biomarkers in ali and ards by mohammed attia, md, frcpch (uk)
TRANSCRIPT
Biomarkers in ALI and Biomarkers in ALI and ARDSARDSMohammed Attia, MD, FRCPCH (UK)

Foretelling using dreamsDreaming of….
a deep wellprison
a mirrora second wife
a shining moonforgiveness
a large cata large crop
If someone sees himself If someone sees himself …………
dead long life
eating crocodile flesh he will become a village official
with his face in a mirrora new life
bringing in cattle will evangelize the spirit of the community
If someone sees himself If someone sees himself …………
uncovering his own backside he will become an orphan
putting one’s face to the groundthe dead want something
plunging into cold watersabsolution of all ills
making love to his wife in daylight god will discover his misdeeds

IntroductionIntroductionALI occurs
◦In 1 – 4% of all PICU cases◦10% of all children receiving
mechanical ventilation on PICUALI is associated with a mortality of
25% to 75% depending on◦Diagnostic criteria used to identify
cases◦Coexisting risk factors ◦Presence of nonpulmonary organ failure

The Ideal BiomarkerThe Ideal BiomarkerIncreases pathologically in the
presence of the disease (high sensitivity)
Does not increase in the absence of the disease (high specificity)
Relates to the disease burden and extent
Changes in accordance with the clinical evolution, reflecting the current status of disease
Anticipates clinical changes before it happens
Shows no major fluctuation in serum level
Adds independent information about the risk or prognosis
Reproducible Easy and cheap determination
Markers in ARDS and ALIMarkers in ARDS and ALIThe main characteristics of the
syndrome are◦Diffuse inflammation◦Increased microvascular
permeabilityAlthough a variety of insults may
lead to ARDS, a common pathway may probably result in the lung damage

A clinically useful biomarker for ALI might add information regarding the development of ARDS in at-risk patients.
The clinically useful marker will help the intensivist to monitor the disease and evaluate or modulate treatments.

