biogen access toolkit - tysabrihcp.com...treatment selected complete the biogen product start form...
TRANSCRIPT
Biogen Access Toolkit
2 | Access Toolkit
Welcome to the Biogen Access Toolkit!
a This resource focuses on specialty pharmacy and does not address the buy-and-bill process for infusible products. The focus is on self-administered drugs, such as orals and injectables, covered under the pharmacy benefit. Contact your Biogen representative for more information on the buy-and-bill process for infused products.
For more information about insurance coverage for Biogen products, contact Above MS at 1-800-456-2255, Monday through Friday, 8:30 AM to 8 PM ET, or at AboveMS.com.
Obtaining approval for your patient’s medication for relapsing multiple sclerosis (RMS) often requires your office to complete several steps, such as gaining approval of a prior authorization (PA), also known as a precertification, or requesting a medical exception (ME).a In addition, your office may need to coordinate with a specialty pharmacy to ensure all payer approvals are obtained and the medication is shipped.
The Biogen Access Toolkit provides a comprehensive resource to assist your office in navigating the process to gain access and approval of your patient’s RMS treatment once prescribed. This toolkit provides various resources to help you with the following along the way:
Understanding the steps to product access. Open this page to see these steps. The action item for each step in the process is included, as well as tips and resources provided in this toolkit.
Completing the Biogen product Start Form.
Submitting PAs and MEs.
Tracking patient benefit and insurance information.
Explaining the differences between medical and pharmacy benefit card information.
Above MS Can Help
The Above MS™ program can assist your office in navigating the process of obtaining coverage for a patient’s prescribed Biogen product for RMS. The program can also help your patients with support along their journey. Here are some of the benefits that Above MS offers:
Above MS can conduct a patient’s benefits investigation and initiate the PA process. This support from Above MS are automatic when your patient signs Sections A and B of the Biogen product Start Form.
If you are concerned with how long the insurance approval process is taking, contact Above MS.
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
3 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Biogen Access Toolkit: Table of Contents
Steps to Product Access ...............................................................................Page 4This foldout resource provides an overview of each step in the product access process, as well as resources provided by Biogen to help with the process of obtaining insurance approval.
Tips to Successfully Completing a Biogen Product Start Form .........................Page 5 This guide explains the Biogen product Start Form and provides tips on how to complete each section.
Medical and Pharmacy Benefit Card Information ...........................................Page 16This section includes information to help your office understand the differences for the commercial, Medicare, and Medicaid medical and pharmacy benefit cards for your patients.
Guide to Prior Authorization Submissions......................................................Page 23 This guide provides steps and tips when submitting a prior authorization.
Guide to Requesting a Medical Exception.....................................................Page 36This guide provides templates and tips for submitting a medical exception.
Sample Letter Templates ............................................................................ Page 43There are 5 different sample letter templates, each based on a different patient insurance coverage situation. Each letter includes a list of the documentation that can accompany the request, if necessary.
Patient Benefit and Insurance Tracker ....................................Available on flash driveThis Excel tracker enables your office to capture information during the benefit investigation and log updates.
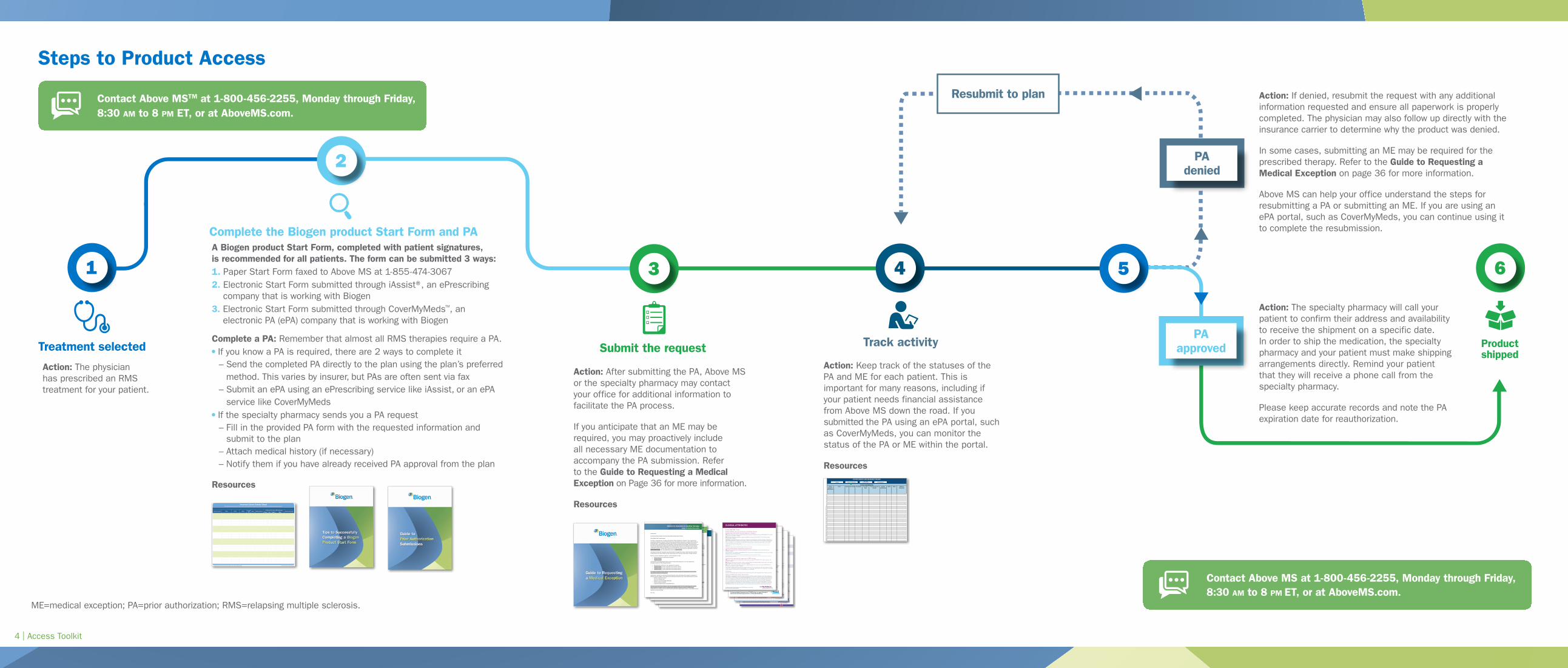
Treatment selected
Complete the Biogen product Start Form and PA
Action: The physician has prescribed an RMS treatment for your patient.
Action: Keep track of the statuses of the PA and ME for each patient. This is important for many reasons, including if your patient needs financial assistance from Above MS down the road. If you submitted the PA using an ePA portal, such as CoverMyMeds, you can monitor the status of the PA or ME within the portal.
Resources
Action: After submitting the PA, Above MS or the specialty pharmacy may contact your office for additional information to facilitate the PA process.
If you anticipate that an ME may be required, you may proactively include all necessary ME documentation to accompany the PA submission. Refer to the Guide to Requesting a Medical Exception on Page 36 for more information.
Resources
A Biogen product Start Form, completed with patient signatures, is recommended for all patients. The form can be submitted 3 ways:1. Paper Start Form faxed to Above MS at 1-855-474-30672. Electronic Start Form submitted through iAssist®, an ePrescribing
company that is working with Biogen3. Electronic Start Form submitted through CoverMyMeds™, an
electronic PA (ePA) company that is working with Biogen
Complete a PA: Remember that almost all RMS therapies require a PA. If you know a PA is required, there are 2 ways to complete it– Send the completed PA directly to the plan using the plan’s preferred
method. This varies by insurer, but PAs are often sent via fax– Submit an ePA using an ePrescribing service like iAssist, or an ePA
service like CoverMyMeds If the specialty pharmacy sends you a PA request– Fill in the provided PA form with the requested information and
submit to the plan– Attach medical history (if necessary)– Notify them if you have already received PA approval from the plan
Resources
Track activity
1 4
Steps to Product Access
Insurance Carrier Name Phone EmailContact
RoleDept. Additional Notes
Preference for PA and/or ME SubmissionsRelevant Web Links
Phone Fax Email Other
Insurance Carrier Contact SheetThe Insurance Carrier Contact Sheet resource will enable you to capture key contact information and related processes for payers.
ME=medical exception; PA=prior authorization.For infusible products, please see the Payer Summary Reference Guide resource available from Biogen.
PatientAccount#/Identification
Name Gender DateofBirth Neurologist PrescribedDrug
PharmacyInsuranceProvider
MemberIdentification
RxBIN RxGrp
1234567891011121314151617181920212223242526272829303132333435363738394041424344454647484950515253545556575859606162636465666768697071727374
PATIENTINFORMATION
PATIENTBENEFITANDINSURANCETRACKER
AdditionalInformation
Pa-entInforma-onHome Benefits Investigation PA Request
Submit the request
3 5
2
Action: If denied, resubmit the request with any additional information requested and ensure all paperwork is properly completed. The physician may also follow up directly with the insurance carrier to determine why the product was denied.
In some cases, submitting an ME may be required for the prescribed therapy. Refer to the Guide to Requesting a Medical Exception on page 36 for more information.
Above MS can help your office understand the steps for resubmitting a PA or submitting an ME. If you are using an ePA portal, such as CoverMyMeds, you can continue using it to complete the resubmission.
PA denied
Treatment-‐naïve patient Letter of Medical Necessity
[Insert Date]
RE: [Patient Name], [Patient Insurance ID Number], [Patient Date of Birth]
Dear [Health Plan Contact Name]:
This letter is regarding your coverage policy of [Enter Product Name] for my patient. I have reviewed your prescription drug policy; however, I feel that the most appropriate treatment for my patient falls outside the established policy. Therapy decisions are best left to be determined by patients and their physicians, and it has been my experience that the disease-‐modifying therapies to treat relapsing multiple sclerosis (RMS) are not interchangeable. They may vary in efficacy, administration, mechanisms of action, and side effects. Based on my extensive experience in treating RMS, the most appropriate medication for initiating therapy for [his/her] RMS is [Enter Product Name].
I have evaluated my patient’s clinical symptoms and have provided a summary below: • [MRI data] • [Physical disability] • [Relapse] • [Laboratory values]
I am prescribing [Enter Product Name] for my patient because I have concluded that it is the most appropriate therapeutic option for [him/her] for the following reason(s):
• [Reason(s) this treatment is most appropriate for patient] • [Choose an item.] [Further explanation for treatment choice] • [Choose an item.] [Further explanation for treatment choice] • [Choose an item.] [Further explanation for treatment choice]
[If a step therapy before [Product Name] is required, include reason(s) why step therapy would not be an appropriate treatment for this patient.]
Also, I ask that you review any clinical information I have submitted regarding my patient when considering my request, as well as reviewing clinical guidelines and recent clinical trial results. I have indicated the additional information that I have submitted with this letter below:
� Relevant medication history � Anti-‐JCV antibody status � MRI data � Patient’s history of relapses � EDSS history
[Provide reason(s) that [Product Name] is the most appropriate treatment for this patient based on medical history, positive or negative anti-‐JCV antibody status, MRI data, history of relapses, or EDSS history.] Please feel free to contact me if you require further information regarding this request. I look forward to your response as soon as possible. Sincerely,
Patient to remain on current therapy Letter Medical Necessity
[Insert Date]
RE: [Patient Name], [Patient Insurance ID Number], [Patient Date of Birth]
Dear [Health Plan Contact Name]:
This letter is regarding your coverage policy that requires me to take my patient off of [Enter Product Name]. I have reviewed your prescription drug policy; however, I feel that the most appropriate therapy at this time is to continue on [Enter Product Name] for my patient’s relapsing multiple sclerosis (RMS). Therapy decisions are best left to be determined by patients and their physicians, and it has been my experience that the disease-‐modifying therapies to treat RMS are not interchangeable. They may vary in efficacy, administration, mechanisms of action, and side effects. Movement to another drug therapy may impact the progress we have made to date.
I have been working with my patient since [Insert Date] to manage their disease. My patient has been on [Enter Product Name] since [Insert Date], and during this time my patient has maintained progress and shown stability with treatment, as summarized below:
• [No new lesions as evidenced by MRI data] since [Insert Date] • [No decline in disability status] as of [Insert Date]
Additionally, in my medical opinion, I believe that transitioning therapy may cause unnecessary harm to my patient for the following reason(s): [Insert reason(s)]. I have included additional documentation regarding my patient, which supports my decision. I ask that you review the information I have indicated below when reviewing my request:
� Relevant medication history � Anti-‐JCV antibody status � MRI data � Patient’s history of relapses � EDSS history
[Provide the reason(s) that [Product Name] is the most appropriate treatment for this patient based on medical history, positive or negative anti-‐JCV antibody status, MRI data, history of relapses, or EDSS history.] Please feel free to contact me if you require further information regarding this request. I look forward to your response as soon as possible.
Sincerely, [Name]
Patient to transition to another therapy Letter of Medical Necessity
[Insert Date]
RE: [Patient Name], [Patient Insurance ID Number], [Patient Date of Birth]
Dear [Health Plan Contact Name]:
This letter is regarding your coverage policy of [Enter Product Name] for my patient. I have reviewed your prescription drug policy; however, I feel that the most appropriate treatment for my patient falls outside the established policy. The appropriate therapy at this juncture is to discontinue [Enter Product Name] and to prescribe [Enter Product Name] to treat my patient’s relapsing multiple sclerosis (RMS). Therapy decisions are best left to be determined by patients and their physicians, and it has been my experience that the disease-‐modifying therapies (DMTs) to treat RMS are not interchangeable. They may vary in efficacy, administration, mechanisms of action, and side effects. Based on my extensive treatment experience with DMTs, I feel that [Enter Product Name] is the most appropriate choice for [Patient Name].
I have been working with my patient since [Insert Date] to manage their disease. They have been on [Enter Product Name] since [Insert Date], and the limited results that I have seen necessitate a change treatment.
My main concerns regarding my patient’s current medication include
• [Reason(s) previous treatment(s) unsuitable] • [Choose an item.] • [Choose an item.]
I recommend converting [Patient Name] to [Enter Product Name] because it is the most appropriate therapeutic option for the following reason(s):
• [Reason(s) this treatment is most appropriate for patient] • [Choose an item.] [Further explanation for treatment choice] • [Choose an item.] [Further explanation for treatment choice] • [Choose an item.] [Further explanation for treatment choice]
[If a step therapy before [Product Name] is required, include reason(s) why step therapy would not be an appropriate treatment for this patient.]
Additionally, I ask that you review the clinical information I have submitted, which supports my decision to change medication. Below, I have indicated the additional information that I have submitted with this letter:
� Relevant medication history � Anti-‐JCV antibody status � Magnetic resonance imaging (MRI) data � Patient’s history of relapses � Expanded Disability Status Scale (EDSS) history
[Provide reason that [Product Name] is the most appropriate treatment for this patient based on medical history, positive or negative anti-‐JCV antibody status, MRI data, history of relapses, or EDSS history.] Please feel free to contact me if you require further information regarding this request. I look forward to your response as soon as possible. Sincerely,
Resubmit to plan
Action: The specialty pharmacy will call your patient to confirm their address and availability to receive the shipment on a specific date. In order to ship the medication, the specialty pharmacy and your patient must make shipping arrangements directly. Remind your patient that they will receive a phone call from the specialty pharmacy.
Please keep accurate records and note the PA expiration date for reauthorization.
PA approved
6
Product shipped
Contact Above MSTM at 1-800-456-2255, Monday through Friday, 8:30 AM to 8 PM ET, or at AboveMS.com.
Contact Above MS at 1-800-456-2255, Monday through Friday, 8:30 AM to 8 PM ET, or at AboveMS.com.
For additional Important Safety Information about AVONEX, please see reverse side and enclosed Full Prescribing Information.
AVONEX Indication and Important Safety InformationIndicationAVONEX® (interferon beta-1a) is indicated for the treatment of patients with relapsing forms of multiple sclerosis to slow the accumulation of physical disability and decrease the frequency of clinical exacerbations. Patients with multiple sclerosis in whom efficacy has been demonstrated include patients who have experienced a first clinical episode and have MRI features consistent with multiple sclerosis.
Important Safety Information Patients and their caregivers should be advised to report immediately any symptoms of depression,
suicidal ideation, or psychosis to their prescribing physician. These symptoms, and cases of suicide, have been reported with increased frequency with patients receiving AVONEX. If a patient develops depression or other severe psychiatric symptoms, cessation of AVONEX therapy should be considered.
Severe hepatic injury, including cases of hepatic failure, has been reported rarely in patients taking AVONEX. Patients should be monitored for signs of hepatic injury and caution exercised when AVONEX is used concomitantly with alcohol or other drugs associated with hepatic injury.
Clinical Attributes
AVONEX delays physical disability progression
37% reduction in risk of increased physical disability with AVONEX at 2 years vs placebo (p=0.02)1
AVONEX significantly reduces relapses and is proven effective for patients with early signs of multiple sclerosis (MS) and clinically isolated syndrome (CIS)
32% reduction in annualized relapse rate (ARR) among patients completing 2 years (p=0.002)2,a
a When the analysis includes patients who did not complete 2 years on therapy, AVONEX reduced ARR by 18% vs placebo (0.67 vs 0.82, respectively; p=0.04).1
51% reduction in clinically definite multiple sclerosis (CDMS) conversion with AVONEX at 3 years vs placebo (adjusted, p<0.001; 44% unadjusted, p=0.002)1,3
AVONEX has been shown to significantly reduce brain lesions
75% reduction in gadolinium-enhancing (Gd+) lesions vs baseline at 2 years1,b,c
91% reduction in T2 lesion volume vs placebo at 18 months (p<0.001)1,d,e
The exact relationship between magnetic resonance imaging (MRI) findings and a patient’s clinical status is unknown.
©2016Biogen. Allrightsreserved. Printed in the U.S.A. 08/16 AVX-US-0193
For additional Important Safety Information about AVONEX, please see reverse side and enclosed Full Prescribing Information.
AVONEX Indication and Important Safety Information (cont’d)Important Safety Information
Rare cases of anaphylaxis have been reported. Other allergic reactions have included dyspnea, orolingual edema, skin rash and urticaria.
While beta interferons do not have any known direct cardiac toxicity, cases of congestive heart failure, cardiomyopathy, and cardiomyopathy with congestive heart failure have been reported in patients without known predisposition. Patients with these pre-existing conditions should be monitored for worsening of their cardiac condition during initiation and continued treatment with AVONEX.
Decreased peripheral blood counts in all cell lines, including rare pancytopenia and thrombocytopenia, have been reported from postmarketing experience.
Cases of thrombotic microangiopathy (TMA), including thrombotic thrombocytopenic purpura and hemolytic uremic syndrome, some fatal, have been reported with interferon beta products, including AVONEX. Cases have been reported several weeks to years after starting interferon beta products. Discontinue AVONEX if clinical symptoms and laboratory findings consistent with TMA occur, and manage as clinically indicated.
Seizures have been reported in patients using AVONEX, including in patients with no prior history of seizure. It is not known whether these events were related to the effects of multiple sclerosis alone, to AVONEX, or to a combination of both.
Autoimmune disorders of multiple target organs have been reported. If patients develop a new autoimmune disorder, consider stopping therapy.
Routine periodic blood chemistry, hematology, liver function, and thyroid function tests are recommended during treatment with AVONEX.
There are no adequate and well-controlled studies in pregnant women. AVONEX should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
The most common side effects associated with AVONEX treatment are flu-like symptoms including chills, fever, myalgia, and asthenia.
b Results from the Multiple Sclerosis Collaborative Research Group (MSCRG) trial, a 2-year, pivotal, randomized, double-blind, placebo-controlled phase III trial of the efficacy of treatment with AVONEX in 301 patients diagnosed with CDMS for at least 1 year who had baseline Expanded Disability Status Scale scores of 1.0 to 3.5.
cCompared with a 30% reduction vs baseline for placebo.
d Results from the Controlled High-Risk Subjects AVONEX Multiple Sclerosis Prevention Study (CHAMPS), a 3-year, pivotal, randomized, double-blind, placebo-controlled phase III trial of the efficacy of treatment with AVONEX after a first clinical event (N=383). Patients had experienced a first acute demyelinating event and had MRI features consistent with MS. Results were adjusted for age, qualifying event, baseline MRI T2 lesion volume, and baseline number of Gd+ lesions shown on MRI.
eChange from baseline in T2 lesion volume: 28 mm
3 (AVONEX) vs 313 mm
3 (placebo).
References: 1. AVONEX [Prescribing Information]. Cambridge, MA: Biogen; March 2016. 2. Jacobs LD, Cookfair DL, Rudick RA, et al; Multiple Sclerosis Collaborative Research Group (MSCRG). Intramuscular interferon beta-1a for disease progression in relapsing multiple sclerosis. Ann Neurol. 1996;39(3): 285-294. 3. Jacobs LD, Beck RW, Simon JH, et al; CHAMPS Study Group. Intramuscular interferon beta-1a therapy initiated during a first demyelinating event in multiple sclerosis. N Engl J Med. 2000;343(13):898-904.
For additional Important Safety Information about PLEGRIDY, please see reverse side and enclosed full Prescribing Information.
Clinical Attributes
PLEGRIDY® (peginterferon beta-1a) had statistically significant effects on
the clinical and MRI endpoints at 1 year1,a
Clinical endpoints• 36% relative risk reduction in annualized relapse rate (ARR)b (PLEGRIDY 0.26 vs placebo 0.40; P=0.0007)
• 39% relative risk reduction in the proportion of patients with relapses (PLEGRIDY 0.19 vs placebo 0.29; P=0.0003)
• 38% relative risk reduction in the proportion of patients with disability progression (PLEGRIDY 0.07 vs placebo 0.11; P=0.0383)
MRI endpoints• 67% relative risk reduction in the mean number of new or newly enlarging T2 hyperintense lesions
(PLEGRIDY 3.6 vs placebo 10.9; P<0.0001)
• 86% relative risk reduction in the mean number of Gd-enhancing lesions (PLEGRIDY 0.2 vs placebo 1.4; P<0.0001)
Every-2-week dosing for only 26 subcutaneous injections per yeara Study population: The study included patients with relapsing MS who had a baseline Expanded Disability Status Scale (EDSS) score of 0.0–5.0 and ≥2 relapses within the 3 years prior to the study, with at least 1 within the 12 months prior to randomization.
Study design: The efficacy of PLEGRIDY was assessed from the placebo-controlled first year (48 weeks) of a 2-year study, including 1512 patients with relapsing MS. The primary endpoint was ARR. Secondary endpoints included the proportion of patients relapsing, new or newly enlarging T2 hyperintense lesions, and time to confirmed disability progression, defined as at least 1-point increase from a baseline EDSS score of 1, or a 1.5-point increase for patients with a baseline EDSS score of 0, sustained for 12 weeks. The trial excluded patients with progressive forms of MS.1,2
bPrimary endpoint.
Indication
PLEGRIDY® (peginterferon beta-1a) is indicated for the treatment of patients with relapsing forms of multiple sclerosis.
Important Safety Information
• PLEGRIDY is contraindicated in patients with a history of hypersensitivity to natural or recombinant interferon beta or peginterferon, or any other component of the formulation.
• Severe hepatic injury, including hepatitis, autoimmune hepatitis, and rare cases of severe hepatic failure, have been reported with interferon beta. Asymptomatic elevation of hepatic transaminases has also been reported, and in some patients has recurred upon rechallenge with interferon beta. Elevations in hepatic enzymes and hepatic injury have been observed with PLEGRIDY in clinical studies. The incidence of elevations of ALT and AST above 5 times the upper limit of normal was 2% in PLEGRIDY-treated patients (1% placebo) and was <1% in PLEGRIDY-treated patients (<1% placebo), respectively. Monitor liver function tests and patients for signs of hepatic injury. Consider discontinuation of PLEGRIDY if hepatic injury occurs.
Important Safety Information (cont’d)
• Depression, suicidal ideation, and suicide occur more frequently in patients receiving interferon beta than in patients receiving placebo. The overall incidence of adverse events related to depression and suicidal ideation was 8% in both the PLEGRIDY and placebo groups. The incidence of serious events was similar and less than 1% in both groups. Advise patients to report immediately any symptom of depression or suicidal ideation. If a patient develops depression or other severe psychiatric symptoms, consider stopping treatment with PLEGRIDY.
• Seizures are associated with the use of interferon beta. The incidence of seizures in clinical studies was less than 1% in patients receiving PLEGRIDY and placebo. Exercise caution when administering PLEGRIDY to patients with a seizure disorder.
• Anaphylaxis and other serious allergic reactions are rare complications of treatment with interferon beta. Less than 1% of PLEGRIDY-treated patients experienced a serious allergic reaction such as angioedema or urticaria. Discontinue PLEGRIDY if a serious allergic reaction occurs.
