binasal visual field defects are not specific to vigabatrin
TRANSCRIPT

Epilepsy & Behavior 16 (2009) 521–526
Contents lists available at ScienceDirect
Epilepsy & Behavior
journal homepage: www.elsevier .com/locate /yebeh
Binasal visual field defects are not specific to vigabatrin
Pedro Gonzalez a, Graeme J. Sills b, Stuart Parks a,*, Kevin Kelly b, Linda J. Stephen b, David Keating a,Gordon N. Dutton a, Martin J. Brodie b
a Tennent Institute of Ophthalmology, Gartnavel General Hospital, Glasgow, Scotland, UKb Epilepsy Unit, University Division of Cardiovascular & Medical Sciences, Western Infirmary, Glasgow, Scotland, UK
a r t i c l e i n f o a b s t r a c t
Article history:Received 13 May 2009Revised 3 September 2009Accepted 6 September 2009Available online 7 October 2009
Keywords:VigabatrinMultifocal electroretinogramVisual field defects
1525-5050/$ - see front matter � 2009 Elsevier Inc. Adoi:10.1016/j.yebeh.2009.09.003
* Corresponding author. Address: Electrodiagnostictute of Ophthalmology, Gartnavel General Hospital,UK. Fax: +44 141 211 6746.
E-mail address: [email protected] (S. Pa
This study investigated the visual defects associated with the antiepileptic drug vigabatrin (VGB). Twohundred four people with epilepsy were grouped on the basis of antiepileptic drug therapy (current,previous, or no exposure to VGB). Groups were matched with respect to age, gender, and seizure fre-quency. All patients underwent objective assessment of electrophysiological function (wide-field multi-focal electroretinography) and conventional visual field testing (static perimetry). Bilateral visual fieldconstriction was observed in 59% of patients currently taking VGB, 43% of patients who previously tookVGB, and 24% of patients with no exposure to VGB. Assessment of retinal function revealed abnormalresponses in 48% of current VGB users and 22% of prior VGB users, but in none of the patients withoutprevious exposure to VGB. Bilateral visual field abnormalities are common in the treated epilepsy popu-lation, irrespective of drug history. Assessment by conventional static perimetry may neither be suffi-ciently sensitive nor specific to reliably identify retinal toxicity associated with VGB.
� 2009 Elsevier Inc. All rights reserved.
1. Introduction
Vigabatrin (VGB) was the first in a series of new antiepilepticagents that arose from a period of unprecedented drug develop-ment in the 1980s and 1990s [1]. It was launched in the UnitedKingdom and Ireland in 1989 and exerts its effects by irreversibleinhibition of the transaminase enzyme responsible for inactivationof the inhibitory neurotransmitter c-aminobutyric acid (GABA) [2].VGB is an effective adjunctive treatment for complex partial sei-zures with or without secondary generalization in adults [3] andmay be the monotherapy of choice in some children with infantilespasms [4–6]. The drug is now licensed in more than 60 countries.Recently, VGB received ‘‘fast track” designation from the U.S. Foodand Drug Administration for the treatment of cocaine and meth-amphetamine dependence.
The initial barrier to marketing approval for epilepsy in the Uni-ted States was the observation of white matter vacuolization fol-lowing chronic VGB administration in experimental animals [7].This pathology has never been reproduced in humans [8]. How-ever, these concerns were compounded in 1997 with initial reportsof bilateral visual field constriction in VGB-treated patients withepilepsy [9]. Subsequent evidence suggested that this may be an is-sue for up to 40% of exposed individuals [10]. Despite the dearth of
ll rights reserved.
Imaging Unit, Tennent Insti-Glasgow G12 0YN, Scotland,
rks).
prospective matched studies or consideration of the inherentvariability in visual field assessment, a binasal field defect isconsidered the key feature of VGB retinal toxicity [11].
We previously proposed, in a pilot study, that there may be sep-arate pathological and physiological effects of VGB on the visualsystem [12,13]. The current study presents data from 204 patientswith epilepsy. It was designed to address three fundamental ques-tions still unresolved in the identification and monitoring of VGBretinal toxicity. Are the binasal visual field defects specific toVGB or are they present in other treated patient groups? Is thetoxic retinal effect previously identified specific to VGB? Lastly,how do these defects impact quality of life? These questions haveimplications for the recent licensing of VGB in the United Statesand for its continued safe monitoring in the rest of the world.
