better medicines for children. from concept to reality
TRANSCRIPT

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 136
Better
Medicinesfor Children
FromConcept to
RealityPROGRESS REPORTON THE PAEDIATRICREGULATION 983080EC983081Ndeg19012006
COM 9830802013983081 443FINAL
Health and
Consumers
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 236
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 336
REPORTFROM THECOMMISSIONTO THE
EUROPEANPARLIAMENTAND THECOUNCIL
Better Medicinesfor ChildrenFrom Concept to Reality
General Report on
experience acquired as a
result of the application
of Regulation (EC)ndeg 19012006 on
medicinal products for
paediatric use
(text with EEA relevance)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 536
5
1IntroductionlsquoBetter Medicines or Childrenrsquo was the
ambitious title o a consultation papero February 2002 in which the European
Commission presented its vision or regu-
latory actions on paediatric medicinal
products1 At that time many o the prod-
ucts used in children were not specifically
studied or authorised in children Instead
doctors ofen used products authorised
or adults sometimes in different dosag-
es with the associated risks o inefficacy
andor adverse reactions
The consultation paper built on a 5-year
discussion process that started in 1997
with a round table meeting at the prem-
ises o the European Medicines Agency
(EMA) and was the blueprint or the sub-
sequent legislative act It outlined many
o the measures that are to be ound in
the Paediatric Regulation (Regulation (EC)
No 19012006 o the European Parlia-
ment and o the Council on medicinal
products or paediatric use2
hereinaferlsquothe Regulationrsquo)
The Regulation was adopted some five
years afer the consultation paper on 12
December 2006 It entered into orce on
26 January 2007 and its main provisions
were applicable rom 26 July 2008 (Ar-
ticle 7) and 26 January 2009 (Article 8)
respectively
Five years on it is time to take stock o
developments and report to the EuropeanParliament and the Council on the experi-
ence acquired as a result o the Regula-
tion in accordance with its Article 50(2)
Are we already seeing the emergence o
lsquobetter medicines or childrenrsquo
This report does not yet provide compre-
hensive answer as it is subject to certain
limitations it should thereore be regard-
ed as an interim report that presents a
first impression o the experience gainedIn view o the development cycles o me-
dicinal products it will take at least 10
years to gain a ull understanding o the
impact o the legislation This actor has
already been accounted or in the legis-
lation which requires the Commission to
provide a second more comprehensive
report in 2017 which in accordance with
Article 50(3) o the Regulation must in-
clude an analysis o the economic impact
o the rewards and incentives together
with an analysis o the Regulationrsquos im-
plications or public health with a view to
proposing any necessary amendments
However at this stage some analyses and
interim conclusions can be made
This document has been prepared in con-
sultation with Member States the EMA
and interested parties The Commission
particularly values the lsquo5-year Report to
the European Commissionrsquo presenting the
views o the EMA and its Paediatric Com-
mittee3 and the responses to the public
consultation the Commission undertook
at the end o 20124
1 httpeceuropaeuhealthfilespharmacosdocs
doc2002ebcd_pediat-rics_enpd
2 OJ L 378 27122006p 1 amended by Regulation
(EC) No 19022006 o theEuropean Parliament and othe Council o 20 December
2006 OJ L 378 27122006p 20
3 5-year report to theEuropean Commission mdashGeneral report on experience
acquired as a result o theapplication o the Paedi-
atric Regulation preparedby the European MedicinesAgency with its Paediatric
Committee httpeceuropa
euhealthfilespaediat-rics2012-09_pediatric_re-
port-annex1-2_enpd
4 httpeceuropaeuhealth
human-usepaediatric-med-icinesdevelopments2013_
paediatric_pc_enhtm
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 636
6
2The Paediatric
RegulationIn 2010 around 21 o Europeans were
children representing more than 100 mil-
lion people Children represent a vulnera-
ble population group with developmental
physiological and psychological differenc-
es rom adults They are not merely lsquosmall
adultsrsquo Age- and development-related
research and the availability o suitable
medicinal products is consequently par-
ticularly important
Studies carried out beore the Regulation
was adopted showed that over 50 o the
medicines used or children had not been
tested or use in this specific age group
What is more only a limited number o
medicinal products had been developed
specifically with children in mind Com-
panies had already developed a range o
products against a number o diseases
prior to the Paediatric Regulation particu-
larly in sectors such as childhood immuni-sation by means o vaccines However the
availability o child-appropriate medicines
was generally unsatisactory Accordingly
the Regulation was seen as a response to
the absence o sufficient numbers o suit-
able authorised medicinal products with
appropriate dosages and pharmaceutical
orms to treat conditions in children in the
European Union (EU)
There are several reasons or the lacko paediatric medicines It would how-
ever be too simplistic to pin the blame
on pharmaceutical companies or not car-
rying out enough research and develop-
ment (RampD) to adapt medicinal products
to the needs o the paediatric popula-
tion This reluctance has long mirrored a
general social and ethical paradigm that
children should be protected rom clinical
research Only in the last two decades has
there been a shif to the current consen-sus o better protecting children through
clinical research
Economic actors certainly rendered pae-
diatric RampD less attractive in terms o
achieving an adequate return on invest-
ment Children are not a homogenous
sub-group mdash subpopulations range rom
neonates to teenagers with different bio-
logical and pharmacological characteris-
tics Age-appropriate research makes the
process more expensive and complex or
organisations that are active in this sec-
tor
However the absence o specifically
tested products ofen lef healthcare
proessionals with no alternative but to
use products lsquooff-labelrsquo with the associ-
ated non-negligible risks o inefficacy or
adverse reactions Such a situation was
contrary to the general goal to providehigh-quality medicinal products to the en-
tire EU population
To address this problem the Regula-
tion establishes a system o obligations
rewards and incentives together with
horizontal measures to ensure that medi-
cines are regularly researched developed
and authorised to meet the therapeutic
needs o children Other than the Orphan
Regulation5
which is limited to providingvarious incentives the Paediatric Regula-
tion has a direct impact on companiesrsquo
RampD expenditure While not questioning
that medicinal development is company
driven it compels companies to consider
the potential paediatric use o medicinal
products they develop
5 Regulation (EC)Ndeg 1412000 o the Euro-
pean Parliament and theCouncil o 16 December
1999 on orphan medicinalproducts OJ L 18 2212000p 1
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 736
7
The key objectives of theRegulation are
bull to ensure high-quality research into
the development o medicines or
children
bull to ensure over time that the major-ity o medicines used by children are
specifically authorised or such use
with appropriate orms and ormula-
tions
bull to ensure the availability of high-
quality inormation about medicines
used by children
The key measures included inthe Regulation are
bull setting up an expert committee with-
in the EMA the Paediatric Commit-
tee
bull requiring companies to submit dataon the use o a medicine in children
in accordance with an agreed paedi-
atric investigation plan when apply-
ing or marketing authorisation or
medicines and line-extensions or
existing patent-protected medicines
bull a system of waivers from the re-
quirement or medicines unlikely to
benefit children and a system o de-
errals in relation to the timing o the
requirement to ensure that medi-
cines are tested in children only whenit is sae to do so and to prevent the
requirements delaying the authorisa-
tion o medicines or adults
bull a reward for complying with the re-
quirement in the orm o a six-month
extension to the Supplementary Pro-
tection Certificate
bull a reward in respect of orphan medi-
cines or compliance in the orm o
an extra two years o market exclu-
sivity added to the existing ten yearsawarded under the EUrsquos Orphan Reg-
ulation
bull a new type of marketing authorisa-
tion the Paediatric Use Marketing
Authorisation (PUMA) to attract newpaediatric indications or off-patent
products
bull measures to maximise the impact of
existing studies on medicines or chil-
dren
bull an EU inventory of the therapeuticneeds o children to ocus the re-
search development and authorisa-
tion o medicines
bull an EU network of investigators and
trial centres to carry out the required
RampD
bull a system of free scientic advice for
the industry provided by the EMA
bull a public database of paediatric stud-
ies
bull a provision on EU funding for re-search to stimulate the development
and authorisation o off-patent med-
icines or children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 836
8
The Regulation gives the EMA and its
Paediatric Committee primary responsi-
bility or handling paediatric investigation
plans deerrals and waivers This provides
the Agency with concrete decision-mak-
ing powers
The operational costs o the PaediatricRegulation are partly covered by a contri-
bution rom the EU budget (see Table 8)
as its main activities do not attract any
ees For the period 2007-12 the EU
budget contribution amounted to more
than EUR 39 million In addition Member
Statesrsquo national competent authorities
contribute resources in kind especially
staff time or the assessment o paediat-
ric investigation plans (see Table 12)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 936
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1036
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1136
11
cantly (see Table 5) despite the act that
issues o pharmaceutical non-clinical and
clinical development are also part o the
discussions o a paediatric investigation
plan To acilitate collaboration with the
Paediatric Committee joint procedures
have been created within the EMA
413 Clinical trials with children
Medicines or use in children need to be
tested with appropriate ormulations in
the paediatric population to ensure their
sae and effective use Hence it is gener-
ally accepted that the Paediatric Regula-
tion will lead to more clinical trials in chil-
dren The figures in the EudraCT database
have not yet shown an increase in paedi-
atric trials The number remained stablebetween 2006 and 2012 averaging 350
trials per year with some fluctuations (see
Table 6) It should be pointed out how-
ever that while the number o paediat-
ric trials remained stable the number o
clinical trials in all populations decreased
between 2007 and 2011
Moreover until recently EudraCT was lim-
ited to paediatric trials commencing in the
EU Data on paediatric trials that are parto a paediatric investigation plan and con-
ducted outside the EU have only become
publicly available since spring 2011
It should also be noted that the initiation
o a considerable percentage o clinical
trials included in a paediatric investiga-
tion plan has been deerred in order to
avoid delays in the authorisation o the
corresponding product or adults Hence
the impact o the Paediatric Regulation on
paediatric trials will become more appar-
ent in EudraCT in the years to come There
has however been an evident increase in
the number o paediatric study partici-
pants in particular or the age group rom
0 to 23 months who were normally not
included in trials prior to 2008 (see Ta-
ble 7) Allowing neonates and inants to
benefit rom research is a positive sign
as these have been the most neglected
groups so ar
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1236
12
414 Optimised framework and
coordination
The Paediatric Regulation osters a com-
prehensive network o expertise in paedi-
atric matters within the EU In this context
the role o the Paediatric Committee ispivotal as it brings together a high level
o expertise and competence
The Committee has contributed to the
scientific guidelines published by the EMA
and has so ar convened 22 expert work-
shops on the development o medicines
or children
In addition the European Network or
Paediatric Research at the EMA (Enpr-
EMA) was established in 2009 While aclosely-knit network o experts existed
prior to the introduction o the Regula-
tion in disease areas such as paediatric
oncology Enpr-EMA provides the added
value o a holistic approach by bringing
together national and European networks
investigators and centres with specific ex-
pertise in designing and conducting high-
quality studies in children
However question still remain as towhether this expertise translates into su-
ficient capacity within the EU to conduct
trials in specialised investigation settings
Well-developed research networks capa-
ble o acilitating the necessary research
to ulfil the commitments included in
paediatric investigation plans do exist in
some but not all Member States
415 International cooperation
On an international level the EMA has de-veloped international links with medicines
agencies in the United States Canada
and Japan O particular interest is the
cooperation with the US Food and Drug
Administration given that already in the
late 1990s the United States introduced
legislation that stimulated the develop-
ment o medicinal products or paediatric
use by means o a combination o incen-
tives and obligations This cooperation is
also o great interest to stakeholders as
it may give companies the possibility o
satisying the legislation in both regions
with the same studies
In addition the EMA participates actively
in the Paediatric medicines regulatory
network16 which was created in 2010 as
part o the WHOrsquos Better Medicines or
Children initiative
42 More medicines available
for children
Over 12 years (rom 1995 to 2006) 108
o all 317 indications o 262 centrally au-
thorised medicines included the paediat-
ric population Since the Paediatric Regu-
lation entered into orce 31 out o 152
new medicines have been authorised or
paediatric use 10 o which met the con-
ditions o Article 7 This is not more than
a lsquosnapshotrsquo o the effects o the Regula-
tion as this figure is likely to increase inthe uture as a considerable number o
the new already authorised medicines
are subject to an investigation plan where
completion was deerred to avoid delays
in the authorisation o the adult product
It ollows that in the years to come many
more o those 152 new medicines are ex-
pected to be authorised or paediatric use
Annual reports on deerred paediatric
studies o authorised medicines indicate
that the majority o paediatric investiga-tion plans are running to schedule Pae-
diatric research is on-going at the same
rate across therapeutic areas such as on-
cology vaccines and immunology-rheu-
matology-transplantation
Furthermore by the end o 2011 72 new
paediatric indications had been approved
or medicines already authorised includ-
ing 30 indications (18 centralised) arising
rom the obligation in Article 8 Moreover26 new pharmaceutical orms were au-
thorised or paediatric use including 18
adapted orms or centrally authorised
medicines
As ar as Paediatric Use Marketing Au-
thorisation is concerned to date only one
authorisation has been granted This alls
short o initial expectations
16 httpwwwwhointchild-medicinespaediatric_regula-
torsen
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1336
13
A detailed inventory o centrally autho-
rised products is provided in Annex II
Rewards and incentives
Companies that have complied with the
obligations o the Regulation may benefit
rom a reward once the product concerned
is authorised or the product inormation isamended The reward takes the orm o a
6-month extension o the supplementary
protection certificate (SPC) provided or
by Regulation (EC) No 469200917 or in
the case o an orphan medicinal product
by an extension o the ten-year period o
orphan market exclusivity to twelve years
No orphan rewards have been awarded
yet In this regard it is observed that some
companies withdrew the orphan designa-tion o a product in order to qualiy or
the SPC reward rather than the orphan
reward which seems to be more attrac-
tive rom an economic perspective As ar
as SPC extensions are concerned national
patent offices in 16 Member States had
by the end o 2011 granted 6-month ex-
tensions to 11 medicinal products which
resulted in a total o more than 100 na-
tional SPCs
It should be pointed out that a ruling othe European Court o Justice urther
increased the value o the paediatric
reward as it made clear that the initial
certificate could have a negative or zero
duration which could then become posi-
tive once the paediatric extension was
granted18
43 Increased information on
medicines used in childrenTo provide better inormation on the use
o medicinal products in children Article
45 o the Paediatric Regulation requires
companies holding data on the saety
or efficacy o authorised products in the
paediatric population to submit these
studies to the competent authorities In
this way the data can be assessed and
where appropriate the authorised prod-
uct inormation amended Article 46 o
the Regulation also requires companies tosubmit newly generated paediatric data
Since 2008 more than 18 000 study re-
ports on roughly 2 200 medicinal prod-
ucts have been submitted revealing the
large amount o existing paediatric inor-
mation available at company level
These study reports have been and
continue to be assessed by the compe-
tent authorities thanks to an impressive
work-sharing project (see Tables 10 and11) For nationally authorised products
this has led to the publication o assess-
ment reports covering more than 140
active substances and in a considerable
number o cases to recommendations
or changes to the summaries o product
characteristics o authorised products re-
sulting in 65 actual changes For centrally
authorised products by 2011 the Agency
had completed the assessment o all the
data submitted under Article 45 covering55 active substances in 61 centrally ap-
17 Regulation (EC) No4692009 o the Euro-
pean Parliament and othe Council o 6 May 2009
concerning the supplemen-tary protection certificateor medicinal products OJ
L 152 1662009 p 1 ThisRegulation is a codificationo Council Regulation (EEC)
No 176892
18 Case C-12510 Merck
Sharp amp Dohme v DeutschesPatent- und Markenamt notyet published in the ECR
paragraph 37 lsquoi the SPCapplication had to be reused
because the calculationprovided or in Article 13(1)o Regulation No 176892
results in a negative or zero
duration the holder o thebasic patent could not obtain
an extension o protectionconerred by such a patenteven i it conducted all the
studies according to the ap-proved paediatric investiga-
tion plan under Article 36 oRegulation No 19012006Such a reusal would be
liable to adversely impacton the useul effect oRegulation No 19012006
and might jeopardise the
objectives o that regulationnamely the compensation
o effort made to evaluatethe paediatric effects o themedicinal product at issuersquo
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1436
14
proved medicinal products The summa-
ries o product characteristics o 12 me-
dicinal products were changed ollowing
the assessment
5Lessonslearnt51 Better access to
treatment
One o the explicit goals o the Paediatric
Regulation is to increase the number oproducts that are researched developed
and authorised or use in children and
to reduce the off-label use o medicinal
products in the paediatric population
The main tool to achieve this result is to
oblige companies to establish a paediat-
ric investigation plan or each newly de-
veloped product or or the line extension
o an already authorised product that is
still under patent protection The plan ismeant to ensure mdash under the supervi-
sion o the Paediatric Committee mdash that
the necessary data are generated so as
to determine the conditions under which
a medicinal product may be authorised
to treat children Since 2008 more than
600 paediatric investigation plans have
been approved However only a minor-
ity o them has been completed to date
the vast majority are still on-going This
is due to the long development cycles omedicinal products ofen lasting more
than a decade and the near-systematic
deerral o paediatric studies The high
number o deerrals may not have been
initially expected but are currently a real-
ity as or most o the medicinal products
that have been authorised so ar the RampD
programme started beore the entering
into orce o the Regulation Consequent-
ly the paediatric requirements could not
be taken into account rom the beginningo the product development
While the Paediatric Regulation has led
to some new authorisations that include
paediatric indications the regulatory in-
strument is recent and it will probably
take at least a decade beore it can be
judged in terms o its output In terms o
pharmaceutical orms there is however
already a visible positive impact
In this context criticism has been voiced
that the Regulation will ail to ensure abreakthrough in areas o particular pae-
diatric need such as paediatric oncology
This argument is related to the act that
the starting point or the majority o pae-
diatric investigation plans is an ongoing
RampD programme or a medicinal product
or adults An intrinsic consequence o this
approach is that these products primarily
target adult conditions They are devel-
oped in areas where there is a need (or a
market) in the adult population This needin the older population does not neces-
sarily correspond to the paediatric popu-
lationrsquos need
Moreover the Regulation grants waivers
rom its obligations where the disease or
condition or which the specific medicinal
product is intended occurs only in adult
populations This legislative approach cre-
ates riction in the case o diseases that
are specific and exclusive to children Italso limits the powers and possibilities o
the Paediatric Committee when reviewing
and agreeing to a paediatric investigation
plan as regards the scope o studies that
the Committee may request rom appli-
cants ollowing the objective and scien-
tific-based assessment o the compound
concerned19
These constraints and boundaries have to
be taken into account when judging the
impact the Regulation is likely to make In
addition the effect o instruments such as
the Orphan Regulation have to be consid-
ered given that or example all paediatric
cancers are rare diseases and all under
the EU policy ramework on rare diseases
All in all the achievements highlighted in
chapter 4 o this report and the number
o products with new paediatric indica-
tions show that there are some encourag-
ing signs afer this first five-year period it
is however too early or comprehensive
answers
19 Case T-5209 Nycomed vEMA not yet published
See the results o the publicconsultation conducted by
the Commission in prepara-tion o this Report
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1536
15
52 The PUMA concept a
disappointment
The Paediatric Regulation introduced a
new type o marketing authorisation mdash
the Paediatric Use Marketing Authorisa-
tion (PUMA) As an incentive to carry out
research into the potential paediatric use
o off-patent medicinal products that have
been authorised or adults this marketing
authorisation offers 8 years o data and
10 years o market exclusivity to any new
off-patent product developed exclusively
or use in the paediatric population Thus
the main goal o the PUMA concept is to
stimulate research in existing products
This scheme has been supported by EU
unding through the EU Framework Pro-
grammes or Research and Technological
Development
However to date only one PUMA has been
granted with a ew more projects cur-
rently in the pipeline
Neither industry nor academic networks
have embraced this opportunity as ully
as the Regulation intended It would seem
that the incentive o data and market ex-
clusivity does not work or these productsor at least that the market opportunities
in this sector are currently considered in-
sufficient to outweigh the inherent eco-
nomic risks o pharmaceutical develop-
ment Researchers are not engaging in
trials with medicines that have been on
the market or years Companies seem to
ear that market exclusivity will not pre-
vent physicians rom continuing to use
competitor products with the same active
ingredient off-label at lower costs or thatsubstitution or cheaper adult orms takes
place at the level o pharmacies Moreo-
ver national pricing and reimbursement
rules in Member States ofen do not al-
low or the additional research needed to
obtain the PUMA to be rewarded in price
negotiations20
Against this background the PUMA con-
cept has ailed so ar to ulfil the initial
expectationsThe EMA will in uture accept paediatric
investigation plans or a PUMA that cover
only certain age groups and not the en-
tire paediatric population This may offset
some o the reservations that currently
hamper better endorsement o the PUMA
concept
53 No impact on adultdevelopment
Studies prior to the adoption o the Regu-
lation have suggested a theoretical risk
that the requirements or research in chil-
dren could lengthen the overall drug de-
velopment process21 The Regulation has
met this risk head-on In order to avoid
any delays in authorising medicines or
other populations it allows or the grant-
ing o deerrals relating to the initiation orcompletion o some or all o the meas-
ures contained in a paediatric investiga-
tion plan
Experience shows that the deerral is a
widely used instrument which suggests
that the risk o delays in the processing o
adult applications is minimal There have
been some transitional problems in cases
where the adult programme was already
established when the Regulation enteredinto orce but these issues seem to have
been resolved
A concern that was raised initially was
that some companies would become
reluctant to develop new indications
pharmaceutical orms and new routes o
administration in small markets and or
products with low sales to avoid being
bound by the paediatric obligation under
Article 8 o the Regulation However thereis no evidence o such effect Moreover
it may also be argued that the incentive
o a potential six-month extension o the
SPC served to counterbalance such an
effect as it may have led companies to
examine more thoroughly the benefits o
a line extension taking into account the
economic value o the paediatric reward
Still industry stakeholders claim that
in rare cases the development or new
medicinal products has been delayedor abandoned in the expectation or as a
consequence o additional costs and re-
quirements associated with paediatric de-
20 See the results o thepublic consultation con-
ducted by the Commission inpreparation o this Report
21 C Commission StaffWorking Document Proposal
or a Regulation o the Euro-pean Parliament and o theCouncil on medicinal prod-
ucts or paediatric use andamending Council Regulation(EEC) No 17692 Directive
200183EC and Regula-tion (EC) No 7262004Extended impact assessment
(COM2004599F)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1636
16
keting authorisation holders are obliged
to ensure that the product inormation
is kept up to date with the current scien-
tific knowledge While preerence should
be given to cooperative approaches the
enorcement tools may need to be used
i companies do not overcome their res-
ervations
On the whole the requirements o Articles
45 and 46 have provided an efficient and
appropriate instrument or collecting and
evaluating existing paediatric studies
55 Clinical trials with
children
It is generally accepted that the Paediatric
Regulation will lead to more clinical trialswith children but that its aims should be
achieved without subjecting children to
unnecessary clinical trials
The youngest paediatric-age subsets
including neonates are particularly sen-
sitive It will be a constant challenge to
balance the therapeutic needs o these
age groups with their specific vulnerability
when considering and deciding on the ap-
propriateness o specific clinical trials or
the specific settings o studies in this age
subset Efforts are thereore continuously
being made to explore alternative means
eg the use o extrapolation modelling
and simulation techniques to reduce the
number o study subjects as much as
possible The Paediatric Committee is ac-
tively contributing to acilitate the devel-
opment and use o such means including
non-conventional trial design
Another challenge is how to avoid dupli-cating trials or different paediatric inves-
tigation plans rom different applicants
Companies embarking on product devel-
opment in similar areas may be required
by the agreed paediatric investigation
plan to conduct studies within similar
settings While collaborative approaches
between companies would be highly de-
sirable and have occurred on rare occa-
sions they ofen conflict with companiesrsquo
understandable reluctance to share datawith competitors in the early stages o
product development and participate in
direct comparisons This situation could
velopment Overall there is however no
evidence that the Regulation has a con-
siderable negative impact on products or
other populations
Rather there are some concerns that the
requirements under the Regulation may
cause delays in the authorisation o prod-ucts with paediatric-only indications as
they bring added complexity to the RampD
and regulatory process or products that
already directly target children The added
value o the submission o a paediatric in-
vestigation plan in these cases will be as-
sessed urther in the 2017 report
54 Reaping the benefits of
existing information
There was widespread speculation prior to
the adoption o the Paediatric Regulation
as to how many studies would be submit-
ted by pharmaceutical companies in ac-
cordance with Articles 45 and 46 The act
that competent authorities received more
than 18 000 studies reveals the consid-
erable amount o paediatric inormation
that existed at company level
Certainly it is true that not all the inor-
mation submitted met modern require-
ments or scientific data and clinical re-
search and that the work-sharing process
o evaluating the inormation is rather
long and resource intensive
Nevertheless compared to the PUMA con-
cept this scheme proved more successul
in terms o output and in recommending
and implementing changes to the sum-
mary o product characteristics o author-
ised products In its public consultationthe Commission called Articles 45 and 46
the lsquohidden gemsrsquo o the Regulation
One drawback that remains however
is reluctance by marketing authorisa-
tion holders to update the summary o
product characteristics on a voluntary
basis This said the Regulation contains
mechanisms to overcome such reluctance
as it empowers competent authorities to
directly update the summary and varythe marketing authorisation accordingly
Moreover in accordance with Article 23
o Directive 200183EC22 and Article 16
o Regulation (EC) No 726200423 mar-
22 Directive 200183EC othe European Parliament and
o the Council o 6 November2001 on the Community
code relating to medicinalproducts or human use OJ L311 28112001 p 67
23 Regulation (EC) No7262004 o the European
Parliament and o the Coun-cil o 31 March 2004 layingdown Community procedures
or the authorisation andsupervision o medicinalproducts or human and
veterinary use and establish-ing a European Medicines
Agency OJ L 136 3042004p 1
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1736
17
lead to competition among companies to
find investigators and study participants
as well as the duplication o trials which
are unnecessary rom a scientific and
ethical point o view
The Paediatric Committee is able to waive
paediatric trial requirements where thespecific medicinal product does not rep-
resent a significant therapeutic benefit
over an existing treatment or paediatric
patients including once the product is au-
thorised (Article 11) However this option
does not provide a way out in the early
stages o product development where
the Committee has to ensure equal treat-
ment and non-discriminatory approaches
The key to avoiding such unnecessary tri-
als is transparency with regard to ongoingand completed trials The situation contin-
ues to be monitored
Finally it is in the interest o the EU that
paediatric trials stemming rom paedi-
atric investigation plans are conducted
within the EU This has less to do with
the standards under which a trial is con-
ducted given that clinical trials carried
out outside the EU have to meet the ethi-
cal and scientific requirements o the EUprovisions on clinical trials24 than with the
act that studies within the EU may pro-
vide patients there with early access to
innovative medicines To date there is in-
sufficient data on the ratio between pae-
diatric trials conducted within and outside
the EU However in view o the upgraded
unctionalities o the EudraCT database it
is expected that more data will be avail-
able in 2017 or the second report
56 Spreading the news mdash
getting new information
to patients and healthcare
professionals
I the Regulation is to be a success it is
not only necessary that data on the use
o a specific product in the paediatric
population are collected but that these
data are then also appropriately commu-
nicated to and used by paediatricians intheir day-to-day work or the benefit o
their patients
In this regard some studies published in
the medical literature suggest a ailure
on the part o practitioners to recognise
the actual amount o off-label prescrib-
ing to children Moreover it is claimed that
the prescribing habits o practitioners are
ofen strongly influenced by personal ex-
perience rather than by evidence-based
inormation or paediatric medicine25
These studies in making generalisations
may not have taken into account the het-
erogeneity o healthcare proessionals
whose receptiveness varies greatly ac-
cording to their work setting and specific
area o specialisation At the same time
such observations may point to a sub-
stantial hurdle in achieving the goal o the
Paediatric Regulation
National competent authorities as well as
organisations or healthcare proessionals
seem particularly qualified to consider ap-
propriate ways o ensuring an adequate
flow o inormation Some Member States
have already established a number o
tools to communicate effectively and e-
ficiently with healthcare proessionals
eg by means o regular meetings web-
based inormation distribution systems ornational ormularies
57 Is the burden greater
than rewards
There can be no doubt that the Paediat-
ric Regulation places a considerable ad-
ditional burden on pharmaceutical com-
panies with its obligations regarding
research on products or use in children
However this approach was adopted be-cause market orces alone proved insu-
ficient to stimulate adequate research
The Regulation requires companies to
submit paediatric investigation plans at
an early stage o product development
However research on some active sub-
stances may be discontinued at later
stages should urther studies ail to show
potential with respect to the saety and
efficacy o the product For every success-
ul authorised medicinal product there aremany that ail to make the finishing line
Hence not all approved paediatric investi-
gation plans will be completed as compa-
24 Directive 200120EC othe European Parliament
and o the Council on theapproximation o the laws
regulations and administra-tive provisions o the Mem-ber States relating to the
implementation o good clini-cal practice in the conducto clinical trials on medicinal
products or human use OJ L121 152001 p 34
25 5-year report to theEuropean Commission (seeootnote 3) page 41
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1836
18
nies may decide to stop the correspond-
ing adult development It is too early still
to obtain reliable statistics that show
the ratio between completed and non-
completed paediatric investigation plans
but in the current context not all approved
plans will eventually result in an approved
medicine with a paediatric indication
In terms o output this entails some un-
necessary effort in compiling and screen-
ing paediatric investigation plans To what
extent this is offset by the benefit o early
submission which ensures that the pae-
diatric development fits smoothly into the
overall product development need ur-
ther monitoring
A urther point o concern is the highnumber o modifications to paediat-
ric investigation plans Figures seem to
suggest that nearly all plans have to
be modified at least once Conceptually
though this does not come as a surprise
in view o the early submission o pae-
diatric investigation plans the length o
adult and paediatric developments and
the substantial deerrals granted An
RampD plan requently has to be adapted
or amended to take account o initial re-sults Recruitment problems or necessary
design changes in the trials may also lead
to modifications While it is acknowledged
that substantial amendments or modifi-
cations to the plan have to be subject to
discussions with the Paediatric Commit-
tee this is less obvious or minor changes
In this context the level o detail required
by the EMA has been repeatedly criticised
In the past five years the EMA and its
Paediatric Committee have made effortsto provide or some flexibility in the plan
so to allow a margin o manoeuvre that
takes account o uncertainties in relation
to certain parameters o a trial
In any case the Commission intends to
review its Communication on the ormat
and content o applications or agree-
ment or modification o a paediatric in-
vestigation plan to take into account the
experience gained including the consider-
able number o modification requests
On a positive note it can be noted that
companies are applying or the rewards
provided by the Regulation primarily the
6-month extension o the Supplementary
Protection Certificate which have been
introduced to offset the additional bur-
den The economic value o the reward
depends on the turnover o the product
concerned In the case o blockbuster
products the amount may be consider-
able while or niche products the effect
is small
An in-depth evaluation o the economic
impact will be included in the 2017 report
in order to draw conclusions on the bal-
ance between burden and rewards and
public health benefits
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1936
19
6Outlook mdash
A fairy-taleending aheadlsquoBetter Medicines or Children mdash From
Concept to Realityrsquo is the title o this re-
port Readers may suggest that based on
the evaluation reerred to above it would
be more appropriate to add a question
mark It is evident that it is too early still
to make a firm statement Despite more
than five years o experience the true im-pact o the Regulation on the health o
children will only become apparent over
time as experience is accumulated in the
longer term
There are encouraging signs though
Paediatric development has become a
more integral part o the overall develop-
ment o medicinal products in the EU A
number o new products with paediatric
indications and age-appropriate pharma-ceutical orms have been authorised and
made available to patients A high num-
ber o agreed paediatric investigation
plans indicates that urther products are
in the pipeline
However it needs to be pointed out that it
would be wrong to expect the Regulation
to be able to solve all problems Instead
it is a major catalyst to improve the situ-
ation o young patients
Finally some weaknesses and deficits
have also become apparent in the last
five years Their impact on the overall
perormance o the Regulation has to be
closely monitored On the basis o the ac-
tions outlined above the Commission in-
tends to fine-tune the current implemen-
tation together with the EMA
Even i better medicines or children are
not yet a reality it should be the ambitiono all stakeholders involved that this piece
o legislation will be or the greater good
o children so that in the 2017 report
the discussion will ocus not on whether a
question mark should be added to the ti-
tle o the report but on whether it should
be an exclamation mark instead
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2036
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2136
21
ANNEXES
Figures and Tables
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2236
22
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2336
23
ANNEX I
Figures and Tables
Table 1Agreed paediatric investigations plans (PIPs) 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Agreed PIPs submitted under Article 7 (without waivers)
Agreed PIPs submitted under Article 8 (without waivers)
Source EMA Paediatric database The numbers on agreed PIPs correspond to EMA decisions
Table 2Agreed paediatric investigations plans (PIPs) compared to ull waivers and modifications 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Submitted modifications of an agreed PIP
Agreed Full waivers
Source EMA Paediatric database The numbers on agreed PIPs and waivers correspond to EMA decisions
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2536
25
Table 5Scientific advice and protocol assistance including ollow-ups (provided by the EMA Scientific Advice Working
Party and the Committee or Human Medicinal Products per year)
259
277321
388 400 433 420
021 32
74 8057
91
0 0 0
68 8067
94
0
100
200
300
400
500
2006 2007 2008 2009 2010 2011 2012
Total number of advice (Scientific Advice and Protocol Assistance)
Sum of paediatric-only and mixed (adult and paediatric development questions)
advice
Paediatric-only or mixed advice that involved a Paediatric Committee member(s) as
expert(s)
Source EMA databases Year o advice letter
Year o start o procedure
Table 6Paediatric clinical trials by year o authorisation
2005 2006 2007 2008 2009 2010 2011 2012
Paediatric trials
(number) 254 316 355 342 404 379 334 332
Paediatric trials
that are part of anagreed PIP 2 1 2 6 16 30 76 76
Proportion of
paediatric trials
that are part of an
agreed PIP among
paediatric trials 1 0 1 2 4 8 23 23
Total number
of trials (adults
and or children) 3 350 3 979 4 749 4 512 4 445 4 026 3 809 3 698
Proportion of
paediatric trials of
all trials 8 8 7 8 9 10 9 9
Source EudraCT Data Warehouse using a predefined query on 6 March 2013 and counting the first authorised trial only in the case o more thanone Member State This partial inormation requires sponsors to use a Clinical Trial Application orm that was only available rom November 2009 or use with version 8 o EudraCT
(available rom 2011)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2636
26
Table 7Number o children to be enrolled in clinical trials
Number
of subjects 2006 2007 2008 2009 2010 2011 2012
Pretermnewborns 0 0 0 207 82 2 281 1 712
Newborns 0 0 5 64 169 1 105 1 172
Infants and
toddlers 330 21 20 59 351 2 788 3 141
Children 2 142 181 200 2 230 2 055 10 325 20 677
Adolescents 368 111 205 1 577 2 861 9 054 13 193
Sum of
above 2 840 313 430 4 137 5 517 25 553 39 895
Reference
number of paediatric
trials 316 355 342 404 379 334 332
Source EudraCT Data Warehouse using a pre-defined query on 6 March 2013 modified by excluding studies or lsquoimmunological medicinal productsrsquo
Table 8EU budget contribution to the Paediatric Regulation and the EMA expenditure
0
1
2
3
4
5
6
7
8
9
10
2006 2007 2008 2009 2010 2011 2012
EU budget contribution (in Million euro)
EMA expenditure for paediatri cs (in Mill ion euro)
EMA expenditure for paediatr ics including support (in Million euro)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2736
27
Table 9Percentage o European Medicines Agencyrsquos human resources working in the paediatric area rom 2006 (inner
circle) to 2012 (outer circle)
733 (2012)
052 (2006)
Table 10Member States acting as rapporteurs or the assessment o studies submitted in accordance with Article 46
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE SE NL FR DK IT BE PL ES NO SK FI IE RO AT HU EL CZ PT LV BG
Study included in worksharing Rapporteur appointed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2836
28
Table 11Member States acting as rapporteur or the assessment o studies submitted in accordance with Article 45
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE NL DK AT FR PL SE ES IE CZ MT IT BE SI EE FI HU NO RO BG EL LV PT IS SK
Wave 1 Wave 2 Wave 3 Wave 4 Wave 5 Wave 6 Wave 7 Wave 8 Wave 9
Wave 10 Wave 11 Wave 12 Wave 13 Wave 14 Wave 15 Wave 16 Wave 17 Wave 18
Table 12Member States acting as rapporteurspeer reviewers in EMArsquos Paediatric Committee procedures (initial PIP
waiver or modification o an agreed PIP)
0
50
100
150
200
250
300
350
400
450
500
A u s t r i a
B el gi um
B ul g a r i a
C y pr u s
C z e c h R e p u b l i c
D enm a r k
E s t oni a
F i nl a n d
F r a n c e
G er m a n y
G r e e c e
H e a l t h c a r e a n d
A c a d emi a
H un g a r y
I c el a n d
I r el a n d
I t a l y
L a t vi a
L i t h u a ni a
L ux em b o ur g
M a l t a
N or w a y
P a t i en t s Or g a ni s a t i on
P ol a n d
P or t u g a l
R om a ni a
S l ov a k i a
S l ov eni a
S p a i n
S w e d en
T h eN e t h er l a n d
s
U ni t e d K i n g d om
Initial PIP applications PIP modifications
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2936
29
ANNEX II
Detailed inventory of centrally authorised medicinalproducts for paediatric use since the entry into force
of the Paediatric Regulation
Table 13Medicinal products authorised centrally since 2007 which include a paediatric indication
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Retapamulin Altargo 2007 No Mixed
Nelarabine Atriance 2007 No Mixed
Human papillomavirus vaccine[types 16 18] Cervarix 2007 No Mixed
Hydroxocobalamin Cyanokit 2007 No Mixed
Idursulase Elaprase 2007 No Mixed
Gadoversetamide Optimark 2007 No Mixed
Betaine anhydrous Cystadane 2007 No Mixed
Stiripentol Diacomit 2007 No Paediatric only
Mecasermin Increlex 2007 No Paediatric only
Rufinamide Inovelon 2007 No Mixed
Hydroxycarbamide Siklos 2007 No Mixed
Human normal
immunoglobulin (ivig) Flebogamma DIF 2007 No Mixed
Fluticasone uroate Avamys 2008 No Mixed
Human normal immunoglobulin Privigen 2008 No Mixed
Lacosamide Vimpat 2008 No Mixed
Micaungin Mycamine 2008 No Mixed
Sapropterin Kuvan 2008 No Mixed
Sugammadex Bridion 2008 No Mixed
Tocoersonal d-alpha
tocopheryl polyethylene glycol
succinate Vedrop 2009 No Paediatric only
Miamurtide Mepact 2009 No Mixed
Rilonacept Rilonacept Regeneron 2009 No Mixed
Tacrolimus Modigra 2009 No Mixed
Pneumoccocal polysaccharideconjugate vaccine (adsorbed) Synflorix 2009 No Paediatric only
Canakinumab
Ilaris (PIP not yet
completed) 2009 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3036
30
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Pneumoccocal polysaccharide
conjugate vaccine (13-valentadsorbed)
Prevenar 13 (PIP not yetcompleted) 2009 Yes Paediatric only
Meningococcal group a c
w135 and y conjugate vaccine Menveo 2010 Yes Mixed
Velaglucerase ala
Vpriv (PIP not yet
completed) 2010 Yes Mixed
Influenza vaccine (live
attenuated nasal) Fluenz (Waiver) 2011 Yes Paediatric only
C1 inhibitor human
Cinryze (PIP not yet
completed) 2011 Yes Mixed
Dihydroartemisinin
piperaquine phosphate
Eurartesim (PIP not yet
completed) 2011 Yes Mixed
Midazolam Buccolam 2011 Yes (PUMA) Paediatric only
EverolimusVotubia(PIP not yet completed) 2011 Yes Mixed
Tobramycin
Tobi Podhaler (PIP not
yet completed) 2011 Yes Mixed
Nomegestrol estradiol Ioa Zoely 2011 Yes Mixed
Colistimethate sodium Colobreathe 2012 Yes Mixed
Mercaptopurine Xaluprine 2012 No Mixed
Catridecacog NovoThirteen 2012 Yes MixedEavirenz Eavirenz Teva 2012 No Mixed
Ivacafor Kalydeco 2012 Yes Mixed
Desloratadine Desloratadine ratiopharm 2012 No Mixed
Desloratadine Desloratadine Actavis 2012 No Mixed
Perampanel Fycompa 2012 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3136
31
Table 14List o centrally authorised medicinal products or which the therapeutic indication was extended to or amend-
ed or the paediatric population
Active substance(s)
Trade
name Date Subject of the extension
Levetiracetam Keppra
2007
2009
Extension o the indication to include adjunctive ther-
apy in the treatment o primary generalised tonic-
clonic (PGTC) seizures in adults and adolescents rom
12 years o age with idiopathic generalised epilepsyExtension o indication to include the adjunctive
treatment o partial seizures with or without second-
ary generalisation in children rom 1 month to lt4
years old
Pneumococcal sac-
charide conjugated
vaccine adsorbed Prevenar 2007
Extension o the indication to include new inorma-
tion on efficacy against disease caused by Strepto-
coccus pneumoniae serotypes 4 6B 9V 14 18C 19F
and 23F in otitis mediaExtension o indication rom active immunisation
against bacteraemic pneumonia to active immunisa-
tion against pneumonia
Infliximab
Remi-
cade 2007
Extension o indication to include treatment o
severe active Crohnrsquos disease in children aged 6 to
17 years
Darbepoetin ala Aranesp 2007
Extension o indication or CRF patients whichrestricted the use o Nespo to paediatric subjects ge
11 years o age
Fosamprenavir Telzir 2007
Extension o indication o Telzir in combination withritonavir or the treatment o Human Immunodefi-
ciency Virus Type 1 (HIV-1) inected adults in combi-nation with other antiretroviral medicinal products to
include paediatric populations
Lamivudine zidovu-
dine Combivir 2007
Extension o indication to include paediatric patients
and replacement o film-coated tablets by scored
film-coated tablets
Desloratadine Aerius 2007Extension o indication rom lsquochronic idiopathic urti-cariarsquo to lsquourticariarsquo
Insulin glulisine Apidra 2007
Extension o indication to include 6 year olds and
older children based on the results o 2 paediatricstudies
Human papilloma virusvaccine [types 6 11
16 18] (recombinantadsorbed) Gardasil 2008
Extension o indication to include the prevention ohigh-grade vaginal dysplastic lesions (VaIN 23)
Adalimumab Humira 20082011
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in adoles-cents rom 13 to 17 years o age
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in the paedi-
atric population aged rom 4 to 12 years
Caspoungin Cancidas 2008
Extension o the indication to include the paediatric
population
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 236
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 336
REPORTFROM THECOMMISSIONTO THE
EUROPEANPARLIAMENTAND THECOUNCIL
Better Medicinesfor ChildrenFrom Concept to Reality
General Report on
experience acquired as a
result of the application
of Regulation (EC)ndeg 19012006 on
medicinal products for
paediatric use
(text with EEA relevance)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 536
5
1IntroductionlsquoBetter Medicines or Childrenrsquo was the
ambitious title o a consultation papero February 2002 in which the European
Commission presented its vision or regu-
latory actions on paediatric medicinal
products1 At that time many o the prod-
ucts used in children were not specifically
studied or authorised in children Instead
doctors ofen used products authorised
or adults sometimes in different dosag-
es with the associated risks o inefficacy
andor adverse reactions
The consultation paper built on a 5-year
discussion process that started in 1997
with a round table meeting at the prem-
ises o the European Medicines Agency
(EMA) and was the blueprint or the sub-
sequent legislative act It outlined many
o the measures that are to be ound in
the Paediatric Regulation (Regulation (EC)
No 19012006 o the European Parlia-
ment and o the Council on medicinal
products or paediatric use2
hereinaferlsquothe Regulationrsquo)
The Regulation was adopted some five
years afer the consultation paper on 12
December 2006 It entered into orce on
26 January 2007 and its main provisions
were applicable rom 26 July 2008 (Ar-
ticle 7) and 26 January 2009 (Article 8)
respectively
Five years on it is time to take stock o
developments and report to the EuropeanParliament and the Council on the experi-
ence acquired as a result o the Regula-
tion in accordance with its Article 50(2)
Are we already seeing the emergence o
lsquobetter medicines or childrenrsquo
This report does not yet provide compre-
hensive answer as it is subject to certain
limitations it should thereore be regard-
ed as an interim report that presents a
first impression o the experience gainedIn view o the development cycles o me-
dicinal products it will take at least 10
years to gain a ull understanding o the
impact o the legislation This actor has
already been accounted or in the legis-
lation which requires the Commission to
provide a second more comprehensive
report in 2017 which in accordance with
Article 50(3) o the Regulation must in-
clude an analysis o the economic impact
o the rewards and incentives together
with an analysis o the Regulationrsquos im-
plications or public health with a view to
proposing any necessary amendments
However at this stage some analyses and
interim conclusions can be made
This document has been prepared in con-
sultation with Member States the EMA
and interested parties The Commission
particularly values the lsquo5-year Report to
the European Commissionrsquo presenting the
views o the EMA and its Paediatric Com-
mittee3 and the responses to the public
consultation the Commission undertook
at the end o 20124
1 httpeceuropaeuhealthfilespharmacosdocs
doc2002ebcd_pediat-rics_enpd
2 OJ L 378 27122006p 1 amended by Regulation
(EC) No 19022006 o theEuropean Parliament and othe Council o 20 December
2006 OJ L 378 27122006p 20
3 5-year report to theEuropean Commission mdashGeneral report on experience
acquired as a result o theapplication o the Paedi-
atric Regulation preparedby the European MedicinesAgency with its Paediatric
Committee httpeceuropa
euhealthfilespaediat-rics2012-09_pediatric_re-
port-annex1-2_enpd
4 httpeceuropaeuhealth
human-usepaediatric-med-icinesdevelopments2013_
paediatric_pc_enhtm
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 636
6
2The Paediatric
RegulationIn 2010 around 21 o Europeans were
children representing more than 100 mil-
lion people Children represent a vulnera-
ble population group with developmental
physiological and psychological differenc-
es rom adults They are not merely lsquosmall
adultsrsquo Age- and development-related
research and the availability o suitable
medicinal products is consequently par-
ticularly important
Studies carried out beore the Regulation
was adopted showed that over 50 o the
medicines used or children had not been
tested or use in this specific age group
What is more only a limited number o
medicinal products had been developed
specifically with children in mind Com-
panies had already developed a range o
products against a number o diseases
prior to the Paediatric Regulation particu-
larly in sectors such as childhood immuni-sation by means o vaccines However the
availability o child-appropriate medicines
was generally unsatisactory Accordingly
the Regulation was seen as a response to
the absence o sufficient numbers o suit-
able authorised medicinal products with
appropriate dosages and pharmaceutical
orms to treat conditions in children in the
European Union (EU)
There are several reasons or the lacko paediatric medicines It would how-
ever be too simplistic to pin the blame
on pharmaceutical companies or not car-
rying out enough research and develop-
ment (RampD) to adapt medicinal products
to the needs o the paediatric popula-
tion This reluctance has long mirrored a
general social and ethical paradigm that
children should be protected rom clinical
research Only in the last two decades has
there been a shif to the current consen-sus o better protecting children through
clinical research
Economic actors certainly rendered pae-
diatric RampD less attractive in terms o
achieving an adequate return on invest-
ment Children are not a homogenous
sub-group mdash subpopulations range rom
neonates to teenagers with different bio-
logical and pharmacological characteris-
tics Age-appropriate research makes the
process more expensive and complex or
organisations that are active in this sec-
tor
However the absence o specifically
tested products ofen lef healthcare
proessionals with no alternative but to
use products lsquooff-labelrsquo with the associ-
ated non-negligible risks o inefficacy or
adverse reactions Such a situation was
contrary to the general goal to providehigh-quality medicinal products to the en-
tire EU population
To address this problem the Regula-
tion establishes a system o obligations
rewards and incentives together with
horizontal measures to ensure that medi-
cines are regularly researched developed
and authorised to meet the therapeutic
needs o children Other than the Orphan
Regulation5
which is limited to providingvarious incentives the Paediatric Regula-
tion has a direct impact on companiesrsquo
RampD expenditure While not questioning
that medicinal development is company
driven it compels companies to consider
the potential paediatric use o medicinal
products they develop
5 Regulation (EC)Ndeg 1412000 o the Euro-
pean Parliament and theCouncil o 16 December
1999 on orphan medicinalproducts OJ L 18 2212000p 1
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 736
7
The key objectives of theRegulation are
bull to ensure high-quality research into
the development o medicines or
children
bull to ensure over time that the major-ity o medicines used by children are
specifically authorised or such use
with appropriate orms and ormula-
tions
bull to ensure the availability of high-
quality inormation about medicines
used by children
The key measures included inthe Regulation are
bull setting up an expert committee with-
in the EMA the Paediatric Commit-
tee
bull requiring companies to submit dataon the use o a medicine in children
in accordance with an agreed paedi-
atric investigation plan when apply-
ing or marketing authorisation or
medicines and line-extensions or
existing patent-protected medicines
bull a system of waivers from the re-
quirement or medicines unlikely to
benefit children and a system o de-
errals in relation to the timing o the
requirement to ensure that medi-
cines are tested in children only whenit is sae to do so and to prevent the
requirements delaying the authorisa-
tion o medicines or adults
bull a reward for complying with the re-
quirement in the orm o a six-month
extension to the Supplementary Pro-
tection Certificate
bull a reward in respect of orphan medi-
cines or compliance in the orm o
an extra two years o market exclu-
sivity added to the existing ten yearsawarded under the EUrsquos Orphan Reg-
ulation
bull a new type of marketing authorisa-
tion the Paediatric Use Marketing
Authorisation (PUMA) to attract newpaediatric indications or off-patent
products
bull measures to maximise the impact of
existing studies on medicines or chil-
dren
bull an EU inventory of the therapeuticneeds o children to ocus the re-
search development and authorisa-
tion o medicines
bull an EU network of investigators and
trial centres to carry out the required
RampD
bull a system of free scientic advice for
the industry provided by the EMA
bull a public database of paediatric stud-
ies
bull a provision on EU funding for re-search to stimulate the development
and authorisation o off-patent med-
icines or children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 836
8
The Regulation gives the EMA and its
Paediatric Committee primary responsi-
bility or handling paediatric investigation
plans deerrals and waivers This provides
the Agency with concrete decision-mak-
ing powers
The operational costs o the PaediatricRegulation are partly covered by a contri-
bution rom the EU budget (see Table 8)
as its main activities do not attract any
ees For the period 2007-12 the EU
budget contribution amounted to more
than EUR 39 million In addition Member
Statesrsquo national competent authorities
contribute resources in kind especially
staff time or the assessment o paediat-
ric investigation plans (see Table 12)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 936
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1036
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1136
11
cantly (see Table 5) despite the act that
issues o pharmaceutical non-clinical and
clinical development are also part o the
discussions o a paediatric investigation
plan To acilitate collaboration with the
Paediatric Committee joint procedures
have been created within the EMA
413 Clinical trials with children
Medicines or use in children need to be
tested with appropriate ormulations in
the paediatric population to ensure their
sae and effective use Hence it is gener-
ally accepted that the Paediatric Regula-
tion will lead to more clinical trials in chil-
dren The figures in the EudraCT database
have not yet shown an increase in paedi-
atric trials The number remained stablebetween 2006 and 2012 averaging 350
trials per year with some fluctuations (see
Table 6) It should be pointed out how-
ever that while the number o paediat-
ric trials remained stable the number o
clinical trials in all populations decreased
between 2007 and 2011
Moreover until recently EudraCT was lim-
ited to paediatric trials commencing in the
EU Data on paediatric trials that are parto a paediatric investigation plan and con-
ducted outside the EU have only become
publicly available since spring 2011
It should also be noted that the initiation
o a considerable percentage o clinical
trials included in a paediatric investiga-
tion plan has been deerred in order to
avoid delays in the authorisation o the
corresponding product or adults Hence
the impact o the Paediatric Regulation on
paediatric trials will become more appar-
ent in EudraCT in the years to come There
has however been an evident increase in
the number o paediatric study partici-
pants in particular or the age group rom
0 to 23 months who were normally not
included in trials prior to 2008 (see Ta-
ble 7) Allowing neonates and inants to
benefit rom research is a positive sign
as these have been the most neglected
groups so ar
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1236
12
414 Optimised framework and
coordination
The Paediatric Regulation osters a com-
prehensive network o expertise in paedi-
atric matters within the EU In this context
the role o the Paediatric Committee ispivotal as it brings together a high level
o expertise and competence
The Committee has contributed to the
scientific guidelines published by the EMA
and has so ar convened 22 expert work-
shops on the development o medicines
or children
In addition the European Network or
Paediatric Research at the EMA (Enpr-
EMA) was established in 2009 While aclosely-knit network o experts existed
prior to the introduction o the Regula-
tion in disease areas such as paediatric
oncology Enpr-EMA provides the added
value o a holistic approach by bringing
together national and European networks
investigators and centres with specific ex-
pertise in designing and conducting high-
quality studies in children
However question still remain as towhether this expertise translates into su-
ficient capacity within the EU to conduct
trials in specialised investigation settings
Well-developed research networks capa-
ble o acilitating the necessary research
to ulfil the commitments included in
paediatric investigation plans do exist in
some but not all Member States
415 International cooperation
On an international level the EMA has de-veloped international links with medicines
agencies in the United States Canada
and Japan O particular interest is the
cooperation with the US Food and Drug
Administration given that already in the
late 1990s the United States introduced
legislation that stimulated the develop-
ment o medicinal products or paediatric
use by means o a combination o incen-
tives and obligations This cooperation is
also o great interest to stakeholders as
it may give companies the possibility o
satisying the legislation in both regions
with the same studies
In addition the EMA participates actively
in the Paediatric medicines regulatory
network16 which was created in 2010 as
part o the WHOrsquos Better Medicines or
Children initiative
42 More medicines available
for children
Over 12 years (rom 1995 to 2006) 108
o all 317 indications o 262 centrally au-
thorised medicines included the paediat-
ric population Since the Paediatric Regu-
lation entered into orce 31 out o 152
new medicines have been authorised or
paediatric use 10 o which met the con-
ditions o Article 7 This is not more than
a lsquosnapshotrsquo o the effects o the Regula-
tion as this figure is likely to increase inthe uture as a considerable number o
the new already authorised medicines
are subject to an investigation plan where
completion was deerred to avoid delays
in the authorisation o the adult product
It ollows that in the years to come many
more o those 152 new medicines are ex-
pected to be authorised or paediatric use
Annual reports on deerred paediatric
studies o authorised medicines indicate
that the majority o paediatric investiga-tion plans are running to schedule Pae-
diatric research is on-going at the same
rate across therapeutic areas such as on-
cology vaccines and immunology-rheu-
matology-transplantation
Furthermore by the end o 2011 72 new
paediatric indications had been approved
or medicines already authorised includ-
ing 30 indications (18 centralised) arising
rom the obligation in Article 8 Moreover26 new pharmaceutical orms were au-
thorised or paediatric use including 18
adapted orms or centrally authorised
medicines
As ar as Paediatric Use Marketing Au-
thorisation is concerned to date only one
authorisation has been granted This alls
short o initial expectations
16 httpwwwwhointchild-medicinespaediatric_regula-
torsen
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1336
13
A detailed inventory o centrally autho-
rised products is provided in Annex II
Rewards and incentives
Companies that have complied with the
obligations o the Regulation may benefit
rom a reward once the product concerned
is authorised or the product inormation isamended The reward takes the orm o a
6-month extension o the supplementary
protection certificate (SPC) provided or
by Regulation (EC) No 469200917 or in
the case o an orphan medicinal product
by an extension o the ten-year period o
orphan market exclusivity to twelve years
No orphan rewards have been awarded
yet In this regard it is observed that some
companies withdrew the orphan designa-tion o a product in order to qualiy or
the SPC reward rather than the orphan
reward which seems to be more attrac-
tive rom an economic perspective As ar
as SPC extensions are concerned national
patent offices in 16 Member States had
by the end o 2011 granted 6-month ex-
tensions to 11 medicinal products which
resulted in a total o more than 100 na-
tional SPCs
It should be pointed out that a ruling othe European Court o Justice urther
increased the value o the paediatric
reward as it made clear that the initial
certificate could have a negative or zero
duration which could then become posi-
tive once the paediatric extension was
granted18
43 Increased information on
medicines used in childrenTo provide better inormation on the use
o medicinal products in children Article
45 o the Paediatric Regulation requires
companies holding data on the saety
or efficacy o authorised products in the
paediatric population to submit these
studies to the competent authorities In
this way the data can be assessed and
where appropriate the authorised prod-
uct inormation amended Article 46 o
the Regulation also requires companies tosubmit newly generated paediatric data
Since 2008 more than 18 000 study re-
ports on roughly 2 200 medicinal prod-
ucts have been submitted revealing the
large amount o existing paediatric inor-
mation available at company level
These study reports have been and
continue to be assessed by the compe-
tent authorities thanks to an impressive
work-sharing project (see Tables 10 and11) For nationally authorised products
this has led to the publication o assess-
ment reports covering more than 140
active substances and in a considerable
number o cases to recommendations
or changes to the summaries o product
characteristics o authorised products re-
sulting in 65 actual changes For centrally
authorised products by 2011 the Agency
had completed the assessment o all the
data submitted under Article 45 covering55 active substances in 61 centrally ap-
17 Regulation (EC) No4692009 o the Euro-
pean Parliament and othe Council o 6 May 2009
concerning the supplemen-tary protection certificateor medicinal products OJ
L 152 1662009 p 1 ThisRegulation is a codificationo Council Regulation (EEC)
No 176892
18 Case C-12510 Merck
Sharp amp Dohme v DeutschesPatent- und Markenamt notyet published in the ECR
paragraph 37 lsquoi the SPCapplication had to be reused
because the calculationprovided or in Article 13(1)o Regulation No 176892
results in a negative or zero
duration the holder o thebasic patent could not obtain
an extension o protectionconerred by such a patenteven i it conducted all the
studies according to the ap-proved paediatric investiga-
tion plan under Article 36 oRegulation No 19012006Such a reusal would be
liable to adversely impacton the useul effect oRegulation No 19012006
and might jeopardise the
objectives o that regulationnamely the compensation
o effort made to evaluatethe paediatric effects o themedicinal product at issuersquo
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1436
14
proved medicinal products The summa-
ries o product characteristics o 12 me-
dicinal products were changed ollowing
the assessment
5Lessonslearnt51 Better access to
treatment
One o the explicit goals o the Paediatric
Regulation is to increase the number oproducts that are researched developed
and authorised or use in children and
to reduce the off-label use o medicinal
products in the paediatric population
The main tool to achieve this result is to
oblige companies to establish a paediat-
ric investigation plan or each newly de-
veloped product or or the line extension
o an already authorised product that is
still under patent protection The plan ismeant to ensure mdash under the supervi-
sion o the Paediatric Committee mdash that
the necessary data are generated so as
to determine the conditions under which
a medicinal product may be authorised
to treat children Since 2008 more than
600 paediatric investigation plans have
been approved However only a minor-
ity o them has been completed to date
the vast majority are still on-going This
is due to the long development cycles omedicinal products ofen lasting more
than a decade and the near-systematic
deerral o paediatric studies The high
number o deerrals may not have been
initially expected but are currently a real-
ity as or most o the medicinal products
that have been authorised so ar the RampD
programme started beore the entering
into orce o the Regulation Consequent-
ly the paediatric requirements could not
be taken into account rom the beginningo the product development
While the Paediatric Regulation has led
to some new authorisations that include
paediatric indications the regulatory in-
strument is recent and it will probably
take at least a decade beore it can be
judged in terms o its output In terms o
pharmaceutical orms there is however
already a visible positive impact
In this context criticism has been voiced
that the Regulation will ail to ensure abreakthrough in areas o particular pae-
diatric need such as paediatric oncology
This argument is related to the act that
the starting point or the majority o pae-
diatric investigation plans is an ongoing
RampD programme or a medicinal product
or adults An intrinsic consequence o this
approach is that these products primarily
target adult conditions They are devel-
oped in areas where there is a need (or a
market) in the adult population This needin the older population does not neces-
sarily correspond to the paediatric popu-
lationrsquos need
Moreover the Regulation grants waivers
rom its obligations where the disease or
condition or which the specific medicinal
product is intended occurs only in adult
populations This legislative approach cre-
ates riction in the case o diseases that
are specific and exclusive to children Italso limits the powers and possibilities o
the Paediatric Committee when reviewing
and agreeing to a paediatric investigation
plan as regards the scope o studies that
the Committee may request rom appli-
cants ollowing the objective and scien-
tific-based assessment o the compound
concerned19
These constraints and boundaries have to
be taken into account when judging the
impact the Regulation is likely to make In
addition the effect o instruments such as
the Orphan Regulation have to be consid-
ered given that or example all paediatric
cancers are rare diseases and all under
the EU policy ramework on rare diseases
All in all the achievements highlighted in
chapter 4 o this report and the number
o products with new paediatric indica-
tions show that there are some encourag-
ing signs afer this first five-year period it
is however too early or comprehensive
answers
19 Case T-5209 Nycomed vEMA not yet published
See the results o the publicconsultation conducted by
the Commission in prepara-tion o this Report
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1536
15
52 The PUMA concept a
disappointment
The Paediatric Regulation introduced a
new type o marketing authorisation mdash
the Paediatric Use Marketing Authorisa-
tion (PUMA) As an incentive to carry out
research into the potential paediatric use
o off-patent medicinal products that have
been authorised or adults this marketing
authorisation offers 8 years o data and
10 years o market exclusivity to any new
off-patent product developed exclusively
or use in the paediatric population Thus
the main goal o the PUMA concept is to
stimulate research in existing products
This scheme has been supported by EU
unding through the EU Framework Pro-
grammes or Research and Technological
Development
However to date only one PUMA has been
granted with a ew more projects cur-
rently in the pipeline
Neither industry nor academic networks
have embraced this opportunity as ully
as the Regulation intended It would seem
that the incentive o data and market ex-
clusivity does not work or these productsor at least that the market opportunities
in this sector are currently considered in-
sufficient to outweigh the inherent eco-
nomic risks o pharmaceutical develop-
ment Researchers are not engaging in
trials with medicines that have been on
the market or years Companies seem to
ear that market exclusivity will not pre-
vent physicians rom continuing to use
competitor products with the same active
ingredient off-label at lower costs or thatsubstitution or cheaper adult orms takes
place at the level o pharmacies Moreo-
ver national pricing and reimbursement
rules in Member States ofen do not al-
low or the additional research needed to
obtain the PUMA to be rewarded in price
negotiations20
Against this background the PUMA con-
cept has ailed so ar to ulfil the initial
expectationsThe EMA will in uture accept paediatric
investigation plans or a PUMA that cover
only certain age groups and not the en-
tire paediatric population This may offset
some o the reservations that currently
hamper better endorsement o the PUMA
concept
53 No impact on adultdevelopment
Studies prior to the adoption o the Regu-
lation have suggested a theoretical risk
that the requirements or research in chil-
dren could lengthen the overall drug de-
velopment process21 The Regulation has
met this risk head-on In order to avoid
any delays in authorising medicines or
other populations it allows or the grant-
ing o deerrals relating to the initiation orcompletion o some or all o the meas-
ures contained in a paediatric investiga-
tion plan
Experience shows that the deerral is a
widely used instrument which suggests
that the risk o delays in the processing o
adult applications is minimal There have
been some transitional problems in cases
where the adult programme was already
established when the Regulation enteredinto orce but these issues seem to have
been resolved
A concern that was raised initially was
that some companies would become
reluctant to develop new indications
pharmaceutical orms and new routes o
administration in small markets and or
products with low sales to avoid being
bound by the paediatric obligation under
Article 8 o the Regulation However thereis no evidence o such effect Moreover
it may also be argued that the incentive
o a potential six-month extension o the
SPC served to counterbalance such an
effect as it may have led companies to
examine more thoroughly the benefits o
a line extension taking into account the
economic value o the paediatric reward
Still industry stakeholders claim that
in rare cases the development or new
medicinal products has been delayedor abandoned in the expectation or as a
consequence o additional costs and re-
quirements associated with paediatric de-
20 See the results o thepublic consultation con-
ducted by the Commission inpreparation o this Report
21 C Commission StaffWorking Document Proposal
or a Regulation o the Euro-pean Parliament and o theCouncil on medicinal prod-
ucts or paediatric use andamending Council Regulation(EEC) No 17692 Directive
200183EC and Regula-tion (EC) No 7262004Extended impact assessment
(COM2004599F)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1636
16
keting authorisation holders are obliged
to ensure that the product inormation
is kept up to date with the current scien-
tific knowledge While preerence should
be given to cooperative approaches the
enorcement tools may need to be used
i companies do not overcome their res-
ervations
On the whole the requirements o Articles
45 and 46 have provided an efficient and
appropriate instrument or collecting and
evaluating existing paediatric studies
55 Clinical trials with
children
It is generally accepted that the Paediatric
Regulation will lead to more clinical trialswith children but that its aims should be
achieved without subjecting children to
unnecessary clinical trials
The youngest paediatric-age subsets
including neonates are particularly sen-
sitive It will be a constant challenge to
balance the therapeutic needs o these
age groups with their specific vulnerability
when considering and deciding on the ap-
propriateness o specific clinical trials or
the specific settings o studies in this age
subset Efforts are thereore continuously
being made to explore alternative means
eg the use o extrapolation modelling
and simulation techniques to reduce the
number o study subjects as much as
possible The Paediatric Committee is ac-
tively contributing to acilitate the devel-
opment and use o such means including
non-conventional trial design
Another challenge is how to avoid dupli-cating trials or different paediatric inves-
tigation plans rom different applicants
Companies embarking on product devel-
opment in similar areas may be required
by the agreed paediatric investigation
plan to conduct studies within similar
settings While collaborative approaches
between companies would be highly de-
sirable and have occurred on rare occa-
sions they ofen conflict with companiesrsquo
understandable reluctance to share datawith competitors in the early stages o
product development and participate in
direct comparisons This situation could
velopment Overall there is however no
evidence that the Regulation has a con-
siderable negative impact on products or
other populations
Rather there are some concerns that the
requirements under the Regulation may
cause delays in the authorisation o prod-ucts with paediatric-only indications as
they bring added complexity to the RampD
and regulatory process or products that
already directly target children The added
value o the submission o a paediatric in-
vestigation plan in these cases will be as-
sessed urther in the 2017 report
54 Reaping the benefits of
existing information
There was widespread speculation prior to
the adoption o the Paediatric Regulation
as to how many studies would be submit-
ted by pharmaceutical companies in ac-
cordance with Articles 45 and 46 The act
that competent authorities received more
than 18 000 studies reveals the consid-
erable amount o paediatric inormation
that existed at company level
Certainly it is true that not all the inor-
mation submitted met modern require-
ments or scientific data and clinical re-
search and that the work-sharing process
o evaluating the inormation is rather
long and resource intensive
Nevertheless compared to the PUMA con-
cept this scheme proved more successul
in terms o output and in recommending
and implementing changes to the sum-
mary o product characteristics o author-
ised products In its public consultationthe Commission called Articles 45 and 46
the lsquohidden gemsrsquo o the Regulation
One drawback that remains however
is reluctance by marketing authorisa-
tion holders to update the summary o
product characteristics on a voluntary
basis This said the Regulation contains
mechanisms to overcome such reluctance
as it empowers competent authorities to
directly update the summary and varythe marketing authorisation accordingly
Moreover in accordance with Article 23
o Directive 200183EC22 and Article 16
o Regulation (EC) No 726200423 mar-
22 Directive 200183EC othe European Parliament and
o the Council o 6 November2001 on the Community
code relating to medicinalproducts or human use OJ L311 28112001 p 67
23 Regulation (EC) No7262004 o the European
Parliament and o the Coun-cil o 31 March 2004 layingdown Community procedures
or the authorisation andsupervision o medicinalproducts or human and
veterinary use and establish-ing a European Medicines
Agency OJ L 136 3042004p 1
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1736
17
lead to competition among companies to
find investigators and study participants
as well as the duplication o trials which
are unnecessary rom a scientific and
ethical point o view
The Paediatric Committee is able to waive
paediatric trial requirements where thespecific medicinal product does not rep-
resent a significant therapeutic benefit
over an existing treatment or paediatric
patients including once the product is au-
thorised (Article 11) However this option
does not provide a way out in the early
stages o product development where
the Committee has to ensure equal treat-
ment and non-discriminatory approaches
The key to avoiding such unnecessary tri-
als is transparency with regard to ongoingand completed trials The situation contin-
ues to be monitored
Finally it is in the interest o the EU that
paediatric trials stemming rom paedi-
atric investigation plans are conducted
within the EU This has less to do with
the standards under which a trial is con-
ducted given that clinical trials carried
out outside the EU have to meet the ethi-
cal and scientific requirements o the EUprovisions on clinical trials24 than with the
act that studies within the EU may pro-
vide patients there with early access to
innovative medicines To date there is in-
sufficient data on the ratio between pae-
diatric trials conducted within and outside
the EU However in view o the upgraded
unctionalities o the EudraCT database it
is expected that more data will be avail-
able in 2017 or the second report
56 Spreading the news mdash
getting new information
to patients and healthcare
professionals
I the Regulation is to be a success it is
not only necessary that data on the use
o a specific product in the paediatric
population are collected but that these
data are then also appropriately commu-
nicated to and used by paediatricians intheir day-to-day work or the benefit o
their patients
In this regard some studies published in
the medical literature suggest a ailure
on the part o practitioners to recognise
the actual amount o off-label prescrib-
ing to children Moreover it is claimed that
the prescribing habits o practitioners are
ofen strongly influenced by personal ex-
perience rather than by evidence-based
inormation or paediatric medicine25
These studies in making generalisations
may not have taken into account the het-
erogeneity o healthcare proessionals
whose receptiveness varies greatly ac-
cording to their work setting and specific
area o specialisation At the same time
such observations may point to a sub-
stantial hurdle in achieving the goal o the
Paediatric Regulation
National competent authorities as well as
organisations or healthcare proessionals
seem particularly qualified to consider ap-
propriate ways o ensuring an adequate
flow o inormation Some Member States
have already established a number o
tools to communicate effectively and e-
ficiently with healthcare proessionals
eg by means o regular meetings web-
based inormation distribution systems ornational ormularies
57 Is the burden greater
than rewards
There can be no doubt that the Paediat-
ric Regulation places a considerable ad-
ditional burden on pharmaceutical com-
panies with its obligations regarding
research on products or use in children
However this approach was adopted be-cause market orces alone proved insu-
ficient to stimulate adequate research
The Regulation requires companies to
submit paediatric investigation plans at
an early stage o product development
However research on some active sub-
stances may be discontinued at later
stages should urther studies ail to show
potential with respect to the saety and
efficacy o the product For every success-
ul authorised medicinal product there aremany that ail to make the finishing line
Hence not all approved paediatric investi-
gation plans will be completed as compa-
24 Directive 200120EC othe European Parliament
and o the Council on theapproximation o the laws
regulations and administra-tive provisions o the Mem-ber States relating to the
implementation o good clini-cal practice in the conducto clinical trials on medicinal
products or human use OJ L121 152001 p 34
25 5-year report to theEuropean Commission (seeootnote 3) page 41
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1836
18
nies may decide to stop the correspond-
ing adult development It is too early still
to obtain reliable statistics that show
the ratio between completed and non-
completed paediatric investigation plans
but in the current context not all approved
plans will eventually result in an approved
medicine with a paediatric indication
In terms o output this entails some un-
necessary effort in compiling and screen-
ing paediatric investigation plans To what
extent this is offset by the benefit o early
submission which ensures that the pae-
diatric development fits smoothly into the
overall product development need ur-
ther monitoring
A urther point o concern is the highnumber o modifications to paediat-
ric investigation plans Figures seem to
suggest that nearly all plans have to
be modified at least once Conceptually
though this does not come as a surprise
in view o the early submission o pae-
diatric investigation plans the length o
adult and paediatric developments and
the substantial deerrals granted An
RampD plan requently has to be adapted
or amended to take account o initial re-sults Recruitment problems or necessary
design changes in the trials may also lead
to modifications While it is acknowledged
that substantial amendments or modifi-
cations to the plan have to be subject to
discussions with the Paediatric Commit-
tee this is less obvious or minor changes
In this context the level o detail required
by the EMA has been repeatedly criticised
In the past five years the EMA and its
Paediatric Committee have made effortsto provide or some flexibility in the plan
so to allow a margin o manoeuvre that
takes account o uncertainties in relation
to certain parameters o a trial
In any case the Commission intends to
review its Communication on the ormat
and content o applications or agree-
ment or modification o a paediatric in-
vestigation plan to take into account the
experience gained including the consider-
able number o modification requests
On a positive note it can be noted that
companies are applying or the rewards
provided by the Regulation primarily the
6-month extension o the Supplementary
Protection Certificate which have been
introduced to offset the additional bur-
den The economic value o the reward
depends on the turnover o the product
concerned In the case o blockbuster
products the amount may be consider-
able while or niche products the effect
is small
An in-depth evaluation o the economic
impact will be included in the 2017 report
in order to draw conclusions on the bal-
ance between burden and rewards and
public health benefits
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1936
19
6Outlook mdash
A fairy-taleending aheadlsquoBetter Medicines or Children mdash From
Concept to Realityrsquo is the title o this re-
port Readers may suggest that based on
the evaluation reerred to above it would
be more appropriate to add a question
mark It is evident that it is too early still
to make a firm statement Despite more
than five years o experience the true im-pact o the Regulation on the health o
children will only become apparent over
time as experience is accumulated in the
longer term
There are encouraging signs though
Paediatric development has become a
more integral part o the overall develop-
ment o medicinal products in the EU A
number o new products with paediatric
indications and age-appropriate pharma-ceutical orms have been authorised and
made available to patients A high num-
ber o agreed paediatric investigation
plans indicates that urther products are
in the pipeline
However it needs to be pointed out that it
would be wrong to expect the Regulation
to be able to solve all problems Instead
it is a major catalyst to improve the situ-
ation o young patients
Finally some weaknesses and deficits
have also become apparent in the last
five years Their impact on the overall
perormance o the Regulation has to be
closely monitored On the basis o the ac-
tions outlined above the Commission in-
tends to fine-tune the current implemen-
tation together with the EMA
Even i better medicines or children are
not yet a reality it should be the ambitiono all stakeholders involved that this piece
o legislation will be or the greater good
o children so that in the 2017 report
the discussion will ocus not on whether a
question mark should be added to the ti-
tle o the report but on whether it should
be an exclamation mark instead
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2036
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2136
21
ANNEXES
Figures and Tables
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2236
22
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2336
23
ANNEX I
Figures and Tables
Table 1Agreed paediatric investigations plans (PIPs) 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Agreed PIPs submitted under Article 7 (without waivers)
Agreed PIPs submitted under Article 8 (without waivers)
Source EMA Paediatric database The numbers on agreed PIPs correspond to EMA decisions
Table 2Agreed paediatric investigations plans (PIPs) compared to ull waivers and modifications 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Submitted modifications of an agreed PIP
Agreed Full waivers
Source EMA Paediatric database The numbers on agreed PIPs and waivers correspond to EMA decisions
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2536
25
Table 5Scientific advice and protocol assistance including ollow-ups (provided by the EMA Scientific Advice Working
Party and the Committee or Human Medicinal Products per year)
259
277321
388 400 433 420
021 32
74 8057
91
0 0 0
68 8067
94
0
100
200
300
400
500
2006 2007 2008 2009 2010 2011 2012
Total number of advice (Scientific Advice and Protocol Assistance)
Sum of paediatric-only and mixed (adult and paediatric development questions)
advice
Paediatric-only or mixed advice that involved a Paediatric Committee member(s) as
expert(s)
Source EMA databases Year o advice letter
Year o start o procedure
Table 6Paediatric clinical trials by year o authorisation
2005 2006 2007 2008 2009 2010 2011 2012
Paediatric trials
(number) 254 316 355 342 404 379 334 332
Paediatric trials
that are part of anagreed PIP 2 1 2 6 16 30 76 76
Proportion of
paediatric trials
that are part of an
agreed PIP among
paediatric trials 1 0 1 2 4 8 23 23