• Injection site reactions, including injection site necrosis, can occur with the use of subcutaneous interferon beta. The incidence of injection site reactions (e.g., injection site erythema, pain, pruritus, or edema) was 66% in the PLEGRIDY group (3% were severe) and 11% in the placebo group (0% were severe). One patient out of 1468 patients who received PLEGRIDY experienced injection site necrosis. Decisions to discontinue therapy following necrosis at a single injection site should be based on the extent of the necrosis. If therapy is continued, avoid administration of PLEGRIDY near the affected area until it is fully healed. If multiple lesions occur, discontinue PLEGRIDY until healing occurs.
• Congestive heart failure, cardiomyopathy, and cardiomyopathy with congestive heart failure occur in patients receiving interferon beta. The incidence of cardiovascular events was 7% in both PLEGRIDY and placebo treatment groups. Monitor patients with significant cardiac disease for worsening of their cardiac condition during initiation and continuation of treatment with PLEGRIDY.
• Interferon beta can cause decreased peripheral blood counts in all cell lines, including rare instances of pancytopenia and severe thrombocytopenia. Decreases in white blood cell counts below 3.0 x 10
9/L
occurred in 7% of patients receiving PLEGRIDY and in 1% receiving placebo. The incidence of clinically significant decreases in lymphocyte counts (below 0.5 x 10
9/L), neutrophil counts (below 1.0 x 10
9/L),
and platelet counts (below 100 x 109/L) were all less than 1% and similar in both placebo and PLEGRIDY
groups. Monitor patients for infections, bleeding, and symptoms of anemia. Monitor complete blood cell counts, differential white blood cell counts, and platelet counts during treatment with PLEGRIDY. Patients with myelosuppression may require more intensive monitoring of blood cell counts.
• Cases of thrombotic microangiopathy (TMA), including thrombotic thrombocytopenic purpura and hemolytic uremic syndrome, some fatal, have been reported several weeks to years after starting interferon beta products. Discontinue PLEGRIDY if clinical symptoms and laboratory findings consistent with TMA occur, and manage as clinically indicated.
• Autoimmune disorders of multiple target organs including idiopathic thrombocytopenia, hyper- and hypothyroidism, and autoimmune hepatitis have been reported with interferon beta. The incidence of autoimmune disorders was less than 1% in both PLEGRIDY and placebo treatment groups. If patients develop a new autoimmune disorder, consider stopping PLEGRIDY.
• The most common adverse reactions (incidence greater than 10% and at least 2% more than placebo) associated with PLEGRIDY treatment are injection site erythema, influenza-like illness, pyrexia, headache, myalgia, chills, injection site pain, asthenia, injection site pruritus, and arthralgia.
For additional Important Safety Information about PLEGRIDY, please see reverse side and enclosed full Prescribing Information.
References: 1. PLEGRIDY [Prescribing Information]. Cambridge, MA: Biogen; October 2015. 2. Calabresi PA, Kieseier BC, Arnold DL, et al; for the ADVANCE Study Investigators. Pegylated interferon beta-1a for relapsing-remitting multiple sclerosis (ADVANCE): a randomised, phase 3, double-blind study. Lancet Neurol. 2014;13(7):657-665.
©2016Biogen. Allrightsreserved. PrintedintheU.S.A. 04/16 PLG-US-0300
14
© 2016 Biogen. All rights reserved. Printed in the U.S.A. 06/16 TYS-US-0557
3
Results of AFFIRM (NAtalizumab Safety and EFFIcacy in Relapsing-Remitting Multiple Sclerosis), a 2-year, global, multicenter, double-blind, parallel-group trial that randomized 942 patients (in a 2:1 ratio) to receive either TYSABRI monotherapy (300 mg by intravenous infusion [n=627]) or placebo (n=315) every 4 weeks for up to 28 months (30 infusions).1,2
a�The�primary�endpoint�at�2�years�was�time�to�onset�of�sustained�increase�in�disability,�defined�as�an�increase�of�≥1.0�point�on�the�EDSS�from�baseline�EDSS�≥1.0�that�was�sustained�for�12�weeks,�or�≥1.5-point�increase�on�the�EDSS�from�baseline�EDSS=0�that�was�sustained�for�12�weeks.�Increase�excluded�disability�confirmation�within�30�days�of a relapse.
CLINICAL ATTRIBUTES
For Important Safety Information about TYSABRI, please see pages 2 through 4 and enclosed Full Prescribing Information, including Boxed Warning.
Contraindications • TYSABRI is contraindicated in patients who have or have had PML.• TYSABRI is contraindicated in patients who have had a hypersensitivity reaction to TYSABRI.
Indication TYSABRI® (natalizumab) is indicated as monotherapy for the treatment of patients with relapsing forms of multiple sclerosis. TYSABRI increases the risk of PML. When initiating and continuing treatment�with�TYSABRI,�physicians�should�consider�whether�the�expected�benefit�of�TYSABRI�is� sufficient�to�offset�this�risk.�See�Important�Safety�Information�regarding�the�risk�of�PML�with�TYSABRI.
Demonstrated Efficacy on Physical Disability Progression
42% relative reduction in the risk of increased physical disability sustained for 12 weeks vs placebo (0.17 vs 0.29)1,a
83% of TYSABRI patients were free of 12-week sustained physical disability progression at 2 years vs 71% of placebo patients (p<0.001)1
Proven Reduction of Relapse Rates
67% relative reduction in annualized relapse rate at 2 years vs placebo (0.22 vs 0.67)1
67% of TYSABRI patients were free of relapse at 2 years vs 41% of placebo patients (p<0.001)1
Established Reduction in MRI activity
92% relative reduction in the mean number of Gd+ lesions at 2 years vs placebo (0.1 vs 1.2; p<0.001)2
83% relative reduction in the mean number of new or enlarging T2-hyperintense lesions at 2 years (1.9 vs 11.0; p<0.001)2
4
Immunosuppression/Infections• The immune system effects of TYSABRI may increase the risk for infections.• In Study MS1, certain types of infections—including pneumonias and urinary tract infections
(including serious cases), gastroenteritis, vaginal infections, tooth infections, tonsillitis, and herpes infections—occurred more often in TYSABRI-treated patients than in placebo-treated patients. One opportunistic infection, a cryptosporidial gastroenteritis with a prolonged course, was observed in a patient who received TYSABRI in Study MS1.
• In Studies MS1 and MS2, an increase in infections was seen in patients concurrently receiving short courses of corticosteroids. However, the increase in infections in TYSABRI-treated patients who received steroids was similar to the increase in placebo-treated patients who received steroids.
• Concurrent use of antineoplastic, immunosuppressant, or immunomodulating agents may further increase the risk of infections over the risk observed with use of TYSABRI alone.
• In�Studies�MS1�and�MS2,�the�rate�of�any�type�of�infection�was�approximately�1.5�per�patient-year�in�both TYSABRI-treated patients and placebo-treated patients.
• In�Study�MS1,�the�incidence�of�serious�infections�was�approximately�3%�in�TYSABRI-treated�patients�and�in placebo-treated patients. Most patients did not interrupt treatment with TYSABRI during infections.
Laboratory Test Abnormalities • In clinical trials, TYSABRI was observed to induce increases in circulating lymphocytes, monocytes,
eosinophils, basophils, and nucleated red blood cells. Observed changes persisted during TYSABRI exposure,�but�were�reversible,�returning�to�baseline�levels�usually�within�16�weeks�after�the�last�dose. Elevations of neutrophils were not observed. TYSABRI induces mild decreases in hemoglobin levels (mean decrease of 0.6g/dL) that are frequently transient.
Adverse Reactions• The�most�common�adverse�reactions�reported�at�an�incidence�of�≥10%�with�TYSABRI�and�≥2%�
difference with placebo were headache (38% vs 33%), fatigue (27% vs 21%), infusion reactions (24% vs 18%), urinary tract infections (21% vs 17%), arthralgia (19% vs 14%), depression (19% vs 16%), pain in�extremity�(16%�vs�14%),�rash�(12%�vs�9%),�gastroenteritis�(11%�vs�9%),�and�vaginitis�(10%�vs�6%).
• The most frequently reported serious adverse reactions in Study MS1 were infections (3.2% vs 2.6% placebo), including urinary tract infection (0.8% vs 0.3%) and pneumonia (0.6% vs 0%), acute hypersensitivity�reactions�(1.1%�vs�0.3%,�including�anaphylaxis/anaphylactoid�reaction�[0.8%�vs�0%]),�depression (1.0% vs 1.0%, including suicidal ideation or attempt [0.6% vs 0.3%]), and cholelithiasis (1.0% vs 0.3%).
• Based on animal data, TYSABRI may cause fetal harm. TYSABRI should be used during pregnancy only�if�the�potential�benefit�justifies�the�potential�risk�to�the�fetus.
For additional Important Safety Information about TYSABRI, please see pages 1 through 3 and enclosed Full Prescribing Information, including Boxed Warning.
References: 1. TYSABRI [Prescribing Information]. Cambridge, MA: Biogen; May 2016. 2. Polman CH, O’Connor PW, Havrdova E, et al. A randomized, placebo-controlled trial of natalizumab for relapsing multiple sclerosis. N Engl J Med. 2006;354(9):899-910.
Contraindications• TYSABRI is contraindicated in patients who have or have had PML. • TYSABRI is contraindicated in patients who have had a hypersensitivity reaction to TYSABRI.
TYSABRI TOUCH Prescribing Program• Because of the risk of PML, TYSABRI is available only through a restricted distribution program under
a REMS called the TOUCH® Prescribing Program.• Patients must be enrolled in the TOUCH Prescribing Program, read the Medication Guide, understand
the risks associated with TYSABRI and complete and sign the Patient-Prescriber Enrollment Form.
Herpes Encephalitis and Meningitis• TYSABRI�increases�the�risk�of�developing�encephalitis�and�meningitis�caused�by�herpes�simplex�and�
varicella zoster viruses.• Serious, life-threatening, and sometimes fatal cases have been reported in the postmarketing setting
in multiple sclerosis patients receiving TYSABRI.• The duration of treatment with TYSABRI prior to onset ranged from a few months to several years.• Monitor patients receiving TYSABRI for signs and symptoms of meningitis and encephalitis. If herpes
encephalitis or meningitis occurs, TYSABRI should be discontinued, and appropriate treatment for herpes encephalitis/meningitis should be administered.
Hepatotoxicity• Clinically�significant�liver�injury,�including�acute�liver�failure�requiring�transplant,�has�been�reported�in�
patients treated with TYSABRI in the postmarketing setting.• Signs�of�liver�injury,�including�markedly�elevated�serum�hepatic�enzymes�and�elevated�total�bilirubin,�occurred�as�early�as�six�days�after�the�first�dose;�signs�of�liver�injury�have�also�been�reported�for�the�first�time�after�multiple�doses.
• TYSABRI�should�be�discontinued�in�patients�with�jaundice�or�other�evidence�of�significant�liver�injury�(e.g., laboratory evidence).
Hypersensitivity/Antibody Formation• Hypersensitivity reactions have occurred in patients receiving TYSABRI, including serious systemic reactions�(e.g.,�anaphylaxis)�which�occurred�at�an�incidence�of�<1%.
• Reactions usually occur within 2 hours of the start of the infusion. Symptoms associated with these reactions�can�include�urticaria,�dizziness,�fever,�rash,�rigors,�pruritus,�nausea,�flushing,�hypotension,�dyspnea, and chest pain.
• If a hypersensitivity reaction occurs, discontinue administration of TYSABRI and initiate appropriate therapy.�Patients�who�experience�a�hypersensitivity�reaction�should�not�be�re-treated�with�TYSABRI.
• Hypersensitivity reactions were more frequent in patients with antibodies to TYSABRI compared with patients�who�did�not�develop�antibodies�to�TYSABRI�in�both�MS�and�CD�studies.
• Patients�who�receive�TYSABRI�for�a�short�exposure�(1�to�2�infusions)�followed�by�an�extended�period�without treatment are at higher risk of developing anti-natalizumab antibodies and/or hypersensitivity reactions�on�re-exposure,�compared�to�patients�who�received�regularly�scheduled�treatment.
For additional Important Safety Information about TYSABRI, please see pages 1, 2, and 4, and enclosed Full Prescribing Information, including Boxed Warning.
In the DEFINEa Trial: Robust efficacy across measures of disease activitySignificantly reduced the risk and frequency of relapses49% relative reduction in risk of relapseb (proportion of patients relapsedc) at 2 years [TECFIDERA 27% (n=410) vs placebo 46% (n=408); P<0.0001]1
53% relative reduction in annualized relapse rate (ARR)d at 2 years [TECFIDERA 0.172 (n=410) vs placebo 0.364 (n=408); P<0.0001]1
a Study Design: A 2-year, double-blind, placebo-controlled study in 1234 patients for the Determination of the Efficacy and Safety of Oral Fumarate in Relapsing-Remitting MS (DEFINE). Patients experienced at least 1 relapse over the year preceding the trial or had a brain magnetic resonance imaging (MRI) scan demonstrating at least 1 gadolinium-enhancing (Gd+) lesion within 6 weeks of randomization and had an Expanded Disability Status Scale (EDSS) score ranging from 0 to 5. MRI evaluations were performed at baseline, month 6, year 1, and year 2 in a subset of patients (44% in DEFINE).1,2
b Relapses were defined as new or recurrent neurologic symptoms not associated with fever or infection that lasted for at least 24 hours and were accompanied by new objective neurologic findings.2
c Proportion of patients relapsed is the number of patients who had a relapse over the course of a trial, independent of how many relapses those patients had.2
dARR=the total number of relapses divided by the number of patient-years in the study.2
Significantly delayed disability progressione 38% relative risk reduction in disability progression at 2 years [TECFIDERA 16% (n=410) vs placebo 27% (n=408); P=0.0050]1
Approximately 5 out of 6 (84%) TECFIDERA patients experienced no disability progression over the 2-year study period (vs 73% of placebo patients)1
In CONFIRM, the reduction in the proportion of patients with disability progression was not statistically significant. e Disability progression is defined as at least a 1-point increase from baseline EDSS of ≥1.0 (or at least a 1.5-point increase for patients with baseline EDSS of 0) sustained for 12 weeks.2
Significantly reduced all measures of MRI activity90% relative odds reduction in the number of Gd+ lesions at 2 years [TECFIDERA 0.1 (n=152) vs placebo 1.8 (n=165); P<0.0001]1
85% relative reduction in the number of new or newly enlarging T2-weighted hyperintense lesions over 2 years [TECFIDERA 2.6 (n=152) vs placebo 17 (n=165); P<0.0001]1,2
72% relative reduction in the number of new T1-weighted hypointense lesions over 2 years [TECFIDERA 1.5 (n=152) vs placebo 5.6 (n=165); P<0.0001]1,3
Percentage of patients with Gd+ lesions at 2 years [0 lesions: 93% TECFIDERA (n=152) vs 62% placebo (n=165); 1 lesion: 5% TECFIDERA vs 10% placebo; 2 lesions: <1% TECFIDERA vs 8% placebo; 3 to 4 lesions: 0% TECFIDERA vs 9% placebo; 5 or more lesions: <1% TECFIDERA vs 11% placebo]1
IndicationTecfidera® (dimethyl fumarate) is indicated for the treatment of patients with relapsing forms of multiple sclerosis.
Selected Important Safety InformationTECFIDERA is contraindicated in patients with known hypersensitivity to dimethyl fumarate or any of the excipients of TECFIDERA, as TECFIDERA can cause anaphylaxis and angioedema. Progressive multifocal leukoencephalopathy (PML) has occurred in patients with MS treated with TECFIDERA. PML has also occurred in the postmarketing setting in the presence of lymphopenia (<0.8 x109/L) persisting for more than 6 months. While the role of lymphopenia in these cases is uncertain, the majority of cases occurred in patients with lymphocyte counts <0.5x109/L. TECFIDERA may cause lymphopenia and flushing. The most common adverse reactions associated with TECFIDERA are flushing and gastrointestinal events. Elevations in hepatic transaminases and mean eosinophil counts have been reported. TECFIDERA should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
For additional Important Safety Information about TECFIDERA, please see reverse side and enclosed full Prescribing Information.
IndicationTecfidera
® (dimethyl fumarate) is indicated for the treatment of patients with relapsing forms of multiple sclerosis.
Important Safety Information (cont’d)TECFIDERA is contraindicated in patients with known hypersensitivity to dimethyl fumarate or any of the excipients of TECFIDERA. TECFIDERA can cause anaphylaxis and angioedema after the first dose or at any time during treatment. Patients experiencing signs and symptoms of anaphylaxis and angioedema (which have included difficulty breathing, urticaria, and swelling of the throat and tongue) should discontinue TECFIDERA and seek immediate medical care.Progressive multifocal leukoencephalopathy (PML) has occurred in patients with MS treated with TECFIDERA. PML is an opportunistic viral infection of the brain caused by the JC virus (JCV) that typically only occurs in patients who are immunocompromised, and that usually leads to death or severe disability. A fatal case of PML occurred in a patient who received TECFIDERA in a clinical trial. PML has also occurred in the postmarketing setting in the presence of lymphopenia (<0.8x10
9/L) persisting for more than 6 months. While the role of lymphopenia in these
cases is uncertain, the majority of cases occurred in patients with lymphocyte counts <0.5x109/L. The symptoms
associated with PML are diverse, progress over days to weeks, and include progressive weakness on one side of the body or clumsiness of limbs, disturbance of vision, and changes in thinking, memory, and orientation leading to confusion and personality changes. At the first sign or symptom suggestive of PML, withhold TECFIDERA and perform an appropriate diagnostic evaluation. MRI findings may be apparent before clinical signs or symptoms.TECFIDERA may decrease lymphocyte counts; in clinical trials there was a mean decrease of ~30% in lymphocyte counts during the first year which then remained stable. Four weeks after stopping TECFIDERA, mean lymphocyte counts increased but not to baseline. Six percent of TECFIDERA patients and <1% of placebo patients had lymphocyte counts <0.5x10
9/L. TECFIDERA has not been studied in patients with pre-existing low lymphocyte counts.
There was no increased incidence of serious infections observed in patients with lymphocyte counts <0.8x109/L or
≤0.5x109/L in controlled trials, although one patient in an extension study developed PML in the setting of prolonged
lymphopenia (lymphocyte counts predominantly <0.5x109/L for 3.5 years). In controlled and uncontrolled clinical
trials, 2% of patients experienced lymphocyte counts <0.5x109/L for at least six months. In these patients, the majority of
lymphocyte counts remained <0.5x109/L with continued therapy. A complete blood count including lymphocyte count
should be obtained before initiating treatment, 6 months after starting, every 6 to 12 months thereafter and as clinically indicated. Consider treatment interruption if lymphocyte counts <0.5x10
9/L persist for more than six months and follow
lymphocyte counts until lymphopenia is resolved. Consider withholding treatment in patients with serious infections until resolved. Decisions about whether or not to restart TECFIDERA should be based on clinical circumstances.TECFIDERA may cause flushing (e.g. warmth, redness, itching, and/or burning sensation). 40% of patients taking TECFIDERA reported flushing, which was mostly mild to moderate in severity. Three percent of patients discontinued TECFIDERA for flushing and <1% had serious flushing events that led to hospitalization. Taking TECFIDERA with food may reduce flushing. Alternatively, administration of non-enteric coated aspirin prior to dosing may reduce the incidence or severity of flushing.TECFIDERA may cause gastrointestinal (GI) events (e.g., nausea, vomiting, diarrhea, abdominal pain, and dyspepsia). Four percent of TECFIDERA patients and <1% of placebo patients discontinued due to GI events. The incidence of serious GI events was 1%. The most common adverse reactions associated with TECFIDERA versus placebo are flushing (40% vs 6%) and GI events: abdominal pain (18% vs 10%), diarrhea (14% vs 11%), nausea (12% vs 9%).Elevations in hepatic transaminases have been reported. A transient increase in mean eosinophil counts was seen during the first two months. TECFIDERA should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. Encourage patients who become pregnant while taking TECFIDERA to enroll in the TECFIDERA pregnancy registry by calling 1-866-810-1462 or visiting www.TECFIDERApregnancyregistry.com.
For additional Important Safety Information about TECFIDERA, please see reverse side and enclosed full Prescribing Information.
References: 1. TECFIDERA [Prescribing Information]. Cambridge, MA: Biogen; February 2016. 2. Gold R, Kappos L, Arnold DL, et al. N Engl J Med. 2012;367:1098-1107. Erratum in: N Engl J Med. 2012;367:2362. 3. Biogen, Data on file.
©2016Biogen. Allrightsreserved. PrintedintheU.S.A. 04/16 TEC-US-0650
CLINICAL ATTRIBUTES
ME=medical exception; PA=prior authorization; RMS=relapsing multiple sclerosis.
4 | Access Toolkit
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates5 | Access Toolkit
Tips to Successfully Completing a Biogen Product Start Form
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
6 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
Your guide to completing the Biogen product Start Form
The Biogen product Start Form is a pathway to providing a prescribed Biogen treatment to your patients with relapsing multiple sclerosis (RMS). Completing the Biogen product Start Form begins an overall process for obtaining Biogen medications and also provides your patient with an opportunity to join Above MS™, the patient support service from Biogen. If requested, Above MS can also help your office understand the benefits investigation and prior authorization (PA) process.
This guide will help you identify the key sections of information to be included on each Biogen product Start Form.
For downloadable copies of each Biogen product Start Form, please visit the product websites. Please note that infused products from Biogen follow a different procurement process. If your patient has been prescribed an infused product from Biogen, ask your Biogen representative for more information.
We have also collaborated with iAssist, an ePrescribing company, and CoverMyMeds, an electronic PA (ePA) company, to offer our Biogen product Start Forms through their portals.
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
7 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
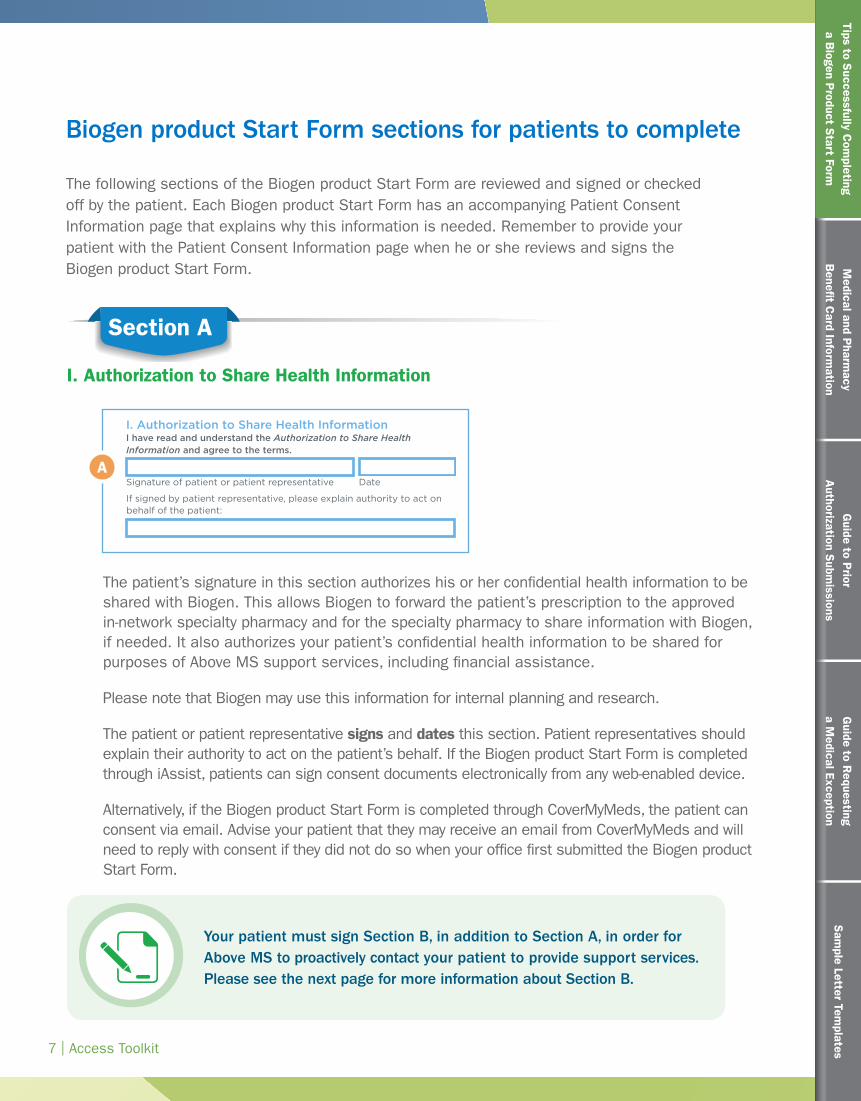
The following sections of the Biogen product Start Form are reviewed and signed or checked off by the patient. Each Biogen product Start Form has an accompanying Patient Consent Information page that explains why this information is needed. Remember to provide your patient with the Patient Consent Information page when he or she reviews and signs the Biogen product Start Form.
If signed by patient representative, please explain authority to act on behalf of the patient:
Morning Afternoon
I. Authorization to Share Health Information I have read and understand the Authorization to Share Health Information and agree to the terms.