2. Methods
2.1. Subjects
This study was approved by the Regional Ethics Committee andall subjects provided written informed consent. A total of 283 adultpatients with focal-onset epilepsy with or without secondary gen-eralization were invited to participate. Each had been treated con-tinuously with a stable regimen of one or more antiepileptic drugs(AEDs) for a minimum of 1 year prior to study entry. Individualswith evidence of photosensitive epilepsy, visual pathology on brainneuroimaging, or a history of retinal pathology were excluded.

522 P. Gonzalez et al. / Epilepsy & Behavior 16 (2009) 521–526
2.2. Study groups
Participants were grouped on the basis of their AED exposure(Table 1) and matched with respect to age, gender, duration of epi-lepsy, and seizure control. Group 1 included patients who had beenreceiving VGB treatment for at least 1 year at the time of study entry.Group 2 included patients who had previously been exposed to VGBfor at least 1 year, but who had not taken VGB for at least 2 years.Group 3 included patients who had never received VGB but werereceiving treatment with other GABAergic AEDs at the time of studyentry. Group 4 included patients who had never been exposed to anyAED with known or presumed GABAergic properties. Total VGB drugload for all subjects in Groups 1 and 2 was estimated by retrospectivereview of clinical case notes with consideration of daily VGB doses,dosage adjustments, and treatment duration.
2.3. Ophthalmological investigations
All patients underwent a full ophthalmological assessment atstudy entry, including logMAR crowded visual acuity test, pupilexamination, slit-lamp examination including intraocular pressuremeasurement, dilated fundal examination, and digital fundus pho-tography. Visual fields were assessed using a Humphrey 120-pointsuprathreshold, three-zone static perimetry test, which was re-ported blind by two experienced ophthalmologists. A cluster offour or more relative or absolute defects was described as anabnormal visual field. All reported abnormalities were bilateral un-less otherwise stated.
2.4. Electroretinography
Both conventional electroretinograms (ERGs) and wide-fieldmultifocal ERGs (WF-mfERGs) were obtained for all participants,the former in accordance to the International Society for ClinicalElectrophysiology of Vision (ISCEV) standards. The five main ERG(rod, maximal, oscillatory potential, cone and flicker) and WF-mfERG responses were assessed with respect to the amplitude andlatency (implicit time) of individual response elements. As discussedin our previous study [13], a delay longer than 2 ms between centraland peripheral WF-mfERG responses was considered abnormal andreflected retinal toxicity. Again, all reported abnormalities werebilateral unless otherwise stated.
2.5. Quality of life
All participants were invited to complete two health-relatedquality-of-life questionnaires prior to initial ophthalmological
Table 1Treatment group definitions and demographics.a
Group name Group 1 (n = 56)Current VGB
Group 2 (n = 49)Previous VGB
Treatment details Ongoing VGB treatmentfor a minimum of 1 year
Previous VGB treatment for at lea1 year; no VGB exposure in past2 years
Current AEDs Any AED or combinationthereof including VGB
Any AED or combination thereofexcluding VGB
Age, years(mean ± SD)
39.9 ± 13.0 43.9 ± 14.6
Female gender 51.8% 71.4%Duration of epilepsy,
years (mean ± SD)20.4 (±9.9) 24.4 (±12.2)
Median monthlyseizure frequency[range]
1 [0–90] 2 [0–750]
a CBZ, carbamazepine; CLB, clobazam; GABA, c-aminobutyric acid; GBP, gabapentin;phenytoin; TGB, tiagabine; TPM, topiramate; VGB, vigabatrin; VPA, sodium valproate.
assessment, one to investigate visual health status (VFQ-25) [14]and the other to explore epilepsy-related quality of life (QOLIE-31)[15]. Individuals repeated both questionnaires on a secondoccasion, with awareness of the initial ophthalmological findings.
