absolute bioavailability data to support regulatory need•
Australian authorities
•
FDA•
Straightforward to accomplish if 14C-API is available
•
If you had 14C-API available, why wouldn’t you implement a “piggyback”
IV Microtracer
on to a future clinical bioavailability or PK study ?