In addition, I authorize the disclosure of my health information to the following designated individual(s) (optional):
Designated individual (print name) Relationship
III. Marketing Opt-in I have read and understand “Opt-In to Receive Marketing Communications” and hereby agree to receive information from Biogen (optional).
START FORM Phone: 1-800-456-2255 Fax: 1-855-474-3067
Signature of patient or patient representative Date
Signature of patient or patient representative Date
Current or most recent therapy
Prescriber Authorization† I authorize Biogen as my designated agent and on behalf of my patient to (1) forward the above statement of medical necessity and furnish any information on this form to the insurer of the above-named patient and (2) forward the above prescription, by fax or other mode of delivery, to the pharmacy chosen by the above-named patient. I certify that the rationale for prescribing PLEGRIDY therapy is for a primary diagnosis of ICD 9: 340/ICD 10: G35, and I will be supervising the patient’s treatment accordingly.
Statement of Medical Necessity
Prescriber Information
Fax
Tax ID#
Phone
NPI#
Address
Prior therapy
Clinical/Hospital affiliation Office contact name
Best time to contact:
Training Notification I have discussed PLEGRIDY and its use with my patient and I believe
that supplemental injection training by a PLEGRIDY nurse educator is appropriate.
Medical Benefit Information
Pharmacy Benefit Information
Prescription Information PLEGRIDY PEN PLEGRIDY Prefilled Syringe
Starter Pack (First month)*
Starter Kit Rx for PLEGRIDY: Day 1: Inject 63 mcg, Day 15: Inject 94 mcg (NO REFILLS)
Maintenance Rx for PLEGRIDY (Months 2–13)
Inject 125 mcg every 14 days (May dispense 90 days at a time)
Refills x 1 year (Dispense all supplies necessary for administration)
Primary insurance Policy #
Group # Insurance company phone
Policy holder first name Policy holder last name
Attach copies of both sides of patient’s pharmacy benefit card(s).
Check if no coverage Check if patient has secondary insurance
No prior disease-modifying therapies
Patient preferred specialty pharmacy
Primary diagnosis: ICD 9: 340/ICD 10: G35
Dates on therapy
Signature stamps not acceptable. † In New York, please attach copies of all prescriptions on Official New York State Prescription forms.
City State ZIP
Prescriber signature (Dispense as Written) Date
Prescriber signature (Substitution Permitted) Date
State license#
Patient Information
Best time to reach me:
Male Female
First name
Address
City State ZIP
Preferred number
Preferred number
OK to leave message
OK to leave message
Home phone
Cell phone
Last name
Date of birth
Pre/post treatment instructions
Office contact phone
First name Last name
* If your patient is already on PLEGRIDY and does not need to titrate, please cross out this option and note “no titration” in pre/post treatment instructions section.
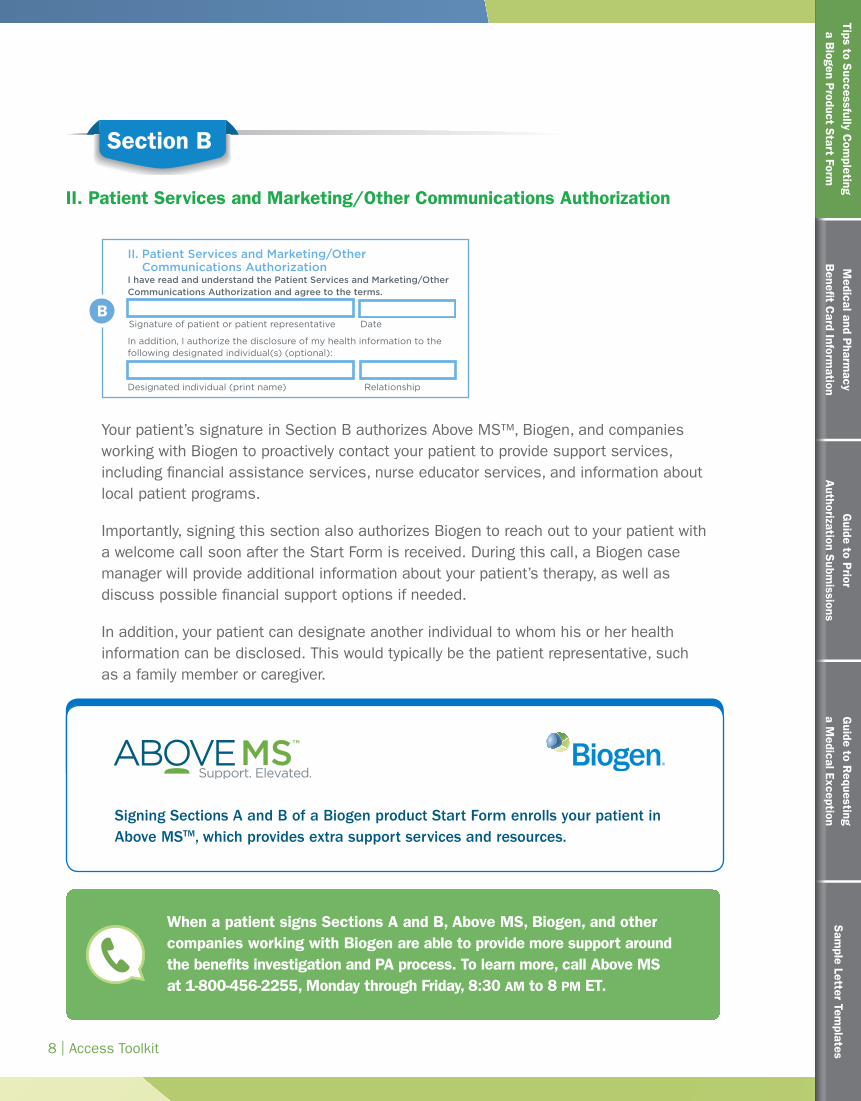
II. Patient Services and Marketing/Other Communications Authorization
I have read and understand the Patient Services and Marketing/Other Communications Authorization and agree to the terms.
PAGE 3 of 46/15 PLG-US-0160
Morning Afternoon Evening
Other therapy Dates on therapy
THE FOLLOWING INFORMATION SHOULD BE FILLED OUT BY YOUR HEALTHCARE PROVIDER
Pen: NDC 64406-011-01 Prefilled Syringe: NDC 64406-015-01
Pen: NDC 64406-012-01 Prefilled Syringe: NDC 64406-016-01
C
B
AA
Your patient must sign Section B, in addition to Section A, in order for Above MS to proactively contact your patient to provide support services. Please see the next page for more information about Section B.
Biogen product Start Form sections for patients to complete
Section A
I. Authorization to Share Health Information
The patient’s signature in this section authorizes his or her confidential health information to be shared with Biogen. This allows Biogen to forward the patient’s prescription to the approved in-network specialty pharmacy and for the specialty pharmacy to share information with Biogen, if needed. It also authorizes your patient’s confidential health information to be shared for purposes of Above MS support services, including financial assistance.
Please note that Biogen may use this information for internal planning and research.
The patient or patient representative signs and dates this section. Patient representatives should explain their authority to act on the patient’s behalf. If the Biogen product Start Form is completed through iAssist, patients can sign consent documents electronically from any web-enabled device.
Alternatively, if the Biogen product Start Form is completed through CoverMyMeds, the patient can consent via email. Advise your patient that they may receive an email from CoverMyMeds and will need to reply with consent if they did not do so when your office first submitted the Biogen product Start Form.
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
8 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
Section B
II. Patient Services and Marketing/Other Communications AuthorizationIf signed by patient representative, please explain authority to act on behalf of the patient:
Morning Afternoon
I. Authorization to Share Health Information I have read and understand the Authorization to Share Health Information and agree to the terms.
In addition, I authorize the disclosure of my health information to the following designated individual(s) (optional):
Designated individual (print name) Relationship
III. Marketing Opt-in I have read and understand “Opt-In to Receive Marketing Communications” and hereby agree to receive information from Biogen (optional).
START FORM Phone: 1-800-456-2255 Fax: 1-855-474-3067
Signature of patient or patient representative Date
Signature of patient or patient representative Date
Current or most recent therapy
Prescriber Authorization† I authorize Biogen as my designated agent and on behalf of my patient to (1) forward the above statement of medical necessity and furnish any information on this form to the insurer of the above-named patient and (2) forward the above prescription, by fax or other mode of delivery, to the pharmacy chosen by the above-named patient. I certify that the rationale for prescribing PLEGRIDY therapy is for a primary diagnosis of ICD 9: 340/ICD 10: G35, and I will be supervising the patient’s treatment accordingly.
Statement of Medical Necessity
Prescriber Information
Fax
Tax ID#
Phone
NPI#
Address
Prior therapy
Clinical/Hospital affiliation Office contact name
Best time to contact:
Training Notification I have discussed PLEGRIDY and its use with my patient and I believe
that supplemental injection training by a PLEGRIDY nurse educator is appropriate.
Medical Benefit Information
Pharmacy Benefit Information
Prescription Information PLEGRIDY PEN PLEGRIDY Prefilled Syringe
Starter Pack (First month)*
Starter Kit Rx for PLEGRIDY: Day 1: Inject 63 mcg, Day 15: Inject 94 mcg (NO REFILLS)
Maintenance Rx for PLEGRIDY (Months 2–13)
Inject 125 mcg every 14 days (May dispense 90 days at a time)
Refills x 1 year (Dispense all supplies necessary for administration)
Primary insurance Policy #
Group # Insurance company phone
Policy holder first name Policy holder last name
Attach copies of both sides of patient’s pharmacy benefit card(s).
Check if no coverage Check if patient has secondary insurance
No prior disease-modifying therapies
Patient preferred specialty pharmacy
Primary diagnosis: ICD 9: 340/ICD 10: G35
Dates on therapy
Signature stamps not acceptable. † In New York, please attach copies of all prescriptions on Official New York State Prescription forms.
City State ZIP
Prescriber signature (Dispense as Written) Date
Prescriber signature (Substitution Permitted) Date
State license#
Patient Information
Best time to reach me:
Male Female
First name
Address
City State ZIP
Preferred number
Preferred number
OK to leave message
OK to leave message
Home phone
Cell phone
Last name
Date of birth
Pre/post treatment instructions
Office contact phone
First name Last name
* If your patient is already on PLEGRIDY and does not need to titrate, please cross out this option and note “no titration” in pre/post treatment instructions section.
II. Patient Services and Marketing/Other Communications Authorization
I have read and understand the Patient Services and Marketing/Other Communications Authorization and agree to the terms.
PAGE 3 of 46/15 PLG-US-0160
Morning Afternoon Evening
Other therapy Dates on therapy
THE FOLLOWING INFORMATION SHOULD BE FILLED OUT BY YOUR HEALTHCARE PROVIDER
Pen: NDC 64406-011-01 Prefilled Syringe: NDC 64406-015-01
Pen: NDC 64406-012-01 Prefilled Syringe: NDC 64406-016-01
C
B
A
B
Signing Sections A and B of a Biogen product Start Form enrolls your patient in Above MSTM, which provides extra support services and resources.
Your patient’s signature in Section B authorizes Above MS™, Biogen, and companies working with Biogen to proactively contact your patient to provide support services, including financial assistance services, nurse educator services, and information about local patient programs.
Importantly, signing this section also authorizes Biogen to reach out to your patient with a welcome call soon after the Start Form is received. During this call, a Biogen case manager will provide additional information about your patient’s therapy, as well as discuss possible financial support options if needed.
In addition, your patient can designate another individual to whom his or her health information can be disclosed. This would typically be the patient representative, such as a family member or caregiver.
When a patient signs Sections A and B, Above MS, Biogen, and other companies working with Biogen are able to provide more support around the benefits investigation and PA process. To learn more, call Above MS at 1-800-456-2255, Monday through Friday, 8:30 AM to 8 PM ET.
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
9 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
Section C
Section C: III. Marketing Opt-in
Here is a checklist of the key sections of the Biogen product Start Form to be signed or checked off by the patient:
Section A: Signature for sharing of the patient’s confidential health information between your office, the insurance company, Above MS, Biogen, and other companies working with Biogen, such as a specialty pharmacy.
Section B: Signature for Above MS, Biogen, and companies working with Biogen to proactively reach out to the patient in order to provide specific support services, such as a welcome call or financial assistance.
Section C (optional): Check to opt-in for automated marketing calls and text messages.
C
If signed by patient representative, please explain authority to act on behalf of the patient:
Morning Afternoon
I. Authorization to Share Health Information I have read and understand the Authorization to Share Health Information and agree to the terms.
In addition, I authorize the disclosure of my health information to the following designated individual(s) (optional):
Designated individual (print name) Relationship
III. Marketing Opt-in I have read and understand “Opt-In to Receive Marketing Communications” and hereby agree to receive information from Biogen (optional).
START FORM Phone: 1-800-456-2255 Fax: 1-855-474-3067
Signature of patient or patient representative Date
Signature of patient or patient representative Date
Current or most recent therapy
Prescriber Authorization† I authorize Biogen as my designated agent and on behalf of my patient to (1) forward the above statement of medical necessity and furnish any information on this form to the insurer of the above-named patient and (2) forward the above prescription, by fax or other mode of delivery, to the pharmacy chosen by the above-named patient. I certify that the rationale for prescribing PLEGRIDY therapy is for a primary diagnosis of ICD 9: 340/ICD 10: G35, and I will be supervising the patient’s treatment accordingly.
Statement of Medical Necessity
Prescriber Information
Fax
Tax ID#
Phone
NPI#
Address
Prior therapy
Clinical/Hospital affiliation Office contact name
Best time to contact:
Training Notification I have discussed PLEGRIDY and its use with my patient and I believe
that supplemental injection training by a PLEGRIDY nurse educator is appropriate.
Medical Benefit Information
Pharmacy Benefit Information
Prescription Information PLEGRIDY PEN PLEGRIDY Prefilled Syringe
Starter Pack (First month)*
Starter Kit Rx for PLEGRIDY: Day 1: Inject 63 mcg, Day 15: Inject 94 mcg (NO REFILLS)
Maintenance Rx for PLEGRIDY (Months 2–13)
Inject 125 mcg every 14 days (May dispense 90 days at a time)
Refills x 1 year (Dispense all supplies necessary for administration)
Primary insurance Policy #
Group # Insurance company phone
Policy holder first name Policy holder last name
Attach copies of both sides of patient’s pharmacy benefit card(s).
Check if no coverage Check if patient has secondary insurance
No prior disease-modifying therapies
Patient preferred specialty pharmacy
Primary diagnosis: ICD 9: 340/ICD 10: G35
Dates on therapy
Signature stamps not acceptable. † In New York, please attach copies of all prescriptions on Official New York State Prescription forms.
City State ZIP
Prescriber signature (Dispense as Written) Date
Prescriber signature (Substitution Permitted) Date
State license#
Patient Information
Best time to reach me:
Male Female
First name
Address
City State ZIP
Preferred number
Preferred number
OK to leave message
OK to leave message
Home phone
Cell phone
Last name
Date of birth
Pre/post treatment instructions
Office contact phone
First name Last name
* If your patient is already on PLEGRIDY and does not need to titrate, please cross out this option and note “no titration” in pre/post treatment instructions section.
II. Patient Services and Marketing/Other Communications Authorization
I have read and understand the Patient Services and Marketing/Other Communications Authorization and agree to the terms.
PAGE 3 of 46/15 PLG-US-0160
Morning Afternoon Evening
Other therapy Dates on therapy
THE FOLLOWING INFORMATION SHOULD BE FILLED OUT BY YOUR HEALTHCARE PROVIDER
Pen: NDC 64406-011-01 Prefilled Syringe: NDC 64406-015-01
Pen: NDC 64406-012-01 Prefilled Syringe: NDC 64406-016-01
C
B
A
Patients should check the optional box in Section C if they consent to receive autodialed and prerecorded marketing calls and text messages from Above MS, Biogen, and companies working with Biogen.
Quick Tip
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
10 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
This section includes basic information that will familiarize Biogen with your patient. It includes gender, date of birth, name, address, email address, and telephone numbers, as well as preference for the best time to reach the patient.
The patient completes this section. Your office should review what your patient completed with him or her to ensure accuracy.
Patient Information
If signed by patient representative, please explain authority to act on behalf of the patient:
Morning Afternoon
I. Authorization to Share Health Information I have read and understand the Authorization to Share Health Information and agree to the terms.
In addition, I authorize the disclosure of my health information to the following designated individual(s) (optional):
Designated individual (print name) Relationship
III. Marketing Opt-in I have read and understand “Opt-In to Receive Marketing Communications” and hereby agree to receive information from Biogen (optional).
START FORM Phone: 1-800-456-2255 Fax: 1-855-474-3067
Signature of patient or patient representative Date
Signature of patient or patient representative Date
Current or most recent therapy
Prescriber Authorization† I authorize Biogen as my designated agent and on behalf of my patient to (1) forward the above statement of medical necessity and furnish any information on this form to the insurer of the above-named patient and (2) forward the above prescription, by fax or other mode of delivery, to the pharmacy chosen by the above-named patient. I certify that the rationale for prescribing PLEGRIDY therapy is for a primary diagnosis of ICD 9: 340/ICD 10: G35, and I will be supervising the patient’s treatment accordingly.
Statement of Medical Necessity
Prescriber Information
Fax
Tax ID#
Phone
NPI#
Address
Prior therapy
Clinical/Hospital affiliation Office contact name
Best time to contact:
Training Notification I have discussed PLEGRIDY and its use with my patient and I believe
that supplemental injection training by a PLEGRIDY nurse educator is appropriate.
Medical Benefit Information
Pharmacy Benefit Information
Prescription Information PLEGRIDY PEN PLEGRIDY Prefilled Syringe
Starter Pack (First month)*
Starter Kit Rx for PLEGRIDY: Day 1: Inject 63 mcg, Day 15: Inject 94 mcg (NO REFILLS)
Maintenance Rx for PLEGRIDY (Months 2–13)
Inject 125 mcg every 14 days (May dispense 90 days at a time)
Refills x 1 year (Dispense all supplies necessary for administration)
Primary insurance Policy #
Group # Insurance company phone
Policy holder first name Policy holder last name
Attach copies of both sides of patient’s pharmacy benefit card(s).
Check if no coverage Check if patient has secondary insurance
No prior disease-modifying therapies
Patient preferred specialty pharmacy
Primary diagnosis: ICD 9: 340/ICD 10: G35
Dates on therapy
Signature stamps not acceptable. † In New York, please attach copies of all prescriptions on Official New York State Prescription forms.
City State ZIP
Prescriber signature (Dispense as Written) Date
Prescriber signature (Substitution Permitted) Date
State license#
Patient Information
Best time to reach me:
Male Female
First name
Address
City State ZIP
Preferred number
Preferred number
OK to leave message
OK to leave message
Home phone
Cell phone
Last name
Date of birth
Pre/post treatment instructions
Office contact phone
First name Last name
* If your patient is already on PLEGRIDY and does not need to titrate, please cross out this option and note “no titration” in pre/post treatment instructions section.
II. Patient Services and Marketing/Other Communications Authorization
I have read and understand the Patient Services and Marketing/Other Communications Authorization and agree to the terms.
PAGE 3 of 46/15 PLG-US-0160
Morning Afternoon Evening
Other therapy Dates on therapy
THE FOLLOWING INFORMATION SHOULD BE FILLED OUT BY YOUR HEALTHCARE PROVIDER
Pen: NDC 64406-011-01 Prefilled Syringe: NDC 64406-015-01
Pen: NDC 64406-012-01 Prefilled Syringe: NDC 64406-016-01
C
B
A
Patient preferred specialty pharmacy
Before a patient leaves the office, check the medical insurance card to determine if you also need to obtain the pharmacy benefit information from a different card.
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
11 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
Biogen product Start Form sections for offices to complete
Prescription Information
The prescription information will vary on each Biogen product Start Form because it is dependent on the type of Biogen product being requested. Make sure to use the correct Biogen product Start Form for your patient’s treatment and check the box for the appropriate dose. You can also use this section to add special instructions for the dispensing pharmacy.
The following sections of the Biogen product Start Form should be completed by your office.
Medical and Pharmacy Benefit Information
It is essential that Biogen has accurate information for the patient’s pharmacy benefit and medical benefit insurance. This information is needed to conduct a benefits investigation, coordinate with the appropriate in-network specialty pharmacy, and provide financial assistance services to your patient, if requested.
The medical benefit generally covers medications that are administered by a healthcare professional in the physician’s office, infusion center, or hospital outpatient center, while the pharmacy benefit generally covers medicines that are self-administered orally, by injection, or inhaled.
For more detail about medical and pharmacy benefit cards for commercial, Medicare, and Medicaid, please see page 16.
Remember that some patients may have 2 insurance cards, a medical card and a pharmacy card.
A Biogen product Start Form may ask for medical and pharmacy benefit information. It is important to complete the Start Form with information for both benefits to minimize callbacks to your office.
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
12 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
Be sure to complete these sections of the Biogen product Start Form with all of the required insurance information for the patient’s medical benefit. The level of information needed may vary.
If signed by patient representative, please explain authority to act on behalf of the patient:
Morning Afternoon
I. Authorization to Share Health Information I have read and understand the Authorization to Share Health Information and agree to the terms.
In addition, I authorize the disclosure of my health information to the following designated individual(s) (optional):
Designated individual (print name) Relationship
III. Marketing Opt-in I have read and understand “Opt-In to Receive Marketing Communications” and hereby agree to receive information from Biogen (optional).
START FORM Phone: 1-800-456-2255 Fax: 1-855-474-3067
Signature of patient or patient representative Date
Signature of patient or patient representative Date
Current or most recent therapy
Prescriber Authorization† I authorize Biogen as my designated agent and on behalf of my patient to (1) forward the above statement of medical necessity and furnish any information on this form to the insurer of the above-named patient and (2) forward the above prescription, by fax or other mode of delivery, to the pharmacy chosen by the above-named patient. I certify that the rationale for prescribing PLEGRIDY therapy is for a primary diagnosis of ICD 9: 340/ICD 10: G35, and I will be supervising the patient’s treatment accordingly.
Statement of Medical Necessity
Prescriber Information
Fax
Tax ID#
Phone
NPI#
Address
Prior therapy
Clinical/Hospital affiliation Office contact name
Best time to contact:
Training Notification I have discussed PLEGRIDY and its use with my patient and I believe
that supplemental injection training by a PLEGRIDY nurse educator is appropriate.
Medical Benefit Information
Pharmacy Benefit Information
Prescription Information PLEGRIDY PEN PLEGRIDY Prefilled Syringe
Starter Pack (First month)*
Starter Kit Rx for PLEGRIDY: Day 1: Inject 63 mcg, Day 15: Inject 94 mcg (NO REFILLS)
Maintenance Rx for PLEGRIDY (Months 2–13)
Inject 125 mcg every 14 days (May dispense 90 days at a time)
Refills x 1 year (Dispense all supplies necessary for administration)
Primary insurance Policy #
Group # Insurance company phone
Policy holder first name Policy holder last name
Attach copies of both sides of patient’s pharmacy benefit card(s).
Check if no coverage Check if patient has secondary insurance
No prior disease-modifying therapies
Patient preferred specialty pharmacy
Primary diagnosis: ICD 9: 340/ICD 10: G35
Dates on therapy
Signature stamps not acceptable. † In New York, please attach copies of all prescriptions on Official New York State Prescription forms.
City State ZIP
Prescriber signature (Dispense as Written) Date
Prescriber signature (Substitution Permitted) Date
State license#
Patient Information
Best time to reach me:
Male Female
First name
Address
City State ZIP
Preferred number
Preferred number
OK to leave message
OK to leave message
Home phone
Cell phone
Last name
Date of birth
Pre/post treatment instructions
Office contact phone
First name Last name
* If your patient is already on PLEGRIDY and does not need to titrate, please cross out this option and note “no titration” in pre/post treatment instructions section.
II. Patient Services and Marketing/Other Communications Authorization
I have read and understand the Patient Services and Marketing/Other Communications Authorization and agree to the terms.
PAGE 3 of 46/15 PLG-US-0160
Morning Afternoon Evening
Other therapy Dates on therapy
THE FOLLOWING INFORMATION SHOULD BE FILLED OUT BY YOUR HEALTHCARE PROVIDER
Pen: NDC 64406-011-01 Prefilled Syringe: NDC 64406-015-01
Pen: NDC 64406-012-01 Prefilled Syringe: NDC 64406-016-01
C
B
A
Ensuring that all of the patient’s insurance information (pharmacy benefit and medical benefit) is accurately completed is a very important part of a Biogen product Start Form.
If signed by patient representative, please explain authority to act on behalf of the patient:
Morning Afternoon
I. Authorization to Share Health Information I have read and understand the Authorization to Share Health Information and agree to the terms.
In addition, I authorize the disclosure of my health information to the following designated individual(s) (optional):
Designated individual (print name) Relationship
III. Marketing Opt-in I have read and understand “Opt-In to Receive Marketing Communications” and hereby agree to receive information from Biogen (optional).