2.6. Data analysis
All statistical analyses were performed using SAS for WindowsVersion 8.2. The incidence of visual field defects and WF-mfERGabnormalities was expressed in a proportional manner, with studygroups compared using the v2 test. j statistics and corresponding95% confidence intervals were reported for the agreement betweenvisual field defects and WF-mfERG abnormalities. ConventionalERG variables were expressed as medians (+interquartile ranges)and compared with the Mann–Whitney test. Group data derivedfrom the VFQ-25 and QOLIE-31 questionnaires were expressed asmeans ± SD and compared using Student’s two-sample t test. Be-tween-visit changes in quality-of-life data derived from VFQ-25and QOLIE-31 questionnaires were compared with Student’spaired t test. Drug load data were expressed as medians (+mini-mum–maximum ranges) and compared with the Mann–Whitneytest. The relative proportions of patients presenting with visualfield defects and WF-mfERG abnormalities were compared usingMcNemar’s exact test. A Bonferroni correction was applied in allcases of multiple testing, and a P value less than 0.05 was consid-ered statistically significant throughout.
3. Results
Of the 272 patients who agreed to participate, a total of 31failed to attend for initial investigation and another 37 were ex-cluded from the analysis on clinical or procedural grounds. Ofthe remaining 204 patients (79 male; median age 41 years, range12–85), 56 were being prescribed VGB at the time of study entry(Group 1), 49 had been treated with VGB in the past (Group 2),46 had no previous exposure to VGB but were receiving GABAergicAEDs at the time of recruitment (Group 3), and 53 had no priorexposure to any GABAergic drug (Group 4).
There were no significant differences in basic demographic data(age, gender, duration of epilepsy, median monthly seizure fre-quency) between individual study groups (Table 1). There was noevident selection bias on the basis of medical, environmental,and social variables, including family history of epilepsy and/orglaucoma, personal history of other chronic disease (asthma, dia-betes, hypertension, ischemic heart disease), cigarette smoking,alcohol use, and levels of employment (data not shown). Therewere similarly no significant differences among study groups in
Group 3 (n = 46)GABA
Group 4 (n = 53)Non-GABA
st No VGB exposure; ongoing treatmentwith GABAergic AEDs
No VGB exposure; no previousexposure to any GABAergic AED
Any AED regimen including at leastone of PB, VPA, CLB, GBP, TPM, TGB,LEV
One or more of PHT, CBZ, LTG orOXC only
46.7 ± 14.8 43.8 (±16.0)
54.4% 67.9%19.3 (±12.8) 13.3 (±10.0)
0 [0–84] 0 [0–30]
LEV, levetiracetam; LTG, lamotrigine; OXC, oxcarbazepine; PB, phenobarbital; PHT,

P. Gonzalez et al. / Epilepsy & Behavior 16 (2009) 521–526 523
terms of routine ophthalmological examination, visual acuity, orcolor vision (data not shown).
Bilateral visual field constriction, as determined by static perimetry, was observed in all four study groups (Fig. 1), with a prev-alence ranging between 59% in Group 1 patients who were beingtreated with VGB at the time of assessment and 21% in Group 4patients who had never been exposed to any GABAergic AED. Incontrast, WF-mfERG abnormalities were observed only in thosepatients who had been exposed to VGB, with a prevalence of 48%in current VGB users and 22% in past VGB users (Fig. 1). A totalof 21 VGB-exposed patients (current and previous) demonstratedvisual field defects (as determined by static perimetry) with noassociated retinal dysfunction (as determined by WF-mfERG),whereas only 3 VGB-exposed patients had demonstrable retinaldysfunction in the absence of apparent visual field constriction.Typical examples of bilateral visual field defects with the ‘‘nasalwedge” defect commonly associated with VGB toxicity are shownin Fig. 2 in patients who have never been exposed to VGB.
Investigation of conventional ERG variables revealed bilateralreductions in the amplitude of rod, oscillatory potential, cone Awave, cone B wave, and flicker responses in subjects with visualfield defects, compared with those without. These reductions werevariously observed in Groups 1 to 3, but not in Group 4. Only thosereductions in oscillatory potential and cone B amplitudes werecommon to all affected groups, and in all cases statistical signifi-cance was lost when the data were corrected for multiple compar-isons. In contrast, there was a selective association between thebilateral reduction in cone B-wave amplitude and the presence ofWF-mfERG abnormalities, which was exclusive to Group 1 patients(current VGB users) and which was maintained in the face of cor-rection for multiple testing.