Total number
of trials (adults
and or children) 3 350 3 979 4 749 4 512 4 445 4 026 3 809 3 698
Proportion of
paediatric trials of
all trials 8 8 7 8 9 10 9 9
Source EudraCT Data Warehouse using a predefined query on 6 March 2013 and counting the first authorised trial only in the case o more thanone Member State This partial inormation requires sponsors to use a Clinical Trial Application orm that was only available rom November 2009 or use with version 8 o EudraCT
(available rom 2011)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2636
26
Table 7Number o children to be enrolled in clinical trials
Number
of subjects 2006 2007 2008 2009 2010 2011 2012
Pretermnewborns 0 0 0 207 82 2 281 1 712
Newborns 0 0 5 64 169 1 105 1 172
Infants and
toddlers 330 21 20 59 351 2 788 3 141
Children 2 142 181 200 2 230 2 055 10 325 20 677
Adolescents 368 111 205 1 577 2 861 9 054 13 193
Sum of
above 2 840 313 430 4 137 5 517 25 553 39 895
Reference
number of paediatric
trials 316 355 342 404 379 334 332
Source EudraCT Data Warehouse using a pre-defined query on 6 March 2013 modified by excluding studies or lsquoimmunological medicinal productsrsquo
Table 8EU budget contribution to the Paediatric Regulation and the EMA expenditure
0
1
2
3
4
5
6
7
8
9
10
2006 2007 2008 2009 2010 2011 2012
EU budget contribution (in Million euro)
EMA expenditure for paediatri cs (in Mill ion euro)
EMA expenditure for paediatr ics including support (in Million euro)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2736
27
Table 9Percentage o European Medicines Agencyrsquos human resources working in the paediatric area rom 2006 (inner
circle) to 2012 (outer circle)
733 (2012)
052 (2006)
Table 10Member States acting as rapporteurs or the assessment o studies submitted in accordance with Article 46
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE SE NL FR DK IT BE PL ES NO SK FI IE RO AT HU EL CZ PT LV BG
Study included in worksharing Rapporteur appointed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2836
28
Table 11Member States acting as rapporteur or the assessment o studies submitted in accordance with Article 45
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE NL DK AT FR PL SE ES IE CZ MT IT BE SI EE FI HU NO RO BG EL LV PT IS SK
Wave 1 Wave 2 Wave 3 Wave 4 Wave 5 Wave 6 Wave 7 Wave 8 Wave 9
Wave 10 Wave 11 Wave 12 Wave 13 Wave 14 Wave 15 Wave 16 Wave 17 Wave 18
Table 12Member States acting as rapporteurspeer reviewers in EMArsquos Paediatric Committee procedures (initial PIP
waiver or modification o an agreed PIP)
0
50
100
150
200
250
300
350
400
450
500
A u s t r i a
B el gi um
B ul g a r i a
C y pr u s
C z e c h R e p u b l i c
D enm a r k
E s t oni a
F i nl a n d
F r a n c e
G er m a n y
G r e e c e
H e a l t h c a r e a n d
A c a d emi a
H un g a r y
I c el a n d
I r el a n d
I t a l y
L a t vi a
L i t h u a ni a
L ux em b o ur g
M a l t a
N or w a y
P a t i en t s Or g a ni s a t i on
P ol a n d
P or t u g a l
R om a ni a
S l ov a k i a
S l ov eni a
S p a i n
S w e d en
T h eN e t h er l a n d
s
U ni t e d K i n g d om
Initial PIP applications PIP modifications
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2936
29
ANNEX II
Detailed inventory of centrally authorised medicinalproducts for paediatric use since the entry into force
of the Paediatric Regulation
Table 13Medicinal products authorised centrally since 2007 which include a paediatric indication
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Retapamulin Altargo 2007 No Mixed
Nelarabine Atriance 2007 No Mixed
Human papillomavirus vaccine[types 16 18] Cervarix 2007 No Mixed
Hydroxocobalamin Cyanokit 2007 No Mixed
Idursulase Elaprase 2007 No Mixed
Gadoversetamide Optimark 2007 No Mixed
Betaine anhydrous Cystadane 2007 No Mixed
Stiripentol Diacomit 2007 No Paediatric only
Mecasermin Increlex 2007 No Paediatric only
Rufinamide Inovelon 2007 No Mixed
Hydroxycarbamide Siklos 2007 No Mixed
Human normal
immunoglobulin (ivig) Flebogamma DIF 2007 No Mixed
Fluticasone uroate Avamys 2008 No Mixed
Human normal immunoglobulin Privigen 2008 No Mixed
Lacosamide Vimpat 2008 No Mixed
Micaungin Mycamine 2008 No Mixed
Sapropterin Kuvan 2008 No Mixed
Sugammadex Bridion 2008 No Mixed
Tocoersonal d-alpha
tocopheryl polyethylene glycol
succinate Vedrop 2009 No Paediatric only
Miamurtide Mepact 2009 No Mixed
Rilonacept Rilonacept Regeneron 2009 No Mixed
Tacrolimus Modigra 2009 No Mixed
Pneumoccocal polysaccharideconjugate vaccine (adsorbed) Synflorix 2009 No Paediatric only
Canakinumab
Ilaris (PIP not yet
completed) 2009 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3036
30
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Pneumoccocal polysaccharide
conjugate vaccine (13-valentadsorbed)
Prevenar 13 (PIP not yetcompleted) 2009 Yes Paediatric only
Meningococcal group a c
w135 and y conjugate vaccine Menveo 2010 Yes Mixed
Velaglucerase ala
Vpriv (PIP not yet
completed) 2010 Yes Mixed
Influenza vaccine (live
attenuated nasal) Fluenz (Waiver) 2011 Yes Paediatric only
C1 inhibitor human
Cinryze (PIP not yet
completed) 2011 Yes Mixed
Dihydroartemisinin
piperaquine phosphate
Eurartesim (PIP not yet
completed) 2011 Yes Mixed
Midazolam Buccolam 2011 Yes (PUMA) Paediatric only
EverolimusVotubia(PIP not yet completed) 2011 Yes Mixed
Tobramycin
Tobi Podhaler (PIP not
yet completed) 2011 Yes Mixed
Nomegestrol estradiol Ioa Zoely 2011 Yes Mixed
Colistimethate sodium Colobreathe 2012 Yes Mixed
Mercaptopurine Xaluprine 2012 No Mixed
Catridecacog NovoThirteen 2012 Yes MixedEavirenz Eavirenz Teva 2012 No Mixed
Ivacafor Kalydeco 2012 Yes Mixed
Desloratadine Desloratadine ratiopharm 2012 No Mixed
Desloratadine Desloratadine Actavis 2012 No Mixed
Perampanel Fycompa 2012 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3136
31
Table 14List o centrally authorised medicinal products or which the therapeutic indication was extended to or amend-
ed or the paediatric population
Active substance(s)
Trade
name Date Subject of the extension
Levetiracetam Keppra
2007
2009
Extension o the indication to include adjunctive ther-
apy in the treatment o primary generalised tonic-
clonic (PGTC) seizures in adults and adolescents rom
12 years o age with idiopathic generalised epilepsyExtension o indication to include the adjunctive
treatment o partial seizures with or without second-
ary generalisation in children rom 1 month to lt4
years old
Pneumococcal sac-
charide conjugated
vaccine adsorbed Prevenar 2007
Extension o the indication to include new inorma-
tion on efficacy against disease caused by Strepto-
coccus pneumoniae serotypes 4 6B 9V 14 18C 19F
and 23F in otitis mediaExtension o indication rom active immunisation
against bacteraemic pneumonia to active immunisa-
tion against pneumonia
Infliximab
Remi-
cade 2007
Extension o indication to include treatment o
severe active Crohnrsquos disease in children aged 6 to
17 years
Darbepoetin ala Aranesp 2007
Extension o indication or CRF patients whichrestricted the use o Nespo to paediatric subjects ge
11 years o age
Fosamprenavir Telzir 2007
Extension o indication o Telzir in combination withritonavir or the treatment o Human Immunodefi-
ciency Virus Type 1 (HIV-1) inected adults in combi-nation with other antiretroviral medicinal products to
include paediatric populations
Lamivudine zidovu-
dine Combivir 2007
Extension o indication to include paediatric patients
and replacement o film-coated tablets by scored
film-coated tablets
Desloratadine Aerius 2007Extension o indication rom lsquochronic idiopathic urti-cariarsquo to lsquourticariarsquo
Insulin glulisine Apidra 2007
Extension o indication to include 6 year olds and
older children based on the results o 2 paediatricstudies
Human papilloma virusvaccine [types 6 11
16 18] (recombinantadsorbed) Gardasil 2008
Extension o indication to include the prevention ohigh-grade vaginal dysplastic lesions (VaIN 23)
Adalimumab Humira 20082011
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in adoles-cents rom 13 to 17 years o age
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in the paedi-
atric population aged rom 4 to 12 years
Caspoungin Cancidas 2008
Extension o the indication to include the paediatric
population
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 336
REPORTFROM THECOMMISSIONTO THE
EUROPEANPARLIAMENTAND THECOUNCIL
Better Medicinesfor ChildrenFrom Concept to Reality
General Report on
experience acquired as a
result of the application
of Regulation (EC)ndeg 19012006 on
medicinal products for
paediatric use
(text with EEA relevance)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 536
5
1IntroductionlsquoBetter Medicines or Childrenrsquo was the
ambitious title o a consultation papero February 2002 in which the European
Commission presented its vision or regu-
latory actions on paediatric medicinal
products1 At that time many o the prod-
ucts used in children were not specifically
studied or authorised in children Instead
doctors ofen used products authorised
or adults sometimes in different dosag-
es with the associated risks o inefficacy
andor adverse reactions
The consultation paper built on a 5-year
discussion process that started in 1997
with a round table meeting at the prem-
ises o the European Medicines Agency
(EMA) and was the blueprint or the sub-
sequent legislative act It outlined many
o the measures that are to be ound in
the Paediatric Regulation (Regulation (EC)
No 19012006 o the European Parlia-
ment and o the Council on medicinal
products or paediatric use2
hereinaferlsquothe Regulationrsquo)
The Regulation was adopted some five
years afer the consultation paper on 12
December 2006 It entered into orce on
26 January 2007 and its main provisions
were applicable rom 26 July 2008 (Ar-
ticle 7) and 26 January 2009 (Article 8)
respectively
Five years on it is time to take stock o
developments and report to the EuropeanParliament and the Council on the experi-
ence acquired as a result o the Regula-
tion in accordance with its Article 50(2)
Are we already seeing the emergence o
lsquobetter medicines or childrenrsquo
This report does not yet provide compre-
hensive answer as it is subject to certain
limitations it should thereore be regard-
ed as an interim report that presents a
first impression o the experience gainedIn view o the development cycles o me-
dicinal products it will take at least 10
years to gain a ull understanding o the
impact o the legislation This actor has
already been accounted or in the legis-
lation which requires the Commission to
provide a second more comprehensive
report in 2017 which in accordance with
Article 50(3) o the Regulation must in-
clude an analysis o the economic impact
o the rewards and incentives together
with an analysis o the Regulationrsquos im-
plications or public health with a view to
proposing any necessary amendments
However at this stage some analyses and
interim conclusions can be made
This document has been prepared in con-
sultation with Member States the EMA
and interested parties The Commission
particularly values the lsquo5-year Report to
the European Commissionrsquo presenting the
views o the EMA and its Paediatric Com-
mittee3 and the responses to the public
consultation the Commission undertook
at the end o 20124
1 httpeceuropaeuhealthfilespharmacosdocs
doc2002ebcd_pediat-rics_enpd
2 OJ L 378 27122006p 1 amended by Regulation
(EC) No 19022006 o theEuropean Parliament and othe Council o 20 December
2006 OJ L 378 27122006p 20
3 5-year report to theEuropean Commission mdashGeneral report on experience
acquired as a result o theapplication o the Paedi-
atric Regulation preparedby the European MedicinesAgency with its Paediatric
Committee httpeceuropa
euhealthfilespaediat-rics2012-09_pediatric_re-
port-annex1-2_enpd
4 httpeceuropaeuhealth
human-usepaediatric-med-icinesdevelopments2013_
paediatric_pc_enhtm
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 636
6
2The Paediatric
RegulationIn 2010 around 21 o Europeans were
children representing more than 100 mil-
lion people Children represent a vulnera-
ble population group with developmental
physiological and psychological differenc-
es rom adults They are not merely lsquosmall
adultsrsquo Age- and development-related
research and the availability o suitable
medicinal products is consequently par-
ticularly important
Studies carried out beore the Regulation
was adopted showed that over 50 o the
medicines used or children had not been
tested or use in this specific age group
What is more only a limited number o
medicinal products had been developed
specifically with children in mind Com-
panies had already developed a range o
products against a number o diseases
prior to the Paediatric Regulation particu-
larly in sectors such as childhood immuni-sation by means o vaccines However the
availability o child-appropriate medicines
was generally unsatisactory Accordingly
the Regulation was seen as a response to
the absence o sufficient numbers o suit-
able authorised medicinal products with
appropriate dosages and pharmaceutical
orms to treat conditions in children in the
European Union (EU)
There are several reasons or the lacko paediatric medicines It would how-
ever be too simplistic to pin the blame
on pharmaceutical companies or not car-
rying out enough research and develop-
ment (RampD) to adapt medicinal products
to the needs o the paediatric popula-
tion This reluctance has long mirrored a
general social and ethical paradigm that
children should be protected rom clinical
research Only in the last two decades has
there been a shif to the current consen-sus o better protecting children through
clinical research
Economic actors certainly rendered pae-
diatric RampD less attractive in terms o
achieving an adequate return on invest-
ment Children are not a homogenous
sub-group mdash subpopulations range rom
neonates to teenagers with different bio-
logical and pharmacological characteris-
tics Age-appropriate research makes the
process more expensive and complex or
organisations that are active in this sec-
tor
However the absence o specifically
tested products ofen lef healthcare
proessionals with no alternative but to
use products lsquooff-labelrsquo with the associ-
ated non-negligible risks o inefficacy or
adverse reactions Such a situation was
contrary to the general goal to providehigh-quality medicinal products to the en-
tire EU population
To address this problem the Regula-
tion establishes a system o obligations
rewards and incentives together with
horizontal measures to ensure that medi-
cines are regularly researched developed
and authorised to meet the therapeutic
needs o children Other than the Orphan
Regulation5
which is limited to providingvarious incentives the Paediatric Regula-
tion has a direct impact on companiesrsquo
RampD expenditure While not questioning
that medicinal development is company
driven it compels companies to consider
the potential paediatric use o medicinal
products they develop
5 Regulation (EC)Ndeg 1412000 o the Euro-
pean Parliament and theCouncil o 16 December
1999 on orphan medicinalproducts OJ L 18 2212000p 1
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 736
7
The key objectives of theRegulation are
bull to ensure high-quality research into
the development o medicines or
children
bull to ensure over time that the major-ity o medicines used by children are
specifically authorised or such use
with appropriate orms and ormula-
tions
bull to ensure the availability of high-
quality inormation about medicines
used by children
The key measures included inthe Regulation are
bull setting up an expert committee with-
in the EMA the Paediatric Commit-
tee
bull requiring companies to submit dataon the use o a medicine in children
in accordance with an agreed paedi-
atric investigation plan when apply-
ing or marketing authorisation or
medicines and line-extensions or
existing patent-protected medicines
bull a system of waivers from the re-
quirement or medicines unlikely to
benefit children and a system o de-
errals in relation to the timing o the
requirement to ensure that medi-
cines are tested in children only whenit is sae to do so and to prevent the
requirements delaying the authorisa-
tion o medicines or adults
bull a reward for complying with the re-
quirement in the orm o a six-month
extension to the Supplementary Pro-
tection Certificate
bull a reward in respect of orphan medi-
cines or compliance in the orm o
an extra two years o market exclu-
sivity added to the existing ten yearsawarded under the EUrsquos Orphan Reg-
ulation
bull a new type of marketing authorisa-
tion the Paediatric Use Marketing
Authorisation (PUMA) to attract newpaediatric indications or off-patent
products
bull measures to maximise the impact of
existing studies on medicines or chil-
dren
bull an EU inventory of the therapeuticneeds o children to ocus the re-
search development and authorisa-
tion o medicines
bull an EU network of investigators and
trial centres to carry out the required
RampD
bull a system of free scientic advice for
the industry provided by the EMA
bull a public database of paediatric stud-
ies
bull a provision on EU funding for re-search to stimulate the development
and authorisation o off-patent med-
icines or children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 836
8
The Regulation gives the EMA and its
Paediatric Committee primary responsi-
bility or handling paediatric investigation
plans deerrals and waivers This provides
the Agency with concrete decision-mak-
ing powers
The operational costs o the PaediatricRegulation are partly covered by a contri-
bution rom the EU budget (see Table 8)
as its main activities do not attract any
ees For the period 2007-12 the EU
budget contribution amounted to more
than EUR 39 million In addition Member
Statesrsquo national competent authorities
contribute resources in kind especially
staff time or the assessment o paediat-
ric investigation plans (see Table 12)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 936
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1036
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1136
11
cantly (see Table 5) despite the act that
issues o pharmaceutical non-clinical and
clinical development are also part o the
discussions o a paediatric investigation
plan To acilitate collaboration with the
Paediatric Committee joint procedures
have been created within the EMA
413 Clinical trials with children
Medicines or use in children need to be
tested with appropriate ormulations in
the paediatric population to ensure their
sae and effective use Hence it is gener-
ally accepted that the Paediatric Regula-
tion will lead to more clinical trials in chil-
dren The figures in the EudraCT database
have not yet shown an increase in paedi-
atric trials The number remained stablebetween 2006 and 2012 averaging 350
trials per year with some fluctuations (see
Table 6) It should be pointed out how-
ever that while the number o paediat-
ric trials remained stable the number o
clinical trials in all populations decreased
between 2007 and 2011
Moreover until recently EudraCT was lim-
ited to paediatric trials commencing in the
EU Data on paediatric trials that are parto a paediatric investigation plan and con-
ducted outside the EU have only become
publicly available since spring 2011
It should also be noted that the initiation
o a considerable percentage o clinical
trials included in a paediatric investiga-
tion plan has been deerred in order to
avoid delays in the authorisation o the
corresponding product or adults Hence
the impact o the Paediatric Regulation on
paediatric trials will become more appar-
ent in EudraCT in the years to come There
has however been an evident increase in
the number o paediatric study partici-
pants in particular or the age group rom
0 to 23 months who were normally not
included in trials prior to 2008 (see Ta-
ble 7) Allowing neonates and inants to
benefit rom research is a positive sign
as these have been the most neglected
groups so ar
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1236
12
414 Optimised framework and
coordination
The Paediatric Regulation osters a com-
prehensive network o expertise in paedi-
atric matters within the EU In this context
the role o the Paediatric Committee ispivotal as it brings together a high level
o expertise and competence
The Committee has contributed to the
scientific guidelines published by the EMA
and has so ar convened 22 expert work-
shops on the development o medicines
or children
In addition the European Network or
Paediatric Research at the EMA (Enpr-
EMA) was established in 2009 While aclosely-knit network o experts existed
prior to the introduction o the Regula-
tion in disease areas such as paediatric
oncology Enpr-EMA provides the added
value o a holistic approach by bringing
together national and European networks
investigators and centres with specific ex-
pertise in designing and conducting high-
quality studies in children
However question still remain as towhether this expertise translates into su-
ficient capacity within the EU to conduct
trials in specialised investigation settings
Well-developed research networks capa-
ble o acilitating the necessary research
to ulfil the commitments included in
paediatric investigation plans do exist in
some but not all Member States
415 International cooperation
On an international level the EMA has de-veloped international links with medicines
agencies in the United States Canada
and Japan O particular interest is the
cooperation with the US Food and Drug
Administration given that already in the
late 1990s the United States introduced
legislation that stimulated the develop-
ment o medicinal products or paediatric
use by means o a combination o incen-
tives and obligations This cooperation is
also o great interest to stakeholders as
it may give companies the possibility o
satisying the legislation in both regions
with the same studies
In addition the EMA participates actively
in the Paediatric medicines regulatory
network16 which was created in 2010 as
part o the WHOrsquos Better Medicines or
Children initiative
42 More medicines available
for children
Over 12 years (rom 1995 to 2006) 108
o all 317 indications o 262 centrally au-
thorised medicines included the paediat-
ric population Since the Paediatric Regu-
lation entered into orce 31 out o 152
new medicines have been authorised or
paediatric use 10 o which met the con-
ditions o Article 7 This is not more than
a lsquosnapshotrsquo o the effects o the Regula-
tion as this figure is likely to increase inthe uture as a considerable number o
the new already authorised medicines
are subject to an investigation plan where
completion was deerred to avoid delays
in the authorisation o the adult product
It ollows that in the years to come many
more o those 152 new medicines are ex-
pected to be authorised or paediatric use
Annual reports on deerred paediatric
studies o authorised medicines indicate
that the majority o paediatric investiga-tion plans are running to schedule Pae-
diatric research is on-going at the same
rate across therapeutic areas such as on-
cology vaccines and immunology-rheu-
matology-transplantation
Furthermore by the end o 2011 72 new
paediatric indications had been approved
or medicines already authorised includ-
ing 30 indications (18 centralised) arising
rom the obligation in Article 8 Moreover26 new pharmaceutical orms were au-
thorised or paediatric use including 18
adapted orms or centrally authorised
medicines
As ar as Paediatric Use Marketing Au-
thorisation is concerned to date only one
authorisation has been granted This alls
short o initial expectations
16 httpwwwwhointchild-medicinespaediatric_regula-
torsen
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1336
13
A detailed inventory o centrally autho-
rised products is provided in Annex II
Rewards and incentives
Companies that have complied with the
obligations o the Regulation may benefit
rom a reward once the product concerned
is authorised or the product inormation isamended The reward takes the orm o a
6-month extension o the supplementary
protection certificate (SPC) provided or
by Regulation (EC) No 469200917 or in
the case o an orphan medicinal product
by an extension o the ten-year period o
orphan market exclusivity to twelve years
No orphan rewards have been awarded
yet In this regard it is observed that some
companies withdrew the orphan designa-tion o a product in order to qualiy or
the SPC reward rather than the orphan
reward which seems to be more attrac-
tive rom an economic perspective As ar
as SPC extensions are concerned national
patent offices in 16 Member States had
by the end o 2011 granted 6-month ex-
tensions to 11 medicinal products which
resulted in a total o more than 100 na-
tional SPCs
It should be pointed out that a ruling othe European Court o Justice urther
increased the value o the paediatric
reward as it made clear that the initial
certificate could have a negative or zero
duration which could then become posi-
tive once the paediatric extension was
granted18
43 Increased information on
medicines used in childrenTo provide better inormation on the use
o medicinal products in children Article
45 o the Paediatric Regulation requires
companies holding data on the saety
or efficacy o authorised products in the
paediatric population to submit these
studies to the competent authorities In
this way the data can be assessed and
where appropriate the authorised prod-
uct inormation amended Article 46 o
the Regulation also requires companies tosubmit newly generated paediatric data
Since 2008 more than 18 000 study re-
ports on roughly 2 200 medicinal prod-
ucts have been submitted revealing the
large amount o existing paediatric inor-
mation available at company level
These study reports have been and
continue to be assessed by the compe-
tent authorities thanks to an impressive
work-sharing project (see Tables 10 and11) For nationally authorised products
this has led to the publication o assess-
ment reports covering more than 140
active substances and in a considerable
number o cases to recommendations
or changes to the summaries o product
characteristics o authorised products re-
sulting in 65 actual changes For centrally
authorised products by 2011 the Agency
had completed the assessment o all the
data submitted under Article 45 covering55 active substances in 61 centrally ap-
17 Regulation (EC) No4692009 o the Euro-
pean Parliament and othe Council o 6 May 2009
concerning the supplemen-tary protection certificateor medicinal products OJ
L 152 1662009 p 1 ThisRegulation is a codificationo Council Regulation (EEC)
No 176892
18 Case C-12510 Merck
Sharp amp Dohme v DeutschesPatent- und Markenamt notyet published in the ECR
paragraph 37 lsquoi the SPCapplication had to be reused
because the calculationprovided or in Article 13(1)o Regulation No 176892
results in a negative or zero
duration the holder o thebasic patent could not obtain
an extension o protectionconerred by such a patenteven i it conducted all the
studies according to the ap-proved paediatric investiga-
tion plan under Article 36 oRegulation No 19012006Such a reusal would be
liable to adversely impacton the useul effect oRegulation No 19012006
and might jeopardise the
objectives o that regulationnamely the compensation
o effort made to evaluatethe paediatric effects o themedicinal product at issuersquo
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1436
14
proved medicinal products The summa-
ries o product characteristics o 12 me-
dicinal products were changed ollowing
the assessment
5Lessonslearnt51 Better access to
treatment
One o the explicit goals o the Paediatric
Regulation is to increase the number oproducts that are researched developed
and authorised or use in children and
to reduce the off-label use o medicinal
products in the paediatric population
The main tool to achieve this result is to
oblige companies to establish a paediat-
ric investigation plan or each newly de-
veloped product or or the line extension
o an already authorised product that is
still under patent protection The plan ismeant to ensure mdash under the supervi-
sion o the Paediatric Committee mdash that
the necessary data are generated so as
to determine the conditions under which
a medicinal product may be authorised
to treat children Since 2008 more than
600 paediatric investigation plans have
been approved However only a minor-
ity o them has been completed to date
the vast majority are still on-going This
is due to the long development cycles omedicinal products ofen lasting more
than a decade and the near-systematic
deerral o paediatric studies The high
number o deerrals may not have been
initially expected but are currently a real-
ity as or most o the medicinal products
that have been authorised so ar the RampD
programme started beore the entering
into orce o the Regulation Consequent-
ly the paediatric requirements could not
be taken into account rom the beginningo the product development
While the Paediatric Regulation has led
to some new authorisations that include
paediatric indications the regulatory in-
strument is recent and it will probably
take at least a decade beore it can be
judged in terms o its output In terms o
pharmaceutical orms there is however
already a visible positive impact
In this context criticism has been voiced
that the Regulation will ail to ensure abreakthrough in areas o particular pae-
diatric need such as paediatric oncology
This argument is related to the act that
the starting point or the majority o pae-
diatric investigation plans is an ongoing
RampD programme or a medicinal product
or adults An intrinsic consequence o this
approach is that these products primarily
target adult conditions They are devel-
oped in areas where there is a need (or a
market) in the adult population This needin the older population does not neces-
sarily correspond to the paediatric popu-
lationrsquos need
Moreover the Regulation grants waivers
rom its obligations where the disease or
condition or which the specific medicinal
product is intended occurs only in adult
populations This legislative approach cre-
ates riction in the case o diseases that
are specific and exclusive to children Italso limits the powers and possibilities o
the Paediatric Committee when reviewing
and agreeing to a paediatric investigation
plan as regards the scope o studies that
the Committee may request rom appli-
cants ollowing the objective and scien-
tific-based assessment o the compound
concerned19
These constraints and boundaries have to
be taken into account when judging the
impact the Regulation is likely to make In
addition the effect o instruments such as
the Orphan Regulation have to be consid-
ered given that or example all paediatric
cancers are rare diseases and all under
the EU policy ramework on rare diseases
All in all the achievements highlighted in
chapter 4 o this report and the number
o products with new paediatric indica-
tions show that there are some encourag-
ing signs afer this first five-year period it
is however too early or comprehensive
answers
19 Case T-5209 Nycomed vEMA not yet published
See the results o the publicconsultation conducted by
the Commission in prepara-tion o this Report
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1536
15
52 The PUMA concept a
disappointment
The Paediatric Regulation introduced a
new type o marketing authorisation mdash
the Paediatric Use Marketing Authorisa-
tion (PUMA) As an incentive to carry out
research into the potential paediatric use
o off-patent medicinal products that have
been authorised or adults this marketing
authorisation offers 8 years o data and
10 years o market exclusivity to any new
off-patent product developed exclusively
or use in the paediatric population Thus
the main goal o the PUMA concept is to
stimulate research in existing products
This scheme has been supported by EU
unding through the EU Framework Pro-
grammes or Research and Technological
Development
However to date only one PUMA has been
granted with a ew more projects cur-
rently in the pipeline
Neither industry nor academic networks
have embraced this opportunity as ully
as the Regulation intended It would seem
that the incentive o data and market ex-
clusivity does not work or these productsor at least that the market opportunities
in this sector are currently considered in-
sufficient to outweigh the inherent eco-
nomic risks o pharmaceutical develop-
ment Researchers are not engaging in
trials with medicines that have been on
the market or years Companies seem to
ear that market exclusivity will not pre-
vent physicians rom continuing to use
competitor products with the same active
ingredient off-label at lower costs or thatsubstitution or cheaper adult orms takes
place at the level o pharmacies Moreo-
ver national pricing and reimbursement
rules in Member States ofen do not al-
low or the additional research needed to
obtain the PUMA to be rewarded in price
negotiations20
Against this background the PUMA con-
cept has ailed so ar to ulfil the initial
expectationsThe EMA will in uture accept paediatric
investigation plans or a PUMA that cover
only certain age groups and not the en-
tire paediatric population This may offset
some o the reservations that currently
hamper better endorsement o the PUMA
concept
53 No impact on adultdevelopment
Studies prior to the adoption o the Regu-
lation have suggested a theoretical risk
that the requirements or research in chil-
dren could lengthen the overall drug de-
velopment process21 The Regulation has
met this risk head-on In order to avoid
any delays in authorising medicines or
other populations it allows or the grant-
ing o deerrals relating to the initiation orcompletion o some or all o the meas-
ures contained in a paediatric investiga-
tion plan
Experience shows that the deerral is a
widely used instrument which suggests
that the risk o delays in the processing o
adult applications is minimal There have
been some transitional problems in cases
where the adult programme was already
established when the Regulation enteredinto orce but these issues seem to have
been resolved
A concern that was raised initially was
that some companies would become
reluctant to develop new indications
pharmaceutical orms and new routes o
administration in small markets and or
products with low sales to avoid being
bound by the paediatric obligation under
Article 8 o the Regulation However thereis no evidence o such effect Moreover
it may also be argued that the incentive
o a potential six-month extension o the
SPC served to counterbalance such an
effect as it may have led companies to
examine more thoroughly the benefits o
a line extension taking into account the
economic value o the paediatric reward
Still industry stakeholders claim that
in rare cases the development or new
medicinal products has been delayedor abandoned in the expectation or as a
consequence o additional costs and re-
quirements associated with paediatric de-
20 See the results o thepublic consultation con-
ducted by the Commission inpreparation o this Report
21 C Commission StaffWorking Document Proposal
or a Regulation o the Euro-pean Parliament and o theCouncil on medicinal prod-
ucts or paediatric use andamending Council Regulation(EEC) No 17692 Directive
200183EC and Regula-tion (EC) No 7262004Extended impact assessment
(COM2004599F)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1636
16
keting authorisation holders are obliged
to ensure that the product inormation
is kept up to date with the current scien-
tific knowledge While preerence should
be given to cooperative approaches the
enorcement tools may need to be used
i companies do not overcome their res-
ervations
On the whole the requirements o Articles
45 and 46 have provided an efficient and
appropriate instrument or collecting and
evaluating existing paediatric studies
55 Clinical trials with
children
It is generally accepted that the Paediatric
Regulation will lead to more clinical trialswith children but that its aims should be
achieved without subjecting children to
unnecessary clinical trials
The youngest paediatric-age subsets
including neonates are particularly sen-
sitive It will be a constant challenge to
balance the therapeutic needs o these
age groups with their specific vulnerability
when considering and deciding on the ap-
propriateness o specific clinical trials or
the specific settings o studies in this age
subset Efforts are thereore continuously
being made to explore alternative means
eg the use o extrapolation modelling
and simulation techniques to reduce the
number o study subjects as much as
possible The Paediatric Committee is ac-
tively contributing to acilitate the devel-
opment and use o such means including
non-conventional trial design
Another challenge is how to avoid dupli-cating trials or different paediatric inves-
tigation plans rom different applicants
Companies embarking on product devel-
opment in similar areas may be required
by the agreed paediatric investigation
plan to conduct studies within similar
settings While collaborative approaches
between companies would be highly de-
sirable and have occurred on rare occa-
sions they ofen conflict with companiesrsquo
understandable reluctance to share datawith competitors in the early stages o
product development and participate in
direct comparisons This situation could
velopment Overall there is however no
evidence that the Regulation has a con-
siderable negative impact on products or
other populations
Rather there are some concerns that the
requirements under the Regulation may
cause delays in the authorisation o prod-ucts with paediatric-only indications as
they bring added complexity to the RampD
and regulatory process or products that
already directly target children The added
value o the submission o a paediatric in-
vestigation plan in these cases will be as-
sessed urther in the 2017 report
54 Reaping the benefits of
existing information
There was widespread speculation prior to
the adoption o the Paediatric Regulation
as to how many studies would be submit-
ted by pharmaceutical companies in ac-
cordance with Articles 45 and 46 The act
that competent authorities received more
than 18 000 studies reveals the consid-
erable amount o paediatric inormation
that existed at company level
Certainly it is true that not all the inor-
mation submitted met modern require-
ments or scientific data and clinical re-
search and that the work-sharing process
o evaluating the inormation is rather
long and resource intensive
Nevertheless compared to the PUMA con-
cept this scheme proved more successul
in terms o output and in recommending
and implementing changes to the sum-
mary o product characteristics o author-
ised products In its public consultationthe Commission called Articles 45 and 46
the lsquohidden gemsrsquo o the Regulation
One drawback that remains however
is reluctance by marketing authorisa-
tion holders to update the summary o
product characteristics on a voluntary
basis This said the Regulation contains
mechanisms to overcome such reluctance
as it empowers competent authorities to
directly update the summary and varythe marketing authorisation accordingly
Moreover in accordance with Article 23
o Directive 200183EC22 and Article 16
o Regulation (EC) No 726200423 mar-
22 Directive 200183EC othe European Parliament and
o the Council o 6 November2001 on the Community
code relating to medicinalproducts or human use OJ L311 28112001 p 67
23 Regulation (EC) No7262004 o the European
Parliament and o the Coun-cil o 31 March 2004 layingdown Community procedures
or the authorisation andsupervision o medicinalproducts or human and
veterinary use and establish-ing a European Medicines
Agency OJ L 136 3042004p 1
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1736
17
lead to competition among companies to
find investigators and study participants
as well as the duplication o trials which
are unnecessary rom a scientific and
ethical point o view
The Paediatric Committee is able to waive
paediatric trial requirements where thespecific medicinal product does not rep-
resent a significant therapeutic benefit
over an existing treatment or paediatric
patients including once the product is au-
thorised (Article 11) However this option
does not provide a way out in the early
stages o product development where
the Committee has to ensure equal treat-
ment and non-discriminatory approaches
The key to avoiding such unnecessary tri-
als is transparency with regard to ongoingand completed trials The situation contin-
ues to be monitored
Finally it is in the interest o the EU that
paediatric trials stemming rom paedi-
atric investigation plans are conducted
within the EU This has less to do with
the standards under which a trial is con-
ducted given that clinical trials carried
out outside the EU have to meet the ethi-
cal and scientific requirements o the EUprovisions on clinical trials24 than with the
act that studies within the EU may pro-
vide patients there with early access to
innovative medicines To date there is in-
sufficient data on the ratio between pae-
diatric trials conducted within and outside
the EU However in view o the upgraded
unctionalities o the EudraCT database it
is expected that more data will be avail-
able in 2017 or the second report
56 Spreading the news mdash
getting new information
to patients and healthcare
professionals
I the Regulation is to be a success it is
not only necessary that data on the use
o a specific product in the paediatric
population are collected but that these
data are then also appropriately commu-
nicated to and used by paediatricians intheir day-to-day work or the benefit o
their patients
In this regard some studies published in
the medical literature suggest a ailure
on the part o practitioners to recognise
the actual amount o off-label prescrib-
ing to children Moreover it is claimed that
the prescribing habits o practitioners are
ofen strongly influenced by personal ex-
perience rather than by evidence-based
inormation or paediatric medicine25
These studies in making generalisations
may not have taken into account the het-
erogeneity o healthcare proessionals
whose receptiveness varies greatly ac-
cording to their work setting and specific
area o specialisation At the same time
such observations may point to a sub-
stantial hurdle in achieving the goal o the
Paediatric Regulation
National competent authorities as well as
organisations or healthcare proessionals
seem particularly qualified to consider ap-
propriate ways o ensuring an adequate
flow o inormation Some Member States
have already established a number o
tools to communicate effectively and e-
ficiently with healthcare proessionals
eg by means o regular meetings web-
based inormation distribution systems ornational ormularies
57 Is the burden greater
than rewards
There can be no doubt that the Paediat-
ric Regulation places a considerable ad-
ditional burden on pharmaceutical com-
panies with its obligations regarding
research on products or use in children
However this approach was adopted be-cause market orces alone proved insu-
ficient to stimulate adequate research
The Regulation requires companies to
submit paediatric investigation plans at
an early stage o product development
However research on some active sub-
stances may be discontinued at later
stages should urther studies ail to show
potential with respect to the saety and
efficacy o the product For every success-
ul authorised medicinal product there aremany that ail to make the finishing line
Hence not all approved paediatric investi-
gation plans will be completed as compa-
24 Directive 200120EC othe European Parliament
and o the Council on theapproximation o the laws
regulations and administra-tive provisions o the Mem-ber States relating to the
implementation o good clini-cal practice in the conducto clinical trials on medicinal
products or human use OJ L121 152001 p 34
25 5-year report to theEuropean Commission (seeootnote 3) page 41
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1836
18
nies may decide to stop the correspond-
ing adult development It is too early still
to obtain reliable statistics that show
the ratio between completed and non-
completed paediatric investigation plans
but in the current context not all approved
plans will eventually result in an approved
medicine with a paediatric indication
In terms o output this entails some un-
necessary effort in compiling and screen-
ing paediatric investigation plans To what
extent this is offset by the benefit o early
submission which ensures that the pae-
diatric development fits smoothly into the
overall product development need ur-
ther monitoring
A urther point o concern is the highnumber o modifications to paediat-
ric investigation plans Figures seem to
suggest that nearly all plans have to
be modified at least once Conceptually
though this does not come as a surprise
in view o the early submission o pae-
diatric investigation plans the length o
adult and paediatric developments and
the substantial deerrals granted An
RampD plan requently has to be adapted
or amended to take account o initial re-sults Recruitment problems or necessary
design changes in the trials may also lead
to modifications While it is acknowledged
that substantial amendments or modifi-
cations to the plan have to be subject to
discussions with the Paediatric Commit-
tee this is less obvious or minor changes
In this context the level o detail required
by the EMA has been repeatedly criticised
In the past five years the EMA and its
Paediatric Committee have made effortsto provide or some flexibility in the plan
so to allow a margin o manoeuvre that
takes account o uncertainties in relation
to certain parameters o a trial
In any case the Commission intends to
review its Communication on the ormat
and content o applications or agree-
ment or modification o a paediatric in-
vestigation plan to take into account the
experience gained including the consider-
able number o modification requests
On a positive note it can be noted that
companies are applying or the rewards
provided by the Regulation primarily the
6-month extension o the Supplementary
Protection Certificate which have been
introduced to offset the additional bur-
den The economic value o the reward
depends on the turnover o the product
concerned In the case o blockbuster
products the amount may be consider-
able while or niche products the effect
is small
An in-depth evaluation o the economic
impact will be included in the 2017 report
in order to draw conclusions on the bal-
ance between burden and rewards and
public health benefits
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1936
19
6Outlook mdash
A fairy-taleending aheadlsquoBetter Medicines or Children mdash From
Concept to Realityrsquo is the title o this re-
port Readers may suggest that based on
the evaluation reerred to above it would
be more appropriate to add a question
mark It is evident that it is too early still
to make a firm statement Despite more
than five years o experience the true im-pact o the Regulation on the health o
children will only become apparent over
time as experience is accumulated in the
longer term
There are encouraging signs though
Paediatric development has become a
more integral part o the overall develop-
ment o medicinal products in the EU A
number o new products with paediatric
indications and age-appropriate pharma-ceutical orms have been authorised and
made available to patients A high num-
ber o agreed paediatric investigation
plans indicates that urther products are
in the pipeline
However it needs to be pointed out that it
would be wrong to expect the Regulation
to be able to solve all problems Instead
it is a major catalyst to improve the situ-
ation o young patients
Finally some weaknesses and deficits
have also become apparent in the last
five years Their impact on the overall
perormance o the Regulation has to be
closely monitored On the basis o the ac-
tions outlined above the Commission in-
tends to fine-tune the current implemen-
tation together with the EMA
Even i better medicines or children are
not yet a reality it should be the ambitiono all stakeholders involved that this piece
o legislation will be or the greater good
o children so that in the 2017 report
the discussion will ocus not on whether a
question mark should be added to the ti-
tle o the report but on whether it should
be an exclamation mark instead
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2036
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2136
21
ANNEXES
Figures and Tables
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2236
22
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2336
23
ANNEX I
Figures and Tables
Table 1Agreed paediatric investigations plans (PIPs) 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Agreed PIPs submitted under Article 7 (without waivers)
Agreed PIPs submitted under Article 8 (without waivers)
Source EMA Paediatric database The numbers on agreed PIPs correspond to EMA decisions
Table 2Agreed paediatric investigations plans (PIPs) compared to ull waivers and modifications 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Submitted modifications of an agreed PIP
Agreed Full waivers
Source EMA Paediatric database The numbers on agreed PIPs and waivers correspond to EMA decisions
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2536
25
Table 5Scientific advice and protocol assistance including ollow-ups (provided by the EMA Scientific Advice Working
Party and the Committee or Human Medicinal Products per year)
259
277321
388 400 433 420
021 32
74 8057
91
0 0 0
68 8067
94
0
100
200
300
400
500
2006 2007 2008 2009 2010 2011 2012
Total number of advice (Scientific Advice and Protocol Assistance)
Sum of paediatric-only and mixed (adult and paediatric development questions)
advice
Paediatric-only or mixed advice that involved a Paediatric Committee member(s) as
expert(s)
Source EMA databases Year o advice letter
Year o start o procedure
Table 6Paediatric clinical trials by year o authorisation
2005 2006 2007 2008 2009 2010 2011 2012
Paediatric trials
(number) 254 316 355 342 404 379 334 332
Paediatric trials
that are part of anagreed PIP 2 1 2 6 16 30 76 76
Proportion of
paediatric trials
that are part of an
agreed PIP among
paediatric trials 1 0 1 2 4 8 23 23
Total number
of trials (adults
and or children) 3 350 3 979 4 749 4 512 4 445 4 026 3 809 3 698
Proportion of
paediatric trials of
all trials 8 8 7 8 9 10 9 9
Source EudraCT Data Warehouse using a predefined query on 6 March 2013 and counting the first authorised trial only in the case o more thanone Member State This partial inormation requires sponsors to use a Clinical Trial Application orm that was only available rom November 2009 or use with version 8 o EudraCT
(available rom 2011)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2636
26
Table 7Number o children to be enrolled in clinical trials
Number
of subjects 2006 2007 2008 2009 2010 2011 2012
Pretermnewborns 0 0 0 207 82 2 281 1 712
Newborns 0 0 5 64 169 1 105 1 172
Infants and
toddlers 330 21 20 59 351 2 788 3 141
Children 2 142 181 200 2 230 2 055 10 325 20 677
Adolescents 368 111 205 1 577 2 861 9 054 13 193
Sum of
above 2 840 313 430 4 137 5 517 25 553 39 895
Reference
number of paediatric
trials 316 355 342 404 379 334 332
Source EudraCT Data Warehouse using a pre-defined query on 6 March 2013 modified by excluding studies or lsquoimmunological medicinal productsrsquo
Table 8EU budget contribution to the Paediatric Regulation and the EMA expenditure
0
1
2
3
4
5
6
7
8
9
10
2006 2007 2008 2009 2010 2011 2012
EU budget contribution (in Million euro)
EMA expenditure for paediatri cs (in Mill ion euro)
EMA expenditure for paediatr ics including support (in Million euro)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2736
27
Table 9Percentage o European Medicines Agencyrsquos human resources working in the paediatric area rom 2006 (inner
circle) to 2012 (outer circle)
733 (2012)
052 (2006)
Table 10Member States acting as rapporteurs or the assessment o studies submitted in accordance with Article 46
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE SE NL FR DK IT BE PL ES NO SK FI IE RO AT HU EL CZ PT LV BG
Study included in worksharing Rapporteur appointed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2836
28
Table 11Member States acting as rapporteur or the assessment o studies submitted in accordance with Article 45
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE NL DK AT FR PL SE ES IE CZ MT IT BE SI EE FI HU NO RO BG EL LV PT IS SK
Wave 1 Wave 2 Wave 3 Wave 4 Wave 5 Wave 6 Wave 7 Wave 8 Wave 9
Wave 10 Wave 11 Wave 12 Wave 13 Wave 14 Wave 15 Wave 16 Wave 17 Wave 18
Table 12Member States acting as rapporteurspeer reviewers in EMArsquos Paediatric Committee procedures (initial PIP
waiver or modification o an agreed PIP)
0
50
100
150
200
250
300
350
400
450
500
A u s t r i a
B el gi um
B ul g a r i a
C y pr u s
C z e c h R e p u b l i c
D enm a r k
E s t oni a
F i nl a n d
F r a n c e
G er m a n y
G r e e c e
H e a l t h c a r e a n d
A c a d emi a
H un g a r y
I c el a n d
I r el a n d
I t a l y
L a t vi a
L i t h u a ni a
L ux em b o ur g
M a l t a
N or w a y
P a t i en t s Or g a ni s a t i on
P ol a n d
P or t u g a l
R om a ni a
S l ov a k i a
S l ov eni a
S p a i n
S w e d en
T h eN e t h er l a n d
s
U ni t e d K i n g d om
Initial PIP applications PIP modifications
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2936
29
ANNEX II
Detailed inventory of centrally authorised medicinalproducts for paediatric use since the entry into force
of the Paediatric Regulation
Table 13Medicinal products authorised centrally since 2007 which include a paediatric indication
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Retapamulin Altargo 2007 No Mixed
Nelarabine Atriance 2007 No Mixed
Human papillomavirus vaccine[types 16 18] Cervarix 2007 No Mixed
Hydroxocobalamin Cyanokit 2007 No Mixed
Idursulase Elaprase 2007 No Mixed
Gadoversetamide Optimark 2007 No Mixed
Betaine anhydrous Cystadane 2007 No Mixed
Stiripentol Diacomit 2007 No Paediatric only
Mecasermin Increlex 2007 No Paediatric only
Rufinamide Inovelon 2007 No Mixed
Hydroxycarbamide Siklos 2007 No Mixed
Human normal
immunoglobulin (ivig) Flebogamma DIF 2007 No Mixed
Fluticasone uroate Avamys 2008 No Mixed
Human normal immunoglobulin Privigen 2008 No Mixed
Lacosamide Vimpat 2008 No Mixed
Micaungin Mycamine 2008 No Mixed
Sapropterin Kuvan 2008 No Mixed
Sugammadex Bridion 2008 No Mixed
Tocoersonal d-alpha
tocopheryl polyethylene glycol
succinate Vedrop 2009 No Paediatric only
Miamurtide Mepact 2009 No Mixed
Rilonacept Rilonacept Regeneron 2009 No Mixed
Tacrolimus Modigra 2009 No Mixed
Pneumoccocal polysaccharideconjugate vaccine (adsorbed) Synflorix 2009 No Paediatric only
Canakinumab
Ilaris (PIP not yet
completed) 2009 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3036
30
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Pneumoccocal polysaccharide
conjugate vaccine (13-valentadsorbed)
Prevenar 13 (PIP not yetcompleted) 2009 Yes Paediatric only
Meningococcal group a c
w135 and y conjugate vaccine Menveo 2010 Yes Mixed
Velaglucerase ala
Vpriv (PIP not yet
completed) 2010 Yes Mixed
Influenza vaccine (live
attenuated nasal) Fluenz (Waiver) 2011 Yes Paediatric only
C1 inhibitor human
Cinryze (PIP not yet
completed) 2011 Yes Mixed
Dihydroartemisinin
piperaquine phosphate
Eurartesim (PIP not yet
completed) 2011 Yes Mixed
Midazolam Buccolam 2011 Yes (PUMA) Paediatric only
EverolimusVotubia(PIP not yet completed) 2011 Yes Mixed
Tobramycin
Tobi Podhaler (PIP not
yet completed) 2011 Yes Mixed
Nomegestrol estradiol Ioa Zoely 2011 Yes Mixed
Colistimethate sodium Colobreathe 2012 Yes Mixed
Mercaptopurine Xaluprine 2012 No Mixed
Catridecacog NovoThirteen 2012 Yes MixedEavirenz Eavirenz Teva 2012 No Mixed
Ivacafor Kalydeco 2012 Yes Mixed
Desloratadine Desloratadine ratiopharm 2012 No Mixed
Desloratadine Desloratadine Actavis 2012 No Mixed
Perampanel Fycompa 2012 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3136
31
Table 14List o centrally authorised medicinal products or which the therapeutic indication was extended to or amend-
ed or the paediatric population
Active substance(s)
Trade
name Date Subject of the extension
Levetiracetam Keppra
2007
2009
Extension o the indication to include adjunctive ther-
apy in the treatment o primary generalised tonic-
clonic (PGTC) seizures in adults and adolescents rom
12 years o age with idiopathic generalised epilepsyExtension o indication to include the adjunctive
treatment o partial seizures with or without second-
ary generalisation in children rom 1 month to lt4
years old
Pneumococcal sac-
charide conjugated
vaccine adsorbed Prevenar 2007
Extension o the indication to include new inorma-
tion on efficacy against disease caused by Strepto-
coccus pneumoniae serotypes 4 6B 9V 14 18C 19F
and 23F in otitis mediaExtension o indication rom active immunisation
against bacteraemic pneumonia to active immunisa-
tion against pneumonia
Infliximab
Remi-
cade 2007
Extension o indication to include treatment o
severe active Crohnrsquos disease in children aged 6 to
17 years
Darbepoetin ala Aranesp 2007
Extension o indication or CRF patients whichrestricted the use o Nespo to paediatric subjects ge
11 years o age
Fosamprenavir Telzir 2007
Extension o indication o Telzir in combination withritonavir or the treatment o Human Immunodefi-
ciency Virus Type 1 (HIV-1) inected adults in combi-nation with other antiretroviral medicinal products to
include paediatric populations
Lamivudine zidovu-
dine Combivir 2007
Extension o indication to include paediatric patients
and replacement o film-coated tablets by scored
film-coated tablets
Desloratadine Aerius 2007Extension o indication rom lsquochronic idiopathic urti-cariarsquo to lsquourticariarsquo
Insulin glulisine Apidra 2007
Extension o indication to include 6 year olds and
older children based on the results o 2 paediatricstudies
Human papilloma virusvaccine [types 6 11
16 18] (recombinantadsorbed) Gardasil 2008
Extension o indication to include the prevention ohigh-grade vaginal dysplastic lesions (VaIN 23)
Adalimumab Humira 20082011
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in adoles-cents rom 13 to 17 years o age
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in the paedi-
atric population aged rom 4 to 12 years
Caspoungin Cancidas 2008
Extension o the indication to include the paediatric
population
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 536
5
1IntroductionlsquoBetter Medicines or Childrenrsquo was the
ambitious title o a consultation papero February 2002 in which the European
Commission presented its vision or regu-
latory actions on paediatric medicinal
products1 At that time many o the prod-
ucts used in children were not specifically
studied or authorised in children Instead
doctors ofen used products authorised
or adults sometimes in different dosag-
es with the associated risks o inefficacy
andor adverse reactions
The consultation paper built on a 5-year
discussion process that started in 1997
with a round table meeting at the prem-
ises o the European Medicines Agency
(EMA) and was the blueprint or the sub-
sequent legislative act It outlined many
o the measures that are to be ound in
the Paediatric Regulation (Regulation (EC)
No 19012006 o the European Parlia-
ment and o the Council on medicinal
products or paediatric use2
hereinaferlsquothe Regulationrsquo)
The Regulation was adopted some five
years afer the consultation paper on 12
December 2006 It entered into orce on
26 January 2007 and its main provisions
were applicable rom 26 July 2008 (Ar-
ticle 7) and 26 January 2009 (Article 8)
respectively
Five years on it is time to take stock o
developments and report to the EuropeanParliament and the Council on the experi-
ence acquired as a result o the Regula-
tion in accordance with its Article 50(2)
Are we already seeing the emergence o
lsquobetter medicines or childrenrsquo
This report does not yet provide compre-
hensive answer as it is subject to certain
limitations it should thereore be regard-
ed as an interim report that presents a
first impression o the experience gainedIn view o the development cycles o me-
dicinal products it will take at least 10
years to gain a ull understanding o the
impact o the legislation This actor has
already been accounted or in the legis-
lation which requires the Commission to
provide a second more comprehensive
report in 2017 which in accordance with
Article 50(3) o the Regulation must in-
clude an analysis o the economic impact
o the rewards and incentives together
with an analysis o the Regulationrsquos im-
plications or public health with a view to
proposing any necessary amendments
However at this stage some analyses and
interim conclusions can be made
This document has been prepared in con-
sultation with Member States the EMA
and interested parties The Commission
particularly values the lsquo5-year Report to
the European Commissionrsquo presenting the
views o the EMA and its Paediatric Com-
mittee3 and the responses to the public
consultation the Commission undertook
at the end o 20124
1 httpeceuropaeuhealthfilespharmacosdocs
doc2002ebcd_pediat-rics_enpd
2 OJ L 378 27122006p 1 amended by Regulation
(EC) No 19022006 o theEuropean Parliament and othe Council o 20 December
2006 OJ L 378 27122006p 20
3 5-year report to theEuropean Commission mdashGeneral report on experience
acquired as a result o theapplication o the Paedi-
atric Regulation preparedby the European MedicinesAgency with its Paediatric
Committee httpeceuropa
euhealthfilespaediat-rics2012-09_pediatric_re-
port-annex1-2_enpd
4 httpeceuropaeuhealth
human-usepaediatric-med-icinesdevelopments2013_
paediatric_pc_enhtm
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 636
6
2The Paediatric
RegulationIn 2010 around 21 o Europeans were
children representing more than 100 mil-
lion people Children represent a vulnera-
ble population group with developmental
physiological and psychological differenc-
es rom adults They are not merely lsquosmall
adultsrsquo Age- and development-related
research and the availability o suitable
medicinal products is consequently par-
ticularly important
Studies carried out beore the Regulation
was adopted showed that over 50 o the
medicines used or children had not been
tested or use in this specific age group
What is more only a limited number o
medicinal products had been developed
specifically with children in mind Com-
panies had already developed a range o
products against a number o diseases
prior to the Paediatric Regulation particu-
larly in sectors such as childhood immuni-sation by means o vaccines However the
availability o child-appropriate medicines
was generally unsatisactory Accordingly
the Regulation was seen as a response to
the absence o sufficient numbers o suit-
able authorised medicinal products with
appropriate dosages and pharmaceutical
orms to treat conditions in children in the
European Union (EU)
There are several reasons or the lacko paediatric medicines It would how-
ever be too simplistic to pin the blame
on pharmaceutical companies or not car-
rying out enough research and develop-
ment (RampD) to adapt medicinal products
to the needs o the paediatric popula-
tion This reluctance has long mirrored a
general social and ethical paradigm that
children should be protected rom clinical
research Only in the last two decades has
there been a shif to the current consen-sus o better protecting children through
clinical research
Economic actors certainly rendered pae-
diatric RampD less attractive in terms o
achieving an adequate return on invest-
ment Children are not a homogenous
sub-group mdash subpopulations range rom
neonates to teenagers with different bio-
logical and pharmacological characteris-
tics Age-appropriate research makes the
process more expensive and complex or
organisations that are active in this sec-
tor
However the absence o specifically
tested products ofen lef healthcare
proessionals with no alternative but to
use products lsquooff-labelrsquo with the associ-
ated non-negligible risks o inefficacy or
adverse reactions Such a situation was
contrary to the general goal to providehigh-quality medicinal products to the en-
tire EU population
To address this problem the Regula-
tion establishes a system o obligations
rewards and incentives together with
horizontal measures to ensure that medi-
cines are regularly researched developed
and authorised to meet the therapeutic
needs o children Other than the Orphan
Regulation5
which is limited to providingvarious incentives the Paediatric Regula-
tion has a direct impact on companiesrsquo
RampD expenditure While not questioning
that medicinal development is company
driven it compels companies to consider
the potential paediatric use o medicinal
products they develop
5 Regulation (EC)Ndeg 1412000 o the Euro-
pean Parliament and theCouncil o 16 December
1999 on orphan medicinalproducts OJ L 18 2212000p 1
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 736
7
The key objectives of theRegulation are
bull to ensure high-quality research into
the development o medicines or
children
bull to ensure over time that the major-ity o medicines used by children are
specifically authorised or such use
with appropriate orms and ormula-
tions
bull to ensure the availability of high-
quality inormation about medicines
used by children
The key measures included inthe Regulation are
bull setting up an expert committee with-
in the EMA the Paediatric Commit-
tee
bull requiring companies to submit dataon the use o a medicine in children
in accordance with an agreed paedi-
atric investigation plan when apply-
ing or marketing authorisation or
medicines and line-extensions or
existing patent-protected medicines
bull a system of waivers from the re-
quirement or medicines unlikely to
benefit children and a system o de-
errals in relation to the timing o the
requirement to ensure that medi-
cines are tested in children only whenit is sae to do so and to prevent the
requirements delaying the authorisa-
tion o medicines or adults
bull a reward for complying with the re-
quirement in the orm o a six-month
extension to the Supplementary Pro-
tection Certificate
bull a reward in respect of orphan medi-
cines or compliance in the orm o
an extra two years o market exclu-
sivity added to the existing ten yearsawarded under the EUrsquos Orphan Reg-
ulation
bull a new type of marketing authorisa-
tion the Paediatric Use Marketing
Authorisation (PUMA) to attract newpaediatric indications or off-patent
products
bull measures to maximise the impact of
existing studies on medicines or chil-
dren
bull an EU inventory of the therapeuticneeds o children to ocus the re-
search development and authorisa-
tion o medicines
bull an EU network of investigators and
trial centres to carry out the required
RampD
bull a system of free scientic advice for
the industry provided by the EMA
bull a public database of paediatric stud-
ies
bull a provision on EU funding for re-search to stimulate the development
and authorisation o off-patent med-
icines or children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 836
8
The Regulation gives the EMA and its
Paediatric Committee primary responsi-
bility or handling paediatric investigation
plans deerrals and waivers This provides
the Agency with concrete decision-mak-
ing powers
The operational costs o the PaediatricRegulation are partly covered by a contri-
bution rom the EU budget (see Table 8)
as its main activities do not attract any
ees For the period 2007-12 the EU
budget contribution amounted to more
than EUR 39 million In addition Member
Statesrsquo national competent authorities
contribute resources in kind especially
staff time or the assessment o paediat-
ric investigation plans (see Table 12)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 936
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1036
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1136
11
cantly (see Table 5) despite the act that
issues o pharmaceutical non-clinical and
clinical development are also part o the
discussions o a paediatric investigation
plan To acilitate collaboration with the
Paediatric Committee joint procedures
have been created within the EMA
413 Clinical trials with children
Medicines or use in children need to be
tested with appropriate ormulations in
the paediatric population to ensure their
sae and effective use Hence it is gener-
ally accepted that the Paediatric Regula-
tion will lead to more clinical trials in chil-
dren The figures in the EudraCT database
have not yet shown an increase in paedi-
atric trials The number remained stablebetween 2006 and 2012 averaging 350
trials per year with some fluctuations (see
Table 6) It should be pointed out how-
ever that while the number o paediat-
ric trials remained stable the number o
clinical trials in all populations decreased
between 2007 and 2011
Moreover until recently EudraCT was lim-
ited to paediatric trials commencing in the
EU Data on paediatric trials that are parto a paediatric investigation plan and con-
ducted outside the EU have only become
publicly available since spring 2011
It should also be noted that the initiation
o a considerable percentage o clinical
trials included in a paediatric investiga-
tion plan has been deerred in order to
avoid delays in the authorisation o the
corresponding product or adults Hence
the impact o the Paediatric Regulation on
paediatric trials will become more appar-
ent in EudraCT in the years to come There
has however been an evident increase in
the number o paediatric study partici-
pants in particular or the age group rom
0 to 23 months who were normally not
included in trials prior to 2008 (see Ta-
ble 7) Allowing neonates and inants to
benefit rom research is a positive sign
as these have been the most neglected
groups so ar
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1236
12
414 Optimised framework and
coordination
The Paediatric Regulation osters a com-
prehensive network o expertise in paedi-
atric matters within the EU In this context
the role o the Paediatric Committee ispivotal as it brings together a high level
o expertise and competence
The Committee has contributed to the
scientific guidelines published by the EMA
and has so ar convened 22 expert work-
shops on the development o medicines
or children
In addition the European Network or
Paediatric Research at the EMA (Enpr-
EMA) was established in 2009 While aclosely-knit network o experts existed
prior to the introduction o the Regula-
tion in disease areas such as paediatric
oncology Enpr-EMA provides the added
value o a holistic approach by bringing
together national and European networks
investigators and centres with specific ex-
pertise in designing and conducting high-
quality studies in children
However question still remain as towhether this expertise translates into su-
ficient capacity within the EU to conduct
trials in specialised investigation settings
Well-developed research networks capa-
ble o acilitating the necessary research
to ulfil the commitments included in
paediatric investigation plans do exist in
some but not all Member States
415 International cooperation
On an international level the EMA has de-veloped international links with medicines
agencies in the United States Canada
and Japan O particular interest is the
cooperation with the US Food and Drug
Administration given that already in the
late 1990s the United States introduced
legislation that stimulated the develop-
ment o medicinal products or paediatric
use by means o a combination o incen-
tives and obligations This cooperation is
also o great interest to stakeholders as
it may give companies the possibility o
satisying the legislation in both regions
with the same studies
In addition the EMA participates actively
in the Paediatric medicines regulatory
network16 which was created in 2010 as
part o the WHOrsquos Better Medicines or
Children initiative
42 More medicines available
for children
Over 12 years (rom 1995 to 2006) 108
o all 317 indications o 262 centrally au-
thorised medicines included the paediat-
ric population Since the Paediatric Regu-
lation entered into orce 31 out o 152
new medicines have been authorised or
paediatric use 10 o which met the con-
ditions o Article 7 This is not more than
a lsquosnapshotrsquo o the effects o the Regula-
tion as this figure is likely to increase inthe uture as a considerable number o
the new already authorised medicines
are subject to an investigation plan where
completion was deerred to avoid delays
in the authorisation o the adult product
It ollows that in the years to come many
more o those 152 new medicines are ex-
pected to be authorised or paediatric use
Annual reports on deerred paediatric
studies o authorised medicines indicate
that the majority o paediatric investiga-tion plans are running to schedule Pae-
diatric research is on-going at the same
rate across therapeutic areas such as on-
cology vaccines and immunology-rheu-
matology-transplantation
Furthermore by the end o 2011 72 new
paediatric indications had been approved
or medicines already authorised includ-
ing 30 indications (18 centralised) arising
rom the obligation in Article 8 Moreover26 new pharmaceutical orms were au-
thorised or paediatric use including 18
adapted orms or centrally authorised
medicines
As ar as Paediatric Use Marketing Au-
thorisation is concerned to date only one
authorisation has been granted This alls
short o initial expectations
16 httpwwwwhointchild-medicinespaediatric_regula-
torsen
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1336
13
A detailed inventory o centrally autho-
rised products is provided in Annex II
Rewards and incentives
Companies that have complied with the
obligations o the Regulation may benefit
rom a reward once the product concerned
is authorised or the product inormation isamended The reward takes the orm o a
6-month extension o the supplementary
protection certificate (SPC) provided or
by Regulation (EC) No 469200917 or in
the case o an orphan medicinal product
by an extension o the ten-year period o
orphan market exclusivity to twelve years
No orphan rewards have been awarded
yet In this regard it is observed that some
companies withdrew the orphan designa-tion o a product in order to qualiy or
the SPC reward rather than the orphan
reward which seems to be more attrac-
tive rom an economic perspective As ar
as SPC extensions are concerned national
patent offices in 16 Member States had
by the end o 2011 granted 6-month ex-
tensions to 11 medicinal products which
resulted in a total o more than 100 na-
tional SPCs
It should be pointed out that a ruling othe European Court o Justice urther
increased the value o the paediatric
reward as it made clear that the initial
certificate could have a negative or zero
duration which could then become posi-
tive once the paediatric extension was
granted18
43 Increased information on
medicines used in childrenTo provide better inormation on the use
o medicinal products in children Article
45 o the Paediatric Regulation requires
companies holding data on the saety
or efficacy o authorised products in the
paediatric population to submit these
studies to the competent authorities In
this way the data can be assessed and
where appropriate the authorised prod-
uct inormation amended Article 46 o
the Regulation also requires companies tosubmit newly generated paediatric data
Since 2008 more than 18 000 study re-
ports on roughly 2 200 medicinal prod-
ucts have been submitted revealing the
large amount o existing paediatric inor-
mation available at company level
These study reports have been and
continue to be assessed by the compe-
tent authorities thanks to an impressive
work-sharing project (see Tables 10 and11) For nationally authorised products
this has led to the publication o assess-
ment reports covering more than 140
active substances and in a considerable
number o cases to recommendations
or changes to the summaries o product
characteristics o authorised products re-
sulting in 65 actual changes For centrally
authorised products by 2011 the Agency
had completed the assessment o all the
data submitted under Article 45 covering55 active substances in 61 centrally ap-
17 Regulation (EC) No4692009 o the Euro-
pean Parliament and othe Council o 6 May 2009
concerning the supplemen-tary protection certificateor medicinal products OJ
L 152 1662009 p 1 ThisRegulation is a codificationo Council Regulation (EEC)
No 176892
18 Case C-12510 Merck
Sharp amp Dohme v DeutschesPatent- und Markenamt notyet published in the ECR
paragraph 37 lsquoi the SPCapplication had to be reused
because the calculationprovided or in Article 13(1)o Regulation No 176892
results in a negative or zero
duration the holder o thebasic patent could not obtain
an extension o protectionconerred by such a patenteven i it conducted all the
studies according to the ap-proved paediatric investiga-
tion plan under Article 36 oRegulation No 19012006Such a reusal would be
liable to adversely impacton the useul effect oRegulation No 19012006
and might jeopardise the
objectives o that regulationnamely the compensation
o effort made to evaluatethe paediatric effects o themedicinal product at issuersquo
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1436
14
proved medicinal products The summa-
ries o product characteristics o 12 me-
dicinal products were changed ollowing
the assessment
5Lessonslearnt51 Better access to
treatment
One o the explicit goals o the Paediatric
Regulation is to increase the number oproducts that are researched developed
and authorised or use in children and
to reduce the off-label use o medicinal
products in the paediatric population
The main tool to achieve this result is to
oblige companies to establish a paediat-
ric investigation plan or each newly de-
veloped product or or the line extension
o an already authorised product that is
still under patent protection The plan ismeant to ensure mdash under the supervi-
sion o the Paediatric Committee mdash that
the necessary data are generated so as
to determine the conditions under which
a medicinal product may be authorised
to treat children Since 2008 more than
600 paediatric investigation plans have
been approved However only a minor-
ity o them has been completed to date
the vast majority are still on-going This
is due to the long development cycles omedicinal products ofen lasting more
than a decade and the near-systematic
deerral o paediatric studies The high
number o deerrals may not have been
initially expected but are currently a real-
ity as or most o the medicinal products
that have been authorised so ar the RampD
programme started beore the entering
into orce o the Regulation Consequent-
ly the paediatric requirements could not
be taken into account rom the beginningo the product development
While the Paediatric Regulation has led
to some new authorisations that include
paediatric indications the regulatory in-
strument is recent and it will probably
take at least a decade beore it can be
judged in terms o its output In terms o
pharmaceutical orms there is however
already a visible positive impact
In this context criticism has been voiced
that the Regulation will ail to ensure abreakthrough in areas o particular pae-
diatric need such as paediatric oncology
This argument is related to the act that
the starting point or the majority o pae-
diatric investigation plans is an ongoing
RampD programme or a medicinal product
or adults An intrinsic consequence o this
approach is that these products primarily
target adult conditions They are devel-
oped in areas where there is a need (or a
market) in the adult population This needin the older population does not neces-
sarily correspond to the paediatric popu-
lationrsquos need
Moreover the Regulation grants waivers
rom its obligations where the disease or
condition or which the specific medicinal
product is intended occurs only in adult
populations This legislative approach cre-
ates riction in the case o diseases that
are specific and exclusive to children Italso limits the powers and possibilities o
the Paediatric Committee when reviewing
and agreeing to a paediatric investigation
plan as regards the scope o studies that
the Committee may request rom appli-
cants ollowing the objective and scien-
tific-based assessment o the compound
concerned19
These constraints and boundaries have to
be taken into account when judging the
impact the Regulation is likely to make In
addition the effect o instruments such as
the Orphan Regulation have to be consid-
ered given that or example all paediatric
cancers are rare diseases and all under
the EU policy ramework on rare diseases
All in all the achievements highlighted in
chapter 4 o this report and the number
o products with new paediatric indica-
tions show that there are some encourag-
ing signs afer this first five-year period it
is however too early or comprehensive
answers
19 Case T-5209 Nycomed vEMA not yet published
See the results o the publicconsultation conducted by
the Commission in prepara-tion o this Report
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1536
15
52 The PUMA concept a
disappointment
The Paediatric Regulation introduced a
new type o marketing authorisation mdash
the Paediatric Use Marketing Authorisa-
tion (PUMA) As an incentive to carry out
research into the potential paediatric use
o off-patent medicinal products that have
been authorised or adults this marketing
authorisation offers 8 years o data and
10 years o market exclusivity to any new
off-patent product developed exclusively
or use in the paediatric population Thus
the main goal o the PUMA concept is to
stimulate research in existing products
This scheme has been supported by EU
unding through the EU Framework Pro-
grammes or Research and Technological
Development
However to date only one PUMA has been
granted with a ew more projects cur-
rently in the pipeline
Neither industry nor academic networks
have embraced this opportunity as ully
as the Regulation intended It would seem
that the incentive o data and market ex-
clusivity does not work or these productsor at least that the market opportunities
in this sector are currently considered in-
sufficient to outweigh the inherent eco-
nomic risks o pharmaceutical develop-
ment Researchers are not engaging in
trials with medicines that have been on
the market or years Companies seem to
ear that market exclusivity will not pre-
vent physicians rom continuing to use
competitor products with the same active
ingredient off-label at lower costs or thatsubstitution or cheaper adult orms takes
place at the level o pharmacies Moreo-
ver national pricing and reimbursement
rules in Member States ofen do not al-
low or the additional research needed to
obtain the PUMA to be rewarded in price
negotiations20
Against this background the PUMA con-
cept has ailed so ar to ulfil the initial
expectationsThe EMA will in uture accept paediatric
investigation plans or a PUMA that cover
only certain age groups and not the en-
tire paediatric population This may offset
some o the reservations that currently
hamper better endorsement o the PUMA
concept
53 No impact on adultdevelopment
Studies prior to the adoption o the Regu-
lation have suggested a theoretical risk
that the requirements or research in chil-
dren could lengthen the overall drug de-
velopment process21 The Regulation has
met this risk head-on In order to avoid
any delays in authorising medicines or
other populations it allows or the grant-
ing o deerrals relating to the initiation orcompletion o some or all o the meas-
ures contained in a paediatric investiga-
tion plan
Experience shows that the deerral is a
widely used instrument which suggests
that the risk o delays in the processing o
adult applications is minimal There have
been some transitional problems in cases
where the adult programme was already
established when the Regulation enteredinto orce but these issues seem to have
been resolved
A concern that was raised initially was
that some companies would become
reluctant to develop new indications
pharmaceutical orms and new routes o
administration in small markets and or
products with low sales to avoid being
bound by the paediatric obligation under
Article 8 o the Regulation However thereis no evidence o such effect Moreover
it may also be argued that the incentive
o a potential six-month extension o the
SPC served to counterbalance such an
effect as it may have led companies to
examine more thoroughly the benefits o
a line extension taking into account the
economic value o the paediatric reward
Still industry stakeholders claim that
in rare cases the development or new
medicinal products has been delayedor abandoned in the expectation or as a
consequence o additional costs and re-
quirements associated with paediatric de-
20 See the results o thepublic consultation con-
ducted by the Commission inpreparation o this Report
21 C Commission StaffWorking Document Proposal
or a Regulation o the Euro-pean Parliament and o theCouncil on medicinal prod-
ucts or paediatric use andamending Council Regulation(EEC) No 17692 Directive
200183EC and Regula-tion (EC) No 7262004Extended impact assessment
(COM2004599F)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1636
16
keting authorisation holders are obliged
to ensure that the product inormation
is kept up to date with the current scien-
tific knowledge While preerence should
be given to cooperative approaches the
enorcement tools may need to be used
i companies do not overcome their res-
ervations
On the whole the requirements o Articles
45 and 46 have provided an efficient and
appropriate instrument or collecting and
evaluating existing paediatric studies
55 Clinical trials with
children
It is generally accepted that the Paediatric
Regulation will lead to more clinical trialswith children but that its aims should be
achieved without subjecting children to
unnecessary clinical trials
The youngest paediatric-age subsets
including neonates are particularly sen-
sitive It will be a constant challenge to
balance the therapeutic needs o these
age groups with their specific vulnerability
when considering and deciding on the ap-
propriateness o specific clinical trials or
the specific settings o studies in this age
subset Efforts are thereore continuously
being made to explore alternative means
eg the use o extrapolation modelling
and simulation techniques to reduce the
number o study subjects as much as
possible The Paediatric Committee is ac-
tively contributing to acilitate the devel-
opment and use o such means including
non-conventional trial design
Another challenge is how to avoid dupli-cating trials or different paediatric inves-
tigation plans rom different applicants
Companies embarking on product devel-
opment in similar areas may be required
by the agreed paediatric investigation
plan to conduct studies within similar
settings While collaborative approaches
between companies would be highly de-
sirable and have occurred on rare occa-
sions they ofen conflict with companiesrsquo
understandable reluctance to share datawith competitors in the early stages o
product development and participate in
direct comparisons This situation could
velopment Overall there is however no
evidence that the Regulation has a con-
siderable negative impact on products or
other populations
Rather there are some concerns that the
requirements under the Regulation may
cause delays in the authorisation o prod-ucts with paediatric-only indications as
they bring added complexity to the RampD
and regulatory process or products that
already directly target children The added
value o the submission o a paediatric in-
vestigation plan in these cases will be as-
sessed urther in the 2017 report
54 Reaping the benefits of
existing information
There was widespread speculation prior to
the adoption o the Paediatric Regulation
as to how many studies would be submit-
ted by pharmaceutical companies in ac-
cordance with Articles 45 and 46 The act
that competent authorities received more
than 18 000 studies reveals the consid-
erable amount o paediatric inormation
that existed at company level
Certainly it is true that not all the inor-
mation submitted met modern require-
ments or scientific data and clinical re-
search and that the work-sharing process
o evaluating the inormation is rather
long and resource intensive
Nevertheless compared to the PUMA con-
cept this scheme proved more successul
in terms o output and in recommending
and implementing changes to the sum-
mary o product characteristics o author-
ised products In its public consultationthe Commission called Articles 45 and 46
the lsquohidden gemsrsquo o the Regulation
One drawback that remains however
is reluctance by marketing authorisa-
tion holders to update the summary o
product characteristics on a voluntary
basis This said the Regulation contains
mechanisms to overcome such reluctance
as it empowers competent authorities to
directly update the summary and varythe marketing authorisation accordingly
Moreover in accordance with Article 23
o Directive 200183EC22 and Article 16
o Regulation (EC) No 726200423 mar-
22 Directive 200183EC othe European Parliament and
o the Council o 6 November2001 on the Community
code relating to medicinalproducts or human use OJ L311 28112001 p 67
23 Regulation (EC) No7262004 o the European
Parliament and o the Coun-cil o 31 March 2004 layingdown Community procedures
or the authorisation andsupervision o medicinalproducts or human and
veterinary use and establish-ing a European Medicines
Agency OJ L 136 3042004p 1
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1736
17
lead to competition among companies to
find investigators and study participants
as well as the duplication o trials which
are unnecessary rom a scientific and
ethical point o view
The Paediatric Committee is able to waive
paediatric trial requirements where thespecific medicinal product does not rep-
resent a significant therapeutic benefit
over an existing treatment or paediatric
patients including once the product is au-
thorised (Article 11) However this option
does not provide a way out in the early
stages o product development where
the Committee has to ensure equal treat-
ment and non-discriminatory approaches
The key to avoiding such unnecessary tri-
als is transparency with regard to ongoingand completed trials The situation contin-
ues to be monitored
Finally it is in the interest o the EU that
paediatric trials stemming rom paedi-
atric investigation plans are conducted
within the EU This has less to do with
the standards under which a trial is con-
ducted given that clinical trials carried
out outside the EU have to meet the ethi-
cal and scientific requirements o the EUprovisions on clinical trials24 than with the
act that studies within the EU may pro-
vide patients there with early access to
innovative medicines To date there is in-
sufficient data on the ratio between pae-
diatric trials conducted within and outside
the EU However in view o the upgraded
unctionalities o the EudraCT database it
is expected that more data will be avail-
able in 2017 or the second report
56 Spreading the news mdash
getting new information
to patients and healthcare
professionals
I the Regulation is to be a success it is
not only necessary that data on the use
o a specific product in the paediatric
population are collected but that these
data are then also appropriately commu-
nicated to and used by paediatricians intheir day-to-day work or the benefit o
their patients
In this regard some studies published in
the medical literature suggest a ailure
on the part o practitioners to recognise
the actual amount o off-label prescrib-
ing to children Moreover it is claimed that
the prescribing habits o practitioners are
ofen strongly influenced by personal ex-
perience rather than by evidence-based
inormation or paediatric medicine25
These studies in making generalisations
may not have taken into account the het-
erogeneity o healthcare proessionals
whose receptiveness varies greatly ac-
cording to their work setting and specific
area o specialisation At the same time
such observations may point to a sub-
stantial hurdle in achieving the goal o the
Paediatric Regulation
National competent authorities as well as
organisations or healthcare proessionals
seem particularly qualified to consider ap-
propriate ways o ensuring an adequate
flow o inormation Some Member States
have already established a number o
tools to communicate effectively and e-
ficiently with healthcare proessionals
eg by means o regular meetings web-
based inormation distribution systems ornational ormularies
57 Is the burden greater
than rewards
There can be no doubt that the Paediat-
ric Regulation places a considerable ad-