START FORM Phone: 1-800-456-2255 Fax: 1-855-474-3067
Signature of patient or patient representative Date
Signature of patient or patient representative Date
Current or most recent therapy
Prescriber Authorization† I authorize Biogen as my designated agent and on behalf of my patient to (1) forward the above statement of medical necessity and furnish any information on this form to the insurer of the above-named patient and (2) forward the above prescription, by fax or other mode of delivery, to the pharmacy chosen by the above-named patient. I certify that the rationale for prescribing PLEGRIDY therapy is for a primary diagnosis of ICD 9: 340/ICD 10: G35, and I will be supervising the patient’s treatment accordingly.
Statement of Medical Necessity
Prescriber Information
Fax
Tax ID#
Phone
NPI#
Address
Prior therapy
Clinical/Hospital affiliation Office contact name
Best time to contact:
Training Notification I have discussed PLEGRIDY and its use with my patient and I believe
that supplemental injection training by a PLEGRIDY nurse educator is appropriate.
Medical Benefit Information
Pharmacy Benefit Information
Prescription Information PLEGRIDY PEN PLEGRIDY Prefilled Syringe
Starter Pack (First month)*
Starter Kit Rx for PLEGRIDY: Day 1: Inject 63 mcg, Day 15: Inject 94 mcg (NO REFILLS)
Maintenance Rx for PLEGRIDY (Months 2–13)
Inject 125 mcg every 14 days (May dispense 90 days at a time)
Refills x 1 year (Dispense all supplies necessary for administration)
Primary insurance Policy #
Group # Insurance company phone
Policy holder first name Policy holder last name
Attach copies of both sides of patient’s pharmacy benefit card(s).
Check if no coverage Check if patient has secondary insurance
No prior disease-modifying therapies
Patient preferred specialty pharmacy
Primary diagnosis: ICD 9: 340/ICD 10: G35
Dates on therapy
Signature stamps not acceptable. † In New York, please attach copies of all prescriptions on Official New York State Prescription forms.
City State ZIP
Prescriber signature (Dispense as Written) Date
Prescriber signature (Substitution Permitted) Date
State license#
Patient Information
Best time to reach me:
Male Female
First name
Address
City State ZIP
Preferred number
Preferred number
OK to leave message
OK to leave message
Home phone
Cell phone
Last name
Date of birth
Pre/post treatment instructions
Office contact phone
First name Last name
* If your patient is already on PLEGRIDY and does not need to titrate, please cross out this option and note “no titration” in pre/post treatment instructions section.
II. Patient Services and Marketing/Other Communications Authorization
I have read and understand the Patient Services and Marketing/Other Communications Authorization and agree to the terms.
PAGE 3 of 46/15 PLG-US-0160
Morning Afternoon Evening
Other therapy Dates on therapy
THE FOLLOWING INFORMATION SHOULD BE FILLED OUT BY YOUR HEALTHCARE PROVIDER
Pen: NDC 64406-011-01 Prefilled Syringe: NDC 64406-015-01
Pen: NDC 64406-012-01 Prefilled Syringe: NDC 64406-016-01
C
B
A
Attaching photocopies or scans of both sides of the patient’s medical and pharmacy insurance cards is a good practice when you submit the Start Form.
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
13 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
Ensure that all the prescriber information is completed in its entirety. This provides Biogen with complete contact details so we may reach out to your office with questions, updates, and other information.
Prescriber Information
If signed by patient representative, please explain authority to act on behalf of the patient:
Morning Afternoon
I. Authorization to Share Health Information I have read and understand the Authorization to Share Health Information and agree to the terms.
In addition, I authorize the disclosure of my health information to the following designated individual(s) (optional):
Designated individual (print name) Relationship
III. Marketing Opt-in I have read and understand “Opt-In to Receive Marketing Communications” and hereby agree to receive information from Biogen (optional).
START FORM Phone: 1-800-456-2255 Fax: 1-855-474-3067
Signature of patient or patient representative Date
Signature of patient or patient representative Date
Current or most recent therapy
Prescriber Authorization† I authorize Biogen as my designated agent and on behalf of my patient to (1) forward the above statement of medical necessity and furnish any information on this form to the insurer of the above-named patient and (2) forward the above prescription, by fax or other mode of delivery, to the pharmacy chosen by the above-named patient. I certify that the rationale for prescribing PLEGRIDY therapy is for a primary diagnosis of ICD 9: 340/ICD 10: G35, and I will be supervising the patient’s treatment accordingly.
Statement of Medical Necessity
Prescriber Information
Fax
Tax ID#
Phone
NPI#
Address
Prior therapy
Clinical/Hospital affiliation Office contact name
Best time to contact:
Training Notification I have discussed PLEGRIDY and its use with my patient and I believe
that supplemental injection training by a PLEGRIDY nurse educator is appropriate.
Medical Benefit Information
Pharmacy Benefit Information
Prescription Information PLEGRIDY PEN PLEGRIDY Prefilled Syringe
Starter Pack (First month)*
Starter Kit Rx for PLEGRIDY: Day 1: Inject 63 mcg, Day 15: Inject 94 mcg (NO REFILLS)
Maintenance Rx for PLEGRIDY (Months 2–13)
Inject 125 mcg every 14 days (May dispense 90 days at a time)
Refills x 1 year (Dispense all supplies necessary for administration)
Primary insurance Policy #
Group # Insurance company phone
Policy holder first name Policy holder last name
Attach copies of both sides of patient’s pharmacy benefit card(s).
Check if no coverage Check if patient has secondary insurance
No prior disease-modifying therapies
Patient preferred specialty pharmacy
Primary diagnosis: ICD 9: 340/ICD 10: G35
Dates on therapy
Signature stamps not acceptable. † In New York, please attach copies of all prescriptions on Official New York State Prescription forms.
City State ZIP
Prescriber signature (Dispense as Written) Date
Prescriber signature (Substitution Permitted) Date
State license#
Patient Information
Best time to reach me:
Male Female
First name
Address
City State ZIP
Preferred number
Preferred number
OK to leave message
OK to leave message
Home phone
Cell phone
Last name
Date of birth
Pre/post treatment instructions
Office contact phone
First name Last name
* If your patient is already on PLEGRIDY and does not need to titrate, please cross out this option and note “no titration” in pre/post treatment instructions section.
II. Patient Services and Marketing/Other Communications Authorization
I have read and understand the Patient Services and Marketing/Other Communications Authorization and agree to the terms.
PAGE 3 of 46/15 PLG-US-0160
Morning Afternoon Evening
Other therapy Dates on therapy
THE FOLLOWING INFORMATION SHOULD BE FILLED OUT BY YOUR HEALTHCARE PROVIDER
Pen: NDC 64406-011-01 Prefilled Syringe: NDC 64406-015-01
Pen: NDC 64406-012-01 Prefilled Syringe: NDC 64406-016-01
C
B
A
Enter the International Classification of Diseases, Tenth Revision (ICD-10) code for the primary diagnosis of multiple sclerosis and ensure that the code is in alignment with the indication for the Biogen product. Include prior therapies and dates.
Statement of Medical Necessity
If signed by patient representative, please explain authority to act on behalf of the patient:
Morning Afternoon
I. Authorization to Share Health Information I have read and understand the Authorization to Share Health Information and agree to the terms.
In addition, I authorize the disclosure of my health information to the following designated individual(s) (optional):
Designated individual (print name) Relationship
III. Marketing Opt-in I have read and understand “Opt-In to Receive Marketing Communications” and hereby agree to receive information from Biogen (optional).
START FORM Phone: 1-800-456-2255 Fax: 1-855-474-3067
Signature of patient or patient representative Date
Signature of patient or patient representative Date
Current or most recent therapy
Prescriber Authorization† I authorize Biogen as my designated agent and on behalf of my patient to (1) forward the above statement of medical necessity and furnish any information on this form to the insurer of the above-named patient and (2) forward the above prescription, by fax or other mode of delivery, to the pharmacy chosen by the above-named patient. I certify that the rationale for prescribing PLEGRIDY therapy is for a primary diagnosis of ICD 9: 340/ICD 10: G35, and I will be supervising the patient’s treatment accordingly.
Statement of Medical Necessity
Prescriber Information
Fax
Tax ID#
Phone
NPI#
Address
Prior therapy
Clinical/Hospital affiliation Office contact name
Best time to contact:
Training Notification I have discussed PLEGRIDY and its use with my patient and I believe
that supplemental injection training by a PLEGRIDY nurse educator is appropriate.
Medical Benefit Information
Pharmacy Benefit Information
Prescription Information PLEGRIDY PEN PLEGRIDY Prefilled Syringe
Starter Pack (First month)*
Starter Kit Rx for PLEGRIDY: Day 1: Inject 63 mcg, Day 15: Inject 94 mcg (NO REFILLS)
Maintenance Rx for PLEGRIDY (Months 2–13)
Inject 125 mcg every 14 days (May dispense 90 days at a time)
Refills x 1 year (Dispense all supplies necessary for administration)
Primary insurance Policy #
Group # Insurance company phone
Policy holder first name Policy holder last name
Attach copies of both sides of patient’s pharmacy benefit card(s).
Check if no coverage Check if patient has secondary insurance
No prior disease-modifying therapies
Patient preferred specialty pharmacy
Primary diagnosis: ICD 9: 340/ICD 10: G35
Dates on therapy
Signature stamps not acceptable. † In New York, please attach copies of all prescriptions on Official New York State Prescription forms.
City State ZIP
Prescriber signature (Dispense as Written) Date
Prescriber signature (Substitution Permitted) Date
State license#
Patient Information
Best time to reach me:
Male Female
First name
Address
City State ZIP
Preferred number
Preferred number
OK to leave message
OK to leave message
Home phone
Cell phone
Last name
Date of birth
Pre/post treatment instructions
Office contact phone
First name Last name
* If your patient is already on PLEGRIDY and does not need to titrate, please cross out this option and note “no titration” in pre/post treatment instructions section.
II. Patient Services and Marketing/Other Communications Authorization
I have read and understand the Patient Services and Marketing/Other Communications Authorization and agree to the terms.
PAGE 3 of 46/15 PLG-US-0160
Morning Afternoon Evening
Other therapy Dates on therapy
THE FOLLOWING INFORMATION SHOULD BE FILLED OUT BY YOUR HEALTHCARE PROVIDER
Pen: NDC 64406-011-01 Prefilled Syringe: NDC 64406-015-01
Pen: NDC 64406-012-01 Prefilled Syringe: NDC 64406-016-01
C
B
A
If signed by patient representative, please explain authority to act on behalf of the patient:
Morning Afternoon
I. Authorization to Share Health Information I have read and understand the Authorization to Share Health Information and agree to the terms.
In addition, I authorize the disclosure of my health information to the following designated individual(s) (optional):
Designated individual (print name) Relationship
III. Marketing Opt-in I have read and understand “Opt-In to Receive Marketing Communications” and hereby agree to receive information from Biogen (optional).
START FORM Phone: 1-800-456-2255 Fax: 1-855-474-3067
Signature of patient or patient representative Date
Signature of patient or patient representative Date
Current or most recent therapy
Prescriber Authorization† I authorize Biogen as my designated agent and on behalf of my patient to (1) forward the above statement of medical necessity and furnish any information on this form to the insurer of the above-named patient and (2) forward the above prescription, by fax or other mode of delivery, to the pharmacy chosen by the above-named patient. I certify that the rationale for prescribing PLEGRIDY therapy is for a primary diagnosis of ICD 9: 340/ICD 10: G35, and I will be supervising the patient’s treatment accordingly.
Statement of Medical Necessity
Prescriber Information
Fax
Tax ID#
Phone
NPI#
Address
Prior therapy
Clinical/Hospital affiliation Office contact name
Best time to contact:
Training Notification I have discussed PLEGRIDY and its use with my patient and I believe
that supplemental injection training by a PLEGRIDY nurse educator is appropriate.
Medical Benefit Information
Pharmacy Benefit Information
Prescription Information PLEGRIDY PEN PLEGRIDY Prefilled Syringe
Starter Pack (First month)*
Starter Kit Rx for PLEGRIDY: Day 1: Inject 63 mcg, Day 15: Inject 94 mcg (NO REFILLS)
Maintenance Rx for PLEGRIDY (Months 2–13)
Inject 125 mcg every 14 days (May dispense 90 days at a time)
Refills x 1 year (Dispense all supplies necessary for administration)
Primary insurance Policy #
Group # Insurance company phone
Policy holder first name Policy holder last name
Attach copies of both sides of patient’s pharmacy benefit card(s).
Check if no coverage Check if patient has secondary insurance
No prior disease-modifying therapies
Patient preferred specialty pharmacy
Primary diagnosis: ICD 9: 340/ICD 10: G35
Dates on therapy
Signature stamps not acceptable. † In New York, please attach copies of all prescriptions on Official New York State Prescription forms.
City State ZIP
Prescriber signature (Dispense as Written) Date
Prescriber signature (Substitution Permitted) Date
State license#
Patient Information
Best time to reach me:
Male Female
First name
Address
City State ZIP
Preferred number
Preferred number
OK to leave message
OK to leave message
Home phone
Cell phone
Last name
Date of birth
Pre/post treatment instructions
Office contact phone
First name Last name
* If your patient is already on PLEGRIDY and does not need to titrate, please cross out this option and note “no titration” in pre/post treatment instructions section.
II. Patient Services and Marketing/Other Communications Authorization
I have read and understand the Patient Services and Marketing/Other Communications Authorization and agree to the terms.
PAGE 3 of 46/15 PLG-US-0160
Morning Afternoon Evening
Other therapy Dates on therapy
THE FOLLOWING INFORMATION SHOULD BE FILLED OUT BY YOUR HEALTHCARE PROVIDER
Pen: NDC 64406-011-01 Prefilled Syringe: NDC 64406-015-01
Pen: NDC 64406-012-01 Prefilled Syringe: NDC 64406-016-01
C
B
A
If signed by patient representative, please explain authority to act on behalf of the patient:
Morning Afternoon
I. Authorization to Share Health Information I have read and understand the Authorization to Share Health Information and agree to the terms.
In addition, I authorize the disclosure of my health information to the following designated individual(s) (optional):
Designated individual (print name) Relationship
III. Marketing Opt-in I have read and understand “Opt-In to Receive Marketing Communications” and hereby agree to receive information from Biogen (optional).
START FORM Phone: 1-800-456-2255 Fax: 1-855-474-3067
Signature of patient or patient representative Date
Signature of patient or patient representative Date
Current or most recent therapy
Prescriber Authorization† I authorize Biogen as my designated agent and on behalf of my patient to (1) forward the above statement of medical necessity and furnish any information on this form to the insurer of the above-named patient and (2) forward the above prescription, by fax or other mode of delivery, to the pharmacy chosen by the above-named patient. I certify that the rationale for prescribing PLEGRIDY therapy is for a primary diagnosis of ICD 9: 340/ICD 10: G35, and I will be supervising the patient’s treatment accordingly.
Statement of Medical Necessity
Prescriber Information
Fax
Tax ID#
Phone
NPI#
Address
Prior therapy
Clinical/Hospital affiliation Office contact name
Best time to contact:
Training Notification I have discussed PLEGRIDY and its use with my patient and I believe
that supplemental injection training by a PLEGRIDY nurse educator is appropriate.
Medical Benefit Information
Pharmacy Benefit Information
Prescription Information PLEGRIDY PEN PLEGRIDY Prefilled Syringe
Starter Pack (First month)*
Starter Kit Rx for PLEGRIDY: Day 1: Inject 63 mcg, Day 15: Inject 94 mcg (NO REFILLS)
Maintenance Rx for PLEGRIDY (Months 2–13)
Inject 125 mcg every 14 days (May dispense 90 days at a time)
Refills x 1 year (Dispense all supplies necessary for administration)
Primary insurance Policy #
Group # Insurance company phone
Policy holder first name Policy holder last name
Attach copies of both sides of patient’s pharmacy benefit card(s).
Check if no coverage Check if patient has secondary insurance
No prior disease-modifying therapies
Patient preferred specialty pharmacy
Primary diagnosis: ICD 9: 340/ICD 10: G35
Dates on therapy
Signature stamps not acceptable. † In New York, please attach copies of all prescriptions on Official New York State Prescription forms.
City State ZIP
Prescriber signature (Dispense as Written) Date
Prescriber signature (Substitution Permitted) Date
State license#
Patient Information
Best time to reach me:
Male Female
First name
Address
City State ZIP
Preferred number
Preferred number
OK to leave message
OK to leave message
Home phone
Cell phone
Last name
Date of birth
Pre/post treatment instructions
Office contact phone
First name Last name
* If your patient is already on PLEGRIDY and does not need to titrate, please cross out this option and note “no titration” in pre/post treatment instructions section.
II. Patient Services and Marketing/Other Communications Authorization
I have read and understand the Patient Services and Marketing/Other Communications Authorization and agree to the terms.
PAGE 3 of 46/15 PLG-US-0160
Morning Afternoon Evening
Other therapy Dates on therapy
THE FOLLOWING INFORMATION SHOULD BE FILLED OUT BY YOUR HEALTHCARE PROVIDER
Pen: NDC 64406-011-01 Prefilled Syringe: NDC 64406-015-01
Pen: NDC 64406-012-01 Prefilled Syringe: NDC 64406-016-01
C
B
A
If signed by patient representative, please explain authority to act on behalf of the patient:
Morning Afternoon
I. Authorization to Share Health Information I have read and understand the Authorization to Share Health Information and agree to the terms.
In addition, I authorize the disclosure of my health information to the following designated individual(s) (optional):
Designated individual (print name) Relationship
III. Marketing Opt-in I have read and understand “Opt-In to Receive Marketing Communications” and hereby agree to receive information from Biogen (optional).
START FORM Phone: 1-800-456-2255 Fax: 1-855-474-3067
Signature of patient or patient representative Date
Signature of patient or patient representative Date
Current or most recent therapy
Prescriber Authorization† I authorize Biogen as my designated agent and on behalf of my patient to (1) forward the above statement of medical necessity and furnish any information on this form to the insurer of the above-named patient and (2) forward the above prescription, by fax or other mode of delivery, to the pharmacy chosen by the above-named patient. I certify that the rationale for prescribing PLEGRIDY therapy is for a primary diagnosis of ICD 9: 340/ICD 10: G35, and I will be supervising the patient’s treatment accordingly.
Statement of Medical Necessity
Prescriber Information
Fax
Tax ID#
Phone
NPI#
Address
Prior therapy
Clinical/Hospital affiliation Office contact name
Best time to contact:
Training Notification I have discussed PLEGRIDY and its use with my patient and I believe
that supplemental injection training by a PLEGRIDY nurse educator is appropriate.
Medical Benefit Information
Pharmacy Benefit Information
Prescription Information PLEGRIDY PEN PLEGRIDY Prefilled Syringe
Starter Pack (First month)*
Starter Kit Rx for PLEGRIDY: Day 1: Inject 63 mcg, Day 15: Inject 94 mcg (NO REFILLS)
Maintenance Rx for PLEGRIDY (Months 2–13)
Inject 125 mcg every 14 days (May dispense 90 days at a time)
Refills x 1 year (Dispense all supplies necessary for administration)
Primary insurance Policy #
Group # Insurance company phone
Policy holder first name Policy holder last name
Attach copies of both sides of patient’s pharmacy benefit card(s).
Check if no coverage Check if patient has secondary insurance
No prior disease-modifying therapies
Patient preferred specialty pharmacy
Primary diagnosis: ICD 9: 340/ICD 10: G35
Dates on therapy
Signature stamps not acceptable. † In New York, please attach copies of all prescriptions on Official New York State Prescription forms.
City State ZIP
Prescriber signature (Dispense as Written) Date
Prescriber signature (Substitution Permitted) Date
State license#
Patient Information
Best time to reach me:
Male Female
First name
Address
City State ZIP
Preferred number
Preferred number
OK to leave message
OK to leave message
Home phone
Cell phone
Last name
Date of birth
Pre/post treatment instructions
Office contact phone
First name Last name
* If your patient is already on PLEGRIDY and does not need to titrate, please cross out this option and note “no titration” in pre/post treatment instructions section.
II. Patient Services and Marketing/Other Communications Authorization
I have read and understand the Patient Services and Marketing/Other Communications Authorization and agree to the terms.
PAGE 3 of 46/15 PLG-US-0160
Morning Afternoon Evening
Other therapy Dates on therapy
THE FOLLOWING INFORMATION SHOULD BE FILLED OUT BY YOUR HEALTHCARE PROVIDER
Pen: NDC 64406-011-01 Prefilled Syringe: NDC 64406-015-01
Pen: NDC 64406-012-01 Prefilled Syringe: NDC 64406-016-01
C
B
A
Dates/Duration
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
14 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
Prescriber Authorization
Ensure that all Biogen product Start Form sections are completed
The physician must sign and date both lines of the form so that the process can move forward. Not having a signature can delay the initiation process.
The physician must sign both lines within the Prescriber Authorization section. The Biogen product Start Form will be returned if the prescriber signature is not included on both lines and patient treatment may be delayed.
Prescriber Authorization† I authorize Biogen as my designated agent and on behalf of my patient to (1) forward the above statement of medical necessity and furnish any information on this form to the insurer of the above-named patient and (2) forward the above prescription, by fax or other mode of delivery, to the pharmacy chosen by the above-named patient. I certify that the rationale for prescribing PRODUCT therapy is for a primary diagnosis of ICD 10: G35, and I will be supervising the patient’s treatment accordingly.
Signature stamps not acceptable. † Prescription forms.
Prescriber signature (Dispense as Written) Date
Prescriber signature (Substitution Permitted) Date
Here is a checklist of the key sections of the Biogen product Start Form to be completed by your office:
Patient information that is verified by your patient.
Prescription information, including appropriate dose.
Medical benefit and pharmacy benefit information. All insurance information (ie, pharmacy/prescription benefit and medical benefit) should be completed as requested.
Statement of medical necessity.
Prescriber information.
Prescriber authorization with physician signature on both lines.
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
15 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
Biogen is here to help
If you have questions about how to fill out any of the Biogen product Start Form, call Above MS™ at 1-800-456-2255, Monday through Friday, 8:30 AM to 8 PM ET.
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates16 | Access Toolkit
Medical and Pharmacy Benefit Card Information
Medical and P
harmacy
Benefit C
ard Information
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
17 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Medical and P
harmacy
Benefit C
ard Information
Understanding medical benefit and pharmacy benefit insurance cards
If you are prescribing a Biogen product, you may be required to fill out a Biogen product Start Form. Correctly completing the patient insurance information on the form can help ensure the request is processed by the specialty pharmacy and the insurance company in a timely manner so that patients can receive treatment quickly.
It may also reduce or limit any callbacks to your office because of incomplete information. It’s important to know that prior authorizations (PAs) may be denied due to incomplete or insufficient prescription information, not because the patient does not have coverage for the drug.
A specialty drug may be covered by a medical or a pharmacy benefit, depending on the type of medication and how it’s administered
Medical benefits generally cover drugs that are injected or infused by a healthcare professional in the doctor’s office, infusion center, or hospital outpatient center
Pharmacy benefits generally cover drugs that are self administered, such as oral, injected, or inhaled
Knowing which insurance card to use on a Biogen product Start Form may help patients receive treatment quickly.
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
18 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Medical and P
harmacy
Benefit C
ard Information
1 card vs 2 cards
Pharmacy vs medical benefits can be determined based on the insurance cards.
1 card for both medical and pharmacy benefits. Health plans may combine the medical and pharmacy benefit into 1 program. The patient will have 1 insurance card that includes member identification information (eg, group number and member ID) for both the medical and pharmacy benefit. Insurance cards for both benefits typically note the pharmacy benefit with terms such as “prescription” or “Rx”
2 cards—1 card for the medical benefit and 1 card for the pharmacy benefit. Health plans may use a third-party provider for the pharmacy benefit, such as a pharmacy benefit manager (PBM). In this instance, the patient will have 1 card for the medical benefit that does not include pharmacy benefit information. The patient will have a different insurance card for the pharmacy benefit information
The Biogen product Start Form may ask for medical and pharmacy benefit information. It is important to complete the Biogen product Start Form with information for both benefits when required. This will provide the specialty pharmacy that is supplying the drug with the information needed to verify the benefit in case the information is out of date or incorrect.
Before a patient leaves the office, check the insurance card information on file to determine if you also need to obtain the pharmacy benefit information from a different card.
It is important to review the patient’s insurance cards carefully to ensure that you are using the proper card (medical or pharmacy) when completing the Biogen product Start Form or applying for claim reimbursement.