An estimate of total VGB drug load was attempted for all partic-ipants in Groups 1 and 2, although only 15 of 49 patients in Group2 (previous VGB exposure) had sufficiently detailed clinical recordsfor a reliable figure to be calculated. There was no clear relation-ship between accumulated ingestion of VGB and the incidence ofvisual field constriction determined by static perimetry. However,patients with abnormal WF-mfERG findings had a significantlyhigher median VGB exposure than those with normal WF-mfERGs(Table 2). An arbitrary threshold of 8000 g VGB was established,which did not correlate with the prevalence of visual field defects(v2 = 2.710, P = 0.100), but above which WF-mfERG abnormalitieswere significantly (v2 = 9.046, P = 0.003) more common.
- visual field constriction
- retinal dysfunction
0
20
40
60
80
Perc
enta
ge o
f par
ticip
ants
Group 1(n=56)
Group 2(n=49)
Group 3(n=45)
Group 4(n=53)
59%
48%46%
22%
30%
0%
21%
0%
- visual field constriction
- retinal dysfunction
0
20
40
Group 1(n=56)
Group 2(n=49)
Group 3(n=45)
Group 4(n=53)
- visual field constriction
- retinal dysfunction
- visual field constriction- visual field constriction
- retinal dysfunction- retinal dysfunction
Group 1(n=56)
Group 2 Group 3 Group 4
59%59%
48%48%46%46%
22%22%
30%30%
0%
21%
0%
Fig. 1. Percentage of participants exhibiting visual field constriction as determinedby Humphrey static perimetry (open bars), and retinal dysfunction as determinedby wide-field multifocal electroretinography (closed bars) in individual patientgroups.
Analysis of quality-of-life questionnaires completed at Visit 1revealed no significant differences in baseline visual health status(VFQ-25) or epilepsy-related quality of life (QOLIE-31) betweenindividual study groups (data not shown). Participants with visualfield constriction identified by static perimetry at Visit 1 (irrespec-tive of study group) reported a significantly lower peripheral visionscore on VFQ-25 than those without visual field defects (P < 0.05;data not shown). They also reported reduced Emotional Well-Being(P < 0.01), Social Functioning (pP < 0.05), and Total QOLIE score(P < 0.05) on QOLIE-31 analysis (data not shown). No such associa-tions were observed when Visit 1 quality-of-life measures werecompared on the basis of initial WF-mfERG findings (Table 3).
Participants completed additional quality-of-life questionnaireswith awareness of the outcome of initial ophthalmological investi-gation. These were analyzed as both group data and individualpaired data on the basis of outcome. Subjects with apparent visualfield constriction (irrespective of study group) reported a signifi-cantly lower mean distance activities score on VFQ-25 (P < 0.05)and a significant reduction in mean Emotional Well-Being on Visit2 QOLIE-31 (P < 0.05) compared with those with normal perimetry(data not shown). There were no associations between quality-of-life measures recorded and retinal dysfunction identified by WF-mfERG (Table 3). When analyzed on an individual patient basis,there were no significant between-visit changes in VFQ-25 or QO-LIE-31 measures that could be attributed to awareness of either vi-sual field constriction or retinal dysfunction.
4. Discussion
The most surprising finding in this study was the presence ofbinasal visual field defects in all patient groups matched for age,duration of epilepsy, and seizure control. The incidence of visualfield defects in patients exposed to VGB was roughly double thatof patients taking other GABAergic drugs and nearly three timesthat of individuals treated with non-GABAergic medications. Thisobservation suggests that a proportion of patients with epilepsyhave binasal visual field defects that cannot be attributed to VGBexposure. In contrast, the WF-mfERG revealed peripheral retinaldysfunction, which was confined to those patients exposed to VGB.
Retinal toxicity was present in twice as many patients currentlytaking VGB as in those who had been exposed previously. This dif-ference would suggest either that a longer critical exposure (postu-lated at 8000-g drug load) is related to a higher incidence or thatthere is some degree of reversal in marginal cases after cessationof VGB treatment [16,17]. The previously exposed group also con-tained more female patients, who may be less likely to develop thiscomplication [11]. As in some other studies, we found little rela-tionship with drug load when comparison was made with visualfield defects alone [17,18]. However, retinal toxicity was relatedto higher drug load in both groups of patients exposed to VGB.