ditional burden on pharmaceutical com-
panies with its obligations regarding
research on products or use in children
However this approach was adopted be-cause market orces alone proved insu-
ficient to stimulate adequate research
The Regulation requires companies to
submit paediatric investigation plans at
an early stage o product development
However research on some active sub-
stances may be discontinued at later
stages should urther studies ail to show
potential with respect to the saety and
efficacy o the product For every success-
ul authorised medicinal product there aremany that ail to make the finishing line
Hence not all approved paediatric investi-
gation plans will be completed as compa-
24 Directive 200120EC othe European Parliament
and o the Council on theapproximation o the laws
regulations and administra-tive provisions o the Mem-ber States relating to the
implementation o good clini-cal practice in the conducto clinical trials on medicinal
products or human use OJ L121 152001 p 34
25 5-year report to theEuropean Commission (seeootnote 3) page 41
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1836
18
nies may decide to stop the correspond-
ing adult development It is too early still
to obtain reliable statistics that show
the ratio between completed and non-
completed paediatric investigation plans
but in the current context not all approved
plans will eventually result in an approved
medicine with a paediatric indication
In terms o output this entails some un-
necessary effort in compiling and screen-
ing paediatric investigation plans To what
extent this is offset by the benefit o early
submission which ensures that the pae-
diatric development fits smoothly into the
overall product development need ur-
ther monitoring
A urther point o concern is the highnumber o modifications to paediat-
ric investigation plans Figures seem to
suggest that nearly all plans have to
be modified at least once Conceptually
though this does not come as a surprise
in view o the early submission o pae-
diatric investigation plans the length o
adult and paediatric developments and
the substantial deerrals granted An
RampD plan requently has to be adapted
or amended to take account o initial re-sults Recruitment problems or necessary
design changes in the trials may also lead
to modifications While it is acknowledged
that substantial amendments or modifi-
cations to the plan have to be subject to
discussions with the Paediatric Commit-
tee this is less obvious or minor changes
In this context the level o detail required
by the EMA has been repeatedly criticised
In the past five years the EMA and its
Paediatric Committee have made effortsto provide or some flexibility in the plan
so to allow a margin o manoeuvre that
takes account o uncertainties in relation
to certain parameters o a trial
In any case the Commission intends to
review its Communication on the ormat
and content o applications or agree-
ment or modification o a paediatric in-
vestigation plan to take into account the
experience gained including the consider-
able number o modification requests
On a positive note it can be noted that
companies are applying or the rewards
provided by the Regulation primarily the
6-month extension o the Supplementary
Protection Certificate which have been
introduced to offset the additional bur-
den The economic value o the reward
depends on the turnover o the product
concerned In the case o blockbuster
products the amount may be consider-
able while or niche products the effect
is small
An in-depth evaluation o the economic
impact will be included in the 2017 report
in order to draw conclusions on the bal-
ance between burden and rewards and
public health benefits
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1936
19
6Outlook mdash
A fairy-taleending aheadlsquoBetter Medicines or Children mdash From
Concept to Realityrsquo is the title o this re-
port Readers may suggest that based on
the evaluation reerred to above it would
be more appropriate to add a question
mark It is evident that it is too early still
to make a firm statement Despite more
than five years o experience the true im-pact o the Regulation on the health o
children will only become apparent over
time as experience is accumulated in the
longer term
There are encouraging signs though
Paediatric development has become a
more integral part o the overall develop-
ment o medicinal products in the EU A
number o new products with paediatric
indications and age-appropriate pharma-ceutical orms have been authorised and
made available to patients A high num-
ber o agreed paediatric investigation
plans indicates that urther products are
in the pipeline
However it needs to be pointed out that it
would be wrong to expect the Regulation
to be able to solve all problems Instead
it is a major catalyst to improve the situ-
ation o young patients
Finally some weaknesses and deficits
have also become apparent in the last
five years Their impact on the overall
perormance o the Regulation has to be
closely monitored On the basis o the ac-
tions outlined above the Commission in-
tends to fine-tune the current implemen-
tation together with the EMA
Even i better medicines or children are
not yet a reality it should be the ambitiono all stakeholders involved that this piece
o legislation will be or the greater good
o children so that in the 2017 report
the discussion will ocus not on whether a
question mark should be added to the ti-
tle o the report but on whether it should
be an exclamation mark instead
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2036
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2136
21
ANNEXES
Figures and Tables
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2236
22
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2336
23
ANNEX I
Figures and Tables
Table 1Agreed paediatric investigations plans (PIPs) 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Agreed PIPs submitted under Article 7 (without waivers)
Agreed PIPs submitted under Article 8 (without waivers)
Source EMA Paediatric database The numbers on agreed PIPs correspond to EMA decisions
Table 2Agreed paediatric investigations plans (PIPs) compared to ull waivers and modifications 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Submitted modifications of an agreed PIP
Agreed Full waivers
Source EMA Paediatric database The numbers on agreed PIPs and waivers correspond to EMA decisions
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2536
25
Table 5Scientific advice and protocol assistance including ollow-ups (provided by the EMA Scientific Advice Working
Party and the Committee or Human Medicinal Products per year)
259
277321
388 400 433 420
021 32
74 8057
91
0 0 0
68 8067
94
0
100
200
300
400
500
2006 2007 2008 2009 2010 2011 2012
Total number of advice (Scientific Advice and Protocol Assistance)
Sum of paediatric-only and mixed (adult and paediatric development questions)
advice
Paediatric-only or mixed advice that involved a Paediatric Committee member(s) as
expert(s)
Source EMA databases Year o advice letter
Year o start o procedure
Table 6Paediatric clinical trials by year o authorisation
2005 2006 2007 2008 2009 2010 2011 2012
Paediatric trials
(number) 254 316 355 342 404 379 334 332
Paediatric trials
that are part of anagreed PIP 2 1 2 6 16 30 76 76
Proportion of
paediatric trials
that are part of an
agreed PIP among
paediatric trials 1 0 1 2 4 8 23 23
Total number
of trials (adults
and or children) 3 350 3 979 4 749 4 512 4 445 4 026 3 809 3 698
Proportion of
paediatric trials of
all trials 8 8 7 8 9 10 9 9
Source EudraCT Data Warehouse using a predefined query on 6 March 2013 and counting the first authorised trial only in the case o more thanone Member State This partial inormation requires sponsors to use a Clinical Trial Application orm that was only available rom November 2009 or use with version 8 o EudraCT
(available rom 2011)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2636
26
Table 7Number o children to be enrolled in clinical trials
Number
of subjects 2006 2007 2008 2009 2010 2011 2012
Pretermnewborns 0 0 0 207 82 2 281 1 712
Newborns 0 0 5 64 169 1 105 1 172
Infants and
toddlers 330 21 20 59 351 2 788 3 141
Children 2 142 181 200 2 230 2 055 10 325 20 677
Adolescents 368 111 205 1 577 2 861 9 054 13 193
Sum of
above 2 840 313 430 4 137 5 517 25 553 39 895
Reference
number of paediatric
trials 316 355 342 404 379 334 332
Source EudraCT Data Warehouse using a pre-defined query on 6 March 2013 modified by excluding studies or lsquoimmunological medicinal productsrsquo
Table 8EU budget contribution to the Paediatric Regulation and the EMA expenditure
0
1
2
3
4
5
6
7
8
9
10
2006 2007 2008 2009 2010 2011 2012
EU budget contribution (in Million euro)
EMA expenditure for paediatri cs (in Mill ion euro)
EMA expenditure for paediatr ics including support (in Million euro)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2736
27
Table 9Percentage o European Medicines Agencyrsquos human resources working in the paediatric area rom 2006 (inner
circle) to 2012 (outer circle)
733 (2012)
052 (2006)
Table 10Member States acting as rapporteurs or the assessment o studies submitted in accordance with Article 46
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE SE NL FR DK IT BE PL ES NO SK FI IE RO AT HU EL CZ PT LV BG
Study included in worksharing Rapporteur appointed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2836
28
Table 11Member States acting as rapporteur or the assessment o studies submitted in accordance with Article 45
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE NL DK AT FR PL SE ES IE CZ MT IT BE SI EE FI HU NO RO BG EL LV PT IS SK
Wave 1 Wave 2 Wave 3 Wave 4 Wave 5 Wave 6 Wave 7 Wave 8 Wave 9
Wave 10 Wave 11 Wave 12 Wave 13 Wave 14 Wave 15 Wave 16 Wave 17 Wave 18
Table 12Member States acting as rapporteurspeer reviewers in EMArsquos Paediatric Committee procedures (initial PIP
waiver or modification o an agreed PIP)
0
50
100
150
200
250
300
350
400
450
500
A u s t r i a
B el gi um
B ul g a r i a
C y pr u s
C z e c h R e p u b l i c
D enm a r k
E s t oni a
F i nl a n d
F r a n c e
G er m a n y
G r e e c e
H e a l t h c a r e a n d
A c a d emi a
H un g a r y
I c el a n d
I r el a n d
I t a l y
L a t vi a
L i t h u a ni a
L ux em b o ur g
M a l t a
N or w a y
P a t i en t s Or g a ni s a t i on
P ol a n d
P or t u g a l
R om a ni a
S l ov a k i a
S l ov eni a
S p a i n
S w e d en
T h eN e t h er l a n d
s
U ni t e d K i n g d om
Initial PIP applications PIP modifications
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2936
29
ANNEX II
Detailed inventory of centrally authorised medicinalproducts for paediatric use since the entry into force
of the Paediatric Regulation
Table 13Medicinal products authorised centrally since 2007 which include a paediatric indication
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Retapamulin Altargo 2007 No Mixed
Nelarabine Atriance 2007 No Mixed
Human papillomavirus vaccine[types 16 18] Cervarix 2007 No Mixed
Hydroxocobalamin Cyanokit 2007 No Mixed
Idursulase Elaprase 2007 No Mixed
Gadoversetamide Optimark 2007 No Mixed
Betaine anhydrous Cystadane 2007 No Mixed
Stiripentol Diacomit 2007 No Paediatric only
Mecasermin Increlex 2007 No Paediatric only
Rufinamide Inovelon 2007 No Mixed
Hydroxycarbamide Siklos 2007 No Mixed
Human normal
immunoglobulin (ivig) Flebogamma DIF 2007 No Mixed
Fluticasone uroate Avamys 2008 No Mixed
Human normal immunoglobulin Privigen 2008 No Mixed
Lacosamide Vimpat 2008 No Mixed
Micaungin Mycamine 2008 No Mixed
Sapropterin Kuvan 2008 No Mixed
Sugammadex Bridion 2008 No Mixed
Tocoersonal d-alpha
tocopheryl polyethylene glycol
succinate Vedrop 2009 No Paediatric only
Miamurtide Mepact 2009 No Mixed
Rilonacept Rilonacept Regeneron 2009 No Mixed
Tacrolimus Modigra 2009 No Mixed
Pneumoccocal polysaccharideconjugate vaccine (adsorbed) Synflorix 2009 No Paediatric only
Canakinumab
Ilaris (PIP not yet
completed) 2009 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3036
30
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Pneumoccocal polysaccharide
conjugate vaccine (13-valentadsorbed)
Prevenar 13 (PIP not yetcompleted) 2009 Yes Paediatric only
Meningococcal group a c
w135 and y conjugate vaccine Menveo 2010 Yes Mixed
Velaglucerase ala
Vpriv (PIP not yet
completed) 2010 Yes Mixed
Influenza vaccine (live
attenuated nasal) Fluenz (Waiver) 2011 Yes Paediatric only
C1 inhibitor human
Cinryze (PIP not yet
completed) 2011 Yes Mixed
Dihydroartemisinin
piperaquine phosphate
Eurartesim (PIP not yet
completed) 2011 Yes Mixed
Midazolam Buccolam 2011 Yes (PUMA) Paediatric only
EverolimusVotubia(PIP not yet completed) 2011 Yes Mixed
Tobramycin
Tobi Podhaler (PIP not
yet completed) 2011 Yes Mixed
Nomegestrol estradiol Ioa Zoely 2011 Yes Mixed
Colistimethate sodium Colobreathe 2012 Yes Mixed
Mercaptopurine Xaluprine 2012 No Mixed
Catridecacog NovoThirteen 2012 Yes MixedEavirenz Eavirenz Teva 2012 No Mixed
Ivacafor Kalydeco 2012 Yes Mixed
Desloratadine Desloratadine ratiopharm 2012 No Mixed
Desloratadine Desloratadine Actavis 2012 No Mixed
Perampanel Fycompa 2012 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3136
31
Table 14List o centrally authorised medicinal products or which the therapeutic indication was extended to or amend-
ed or the paediatric population
Active substance(s)
Trade
name Date Subject of the extension
Levetiracetam Keppra
2007
2009
Extension o the indication to include adjunctive ther-
apy in the treatment o primary generalised tonic-
clonic (PGTC) seizures in adults and adolescents rom
12 years o age with idiopathic generalised epilepsyExtension o indication to include the adjunctive
treatment o partial seizures with or without second-
ary generalisation in children rom 1 month to lt4
years old
Pneumococcal sac-
charide conjugated
vaccine adsorbed Prevenar 2007
Extension o the indication to include new inorma-
tion on efficacy against disease caused by Strepto-
coccus pneumoniae serotypes 4 6B 9V 14 18C 19F
and 23F in otitis mediaExtension o indication rom active immunisation
against bacteraemic pneumonia to active immunisa-
tion against pneumonia
Infliximab
Remi-
cade 2007
Extension o indication to include treatment o
severe active Crohnrsquos disease in children aged 6 to
17 years
Darbepoetin ala Aranesp 2007
Extension o indication or CRF patients whichrestricted the use o Nespo to paediatric subjects ge
11 years o age
Fosamprenavir Telzir 2007
Extension o indication o Telzir in combination withritonavir or the treatment o Human Immunodefi-
ciency Virus Type 1 (HIV-1) inected adults in combi-nation with other antiretroviral medicinal products to
include paediatric populations
Lamivudine zidovu-
dine Combivir 2007
Extension o indication to include paediatric patients
and replacement o film-coated tablets by scored
film-coated tablets
Desloratadine Aerius 2007Extension o indication rom lsquochronic idiopathic urti-cariarsquo to lsquourticariarsquo
Insulin glulisine Apidra 2007
Extension o indication to include 6 year olds and
older children based on the results o 2 paediatricstudies
Human papilloma virusvaccine [types 6 11
16 18] (recombinantadsorbed) Gardasil 2008
Extension o indication to include the prevention ohigh-grade vaginal dysplastic lesions (VaIN 23)
Adalimumab Humira 20082011
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in adoles-cents rom 13 to 17 years o age
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in the paedi-
atric population aged rom 4 to 12 years
Caspoungin Cancidas 2008
Extension o the indication to include the paediatric
population
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 536
5
1IntroductionlsquoBetter Medicines or Childrenrsquo was the
ambitious title o a consultation papero February 2002 in which the European
Commission presented its vision or regu-
latory actions on paediatric medicinal
products1 At that time many o the prod-
ucts used in children were not specifically
studied or authorised in children Instead
doctors ofen used products authorised
or adults sometimes in different dosag-
es with the associated risks o inefficacy
andor adverse reactions
The consultation paper built on a 5-year
discussion process that started in 1997
with a round table meeting at the prem-
ises o the European Medicines Agency
(EMA) and was the blueprint or the sub-
sequent legislative act It outlined many
o the measures that are to be ound in
the Paediatric Regulation (Regulation (EC)
No 19012006 o the European Parlia-
ment and o the Council on medicinal
products or paediatric use2
hereinaferlsquothe Regulationrsquo)
The Regulation was adopted some five
years afer the consultation paper on 12
December 2006 It entered into orce on
26 January 2007 and its main provisions
were applicable rom 26 July 2008 (Ar-
ticle 7) and 26 January 2009 (Article 8)
respectively
Five years on it is time to take stock o
developments and report to the EuropeanParliament and the Council on the experi-
ence acquired as a result o the Regula-
tion in accordance with its Article 50(2)
Are we already seeing the emergence o
lsquobetter medicines or childrenrsquo
This report does not yet provide compre-
hensive answer as it is subject to certain
limitations it should thereore be regard-
ed as an interim report that presents a
first impression o the experience gainedIn view o the development cycles o me-
dicinal products it will take at least 10
years to gain a ull understanding o the
impact o the legislation This actor has
already been accounted or in the legis-
lation which requires the Commission to
provide a second more comprehensive
report in 2017 which in accordance with
Article 50(3) o the Regulation must in-
clude an analysis o the economic impact
o the rewards and incentives together
with an analysis o the Regulationrsquos im-
plications or public health with a view to
proposing any necessary amendments
However at this stage some analyses and
interim conclusions can be made
This document has been prepared in con-
sultation with Member States the EMA
and interested parties The Commission
particularly values the lsquo5-year Report to
the European Commissionrsquo presenting the
views o the EMA and its Paediatric Com-
mittee3 and the responses to the public
consultation the Commission undertook
at the end o 20124
1 httpeceuropaeuhealthfilespharmacosdocs
doc2002ebcd_pediat-rics_enpd
2 OJ L 378 27122006p 1 amended by Regulation
(EC) No 19022006 o theEuropean Parliament and othe Council o 20 December
2006 OJ L 378 27122006p 20
3 5-year report to theEuropean Commission mdashGeneral report on experience
acquired as a result o theapplication o the Paedi-
atric Regulation preparedby the European MedicinesAgency with its Paediatric
Committee httpeceuropa
euhealthfilespaediat-rics2012-09_pediatric_re-
port-annex1-2_enpd
4 httpeceuropaeuhealth
human-usepaediatric-med-icinesdevelopments2013_
paediatric_pc_enhtm
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 636
6
2The Paediatric
RegulationIn 2010 around 21 o Europeans were
children representing more than 100 mil-
lion people Children represent a vulnera-
ble population group with developmental
physiological and psychological differenc-
es rom adults They are not merely lsquosmall
adultsrsquo Age- and development-related
research and the availability o suitable
medicinal products is consequently par-
ticularly important
Studies carried out beore the Regulation
was adopted showed that over 50 o the
medicines used or children had not been
tested or use in this specific age group
What is more only a limited number o
medicinal products had been developed
specifically with children in mind Com-
panies had already developed a range o
products against a number o diseases
prior to the Paediatric Regulation particu-
larly in sectors such as childhood immuni-sation by means o vaccines However the
availability o child-appropriate medicines
was generally unsatisactory Accordingly
the Regulation was seen as a response to
the absence o sufficient numbers o suit-
able authorised medicinal products with
appropriate dosages and pharmaceutical
orms to treat conditions in children in the
European Union (EU)
There are several reasons or the lacko paediatric medicines It would how-
ever be too simplistic to pin the blame
on pharmaceutical companies or not car-
rying out enough research and develop-
ment (RampD) to adapt medicinal products
to the needs o the paediatric popula-
tion This reluctance has long mirrored a
general social and ethical paradigm that
children should be protected rom clinical
research Only in the last two decades has
there been a shif to the current consen-sus o better protecting children through
clinical research
Economic actors certainly rendered pae-
diatric RampD less attractive in terms o
achieving an adequate return on invest-
ment Children are not a homogenous
sub-group mdash subpopulations range rom
neonates to teenagers with different bio-
logical and pharmacological characteris-
tics Age-appropriate research makes the
process more expensive and complex or
organisations that are active in this sec-
tor
However the absence o specifically
tested products ofen lef healthcare
proessionals with no alternative but to
use products lsquooff-labelrsquo with the associ-
ated non-negligible risks o inefficacy or
adverse reactions Such a situation was
contrary to the general goal to providehigh-quality medicinal products to the en-
tire EU population
To address this problem the Regula-
tion establishes a system o obligations
rewards and incentives together with
horizontal measures to ensure that medi-
cines are regularly researched developed
and authorised to meet the therapeutic
needs o children Other than the Orphan
Regulation5
which is limited to providingvarious incentives the Paediatric Regula-
tion has a direct impact on companiesrsquo
RampD expenditure While not questioning
that medicinal development is company
driven it compels companies to consider
the potential paediatric use o medicinal
products they develop
5 Regulation (EC)Ndeg 1412000 o the Euro-
pean Parliament and theCouncil o 16 December
1999 on orphan medicinalproducts OJ L 18 2212000p 1
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 736
7
The key objectives of theRegulation are
bull to ensure high-quality research into
the development o medicines or
children
bull to ensure over time that the major-ity o medicines used by children are
specifically authorised or such use
with appropriate orms and ormula-
tions
bull to ensure the availability of high-
quality inormation about medicines
used by children
The key measures included inthe Regulation are
bull setting up an expert committee with-
in the EMA the Paediatric Commit-
tee
bull requiring companies to submit dataon the use o a medicine in children
in accordance with an agreed paedi-
atric investigation plan when apply-
ing or marketing authorisation or
medicines and line-extensions or
existing patent-protected medicines
bull a system of waivers from the re-
quirement or medicines unlikely to
benefit children and a system o de-
errals in relation to the timing o the
requirement to ensure that medi-
cines are tested in children only whenit is sae to do so and to prevent the
requirements delaying the authorisa-
tion o medicines or adults
bull a reward for complying with the re-
quirement in the orm o a six-month
extension to the Supplementary Pro-
tection Certificate
bull a reward in respect of orphan medi-
cines or compliance in the orm o
an extra two years o market exclu-
sivity added to the existing ten yearsawarded under the EUrsquos Orphan Reg-
ulation
bull a new type of marketing authorisa-
tion the Paediatric Use Marketing
Authorisation (PUMA) to attract newpaediatric indications or off-patent
products
bull measures to maximise the impact of
existing studies on medicines or chil-
dren
bull an EU inventory of the therapeuticneeds o children to ocus the re-
search development and authorisa-
tion o medicines
bull an EU network of investigators and
trial centres to carry out the required
RampD
bull a system of free scientic advice for
the industry provided by the EMA
bull a public database of paediatric stud-
ies
bull a provision on EU funding for re-search to stimulate the development
and authorisation o off-patent med-
icines or children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 836
8
The Regulation gives the EMA and its
Paediatric Committee primary responsi-
bility or handling paediatric investigation
plans deerrals and waivers This provides
the Agency with concrete decision-mak-
ing powers
The operational costs o the PaediatricRegulation are partly covered by a contri-
bution rom the EU budget (see Table 8)
as its main activities do not attract any
ees For the period 2007-12 the EU
budget contribution amounted to more
than EUR 39 million In addition Member
Statesrsquo national competent authorities
contribute resources in kind especially
staff time or the assessment o paediat-
ric investigation plans (see Table 12)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 936
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1036
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1136
11
cantly (see Table 5) despite the act that
issues o pharmaceutical non-clinical and
clinical development are also part o the
discussions o a paediatric investigation
plan To acilitate collaboration with the
Paediatric Committee joint procedures
have been created within the EMA
413 Clinical trials with children
Medicines or use in children need to be
tested with appropriate ormulations in
the paediatric population to ensure their
sae and effective use Hence it is gener-
ally accepted that the Paediatric Regula-
tion will lead to more clinical trials in chil-
dren The figures in the EudraCT database
have not yet shown an increase in paedi-
atric trials The number remained stablebetween 2006 and 2012 averaging 350
trials per year with some fluctuations (see
Table 6) It should be pointed out how-
ever that while the number o paediat-
ric trials remained stable the number o
clinical trials in all populations decreased
between 2007 and 2011
Moreover until recently EudraCT was lim-
ited to paediatric trials commencing in the
EU Data on paediatric trials that are parto a paediatric investigation plan and con-
ducted outside the EU have only become
publicly available since spring 2011
It should also be noted that the initiation
o a considerable percentage o clinical
trials included in a paediatric investiga-
tion plan has been deerred in order to
avoid delays in the authorisation o the
corresponding product or adults Hence
the impact o the Paediatric Regulation on
paediatric trials will become more appar-
ent in EudraCT in the years to come There
has however been an evident increase in
the number o paediatric study partici-
pants in particular or the age group rom
0 to 23 months who were normally not
included in trials prior to 2008 (see Ta-
ble 7) Allowing neonates and inants to
benefit rom research is a positive sign
as these have been the most neglected
groups so ar
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1236
12
414 Optimised framework and
coordination
The Paediatric Regulation osters a com-
prehensive network o expertise in paedi-
atric matters within the EU In this context
the role o the Paediatric Committee ispivotal as it brings together a high level
o expertise and competence
The Committee has contributed to the
scientific guidelines published by the EMA
and has so ar convened 22 expert work-
shops on the development o medicines
or children
In addition the European Network or
Paediatric Research at the EMA (Enpr-
EMA) was established in 2009 While aclosely-knit network o experts existed
prior to the introduction o the Regula-
tion in disease areas such as paediatric
oncology Enpr-EMA provides the added
value o a holistic approach by bringing
together national and European networks
investigators and centres with specific ex-
pertise in designing and conducting high-
quality studies in children
However question still remain as towhether this expertise translates into su-
ficient capacity within the EU to conduct
trials in specialised investigation settings
Well-developed research networks capa-
ble o acilitating the necessary research
to ulfil the commitments included in
paediatric investigation plans do exist in
some but not all Member States
415 International cooperation
On an international level the EMA has de-veloped international links with medicines
agencies in the United States Canada
and Japan O particular interest is the
cooperation with the US Food and Drug
Administration given that already in the
late 1990s the United States introduced
legislation that stimulated the develop-
ment o medicinal products or paediatric
use by means o a combination o incen-
tives and obligations This cooperation is
also o great interest to stakeholders as
it may give companies the possibility o
satisying the legislation in both regions
with the same studies
In addition the EMA participates actively
in the Paediatric medicines regulatory
network16 which was created in 2010 as
part o the WHOrsquos Better Medicines or
Children initiative
42 More medicines available
for children
Over 12 years (rom 1995 to 2006) 108
o all 317 indications o 262 centrally au-
thorised medicines included the paediat-
ric population Since the Paediatric Regu-
lation entered into orce 31 out o 152
new medicines have been authorised or
paediatric use 10 o which met the con-
ditions o Article 7 This is not more than
a lsquosnapshotrsquo o the effects o the Regula-
tion as this figure is likely to increase inthe uture as a considerable number o
the new already authorised medicines
are subject to an investigation plan where
completion was deerred to avoid delays
in the authorisation o the adult product
It ollows that in the years to come many
more o those 152 new medicines are ex-
pected to be authorised or paediatric use
Annual reports on deerred paediatric
studies o authorised medicines indicate
that the majority o paediatric investiga-tion plans are running to schedule Pae-
diatric research is on-going at the same
rate across therapeutic areas such as on-
cology vaccines and immunology-rheu-
matology-transplantation
Furthermore by the end o 2011 72 new
paediatric indications had been approved
or medicines already authorised includ-
ing 30 indications (18 centralised) arising
rom the obligation in Article 8 Moreover26 new pharmaceutical orms were au-
thorised or paediatric use including 18
adapted orms or centrally authorised
medicines
As ar as Paediatric Use Marketing Au-
thorisation is concerned to date only one
authorisation has been granted This alls
short o initial expectations
16 httpwwwwhointchild-medicinespaediatric_regula-
torsen
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1336
13
A detailed inventory o centrally autho-
rised products is provided in Annex II
Rewards and incentives
Companies that have complied with the
obligations o the Regulation may benefit
rom a reward once the product concerned
is authorised or the product inormation isamended The reward takes the orm o a
6-month extension o the supplementary
protection certificate (SPC) provided or
by Regulation (EC) No 469200917 or in
the case o an orphan medicinal product
by an extension o the ten-year period o
orphan market exclusivity to twelve years
No orphan rewards have been awarded
yet In this regard it is observed that some
companies withdrew the orphan designa-tion o a product in order to qualiy or
the SPC reward rather than the orphan
reward which seems to be more attrac-
tive rom an economic perspective As ar
as SPC extensions are concerned national
patent offices in 16 Member States had
by the end o 2011 granted 6-month ex-
tensions to 11 medicinal products which
resulted in a total o more than 100 na-
tional SPCs
It should be pointed out that a ruling othe European Court o Justice urther
increased the value o the paediatric
reward as it made clear that the initial
certificate could have a negative or zero
duration which could then become posi-
tive once the paediatric extension was
granted18
43 Increased information on
medicines used in childrenTo provide better inormation on the use
o medicinal products in children Article
45 o the Paediatric Regulation requires
companies holding data on the saety
or efficacy o authorised products in the
paediatric population to submit these
studies to the competent authorities In
this way the data can be assessed and
where appropriate the authorised prod-
uct inormation amended Article 46 o
the Regulation also requires companies tosubmit newly generated paediatric data
Since 2008 more than 18 000 study re-
ports on roughly 2 200 medicinal prod-
ucts have been submitted revealing the
large amount o existing paediatric inor-
mation available at company level
These study reports have been and
continue to be assessed by the compe-
tent authorities thanks to an impressive
work-sharing project (see Tables 10 and11) For nationally authorised products
this has led to the publication o assess-
ment reports covering more than 140
active substances and in a considerable
number o cases to recommendations
or changes to the summaries o product
characteristics o authorised products re-
sulting in 65 actual changes For centrally
authorised products by 2011 the Agency
had completed the assessment o all the
data submitted under Article 45 covering55 active substances in 61 centrally ap-
17 Regulation (EC) No4692009 o the Euro-
pean Parliament and othe Council o 6 May 2009
concerning the supplemen-tary protection certificateor medicinal products OJ
L 152 1662009 p 1 ThisRegulation is a codificationo Council Regulation (EEC)
No 176892
18 Case C-12510 Merck
Sharp amp Dohme v DeutschesPatent- und Markenamt notyet published in the ECR
paragraph 37 lsquoi the SPCapplication had to be reused
because the calculationprovided or in Article 13(1)o Regulation No 176892
results in a negative or zero
duration the holder o thebasic patent could not obtain
an extension o protectionconerred by such a patenteven i it conducted all the
studies according to the ap-proved paediatric investiga-
tion plan under Article 36 oRegulation No 19012006Such a reusal would be
liable to adversely impacton the useul effect oRegulation No 19012006
and might jeopardise the
objectives o that regulationnamely the compensation
o effort made to evaluatethe paediatric effects o themedicinal product at issuersquo
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1436
14
proved medicinal products The summa-
ries o product characteristics o 12 me-
dicinal products were changed ollowing
the assessment
5Lessonslearnt51 Better access to
treatment
One o the explicit goals o the Paediatric
Regulation is to increase the number oproducts that are researched developed
and authorised or use in children and
to reduce the off-label use o medicinal
products in the paediatric population
The main tool to achieve this result is to
oblige companies to establish a paediat-
ric investigation plan or each newly de-
veloped product or or the line extension
o an already authorised product that is
still under patent protection The plan ismeant to ensure mdash under the supervi-
sion o the Paediatric Committee mdash that
the necessary data are generated so as
to determine the conditions under which
a medicinal product may be authorised
to treat children Since 2008 more than
600 paediatric investigation plans have
been approved However only a minor-
ity o them has been completed to date
the vast majority are still on-going This
is due to the long development cycles omedicinal products ofen lasting more
than a decade and the near-systematic
deerral o paediatric studies The high
number o deerrals may not have been
initially expected but are currently a real-
ity as or most o the medicinal products
that have been authorised so ar the RampD
programme started beore the entering
into orce o the Regulation Consequent-
ly the paediatric requirements could not
be taken into account rom the beginningo the product development
While the Paediatric Regulation has led
to some new authorisations that include
paediatric indications the regulatory in-
strument is recent and it will probably
take at least a decade beore it can be
judged in terms o its output In terms o
pharmaceutical orms there is however
already a visible positive impact
In this context criticism has been voiced
that the Regulation will ail to ensure abreakthrough in areas o particular pae-
diatric need such as paediatric oncology
This argument is related to the act that
the starting point or the majority o pae-
diatric investigation plans is an ongoing
RampD programme or a medicinal product
or adults An intrinsic consequence o this
approach is that these products primarily
target adult conditions They are devel-
oped in areas where there is a need (or a
market) in the adult population This needin the older population does not neces-
sarily correspond to the paediatric popu-
lationrsquos need
Moreover the Regulation grants waivers
rom its obligations where the disease or
condition or which the specific medicinal
product is intended occurs only in adult
populations This legislative approach cre-
ates riction in the case o diseases that
are specific and exclusive to children Italso limits the powers and possibilities o
the Paediatric Committee when reviewing
and agreeing to a paediatric investigation
plan as regards the scope o studies that
the Committee may request rom appli-
cants ollowing the objective and scien-
tific-based assessment o the compound
concerned19
These constraints and boundaries have to
be taken into account when judging the
impact the Regulation is likely to make In
addition the effect o instruments such as
the Orphan Regulation have to be consid-
ered given that or example all paediatric
cancers are rare diseases and all under
the EU policy ramework on rare diseases
All in all the achievements highlighted in
chapter 4 o this report and the number
o products with new paediatric indica-
tions show that there are some encourag-
ing signs afer this first five-year period it
is however too early or comprehensive
answers
19 Case T-5209 Nycomed vEMA not yet published
See the results o the publicconsultation conducted by
the Commission in prepara-tion o this Report
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1536
15
52 The PUMA concept a
disappointment
The Paediatric Regulation introduced a
new type o marketing authorisation mdash
the Paediatric Use Marketing Authorisa-
tion (PUMA) As an incentive to carry out
research into the potential paediatric use
o off-patent medicinal products that have
been authorised or adults this marketing
authorisation offers 8 years o data and
10 years o market exclusivity to any new
off-patent product developed exclusively
or use in the paediatric population Thus
the main goal o the PUMA concept is to
stimulate research in existing products
This scheme has been supported by EU
unding through the EU Framework Pro-
grammes or Research and Technological
Development
However to date only one PUMA has been
granted with a ew more projects cur-
rently in the pipeline
Neither industry nor academic networks
have embraced this opportunity as ully
as the Regulation intended It would seem
that the incentive o data and market ex-
clusivity does not work or these productsor at least that the market opportunities
in this sector are currently considered in-
sufficient to outweigh the inherent eco-
nomic risks o pharmaceutical develop-
ment Researchers are not engaging in
trials with medicines that have been on
the market or years Companies seem to
ear that market exclusivity will not pre-
vent physicians rom continuing to use
competitor products with the same active
ingredient off-label at lower costs or thatsubstitution or cheaper adult orms takes
place at the level o pharmacies Moreo-
ver national pricing and reimbursement
rules in Member States ofen do not al-
low or the additional research needed to
obtain the PUMA to be rewarded in price
negotiations20
Against this background the PUMA con-
cept has ailed so ar to ulfil the initial
expectationsThe EMA will in uture accept paediatric
investigation plans or a PUMA that cover
only certain age groups and not the en-
tire paediatric population This may offset
some o the reservations that currently
hamper better endorsement o the PUMA
concept
53 No impact on adultdevelopment
Studies prior to the adoption o the Regu-
lation have suggested a theoretical risk
that the requirements or research in chil-
dren could lengthen the overall drug de-
velopment process21 The Regulation has
met this risk head-on In order to avoid
any delays in authorising medicines or
other populations it allows or the grant-
ing o deerrals relating to the initiation orcompletion o some or all o the meas-
ures contained in a paediatric investiga-
tion plan
Experience shows that the deerral is a
widely used instrument which suggests
that the risk o delays in the processing o
adult applications is minimal There have
been some transitional problems in cases
where the adult programme was already
established when the Regulation enteredinto orce but these issues seem to have
been resolved
A concern that was raised initially was
that some companies would become
reluctant to develop new indications
pharmaceutical orms and new routes o
administration in small markets and or
products with low sales to avoid being
bound by the paediatric obligation under
Article 8 o the Regulation However thereis no evidence o such effect Moreover
it may also be argued that the incentive
o a potential six-month extension o the
SPC served to counterbalance such an
effect as it may have led companies to
examine more thoroughly the benefits o
a line extension taking into account the
economic value o the paediatric reward
Still industry stakeholders claim that
in rare cases the development or new
medicinal products has been delayedor abandoned in the expectation or as a
consequence o additional costs and re-
quirements associated with paediatric de-
20 See the results o thepublic consultation con-
ducted by the Commission inpreparation o this Report
21 C Commission StaffWorking Document Proposal
or a Regulation o the Euro-pean Parliament and o theCouncil on medicinal prod-
ucts or paediatric use andamending Council Regulation(EEC) No 17692 Directive
200183EC and Regula-tion (EC) No 7262004Extended impact assessment
(COM2004599F)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1636
16
keting authorisation holders are obliged
to ensure that the product inormation
is kept up to date with the current scien-
tific knowledge While preerence should
be given to cooperative approaches the
enorcement tools may need to be used
i companies do not overcome their res-
ervations
On the whole the requirements o Articles
45 and 46 have provided an efficient and
appropriate instrument or collecting and
evaluating existing paediatric studies
55 Clinical trials with
children
It is generally accepted that the Paediatric
Regulation will lead to more clinical trialswith children but that its aims should be
achieved without subjecting children to
unnecessary clinical trials
The youngest paediatric-age subsets
including neonates are particularly sen-
sitive It will be a constant challenge to
balance the therapeutic needs o these
age groups with their specific vulnerability
when considering and deciding on the ap-
propriateness o specific clinical trials or
the specific settings o studies in this age
subset Efforts are thereore continuously
being made to explore alternative means
eg the use o extrapolation modelling
and simulation techniques to reduce the
number o study subjects as much as
possible The Paediatric Committee is ac-
tively contributing to acilitate the devel-
opment and use o such means including
non-conventional trial design
Another challenge is how to avoid dupli-cating trials or different paediatric inves-
tigation plans rom different applicants
Companies embarking on product devel-
opment in similar areas may be required
by the agreed paediatric investigation
plan to conduct studies within similar
settings While collaborative approaches
between companies would be highly de-
sirable and have occurred on rare occa-
sions they ofen conflict with companiesrsquo
understandable reluctance to share datawith competitors in the early stages o
product development and participate in
direct comparisons This situation could
velopment Overall there is however no
evidence that the Regulation has a con-
siderable negative impact on products or
other populations
Rather there are some concerns that the
requirements under the Regulation may
cause delays in the authorisation o prod-ucts with paediatric-only indications as
they bring added complexity to the RampD
and regulatory process or products that
already directly target children The added
value o the submission o a paediatric in-
vestigation plan in these cases will be as-
sessed urther in the 2017 report
54 Reaping the benefits of
existing information
There was widespread speculation prior to
the adoption o the Paediatric Regulation
as to how many studies would be submit-
ted by pharmaceutical companies in ac-
cordance with Articles 45 and 46 The act
that competent authorities received more
than 18 000 studies reveals the consid-
erable amount o paediatric inormation
that existed at company level
Certainly it is true that not all the inor-
mation submitted met modern require-
ments or scientific data and clinical re-
search and that the work-sharing process
o evaluating the inormation is rather
long and resource intensive
Nevertheless compared to the PUMA con-
cept this scheme proved more successul
in terms o output and in recommending
and implementing changes to the sum-
mary o product characteristics o author-
ised products In its public consultationthe Commission called Articles 45 and 46
the lsquohidden gemsrsquo o the Regulation
One drawback that remains however
is reluctance by marketing authorisa-
tion holders to update the summary o
product characteristics on a voluntary
basis This said the Regulation contains
mechanisms to overcome such reluctance
as it empowers competent authorities to
directly update the summary and varythe marketing authorisation accordingly
Moreover in accordance with Article 23
o Directive 200183EC22 and Article 16
o Regulation (EC) No 726200423 mar-
22 Directive 200183EC othe European Parliament and
o the Council o 6 November2001 on the Community
code relating to medicinalproducts or human use OJ L311 28112001 p 67
23 Regulation (EC) No7262004 o the European
Parliament and o the Coun-cil o 31 March 2004 layingdown Community procedures
or the authorisation andsupervision o medicinalproducts or human and
veterinary use and establish-ing a European Medicines
Agency OJ L 136 3042004p 1
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1736
17
lead to competition among companies to
find investigators and study participants
as well as the duplication o trials which
are unnecessary rom a scientific and
ethical point o view
The Paediatric Committee is able to waive
paediatric trial requirements where thespecific medicinal product does not rep-
resent a significant therapeutic benefit
over an existing treatment or paediatric
patients including once the product is au-
thorised (Article 11) However this option
does not provide a way out in the early
stages o product development where
the Committee has to ensure equal treat-
ment and non-discriminatory approaches
The key to avoiding such unnecessary tri-
als is transparency with regard to ongoingand completed trials The situation contin-
ues to be monitored
Finally it is in the interest o the EU that
paediatric trials stemming rom paedi-
atric investigation plans are conducted
within the EU This has less to do with
the standards under which a trial is con-
ducted given that clinical trials carried
out outside the EU have to meet the ethi-
cal and scientific requirements o the EUprovisions on clinical trials24 than with the
act that studies within the EU may pro-
vide patients there with early access to
innovative medicines To date there is in-
sufficient data on the ratio between pae-
diatric trials conducted within and outside
the EU However in view o the upgraded
unctionalities o the EudraCT database it
is expected that more data will be avail-
able in 2017 or the second report
56 Spreading the news mdash
getting new information
to patients and healthcare
professionals
I the Regulation is to be a success it is
not only necessary that data on the use
o a specific product in the paediatric
population are collected but that these
data are then also appropriately commu-
nicated to and used by paediatricians intheir day-to-day work or the benefit o
their patients
In this regard some studies published in
the medical literature suggest a ailure
on the part o practitioners to recognise
the actual amount o off-label prescrib-
ing to children Moreover it is claimed that
the prescribing habits o practitioners are
ofen strongly influenced by personal ex-
perience rather than by evidence-based
inormation or paediatric medicine25
These studies in making generalisations
may not have taken into account the het-
erogeneity o healthcare proessionals
whose receptiveness varies greatly ac-
cording to their work setting and specific
area o specialisation At the same time
such observations may point to a sub-
stantial hurdle in achieving the goal o the
Paediatric Regulation
National competent authorities as well as
organisations or healthcare proessionals
seem particularly qualified to consider ap-
propriate ways o ensuring an adequate
flow o inormation Some Member States
have already established a number o
tools to communicate effectively and e-
ficiently with healthcare proessionals
eg by means o regular meetings web-
based inormation distribution systems ornational ormularies
57 Is the burden greater
than rewards
There can be no doubt that the Paediat-
ric Regulation places a considerable ad-
ditional burden on pharmaceutical com-
panies with its obligations regarding
research on products or use in children
However this approach was adopted be-cause market orces alone proved insu-
ficient to stimulate adequate research
The Regulation requires companies to
submit paediatric investigation plans at
an early stage o product development
However research on some active sub-
stances may be discontinued at later
stages should urther studies ail to show
potential with respect to the saety and
efficacy o the product For every success-
ul authorised medicinal product there aremany that ail to make the finishing line
Hence not all approved paediatric investi-
gation plans will be completed as compa-
24 Directive 200120EC othe European Parliament
and o the Council on theapproximation o the laws
regulations and administra-tive provisions o the Mem-ber States relating to the
implementation o good clini-cal practice in the conducto clinical trials on medicinal
products or human use OJ L121 152001 p 34
25 5-year report to theEuropean Commission (seeootnote 3) page 41
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1836
18
nies may decide to stop the correspond-
ing adult development It is too early still
to obtain reliable statistics that show
the ratio between completed and non-
completed paediatric investigation plans
but in the current context not all approved
plans will eventually result in an approved
medicine with a paediatric indication
In terms o output this entails some un-
necessary effort in compiling and screen-
ing paediatric investigation plans To what
extent this is offset by the benefit o early
submission which ensures that the pae-
diatric development fits smoothly into the
overall product development need ur-
ther monitoring
A urther point o concern is the highnumber o modifications to paediat-
ric investigation plans Figures seem to
suggest that nearly all plans have to
be modified at least once Conceptually
though this does not come as a surprise
in view o the early submission o pae-
diatric investigation plans the length o
adult and paediatric developments and
the substantial deerrals granted An
RampD plan requently has to be adapted
or amended to take account o initial re-sults Recruitment problems or necessary
design changes in the trials may also lead
to modifications While it is acknowledged
that substantial amendments or modifi-
cations to the plan have to be subject to
discussions with the Paediatric Commit-
tee this is less obvious or minor changes
In this context the level o detail required
by the EMA has been repeatedly criticised
In the past five years the EMA and its
Paediatric Committee have made effortsto provide or some flexibility in the plan
so to allow a margin o manoeuvre that
takes account o uncertainties in relation
to certain parameters o a trial
In any case the Commission intends to
review its Communication on the ormat
and content o applications or agree-
ment or modification o a paediatric in-
vestigation plan to take into account the
experience gained including the consider-
able number o modification requests
On a positive note it can be noted that
companies are applying or the rewards
provided by the Regulation primarily the
6-month extension o the Supplementary
Protection Certificate which have been
introduced to offset the additional bur-
den The economic value o the reward
depends on the turnover o the product
concerned In the case o blockbuster
products the amount may be consider-
able while or niche products the effect
is small
An in-depth evaluation o the economic
impact will be included in the 2017 report
in order to draw conclusions on the bal-
ance between burden and rewards and
public health benefits
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1936
19
6Outlook mdash
A fairy-taleending aheadlsquoBetter Medicines or Children mdash From
Concept to Realityrsquo is the title o this re-
port Readers may suggest that based on
the evaluation reerred to above it would
be more appropriate to add a question
mark It is evident that it is too early still
to make a firm statement Despite more
than five years o experience the true im-pact o the Regulation on the health o
children will only become apparent over
time as experience is accumulated in the
longer term
There are encouraging signs though
Paediatric development has become a
more integral part o the overall develop-
ment o medicinal products in the EU A
number o new products with paediatric
indications and age-appropriate pharma-ceutical orms have been authorised and
made available to patients A high num-
ber o agreed paediatric investigation
plans indicates that urther products are
in the pipeline
However it needs to be pointed out that it
would be wrong to expect the Regulation
to be able to solve all problems Instead
it is a major catalyst to improve the situ-
ation o young patients
Finally some weaknesses and deficits
have also become apparent in the last
five years Their impact on the overall
perormance o the Regulation has to be
closely monitored On the basis o the ac-
tions outlined above the Commission in-
tends to fine-tune the current implemen-
tation together with the EMA
Even i better medicines or children are
not yet a reality it should be the ambitiono all stakeholders involved that this piece
o legislation will be or the greater good
o children so that in the 2017 report
the discussion will ocus not on whether a
question mark should be added to the ti-
tle o the report but on whether it should
be an exclamation mark instead
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2036
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2136
21
ANNEXES
Figures and Tables
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2236
22
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2336
23
ANNEX I
Figures and Tables
Table 1Agreed paediatric investigations plans (PIPs) 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Agreed PIPs submitted under Article 7 (without waivers)
Agreed PIPs submitted under Article 8 (without waivers)
Source EMA Paediatric database The numbers on agreed PIPs correspond to EMA decisions
Table 2Agreed paediatric investigations plans (PIPs) compared to ull waivers and modifications 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Submitted modifications of an agreed PIP
Agreed Full waivers
Source EMA Paediatric database The numbers on agreed PIPs and waivers correspond to EMA decisions
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2536
25
Table 5Scientific advice and protocol assistance including ollow-ups (provided by the EMA Scientific Advice Working
Party and the Committee or Human Medicinal Products per year)
259
277321
388 400 433 420
021 32
74 8057
91
0 0 0
68 8067
94
0
100
200
300
400
500
2006 2007 2008 2009 2010 2011 2012
Total number of advice (Scientific Advice and Protocol Assistance)
Sum of paediatric-only and mixed (adult and paediatric development questions)
advice
Paediatric-only or mixed advice that involved a Paediatric Committee member(s) as
expert(s)
Source EMA databases Year o advice letter
Year o start o procedure
Table 6Paediatric clinical trials by year o authorisation
2005 2006 2007 2008 2009 2010 2011 2012
Paediatric trials
(number) 254 316 355 342 404 379 334 332
Paediatric trials
that are part of anagreed PIP 2 1 2 6 16 30 76 76
Proportion of
paediatric trials
that are part of an
agreed PIP among
paediatric trials 1 0 1 2 4 8 23 23
Total number
of trials (adults
and or children) 3 350 3 979 4 749 4 512 4 445 4 026 3 809 3 698
Proportion of
paediatric trials of
all trials 8 8 7 8 9 10 9 9
Source EudraCT Data Warehouse using a predefined query on 6 March 2013 and counting the first authorised trial only in the case o more thanone Member State This partial inormation requires sponsors to use a Clinical Trial Application orm that was only available rom November 2009 or use with version 8 o EudraCT
(available rom 2011)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2636
26
Table 7Number o children to be enrolled in clinical trials
Number
of subjects 2006 2007 2008 2009 2010 2011 2012
Pretermnewborns 0 0 0 207 82 2 281 1 712
Newborns 0 0 5 64 169 1 105 1 172
Infants and
toddlers 330 21 20 59 351 2 788 3 141
Children 2 142 181 200 2 230 2 055 10 325 20 677
Adolescents 368 111 205 1 577 2 861 9 054 13 193
Sum of
above 2 840 313 430 4 137 5 517 25 553 39 895
Reference
number of paediatric
trials 316 355 342 404 379 334 332
Source EudraCT Data Warehouse using a pre-defined query on 6 March 2013 modified by excluding studies or lsquoimmunological medicinal productsrsquo
Table 8EU budget contribution to the Paediatric Regulation and the EMA expenditure
0
1
2
3
4
5
6
7
8
9
10
2006 2007 2008 2009 2010 2011 2012
EU budget contribution (in Million euro)
EMA expenditure for paediatri cs (in Mill ion euro)
EMA expenditure for paediatr ics including support (in Million euro)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2736
27
Table 9Percentage o European Medicines Agencyrsquos human resources working in the paediatric area rom 2006 (inner
circle) to 2012 (outer circle)
733 (2012)
052 (2006)
Table 10Member States acting as rapporteurs or the assessment o studies submitted in accordance with Article 46
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE SE NL FR DK IT BE PL ES NO SK FI IE RO AT HU EL CZ PT LV BG
Study included in worksharing Rapporteur appointed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2836
28
Table 11Member States acting as rapporteur or the assessment o studies submitted in accordance with Article 45
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE NL DK AT FR PL SE ES IE CZ MT IT BE SI EE FI HU NO RO BG EL LV PT IS SK
Wave 1 Wave 2 Wave 3 Wave 4 Wave 5 Wave 6 Wave 7 Wave 8 Wave 9
Wave 10 Wave 11 Wave 12 Wave 13 Wave 14 Wave 15 Wave 16 Wave 17 Wave 18
Table 12Member States acting as rapporteurspeer reviewers in EMArsquos Paediatric Committee procedures (initial PIP
waiver or modification o an agreed PIP)
0
50
100
150
200
250
300
350
400
450
500
A u s t r i a
B el gi um
B ul g a r i a
C y pr u s
C z e c h R e p u b l i c
D enm a r k
E s t oni a
F i nl a n d
F r a n c e
G er m a n y
G r e e c e
H e a l t h c a r e a n d
A c a d emi a
H un g a r y
I c el a n d
I r el a n d
I t a l y
L a t vi a
L i t h u a ni a
L ux em b o ur g
M a l t a
N or w a y
P a t i en t s Or g a ni s a t i on
P ol a n d
P or t u g a l
R om a ni a
S l ov a k i a
S l ov eni a
S p a i n
S w e d en
T h eN e t h er l a n d
s
U ni t e d K i n g d om
Initial PIP applications PIP modifications
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2936
29
ANNEX II
Detailed inventory of centrally authorised medicinalproducts for paediatric use since the entry into force
of the Paediatric Regulation
Table 13Medicinal products authorised centrally since 2007 which include a paediatric indication
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Retapamulin Altargo 2007 No Mixed
Nelarabine Atriance 2007 No Mixed
Human papillomavirus vaccine[types 16 18] Cervarix 2007 No Mixed
Hydroxocobalamin Cyanokit 2007 No Mixed
Idursulase Elaprase 2007 No Mixed
Gadoversetamide Optimark 2007 No Mixed
Betaine anhydrous Cystadane 2007 No Mixed
Stiripentol Diacomit 2007 No Paediatric only
Mecasermin Increlex 2007 No Paediatric only
Rufinamide Inovelon 2007 No Mixed
Hydroxycarbamide Siklos 2007 No Mixed
Human normal
immunoglobulin (ivig) Flebogamma DIF 2007 No Mixed
Fluticasone uroate Avamys 2008 No Mixed
Human normal immunoglobulin Privigen 2008 No Mixed
Lacosamide Vimpat 2008 No Mixed
Micaungin Mycamine 2008 No Mixed
Sapropterin Kuvan 2008 No Mixed
Sugammadex Bridion 2008 No Mixed
Tocoersonal d-alpha
tocopheryl polyethylene glycol
succinate Vedrop 2009 No Paediatric only
Miamurtide Mepact 2009 No Mixed
Rilonacept Rilonacept Regeneron 2009 No Mixed
Tacrolimus Modigra 2009 No Mixed
Pneumoccocal polysaccharideconjugate vaccine (adsorbed) Synflorix 2009 No Paediatric only
Canakinumab
Ilaris (PIP not yet
completed) 2009 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3036
30
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Pneumoccocal polysaccharide
conjugate vaccine (13-valentadsorbed)
Prevenar 13 (PIP not yetcompleted) 2009 Yes Paediatric only
Meningococcal group a c
w135 and y conjugate vaccine Menveo 2010 Yes Mixed
Velaglucerase ala
Vpriv (PIP not yet
completed) 2010 Yes Mixed
Influenza vaccine (live
attenuated nasal) Fluenz (Waiver) 2011 Yes Paediatric only
C1 inhibitor human
Cinryze (PIP not yet
completed) 2011 Yes Mixed
Dihydroartemisinin
piperaquine phosphate
Eurartesim (PIP not yet
completed) 2011 Yes Mixed
Midazolam Buccolam 2011 Yes (PUMA) Paediatric only
EverolimusVotubia(PIP not yet completed) 2011 Yes Mixed
Tobramycin
Tobi Podhaler (PIP not
yet completed) 2011 Yes Mixed
Nomegestrol estradiol Ioa Zoely 2011 Yes Mixed
Colistimethate sodium Colobreathe 2012 Yes Mixed
Mercaptopurine Xaluprine 2012 No Mixed
Catridecacog NovoThirteen 2012 Yes MixedEavirenz Eavirenz Teva 2012 No Mixed
Ivacafor Kalydeco 2012 Yes Mixed
Desloratadine Desloratadine ratiopharm 2012 No Mixed
Desloratadine Desloratadine Actavis 2012 No Mixed
Perampanel Fycompa 2012 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3136
31
Table 14List o centrally authorised medicinal products or which the therapeutic indication was extended to or amend-
ed or the paediatric population
Active substance(s)
Trade
name Date Subject of the extension
Levetiracetam Keppra
2007
2009
Extension o the indication to include adjunctive ther-
apy in the treatment o primary generalised tonic-
clonic (PGTC) seizures in adults and adolescents rom
12 years o age with idiopathic generalised epilepsyExtension o indication to include the adjunctive
treatment o partial seizures with or without second-
ary generalisation in children rom 1 month to lt4
years old
Pneumococcal sac-
charide conjugated
vaccine adsorbed Prevenar 2007
Extension o the indication to include new inorma-
tion on efficacy against disease caused by Strepto-
coccus pneumoniae serotypes 4 6B 9V 14 18C 19F
and 23F in otitis mediaExtension o indication rom active immunisation
against bacteraemic pneumonia to active immunisa-
tion against pneumonia
Infliximab
Remi-
cade 2007
Extension o indication to include treatment o
severe active Crohnrsquos disease in children aged 6 to
17 years
Darbepoetin ala Aranesp 2007
Extension o indication or CRF patients whichrestricted the use o Nespo to paediatric subjects ge
11 years o age
Fosamprenavir Telzir 2007
Extension o indication o Telzir in combination withritonavir or the treatment o Human Immunodefi-
ciency Virus Type 1 (HIV-1) inected adults in combi-nation with other antiretroviral medicinal products to
include paediatric populations
Lamivudine zidovu-
dine Combivir 2007
Extension o indication to include paediatric patients
and replacement o film-coated tablets by scored
film-coated tablets
Desloratadine Aerius 2007Extension o indication rom lsquochronic idiopathic urti-cariarsquo to lsquourticariarsquo
Insulin glulisine Apidra 2007
Extension o indication to include 6 year olds and
older children based on the results o 2 paediatricstudies
Human papilloma virusvaccine [types 6 11
16 18] (recombinantadsorbed) Gardasil 2008
Extension o indication to include the prevention ohigh-grade vaginal dysplastic lesions (VaIN 23)
Adalimumab Humira 20082011
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in adoles-cents rom 13 to 17 years o age
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in the paedi-
atric population aged rom 4 to 12 years
Caspoungin Cancidas 2008
Extension o the indication to include the paediatric
population
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 636
6
2The Paediatric
RegulationIn 2010 around 21 o Europeans were
children representing more than 100 mil-
lion people Children represent a vulnera-
ble population group with developmental
physiological and psychological differenc-
es rom adults They are not merely lsquosmall
adultsrsquo Age- and development-related
research and the availability o suitable
medicinal products is consequently par-
ticularly important
Studies carried out beore the Regulation
was adopted showed that over 50 o the
medicines used or children had not been
tested or use in this specific age group
What is more only a limited number o
medicinal products had been developed
specifically with children in mind Com-
panies had already developed a range o
products against a number o diseases
prior to the Paediatric Regulation particu-
larly in sectors such as childhood immuni-sation by means o vaccines However the
availability o child-appropriate medicines
was generally unsatisactory Accordingly
the Regulation was seen as a response to
the absence o sufficient numbers o suit-
able authorised medicinal products with
appropriate dosages and pharmaceutical
orms to treat conditions in children in the
European Union (EU)
There are several reasons or the lacko paediatric medicines It would how-
ever be too simplistic to pin the blame
on pharmaceutical companies or not car-
rying out enough research and develop-
ment (RampD) to adapt medicinal products
to the needs o the paediatric popula-
tion This reluctance has long mirrored a
general social and ethical paradigm that
children should be protected rom clinical
research Only in the last two decades has
there been a shif to the current consen-sus o better protecting children through
clinical research
Economic actors certainly rendered pae-
diatric RampD less attractive in terms o
achieving an adequate return on invest-
ment Children are not a homogenous
sub-group mdash subpopulations range rom
neonates to teenagers with different bio-
logical and pharmacological characteris-
tics Age-appropriate research makes the
process more expensive and complex or
organisations that are active in this sec-
tor
However the absence o specifically
tested products ofen lef healthcare
proessionals with no alternative but to
use products lsquooff-labelrsquo with the associ-
ated non-negligible risks o inefficacy or
adverse reactions Such a situation was
contrary to the general goal to providehigh-quality medicinal products to the en-
tire EU population
To address this problem the Regula-
tion establishes a system o obligations
rewards and incentives together with
horizontal measures to ensure that medi-
cines are regularly researched developed
and authorised to meet the therapeutic
needs o children Other than the Orphan
Regulation5
which is limited to providingvarious incentives the Paediatric Regula-
tion has a direct impact on companiesrsquo
RampD expenditure While not questioning
that medicinal development is company
driven it compels companies to consider
the potential paediatric use o medicinal
products they develop
5 Regulation (EC)Ndeg 1412000 o the Euro-
pean Parliament and theCouncil o 16 December
1999 on orphan medicinalproducts OJ L 18 2212000p 1
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 736
7
The key objectives of theRegulation are
bull to ensure high-quality research into
the development o medicines or
children
bull to ensure over time that the major-ity o medicines used by children are
specifically authorised or such use
with appropriate orms and ormula-
tions
bull to ensure the availability of high-
quality inormation about medicines
used by children
The key measures included inthe Regulation are
bull setting up an expert committee with-
in the EMA the Paediatric Commit-
tee
bull requiring companies to submit dataon the use o a medicine in children
in accordance with an agreed paedi-
atric investigation plan when apply-
ing or marketing authorisation or
medicines and line-extensions or
existing patent-protected medicines
bull a system of waivers from the re-
quirement or medicines unlikely to
benefit children and a system o de-
errals in relation to the timing o the
requirement to ensure that medi-
cines are tested in children only whenit is sae to do so and to prevent the
requirements delaying the authorisa-
tion o medicines or adults
bull a reward for complying with the re-
quirement in the orm o a six-month
extension to the Supplementary Pro-
tection Certificate
bull a reward in respect of orphan medi-
cines or compliance in the orm o
an extra two years o market exclu-
sivity added to the existing ten yearsawarded under the EUrsquos Orphan Reg-
ulation
bull a new type of marketing authorisa-
tion the Paediatric Use Marketing
Authorisation (PUMA) to attract newpaediatric indications or off-patent
products
bull measures to maximise the impact of
existing studies on medicines or chil-
dren
bull an EU inventory of the therapeuticneeds o children to ocus the re-
search development and authorisa-
tion o medicines
bull an EU network of investigators and
trial centres to carry out the required
RampD
bull a system of free scientic advice for
the industry provided by the EMA
bull a public database of paediatric stud-
ies
bull a provision on EU funding for re-search to stimulate the development
and authorisation o off-patent med-
icines or children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 836
8
The Regulation gives the EMA and its
Paediatric Committee primary responsi-
bility or handling paediatric investigation
plans deerrals and waivers This provides
the Agency with concrete decision-mak-
ing powers
The operational costs o the PaediatricRegulation are partly covered by a contri-
bution rom the EU budget (see Table 8)
as its main activities do not attract any
ees For the period 2007-12 the EU
budget contribution amounted to more
than EUR 39 million In addition Member
Statesrsquo national competent authorities
contribute resources in kind especially
staff time or the assessment o paediat-
ric investigation plans (see Table 12)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 936
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1036
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1136
11
cantly (see Table 5) despite the act that
issues o pharmaceutical non-clinical and
clinical development are also part o the
discussions o a paediatric investigation
plan To acilitate collaboration with the
Paediatric Committee joint procedures
have been created within the EMA
413 Clinical trials with children
Medicines or use in children need to be
tested with appropriate ormulations in
the paediatric population to ensure their
sae and effective use Hence it is gener-
ally accepted that the Paediatric Regula-
tion will lead to more clinical trials in chil-
dren The figures in the EudraCT database
have not yet shown an increase in paedi-
atric trials The number remained stablebetween 2006 and 2012 averaging 350
trials per year with some fluctuations (see
Table 6) It should be pointed out how-
ever that while the number o paediat-
ric trials remained stable the number o
clinical trials in all populations decreased
between 2007 and 2011
Moreover until recently EudraCT was lim-
ited to paediatric trials commencing in the
EU Data on paediatric trials that are parto a paediatric investigation plan and con-
ducted outside the EU have only become
publicly available since spring 2011
It should also be noted that the initiation
o a considerable percentage o clinical
trials included in a paediatric investiga-
tion plan has been deerred in order to
avoid delays in the authorisation o the
corresponding product or adults Hence
the impact o the Paediatric Regulation on
paediatric trials will become more appar-
ent in EudraCT in the years to come There
has however been an evident increase in
the number o paediatric study partici-
pants in particular or the age group rom
0 to 23 months who were normally not
included in trials prior to 2008 (see Ta-
ble 7) Allowing neonates and inants to
benefit rom research is a positive sign
as these have been the most neglected
groups so ar
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1236
12
414 Optimised framework and
coordination
The Paediatric Regulation osters a com-
prehensive network o expertise in paedi-
atric matters within the EU In this context
the role o the Paediatric Committee ispivotal as it brings together a high level
o expertise and competence
The Committee has contributed to the
scientific guidelines published by the EMA
and has so ar convened 22 expert work-
shops on the development o medicines
or children
In addition the European Network or
Paediatric Research at the EMA (Enpr-
EMA) was established in 2009 While aclosely-knit network o experts existed
prior to the introduction o the Regula-
tion in disease areas such as paediatric
oncology Enpr-EMA provides the added
value o a holistic approach by bringing
together national and European networks
investigators and centres with specific ex-
pertise in designing and conducting high-
quality studies in children
However question still remain as towhether this expertise translates into su-
ficient capacity within the EU to conduct
trials in specialised investigation settings
Well-developed research networks capa-
ble o acilitating the necessary research
to ulfil the commitments included in
paediatric investigation plans do exist in
some but not all Member States
415 International cooperation
On an international level the EMA has de-veloped international links with medicines
agencies in the United States Canada
and Japan O particular interest is the
cooperation with the US Food and Drug
Administration given that already in the
late 1990s the United States introduced
legislation that stimulated the develop-
ment o medicinal products or paediatric
use by means o a combination o incen-
tives and obligations This cooperation is
also o great interest to stakeholders as
it may give companies the possibility o
satisying the legislation in both regions
with the same studies
In addition the EMA participates actively
in the Paediatric medicines regulatory
network16 which was created in 2010 as
part o the WHOrsquos Better Medicines or
Children initiative
42 More medicines available
for children
Over 12 years (rom 1995 to 2006) 108
o all 317 indications o 262 centrally au-
thorised medicines included the paediat-
ric population Since the Paediatric Regu-
lation entered into orce 31 out o 152
new medicines have been authorised or
paediatric use 10 o which met the con-
ditions o Article 7 This is not more than
a lsquosnapshotrsquo o the effects o the Regula-
tion as this figure is likely to increase inthe uture as a considerable number o
the new already authorised medicines
are subject to an investigation plan where
completion was deerred to avoid delays
in the authorisation o the adult product
It ollows that in the years to come many
more o those 152 new medicines are ex-
pected to be authorised or paediatric use
Annual reports on deerred paediatric
studies o authorised medicines indicate
that the majority o paediatric investiga-tion plans are running to schedule Pae-
diatric research is on-going at the same
rate across therapeutic areas such as on-
cology vaccines and immunology-rheu-
matology-transplantation
Furthermore by the end o 2011 72 new
paediatric indications had been approved
or medicines already authorised includ-
ing 30 indications (18 centralised) arising
rom the obligation in Article 8 Moreover26 new pharmaceutical orms were au-
thorised or paediatric use including 18
adapted orms or centrally authorised
medicines
As ar as Paediatric Use Marketing Au-
thorisation is concerned to date only one
authorisation has been granted This alls
short o initial expectations
16 httpwwwwhointchild-medicinespaediatric_regula-
torsen
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1336
13
A detailed inventory o centrally autho-
rised products is provided in Annex II
Rewards and incentives
Companies that have complied with the
obligations o the Regulation may benefit
rom a reward once the product concerned
is authorised or the product inormation isamended The reward takes the orm o a
6-month extension o the supplementary
protection certificate (SPC) provided or
by Regulation (EC) No 469200917 or in
the case o an orphan medicinal product
by an extension o the ten-year period o
orphan market exclusivity to twelve years
No orphan rewards have been awarded
yet In this regard it is observed that some
companies withdrew the orphan designa-tion o a product in order to qualiy or
the SPC reward rather than the orphan
reward which seems to be more attrac-
tive rom an economic perspective As ar
as SPC extensions are concerned national
patent offices in 16 Member States had
by the end o 2011 granted 6-month ex-
tensions to 11 medicinal products which
resulted in a total o more than 100 na-
tional SPCs
It should be pointed out that a ruling othe European Court o Justice urther
increased the value o the paediatric
reward as it made clear that the initial
certificate could have a negative or zero
duration which could then become posi-
tive once the paediatric extension was
granted18
43 Increased information on
medicines used in childrenTo provide better inormation on the use
o medicinal products in children Article
45 o the Paediatric Regulation requires
companies holding data on the saety
or efficacy o authorised products in the
paediatric population to submit these
studies to the competent authorities In
this way the data can be assessed and
where appropriate the authorised prod-
uct inormation amended Article 46 o
the Regulation also requires companies tosubmit newly generated paediatric data
Since 2008 more than 18 000 study re-
ports on roughly 2 200 medicinal prod-
ucts have been submitted revealing the
large amount o existing paediatric inor-
mation available at company level
These study reports have been and
continue to be assessed by the compe-
tent authorities thanks to an impressive
work-sharing project (see Tables 10 and11) For nationally authorised products
this has led to the publication o assess-
ment reports covering more than 140
active substances and in a considerable
number o cases to recommendations
or changes to the summaries o product
characteristics o authorised products re-
sulting in 65 actual changes For centrally
authorised products by 2011 the Agency
had completed the assessment o all the
data submitted under Article 45 covering55 active substances in 61 centrally ap-
17 Regulation (EC) No4692009 o the Euro-
pean Parliament and othe Council o 6 May 2009
concerning the supplemen-tary protection certificateor medicinal products OJ
L 152 1662009 p 1 ThisRegulation is a codificationo Council Regulation (EEC)
No 176892
18 Case C-12510 Merck
Sharp amp Dohme v DeutschesPatent- und Markenamt notyet published in the ECR
paragraph 37 lsquoi the SPCapplication had to be reused
because the calculationprovided or in Article 13(1)o Regulation No 176892
results in a negative or zero
duration the holder o thebasic patent could not obtain
an extension o protectionconerred by such a patenteven i it conducted all the
studies according to the ap-proved paediatric investiga-
tion plan under Article 36 oRegulation No 19012006Such a reusal would be
liable to adversely impacton the useul effect oRegulation No 19012006
and might jeopardise the
objectives o that regulationnamely the compensation
o effort made to evaluatethe paediatric effects o themedicinal product at issuersquo
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1436
14
proved medicinal products The summa-
ries o product characteristics o 12 me-
dicinal products were changed ollowing
the assessment
5Lessonslearnt51 Better access to
treatment
One o the explicit goals o the Paediatric
Regulation is to increase the number oproducts that are researched developed
and authorised or use in children and
to reduce the off-label use o medicinal
products in the paediatric population
The main tool to achieve this result is to
oblige companies to establish a paediat-
ric investigation plan or each newly de-
veloped product or or the line extension
o an already authorised product that is
still under patent protection The plan ismeant to ensure mdash under the supervi-
sion o the Paediatric Committee mdash that
the necessary data are generated so as
to determine the conditions under which
a medicinal product may be authorised
to treat children Since 2008 more than
600 paediatric investigation plans have
been approved However only a minor-
ity o them has been completed to date
the vast majority are still on-going This
is due to the long development cycles omedicinal products ofen lasting more
than a decade and the near-systematic
deerral o paediatric studies The high
number o deerrals may not have been
initially expected but are currently a real-
ity as or most o the medicinal products
that have been authorised so ar the RampD
programme started beore the entering
into orce o the Regulation Consequent-
ly the paediatric requirements could not
be taken into account rom the beginningo the product development
While the Paediatric Regulation has led
to some new authorisations that include
paediatric indications the regulatory in-
strument is recent and it will probably
take at least a decade beore it can be
judged in terms o its output In terms o
pharmaceutical orms there is however
already a visible positive impact
In this context criticism has been voiced
that the Regulation will ail to ensure abreakthrough in areas o particular pae-
diatric need such as paediatric oncology
This argument is related to the act that
the starting point or the majority o pae-
diatric investigation plans is an ongoing
RampD programme or a medicinal product
or adults An intrinsic consequence o this
approach is that these products primarily
target adult conditions They are devel-
oped in areas where there is a need (or a
market) in the adult population This needin the older population does not neces-
sarily correspond to the paediatric popu-
lationrsquos need
Moreover the Regulation grants waivers
rom its obligations where the disease or
condition or which the specific medicinal
product is intended occurs only in adult
populations This legislative approach cre-
ates riction in the case o diseases that
are specific and exclusive to children Italso limits the powers and possibilities o
the Paediatric Committee when reviewing
and agreeing to a paediatric investigation
plan as regards the scope o studies that
the Committee may request rom appli-
cants ollowing the objective and scien-
tific-based assessment o the compound
concerned19
These constraints and boundaries have to
be taken into account when judging the
impact the Regulation is likely to make In
addition the effect o instruments such as
the Orphan Regulation have to be consid-
ered given that or example all paediatric
cancers are rare diseases and all under
the EU policy ramework on rare diseases
All in all the achievements highlighted in
chapter 4 o this report and the number
o products with new paediatric indica-
tions show that there are some encourag-
ing signs afer this first five-year period it
is however too early or comprehensive
answers
19 Case T-5209 Nycomed vEMA not yet published
See the results o the publicconsultation conducted by
the Commission in prepara-tion o this Report
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1536
15
52 The PUMA concept a
disappointment
The Paediatric Regulation introduced a
new type o marketing authorisation mdash
the Paediatric Use Marketing Authorisa-
tion (PUMA) As an incentive to carry out
research into the potential paediatric use
o off-patent medicinal products that have
been authorised or adults this marketing
authorisation offers 8 years o data and
10 years o market exclusivity to any new
off-patent product developed exclusively
or use in the paediatric population Thus
the main goal o the PUMA concept is to
stimulate research in existing products
This scheme has been supported by EU
unding through the EU Framework Pro-
grammes or Research and Technological
Development
However to date only one PUMA has been
granted with a ew more projects cur-
rently in the pipeline
Neither industry nor academic networks
have embraced this opportunity as ully
as the Regulation intended It would seem
that the incentive o data and market ex-
clusivity does not work or these productsor at least that the market opportunities
in this sector are currently considered in-
sufficient to outweigh the inherent eco-
nomic risks o pharmaceutical develop-
ment Researchers are not engaging in
trials with medicines that have been on
the market or years Companies seem to
ear that market exclusivity will not pre-
vent physicians rom continuing to use
competitor products with the same active
ingredient off-label at lower costs or thatsubstitution or cheaper adult orms takes
place at the level o pharmacies Moreo-
ver national pricing and reimbursement
rules in Member States ofen do not al-
low or the additional research needed to
obtain the PUMA to be rewarded in price
negotiations20
Against this background the PUMA con-
cept has ailed so ar to ulfil the initial
expectationsThe EMA will in uture accept paediatric
investigation plans or a PUMA that cover
only certain age groups and not the en-
tire paediatric population This may offset
some o the reservations that currently
hamper better endorsement o the PUMA
concept
53 No impact on adultdevelopment
Studies prior to the adoption o the Regu-
lation have suggested a theoretical risk
that the requirements or research in chil-
dren could lengthen the overall drug de-
velopment process21 The Regulation has
met this risk head-on In order to avoid
any delays in authorising medicines or
other populations it allows or the grant-
ing o deerrals relating to the initiation orcompletion o some or all o the meas-
ures contained in a paediatric investiga-
tion plan
Experience shows that the deerral is a
widely used instrument which suggests
that the risk o delays in the processing o
adult applications is minimal There have
been some transitional problems in cases
where the adult programme was already
established when the Regulation enteredinto orce but these issues seem to have
been resolved
A concern that was raised initially was
that some companies would become
reluctant to develop new indications
pharmaceutical orms and new routes o
administration in small markets and or
products with low sales to avoid being
bound by the paediatric obligation under
Article 8 o the Regulation However thereis no evidence o such effect Moreover
it may also be argued that the incentive
o a potential six-month extension o the
SPC served to counterbalance such an
effect as it may have led companies to
examine more thoroughly the benefits o
a line extension taking into account the
economic value o the paediatric reward
Still industry stakeholders claim that
in rare cases the development or new
medicinal products has been delayedor abandoned in the expectation or as a
consequence o additional costs and re-
quirements associated with paediatric de-
20 See the results o thepublic consultation con-
ducted by the Commission inpreparation o this Report
21 C Commission StaffWorking Document Proposal
or a Regulation o the Euro-pean Parliament and o theCouncil on medicinal prod-
ucts or paediatric use andamending Council Regulation(EEC) No 17692 Directive
200183EC and Regula-tion (EC) No 7262004Extended impact assessment
(COM2004599F)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1636
16
keting authorisation holders are obliged
to ensure that the product inormation
is kept up to date with the current scien-
tific knowledge While preerence should
be given to cooperative approaches the
enorcement tools may need to be used
i companies do not overcome their res-
ervations
On the whole the requirements o Articles
45 and 46 have provided an efficient and
appropriate instrument or collecting and
evaluating existing paediatric studies
55 Clinical trials with
children
It is generally accepted that the Paediatric
Regulation will lead to more clinical trialswith children but that its aims should be
achieved without subjecting children to
unnecessary clinical trials
The youngest paediatric-age subsets
including neonates are particularly sen-
sitive It will be a constant challenge to
balance the therapeutic needs o these
age groups with their specific vulnerability
when considering and deciding on the ap-
propriateness o specific clinical trials or
the specific settings o studies in this age
subset Efforts are thereore continuously
being made to explore alternative means
eg the use o extrapolation modelling
and simulation techniques to reduce the
number o study subjects as much as
possible The Paediatric Committee is ac-
tively contributing to acilitate the devel-
opment and use o such means including
non-conventional trial design
Another challenge is how to avoid dupli-cating trials or different paediatric inves-
tigation plans rom different applicants
Companies embarking on product devel-
opment in similar areas may be required
by the agreed paediatric investigation
plan to conduct studies within similar
settings While collaborative approaches
between companies would be highly de-
sirable and have occurred on rare occa-
sions they ofen conflict with companiesrsquo
understandable reluctance to share datawith competitors in the early stages o
product development and participate in
direct comparisons This situation could
velopment Overall there is however no
evidence that the Regulation has a con-
siderable negative impact on products or
other populations
Rather there are some concerns that the
requirements under the Regulation may
cause delays in the authorisation o prod-ucts with paediatric-only indications as
they bring added complexity to the RampD
and regulatory process or products that
already directly target children The added
value o the submission o a paediatric in-
vestigation plan in these cases will be as-
sessed urther in the 2017 report
54 Reaping the benefits of
existing information
There was widespread speculation prior to
the adoption o the Paediatric Regulation
as to how many studies would be submit-
ted by pharmaceutical companies in ac-
cordance with Articles 45 and 46 The act
that competent authorities received more
than 18 000 studies reveals the consid-
erable amount o paediatric inormation
that existed at company level
Certainly it is true that not all the inor-
mation submitted met modern require-
ments or scientific data and clinical re-
search and that the work-sharing process
o evaluating the inormation is rather
long and resource intensive
Nevertheless compared to the PUMA con-
cept this scheme proved more successul
in terms o output and in recommending
and implementing changes to the sum-
mary o product characteristics o author-
ised products In its public consultationthe Commission called Articles 45 and 46
the lsquohidden gemsrsquo o the Regulation
One drawback that remains however
is reluctance by marketing authorisa-
tion holders to update the summary o
product characteristics on a voluntary
basis This said the Regulation contains
mechanisms to overcome such reluctance
as it empowers competent authorities to