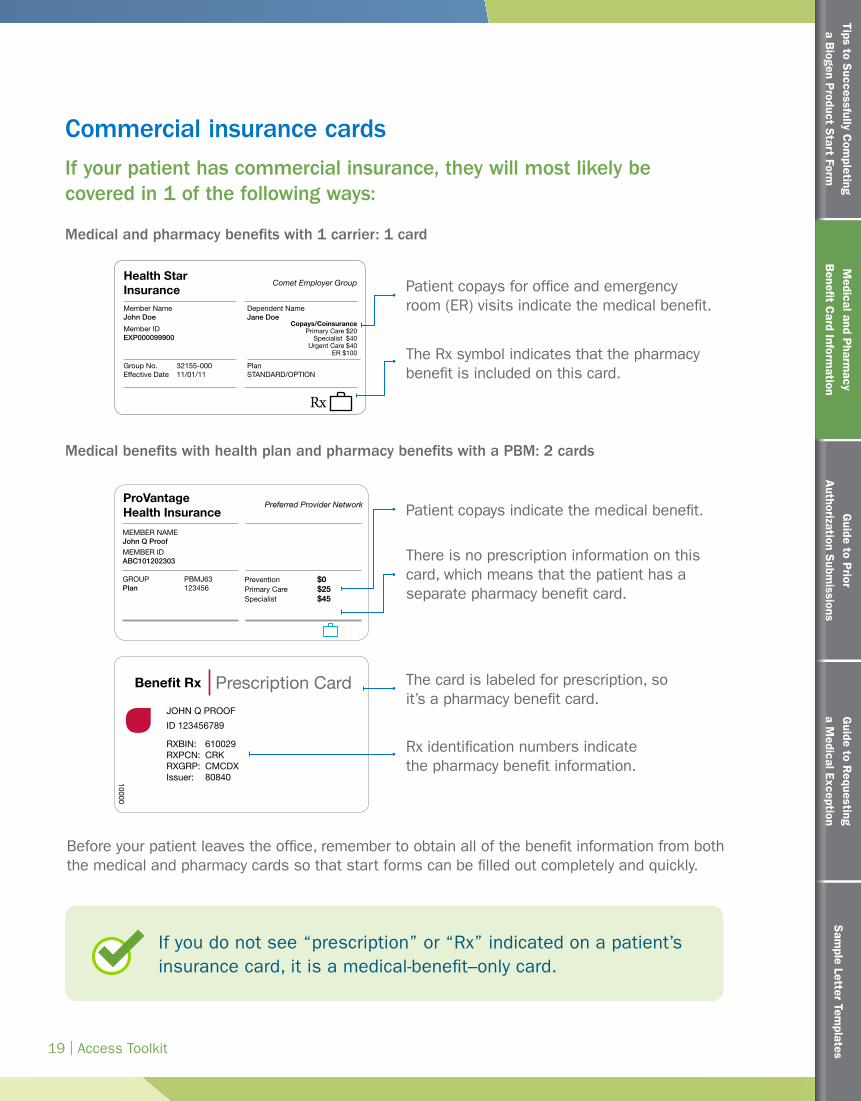
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
19 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Medical and P
harmacy
Benefit C
ard Information
Commercial insurance cardsIf your patient has commercial insurance, they will most likely be covered in 1 of the following ways:
Medical and pharmacy benefits with 1 carrier: 1 card
Health Star Insurance
Comet Employer Group
Rx
Copays/CoinsurancePrimary Care $20
Specialist $40Urgent Care $40
ER $100
Member NameJohn Doe
Member IDEXP000099900
Dependent NameJane Doe
Group No. 32155-000Effective Date 11/01/11
PlanSTANDARD/OPTION
Patient copays for office and emergency room (ER) visits indicate the medical benefit.
Patient copays indicate the medical benefit.
There is no prescription information on this card, which means that the patient has a separate pharmacy benefit card.
The card is labeled for prescription, so it’s a pharmacy benefit card.
Rx identification numbers indicate the pharmacy benefit information.
The Rx symbol indicates that the pharmacy benefit is included on this card.
Medical benefits with health plan and pharmacy benefits with a PBM: 2 cards
Benefit Rx Prescription Card
ProVantage Health Insurance
Preferred Provider Network
MEMBER NAMEJohn Q ProofMEMBER IDABC101202303
Prevention $0Primary Care $25Specialist $45
PBMJ63123456
GROUPPlan
JOHN Q PROOF
ID 123456789
RXBIN: 610029RXPCN: CRKRXGRP: CMCDXIssuer: 8084010000
Before your patient leaves the office, remember to obtain all of the benefit information from both the medical and pharmacy cards so that start forms can be filled out completely and quickly.
If you do not see “prescription” or “Rx” indicated on a patient’s insurance card, it is a medical-benefit–only card.
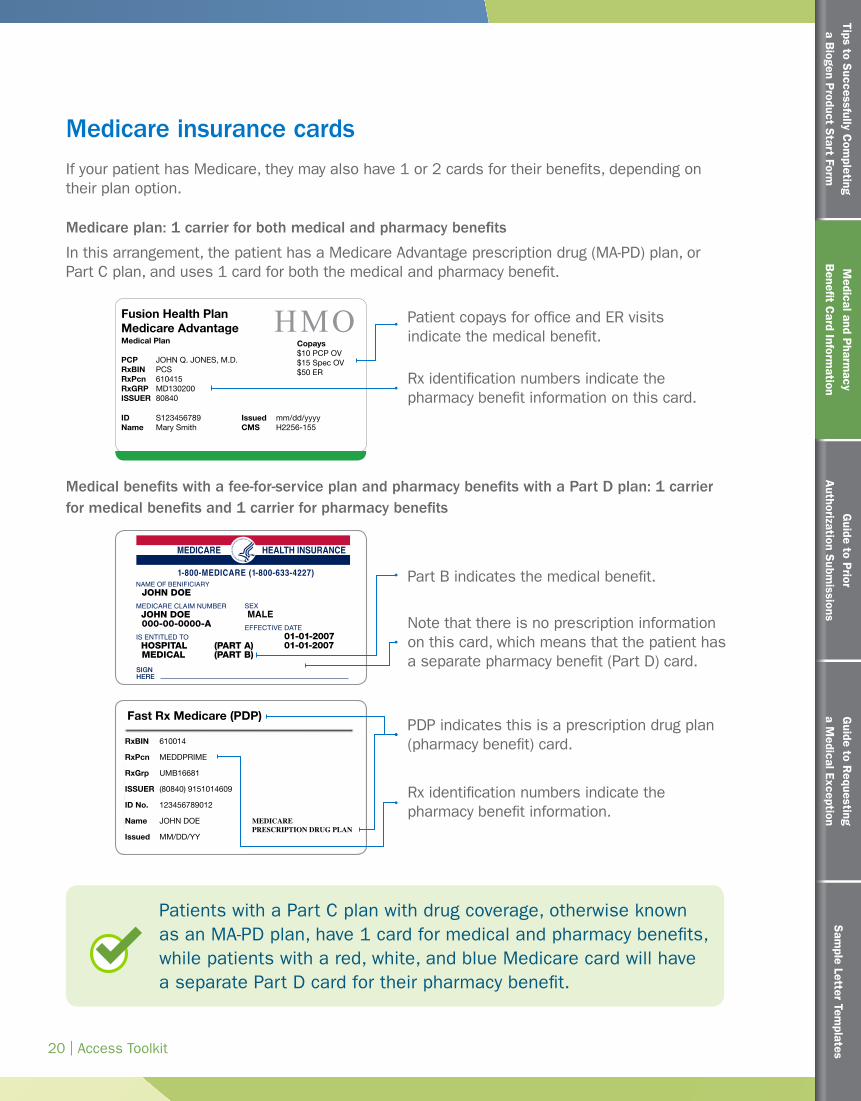
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
20 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Medical and P
harmacy
Benefit C
ard Information
Medicare insurance cardsIf your patient has Medicare, they may also have 1 or 2 cards for their benefits, depending on their plan option.
Medicare plan: 1 carrier for both medical and pharmacy benefits
In this arrangement, the patient has a Medicare Advantage prescription drug (MA-PD) plan, or Part C plan, and uses 1 card for both the medical and pharmacy benefit.
Patient copays for office and ER visits indicate the medical benefit.
Rx identification numbers indicate the pharmacy benefit information on this card.
Fusion Health PlanMedicare Advantage HMOMedical Plan PCP JOHN Q. JONES, M.D.RxBIN PCSRxPcn 610415RxGRP MD130200ISSUER 80840
ID S123456789Name MARY SMITHID S123456789Name Mary Smith
Issued mm/dd/yyyyCMS H2256-155
Copays $10 PCP OV$15 Spec OV$50 ER
Medical benefits with a fee-for-service plan and pharmacy benefits with a Part D plan: 1 carrier for medical benefits and 1 carrier for pharmacy benefits
HEALTH INSURANCEMEDICARE
1-800-MEDICARE (1-800-633-4227)NAME OF BENIFICIARY JOHN DOEMEDICARE CLAIM NUMBER JOHN DOE 000-00-0000-AIS ENTITLED TO HOSPITAL (PART A) MEDICAL (PART B)
SEXMALE
EFFECTIVE DATE 01-01-2007 01-01-2007
SIGNHERE
RxBIN 610014
RxPcn MEDDPRIME
RxGrp UMB16681
ISSUER (80840) 9151014609
ID No. 123456789012
Name JOHN DOE
Issued MM/DD/YY
MEDICARE PRESCRIPTION DRUG PLAN
Fast Rx Medicare (PDP)
Part B indicates the medical benefit.
PDP indicates this is a prescription drug plan (pharmacy benefit) card.
Rx identification numbers indicate the pharmacy benefit information.
Note that there is no prescription information on this card, which means that the patient has a separate pharmacy benefit (Part D) card.
Patients with a Part C plan with drug coverage, otherwise known as an MA-PD plan, have 1 card for medical and pharmacy benefits, while patients with a red, white, and blue Medicare card will have a separate Part D card for their pharmacy benefit.
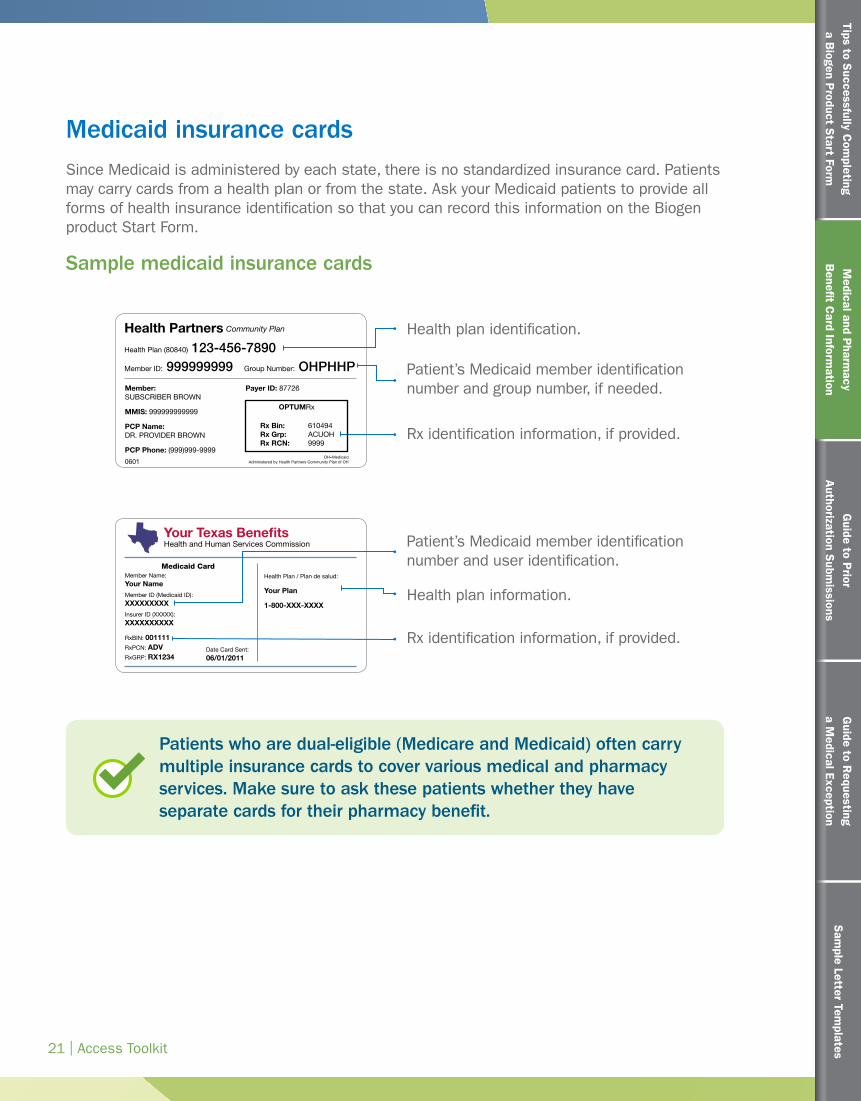
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
21 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Medical and P
harmacy
Benefit C
ard Information
Medicaid insurance cardsSince Medicaid is administered by each state, there is no standardized insurance card. Patients may carry cards from a health plan or from the state. Ask your Medicaid patients to provide all forms of health insurance identification so that you can record this information on the Biogen product Start Form.
Sample medicaid insurance cards
Health Partners
Your Texas BenefitsHealth and Human Services Commission
Community Plan Health plan identification.
Patient’s Medicaid member identification number and user identification.
Patient’s Medicaid member identification number and group number, if needed.
Health plan information.
Rx identification information, if provided.
Rx identification information, if provided.
Health Plan (80840) 123-456-7890Member ID: 999999999 Group Number: OHPHHP
Member:SUBSCRIBER BROWN
MMIS: 999999999999
PCP Name:DR. PROVIDER BROWN
PCP Phone: (999)999-9999
Medicaid CardMember Name:
Your NameMember ID (Medicaid ID):
XXXXXXXXXInsurer ID (XXXXX):
XXXXXXXXXX
RxBIN: 001111RxPCN: ADVRxGRP: RX1234
0601OH=Medicaid
Administered by Health Partners Community Plan of OH
Rx Bin: 610494Rx Grp: ACUOHRx RCN: 9999
Payer ID: 87726
OPTUMRx
Date Card Sent:
06/01/2011
Health Plan / Plan de salud:
Your Plan
1-800-XXX-XXXX
Patients who are dual-eligible (Medicare and Medicaid) often carry multiple insurance cards to cover various medical and pharmacy services. Make sure to ask these patients whether they have separate cards for their pharmacy benefit.
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
22 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Medical and P
harmacy
Benefit C
ard Information
Tips to help your officeUsing the appropriate insurance card on the Biogen product Start Form may help your office expedite new patient starts
For commercial and Medicare patients, some patients have 1 card and some patients have 2 cards
If the patient’s medical insurance card does not have “prescription,” “Rx,” or other similar terms that indicate that the pharmacy benefit is included, you will need to gather the pharmacy benefit information from a separate card
Remember to check the Biogen product Start Form before the patient leaves the office to ensure that you have the required insurance information (medical and pharmacy) on file
Confirming that the insurance information on the Biogen product Start Form is correct upfront may eliminate unnecessary administrative work or callbacks
PAs may be denied due to incomplete or insufficient insurance information, not because the patient does not have coverage for the drug
Eng KJ. Medical benefit specialty drug management—a call to action. Specialty Pharmacy Times website. https://www.specialtypharmacytimes.com/publications/specialty-pharmacy-times/2017/january-2017/medical-benefit-specialty-drug-management-a-call-to-action. Published February 14, 2017. Accessed July 12, 2017.
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates23 | Access Toolkit
Guide to Prior Authorization Submissions
Guide to P
rior A
uthorization Subm
issions
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
24 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Guide to P
rior A
uthorization Subm
issions
Introduction to prior authorizations
In certain instances, your office may need to obtain prior approval from an insurance carrier before the insurer will cover a specific drug for a patient. This request for approval is referred to as prior authorization (PA), precertification, or coverage determination.
PAs are very common for drugs that treat specialty conditions, such as multiple sclerosis (MS), because they enable insurance carriers to monitor costs and ensure that drugs are being used for appropriate patients only. For many drugs that treat specialty conditions, insurance carriers may require a PA renewal after a certain period (typically 1 year). This is true regardless of whether the patient is remaining on the same treatment or transitioning to another treatment.
All insurance carriers are not the same
Each insurance carrier develops its own coverage policies for each drug. The list of covered drugs is called a formulary. Within the formulary, certain drugs are preferred and others are nonpreferred. Nonpreferred drugs are often approved for use only after the patient has tried a preferred therapy. This type of restriction is called step therapy or a step edit because the patient must “step through” the preferred drug(s) first before their insurance will pay for a nonpreferred drug. Nonpreferred drugs often come with higher copays. If the physician determines that a preferred drug is not appropriate for a patient, the physician can submit a medical exception (ME) request to bypass the use of a preferred drug and move to the requested nonpreferred drug.
There are also times when a nonpreferred drug does not have a step therapy restriction, but just a higher copay. It’s important to understand the specific requirements of each insurance carrier.
Above MS™ can help your office understand the PA requirements for most individual insurance carriers in your area. Call Above MS at 1-800-456-2255, Monday through Friday, 8:30 AM to 8 PM ET.
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
25 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Guide to P
rior A
uthorization Subm
issions
How this guide can help with prior authorization submissions
To help you in understanding the submission process for a PA for a Biogen relapsing MS (RMS) therapy, this guide will provide information on
In situations when a drug is not on an insurance carrier’s formulary, the physician may still prescribe it if he or she requests an ME. These requests are typically more complex than PAs and require specific documentation, including a letter of medical necessity and more information about the patient’s medical history. If a drug is on the formulary but covered only after other medications have been tried, the ME process may be used to bypass step therapy requirements.
For more information about the ME process and its requirements, refer to the Guide to Requesting a Medical Exception on page 36 of this toolkit. You can use this guide to supplement other information and resources you have about the ME process.
Prior Authorization vs Medical Exception
Key steps to submitting a PA
Fields to complete on a PA form
Supporting documentation that may be required
Guide to Requestinga Medical Exception
Guide to R
equestinga M
edical Exception
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
26 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Guide to P
rior A
uthorization Subm
issions
Ways to complete a prior authorization
If your patients are prescribed a Biogen product for RMS, there are 3 ways that your office can complete the PA process:
If you faxed a paper Start Form to Above MS™, the in-network specialty pharmacy will conduct a benefits investigation and contact your office to complete the PA submission.
If you are already familiar with the PA process for the insurance carrier in question, you may initiate the PA request yourself and submit the PA request directly to them without waiting for the specialty pharmacy. The remainder of this guide provides step-by-step guidance for this process.
If you are using an ePA portal such as CoverMyMeds, you can initiate, submit, and monitor the status of the PA directly in the portal.
Biogen is working with CoverMyMeds to provide additional support for Biogen product PAs submitted through this portal. Contact Above MS to learn more.
You may also be able to submit the PA using an ePrescribing service, such as iAssist. Biogen is working with iAssist to facilitate ePrescribing of Biogen RMS products.
A
B
C
Above MS and CoverMyMeds can support your office with the PA re-authorization process. Contact Above MS, Monday through
Friday, 8:30 AM to 8 PM ET, at 1-800-456-2255 to learn more.
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
27 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Guide to P
rior A
uthorization Subm
issions
Complete a benefits investigation.Step 1
Steps to completing a prior authorization
A benefits investigation is needed to determine whether your patient has insurance coverage for the prescribed drug. It typically provides information about whether a step edit or other restriction is in place, whether the insurance carrier has restrictions on where the drug can be administered, which specialty pharmacy can ship the drug, and the patient cost-sharing requirements.
If your office submitted a completed Biogen product Start Form to Above MS or directly to an in-network specialty pharmacy, the specialty pharmacy should conduct the benefits investigation on your behalf. The specialty pharmacy may also be able to initiate the PA process, but will likely need additional information from your office. Make sure you respond to the specialty pharmacy to minimize delays in the PA process.
If the physician does not agree with the site of care restriction, you may consider submitting an ME. Refer to the Sample Letter Templates section on page 43 for an additional resource that you may find useful for submitting an ME.
During the benefits investigation for an infused therapy, you may learn that the insurance carrier has restrictions on the site of care where the infusion is administered. For example, the insurance carrier may deny a claim if the infusion is administered at the physician’s office, at a separate infusion center, or in a hospital.
Did You Know?Biogen offers a $0 Copay Program for eligible patients treated with Biogen products. Contact Above MS for more information.
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
28 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Guide to P
rior A
uthorization Subm
issions
Submit the prior authorization form.Step 3
Determine whether the information should be phoned in, faxed, emailed, or submitted via a specific website to the insurance carrier. This information is often listed on the form from CoverMyMeds or a similar ePA service
Add the insurance carrier contact information, proper submission requirements, and other tips to the Insurance Carrier Contact Sheet
Keep a copy of everything your office submits with the request. You may need to reference these documents for many reasons, including if your patient requests Above MS financial assistance services later on
Complete the prior authorization form. Step 2
Review page 30 to learn how supplemental documentation may increase your PA success.
Make sure you have the proper PA form for that payer. Some payers have PA forms specific to MS that differ from their standard PA forms. PAs can be denied simply because the wrong form has been submitted. Contact Above MS™ if you need help finding the proper PA form to use for a Biogen RMS product
Oftentimes the SP may be able to initiate the PA process but may contact your office to collect additional information. Please respond to these communications as soon as you can to help minimize delays
Remember to fill out the form completely. PAs are often denied because the form is missing information
Keep in mind that your office may need to provide additional information to complete the PA form if the specialty pharmacy initiated it on your behalf
For PA reauthorizations, you do not need to submit a Biogen product Start Form; however, other documentation may be required by the insurance carrier.
Biogen is working with CoverMyMeds to facilitate the PA reauthorization process for Biogen RMS products. Contact Above MS for more information.
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
29 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Guide to P
rior A
uthorization Subm
issions
Track the status of the prior authorization request.
Send additional documentation, if required.
Step 4
Step 5
Use the Patient Benefit and Insurance Tracker to keep track of the PA request process
It is important to keep a thorough log of the PA submissions and denials for each patient as this information will be needed if the patient wishes to apply for Above MS financial support services
If additional documentation is requested at any point, make sure to provide it as soon as possible
Did You Know?The PA process can sometimes take longer than expected. If you are concerned with how long the insurance approvalprocess is taking, contact Above MS.
Throughout the PA process, your office may receive calls or emails from Above MS, the specialty pharmacy, or companies working with Biogen to collect more information. Please respond to these communications as soon as you can to help minimize delays in the PA process. Contact Above MS if you have questions about the information that is being requested.
TIPIf you have submitted the PA though an ePA service such as CoverMyMeds, you may be able to track the status of the PA through their portal.
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
30 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Guide to P
rior A
uthorization Subm
issions
Providing supplemental documentation can help increase your chance of successEach insurance carrier is unique in its requirements, so it is essential to identify the specific documents you will need before submitting a PA request. While the preferred forms of documentation may vary, here is a list of items that may be required with your submission:
Completed PA form (forms vary per insurance carrier)
Relevant literature
Clinical patient notes and relevant patient medical history that supports the prescribed therapy
Documented treatment failure of another product
Letter of medical necessity
– In some cases, if a prescription is not consistent with insurance carrier policy, a letter of medical necessity may be required in addition to the PA
• Review the Sample Letter Templates starting on page 43
A successful prior authorization begins with an accurate and complete form
The sample form on the following pages is meant to guide you as you complete a PA form. It cannot be submitted. PA forms vary by insurance carrier and may require more documentation than what is listed on this sample.
Make sure to fill out the insurance carrier’s PA form(s) properly and completely. Failure to do so could delay your patient’s treatment.
TIPMake sure to keep copies of all PA request documents and correspondence for your records.