We speculated previously that there could be two effects on thevisual system: the pathological effect on retinal function (toxicity)and the physiological effect of dampening of the visual system dueto the inhibitory nature of AEDs, which may also lead to the devel-opment of visual field defects [13]. If visual field defects are symp-tomatic of a combination of two independent processes, this couldexplain why there is, at best, only a weak relationship with drugload or dose in some studies [18,19], whereas other studies reporta more robust relationship [17,19].
Visual field defects (pathological or physiological) correlatedwith significantly lower quality-of-life measures. This did notchange even after patients were informed of the outcome of theirinvestigations. There was no similar relationship with retinal dys-function. One possible explanation is that these patients have con-comitant neuropsychological or behavioral side effects relating to
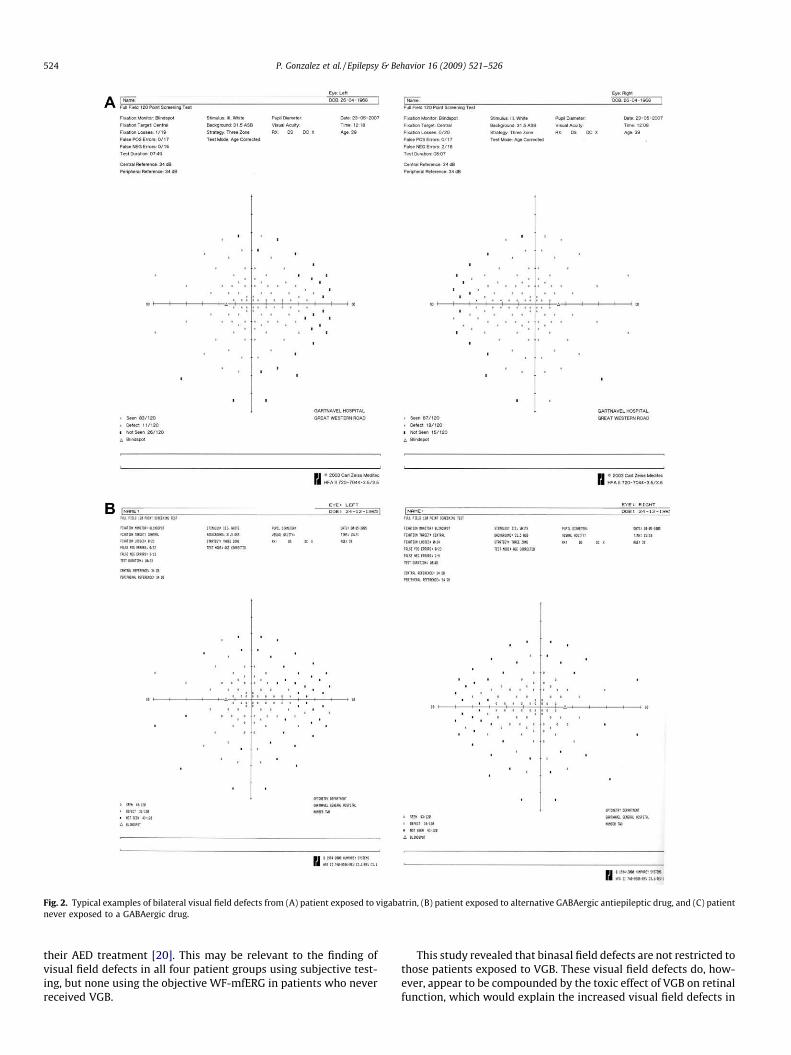
Fig. 2. Typical examples of bilateral visual field defects from (A) patient exposed to vigabatrin, (B) patient exposed to alternative GABAergic antiepileptic drug, and (C) patientnever exposed to a GABAergic drug.
524 P. Gonzalez et al. / Epilepsy & Behavior 16 (2009) 521–526
their AED treatment [20]. This may be relevant to the finding ofvisual field defects in all four patient groups using subjective test-ing, but none using the objective WF-mfERG in patients who neverreceived VGB.