directly update the summary and varythe marketing authorisation accordingly
Moreover in accordance with Article 23
o Directive 200183EC22 and Article 16
o Regulation (EC) No 726200423 mar-
22 Directive 200183EC othe European Parliament and
o the Council o 6 November2001 on the Community
code relating to medicinalproducts or human use OJ L311 28112001 p 67
23 Regulation (EC) No7262004 o the European
Parliament and o the Coun-cil o 31 March 2004 layingdown Community procedures
or the authorisation andsupervision o medicinalproducts or human and
veterinary use and establish-ing a European Medicines
Agency OJ L 136 3042004p 1
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1736
17
lead to competition among companies to
find investigators and study participants
as well as the duplication o trials which
are unnecessary rom a scientific and
ethical point o view
The Paediatric Committee is able to waive
paediatric trial requirements where thespecific medicinal product does not rep-
resent a significant therapeutic benefit
over an existing treatment or paediatric
patients including once the product is au-
thorised (Article 11) However this option
does not provide a way out in the early
stages o product development where
the Committee has to ensure equal treat-
ment and non-discriminatory approaches
The key to avoiding such unnecessary tri-
als is transparency with regard to ongoingand completed trials The situation contin-
ues to be monitored
Finally it is in the interest o the EU that
paediatric trials stemming rom paedi-
atric investigation plans are conducted
within the EU This has less to do with
the standards under which a trial is con-
ducted given that clinical trials carried
out outside the EU have to meet the ethi-
cal and scientific requirements o the EUprovisions on clinical trials24 than with the
act that studies within the EU may pro-
vide patients there with early access to
innovative medicines To date there is in-
sufficient data on the ratio between pae-
diatric trials conducted within and outside
the EU However in view o the upgraded
unctionalities o the EudraCT database it
is expected that more data will be avail-
able in 2017 or the second report
56 Spreading the news mdash
getting new information
to patients and healthcare
professionals
I the Regulation is to be a success it is
not only necessary that data on the use
o a specific product in the paediatric
population are collected but that these
data are then also appropriately commu-
nicated to and used by paediatricians intheir day-to-day work or the benefit o
their patients
In this regard some studies published in
the medical literature suggest a ailure
on the part o practitioners to recognise
the actual amount o off-label prescrib-
ing to children Moreover it is claimed that
the prescribing habits o practitioners are
ofen strongly influenced by personal ex-
perience rather than by evidence-based
inormation or paediatric medicine25
These studies in making generalisations
may not have taken into account the het-
erogeneity o healthcare proessionals
whose receptiveness varies greatly ac-
cording to their work setting and specific
area o specialisation At the same time
such observations may point to a sub-
stantial hurdle in achieving the goal o the
Paediatric Regulation
National competent authorities as well as
organisations or healthcare proessionals
seem particularly qualified to consider ap-
propriate ways o ensuring an adequate
flow o inormation Some Member States
have already established a number o
tools to communicate effectively and e-
ficiently with healthcare proessionals
eg by means o regular meetings web-
based inormation distribution systems ornational ormularies
57 Is the burden greater
than rewards
There can be no doubt that the Paediat-
ric Regulation places a considerable ad-
ditional burden on pharmaceutical com-
panies with its obligations regarding
research on products or use in children
However this approach was adopted be-cause market orces alone proved insu-
ficient to stimulate adequate research
The Regulation requires companies to
submit paediatric investigation plans at
an early stage o product development
However research on some active sub-
stances may be discontinued at later
stages should urther studies ail to show
potential with respect to the saety and
efficacy o the product For every success-
ul authorised medicinal product there aremany that ail to make the finishing line
Hence not all approved paediatric investi-
gation plans will be completed as compa-
24 Directive 200120EC othe European Parliament
and o the Council on theapproximation o the laws
regulations and administra-tive provisions o the Mem-ber States relating to the
implementation o good clini-cal practice in the conducto clinical trials on medicinal
products or human use OJ L121 152001 p 34
25 5-year report to theEuropean Commission (seeootnote 3) page 41
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1836
18
nies may decide to stop the correspond-
ing adult development It is too early still
to obtain reliable statistics that show
the ratio between completed and non-
completed paediatric investigation plans
but in the current context not all approved
plans will eventually result in an approved
medicine with a paediatric indication
In terms o output this entails some un-
necessary effort in compiling and screen-
ing paediatric investigation plans To what
extent this is offset by the benefit o early
submission which ensures that the pae-
diatric development fits smoothly into the
overall product development need ur-
ther monitoring
A urther point o concern is the highnumber o modifications to paediat-
ric investigation plans Figures seem to
suggest that nearly all plans have to
be modified at least once Conceptually
though this does not come as a surprise
in view o the early submission o pae-
diatric investigation plans the length o
adult and paediatric developments and
the substantial deerrals granted An
RampD plan requently has to be adapted
or amended to take account o initial re-sults Recruitment problems or necessary
design changes in the trials may also lead
to modifications While it is acknowledged
that substantial amendments or modifi-
cations to the plan have to be subject to
discussions with the Paediatric Commit-
tee this is less obvious or minor changes
In this context the level o detail required
by the EMA has been repeatedly criticised
In the past five years the EMA and its
Paediatric Committee have made effortsto provide or some flexibility in the plan
so to allow a margin o manoeuvre that
takes account o uncertainties in relation
to certain parameters o a trial
In any case the Commission intends to
review its Communication on the ormat
and content o applications or agree-
ment or modification o a paediatric in-
vestigation plan to take into account the
experience gained including the consider-
able number o modification requests
On a positive note it can be noted that
companies are applying or the rewards
provided by the Regulation primarily the
6-month extension o the Supplementary
Protection Certificate which have been
introduced to offset the additional bur-
den The economic value o the reward
depends on the turnover o the product
concerned In the case o blockbuster
products the amount may be consider-
able while or niche products the effect
is small
An in-depth evaluation o the economic
impact will be included in the 2017 report
in order to draw conclusions on the bal-
ance between burden and rewards and
public health benefits
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1936
19
6Outlook mdash
A fairy-taleending aheadlsquoBetter Medicines or Children mdash From
Concept to Realityrsquo is the title o this re-
port Readers may suggest that based on
the evaluation reerred to above it would
be more appropriate to add a question
mark It is evident that it is too early still
to make a firm statement Despite more
than five years o experience the true im-pact o the Regulation on the health o
children will only become apparent over
time as experience is accumulated in the
longer term
There are encouraging signs though
Paediatric development has become a
more integral part o the overall develop-
ment o medicinal products in the EU A
number o new products with paediatric
indications and age-appropriate pharma-ceutical orms have been authorised and
made available to patients A high num-
ber o agreed paediatric investigation
plans indicates that urther products are
in the pipeline
However it needs to be pointed out that it
would be wrong to expect the Regulation
to be able to solve all problems Instead
it is a major catalyst to improve the situ-
ation o young patients
Finally some weaknesses and deficits
have also become apparent in the last
five years Their impact on the overall
perormance o the Regulation has to be
closely monitored On the basis o the ac-
tions outlined above the Commission in-
tends to fine-tune the current implemen-
tation together with the EMA
Even i better medicines or children are
not yet a reality it should be the ambitiono all stakeholders involved that this piece
o legislation will be or the greater good
o children so that in the 2017 report
the discussion will ocus not on whether a
question mark should be added to the ti-
tle o the report but on whether it should
be an exclamation mark instead
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2036
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2136
21
ANNEXES
Figures and Tables
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2236
22
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2336
23
ANNEX I
Figures and Tables
Table 1Agreed paediatric investigations plans (PIPs) 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Agreed PIPs submitted under Article 7 (without waivers)
Agreed PIPs submitted under Article 8 (without waivers)
Source EMA Paediatric database The numbers on agreed PIPs correspond to EMA decisions
Table 2Agreed paediatric investigations plans (PIPs) compared to ull waivers and modifications 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Submitted modifications of an agreed PIP
Agreed Full waivers
Source EMA Paediatric database The numbers on agreed PIPs and waivers correspond to EMA decisions
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2536
25
Table 5Scientific advice and protocol assistance including ollow-ups (provided by the EMA Scientific Advice Working
Party and the Committee or Human Medicinal Products per year)
259
277321
388 400 433 420
021 32
74 8057
91
0 0 0
68 8067
94
0
100
200
300
400
500
2006 2007 2008 2009 2010 2011 2012
Total number of advice (Scientific Advice and Protocol Assistance)
Sum of paediatric-only and mixed (adult and paediatric development questions)
advice
Paediatric-only or mixed advice that involved a Paediatric Committee member(s) as
expert(s)
Source EMA databases Year o advice letter
Year o start o procedure
Table 6Paediatric clinical trials by year o authorisation
2005 2006 2007 2008 2009 2010 2011 2012
Paediatric trials
(number) 254 316 355 342 404 379 334 332
Paediatric trials
that are part of anagreed PIP 2 1 2 6 16 30 76 76
Proportion of
paediatric trials
that are part of an
agreed PIP among
paediatric trials 1 0 1 2 4 8 23 23
Total number
of trials (adults
and or children) 3 350 3 979 4 749 4 512 4 445 4 026 3 809 3 698
Proportion of
paediatric trials of
all trials 8 8 7 8 9 10 9 9
Source EudraCT Data Warehouse using a predefined query on 6 March 2013 and counting the first authorised trial only in the case o more thanone Member State This partial inormation requires sponsors to use a Clinical Trial Application orm that was only available rom November 2009 or use with version 8 o EudraCT
(available rom 2011)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2636
26
Table 7Number o children to be enrolled in clinical trials
Number
of subjects 2006 2007 2008 2009 2010 2011 2012
Pretermnewborns 0 0 0 207 82 2 281 1 712
Newborns 0 0 5 64 169 1 105 1 172
Infants and
toddlers 330 21 20 59 351 2 788 3 141
Children 2 142 181 200 2 230 2 055 10 325 20 677
Adolescents 368 111 205 1 577 2 861 9 054 13 193
Sum of
above 2 840 313 430 4 137 5 517 25 553 39 895
Reference
number of paediatric
trials 316 355 342 404 379 334 332
Source EudraCT Data Warehouse using a pre-defined query on 6 March 2013 modified by excluding studies or lsquoimmunological medicinal productsrsquo
Table 8EU budget contribution to the Paediatric Regulation and the EMA expenditure
0
1
2
3
4
5
6
7
8
9
10
2006 2007 2008 2009 2010 2011 2012
EU budget contribution (in Million euro)
EMA expenditure for paediatri cs (in Mill ion euro)
EMA expenditure for paediatr ics including support (in Million euro)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2736
27
Table 9Percentage o European Medicines Agencyrsquos human resources working in the paediatric area rom 2006 (inner
circle) to 2012 (outer circle)
733 (2012)
052 (2006)
Table 10Member States acting as rapporteurs or the assessment o studies submitted in accordance with Article 46
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE SE NL FR DK IT BE PL ES NO SK FI IE RO AT HU EL CZ PT LV BG
Study included in worksharing Rapporteur appointed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2836
28
Table 11Member States acting as rapporteur or the assessment o studies submitted in accordance with Article 45
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE NL DK AT FR PL SE ES IE CZ MT IT BE SI EE FI HU NO RO BG EL LV PT IS SK
Wave 1 Wave 2 Wave 3 Wave 4 Wave 5 Wave 6 Wave 7 Wave 8 Wave 9
Wave 10 Wave 11 Wave 12 Wave 13 Wave 14 Wave 15 Wave 16 Wave 17 Wave 18
Table 12Member States acting as rapporteurspeer reviewers in EMArsquos Paediatric Committee procedures (initial PIP
waiver or modification o an agreed PIP)
0
50
100
150
200
250
300
350
400
450
500
A u s t r i a
B el gi um
B ul g a r i a
C y pr u s
C z e c h R e p u b l i c
D enm a r k
E s t oni a
F i nl a n d
F r a n c e
G er m a n y
G r e e c e
H e a l t h c a r e a n d
A c a d emi a
H un g a r y
I c el a n d
I r el a n d
I t a l y
L a t vi a
L i t h u a ni a
L ux em b o ur g
M a l t a
N or w a y
P a t i en t s Or g a ni s a t i on
P ol a n d
P or t u g a l
R om a ni a
S l ov a k i a
S l ov eni a
S p a i n
S w e d en
T h eN e t h er l a n d
s
U ni t e d K i n g d om
Initial PIP applications PIP modifications
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2936
29
ANNEX II
Detailed inventory of centrally authorised medicinalproducts for paediatric use since the entry into force
of the Paediatric Regulation
Table 13Medicinal products authorised centrally since 2007 which include a paediatric indication
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Retapamulin Altargo 2007 No Mixed
Nelarabine Atriance 2007 No Mixed
Human papillomavirus vaccine[types 16 18] Cervarix 2007 No Mixed
Hydroxocobalamin Cyanokit 2007 No Mixed
Idursulase Elaprase 2007 No Mixed
Gadoversetamide Optimark 2007 No Mixed
Betaine anhydrous Cystadane 2007 No Mixed
Stiripentol Diacomit 2007 No Paediatric only
Mecasermin Increlex 2007 No Paediatric only
Rufinamide Inovelon 2007 No Mixed
Hydroxycarbamide Siklos 2007 No Mixed
Human normal
immunoglobulin (ivig) Flebogamma DIF 2007 No Mixed
Fluticasone uroate Avamys 2008 No Mixed
Human normal immunoglobulin Privigen 2008 No Mixed
Lacosamide Vimpat 2008 No Mixed
Micaungin Mycamine 2008 No Mixed
Sapropterin Kuvan 2008 No Mixed
Sugammadex Bridion 2008 No Mixed
Tocoersonal d-alpha
tocopheryl polyethylene glycol
succinate Vedrop 2009 No Paediatric only
Miamurtide Mepact 2009 No Mixed
Rilonacept Rilonacept Regeneron 2009 No Mixed
Tacrolimus Modigra 2009 No Mixed
Pneumoccocal polysaccharideconjugate vaccine (adsorbed) Synflorix 2009 No Paediatric only
Canakinumab
Ilaris (PIP not yet
completed) 2009 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3036
30
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Pneumoccocal polysaccharide
conjugate vaccine (13-valentadsorbed)
Prevenar 13 (PIP not yetcompleted) 2009 Yes Paediatric only
Meningococcal group a c
w135 and y conjugate vaccine Menveo 2010 Yes Mixed
Velaglucerase ala
Vpriv (PIP not yet
completed) 2010 Yes Mixed
Influenza vaccine (live
attenuated nasal) Fluenz (Waiver) 2011 Yes Paediatric only
C1 inhibitor human
Cinryze (PIP not yet
completed) 2011 Yes Mixed
Dihydroartemisinin
piperaquine phosphate
Eurartesim (PIP not yet
completed) 2011 Yes Mixed
Midazolam Buccolam 2011 Yes (PUMA) Paediatric only
EverolimusVotubia(PIP not yet completed) 2011 Yes Mixed
Tobramycin
Tobi Podhaler (PIP not
yet completed) 2011 Yes Mixed
Nomegestrol estradiol Ioa Zoely 2011 Yes Mixed
Colistimethate sodium Colobreathe 2012 Yes Mixed
Mercaptopurine Xaluprine 2012 No Mixed
Catridecacog NovoThirteen 2012 Yes MixedEavirenz Eavirenz Teva 2012 No Mixed
Ivacafor Kalydeco 2012 Yes Mixed
Desloratadine Desloratadine ratiopharm 2012 No Mixed
Desloratadine Desloratadine Actavis 2012 No Mixed
Perampanel Fycompa 2012 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3136
31
Table 14List o centrally authorised medicinal products or which the therapeutic indication was extended to or amend-
ed or the paediatric population
Active substance(s)
Trade
name Date Subject of the extension
Levetiracetam Keppra
2007
2009
Extension o the indication to include adjunctive ther-
apy in the treatment o primary generalised tonic-
clonic (PGTC) seizures in adults and adolescents rom
12 years o age with idiopathic generalised epilepsyExtension o indication to include the adjunctive
treatment o partial seizures with or without second-
ary generalisation in children rom 1 month to lt4
years old
Pneumococcal sac-
charide conjugated
vaccine adsorbed Prevenar 2007
Extension o the indication to include new inorma-
tion on efficacy against disease caused by Strepto-
coccus pneumoniae serotypes 4 6B 9V 14 18C 19F
and 23F in otitis mediaExtension o indication rom active immunisation
against bacteraemic pneumonia to active immunisa-
tion against pneumonia
Infliximab
Remi-
cade 2007
Extension o indication to include treatment o
severe active Crohnrsquos disease in children aged 6 to
17 years
Darbepoetin ala Aranesp 2007
Extension o indication or CRF patients whichrestricted the use o Nespo to paediatric subjects ge
11 years o age
Fosamprenavir Telzir 2007
Extension o indication o Telzir in combination withritonavir or the treatment o Human Immunodefi-
ciency Virus Type 1 (HIV-1) inected adults in combi-nation with other antiretroviral medicinal products to
include paediatric populations
Lamivudine zidovu-
dine Combivir 2007
Extension o indication to include paediatric patients
and replacement o film-coated tablets by scored
film-coated tablets
Desloratadine Aerius 2007Extension o indication rom lsquochronic idiopathic urti-cariarsquo to lsquourticariarsquo
Insulin glulisine Apidra 2007
Extension o indication to include 6 year olds and
older children based on the results o 2 paediatricstudies
Human papilloma virusvaccine [types 6 11
16 18] (recombinantadsorbed) Gardasil 2008
Extension o indication to include the prevention ohigh-grade vaginal dysplastic lesions (VaIN 23)
Adalimumab Humira 20082011
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in adoles-cents rom 13 to 17 years o age
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in the paedi-
atric population aged rom 4 to 12 years
Caspoungin Cancidas 2008
Extension o the indication to include the paediatric
population
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 736
7
The key objectives of theRegulation are
bull to ensure high-quality research into
the development o medicines or
children
bull to ensure over time that the major-ity o medicines used by children are
specifically authorised or such use
with appropriate orms and ormula-
tions
bull to ensure the availability of high-
quality inormation about medicines
used by children
The key measures included inthe Regulation are
bull setting up an expert committee with-
in the EMA the Paediatric Commit-
tee
bull requiring companies to submit dataon the use o a medicine in children
in accordance with an agreed paedi-
atric investigation plan when apply-
ing or marketing authorisation or
medicines and line-extensions or
existing patent-protected medicines
bull a system of waivers from the re-
quirement or medicines unlikely to
benefit children and a system o de-
errals in relation to the timing o the
requirement to ensure that medi-
cines are tested in children only whenit is sae to do so and to prevent the
requirements delaying the authorisa-
tion o medicines or adults
bull a reward for complying with the re-
quirement in the orm o a six-month
extension to the Supplementary Pro-
tection Certificate
bull a reward in respect of orphan medi-
cines or compliance in the orm o
an extra two years o market exclu-
sivity added to the existing ten yearsawarded under the EUrsquos Orphan Reg-
ulation
bull a new type of marketing authorisa-
tion the Paediatric Use Marketing
Authorisation (PUMA) to attract newpaediatric indications or off-patent
products
bull measures to maximise the impact of
existing studies on medicines or chil-
dren
bull an EU inventory of the therapeuticneeds o children to ocus the re-
search development and authorisa-
tion o medicines
bull an EU network of investigators and
trial centres to carry out the required
RampD
bull a system of free scientic advice for
the industry provided by the EMA
bull a public database of paediatric stud-
ies
bull a provision on EU funding for re-search to stimulate the development
and authorisation o off-patent med-
icines or children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 836
8
The Regulation gives the EMA and its
Paediatric Committee primary responsi-
bility or handling paediatric investigation
plans deerrals and waivers This provides
the Agency with concrete decision-mak-
ing powers
The operational costs o the PaediatricRegulation are partly covered by a contri-
bution rom the EU budget (see Table 8)
as its main activities do not attract any
ees For the period 2007-12 the EU
budget contribution amounted to more
than EUR 39 million In addition Member
Statesrsquo national competent authorities
contribute resources in kind especially
staff time or the assessment o paediat-
ric investigation plans (see Table 12)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 936
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1036
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1136
11
cantly (see Table 5) despite the act that
issues o pharmaceutical non-clinical and
clinical development are also part o the
discussions o a paediatric investigation
plan To acilitate collaboration with the
Paediatric Committee joint procedures
have been created within the EMA
413 Clinical trials with children
Medicines or use in children need to be
tested with appropriate ormulations in
the paediatric population to ensure their
sae and effective use Hence it is gener-
ally accepted that the Paediatric Regula-
tion will lead to more clinical trials in chil-
dren The figures in the EudraCT database
have not yet shown an increase in paedi-
atric trials The number remained stablebetween 2006 and 2012 averaging 350
trials per year with some fluctuations (see
Table 6) It should be pointed out how-
ever that while the number o paediat-
ric trials remained stable the number o
clinical trials in all populations decreased
between 2007 and 2011
Moreover until recently EudraCT was lim-
ited to paediatric trials commencing in the
EU Data on paediatric trials that are parto a paediatric investigation plan and con-
ducted outside the EU have only become
publicly available since spring 2011
It should also be noted that the initiation
o a considerable percentage o clinical
trials included in a paediatric investiga-
tion plan has been deerred in order to
avoid delays in the authorisation o the
corresponding product or adults Hence
the impact o the Paediatric Regulation on
paediatric trials will become more appar-
ent in EudraCT in the years to come There
has however been an evident increase in
the number o paediatric study partici-
pants in particular or the age group rom
0 to 23 months who were normally not
included in trials prior to 2008 (see Ta-
ble 7) Allowing neonates and inants to
benefit rom research is a positive sign
as these have been the most neglected
groups so ar
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1236
12
414 Optimised framework and
coordination
The Paediatric Regulation osters a com-
prehensive network o expertise in paedi-
atric matters within the EU In this context
the role o the Paediatric Committee ispivotal as it brings together a high level
o expertise and competence
The Committee has contributed to the
scientific guidelines published by the EMA
and has so ar convened 22 expert work-
shops on the development o medicines
or children
In addition the European Network or
Paediatric Research at the EMA (Enpr-
EMA) was established in 2009 While aclosely-knit network o experts existed
prior to the introduction o the Regula-
tion in disease areas such as paediatric
oncology Enpr-EMA provides the added
value o a holistic approach by bringing
together national and European networks
investigators and centres with specific ex-
pertise in designing and conducting high-
quality studies in children
However question still remain as towhether this expertise translates into su-
ficient capacity within the EU to conduct
trials in specialised investigation settings
Well-developed research networks capa-
ble o acilitating the necessary research
to ulfil the commitments included in
paediatric investigation plans do exist in
some but not all Member States
415 International cooperation
On an international level the EMA has de-veloped international links with medicines
agencies in the United States Canada
and Japan O particular interest is the
cooperation with the US Food and Drug
Administration given that already in the
late 1990s the United States introduced
legislation that stimulated the develop-
ment o medicinal products or paediatric
use by means o a combination o incen-
tives and obligations This cooperation is
also o great interest to stakeholders as
it may give companies the possibility o
satisying the legislation in both regions
with the same studies
In addition the EMA participates actively
in the Paediatric medicines regulatory
network16 which was created in 2010 as
part o the WHOrsquos Better Medicines or
Children initiative
42 More medicines available
for children
Over 12 years (rom 1995 to 2006) 108
o all 317 indications o 262 centrally au-
thorised medicines included the paediat-
ric population Since the Paediatric Regu-
lation entered into orce 31 out o 152
new medicines have been authorised or
paediatric use 10 o which met the con-
ditions o Article 7 This is not more than
a lsquosnapshotrsquo o the effects o the Regula-
tion as this figure is likely to increase inthe uture as a considerable number o
the new already authorised medicines
are subject to an investigation plan where
completion was deerred to avoid delays
in the authorisation o the adult product
It ollows that in the years to come many
more o those 152 new medicines are ex-
pected to be authorised or paediatric use
Annual reports on deerred paediatric
studies o authorised medicines indicate
that the majority o paediatric investiga-tion plans are running to schedule Pae-
diatric research is on-going at the same
rate across therapeutic areas such as on-
cology vaccines and immunology-rheu-
matology-transplantation
Furthermore by the end o 2011 72 new
paediatric indications had been approved
or medicines already authorised includ-
ing 30 indications (18 centralised) arising
rom the obligation in Article 8 Moreover26 new pharmaceutical orms were au-
thorised or paediatric use including 18
adapted orms or centrally authorised
medicines
As ar as Paediatric Use Marketing Au-
thorisation is concerned to date only one
authorisation has been granted This alls
short o initial expectations
16 httpwwwwhointchild-medicinespaediatric_regula-
torsen
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1336
13
A detailed inventory o centrally autho-
rised products is provided in Annex II
Rewards and incentives
Companies that have complied with the
obligations o the Regulation may benefit
rom a reward once the product concerned
is authorised or the product inormation isamended The reward takes the orm o a
6-month extension o the supplementary
protection certificate (SPC) provided or
by Regulation (EC) No 469200917 or in
the case o an orphan medicinal product
by an extension o the ten-year period o
orphan market exclusivity to twelve years
No orphan rewards have been awarded
yet In this regard it is observed that some
companies withdrew the orphan designa-tion o a product in order to qualiy or
the SPC reward rather than the orphan
reward which seems to be more attrac-
tive rom an economic perspective As ar
as SPC extensions are concerned national
patent offices in 16 Member States had
by the end o 2011 granted 6-month ex-
tensions to 11 medicinal products which
resulted in a total o more than 100 na-
tional SPCs
It should be pointed out that a ruling othe European Court o Justice urther
increased the value o the paediatric
reward as it made clear that the initial
certificate could have a negative or zero
duration which could then become posi-
tive once the paediatric extension was
granted18
43 Increased information on
medicines used in childrenTo provide better inormation on the use
o medicinal products in children Article
45 o the Paediatric Regulation requires
companies holding data on the saety
or efficacy o authorised products in the
paediatric population to submit these
studies to the competent authorities In
this way the data can be assessed and
where appropriate the authorised prod-
uct inormation amended Article 46 o
the Regulation also requires companies tosubmit newly generated paediatric data
Since 2008 more than 18 000 study re-
ports on roughly 2 200 medicinal prod-
ucts have been submitted revealing the
large amount o existing paediatric inor-
mation available at company level
These study reports have been and
continue to be assessed by the compe-
tent authorities thanks to an impressive
work-sharing project (see Tables 10 and11) For nationally authorised products
this has led to the publication o assess-
ment reports covering more than 140
active substances and in a considerable
number o cases to recommendations
or changes to the summaries o product
characteristics o authorised products re-
sulting in 65 actual changes For centrally
authorised products by 2011 the Agency
had completed the assessment o all the
data submitted under Article 45 covering55 active substances in 61 centrally ap-
17 Regulation (EC) No4692009 o the Euro-
pean Parliament and othe Council o 6 May 2009
concerning the supplemen-tary protection certificateor medicinal products OJ
L 152 1662009 p 1 ThisRegulation is a codificationo Council Regulation (EEC)
No 176892
18 Case C-12510 Merck
Sharp amp Dohme v DeutschesPatent- und Markenamt notyet published in the ECR
paragraph 37 lsquoi the SPCapplication had to be reused
because the calculationprovided or in Article 13(1)o Regulation No 176892
results in a negative or zero
duration the holder o thebasic patent could not obtain
an extension o protectionconerred by such a patenteven i it conducted all the
studies according to the ap-proved paediatric investiga-
tion plan under Article 36 oRegulation No 19012006Such a reusal would be
liable to adversely impacton the useul effect oRegulation No 19012006
and might jeopardise the
objectives o that regulationnamely the compensation
o effort made to evaluatethe paediatric effects o themedicinal product at issuersquo
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1436
14
proved medicinal products The summa-
ries o product characteristics o 12 me-
dicinal products were changed ollowing
the assessment
5Lessonslearnt51 Better access to
treatment
One o the explicit goals o the Paediatric
Regulation is to increase the number oproducts that are researched developed
and authorised or use in children and
to reduce the off-label use o medicinal
products in the paediatric population
The main tool to achieve this result is to
oblige companies to establish a paediat-
ric investigation plan or each newly de-
veloped product or or the line extension
o an already authorised product that is
still under patent protection The plan ismeant to ensure mdash under the supervi-
sion o the Paediatric Committee mdash that
the necessary data are generated so as
to determine the conditions under which
a medicinal product may be authorised
to treat children Since 2008 more than
600 paediatric investigation plans have
been approved However only a minor-
ity o them has been completed to date
the vast majority are still on-going This
is due to the long development cycles omedicinal products ofen lasting more
than a decade and the near-systematic
deerral o paediatric studies The high
number o deerrals may not have been
initially expected but are currently a real-
ity as or most o the medicinal products
that have been authorised so ar the RampD
programme started beore the entering
into orce o the Regulation Consequent-
ly the paediatric requirements could not
be taken into account rom the beginningo the product development
While the Paediatric Regulation has led
to some new authorisations that include
paediatric indications the regulatory in-
strument is recent and it will probably
take at least a decade beore it can be
judged in terms o its output In terms o
pharmaceutical orms there is however
already a visible positive impact
In this context criticism has been voiced
that the Regulation will ail to ensure abreakthrough in areas o particular pae-
diatric need such as paediatric oncology
This argument is related to the act that
the starting point or the majority o pae-
diatric investigation plans is an ongoing
RampD programme or a medicinal product
or adults An intrinsic consequence o this
approach is that these products primarily
target adult conditions They are devel-
oped in areas where there is a need (or a
market) in the adult population This needin the older population does not neces-
sarily correspond to the paediatric popu-
lationrsquos need
Moreover the Regulation grants waivers
rom its obligations where the disease or
condition or which the specific medicinal
product is intended occurs only in adult
populations This legislative approach cre-
ates riction in the case o diseases that
are specific and exclusive to children Italso limits the powers and possibilities o
the Paediatric Committee when reviewing
and agreeing to a paediatric investigation
plan as regards the scope o studies that
the Committee may request rom appli-
cants ollowing the objective and scien-
tific-based assessment o the compound
concerned19
These constraints and boundaries have to
be taken into account when judging the
impact the Regulation is likely to make In
addition the effect o instruments such as
the Orphan Regulation have to be consid-
ered given that or example all paediatric
cancers are rare diseases and all under
the EU policy ramework on rare diseases
All in all the achievements highlighted in
chapter 4 o this report and the number
o products with new paediatric indica-
tions show that there are some encourag-
ing signs afer this first five-year period it
is however too early or comprehensive
answers
19 Case T-5209 Nycomed vEMA not yet published
See the results o the publicconsultation conducted by
the Commission in prepara-tion o this Report
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1536
15
52 The PUMA concept a
disappointment
The Paediatric Regulation introduced a
new type o marketing authorisation mdash
the Paediatric Use Marketing Authorisa-
tion (PUMA) As an incentive to carry out
research into the potential paediatric use
o off-patent medicinal products that have
been authorised or adults this marketing
authorisation offers 8 years o data and
10 years o market exclusivity to any new
off-patent product developed exclusively
or use in the paediatric population Thus
the main goal o the PUMA concept is to
stimulate research in existing products
This scheme has been supported by EU
unding through the EU Framework Pro-
grammes or Research and Technological
Development
However to date only one PUMA has been
granted with a ew more projects cur-
rently in the pipeline
Neither industry nor academic networks
have embraced this opportunity as ully
as the Regulation intended It would seem
that the incentive o data and market ex-
clusivity does not work or these productsor at least that the market opportunities
in this sector are currently considered in-
sufficient to outweigh the inherent eco-
nomic risks o pharmaceutical develop-
ment Researchers are not engaging in
trials with medicines that have been on
the market or years Companies seem to
ear that market exclusivity will not pre-
vent physicians rom continuing to use
competitor products with the same active
ingredient off-label at lower costs or thatsubstitution or cheaper adult orms takes
place at the level o pharmacies Moreo-
ver national pricing and reimbursement
rules in Member States ofen do not al-
low or the additional research needed to
obtain the PUMA to be rewarded in price
negotiations20
Against this background the PUMA con-
cept has ailed so ar to ulfil the initial
expectationsThe EMA will in uture accept paediatric
investigation plans or a PUMA that cover
only certain age groups and not the en-
tire paediatric population This may offset
some o the reservations that currently
hamper better endorsement o the PUMA
concept
53 No impact on adultdevelopment
Studies prior to the adoption o the Regu-
lation have suggested a theoretical risk
that the requirements or research in chil-
dren could lengthen the overall drug de-
velopment process21 The Regulation has
met this risk head-on In order to avoid
any delays in authorising medicines or
other populations it allows or the grant-
ing o deerrals relating to the initiation orcompletion o some or all o the meas-
ures contained in a paediatric investiga-
tion plan
Experience shows that the deerral is a
widely used instrument which suggests
that the risk o delays in the processing o
adult applications is minimal There have
been some transitional problems in cases
where the adult programme was already
established when the Regulation enteredinto orce but these issues seem to have
been resolved
A concern that was raised initially was
that some companies would become
reluctant to develop new indications
pharmaceutical orms and new routes o
administration in small markets and or
products with low sales to avoid being
bound by the paediatric obligation under
Article 8 o the Regulation However thereis no evidence o such effect Moreover
it may also be argued that the incentive
o a potential six-month extension o the
SPC served to counterbalance such an
effect as it may have led companies to
examine more thoroughly the benefits o
a line extension taking into account the
economic value o the paediatric reward
Still industry stakeholders claim that
in rare cases the development or new
medicinal products has been delayedor abandoned in the expectation or as a
consequence o additional costs and re-
quirements associated with paediatric de-
20 See the results o thepublic consultation con-
ducted by the Commission inpreparation o this Report
21 C Commission StaffWorking Document Proposal
or a Regulation o the Euro-pean Parliament and o theCouncil on medicinal prod-
ucts or paediatric use andamending Council Regulation(EEC) No 17692 Directive
200183EC and Regula-tion (EC) No 7262004Extended impact assessment
(COM2004599F)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1636
16
keting authorisation holders are obliged
to ensure that the product inormation
is kept up to date with the current scien-
tific knowledge While preerence should
be given to cooperative approaches the
enorcement tools may need to be used
i companies do not overcome their res-
ervations
On the whole the requirements o Articles
45 and 46 have provided an efficient and
appropriate instrument or collecting and
evaluating existing paediatric studies
55 Clinical trials with
children
It is generally accepted that the Paediatric
Regulation will lead to more clinical trialswith children but that its aims should be
achieved without subjecting children to
unnecessary clinical trials
The youngest paediatric-age subsets
including neonates are particularly sen-
sitive It will be a constant challenge to
balance the therapeutic needs o these
age groups with their specific vulnerability
when considering and deciding on the ap-
propriateness o specific clinical trials or
the specific settings o studies in this age
subset Efforts are thereore continuously
being made to explore alternative means
eg the use o extrapolation modelling
and simulation techniques to reduce the
number o study subjects as much as
possible The Paediatric Committee is ac-
tively contributing to acilitate the devel-
opment and use o such means including
non-conventional trial design
Another challenge is how to avoid dupli-cating trials or different paediatric inves-
tigation plans rom different applicants
Companies embarking on product devel-
opment in similar areas may be required
by the agreed paediatric investigation
plan to conduct studies within similar
settings While collaborative approaches
between companies would be highly de-
sirable and have occurred on rare occa-
sions they ofen conflict with companiesrsquo
understandable reluctance to share datawith competitors in the early stages o
product development and participate in
direct comparisons This situation could
velopment Overall there is however no
evidence that the Regulation has a con-
siderable negative impact on products or
other populations
Rather there are some concerns that the
requirements under the Regulation may
cause delays in the authorisation o prod-ucts with paediatric-only indications as
they bring added complexity to the RampD
and regulatory process or products that
already directly target children The added
value o the submission o a paediatric in-
vestigation plan in these cases will be as-
sessed urther in the 2017 report
54 Reaping the benefits of
existing information
There was widespread speculation prior to
the adoption o the Paediatric Regulation
as to how many studies would be submit-
ted by pharmaceutical companies in ac-
cordance with Articles 45 and 46 The act
that competent authorities received more
than 18 000 studies reveals the consid-
erable amount o paediatric inormation
that existed at company level
Certainly it is true that not all the inor-
mation submitted met modern require-
ments or scientific data and clinical re-
search and that the work-sharing process
o evaluating the inormation is rather
long and resource intensive
Nevertheless compared to the PUMA con-
cept this scheme proved more successul
in terms o output and in recommending
and implementing changes to the sum-
mary o product characteristics o author-
ised products In its public consultationthe Commission called Articles 45 and 46
the lsquohidden gemsrsquo o the Regulation
One drawback that remains however
is reluctance by marketing authorisa-
tion holders to update the summary o
product characteristics on a voluntary
basis This said the Regulation contains
mechanisms to overcome such reluctance
as it empowers competent authorities to
directly update the summary and varythe marketing authorisation accordingly
Moreover in accordance with Article 23
o Directive 200183EC22 and Article 16
o Regulation (EC) No 726200423 mar-
22 Directive 200183EC othe European Parliament and
o the Council o 6 November2001 on the Community
code relating to medicinalproducts or human use OJ L311 28112001 p 67
23 Regulation (EC) No7262004 o the European
Parliament and o the Coun-cil o 31 March 2004 layingdown Community procedures
or the authorisation andsupervision o medicinalproducts or human and
veterinary use and establish-ing a European Medicines
Agency OJ L 136 3042004p 1
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1736
17
lead to competition among companies to
find investigators and study participants
as well as the duplication o trials which
are unnecessary rom a scientific and
ethical point o view
The Paediatric Committee is able to waive
paediatric trial requirements where thespecific medicinal product does not rep-
resent a significant therapeutic benefit
over an existing treatment or paediatric
patients including once the product is au-
thorised (Article 11) However this option
does not provide a way out in the early
stages o product development where
the Committee has to ensure equal treat-
ment and non-discriminatory approaches
The key to avoiding such unnecessary tri-
als is transparency with regard to ongoingand completed trials The situation contin-
ues to be monitored
Finally it is in the interest o the EU that
paediatric trials stemming rom paedi-
atric investigation plans are conducted
within the EU This has less to do with
the standards under which a trial is con-
ducted given that clinical trials carried
out outside the EU have to meet the ethi-
cal and scientific requirements o the EUprovisions on clinical trials24 than with the
act that studies within the EU may pro-
vide patients there with early access to
innovative medicines To date there is in-
sufficient data on the ratio between pae-
diatric trials conducted within and outside
the EU However in view o the upgraded
unctionalities o the EudraCT database it
is expected that more data will be avail-
able in 2017 or the second report
56 Spreading the news mdash
getting new information
to patients and healthcare
professionals
I the Regulation is to be a success it is
not only necessary that data on the use
o a specific product in the paediatric
population are collected but that these
data are then also appropriately commu-
nicated to and used by paediatricians intheir day-to-day work or the benefit o
their patients
In this regard some studies published in
the medical literature suggest a ailure
on the part o practitioners to recognise
the actual amount o off-label prescrib-
ing to children Moreover it is claimed that
the prescribing habits o practitioners are
ofen strongly influenced by personal ex-
perience rather than by evidence-based
inormation or paediatric medicine25
These studies in making generalisations
may not have taken into account the het-
erogeneity o healthcare proessionals
whose receptiveness varies greatly ac-
cording to their work setting and specific
area o specialisation At the same time
such observations may point to a sub-
stantial hurdle in achieving the goal o the
Paediatric Regulation
National competent authorities as well as
organisations or healthcare proessionals
seem particularly qualified to consider ap-
propriate ways o ensuring an adequate
flow o inormation Some Member States
have already established a number o
tools to communicate effectively and e-
ficiently with healthcare proessionals
eg by means o regular meetings web-
based inormation distribution systems ornational ormularies
57 Is the burden greater
than rewards
There can be no doubt that the Paediat-
ric Regulation places a considerable ad-
ditional burden on pharmaceutical com-
panies with its obligations regarding
research on products or use in children
However this approach was adopted be-cause market orces alone proved insu-
ficient to stimulate adequate research
The Regulation requires companies to
submit paediatric investigation plans at
an early stage o product development
However research on some active sub-
stances may be discontinued at later
stages should urther studies ail to show
potential with respect to the saety and
efficacy o the product For every success-
ul authorised medicinal product there aremany that ail to make the finishing line
Hence not all approved paediatric investi-
gation plans will be completed as compa-
24 Directive 200120EC othe European Parliament
and o the Council on theapproximation o the laws
regulations and administra-tive provisions o the Mem-ber States relating to the
implementation o good clini-cal practice in the conducto clinical trials on medicinal
products or human use OJ L121 152001 p 34
25 5-year report to theEuropean Commission (seeootnote 3) page 41
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1836
18
nies may decide to stop the correspond-
ing adult development It is too early still
to obtain reliable statistics that show
the ratio between completed and non-
completed paediatric investigation plans
but in the current context not all approved
plans will eventually result in an approved
medicine with a paediatric indication
In terms o output this entails some un-
necessary effort in compiling and screen-
ing paediatric investigation plans To what
extent this is offset by the benefit o early
submission which ensures that the pae-
diatric development fits smoothly into the
overall product development need ur-
ther monitoring
A urther point o concern is the highnumber o modifications to paediat-
ric investigation plans Figures seem to
suggest that nearly all plans have to
be modified at least once Conceptually
though this does not come as a surprise
in view o the early submission o pae-
diatric investigation plans the length o
adult and paediatric developments and
the substantial deerrals granted An
RampD plan requently has to be adapted
or amended to take account o initial re-sults Recruitment problems or necessary
design changes in the trials may also lead
to modifications While it is acknowledged
that substantial amendments or modifi-
cations to the plan have to be subject to
discussions with the Paediatric Commit-
tee this is less obvious or minor changes
In this context the level o detail required
by the EMA has been repeatedly criticised
In the past five years the EMA and its
Paediatric Committee have made effortsto provide or some flexibility in the plan
so to allow a margin o manoeuvre that
takes account o uncertainties in relation
to certain parameters o a trial
In any case the Commission intends to
review its Communication on the ormat
and content o applications or agree-
ment or modification o a paediatric in-
vestigation plan to take into account the
experience gained including the consider-
able number o modification requests
On a positive note it can be noted that
companies are applying or the rewards
provided by the Regulation primarily the
6-month extension o the Supplementary
Protection Certificate which have been
introduced to offset the additional bur-
den The economic value o the reward
depends on the turnover o the product
concerned In the case o blockbuster
products the amount may be consider-
able while or niche products the effect
is small
An in-depth evaluation o the economic
impact will be included in the 2017 report
in order to draw conclusions on the bal-
ance between burden and rewards and
public health benefits
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1936
19
6Outlook mdash
A fairy-taleending aheadlsquoBetter Medicines or Children mdash From
Concept to Realityrsquo is the title o this re-
port Readers may suggest that based on
the evaluation reerred to above it would
be more appropriate to add a question
mark It is evident that it is too early still
to make a firm statement Despite more
than five years o experience the true im-pact o the Regulation on the health o
children will only become apparent over
time as experience is accumulated in the
longer term
There are encouraging signs though
Paediatric development has become a
more integral part o the overall develop-
ment o medicinal products in the EU A
number o new products with paediatric
indications and age-appropriate pharma-ceutical orms have been authorised and
made available to patients A high num-
ber o agreed paediatric investigation
plans indicates that urther products are
in the pipeline
However it needs to be pointed out that it
would be wrong to expect the Regulation
to be able to solve all problems Instead
it is a major catalyst to improve the situ-
ation o young patients
Finally some weaknesses and deficits
have also become apparent in the last
five years Their impact on the overall
perormance o the Regulation has to be
closely monitored On the basis o the ac-
tions outlined above the Commission in-
tends to fine-tune the current implemen-
tation together with the EMA
Even i better medicines or children are
not yet a reality it should be the ambitiono all stakeholders involved that this piece
o legislation will be or the greater good
o children so that in the 2017 report
the discussion will ocus not on whether a
question mark should be added to the ti-
tle o the report but on whether it should
be an exclamation mark instead
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2036
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2136
21
ANNEXES
Figures and Tables
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2236
22
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2336
23
ANNEX I
Figures and Tables
Table 1Agreed paediatric investigations plans (PIPs) 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Agreed PIPs submitted under Article 7 (without waivers)
Agreed PIPs submitted under Article 8 (without waivers)
Source EMA Paediatric database The numbers on agreed PIPs correspond to EMA decisions
Table 2Agreed paediatric investigations plans (PIPs) compared to ull waivers and modifications 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Submitted modifications of an agreed PIP
Agreed Full waivers
Source EMA Paediatric database The numbers on agreed PIPs and waivers correspond to EMA decisions
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2536
25
Table 5Scientific advice and protocol assistance including ollow-ups (provided by the EMA Scientific Advice Working
Party and the Committee or Human Medicinal Products per year)
259
277321
388 400 433 420
021 32
74 8057
91
0 0 0
68 8067
94
0
100
200
300
400
500
2006 2007 2008 2009 2010 2011 2012
Total number of advice (Scientific Advice and Protocol Assistance)
Sum of paediatric-only and mixed (adult and paediatric development questions)
advice
Paediatric-only or mixed advice that involved a Paediatric Committee member(s) as
expert(s)
Source EMA databases Year o advice letter
Year o start o procedure
Table 6Paediatric clinical trials by year o authorisation
2005 2006 2007 2008 2009 2010 2011 2012
Paediatric trials
(number) 254 316 355 342 404 379 334 332
Paediatric trials
that are part of anagreed PIP 2 1 2 6 16 30 76 76
Proportion of
paediatric trials
that are part of an
agreed PIP among
paediatric trials 1 0 1 2 4 8 23 23
Total number
of trials (adults
and or children) 3 350 3 979 4 749 4 512 4 445 4 026 3 809 3 698
Proportion of
paediatric trials of
all trials 8 8 7 8 9 10 9 9
Source EudraCT Data Warehouse using a predefined query on 6 March 2013 and counting the first authorised trial only in the case o more thanone Member State This partial inormation requires sponsors to use a Clinical Trial Application orm that was only available rom November 2009 or use with version 8 o EudraCT
(available rom 2011)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2636
26
Table 7Number o children to be enrolled in clinical trials
Number
of subjects 2006 2007 2008 2009 2010 2011 2012
Pretermnewborns 0 0 0 207 82 2 281 1 712
Newborns 0 0 5 64 169 1 105 1 172
Infants and
toddlers 330 21 20 59 351 2 788 3 141
Children 2 142 181 200 2 230 2 055 10 325 20 677
Adolescents 368 111 205 1 577 2 861 9 054 13 193
Sum of
above 2 840 313 430 4 137 5 517 25 553 39 895
Reference
number of paediatric
trials 316 355 342 404 379 334 332
Source EudraCT Data Warehouse using a pre-defined query on 6 March 2013 modified by excluding studies or lsquoimmunological medicinal productsrsquo
Table 8EU budget contribution to the Paediatric Regulation and the EMA expenditure
0
1
2
3
4
5
6
7
8
9
10
2006 2007 2008 2009 2010 2011 2012
EU budget contribution (in Million euro)
EMA expenditure for paediatri cs (in Mill ion euro)
EMA expenditure for paediatr ics including support (in Million euro)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2736
27
Table 9Percentage o European Medicines Agencyrsquos human resources working in the paediatric area rom 2006 (inner
circle) to 2012 (outer circle)
733 (2012)
052 (2006)
Table 10Member States acting as rapporteurs or the assessment o studies submitted in accordance with Article 46
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE SE NL FR DK IT BE PL ES NO SK FI IE RO AT HU EL CZ PT LV BG
Study included in worksharing Rapporteur appointed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2836
28
Table 11Member States acting as rapporteur or the assessment o studies submitted in accordance with Article 45
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE NL DK AT FR PL SE ES IE CZ MT IT BE SI EE FI HU NO RO BG EL LV PT IS SK
Wave 1 Wave 2 Wave 3 Wave 4 Wave 5 Wave 6 Wave 7 Wave 8 Wave 9
Wave 10 Wave 11 Wave 12 Wave 13 Wave 14 Wave 15 Wave 16 Wave 17 Wave 18
Table 12Member States acting as rapporteurspeer reviewers in EMArsquos Paediatric Committee procedures (initial PIP
waiver or modification o an agreed PIP)
0
50
100
150
200
250
300
350
400
450
500
A u s t r i a
B el gi um
B ul g a r i a
C y pr u s
C z e c h R e p u b l i c
D enm a r k
E s t oni a
F i nl a n d
F r a n c e
G er m a n y
G r e e c e
H e a l t h c a r e a n d
A c a d emi a
H un g a r y
I c el a n d
I r el a n d
I t a l y
L a t vi a
L i t h u a ni a
L ux em b o ur g
M a l t a
N or w a y
P a t i en t s Or g a ni s a t i on
P ol a n d
P or t u g a l
R om a ni a
S l ov a k i a
S l ov eni a
S p a i n
S w e d en
T h eN e t h er l a n d
s
U ni t e d K i n g d om
Initial PIP applications PIP modifications
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2936
29
ANNEX II
Detailed inventory of centrally authorised medicinalproducts for paediatric use since the entry into force
of the Paediatric Regulation
Table 13Medicinal products authorised centrally since 2007 which include a paediatric indication
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Retapamulin Altargo 2007 No Mixed
Nelarabine Atriance 2007 No Mixed
Human papillomavirus vaccine[types 16 18] Cervarix 2007 No Mixed
Hydroxocobalamin Cyanokit 2007 No Mixed
Idursulase Elaprase 2007 No Mixed
Gadoversetamide Optimark 2007 No Mixed
Betaine anhydrous Cystadane 2007 No Mixed
Stiripentol Diacomit 2007 No Paediatric only
Mecasermin Increlex 2007 No Paediatric only
Rufinamide Inovelon 2007 No Mixed
Hydroxycarbamide Siklos 2007 No Mixed
Human normal
immunoglobulin (ivig) Flebogamma DIF 2007 No Mixed
Fluticasone uroate Avamys 2008 No Mixed
Human normal immunoglobulin Privigen 2008 No Mixed
Lacosamide Vimpat 2008 No Mixed
Micaungin Mycamine 2008 No Mixed
Sapropterin Kuvan 2008 No Mixed
Sugammadex Bridion 2008 No Mixed
Tocoersonal d-alpha
tocopheryl polyethylene glycol
succinate Vedrop 2009 No Paediatric only
Miamurtide Mepact 2009 No Mixed
Rilonacept Rilonacept Regeneron 2009 No Mixed
Tacrolimus Modigra 2009 No Mixed
Pneumoccocal polysaccharideconjugate vaccine (adsorbed) Synflorix 2009 No Paediatric only
Canakinumab
Ilaris (PIP not yet
completed) 2009 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3036
30
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Pneumoccocal polysaccharide
conjugate vaccine (13-valentadsorbed)
Prevenar 13 (PIP not yetcompleted) 2009 Yes Paediatric only
Meningococcal group a c
w135 and y conjugate vaccine Menveo 2010 Yes Mixed
Velaglucerase ala
Vpriv (PIP not yet
completed) 2010 Yes Mixed
Influenza vaccine (live
attenuated nasal) Fluenz (Waiver) 2011 Yes Paediatric only
C1 inhibitor human
Cinryze (PIP not yet
completed) 2011 Yes Mixed
Dihydroartemisinin
piperaquine phosphate
Eurartesim (PIP not yet
completed) 2011 Yes Mixed
Midazolam Buccolam 2011 Yes (PUMA) Paediatric only
EverolimusVotubia(PIP not yet completed) 2011 Yes Mixed
Tobramycin
Tobi Podhaler (PIP not
yet completed) 2011 Yes Mixed
Nomegestrol estradiol Ioa Zoely 2011 Yes Mixed
Colistimethate sodium Colobreathe 2012 Yes Mixed
Mercaptopurine Xaluprine 2012 No Mixed
Catridecacog NovoThirteen 2012 Yes MixedEavirenz Eavirenz Teva 2012 No Mixed
Ivacafor Kalydeco 2012 Yes Mixed
Desloratadine Desloratadine ratiopharm 2012 No Mixed
Desloratadine Desloratadine Actavis 2012 No Mixed
Perampanel Fycompa 2012 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3136
31
Table 14List o centrally authorised medicinal products or which the therapeutic indication was extended to or amend-
ed or the paediatric population
Active substance(s)
Trade
name Date Subject of the extension
Levetiracetam Keppra
2007
2009
Extension o the indication to include adjunctive ther-
apy in the treatment o primary generalised tonic-
clonic (PGTC) seizures in adults and adolescents rom
12 years o age with idiopathic generalised epilepsyExtension o indication to include the adjunctive
treatment o partial seizures with or without second-
ary generalisation in children rom 1 month to lt4
years old
Pneumococcal sac-
charide conjugated
vaccine adsorbed Prevenar 2007
Extension o the indication to include new inorma-
tion on efficacy against disease caused by Strepto-
coccus pneumoniae serotypes 4 6B 9V 14 18C 19F
and 23F in otitis mediaExtension o indication rom active immunisation
against bacteraemic pneumonia to active immunisa-
tion against pneumonia
Infliximab
Remi-
cade 2007
Extension o indication to include treatment o
severe active Crohnrsquos disease in children aged 6 to
17 years
Darbepoetin ala Aranesp 2007
Extension o indication or CRF patients whichrestricted the use o Nespo to paediatric subjects ge
11 years o age
Fosamprenavir Telzir 2007
Extension o indication o Telzir in combination withritonavir or the treatment o Human Immunodefi-
ciency Virus Type 1 (HIV-1) inected adults in combi-nation with other antiretroviral medicinal products to
include paediatric populations
Lamivudine zidovu-
dine Combivir 2007
Extension o indication to include paediatric patients
and replacement o film-coated tablets by scored
film-coated tablets
Desloratadine Aerius 2007Extension o indication rom lsquochronic idiopathic urti-cariarsquo to lsquourticariarsquo
Insulin glulisine Apidra 2007
Extension o indication to include 6 year olds and
older children based on the results o 2 paediatricstudies
Human papilloma virusvaccine [types 6 11
16 18] (recombinantadsorbed) Gardasil 2008
Extension o indication to include the prevention ohigh-grade vaginal dysplastic lesions (VaIN 23)
Adalimumab Humira 20082011
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in adoles-cents rom 13 to 17 years o age
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in the paedi-
atric population aged rom 4 to 12 years
Caspoungin Cancidas 2008
Extension o the indication to include the paediatric
population
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 836
8
The Regulation gives the EMA and its
Paediatric Committee primary responsi-
bility or handling paediatric investigation
plans deerrals and waivers This provides
the Agency with concrete decision-mak-
ing powers
The operational costs o the PaediatricRegulation are partly covered by a contri-
bution rom the EU budget (see Table 8)
as its main activities do not attract any
ees For the period 2007-12 the EU
budget contribution amounted to more
than EUR 39 million In addition Member
Statesrsquo national competent authorities
contribute resources in kind especially
staff time or the assessment o paediat-
ric investigation plans (see Table 12)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 936
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1036
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1136
11
cantly (see Table 5) despite the act that
issues o pharmaceutical non-clinical and
clinical development are also part o the
discussions o a paediatric investigation
plan To acilitate collaboration with the
Paediatric Committee joint procedures
have been created within the EMA
413 Clinical trials with children
Medicines or use in children need to be
tested with appropriate ormulations in
the paediatric population to ensure their
sae and effective use Hence it is gener-
ally accepted that the Paediatric Regula-
tion will lead to more clinical trials in chil-
dren The figures in the EudraCT database
have not yet shown an increase in paedi-
atric trials The number remained stablebetween 2006 and 2012 averaging 350
trials per year with some fluctuations (see
Table 6) It should be pointed out how-
ever that while the number o paediat-
ric trials remained stable the number o
clinical trials in all populations decreased
between 2007 and 2011
Moreover until recently EudraCT was lim-
ited to paediatric trials commencing in the
EU Data on paediatric trials that are parto a paediatric investigation plan and con-
ducted outside the EU have only become
publicly available since spring 2011
It should also be noted that the initiation
o a considerable percentage o clinical
trials included in a paediatric investiga-
tion plan has been deerred in order to
avoid delays in the authorisation o the
corresponding product or adults Hence
the impact o the Paediatric Regulation on
paediatric trials will become more appar-
ent in EudraCT in the years to come There
has however been an evident increase in
the number o paediatric study partici-
pants in particular or the age group rom
0 to 23 months who were normally not
included in trials prior to 2008 (see Ta-
ble 7) Allowing neonates and inants to
benefit rom research is a positive sign
as these have been the most neglected
groups so ar
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1236
12
414 Optimised framework and
coordination
The Paediatric Regulation osters a com-
prehensive network o expertise in paedi-
atric matters within the EU In this context
the role o the Paediatric Committee ispivotal as it brings together a high level
o expertise and competence
The Committee has contributed to the
scientific guidelines published by the EMA
and has so ar convened 22 expert work-
shops on the development o medicines
or children
In addition the European Network or
Paediatric Research at the EMA (Enpr-
EMA) was established in 2009 While aclosely-knit network o experts existed
prior to the introduction o the Regula-
tion in disease areas such as paediatric
oncology Enpr-EMA provides the added
value o a holistic approach by bringing
together national and European networks
investigators and centres with specific ex-
pertise in designing and conducting high-
quality studies in children
However question still remain as towhether this expertise translates into su-
ficient capacity within the EU to conduct
trials in specialised investigation settings
Well-developed research networks capa-
ble o acilitating the necessary research
to ulfil the commitments included in
paediatric investigation plans do exist in
some but not all Member States
415 International cooperation
On an international level the EMA has de-veloped international links with medicines
agencies in the United States Canada
and Japan O particular interest is the
cooperation with the US Food and Drug
Administration given that already in the
late 1990s the United States introduced
legislation that stimulated the develop-
ment o medicinal products or paediatric
use by means o a combination o incen-
tives and obligations This cooperation is
also o great interest to stakeholders as
it may give companies the possibility o
satisying the legislation in both regions
with the same studies
In addition the EMA participates actively
in the Paediatric medicines regulatory
network16 which was created in 2010 as
part o the WHOrsquos Better Medicines or
Children initiative
42 More medicines available
for children
Over 12 years (rom 1995 to 2006) 108
o all 317 indications o 262 centrally au-
thorised medicines included the paediat-
ric population Since the Paediatric Regu-
lation entered into orce 31 out o 152
new medicines have been authorised or
paediatric use 10 o which met the con-
ditions o Article 7 This is not more than
a lsquosnapshotrsquo o the effects o the Regula-
tion as this figure is likely to increase inthe uture as a considerable number o
the new already authorised medicines
are subject to an investigation plan where
completion was deerred to avoid delays
in the authorisation o the adult product
It ollows that in the years to come many
more o those 152 new medicines are ex-
pected to be authorised or paediatric use
Annual reports on deerred paediatric
studies o authorised medicines indicate
that the majority o paediatric investiga-tion plans are running to schedule Pae-
diatric research is on-going at the same
rate across therapeutic areas such as on-
cology vaccines and immunology-rheu-
matology-transplantation
Furthermore by the end o 2011 72 new
paediatric indications had been approved
or medicines already authorised includ-
ing 30 indications (18 centralised) arising
rom the obligation in Article 8 Moreover26 new pharmaceutical orms were au-
thorised or paediatric use including 18
adapted orms or centrally authorised
medicines
As ar as Paediatric Use Marketing Au-
thorisation is concerned to date only one
authorisation has been granted This alls
short o initial expectations
16 httpwwwwhointchild-medicinespaediatric_regula-
torsen
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1336
13
A detailed inventory o centrally autho-
rised products is provided in Annex II
Rewards and incentives
Companies that have complied with the
obligations o the Regulation may benefit
rom a reward once the product concerned
is authorised or the product inormation isamended The reward takes the orm o a
6-month extension o the supplementary
protection certificate (SPC) provided or
by Regulation (EC) No 469200917 or in
the case o an orphan medicinal product
by an extension o the ten-year period o
orphan market exclusivity to twelve years
No orphan rewards have been awarded
yet In this regard it is observed that some
companies withdrew the orphan designa-tion o a product in order to qualiy or
the SPC reward rather than the orphan
reward which seems to be more attrac-
tive rom an economic perspective As ar
as SPC extensions are concerned national
patent offices in 16 Member States had
by the end o 2011 granted 6-month ex-
tensions to 11 medicinal products which
resulted in a total o more than 100 na-
tional SPCs
It should be pointed out that a ruling othe European Court o Justice urther
increased the value o the paediatric
reward as it made clear that the initial
certificate could have a negative or zero
duration which could then become posi-
tive once the paediatric extension was
granted18
43 Increased information on
medicines used in childrenTo provide better inormation on the use
o medicinal products in children Article
45 o the Paediatric Regulation requires
companies holding data on the saety
or efficacy o authorised products in the
paediatric population to submit these
studies to the competent authorities In
this way the data can be assessed and
where appropriate the authorised prod-
uct inormation amended Article 46 o
the Regulation also requires companies tosubmit newly generated paediatric data
Since 2008 more than 18 000 study re-
ports on roughly 2 200 medicinal prod-
ucts have been submitted revealing the
large amount o existing paediatric inor-
mation available at company level
These study reports have been and
continue to be assessed by the compe-
tent authorities thanks to an impressive
work-sharing project (see Tables 10 and11) For nationally authorised products
this has led to the publication o assess-
ment reports covering more than 140
active substances and in a considerable
number o cases to recommendations
or changes to the summaries o product
characteristics o authorised products re-
sulting in 65 actual changes For centrally
authorised products by 2011 the Agency
had completed the assessment o all the
data submitted under Article 45 covering55 active substances in 61 centrally ap-
17 Regulation (EC) No4692009 o the Euro-
pean Parliament and othe Council o 6 May 2009
concerning the supplemen-tary protection certificateor medicinal products OJ
L 152 1662009 p 1 ThisRegulation is a codificationo Council Regulation (EEC)
No 176892
18 Case C-12510 Merck
Sharp amp Dohme v DeutschesPatent- und Markenamt notyet published in the ECR
paragraph 37 lsquoi the SPCapplication had to be reused
because the calculationprovided or in Article 13(1)o Regulation No 176892
results in a negative or zero
duration the holder o thebasic patent could not obtain
an extension o protectionconerred by such a patenteven i it conducted all the
studies according to the ap-proved paediatric investiga-
tion plan under Article 36 oRegulation No 19012006Such a reusal would be
liable to adversely impacton the useul effect oRegulation No 19012006
and might jeopardise the
objectives o that regulationnamely the compensation
o effort made to evaluatethe paediatric effects o themedicinal product at issuersquo
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1436
14
proved medicinal products The summa-
ries o product characteristics o 12 me-
dicinal products were changed ollowing
the assessment
5Lessonslearnt51 Better access to
treatment
One o the explicit goals o the Paediatric
Regulation is to increase the number oproducts that are researched developed
and authorised or use in children and
to reduce the off-label use o medicinal
products in the paediatric population
The main tool to achieve this result is to
oblige companies to establish a paediat-
ric investigation plan or each newly de-
veloped product or or the line extension
o an already authorised product that is
still under patent protection The plan ismeant to ensure mdash under the supervi-
sion o the Paediatric Committee mdash that
the necessary data are generated so as
to determine the conditions under which
a medicinal product may be authorised
to treat children Since 2008 more than
600 paediatric investigation plans have
been approved However only a minor-
ity o them has been completed to date
the vast majority are still on-going This
is due to the long development cycles omedicinal products ofen lasting more
than a decade and the near-systematic
deerral o paediatric studies The high
number o deerrals may not have been
initially expected but are currently a real-
ity as or most o the medicinal products
that have been authorised so ar the RampD
programme started beore the entering
into orce o the Regulation Consequent-
ly the paediatric requirements could not
be taken into account rom the beginningo the product development
While the Paediatric Regulation has led
to some new authorisations that include
paediatric indications the regulatory in-
strument is recent and it will probably
take at least a decade beore it can be
judged in terms o its output In terms o
pharmaceutical orms there is however
already a visible positive impact
In this context criticism has been voiced
that the Regulation will ail to ensure abreakthrough in areas o particular pae-
diatric need such as paediatric oncology
This argument is related to the act that
the starting point or the majority o pae-
diatric investigation plans is an ongoing
RampD programme or a medicinal product
or adults An intrinsic consequence o this
approach is that these products primarily
target adult conditions They are devel-
oped in areas where there is a need (or a
market) in the adult population This needin the older population does not neces-
sarily correspond to the paediatric popu-
lationrsquos need
Moreover the Regulation grants waivers
rom its obligations where the disease or
condition or which the specific medicinal
product is intended occurs only in adult
populations This legislative approach cre-
ates riction in the case o diseases that
are specific and exclusive to children Italso limits the powers and possibilities o
the Paediatric Committee when reviewing
and agreeing to a paediatric investigation
plan as regards the scope o studies that
the Committee may request rom appli-
cants ollowing the objective and scien-
tific-based assessment o the compound
concerned19
These constraints and boundaries have to
be taken into account when judging the
impact the Regulation is likely to make In
addition the effect o instruments such as
the Orphan Regulation have to be consid-
ered given that or example all paediatric
cancers are rare diseases and all under
the EU policy ramework on rare diseases
All in all the achievements highlighted in
chapter 4 o this report and the number
o products with new paediatric indica-
tions show that there are some encourag-
ing signs afer this first five-year period it
is however too early or comprehensive
answers
19 Case T-5209 Nycomed vEMA not yet published
See the results o the publicconsultation conducted by
the Commission in prepara-tion o this Report
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1536
15
52 The PUMA concept a
disappointment
The Paediatric Regulation introduced a
new type o marketing authorisation mdash
the Paediatric Use Marketing Authorisa-
tion (PUMA) As an incentive to carry out
research into the potential paediatric use
o off-patent medicinal products that have
been authorised or adults this marketing
authorisation offers 8 years o data and
10 years o market exclusivity to any new
off-patent product developed exclusively
or use in the paediatric population Thus
the main goal o the PUMA concept is to
stimulate research in existing products
This scheme has been supported by EU
unding through the EU Framework Pro-
grammes or Research and Technological
Development
However to date only one PUMA has been
granted with a ew more projects cur-
rently in the pipeline
Neither industry nor academic networks
have embraced this opportunity as ully
as the Regulation intended It would seem
that the incentive o data and market ex-
clusivity does not work or these productsor at least that the market opportunities
in this sector are currently considered in-
sufficient to outweigh the inherent eco-
nomic risks o pharmaceutical develop-
ment Researchers are not engaging in
trials with medicines that have been on
the market or years Companies seem to
ear that market exclusivity will not pre-
vent physicians rom continuing to use
competitor products with the same active
ingredient off-label at lower costs or thatsubstitution or cheaper adult orms takes
place at the level o pharmacies Moreo-
ver national pricing and reimbursement
rules in Member States ofen do not al-
low or the additional research needed to
obtain the PUMA to be rewarded in price
negotiations20
Against this background the PUMA con-
cept has ailed so ar to ulfil the initial
expectationsThe EMA will in uture accept paediatric
investigation plans or a PUMA that cover
only certain age groups and not the en-
tire paediatric population This may offset
some o the reservations that currently
hamper better endorsement o the PUMA
concept
53 No impact on adultdevelopment
Studies prior to the adoption o the Regu-
lation have suggested a theoretical risk
that the requirements or research in chil-
dren could lengthen the overall drug de-
velopment process21 The Regulation has
met this risk head-on In order to avoid
any delays in authorising medicines or
other populations it allows or the grant-
ing o deerrals relating to the initiation orcompletion o some or all o the meas-
ures contained in a paediatric investiga-
tion plan
Experience shows that the deerral is a
widely used instrument which suggests
that the risk o delays in the processing o
adult applications is minimal There have
been some transitional problems in cases
where the adult programme was already
established when the Regulation enteredinto orce but these issues seem to have
been resolved
A concern that was raised initially was
that some companies would become
reluctant to develop new indications
pharmaceutical orms and new routes o
administration in small markets and or
products with low sales to avoid being
bound by the paediatric obligation under
Article 8 o the Regulation However thereis no evidence o such effect Moreover
it may also be argued that the incentive
o a potential six-month extension o the
SPC served to counterbalance such an
effect as it may have led companies to
examine more thoroughly the benefits o
a line extension taking into account the
economic value o the paediatric reward
Still industry stakeholders claim that
in rare cases the development or new
medicinal products has been delayedor abandoned in the expectation or as a
consequence o additional costs and re-
quirements associated with paediatric de-
20 See the results o thepublic consultation con-
ducted by the Commission inpreparation o this Report
21 C Commission StaffWorking Document Proposal
or a Regulation o the Euro-pean Parliament and o theCouncil on medicinal prod-
ucts or paediatric use andamending Council Regulation(EEC) No 17692 Directive
200183EC and Regula-tion (EC) No 7262004Extended impact assessment
(COM2004599F)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1636
16
keting authorisation holders are obliged
to ensure that the product inormation
is kept up to date with the current scien-
tific knowledge While preerence should
be given to cooperative approaches the
enorcement tools may need to be used
i companies do not overcome their res-
ervations
On the whole the requirements o Articles
45 and 46 have provided an efficient and
appropriate instrument or collecting and
evaluating existing paediatric studies
55 Clinical trials with
children
It is generally accepted that the Paediatric
Regulation will lead to more clinical trialswith children but that its aims should be
achieved without subjecting children to
unnecessary clinical trials
The youngest paediatric-age subsets
including neonates are particularly sen-
sitive It will be a constant challenge to
balance the therapeutic needs o these
age groups with their specific vulnerability
when considering and deciding on the ap-
propriateness o specific clinical trials or
the specific settings o studies in this age
subset Efforts are thereore continuously
being made to explore alternative means
eg the use o extrapolation modelling
and simulation techniques to reduce the
number o study subjects as much as
possible The Paediatric Committee is ac-
tively contributing to acilitate the devel-
opment and use o such means including
non-conventional trial design
Another challenge is how to avoid dupli-cating trials or different paediatric inves-
tigation plans rom different applicants
Companies embarking on product devel-
opment in similar areas may be required
by the agreed paediatric investigation
plan to conduct studies within similar
settings While collaborative approaches
between companies would be highly de-
sirable and have occurred on rare occa-
sions they ofen conflict with companiesrsquo
understandable reluctance to share datawith competitors in the early stages o
product development and participate in
direct comparisons This situation could
velopment Overall there is however no
evidence that the Regulation has a con-
siderable negative impact on products or
other populations
Rather there are some concerns that the
requirements under the Regulation may
cause delays in the authorisation o prod-ucts with paediatric-only indications as
they bring added complexity to the RampD
and regulatory process or products that
already directly target children The added
value o the submission o a paediatric in-
vestigation plan in these cases will be as-
sessed urther in the 2017 report
54 Reaping the benefits of
existing information
There was widespread speculation prior to
the adoption o the Paediatric Regulation
as to how many studies would be submit-
ted by pharmaceutical companies in ac-
cordance with Articles 45 and 46 The act
that competent authorities received more
than 18 000 studies reveals the consid-
erable amount o paediatric inormation
that existed at company level
Certainly it is true that not all the inor-
mation submitted met modern require-
ments or scientific data and clinical re-
search and that the work-sharing process
o evaluating the inormation is rather
long and resource intensive
Nevertheless compared to the PUMA con-
cept this scheme proved more successul
in terms o output and in recommending
and implementing changes to the sum-
mary o product characteristics o author-
ised products In its public consultationthe Commission called Articles 45 and 46
the lsquohidden gemsrsquo o the Regulation
One drawback that remains however
is reluctance by marketing authorisa-
tion holders to update the summary o
product characteristics on a voluntary
basis This said the Regulation contains
mechanisms to overcome such reluctance
as it empowers competent authorities to
directly update the summary and varythe marketing authorisation accordingly
Moreover in accordance with Article 23
o Directive 200183EC22 and Article 16
o Regulation (EC) No 726200423 mar-
22 Directive 200183EC othe European Parliament and
o the Council o 6 November2001 on the Community
code relating to medicinalproducts or human use OJ L311 28112001 p 67
23 Regulation (EC) No7262004 o the European
Parliament and o the Coun-cil o 31 March 2004 layingdown Community procedures
or the authorisation andsupervision o medicinalproducts or human and
veterinary use and establish-ing a European Medicines
Agency OJ L 136 3042004p 1
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1736
17
lead to competition among companies to
find investigators and study participants
as well as the duplication o trials which
are unnecessary rom a scientific and
ethical point o view
The Paediatric Committee is able to waive
paediatric trial requirements where thespecific medicinal product does not rep-
resent a significant therapeutic benefit
over an existing treatment or paediatric
patients including once the product is au-
thorised (Article 11) However this option
does not provide a way out in the early
stages o product development where
the Committee has to ensure equal treat-
ment and non-discriminatory approaches
The key to avoiding such unnecessary tri-
als is transparency with regard to ongoingand completed trials The situation contin-
ues to be monitored
Finally it is in the interest o the EU that
paediatric trials stemming rom paedi-
atric investigation plans are conducted
within the EU This has less to do with
the standards under which a trial is con-
ducted given that clinical trials carried
out outside the EU have to meet the ethi-
cal and scientific requirements o the EUprovisions on clinical trials24 than with the
act that studies within the EU may pro-
vide patients there with early access to
innovative medicines To date there is in-
sufficient data on the ratio between pae-
diatric trials conducted within and outside
the EU However in view o the upgraded
unctionalities o the EudraCT database it
is expected that more data will be avail-
able in 2017 or the second report
56 Spreading the news mdash
getting new information
to patients and healthcare
professionals
I the Regulation is to be a success it is
not only necessary that data on the use
o a specific product in the paediatric
population are collected but that these
data are then also appropriately commu-
nicated to and used by paediatricians intheir day-to-day work or the benefit o
their patients
In this regard some studies published in
the medical literature suggest a ailure
on the part o practitioners to recognise
the actual amount o off-label prescrib-
ing to children Moreover it is claimed that
the prescribing habits o practitioners are
ofen strongly influenced by personal ex-
perience rather than by evidence-based
inormation or paediatric medicine25
These studies in making generalisations
may not have taken into account the het-
erogeneity o healthcare proessionals
whose receptiveness varies greatly ac-
cording to their work setting and specific
area o specialisation At the same time
such observations may point to a sub-
stantial hurdle in achieving the goal o the
Paediatric Regulation
National competent authorities as well as
organisations or healthcare proessionals
seem particularly qualified to consider ap-
propriate ways o ensuring an adequate
flow o inormation Some Member States
have already established a number o
tools to communicate effectively and e-
ficiently with healthcare proessionals
eg by means o regular meetings web-
based inormation distribution systems ornational ormularies
57 Is the burden greater
than rewards
There can be no doubt that the Paediat-
ric Regulation places a considerable ad-
ditional burden on pharmaceutical com-
panies with its obligations regarding
research on products or use in children
However this approach was adopted be-cause market orces alone proved insu-
ficient to stimulate adequate research
The Regulation requires companies to
submit paediatric investigation plans at
an early stage o product development
However research on some active sub-
stances may be discontinued at later
stages should urther studies ail to show
potential with respect to the saety and
efficacy o the product For every success-
ul authorised medicinal product there aremany that ail to make the finishing line
Hence not all approved paediatric investi-
gation plans will be completed as compa-
24 Directive 200120EC othe European Parliament
and o the Council on theapproximation o the laws
regulations and administra-tive provisions o the Mem-ber States relating to the
implementation o good clini-cal practice in the conducto clinical trials on medicinal
products or human use OJ L121 152001 p 34
25 5-year report to theEuropean Commission (seeootnote 3) page 41
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1836
18
nies may decide to stop the correspond-
ing adult development It is too early still
to obtain reliable statistics that show
the ratio between completed and non-
completed paediatric investigation plans
but in the current context not all approved
plans will eventually result in an approved
medicine with a paediatric indication
In terms o output this entails some un-
necessary effort in compiling and screen-
ing paediatric investigation plans To what
extent this is offset by the benefit o early
submission which ensures that the pae-
diatric development fits smoothly into the
overall product development need ur-
ther monitoring
A urther point o concern is the highnumber o modifications to paediat-
ric investigation plans Figures seem to
suggest that nearly all plans have to
be modified at least once Conceptually
though this does not come as a surprise
in view o the early submission o pae-
diatric investigation plans the length o
adult and paediatric developments and
the substantial deerrals granted An
RampD plan requently has to be adapted
or amended to take account o initial re-sults Recruitment problems or necessary
design changes in the trials may also lead
to modifications While it is acknowledged
that substantial amendments or modifi-
cations to the plan have to be subject to
discussions with the Paediatric Commit-
tee this is less obvious or minor changes
In this context the level o detail required
by the EMA has been repeatedly criticised
In the past five years the EMA and its
Paediatric Committee have made effortsto provide or some flexibility in the plan
so to allow a margin o manoeuvre that
takes account o uncertainties in relation
to certain parameters o a trial
In any case the Commission intends to
review its Communication on the ormat
and content o applications or agree-
ment or modification o a paediatric in-
vestigation plan to take into account the
experience gained including the consider-
able number o modification requests
On a positive note it can be noted that
companies are applying or the rewards
provided by the Regulation primarily the
6-month extension o the Supplementary
Protection Certificate which have been
introduced to offset the additional bur-
den The economic value o the reward
depends on the turnover o the product
concerned In the case o blockbuster
products the amount may be consider-
able while or niche products the effect
is small
An in-depth evaluation o the economic
impact will be included in the 2017 report
in order to draw conclusions on the bal-
ance between burden and rewards and
public health benefits
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1936
19
6Outlook mdash
A fairy-taleending aheadlsquoBetter Medicines or Children mdash From
Concept to Realityrsquo is the title o this re-
port Readers may suggest that based on
the evaluation reerred to above it would
be more appropriate to add a question
mark It is evident that it is too early still
to make a firm statement Despite more
than five years o experience the true im-pact o the Regulation on the health o
children will only become apparent over
time as experience is accumulated in the
longer term
There are encouraging signs though
Paediatric development has become a