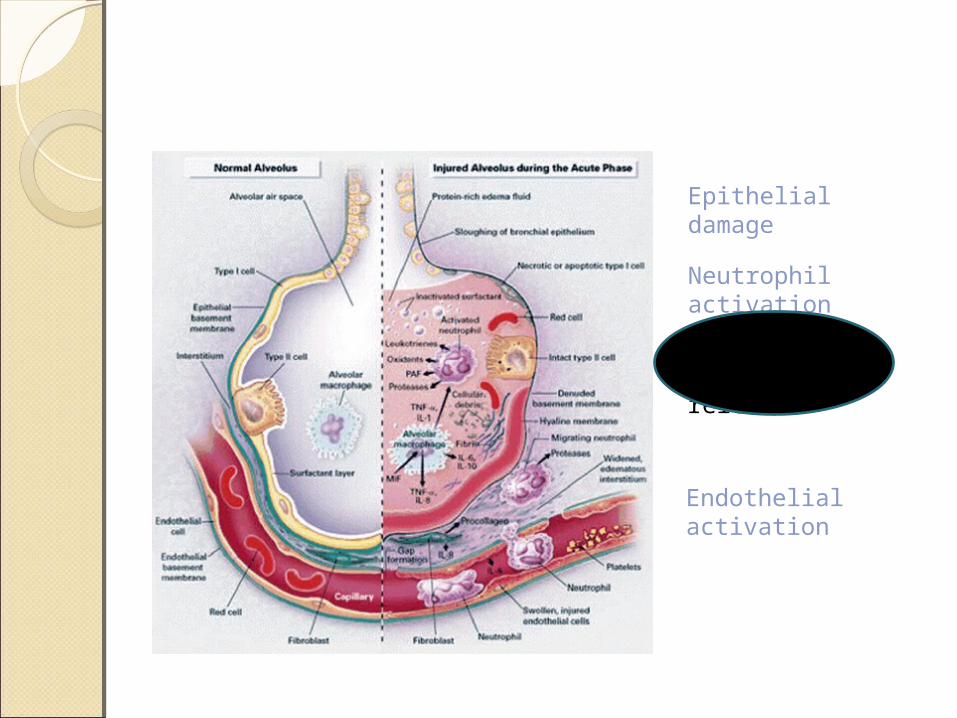
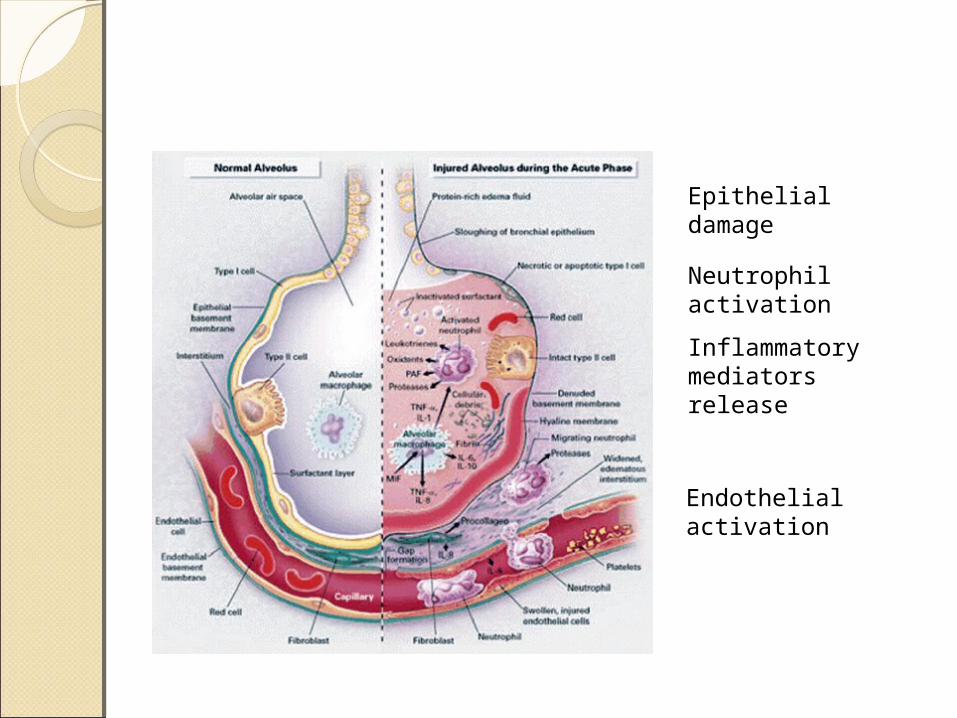
Endothelial activation
Epithelial damage
Neutrophil activation
Inflammatory mediators release
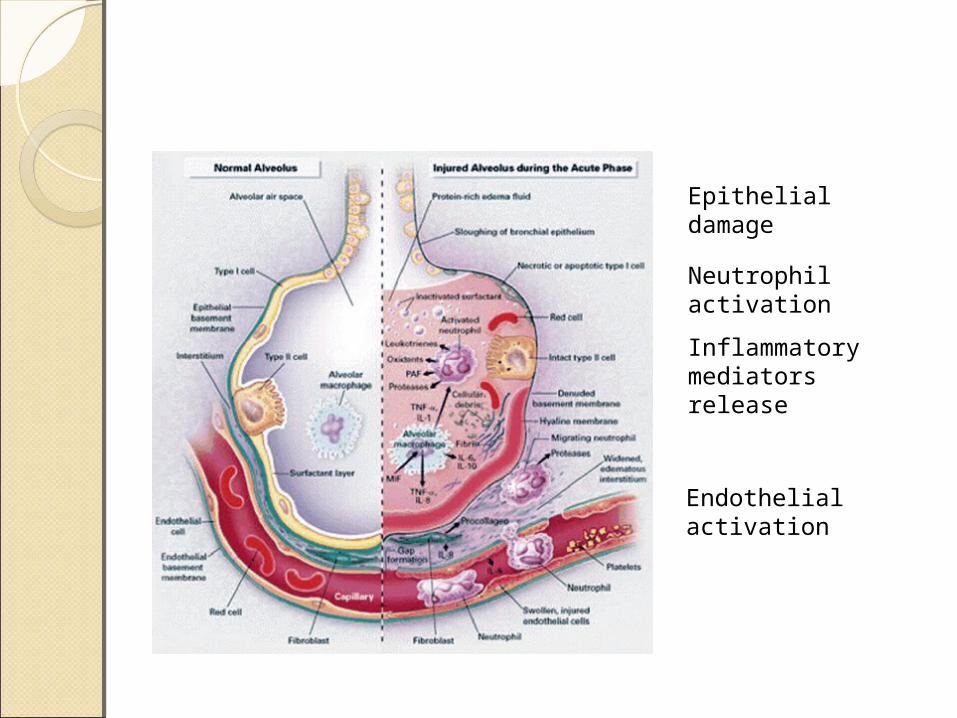
Endothelial activation
Epithelial damage
Neutrophil activation
Inflammatory mediators release