This study revealed that binasal field defects are not restricted tothose patients exposed to VGB. These visual field defects do, how-ever, appear to be compounded by the toxic effect of VGB on retinalfunction, which would explain the increased visual field defects in

Fig. 2 (continued)
Table 2Comparison of total vigabatrin drug load in patients with normal/abnormal visual fields and normal/abnormal wide-field multifocal electroretinography (WF-mfERG).
Visual field defects WF-mfERG abnormalities
Yes No P value Yes No P value
Group 1 8,910g[33; 180–21,056]
5,120g[19; 1,500–16,875]
0.069 9,416g[27; 893–21,056]
5,201g[29; 180–16,875]
0.008
Group 2 6,527g[8; 512–9,100]
4,745g[7; 3,000–8,612]
0.722 7,690g[4; 512–9,100]
4,745g[11; 3,000–8,612]
0.410
Groups 1 and 2 8,225g[41; 180–21,056]
4,878g[26; 1,500–16,875]
0.051 9,012g[31; 512–21,056]
5,065[40; 180–16,875]
0.004
Note. Results are expressed as median [n; +minimum–maximum range] drug load in grams, with statistical comparison of normal/abnormal data by Mann–Whitney test.
Table 3Investigation of epilepsy-related quality of life (QOLIE-31) findings on the basis of retinal dysfunction identified by wide-field multifocal electroretinography (WF-mfERG).
QOLIE-31 at Visit 1 QOLIE-31 at Visit 2
Normal WF-mfERG(n = 157)
Abnormal WF-mfERG(n = 32)
P value Normal WF-mfERG(n = 75)
Abnormal WF-mfERG(n = 14)
P value
Seizure worry 55.6 ± 28.6 60.1 ± 23.1 0.335 57.8 ± 30.1 63.7 ± 30.6 0.515Overall QOL 64.1 ± 18.2 62.3 ± 17.2 0.589 62.6 ± 19.6 60.5 ± 20.8 0.741Emotional well-being 65.3 ± 18.8 61.4 ± 19.3 0.291 65.0 ± 20.2 61.7 ± 28.5 0.684Energy/fatigue 51.2 ± 11.9 53.4 ± 11.6 0.342 51.3 ± 12.4 52.6 ± 14.0 0.747Cognitive functioning 58.0 ± 24.8 55.1 ± 25.6 0.562 60.7 ± 28.5 52.8 ± 29.9 0.372Medication effects 64.6 ± 24.7 66.8 ± 21.7 0.619 65.2 ± 26.2 68.1 ± 24.4 0.375Social functioning 65.1 ± 23.9 59.9 ± 20.6 0.216 67.6 ± 26.2 63.0 ± 24.7 0.535Total QOLIE score 60.7 ± 17.4 58.6 ± 16.4 0.513 61.7 ± 19.8 58.7 ± 19.5 0.603
Note. Results are expressed as means ± SD for individual components of the questionnaire, with statistical comparison of patients with normal versus abnormal WF-mfERGsby two-sample t test. Reported P values have not been corrected for multiple comparisons.
P. Gonzalez et al. / Epilepsy & Behavior 16 (2009) 521–526 525
those patients exposed to VGB. To some extent, it is comforting thatvisual field defects appear to be overreported by the inclusion of falsepositives, but it would be prudent to include an appropriate objec-tive measure of retinal function in the assessment of this importantadverse drug effect as objective measures of retinal functionindicated that toxicity was restricted to those exposed to VGB. Thus,
patients with current or previous exposure to VGB should be consid-ered for assessment with a WF-mfERG, which is more likely to reli-ably identify retinal dysfunction and, by implication, toxicity. Thisshould be an essential requirement for patients receiving VGB forepilepsy and also for other indications, such as the treatment of co-caine and methamphetamine abuse [21].

526 P. Gonzalez et al. / Epilepsy & Behavior 16 (2009) 521–526
Contributors
All statistical analysis was conducted by the Robertson Centrefor Biostatistics, Glasgow University, Scotland.
Acknowledgments
The authors thank Heather Murray at the Robertson Centre forBiostatistics, University of Glasgow, for her contribution to the dataanalysis. This study was supported by a project grant award (CZB/4/78) from the Chief Scientist Office, Scotland.