more integral part o the overall develop-
ment o medicinal products in the EU A
number o new products with paediatric
indications and age-appropriate pharma-ceutical orms have been authorised and
made available to patients A high num-
ber o agreed paediatric investigation
plans indicates that urther products are
in the pipeline
However it needs to be pointed out that it
would be wrong to expect the Regulation
to be able to solve all problems Instead
it is a major catalyst to improve the situ-
ation o young patients
Finally some weaknesses and deficits
have also become apparent in the last
five years Their impact on the overall
perormance o the Regulation has to be
closely monitored On the basis o the ac-
tions outlined above the Commission in-
tends to fine-tune the current implemen-
tation together with the EMA
Even i better medicines or children are
not yet a reality it should be the ambitiono all stakeholders involved that this piece
o legislation will be or the greater good
o children so that in the 2017 report
the discussion will ocus not on whether a
question mark should be added to the ti-
tle o the report but on whether it should
be an exclamation mark instead
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2036
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2136
21
ANNEXES
Figures and Tables
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2236
22
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2336
23
ANNEX I
Figures and Tables
Table 1Agreed paediatric investigations plans (PIPs) 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Agreed PIPs submitted under Article 7 (without waivers)
Agreed PIPs submitted under Article 8 (without waivers)
Source EMA Paediatric database The numbers on agreed PIPs correspond to EMA decisions
Table 2Agreed paediatric investigations plans (PIPs) compared to ull waivers and modifications 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Submitted modifications of an agreed PIP
Agreed Full waivers
Source EMA Paediatric database The numbers on agreed PIPs and waivers correspond to EMA decisions
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2536
25
Table 5Scientific advice and protocol assistance including ollow-ups (provided by the EMA Scientific Advice Working
Party and the Committee or Human Medicinal Products per year)
259
277321
388 400 433 420
021 32
74 8057
91
0 0 0
68 8067
94
0
100
200
300
400
500
2006 2007 2008 2009 2010 2011 2012
Total number of advice (Scientific Advice and Protocol Assistance)
Sum of paediatric-only and mixed (adult and paediatric development questions)
advice
Paediatric-only or mixed advice that involved a Paediatric Committee member(s) as
expert(s)
Source EMA databases Year o advice letter
Year o start o procedure
Table 6Paediatric clinical trials by year o authorisation
2005 2006 2007 2008 2009 2010 2011 2012
Paediatric trials
(number) 254 316 355 342 404 379 334 332
Paediatric trials
that are part of anagreed PIP 2 1 2 6 16 30 76 76
Proportion of
paediatric trials
that are part of an
agreed PIP among
paediatric trials 1 0 1 2 4 8 23 23
Total number
of trials (adults
and or children) 3 350 3 979 4 749 4 512 4 445 4 026 3 809 3 698
Proportion of
paediatric trials of
all trials 8 8 7 8 9 10 9 9
Source EudraCT Data Warehouse using a predefined query on 6 March 2013 and counting the first authorised trial only in the case o more thanone Member State This partial inormation requires sponsors to use a Clinical Trial Application orm that was only available rom November 2009 or use with version 8 o EudraCT
(available rom 2011)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2636
26
Table 7Number o children to be enrolled in clinical trials
Number
of subjects 2006 2007 2008 2009 2010 2011 2012
Pretermnewborns 0 0 0 207 82 2 281 1 712
Newborns 0 0 5 64 169 1 105 1 172
Infants and
toddlers 330 21 20 59 351 2 788 3 141
Children 2 142 181 200 2 230 2 055 10 325 20 677
Adolescents 368 111 205 1 577 2 861 9 054 13 193
Sum of
above 2 840 313 430 4 137 5 517 25 553 39 895
Reference
number of paediatric
trials 316 355 342 404 379 334 332
Source EudraCT Data Warehouse using a pre-defined query on 6 March 2013 modified by excluding studies or lsquoimmunological medicinal productsrsquo
Table 8EU budget contribution to the Paediatric Regulation and the EMA expenditure
0
1
2
3
4
5
6
7
8
9
10
2006 2007 2008 2009 2010 2011 2012
EU budget contribution (in Million euro)
EMA expenditure for paediatri cs (in Mill ion euro)
EMA expenditure for paediatr ics including support (in Million euro)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2736
27
Table 9Percentage o European Medicines Agencyrsquos human resources working in the paediatric area rom 2006 (inner
circle) to 2012 (outer circle)
733 (2012)
052 (2006)
Table 10Member States acting as rapporteurs or the assessment o studies submitted in accordance with Article 46
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE SE NL FR DK IT BE PL ES NO SK FI IE RO AT HU EL CZ PT LV BG
Study included in worksharing Rapporteur appointed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2836
28
Table 11Member States acting as rapporteur or the assessment o studies submitted in accordance with Article 45
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE NL DK AT FR PL SE ES IE CZ MT IT BE SI EE FI HU NO RO BG EL LV PT IS SK
Wave 1 Wave 2 Wave 3 Wave 4 Wave 5 Wave 6 Wave 7 Wave 8 Wave 9
Wave 10 Wave 11 Wave 12 Wave 13 Wave 14 Wave 15 Wave 16 Wave 17 Wave 18
Table 12Member States acting as rapporteurspeer reviewers in EMArsquos Paediatric Committee procedures (initial PIP
waiver or modification o an agreed PIP)
0
50
100
150
200
250
300
350
400
450
500
A u s t r i a
B el gi um
B ul g a r i a
C y pr u s
C z e c h R e p u b l i c
D enm a r k
E s t oni a
F i nl a n d
F r a n c e
G er m a n y
G r e e c e
H e a l t h c a r e a n d
A c a d emi a
H un g a r y
I c el a n d
I r el a n d
I t a l y
L a t vi a
L i t h u a ni a
L ux em b o ur g
M a l t a
N or w a y
P a t i en t s Or g a ni s a t i on
P ol a n d
P or t u g a l
R om a ni a
S l ov a k i a
S l ov eni a
S p a i n
S w e d en
T h eN e t h er l a n d
s
U ni t e d K i n g d om
Initial PIP applications PIP modifications
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2936
29
ANNEX II
Detailed inventory of centrally authorised medicinalproducts for paediatric use since the entry into force
of the Paediatric Regulation
Table 13Medicinal products authorised centrally since 2007 which include a paediatric indication
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Retapamulin Altargo 2007 No Mixed
Nelarabine Atriance 2007 No Mixed
Human papillomavirus vaccine[types 16 18] Cervarix 2007 No Mixed
Hydroxocobalamin Cyanokit 2007 No Mixed
Idursulase Elaprase 2007 No Mixed
Gadoversetamide Optimark 2007 No Mixed
Betaine anhydrous Cystadane 2007 No Mixed
Stiripentol Diacomit 2007 No Paediatric only
Mecasermin Increlex 2007 No Paediatric only
Rufinamide Inovelon 2007 No Mixed
Hydroxycarbamide Siklos 2007 No Mixed
Human normal
immunoglobulin (ivig) Flebogamma DIF 2007 No Mixed
Fluticasone uroate Avamys 2008 No Mixed
Human normal immunoglobulin Privigen 2008 No Mixed
Lacosamide Vimpat 2008 No Mixed
Micaungin Mycamine 2008 No Mixed
Sapropterin Kuvan 2008 No Mixed
Sugammadex Bridion 2008 No Mixed
Tocoersonal d-alpha
tocopheryl polyethylene glycol
succinate Vedrop 2009 No Paediatric only
Miamurtide Mepact 2009 No Mixed
Rilonacept Rilonacept Regeneron 2009 No Mixed
Tacrolimus Modigra 2009 No Mixed
Pneumoccocal polysaccharideconjugate vaccine (adsorbed) Synflorix 2009 No Paediatric only
Canakinumab
Ilaris (PIP not yet
completed) 2009 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3036
30
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Pneumoccocal polysaccharide
conjugate vaccine (13-valentadsorbed)
Prevenar 13 (PIP not yetcompleted) 2009 Yes Paediatric only
Meningococcal group a c
w135 and y conjugate vaccine Menveo 2010 Yes Mixed
Velaglucerase ala
Vpriv (PIP not yet
completed) 2010 Yes Mixed
Influenza vaccine (live
attenuated nasal) Fluenz (Waiver) 2011 Yes Paediatric only
C1 inhibitor human
Cinryze (PIP not yet
completed) 2011 Yes Mixed
Dihydroartemisinin
piperaquine phosphate
Eurartesim (PIP not yet
completed) 2011 Yes Mixed
Midazolam Buccolam 2011 Yes (PUMA) Paediatric only
EverolimusVotubia(PIP not yet completed) 2011 Yes Mixed
Tobramycin
Tobi Podhaler (PIP not
yet completed) 2011 Yes Mixed
Nomegestrol estradiol Ioa Zoely 2011 Yes Mixed
Colistimethate sodium Colobreathe 2012 Yes Mixed
Mercaptopurine Xaluprine 2012 No Mixed
Catridecacog NovoThirteen 2012 Yes MixedEavirenz Eavirenz Teva 2012 No Mixed
Ivacafor Kalydeco 2012 Yes Mixed
Desloratadine Desloratadine ratiopharm 2012 No Mixed
Desloratadine Desloratadine Actavis 2012 No Mixed
Perampanel Fycompa 2012 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3136
31
Table 14List o centrally authorised medicinal products or which the therapeutic indication was extended to or amend-
ed or the paediatric population
Active substance(s)
Trade
name Date Subject of the extension
Levetiracetam Keppra
2007
2009
Extension o the indication to include adjunctive ther-
apy in the treatment o primary generalised tonic-
clonic (PGTC) seizures in adults and adolescents rom
12 years o age with idiopathic generalised epilepsyExtension o indication to include the adjunctive
treatment o partial seizures with or without second-
ary generalisation in children rom 1 month to lt4
years old
Pneumococcal sac-
charide conjugated
vaccine adsorbed Prevenar 2007
Extension o the indication to include new inorma-
tion on efficacy against disease caused by Strepto-
coccus pneumoniae serotypes 4 6B 9V 14 18C 19F
and 23F in otitis mediaExtension o indication rom active immunisation
against bacteraemic pneumonia to active immunisa-
tion against pneumonia
Infliximab
Remi-
cade 2007
Extension o indication to include treatment o
severe active Crohnrsquos disease in children aged 6 to
17 years
Darbepoetin ala Aranesp 2007
Extension o indication or CRF patients whichrestricted the use o Nespo to paediatric subjects ge
11 years o age
Fosamprenavir Telzir 2007
Extension o indication o Telzir in combination withritonavir or the treatment o Human Immunodefi-
ciency Virus Type 1 (HIV-1) inected adults in combi-nation with other antiretroviral medicinal products to
include paediatric populations
Lamivudine zidovu-
dine Combivir 2007
Extension o indication to include paediatric patients
and replacement o film-coated tablets by scored
film-coated tablets
Desloratadine Aerius 2007Extension o indication rom lsquochronic idiopathic urti-cariarsquo to lsquourticariarsquo
Insulin glulisine Apidra 2007
Extension o indication to include 6 year olds and
older children based on the results o 2 paediatricstudies
Human papilloma virusvaccine [types 6 11
16 18] (recombinantadsorbed) Gardasil 2008
Extension o indication to include the prevention ohigh-grade vaginal dysplastic lesions (VaIN 23)
Adalimumab Humira 20082011
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in adoles-cents rom 13 to 17 years o age
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in the paedi-
atric population aged rom 4 to 12 years
Caspoungin Cancidas 2008
Extension o the indication to include the paediatric
population
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 936
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1036
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1136
11
cantly (see Table 5) despite the act that
issues o pharmaceutical non-clinical and
clinical development are also part o the
discussions o a paediatric investigation
plan To acilitate collaboration with the
Paediatric Committee joint procedures
have been created within the EMA
413 Clinical trials with children
Medicines or use in children need to be
tested with appropriate ormulations in
the paediatric population to ensure their
sae and effective use Hence it is gener-
ally accepted that the Paediatric Regula-
tion will lead to more clinical trials in chil-
dren The figures in the EudraCT database
have not yet shown an increase in paedi-
atric trials The number remained stablebetween 2006 and 2012 averaging 350
trials per year with some fluctuations (see
Table 6) It should be pointed out how-
ever that while the number o paediat-
ric trials remained stable the number o
clinical trials in all populations decreased
between 2007 and 2011
Moreover until recently EudraCT was lim-
ited to paediatric trials commencing in the
EU Data on paediatric trials that are parto a paediatric investigation plan and con-
ducted outside the EU have only become
publicly available since spring 2011
It should also be noted that the initiation
o a considerable percentage o clinical
trials included in a paediatric investiga-
tion plan has been deerred in order to
avoid delays in the authorisation o the
corresponding product or adults Hence
the impact o the Paediatric Regulation on
paediatric trials will become more appar-
ent in EudraCT in the years to come There
has however been an evident increase in
the number o paediatric study partici-
pants in particular or the age group rom
0 to 23 months who were normally not
included in trials prior to 2008 (see Ta-
ble 7) Allowing neonates and inants to
benefit rom research is a positive sign
as these have been the most neglected
groups so ar
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1236
12
414 Optimised framework and
coordination
The Paediatric Regulation osters a com-
prehensive network o expertise in paedi-
atric matters within the EU In this context
the role o the Paediatric Committee ispivotal as it brings together a high level
o expertise and competence
The Committee has contributed to the
scientific guidelines published by the EMA
and has so ar convened 22 expert work-
shops on the development o medicines
or children
In addition the European Network or
Paediatric Research at the EMA (Enpr-
EMA) was established in 2009 While aclosely-knit network o experts existed
prior to the introduction o the Regula-
tion in disease areas such as paediatric
oncology Enpr-EMA provides the added
value o a holistic approach by bringing
together national and European networks
investigators and centres with specific ex-
pertise in designing and conducting high-
quality studies in children
However question still remain as towhether this expertise translates into su-
ficient capacity within the EU to conduct
trials in specialised investigation settings
Well-developed research networks capa-
ble o acilitating the necessary research
to ulfil the commitments included in
paediatric investigation plans do exist in
some but not all Member States
415 International cooperation
On an international level the EMA has de-veloped international links with medicines
agencies in the United States Canada
and Japan O particular interest is the
cooperation with the US Food and Drug
Administration given that already in the
late 1990s the United States introduced
legislation that stimulated the develop-
ment o medicinal products or paediatric
use by means o a combination o incen-
tives and obligations This cooperation is
also o great interest to stakeholders as
it may give companies the possibility o
satisying the legislation in both regions
with the same studies
In addition the EMA participates actively
in the Paediatric medicines regulatory
network16 which was created in 2010 as
part o the WHOrsquos Better Medicines or
Children initiative
42 More medicines available
for children
Over 12 years (rom 1995 to 2006) 108
o all 317 indications o 262 centrally au-
thorised medicines included the paediat-
ric population Since the Paediatric Regu-
lation entered into orce 31 out o 152
new medicines have been authorised or
paediatric use 10 o which met the con-
ditions o Article 7 This is not more than
a lsquosnapshotrsquo o the effects o the Regula-
tion as this figure is likely to increase inthe uture as a considerable number o
the new already authorised medicines
are subject to an investigation plan where
completion was deerred to avoid delays
in the authorisation o the adult product
It ollows that in the years to come many
more o those 152 new medicines are ex-
pected to be authorised or paediatric use
Annual reports on deerred paediatric
studies o authorised medicines indicate
that the majority o paediatric investiga-tion plans are running to schedule Pae-
diatric research is on-going at the same
rate across therapeutic areas such as on-
cology vaccines and immunology-rheu-
matology-transplantation
Furthermore by the end o 2011 72 new
paediatric indications had been approved
or medicines already authorised includ-
ing 30 indications (18 centralised) arising
rom the obligation in Article 8 Moreover26 new pharmaceutical orms were au-
thorised or paediatric use including 18
adapted orms or centrally authorised
medicines
As ar as Paediatric Use Marketing Au-
thorisation is concerned to date only one
authorisation has been granted This alls
short o initial expectations
16 httpwwwwhointchild-medicinespaediatric_regula-
torsen
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1336
13
A detailed inventory o centrally autho-
rised products is provided in Annex II
Rewards and incentives
Companies that have complied with the
obligations o the Regulation may benefit
rom a reward once the product concerned
is authorised or the product inormation isamended The reward takes the orm o a
6-month extension o the supplementary
protection certificate (SPC) provided or
by Regulation (EC) No 469200917 or in
the case o an orphan medicinal product
by an extension o the ten-year period o
orphan market exclusivity to twelve years
No orphan rewards have been awarded
yet In this regard it is observed that some
companies withdrew the orphan designa-tion o a product in order to qualiy or
the SPC reward rather than the orphan
reward which seems to be more attrac-
tive rom an economic perspective As ar
as SPC extensions are concerned national
patent offices in 16 Member States had
by the end o 2011 granted 6-month ex-
tensions to 11 medicinal products which
resulted in a total o more than 100 na-
tional SPCs
It should be pointed out that a ruling othe European Court o Justice urther
increased the value o the paediatric
reward as it made clear that the initial
certificate could have a negative or zero
duration which could then become posi-
tive once the paediatric extension was
granted18
43 Increased information on
medicines used in childrenTo provide better inormation on the use
o medicinal products in children Article
45 o the Paediatric Regulation requires
companies holding data on the saety
or efficacy o authorised products in the
paediatric population to submit these
studies to the competent authorities In
this way the data can be assessed and
where appropriate the authorised prod-
uct inormation amended Article 46 o
the Regulation also requires companies tosubmit newly generated paediatric data
Since 2008 more than 18 000 study re-
ports on roughly 2 200 medicinal prod-
ucts have been submitted revealing the
large amount o existing paediatric inor-
mation available at company level
These study reports have been and
continue to be assessed by the compe-
tent authorities thanks to an impressive
work-sharing project (see Tables 10 and11) For nationally authorised products
this has led to the publication o assess-
ment reports covering more than 140
active substances and in a considerable
number o cases to recommendations
or changes to the summaries o product
characteristics o authorised products re-
sulting in 65 actual changes For centrally
authorised products by 2011 the Agency
had completed the assessment o all the
data submitted under Article 45 covering55 active substances in 61 centrally ap-
17 Regulation (EC) No4692009 o the Euro-
pean Parliament and othe Council o 6 May 2009
concerning the supplemen-tary protection certificateor medicinal products OJ
L 152 1662009 p 1 ThisRegulation is a codificationo Council Regulation (EEC)
No 176892
18 Case C-12510 Merck
Sharp amp Dohme v DeutschesPatent- und Markenamt notyet published in the ECR
paragraph 37 lsquoi the SPCapplication had to be reused
because the calculationprovided or in Article 13(1)o Regulation No 176892
results in a negative or zero
duration the holder o thebasic patent could not obtain
an extension o protectionconerred by such a patenteven i it conducted all the
studies according to the ap-proved paediatric investiga-
tion plan under Article 36 oRegulation No 19012006Such a reusal would be
liable to adversely impacton the useul effect oRegulation No 19012006
and might jeopardise the
objectives o that regulationnamely the compensation
o effort made to evaluatethe paediatric effects o themedicinal product at issuersquo
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1436
14
proved medicinal products The summa-
ries o product characteristics o 12 me-
dicinal products were changed ollowing
the assessment
5Lessonslearnt51 Better access to
treatment
One o the explicit goals o the Paediatric
Regulation is to increase the number oproducts that are researched developed
and authorised or use in children and
to reduce the off-label use o medicinal
products in the paediatric population
The main tool to achieve this result is to
oblige companies to establish a paediat-
ric investigation plan or each newly de-
veloped product or or the line extension
o an already authorised product that is
still under patent protection The plan ismeant to ensure mdash under the supervi-
sion o the Paediatric Committee mdash that
the necessary data are generated so as
to determine the conditions under which
a medicinal product may be authorised
to treat children Since 2008 more than
600 paediatric investigation plans have
been approved However only a minor-
ity o them has been completed to date
the vast majority are still on-going This
is due to the long development cycles omedicinal products ofen lasting more
than a decade and the near-systematic
deerral o paediatric studies The high
number o deerrals may not have been
initially expected but are currently a real-
ity as or most o the medicinal products
that have been authorised so ar the RampD
programme started beore the entering
into orce o the Regulation Consequent-
ly the paediatric requirements could not
be taken into account rom the beginningo the product development
While the Paediatric Regulation has led
to some new authorisations that include
paediatric indications the regulatory in-
strument is recent and it will probably
take at least a decade beore it can be
judged in terms o its output In terms o
pharmaceutical orms there is however
already a visible positive impact
In this context criticism has been voiced
that the Regulation will ail to ensure abreakthrough in areas o particular pae-
diatric need such as paediatric oncology
This argument is related to the act that
the starting point or the majority o pae-
diatric investigation plans is an ongoing
RampD programme or a medicinal product
or adults An intrinsic consequence o this
approach is that these products primarily
target adult conditions They are devel-
oped in areas where there is a need (or a
market) in the adult population This needin the older population does not neces-
sarily correspond to the paediatric popu-
lationrsquos need
Moreover the Regulation grants waivers
rom its obligations where the disease or
condition or which the specific medicinal
product is intended occurs only in adult
populations This legislative approach cre-
ates riction in the case o diseases that
are specific and exclusive to children Italso limits the powers and possibilities o
the Paediatric Committee when reviewing
and agreeing to a paediatric investigation
plan as regards the scope o studies that
the Committee may request rom appli-
cants ollowing the objective and scien-
tific-based assessment o the compound
concerned19
These constraints and boundaries have to
be taken into account when judging the
impact the Regulation is likely to make In
addition the effect o instruments such as
the Orphan Regulation have to be consid-
ered given that or example all paediatric
cancers are rare diseases and all under
the EU policy ramework on rare diseases
All in all the achievements highlighted in
chapter 4 o this report and the number
o products with new paediatric indica-
tions show that there are some encourag-
ing signs afer this first five-year period it
is however too early or comprehensive
answers
19 Case T-5209 Nycomed vEMA not yet published
See the results o the publicconsultation conducted by
the Commission in prepara-tion o this Report
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1536
15
52 The PUMA concept a
disappointment
The Paediatric Regulation introduced a
new type o marketing authorisation mdash
the Paediatric Use Marketing Authorisa-
tion (PUMA) As an incentive to carry out
research into the potential paediatric use
o off-patent medicinal products that have
been authorised or adults this marketing
authorisation offers 8 years o data and
10 years o market exclusivity to any new
off-patent product developed exclusively
or use in the paediatric population Thus
the main goal o the PUMA concept is to
stimulate research in existing products
This scheme has been supported by EU
unding through the EU Framework Pro-
grammes or Research and Technological
Development
However to date only one PUMA has been
granted with a ew more projects cur-
rently in the pipeline
Neither industry nor academic networks
have embraced this opportunity as ully
as the Regulation intended It would seem
that the incentive o data and market ex-
clusivity does not work or these productsor at least that the market opportunities
in this sector are currently considered in-
sufficient to outweigh the inherent eco-
nomic risks o pharmaceutical develop-
ment Researchers are not engaging in
trials with medicines that have been on
the market or years Companies seem to
ear that market exclusivity will not pre-
vent physicians rom continuing to use
competitor products with the same active
ingredient off-label at lower costs or thatsubstitution or cheaper adult orms takes
place at the level o pharmacies Moreo-
ver national pricing and reimbursement
rules in Member States ofen do not al-
low or the additional research needed to
obtain the PUMA to be rewarded in price
negotiations20
Against this background the PUMA con-
cept has ailed so ar to ulfil the initial
expectationsThe EMA will in uture accept paediatric
investigation plans or a PUMA that cover
only certain age groups and not the en-
tire paediatric population This may offset
some o the reservations that currently
hamper better endorsement o the PUMA
concept
53 No impact on adultdevelopment
Studies prior to the adoption o the Regu-
lation have suggested a theoretical risk
that the requirements or research in chil-
dren could lengthen the overall drug de-
velopment process21 The Regulation has
met this risk head-on In order to avoid
any delays in authorising medicines or
other populations it allows or the grant-
ing o deerrals relating to the initiation orcompletion o some or all o the meas-
ures contained in a paediatric investiga-
tion plan
Experience shows that the deerral is a
widely used instrument which suggests
that the risk o delays in the processing o
adult applications is minimal There have
been some transitional problems in cases
where the adult programme was already
established when the Regulation enteredinto orce but these issues seem to have
been resolved
A concern that was raised initially was
that some companies would become
reluctant to develop new indications
pharmaceutical orms and new routes o
administration in small markets and or
products with low sales to avoid being
bound by the paediatric obligation under
Article 8 o the Regulation However thereis no evidence o such effect Moreover
it may also be argued that the incentive
o a potential six-month extension o the
SPC served to counterbalance such an
effect as it may have led companies to
examine more thoroughly the benefits o
a line extension taking into account the
economic value o the paediatric reward
Still industry stakeholders claim that
in rare cases the development or new
medicinal products has been delayedor abandoned in the expectation or as a
consequence o additional costs and re-
quirements associated with paediatric de-
20 See the results o thepublic consultation con-
ducted by the Commission inpreparation o this Report
21 C Commission StaffWorking Document Proposal
or a Regulation o the Euro-pean Parliament and o theCouncil on medicinal prod-
ucts or paediatric use andamending Council Regulation(EEC) No 17692 Directive
200183EC and Regula-tion (EC) No 7262004Extended impact assessment
(COM2004599F)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1636
16
keting authorisation holders are obliged
to ensure that the product inormation
is kept up to date with the current scien-
tific knowledge While preerence should
be given to cooperative approaches the
enorcement tools may need to be used
i companies do not overcome their res-
ervations
On the whole the requirements o Articles
45 and 46 have provided an efficient and
appropriate instrument or collecting and
evaluating existing paediatric studies
55 Clinical trials with
children
It is generally accepted that the Paediatric
Regulation will lead to more clinical trialswith children but that its aims should be
achieved without subjecting children to
unnecessary clinical trials
The youngest paediatric-age subsets
including neonates are particularly sen-
sitive It will be a constant challenge to
balance the therapeutic needs o these
age groups with their specific vulnerability
when considering and deciding on the ap-
propriateness o specific clinical trials or
the specific settings o studies in this age
subset Efforts are thereore continuously
being made to explore alternative means
eg the use o extrapolation modelling
and simulation techniques to reduce the
number o study subjects as much as
possible The Paediatric Committee is ac-
tively contributing to acilitate the devel-
opment and use o such means including
non-conventional trial design
Another challenge is how to avoid dupli-cating trials or different paediatric inves-
tigation plans rom different applicants
Companies embarking on product devel-
opment in similar areas may be required
by the agreed paediatric investigation
plan to conduct studies within similar
settings While collaborative approaches
between companies would be highly de-
sirable and have occurred on rare occa-
sions they ofen conflict with companiesrsquo
understandable reluctance to share datawith competitors in the early stages o
product development and participate in
direct comparisons This situation could
velopment Overall there is however no
evidence that the Regulation has a con-
siderable negative impact on products or
other populations
Rather there are some concerns that the
requirements under the Regulation may
cause delays in the authorisation o prod-ucts with paediatric-only indications as
they bring added complexity to the RampD
and regulatory process or products that
already directly target children The added
value o the submission o a paediatric in-
vestigation plan in these cases will be as-
sessed urther in the 2017 report
54 Reaping the benefits of
existing information
There was widespread speculation prior to
the adoption o the Paediatric Regulation
as to how many studies would be submit-
ted by pharmaceutical companies in ac-
cordance with Articles 45 and 46 The act
that competent authorities received more
than 18 000 studies reveals the consid-
erable amount o paediatric inormation
that existed at company level
Certainly it is true that not all the inor-
mation submitted met modern require-
ments or scientific data and clinical re-
search and that the work-sharing process
o evaluating the inormation is rather
long and resource intensive
Nevertheless compared to the PUMA con-
cept this scheme proved more successul
in terms o output and in recommending
and implementing changes to the sum-
mary o product characteristics o author-
ised products In its public consultationthe Commission called Articles 45 and 46
the lsquohidden gemsrsquo o the Regulation
One drawback that remains however
is reluctance by marketing authorisa-
tion holders to update the summary o
product characteristics on a voluntary
basis This said the Regulation contains
mechanisms to overcome such reluctance
as it empowers competent authorities to
directly update the summary and varythe marketing authorisation accordingly
Moreover in accordance with Article 23
o Directive 200183EC22 and Article 16
o Regulation (EC) No 726200423 mar-
22 Directive 200183EC othe European Parliament and
o the Council o 6 November2001 on the Community
code relating to medicinalproducts or human use OJ L311 28112001 p 67
23 Regulation (EC) No7262004 o the European
Parliament and o the Coun-cil o 31 March 2004 layingdown Community procedures
or the authorisation andsupervision o medicinalproducts or human and
veterinary use and establish-ing a European Medicines
Agency OJ L 136 3042004p 1
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1736
17
lead to competition among companies to
find investigators and study participants
as well as the duplication o trials which
are unnecessary rom a scientific and
ethical point o view
The Paediatric Committee is able to waive
paediatric trial requirements where thespecific medicinal product does not rep-
resent a significant therapeutic benefit
over an existing treatment or paediatric
patients including once the product is au-
thorised (Article 11) However this option
does not provide a way out in the early
stages o product development where
the Committee has to ensure equal treat-
ment and non-discriminatory approaches
The key to avoiding such unnecessary tri-
als is transparency with regard to ongoingand completed trials The situation contin-
ues to be monitored
Finally it is in the interest o the EU that
paediatric trials stemming rom paedi-
atric investigation plans are conducted
within the EU This has less to do with
the standards under which a trial is con-
ducted given that clinical trials carried
out outside the EU have to meet the ethi-
cal and scientific requirements o the EUprovisions on clinical trials24 than with the
act that studies within the EU may pro-
vide patients there with early access to
innovative medicines To date there is in-
sufficient data on the ratio between pae-
diatric trials conducted within and outside
the EU However in view o the upgraded
unctionalities o the EudraCT database it
is expected that more data will be avail-
able in 2017 or the second report
56 Spreading the news mdash
getting new information
to patients and healthcare
professionals
I the Regulation is to be a success it is
not only necessary that data on the use
o a specific product in the paediatric
population are collected but that these
data are then also appropriately commu-
nicated to and used by paediatricians intheir day-to-day work or the benefit o
their patients
In this regard some studies published in
the medical literature suggest a ailure
on the part o practitioners to recognise
the actual amount o off-label prescrib-
ing to children Moreover it is claimed that
the prescribing habits o practitioners are
ofen strongly influenced by personal ex-
perience rather than by evidence-based
inormation or paediatric medicine25
These studies in making generalisations
may not have taken into account the het-
erogeneity o healthcare proessionals
whose receptiveness varies greatly ac-
cording to their work setting and specific
area o specialisation At the same time
such observations may point to a sub-
stantial hurdle in achieving the goal o the
Paediatric Regulation
National competent authorities as well as
organisations or healthcare proessionals
seem particularly qualified to consider ap-
propriate ways o ensuring an adequate
flow o inormation Some Member States
have already established a number o
tools to communicate effectively and e-
ficiently with healthcare proessionals
eg by means o regular meetings web-
based inormation distribution systems ornational ormularies
57 Is the burden greater
than rewards
There can be no doubt that the Paediat-
ric Regulation places a considerable ad-
ditional burden on pharmaceutical com-
panies with its obligations regarding
research on products or use in children
However this approach was adopted be-cause market orces alone proved insu-
ficient to stimulate adequate research
The Regulation requires companies to
submit paediatric investigation plans at
an early stage o product development
However research on some active sub-
stances may be discontinued at later
stages should urther studies ail to show
potential with respect to the saety and
efficacy o the product For every success-
ul authorised medicinal product there aremany that ail to make the finishing line
Hence not all approved paediatric investi-
gation plans will be completed as compa-
24 Directive 200120EC othe European Parliament
and o the Council on theapproximation o the laws
regulations and administra-tive provisions o the Mem-ber States relating to the
implementation o good clini-cal practice in the conducto clinical trials on medicinal
products or human use OJ L121 152001 p 34
25 5-year report to theEuropean Commission (seeootnote 3) page 41
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1836
18
nies may decide to stop the correspond-
ing adult development It is too early still
to obtain reliable statistics that show
the ratio between completed and non-
completed paediatric investigation plans
but in the current context not all approved
plans will eventually result in an approved
medicine with a paediatric indication
In terms o output this entails some un-
necessary effort in compiling and screen-
ing paediatric investigation plans To what
extent this is offset by the benefit o early
submission which ensures that the pae-
diatric development fits smoothly into the
overall product development need ur-
ther monitoring
A urther point o concern is the highnumber o modifications to paediat-
ric investigation plans Figures seem to
suggest that nearly all plans have to
be modified at least once Conceptually
though this does not come as a surprise
in view o the early submission o pae-
diatric investigation plans the length o
adult and paediatric developments and
the substantial deerrals granted An
RampD plan requently has to be adapted
or amended to take account o initial re-sults Recruitment problems or necessary
design changes in the trials may also lead
to modifications While it is acknowledged
that substantial amendments or modifi-
cations to the plan have to be subject to
discussions with the Paediatric Commit-
tee this is less obvious or minor changes
In this context the level o detail required
by the EMA has been repeatedly criticised
In the past five years the EMA and its
Paediatric Committee have made effortsto provide or some flexibility in the plan
so to allow a margin o manoeuvre that
takes account o uncertainties in relation
to certain parameters o a trial
In any case the Commission intends to
review its Communication on the ormat
and content o applications or agree-
ment or modification o a paediatric in-
vestigation plan to take into account the
experience gained including the consider-
able number o modification requests
On a positive note it can be noted that
companies are applying or the rewards
provided by the Regulation primarily the
6-month extension o the Supplementary
Protection Certificate which have been
introduced to offset the additional bur-
den The economic value o the reward
depends on the turnover o the product
concerned In the case o blockbuster
products the amount may be consider-
able while or niche products the effect
is small
An in-depth evaluation o the economic
impact will be included in the 2017 report
in order to draw conclusions on the bal-
ance between burden and rewards and
public health benefits
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1936
19
6Outlook mdash
A fairy-taleending aheadlsquoBetter Medicines or Children mdash From
Concept to Realityrsquo is the title o this re-
port Readers may suggest that based on
the evaluation reerred to above it would
be more appropriate to add a question
mark It is evident that it is too early still
to make a firm statement Despite more
than five years o experience the true im-pact o the Regulation on the health o
children will only become apparent over
time as experience is accumulated in the
longer term
There are encouraging signs though
Paediatric development has become a
more integral part o the overall develop-
ment o medicinal products in the EU A
number o new products with paediatric
indications and age-appropriate pharma-ceutical orms have been authorised and
made available to patients A high num-
ber o agreed paediatric investigation
plans indicates that urther products are
in the pipeline
However it needs to be pointed out that it
would be wrong to expect the Regulation
to be able to solve all problems Instead
it is a major catalyst to improve the situ-
ation o young patients
Finally some weaknesses and deficits
have also become apparent in the last
five years Their impact on the overall
perormance o the Regulation has to be
closely monitored On the basis o the ac-
tions outlined above the Commission in-
tends to fine-tune the current implemen-
tation together with the EMA
Even i better medicines or children are
not yet a reality it should be the ambitiono all stakeholders involved that this piece
o legislation will be or the greater good
o children so that in the 2017 report
the discussion will ocus not on whether a
question mark should be added to the ti-
tle o the report but on whether it should
be an exclamation mark instead
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2036
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2136
21
ANNEXES
Figures and Tables
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2236
22
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2336
23
ANNEX I
Figures and Tables
Table 1Agreed paediatric investigations plans (PIPs) 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Agreed PIPs submitted under Article 7 (without waivers)
Agreed PIPs submitted under Article 8 (without waivers)
Source EMA Paediatric database The numbers on agreed PIPs correspond to EMA decisions
Table 2Agreed paediatric investigations plans (PIPs) compared to ull waivers and modifications 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Submitted modifications of an agreed PIP
Agreed Full waivers
Source EMA Paediatric database The numbers on agreed PIPs and waivers correspond to EMA decisions
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2536
25
Table 5Scientific advice and protocol assistance including ollow-ups (provided by the EMA Scientific Advice Working
Party and the Committee or Human Medicinal Products per year)
259
277321
388 400 433 420
021 32
74 8057
91
0 0 0
68 8067
94
0
100
200
300
400
500
2006 2007 2008 2009 2010 2011 2012
Total number of advice (Scientific Advice and Protocol Assistance)
Sum of paediatric-only and mixed (adult and paediatric development questions)
advice
Paediatric-only or mixed advice that involved a Paediatric Committee member(s) as
expert(s)
Source EMA databases Year o advice letter
Year o start o procedure
Table 6Paediatric clinical trials by year o authorisation
2005 2006 2007 2008 2009 2010 2011 2012
Paediatric trials
(number) 254 316 355 342 404 379 334 332
Paediatric trials
that are part of anagreed PIP 2 1 2 6 16 30 76 76
Proportion of
paediatric trials
that are part of an
agreed PIP among
paediatric trials 1 0 1 2 4 8 23 23
Total number
of trials (adults
and or children) 3 350 3 979 4 749 4 512 4 445 4 026 3 809 3 698
Proportion of
paediatric trials of
all trials 8 8 7 8 9 10 9 9
Source EudraCT Data Warehouse using a predefined query on 6 March 2013 and counting the first authorised trial only in the case o more thanone Member State This partial inormation requires sponsors to use a Clinical Trial Application orm that was only available rom November 2009 or use with version 8 o EudraCT
(available rom 2011)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2636
26
Table 7Number o children to be enrolled in clinical trials
Number
of subjects 2006 2007 2008 2009 2010 2011 2012
Pretermnewborns 0 0 0 207 82 2 281 1 712
Newborns 0 0 5 64 169 1 105 1 172
Infants and
toddlers 330 21 20 59 351 2 788 3 141
Children 2 142 181 200 2 230 2 055 10 325 20 677
Adolescents 368 111 205 1 577 2 861 9 054 13 193
Sum of
above 2 840 313 430 4 137 5 517 25 553 39 895
Reference
number of paediatric
trials 316 355 342 404 379 334 332
Source EudraCT Data Warehouse using a pre-defined query on 6 March 2013 modified by excluding studies or lsquoimmunological medicinal productsrsquo
Table 8EU budget contribution to the Paediatric Regulation and the EMA expenditure
0
1
2
3
4
5
6
7
8
9
10
2006 2007 2008 2009 2010 2011 2012
EU budget contribution (in Million euro)
EMA expenditure for paediatri cs (in Mill ion euro)
EMA expenditure for paediatr ics including support (in Million euro)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2736
27
Table 9Percentage o European Medicines Agencyrsquos human resources working in the paediatric area rom 2006 (inner
circle) to 2012 (outer circle)
733 (2012)
052 (2006)
Table 10Member States acting as rapporteurs or the assessment o studies submitted in accordance with Article 46
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE SE NL FR DK IT BE PL ES NO SK FI IE RO AT HU EL CZ PT LV BG
Study included in worksharing Rapporteur appointed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2836
28
Table 11Member States acting as rapporteur or the assessment o studies submitted in accordance with Article 45
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE NL DK AT FR PL SE ES IE CZ MT IT BE SI EE FI HU NO RO BG EL LV PT IS SK
Wave 1 Wave 2 Wave 3 Wave 4 Wave 5 Wave 6 Wave 7 Wave 8 Wave 9
Wave 10 Wave 11 Wave 12 Wave 13 Wave 14 Wave 15 Wave 16 Wave 17 Wave 18
Table 12Member States acting as rapporteurspeer reviewers in EMArsquos Paediatric Committee procedures (initial PIP
waiver or modification o an agreed PIP)
0
50
100
150
200
250
300
350
400
450
500
A u s t r i a
B el gi um
B ul g a r i a
C y pr u s
C z e c h R e p u b l i c
D enm a r k
E s t oni a
F i nl a n d
F r a n c e
G er m a n y
G r e e c e
H e a l t h c a r e a n d
A c a d emi a
H un g a r y
I c el a n d
I r el a n d
I t a l y
L a t vi a
L i t h u a ni a
L ux em b o ur g
M a l t a
N or w a y
P a t i en t s Or g a ni s a t i on
P ol a n d
P or t u g a l
R om a ni a
S l ov a k i a
S l ov eni a
S p a i n
S w e d en
T h eN e t h er l a n d
s
U ni t e d K i n g d om
Initial PIP applications PIP modifications
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2936
29
ANNEX II
Detailed inventory of centrally authorised medicinalproducts for paediatric use since the entry into force
of the Paediatric Regulation
Table 13Medicinal products authorised centrally since 2007 which include a paediatric indication
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Retapamulin Altargo 2007 No Mixed
Nelarabine Atriance 2007 No Mixed
Human papillomavirus vaccine[types 16 18] Cervarix 2007 No Mixed
Hydroxocobalamin Cyanokit 2007 No Mixed
Idursulase Elaprase 2007 No Mixed
Gadoversetamide Optimark 2007 No Mixed
Betaine anhydrous Cystadane 2007 No Mixed
Stiripentol Diacomit 2007 No Paediatric only
Mecasermin Increlex 2007 No Paediatric only
Rufinamide Inovelon 2007 No Mixed
Hydroxycarbamide Siklos 2007 No Mixed
Human normal
immunoglobulin (ivig) Flebogamma DIF 2007 No Mixed
Fluticasone uroate Avamys 2008 No Mixed
Human normal immunoglobulin Privigen 2008 No Mixed
Lacosamide Vimpat 2008 No Mixed
Micaungin Mycamine 2008 No Mixed
Sapropterin Kuvan 2008 No Mixed
Sugammadex Bridion 2008 No Mixed
Tocoersonal d-alpha
tocopheryl polyethylene glycol
succinate Vedrop 2009 No Paediatric only
Miamurtide Mepact 2009 No Mixed
Rilonacept Rilonacept Regeneron 2009 No Mixed
Tacrolimus Modigra 2009 No Mixed
Pneumoccocal polysaccharideconjugate vaccine (adsorbed) Synflorix 2009 No Paediatric only
Canakinumab
Ilaris (PIP not yet
completed) 2009 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3036
30
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Pneumoccocal polysaccharide
conjugate vaccine (13-valentadsorbed)
Prevenar 13 (PIP not yetcompleted) 2009 Yes Paediatric only
Meningococcal group a c
w135 and y conjugate vaccine Menveo 2010 Yes Mixed
Velaglucerase ala
Vpriv (PIP not yet
completed) 2010 Yes Mixed
Influenza vaccine (live
attenuated nasal) Fluenz (Waiver) 2011 Yes Paediatric only
C1 inhibitor human
Cinryze (PIP not yet
completed) 2011 Yes Mixed
Dihydroartemisinin
piperaquine phosphate
Eurartesim (PIP not yet
completed) 2011 Yes Mixed
Midazolam Buccolam 2011 Yes (PUMA) Paediatric only
EverolimusVotubia(PIP not yet completed) 2011 Yes Mixed
Tobramycin
Tobi Podhaler (PIP not
yet completed) 2011 Yes Mixed
Nomegestrol estradiol Ioa Zoely 2011 Yes Mixed
Colistimethate sodium Colobreathe 2012 Yes Mixed
Mercaptopurine Xaluprine 2012 No Mixed
Catridecacog NovoThirteen 2012 Yes MixedEavirenz Eavirenz Teva 2012 No Mixed
Ivacafor Kalydeco 2012 Yes Mixed
Desloratadine Desloratadine ratiopharm 2012 No Mixed
Desloratadine Desloratadine Actavis 2012 No Mixed
Perampanel Fycompa 2012 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3136
31
Table 14List o centrally authorised medicinal products or which the therapeutic indication was extended to or amend-
ed or the paediatric population
Active substance(s)
Trade
name Date Subject of the extension
Levetiracetam Keppra
2007
2009
Extension o the indication to include adjunctive ther-
apy in the treatment o primary generalised tonic-
clonic (PGTC) seizures in adults and adolescents rom
12 years o age with idiopathic generalised epilepsyExtension o indication to include the adjunctive
treatment o partial seizures with or without second-
ary generalisation in children rom 1 month to lt4
years old
Pneumococcal sac-
charide conjugated
vaccine adsorbed Prevenar 2007
Extension o the indication to include new inorma-
tion on efficacy against disease caused by Strepto-
coccus pneumoniae serotypes 4 6B 9V 14 18C 19F
and 23F in otitis mediaExtension o indication rom active immunisation
against bacteraemic pneumonia to active immunisa-
tion against pneumonia
Infliximab
Remi-
cade 2007
Extension o indication to include treatment o
severe active Crohnrsquos disease in children aged 6 to
17 years
Darbepoetin ala Aranesp 2007
Extension o indication or CRF patients whichrestricted the use o Nespo to paediatric subjects ge
11 years o age
Fosamprenavir Telzir 2007
Extension o indication o Telzir in combination withritonavir or the treatment o Human Immunodefi-
ciency Virus Type 1 (HIV-1) inected adults in combi-nation with other antiretroviral medicinal products to
include paediatric populations
Lamivudine zidovu-
dine Combivir 2007
Extension o indication to include paediatric patients
and replacement o film-coated tablets by scored
film-coated tablets
Desloratadine Aerius 2007Extension o indication rom lsquochronic idiopathic urti-cariarsquo to lsquourticariarsquo
Insulin glulisine Apidra 2007
Extension o indication to include 6 year olds and
older children based on the results o 2 paediatricstudies
Human papilloma virusvaccine [types 6 11
16 18] (recombinantadsorbed) Gardasil 2008
Extension o indication to include the prevention ohigh-grade vaginal dysplastic lesions (VaIN 23)
Adalimumab Humira 20082011
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in adoles-cents rom 13 to 17 years o age
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in the paedi-
atric population aged rom 4 to 12 years
Caspoungin Cancidas 2008
Extension o the indication to include the paediatric
population
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1036
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1136
11
cantly (see Table 5) despite the act that
issues o pharmaceutical non-clinical and
clinical development are also part o the
discussions o a paediatric investigation
plan To acilitate collaboration with the
Paediatric Committee joint procedures
have been created within the EMA
413 Clinical trials with children
Medicines or use in children need to be
tested with appropriate ormulations in
the paediatric population to ensure their
sae and effective use Hence it is gener-
ally accepted that the Paediatric Regula-
tion will lead to more clinical trials in chil-
dren The figures in the EudraCT database
have not yet shown an increase in paedi-
atric trials The number remained stablebetween 2006 and 2012 averaging 350
trials per year with some fluctuations (see
Table 6) It should be pointed out how-
ever that while the number o paediat-
ric trials remained stable the number o
clinical trials in all populations decreased
between 2007 and 2011
Moreover until recently EudraCT was lim-
ited to paediatric trials commencing in the
EU Data on paediatric trials that are parto a paediatric investigation plan and con-
ducted outside the EU have only become
publicly available since spring 2011
It should also be noted that the initiation
o a considerable percentage o clinical
trials included in a paediatric investiga-
tion plan has been deerred in order to
avoid delays in the authorisation o the
corresponding product or adults Hence
the impact o the Paediatric Regulation on
paediatric trials will become more appar-
ent in EudraCT in the years to come There
has however been an evident increase in
the number o paediatric study partici-
pants in particular or the age group rom
0 to 23 months who were normally not
included in trials prior to 2008 (see Ta-
ble 7) Allowing neonates and inants to
benefit rom research is a positive sign
as these have been the most neglected
groups so ar
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1236
12
414 Optimised framework and
coordination
The Paediatric Regulation osters a com-
prehensive network o expertise in paedi-
atric matters within the EU In this context
the role o the Paediatric Committee ispivotal as it brings together a high level
o expertise and competence
The Committee has contributed to the
scientific guidelines published by the EMA
and has so ar convened 22 expert work-
shops on the development o medicines
or children
In addition the European Network or
Paediatric Research at the EMA (Enpr-
EMA) was established in 2009 While aclosely-knit network o experts existed
prior to the introduction o the Regula-
tion in disease areas such as paediatric
oncology Enpr-EMA provides the added
value o a holistic approach by bringing
together national and European networks
investigators and centres with specific ex-
pertise in designing and conducting high-
quality studies in children
However question still remain as towhether this expertise translates into su-
ficient capacity within the EU to conduct
trials in specialised investigation settings
Well-developed research networks capa-
ble o acilitating the necessary research
to ulfil the commitments included in
paediatric investigation plans do exist in
some but not all Member States
415 International cooperation
On an international level the EMA has de-veloped international links with medicines
agencies in the United States Canada
and Japan O particular interest is the
cooperation with the US Food and Drug
Administration given that already in the
late 1990s the United States introduced
legislation that stimulated the develop-
ment o medicinal products or paediatric
use by means o a combination o incen-
tives and obligations This cooperation is
also o great interest to stakeholders as
it may give companies the possibility o
satisying the legislation in both regions
with the same studies
In addition the EMA participates actively
in the Paediatric medicines regulatory
network16 which was created in 2010 as
part o the WHOrsquos Better Medicines or
Children initiative
42 More medicines available
for children
Over 12 years (rom 1995 to 2006) 108
o all 317 indications o 262 centrally au-
thorised medicines included the paediat-
ric population Since the Paediatric Regu-
lation entered into orce 31 out o 152
new medicines have been authorised or
paediatric use 10 o which met the con-
ditions o Article 7 This is not more than
a lsquosnapshotrsquo o the effects o the Regula-
tion as this figure is likely to increase inthe uture as a considerable number o
the new already authorised medicines
are subject to an investigation plan where
completion was deerred to avoid delays
in the authorisation o the adult product
It ollows that in the years to come many
more o those 152 new medicines are ex-
pected to be authorised or paediatric use
Annual reports on deerred paediatric
studies o authorised medicines indicate
that the majority o paediatric investiga-tion plans are running to schedule Pae-
diatric research is on-going at the same
rate across therapeutic areas such as on-
cology vaccines and immunology-rheu-
matology-transplantation
Furthermore by the end o 2011 72 new
paediatric indications had been approved
or medicines already authorised includ-
ing 30 indications (18 centralised) arising
rom the obligation in Article 8 Moreover26 new pharmaceutical orms were au-
thorised or paediatric use including 18
adapted orms or centrally authorised
medicines
As ar as Paediatric Use Marketing Au-
thorisation is concerned to date only one
authorisation has been granted This alls
short o initial expectations
16 httpwwwwhointchild-medicinespaediatric_regula-
torsen
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1336
13
A detailed inventory o centrally autho-
rised products is provided in Annex II
Rewards and incentives
Companies that have complied with the
obligations o the Regulation may benefit
rom a reward once the product concerned
is authorised or the product inormation isamended The reward takes the orm o a
6-month extension o the supplementary
protection certificate (SPC) provided or
by Regulation (EC) No 469200917 or in
the case o an orphan medicinal product
by an extension o the ten-year period o
orphan market exclusivity to twelve years
No orphan rewards have been awarded
yet In this regard it is observed that some
companies withdrew the orphan designa-tion o a product in order to qualiy or
the SPC reward rather than the orphan
reward which seems to be more attrac-
tive rom an economic perspective As ar
as SPC extensions are concerned national
patent offices in 16 Member States had
by the end o 2011 granted 6-month ex-
tensions to 11 medicinal products which
resulted in a total o more than 100 na-
tional SPCs
It should be pointed out that a ruling othe European Court o Justice urther
increased the value o the paediatric
reward as it made clear that the initial
certificate could have a negative or zero
duration which could then become posi-
tive once the paediatric extension was
granted18
43 Increased information on
medicines used in childrenTo provide better inormation on the use
o medicinal products in children Article
45 o the Paediatric Regulation requires
companies holding data on the saety
or efficacy o authorised products in the
paediatric population to submit these
studies to the competent authorities In
this way the data can be assessed and
where appropriate the authorised prod-
uct inormation amended Article 46 o
the Regulation also requires companies tosubmit newly generated paediatric data
Since 2008 more than 18 000 study re-
ports on roughly 2 200 medicinal prod-
ucts have been submitted revealing the
large amount o existing paediatric inor-
mation available at company level
These study reports have been and
continue to be assessed by the compe-
tent authorities thanks to an impressive
work-sharing project (see Tables 10 and11) For nationally authorised products
this has led to the publication o assess-
ment reports covering more than 140
active substances and in a considerable
number o cases to recommendations
or changes to the summaries o product
characteristics o authorised products re-
sulting in 65 actual changes For centrally
authorised products by 2011 the Agency
had completed the assessment o all the
data submitted under Article 45 covering55 active substances in 61 centrally ap-
17 Regulation (EC) No4692009 o the Euro-
pean Parliament and othe Council o 6 May 2009
concerning the supplemen-tary protection certificateor medicinal products OJ
L 152 1662009 p 1 ThisRegulation is a codificationo Council Regulation (EEC)
No 176892
18 Case C-12510 Merck
Sharp amp Dohme v DeutschesPatent- und Markenamt notyet published in the ECR
paragraph 37 lsquoi the SPCapplication had to be reused
because the calculationprovided or in Article 13(1)o Regulation No 176892
results in a negative or zero
duration the holder o thebasic patent could not obtain
an extension o protectionconerred by such a patenteven i it conducted all the
studies according to the ap-proved paediatric investiga-
tion plan under Article 36 oRegulation No 19012006Such a reusal would be
liable to adversely impacton the useul effect oRegulation No 19012006
and might jeopardise the
objectives o that regulationnamely the compensation
o effort made to evaluatethe paediatric effects o themedicinal product at issuersquo
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1436
14
proved medicinal products The summa-
ries o product characteristics o 12 me-
dicinal products were changed ollowing
the assessment
5Lessonslearnt51 Better access to
treatment
One o the explicit goals o the Paediatric
Regulation is to increase the number oproducts that are researched developed
and authorised or use in children and
to reduce the off-label use o medicinal
products in the paediatric population
The main tool to achieve this result is to
oblige companies to establish a paediat-
ric investigation plan or each newly de-
veloped product or or the line extension
o an already authorised product that is
still under patent protection The plan ismeant to ensure mdash under the supervi-
sion o the Paediatric Committee mdash that
the necessary data are generated so as
to determine the conditions under which
a medicinal product may be authorised
to treat children Since 2008 more than
600 paediatric investigation plans have
been approved However only a minor-
ity o them has been completed to date
the vast majority are still on-going This
is due to the long development cycles omedicinal products ofen lasting more
than a decade and the near-systematic
deerral o paediatric studies The high
number o deerrals may not have been
initially expected but are currently a real-
ity as or most o the medicinal products
that have been authorised so ar the RampD
programme started beore the entering
into orce o the Regulation Consequent-
ly the paediatric requirements could not
be taken into account rom the beginningo the product development
While the Paediatric Regulation has led
to some new authorisations that include
paediatric indications the regulatory in-
strument is recent and it will probably
take at least a decade beore it can be
judged in terms o its output In terms o
pharmaceutical orms there is however
already a visible positive impact
In this context criticism has been voiced
that the Regulation will ail to ensure abreakthrough in areas o particular pae-
diatric need such as paediatric oncology
This argument is related to the act that
the starting point or the majority o pae-
diatric investigation plans is an ongoing
RampD programme or a medicinal product
or adults An intrinsic consequence o this
approach is that these products primarily
target adult conditions They are devel-
oped in areas where there is a need (or a
market) in the adult population This needin the older population does not neces-
sarily correspond to the paediatric popu-
lationrsquos need
Moreover the Regulation grants waivers
rom its obligations where the disease or
condition or which the specific medicinal
product is intended occurs only in adult
populations This legislative approach cre-
ates riction in the case o diseases that
are specific and exclusive to children Italso limits the powers and possibilities o
the Paediatric Committee when reviewing
and agreeing to a paediatric investigation
plan as regards the scope o studies that
the Committee may request rom appli-
cants ollowing the objective and scien-
tific-based assessment o the compound
concerned19
These constraints and boundaries have to
be taken into account when judging the
impact the Regulation is likely to make In
addition the effect o instruments such as
the Orphan Regulation have to be consid-
ered given that or example all paediatric
cancers are rare diseases and all under
the EU policy ramework on rare diseases
All in all the achievements highlighted in
chapter 4 o this report and the number
o products with new paediatric indica-
tions show that there are some encourag-
ing signs afer this first five-year period it
is however too early or comprehensive
answers
19 Case T-5209 Nycomed vEMA not yet published
See the results o the publicconsultation conducted by
the Commission in prepara-tion o this Report
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1536
15
52 The PUMA concept a
disappointment
The Paediatric Regulation introduced a
new type o marketing authorisation mdash
the Paediatric Use Marketing Authorisa-
tion (PUMA) As an incentive to carry out
research into the potential paediatric use
o off-patent medicinal products that have
been authorised or adults this marketing
authorisation offers 8 years o data and
10 years o market exclusivity to any new
off-patent product developed exclusively
or use in the paediatric population Thus
the main goal o the PUMA concept is to
stimulate research in existing products
This scheme has been supported by EU
unding through the EU Framework Pro-
grammes or Research and Technological
Development
However to date only one PUMA has been
granted with a ew more projects cur-
rently in the pipeline
Neither industry nor academic networks
have embraced this opportunity as ully
as the Regulation intended It would seem
that the incentive o data and market ex-
clusivity does not work or these productsor at least that the market opportunities
in this sector are currently considered in-
sufficient to outweigh the inherent eco-
nomic risks o pharmaceutical develop-
ment Researchers are not engaging in
trials with medicines that have been on
the market or years Companies seem to
ear that market exclusivity will not pre-
vent physicians rom continuing to use
competitor products with the same active
ingredient off-label at lower costs or thatsubstitution or cheaper adult orms takes
place at the level o pharmacies Moreo-
ver national pricing and reimbursement
rules in Member States ofen do not al-
low or the additional research needed to
obtain the PUMA to be rewarded in price
negotiations20
Against this background the PUMA con-
cept has ailed so ar to ulfil the initial
expectationsThe EMA will in uture accept paediatric
investigation plans or a PUMA that cover
only certain age groups and not the en-
tire paediatric population This may offset
some o the reservations that currently
hamper better endorsement o the PUMA
concept
53 No impact on adultdevelopment
Studies prior to the adoption o the Regu-
lation have suggested a theoretical risk
that the requirements or research in chil-
dren could lengthen the overall drug de-
velopment process21 The Regulation has
met this risk head-on In order to avoid
any delays in authorising medicines or
other populations it allows or the grant-
ing o deerrals relating to the initiation orcompletion o some or all o the meas-
ures contained in a paediatric investiga-
tion plan
Experience shows that the deerral is a
widely used instrument which suggests
that the risk o delays in the processing o
adult applications is minimal There have
been some transitional problems in cases
where the adult programme was already
established when the Regulation enteredinto orce but these issues seem to have
been resolved
A concern that was raised initially was
that some companies would become
reluctant to develop new indications
pharmaceutical orms and new routes o
administration in small markets and or
products with low sales to avoid being
bound by the paediatric obligation under
Article 8 o the Regulation However thereis no evidence o such effect Moreover
it may also be argued that the incentive
o a potential six-month extension o the
SPC served to counterbalance such an
effect as it may have led companies to
examine more thoroughly the benefits o
a line extension taking into account the
economic value o the paediatric reward
Still industry stakeholders claim that
in rare cases the development or new
medicinal products has been delayedor abandoned in the expectation or as a
consequence o additional costs and re-
quirements associated with paediatric de-
20 See the results o thepublic consultation con-
ducted by the Commission inpreparation o this Report
21 C Commission StaffWorking Document Proposal
or a Regulation o the Euro-pean Parliament and o theCouncil on medicinal prod-
ucts or paediatric use andamending Council Regulation(EEC) No 17692 Directive
200183EC and Regula-tion (EC) No 7262004Extended impact assessment
(COM2004599F)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1636
16
keting authorisation holders are obliged
to ensure that the product inormation
is kept up to date with the current scien-
tific knowledge While preerence should
be given to cooperative approaches the
enorcement tools may need to be used
i companies do not overcome their res-
ervations
On the whole the requirements o Articles
45 and 46 have provided an efficient and
appropriate instrument or collecting and
evaluating existing paediatric studies
55 Clinical trials with
children
It is generally accepted that the Paediatric
Regulation will lead to more clinical trialswith children but that its aims should be
achieved without subjecting children to
unnecessary clinical trials
The youngest paediatric-age subsets
including neonates are particularly sen-
sitive It will be a constant challenge to
balance the therapeutic needs o these
age groups with their specific vulnerability
when considering and deciding on the ap-
propriateness o specific clinical trials or
the specific settings o studies in this age
subset Efforts are thereore continuously
being made to explore alternative means
eg the use o extrapolation modelling
and simulation techniques to reduce the
number o study subjects as much as
possible The Paediatric Committee is ac-
tively contributing to acilitate the devel-
opment and use o such means including
non-conventional trial design
Another challenge is how to avoid dupli-cating trials or different paediatric inves-
tigation plans rom different applicants
Companies embarking on product devel-
opment in similar areas may be required
by the agreed paediatric investigation
plan to conduct studies within similar
settings While collaborative approaches
between companies would be highly de-
sirable and have occurred on rare occa-
sions they ofen conflict with companiesrsquo
understandable reluctance to share datawith competitors in the early stages o
product development and participate in
direct comparisons This situation could
velopment Overall there is however no
evidence that the Regulation has a con-
siderable negative impact on products or
other populations
Rather there are some concerns that the
requirements under the Regulation may
cause delays in the authorisation o prod-ucts with paediatric-only indications as
they bring added complexity to the RampD
and regulatory process or products that
already directly target children The added
value o the submission o a paediatric in-
vestigation plan in these cases will be as-
sessed urther in the 2017 report
54 Reaping the benefits of
existing information
There was widespread speculation prior to
the adoption o the Paediatric Regulation
as to how many studies would be submit-
ted by pharmaceutical companies in ac-
cordance with Articles 45 and 46 The act
that competent authorities received more
than 18 000 studies reveals the consid-
erable amount o paediatric inormation
that existed at company level
Certainly it is true that not all the inor-
mation submitted met modern require-
ments or scientific data and clinical re-
search and that the work-sharing process
o evaluating the inormation is rather
long and resource intensive
Nevertheless compared to the PUMA con-
cept this scheme proved more successul
in terms o output and in recommending
and implementing changes to the sum-
mary o product characteristics o author-
ised products In its public consultationthe Commission called Articles 45 and 46
the lsquohidden gemsrsquo o the Regulation
One drawback that remains however
is reluctance by marketing authorisa-
tion holders to update the summary o
product characteristics on a voluntary
basis This said the Regulation contains
mechanisms to overcome such reluctance
as it empowers competent authorities to
directly update the summary and varythe marketing authorisation accordingly
Moreover in accordance with Article 23
o Directive 200183EC22 and Article 16
o Regulation (EC) No 726200423 mar-
22 Directive 200183EC othe European Parliament and
o the Council o 6 November2001 on the Community
code relating to medicinalproducts or human use OJ L311 28112001 p 67
23 Regulation (EC) No7262004 o the European
Parliament and o the Coun-cil o 31 March 2004 layingdown Community procedures
or the authorisation andsupervision o medicinalproducts or human and
veterinary use and establish-ing a European Medicines
Agency OJ L 136 3042004p 1
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1736
17
lead to competition among companies to
find investigators and study participants
as well as the duplication o trials which
are unnecessary rom a scientific and
ethical point o view
The Paediatric Committee is able to waive
paediatric trial requirements where thespecific medicinal product does not rep-
resent a significant therapeutic benefit
over an existing treatment or paediatric
patients including once the product is au-
thorised (Article 11) However this option
does not provide a way out in the early
stages o product development where
the Committee has to ensure equal treat-
ment and non-discriminatory approaches
The key to avoiding such unnecessary tri-
als is transparency with regard to ongoingand completed trials The situation contin-
ues to be monitored
Finally it is in the interest o the EU that
paediatric trials stemming rom paedi-
atric investigation plans are conducted
within the EU This has less to do with
the standards under which a trial is con-
ducted given that clinical trials carried
out outside the EU have to meet the ethi-
cal and scientific requirements o the EUprovisions on clinical trials24 than with the
act that studies within the EU may pro-
vide patients there with early access to
innovative medicines To date there is in-
sufficient data on the ratio between pae-
diatric trials conducted within and outside
the EU However in view o the upgraded
unctionalities o the EudraCT database it
is expected that more data will be avail-
able in 2017 or the second report
56 Spreading the news mdash
getting new information
to patients and healthcare
professionals
I the Regulation is to be a success it is
not only necessary that data on the use
o a specific product in the paediatric
population are collected but that these
data are then also appropriately commu-
nicated to and used by paediatricians intheir day-to-day work or the benefit o
their patients
In this regard some studies published in
the medical literature suggest a ailure
on the part o practitioners to recognise
the actual amount o off-label prescrib-
ing to children Moreover it is claimed that
the prescribing habits o practitioners are
ofen strongly influenced by personal ex-
perience rather than by evidence-based
inormation or paediatric medicine25
These studies in making generalisations
may not have taken into account the het-
erogeneity o healthcare proessionals
whose receptiveness varies greatly ac-
cording to their work setting and specific
area o specialisation At the same time
such observations may point to a sub-
stantial hurdle in achieving the goal o the
Paediatric Regulation
National competent authorities as well as
organisations or healthcare proessionals
seem particularly qualified to consider ap-
propriate ways o ensuring an adequate
flow o inormation Some Member States
have already established a number o
tools to communicate effectively and e-
ficiently with healthcare proessionals
eg by means o regular meetings web-
based inormation distribution systems ornational ormularies
57 Is the burden greater
than rewards
There can be no doubt that the Paediat-
ric Regulation places a considerable ad-
ditional burden on pharmaceutical com-
panies with its obligations regarding
research on products or use in children
However this approach was adopted be-cause market orces alone proved insu-
ficient to stimulate adequate research
The Regulation requires companies to
submit paediatric investigation plans at
an early stage o product development
However research on some active sub-
stances may be discontinued at later
stages should urther studies ail to show
potential with respect to the saety and
efficacy o the product For every success-
ul authorised medicinal product there aremany that ail to make the finishing line
Hence not all approved paediatric investi-
gation plans will be completed as compa-
24 Directive 200120EC othe European Parliament
and o the Council on theapproximation o the laws
regulations and administra-tive provisions o the Mem-ber States relating to the
implementation o good clini-cal practice in the conducto clinical trials on medicinal
products or human use OJ L121 152001 p 34
25 5-year report to theEuropean Commission (seeootnote 3) page 41
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1836
18
nies may decide to stop the correspond-
ing adult development It is too early still
to obtain reliable statistics that show
the ratio between completed and non-
completed paediatric investigation plans
but in the current context not all approved
plans will eventually result in an approved
medicine with a paediatric indication
In terms o output this entails some un-
necessary effort in compiling and screen-
ing paediatric investigation plans To what
extent this is offset by the benefit o early
submission which ensures that the pae-
diatric development fits smoothly into the
overall product development need ur-
ther monitoring
A urther point o concern is the highnumber o modifications to paediat-
ric investigation plans Figures seem to
suggest that nearly all plans have to
be modified at least once Conceptually
though this does not come as a surprise
in view o the early submission o pae-
diatric investigation plans the length o
adult and paediatric developments and
the substantial deerrals granted An
RampD plan requently has to be adapted
or amended to take account o initial re-sults Recruitment problems or necessary
design changes in the trials may also lead
to modifications While it is acknowledged
that substantial amendments or modifi-
cations to the plan have to be subject to
discussions with the Paediatric Commit-
tee this is less obvious or minor changes
In this context the level o detail required
by the EMA has been repeatedly criticised
In the past five years the EMA and its
Paediatric Committee have made effortsto provide or some flexibility in the plan
so to allow a margin o manoeuvre that
takes account o uncertainties in relation
to certain parameters o a trial
In any case the Commission intends to
review its Communication on the ormat
and content o applications or agree-
ment or modification o a paediatric in-
vestigation plan to take into account the
experience gained including the consider-
able number o modification requests
On a positive note it can be noted that
companies are applying or the rewards
provided by the Regulation primarily the
6-month extension o the Supplementary
Protection Certificate which have been
introduced to offset the additional bur-
den The economic value o the reward
depends on the turnover o the product
concerned In the case o blockbuster
products the amount may be consider-
able while or niche products the effect
is small
An in-depth evaluation o the economic
impact will be included in the 2017 report
in order to draw conclusions on the bal-
ance between burden and rewards and
public health benefits
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1936
19
6Outlook mdash
A fairy-taleending aheadlsquoBetter Medicines or Children mdash From
Concept to Realityrsquo is the title o this re-
port Readers may suggest that based on
the evaluation reerred to above it would
be more appropriate to add a question
mark It is evident that it is too early still
to make a firm statement Despite more
than five years o experience the true im-pact o the Regulation on the health o
children will only become apparent over
time as experience is accumulated in the
longer term
There are encouraging signs though
Paediatric development has become a
more integral part o the overall develop-
ment o medicinal products in the EU A
number o new products with paediatric
indications and age-appropriate pharma-ceutical orms have been authorised and
made available to patients A high num-
ber o agreed paediatric investigation
plans indicates that urther products are
in the pipeline
However it needs to be pointed out that it
would be wrong to expect the Regulation
to be able to solve all problems Instead
it is a major catalyst to improve the situ-
ation o young patients
Finally some weaknesses and deficits
have also become apparent in the last
five years Their impact on the overall
perormance o the Regulation has to be
closely monitored On the basis o the ac-
tions outlined above the Commission in-
tends to fine-tune the current implemen-
tation together with the EMA
Even i better medicines or children are
not yet a reality it should be the ambitiono all stakeholders involved that this piece
o legislation will be or the greater good
o children so that in the 2017 report
the discussion will ocus not on whether a
question mark should be added to the ti-
tle o the report but on whether it should
be an exclamation mark instead
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2036
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2136
21
ANNEXES
Figures and Tables
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2236
22
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2336
23
ANNEX I
Figures and Tables
Table 1Agreed paediatric investigations plans (PIPs) 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Agreed PIPs submitted under Article 7 (without waivers)
Agreed PIPs submitted under Article 8 (without waivers)
Source EMA Paediatric database The numbers on agreed PIPs correspond to EMA decisions
Table 2Agreed paediatric investigations plans (PIPs) compared to ull waivers and modifications 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Submitted modifications of an agreed PIP
Agreed Full waivers
Source EMA Paediatric database The numbers on agreed PIPs and waivers correspond to EMA decisions
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2536
25
Table 5Scientific advice and protocol assistance including ollow-ups (provided by the EMA Scientific Advice Working
Party and the Committee or Human Medicinal Products per year)
259
277321
388 400 433 420
021 32
74 8057
91
0 0 0
68 8067
94
0
100
200
300
400
500
2006 2007 2008 2009 2010 2011 2012
Total number of advice (Scientific Advice and Protocol Assistance)
Sum of paediatric-only and mixed (adult and paediatric development questions)
advice
Paediatric-only or mixed advice that involved a Paediatric Committee member(s) as
expert(s)
Source EMA databases Year o advice letter
Year o start o procedure
Table 6Paediatric clinical trials by year o authorisation
2005 2006 2007 2008 2009 2010 2011 2012
Paediatric trials
(number) 254 316 355 342 404 379 334 332
Paediatric trials
that are part of anagreed PIP 2 1 2 6 16 30 76 76
Proportion of
paediatric trials
that are part of an
agreed PIP among
paediatric trials 1 0 1 2 4 8 23 23
Total number
of trials (adults
and or children) 3 350 3 979 4 749 4 512 4 445 4 026 3 809 3 698
Proportion of
paediatric trials of
all trials 8 8 7 8 9 10 9 9
Source EudraCT Data Warehouse using a predefined query on 6 March 2013 and counting the first authorised trial only in the case o more thanone Member State This partial inormation requires sponsors to use a Clinical Trial Application orm that was only available rom November 2009 or use with version 8 o EudraCT
(available rom 2011)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2636
26
Table 7Number o children to be enrolled in clinical trials
Number
of subjects 2006 2007 2008 2009 2010 2011 2012
Pretermnewborns 0 0 0 207 82 2 281 1 712
Newborns 0 0 5 64 169 1 105 1 172
Infants and
toddlers 330 21 20 59 351 2 788 3 141
Children 2 142 181 200 2 230 2 055 10 325 20 677
Adolescents 368 111 205 1 577 2 861 9 054 13 193
Sum of
above 2 840 313 430 4 137 5 517 25 553 39 895
Reference
number of paediatric
trials 316 355 342 404 379 334 332
Source EudraCT Data Warehouse using a pre-defined query on 6 March 2013 modified by excluding studies or lsquoimmunological medicinal productsrsquo
Table 8EU budget contribution to the Paediatric Regulation and the EMA expenditure
0
1
2
3
4
5
6
7
8
9
10
2006 2007 2008 2009 2010 2011 2012
EU budget contribution (in Million euro)
EMA expenditure for paediatri cs (in Mill ion euro)
EMA expenditure for paediatr ics including support (in Million euro)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2736
27
Table 9Percentage o European Medicines Agencyrsquos human resources working in the paediatric area rom 2006 (inner
circle) to 2012 (outer circle)
733 (2012)
052 (2006)
Table 10Member States acting as rapporteurs or the assessment o studies submitted in accordance with Article 46
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE SE NL FR DK IT BE PL ES NO SK FI IE RO AT HU EL CZ PT LV BG
Study included in worksharing Rapporteur appointed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2836
28
Table 11Member States acting as rapporteur or the assessment o studies submitted in accordance with Article 45
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE NL DK AT FR PL SE ES IE CZ MT IT BE SI EE FI HU NO RO BG EL LV PT IS SK
Wave 1 Wave 2 Wave 3 Wave 4 Wave 5 Wave 6 Wave 7 Wave 8 Wave 9
Wave 10 Wave 11 Wave 12 Wave 13 Wave 14 Wave 15 Wave 16 Wave 17 Wave 18
Table 12Member States acting as rapporteurspeer reviewers in EMArsquos Paediatric Committee procedures (initial PIP
waiver or modification o an agreed PIP)
0
50
100
150
200
250
300
350
400
450
500
A u s t r i a
B el gi um
B ul g a r i a
C y pr u s
C z e c h R e p u b l i c
D enm a r k
E s t oni a
F i nl a n d
F r a n c e
G er m a n y
G r e e c e
H e a l t h c a r e a n d
A c a d emi a
H un g a r y
I c el a n d
I r el a n d
I t a l y
L a t vi a
L i t h u a ni a
L ux em b o ur g
M a l t a
N or w a y
P a t i en t s Or g a ni s a t i on
P ol a n d
P or t u g a l
R om a ni a
S l ov a k i a
S l ov eni a
S p a i n
S w e d en
T h eN e t h er l a n d
s
U ni t e d K i n g d om
Initial PIP applications PIP modifications
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2936
29
ANNEX II
Detailed inventory of centrally authorised medicinalproducts for paediatric use since the entry into force
of the Paediatric Regulation
Table 13Medicinal products authorised centrally since 2007 which include a paediatric indication
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Retapamulin Altargo 2007 No Mixed
Nelarabine Atriance 2007 No Mixed
Human papillomavirus vaccine[types 16 18] Cervarix 2007 No Mixed
Hydroxocobalamin Cyanokit 2007 No Mixed
Idursulase Elaprase 2007 No Mixed
Gadoversetamide Optimark 2007 No Mixed
Betaine anhydrous Cystadane 2007 No Mixed
Stiripentol Diacomit 2007 No Paediatric only
Mecasermin Increlex 2007 No Paediatric only
Rufinamide Inovelon 2007 No Mixed
Hydroxycarbamide Siklos 2007 No Mixed
Human normal
immunoglobulin (ivig) Flebogamma DIF 2007 No Mixed
Fluticasone uroate Avamys 2008 No Mixed
Human normal immunoglobulin Privigen 2008 No Mixed
Lacosamide Vimpat 2008 No Mixed
Micaungin Mycamine 2008 No Mixed
Sapropterin Kuvan 2008 No Mixed
Sugammadex Bridion 2008 No Mixed
Tocoersonal d-alpha
tocopheryl polyethylene glycol
succinate Vedrop 2009 No Paediatric only
Miamurtide Mepact 2009 No Mixed
Rilonacept Rilonacept Regeneron 2009 No Mixed
Tacrolimus Modigra 2009 No Mixed
Pneumoccocal polysaccharideconjugate vaccine (adsorbed) Synflorix 2009 No Paediatric only
Canakinumab
Ilaris (PIP not yet
completed) 2009 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3036
30
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Pneumoccocal polysaccharide
conjugate vaccine (13-valentadsorbed)
Prevenar 13 (PIP not yetcompleted) 2009 Yes Paediatric only
Meningococcal group a c
w135 and y conjugate vaccine Menveo 2010 Yes Mixed
Velaglucerase ala
Vpriv (PIP not yet
completed) 2010 Yes Mixed
Influenza vaccine (live
attenuated nasal) Fluenz (Waiver) 2011 Yes Paediatric only
C1 inhibitor human
Cinryze (PIP not yet
completed) 2011 Yes Mixed
Dihydroartemisinin
piperaquine phosphate
Eurartesim (PIP not yet
completed) 2011 Yes Mixed
Midazolam Buccolam 2011 Yes (PUMA) Paediatric only
EverolimusVotubia(PIP not yet completed) 2011 Yes Mixed
Tobramycin
Tobi Podhaler (PIP not
yet completed) 2011 Yes Mixed
Nomegestrol estradiol Ioa Zoely 2011 Yes Mixed
Colistimethate sodium Colobreathe 2012 Yes Mixed
Mercaptopurine Xaluprine 2012 No Mixed
Catridecacog NovoThirteen 2012 Yes MixedEavirenz Eavirenz Teva 2012 No Mixed
Ivacafor Kalydeco 2012 Yes Mixed
Desloratadine Desloratadine ratiopharm 2012 No Mixed
Desloratadine Desloratadine Actavis 2012 No Mixed
Perampanel Fycompa 2012 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3136
31
Table 14List o centrally authorised medicinal products or which the therapeutic indication was extended to or amend-
ed or the paediatric population
Active substance(s)
Trade
name Date Subject of the extension
Levetiracetam Keppra
2007
2009
Extension o the indication to include adjunctive ther-
apy in the treatment o primary generalised tonic-
clonic (PGTC) seizures in adults and adolescents rom
12 years o age with idiopathic generalised epilepsyExtension o indication to include the adjunctive
treatment o partial seizures with or without second-
ary generalisation in children rom 1 month to lt4
years old
Pneumococcal sac-
charide conjugated
vaccine adsorbed Prevenar 2007
Extension o the indication to include new inorma-
tion on efficacy against disease caused by Strepto-
coccus pneumoniae serotypes 4 6B 9V 14 18C 19F
and 23F in otitis mediaExtension o indication rom active immunisation
against bacteraemic pneumonia to active immunisa-
tion against pneumonia
Infliximab
Remi-
cade 2007
Extension o indication to include treatment o
severe active Crohnrsquos disease in children aged 6 to
17 years
Darbepoetin ala Aranesp 2007
Extension o indication or CRF patients whichrestricted the use o Nespo to paediatric subjects ge
11 years o age
Fosamprenavir Telzir 2007
Extension o indication o Telzir in combination withritonavir or the treatment o Human Immunodefi-
ciency Virus Type 1 (HIV-1) inected adults in combi-nation with other antiretroviral medicinal products to
include paediatric populations
Lamivudine zidovu-
dine Combivir 2007
Extension o indication to include paediatric patients
and replacement o film-coated tablets by scored
film-coated tablets
Desloratadine Aerius 2007Extension o indication rom lsquochronic idiopathic urti-cariarsquo to lsquourticariarsquo
Insulin glulisine Apidra 2007
Extension o indication to include 6 year olds and
older children based on the results o 2 paediatricstudies
Human papilloma virusvaccine [types 6 11
16 18] (recombinantadsorbed) Gardasil 2008
Extension o indication to include the prevention ohigh-grade vaginal dysplastic lesions (VaIN 23)
Adalimumab Humira 20082011
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in adoles-cents rom 13 to 17 years o age
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in the paedi-
atric population aged rom 4 to 12 years
Caspoungin Cancidas 2008
Extension o the indication to include the paediatric
population
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1136
11
cantly (see Table 5) despite the act that
issues o pharmaceutical non-clinical and
clinical development are also part o the
discussions o a paediatric investigation
plan To acilitate collaboration with the
Paediatric Committee joint procedures
have been created within the EMA
413 Clinical trials with children
Medicines or use in children need to be
tested with appropriate ormulations in
the paediatric population to ensure their
sae and effective use Hence it is gener-