Biomarkers of ARDS and Biomarkers of ARDS and ALI ALI Cytokines
◦IL-1◦IL-2◦IL-6◦IL-8◦IL-15◦TNF-α◦IL-10◦IL-1 ra
Endothelial activation
Epithelial damage
Neutrophil activation
Inflammatory mediators release

Endothelial activation
Epithelial damage
Neutrophil activation
Inflammatory mediators release
Biomarkers of ARDS and Biomarkers of ARDS and ALI ALI Markers of endothelium activation◦Adhesion molecules
E, L-selectin I-CAM-1 V-CAM-1
◦VWF

Endothelial activation
Epithelial damage
Neutrophil activation
Inflammatory mediators release

Endothelial activation
Epithelial damage
Neutrophil activation
Inflammatory mediators release

Biomarkers of ARDS and Biomarkers of ARDS and ALI ALI Markers of neutrophil activation◦Matrix metalloproteinase-9 (MMP-9)◦LTB4
Endothelial activation
Epithelial damage
Neutrophil activation
Inflammatory mediators release

Endothelial activation
Epithelial damage
Neutrophil activation
Inflammatory mediators release

Biomarkers of ARDS and Biomarkers of ARDS and ALI ALI Lung epithelium specific proteins◦Surfactant-associated proteins
SP-A SP-B SP-D
◦Mucin-associated antigens Krebs von den Lungen-6 (KL-6/MUC1)
CytokinesCytokines

Pro-inflammatory cytokines
Anti-inflammatory cytokines
TNF-αIL-10
IL-1IL-1ra
IL-6sTNFR1
IL-8sTNFR2
IL-4IL-6

CytokinesCytokinesCytokines are produced either by
◦local resident cells Alveolar macrophages Pneumocytes Endothelial cells Fibroblasts
◦cells arriving to the lung in response to local or systemic injury Neutrophils Lymphocytes Platelets
TNF-α and IL-1 serum levels are related to ARDS disease severity and mortality(1,2).
Serum levels of IL-6, IL-8 and CD 11b could identify patients with septic shock at risk for organ failure, including respiratory failure (3,4).
1- Marks JD et al., Am Rev Respir Dis 1990, 141:94-7.2- Damas P et al., Crit Care Med 1989, 17:975-8.3- Pinsky MR et al., Chest 1993,103:565-75.4- Takala A et al., Clin Sci (Lond) 1999, 97:529-38.
Some researchers found that serum cytokines could not be used as a routine laboratory test to predict the outcome in septic-shock patients.
Calandra T et al., Am J Med 1991, 91:23-9.

With multiple study limitations, it was found that plasma TNF-α, IL-6, IL-8 fail to associate with severity and course of ARDS in 19 leukocytopenic patients.
Meanwhile, BALF levels appeared to differentiate between responders and non-responders to treatment before clinical differences become apparent.
Kiehl MG et al., Crit Care Med 1998,26:1194-9

Meduri et al. studied plasma levels of various cytokines in 27 ARDS patients.
Consistent, efficient and independent predictive value for IL-1β and IL-6 serum concentrations over time in severe ARDS.
Superiority of IL-1β and IL-6 plasma levels monitoring over commonly applied clinico physiologic parameters.
Meduri GU et al., Chest 1995, 107:1062-73

Agouridakis et al. found an excellent predictive value of plasma IL-2 and IL-15 levels compared to those observed in BALF.
A remarkable finding was the emergence of the discriminative usefulness of elevated IL-2 and IL-15 serum levels in patients with ARDS or at risk for ARDS.
Agouridakis P, et al., Eur J Clin Invest 2002, 32:862-7.