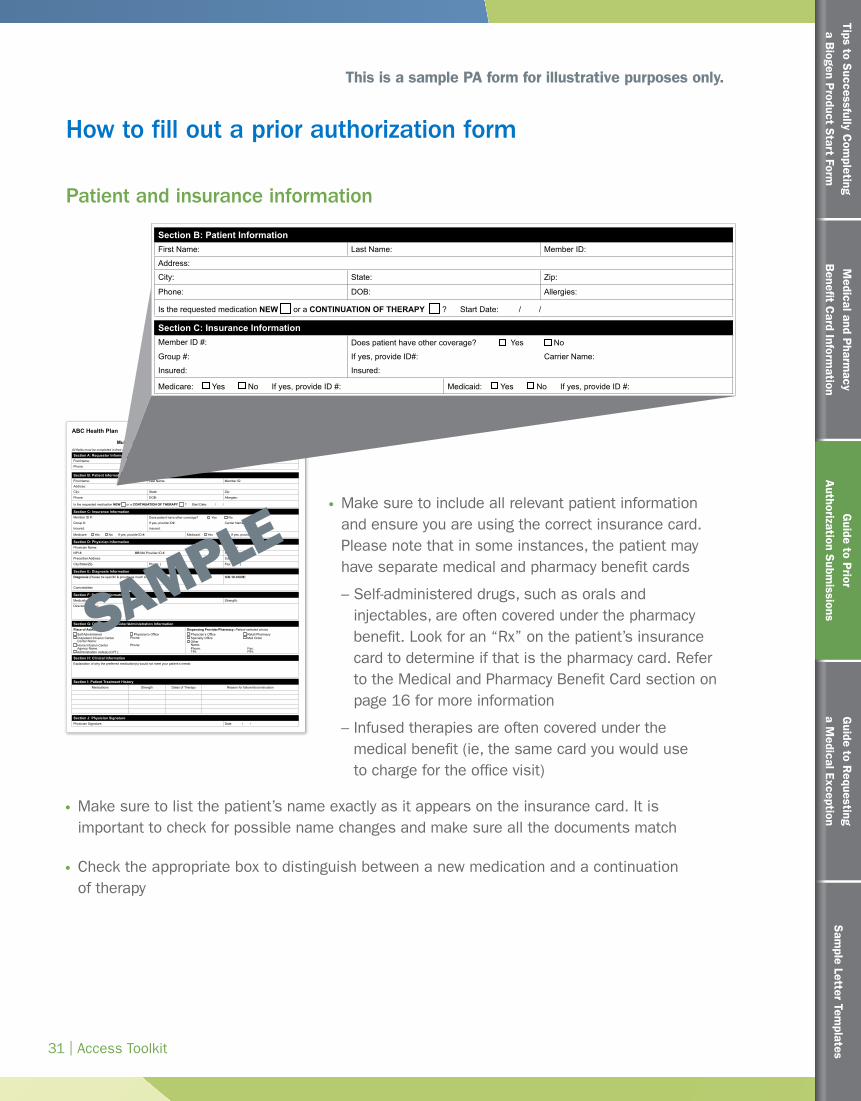
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
31 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Guide to P
rior A
uthorization Subm
issions
How to fill out a prior authorization form
ABC Health Plan
Multiple Sclerosis Therapy Prior Authorization Request FormAll fields must be completed in their entirety and legible.
123 Park Ave. • Hometown, IA • 55555 | Phone: 1-888-555-1234 Fax: 1-888-555-5678 For Medicare Part B — Fax: 1-888-555-9191
Section A: Requestor InformationFirst Name: Last Name:
Phone: Fax: E-mail:
Section B: Patient InformationFirst Name: Last Name: Member ID:
Address:
City: State: Zip:
Phone: DOB: Allergies:
Is the requested medication NEW or a CONTINUATION OF THERAPY ? Start Date: / /
Section I: Patient Treatment HistoryMedications Strength Dates of Therapy Reason for failure/discontinuation
Section G: Dispensing Provider/Administration InformationPlace of Administration: Dispensing Provider/Pharmacy: Patient selected choice
Self Administered Physician’s Office Physician’s Office Retail Pharmacy Outpatient Infusion Center Phone: Specialty Office Mail Order
Center Name: Other Home Infusion Center Phone: Name:
Agency Name: Phone: Fax: Administration code(s) (CPT): TIN: PIN:
Section D: Physician InformationPhysician Name: Specialty:
NPI #: OR MA Provider ID #: State License:
Prescriber Address: Suite #:
City/State/Zip Phone: ( ) Fax: ( )
Section E: Diagnosis InformationDiagnosis (Please be specific & provide as much information as possible): ICD-10-CODE:
Comorbidities
Section H: Clinical InformationExplanation of why the preferred medication(s) would not meet your patient’s needs:
Section F: Product InformationMedication: Strength:
Directions for use:
Section J: Physician SignaturePhysician Signature: Date / /
Section C: Insurance InformationMember ID #: Does patient have other coverage? Yes No
Group #: If yes, provide ID#: Carrier Name:
Insured: Insured:
Medicare: Yes No If yes, provide ID #: Medicaid: Yes No If yes, provide ID #:
Make sure to include all relevant patient information and ensure you are using the correct insurance card. Please note that in some instances, the patient may have separate medical and pharmacy benefit cards
– Self-administered drugs, such as orals and injectables, are often covered under the pharmacy benefit. Look for an “Rx” on the patient’s insurance card to determine if that is the pharmacy card. Refer to the Medical and Pharmacy Benefit Card section on page 16 for more information
– Infused therapies are often covered under the medical benefit (ie, the same card you would use to charge for the office visit)
ABC Health Plan
Multiple Sclerosis Therapy Prior Authorization Request FormAll fields must be completed in their entirety and legible.
123 Park Ave. • Hometown, IA • 55555 | Phone: 1-888-555-1234 Fax: 1-888-555-5678 For Medicare Part B — Fax: 1-888-555-9191
Section A: Requestor InformationFirst Name: Last Name:
Phone: Fax: E-mail:
Section B: Patient InformationFirst Name: Last Name: Member ID:
Address:
City: State: Zip:
Phone: DOB: Allergies:
Is the requested medication NEW or a CONTINUATION OF THERAPY ? Start Date: / /
Section I: Patient Treatment HistoryMedications Strength Dates of Therapy Reason for failure/discontinuation
Section G: Dispensing Provider/Administration InformationPlace of Administration: Dispensing Provider/Pharmacy: Patient selected choice
Self Administered Physician’s Office Physician’s Office Retail Pharmacy Outpatient Infusion Center Phone: Specialty Office Mail Order
Center Name: Other Home Infusion Center Phone: Name:
Agency Name: Phone: Fax: Administration code(s) (CPT): TIN: PIN:
Section D: Physician InformationPhysician Name: Specialty:
NPI #: OR MA Provider ID #: State License:
Prescriber Address: Suite #:
City/State/Zip Phone: ( ) Fax: ( )
Section E: Diagnosis InformationDiagnosis (Please be specific & provide as much information as possible): ICD-10-CODE:
Comorbidities
Section H: Clinical InformationExplanation of why the preferred medication(s) would not meet your patient’s needs:
Section F: Product InformationMedication: Strength:
Directions for use:
Section J: Physician SignaturePhysician Signature: Date / /
Section C: Insurance InformationMember ID #: Does patient have other coverage? Yes No
Group #: If yes, provide ID#: Carrier Name:
Insured: Insured:
Medicare: Yes No If yes, provide ID #: Medicaid: Yes No If yes, provide ID #:
Patient and insurance information
SAMPLE
This is a sample PA form for illustrative purposes only.
Make sure to list the patient’s name exactly as it appears on the insurance card. It is important to check for possible name changes and make sure all the documents match
Check the appropriate box to distinguish between a new medication and a continuation of therapy
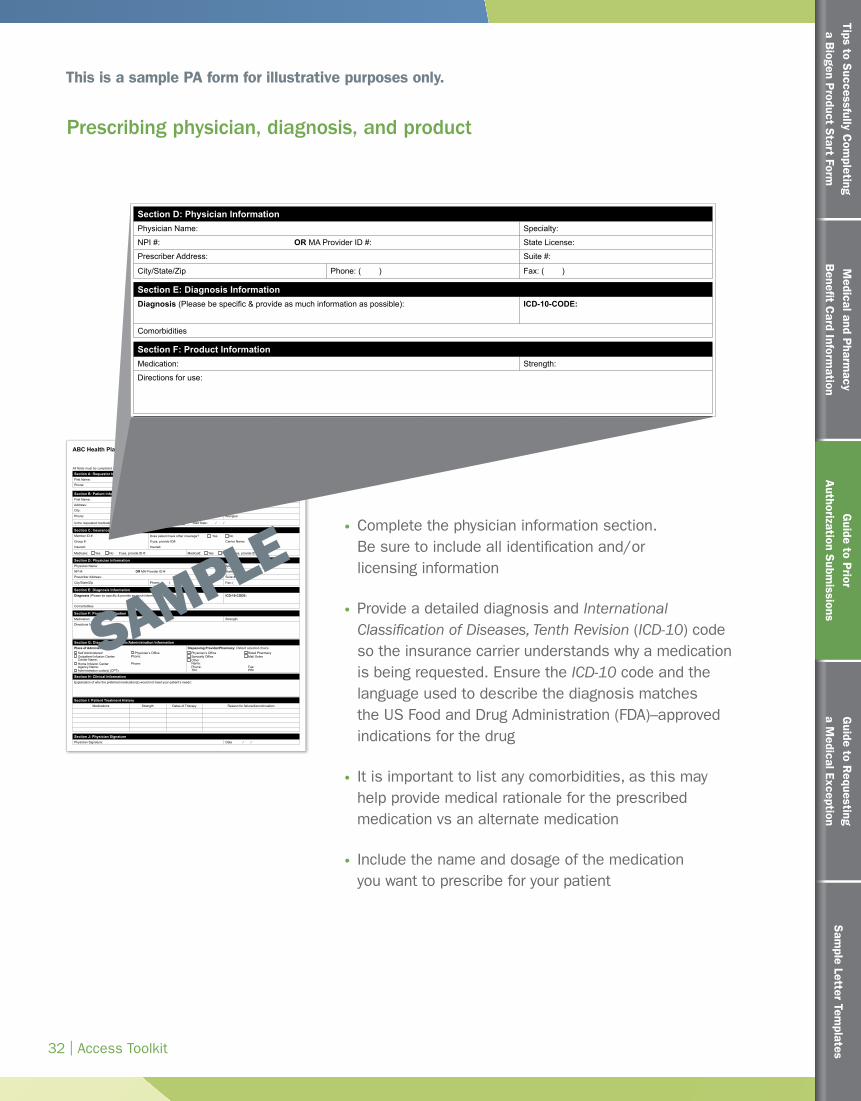
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
32 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Guide to P
rior A
uthorization Subm
issions
ABC Health Plan
Multiple Sclerosis Therapy Prior Authorization Request FormAll fields must be completed in their entirety and legible.
123 Park Ave. • Hometown, IA • 55555 | Phone: 1-888-555-1234 Fax: 1-888-555-5678 For Medicare Part B — Fax: 1-888-555-9191
Section A: Requestor InformationFirst Name: Last Name:
Phone: Fax: E-mail:
Section B: Patient InformationFirst Name: Last Name: Member ID:
Address:
City: State: Zip:
Phone: DOB: Allergies:
Is the requested medication NEW or a CONTINUATION OF THERAPY ? Start Date: / /
Section I: Patient Treatment HistoryMedications Strength Dates of Therapy Reason for failure/discontinuation
Section G: Dispensing Provider/Administration InformationPlace of Administration: Dispensing Provider/Pharmacy: Patient selected choice
Self Administered Physician’s Office Physician’s Office Retail Pharmacy Outpatient Infusion Center Phone: Specialty Office Mail Order
Center Name: Other Home Infusion Center Phone: Name:
Agency Name: Phone: Fax: Administration code(s) (CPT): TIN: PIN:
Section D: Physician InformationPhysician Name: Specialty:
NPI #: OR MA Provider ID #: State License:
Prescriber Address: Suite #:
City/State/Zip Phone: ( ) Fax: ( )
Section E: Diagnosis InformationDiagnosis (Please be specific & provide as much information as possible): ICD-10-CODE:
Comorbidities
Section H: Clinical InformationExplanation of why the preferred medication(s) would not meet your patient’s needs:
Section F: Product InformationMedication: Strength:
Directions for use:
Section J: Physician SignaturePhysician Signature: Date / /
Section C: Insurance InformationMember ID #: Does patient have other coverage? Yes No
Group #: If yes, provide ID#: Carrier Name:
Insured: Insured:
Medicare: Yes No If yes, provide ID #: Medicaid: Yes No If yes, provide ID #:
Complete the physician information section. Be sure to include all identification and/or licensing information
Provide a detailed diagnosis and International Classification of Diseases, Tenth Revision (ICD-10) code so the insurance carrier understands why a medication is being requested. Ensure the ICD-10 code and the language used to describe the diagnosis matches the US Food and Drug Administration (FDA)–approved indications for the drug
It is important to list any comorbidities, as this may help provide medical rationale for the prescribed medication vs an alternate medication
Include the name and dosage of the medication you want to prescribe for your patient
ABC Health Plan
Multiple Sclerosis Therapy Prior Authorization Request FormAll fields must be completed in their entirety and legible.
123 Park Ave. • Hometown, IA • 55555 | Phone: 1-888-555-1234 Fax: 1-888-555-5678 For Medicare Part B — Fax: 1-888-555-9191
Section A: Requestor InformationFirst Name: Last Name:
Phone: Fax: E-mail:
Section B: Patient InformationFirst Name: Last Name: Member ID:
Address:
City: State: Zip:
Phone: DOB: Allergies:
Is the requested medication NEW or a CONTINUATION OF THERAPY ? Start Date: / /
Section I: Patient Treatment HistoryMedications Strength Dates of Therapy Reason for failure/discontinuation
Section G: Dispensing Provider/Administration InformationPlace of Administration: Dispensing Provider/Pharmacy: Patient selected choice
Self Administered Physician’s Office Physician’s Office Retail Pharmacy Outpatient Infusion Center Phone: Specialty Office Mail Order
Center Name: Other Home Infusion Center Phone: Name:
Agency Name: Phone: Fax: Administration code(s) (CPT): TIN: PIN:
Section D: Physician InformationPhysician Name: Specialty:
NPI #: OR MA Provider ID #: State License:
Prescriber Address: Suite #:
City/State/Zip Phone: ( ) Fax: ( )
Section E: Diagnosis InformationDiagnosis (Please be specific & provide as much information as possible): ICD-10-CODE:
Comorbidities
Section H: Clinical InformationExplanation of why the preferred medication(s) would not meet your patient’s needs:
Section F: Product InformationMedication: Strength:
Directions for use:
Section J: Physician SignaturePhysician Signature: Date / /
Section C: Insurance InformationMember ID #: Does patient have other coverage? Yes No
Group #: If yes, provide ID#: Carrier Name:
Insured: Insured:
Medicare: Yes No If yes, provide ID #: Medicaid: Yes No If yes, provide ID #:
Prescribing physician, diagnosis, and product
This is a sample PA form for illustrative purposes only.
SAMPLE

Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
33 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Guide to P
rior A
uthorization Subm
issions
ABC Health Plan
Multiple Sclerosis Therapy Prior Authorization Request FormAll fields must be completed in their entirety and legible.
123 Park Ave. • Hometown, IA • 55555 | Phone: 1-888-555-1234 Fax: 1-888-555-5678 For Medicare Part B — Fax: 1-888-555-9191
Section A: Requestor InformationFirst Name: Last Name:
Phone: Fax: E-mail:
Section B: Patient InformationFirst Name: Last Name: Member ID:
Address:
City: State: Zip:
Phone: DOB: Allergies:
Is the requested medication NEW or a CONTINUATION OF THERAPY ? Start Date: / /
Section I: Patient Treatment HistoryMedications Strength Dates of Therapy Reason for failure/discontinuation
Section G: Dispensing Provider/Administration InformationPlace of Administration: Dispensing Provider/Pharmacy: Patient selected choice
Self Administered Physician’s Office Physician’s Office Retail Pharmacy Outpatient Infusion Center Phone: Specialty Office Mail Order
Center Name: Other Home Infusion Center Phone: Name:
Agency Name: Phone: Fax: Administration code(s) (CPT): TIN: PIN:
Section D: Physician InformationPhysician Name: Specialty:
NPI #: OR MA Provider ID #: State License:
Prescriber Address: Suite #:
City/State/Zip Phone: ( ) Fax: ( )
Section E: Diagnosis InformationDiagnosis (Please be specific & provide as much information as possible): ICD-10-CODE:
Comorbidities
Section H: Clinical InformationExplanation of why the preferred medication(s) would not meet your patient’s needs:
Section F: Product InformationMedication: Strength:
Directions for use:
Section J: Physician SignaturePhysician Signature: Date / /
Section C: Insurance InformationMember ID #: Does patient have other coverage? Yes No
Group #: If yes, provide ID#: Carrier Name:
Insured: Insured:
Medicare: Yes No If yes, provide ID #: Medicaid: Yes No If yes, provide ID #:
The place of administration is the site of care. It is important that you specify the site of care here, even if the drug is self administered (eg, an oral or an injectable)
For the Dispensing Provider/Pharmacy section, make sure to use the information found from the benefits investigation to ensure you are listing a specialty pharmacy that is in-network. Above MS™ can help you determine the correct specialty pharmacy
If the prescribed medication is nonpreferred or not covered on the insurance carrier’s formulary, provide a detailed explanation describing why the preferred formulary medications are not appropriate for your patient. Review the Sample Letter Templates starting on page 43 and the Biogen Product Clinical Cardsa as examples when developing your explanation. You may need to provide additional documentation, such as medical literature and the patient’s medical history
ABC Health Plan
Multiple Sclerosis Therapy Prior Authorization Request FormAll fields must be completed in their entirety and legible.
123 Park Ave. • Hometown, IA • 55555 | Phone: 1-888-555-1234 Fax: 1-888-555-5678 For Medicare Part B — Fax: 1-888-555-9191
Section A: Requestor InformationFirst Name: Last Name:
Phone: Fax: E-mail:
Section B: Patient InformationFirst Name: Last Name: Member ID:
Address:
City: State: Zip:
Phone: DOB: Allergies:
Is the requested medication NEW or a CONTINUATION OF THERAPY ? Start Date: / /
Section I: Patient Treatment HistoryMedications Strength Dates of Therapy Reason for failure/discontinuation
Section G: Dispensing Provider/Administration InformationPlace of Administration: Dispensing Provider/Pharmacy: Patient selected choice
Self Administered Physician’s Office Physician’s Office Retail Pharmacy Outpatient Infusion Center Phone: Specialty Office Mail Order
Center Name: Other Home Infusion Center Phone: Name:
Agency Name: Phone: Fax: Administration code(s) (CPT): TIN: PIN:
Section D: Physician InformationPhysician Name: Specialty:
NPI #: OR MA Provider ID #: State License:
Prescriber Address: Suite #:
City/State/Zip Phone: ( ) Fax: ( )
Section E: Diagnosis InformationDiagnosis (Please be specific & provide as much information as possible): ICD-10-CODE:
Comorbidities
Section H: Clinical InformationExplanation of why the preferred medication(s) would not meet your patient’s needs:
Section F: Product InformationMedication: Strength:
Directions for use:
Section J: Physician SignaturePhysician Signature: Date / /
Section C: Insurance InformationMember ID #: Does patient have other coverage? Yes No
Group #: If yes, provide ID#: Carrier Name:
Insured: Insured:
Medicare: Yes No If yes, provide ID #: Medicaid: Yes No If yes, provide ID #:
Place of administration, dispensing provider/pharmacy, and clinical information
This is a sample PA form for illustrative purposes only.
SAMPLE
a Ask your Biogen representative about the Biogen Product Clinical Cards in the printed version of the Access Toolkit.
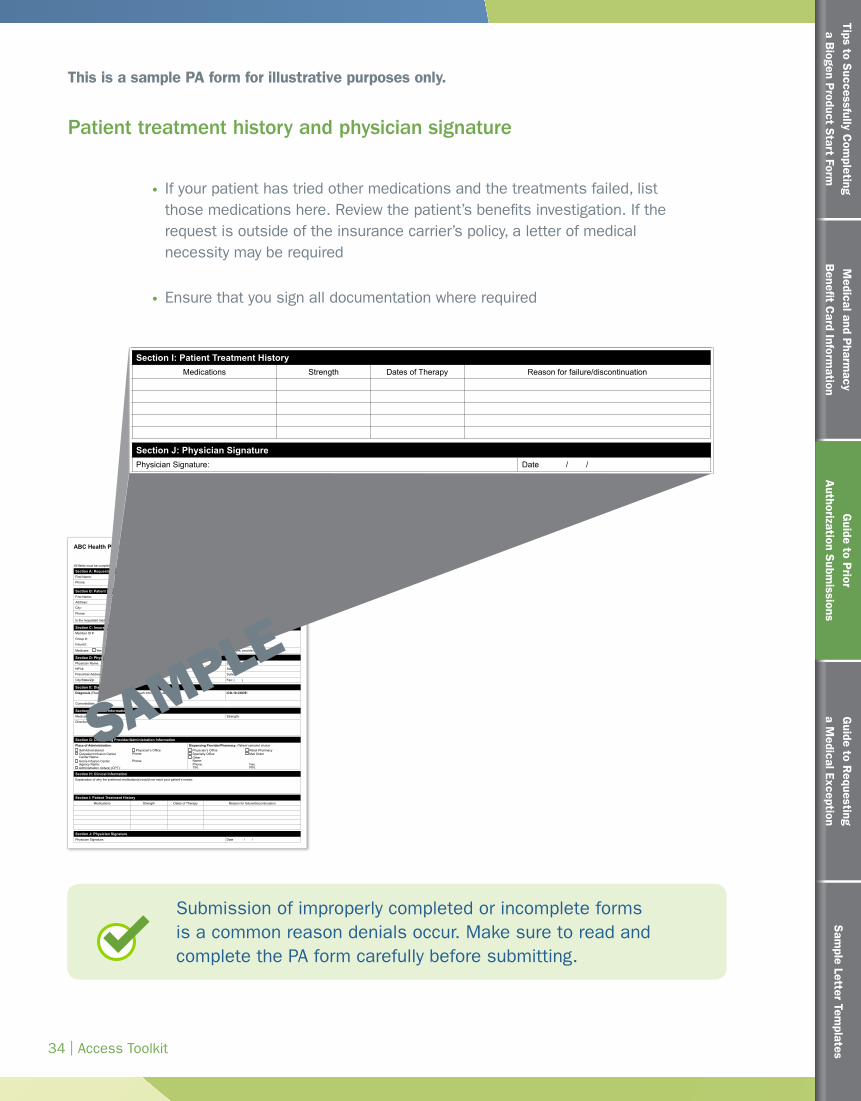
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
34 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Guide to P
rior A
uthorization Subm
issions
Submission of improperly completed or incomplete forms is a common reason denials occur. Make sure to read and complete the PA form carefully before submitting.
ABC Health Plan
Multiple Sclerosis Therapy Prior Authorization Request FormAll fields must be completed in their entirety and legible.
123 Park Ave. • Hometown, IA • 55555 | Phone: 1-888-555-1234 Fax: 1-888-555-5678 For Medicare Part B — Fax: 1-888-555-9191
Section A: Requestor InformationFirst Name: Last Name:
Phone: Fax: E-mail:
Section B: Patient InformationFirst Name: Last Name: Member ID:
Address:
City: State: Zip:
Phone: DOB: Allergies:
Is the requested medication NEW or a CONTINUATION OF THERAPY ? Start Date: / /
Section I: Patient Treatment HistoryMedications Strength Dates of Therapy Reason for failure/discontinuation
Section G: Dispensing Provider/Administration InformationPlace of Administration: Dispensing Provider/Pharmacy: Patient selected choice
Self Administered Physician’s Office Physician’s Office Retail Pharmacy Outpatient Infusion Center Phone: Specialty Office Mail Order
Center Name: Other Home Infusion Center Phone: Name:
Agency Name: Phone: Fax: Administration code(s) (CPT): TIN: PIN:
Section D: Physician InformationPhysician Name: Specialty:
NPI #: OR MA Provider ID #: State License:
Prescriber Address: Suite #:
City/State/Zip Phone: ( ) Fax: ( )
Section E: Diagnosis InformationDiagnosis (Please be specific & provide as much information as possible): ICD-10-CODE:
Comorbidities
Section H: Clinical InformationExplanation of why the preferred medication(s) would not meet your patient’s needs:
Section F: Product InformationMedication: Strength:
Directions for use:
Section J: Physician SignaturePhysician Signature: Date / /
Section C: Insurance InformationMember ID #: Does patient have other coverage? Yes No
Group #: If yes, provide ID#: Carrier Name:
Insured: Insured:
Medicare: Yes No If yes, provide ID #: Medicaid: Yes No If yes, provide ID #:
If your patient has tried other medications and the treatments failed, list those medications here. Review the patient’s benefits investigation. If the request is outside of the insurance carrier’s policy, a letter of medical necessity may be required
Ensure that you sign all documentation where required
ABC Health Plan
Multiple Sclerosis Therapy Prior Authorization Request FormAll fields must be completed in their entirety and legible.
123 Park Ave. • Hometown, IA • 55555 | Phone: 1-888-555-1234 Fax: 1-888-555-5678 For Medicare Part B — Fax: 1-888-555-9191
Section A: Requestor InformationFirst Name: Last Name:
Phone: Fax: E-mail:
Section B: Patient InformationFirst Name: Last Name: Member ID:
Address:
City: State: Zip:
Phone: DOB: Allergies:
Is the requested medication NEW or a CONTINUATION OF THERAPY ? Start Date: / /
Section I: Patient Treatment HistoryMedications Strength Dates of Therapy Reason for failure/discontinuation
Section G: Dispensing Provider/Administration InformationPlace of Administration: Dispensing Provider/Pharmacy: Patient selected choice
Self Administered Physician’s Office Physician’s Office Retail Pharmacy Outpatient Infusion Center Phone: Specialty Office Mail Order
Center Name: Other Home Infusion Center Phone: Name:
Agency Name: Phone: Fax: Administration code(s) (CPT): TIN: PIN:
Section D: Physician InformationPhysician Name: Specialty:
NPI #: OR MA Provider ID #: State License:
Prescriber Address: Suite #:
City/State/Zip Phone: ( ) Fax: ( )
Section E: Diagnosis InformationDiagnosis (Please be specific & provide as much information as possible): ICD-10-CODE:
Comorbidities
Section H: Clinical InformationExplanation of why the preferred medication(s) would not meet your patient’s needs:
Section F: Product InformationMedication: Strength:
Directions for use:
Section J: Physician SignaturePhysician Signature: Date / /
Section C: Insurance InformationMember ID #: Does patient have other coverage? Yes No
Group #: If yes, provide ID#: Carrier Name:
Insured: Insured:
Medicare: Yes No If yes, provide ID #: Medicaid: Yes No If yes, provide ID #:
Patient treatment history and physician signature
SAMPLE
This is a sample PA form for illustrative purposes only.