References
[1] Dichter MA, Brodie MJ. New antiepileptic drugs. N Engl J Med 1996;334:1583–90.[2] Jung MJ, Lippert B, Metcalf BW, Böhlen P, Schechter PJ. C-Vinyl GABA (4-
amino-hex-5-enoic acid), a new selective irreversible inhibitor of GABA-T:effects on brain GABA metabolism in mice. J Neurochem 1977;29:797–802.
[3] Marson AG, Kadir ZA, Hutton JL, Chadwick DW. The new antiepileptic drugs: asystematic review of their efficacy and tolerability. Epilepsia 1997;38:859–80.
[4] Chiron C, Dumas C, Jambaque I, Mumford J, Dulac O. Randomized trialcomparing vigabatrin and hydrocortisone in infantile spasms due to tuberoussclerosis. Epilepsy Res 1997;26:389–95.
[5] Appleton RE, Peters AC, Mumford JP, Shaw DE. Randomised, placebo-controlledstudy of vigabatrin as first-line treatment of infantile spasms. Epilepsia1999;40:1627–33.
[6] Elterman RD, Shields WD, Mansfield KA, Nakagawa J, and the U.S. InfantileSpasms Vigabatrin Study Group. Randomized trial of vigabatrin in patientswith infantile spasms. Neurology 2001;57:1416–21.
[7] Gibson JP, Yarrington JT, Loudy DE, Gerbig CG, Hurst GH, Newberne JW.Chronic toxicity studies with vigabatrin, a GABA-transaminase inhibitor.Toxicol Pathol 1990;18:225–38.
[8] Cohen JA, Fisher RS, Brigell MG, Peyster RG, Sze G. The potential forvigabatrin-induced intramyelinic edema in humans. Epilepsia2000;41:148–57.
[9] Eke T, Talbot JF, Lawden MC. Severe persistent visual field constrictionassociated with vigabatrin. Br Med J 1997;314:180–1.
[10] Kälviäinen R, Nousiainen I, Mäntyjärvi M, et al. Vigabatrin, a gabaergicantiepileptic drug, causes concentric visual field defects. Neurology1999;53:922–6.
[11] Wild JM, Hyo-Sook A, Baulac M, et al. Vigabatrin and epilepsy: lessons learned.Epilepsia 2007;48:1318–27.
[12] McDonagh J, Grierson DJ, Keating D, Parks S. The wide field multifocal ERGreveals a retinal defect caused by vigabatrin toxicity? Br J Ophthalmol2001;85:119–20.
[13] McDonagh J, Stephen LJ, Dolan FM, et al. Peripheral retinal dysfunction inpatients taking vigabatrin. Neurology 2003;61:1690–4.
[14] Mangione CM, Lee PP, Gutierrez PR, Spritzer K, Berry S, Hays RD. Developmentof the 25-item National Eye Institute Visual Function Questionnaire. ArchOphthalmol 2001;119:1050–8.
[15] Cramer JA, Perrine K, Devinsky O, Bryant-Comstock L, Meador K, Hermann B.Development and cross-cultural translations of a 31-item Quality of Life inEpilepsy inventory. Epilepsia 1998;39:81–8.
[16] Krakow K, Polizzi G, Riordan-Eva P, Holder G, Macleod WN, Fish DR. Recoveryof visual field constriction following discontinuation of vigabatrin. Seizure2000;9:287–90.
[17] Johnson MA, Krauss GL, Miller NR, Medura M, Paul SR. Visual function lossfrom vigabatrin: effect of stopping the drug. Neurology 2000;55:40–5.
[18] Kinirons P, Cavalleri GL, O’Rourke DO, et al. Vigabatrin retinopathy in an Irishcohort: lack of correlation with dose. Epilepsia 2006;47:311–7.
[19] Conway M, Cubbidge RP, Hosking SL. Visual field severity indices demonstratedose-dependent visual loss from vigabatrin therapy. Epilepsia 2008;49:108–16.
[20] Loring DW, Marino S, Meador KJ. Neuropsychological and behavioural effectsof antiepileptic drugs. Neuropsychol Rev 2007;17:413–25.
[21] Fechtner RD, Khouri AS, Figueroa E, et al. Short-term treatment of cocaine and/or methamphetamine abuse with vigabatrin. Arch Ophthalmol2006;124:1257–62.