ally accepted that the Paediatric Regula-
tion will lead to more clinical trials in chil-
dren The figures in the EudraCT database
have not yet shown an increase in paedi-
atric trials The number remained stablebetween 2006 and 2012 averaging 350
trials per year with some fluctuations (see
Table 6) It should be pointed out how-
ever that while the number o paediat-
ric trials remained stable the number o
clinical trials in all populations decreased
between 2007 and 2011
Moreover until recently EudraCT was lim-
ited to paediatric trials commencing in the
EU Data on paediatric trials that are parto a paediatric investigation plan and con-
ducted outside the EU have only become
publicly available since spring 2011
It should also be noted that the initiation
o a considerable percentage o clinical
trials included in a paediatric investiga-
tion plan has been deerred in order to
avoid delays in the authorisation o the
corresponding product or adults Hence
the impact o the Paediatric Regulation on
paediatric trials will become more appar-
ent in EudraCT in the years to come There
has however been an evident increase in
the number o paediatric study partici-
pants in particular or the age group rom
0 to 23 months who were normally not
included in trials prior to 2008 (see Ta-
ble 7) Allowing neonates and inants to
benefit rom research is a positive sign
as these have been the most neglected
groups so ar
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1236
12
414 Optimised framework and
coordination
The Paediatric Regulation osters a com-
prehensive network o expertise in paedi-
atric matters within the EU In this context
the role o the Paediatric Committee ispivotal as it brings together a high level
o expertise and competence
The Committee has contributed to the
scientific guidelines published by the EMA
and has so ar convened 22 expert work-
shops on the development o medicines
or children
In addition the European Network or
Paediatric Research at the EMA (Enpr-
EMA) was established in 2009 While aclosely-knit network o experts existed
prior to the introduction o the Regula-
tion in disease areas such as paediatric
oncology Enpr-EMA provides the added
value o a holistic approach by bringing
together national and European networks
investigators and centres with specific ex-
pertise in designing and conducting high-
quality studies in children
However question still remain as towhether this expertise translates into su-
ficient capacity within the EU to conduct
trials in specialised investigation settings
Well-developed research networks capa-
ble o acilitating the necessary research
to ulfil the commitments included in
paediatric investigation plans do exist in
some but not all Member States
415 International cooperation
On an international level the EMA has de-veloped international links with medicines
agencies in the United States Canada
and Japan O particular interest is the
cooperation with the US Food and Drug
Administration given that already in the
late 1990s the United States introduced
legislation that stimulated the develop-
ment o medicinal products or paediatric
use by means o a combination o incen-
tives and obligations This cooperation is
also o great interest to stakeholders as
it may give companies the possibility o
satisying the legislation in both regions
with the same studies
In addition the EMA participates actively
in the Paediatric medicines regulatory
network16 which was created in 2010 as
part o the WHOrsquos Better Medicines or
Children initiative
42 More medicines available
for children
Over 12 years (rom 1995 to 2006) 108
o all 317 indications o 262 centrally au-
thorised medicines included the paediat-
ric population Since the Paediatric Regu-
lation entered into orce 31 out o 152
new medicines have been authorised or
paediatric use 10 o which met the con-
ditions o Article 7 This is not more than
a lsquosnapshotrsquo o the effects o the Regula-
tion as this figure is likely to increase inthe uture as a considerable number o
the new already authorised medicines
are subject to an investigation plan where
completion was deerred to avoid delays
in the authorisation o the adult product
It ollows that in the years to come many
more o those 152 new medicines are ex-
pected to be authorised or paediatric use
Annual reports on deerred paediatric
studies o authorised medicines indicate
that the majority o paediatric investiga-tion plans are running to schedule Pae-
diatric research is on-going at the same
rate across therapeutic areas such as on-
cology vaccines and immunology-rheu-
matology-transplantation
Furthermore by the end o 2011 72 new
paediatric indications had been approved
or medicines already authorised includ-
ing 30 indications (18 centralised) arising
rom the obligation in Article 8 Moreover26 new pharmaceutical orms were au-
thorised or paediatric use including 18
adapted orms or centrally authorised
medicines
As ar as Paediatric Use Marketing Au-
thorisation is concerned to date only one
authorisation has been granted This alls
short o initial expectations
16 httpwwwwhointchild-medicinespaediatric_regula-
torsen
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1336
13
A detailed inventory o centrally autho-
rised products is provided in Annex II
Rewards and incentives
Companies that have complied with the
obligations o the Regulation may benefit
rom a reward once the product concerned
is authorised or the product inormation isamended The reward takes the orm o a
6-month extension o the supplementary
protection certificate (SPC) provided or
by Regulation (EC) No 469200917 or in
the case o an orphan medicinal product
by an extension o the ten-year period o
orphan market exclusivity to twelve years
No orphan rewards have been awarded
yet In this regard it is observed that some
companies withdrew the orphan designa-tion o a product in order to qualiy or
the SPC reward rather than the orphan
reward which seems to be more attrac-
tive rom an economic perspective As ar
as SPC extensions are concerned national
patent offices in 16 Member States had
by the end o 2011 granted 6-month ex-
tensions to 11 medicinal products which
resulted in a total o more than 100 na-
tional SPCs
It should be pointed out that a ruling othe European Court o Justice urther
increased the value o the paediatric
reward as it made clear that the initial
certificate could have a negative or zero
duration which could then become posi-
tive once the paediatric extension was
granted18
43 Increased information on
medicines used in childrenTo provide better inormation on the use
o medicinal products in children Article
45 o the Paediatric Regulation requires
companies holding data on the saety
or efficacy o authorised products in the
paediatric population to submit these
studies to the competent authorities In
this way the data can be assessed and
where appropriate the authorised prod-
uct inormation amended Article 46 o
the Regulation also requires companies tosubmit newly generated paediatric data
Since 2008 more than 18 000 study re-
ports on roughly 2 200 medicinal prod-
ucts have been submitted revealing the
large amount o existing paediatric inor-
mation available at company level
These study reports have been and
continue to be assessed by the compe-
tent authorities thanks to an impressive
work-sharing project (see Tables 10 and11) For nationally authorised products
this has led to the publication o assess-
ment reports covering more than 140
active substances and in a considerable
number o cases to recommendations
or changes to the summaries o product
characteristics o authorised products re-
sulting in 65 actual changes For centrally
authorised products by 2011 the Agency
had completed the assessment o all the
data submitted under Article 45 covering55 active substances in 61 centrally ap-
17 Regulation (EC) No4692009 o the Euro-
pean Parliament and othe Council o 6 May 2009
concerning the supplemen-tary protection certificateor medicinal products OJ
L 152 1662009 p 1 ThisRegulation is a codificationo Council Regulation (EEC)
No 176892
18 Case C-12510 Merck
Sharp amp Dohme v DeutschesPatent- und Markenamt notyet published in the ECR
paragraph 37 lsquoi the SPCapplication had to be reused
because the calculationprovided or in Article 13(1)o Regulation No 176892
results in a negative or zero
duration the holder o thebasic patent could not obtain
an extension o protectionconerred by such a patenteven i it conducted all the
studies according to the ap-proved paediatric investiga-
tion plan under Article 36 oRegulation No 19012006Such a reusal would be
liable to adversely impacton the useul effect oRegulation No 19012006
and might jeopardise the
objectives o that regulationnamely the compensation
o effort made to evaluatethe paediatric effects o themedicinal product at issuersquo
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1436
14
proved medicinal products The summa-
ries o product characteristics o 12 me-
dicinal products were changed ollowing
the assessment
5Lessonslearnt51 Better access to
treatment
One o the explicit goals o the Paediatric
Regulation is to increase the number oproducts that are researched developed
and authorised or use in children and
to reduce the off-label use o medicinal
products in the paediatric population
The main tool to achieve this result is to
oblige companies to establish a paediat-
ric investigation plan or each newly de-
veloped product or or the line extension
o an already authorised product that is
still under patent protection The plan ismeant to ensure mdash under the supervi-
sion o the Paediatric Committee mdash that
the necessary data are generated so as
to determine the conditions under which
a medicinal product may be authorised
to treat children Since 2008 more than
600 paediatric investigation plans have
been approved However only a minor-
ity o them has been completed to date
the vast majority are still on-going This
is due to the long development cycles omedicinal products ofen lasting more
than a decade and the near-systematic
deerral o paediatric studies The high
number o deerrals may not have been
initially expected but are currently a real-
ity as or most o the medicinal products
that have been authorised so ar the RampD
programme started beore the entering
into orce o the Regulation Consequent-
ly the paediatric requirements could not
be taken into account rom the beginningo the product development
While the Paediatric Regulation has led
to some new authorisations that include
paediatric indications the regulatory in-
strument is recent and it will probably
take at least a decade beore it can be
judged in terms o its output In terms o
pharmaceutical orms there is however
already a visible positive impact
In this context criticism has been voiced
that the Regulation will ail to ensure abreakthrough in areas o particular pae-
diatric need such as paediatric oncology
This argument is related to the act that
the starting point or the majority o pae-
diatric investigation plans is an ongoing
RampD programme or a medicinal product
or adults An intrinsic consequence o this
approach is that these products primarily
target adult conditions They are devel-
oped in areas where there is a need (or a
market) in the adult population This needin the older population does not neces-
sarily correspond to the paediatric popu-
lationrsquos need
Moreover the Regulation grants waivers
rom its obligations where the disease or
condition or which the specific medicinal
product is intended occurs only in adult
populations This legislative approach cre-
ates riction in the case o diseases that
are specific and exclusive to children Italso limits the powers and possibilities o
the Paediatric Committee when reviewing
and agreeing to a paediatric investigation
plan as regards the scope o studies that
the Committee may request rom appli-
cants ollowing the objective and scien-
tific-based assessment o the compound
concerned19
These constraints and boundaries have to
be taken into account when judging the
impact the Regulation is likely to make In
addition the effect o instruments such as
the Orphan Regulation have to be consid-
ered given that or example all paediatric
cancers are rare diseases and all under
the EU policy ramework on rare diseases
All in all the achievements highlighted in
chapter 4 o this report and the number
o products with new paediatric indica-
tions show that there are some encourag-
ing signs afer this first five-year period it
is however too early or comprehensive
answers
19 Case T-5209 Nycomed vEMA not yet published
See the results o the publicconsultation conducted by
the Commission in prepara-tion o this Report
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1536
15
52 The PUMA concept a
disappointment
The Paediatric Regulation introduced a
new type o marketing authorisation mdash
the Paediatric Use Marketing Authorisa-
tion (PUMA) As an incentive to carry out
research into the potential paediatric use
o off-patent medicinal products that have
been authorised or adults this marketing
authorisation offers 8 years o data and
10 years o market exclusivity to any new
off-patent product developed exclusively
or use in the paediatric population Thus
the main goal o the PUMA concept is to
stimulate research in existing products
This scheme has been supported by EU
unding through the EU Framework Pro-
grammes or Research and Technological
Development
However to date only one PUMA has been
granted with a ew more projects cur-
rently in the pipeline
Neither industry nor academic networks
have embraced this opportunity as ully
as the Regulation intended It would seem
that the incentive o data and market ex-
clusivity does not work or these productsor at least that the market opportunities
in this sector are currently considered in-
sufficient to outweigh the inherent eco-
nomic risks o pharmaceutical develop-
ment Researchers are not engaging in
trials with medicines that have been on
the market or years Companies seem to
ear that market exclusivity will not pre-
vent physicians rom continuing to use
competitor products with the same active
ingredient off-label at lower costs or thatsubstitution or cheaper adult orms takes
place at the level o pharmacies Moreo-
ver national pricing and reimbursement
rules in Member States ofen do not al-
low or the additional research needed to
obtain the PUMA to be rewarded in price
negotiations20
Against this background the PUMA con-
cept has ailed so ar to ulfil the initial
expectationsThe EMA will in uture accept paediatric
investigation plans or a PUMA that cover
only certain age groups and not the en-
tire paediatric population This may offset
some o the reservations that currently
hamper better endorsement o the PUMA
concept
53 No impact on adultdevelopment
Studies prior to the adoption o the Regu-
lation have suggested a theoretical risk
that the requirements or research in chil-
dren could lengthen the overall drug de-
velopment process21 The Regulation has
met this risk head-on In order to avoid
any delays in authorising medicines or
other populations it allows or the grant-
ing o deerrals relating to the initiation orcompletion o some or all o the meas-
ures contained in a paediatric investiga-
tion plan
Experience shows that the deerral is a
widely used instrument which suggests
that the risk o delays in the processing o
adult applications is minimal There have
been some transitional problems in cases
where the adult programme was already
established when the Regulation enteredinto orce but these issues seem to have
been resolved
A concern that was raised initially was
that some companies would become
reluctant to develop new indications
pharmaceutical orms and new routes o
administration in small markets and or
products with low sales to avoid being
bound by the paediatric obligation under
Article 8 o the Regulation However thereis no evidence o such effect Moreover
it may also be argued that the incentive
o a potential six-month extension o the
SPC served to counterbalance such an
effect as it may have led companies to
examine more thoroughly the benefits o
a line extension taking into account the
economic value o the paediatric reward
Still industry stakeholders claim that
in rare cases the development or new
medicinal products has been delayedor abandoned in the expectation or as a
consequence o additional costs and re-
quirements associated with paediatric de-
20 See the results o thepublic consultation con-
ducted by the Commission inpreparation o this Report
21 C Commission StaffWorking Document Proposal
or a Regulation o the Euro-pean Parliament and o theCouncil on medicinal prod-
ucts or paediatric use andamending Council Regulation(EEC) No 17692 Directive
200183EC and Regula-tion (EC) No 7262004Extended impact assessment
(COM2004599F)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1636
16
keting authorisation holders are obliged
to ensure that the product inormation
is kept up to date with the current scien-
tific knowledge While preerence should
be given to cooperative approaches the
enorcement tools may need to be used
i companies do not overcome their res-
ervations
On the whole the requirements o Articles
45 and 46 have provided an efficient and
appropriate instrument or collecting and
evaluating existing paediatric studies
55 Clinical trials with
children
It is generally accepted that the Paediatric
Regulation will lead to more clinical trialswith children but that its aims should be
achieved without subjecting children to
unnecessary clinical trials
The youngest paediatric-age subsets
including neonates are particularly sen-
sitive It will be a constant challenge to
balance the therapeutic needs o these
age groups with their specific vulnerability
when considering and deciding on the ap-
propriateness o specific clinical trials or
the specific settings o studies in this age
subset Efforts are thereore continuously
being made to explore alternative means
eg the use o extrapolation modelling
and simulation techniques to reduce the
number o study subjects as much as
possible The Paediatric Committee is ac-
tively contributing to acilitate the devel-
opment and use o such means including
non-conventional trial design
Another challenge is how to avoid dupli-cating trials or different paediatric inves-
tigation plans rom different applicants
Companies embarking on product devel-
opment in similar areas may be required
by the agreed paediatric investigation
plan to conduct studies within similar
settings While collaborative approaches
between companies would be highly de-
sirable and have occurred on rare occa-
sions they ofen conflict with companiesrsquo
understandable reluctance to share datawith competitors in the early stages o
product development and participate in
direct comparisons This situation could
velopment Overall there is however no
evidence that the Regulation has a con-
siderable negative impact on products or
other populations
Rather there are some concerns that the
requirements under the Regulation may
cause delays in the authorisation o prod-ucts with paediatric-only indications as
they bring added complexity to the RampD
and regulatory process or products that
already directly target children The added
value o the submission o a paediatric in-
vestigation plan in these cases will be as-
sessed urther in the 2017 report
54 Reaping the benefits of
existing information
There was widespread speculation prior to
the adoption o the Paediatric Regulation
as to how many studies would be submit-
ted by pharmaceutical companies in ac-
cordance with Articles 45 and 46 The act
that competent authorities received more
than 18 000 studies reveals the consid-
erable amount o paediatric inormation
that existed at company level
Certainly it is true that not all the inor-
mation submitted met modern require-
ments or scientific data and clinical re-
search and that the work-sharing process
o evaluating the inormation is rather
long and resource intensive
Nevertheless compared to the PUMA con-
cept this scheme proved more successul
in terms o output and in recommending
and implementing changes to the sum-
mary o product characteristics o author-
ised products In its public consultationthe Commission called Articles 45 and 46
the lsquohidden gemsrsquo o the Regulation
One drawback that remains however
is reluctance by marketing authorisa-
tion holders to update the summary o
product characteristics on a voluntary
basis This said the Regulation contains
mechanisms to overcome such reluctance
as it empowers competent authorities to
directly update the summary and varythe marketing authorisation accordingly
Moreover in accordance with Article 23
o Directive 200183EC22 and Article 16
o Regulation (EC) No 726200423 mar-
22 Directive 200183EC othe European Parliament and
o the Council o 6 November2001 on the Community
code relating to medicinalproducts or human use OJ L311 28112001 p 67
23 Regulation (EC) No7262004 o the European
Parliament and o the Coun-cil o 31 March 2004 layingdown Community procedures
or the authorisation andsupervision o medicinalproducts or human and
veterinary use and establish-ing a European Medicines
Agency OJ L 136 3042004p 1
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1736
17
lead to competition among companies to
find investigators and study participants
as well as the duplication o trials which
are unnecessary rom a scientific and
ethical point o view
The Paediatric Committee is able to waive
paediatric trial requirements where thespecific medicinal product does not rep-
resent a significant therapeutic benefit
over an existing treatment or paediatric
patients including once the product is au-
thorised (Article 11) However this option
does not provide a way out in the early
stages o product development where
the Committee has to ensure equal treat-
ment and non-discriminatory approaches
The key to avoiding such unnecessary tri-
als is transparency with regard to ongoingand completed trials The situation contin-
ues to be monitored
Finally it is in the interest o the EU that
paediatric trials stemming rom paedi-
atric investigation plans are conducted
within the EU This has less to do with
the standards under which a trial is con-
ducted given that clinical trials carried
out outside the EU have to meet the ethi-
cal and scientific requirements o the EUprovisions on clinical trials24 than with the
act that studies within the EU may pro-
vide patients there with early access to
innovative medicines To date there is in-
sufficient data on the ratio between pae-
diatric trials conducted within and outside
the EU However in view o the upgraded
unctionalities o the EudraCT database it
is expected that more data will be avail-
able in 2017 or the second report
56 Spreading the news mdash
getting new information
to patients and healthcare
professionals
I the Regulation is to be a success it is
not only necessary that data on the use
o a specific product in the paediatric
population are collected but that these
data are then also appropriately commu-
nicated to and used by paediatricians intheir day-to-day work or the benefit o
their patients
In this regard some studies published in
the medical literature suggest a ailure
on the part o practitioners to recognise
the actual amount o off-label prescrib-
ing to children Moreover it is claimed that
the prescribing habits o practitioners are
ofen strongly influenced by personal ex-
perience rather than by evidence-based
inormation or paediatric medicine25
These studies in making generalisations
may not have taken into account the het-
erogeneity o healthcare proessionals
whose receptiveness varies greatly ac-
cording to their work setting and specific
area o specialisation At the same time
such observations may point to a sub-
stantial hurdle in achieving the goal o the
Paediatric Regulation
National competent authorities as well as
organisations or healthcare proessionals
seem particularly qualified to consider ap-
propriate ways o ensuring an adequate
flow o inormation Some Member States
have already established a number o
tools to communicate effectively and e-
ficiently with healthcare proessionals
eg by means o regular meetings web-
based inormation distribution systems ornational ormularies
57 Is the burden greater
than rewards
There can be no doubt that the Paediat-
ric Regulation places a considerable ad-
ditional burden on pharmaceutical com-
panies with its obligations regarding
research on products or use in children
However this approach was adopted be-cause market orces alone proved insu-
ficient to stimulate adequate research
The Regulation requires companies to
submit paediatric investigation plans at
an early stage o product development
However research on some active sub-
stances may be discontinued at later
stages should urther studies ail to show
potential with respect to the saety and
efficacy o the product For every success-
ul authorised medicinal product there aremany that ail to make the finishing line
Hence not all approved paediatric investi-
gation plans will be completed as compa-
24 Directive 200120EC othe European Parliament
and o the Council on theapproximation o the laws
regulations and administra-tive provisions o the Mem-ber States relating to the
implementation o good clini-cal practice in the conducto clinical trials on medicinal
products or human use OJ L121 152001 p 34
25 5-year report to theEuropean Commission (seeootnote 3) page 41
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1836
18
nies may decide to stop the correspond-
ing adult development It is too early still
to obtain reliable statistics that show
the ratio between completed and non-
completed paediatric investigation plans
but in the current context not all approved
plans will eventually result in an approved
medicine with a paediatric indication
In terms o output this entails some un-
necessary effort in compiling and screen-
ing paediatric investigation plans To what
extent this is offset by the benefit o early
submission which ensures that the pae-
diatric development fits smoothly into the
overall product development need ur-
ther monitoring
A urther point o concern is the highnumber o modifications to paediat-
ric investigation plans Figures seem to
suggest that nearly all plans have to
be modified at least once Conceptually
though this does not come as a surprise
in view o the early submission o pae-
diatric investigation plans the length o
adult and paediatric developments and
the substantial deerrals granted An
RampD plan requently has to be adapted
or amended to take account o initial re-sults Recruitment problems or necessary
design changes in the trials may also lead
to modifications While it is acknowledged
that substantial amendments or modifi-
cations to the plan have to be subject to
discussions with the Paediatric Commit-
tee this is less obvious or minor changes
In this context the level o detail required
by the EMA has been repeatedly criticised
In the past five years the EMA and its
Paediatric Committee have made effortsto provide or some flexibility in the plan
so to allow a margin o manoeuvre that
takes account o uncertainties in relation
to certain parameters o a trial
In any case the Commission intends to
review its Communication on the ormat
and content o applications or agree-
ment or modification o a paediatric in-
vestigation plan to take into account the
experience gained including the consider-
able number o modification requests
On a positive note it can be noted that
companies are applying or the rewards
provided by the Regulation primarily the
6-month extension o the Supplementary
Protection Certificate which have been
introduced to offset the additional bur-
den The economic value o the reward
depends on the turnover o the product
concerned In the case o blockbuster
products the amount may be consider-
able while or niche products the effect
is small
An in-depth evaluation o the economic
impact will be included in the 2017 report
in order to draw conclusions on the bal-
ance between burden and rewards and
public health benefits
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1936
19
6Outlook mdash
A fairy-taleending aheadlsquoBetter Medicines or Children mdash From
Concept to Realityrsquo is the title o this re-
port Readers may suggest that based on
the evaluation reerred to above it would
be more appropriate to add a question
mark It is evident that it is too early still
to make a firm statement Despite more
than five years o experience the true im-pact o the Regulation on the health o
children will only become apparent over
time as experience is accumulated in the
longer term
There are encouraging signs though
Paediatric development has become a
more integral part o the overall develop-
ment o medicinal products in the EU A
number o new products with paediatric
indications and age-appropriate pharma-ceutical orms have been authorised and
made available to patients A high num-
ber o agreed paediatric investigation
plans indicates that urther products are
in the pipeline
However it needs to be pointed out that it
would be wrong to expect the Regulation
to be able to solve all problems Instead
it is a major catalyst to improve the situ-
ation o young patients
Finally some weaknesses and deficits
have also become apparent in the last
five years Their impact on the overall
perormance o the Regulation has to be
closely monitored On the basis o the ac-
tions outlined above the Commission in-
tends to fine-tune the current implemen-
tation together with the EMA
Even i better medicines or children are
not yet a reality it should be the ambitiono all stakeholders involved that this piece
o legislation will be or the greater good
o children so that in the 2017 report
the discussion will ocus not on whether a
question mark should be added to the ti-
tle o the report but on whether it should
be an exclamation mark instead
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2036
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2136
21
ANNEXES
Figures and Tables
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2236
22
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2336
23
ANNEX I
Figures and Tables
Table 1Agreed paediatric investigations plans (PIPs) 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Agreed PIPs submitted under Article 7 (without waivers)
Agreed PIPs submitted under Article 8 (without waivers)
Source EMA Paediatric database The numbers on agreed PIPs correspond to EMA decisions
Table 2Agreed paediatric investigations plans (PIPs) compared to ull waivers and modifications 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Submitted modifications of an agreed PIP
Agreed Full waivers
Source EMA Paediatric database The numbers on agreed PIPs and waivers correspond to EMA decisions
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2536
25
Table 5Scientific advice and protocol assistance including ollow-ups (provided by the EMA Scientific Advice Working
Party and the Committee or Human Medicinal Products per year)
259
277321
388 400 433 420
021 32
74 8057
91
0 0 0
68 8067
94
0
100
200
300
400
500
2006 2007 2008 2009 2010 2011 2012
Total number of advice (Scientific Advice and Protocol Assistance)
Sum of paediatric-only and mixed (adult and paediatric development questions)
advice
Paediatric-only or mixed advice that involved a Paediatric Committee member(s) as
expert(s)
Source EMA databases Year o advice letter
Year o start o procedure
Table 6Paediatric clinical trials by year o authorisation
2005 2006 2007 2008 2009 2010 2011 2012
Paediatric trials
(number) 254 316 355 342 404 379 334 332
Paediatric trials
that are part of anagreed PIP 2 1 2 6 16 30 76 76
Proportion of
paediatric trials
that are part of an
agreed PIP among
paediatric trials 1 0 1 2 4 8 23 23
Total number
of trials (adults
and or children) 3 350 3 979 4 749 4 512 4 445 4 026 3 809 3 698
Proportion of
paediatric trials of
all trials 8 8 7 8 9 10 9 9
Source EudraCT Data Warehouse using a predefined query on 6 March 2013 and counting the first authorised trial only in the case o more thanone Member State This partial inormation requires sponsors to use a Clinical Trial Application orm that was only available rom November 2009 or use with version 8 o EudraCT
(available rom 2011)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2636
26
Table 7Number o children to be enrolled in clinical trials
Number
of subjects 2006 2007 2008 2009 2010 2011 2012
Pretermnewborns 0 0 0 207 82 2 281 1 712
Newborns 0 0 5 64 169 1 105 1 172
Infants and
toddlers 330 21 20 59 351 2 788 3 141
Children 2 142 181 200 2 230 2 055 10 325 20 677
Adolescents 368 111 205 1 577 2 861 9 054 13 193
Sum of
above 2 840 313 430 4 137 5 517 25 553 39 895
Reference
number of paediatric
trials 316 355 342 404 379 334 332
Source EudraCT Data Warehouse using a pre-defined query on 6 March 2013 modified by excluding studies or lsquoimmunological medicinal productsrsquo
Table 8EU budget contribution to the Paediatric Regulation and the EMA expenditure
0
1
2
3
4
5
6
7
8
9
10
2006 2007 2008 2009 2010 2011 2012
EU budget contribution (in Million euro)
EMA expenditure for paediatri cs (in Mill ion euro)
EMA expenditure for paediatr ics including support (in Million euro)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2736
27
Table 9Percentage o European Medicines Agencyrsquos human resources working in the paediatric area rom 2006 (inner
circle) to 2012 (outer circle)
733 (2012)
052 (2006)
Table 10Member States acting as rapporteurs or the assessment o studies submitted in accordance with Article 46
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE SE NL FR DK IT BE PL ES NO SK FI IE RO AT HU EL CZ PT LV BG
Study included in worksharing Rapporteur appointed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2836
28
Table 11Member States acting as rapporteur or the assessment o studies submitted in accordance with Article 45
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE NL DK AT FR PL SE ES IE CZ MT IT BE SI EE FI HU NO RO BG EL LV PT IS SK
Wave 1 Wave 2 Wave 3 Wave 4 Wave 5 Wave 6 Wave 7 Wave 8 Wave 9
Wave 10 Wave 11 Wave 12 Wave 13 Wave 14 Wave 15 Wave 16 Wave 17 Wave 18
Table 12Member States acting as rapporteurspeer reviewers in EMArsquos Paediatric Committee procedures (initial PIP
waiver or modification o an agreed PIP)
0
50
100
150
200
250
300
350
400
450
500
A u s t r i a
B el gi um
B ul g a r i a
C y pr u s
C z e c h R e p u b l i c
D enm a r k
E s t oni a
F i nl a n d
F r a n c e
G er m a n y
G r e e c e
H e a l t h c a r e a n d
A c a d emi a
H un g a r y
I c el a n d
I r el a n d
I t a l y
L a t vi a
L i t h u a ni a
L ux em b o ur g
M a l t a
N or w a y
P a t i en t s Or g a ni s a t i on
P ol a n d
P or t u g a l
R om a ni a
S l ov a k i a
S l ov eni a
S p a i n
S w e d en
T h eN e t h er l a n d
s
U ni t e d K i n g d om
Initial PIP applications PIP modifications
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2936
29
ANNEX II
Detailed inventory of centrally authorised medicinalproducts for paediatric use since the entry into force
of the Paediatric Regulation
Table 13Medicinal products authorised centrally since 2007 which include a paediatric indication
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Retapamulin Altargo 2007 No Mixed
Nelarabine Atriance 2007 No Mixed
Human papillomavirus vaccine[types 16 18] Cervarix 2007 No Mixed
Hydroxocobalamin Cyanokit 2007 No Mixed
Idursulase Elaprase 2007 No Mixed
Gadoversetamide Optimark 2007 No Mixed
Betaine anhydrous Cystadane 2007 No Mixed
Stiripentol Diacomit 2007 No Paediatric only
Mecasermin Increlex 2007 No Paediatric only
Rufinamide Inovelon 2007 No Mixed
Hydroxycarbamide Siklos 2007 No Mixed
Human normal
immunoglobulin (ivig) Flebogamma DIF 2007 No Mixed
Fluticasone uroate Avamys 2008 No Mixed
Human normal immunoglobulin Privigen 2008 No Mixed
Lacosamide Vimpat 2008 No Mixed
Micaungin Mycamine 2008 No Mixed
Sapropterin Kuvan 2008 No Mixed
Sugammadex Bridion 2008 No Mixed
Tocoersonal d-alpha
tocopheryl polyethylene glycol
succinate Vedrop 2009 No Paediatric only
Miamurtide Mepact 2009 No Mixed
Rilonacept Rilonacept Regeneron 2009 No Mixed
Tacrolimus Modigra 2009 No Mixed
Pneumoccocal polysaccharideconjugate vaccine (adsorbed) Synflorix 2009 No Paediatric only
Canakinumab
Ilaris (PIP not yet
completed) 2009 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3036
30
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Pneumoccocal polysaccharide
conjugate vaccine (13-valentadsorbed)
Prevenar 13 (PIP not yetcompleted) 2009 Yes Paediatric only
Meningococcal group a c
w135 and y conjugate vaccine Menveo 2010 Yes Mixed
Velaglucerase ala
Vpriv (PIP not yet
completed) 2010 Yes Mixed
Influenza vaccine (live
attenuated nasal) Fluenz (Waiver) 2011 Yes Paediatric only
C1 inhibitor human
Cinryze (PIP not yet
completed) 2011 Yes Mixed
Dihydroartemisinin
piperaquine phosphate
Eurartesim (PIP not yet
completed) 2011 Yes Mixed
Midazolam Buccolam 2011 Yes (PUMA) Paediatric only
EverolimusVotubia(PIP not yet completed) 2011 Yes Mixed
Tobramycin
Tobi Podhaler (PIP not
yet completed) 2011 Yes Mixed
Nomegestrol estradiol Ioa Zoely 2011 Yes Mixed
Colistimethate sodium Colobreathe 2012 Yes Mixed
Mercaptopurine Xaluprine 2012 No Mixed
Catridecacog NovoThirteen 2012 Yes MixedEavirenz Eavirenz Teva 2012 No Mixed
Ivacafor Kalydeco 2012 Yes Mixed
Desloratadine Desloratadine ratiopharm 2012 No Mixed
Desloratadine Desloratadine Actavis 2012 No Mixed
Perampanel Fycompa 2012 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3136
31
Table 14List o centrally authorised medicinal products or which the therapeutic indication was extended to or amend-
ed or the paediatric population
Active substance(s)
Trade
name Date Subject of the extension
Levetiracetam Keppra
2007
2009
Extension o the indication to include adjunctive ther-
apy in the treatment o primary generalised tonic-
clonic (PGTC) seizures in adults and adolescents rom
12 years o age with idiopathic generalised epilepsyExtension o indication to include the adjunctive
treatment o partial seizures with or without second-
ary generalisation in children rom 1 month to lt4
years old
Pneumococcal sac-
charide conjugated
vaccine adsorbed Prevenar 2007
Extension o the indication to include new inorma-
tion on efficacy against disease caused by Strepto-
coccus pneumoniae serotypes 4 6B 9V 14 18C 19F
and 23F in otitis mediaExtension o indication rom active immunisation
against bacteraemic pneumonia to active immunisa-
tion against pneumonia
Infliximab
Remi-
cade 2007
Extension o indication to include treatment o
severe active Crohnrsquos disease in children aged 6 to
17 years
Darbepoetin ala Aranesp 2007
Extension o indication or CRF patients whichrestricted the use o Nespo to paediatric subjects ge
11 years o age
Fosamprenavir Telzir 2007
Extension o indication o Telzir in combination withritonavir or the treatment o Human Immunodefi-
ciency Virus Type 1 (HIV-1) inected adults in combi-nation with other antiretroviral medicinal products to
include paediatric populations
Lamivudine zidovu-
dine Combivir 2007
Extension o indication to include paediatric patients
and replacement o film-coated tablets by scored
film-coated tablets
Desloratadine Aerius 2007Extension o indication rom lsquochronic idiopathic urti-cariarsquo to lsquourticariarsquo
Insulin glulisine Apidra 2007
Extension o indication to include 6 year olds and
older children based on the results o 2 paediatricstudies
Human papilloma virusvaccine [types 6 11
16 18] (recombinantadsorbed) Gardasil 2008
Extension o indication to include the prevention ohigh-grade vaginal dysplastic lesions (VaIN 23)
Adalimumab Humira 20082011
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in adoles-cents rom 13 to 17 years o age
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in the paedi-
atric population aged rom 4 to 12 years
Caspoungin Cancidas 2008
Extension o the indication to include the paediatric
population
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1236
12
414 Optimised framework and
coordination
The Paediatric Regulation osters a com-
prehensive network o expertise in paedi-
atric matters within the EU In this context
the role o the Paediatric Committee ispivotal as it brings together a high level
o expertise and competence
The Committee has contributed to the
scientific guidelines published by the EMA
and has so ar convened 22 expert work-
shops on the development o medicines
or children
In addition the European Network or
Paediatric Research at the EMA (Enpr-
EMA) was established in 2009 While aclosely-knit network o experts existed
prior to the introduction o the Regula-
tion in disease areas such as paediatric
oncology Enpr-EMA provides the added
value o a holistic approach by bringing
together national and European networks
investigators and centres with specific ex-
pertise in designing and conducting high-
quality studies in children
However question still remain as towhether this expertise translates into su-
ficient capacity within the EU to conduct
trials in specialised investigation settings
Well-developed research networks capa-
ble o acilitating the necessary research
to ulfil the commitments included in
paediatric investigation plans do exist in
some but not all Member States
415 International cooperation
On an international level the EMA has de-veloped international links with medicines
agencies in the United States Canada
and Japan O particular interest is the
cooperation with the US Food and Drug
Administration given that already in the
late 1990s the United States introduced
legislation that stimulated the develop-
ment o medicinal products or paediatric
use by means o a combination o incen-
tives and obligations This cooperation is
also o great interest to stakeholders as
it may give companies the possibility o
satisying the legislation in both regions
with the same studies
In addition the EMA participates actively
in the Paediatric medicines regulatory
network16 which was created in 2010 as
part o the WHOrsquos Better Medicines or
Children initiative
42 More medicines available
for children
Over 12 years (rom 1995 to 2006) 108
o all 317 indications o 262 centrally au-
thorised medicines included the paediat-
ric population Since the Paediatric Regu-
lation entered into orce 31 out o 152
new medicines have been authorised or
paediatric use 10 o which met the con-
ditions o Article 7 This is not more than
a lsquosnapshotrsquo o the effects o the Regula-
tion as this figure is likely to increase inthe uture as a considerable number o
the new already authorised medicines
are subject to an investigation plan where
completion was deerred to avoid delays
in the authorisation o the adult product
It ollows that in the years to come many
more o those 152 new medicines are ex-
pected to be authorised or paediatric use
Annual reports on deerred paediatric
studies o authorised medicines indicate
that the majority o paediatric investiga-tion plans are running to schedule Pae-
diatric research is on-going at the same
rate across therapeutic areas such as on-
cology vaccines and immunology-rheu-
matology-transplantation
Furthermore by the end o 2011 72 new
paediatric indications had been approved
or medicines already authorised includ-
ing 30 indications (18 centralised) arising
rom the obligation in Article 8 Moreover26 new pharmaceutical orms were au-
thorised or paediatric use including 18
adapted orms or centrally authorised
medicines
As ar as Paediatric Use Marketing Au-
thorisation is concerned to date only one
authorisation has been granted This alls
short o initial expectations
16 httpwwwwhointchild-medicinespaediatric_regula-
torsen
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1336
13
A detailed inventory o centrally autho-
rised products is provided in Annex II
Rewards and incentives
Companies that have complied with the
obligations o the Regulation may benefit
rom a reward once the product concerned
is authorised or the product inormation isamended The reward takes the orm o a
6-month extension o the supplementary
protection certificate (SPC) provided or
by Regulation (EC) No 469200917 or in
the case o an orphan medicinal product
by an extension o the ten-year period o
orphan market exclusivity to twelve years
No orphan rewards have been awarded
yet In this regard it is observed that some
companies withdrew the orphan designa-tion o a product in order to qualiy or
the SPC reward rather than the orphan
reward which seems to be more attrac-
tive rom an economic perspective As ar
as SPC extensions are concerned national
patent offices in 16 Member States had
by the end o 2011 granted 6-month ex-
tensions to 11 medicinal products which
resulted in a total o more than 100 na-
tional SPCs
It should be pointed out that a ruling othe European Court o Justice urther
increased the value o the paediatric
reward as it made clear that the initial
certificate could have a negative or zero
duration which could then become posi-
tive once the paediatric extension was
granted18
43 Increased information on
medicines used in childrenTo provide better inormation on the use
o medicinal products in children Article
45 o the Paediatric Regulation requires
companies holding data on the saety
or efficacy o authorised products in the
paediatric population to submit these
studies to the competent authorities In
this way the data can be assessed and
where appropriate the authorised prod-
uct inormation amended Article 46 o
the Regulation also requires companies tosubmit newly generated paediatric data
Since 2008 more than 18 000 study re-
ports on roughly 2 200 medicinal prod-
ucts have been submitted revealing the
large amount o existing paediatric inor-
mation available at company level
These study reports have been and
continue to be assessed by the compe-
tent authorities thanks to an impressive
work-sharing project (see Tables 10 and11) For nationally authorised products
this has led to the publication o assess-
ment reports covering more than 140
active substances and in a considerable
number o cases to recommendations
or changes to the summaries o product
characteristics o authorised products re-
sulting in 65 actual changes For centrally
authorised products by 2011 the Agency
had completed the assessment o all the
data submitted under Article 45 covering55 active substances in 61 centrally ap-
17 Regulation (EC) No4692009 o the Euro-
pean Parliament and othe Council o 6 May 2009
concerning the supplemen-tary protection certificateor medicinal products OJ
L 152 1662009 p 1 ThisRegulation is a codificationo Council Regulation (EEC)
No 176892
18 Case C-12510 Merck
Sharp amp Dohme v DeutschesPatent- und Markenamt notyet published in the ECR
paragraph 37 lsquoi the SPCapplication had to be reused
because the calculationprovided or in Article 13(1)o Regulation No 176892
results in a negative or zero
duration the holder o thebasic patent could not obtain
an extension o protectionconerred by such a patenteven i it conducted all the
studies according to the ap-proved paediatric investiga-
tion plan under Article 36 oRegulation No 19012006Such a reusal would be
liable to adversely impacton the useul effect oRegulation No 19012006
and might jeopardise the
objectives o that regulationnamely the compensation
o effort made to evaluatethe paediatric effects o themedicinal product at issuersquo
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1436
14
proved medicinal products The summa-
ries o product characteristics o 12 me-
dicinal products were changed ollowing
the assessment
5Lessonslearnt51 Better access to
treatment
One o the explicit goals o the Paediatric
Regulation is to increase the number oproducts that are researched developed
and authorised or use in children and
to reduce the off-label use o medicinal
products in the paediatric population
The main tool to achieve this result is to
oblige companies to establish a paediat-
ric investigation plan or each newly de-
veloped product or or the line extension
o an already authorised product that is
still under patent protection The plan ismeant to ensure mdash under the supervi-
sion o the Paediatric Committee mdash that
the necessary data are generated so as
to determine the conditions under which
a medicinal product may be authorised
to treat children Since 2008 more than
600 paediatric investigation plans have
been approved However only a minor-
ity o them has been completed to date
the vast majority are still on-going This
is due to the long development cycles omedicinal products ofen lasting more
than a decade and the near-systematic
deerral o paediatric studies The high
number o deerrals may not have been
initially expected but are currently a real-
ity as or most o the medicinal products
that have been authorised so ar the RampD
programme started beore the entering
into orce o the Regulation Consequent-
ly the paediatric requirements could not
be taken into account rom the beginningo the product development
While the Paediatric Regulation has led
to some new authorisations that include
paediatric indications the regulatory in-
strument is recent and it will probably
take at least a decade beore it can be
judged in terms o its output In terms o
pharmaceutical orms there is however
already a visible positive impact
In this context criticism has been voiced
that the Regulation will ail to ensure abreakthrough in areas o particular pae-
diatric need such as paediatric oncology
This argument is related to the act that
the starting point or the majority o pae-
diatric investigation plans is an ongoing
RampD programme or a medicinal product
or adults An intrinsic consequence o this
approach is that these products primarily
target adult conditions They are devel-
oped in areas where there is a need (or a
market) in the adult population This needin the older population does not neces-
sarily correspond to the paediatric popu-
lationrsquos need
Moreover the Regulation grants waivers
rom its obligations where the disease or
condition or which the specific medicinal
product is intended occurs only in adult
populations This legislative approach cre-
ates riction in the case o diseases that
are specific and exclusive to children Italso limits the powers and possibilities o
the Paediatric Committee when reviewing
and agreeing to a paediatric investigation
plan as regards the scope o studies that
the Committee may request rom appli-
cants ollowing the objective and scien-
tific-based assessment o the compound
concerned19
These constraints and boundaries have to
be taken into account when judging the
impact the Regulation is likely to make In
addition the effect o instruments such as
the Orphan Regulation have to be consid-
ered given that or example all paediatric
cancers are rare diseases and all under
the EU policy ramework on rare diseases
All in all the achievements highlighted in
chapter 4 o this report and the number
o products with new paediatric indica-
tions show that there are some encourag-
ing signs afer this first five-year period it
is however too early or comprehensive
answers
19 Case T-5209 Nycomed vEMA not yet published
See the results o the publicconsultation conducted by
the Commission in prepara-tion o this Report
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1536
15
52 The PUMA concept a
disappointment
The Paediatric Regulation introduced a
new type o marketing authorisation mdash
the Paediatric Use Marketing Authorisa-
tion (PUMA) As an incentive to carry out
research into the potential paediatric use
o off-patent medicinal products that have
been authorised or adults this marketing
authorisation offers 8 years o data and
10 years o market exclusivity to any new
off-patent product developed exclusively
or use in the paediatric population Thus
the main goal o the PUMA concept is to
stimulate research in existing products
This scheme has been supported by EU
unding through the EU Framework Pro-
grammes or Research and Technological
Development
However to date only one PUMA has been
granted with a ew more projects cur-
rently in the pipeline
Neither industry nor academic networks
have embraced this opportunity as ully
as the Regulation intended It would seem
that the incentive o data and market ex-
clusivity does not work or these productsor at least that the market opportunities
in this sector are currently considered in-
sufficient to outweigh the inherent eco-
nomic risks o pharmaceutical develop-
ment Researchers are not engaging in
trials with medicines that have been on
the market or years Companies seem to
ear that market exclusivity will not pre-
vent physicians rom continuing to use
competitor products with the same active
ingredient off-label at lower costs or thatsubstitution or cheaper adult orms takes
place at the level o pharmacies Moreo-
ver national pricing and reimbursement
rules in Member States ofen do not al-
low or the additional research needed to
obtain the PUMA to be rewarded in price
negotiations20
Against this background the PUMA con-
cept has ailed so ar to ulfil the initial
expectationsThe EMA will in uture accept paediatric
investigation plans or a PUMA that cover
only certain age groups and not the en-
tire paediatric population This may offset
some o the reservations that currently
hamper better endorsement o the PUMA
concept
53 No impact on adultdevelopment
Studies prior to the adoption o the Regu-
lation have suggested a theoretical risk
that the requirements or research in chil-
dren could lengthen the overall drug de-
velopment process21 The Regulation has
met this risk head-on In order to avoid
any delays in authorising medicines or
other populations it allows or the grant-
ing o deerrals relating to the initiation orcompletion o some or all o the meas-
ures contained in a paediatric investiga-
tion plan
Experience shows that the deerral is a
widely used instrument which suggests
that the risk o delays in the processing o
adult applications is minimal There have
been some transitional problems in cases
where the adult programme was already
established when the Regulation enteredinto orce but these issues seem to have
been resolved
A concern that was raised initially was
that some companies would become
reluctant to develop new indications
pharmaceutical orms and new routes o
administration in small markets and or
products with low sales to avoid being
bound by the paediatric obligation under
Article 8 o the Regulation However thereis no evidence o such effect Moreover
it may also be argued that the incentive
o a potential six-month extension o the
SPC served to counterbalance such an
effect as it may have led companies to
examine more thoroughly the benefits o
a line extension taking into account the
economic value o the paediatric reward
Still industry stakeholders claim that
in rare cases the development or new
medicinal products has been delayedor abandoned in the expectation or as a
consequence o additional costs and re-
quirements associated with paediatric de-
20 See the results o thepublic consultation con-
ducted by the Commission inpreparation o this Report
21 C Commission StaffWorking Document Proposal
or a Regulation o the Euro-pean Parliament and o theCouncil on medicinal prod-
ucts or paediatric use andamending Council Regulation(EEC) No 17692 Directive
200183EC and Regula-tion (EC) No 7262004Extended impact assessment
(COM2004599F)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1636
16
keting authorisation holders are obliged
to ensure that the product inormation
is kept up to date with the current scien-
tific knowledge While preerence should
be given to cooperative approaches the
enorcement tools may need to be used
i companies do not overcome their res-
ervations
On the whole the requirements o Articles
45 and 46 have provided an efficient and
appropriate instrument or collecting and
evaluating existing paediatric studies
55 Clinical trials with
children
It is generally accepted that the Paediatric
Regulation will lead to more clinical trialswith children but that its aims should be
achieved without subjecting children to
unnecessary clinical trials
The youngest paediatric-age subsets
including neonates are particularly sen-
sitive It will be a constant challenge to
balance the therapeutic needs o these
age groups with their specific vulnerability
when considering and deciding on the ap-
propriateness o specific clinical trials or
the specific settings o studies in this age
subset Efforts are thereore continuously
being made to explore alternative means
eg the use o extrapolation modelling
and simulation techniques to reduce the
number o study subjects as much as
possible The Paediatric Committee is ac-
tively contributing to acilitate the devel-
opment and use o such means including
non-conventional trial design
Another challenge is how to avoid dupli-cating trials or different paediatric inves-
tigation plans rom different applicants
Companies embarking on product devel-
opment in similar areas may be required
by the agreed paediatric investigation
plan to conduct studies within similar
settings While collaborative approaches
between companies would be highly de-
sirable and have occurred on rare occa-
sions they ofen conflict with companiesrsquo
understandable reluctance to share datawith competitors in the early stages o
product development and participate in
direct comparisons This situation could
velopment Overall there is however no
evidence that the Regulation has a con-
siderable negative impact on products or
other populations
Rather there are some concerns that the
requirements under the Regulation may
cause delays in the authorisation o prod-ucts with paediatric-only indications as
they bring added complexity to the RampD
and regulatory process or products that
already directly target children The added
value o the submission o a paediatric in-
vestigation plan in these cases will be as-
sessed urther in the 2017 report
54 Reaping the benefits of
existing information
There was widespread speculation prior to
the adoption o the Paediatric Regulation
as to how many studies would be submit-
ted by pharmaceutical companies in ac-
cordance with Articles 45 and 46 The act
that competent authorities received more
than 18 000 studies reveals the consid-
erable amount o paediatric inormation
that existed at company level
Certainly it is true that not all the inor-
mation submitted met modern require-
ments or scientific data and clinical re-
search and that the work-sharing process
o evaluating the inormation is rather
long and resource intensive
Nevertheless compared to the PUMA con-
cept this scheme proved more successul
in terms o output and in recommending
and implementing changes to the sum-
mary o product characteristics o author-
ised products In its public consultationthe Commission called Articles 45 and 46
the lsquohidden gemsrsquo o the Regulation
One drawback that remains however
is reluctance by marketing authorisa-
tion holders to update the summary o
product characteristics on a voluntary
basis This said the Regulation contains
mechanisms to overcome such reluctance
as it empowers competent authorities to
directly update the summary and varythe marketing authorisation accordingly
Moreover in accordance with Article 23
o Directive 200183EC22 and Article 16
o Regulation (EC) No 726200423 mar-
22 Directive 200183EC othe European Parliament and
o the Council o 6 November2001 on the Community
code relating to medicinalproducts or human use OJ L311 28112001 p 67
23 Regulation (EC) No7262004 o the European
Parliament and o the Coun-cil o 31 March 2004 layingdown Community procedures
or the authorisation andsupervision o medicinalproducts or human and
veterinary use and establish-ing a European Medicines
Agency OJ L 136 3042004p 1
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1736
17
lead to competition among companies to
find investigators and study participants
as well as the duplication o trials which
are unnecessary rom a scientific and
ethical point o view
The Paediatric Committee is able to waive
paediatric trial requirements where thespecific medicinal product does not rep-
resent a significant therapeutic benefit
over an existing treatment or paediatric
patients including once the product is au-
thorised (Article 11) However this option
does not provide a way out in the early
stages o product development where
the Committee has to ensure equal treat-
ment and non-discriminatory approaches
The key to avoiding such unnecessary tri-
als is transparency with regard to ongoingand completed trials The situation contin-
ues to be monitored
Finally it is in the interest o the EU that
paediatric trials stemming rom paedi-
atric investigation plans are conducted
within the EU This has less to do with
the standards under which a trial is con-
ducted given that clinical trials carried
out outside the EU have to meet the ethi-
cal and scientific requirements o the EUprovisions on clinical trials24 than with the
act that studies within the EU may pro-
vide patients there with early access to
innovative medicines To date there is in-
sufficient data on the ratio between pae-
diatric trials conducted within and outside
the EU However in view o the upgraded
unctionalities o the EudraCT database it
is expected that more data will be avail-
able in 2017 or the second report
56 Spreading the news mdash
getting new information
to patients and healthcare
professionals
I the Regulation is to be a success it is
not only necessary that data on the use
o a specific product in the paediatric
population are collected but that these
data are then also appropriately commu-
nicated to and used by paediatricians intheir day-to-day work or the benefit o
their patients
In this regard some studies published in
the medical literature suggest a ailure
on the part o practitioners to recognise
the actual amount o off-label prescrib-
ing to children Moreover it is claimed that
the prescribing habits o practitioners are
ofen strongly influenced by personal ex-
perience rather than by evidence-based
inormation or paediatric medicine25
These studies in making generalisations
may not have taken into account the het-
erogeneity o healthcare proessionals
whose receptiveness varies greatly ac-
cording to their work setting and specific
area o specialisation At the same time
such observations may point to a sub-
stantial hurdle in achieving the goal o the
Paediatric Regulation
National competent authorities as well as
organisations or healthcare proessionals
seem particularly qualified to consider ap-
propriate ways o ensuring an adequate
flow o inormation Some Member States
have already established a number o
tools to communicate effectively and e-
ficiently with healthcare proessionals
eg by means o regular meetings web-
based inormation distribution systems ornational ormularies
57 Is the burden greater
than rewards
There can be no doubt that the Paediat-
ric Regulation places a considerable ad-
ditional burden on pharmaceutical com-
panies with its obligations regarding
research on products or use in children
However this approach was adopted be-cause market orces alone proved insu-
ficient to stimulate adequate research
The Regulation requires companies to
submit paediatric investigation plans at
an early stage o product development
However research on some active sub-
stances may be discontinued at later
stages should urther studies ail to show
potential with respect to the saety and
efficacy o the product For every success-
ul authorised medicinal product there aremany that ail to make the finishing line
Hence not all approved paediatric investi-
gation plans will be completed as compa-
24 Directive 200120EC othe European Parliament
and o the Council on theapproximation o the laws
regulations and administra-tive provisions o the Mem-ber States relating to the
implementation o good clini-cal practice in the conducto clinical trials on medicinal
products or human use OJ L121 152001 p 34
25 5-year report to theEuropean Commission (seeootnote 3) page 41
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1836
18
nies may decide to stop the correspond-
ing adult development It is too early still
to obtain reliable statistics that show
the ratio between completed and non-
completed paediatric investigation plans
but in the current context not all approved
plans will eventually result in an approved
medicine with a paediatric indication
In terms o output this entails some un-
necessary effort in compiling and screen-
ing paediatric investigation plans To what
extent this is offset by the benefit o early
submission which ensures that the pae-
diatric development fits smoothly into the
overall product development need ur-
ther monitoring
A urther point o concern is the highnumber o modifications to paediat-
ric investigation plans Figures seem to
suggest that nearly all plans have to
be modified at least once Conceptually
though this does not come as a surprise
in view o the early submission o pae-
diatric investigation plans the length o
adult and paediatric developments and
the substantial deerrals granted An
RampD plan requently has to be adapted
or amended to take account o initial re-sults Recruitment problems or necessary
design changes in the trials may also lead
to modifications While it is acknowledged
that substantial amendments or modifi-
cations to the plan have to be subject to
discussions with the Paediatric Commit-
tee this is less obvious or minor changes
In this context the level o detail required
by the EMA has been repeatedly criticised
In the past five years the EMA and its
Paediatric Committee have made effortsto provide or some flexibility in the plan
so to allow a margin o manoeuvre that
takes account o uncertainties in relation
to certain parameters o a trial
In any case the Commission intends to
review its Communication on the ormat
and content o applications or agree-
ment or modification o a paediatric in-
vestigation plan to take into account the
experience gained including the consider-
able number o modification requests
On a positive note it can be noted that
companies are applying or the rewards
provided by the Regulation primarily the
6-month extension o the Supplementary
Protection Certificate which have been
introduced to offset the additional bur-
den The economic value o the reward
depends on the turnover o the product
concerned In the case o blockbuster
products the amount may be consider-
able while or niche products the effect
is small
An in-depth evaluation o the economic
impact will be included in the 2017 report
in order to draw conclusions on the bal-
ance between burden and rewards and
public health benefits
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1936
19
6Outlook mdash
A fairy-taleending aheadlsquoBetter Medicines or Children mdash From
Concept to Realityrsquo is the title o this re-
port Readers may suggest that based on
the evaluation reerred to above it would
be more appropriate to add a question
mark It is evident that it is too early still
to make a firm statement Despite more
than five years o experience the true im-pact o the Regulation on the health o
children will only become apparent over
time as experience is accumulated in the
longer term
There are encouraging signs though
Paediatric development has become a
more integral part o the overall develop-
ment o medicinal products in the EU A
number o new products with paediatric
indications and age-appropriate pharma-ceutical orms have been authorised and
made available to patients A high num-
ber o agreed paediatric investigation
plans indicates that urther products are
in the pipeline
However it needs to be pointed out that it
would be wrong to expect the Regulation
to be able to solve all problems Instead
it is a major catalyst to improve the situ-
ation o young patients
Finally some weaknesses and deficits
have also become apparent in the last
five years Their impact on the overall
perormance o the Regulation has to be
closely monitored On the basis o the ac-
tions outlined above the Commission in-
tends to fine-tune the current implemen-
tation together with the EMA
Even i better medicines or children are
not yet a reality it should be the ambitiono all stakeholders involved that this piece
o legislation will be or the greater good
o children so that in the 2017 report
the discussion will ocus not on whether a
question mark should be added to the ti-
tle o the report but on whether it should
be an exclamation mark instead
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2036
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2136
21
ANNEXES
Figures and Tables
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2236
22
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2336
23
ANNEX I
Figures and Tables
Table 1Agreed paediatric investigations plans (PIPs) 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Agreed PIPs submitted under Article 7 (without waivers)
Agreed PIPs submitted under Article 8 (without waivers)
Source EMA Paediatric database The numbers on agreed PIPs correspond to EMA decisions
Table 2Agreed paediatric investigations plans (PIPs) compared to ull waivers and modifications 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Submitted modifications of an agreed PIP
Agreed Full waivers
Source EMA Paediatric database The numbers on agreed PIPs and waivers correspond to EMA decisions
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2536
25
Table 5Scientific advice and protocol assistance including ollow-ups (provided by the EMA Scientific Advice Working
Party and the Committee or Human Medicinal Products per year)
259
277321
388 400 433 420
021 32
74 8057
91
0 0 0
68 8067
94
0
100
200
300
400
500
2006 2007 2008 2009 2010 2011 2012
Total number of advice (Scientific Advice and Protocol Assistance)
Sum of paediatric-only and mixed (adult and paediatric development questions)
advice
Paediatric-only or mixed advice that involved a Paediatric Committee member(s) as
expert(s)
Source EMA databases Year o advice letter
Year o start o procedure
Table 6Paediatric clinical trials by year o authorisation
2005 2006 2007 2008 2009 2010 2011 2012
Paediatric trials
(number) 254 316 355 342 404 379 334 332
Paediatric trials
that are part of anagreed PIP 2 1 2 6 16 30 76 76
Proportion of
paediatric trials
that are part of an
agreed PIP among
paediatric trials 1 0 1 2 4 8 23 23
Total number
of trials (adults
and or children) 3 350 3 979 4 749 4 512 4 445 4 026 3 809 3 698
Proportion of
paediatric trials of
all trials 8 8 7 8 9 10 9 9
Source EudraCT Data Warehouse using a predefined query on 6 March 2013 and counting the first authorised trial only in the case o more thanone Member State This partial inormation requires sponsors to use a Clinical Trial Application orm that was only available rom November 2009 or use with version 8 o EudraCT
(available rom 2011)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2636
26
Table 7Number o children to be enrolled in clinical trials
Number
of subjects 2006 2007 2008 2009 2010 2011 2012
Pretermnewborns 0 0 0 207 82 2 281 1 712
Newborns 0 0 5 64 169 1 105 1 172
Infants and
toddlers 330 21 20 59 351 2 788 3 141
Children 2 142 181 200 2 230 2 055 10 325 20 677
Adolescents 368 111 205 1 577 2 861 9 054 13 193
Sum of
above 2 840 313 430 4 137 5 517 25 553 39 895
Reference
number of paediatric
trials 316 355 342 404 379 334 332
Source EudraCT Data Warehouse using a pre-defined query on 6 March 2013 modified by excluding studies or lsquoimmunological medicinal productsrsquo
Table 8EU budget contribution to the Paediatric Regulation and the EMA expenditure
0
1
2
3
4
5
6
7
8
9
10
2006 2007 2008 2009 2010 2011 2012
EU budget contribution (in Million euro)
EMA expenditure for paediatri cs (in Mill ion euro)
EMA expenditure for paediatr ics including support (in Million euro)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2736
27
Table 9Percentage o European Medicines Agencyrsquos human resources working in the paediatric area rom 2006 (inner
circle) to 2012 (outer circle)
733 (2012)
052 (2006)
Table 10Member States acting as rapporteurs or the assessment o studies submitted in accordance with Article 46
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE SE NL FR DK IT BE PL ES NO SK FI IE RO AT HU EL CZ PT LV BG
Study included in worksharing Rapporteur appointed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2836
28
Table 11Member States acting as rapporteur or the assessment o studies submitted in accordance with Article 45
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE NL DK AT FR PL SE ES IE CZ MT IT BE SI EE FI HU NO RO BG EL LV PT IS SK
Wave 1 Wave 2 Wave 3 Wave 4 Wave 5 Wave 6 Wave 7 Wave 8 Wave 9
Wave 10 Wave 11 Wave 12 Wave 13 Wave 14 Wave 15 Wave 16 Wave 17 Wave 18
Table 12Member States acting as rapporteurspeer reviewers in EMArsquos Paediatric Committee procedures (initial PIP
waiver or modification o an agreed PIP)
0
50
100
150
200
250
300
350
400
450
500
A u s t r i a
B el gi um
B ul g a r i a
C y pr u s
C z e c h R e p u b l i c
D enm a r k
E s t oni a
F i nl a n d
F r a n c e
G er m a n y
G r e e c e
H e a l t h c a r e a n d
A c a d emi a
H un g a r y
I c el a n d
I r el a n d
I t a l y
L a t vi a
L i t h u a ni a
L ux em b o ur g
M a l t a
N or w a y
P a t i en t s Or g a ni s a t i on
P ol a n d
P or t u g a l
R om a ni a
S l ov a k i a
S l ov eni a
S p a i n
S w e d en
T h eN e t h er l a n d
s
U ni t e d K i n g d om
Initial PIP applications PIP modifications
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2936
29
ANNEX II
Detailed inventory of centrally authorised medicinalproducts for paediatric use since the entry into force
of the Paediatric Regulation
Table 13Medicinal products authorised centrally since 2007 which include a paediatric indication
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Retapamulin Altargo 2007 No Mixed
Nelarabine Atriance 2007 No Mixed
Human papillomavirus vaccine[types 16 18] Cervarix 2007 No Mixed
Hydroxocobalamin Cyanokit 2007 No Mixed
Idursulase Elaprase 2007 No Mixed
Gadoversetamide Optimark 2007 No Mixed
Betaine anhydrous Cystadane 2007 No Mixed
Stiripentol Diacomit 2007 No Paediatric only
Mecasermin Increlex 2007 No Paediatric only
Rufinamide Inovelon 2007 No Mixed
Hydroxycarbamide Siklos 2007 No Mixed
Human normal
immunoglobulin (ivig) Flebogamma DIF 2007 No Mixed
Fluticasone uroate Avamys 2008 No Mixed
Human normal immunoglobulin Privigen 2008 No Mixed
Lacosamide Vimpat 2008 No Mixed
Micaungin Mycamine 2008 No Mixed
Sapropterin Kuvan 2008 No Mixed
Sugammadex Bridion 2008 No Mixed
Tocoersonal d-alpha
tocopheryl polyethylene glycol
succinate Vedrop 2009 No Paediatric only
Miamurtide Mepact 2009 No Mixed
Rilonacept Rilonacept Regeneron 2009 No Mixed
Tacrolimus Modigra 2009 No Mixed
Pneumoccocal polysaccharideconjugate vaccine (adsorbed) Synflorix 2009 No Paediatric only
Canakinumab
Ilaris (PIP not yet
completed) 2009 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3036
30
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Pneumoccocal polysaccharide
conjugate vaccine (13-valentadsorbed)
Prevenar 13 (PIP not yetcompleted) 2009 Yes Paediatric only
Meningococcal group a c
w135 and y conjugate vaccine Menveo 2010 Yes Mixed
Velaglucerase ala
Vpriv (PIP not yet
completed) 2010 Yes Mixed
Influenza vaccine (live
attenuated nasal) Fluenz (Waiver) 2011 Yes Paediatric only
C1 inhibitor human
Cinryze (PIP not yet
completed) 2011 Yes Mixed
Dihydroartemisinin
piperaquine phosphate
Eurartesim (PIP not yet
completed) 2011 Yes Mixed
Midazolam Buccolam 2011 Yes (PUMA) Paediatric only
EverolimusVotubia(PIP not yet completed) 2011 Yes Mixed
Tobramycin
Tobi Podhaler (PIP not
yet completed) 2011 Yes Mixed
Nomegestrol estradiol Ioa Zoely 2011 Yes Mixed
Colistimethate sodium Colobreathe 2012 Yes Mixed
Mercaptopurine Xaluprine 2012 No Mixed
Catridecacog NovoThirteen 2012 Yes MixedEavirenz Eavirenz Teva 2012 No Mixed
Ivacafor Kalydeco 2012 Yes Mixed
Desloratadine Desloratadine ratiopharm 2012 No Mixed
Desloratadine Desloratadine Actavis 2012 No Mixed
Perampanel Fycompa 2012 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3136
31
Table 14List o centrally authorised medicinal products or which the therapeutic indication was extended to or amend-
ed or the paediatric population
Active substance(s)
Trade
name Date Subject of the extension
Levetiracetam Keppra
2007
2009
Extension o the indication to include adjunctive ther-
apy in the treatment o primary generalised tonic-
clonic (PGTC) seizures in adults and adolescents rom
12 years o age with idiopathic generalised epilepsyExtension o indication to include the adjunctive
treatment o partial seizures with or without second-
ary generalisation in children rom 1 month to lt4
years old
Pneumococcal sac-
charide conjugated
vaccine adsorbed Prevenar 2007
Extension o the indication to include new inorma-
tion on efficacy against disease caused by Strepto-
coccus pneumoniae serotypes 4 6B 9V 14 18C 19F
and 23F in otitis mediaExtension o indication rom active immunisation
against bacteraemic pneumonia to active immunisa-
tion against pneumonia
Infliximab
Remi-
cade 2007
Extension o indication to include treatment o
severe active Crohnrsquos disease in children aged 6 to
17 years
Darbepoetin ala Aranesp 2007
Extension o indication or CRF patients whichrestricted the use o Nespo to paediatric subjects ge
11 years o age
Fosamprenavir Telzir 2007
Extension o indication o Telzir in combination withritonavir or the treatment o Human Immunodefi-
ciency Virus Type 1 (HIV-1) inected adults in combi-nation with other antiretroviral medicinal products to
include paediatric populations
Lamivudine zidovu-
dine Combivir 2007
Extension o indication to include paediatric patients
and replacement o film-coated tablets by scored
film-coated tablets
Desloratadine Aerius 2007Extension o indication rom lsquochronic idiopathic urti-cariarsquo to lsquourticariarsquo
Insulin glulisine Apidra 2007
Extension o indication to include 6 year olds and
older children based on the results o 2 paediatricstudies
Human papilloma virusvaccine [types 6 11
16 18] (recombinantadsorbed) Gardasil 2008
Extension o indication to include the prevention ohigh-grade vaginal dysplastic lesions (VaIN 23)
Adalimumab Humira 20082011
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in adoles-cents rom 13 to 17 years o age
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in the paedi-
atric population aged rom 4 to 12 years
Caspoungin Cancidas 2008
Extension o the indication to include the paediatric
population
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1336
13
A detailed inventory o centrally autho-
rised products is provided in Annex II
Rewards and incentives
Companies that have complied with the
obligations o the Regulation may benefit
rom a reward once the product concerned
is authorised or the product inormation isamended The reward takes the orm o a
6-month extension o the supplementary
protection certificate (SPC) provided or
by Regulation (EC) No 469200917 or in
the case o an orphan medicinal product
by an extension o the ten-year period o
orphan market exclusivity to twelve years
No orphan rewards have been awarded
yet In this regard it is observed that some
companies withdrew the orphan designa-tion o a product in order to qualiy or
the SPC reward rather than the orphan
reward which seems to be more attrac-
tive rom an economic perspective As ar
as SPC extensions are concerned national
patent offices in 16 Member States had
by the end o 2011 granted 6-month ex-
tensions to 11 medicinal products which
resulted in a total o more than 100 na-
tional SPCs
It should be pointed out that a ruling othe European Court o Justice urther
increased the value o the paediatric
reward as it made clear that the initial
certificate could have a negative or zero
duration which could then become posi-
tive once the paediatric extension was
granted18
43 Increased information on
medicines used in childrenTo provide better inormation on the use
o medicinal products in children Article
45 o the Paediatric Regulation requires
companies holding data on the saety
or efficacy o authorised products in the
paediatric population to submit these
studies to the competent authorities In
this way the data can be assessed and
where appropriate the authorised prod-
uct inormation amended Article 46 o
the Regulation also requires companies tosubmit newly generated paediatric data
Since 2008 more than 18 000 study re-
ports on roughly 2 200 medicinal prod-
ucts have been submitted revealing the
large amount o existing paediatric inor-
mation available at company level
These study reports have been and
continue to be assessed by the compe-
tent authorities thanks to an impressive
work-sharing project (see Tables 10 and11) For nationally authorised products
this has led to the publication o assess-
ment reports covering more than 140
active substances and in a considerable
number o cases to recommendations
or changes to the summaries o product
characteristics o authorised products re-
sulting in 65 actual changes For centrally
authorised products by 2011 the Agency
had completed the assessment o all the
data submitted under Article 45 covering55 active substances in 61 centrally ap-
17 Regulation (EC) No4692009 o the Euro-
pean Parliament and othe Council o 6 May 2009
concerning the supplemen-tary protection certificateor medicinal products OJ
L 152 1662009 p 1 ThisRegulation is a codificationo Council Regulation (EEC)
No 176892
18 Case C-12510 Merck
Sharp amp Dohme v DeutschesPatent- und Markenamt notyet published in the ECR
paragraph 37 lsquoi the SPCapplication had to be reused
because the calculationprovided or in Article 13(1)o Regulation No 176892
results in a negative or zero
duration the holder o thebasic patent could not obtain
an extension o protectionconerred by such a patenteven i it conducted all the
studies according to the ap-proved paediatric investiga-
tion plan under Article 36 oRegulation No 19012006Such a reusal would be
liable to adversely impacton the useul effect oRegulation No 19012006
and might jeopardise the
objectives o that regulationnamely the compensation
o effort made to evaluatethe paediatric effects o themedicinal product at issuersquo
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1436
14
proved medicinal products The summa-
ries o product characteristics o 12 me-
dicinal products were changed ollowing
the assessment
5Lessonslearnt51 Better access to
treatment
One o the explicit goals o the Paediatric
Regulation is to increase the number oproducts that are researched developed
and authorised or use in children and
to reduce the off-label use o medicinal
products in the paediatric population
The main tool to achieve this result is to
oblige companies to establish a paediat-
ric investigation plan or each newly de-
veloped product or or the line extension
o an already authorised product that is
still under patent protection The plan ismeant to ensure mdash under the supervi-
sion o the Paediatric Committee mdash that
the necessary data are generated so as
to determine the conditions under which
a medicinal product may be authorised
to treat children Since 2008 more than
600 paediatric investigation plans have
been approved However only a minor-
ity o them has been completed to date
the vast majority are still on-going This
is due to the long development cycles omedicinal products ofen lasting more
than a decade and the near-systematic
deerral o paediatric studies The high
number o deerrals may not have been
initially expected but are currently a real-
ity as or most o the medicinal products
that have been authorised so ar the RampD
programme started beore the entering
into orce o the Regulation Consequent-
ly the paediatric requirements could not
be taken into account rom the beginningo the product development
While the Paediatric Regulation has led
to some new authorisations that include
paediatric indications the regulatory in-
strument is recent and it will probably
take at least a decade beore it can be
judged in terms o its output In terms o
pharmaceutical orms there is however
already a visible positive impact
In this context criticism has been voiced
that the Regulation will ail to ensure abreakthrough in areas o particular pae-
diatric need such as paediatric oncology
This argument is related to the act that
the starting point or the majority o pae-
diatric investigation plans is an ongoing
RampD programme or a medicinal product
or adults An intrinsic consequence o this
approach is that these products primarily
target adult conditions They are devel-
oped in areas where there is a need (or a
market) in the adult population This needin the older population does not neces-
sarily correspond to the paediatric popu-
lationrsquos need
Moreover the Regulation grants waivers
rom its obligations where the disease or
condition or which the specific medicinal
product is intended occurs only in adult
populations This legislative approach cre-
ates riction in the case o diseases that
are specific and exclusive to children Italso limits the powers and possibilities o
the Paediatric Committee when reviewing
and agreeing to a paediatric investigation
plan as regards the scope o studies that
the Committee may request rom appli-
cants ollowing the objective and scien-
tific-based assessment o the compound
concerned19
These constraints and boundaries have to
be taken into account when judging the
impact the Regulation is likely to make In
addition the effect o instruments such as
the Orphan Regulation have to be consid-
ered given that or example all paediatric
cancers are rare diseases and all under
the EU policy ramework on rare diseases
All in all the achievements highlighted in
chapter 4 o this report and the number
o products with new paediatric indica-
tions show that there are some encourag-
ing signs afer this first five-year period it
is however too early or comprehensive
answers
19 Case T-5209 Nycomed vEMA not yet published
See the results o the publicconsultation conducted by
the Commission in prepara-tion o this Report
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1536
15
52 The PUMA concept a
disappointment
The Paediatric Regulation introduced a
new type o marketing authorisation mdash
the Paediatric Use Marketing Authorisa-
tion (PUMA) As an incentive to carry out
research into the potential paediatric use
o off-patent medicinal products that have
been authorised or adults this marketing
authorisation offers 8 years o data and
10 years o market exclusivity to any new
off-patent product developed exclusively
or use in the paediatric population Thus
the main goal o the PUMA concept is to
stimulate research in existing products
This scheme has been supported by EU
unding through the EU Framework Pro-
grammes or Research and Technological
Development
However to date only one PUMA has been
granted with a ew more projects cur-
rently in the pipeline
Neither industry nor academic networks
have embraced this opportunity as ully
as the Regulation intended It would seem
that the incentive o data and market ex-
clusivity does not work or these productsor at least that the market opportunities
in this sector are currently considered in-
sufficient to outweigh the inherent eco-
nomic risks o pharmaceutical develop-
ment Researchers are not engaging in
trials with medicines that have been on
the market or years Companies seem to
ear that market exclusivity will not pre-
vent physicians rom continuing to use
competitor products with the same active
ingredient off-label at lower costs or thatsubstitution or cheaper adult orms takes
place at the level o pharmacies Moreo-
ver national pricing and reimbursement
rules in Member States ofen do not al-
low or the additional research needed to
obtain the PUMA to be rewarded in price
negotiations20
Against this background the PUMA con-
cept has ailed so ar to ulfil the initial
expectationsThe EMA will in uture accept paediatric
investigation plans or a PUMA that cover
only certain age groups and not the en-
tire paediatric population This may offset
some o the reservations that currently
hamper better endorsement o the PUMA
concept
53 No impact on adultdevelopment
Studies prior to the adoption o the Regu-
lation have suggested a theoretical risk
that the requirements or research in chil-
dren could lengthen the overall drug de-
velopment process21 The Regulation has
met this risk head-on In order to avoid
any delays in authorising medicines or
other populations it allows or the grant-
ing o deerrals relating to the initiation orcompletion o some or all o the meas-
ures contained in a paediatric investiga-
tion plan
Experience shows that the deerral is a
widely used instrument which suggests
that the risk o delays in the processing o
adult applications is minimal There have
been some transitional problems in cases
where the adult programme was already
established when the Regulation enteredinto orce but these issues seem to have
been resolved
A concern that was raised initially was
that some companies would become
reluctant to develop new indications
pharmaceutical orms and new routes o
administration in small markets and or
products with low sales to avoid being
bound by the paediatric obligation under
Article 8 o the Regulation However thereis no evidence o such effect Moreover
it may also be argued that the incentive
o a potential six-month extension o the
SPC served to counterbalance such an
effect as it may have led companies to
examine more thoroughly the benefits o
a line extension taking into account the
economic value o the paediatric reward
Still industry stakeholders claim that
in rare cases the development or new
medicinal products has been delayedor abandoned in the expectation or as a
consequence o additional costs and re-
quirements associated with paediatric de-
20 See the results o thepublic consultation con-
ducted by the Commission inpreparation o this Report
21 C Commission StaffWorking Document Proposal
or a Regulation o the Euro-pean Parliament and o theCouncil on medicinal prod-
ucts or paediatric use andamending Council Regulation(EEC) No 17692 Directive
200183EC and Regula-tion (EC) No 7262004Extended impact assessment
(COM2004599F)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1636
16
keting authorisation holders are obliged
to ensure that the product inormation
is kept up to date with the current scien-
tific knowledge While preerence should
be given to cooperative approaches the
enorcement tools may need to be used
i companies do not overcome their res-
ervations
On the whole the requirements o Articles
45 and 46 have provided an efficient and
appropriate instrument or collecting and
evaluating existing paediatric studies
55 Clinical trials with
children
It is generally accepted that the Paediatric
Regulation will lead to more clinical trialswith children but that its aims should be
achieved without subjecting children to
unnecessary clinical trials
The youngest paediatric-age subsets
including neonates are particularly sen-
sitive It will be a constant challenge to
balance the therapeutic needs o these
age groups with their specific vulnerability
when considering and deciding on the ap-
propriateness o specific clinical trials or
the specific settings o studies in this age
subset Efforts are thereore continuously
being made to explore alternative means
eg the use o extrapolation modelling
and simulation techniques to reduce the
number o study subjects as much as
possible The Paediatric Committee is ac-
tively contributing to acilitate the devel-
opment and use o such means including
non-conventional trial design
Another challenge is how to avoid dupli-cating trials or different paediatric inves-
tigation plans rom different applicants
Companies embarking on product devel-
opment in similar areas may be required
by the agreed paediatric investigation
plan to conduct studies within similar
settings While collaborative approaches
between companies would be highly de-
sirable and have occurred on rare occa-
sions they ofen conflict with companiesrsquo
understandable reluctance to share datawith competitors in the early stages o
product development and participate in
direct comparisons This situation could
velopment Overall there is however no
evidence that the Regulation has a con-
siderable negative impact on products or
other populations
Rather there are some concerns that the
requirements under the Regulation may
cause delays in the authorisation o prod-ucts with paediatric-only indications as
they bring added complexity to the RampD
and regulatory process or products that
already directly target children The added
value o the submission o a paediatric in-
vestigation plan in these cases will be as-
sessed urther in the 2017 report
54 Reaping the benefits of
existing information
There was widespread speculation prior to
the adoption o the Paediatric Regulation
as to how many studies would be submit-