In contrast Lesur et al. found lower blood IL-2 levels in patients with ARDS compared to those that never developed ARDS.
There was a strong association of early low serum IL-2 levels with the patients’ survival
A major criticism to this study is opposite and disproportional fluctuations of IL-2 content in serum and BALF in patients with or without ARDS
Lesur O et al., Crit Care Med 2000, 28:3814-22.
Anti-inflammatory Anti-inflammatory cytokinescytokinesA large prospective (77 patients
at risk of ARDS) found that ◦IL-1ra and IL-10 were elevated in
patients at risk for ARDS
◦IL-1ra and IL-10 exhibited a remarkable association with the disease outcome, but could not predict the development of the syndrome
Parsons PE et al., . Am J Respir Crit Care Med 1997, 155:1469-73.
The inability of serum cytokine levels to predict the development of ARDS in patients with ALI was reproduced by other researchers(1,2).
1- Takala A et al., Shock2002, 17:252-7.2- Bouros D et al., BMC Pulm Med 2004, 4:6.
There is a remarkable consistently elevated serum levels of IL-6 and IL-8 in ARDS and/or severe pneumonia, differentiating these entities from cardiogenic pulmonary oedema.
Serum IL-6 and IL-8 were unable to differentiate ARDS from severe pneumonia
Schutte H, et al., Eur Respir J1996, 9:1858-67.
Limitations in cytokine Limitations in cytokine researchesresearchesNumber of patients is small in
most studiesIncluding heterogeneous groups
of patients in the same studyBlood versus BALF levels of
cytokinesStudying limited number of
molecules
Limitations in cytokine Limitations in cytokine researchesresearchesNot looking at the anti-
inflammatory limb of the cytokine cascade
Lack of serial measurementsStatistical analysis not including
ROC and not reporting cut-off values

Markers of endothelium Markers of endothelium activationactivation

The patho-physiologic sequence characterizing ALI involves a cascade of leukocyte-endothelium interactions and adhesions.
The adhesion is followed by transendothelial migration of neutrophils and release of their cytotoxic products resulting in microvascular and tissue injury.

Adhesion of neutrophils to the endothelium is regulated by ◦selectins (E, L and P)◦Integrins◦immunoglobulin superfamily
ICAM-1 VCAM-1
Interactions of leukocytes and the endothelium ◦An initial “loose” contact (rolling):
selectin ◦Firm adhesion: integrin (β2) and
ICAM-1

Adhesion MoleculesAdhesion MoleculesSoluble isoforms have been detected in
the blood under various inflammatory conditions◦ s-E-selectin◦ sICAM-1◦ sVCAM-1
Mechanisms to explain an increase in circulating adhesion molecules:◦ overexpression by the endothelial cells
induced by cytokines (IL-1, TNF-α)◦ increased proteolytic cleavage of
endothelial-bound adhesion molecules secondary to endothelial damage
Adhesion MoleculesAdhesion MoleculesThe expression is almost
restricted to stimulated endothelial cells
Their presence in serum should potentially reflect the state of endothelium in disease and subsequently the disease severity in ALI

von-Willebrand factor von-Willebrand factor antigenantigenA macromolecular antigen that is
produced by◦endothelial cells◦platelets and megakaryocytes
Endothelial injury (as in ARDS) results in the release of VWF from preformed stores into the circulation.
Donnelly et al. demonstrated in a large cohort of patients at risk for ARDS that◦Mean circulating levels of sE-selectin
were not correlated with subsequent ARDS development and patients' mortality.
◦Low values of sL-selectin exhibited a significant prognostic value
Donnelly SC et al. , Lancet 1994,23(344):215-9

Cowley et al. showed a superiority plasma levels of sE-selectin in predicting organ dysfunction and death in a group of patients with SIRS compared to sICAM-1 peripheral concentrations.
Cowley HC et al., Crit Care Med 1994,22:651-7.
sICAM-1 sequential plasma levels, were suggestive of a strong association between the severity of shock◦the presence of hypotension◦the requirement of vasoactive drugs
and the circulating concentrations of the sICAM-1.
Sessler CN et al., Am J Respir Crit Care Med 1995, 151:1420-7.Kayal S et al., Am J Respir Crit Care Med 1998, 157:776-84.