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
35 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Guide to P
rior A
uthorization Subm
issions
In the case of a denial
There are many reasons why a PA may be denied. One of the main reasons PA requests are denied is incomplete or inaccurate information on the PA form. Check to ensure all information is accurately completed and resubmit the form, if necessary.
In the event that the PA request has been denied, the physician can appeal the decision by contacting the insurance carrier directly to have a peer-to-peer discussion regarding the patient, the clinical issues, and the reasons for requesting a specific drug. If a phone call is not possible, you may submit a written ME request. Refer to the next section, Guide to Requesting a Medical Exception on page 36 for more information.
Help with PA requests for Biogen products
If you are having difficulty obtaining approval for a Biogen product, contact Above MS™ to receive further assistance at 1-800-456-2255, Monday through Friday, 8:30 AM to 8 PM ET.
TIP
If you work with a specific individual at the insurance carrier to handle denials of PA requests, be sure to record that individual’s contact information on the Insurance Carrier Contact Sheet
Record the denial number or code on the Patient Benefit and Insurance Tracker
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates36 | Access Toolkit
Guide to Requestinga Medical Exception
Guide to R
equestinga M
edical Exception
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
37 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Guide to R
equestinga M
edical Exception
If you have questions about the ME process for a Biogen product, call Above MS™ at 1-800-456-2255, Monday through Friday, 8:30 am to 8 pm ET.
If you are concerned with how long the insurance approval process is taking, contact Above MS.
Reviewing the steps to a medical exception approval
There are occasions when a physician may wish to prescribe a medication outside of an insurance carrier’s standard coverage policy. This request for approval is called a medical exception (ME). An ME communicates a physician’s request to use medication that is nonpreferred or not covered due to the patient’s individual circumstances.
When to use a medical exception
If a medication is on formulary but not preferred, the ME process may be used to bypass step therapy requirements. An ME request is typically more complex than a prior authorization (PA) or precertification and requires specific documentation, such as a specific ME form or a letter of medical necessity.

Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
38 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Guide to R
equestinga M
edical Exception
Steps to completing a medical exception— when a medical exception is needed
STEP 1 Determine the need for a medical exception.
Determine if the plan will require an ME for the prescribed therapy for your patient. You may already be familiar with a plan’s requirements from a previous experience.
If a specialty pharmacy completes the benefits investigation on your behalf, they may notify you that an ME is required based on the plan’s formulary or coverage policies.
If the PA was rejected and the physician still feels that the prescribed medication is appropriate for the patient, he or she may choose to submit an ME.
This guide provides information and considerations for preparing a comprehensive ME package—from submitting the ME request and additional documentation to tracking the process.
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
39 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Request for formulary tier exception Sample Letter Template
[Insert Date]
[Insert Date]
Request for Formulary Tier Exception for Patient Prescribed [Insert Product Name] for Relapsing Multiple Sclerosis (RMS)
RE: [Patient Name], [Patient Insurance ID Number], [Patient Date of Birth]
Dear [Health Plan Contact Name]:
I am writing to request a formulary tier exception for my patient. The standard [copay/coinsurance] associated with the assigned tier for [Insert Product Name] would present a significant financial burden to my patient. Based on my [XX] years of treating this patient and my experience in treating MS, the most appropriate medication for my patient at this time is [Insert Product Name]. However, the current [copay/coinsurance] prevents my patient from receiving this medication. I am requesting that [Insert Product Name] be made available to my patient for the same out-of-pocket cost as a preferred medication.
In the past, [Patient Name] has attempted other treatments for RMS.
Medication Strength Dates of therapy Reason for failure/discontinuation
Additionally, I have included documentation regarding my patient that supports my decision. I ask that you review the information I have indicated below when reviewing my request
☐ Relevant medication history ☐ Anti-JCV antibody status ☐ MRI data ☐ Patient’s history of relapses ☐ EDSS history
In the case that this request is denied, I am also at this time requesting a peer-to-peer discussion with a plan Medical Director. Please feel free to contact me if you require further information regarding this request. I look forward to your response as soon as possible. Sincerely, [Name]
50
49
Placeholder:SOC letter of medical necessity
Request for site of care exceptionLetter of Medical Necessity
[Insert Date] Request for patient to [Continue Receiving Infusions OR Receive Infusions] at [Insert Name of Site of Care] [Optional: Claim rejection number] RE: [Patient Name], [Patient Insurance ID Number], [Patient Date of Birth] Dear [Health Plan Contact Name]: This letter is regarding your site of care policy of [Insert Product Name] for my patient. I feel that [Insert Name of Site of Care] is the most appropriate location for [Patient Name] to receive [his/her] [Insert Product Name] treatment. [Patient Name] has been receiving [Insert Product Name] at [Insert Name of Site of Care] for [XX] years. [Patient Name] is treated at this site approximately every month. The staff is very familiar with [his/her] health status and treatment plan. I do not want my patient to have any disruption in this continuity of care. I would like my patient to remain at their current site of care for the following reason(s): [Include any additional information related to this patient’s history that supports them continuing treatment at the current site of care, for example: • The new location is too far from my patient’s home (specify distance, if significant) • My patient relies on transportation from others/public transportation and the new location would
represent a burden to coordinate a new method of travel • My patient has disease complexity (List disease complexity, ie, fatigue, lower extremity impairment,
difficultly following a treatment plan) that would make transitioning to a different site of care difficult • My patient is acclimated to the current location’s process and consistent treatment plan • The clinical staff at the current location is familiar with the patient's medical history and symptomatic
response to the infusion process • Any information the patient has communicated to the HCP about why this site of care is preferred] In the case that this application for [Patient Name] to remain at [Insert Name of Site of Care] for treatment is denied, I am also at this time requesting a peer-to-peer discussion with a plan medical director. Please feel free to contact me if you require further information regarding this request. I look forward to your response as soon as possible. Sincerely, [Name]
Completing the ME request may require a special ME form from the insurance carrier or a separate letter from your office
Provide any additional information and documentation. Review the sample Letter of Medical Necessity templates starting on page 43 as additional examples for consideration
Refer to the Biogen Product Clinical Cardsa for efficacy and safety information that you may consider including in your letter of medical necessity
If a product is on a nonpreferred tier and has a high copay that your patient may not be able to afford, the Formulary Tier Exception Letter template on page 50 may be one option to potentially help
PatienttoremainoncurrenttherapyLetterofMedicalNecessity
©2016Biogen. Allrightsreserved. PrintedintheU.S.A. 08/16 FCH-US-XXXX
[InsertDate]
RequestforPatienttoRemainonCurrentRelapsingMultipleSclerosis(RMS)Therapy[InsertProductName]
[Optional:Claimrejectionnumber]
RE:[PatientName],[PatientInsuranceIDNumber],[PatientDateofBirth]
Dear[HealthPlanContactName]:
Thisletterisregardingyourcoveragepolicythatrequiresmetotakemypatientoffof[InsertProductName].Ihavereviewedyourprescriptiondrugpolicy;however,Ifeelthatthemostappropriatetreatmentformypatientfallsoutsidetheestablishedpolicy.Asthephysician,Imaybeheldaccountablefortherisksandconsequencesstemmingfromtreatmentdecisions,andassuchImustbeempoweredtomakeinformedtherapydecisionsfollowingseriousconsiderationofallbenefitsandrisksuniquetomypatient.ThisisespeciallycrucialinadiseaseascomplexandheterogeneousasMS,forwhichtheAmericanAcademyofNeurologyhasnotissuedtreatmentguidelines.Ithasbeenmyexperiencethatdisease-modifyingtherapiestotreatRMSarenotinterchangeable.Theymayvaryinefficacy,administration,mechanismsofaction,andsideeffects.Movementtoanotherdrugtherapymayimpacttheprogresswehavemadetodate.
Ihavebeenworkingwithmypatientsince[InsertDate]tomanagetheirdisease.Mypatienthasbeenon[InsertProductName]since[InsertDate],andduringthistimemypatienthasshownstabilitywithtreatment,assummarizedbelow:
• [NonewlesionsasevidencedbyMRIdata]since[InsertDate]• [Nodeclineindisabilitystatus]asof[InsertDate]
Additionally,inmymedicalopinion,Ibelievethattransitioningtherapymaycauseunnecessaryharmtomypatientforthefollowingreason(s):[Insertreason(s)].Ihaveincludedadditionaldocumentationregardingmypatient,whichsupportsmydecision.IaskthatyoureviewtheinformationIhaveindicatedbelowwhenreviewingmyrequest:
� Relevantmedicationhistory� Anti-JCVantibodystatus� MRIdata� Patient’shistoryofrelapses� EDSShistory
[Providethereason(s)that[ProductName]isthemostappropriatetreatmentforthispatientbasedonmedicalhistory,positiveornegativeanti-JCVantibodystatus,MRIdata,historyofrelapses,orEDSShistory.]Inthecasethatthisappealisdenied,IamalsoatthistimerequestingapeertopeerwithaplanMedicalDirector.Pleasefeelfreetocontactmeifyourequirefurtherinformationregardingthisrequest.Ilookforwardtoyourresponseassoonaspossible.Sincerely,[Name]
STEP 2 Complete the medical exception request with a letter of medical necessity, as needed.
A common reason that MEs are denied is because there is missing or incorrect information on the form. This may delay treatment for your patient. Remember to carefully and accurately complete the ME request form.
An effective letter of medical necessity focuses on your specific patient’s needs
Be clear about your patient’s individual circumstance—it is important that your letter includes whether you are initiating or changing treatment, or whether you want to continue your patient’s therapy but his or her health insurance benefits have changed. The following are key considerations when writing a letter of medical necessity.
Provide a background on your patient’s RMS
Summarize his or her disease measures, such as magnetic resonance imaging (MRI) data, Expanded Disability Status Scale (EDSS) score, and relapse history
If appropriate, list any failed medications and provide clinical evidence of the patient’s inadequate response
Steps to completing a medical exception— letter of medical necessity
PatienttotransitiontoanothertherapyLetterofMedicalNecessity
©2016Biogen.Allrightsreserved.PrintedintheU.S.A.08/16FCH-US-XXXX
[InsertDate]
RequestforPatienttoTransitiontoAnotherRelapsingMultipleSclerosis(RMS)Therapy[InsertProductName]
[Optional:Claimrejectionnumber]
RE:[PatientName],[PatientInsuranceIDNumber],[PatientDateofBirth]
Dear[HealthPlanContactName]:
Thisletterisregardingyourcoveragepolicyof[InsertProductName]formypatient.Ihavereviewedyourprescriptiondrugpolicy;however,Ifeelthatthemostappropriatetreatmentformypatientfallsoutsidetheestablishedpolicy.Asthephysician,Imaybeheldaccountablefortherisksandconsequencesstemmingfromtreatmentdecisions,andassuchImustbeempoweredtomakeinformedtherapydecisionsfollowingseriousconsiderationofallbenefitsandrisksuniquetomypatient.ThisisespeciallycrucialinadiseaseascomplexandheterogeneousasMS,forwhichtheAmericanAcademyofNeurologyhasnotissuedtreatmentguidelines.Disease-modifyingtherapiestotreatRMSarenotinterchangeableandmayvarysubstantiallyintheirreal-worldeffectivenessandsafetyindifferentpatients.Basedonmy[XX]yearstreatingthispatientandmyextensiveexperienceintreatingMS,Ifeelthat[InsertProductName]isthemostappropriatechoicefor[PatientName].
Ihavebeenworkingwithmypatientsince[InsertDate]tomanagetheirdisease.Theyhavebeenon[InsertProductName]since[InsertDate],andthelimitedresultsthatIhaveseennecessitateachangeintreatment.
Mymainconcernsregardingmypatient’scurrentmedicationinclude
• [Reason(s)previoustreatment(s)unsuitable]• [Chooseanitem.]• [Chooseanitem.]
Irecommendtransitioning[PatientName]to[InsertProductName]becauseitisthemostappropriatetherapeuticoptionforthefollowingreason(s):
• [Reason(s)thistreatmentismostappropriateforpatient,suchasefficacyprofileofthisproduct,safetyandtolerabilityprofileofthisproduct,andpatientpreference]
[Ifasteptherapybefore[ProductName]isrequired,includereason(s)whysteptherapywouldnotbeanappropriatetreatmentforthispatient.]
Additionally,IaskthatyoureviewtheclinicalinformationIhavesubmitted,whichsupportsmydecisiontochangemedication.Below,IhaveindicatedtheadditionalinformationthatIhavesubmittedwiththisletter:
� Relevantmedicationhistory� Anti-JCVantibodystatus� MRIdata� Patient’shistoryofrelapses� EDSShistory
[Providereasonthat[ProductName]isthemostappropriatetreatmentforthispatientbasedonmedicalhistory,positiveornegativeanti-JCVantibodystatus,MRIdata,historyofrelapses,orEDSShistory.]Inthecasethatthisappealisdenied,IamalsoatthistimerequestingapeertopeerwithaplanMedicalDirector.Pleasefeelfreetocontactmeifyourequirefurtherinformationregardingthisrequest.Ilookforwardtoyourresponseassoonaspossible.Sincerely,[Name]
PatientstartingnewtherapyLetterofMedicalNecessity
[InsertDate]
RequestforPatientNotPreviouslyTreatedWithaDisease-ModifyingTherapyforRelapsingMultipleSclerosis(RMS)toReceive[InsertProductName]
[Optional:Claimrejectionnumber]
RE:[PatientName],[PatientInsuranceIDNumber],[PatientDateofBirth]
Dear[HealthPlanContactName]:
Thisletterisregardingyourcoveragepolicyof[InsertProductName]formypatient.Ihavereviewedyourprescriptiondrugpolicy;however,Ifeelthatthemostappropriatetreatmentformypatientfallsoutsidetheestablishedpolicy.Asthephysician,Imaybeheldaccountablefortherisksandconsequencesstemmingfromtreatmentdecisions,andassuchImustbeempoweredtomakeinformedtherapydecisionsfollowingseriousconsiderationofallbenefitsandrisksuniquetomypatient.ThisisespeciallycrucialinadiseaseascomplexandheterogeneousasMS,forwhichtheAmericanAcademyofNeurologyhasnotissuedtreatmentguidelines.Disease-modifyingtherapiestotreatRMSarenotinterchangeableandmayvarysubstantiallyintheirreal-worldeffectivenessandsafetyindifferentpatients.Basedonmy[XX]yearstreatingthispatientandmyextensiveexperienceintreatingMS,theRMSmedicationspreferredbyyourcoveragepolicyarenotappropriateformypatientandmypatient’sMS,andthemostappropriatemedicationforinitiatingtherapyfor[his/her]RMSis[InsertProductName].
Ihaveevaluatedmypatient’sclinicalsymptomsandhaveprovidedasummarybelow:• [MRIdata]• [Physicaldisability]• [Relapse]• [Laboratoryvalues]
Iamprescribing[InsertProductName]formypatientbecauseIhaveconcludedthatitisthemostappropriatetherapeuticoptionfor[him/her]forthefollowingreason(s):
• [Reason(s)thistreatmentismostappropriateforpatient,suchasefficacyprofileofthisproduct,safetyandtolerabilityprofileofthisproduct,andpatientpreference]
[Ifasteptherapybefore[ProductName]isrequired,includereason(s)whysteptherapywouldnotbeanappropriatetreatmentforthispatient.]
Also,IaskthatyoureviewanyclinicalinformationIhavesubmittedregardingmypatientwhenconsideringmyrequest,aswellasreviewingclinicalguidelinesandrecentclinicaltrialresults.IhaveindicatedtheadditionalinformationthatIhavesubmittedwiththisletterbelow:
� Relevantmedicationhistory� Anti-JCVantibodystatus� MRIdata� Patient’shistoryofrelapses� EDSShistory
[Providereason(s)that[ProductName]isthemostappropriatetreatmentforthispatientbasedonmedicalhistory,positiveornegativeanti-JCVantibodystatus,MRIdata,historyofrelapses,orEDSShistory.]
aAsk your Biogen representative about the Biogen Product Clinical Cards in the printed version of the Access Toolkit.
Guide to R
equestinga M
edical Exception
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
40 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Guide to R
equestinga M
edical Exception
Explain why the treatment you prescribed is the appropriate choice for your patient
Provide a clinical justification supporting the treatment you have chosen for your patient
State any patient-specific reasons for the treatment choice such as efficacy, tolerability issues, or route of administration or comorbidities that preclude the insurance carrier’s preferred medication
Cite relevant literature
Explain why the insurer’s preferred treatments are not appropriate for your patient
Include detailed reasons why all preferred drugs on the insurance carrier’s formulary are not appropriate for your patient
List side effects or adverse events that the patient may experience on the insurer’s suggested treatment
Cite experience on similar treatments and why they are not suitable for your patient
List any compliance concerns
Describe individual patient considerations that impact the choice of treatment
Be sure to note if the healthcare provider is a multiple sclerosis specialist, many health plans value indicating this information in the letter of medical necessity
Additional documentation that supports your decision will strengthen your request.
Details from the patient’s medical record
EDSS scores, MRI data, and relapse history
If appropriate, general medical history listing comorbidities and any medication history, including contraindications
Provide documentation of clinical evidence for treatment failure such as inadequate response, adverse events, or side effects
Other relevant patient information may also be included, as appropriate
Other documentation
Letters from consultants or other healthcare professionals that support your treatment choice
Clinical information regarding your treatment choice, such as published literature
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
41 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Guide to R
equestinga M
edical Exception
Determine whether the ME needs to be submitted to the insurance carrier via phone, fax, email, or a specific website
Determine the appropriate individual to contact regarding the ME request
Update the Insurance Carrier Contact Sheet with specific information related to submitting an ME for the insurance carrier, such as submission format (eg, fax or email)
ME requests for Biogen RMS products can also be submitted through the CoverMyMeds portal
Track the ME request using the Patient Benefit and Insurance Tracker
Remember to document the date, time, and method of submission. In addition, you can use this tracker to document your follow up with the insurance carrier
STEP 3
STEP 4
Determine how to submit the medical exception
Track the status of the medical exception request.
Steps to completing a medical exception— submission and tracking
Some states have legislation that requires insurance carriers to respond to ME requests within a certain period of time. Contact Above MS™ to learn whether this applies in your state.
Insurance Carrier Name Phone EmailContact
RoleDept. Additional Notes
Preference for PA and/or ME SubmissionsRelevant Web Links
Phone Fax Email Other
Insurance Carrier Contact SheetThe Insurance Carrier Contact Sheet resource will enable you to capture key contact information and related processes for payers.
ME=medical exception; PA=prior authorization.For infusible products, please see the Payer Summary Reference Guide resource available from Biogen.
PatientAccount#/Identification
Name Gender DateofBirth Neurologist PrescribedDrug
PharmacyInsuranceProvider
MemberIdentification
RxBIN RxGrp
1234567891011121314151617181920212223242526272829303132333435363738394041424344454647484950515253545556575859606162636465666768697071727374
PATIENTINFORMATION
PATIENTBENEFITANDINSURANCETRACKER
AdditionalInformation
Pa-entInforma-onHome Benefits Investigation PA Request
PATIENT BENEFIT AND INSURANCE TRACKER - GUIDE & INSTRUCTIONSThisPatientBenefitandInsuranceTrackermayhelpyourofficekeeptrackofpatientbenefitsinvestigationsandthestatusofpriorauthorizations(PA),appeals,and/ormedicalexception(ME)requestsforself-administered(oral,injectable)therapies.AboveMS™cancompletethebenefitsinvestigationifyoudecidetoenrollyourpatientsintheprogram.Contact1-800-456-2255today.
PleasenotethatBiogenalsooffersseparateresourcestohelpkeeptrackofthebuy-and-billprocessforinfusibletreatments.PleasecontactyourBiogenrepresentativeformoreinformationabouttheseresources.
Thistemplateisdesignedwith4spreadsheetstocapturethefollowing:1.PatientInformation2.BenefitsInvestigationInformation3.PAInformation4.MEInformation
Eachrowhasauniqueidentifiertoguideyouthroughenteringthepatientdataacrossthe4sheets,asnecessary.Thismeansyouwillneedtoenterauniquenumberforeachpatient.Toenhanceeaseofuse,manyfieldswillpopulatebasedonpriorinformationenteredorwillallowfordrop-downselections.Therefore,itisnecessarytostartyourdataentrywiththePatientInformationsheet.
Oncecompleted,thePatientBenefitandInsuranceTrackerincludespatientprotectedhealthinformationandisonlymeanttobeaquickreferencetrackingtoollimitedtothehealthcareprofessional’soffice.Thislogdoesnotreplaceanyauthorizationformsthatmustbefilledoutbythepatient,healthcareprofessional,office,orotherpersonnel.TocomplywiththeHealthInsurancePortabilityandAccountabilityActorHIPAArequirements,andtoprotecttheprivacyofprotectedhealthinformation,noinformationshouldbedisseminatedtoindividualsorthirdparties.PleasedonotshareanypatientinformationwithyourBiogenrepresentative.
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
42 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Guide to R
equestinga M
edical Exception
There are many reasons why an ME may be denied. A common reason is that there is inaccurate or incomplete information on the request. Carefully review the request to ensure that the information is correct and that no information has been omitted. Resubmit the request, if necessary. Above MS can help you understand the process for handling an ME denial. Make sure to provide the denial number so Above MS can help more quickly.
If all information was complete, but the ME was denied due to clinical reasons, the prescribing physician in your office may also contact the insurance carrier directly to speak with a clinical representative. This individual is typically someone with a medical background and may be called a medical director. A peer-to-peer discussion regarding the patient that includes more detailed information about the patient’s medical history and clinical considerations as well as the reason for the requested treatment can take place. This discussion may help the insurance carrier understand the concerns for your patient with the preferred formulary drugs and why there is an ME request for a different treatment.
If the healthcare provider is able to obtain the direct contact information for the clinical representative for future peer-to-peer discussion, be sure to track that information in the Insurance Carrier Contact Sheet.
If the medical exception is denied
Above MS can help your office and your patient
The Above MSTM program can help your office work through the process of obtaining insurance approval for a Biogen product for relapsing multiple sclerosis, including prior authorizations (PAs) and MEs.
Biogen is dedicated to helping your patients access the medication they need. You and your patients can call a Support Coordinator at 1-800-456-2255, Monday through Friday, 8:30 AM to 8 PM ET, or go to AboveMS.com.