ted by pharmaceutical companies in ac-
cordance with Articles 45 and 46 The act
that competent authorities received more
than 18 000 studies reveals the consid-
erable amount o paediatric inormation
that existed at company level
Certainly it is true that not all the inor-
mation submitted met modern require-
ments or scientific data and clinical re-
search and that the work-sharing process
o evaluating the inormation is rather
long and resource intensive
Nevertheless compared to the PUMA con-
cept this scheme proved more successul
in terms o output and in recommending
and implementing changes to the sum-
mary o product characteristics o author-
ised products In its public consultationthe Commission called Articles 45 and 46
the lsquohidden gemsrsquo o the Regulation
One drawback that remains however
is reluctance by marketing authorisa-
tion holders to update the summary o
product characteristics on a voluntary
basis This said the Regulation contains
mechanisms to overcome such reluctance
as it empowers competent authorities to
directly update the summary and varythe marketing authorisation accordingly
Moreover in accordance with Article 23
o Directive 200183EC22 and Article 16
o Regulation (EC) No 726200423 mar-
22 Directive 200183EC othe European Parliament and
o the Council o 6 November2001 on the Community
code relating to medicinalproducts or human use OJ L311 28112001 p 67
23 Regulation (EC) No7262004 o the European
Parliament and o the Coun-cil o 31 March 2004 layingdown Community procedures
or the authorisation andsupervision o medicinalproducts or human and
veterinary use and establish-ing a European Medicines
Agency OJ L 136 3042004p 1
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1736
17
lead to competition among companies to
find investigators and study participants
as well as the duplication o trials which
are unnecessary rom a scientific and
ethical point o view
The Paediatric Committee is able to waive
paediatric trial requirements where thespecific medicinal product does not rep-
resent a significant therapeutic benefit
over an existing treatment or paediatric
patients including once the product is au-
thorised (Article 11) However this option
does not provide a way out in the early
stages o product development where
the Committee has to ensure equal treat-
ment and non-discriminatory approaches
The key to avoiding such unnecessary tri-
als is transparency with regard to ongoingand completed trials The situation contin-
ues to be monitored
Finally it is in the interest o the EU that
paediatric trials stemming rom paedi-
atric investigation plans are conducted
within the EU This has less to do with
the standards under which a trial is con-
ducted given that clinical trials carried
out outside the EU have to meet the ethi-
cal and scientific requirements o the EUprovisions on clinical trials24 than with the
act that studies within the EU may pro-
vide patients there with early access to
innovative medicines To date there is in-
sufficient data on the ratio between pae-
diatric trials conducted within and outside
the EU However in view o the upgraded
unctionalities o the EudraCT database it
is expected that more data will be avail-
able in 2017 or the second report
56 Spreading the news mdash
getting new information
to patients and healthcare
professionals
I the Regulation is to be a success it is
not only necessary that data on the use
o a specific product in the paediatric
population are collected but that these
data are then also appropriately commu-
nicated to and used by paediatricians intheir day-to-day work or the benefit o
their patients
In this regard some studies published in
the medical literature suggest a ailure
on the part o practitioners to recognise
the actual amount o off-label prescrib-
ing to children Moreover it is claimed that
the prescribing habits o practitioners are
ofen strongly influenced by personal ex-
perience rather than by evidence-based
inormation or paediatric medicine25
These studies in making generalisations
may not have taken into account the het-
erogeneity o healthcare proessionals
whose receptiveness varies greatly ac-
cording to their work setting and specific
area o specialisation At the same time
such observations may point to a sub-
stantial hurdle in achieving the goal o the
Paediatric Regulation
National competent authorities as well as
organisations or healthcare proessionals
seem particularly qualified to consider ap-
propriate ways o ensuring an adequate
flow o inormation Some Member States
have already established a number o
tools to communicate effectively and e-
ficiently with healthcare proessionals
eg by means o regular meetings web-
based inormation distribution systems ornational ormularies
57 Is the burden greater
than rewards
There can be no doubt that the Paediat-
ric Regulation places a considerable ad-
ditional burden on pharmaceutical com-
panies with its obligations regarding
research on products or use in children
However this approach was adopted be-cause market orces alone proved insu-
ficient to stimulate adequate research
The Regulation requires companies to
submit paediatric investigation plans at
an early stage o product development
However research on some active sub-
stances may be discontinued at later
stages should urther studies ail to show
potential with respect to the saety and
efficacy o the product For every success-
ul authorised medicinal product there aremany that ail to make the finishing line
Hence not all approved paediatric investi-
gation plans will be completed as compa-
24 Directive 200120EC othe European Parliament
and o the Council on theapproximation o the laws
regulations and administra-tive provisions o the Mem-ber States relating to the
implementation o good clini-cal practice in the conducto clinical trials on medicinal
products or human use OJ L121 152001 p 34
25 5-year report to theEuropean Commission (seeootnote 3) page 41
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1836
18
nies may decide to stop the correspond-
ing adult development It is too early still
to obtain reliable statistics that show
the ratio between completed and non-
completed paediatric investigation plans
but in the current context not all approved
plans will eventually result in an approved
medicine with a paediatric indication
In terms o output this entails some un-
necessary effort in compiling and screen-
ing paediatric investigation plans To what
extent this is offset by the benefit o early
submission which ensures that the pae-
diatric development fits smoothly into the
overall product development need ur-
ther monitoring
A urther point o concern is the highnumber o modifications to paediat-
ric investigation plans Figures seem to
suggest that nearly all plans have to
be modified at least once Conceptually
though this does not come as a surprise
in view o the early submission o pae-
diatric investigation plans the length o
adult and paediatric developments and
the substantial deerrals granted An
RampD plan requently has to be adapted
or amended to take account o initial re-sults Recruitment problems or necessary
design changes in the trials may also lead
to modifications While it is acknowledged
that substantial amendments or modifi-
cations to the plan have to be subject to
discussions with the Paediatric Commit-
tee this is less obvious or minor changes
In this context the level o detail required
by the EMA has been repeatedly criticised
In the past five years the EMA and its
Paediatric Committee have made effortsto provide or some flexibility in the plan
so to allow a margin o manoeuvre that
takes account o uncertainties in relation
to certain parameters o a trial
In any case the Commission intends to
review its Communication on the ormat
and content o applications or agree-
ment or modification o a paediatric in-
vestigation plan to take into account the
experience gained including the consider-
able number o modification requests
On a positive note it can be noted that
companies are applying or the rewards
provided by the Regulation primarily the
6-month extension o the Supplementary
Protection Certificate which have been
introduced to offset the additional bur-
den The economic value o the reward
depends on the turnover o the product
concerned In the case o blockbuster
products the amount may be consider-
able while or niche products the effect
is small
An in-depth evaluation o the economic
impact will be included in the 2017 report
in order to draw conclusions on the bal-
ance between burden and rewards and
public health benefits
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1936
19
6Outlook mdash
A fairy-taleending aheadlsquoBetter Medicines or Children mdash From
Concept to Realityrsquo is the title o this re-
port Readers may suggest that based on
the evaluation reerred to above it would
be more appropriate to add a question
mark It is evident that it is too early still
to make a firm statement Despite more
than five years o experience the true im-pact o the Regulation on the health o
children will only become apparent over
time as experience is accumulated in the
longer term
There are encouraging signs though
Paediatric development has become a
more integral part o the overall develop-
ment o medicinal products in the EU A
number o new products with paediatric
indications and age-appropriate pharma-ceutical orms have been authorised and
made available to patients A high num-
ber o agreed paediatric investigation
plans indicates that urther products are
in the pipeline
However it needs to be pointed out that it
would be wrong to expect the Regulation
to be able to solve all problems Instead
it is a major catalyst to improve the situ-
ation o young patients
Finally some weaknesses and deficits
have also become apparent in the last
five years Their impact on the overall
perormance o the Regulation has to be
closely monitored On the basis o the ac-
tions outlined above the Commission in-
tends to fine-tune the current implemen-
tation together with the EMA
Even i better medicines or children are
not yet a reality it should be the ambitiono all stakeholders involved that this piece
o legislation will be or the greater good
o children so that in the 2017 report
the discussion will ocus not on whether a
question mark should be added to the ti-
tle o the report but on whether it should
be an exclamation mark instead
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2036
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2136
21
ANNEXES
Figures and Tables
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2236
22
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2336
23
ANNEX I
Figures and Tables
Table 1Agreed paediatric investigations plans (PIPs) 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Agreed PIPs submitted under Article 7 (without waivers)
Agreed PIPs submitted under Article 8 (without waivers)
Source EMA Paediatric database The numbers on agreed PIPs correspond to EMA decisions
Table 2Agreed paediatric investigations plans (PIPs) compared to ull waivers and modifications 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Submitted modifications of an agreed PIP
Agreed Full waivers
Source EMA Paediatric database The numbers on agreed PIPs and waivers correspond to EMA decisions
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2536
25
Table 5Scientific advice and protocol assistance including ollow-ups (provided by the EMA Scientific Advice Working
Party and the Committee or Human Medicinal Products per year)
259
277321
388 400 433 420
021 32
74 8057
91
0 0 0
68 8067
94
0
100
200
300
400
500
2006 2007 2008 2009 2010 2011 2012
Total number of advice (Scientific Advice and Protocol Assistance)
Sum of paediatric-only and mixed (adult and paediatric development questions)
advice
Paediatric-only or mixed advice that involved a Paediatric Committee member(s) as
expert(s)
Source EMA databases Year o advice letter
Year o start o procedure
Table 6Paediatric clinical trials by year o authorisation
2005 2006 2007 2008 2009 2010 2011 2012
Paediatric trials
(number) 254 316 355 342 404 379 334 332
Paediatric trials
that are part of anagreed PIP 2 1 2 6 16 30 76 76
Proportion of
paediatric trials
that are part of an
agreed PIP among
paediatric trials 1 0 1 2 4 8 23 23
Total number
of trials (adults
and or children) 3 350 3 979 4 749 4 512 4 445 4 026 3 809 3 698
Proportion of
paediatric trials of
all trials 8 8 7 8 9 10 9 9
Source EudraCT Data Warehouse using a predefined query on 6 March 2013 and counting the first authorised trial only in the case o more thanone Member State This partial inormation requires sponsors to use a Clinical Trial Application orm that was only available rom November 2009 or use with version 8 o EudraCT
(available rom 2011)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2636
26
Table 7Number o children to be enrolled in clinical trials
Number
of subjects 2006 2007 2008 2009 2010 2011 2012
Pretermnewborns 0 0 0 207 82 2 281 1 712
Newborns 0 0 5 64 169 1 105 1 172
Infants and
toddlers 330 21 20 59 351 2 788 3 141
Children 2 142 181 200 2 230 2 055 10 325 20 677
Adolescents 368 111 205 1 577 2 861 9 054 13 193
Sum of
above 2 840 313 430 4 137 5 517 25 553 39 895
Reference
number of paediatric
trials 316 355 342 404 379 334 332
Source EudraCT Data Warehouse using a pre-defined query on 6 March 2013 modified by excluding studies or lsquoimmunological medicinal productsrsquo
Table 8EU budget contribution to the Paediatric Regulation and the EMA expenditure
0
1
2
3
4
5
6
7
8
9
10
2006 2007 2008 2009 2010 2011 2012
EU budget contribution (in Million euro)
EMA expenditure for paediatri cs (in Mill ion euro)
EMA expenditure for paediatr ics including support (in Million euro)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2736
27
Table 9Percentage o European Medicines Agencyrsquos human resources working in the paediatric area rom 2006 (inner
circle) to 2012 (outer circle)
733 (2012)
052 (2006)
Table 10Member States acting as rapporteurs or the assessment o studies submitted in accordance with Article 46
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE SE NL FR DK IT BE PL ES NO SK FI IE RO AT HU EL CZ PT LV BG
Study included in worksharing Rapporteur appointed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2836
28
Table 11Member States acting as rapporteur or the assessment o studies submitted in accordance with Article 45
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE NL DK AT FR PL SE ES IE CZ MT IT BE SI EE FI HU NO RO BG EL LV PT IS SK
Wave 1 Wave 2 Wave 3 Wave 4 Wave 5 Wave 6 Wave 7 Wave 8 Wave 9
Wave 10 Wave 11 Wave 12 Wave 13 Wave 14 Wave 15 Wave 16 Wave 17 Wave 18
Table 12Member States acting as rapporteurspeer reviewers in EMArsquos Paediatric Committee procedures (initial PIP
waiver or modification o an agreed PIP)
0
50
100
150
200
250
300
350
400
450
500
A u s t r i a
B el gi um
B ul g a r i a
C y pr u s
C z e c h R e p u b l i c
D enm a r k
E s t oni a
F i nl a n d
F r a n c e
G er m a n y
G r e e c e
H e a l t h c a r e a n d
A c a d emi a
H un g a r y
I c el a n d
I r el a n d
I t a l y
L a t vi a
L i t h u a ni a
L ux em b o ur g
M a l t a
N or w a y
P a t i en t s Or g a ni s a t i on
P ol a n d
P or t u g a l
R om a ni a
S l ov a k i a
S l ov eni a
S p a i n
S w e d en
T h eN e t h er l a n d
s
U ni t e d K i n g d om
Initial PIP applications PIP modifications
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2936
29
ANNEX II
Detailed inventory of centrally authorised medicinalproducts for paediatric use since the entry into force
of the Paediatric Regulation
Table 13Medicinal products authorised centrally since 2007 which include a paediatric indication
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Retapamulin Altargo 2007 No Mixed
Nelarabine Atriance 2007 No Mixed
Human papillomavirus vaccine[types 16 18] Cervarix 2007 No Mixed
Hydroxocobalamin Cyanokit 2007 No Mixed
Idursulase Elaprase 2007 No Mixed
Gadoversetamide Optimark 2007 No Mixed
Betaine anhydrous Cystadane 2007 No Mixed
Stiripentol Diacomit 2007 No Paediatric only
Mecasermin Increlex 2007 No Paediatric only
Rufinamide Inovelon 2007 No Mixed
Hydroxycarbamide Siklos 2007 No Mixed
Human normal
immunoglobulin (ivig) Flebogamma DIF 2007 No Mixed
Fluticasone uroate Avamys 2008 No Mixed
Human normal immunoglobulin Privigen 2008 No Mixed
Lacosamide Vimpat 2008 No Mixed
Micaungin Mycamine 2008 No Mixed
Sapropterin Kuvan 2008 No Mixed
Sugammadex Bridion 2008 No Mixed
Tocoersonal d-alpha
tocopheryl polyethylene glycol
succinate Vedrop 2009 No Paediatric only
Miamurtide Mepact 2009 No Mixed
Rilonacept Rilonacept Regeneron 2009 No Mixed
Tacrolimus Modigra 2009 No Mixed
Pneumoccocal polysaccharideconjugate vaccine (adsorbed) Synflorix 2009 No Paediatric only
Canakinumab
Ilaris (PIP not yet
completed) 2009 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3036
30
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Pneumoccocal polysaccharide
conjugate vaccine (13-valentadsorbed)
Prevenar 13 (PIP not yetcompleted) 2009 Yes Paediatric only
Meningococcal group a c
w135 and y conjugate vaccine Menveo 2010 Yes Mixed
Velaglucerase ala
Vpriv (PIP not yet
completed) 2010 Yes Mixed
Influenza vaccine (live
attenuated nasal) Fluenz (Waiver) 2011 Yes Paediatric only
C1 inhibitor human
Cinryze (PIP not yet
completed) 2011 Yes Mixed
Dihydroartemisinin
piperaquine phosphate
Eurartesim (PIP not yet
completed) 2011 Yes Mixed
Midazolam Buccolam 2011 Yes (PUMA) Paediatric only
EverolimusVotubia(PIP not yet completed) 2011 Yes Mixed
Tobramycin
Tobi Podhaler (PIP not
yet completed) 2011 Yes Mixed
Nomegestrol estradiol Ioa Zoely 2011 Yes Mixed
Colistimethate sodium Colobreathe 2012 Yes Mixed
Mercaptopurine Xaluprine 2012 No Mixed
Catridecacog NovoThirteen 2012 Yes MixedEavirenz Eavirenz Teva 2012 No Mixed
Ivacafor Kalydeco 2012 Yes Mixed
Desloratadine Desloratadine ratiopharm 2012 No Mixed
Desloratadine Desloratadine Actavis 2012 No Mixed
Perampanel Fycompa 2012 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3136
31
Table 14List o centrally authorised medicinal products or which the therapeutic indication was extended to or amend-
ed or the paediatric population
Active substance(s)
Trade
name Date Subject of the extension
Levetiracetam Keppra
2007
2009
Extension o the indication to include adjunctive ther-
apy in the treatment o primary generalised tonic-
clonic (PGTC) seizures in adults and adolescents rom
12 years o age with idiopathic generalised epilepsyExtension o indication to include the adjunctive
treatment o partial seizures with or without second-
ary generalisation in children rom 1 month to lt4
years old
Pneumococcal sac-
charide conjugated
vaccine adsorbed Prevenar 2007
Extension o the indication to include new inorma-
tion on efficacy against disease caused by Strepto-
coccus pneumoniae serotypes 4 6B 9V 14 18C 19F
and 23F in otitis mediaExtension o indication rom active immunisation
against bacteraemic pneumonia to active immunisa-
tion against pneumonia
Infliximab
Remi-
cade 2007
Extension o indication to include treatment o
severe active Crohnrsquos disease in children aged 6 to
17 years
Darbepoetin ala Aranesp 2007
Extension o indication or CRF patients whichrestricted the use o Nespo to paediatric subjects ge
11 years o age
Fosamprenavir Telzir 2007
Extension o indication o Telzir in combination withritonavir or the treatment o Human Immunodefi-
ciency Virus Type 1 (HIV-1) inected adults in combi-nation with other antiretroviral medicinal products to
include paediatric populations
Lamivudine zidovu-
dine Combivir 2007
Extension o indication to include paediatric patients
and replacement o film-coated tablets by scored
film-coated tablets
Desloratadine Aerius 2007Extension o indication rom lsquochronic idiopathic urti-cariarsquo to lsquourticariarsquo
Insulin glulisine Apidra 2007
Extension o indication to include 6 year olds and
older children based on the results o 2 paediatricstudies
Human papilloma virusvaccine [types 6 11
16 18] (recombinantadsorbed) Gardasil 2008
Extension o indication to include the prevention ohigh-grade vaginal dysplastic lesions (VaIN 23)
Adalimumab Humira 20082011
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in adoles-cents rom 13 to 17 years o age
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in the paedi-
atric population aged rom 4 to 12 years
Caspoungin Cancidas 2008
Extension o the indication to include the paediatric
population
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1436
14
proved medicinal products The summa-
ries o product characteristics o 12 me-
dicinal products were changed ollowing
the assessment
5Lessonslearnt51 Better access to
treatment
One o the explicit goals o the Paediatric
Regulation is to increase the number oproducts that are researched developed
and authorised or use in children and
to reduce the off-label use o medicinal
products in the paediatric population
The main tool to achieve this result is to
oblige companies to establish a paediat-
ric investigation plan or each newly de-
veloped product or or the line extension
o an already authorised product that is
still under patent protection The plan ismeant to ensure mdash under the supervi-
sion o the Paediatric Committee mdash that
the necessary data are generated so as
to determine the conditions under which
a medicinal product may be authorised
to treat children Since 2008 more than
600 paediatric investigation plans have
been approved However only a minor-
ity o them has been completed to date
the vast majority are still on-going This
is due to the long development cycles omedicinal products ofen lasting more
than a decade and the near-systematic
deerral o paediatric studies The high
number o deerrals may not have been
initially expected but are currently a real-
ity as or most o the medicinal products
that have been authorised so ar the RampD
programme started beore the entering
into orce o the Regulation Consequent-
ly the paediatric requirements could not
be taken into account rom the beginningo the product development
While the Paediatric Regulation has led
to some new authorisations that include
paediatric indications the regulatory in-
strument is recent and it will probably
take at least a decade beore it can be
judged in terms o its output In terms o
pharmaceutical orms there is however
already a visible positive impact
In this context criticism has been voiced
that the Regulation will ail to ensure abreakthrough in areas o particular pae-
diatric need such as paediatric oncology
This argument is related to the act that
the starting point or the majority o pae-
diatric investigation plans is an ongoing
RampD programme or a medicinal product
or adults An intrinsic consequence o this
approach is that these products primarily
target adult conditions They are devel-
oped in areas where there is a need (or a
market) in the adult population This needin the older population does not neces-
sarily correspond to the paediatric popu-
lationrsquos need
Moreover the Regulation grants waivers
rom its obligations where the disease or
condition or which the specific medicinal
product is intended occurs only in adult
populations This legislative approach cre-
ates riction in the case o diseases that
are specific and exclusive to children Italso limits the powers and possibilities o
the Paediatric Committee when reviewing
and agreeing to a paediatric investigation
plan as regards the scope o studies that
the Committee may request rom appli-
cants ollowing the objective and scien-
tific-based assessment o the compound
concerned19
These constraints and boundaries have to
be taken into account when judging the
impact the Regulation is likely to make In
addition the effect o instruments such as
the Orphan Regulation have to be consid-
ered given that or example all paediatric
cancers are rare diseases and all under
the EU policy ramework on rare diseases
All in all the achievements highlighted in
chapter 4 o this report and the number
o products with new paediatric indica-
tions show that there are some encourag-
ing signs afer this first five-year period it
is however too early or comprehensive
answers
19 Case T-5209 Nycomed vEMA not yet published
See the results o the publicconsultation conducted by
the Commission in prepara-tion o this Report
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1536
15
52 The PUMA concept a
disappointment
The Paediatric Regulation introduced a
new type o marketing authorisation mdash
the Paediatric Use Marketing Authorisa-
tion (PUMA) As an incentive to carry out
research into the potential paediatric use
o off-patent medicinal products that have
been authorised or adults this marketing
authorisation offers 8 years o data and
10 years o market exclusivity to any new
off-patent product developed exclusively
or use in the paediatric population Thus
the main goal o the PUMA concept is to
stimulate research in existing products
This scheme has been supported by EU
unding through the EU Framework Pro-
grammes or Research and Technological
Development
However to date only one PUMA has been
granted with a ew more projects cur-
rently in the pipeline
Neither industry nor academic networks
have embraced this opportunity as ully
as the Regulation intended It would seem
that the incentive o data and market ex-
clusivity does not work or these productsor at least that the market opportunities
in this sector are currently considered in-
sufficient to outweigh the inherent eco-
nomic risks o pharmaceutical develop-
ment Researchers are not engaging in
trials with medicines that have been on
the market or years Companies seem to
ear that market exclusivity will not pre-
vent physicians rom continuing to use
competitor products with the same active
ingredient off-label at lower costs or thatsubstitution or cheaper adult orms takes
place at the level o pharmacies Moreo-
ver national pricing and reimbursement
rules in Member States ofen do not al-
low or the additional research needed to
obtain the PUMA to be rewarded in price
negotiations20
Against this background the PUMA con-
cept has ailed so ar to ulfil the initial
expectationsThe EMA will in uture accept paediatric
investigation plans or a PUMA that cover
only certain age groups and not the en-
tire paediatric population This may offset
some o the reservations that currently
hamper better endorsement o the PUMA
concept
53 No impact on adultdevelopment
Studies prior to the adoption o the Regu-
lation have suggested a theoretical risk
that the requirements or research in chil-
dren could lengthen the overall drug de-
velopment process21 The Regulation has
met this risk head-on In order to avoid
any delays in authorising medicines or
other populations it allows or the grant-
ing o deerrals relating to the initiation orcompletion o some or all o the meas-
ures contained in a paediatric investiga-
tion plan
Experience shows that the deerral is a
widely used instrument which suggests
that the risk o delays in the processing o
adult applications is minimal There have
been some transitional problems in cases
where the adult programme was already
established when the Regulation enteredinto orce but these issues seem to have
been resolved
A concern that was raised initially was
that some companies would become
reluctant to develop new indications
pharmaceutical orms and new routes o
administration in small markets and or
products with low sales to avoid being
bound by the paediatric obligation under
Article 8 o the Regulation However thereis no evidence o such effect Moreover
it may also be argued that the incentive
o a potential six-month extension o the
SPC served to counterbalance such an
effect as it may have led companies to
examine more thoroughly the benefits o
a line extension taking into account the
economic value o the paediatric reward
Still industry stakeholders claim that
in rare cases the development or new
medicinal products has been delayedor abandoned in the expectation or as a
consequence o additional costs and re-
quirements associated with paediatric de-
20 See the results o thepublic consultation con-
ducted by the Commission inpreparation o this Report
21 C Commission StaffWorking Document Proposal
or a Regulation o the Euro-pean Parliament and o theCouncil on medicinal prod-
ucts or paediatric use andamending Council Regulation(EEC) No 17692 Directive
200183EC and Regula-tion (EC) No 7262004Extended impact assessment
(COM2004599F)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1636
16
keting authorisation holders are obliged
to ensure that the product inormation
is kept up to date with the current scien-
tific knowledge While preerence should
be given to cooperative approaches the
enorcement tools may need to be used
i companies do not overcome their res-
ervations
On the whole the requirements o Articles
45 and 46 have provided an efficient and
appropriate instrument or collecting and
evaluating existing paediatric studies
55 Clinical trials with
children
It is generally accepted that the Paediatric
Regulation will lead to more clinical trialswith children but that its aims should be
achieved without subjecting children to
unnecessary clinical trials
The youngest paediatric-age subsets
including neonates are particularly sen-
sitive It will be a constant challenge to
balance the therapeutic needs o these
age groups with their specific vulnerability
when considering and deciding on the ap-
propriateness o specific clinical trials or
the specific settings o studies in this age
subset Efforts are thereore continuously
being made to explore alternative means
eg the use o extrapolation modelling
and simulation techniques to reduce the
number o study subjects as much as
possible The Paediatric Committee is ac-
tively contributing to acilitate the devel-
opment and use o such means including
non-conventional trial design
Another challenge is how to avoid dupli-cating trials or different paediatric inves-
tigation plans rom different applicants
Companies embarking on product devel-
opment in similar areas may be required
by the agreed paediatric investigation
plan to conduct studies within similar
settings While collaborative approaches
between companies would be highly de-
sirable and have occurred on rare occa-
sions they ofen conflict with companiesrsquo
understandable reluctance to share datawith competitors in the early stages o
product development and participate in
direct comparisons This situation could
velopment Overall there is however no
evidence that the Regulation has a con-
siderable negative impact on products or
other populations
Rather there are some concerns that the
requirements under the Regulation may
cause delays in the authorisation o prod-ucts with paediatric-only indications as
they bring added complexity to the RampD
and regulatory process or products that
already directly target children The added
value o the submission o a paediatric in-
vestigation plan in these cases will be as-
sessed urther in the 2017 report
54 Reaping the benefits of
existing information
There was widespread speculation prior to
the adoption o the Paediatric Regulation
as to how many studies would be submit-
ted by pharmaceutical companies in ac-
cordance with Articles 45 and 46 The act
that competent authorities received more
than 18 000 studies reveals the consid-
erable amount o paediatric inormation
that existed at company level
Certainly it is true that not all the inor-
mation submitted met modern require-
ments or scientific data and clinical re-
search and that the work-sharing process
o evaluating the inormation is rather
long and resource intensive
Nevertheless compared to the PUMA con-
cept this scheme proved more successul
in terms o output and in recommending
and implementing changes to the sum-
mary o product characteristics o author-
ised products In its public consultationthe Commission called Articles 45 and 46
the lsquohidden gemsrsquo o the Regulation
One drawback that remains however
is reluctance by marketing authorisa-
tion holders to update the summary o
product characteristics on a voluntary
basis This said the Regulation contains
mechanisms to overcome such reluctance
as it empowers competent authorities to
directly update the summary and varythe marketing authorisation accordingly
Moreover in accordance with Article 23
o Directive 200183EC22 and Article 16
o Regulation (EC) No 726200423 mar-
22 Directive 200183EC othe European Parliament and
o the Council o 6 November2001 on the Community
code relating to medicinalproducts or human use OJ L311 28112001 p 67
23 Regulation (EC) No7262004 o the European
Parliament and o the Coun-cil o 31 March 2004 layingdown Community procedures
or the authorisation andsupervision o medicinalproducts or human and
veterinary use and establish-ing a European Medicines
Agency OJ L 136 3042004p 1
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1736
17
lead to competition among companies to
find investigators and study participants
as well as the duplication o trials which
are unnecessary rom a scientific and
ethical point o view
The Paediatric Committee is able to waive
paediatric trial requirements where thespecific medicinal product does not rep-
resent a significant therapeutic benefit
over an existing treatment or paediatric
patients including once the product is au-
thorised (Article 11) However this option
does not provide a way out in the early
stages o product development where
the Committee has to ensure equal treat-
ment and non-discriminatory approaches
The key to avoiding such unnecessary tri-
als is transparency with regard to ongoingand completed trials The situation contin-
ues to be monitored
Finally it is in the interest o the EU that
paediatric trials stemming rom paedi-
atric investigation plans are conducted
within the EU This has less to do with
the standards under which a trial is con-
ducted given that clinical trials carried
out outside the EU have to meet the ethi-
cal and scientific requirements o the EUprovisions on clinical trials24 than with the
act that studies within the EU may pro-
vide patients there with early access to
innovative medicines To date there is in-
sufficient data on the ratio between pae-
diatric trials conducted within and outside
the EU However in view o the upgraded
unctionalities o the EudraCT database it
is expected that more data will be avail-
able in 2017 or the second report
56 Spreading the news mdash
getting new information
to patients and healthcare
professionals
I the Regulation is to be a success it is
not only necessary that data on the use
o a specific product in the paediatric
population are collected but that these
data are then also appropriately commu-
nicated to and used by paediatricians intheir day-to-day work or the benefit o
their patients
In this regard some studies published in
the medical literature suggest a ailure
on the part o practitioners to recognise
the actual amount o off-label prescrib-
ing to children Moreover it is claimed that
the prescribing habits o practitioners are
ofen strongly influenced by personal ex-
perience rather than by evidence-based
inormation or paediatric medicine25
These studies in making generalisations
may not have taken into account the het-
erogeneity o healthcare proessionals
whose receptiveness varies greatly ac-
cording to their work setting and specific
area o specialisation At the same time
such observations may point to a sub-
stantial hurdle in achieving the goal o the
Paediatric Regulation
National competent authorities as well as
organisations or healthcare proessionals
seem particularly qualified to consider ap-
propriate ways o ensuring an adequate
flow o inormation Some Member States
have already established a number o
tools to communicate effectively and e-
ficiently with healthcare proessionals
eg by means o regular meetings web-
based inormation distribution systems ornational ormularies
57 Is the burden greater
than rewards
There can be no doubt that the Paediat-
ric Regulation places a considerable ad-
ditional burden on pharmaceutical com-
panies with its obligations regarding
research on products or use in children
However this approach was adopted be-cause market orces alone proved insu-
ficient to stimulate adequate research
The Regulation requires companies to
submit paediatric investigation plans at
an early stage o product development
However research on some active sub-
stances may be discontinued at later
stages should urther studies ail to show
potential with respect to the saety and
efficacy o the product For every success-
ul authorised medicinal product there aremany that ail to make the finishing line
Hence not all approved paediatric investi-
gation plans will be completed as compa-
24 Directive 200120EC othe European Parliament
and o the Council on theapproximation o the laws
regulations and administra-tive provisions o the Mem-ber States relating to the
implementation o good clini-cal practice in the conducto clinical trials on medicinal
products or human use OJ L121 152001 p 34
25 5-year report to theEuropean Commission (seeootnote 3) page 41
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1836
18
nies may decide to stop the correspond-
ing adult development It is too early still
to obtain reliable statistics that show
the ratio between completed and non-
completed paediatric investigation plans
but in the current context not all approved
plans will eventually result in an approved
medicine with a paediatric indication
In terms o output this entails some un-
necessary effort in compiling and screen-
ing paediatric investigation plans To what
extent this is offset by the benefit o early
submission which ensures that the pae-
diatric development fits smoothly into the
overall product development need ur-
ther monitoring
A urther point o concern is the highnumber o modifications to paediat-
ric investigation plans Figures seem to
suggest that nearly all plans have to
be modified at least once Conceptually
though this does not come as a surprise
in view o the early submission o pae-
diatric investigation plans the length o
adult and paediatric developments and
the substantial deerrals granted An
RampD plan requently has to be adapted
or amended to take account o initial re-sults Recruitment problems or necessary
design changes in the trials may also lead
to modifications While it is acknowledged
that substantial amendments or modifi-
cations to the plan have to be subject to
discussions with the Paediatric Commit-
tee this is less obvious or minor changes
In this context the level o detail required
by the EMA has been repeatedly criticised
In the past five years the EMA and its
Paediatric Committee have made effortsto provide or some flexibility in the plan
so to allow a margin o manoeuvre that
takes account o uncertainties in relation
to certain parameters o a trial
In any case the Commission intends to
review its Communication on the ormat
and content o applications or agree-
ment or modification o a paediatric in-
vestigation plan to take into account the
experience gained including the consider-
able number o modification requests
On a positive note it can be noted that
companies are applying or the rewards
provided by the Regulation primarily the
6-month extension o the Supplementary
Protection Certificate which have been
introduced to offset the additional bur-
den The economic value o the reward
depends on the turnover o the product
concerned In the case o blockbuster
products the amount may be consider-
able while or niche products the effect
is small
An in-depth evaluation o the economic
impact will be included in the 2017 report
in order to draw conclusions on the bal-
ance between burden and rewards and
public health benefits
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1936
19
6Outlook mdash
A fairy-taleending aheadlsquoBetter Medicines or Children mdash From
Concept to Realityrsquo is the title o this re-
port Readers may suggest that based on
the evaluation reerred to above it would
be more appropriate to add a question
mark It is evident that it is too early still
to make a firm statement Despite more
than five years o experience the true im-pact o the Regulation on the health o
children will only become apparent over
time as experience is accumulated in the
longer term
There are encouraging signs though
Paediatric development has become a
more integral part o the overall develop-
ment o medicinal products in the EU A
number o new products with paediatric
indications and age-appropriate pharma-ceutical orms have been authorised and
made available to patients A high num-
ber o agreed paediatric investigation
plans indicates that urther products are
in the pipeline
However it needs to be pointed out that it
would be wrong to expect the Regulation
to be able to solve all problems Instead
it is a major catalyst to improve the situ-
ation o young patients
Finally some weaknesses and deficits
have also become apparent in the last
five years Their impact on the overall
perormance o the Regulation has to be
closely monitored On the basis o the ac-
tions outlined above the Commission in-
tends to fine-tune the current implemen-
tation together with the EMA
Even i better medicines or children are
not yet a reality it should be the ambitiono all stakeholders involved that this piece
o legislation will be or the greater good
o children so that in the 2017 report
the discussion will ocus not on whether a
question mark should be added to the ti-
tle o the report but on whether it should
be an exclamation mark instead
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2036
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2136
21
ANNEXES
Figures and Tables
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2236
22
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2336
23
ANNEX I
Figures and Tables
Table 1Agreed paediatric investigations plans (PIPs) 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Agreed PIPs submitted under Article 7 (without waivers)
Agreed PIPs submitted under Article 8 (without waivers)
Source EMA Paediatric database The numbers on agreed PIPs correspond to EMA decisions
Table 2Agreed paediatric investigations plans (PIPs) compared to ull waivers and modifications 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Submitted modifications of an agreed PIP
Agreed Full waivers
Source EMA Paediatric database The numbers on agreed PIPs and waivers correspond to EMA decisions
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2536
25
Table 5Scientific advice and protocol assistance including ollow-ups (provided by the EMA Scientific Advice Working
Party and the Committee or Human Medicinal Products per year)
259
277321
388 400 433 420
021 32
74 8057
91
0 0 0
68 8067
94
0
100
200
300
400
500
2006 2007 2008 2009 2010 2011 2012
Total number of advice (Scientific Advice and Protocol Assistance)
Sum of paediatric-only and mixed (adult and paediatric development questions)
advice
Paediatric-only or mixed advice that involved a Paediatric Committee member(s) as
expert(s)
Source EMA databases Year o advice letter
Year o start o procedure
Table 6Paediatric clinical trials by year o authorisation
2005 2006 2007 2008 2009 2010 2011 2012
Paediatric trials
(number) 254 316 355 342 404 379 334 332
Paediatric trials
that are part of anagreed PIP 2 1 2 6 16 30 76 76
Proportion of
paediatric trials
that are part of an
agreed PIP among
paediatric trials 1 0 1 2 4 8 23 23
Total number
of trials (adults
and or children) 3 350 3 979 4 749 4 512 4 445 4 026 3 809 3 698
Proportion of
paediatric trials of
all trials 8 8 7 8 9 10 9 9
Source EudraCT Data Warehouse using a predefined query on 6 March 2013 and counting the first authorised trial only in the case o more thanone Member State This partial inormation requires sponsors to use a Clinical Trial Application orm that was only available rom November 2009 or use with version 8 o EudraCT
(available rom 2011)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2636
26
Table 7Number o children to be enrolled in clinical trials
Number
of subjects 2006 2007 2008 2009 2010 2011 2012
Pretermnewborns 0 0 0 207 82 2 281 1 712
Newborns 0 0 5 64 169 1 105 1 172
Infants and
toddlers 330 21 20 59 351 2 788 3 141
Children 2 142 181 200 2 230 2 055 10 325 20 677
Adolescents 368 111 205 1 577 2 861 9 054 13 193
Sum of
above 2 840 313 430 4 137 5 517 25 553 39 895
Reference
number of paediatric
trials 316 355 342 404 379 334 332
Source EudraCT Data Warehouse using a pre-defined query on 6 March 2013 modified by excluding studies or lsquoimmunological medicinal productsrsquo
Table 8EU budget contribution to the Paediatric Regulation and the EMA expenditure
0
1
2
3
4
5
6
7
8
9
10
2006 2007 2008 2009 2010 2011 2012
EU budget contribution (in Million euro)
EMA expenditure for paediatri cs (in Mill ion euro)
EMA expenditure for paediatr ics including support (in Million euro)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2736
27
Table 9Percentage o European Medicines Agencyrsquos human resources working in the paediatric area rom 2006 (inner
circle) to 2012 (outer circle)
733 (2012)
052 (2006)
Table 10Member States acting as rapporteurs or the assessment o studies submitted in accordance with Article 46
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE SE NL FR DK IT BE PL ES NO SK FI IE RO AT HU EL CZ PT LV BG
Study included in worksharing Rapporteur appointed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2836
28
Table 11Member States acting as rapporteur or the assessment o studies submitted in accordance with Article 45
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE NL DK AT FR PL SE ES IE CZ MT IT BE SI EE FI HU NO RO BG EL LV PT IS SK
Wave 1 Wave 2 Wave 3 Wave 4 Wave 5 Wave 6 Wave 7 Wave 8 Wave 9
Wave 10 Wave 11 Wave 12 Wave 13 Wave 14 Wave 15 Wave 16 Wave 17 Wave 18
Table 12Member States acting as rapporteurspeer reviewers in EMArsquos Paediatric Committee procedures (initial PIP
waiver or modification o an agreed PIP)
0
50
100
150
200
250
300
350
400
450
500
A u s t r i a
B el gi um
B ul g a r i a
C y pr u s
C z e c h R e p u b l i c
D enm a r k
E s t oni a
F i nl a n d
F r a n c e
G er m a n y
G r e e c e
H e a l t h c a r e a n d
A c a d emi a
H un g a r y
I c el a n d
I r el a n d
I t a l y
L a t vi a
L i t h u a ni a
L ux em b o ur g
M a l t a
N or w a y
P a t i en t s Or g a ni s a t i on
P ol a n d
P or t u g a l
R om a ni a
S l ov a k i a
S l ov eni a
S p a i n
S w e d en
T h eN e t h er l a n d
s
U ni t e d K i n g d om
Initial PIP applications PIP modifications
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2936
29
ANNEX II
Detailed inventory of centrally authorised medicinalproducts for paediatric use since the entry into force
of the Paediatric Regulation
Table 13Medicinal products authorised centrally since 2007 which include a paediatric indication
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Retapamulin Altargo 2007 No Mixed
Nelarabine Atriance 2007 No Mixed
Human papillomavirus vaccine[types 16 18] Cervarix 2007 No Mixed
Hydroxocobalamin Cyanokit 2007 No Mixed
Idursulase Elaprase 2007 No Mixed
Gadoversetamide Optimark 2007 No Mixed
Betaine anhydrous Cystadane 2007 No Mixed
Stiripentol Diacomit 2007 No Paediatric only
Mecasermin Increlex 2007 No Paediatric only
Rufinamide Inovelon 2007 No Mixed
Hydroxycarbamide Siklos 2007 No Mixed
Human normal
immunoglobulin (ivig) Flebogamma DIF 2007 No Mixed
Fluticasone uroate Avamys 2008 No Mixed
Human normal immunoglobulin Privigen 2008 No Mixed
Lacosamide Vimpat 2008 No Mixed
Micaungin Mycamine 2008 No Mixed
Sapropterin Kuvan 2008 No Mixed
Sugammadex Bridion 2008 No Mixed
Tocoersonal d-alpha
tocopheryl polyethylene glycol
succinate Vedrop 2009 No Paediatric only
Miamurtide Mepact 2009 No Mixed
Rilonacept Rilonacept Regeneron 2009 No Mixed
Tacrolimus Modigra 2009 No Mixed
Pneumoccocal polysaccharideconjugate vaccine (adsorbed) Synflorix 2009 No Paediatric only
Canakinumab
Ilaris (PIP not yet
completed) 2009 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3036
30
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Pneumoccocal polysaccharide
conjugate vaccine (13-valentadsorbed)
Prevenar 13 (PIP not yetcompleted) 2009 Yes Paediatric only
Meningococcal group a c
w135 and y conjugate vaccine Menveo 2010 Yes Mixed
Velaglucerase ala
Vpriv (PIP not yet
completed) 2010 Yes Mixed
Influenza vaccine (live
attenuated nasal) Fluenz (Waiver) 2011 Yes Paediatric only
C1 inhibitor human
Cinryze (PIP not yet
completed) 2011 Yes Mixed
Dihydroartemisinin
piperaquine phosphate
Eurartesim (PIP not yet
completed) 2011 Yes Mixed
Midazolam Buccolam 2011 Yes (PUMA) Paediatric only
EverolimusVotubia(PIP not yet completed) 2011 Yes Mixed
Tobramycin
Tobi Podhaler (PIP not
yet completed) 2011 Yes Mixed
Nomegestrol estradiol Ioa Zoely 2011 Yes Mixed
Colistimethate sodium Colobreathe 2012 Yes Mixed
Mercaptopurine Xaluprine 2012 No Mixed
Catridecacog NovoThirteen 2012 Yes MixedEavirenz Eavirenz Teva 2012 No Mixed
Ivacafor Kalydeco 2012 Yes Mixed
Desloratadine Desloratadine ratiopharm 2012 No Mixed
Desloratadine Desloratadine Actavis 2012 No Mixed
Perampanel Fycompa 2012 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3136
31
Table 14List o centrally authorised medicinal products or which the therapeutic indication was extended to or amend-
ed or the paediatric population
Active substance(s)
Trade
name Date Subject of the extension
Levetiracetam Keppra
2007
2009
Extension o the indication to include adjunctive ther-
apy in the treatment o primary generalised tonic-
clonic (PGTC) seizures in adults and adolescents rom
12 years o age with idiopathic generalised epilepsyExtension o indication to include the adjunctive
treatment o partial seizures with or without second-
ary generalisation in children rom 1 month to lt4
years old
Pneumococcal sac-
charide conjugated
vaccine adsorbed Prevenar 2007
Extension o the indication to include new inorma-
tion on efficacy against disease caused by Strepto-
coccus pneumoniae serotypes 4 6B 9V 14 18C 19F
and 23F in otitis mediaExtension o indication rom active immunisation
against bacteraemic pneumonia to active immunisa-
tion against pneumonia
Infliximab
Remi-
cade 2007
Extension o indication to include treatment o
severe active Crohnrsquos disease in children aged 6 to
17 years
Darbepoetin ala Aranesp 2007
Extension o indication or CRF patients whichrestricted the use o Nespo to paediatric subjects ge
11 years o age
Fosamprenavir Telzir 2007
Extension o indication o Telzir in combination withritonavir or the treatment o Human Immunodefi-
ciency Virus Type 1 (HIV-1) inected adults in combi-nation with other antiretroviral medicinal products to
include paediatric populations
Lamivudine zidovu-
dine Combivir 2007
Extension o indication to include paediatric patients
and replacement o film-coated tablets by scored
film-coated tablets
Desloratadine Aerius 2007Extension o indication rom lsquochronic idiopathic urti-cariarsquo to lsquourticariarsquo
Insulin glulisine Apidra 2007
Extension o indication to include 6 year olds and
older children based on the results o 2 paediatricstudies
Human papilloma virusvaccine [types 6 11
16 18] (recombinantadsorbed) Gardasil 2008
Extension o indication to include the prevention ohigh-grade vaginal dysplastic lesions (VaIN 23)
Adalimumab Humira 20082011
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in adoles-cents rom 13 to 17 years o age
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in the paedi-
atric population aged rom 4 to 12 years
Caspoungin Cancidas 2008
Extension o the indication to include the paediatric
population
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1536
15
52 The PUMA concept a
disappointment
The Paediatric Regulation introduced a
new type o marketing authorisation mdash
the Paediatric Use Marketing Authorisa-
tion (PUMA) As an incentive to carry out
research into the potential paediatric use
o off-patent medicinal products that have
been authorised or adults this marketing
authorisation offers 8 years o data and
10 years o market exclusivity to any new
off-patent product developed exclusively
or use in the paediatric population Thus
the main goal o the PUMA concept is to
stimulate research in existing products
This scheme has been supported by EU
unding through the EU Framework Pro-
grammes or Research and Technological
Development
However to date only one PUMA has been
granted with a ew more projects cur-
rently in the pipeline
Neither industry nor academic networks
have embraced this opportunity as ully
as the Regulation intended It would seem
that the incentive o data and market ex-
clusivity does not work or these productsor at least that the market opportunities
in this sector are currently considered in-
sufficient to outweigh the inherent eco-
nomic risks o pharmaceutical develop-
ment Researchers are not engaging in
trials with medicines that have been on
the market or years Companies seem to
ear that market exclusivity will not pre-
vent physicians rom continuing to use
competitor products with the same active
ingredient off-label at lower costs or thatsubstitution or cheaper adult orms takes
place at the level o pharmacies Moreo-
ver national pricing and reimbursement
rules in Member States ofen do not al-
low or the additional research needed to
obtain the PUMA to be rewarded in price
negotiations20
Against this background the PUMA con-
cept has ailed so ar to ulfil the initial
expectationsThe EMA will in uture accept paediatric
investigation plans or a PUMA that cover
only certain age groups and not the en-
tire paediatric population This may offset
some o the reservations that currently
hamper better endorsement o the PUMA
concept
53 No impact on adultdevelopment
Studies prior to the adoption o the Regu-
lation have suggested a theoretical risk
that the requirements or research in chil-
dren could lengthen the overall drug de-
velopment process21 The Regulation has
met this risk head-on In order to avoid
any delays in authorising medicines or
other populations it allows or the grant-
ing o deerrals relating to the initiation orcompletion o some or all o the meas-
ures contained in a paediatric investiga-
tion plan
Experience shows that the deerral is a
widely used instrument which suggests
that the risk o delays in the processing o
adult applications is minimal There have
been some transitional problems in cases
where the adult programme was already
established when the Regulation enteredinto orce but these issues seem to have
been resolved
A concern that was raised initially was
that some companies would become
reluctant to develop new indications
pharmaceutical orms and new routes o
administration in small markets and or
products with low sales to avoid being
bound by the paediatric obligation under
Article 8 o the Regulation However thereis no evidence o such effect Moreover
it may also be argued that the incentive
o a potential six-month extension o the
SPC served to counterbalance such an
effect as it may have led companies to
examine more thoroughly the benefits o
a line extension taking into account the
economic value o the paediatric reward
Still industry stakeholders claim that
in rare cases the development or new
medicinal products has been delayedor abandoned in the expectation or as a
consequence o additional costs and re-
quirements associated with paediatric de-
20 See the results o thepublic consultation con-
ducted by the Commission inpreparation o this Report
21 C Commission StaffWorking Document Proposal
or a Regulation o the Euro-pean Parliament and o theCouncil on medicinal prod-
ucts or paediatric use andamending Council Regulation(EEC) No 17692 Directive
200183EC and Regula-tion (EC) No 7262004Extended impact assessment
(COM2004599F)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1636
16
keting authorisation holders are obliged
to ensure that the product inormation
is kept up to date with the current scien-
tific knowledge While preerence should
be given to cooperative approaches the
enorcement tools may need to be used
i companies do not overcome their res-
ervations
On the whole the requirements o Articles
45 and 46 have provided an efficient and
appropriate instrument or collecting and
evaluating existing paediatric studies
55 Clinical trials with
children
It is generally accepted that the Paediatric
Regulation will lead to more clinical trialswith children but that its aims should be
achieved without subjecting children to
unnecessary clinical trials
The youngest paediatric-age subsets
including neonates are particularly sen-
sitive It will be a constant challenge to
balance the therapeutic needs o these
age groups with their specific vulnerability
when considering and deciding on the ap-
propriateness o specific clinical trials or
the specific settings o studies in this age
subset Efforts are thereore continuously
being made to explore alternative means
eg the use o extrapolation modelling
and simulation techniques to reduce the
number o study subjects as much as
possible The Paediatric Committee is ac-
tively contributing to acilitate the devel-
opment and use o such means including
non-conventional trial design
Another challenge is how to avoid dupli-cating trials or different paediatric inves-
tigation plans rom different applicants
Companies embarking on product devel-
opment in similar areas may be required
by the agreed paediatric investigation
plan to conduct studies within similar
settings While collaborative approaches
between companies would be highly de-
sirable and have occurred on rare occa-
sions they ofen conflict with companiesrsquo
understandable reluctance to share datawith competitors in the early stages o
product development and participate in
direct comparisons This situation could
velopment Overall there is however no
evidence that the Regulation has a con-
siderable negative impact on products or
other populations
Rather there are some concerns that the
requirements under the Regulation may
cause delays in the authorisation o prod-ucts with paediatric-only indications as
they bring added complexity to the RampD
and regulatory process or products that
already directly target children The added
value o the submission o a paediatric in-
vestigation plan in these cases will be as-
sessed urther in the 2017 report
54 Reaping the benefits of
existing information
There was widespread speculation prior to
the adoption o the Paediatric Regulation
as to how many studies would be submit-
ted by pharmaceutical companies in ac-
cordance with Articles 45 and 46 The act
that competent authorities received more
than 18 000 studies reveals the consid-
erable amount o paediatric inormation
that existed at company level
Certainly it is true that not all the inor-
mation submitted met modern require-
ments or scientific data and clinical re-
search and that the work-sharing process
o evaluating the inormation is rather
long and resource intensive
Nevertheless compared to the PUMA con-
cept this scheme proved more successul
in terms o output and in recommending
and implementing changes to the sum-
mary o product characteristics o author-
ised products In its public consultationthe Commission called Articles 45 and 46
the lsquohidden gemsrsquo o the Regulation
One drawback that remains however
is reluctance by marketing authorisa-
tion holders to update the summary o
product characteristics on a voluntary
basis This said the Regulation contains
mechanisms to overcome such reluctance
as it empowers competent authorities to
directly update the summary and varythe marketing authorisation accordingly
Moreover in accordance with Article 23
o Directive 200183EC22 and Article 16
o Regulation (EC) No 726200423 mar-
22 Directive 200183EC othe European Parliament and
o the Council o 6 November2001 on the Community
code relating to medicinalproducts or human use OJ L311 28112001 p 67
23 Regulation (EC) No7262004 o the European
Parliament and o the Coun-cil o 31 March 2004 layingdown Community procedures
or the authorisation andsupervision o medicinalproducts or human and
veterinary use and establish-ing a European Medicines
Agency OJ L 136 3042004p 1
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1736
17
lead to competition among companies to
find investigators and study participants
as well as the duplication o trials which
are unnecessary rom a scientific and
ethical point o view
The Paediatric Committee is able to waive
paediatric trial requirements where thespecific medicinal product does not rep-
resent a significant therapeutic benefit
over an existing treatment or paediatric
patients including once the product is au-
thorised (Article 11) However this option
does not provide a way out in the early
stages o product development where
the Committee has to ensure equal treat-
ment and non-discriminatory approaches
The key to avoiding such unnecessary tri-
als is transparency with regard to ongoingand completed trials The situation contin-
ues to be monitored
Finally it is in the interest o the EU that
paediatric trials stemming rom paedi-
atric investigation plans are conducted
within the EU This has less to do with
the standards under which a trial is con-
ducted given that clinical trials carried
out outside the EU have to meet the ethi-
cal and scientific requirements o the EUprovisions on clinical trials24 than with the
act that studies within the EU may pro-
vide patients there with early access to
innovative medicines To date there is in-
sufficient data on the ratio between pae-
diatric trials conducted within and outside
the EU However in view o the upgraded
unctionalities o the EudraCT database it
is expected that more data will be avail-
able in 2017 or the second report
56 Spreading the news mdash
getting new information
to patients and healthcare
professionals
I the Regulation is to be a success it is
not only necessary that data on the use
o a specific product in the paediatric
population are collected but that these
data are then also appropriately commu-
nicated to and used by paediatricians intheir day-to-day work or the benefit o
their patients
In this regard some studies published in
the medical literature suggest a ailure
on the part o practitioners to recognise
the actual amount o off-label prescrib-
ing to children Moreover it is claimed that
the prescribing habits o practitioners are
ofen strongly influenced by personal ex-
perience rather than by evidence-based
inormation or paediatric medicine25
These studies in making generalisations
may not have taken into account the het-
erogeneity o healthcare proessionals
whose receptiveness varies greatly ac-
cording to their work setting and specific
area o specialisation At the same time
such observations may point to a sub-
stantial hurdle in achieving the goal o the
Paediatric Regulation
National competent authorities as well as
organisations or healthcare proessionals
seem particularly qualified to consider ap-
propriate ways o ensuring an adequate
flow o inormation Some Member States
have already established a number o
tools to communicate effectively and e-
ficiently with healthcare proessionals
eg by means o regular meetings web-
based inormation distribution systems ornational ormularies
57 Is the burden greater
than rewards
There can be no doubt that the Paediat-
ric Regulation places a considerable ad-
ditional burden on pharmaceutical com-
panies with its obligations regarding
research on products or use in children
However this approach was adopted be-cause market orces alone proved insu-
ficient to stimulate adequate research
The Regulation requires companies to
submit paediatric investigation plans at
an early stage o product development
However research on some active sub-
stances may be discontinued at later
stages should urther studies ail to show
potential with respect to the saety and
efficacy o the product For every success-
ul authorised medicinal product there aremany that ail to make the finishing line
Hence not all approved paediatric investi-
gation plans will be completed as compa-
24 Directive 200120EC othe European Parliament
and o the Council on theapproximation o the laws
regulations and administra-tive provisions o the Mem-ber States relating to the
implementation o good clini-cal practice in the conducto clinical trials on medicinal
products or human use OJ L121 152001 p 34
25 5-year report to theEuropean Commission (seeootnote 3) page 41
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1836
18
nies may decide to stop the correspond-
ing adult development It is too early still
to obtain reliable statistics that show
the ratio between completed and non-
completed paediatric investigation plans
but in the current context not all approved
plans will eventually result in an approved
medicine with a paediatric indication
In terms o output this entails some un-
necessary effort in compiling and screen-
ing paediatric investigation plans To what
extent this is offset by the benefit o early
submission which ensures that the pae-
diatric development fits smoothly into the
overall product development need ur-
ther monitoring
A urther point o concern is the highnumber o modifications to paediat-
ric investigation plans Figures seem to
suggest that nearly all plans have to
be modified at least once Conceptually
though this does not come as a surprise
in view o the early submission o pae-
diatric investigation plans the length o
adult and paediatric developments and
the substantial deerrals granted An
RampD plan requently has to be adapted
or amended to take account o initial re-sults Recruitment problems or necessary
design changes in the trials may also lead
to modifications While it is acknowledged
that substantial amendments or modifi-
cations to the plan have to be subject to
discussions with the Paediatric Commit-
tee this is less obvious or minor changes
In this context the level o detail required
by the EMA has been repeatedly criticised
In the past five years the EMA and its
Paediatric Committee have made effortsto provide or some flexibility in the plan
so to allow a margin o manoeuvre that
takes account o uncertainties in relation
to certain parameters o a trial
In any case the Commission intends to
review its Communication on the ormat
and content o applications or agree-
ment or modification o a paediatric in-
vestigation plan to take into account the
experience gained including the consider-
able number o modification requests
On a positive note it can be noted that
companies are applying or the rewards
provided by the Regulation primarily the
6-month extension o the Supplementary
Protection Certificate which have been
introduced to offset the additional bur-
den The economic value o the reward
depends on the turnover o the product
concerned In the case o blockbuster
products the amount may be consider-
able while or niche products the effect
is small
An in-depth evaluation o the economic
impact will be included in the 2017 report
in order to draw conclusions on the bal-
ance between burden and rewards and
public health benefits
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1936
19
6Outlook mdash
A fairy-taleending aheadlsquoBetter Medicines or Children mdash From
Concept to Realityrsquo is the title o this re-
port Readers may suggest that based on
the evaluation reerred to above it would
be more appropriate to add a question
mark It is evident that it is too early still
to make a firm statement Despite more
than five years o experience the true im-pact o the Regulation on the health o
children will only become apparent over
time as experience is accumulated in the
longer term
There are encouraging signs though
Paediatric development has become a
more integral part o the overall develop-
ment o medicinal products in the EU A
number o new products with paediatric
indications and age-appropriate pharma-ceutical orms have been authorised and
made available to patients A high num-
ber o agreed paediatric investigation
plans indicates that urther products are
in the pipeline
However it needs to be pointed out that it
would be wrong to expect the Regulation
to be able to solve all problems Instead
it is a major catalyst to improve the situ-
ation o young patients
Finally some weaknesses and deficits
have also become apparent in the last
five years Their impact on the overall
perormance o the Regulation has to be
closely monitored On the basis o the ac-
tions outlined above the Commission in-
tends to fine-tune the current implemen-
tation together with the EMA
Even i better medicines or children are
not yet a reality it should be the ambitiono all stakeholders involved that this piece
o legislation will be or the greater good
o children so that in the 2017 report
the discussion will ocus not on whether a
question mark should be added to the ti-
tle o the report but on whether it should
be an exclamation mark instead
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2036
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2136
21
ANNEXES
Figures and Tables
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2236
22
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2336
23
ANNEX I
Figures and Tables
Table 1Agreed paediatric investigations plans (PIPs) 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Agreed PIPs submitted under Article 7 (without waivers)
Agreed PIPs submitted under Article 8 (without waivers)
Source EMA Paediatric database The numbers on agreed PIPs correspond to EMA decisions
Table 2Agreed paediatric investigations plans (PIPs) compared to ull waivers and modifications 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Submitted modifications of an agreed PIP
Agreed Full waivers
Source EMA Paediatric database The numbers on agreed PIPs and waivers correspond to EMA decisions
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2536
25
Table 5Scientific advice and protocol assistance including ollow-ups (provided by the EMA Scientific Advice Working
Party and the Committee or Human Medicinal Products per year)
259
277321
388 400 433 420
021 32
74 8057
91
0 0 0
68 8067
94
0
100
200
300
400
500
2006 2007 2008 2009 2010 2011 2012
Total number of advice (Scientific Advice and Protocol Assistance)
Sum of paediatric-only and mixed (adult and paediatric development questions)
advice
Paediatric-only or mixed advice that involved a Paediatric Committee member(s) as
expert(s)
Source EMA databases Year o advice letter
Year o start o procedure
Table 6Paediatric clinical trials by year o authorisation
2005 2006 2007 2008 2009 2010 2011 2012
Paediatric trials
(number) 254 316 355 342 404 379 334 332
Paediatric trials
that are part of anagreed PIP 2 1 2 6 16 30 76 76
Proportion of
paediatric trials
that are part of an
agreed PIP among
paediatric trials 1 0 1 2 4 8 23 23
Total number
of trials (adults
and or children) 3 350 3 979 4 749 4 512 4 445 4 026 3 809 3 698
Proportion of
paediatric trials of
all trials 8 8 7 8 9 10 9 9
Source EudraCT Data Warehouse using a predefined query on 6 March 2013 and counting the first authorised trial only in the case o more thanone Member State This partial inormation requires sponsors to use a Clinical Trial Application orm that was only available rom November 2009 or use with version 8 o EudraCT
(available rom 2011)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2636
26
Table 7Number o children to be enrolled in clinical trials
Number
of subjects 2006 2007 2008 2009 2010 2011 2012
Pretermnewborns 0 0 0 207 82 2 281 1 712
Newborns 0 0 5 64 169 1 105 1 172
Infants and
toddlers 330 21 20 59 351 2 788 3 141
Children 2 142 181 200 2 230 2 055 10 325 20 677
Adolescents 368 111 205 1 577 2 861 9 054 13 193
Sum of
above 2 840 313 430 4 137 5 517 25 553 39 895
Reference
number of paediatric
trials 316 355 342 404 379 334 332
Source EudraCT Data Warehouse using a pre-defined query on 6 March 2013 modified by excluding studies or lsquoimmunological medicinal productsrsquo
Table 8EU budget contribution to the Paediatric Regulation and the EMA expenditure
0
1
2
3
4
5
6
7
8
9
10
2006 2007 2008 2009 2010 2011 2012
EU budget contribution (in Million euro)
EMA expenditure for paediatri cs (in Mill ion euro)
EMA expenditure for paediatr ics including support (in Million euro)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2736
27
Table 9Percentage o European Medicines Agencyrsquos human resources working in the paediatric area rom 2006 (inner
circle) to 2012 (outer circle)
733 (2012)
052 (2006)
Table 10Member States acting as rapporteurs or the assessment o studies submitted in accordance with Article 46
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE SE NL FR DK IT BE PL ES NO SK FI IE RO AT HU EL CZ PT LV BG
Study included in worksharing Rapporteur appointed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2836
28
Table 11Member States acting as rapporteur or the assessment o studies submitted in accordance with Article 45
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE NL DK AT FR PL SE ES IE CZ MT IT BE SI EE FI HU NO RO BG EL LV PT IS SK
Wave 1 Wave 2 Wave 3 Wave 4 Wave 5 Wave 6 Wave 7 Wave 8 Wave 9
Wave 10 Wave 11 Wave 12 Wave 13 Wave 14 Wave 15 Wave 16 Wave 17 Wave 18
Table 12Member States acting as rapporteurspeer reviewers in EMArsquos Paediatric Committee procedures (initial PIP
waiver or modification o an agreed PIP)
0
50
100
150
200
250
300
350
400
450
500
A u s t r i a
B el gi um
B ul g a r i a
C y pr u s
C z e c h R e p u b l i c
D enm a r k
E s t oni a
F i nl a n d
F r a n c e
G er m a n y
G r e e c e
H e a l t h c a r e a n d
A c a d emi a
H un g a r y
I c el a n d
I r el a n d
I t a l y
L a t vi a
L i t h u a ni a
L ux em b o ur g
M a l t a
N or w a y
P a t i en t s Or g a ni s a t i on
P ol a n d
P or t u g a l
R om a ni a
S l ov a k i a
S l ov eni a
S p a i n
S w e d en
T h eN e t h er l a n d
s
U ni t e d K i n g d om
Initial PIP applications PIP modifications
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2936
29
ANNEX II
Detailed inventory of centrally authorised medicinalproducts for paediatric use since the entry into force
of the Paediatric Regulation
Table 13Medicinal products authorised centrally since 2007 which include a paediatric indication
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Retapamulin Altargo 2007 No Mixed
Nelarabine Atriance 2007 No Mixed
Human papillomavirus vaccine[types 16 18] Cervarix 2007 No Mixed
Hydroxocobalamin Cyanokit 2007 No Mixed
Idursulase Elaprase 2007 No Mixed
Gadoversetamide Optimark 2007 No Mixed
Betaine anhydrous Cystadane 2007 No Mixed
Stiripentol Diacomit 2007 No Paediatric only
Mecasermin Increlex 2007 No Paediatric only
Rufinamide Inovelon 2007 No Mixed
Hydroxycarbamide Siklos 2007 No Mixed
Human normal
immunoglobulin (ivig) Flebogamma DIF 2007 No Mixed
Fluticasone uroate Avamys 2008 No Mixed
Human normal immunoglobulin Privigen 2008 No Mixed
Lacosamide Vimpat 2008 No Mixed
Micaungin Mycamine 2008 No Mixed
Sapropterin Kuvan 2008 No Mixed
Sugammadex Bridion 2008 No Mixed
Tocoersonal d-alpha
tocopheryl polyethylene glycol
succinate Vedrop 2009 No Paediatric only
Miamurtide Mepact 2009 No Mixed
Rilonacept Rilonacept Regeneron 2009 No Mixed
Tacrolimus Modigra 2009 No Mixed
Pneumoccocal polysaccharideconjugate vaccine (adsorbed) Synflorix 2009 No Paediatric only
Canakinumab
Ilaris (PIP not yet
completed) 2009 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3036
30
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Pneumoccocal polysaccharide
conjugate vaccine (13-valentadsorbed)
Prevenar 13 (PIP not yetcompleted) 2009 Yes Paediatric only
Meningococcal group a c
w135 and y conjugate vaccine Menveo 2010 Yes Mixed
Velaglucerase ala
Vpriv (PIP not yet
completed) 2010 Yes Mixed
Influenza vaccine (live
attenuated nasal) Fluenz (Waiver) 2011 Yes Paediatric only
C1 inhibitor human
Cinryze (PIP not yet
completed) 2011 Yes Mixed
Dihydroartemisinin
piperaquine phosphate
Eurartesim (PIP not yet
completed) 2011 Yes Mixed
Midazolam Buccolam 2011 Yes (PUMA) Paediatric only
EverolimusVotubia(PIP not yet completed) 2011 Yes Mixed
Tobramycin
Tobi Podhaler (PIP not
yet completed) 2011 Yes Mixed
Nomegestrol estradiol Ioa Zoely 2011 Yes Mixed
Colistimethate sodium Colobreathe 2012 Yes Mixed
Mercaptopurine Xaluprine 2012 No Mixed
Catridecacog NovoThirteen 2012 Yes MixedEavirenz Eavirenz Teva 2012 No Mixed
Ivacafor Kalydeco 2012 Yes Mixed
Desloratadine Desloratadine ratiopharm 2012 No Mixed
Desloratadine Desloratadine Actavis 2012 No Mixed
Perampanel Fycompa 2012 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3136
31
Table 14List o centrally authorised medicinal products or which the therapeutic indication was extended to or amend-
ed or the paediatric population
Active substance(s)
Trade
name Date Subject of the extension
Levetiracetam Keppra
2007
2009
Extension o the indication to include adjunctive ther-
apy in the treatment o primary generalised tonic-
clonic (PGTC) seizures in adults and adolescents rom
12 years o age with idiopathic generalised epilepsyExtension o indication to include the adjunctive
treatment o partial seizures with or without second-
ary generalisation in children rom 1 month to lt4
years old
Pneumococcal sac-
charide conjugated
vaccine adsorbed Prevenar 2007
Extension o the indication to include new inorma-
tion on efficacy against disease caused by Strepto-
coccus pneumoniae serotypes 4 6B 9V 14 18C 19F
and 23F in otitis mediaExtension o indication rom active immunisation
against bacteraemic pneumonia to active immunisa-
tion against pneumonia
Infliximab
Remi-
cade 2007
Extension o indication to include treatment o
severe active Crohnrsquos disease in children aged 6 to
17 years
Darbepoetin ala Aranesp 2007
Extension o indication or CRF patients whichrestricted the use o Nespo to paediatric subjects ge
11 years o age
Fosamprenavir Telzir 2007
Extension o indication o Telzir in combination withritonavir or the treatment o Human Immunodefi-
ciency Virus Type 1 (HIV-1) inected adults in combi-nation with other antiretroviral medicinal products to
include paediatric populations
Lamivudine zidovu-
dine Combivir 2007
Extension o indication to include paediatric patients
and replacement o film-coated tablets by scored
film-coated tablets
Desloratadine Aerius 2007Extension o indication rom lsquochronic idiopathic urti-cariarsquo to lsquourticariarsquo
Insulin glulisine Apidra 2007
Extension o indication to include 6 year olds and
older children based on the results o 2 paediatricstudies
Human papilloma virusvaccine [types 6 11
16 18] (recombinantadsorbed) Gardasil 2008
Extension o indication to include the prevention ohigh-grade vaginal dysplastic lesions (VaIN 23)
Adalimumab Humira 20082011
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in adoles-cents rom 13 to 17 years o age
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in the paedi-
atric population aged rom 4 to 12 years
Caspoungin Cancidas 2008
Extension o the indication to include the paediatric
population
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1636
16
keting authorisation holders are obliged
to ensure that the product inormation
is kept up to date with the current scien-
tific knowledge While preerence should
be given to cooperative approaches the
enorcement tools may need to be used
i companies do not overcome their res-
ervations
On the whole the requirements o Articles
45 and 46 have provided an efficient and
appropriate instrument or collecting and
evaluating existing paediatric studies
55 Clinical trials with
children
It is generally accepted that the Paediatric
Regulation will lead to more clinical trialswith children but that its aims should be
achieved without subjecting children to
unnecessary clinical trials
The youngest paediatric-age subsets
including neonates are particularly sen-
sitive It will be a constant challenge to
balance the therapeutic needs o these
age groups with their specific vulnerability
when considering and deciding on the ap-
propriateness o specific clinical trials or
the specific settings o studies in this age
subset Efforts are thereore continuously
being made to explore alternative means
eg the use o extrapolation modelling
and simulation techniques to reduce the
number o study subjects as much as
possible The Paediatric Committee is ac-
tively contributing to acilitate the devel-
opment and use o such means including
non-conventional trial design
Another challenge is how to avoid dupli-cating trials or different paediatric inves-
tigation plans rom different applicants
Companies embarking on product devel-
opment in similar areas may be required
by the agreed paediatric investigation
plan to conduct studies within similar
settings While collaborative approaches
between companies would be highly de-
sirable and have occurred on rare occa-
sions they ofen conflict with companiesrsquo
understandable reluctance to share datawith competitors in the early stages o
product development and participate in
direct comparisons This situation could
velopment Overall there is however no
evidence that the Regulation has a con-
siderable negative impact on products or
other populations
Rather there are some concerns that the
requirements under the Regulation may
cause delays in the authorisation o prod-ucts with paediatric-only indications as
they bring added complexity to the RampD
and regulatory process or products that
already directly target children The added
value o the submission o a paediatric in-
vestigation plan in these cases will be as-
sessed urther in the 2017 report
54 Reaping the benefits of
existing information
There was widespread speculation prior to
the adoption o the Paediatric Regulation
as to how many studies would be submit-
ted by pharmaceutical companies in ac-
cordance with Articles 45 and 46 The act
that competent authorities received more
than 18 000 studies reveals the consid-
erable amount o paediatric inormation
that existed at company level
Certainly it is true that not all the inor-
mation submitted met modern require-
ments or scientific data and clinical re-
search and that the work-sharing process
o evaluating the inormation is rather
long and resource intensive
Nevertheless compared to the PUMA con-
cept this scheme proved more successul
in terms o output and in recommending
and implementing changes to the sum-
mary o product characteristics o author-
ised products In its public consultationthe Commission called Articles 45 and 46
the lsquohidden gemsrsquo o the Regulation
One drawback that remains however
is reluctance by marketing authorisa-
tion holders to update the summary o
product characteristics on a voluntary
basis This said the Regulation contains
mechanisms to overcome such reluctance
as it empowers competent authorities to
directly update the summary and varythe marketing authorisation accordingly
Moreover in accordance with Article 23
o Directive 200183EC22 and Article 16
o Regulation (EC) No 726200423 mar-
22 Directive 200183EC othe European Parliament and
o the Council o 6 November2001 on the Community
code relating to medicinalproducts or human use OJ L311 28112001 p 67
23 Regulation (EC) No7262004 o the European
Parliament and o the Coun-cil o 31 March 2004 layingdown Community procedures
or the authorisation andsupervision o medicinalproducts or human and
veterinary use and establish-ing a European Medicines
Agency OJ L 136 3042004p 1
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1736
17
lead to competition among companies to
find investigators and study participants
as well as the duplication o trials which
are unnecessary rom a scientific and
ethical point o view
The Paediatric Committee is able to waive
paediatric trial requirements where thespecific medicinal product does not rep-
resent a significant therapeutic benefit
over an existing treatment or paediatric
patients including once the product is au-
thorised (Article 11) However this option
does not provide a way out in the early
stages o product development where
the Committee has to ensure equal treat-
ment and non-discriminatory approaches
The key to avoiding such unnecessary tri-
als is transparency with regard to ongoingand completed trials The situation contin-
ues to be monitored
Finally it is in the interest o the EU that
paediatric trials stemming rom paedi-
atric investigation plans are conducted
within the EU This has less to do with
the standards under which a trial is con-
ducted given that clinical trials carried
out outside the EU have to meet the ethi-
cal and scientific requirements o the EUprovisions on clinical trials24 than with the
act that studies within the EU may pro-
vide patients there with early access to
innovative medicines To date there is in-
sufficient data on the ratio between pae-
diatric trials conducted within and outside
the EU However in view o the upgraded
unctionalities o the EudraCT database it
is expected that more data will be avail-
able in 2017 or the second report
56 Spreading the news mdash
getting new information
to patients and healthcare
professionals
I the Regulation is to be a success it is
not only necessary that data on the use
o a specific product in the paediatric
population are collected but that these
data are then also appropriately commu-
nicated to and used by paediatricians intheir day-to-day work or the benefit o
their patients
In this regard some studies published in
the medical literature suggest a ailure
on the part o practitioners to recognise
the actual amount o off-label prescrib-
ing to children Moreover it is claimed that
the prescribing habits o practitioners are
ofen strongly influenced by personal ex-
perience rather than by evidence-based
inormation or paediatric medicine25
These studies in making generalisations
may not have taken into account the het-
erogeneity o healthcare proessionals
whose receptiveness varies greatly ac-
cording to their work setting and specific
area o specialisation At the same time
such observations may point to a sub-
stantial hurdle in achieving the goal o the
Paediatric Regulation
National competent authorities as well as
organisations or healthcare proessionals
seem particularly qualified to consider ap-
propriate ways o ensuring an adequate
flow o inormation Some Member States
have already established a number o
tools to communicate effectively and e-
ficiently with healthcare proessionals
eg by means o regular meetings web-
based inormation distribution systems ornational ormularies
57 Is the burden greater
than rewards
There can be no doubt that the Paediat-
ric Regulation places a considerable ad-
ditional burden on pharmaceutical com-
panies with its obligations regarding
research on products or use in children
However this approach was adopted be-cause market orces alone proved insu-
ficient to stimulate adequate research
The Regulation requires companies to
submit paediatric investigation plans at
an early stage o product development
However research on some active sub-
stances may be discontinued at later
stages should urther studies ail to show
potential with respect to the saety and
efficacy o the product For every success-
ul authorised medicinal product there aremany that ail to make the finishing line
Hence not all approved paediatric investi-
gation plans will be completed as compa-
24 Directive 200120EC othe European Parliament
and o the Council on theapproximation o the laws
regulations and administra-tive provisions o the Mem-ber States relating to the
implementation o good clini-cal practice in the conducto clinical trials on medicinal
products or human use OJ L121 152001 p 34
25 5-year report to theEuropean Commission (seeootnote 3) page 41
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1836
18
nies may decide to stop the correspond-
ing adult development It is too early still
to obtain reliable statistics that show
the ratio between completed and non-
completed paediatric investigation plans
but in the current context not all approved
plans will eventually result in an approved
medicine with a paediatric indication
In terms o output this entails some un-
necessary effort in compiling and screen-
ing paediatric investigation plans To what
extent this is offset by the benefit o early
submission which ensures that the pae-
diatric development fits smoothly into the
overall product development need ur-
ther monitoring
A urther point o concern is the highnumber o modifications to paediat-
ric investigation plans Figures seem to
suggest that nearly all plans have to
be modified at least once Conceptually
though this does not come as a surprise
in view o the early submission o pae-
diatric investigation plans the length o
adult and paediatric developments and
the substantial deerrals granted An
RampD plan requently has to be adapted
or amended to take account o initial re-sults Recruitment problems or necessary
design changes in the trials may also lead
to modifications While it is acknowledged
that substantial amendments or modifi-
cations to the plan have to be subject to
discussions with the Paediatric Commit-
tee this is less obvious or minor changes
In this context the level o detail required
by the EMA has been repeatedly criticised
In the past five years the EMA and its
Paediatric Committee have made effortsto provide or some flexibility in the plan
so to allow a margin o manoeuvre that
takes account o uncertainties in relation
to certain parameters o a trial
In any case the Commission intends to
review its Communication on the ormat
and content o applications or agree-
ment or modification o a paediatric in-
vestigation plan to take into account the
experience gained including the consider-
able number o modification requests
On a positive note it can be noted that
companies are applying or the rewards
provided by the Regulation primarily the
6-month extension o the Supplementary
Protection Certificate which have been
introduced to offset the additional bur-
den The economic value o the reward
depends on the turnover o the product
concerned In the case o blockbuster
products the amount may be consider-
able while or niche products the effect
is small
An in-depth evaluation o the economic
impact will be included in the 2017 report
in order to draw conclusions on the bal-
ance between burden and rewards and
public health benefits
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1936
19
6Outlook mdash
A fairy-taleending aheadlsquoBetter Medicines or Children mdash From
Concept to Realityrsquo is the title o this re-
port Readers may suggest that based on
the evaluation reerred to above it would
be more appropriate to add a question
mark It is evident that it is too early still
to make a firm statement Despite more
than five years o experience the true im-pact o the Regulation on the health o
children will only become apparent over
time as experience is accumulated in the
longer term
There are encouraging signs though
Paediatric development has become a
more integral part o the overall develop-
ment o medicinal products in the EU A
number o new products with paediatric
indications and age-appropriate pharma-ceutical orms have been authorised and
made available to patients A high num-
ber o agreed paediatric investigation
plans indicates that urther products are
in the pipeline
However it needs to be pointed out that it
would be wrong to expect the Regulation
to be able to solve all problems Instead
it is a major catalyst to improve the situ-
ation o young patients
Finally some weaknesses and deficits
have also become apparent in the last
five years Their impact on the overall
perormance o the Regulation has to be
closely monitored On the basis o the ac-
tions outlined above the Commission in-
tends to fine-tune the current implemen-
tation together with the EMA
Even i better medicines or children are
not yet a reality it should be the ambitiono all stakeholders involved that this piece
o legislation will be or the greater good
o children so that in the 2017 report
the discussion will ocus not on whether a
question mark should be added to the ti-
tle o the report but on whether it should
be an exclamation mark instead
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2036
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2136
21
ANNEXES
Figures and Tables
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2236
22
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2336
23
ANNEX I
Figures and Tables
Table 1Agreed paediatric investigations plans (PIPs) 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Agreed PIPs submitted under Article 7 (without waivers)
Agreed PIPs submitted under Article 8 (without waivers)
Source EMA Paediatric database The numbers on agreed PIPs correspond to EMA decisions
Table 2Agreed paediatric investigations plans (PIPs) compared to ull waivers and modifications 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Submitted modifications of an agreed PIP
Agreed Full waivers
Source EMA Paediatric database The numbers on agreed PIPs and waivers correspond to EMA decisions