ICAM-1 and VCAM-1 ICAM-1 and VCAM-1 Were not found to be independent
factor for ARDS development,Exhibited a considerable negative
predictive value for ARDS development.
ROC curve analysis showed a clear superiority of plasma parameters in correlating with the disease outcome compared with BALF molecules
Agouridakis P et al., Respir Res 2002, 3:25.
VWFVWFMarked and independent
association of circulating VWF with the disease severity as assessed by other commonly applied clinical variables.
Serum VWF levels were an independent predictor of hospital mortality and were associated with longer duration of MV
Kayal S et al., Am J Respir Crit Care Med 1998, 157:776-84.Ware LB et al., Crit Care Med 2001, 29:2325-31.
VWFVWFIn a multicenter study of 559 patients with
ALI and ARDS A significant correlation of elevated VWF
plasma levels with adverse outcomes ◦ Mortality◦ duration of unassisted ventilation◦ organ failure
An association between vWF and presence or absence of sepsis, supporting the hypothesis that ALI might be an independent cause of systemic endothelial activation and injury.
No modulation of plasma VWF concentrations by protective mechanical ventilation.
Ware LB et al., Crit Care Med 2001, 29:2325-31.
Markers of neutrophil Markers of neutrophil activationactivation
There is an increasing evidence implicating neutrophils in most cases of ARDS.
Neutrophils have been reported by several studies to exert an important role in the early phase of ALI characterized by ◦architecture remodeling◦Surfactant and epithelial toxicity

Neutrophils use a wide array of enzymes during the process of transmigration through alveolar-capillary barrier.
These enzymes include, metalloproteinases (MMPs) such as MMP-9 also called gelatinase B which is secreted from preformed neutrophil granules in response to proinflammatory cytokines (IL-8, TNF-α).
MMP-9 is secreted as a zymogen, and then activated by other proteases such as elastase, and plays a crucial role in digesting basement membranes.
Pulmonary edema fluid levels of IL-8, MMP-2, MMP-9 could differentiate ARDS and cardiogenic pulmonary edema whereas plasma levels proved to be of poor discriminative value.
These findings raise the issue that the inflammatory response of ARDS patients is well compartmentalized, with little spillover into the circulation.
Pugin J et al., CritCare Med 1999, 27:304-12.

LeukotrienesLeukotrienesLTs (B4, C4, D4, E4) exert a
synergistic role with IL-8 in the neutrophil influx and activation leading to a massive recruitment of neutrophils and a massive inflammatory response.
Their BALF levels have been found elevated in patients with ARDS.
Contribute to alterations of microvascular permeability and accumulation of pulmonary edema.
LTB4 plasma levels could serve as a valuable predictive marker of ARDS in terms of specificity and sensitivity.
There is a strong association of both LTB4 and IL-8 peripheral concentrations with the patients' survival.
Amat M et al., Crit Care Med 2000, 28:57-62.
Lung epithelium-specific Lung epithelium-specific proteinsproteins

The lung epithelium produces mucus blanket and surfactant proteins
Study of BALF is the classical means of studying the proteins secreted by the lung epithelium and investigating their alterations in lung disorders.

The presence of these proteins in the bloodstream can be explained by several mechanisms including◦leakage from the lung into the
bloodstream◦Increased production by the alveolar
type II cells◦diminished clearance rates from the
circulation

Surfactant-associated Surfactant-associated ProteinsProteinsPulmonary surfactant is a
complex and highly surface active material covering the alveolar space of the lung.
Structure◦Mainly phospholipids◦Surfactant proteins
Surfactant-associated Surfactant-associated ProteinsProteinsFunctions of the alveolar
surfactant system:◦Reduce surface tensions of alveoli◦Prevention of alveolar edema◦Pronounced influence, especially of
the collectins (SP-A and SP-D) in the innate immune system of the lung
Serum levels reflect the epithelial damage and turnover.

Surfactant-associated Surfactant-associated ProteinsProteinsFour surfactant-specific proteins
◦SP-A◦SP-B◦SP-C◦SP-D
SP-B and SP-C are low MW hydrophobic
SP-A and SP-D are high MW hydrophilic
SP-A and SP-D belong to the collectin subgroup of the C-type lectin superfamily.
SP-A and SP-D are produced by two types of epithelial cells in the peripheral airway◦Clara cells◦Alveolar type II cells.
SP-ASP-AAcute indicator of lung function
and alveolocapillary membrane injury (1)
SP-A BALF levels are strongly related to outcome and likelihood of disease progression (2)
Plasma levels are associated with severity of clinical lung injury and with disease outcome (3)
1- Doyle IR et al., Am J Respir Crit Care Med 1995, 152:307-17.2- Greene KE et al., Am J Respir Crit Care Med 1999, 160:1843-50.3- Cheng IW et al., Crit Care Med 2003, 31:20-7.
SP-ASP-AThere is a potential value of SP-A
plasma levels in discriminating at risk patients who developed ARDS from those with sepsis and aspiration.(1)
discriminating patients with ALI of various etiologic factors ◦severe pneumonia◦cardiogenic lung edema.
(2)
1- Greene KE et al., Chest 1999, 116:90S-91S.2- Gunther A et al., Am J Respir Crit Care Med 1996, 153:176-84
SP-BSP-BSuperior to SP-A plasma levels as a
marker of ◦lung function◦alveolocapillary membrane injury.(1)
SP-B cut-off plasma levels predict ARDS development in at-risk patients suffering a direct lung injury
An increase of blood SP-B levels was observed before other changes of ALI become apparent.(2)
1- Doyle IR et al., Am J Respir Crit Care Med 1997, 156:1217-29.2- Bersten AD et al., Am J Respir Crit Care Med 2001, 164:648-52.