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates43 | Access Toolkit
Sample Letter Templates
Sam
ple Letter Templates
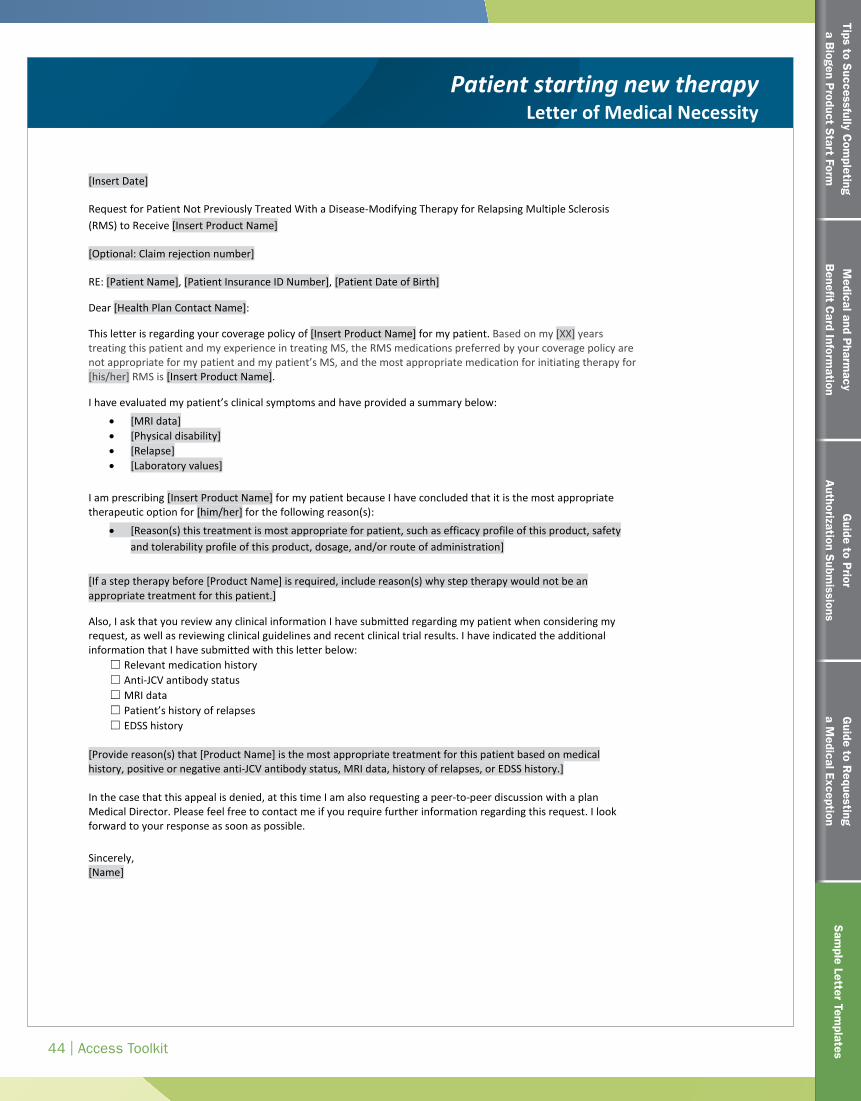
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
44 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Sam
ple Letter Templates
PatientstartingnewtherapyLetterofMedicalNecessity
[InsertDate]
RequestforPatientNotPreviouslyTreatedWithaDisease-ModifyingTherapyforRelapsingMultipleSclerosis(RMS)toReceive[InsertProductName]
[Optional:Claimrejectionnumber]
RE:[PatientName],[PatientInsuranceIDNumber],[PatientDateofBirth]
Dear[HealthPlanContactName]:
Thisletterisregardingyourcoveragepolicyof[InsertProductName]formypatient.Ihavereviewedyourprescriptiondrugpolicy;however,Ifeelthatthemostappropriatetreatmentformypatientfallsoutsidetheestablishedpolicy.Asthephysician,Imaybeheldaccountablefortherisksandconsequencesstemmingfromtreatmentdecisions,andassuchImustbeempoweredtomakeinformedtherapydecisionsfollowingseriousconsiderationofallbenefitsandrisksuniquetomypatient.ThisisespeciallycrucialinadiseaseascomplexandheterogeneousasMS,forwhichtheAmericanAcademyofNeurologyhasnotissuedtreatmentguidelines.Disease-modifyingtherapiestotreatRMSarenotinterchangeableandmayvarysubstantiallyintheirreal-worldeffectivenessandsafetyindifferentpatients.Basedonmy[XX]yearstreatingthispatientandmyextensiveexperienceintreatingMS,theRMSmedicationspreferredbyyourcoveragepolicyarenotappropriateformypatientandmypatient’sMS,andthemostappropriatemedicationforinitiatingtherapyfor[his/her]RMSis[InsertProductName].
Ihaveevaluatedmypatient’sclinicalsymptomsandhaveprovidedasummarybelow:• [MRIdata]• [Physicaldisability]• [Relapse]• [Laboratoryvalues]
Iamprescribing[InsertProductName]formypatientbecauseIhaveconcludedthatitisthemostappropriatetherapeuticoptionfor[him/her]forthefollowingreason(s):
• [Reason(s)thistreatmentismostappropriateforpatient,suchasefficacyprofileofthisproduct,safetyandtolerabilityprofileofthisproduct,andpatientpreference]
[Ifasteptherapybefore[ProductName]isrequired,includereason(s)whysteptherapywouldnotbeanappropriatetreatmentforthispatient.]
Also,IaskthatyoureviewanyclinicalinformationIhavesubmittedregardingmypatientwhenconsideringmyrequest,aswellasreviewingclinicalguidelinesandrecentclinicaltrialresults.IhaveindicatedtheadditionalinformationthatIhavesubmittedwiththisletterbelow:
� Relevantmedicationhistory� Anti-JCVantibodystatus� MRIdata� Patient’shistoryofrelapses� EDSShistory
[Providereason(s)that[ProductName]isthemostappropriatetreatmentforthispatientbasedonmedicalhistory,positiveornegativeanti-JCVantibodystatus,MRIdata,historyofrelapses,orEDSShistory.]
[Insert Date]
Request for Patient Not Previously Treated With a Disease-Modifying Therapy for Relapsing Multiple Sclerosis (RMS) to Receive [Insert Product Name]
[Optional: Claim rejection number]
RE: [Patient Name], [Patient Insurance ID Number], [Patient Date of Birth]
Dear [Health Plan Contact Name]:
This letter is regarding your coverage policy of [Insert Product Name] for my patient. Based on my [XX] years treating this patient and my experience in treating MS, the RMS medications preferred by your coverage policy are not appropriate for my patient and my patient’s MS, and the most appropriate medication for initiating therapy for [his/her] RMS is [Insert Product Name].
I have evaluated my patient’s clinical symptoms and have provided a summary below:
• [MRI data] • [Physical disability] • [Relapse] • [Laboratory values]
I am prescribing [Insert Product Name] for my patient because I have concluded that it is the most appropriate therapeutic option for [him/her] for the following reason(s):
• [Reason(s) this treatment is most appropriate for patient, such as efficacy profile of this product, safety and tolerability profile of this product, dosage, and/or route of administration]
[If a step therapy before [Product Name] is required, include reason(s) why step therapy would not be an appropriate treatment for this patient.]
Also, I ask that you review any clinical information I have submitted regarding my patient when considering my request, as well as reviewing clinical guidelines and recent clinical trial results. I have indicated the additional information that I have submitted with this letter below:
☐ Relevant medication history ☐ Anti-JCV antibody status ☐ MRI data ☐ Patient’s history of relapses ☐ EDSS history
[Provide reason(s) that [Product Name] is the most appropriate treatment for this patient based on medical history, positive or negative anti-JCV antibody status, MRI data, history of relapses, or EDSS history.] In the case that this appeal is denied, at this time I am also requesting a peer-to-peer discussion with a plan Medical Director. Please feel free to contact me if you require further information regarding this request. I look forward to your response as soon as possible. Sincerely, [Name]
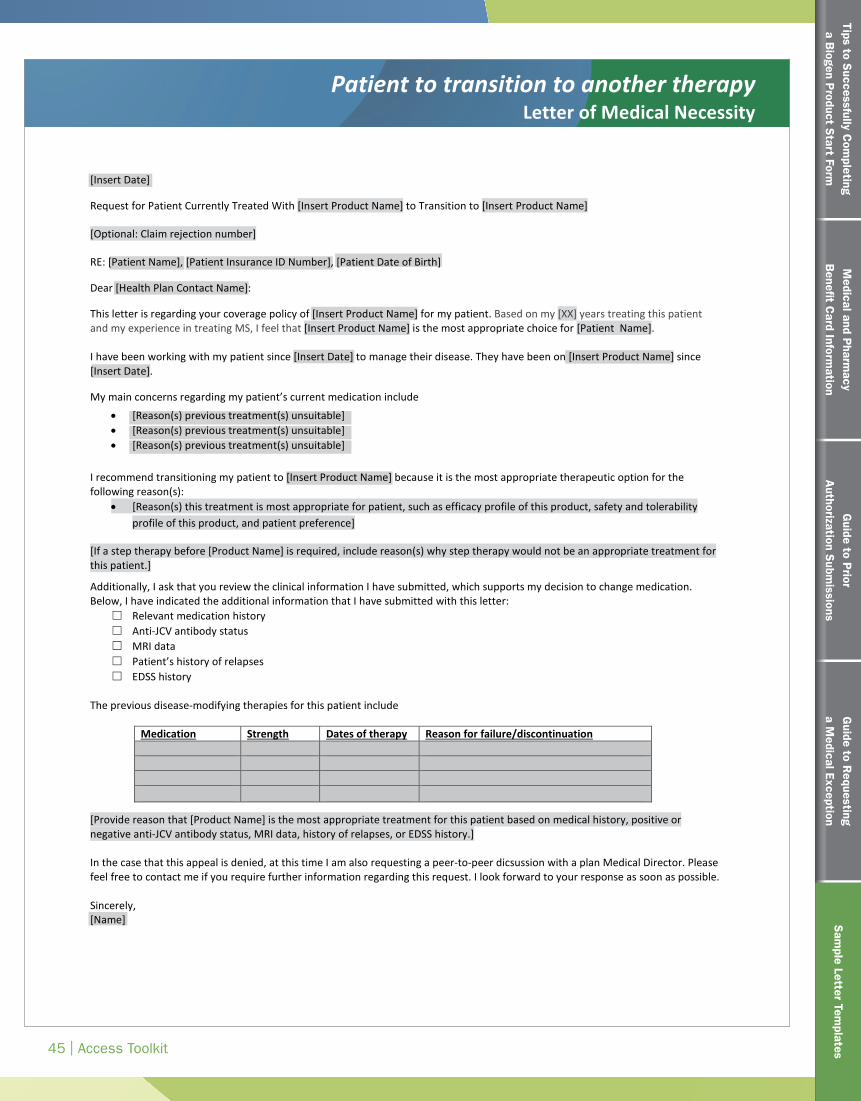
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
45 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Sam
ple Letter Templates
PatienttotransitiontoanothertherapyLetterofMedicalNecessity
©2016Biogen.Allrightsreserved.PrintedintheU.S.A.08/16FCH-US-XXXX
[InsertDate]
RequestforPatienttoTransitiontoAnotherRelapsingMultipleSclerosis(RMS)Therapy[InsertProductName]
[Optional:Claimrejectionnumber]
RE:[PatientName],[PatientInsuranceIDNumber],[PatientDateofBirth]
Dear[HealthPlanContactName]:
Thisletterisregardingyourcoveragepolicyof[InsertProductName]formypatient.Ihavereviewedyourprescriptiondrugpolicy;however,Ifeelthatthemostappropriatetreatmentformypatientfallsoutsidetheestablishedpolicy.Asthephysician,Imaybeheldaccountablefortherisksandconsequencesstemmingfromtreatmentdecisions,andassuchImustbeempoweredtomakeinformedtherapydecisionsfollowingseriousconsiderationofallbenefitsandrisksuniquetomypatient.ThisisespeciallycrucialinadiseaseascomplexandheterogeneousasMS,forwhichtheAmericanAcademyofNeurologyhasnotissuedtreatmentguidelines.Disease-modifyingtherapiestotreatRMSarenotinterchangeableandmayvarysubstantiallyintheirreal-worldeffectivenessandsafetyindifferentpatients.Basedonmy[XX]yearstreatingthispatientandmyextensiveexperienceintreatingMS,Ifeelthat[InsertProductName]isthemostappropriatechoicefor[PatientName].
Ihavebeenworkingwithmypatientsince[InsertDate]tomanagetheirdisease.Theyhavebeenon[InsertProductName]since[InsertDate],andthelimitedresultsthatIhaveseennecessitateachangeintreatment.
Mymainconcernsregardingmypatient’scurrentmedicationinclude
• [Reason(s)previoustreatment(s)unsuitable]• [Chooseanitem.]• [Chooseanitem.]
Irecommendtransitioning[PatientName]to[InsertProductName]becauseitisthemostappropriatetherapeuticoptionforthefollowingreason(s):
• [Reason(s)thistreatmentismostappropriateforpatient,suchasefficacyprofileofthisproduct,safetyandtolerabilityprofileofthisproduct,andpatientpreference]
[Ifasteptherapybefore[ProductName]isrequired,includereason(s)whysteptherapywouldnotbeanappropriatetreatmentforthispatient.]
Additionally,IaskthatyoureviewtheclinicalinformationIhavesubmitted,whichsupportsmydecisiontochangemedication.Below,IhaveindicatedtheadditionalinformationthatIhavesubmittedwiththisletter:
� Relevantmedicationhistory� Anti-JCVantibodystatus� MRIdata� Patient’shistoryofrelapses� EDSShistory
[Providereasonthat[ProductName]isthemostappropriatetreatmentforthispatientbasedonmedicalhistory,positiveornegativeanti-JCVantibodystatus,MRIdata,historyofrelapses,orEDSShistory.]Inthecasethatthisappealisdenied,IamalsoatthistimerequestingapeertopeerwithaplanMedicalDirector.Pleasefeelfreetocontactmeifyourequirefurtherinformationregardingthisrequest.Ilookforwardtoyourresponseassoonaspossible.Sincerely,[Name]
[Insert Date]
Request for Patient Currently Treated With [Insert Product Name] to Transition to [Insert Product Name]
[Optional: Claim rejection number]
RE: [Patient Name], [Patient Insurance ID Number], [Patient Date of Birth]
Dear [Health Plan Contact Name]:
This letter is regarding your coverage policy of [Insert Product Name] for my patient. Based on my [XX] years treating this patient and my experience in treating MS, I feel that [Insert Product Name] is the most appropriate choice for [Patient Name]. I have been working with my patient since [Insert Date] to manage their disease. They have been on [Insert Product Name] since [Insert Date].
My main concerns regarding my patient’s current medication include
• [Reason(s) previous treatment(s) unsuitable] • [Reason(s) previous treatment(s) unsuitable] • [Reason(s) previous treatment(s) unsuitable]
I recommend transitioning my patient to [Insert Product Name] because it is the most appropriate therapeutic option for the following reason(s):
• [Reason(s) this treatment is most appropriate for patient, such as efficacy profile of this product, safety and tolerability profile of this product, and patient preference]
[If a step therapy before [Product Name] is required, include reason(s) why step therapy would not be an appropriate treatment for this patient.]
Additionally, I ask that you review the clinical information I have submitted, which supports my decision to change medication. Below, I have indicated the additional information that I have submitted with this letter:
☐ Relevant medication history ☐ Anti-JCV antibody status ☐ MRI data ☐ Patient’s history of relapses ☐ EDSS history
The previous disease-modifying therapies for this patient include
[Provide reason that [Product Name] is the most appropriate treatment for this patient based on medical history, positive or negative anti-JCV antibody status, MRI data, history of relapses, or EDSS history.] In the case that this appeal is denied, at this time I am also requesting a peer-to-peer dicsussion with a plan Medical Director. Please feel free to contact me if you require further information regarding this request. I look forward to your response as soon as possible. Sincerely, [Name]
Medication Strength Dates of therapy Reason for failure/discontinuation
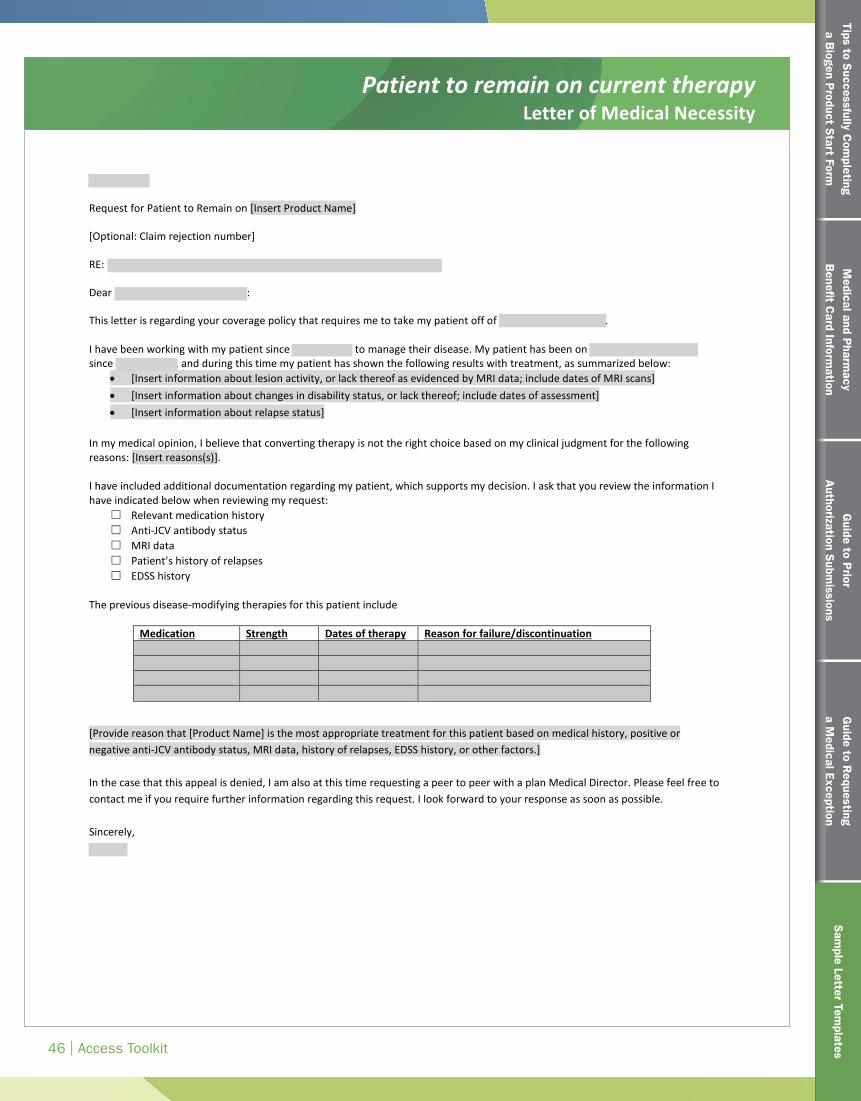
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
46 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Sam
ple Letter Templates
PatienttoremainoncurrenttherapyLetterofMedicalNecessity
©2016Biogen. Allrightsreserved. PrintedintheU.S.A. 08/16 FCH-US-XXXX
[InsertDate]
RequestforPatienttoRemainonCurrentRelapsingMultipleSclerosis(RMS)Therapy[InsertProductName]
[Optional:Claimrejectionnumber]
RE:[PatientName],[PatientInsuranceIDNumber],[PatientDateofBirth]
Dear[HealthPlanContactName]:
Thisletterisregardingyourcoveragepolicythatrequiresmetotakemypatientoffof[InsertProductName].Ihavereviewedyourprescriptiondrugpolicy;however,Ifeelthatthemostappropriatetreatmentformypatientfallsoutsidetheestablishedpolicy.Asthephysician,Imaybeheldaccountablefortherisksandconsequencesstemmingfromtreatmentdecisions,andassuchImustbeempoweredtomakeinformedtherapydecisionsfollowingseriousconsiderationofallbenefitsandrisksuniquetomypatient.ThisisespeciallycrucialinadiseaseascomplexandheterogeneousasMS,forwhichtheAmericanAcademyofNeurologyhasnotissuedtreatmentguidelines.Ithasbeenmyexperiencethatdisease-modifyingtherapiestotreatRMSarenotinterchangeable.Theymayvaryinefficacy,administration,mechanismsofaction,andsideeffects.Movementtoanotherdrugtherapymayimpacttheprogresswehavemadetodate.
Ihavebeenworkingwithmypatientsince[InsertDate]tomanagetheirdisease.Mypatienthasbeenon[InsertProductName]since[InsertDate],andduringthistimemypatienthasshownstabilitywithtreatment,assummarizedbelow:
• [NonewlesionsasevidencedbyMRIdata]since[InsertDate]• [Nodeclineindisabilitystatus]asof[InsertDate]
Additionally,inmymedicalopinion,Ibelievethattransitioningtherapymaycauseunnecessaryharmtomypatientforthefollowingreason(s):[Insertreason(s)].Ihaveincludedadditionaldocumentationregardingmypatient,whichsupportsmydecision.IaskthatyoureviewtheinformationIhaveindicatedbelowwhenreviewingmyrequest:
� Relevantmedicationhistory� Anti-JCVantibodystatus� MRIdata� Patient’shistoryofrelapses� EDSShistory
[Providethereason(s)that[ProductName]isthemostappropriatetreatmentforthispatientbasedonmedicalhistory,positiveornegativeanti-JCVantibodystatus,MRIdata,historyofrelapses,orEDSShistory.]Inthecasethatthisappealisdenied,IamalsoatthistimerequestingapeertopeerwithaplanMedicalDirector.Pleasefeelfreetocontactmeifyourequirefurtherinformationregardingthisrequest.Ilookforwardtoyourresponseassoonaspossible.Sincerely,[Name]
[Insert Date]
Request for Patient to Remain on [Insert Product Name]
[Optional: Claim rejection number]
RE: [Patient Name], [Patient Insurance ID Number], [Patient Date of Birth]
Dear [Health Plan Contact Name]:
This letter is regarding your coverage policy that requires me to take my patient off of [Insert Product Name]. I have been working with my patient since [Insert Date] to manage their disease. My patient has been on [Insert Product Name] since [Insert Date], and during this time my patient has shown the following results with treatment, as summarized below:
• [Insert information about lesion activity, or lack thereof as evidenced by MRI data; include dates of MRI scans] • [Insert information about changes in disability status, or lack thereof; include dates of assessment] • [Insert information about relapse status]
In my medical opinion, I believe that converting therapy is not the right choice based on my clinical judgment for the following reasons: [Insert reasons(s)]. I have included additional documentation regarding my patient, which supports my decision. I ask that you review the information I have indicated below when reviewing my request:
☐ Relevant medication history ☐ Anti-JCV antibody status ☐ MRI data ☐ Patient’s history of relapses ☐ EDSS history
The previous disease-modifying therapies for this patient include
[Provide reason that [Product Name] is the most appropriate treatment for this patient based on medical history, positive or negative anti-JCV antibody status, MRI data, history of relapses, EDSS history, or other factors.] In the case that this appeal is denied, I am also at this time requesting a peer to peer with a plan Medical Director. Please feel free to contact me if you require further information regarding this request. I look forward to your response as soon as possible. Sincerely, [Name]
Medication Strength Dates of therapy Reason for failure/discontinuation
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
47 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Sam
ple Letter Templates
Placeholder:SOC letter of medical necessity
Request for site of care exceptionLetter of Medical Necessity
[Insert Date] Request for patient to [Continue Receiving Infusions OR Receive Infusions] at [Insert Name of Site of Care] [Optional: Claim rejection number] RE: [Patient Name], [Patient Insurance ID Number], [Patient Date of Birth] Dear [Health Plan Contact Name]: This letter is regarding your site of care policy of [Insert Product Name] for my patient. I feel that [Insert Name of Site of Care] is the most appropriate location for [Patient Name] to receive [his/her] [Insert Product Name] treatment. [Patient Name] has been receiving [Insert Product Name] at [Insert Name of Site of Care] for [XX] years. [Patient Name] is treated at this site approximately every month. The staff is very familiar with [his/her] health status and treatment plan. I do not want my patient to have any disruption in this continuity of care. I would like my patient to remain at their current site of care for the following reason(s): [Include any additional information related to this patient’s history that supports them continuing treatment at the current site of care, for example: • List details about the patient's logistical ability to travel to the infusion site, for example, distance or
transportation • List details about patient considerations such as:
o Physical and cognitive limitations o Familiarity and comfort between patient site and patient o Potential disruption to multiple sclerosis treatment plan
• Any information the patient has communicated to the HCP about why this site of care is preferred]
In the case that this application for [Patient Name] to remain at [Insert Name of Site of Care] for treatment is denied, I am also requesting a peer-to-peer discussion with a plan medical director. Please feel free to contact me if you require further information regarding this request. I look forward to your response as soon as possible. Sincerely, [Name]
Tips to Successfully C
ompleting
a Biogen P
roduct Start Form
48 | Access Toolkit
Medical and P
harmacy
Benefit C
ard Information
Guide to P
rior A
uthorization Subm
issionsG
uide to Requesting
a Medical Exception
Sam
ple Letter Templates
Sam
ple Letter Templates
Request for formulary tier exception Sample Letter Template
[Insert Date]
[Insert Date]
Request for Formulary Tier Exception for Patient Prescribed [Insert Product Name] for Relapsing Multiple Sclerosis (RMS)
RE: [Patient Name], [Patient Insurance ID Number], [Patient Date of Birth]
Dear [Health Plan Contact Name]:
I am writing to request a formulary tier exception for my patient. The standard [copay/coinsurance] associated with the assigned tier for [Insert Product Name] would present a significant financial burden to my patient. Based on my [XX] years of treating this patient and my experience in treating MS, the most appropriate medication for my patient at this time is [Insert Product Name]. However, the current [copay/coinsurance] prevents my patient from receiving this medication. I am requesting that [Insert Product Name] be made available to my patient for the same out-of-pocket cost as a preferred medication.
In the past, [Patient Name] has attempted other treatments for RMS.
Medication Strength Dates of therapy Reason for failure/discontinuation
Additionally, I have included documentation regarding my patient that supports my decision. I ask that you review the information I have indicated below when reviewing my request
☐ Relevant medication history ☐ Anti-JCV antibody status ☐ MRI data ☐ Patient’s history of relapses ☐ EDSS history
In the case that this request is denied, I am also at this time requesting a peer-to-peer discussion with a plan Medical Director. Please feel free to contact me if you require further information regarding this request. I look forward to your response as soon as possible. Sincerely, [Name]

© 2017 Biogen. All rights reserved. 11/17 FCH-US-3125