SP-DSP-DSP-A BALF levels are strongly
related to outcome and likelihood of disease progression.(1)
In a large RCT◦Elevated SPD levels were associated
with worse clinical outcomes Greater risk of death Fewer ventilator- free days Fewer organ failure-free days
◦Attenuation of SP-D plasma levels by lower volume ventilation strategies .(2)
1- Greene KE et al., Am J Respir Crit Care Med 1999, 160:1843-50.2- Eisner MD et al., Thorax 2003, 58:983-8.

Mucin-associated AntigensMucin-associated AntigensMucins are major components of
the mucus layer covering the airway epithelium.
Mucins are either ◦associated with cell membranes or ◦secreted at the surface of the
respiratory tract

KL-6KL-6Krebs von den Lungen-(KL)-6 is a
mucin-associated antigen mainly associated with cellular membranes.
KL-6 is mainly detected in ◦alveolar type II cells◦epithelial cells of the respiratory
bronchioles.It is also present on other somatic
cells◦pancreatic cells◦eosophageal cells◦fundic cells of the stomach
KL-6KL-6 KL-6 is a sensitive indicator of
damage to alveolar type II cellsIts raise would theoretically
represent ◦the destruction of the normal lung
parenchyma and architecture◦the increased permeability of the air-
blood barrier
KL-6KL-6Association of optimal cut-off
values of KL-6 serum levels with patients' mortality with high sensitivity (87%) and specificity (100%)
This finding supports the theory that disruption of the alveolar barrier represents a major determinant of prognosis of ALI
Ishizaka A et al., Am J Physiol Lung Cell Mol Physiol 2004, 286:L1088-94.

KL-6KL-6Association of KL-6 serum levels
with variables of lung injury severity and with mortality rates.
No statistically significant correlation between blood levels and ventilation strategies.
Sato H et al., Eur Respir J 2004,23:142-5.
SummarySummaryThe ideal biomarkerCytokinesProducts of endothelial activationProducts of neutrophil activationLung epithelium-specific proteins
Future directionsFuture directionsFinding and applying the ideal
biomarker in the clinical setting would be very helpful in terms of ◦Defining categories of patients for
different therapies or prognosis.◦For the purpose of counseling
families and patients regarding high/low risk of complications.
◦Possibly identifying novel therapeutic targets.

Future directionsFuture directionsDevelopment of a prognostic
index that combines clinical and biological determinants may be useful to ameliorate the limitations encountered using only biomarkers.
A combination index could be crucial for the selection of more homogeneous groups of patients with ALI/ARDS for further studies.
Future directionsFuture directionsCrossing the boundary from
research to clinical application requires ◦Validation in multiple settings◦Experimental evidence supporting a
pathophysiologic role ◦Ideally intervention trials showing
that modification improves the outcome

ConclusionConclusion

ConclusionConclusionCurrently, the application status in
routine clinical practice for most of these biologic markers of ALI is still in its infancy and remains exploratory.
It is important to note that the greatest promise is in only few (VWF, IL-1β, IL-6, ICAM-1, VCAM-I, E-selectin) which exhibited independent discriminatory power.

ConclusionConclusionThere is a necessity for further
investigations in the context of large prospective studies analyzing homogeneous and well defined group of ARDS or at risk patients and the assessment of novel molecules to serve as diagnostic and prognostic tools, as well as markers of the disease activity and severity.
The question remains ….The question remains ….

How much have we moved How much have we moved from here?from here?

Thank youThank you