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2536
25
Table 5Scientific advice and protocol assistance including ollow-ups (provided by the EMA Scientific Advice Working
Party and the Committee or Human Medicinal Products per year)
259
277321
388 400 433 420
021 32
74 8057
91
0 0 0
68 8067
94
0
100
200
300
400
500
2006 2007 2008 2009 2010 2011 2012
Total number of advice (Scientific Advice and Protocol Assistance)
Sum of paediatric-only and mixed (adult and paediatric development questions)
advice
Paediatric-only or mixed advice that involved a Paediatric Committee member(s) as
expert(s)
Source EMA databases Year o advice letter
Year o start o procedure
Table 6Paediatric clinical trials by year o authorisation
2005 2006 2007 2008 2009 2010 2011 2012
Paediatric trials
(number) 254 316 355 342 404 379 334 332
Paediatric trials
that are part of anagreed PIP 2 1 2 6 16 30 76 76
Proportion of
paediatric trials
that are part of an
agreed PIP among
paediatric trials 1 0 1 2 4 8 23 23
Total number
of trials (adults
and or children) 3 350 3 979 4 749 4 512 4 445 4 026 3 809 3 698
Proportion of
paediatric trials of
all trials 8 8 7 8 9 10 9 9
Source EudraCT Data Warehouse using a predefined query on 6 March 2013 and counting the first authorised trial only in the case o more thanone Member State This partial inormation requires sponsors to use a Clinical Trial Application orm that was only available rom November 2009 or use with version 8 o EudraCT
(available rom 2011)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2636
26
Table 7Number o children to be enrolled in clinical trials
Number
of subjects 2006 2007 2008 2009 2010 2011 2012
Pretermnewborns 0 0 0 207 82 2 281 1 712
Newborns 0 0 5 64 169 1 105 1 172
Infants and
toddlers 330 21 20 59 351 2 788 3 141
Children 2 142 181 200 2 230 2 055 10 325 20 677
Adolescents 368 111 205 1 577 2 861 9 054 13 193
Sum of
above 2 840 313 430 4 137 5 517 25 553 39 895
Reference
number of paediatric
trials 316 355 342 404 379 334 332
Source EudraCT Data Warehouse using a pre-defined query on 6 March 2013 modified by excluding studies or lsquoimmunological medicinal productsrsquo
Table 8EU budget contribution to the Paediatric Regulation and the EMA expenditure
0
1
2
3
4
5
6
7
8
9
10
2006 2007 2008 2009 2010 2011 2012
EU budget contribution (in Million euro)
EMA expenditure for paediatri cs (in Mill ion euro)
EMA expenditure for paediatr ics including support (in Million euro)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2736
27
Table 9Percentage o European Medicines Agencyrsquos human resources working in the paediatric area rom 2006 (inner
circle) to 2012 (outer circle)
733 (2012)
052 (2006)
Table 10Member States acting as rapporteurs or the assessment o studies submitted in accordance with Article 46
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE SE NL FR DK IT BE PL ES NO SK FI IE RO AT HU EL CZ PT LV BG
Study included in worksharing Rapporteur appointed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2836
28
Table 11Member States acting as rapporteur or the assessment o studies submitted in accordance with Article 45
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE NL DK AT FR PL SE ES IE CZ MT IT BE SI EE FI HU NO RO BG EL LV PT IS SK
Wave 1 Wave 2 Wave 3 Wave 4 Wave 5 Wave 6 Wave 7 Wave 8 Wave 9
Wave 10 Wave 11 Wave 12 Wave 13 Wave 14 Wave 15 Wave 16 Wave 17 Wave 18
Table 12Member States acting as rapporteurspeer reviewers in EMArsquos Paediatric Committee procedures (initial PIP
waiver or modification o an agreed PIP)
0
50
100
150
200
250
300
350
400
450
500
A u s t r i a
B el gi um
B ul g a r i a
C y pr u s
C z e c h R e p u b l i c
D enm a r k
E s t oni a
F i nl a n d
F r a n c e
G er m a n y
G r e e c e
H e a l t h c a r e a n d
A c a d emi a
H un g a r y
I c el a n d
I r el a n d
I t a l y
L a t vi a
L i t h u a ni a
L ux em b o ur g
M a l t a
N or w a y
P a t i en t s Or g a ni s a t i on
P ol a n d
P or t u g a l
R om a ni a
S l ov a k i a
S l ov eni a
S p a i n
S w e d en
T h eN e t h er l a n d
s
U ni t e d K i n g d om
Initial PIP applications PIP modifications
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2936
29
ANNEX II
Detailed inventory of centrally authorised medicinalproducts for paediatric use since the entry into force
of the Paediatric Regulation
Table 13Medicinal products authorised centrally since 2007 which include a paediatric indication
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Retapamulin Altargo 2007 No Mixed
Nelarabine Atriance 2007 No Mixed
Human papillomavirus vaccine[types 16 18] Cervarix 2007 No Mixed
Hydroxocobalamin Cyanokit 2007 No Mixed
Idursulase Elaprase 2007 No Mixed
Gadoversetamide Optimark 2007 No Mixed
Betaine anhydrous Cystadane 2007 No Mixed
Stiripentol Diacomit 2007 No Paediatric only
Mecasermin Increlex 2007 No Paediatric only
Rufinamide Inovelon 2007 No Mixed
Hydroxycarbamide Siklos 2007 No Mixed
Human normal
immunoglobulin (ivig) Flebogamma DIF 2007 No Mixed
Fluticasone uroate Avamys 2008 No Mixed
Human normal immunoglobulin Privigen 2008 No Mixed
Lacosamide Vimpat 2008 No Mixed
Micaungin Mycamine 2008 No Mixed
Sapropterin Kuvan 2008 No Mixed
Sugammadex Bridion 2008 No Mixed
Tocoersonal d-alpha
tocopheryl polyethylene glycol
succinate Vedrop 2009 No Paediatric only
Miamurtide Mepact 2009 No Mixed
Rilonacept Rilonacept Regeneron 2009 No Mixed
Tacrolimus Modigra 2009 No Mixed
Pneumoccocal polysaccharideconjugate vaccine (adsorbed) Synflorix 2009 No Paediatric only
Canakinumab
Ilaris (PIP not yet
completed) 2009 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3036
30
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Pneumoccocal polysaccharide
conjugate vaccine (13-valentadsorbed)
Prevenar 13 (PIP not yetcompleted) 2009 Yes Paediatric only
Meningococcal group a c
w135 and y conjugate vaccine Menveo 2010 Yes Mixed
Velaglucerase ala
Vpriv (PIP not yet
completed) 2010 Yes Mixed
Influenza vaccine (live
attenuated nasal) Fluenz (Waiver) 2011 Yes Paediatric only
C1 inhibitor human
Cinryze (PIP not yet
completed) 2011 Yes Mixed
Dihydroartemisinin
piperaquine phosphate
Eurartesim (PIP not yet
completed) 2011 Yes Mixed
Midazolam Buccolam 2011 Yes (PUMA) Paediatric only
EverolimusVotubia(PIP not yet completed) 2011 Yes Mixed
Tobramycin
Tobi Podhaler (PIP not
yet completed) 2011 Yes Mixed
Nomegestrol estradiol Ioa Zoely 2011 Yes Mixed
Colistimethate sodium Colobreathe 2012 Yes Mixed
Mercaptopurine Xaluprine 2012 No Mixed
Catridecacog NovoThirteen 2012 Yes MixedEavirenz Eavirenz Teva 2012 No Mixed
Ivacafor Kalydeco 2012 Yes Mixed
Desloratadine Desloratadine ratiopharm 2012 No Mixed
Desloratadine Desloratadine Actavis 2012 No Mixed
Perampanel Fycompa 2012 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3136
31
Table 14List o centrally authorised medicinal products or which the therapeutic indication was extended to or amend-
ed or the paediatric population
Active substance(s)
Trade
name Date Subject of the extension
Levetiracetam Keppra
2007
2009
Extension o the indication to include adjunctive ther-
apy in the treatment o primary generalised tonic-
clonic (PGTC) seizures in adults and adolescents rom
12 years o age with idiopathic generalised epilepsyExtension o indication to include the adjunctive
treatment o partial seizures with or without second-
ary generalisation in children rom 1 month to lt4
years old
Pneumococcal sac-
charide conjugated
vaccine adsorbed Prevenar 2007
Extension o the indication to include new inorma-
tion on efficacy against disease caused by Strepto-
coccus pneumoniae serotypes 4 6B 9V 14 18C 19F
and 23F in otitis mediaExtension o indication rom active immunisation
against bacteraemic pneumonia to active immunisa-
tion against pneumonia
Infliximab
Remi-
cade 2007
Extension o indication to include treatment o
severe active Crohnrsquos disease in children aged 6 to
17 years
Darbepoetin ala Aranesp 2007
Extension o indication or CRF patients whichrestricted the use o Nespo to paediatric subjects ge
11 years o age
Fosamprenavir Telzir 2007
Extension o indication o Telzir in combination withritonavir or the treatment o Human Immunodefi-
ciency Virus Type 1 (HIV-1) inected adults in combi-nation with other antiretroviral medicinal products to
include paediatric populations
Lamivudine zidovu-
dine Combivir 2007
Extension o indication to include paediatric patients
and replacement o film-coated tablets by scored
film-coated tablets
Desloratadine Aerius 2007Extension o indication rom lsquochronic idiopathic urti-cariarsquo to lsquourticariarsquo
Insulin glulisine Apidra 2007
Extension o indication to include 6 year olds and
older children based on the results o 2 paediatricstudies
Human papilloma virusvaccine [types 6 11
16 18] (recombinantadsorbed) Gardasil 2008
Extension o indication to include the prevention ohigh-grade vaginal dysplastic lesions (VaIN 23)
Adalimumab Humira 20082011
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in adoles-cents rom 13 to 17 years o age
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in the paedi-
atric population aged rom 4 to 12 years
Caspoungin Cancidas 2008
Extension o the indication to include the paediatric
population
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1736
17
lead to competition among companies to
find investigators and study participants
as well as the duplication o trials which
are unnecessary rom a scientific and
ethical point o view
The Paediatric Committee is able to waive
paediatric trial requirements where thespecific medicinal product does not rep-
resent a significant therapeutic benefit
over an existing treatment or paediatric
patients including once the product is au-
thorised (Article 11) However this option
does not provide a way out in the early
stages o product development where
the Committee has to ensure equal treat-
ment and non-discriminatory approaches
The key to avoiding such unnecessary tri-
als is transparency with regard to ongoingand completed trials The situation contin-
ues to be monitored
Finally it is in the interest o the EU that
paediatric trials stemming rom paedi-
atric investigation plans are conducted
within the EU This has less to do with
the standards under which a trial is con-
ducted given that clinical trials carried
out outside the EU have to meet the ethi-
cal and scientific requirements o the EUprovisions on clinical trials24 than with the
act that studies within the EU may pro-
vide patients there with early access to
innovative medicines To date there is in-
sufficient data on the ratio between pae-
diatric trials conducted within and outside
the EU However in view o the upgraded
unctionalities o the EudraCT database it
is expected that more data will be avail-
able in 2017 or the second report
56 Spreading the news mdash
getting new information
to patients and healthcare
professionals
I the Regulation is to be a success it is
not only necessary that data on the use
o a specific product in the paediatric
population are collected but that these
data are then also appropriately commu-
nicated to and used by paediatricians intheir day-to-day work or the benefit o
their patients
In this regard some studies published in
the medical literature suggest a ailure
on the part o practitioners to recognise
the actual amount o off-label prescrib-
ing to children Moreover it is claimed that
the prescribing habits o practitioners are
ofen strongly influenced by personal ex-
perience rather than by evidence-based
inormation or paediatric medicine25
These studies in making generalisations
may not have taken into account the het-
erogeneity o healthcare proessionals
whose receptiveness varies greatly ac-
cording to their work setting and specific
area o specialisation At the same time
such observations may point to a sub-
stantial hurdle in achieving the goal o the
Paediatric Regulation
National competent authorities as well as
organisations or healthcare proessionals
seem particularly qualified to consider ap-
propriate ways o ensuring an adequate
flow o inormation Some Member States
have already established a number o
tools to communicate effectively and e-
ficiently with healthcare proessionals
eg by means o regular meetings web-
based inormation distribution systems ornational ormularies
57 Is the burden greater
than rewards
There can be no doubt that the Paediat-
ric Regulation places a considerable ad-
ditional burden on pharmaceutical com-
panies with its obligations regarding
research on products or use in children
However this approach was adopted be-cause market orces alone proved insu-
ficient to stimulate adequate research
The Regulation requires companies to
submit paediatric investigation plans at
an early stage o product development
However research on some active sub-
stances may be discontinued at later
stages should urther studies ail to show
potential with respect to the saety and
efficacy o the product For every success-
ul authorised medicinal product there aremany that ail to make the finishing line
Hence not all approved paediatric investi-
gation plans will be completed as compa-
24 Directive 200120EC othe European Parliament
and o the Council on theapproximation o the laws
regulations and administra-tive provisions o the Mem-ber States relating to the
implementation o good clini-cal practice in the conducto clinical trials on medicinal
products or human use OJ L121 152001 p 34
25 5-year report to theEuropean Commission (seeootnote 3) page 41
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1836
18
nies may decide to stop the correspond-
ing adult development It is too early still
to obtain reliable statistics that show
the ratio between completed and non-
completed paediatric investigation plans
but in the current context not all approved
plans will eventually result in an approved
medicine with a paediatric indication
In terms o output this entails some un-
necessary effort in compiling and screen-
ing paediatric investigation plans To what
extent this is offset by the benefit o early
submission which ensures that the pae-
diatric development fits smoothly into the
overall product development need ur-
ther monitoring
A urther point o concern is the highnumber o modifications to paediat-
ric investigation plans Figures seem to
suggest that nearly all plans have to
be modified at least once Conceptually
though this does not come as a surprise
in view o the early submission o pae-
diatric investigation plans the length o
adult and paediatric developments and
the substantial deerrals granted An
RampD plan requently has to be adapted
or amended to take account o initial re-sults Recruitment problems or necessary
design changes in the trials may also lead
to modifications While it is acknowledged
that substantial amendments or modifi-
cations to the plan have to be subject to
discussions with the Paediatric Commit-
tee this is less obvious or minor changes
In this context the level o detail required
by the EMA has been repeatedly criticised
In the past five years the EMA and its
Paediatric Committee have made effortsto provide or some flexibility in the plan
so to allow a margin o manoeuvre that
takes account o uncertainties in relation
to certain parameters o a trial
In any case the Commission intends to
review its Communication on the ormat
and content o applications or agree-
ment or modification o a paediatric in-
vestigation plan to take into account the
experience gained including the consider-
able number o modification requests
On a positive note it can be noted that
companies are applying or the rewards
provided by the Regulation primarily the
6-month extension o the Supplementary
Protection Certificate which have been
introduced to offset the additional bur-
den The economic value o the reward
depends on the turnover o the product
concerned In the case o blockbuster
products the amount may be consider-
able while or niche products the effect
is small
An in-depth evaluation o the economic
impact will be included in the 2017 report
in order to draw conclusions on the bal-
ance between burden and rewards and
public health benefits
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1936
19
6Outlook mdash
A fairy-taleending aheadlsquoBetter Medicines or Children mdash From
Concept to Realityrsquo is the title o this re-
port Readers may suggest that based on
the evaluation reerred to above it would
be more appropriate to add a question
mark It is evident that it is too early still
to make a firm statement Despite more
than five years o experience the true im-pact o the Regulation on the health o
children will only become apparent over
time as experience is accumulated in the
longer term
There are encouraging signs though
Paediatric development has become a
more integral part o the overall develop-
ment o medicinal products in the EU A
number o new products with paediatric
indications and age-appropriate pharma-ceutical orms have been authorised and
made available to patients A high num-
ber o agreed paediatric investigation
plans indicates that urther products are
in the pipeline
However it needs to be pointed out that it
would be wrong to expect the Regulation
to be able to solve all problems Instead
it is a major catalyst to improve the situ-
ation o young patients
Finally some weaknesses and deficits
have also become apparent in the last
five years Their impact on the overall
perormance o the Regulation has to be
closely monitored On the basis o the ac-
tions outlined above the Commission in-
tends to fine-tune the current implemen-
tation together with the EMA
Even i better medicines or children are
not yet a reality it should be the ambitiono all stakeholders involved that this piece
o legislation will be or the greater good
o children so that in the 2017 report
the discussion will ocus not on whether a
question mark should be added to the ti-
tle o the report but on whether it should
be an exclamation mark instead
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2036
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2136
21
ANNEXES
Figures and Tables
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2236
22
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2336
23
ANNEX I
Figures and Tables
Table 1Agreed paediatric investigations plans (PIPs) 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Agreed PIPs submitted under Article 7 (without waivers)
Agreed PIPs submitted under Article 8 (without waivers)
Source EMA Paediatric database The numbers on agreed PIPs correspond to EMA decisions
Table 2Agreed paediatric investigations plans (PIPs) compared to ull waivers and modifications 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Submitted modifications of an agreed PIP
Agreed Full waivers
Source EMA Paediatric database The numbers on agreed PIPs and waivers correspond to EMA decisions
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2536
25
Table 5Scientific advice and protocol assistance including ollow-ups (provided by the EMA Scientific Advice Working
Party and the Committee or Human Medicinal Products per year)
259
277321
388 400 433 420
021 32
74 8057
91
0 0 0
68 8067
94
0
100
200
300
400
500
2006 2007 2008 2009 2010 2011 2012
Total number of advice (Scientific Advice and Protocol Assistance)
Sum of paediatric-only and mixed (adult and paediatric development questions)
advice
Paediatric-only or mixed advice that involved a Paediatric Committee member(s) as
expert(s)
Source EMA databases Year o advice letter
Year o start o procedure
Table 6Paediatric clinical trials by year o authorisation
2005 2006 2007 2008 2009 2010 2011 2012
Paediatric trials
(number) 254 316 355 342 404 379 334 332
Paediatric trials
that are part of anagreed PIP 2 1 2 6 16 30 76 76
Proportion of
paediatric trials
that are part of an
agreed PIP among
paediatric trials 1 0 1 2 4 8 23 23
Total number
of trials (adults
and or children) 3 350 3 979 4 749 4 512 4 445 4 026 3 809 3 698
Proportion of
paediatric trials of
all trials 8 8 7 8 9 10 9 9
Source EudraCT Data Warehouse using a predefined query on 6 March 2013 and counting the first authorised trial only in the case o more thanone Member State This partial inormation requires sponsors to use a Clinical Trial Application orm that was only available rom November 2009 or use with version 8 o EudraCT
(available rom 2011)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2636
26
Table 7Number o children to be enrolled in clinical trials
Number
of subjects 2006 2007 2008 2009 2010 2011 2012
Pretermnewborns 0 0 0 207 82 2 281 1 712
Newborns 0 0 5 64 169 1 105 1 172
Infants and
toddlers 330 21 20 59 351 2 788 3 141
Children 2 142 181 200 2 230 2 055 10 325 20 677
Adolescents 368 111 205 1 577 2 861 9 054 13 193
Sum of
above 2 840 313 430 4 137 5 517 25 553 39 895
Reference
number of paediatric
trials 316 355 342 404 379 334 332
Source EudraCT Data Warehouse using a pre-defined query on 6 March 2013 modified by excluding studies or lsquoimmunological medicinal productsrsquo
Table 8EU budget contribution to the Paediatric Regulation and the EMA expenditure
0
1
2
3
4
5
6
7
8
9
10
2006 2007 2008 2009 2010 2011 2012
EU budget contribution (in Million euro)
EMA expenditure for paediatri cs (in Mill ion euro)
EMA expenditure for paediatr ics including support (in Million euro)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2736
27
Table 9Percentage o European Medicines Agencyrsquos human resources working in the paediatric area rom 2006 (inner
circle) to 2012 (outer circle)
733 (2012)
052 (2006)
Table 10Member States acting as rapporteurs or the assessment o studies submitted in accordance with Article 46
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE SE NL FR DK IT BE PL ES NO SK FI IE RO AT HU EL CZ PT LV BG
Study included in worksharing Rapporteur appointed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2836
28
Table 11Member States acting as rapporteur or the assessment o studies submitted in accordance with Article 45
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE NL DK AT FR PL SE ES IE CZ MT IT BE SI EE FI HU NO RO BG EL LV PT IS SK
Wave 1 Wave 2 Wave 3 Wave 4 Wave 5 Wave 6 Wave 7 Wave 8 Wave 9
Wave 10 Wave 11 Wave 12 Wave 13 Wave 14 Wave 15 Wave 16 Wave 17 Wave 18
Table 12Member States acting as rapporteurspeer reviewers in EMArsquos Paediatric Committee procedures (initial PIP
waiver or modification o an agreed PIP)
0
50
100
150
200
250
300
350
400
450
500
A u s t r i a
B el gi um
B ul g a r i a
C y pr u s
C z e c h R e p u b l i c
D enm a r k
E s t oni a
F i nl a n d
F r a n c e
G er m a n y
G r e e c e
H e a l t h c a r e a n d
A c a d emi a
H un g a r y
I c el a n d
I r el a n d
I t a l y
L a t vi a
L i t h u a ni a
L ux em b o ur g
M a l t a
N or w a y
P a t i en t s Or g a ni s a t i on
P ol a n d
P or t u g a l
R om a ni a
S l ov a k i a
S l ov eni a
S p a i n
S w e d en
T h eN e t h er l a n d
s
U ni t e d K i n g d om
Initial PIP applications PIP modifications
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2936
29
ANNEX II
Detailed inventory of centrally authorised medicinalproducts for paediatric use since the entry into force
of the Paediatric Regulation
Table 13Medicinal products authorised centrally since 2007 which include a paediatric indication
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Retapamulin Altargo 2007 No Mixed
Nelarabine Atriance 2007 No Mixed
Human papillomavirus vaccine[types 16 18] Cervarix 2007 No Mixed
Hydroxocobalamin Cyanokit 2007 No Mixed
Idursulase Elaprase 2007 No Mixed
Gadoversetamide Optimark 2007 No Mixed
Betaine anhydrous Cystadane 2007 No Mixed
Stiripentol Diacomit 2007 No Paediatric only
Mecasermin Increlex 2007 No Paediatric only
Rufinamide Inovelon 2007 No Mixed
Hydroxycarbamide Siklos 2007 No Mixed
Human normal
immunoglobulin (ivig) Flebogamma DIF 2007 No Mixed
Fluticasone uroate Avamys 2008 No Mixed
Human normal immunoglobulin Privigen 2008 No Mixed
Lacosamide Vimpat 2008 No Mixed
Micaungin Mycamine 2008 No Mixed
Sapropterin Kuvan 2008 No Mixed
Sugammadex Bridion 2008 No Mixed
Tocoersonal d-alpha
tocopheryl polyethylene glycol
succinate Vedrop 2009 No Paediatric only
Miamurtide Mepact 2009 No Mixed
Rilonacept Rilonacept Regeneron 2009 No Mixed
Tacrolimus Modigra 2009 No Mixed
Pneumoccocal polysaccharideconjugate vaccine (adsorbed) Synflorix 2009 No Paediatric only
Canakinumab
Ilaris (PIP not yet
completed) 2009 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3036
30
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Pneumoccocal polysaccharide
conjugate vaccine (13-valentadsorbed)
Prevenar 13 (PIP not yetcompleted) 2009 Yes Paediatric only
Meningococcal group a c
w135 and y conjugate vaccine Menveo 2010 Yes Mixed
Velaglucerase ala
Vpriv (PIP not yet
completed) 2010 Yes Mixed
Influenza vaccine (live
attenuated nasal) Fluenz (Waiver) 2011 Yes Paediatric only
C1 inhibitor human
Cinryze (PIP not yet
completed) 2011 Yes Mixed
Dihydroartemisinin
piperaquine phosphate
Eurartesim (PIP not yet
completed) 2011 Yes Mixed
Midazolam Buccolam 2011 Yes (PUMA) Paediatric only
EverolimusVotubia(PIP not yet completed) 2011 Yes Mixed
Tobramycin
Tobi Podhaler (PIP not
yet completed) 2011 Yes Mixed
Nomegestrol estradiol Ioa Zoely 2011 Yes Mixed
Colistimethate sodium Colobreathe 2012 Yes Mixed
Mercaptopurine Xaluprine 2012 No Mixed
Catridecacog NovoThirteen 2012 Yes MixedEavirenz Eavirenz Teva 2012 No Mixed
Ivacafor Kalydeco 2012 Yes Mixed
Desloratadine Desloratadine ratiopharm 2012 No Mixed
Desloratadine Desloratadine Actavis 2012 No Mixed
Perampanel Fycompa 2012 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3136
31
Table 14List o centrally authorised medicinal products or which the therapeutic indication was extended to or amend-
ed or the paediatric population
Active substance(s)
Trade
name Date Subject of the extension
Levetiracetam Keppra
2007
2009
Extension o the indication to include adjunctive ther-
apy in the treatment o primary generalised tonic-
clonic (PGTC) seizures in adults and adolescents rom
12 years o age with idiopathic generalised epilepsyExtension o indication to include the adjunctive
treatment o partial seizures with or without second-
ary generalisation in children rom 1 month to lt4
years old
Pneumococcal sac-
charide conjugated
vaccine adsorbed Prevenar 2007
Extension o the indication to include new inorma-
tion on efficacy against disease caused by Strepto-
coccus pneumoniae serotypes 4 6B 9V 14 18C 19F
and 23F in otitis mediaExtension o indication rom active immunisation
against bacteraemic pneumonia to active immunisa-
tion against pneumonia
Infliximab
Remi-
cade 2007
Extension o indication to include treatment o
severe active Crohnrsquos disease in children aged 6 to
17 years
Darbepoetin ala Aranesp 2007
Extension o indication or CRF patients whichrestricted the use o Nespo to paediatric subjects ge
11 years o age
Fosamprenavir Telzir 2007
Extension o indication o Telzir in combination withritonavir or the treatment o Human Immunodefi-
ciency Virus Type 1 (HIV-1) inected adults in combi-nation with other antiretroviral medicinal products to
include paediatric populations
Lamivudine zidovu-
dine Combivir 2007
Extension o indication to include paediatric patients
and replacement o film-coated tablets by scored
film-coated tablets
Desloratadine Aerius 2007Extension o indication rom lsquochronic idiopathic urti-cariarsquo to lsquourticariarsquo
Insulin glulisine Apidra 2007
Extension o indication to include 6 year olds and
older children based on the results o 2 paediatricstudies
Human papilloma virusvaccine [types 6 11
16 18] (recombinantadsorbed) Gardasil 2008
Extension o indication to include the prevention ohigh-grade vaginal dysplastic lesions (VaIN 23)
Adalimumab Humira 20082011
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in adoles-cents rom 13 to 17 years o age
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in the paedi-
atric population aged rom 4 to 12 years
Caspoungin Cancidas 2008
Extension o the indication to include the paediatric
population
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1836
18
nies may decide to stop the correspond-
ing adult development It is too early still
to obtain reliable statistics that show
the ratio between completed and non-
completed paediatric investigation plans
but in the current context not all approved
plans will eventually result in an approved
medicine with a paediatric indication
In terms o output this entails some un-
necessary effort in compiling and screen-
ing paediatric investigation plans To what
extent this is offset by the benefit o early
submission which ensures that the pae-
diatric development fits smoothly into the
overall product development need ur-
ther monitoring
A urther point o concern is the highnumber o modifications to paediat-
ric investigation plans Figures seem to
suggest that nearly all plans have to
be modified at least once Conceptually
though this does not come as a surprise
in view o the early submission o pae-
diatric investigation plans the length o
adult and paediatric developments and
the substantial deerrals granted An
RampD plan requently has to be adapted
or amended to take account o initial re-sults Recruitment problems or necessary
design changes in the trials may also lead
to modifications While it is acknowledged
that substantial amendments or modifi-
cations to the plan have to be subject to
discussions with the Paediatric Commit-
tee this is less obvious or minor changes
In this context the level o detail required
by the EMA has been repeatedly criticised
In the past five years the EMA and its
Paediatric Committee have made effortsto provide or some flexibility in the plan
so to allow a margin o manoeuvre that
takes account o uncertainties in relation
to certain parameters o a trial
In any case the Commission intends to
review its Communication on the ormat
and content o applications or agree-
ment or modification o a paediatric in-
vestigation plan to take into account the
experience gained including the consider-
able number o modification requests
On a positive note it can be noted that
companies are applying or the rewards
provided by the Regulation primarily the
6-month extension o the Supplementary
Protection Certificate which have been
introduced to offset the additional bur-
den The economic value o the reward
depends on the turnover o the product
concerned In the case o blockbuster
products the amount may be consider-
able while or niche products the effect
is small
An in-depth evaluation o the economic
impact will be included in the 2017 report
in order to draw conclusions on the bal-
ance between burden and rewards and
public health benefits
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1936
19
6Outlook mdash
A fairy-taleending aheadlsquoBetter Medicines or Children mdash From
Concept to Realityrsquo is the title o this re-
port Readers may suggest that based on
the evaluation reerred to above it would
be more appropriate to add a question
mark It is evident that it is too early still
to make a firm statement Despite more
than five years o experience the true im-pact o the Regulation on the health o
children will only become apparent over
time as experience is accumulated in the
longer term
There are encouraging signs though
Paediatric development has become a
more integral part o the overall develop-
ment o medicinal products in the EU A
number o new products with paediatric
indications and age-appropriate pharma-ceutical orms have been authorised and
made available to patients A high num-
ber o agreed paediatric investigation
plans indicates that urther products are
in the pipeline
However it needs to be pointed out that it
would be wrong to expect the Regulation
to be able to solve all problems Instead
it is a major catalyst to improve the situ-
ation o young patients
Finally some weaknesses and deficits
have also become apparent in the last
five years Their impact on the overall
perormance o the Regulation has to be
closely monitored On the basis o the ac-
tions outlined above the Commission in-
tends to fine-tune the current implemen-
tation together with the EMA
Even i better medicines or children are
not yet a reality it should be the ambitiono all stakeholders involved that this piece
o legislation will be or the greater good
o children so that in the 2017 report
the discussion will ocus not on whether a
question mark should be added to the ti-
tle o the report but on whether it should
be an exclamation mark instead
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2036
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2136
21
ANNEXES
Figures and Tables
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2236
22
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2336
23
ANNEX I
Figures and Tables
Table 1Agreed paediatric investigations plans (PIPs) 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Agreed PIPs submitted under Article 7 (without waivers)
Agreed PIPs submitted under Article 8 (without waivers)
Source EMA Paediatric database The numbers on agreed PIPs correspond to EMA decisions
Table 2Agreed paediatric investigations plans (PIPs) compared to ull waivers and modifications 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Submitted modifications of an agreed PIP
Agreed Full waivers
Source EMA Paediatric database The numbers on agreed PIPs and waivers correspond to EMA decisions
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2536
25
Table 5Scientific advice and protocol assistance including ollow-ups (provided by the EMA Scientific Advice Working
Party and the Committee or Human Medicinal Products per year)
259
277321
388 400 433 420
021 32
74 8057
91
0 0 0
68 8067
94
0
100
200
300
400
500
2006 2007 2008 2009 2010 2011 2012
Total number of advice (Scientific Advice and Protocol Assistance)
Sum of paediatric-only and mixed (adult and paediatric development questions)
advice
Paediatric-only or mixed advice that involved a Paediatric Committee member(s) as
expert(s)
Source EMA databases Year o advice letter
Year o start o procedure
Table 6Paediatric clinical trials by year o authorisation
2005 2006 2007 2008 2009 2010 2011 2012
Paediatric trials
(number) 254 316 355 342 404 379 334 332
Paediatric trials
that are part of anagreed PIP 2 1 2 6 16 30 76 76
Proportion of
paediatric trials
that are part of an
agreed PIP among
paediatric trials 1 0 1 2 4 8 23 23
Total number
of trials (adults
and or children) 3 350 3 979 4 749 4 512 4 445 4 026 3 809 3 698
Proportion of
paediatric trials of
all trials 8 8 7 8 9 10 9 9
Source EudraCT Data Warehouse using a predefined query on 6 March 2013 and counting the first authorised trial only in the case o more thanone Member State This partial inormation requires sponsors to use a Clinical Trial Application orm that was only available rom November 2009 or use with version 8 o EudraCT
(available rom 2011)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2636
26
Table 7Number o children to be enrolled in clinical trials
Number
of subjects 2006 2007 2008 2009 2010 2011 2012
Pretermnewborns 0 0 0 207 82 2 281 1 712
Newborns 0 0 5 64 169 1 105 1 172
Infants and
toddlers 330 21 20 59 351 2 788 3 141
Children 2 142 181 200 2 230 2 055 10 325 20 677
Adolescents 368 111 205 1 577 2 861 9 054 13 193
Sum of
above 2 840 313 430 4 137 5 517 25 553 39 895
Reference
number of paediatric
trials 316 355 342 404 379 334 332
Source EudraCT Data Warehouse using a pre-defined query on 6 March 2013 modified by excluding studies or lsquoimmunological medicinal productsrsquo
Table 8EU budget contribution to the Paediatric Regulation and the EMA expenditure
0
1
2
3
4
5
6
7
8
9
10
2006 2007 2008 2009 2010 2011 2012
EU budget contribution (in Million euro)
EMA expenditure for paediatri cs (in Mill ion euro)
EMA expenditure for paediatr ics including support (in Million euro)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2736
27
Table 9Percentage o European Medicines Agencyrsquos human resources working in the paediatric area rom 2006 (inner
circle) to 2012 (outer circle)
733 (2012)
052 (2006)
Table 10Member States acting as rapporteurs or the assessment o studies submitted in accordance with Article 46
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE SE NL FR DK IT BE PL ES NO SK FI IE RO AT HU EL CZ PT LV BG
Study included in worksharing Rapporteur appointed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2836
28
Table 11Member States acting as rapporteur or the assessment o studies submitted in accordance with Article 45
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE NL DK AT FR PL SE ES IE CZ MT IT BE SI EE FI HU NO RO BG EL LV PT IS SK
Wave 1 Wave 2 Wave 3 Wave 4 Wave 5 Wave 6 Wave 7 Wave 8 Wave 9
Wave 10 Wave 11 Wave 12 Wave 13 Wave 14 Wave 15 Wave 16 Wave 17 Wave 18
Table 12Member States acting as rapporteurspeer reviewers in EMArsquos Paediatric Committee procedures (initial PIP
waiver or modification o an agreed PIP)
0
50
100
150
200
250
300
350
400
450
500
A u s t r i a
B el gi um
B ul g a r i a
C y pr u s
C z e c h R e p u b l i c
D enm a r k
E s t oni a
F i nl a n d
F r a n c e
G er m a n y
G r e e c e
H e a l t h c a r e a n d
A c a d emi a
H un g a r y
I c el a n d
I r el a n d
I t a l y
L a t vi a
L i t h u a ni a
L ux em b o ur g
M a l t a
N or w a y
P a t i en t s Or g a ni s a t i on
P ol a n d
P or t u g a l
R om a ni a
S l ov a k i a
S l ov eni a
S p a i n
S w e d en
T h eN e t h er l a n d
s
U ni t e d K i n g d om
Initial PIP applications PIP modifications
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2936
29
ANNEX II
Detailed inventory of centrally authorised medicinalproducts for paediatric use since the entry into force
of the Paediatric Regulation
Table 13Medicinal products authorised centrally since 2007 which include a paediatric indication
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Retapamulin Altargo 2007 No Mixed
Nelarabine Atriance 2007 No Mixed
Human papillomavirus vaccine[types 16 18] Cervarix 2007 No Mixed
Hydroxocobalamin Cyanokit 2007 No Mixed
Idursulase Elaprase 2007 No Mixed
Gadoversetamide Optimark 2007 No Mixed
Betaine anhydrous Cystadane 2007 No Mixed
Stiripentol Diacomit 2007 No Paediatric only
Mecasermin Increlex 2007 No Paediatric only
Rufinamide Inovelon 2007 No Mixed
Hydroxycarbamide Siklos 2007 No Mixed
Human normal
immunoglobulin (ivig) Flebogamma DIF 2007 No Mixed
Fluticasone uroate Avamys 2008 No Mixed
Human normal immunoglobulin Privigen 2008 No Mixed
Lacosamide Vimpat 2008 No Mixed
Micaungin Mycamine 2008 No Mixed
Sapropterin Kuvan 2008 No Mixed
Sugammadex Bridion 2008 No Mixed
Tocoersonal d-alpha
tocopheryl polyethylene glycol
succinate Vedrop 2009 No Paediatric only
Miamurtide Mepact 2009 No Mixed
Rilonacept Rilonacept Regeneron 2009 No Mixed
Tacrolimus Modigra 2009 No Mixed
Pneumoccocal polysaccharideconjugate vaccine (adsorbed) Synflorix 2009 No Paediatric only
Canakinumab
Ilaris (PIP not yet
completed) 2009 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3036
30
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Pneumoccocal polysaccharide
conjugate vaccine (13-valentadsorbed)
Prevenar 13 (PIP not yetcompleted) 2009 Yes Paediatric only
Meningococcal group a c
w135 and y conjugate vaccine Menveo 2010 Yes Mixed
Velaglucerase ala
Vpriv (PIP not yet
completed) 2010 Yes Mixed
Influenza vaccine (live
attenuated nasal) Fluenz (Waiver) 2011 Yes Paediatric only
C1 inhibitor human
Cinryze (PIP not yet
completed) 2011 Yes Mixed
Dihydroartemisinin
piperaquine phosphate
Eurartesim (PIP not yet
completed) 2011 Yes Mixed
Midazolam Buccolam 2011 Yes (PUMA) Paediatric only
EverolimusVotubia(PIP not yet completed) 2011 Yes Mixed
Tobramycin
Tobi Podhaler (PIP not
yet completed) 2011 Yes Mixed
Nomegestrol estradiol Ioa Zoely 2011 Yes Mixed
Colistimethate sodium Colobreathe 2012 Yes Mixed
Mercaptopurine Xaluprine 2012 No Mixed
Catridecacog NovoThirteen 2012 Yes MixedEavirenz Eavirenz Teva 2012 No Mixed
Ivacafor Kalydeco 2012 Yes Mixed
Desloratadine Desloratadine ratiopharm 2012 No Mixed
Desloratadine Desloratadine Actavis 2012 No Mixed
Perampanel Fycompa 2012 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3136
31
Table 14List o centrally authorised medicinal products or which the therapeutic indication was extended to or amend-
ed or the paediatric population
Active substance(s)
Trade
name Date Subject of the extension
Levetiracetam Keppra
2007
2009
Extension o the indication to include adjunctive ther-
apy in the treatment o primary generalised tonic-
clonic (PGTC) seizures in adults and adolescents rom
12 years o age with idiopathic generalised epilepsyExtension o indication to include the adjunctive
treatment o partial seizures with or without second-
ary generalisation in children rom 1 month to lt4
years old
Pneumococcal sac-
charide conjugated
vaccine adsorbed Prevenar 2007
Extension o the indication to include new inorma-
tion on efficacy against disease caused by Strepto-
coccus pneumoniae serotypes 4 6B 9V 14 18C 19F
and 23F in otitis mediaExtension o indication rom active immunisation
against bacteraemic pneumonia to active immunisa-
tion against pneumonia
Infliximab
Remi-
cade 2007
Extension o indication to include treatment o
severe active Crohnrsquos disease in children aged 6 to
17 years
Darbepoetin ala Aranesp 2007
Extension o indication or CRF patients whichrestricted the use o Nespo to paediatric subjects ge
11 years o age
Fosamprenavir Telzir 2007
Extension o indication o Telzir in combination withritonavir or the treatment o Human Immunodefi-
ciency Virus Type 1 (HIV-1) inected adults in combi-nation with other antiretroviral medicinal products to
include paediatric populations
Lamivudine zidovu-
dine Combivir 2007
Extension o indication to include paediatric patients
and replacement o film-coated tablets by scored
film-coated tablets
Desloratadine Aerius 2007Extension o indication rom lsquochronic idiopathic urti-cariarsquo to lsquourticariarsquo
Insulin glulisine Apidra 2007
Extension o indication to include 6 year olds and
older children based on the results o 2 paediatricstudies
Human papilloma virusvaccine [types 6 11
16 18] (recombinantadsorbed) Gardasil 2008
Extension o indication to include the prevention ohigh-grade vaginal dysplastic lesions (VaIN 23)
Adalimumab Humira 20082011
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in adoles-cents rom 13 to 17 years o age
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in the paedi-
atric population aged rom 4 to 12 years
Caspoungin Cancidas 2008
Extension o the indication to include the paediatric
population
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 1936
19
6Outlook mdash
A fairy-taleending aheadlsquoBetter Medicines or Children mdash From
Concept to Realityrsquo is the title o this re-
port Readers may suggest that based on
the evaluation reerred to above it would
be more appropriate to add a question
mark It is evident that it is too early still
to make a firm statement Despite more
than five years o experience the true im-pact o the Regulation on the health o
children will only become apparent over
time as experience is accumulated in the
longer term
There are encouraging signs though
Paediatric development has become a
more integral part o the overall develop-
ment o medicinal products in the EU A
number o new products with paediatric
indications and age-appropriate pharma-ceutical orms have been authorised and
made available to patients A high num-
ber o agreed paediatric investigation
plans indicates that urther products are
in the pipeline
However it needs to be pointed out that it
would be wrong to expect the Regulation
to be able to solve all problems Instead
it is a major catalyst to improve the situ-
ation o young patients
Finally some weaknesses and deficits
have also become apparent in the last
five years Their impact on the overall
perormance o the Regulation has to be
closely monitored On the basis o the ac-
tions outlined above the Commission in-
tends to fine-tune the current implemen-
tation together with the EMA
Even i better medicines or children are
not yet a reality it should be the ambitiono all stakeholders involved that this piece
o legislation will be or the greater good
o children so that in the 2017 report
the discussion will ocus not on whether a
question mark should be added to the ti-
tle o the report but on whether it should
be an exclamation mark instead
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2036
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2136
21
ANNEXES
Figures and Tables
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2236
22
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2336
23
ANNEX I
Figures and Tables
Table 1Agreed paediatric investigations plans (PIPs) 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Agreed PIPs submitted under Article 7 (without waivers)
Agreed PIPs submitted under Article 8 (without waivers)
Source EMA Paediatric database The numbers on agreed PIPs correspond to EMA decisions
Table 2Agreed paediatric investigations plans (PIPs) compared to ull waivers and modifications 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Submitted modifications of an agreed PIP
Agreed Full waivers
Source EMA Paediatric database The numbers on agreed PIPs and waivers correspond to EMA decisions
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2536
25
Table 5Scientific advice and protocol assistance including ollow-ups (provided by the EMA Scientific Advice Working
Party and the Committee or Human Medicinal Products per year)
259
277321
388 400 433 420
021 32
74 8057
91
0 0 0
68 8067
94
0
100
200
300
400
500
2006 2007 2008 2009 2010 2011 2012
Total number of advice (Scientific Advice and Protocol Assistance)
Sum of paediatric-only and mixed (adult and paediatric development questions)
advice
Paediatric-only or mixed advice that involved a Paediatric Committee member(s) as
expert(s)
Source EMA databases Year o advice letter
Year o start o procedure
Table 6Paediatric clinical trials by year o authorisation
2005 2006 2007 2008 2009 2010 2011 2012
Paediatric trials
(number) 254 316 355 342 404 379 334 332
Paediatric trials
that are part of anagreed PIP 2 1 2 6 16 30 76 76
Proportion of
paediatric trials
that are part of an
agreed PIP among
paediatric trials 1 0 1 2 4 8 23 23
Total number
of trials (adults
and or children) 3 350 3 979 4 749 4 512 4 445 4 026 3 809 3 698
Proportion of
paediatric trials of
all trials 8 8 7 8 9 10 9 9
Source EudraCT Data Warehouse using a predefined query on 6 March 2013 and counting the first authorised trial only in the case o more thanone Member State This partial inormation requires sponsors to use a Clinical Trial Application orm that was only available rom November 2009 or use with version 8 o EudraCT
(available rom 2011)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2636
26
Table 7Number o children to be enrolled in clinical trials
Number
of subjects 2006 2007 2008 2009 2010 2011 2012
Pretermnewborns 0 0 0 207 82 2 281 1 712
Newborns 0 0 5 64 169 1 105 1 172
Infants and
toddlers 330 21 20 59 351 2 788 3 141
Children 2 142 181 200 2 230 2 055 10 325 20 677
Adolescents 368 111 205 1 577 2 861 9 054 13 193
Sum of
above 2 840 313 430 4 137 5 517 25 553 39 895
Reference
number of paediatric
trials 316 355 342 404 379 334 332
Source EudraCT Data Warehouse using a pre-defined query on 6 March 2013 modified by excluding studies or lsquoimmunological medicinal productsrsquo
Table 8EU budget contribution to the Paediatric Regulation and the EMA expenditure
0
1
2
3
4
5
6
7
8
9
10
2006 2007 2008 2009 2010 2011 2012
EU budget contribution (in Million euro)
EMA expenditure for paediatri cs (in Mill ion euro)
EMA expenditure for paediatr ics including support (in Million euro)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2736
27
Table 9Percentage o European Medicines Agencyrsquos human resources working in the paediatric area rom 2006 (inner
circle) to 2012 (outer circle)
733 (2012)
052 (2006)
Table 10Member States acting as rapporteurs or the assessment o studies submitted in accordance with Article 46
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE SE NL FR DK IT BE PL ES NO SK FI IE RO AT HU EL CZ PT LV BG
Study included in worksharing Rapporteur appointed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2836
28
Table 11Member States acting as rapporteur or the assessment o studies submitted in accordance with Article 45
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE NL DK AT FR PL SE ES IE CZ MT IT BE SI EE FI HU NO RO BG EL LV PT IS SK
Wave 1 Wave 2 Wave 3 Wave 4 Wave 5 Wave 6 Wave 7 Wave 8 Wave 9
Wave 10 Wave 11 Wave 12 Wave 13 Wave 14 Wave 15 Wave 16 Wave 17 Wave 18
Table 12Member States acting as rapporteurspeer reviewers in EMArsquos Paediatric Committee procedures (initial PIP
waiver or modification o an agreed PIP)
0
50
100
150
200
250
300
350
400
450
500
A u s t r i a
B el gi um
B ul g a r i a
C y pr u s
C z e c h R e p u b l i c
D enm a r k
E s t oni a
F i nl a n d
F r a n c e
G er m a n y
G r e e c e
H e a l t h c a r e a n d
A c a d emi a
H un g a r y
I c el a n d
I r el a n d
I t a l y
L a t vi a
L i t h u a ni a
L ux em b o ur g
M a l t a
N or w a y
P a t i en t s Or g a ni s a t i on
P ol a n d
P or t u g a l
R om a ni a
S l ov a k i a
S l ov eni a
S p a i n
S w e d en
T h eN e t h er l a n d
s
U ni t e d K i n g d om
Initial PIP applications PIP modifications
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2936
29
ANNEX II
Detailed inventory of centrally authorised medicinalproducts for paediatric use since the entry into force
of the Paediatric Regulation
Table 13Medicinal products authorised centrally since 2007 which include a paediatric indication
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Retapamulin Altargo 2007 No Mixed
Nelarabine Atriance 2007 No Mixed
Human papillomavirus vaccine[types 16 18] Cervarix 2007 No Mixed
Hydroxocobalamin Cyanokit 2007 No Mixed
Idursulase Elaprase 2007 No Mixed
Gadoversetamide Optimark 2007 No Mixed
Betaine anhydrous Cystadane 2007 No Mixed
Stiripentol Diacomit 2007 No Paediatric only
Mecasermin Increlex 2007 No Paediatric only
Rufinamide Inovelon 2007 No Mixed
Hydroxycarbamide Siklos 2007 No Mixed
Human normal
immunoglobulin (ivig) Flebogamma DIF 2007 No Mixed
Fluticasone uroate Avamys 2008 No Mixed
Human normal immunoglobulin Privigen 2008 No Mixed
Lacosamide Vimpat 2008 No Mixed
Micaungin Mycamine 2008 No Mixed
Sapropterin Kuvan 2008 No Mixed
Sugammadex Bridion 2008 No Mixed
Tocoersonal d-alpha
tocopheryl polyethylene glycol
succinate Vedrop 2009 No Paediatric only
Miamurtide Mepact 2009 No Mixed
Rilonacept Rilonacept Regeneron 2009 No Mixed
Tacrolimus Modigra 2009 No Mixed
Pneumoccocal polysaccharideconjugate vaccine (adsorbed) Synflorix 2009 No Paediatric only
Canakinumab
Ilaris (PIP not yet
completed) 2009 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3036
30
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Pneumoccocal polysaccharide
conjugate vaccine (13-valentadsorbed)
Prevenar 13 (PIP not yetcompleted) 2009 Yes Paediatric only
Meningococcal group a c
w135 and y conjugate vaccine Menveo 2010 Yes Mixed
Velaglucerase ala
Vpriv (PIP not yet
completed) 2010 Yes Mixed
Influenza vaccine (live
attenuated nasal) Fluenz (Waiver) 2011 Yes Paediatric only
C1 inhibitor human
Cinryze (PIP not yet
completed) 2011 Yes Mixed
Dihydroartemisinin
piperaquine phosphate
Eurartesim (PIP not yet
completed) 2011 Yes Mixed
Midazolam Buccolam 2011 Yes (PUMA) Paediatric only
EverolimusVotubia(PIP not yet completed) 2011 Yes Mixed
Tobramycin
Tobi Podhaler (PIP not
yet completed) 2011 Yes Mixed
Nomegestrol estradiol Ioa Zoely 2011 Yes Mixed
Colistimethate sodium Colobreathe 2012 Yes Mixed
Mercaptopurine Xaluprine 2012 No Mixed
Catridecacog NovoThirteen 2012 Yes MixedEavirenz Eavirenz Teva 2012 No Mixed
Ivacafor Kalydeco 2012 Yes Mixed
Desloratadine Desloratadine ratiopharm 2012 No Mixed
Desloratadine Desloratadine Actavis 2012 No Mixed
Perampanel Fycompa 2012 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3136
31
Table 14List o centrally authorised medicinal products or which the therapeutic indication was extended to or amend-
ed or the paediatric population
Active substance(s)
Trade
name Date Subject of the extension
Levetiracetam Keppra
2007
2009
Extension o the indication to include adjunctive ther-
apy in the treatment o primary generalised tonic-
clonic (PGTC) seizures in adults and adolescents rom
12 years o age with idiopathic generalised epilepsyExtension o indication to include the adjunctive
treatment o partial seizures with or without second-
ary generalisation in children rom 1 month to lt4
years old
Pneumococcal sac-
charide conjugated
vaccine adsorbed Prevenar 2007
Extension o the indication to include new inorma-
tion on efficacy against disease caused by Strepto-
coccus pneumoniae serotypes 4 6B 9V 14 18C 19F
and 23F in otitis mediaExtension o indication rom active immunisation
against bacteraemic pneumonia to active immunisa-
tion against pneumonia
Infliximab
Remi-
cade 2007
Extension o indication to include treatment o
severe active Crohnrsquos disease in children aged 6 to
17 years
Darbepoetin ala Aranesp 2007
Extension o indication or CRF patients whichrestricted the use o Nespo to paediatric subjects ge
11 years o age
Fosamprenavir Telzir 2007
Extension o indication o Telzir in combination withritonavir or the treatment o Human Immunodefi-
ciency Virus Type 1 (HIV-1) inected adults in combi-nation with other antiretroviral medicinal products to
include paediatric populations
Lamivudine zidovu-
dine Combivir 2007
Extension o indication to include paediatric patients
and replacement o film-coated tablets by scored
film-coated tablets
Desloratadine Aerius 2007Extension o indication rom lsquochronic idiopathic urti-cariarsquo to lsquourticariarsquo
Insulin glulisine Apidra 2007
Extension o indication to include 6 year olds and
older children based on the results o 2 paediatricstudies
Human papilloma virusvaccine [types 6 11
16 18] (recombinantadsorbed) Gardasil 2008
Extension o indication to include the prevention ohigh-grade vaginal dysplastic lesions (VaIN 23)
Adalimumab Humira 20082011
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in adoles-cents rom 13 to 17 years o age
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in the paedi-
atric population aged rom 4 to 12 years
Caspoungin Cancidas 2008
Extension o the indication to include the paediatric
population
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2036
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2136
21
ANNEXES
Figures and Tables
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2236
22
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2336
23
ANNEX I
Figures and Tables
Table 1Agreed paediatric investigations plans (PIPs) 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Agreed PIPs submitted under Article 7 (without waivers)
Agreed PIPs submitted under Article 8 (without waivers)
Source EMA Paediatric database The numbers on agreed PIPs correspond to EMA decisions
Table 2Agreed paediatric investigations plans (PIPs) compared to ull waivers and modifications 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Submitted modifications of an agreed PIP
Agreed Full waivers
Source EMA Paediatric database The numbers on agreed PIPs and waivers correspond to EMA decisions
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2536
25
Table 5Scientific advice and protocol assistance including ollow-ups (provided by the EMA Scientific Advice Working
Party and the Committee or Human Medicinal Products per year)
259
277321
388 400 433 420
021 32
74 8057
91
0 0 0
68 8067
94
0
100
200
300
400
500
2006 2007 2008 2009 2010 2011 2012
Total number of advice (Scientific Advice and Protocol Assistance)
Sum of paediatric-only and mixed (adult and paediatric development questions)
advice
Paediatric-only or mixed advice that involved a Paediatric Committee member(s) as
expert(s)
Source EMA databases Year o advice letter
Year o start o procedure
Table 6Paediatric clinical trials by year o authorisation
2005 2006 2007 2008 2009 2010 2011 2012
Paediatric trials
(number) 254 316 355 342 404 379 334 332
Paediatric trials
that are part of anagreed PIP 2 1 2 6 16 30 76 76
Proportion of
paediatric trials
that are part of an
agreed PIP among
paediatric trials 1 0 1 2 4 8 23 23
Total number
of trials (adults
and or children) 3 350 3 979 4 749 4 512 4 445 4 026 3 809 3 698
Proportion of
paediatric trials of
all trials 8 8 7 8 9 10 9 9
Source EudraCT Data Warehouse using a predefined query on 6 March 2013 and counting the first authorised trial only in the case o more thanone Member State This partial inormation requires sponsors to use a Clinical Trial Application orm that was only available rom November 2009 or use with version 8 o EudraCT
(available rom 2011)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2636
26
Table 7Number o children to be enrolled in clinical trials
Number
of subjects 2006 2007 2008 2009 2010 2011 2012
Pretermnewborns 0 0 0 207 82 2 281 1 712
Newborns 0 0 5 64 169 1 105 1 172
Infants and
toddlers 330 21 20 59 351 2 788 3 141
Children 2 142 181 200 2 230 2 055 10 325 20 677
Adolescents 368 111 205 1 577 2 861 9 054 13 193
Sum of
above 2 840 313 430 4 137 5 517 25 553 39 895
Reference
number of paediatric
trials 316 355 342 404 379 334 332
Source EudraCT Data Warehouse using a pre-defined query on 6 March 2013 modified by excluding studies or lsquoimmunological medicinal productsrsquo
Table 8EU budget contribution to the Paediatric Regulation and the EMA expenditure
0
1
2
3
4
5
6
7
8
9
10
2006 2007 2008 2009 2010 2011 2012
EU budget contribution (in Million euro)
EMA expenditure for paediatri cs (in Mill ion euro)
EMA expenditure for paediatr ics including support (in Million euro)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2736
27
Table 9Percentage o European Medicines Agencyrsquos human resources working in the paediatric area rom 2006 (inner
circle) to 2012 (outer circle)
733 (2012)
052 (2006)
Table 10Member States acting as rapporteurs or the assessment o studies submitted in accordance with Article 46
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE SE NL FR DK IT BE PL ES NO SK FI IE RO AT HU EL CZ PT LV BG
Study included in worksharing Rapporteur appointed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2836
28
Table 11Member States acting as rapporteur or the assessment o studies submitted in accordance with Article 45
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE NL DK AT FR PL SE ES IE CZ MT IT BE SI EE FI HU NO RO BG EL LV PT IS SK
Wave 1 Wave 2 Wave 3 Wave 4 Wave 5 Wave 6 Wave 7 Wave 8 Wave 9
Wave 10 Wave 11 Wave 12 Wave 13 Wave 14 Wave 15 Wave 16 Wave 17 Wave 18
Table 12Member States acting as rapporteurspeer reviewers in EMArsquos Paediatric Committee procedures (initial PIP
waiver or modification o an agreed PIP)
0
50
100
150
200
250
300
350
400
450
500
A u s t r i a
B el gi um
B ul g a r i a
C y pr u s
C z e c h R e p u b l i c
D enm a r k
E s t oni a
F i nl a n d
F r a n c e
G er m a n y
G r e e c e
H e a l t h c a r e a n d
A c a d emi a
H un g a r y
I c el a n d
I r el a n d
I t a l y
L a t vi a
L i t h u a ni a
L ux em b o ur g
M a l t a
N or w a y
P a t i en t s Or g a ni s a t i on
P ol a n d
P or t u g a l
R om a ni a
S l ov a k i a
S l ov eni a
S p a i n
S w e d en
T h eN e t h er l a n d
s
U ni t e d K i n g d om
Initial PIP applications PIP modifications
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2936
29
ANNEX II
Detailed inventory of centrally authorised medicinalproducts for paediatric use since the entry into force
of the Paediatric Regulation
Table 13Medicinal products authorised centrally since 2007 which include a paediatric indication
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Retapamulin Altargo 2007 No Mixed
Nelarabine Atriance 2007 No Mixed
Human papillomavirus vaccine[types 16 18] Cervarix 2007 No Mixed
Hydroxocobalamin Cyanokit 2007 No Mixed
Idursulase Elaprase 2007 No Mixed
Gadoversetamide Optimark 2007 No Mixed
Betaine anhydrous Cystadane 2007 No Mixed
Stiripentol Diacomit 2007 No Paediatric only
Mecasermin Increlex 2007 No Paediatric only
Rufinamide Inovelon 2007 No Mixed
Hydroxycarbamide Siklos 2007 No Mixed
Human normal
immunoglobulin (ivig) Flebogamma DIF 2007 No Mixed
Fluticasone uroate Avamys 2008 No Mixed
Human normal immunoglobulin Privigen 2008 No Mixed
Lacosamide Vimpat 2008 No Mixed
Micaungin Mycamine 2008 No Mixed
Sapropterin Kuvan 2008 No Mixed
Sugammadex Bridion 2008 No Mixed
Tocoersonal d-alpha
tocopheryl polyethylene glycol
succinate Vedrop 2009 No Paediatric only
Miamurtide Mepact 2009 No Mixed
Rilonacept Rilonacept Regeneron 2009 No Mixed
Tacrolimus Modigra 2009 No Mixed
Pneumoccocal polysaccharideconjugate vaccine (adsorbed) Synflorix 2009 No Paediatric only
Canakinumab
Ilaris (PIP not yet
completed) 2009 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3036
30
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Pneumoccocal polysaccharide
conjugate vaccine (13-valentadsorbed)
Prevenar 13 (PIP not yetcompleted) 2009 Yes Paediatric only
Meningococcal group a c
w135 and y conjugate vaccine Menveo 2010 Yes Mixed
Velaglucerase ala
Vpriv (PIP not yet
completed) 2010 Yes Mixed
Influenza vaccine (live
attenuated nasal) Fluenz (Waiver) 2011 Yes Paediatric only
C1 inhibitor human
Cinryze (PIP not yet
completed) 2011 Yes Mixed
Dihydroartemisinin
piperaquine phosphate
Eurartesim (PIP not yet
completed) 2011 Yes Mixed
Midazolam Buccolam 2011 Yes (PUMA) Paediatric only
EverolimusVotubia(PIP not yet completed) 2011 Yes Mixed
Tobramycin
Tobi Podhaler (PIP not
yet completed) 2011 Yes Mixed
Nomegestrol estradiol Ioa Zoely 2011 Yes Mixed
Colistimethate sodium Colobreathe 2012 Yes Mixed
Mercaptopurine Xaluprine 2012 No Mixed
Catridecacog NovoThirteen 2012 Yes MixedEavirenz Eavirenz Teva 2012 No Mixed
Ivacafor Kalydeco 2012 Yes Mixed
Desloratadine Desloratadine ratiopharm 2012 No Mixed
Desloratadine Desloratadine Actavis 2012 No Mixed
Perampanel Fycompa 2012 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3136
31
Table 14List o centrally authorised medicinal products or which the therapeutic indication was extended to or amend-
ed or the paediatric population
Active substance(s)
Trade
name Date Subject of the extension
Levetiracetam Keppra
2007
2009
Extension o the indication to include adjunctive ther-
apy in the treatment o primary generalised tonic-
clonic (PGTC) seizures in adults and adolescents rom
12 years o age with idiopathic generalised epilepsyExtension o indication to include the adjunctive
treatment o partial seizures with or without second-
ary generalisation in children rom 1 month to lt4
years old
Pneumococcal sac-
charide conjugated
vaccine adsorbed Prevenar 2007
Extension o the indication to include new inorma-
tion on efficacy against disease caused by Strepto-
coccus pneumoniae serotypes 4 6B 9V 14 18C 19F
and 23F in otitis mediaExtension o indication rom active immunisation
against bacteraemic pneumonia to active immunisa-
tion against pneumonia
Infliximab
Remi-
cade 2007
Extension o indication to include treatment o
severe active Crohnrsquos disease in children aged 6 to
17 years
Darbepoetin ala Aranesp 2007
Extension o indication or CRF patients whichrestricted the use o Nespo to paediatric subjects ge
11 years o age
Fosamprenavir Telzir 2007
Extension o indication o Telzir in combination withritonavir or the treatment o Human Immunodefi-
ciency Virus Type 1 (HIV-1) inected adults in combi-nation with other antiretroviral medicinal products to
include paediatric populations
Lamivudine zidovu-
dine Combivir 2007
Extension o indication to include paediatric patients
and replacement o film-coated tablets by scored
film-coated tablets
Desloratadine Aerius 2007Extension o indication rom lsquochronic idiopathic urti-cariarsquo to lsquourticariarsquo
Insulin glulisine Apidra 2007
Extension o indication to include 6 year olds and
older children based on the results o 2 paediatricstudies
Human papilloma virusvaccine [types 6 11
16 18] (recombinantadsorbed) Gardasil 2008
Extension o indication to include the prevention ohigh-grade vaginal dysplastic lesions (VaIN 23)
Adalimumab Humira 20082011
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in adoles-cents rom 13 to 17 years o age
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in the paedi-
atric population aged rom 4 to 12 years
Caspoungin Cancidas 2008
Extension o the indication to include the paediatric
population
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2136
21
ANNEXES
Figures and Tables
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2236
22
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2336
23
ANNEX I
Figures and Tables
Table 1Agreed paediatric investigations plans (PIPs) 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Agreed PIPs submitted under Article 7 (without waivers)
Agreed PIPs submitted under Article 8 (without waivers)
Source EMA Paediatric database The numbers on agreed PIPs correspond to EMA decisions
Table 2Agreed paediatric investigations plans (PIPs) compared to ull waivers and modifications 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Submitted modifications of an agreed PIP
Agreed Full waivers
Source EMA Paediatric database The numbers on agreed PIPs and waivers correspond to EMA decisions
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2536
25
Table 5Scientific advice and protocol assistance including ollow-ups (provided by the EMA Scientific Advice Working
Party and the Committee or Human Medicinal Products per year)
259
277321
388 400 433 420
021 32
74 8057
91
0 0 0
68 8067
94
0
100
200
300
400
500
2006 2007 2008 2009 2010 2011 2012
Total number of advice (Scientific Advice and Protocol Assistance)
Sum of paediatric-only and mixed (adult and paediatric development questions)
advice
Paediatric-only or mixed advice that involved a Paediatric Committee member(s) as
expert(s)
Source EMA databases Year o advice letter
Year o start o procedure
Table 6Paediatric clinical trials by year o authorisation
2005 2006 2007 2008 2009 2010 2011 2012
Paediatric trials
(number) 254 316 355 342 404 379 334 332
Paediatric trials
that are part of anagreed PIP 2 1 2 6 16 30 76 76
Proportion of
paediatric trials
that are part of an
agreed PIP among
paediatric trials 1 0 1 2 4 8 23 23
Total number
of trials (adults
and or children) 3 350 3 979 4 749 4 512 4 445 4 026 3 809 3 698
Proportion of
paediatric trials of
all trials 8 8 7 8 9 10 9 9
Source EudraCT Data Warehouse using a predefined query on 6 March 2013 and counting the first authorised trial only in the case o more thanone Member State This partial inormation requires sponsors to use a Clinical Trial Application orm that was only available rom November 2009 or use with version 8 o EudraCT
(available rom 2011)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2636
26
Table 7Number o children to be enrolled in clinical trials
Number
of subjects 2006 2007 2008 2009 2010 2011 2012
Pretermnewborns 0 0 0 207 82 2 281 1 712
Newborns 0 0 5 64 169 1 105 1 172
Infants and
toddlers 330 21 20 59 351 2 788 3 141
Children 2 142 181 200 2 230 2 055 10 325 20 677
Adolescents 368 111 205 1 577 2 861 9 054 13 193
Sum of
above 2 840 313 430 4 137 5 517 25 553 39 895
Reference
number of paediatric
trials 316 355 342 404 379 334 332
Source EudraCT Data Warehouse using a pre-defined query on 6 March 2013 modified by excluding studies or lsquoimmunological medicinal productsrsquo
Table 8EU budget contribution to the Paediatric Regulation and the EMA expenditure
0
1
2
3
4
5
6
7
8
9
10
2006 2007 2008 2009 2010 2011 2012
EU budget contribution (in Million euro)
EMA expenditure for paediatri cs (in Mill ion euro)
EMA expenditure for paediatr ics including support (in Million euro)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2736
27
Table 9Percentage o European Medicines Agencyrsquos human resources working in the paediatric area rom 2006 (inner
circle) to 2012 (outer circle)
733 (2012)
052 (2006)
Table 10Member States acting as rapporteurs or the assessment o studies submitted in accordance with Article 46
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE SE NL FR DK IT BE PL ES NO SK FI IE RO AT HU EL CZ PT LV BG
Study included in worksharing Rapporteur appointed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2836
28
Table 11Member States acting as rapporteur or the assessment o studies submitted in accordance with Article 45
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE NL DK AT FR PL SE ES IE CZ MT IT BE SI EE FI HU NO RO BG EL LV PT IS SK
Wave 1 Wave 2 Wave 3 Wave 4 Wave 5 Wave 6 Wave 7 Wave 8 Wave 9
Wave 10 Wave 11 Wave 12 Wave 13 Wave 14 Wave 15 Wave 16 Wave 17 Wave 18
Table 12Member States acting as rapporteurspeer reviewers in EMArsquos Paediatric Committee procedures (initial PIP
waiver or modification o an agreed PIP)
0
50
100
150
200
250
300
350
400
450
500
A u s t r i a
B el gi um
B ul g a r i a
C y pr u s
C z e c h R e p u b l i c
D enm a r k
E s t oni a
F i nl a n d
F r a n c e
G er m a n y
G r e e c e
H e a l t h c a r e a n d
A c a d emi a
H un g a r y
I c el a n d
I r el a n d
I t a l y
L a t vi a
L i t h u a ni a
L ux em b o ur g
M a l t a
N or w a y
P a t i en t s Or g a ni s a t i on
P ol a n d
P or t u g a l
R om a ni a
S l ov a k i a
S l ov eni a
S p a i n
S w e d en
T h eN e t h er l a n d
s
U ni t e d K i n g d om
Initial PIP applications PIP modifications
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2936
29
ANNEX II
Detailed inventory of centrally authorised medicinalproducts for paediatric use since the entry into force
of the Paediatric Regulation
Table 13Medicinal products authorised centrally since 2007 which include a paediatric indication
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Retapamulin Altargo 2007 No Mixed
Nelarabine Atriance 2007 No Mixed
Human papillomavirus vaccine[types 16 18] Cervarix 2007 No Mixed
Hydroxocobalamin Cyanokit 2007 No Mixed
Idursulase Elaprase 2007 No Mixed
Gadoversetamide Optimark 2007 No Mixed
Betaine anhydrous Cystadane 2007 No Mixed
Stiripentol Diacomit 2007 No Paediatric only
Mecasermin Increlex 2007 No Paediatric only
Rufinamide Inovelon 2007 No Mixed
Hydroxycarbamide Siklos 2007 No Mixed
Human normal
immunoglobulin (ivig) Flebogamma DIF 2007 No Mixed
Fluticasone uroate Avamys 2008 No Mixed
Human normal immunoglobulin Privigen 2008 No Mixed
Lacosamide Vimpat 2008 No Mixed
Micaungin Mycamine 2008 No Mixed
Sapropterin Kuvan 2008 No Mixed
Sugammadex Bridion 2008 No Mixed
Tocoersonal d-alpha
tocopheryl polyethylene glycol
succinate Vedrop 2009 No Paediatric only
Miamurtide Mepact 2009 No Mixed
Rilonacept Rilonacept Regeneron 2009 No Mixed
Tacrolimus Modigra 2009 No Mixed
Pneumoccocal polysaccharideconjugate vaccine (adsorbed) Synflorix 2009 No Paediatric only
Canakinumab
Ilaris (PIP not yet
completed) 2009 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3036
30
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Pneumoccocal polysaccharide
conjugate vaccine (13-valentadsorbed)
Prevenar 13 (PIP not yetcompleted) 2009 Yes Paediatric only
Meningococcal group a c
w135 and y conjugate vaccine Menveo 2010 Yes Mixed
Velaglucerase ala
Vpriv (PIP not yet
completed) 2010 Yes Mixed
Influenza vaccine (live
attenuated nasal) Fluenz (Waiver) 2011 Yes Paediatric only
C1 inhibitor human
Cinryze (PIP not yet
completed) 2011 Yes Mixed
Dihydroartemisinin
piperaquine phosphate
Eurartesim (PIP not yet
completed) 2011 Yes Mixed
Midazolam Buccolam 2011 Yes (PUMA) Paediatric only
EverolimusVotubia(PIP not yet completed) 2011 Yes Mixed
Tobramycin
Tobi Podhaler (PIP not
yet completed) 2011 Yes Mixed
Nomegestrol estradiol Ioa Zoely 2011 Yes Mixed
Colistimethate sodium Colobreathe 2012 Yes Mixed
Mercaptopurine Xaluprine 2012 No Mixed
Catridecacog NovoThirteen 2012 Yes MixedEavirenz Eavirenz Teva 2012 No Mixed
Ivacafor Kalydeco 2012 Yes Mixed
Desloratadine Desloratadine ratiopharm 2012 No Mixed
Desloratadine Desloratadine Actavis 2012 No Mixed
Perampanel Fycompa 2012 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3136
31
Table 14List o centrally authorised medicinal products or which the therapeutic indication was extended to or amend-
ed or the paediatric population
Active substance(s)
Trade
name Date Subject of the extension
Levetiracetam Keppra
2007
2009
Extension o the indication to include adjunctive ther-
apy in the treatment o primary generalised tonic-
clonic (PGTC) seizures in adults and adolescents rom
12 years o age with idiopathic generalised epilepsyExtension o indication to include the adjunctive
treatment o partial seizures with or without second-
ary generalisation in children rom 1 month to lt4
years old
Pneumococcal sac-
charide conjugated
vaccine adsorbed Prevenar 2007
Extension o the indication to include new inorma-
tion on efficacy against disease caused by Strepto-
coccus pneumoniae serotypes 4 6B 9V 14 18C 19F
and 23F in otitis mediaExtension o indication rom active immunisation
against bacteraemic pneumonia to active immunisa-
tion against pneumonia
Infliximab
Remi-
cade 2007
Extension o indication to include treatment o
severe active Crohnrsquos disease in children aged 6 to
17 years
Darbepoetin ala Aranesp 2007
Extension o indication or CRF patients whichrestricted the use o Nespo to paediatric subjects ge
11 years o age
Fosamprenavir Telzir 2007
Extension o indication o Telzir in combination withritonavir or the treatment o Human Immunodefi-
ciency Virus Type 1 (HIV-1) inected adults in combi-nation with other antiretroviral medicinal products to
include paediatric populations
Lamivudine zidovu-
dine Combivir 2007
Extension o indication to include paediatric patients
and replacement o film-coated tablets by scored
film-coated tablets
Desloratadine Aerius 2007Extension o indication rom lsquochronic idiopathic urti-cariarsquo to lsquourticariarsquo
Insulin glulisine Apidra 2007
Extension o indication to include 6 year olds and
older children based on the results o 2 paediatricstudies
Human papilloma virusvaccine [types 6 11
16 18] (recombinantadsorbed) Gardasil 2008
Extension o indication to include the prevention ohigh-grade vaginal dysplastic lesions (VaIN 23)
Adalimumab Humira 20082011
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in adoles-cents rom 13 to 17 years o age
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in the paedi-
atric population aged rom 4 to 12 years
Caspoungin Cancidas 2008
Extension o the indication to include the paediatric
population
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2236
22
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2336
23
ANNEX I
Figures and Tables
Table 1Agreed paediatric investigations plans (PIPs) 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Agreed PIPs submitted under Article 7 (without waivers)
Agreed PIPs submitted under Article 8 (without waivers)
Source EMA Paediatric database The numbers on agreed PIPs correspond to EMA decisions
Table 2Agreed paediatric investigations plans (PIPs) compared to ull waivers and modifications 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Submitted modifications of an agreed PIP
Agreed Full waivers
Source EMA Paediatric database The numbers on agreed PIPs and waivers correspond to EMA decisions
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2536
25
Table 5Scientific advice and protocol assistance including ollow-ups (provided by the EMA Scientific Advice Working
Party and the Committee or Human Medicinal Products per year)
259
277321
388 400 433 420
021 32
74 8057
91
0 0 0
68 8067
94
0
100
200
300
400
500
2006 2007 2008 2009 2010 2011 2012
Total number of advice (Scientific Advice and Protocol Assistance)
Sum of paediatric-only and mixed (adult and paediatric development questions)
advice
Paediatric-only or mixed advice that involved a Paediatric Committee member(s) as
expert(s)
Source EMA databases Year o advice letter
Year o start o procedure
Table 6Paediatric clinical trials by year o authorisation
2005 2006 2007 2008 2009 2010 2011 2012
Paediatric trials
(number) 254 316 355 342 404 379 334 332
Paediatric trials
that are part of anagreed PIP 2 1 2 6 16 30 76 76
Proportion of
paediatric trials
that are part of an
agreed PIP among
paediatric trials 1 0 1 2 4 8 23 23
Total number
of trials (adults
and or children) 3 350 3 979 4 749 4 512 4 445 4 026 3 809 3 698
Proportion of
paediatric trials of
all trials 8 8 7 8 9 10 9 9
Source EudraCT Data Warehouse using a predefined query on 6 March 2013 and counting the first authorised trial only in the case o more thanone Member State This partial inormation requires sponsors to use a Clinical Trial Application orm that was only available rom November 2009 or use with version 8 o EudraCT
(available rom 2011)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2636
26
Table 7Number o children to be enrolled in clinical trials
Number
of subjects 2006 2007 2008 2009 2010 2011 2012
Pretermnewborns 0 0 0 207 82 2 281 1 712
Newborns 0 0 5 64 169 1 105 1 172
Infants and
toddlers 330 21 20 59 351 2 788 3 141
Children 2 142 181 200 2 230 2 055 10 325 20 677
Adolescents 368 111 205 1 577 2 861 9 054 13 193
Sum of
above 2 840 313 430 4 137 5 517 25 553 39 895
Reference
number of paediatric
trials 316 355 342 404 379 334 332
Source EudraCT Data Warehouse using a pre-defined query on 6 March 2013 modified by excluding studies or lsquoimmunological medicinal productsrsquo
Table 8EU budget contribution to the Paediatric Regulation and the EMA expenditure
0
1
2
3
4
5
6
7
8
9
10
2006 2007 2008 2009 2010 2011 2012
EU budget contribution (in Million euro)
EMA expenditure for paediatri cs (in Mill ion euro)
EMA expenditure for paediatr ics including support (in Million euro)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2736
27
Table 9Percentage o European Medicines Agencyrsquos human resources working in the paediatric area rom 2006 (inner
circle) to 2012 (outer circle)
733 (2012)
052 (2006)
Table 10Member States acting as rapporteurs or the assessment o studies submitted in accordance with Article 46
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE SE NL FR DK IT BE PL ES NO SK FI IE RO AT HU EL CZ PT LV BG
Study included in worksharing Rapporteur appointed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2836
28
Table 11Member States acting as rapporteur or the assessment o studies submitted in accordance with Article 45
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE NL DK AT FR PL SE ES IE CZ MT IT BE SI EE FI HU NO RO BG EL LV PT IS SK
Wave 1 Wave 2 Wave 3 Wave 4 Wave 5 Wave 6 Wave 7 Wave 8 Wave 9
Wave 10 Wave 11 Wave 12 Wave 13 Wave 14 Wave 15 Wave 16 Wave 17 Wave 18
Table 12Member States acting as rapporteurspeer reviewers in EMArsquos Paediatric Committee procedures (initial PIP
waiver or modification o an agreed PIP)
0
50
100
150
200
250
300
350
400
450
500
A u s t r i a
B el gi um
B ul g a r i a
C y pr u s
C z e c h R e p u b l i c
D enm a r k
E s t oni a
F i nl a n d
F r a n c e
G er m a n y
G r e e c e
H e a l t h c a r e a n d
A c a d emi a
H un g a r y
I c el a n d
I r el a n d
I t a l y
L a t vi a
L i t h u a ni a
L ux em b o ur g
M a l t a
N or w a y
P a t i en t s Or g a ni s a t i on
P ol a n d
P or t u g a l
R om a ni a
S l ov a k i a
S l ov eni a
S p a i n
S w e d en
T h eN e t h er l a n d
s
U ni t e d K i n g d om
Initial PIP applications PIP modifications
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2936
29
ANNEX II
Detailed inventory of centrally authorised medicinalproducts for paediatric use since the entry into force
of the Paediatric Regulation
Table 13Medicinal products authorised centrally since 2007 which include a paediatric indication
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Retapamulin Altargo 2007 No Mixed
Nelarabine Atriance 2007 No Mixed
Human papillomavirus vaccine[types 16 18] Cervarix 2007 No Mixed
Hydroxocobalamin Cyanokit 2007 No Mixed
Idursulase Elaprase 2007 No Mixed
Gadoversetamide Optimark 2007 No Mixed
Betaine anhydrous Cystadane 2007 No Mixed
Stiripentol Diacomit 2007 No Paediatric only
Mecasermin Increlex 2007 No Paediatric only
Rufinamide Inovelon 2007 No Mixed
Hydroxycarbamide Siklos 2007 No Mixed
Human normal
immunoglobulin (ivig) Flebogamma DIF 2007 No Mixed
Fluticasone uroate Avamys 2008 No Mixed
Human normal immunoglobulin Privigen 2008 No Mixed
Lacosamide Vimpat 2008 No Mixed
Micaungin Mycamine 2008 No Mixed
Sapropterin Kuvan 2008 No Mixed
Sugammadex Bridion 2008 No Mixed
Tocoersonal d-alpha
tocopheryl polyethylene glycol
succinate Vedrop 2009 No Paediatric only
Miamurtide Mepact 2009 No Mixed
Rilonacept Rilonacept Regeneron 2009 No Mixed
Tacrolimus Modigra 2009 No Mixed
Pneumoccocal polysaccharideconjugate vaccine (adsorbed) Synflorix 2009 No Paediatric only
Canakinumab
Ilaris (PIP not yet
completed) 2009 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3036
30
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Pneumoccocal polysaccharide
conjugate vaccine (13-valentadsorbed)
Prevenar 13 (PIP not yetcompleted) 2009 Yes Paediatric only
Meningococcal group a c
w135 and y conjugate vaccine Menveo 2010 Yes Mixed
Velaglucerase ala
Vpriv (PIP not yet
completed) 2010 Yes Mixed
Influenza vaccine (live
attenuated nasal) Fluenz (Waiver) 2011 Yes Paediatric only
C1 inhibitor human
Cinryze (PIP not yet
completed) 2011 Yes Mixed
Dihydroartemisinin
piperaquine phosphate
Eurartesim (PIP not yet
completed) 2011 Yes Mixed
Midazolam Buccolam 2011 Yes (PUMA) Paediatric only
EverolimusVotubia(PIP not yet completed) 2011 Yes Mixed
Tobramycin
Tobi Podhaler (PIP not
yet completed) 2011 Yes Mixed
Nomegestrol estradiol Ioa Zoely 2011 Yes Mixed
Colistimethate sodium Colobreathe 2012 Yes Mixed
Mercaptopurine Xaluprine 2012 No Mixed
Catridecacog NovoThirteen 2012 Yes MixedEavirenz Eavirenz Teva 2012 No Mixed
Ivacafor Kalydeco 2012 Yes Mixed
Desloratadine Desloratadine ratiopharm 2012 No Mixed
Desloratadine Desloratadine Actavis 2012 No Mixed
Perampanel Fycompa 2012 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3136
31
Table 14List o centrally authorised medicinal products or which the therapeutic indication was extended to or amend-
ed or the paediatric population
Active substance(s)
Trade
name Date Subject of the extension
Levetiracetam Keppra
2007
2009
Extension o the indication to include adjunctive ther-
apy in the treatment o primary generalised tonic-
clonic (PGTC) seizures in adults and adolescents rom
12 years o age with idiopathic generalised epilepsyExtension o indication to include the adjunctive
treatment o partial seizures with or without second-
ary generalisation in children rom 1 month to lt4
years old
Pneumococcal sac-
charide conjugated
vaccine adsorbed Prevenar 2007
Extension o the indication to include new inorma-
tion on efficacy against disease caused by Strepto-
coccus pneumoniae serotypes 4 6B 9V 14 18C 19F
and 23F in otitis mediaExtension o indication rom active immunisation
against bacteraemic pneumonia to active immunisa-
tion against pneumonia
Infliximab
Remi-
cade 2007
Extension o indication to include treatment o
severe active Crohnrsquos disease in children aged 6 to
17 years
Darbepoetin ala Aranesp 2007
Extension o indication or CRF patients whichrestricted the use o Nespo to paediatric subjects ge
11 years o age
Fosamprenavir Telzir 2007
Extension o indication o Telzir in combination withritonavir or the treatment o Human Immunodefi-
ciency Virus Type 1 (HIV-1) inected adults in combi-nation with other antiretroviral medicinal products to
include paediatric populations
Lamivudine zidovu-
dine Combivir 2007
Extension o indication to include paediatric patients
and replacement o film-coated tablets by scored
film-coated tablets
Desloratadine Aerius 2007Extension o indication rom lsquochronic idiopathic urti-cariarsquo to lsquourticariarsquo
Insulin glulisine Apidra 2007
Extension o indication to include 6 year olds and
older children based on the results o 2 paediatricstudies
Human papilloma virusvaccine [types 6 11
16 18] (recombinantadsorbed) Gardasil 2008
Extension o indication to include the prevention ohigh-grade vaginal dysplastic lesions (VaIN 23)
Adalimumab Humira 20082011
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in adoles-cents rom 13 to 17 years o age
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in the paedi-
atric population aged rom 4 to 12 years
Caspoungin Cancidas 2008
Extension o the indication to include the paediatric
population
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2336
23
ANNEX I
Figures and Tables
Table 1Agreed paediatric investigations plans (PIPs) 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Agreed PIPs submitted under Article 7 (without waivers)
Agreed PIPs submitted under Article 8 (without waivers)
Source EMA Paediatric database The numbers on agreed PIPs correspond to EMA decisions
Table 2Agreed paediatric investigations plans (PIPs) compared to ull waivers and modifications 2007-2012
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012
Agreed PIPs (total number)
Submitted modifications of an agreed PIP
Agreed Full waivers
Source EMA Paediatric database The numbers on agreed PIPs and waivers correspond to EMA decisions
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2536
25
Table 5Scientific advice and protocol assistance including ollow-ups (provided by the EMA Scientific Advice Working
Party and the Committee or Human Medicinal Products per year)
259
277321
388 400 433 420
021 32
74 8057
91
0 0 0
68 8067
94
0
100
200
300
400
500
2006 2007 2008 2009 2010 2011 2012
Total number of advice (Scientific Advice and Protocol Assistance)
Sum of paediatric-only and mixed (adult and paediatric development questions)
advice
Paediatric-only or mixed advice that involved a Paediatric Committee member(s) as
expert(s)
Source EMA databases Year o advice letter
Year o start o procedure
Table 6Paediatric clinical trials by year o authorisation
2005 2006 2007 2008 2009 2010 2011 2012
Paediatric trials
(number) 254 316 355 342 404 379 334 332
Paediatric trials
that are part of anagreed PIP 2 1 2 6 16 30 76 76
Proportion of
paediatric trials
that are part of an
agreed PIP among
paediatric trials 1 0 1 2 4 8 23 23
Total number
of trials (adults
and or children) 3 350 3 979 4 749 4 512 4 445 4 026 3 809 3 698
Proportion of
paediatric trials of
all trials 8 8 7 8 9 10 9 9
Source EudraCT Data Warehouse using a predefined query on 6 March 2013 and counting the first authorised trial only in the case o more thanone Member State This partial inormation requires sponsors to use a Clinical Trial Application orm that was only available rom November 2009 or use with version 8 o EudraCT
(available rom 2011)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2636
26
Table 7Number o children to be enrolled in clinical trials
Number
of subjects 2006 2007 2008 2009 2010 2011 2012
Pretermnewborns 0 0 0 207 82 2 281 1 712
Newborns 0 0 5 64 169 1 105 1 172
Infants and
toddlers 330 21 20 59 351 2 788 3 141
Children 2 142 181 200 2 230 2 055 10 325 20 677
Adolescents 368 111 205 1 577 2 861 9 054 13 193
Sum of
above 2 840 313 430 4 137 5 517 25 553 39 895
Reference
number of paediatric
trials 316 355 342 404 379 334 332
Source EudraCT Data Warehouse using a pre-defined query on 6 March 2013 modified by excluding studies or lsquoimmunological medicinal productsrsquo
Table 8EU budget contribution to the Paediatric Regulation and the EMA expenditure
0
1
2
3
4
5
6
7
8
9
10
2006 2007 2008 2009 2010 2011 2012
EU budget contribution (in Million euro)
EMA expenditure for paediatri cs (in Mill ion euro)
EMA expenditure for paediatr ics including support (in Million euro)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2736
27
Table 9Percentage o European Medicines Agencyrsquos human resources working in the paediatric area rom 2006 (inner
circle) to 2012 (outer circle)
733 (2012)
052 (2006)
Table 10Member States acting as rapporteurs or the assessment o studies submitted in accordance with Article 46
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE SE NL FR DK IT BE PL ES NO SK FI IE RO AT HU EL CZ PT LV BG
Study included in worksharing Rapporteur appointed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2836
28
Table 11Member States acting as rapporteur or the assessment o studies submitted in accordance with Article 45
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE NL DK AT FR PL SE ES IE CZ MT IT BE SI EE FI HU NO RO BG EL LV PT IS SK
Wave 1 Wave 2 Wave 3 Wave 4 Wave 5 Wave 6 Wave 7 Wave 8 Wave 9
Wave 10 Wave 11 Wave 12 Wave 13 Wave 14 Wave 15 Wave 16 Wave 17 Wave 18
Table 12Member States acting as rapporteurspeer reviewers in EMArsquos Paediatric Committee procedures (initial PIP
waiver or modification o an agreed PIP)
0
50
100
150
200
250
300
350
400
450
500
A u s t r i a
B el gi um
B ul g a r i a
C y pr u s
C z e c h R e p u b l i c
D enm a r k
E s t oni a
F i nl a n d
F r a n c e
G er m a n y
G r e e c e
H e a l t h c a r e a n d
A c a d emi a
H un g a r y
I c el a n d
I r el a n d
I t a l y
L a t vi a
L i t h u a ni a
L ux em b o ur g
M a l t a
N or w a y
P a t i en t s Or g a ni s a t i on
P ol a n d
P or t u g a l
R om a ni a
S l ov a k i a
S l ov eni a
S p a i n
S w e d en
T h eN e t h er l a n d
s
U ni t e d K i n g d om
Initial PIP applications PIP modifications
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2936
29
ANNEX II
Detailed inventory of centrally authorised medicinalproducts for paediatric use since the entry into force
of the Paediatric Regulation
Table 13Medicinal products authorised centrally since 2007 which include a paediatric indication
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Retapamulin Altargo 2007 No Mixed
Nelarabine Atriance 2007 No Mixed
Human papillomavirus vaccine[types 16 18] Cervarix 2007 No Mixed
Hydroxocobalamin Cyanokit 2007 No Mixed
Idursulase Elaprase 2007 No Mixed
Gadoversetamide Optimark 2007 No Mixed
Betaine anhydrous Cystadane 2007 No Mixed
Stiripentol Diacomit 2007 No Paediatric only
Mecasermin Increlex 2007 No Paediatric only
Rufinamide Inovelon 2007 No Mixed
Hydroxycarbamide Siklos 2007 No Mixed
Human normal
immunoglobulin (ivig) Flebogamma DIF 2007 No Mixed
Fluticasone uroate Avamys 2008 No Mixed
Human normal immunoglobulin Privigen 2008 No Mixed
Lacosamide Vimpat 2008 No Mixed
Micaungin Mycamine 2008 No Mixed
Sapropterin Kuvan 2008 No Mixed
Sugammadex Bridion 2008 No Mixed
Tocoersonal d-alpha
tocopheryl polyethylene glycol
succinate Vedrop 2009 No Paediatric only
Miamurtide Mepact 2009 No Mixed
Rilonacept Rilonacept Regeneron 2009 No Mixed
Tacrolimus Modigra 2009 No Mixed
Pneumoccocal polysaccharideconjugate vaccine (adsorbed) Synflorix 2009 No Paediatric only
Canakinumab
Ilaris (PIP not yet
completed) 2009 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3036
30
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Pneumoccocal polysaccharide
conjugate vaccine (13-valentadsorbed)
Prevenar 13 (PIP not yetcompleted) 2009 Yes Paediatric only
Meningococcal group a c
w135 and y conjugate vaccine Menveo 2010 Yes Mixed
Velaglucerase ala
Vpriv (PIP not yet
completed) 2010 Yes Mixed
Influenza vaccine (live
attenuated nasal) Fluenz (Waiver) 2011 Yes Paediatric only
C1 inhibitor human
Cinryze (PIP not yet
completed) 2011 Yes Mixed
Dihydroartemisinin
piperaquine phosphate
Eurartesim (PIP not yet
completed) 2011 Yes Mixed
Midazolam Buccolam 2011 Yes (PUMA) Paediatric only
EverolimusVotubia(PIP not yet completed) 2011 Yes Mixed
Tobramycin
Tobi Podhaler (PIP not
yet completed) 2011 Yes Mixed
Nomegestrol estradiol Ioa Zoely 2011 Yes Mixed
Colistimethate sodium Colobreathe 2012 Yes Mixed
Mercaptopurine Xaluprine 2012 No Mixed
Catridecacog NovoThirteen 2012 Yes MixedEavirenz Eavirenz Teva 2012 No Mixed
Ivacafor Kalydeco 2012 Yes Mixed
Desloratadine Desloratadine ratiopharm 2012 No Mixed
Desloratadine Desloratadine Actavis 2012 No Mixed
Perampanel Fycompa 2012 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3136
31
Table 14List o centrally authorised medicinal products or which the therapeutic indication was extended to or amend-
ed or the paediatric population
Active substance(s)
Trade
name Date Subject of the extension
Levetiracetam Keppra
2007
2009
Extension o the indication to include adjunctive ther-
apy in the treatment o primary generalised tonic-
clonic (PGTC) seizures in adults and adolescents rom
12 years o age with idiopathic generalised epilepsyExtension o indication to include the adjunctive
treatment o partial seizures with or without second-
ary generalisation in children rom 1 month to lt4
years old
Pneumococcal sac-
charide conjugated
vaccine adsorbed Prevenar 2007
Extension o the indication to include new inorma-
tion on efficacy against disease caused by Strepto-
coccus pneumoniae serotypes 4 6B 9V 14 18C 19F
and 23F in otitis mediaExtension o indication rom active immunisation
against bacteraemic pneumonia to active immunisa-
tion against pneumonia
Infliximab
Remi-
cade 2007
Extension o indication to include treatment o
severe active Crohnrsquos disease in children aged 6 to
17 years
Darbepoetin ala Aranesp 2007
Extension o indication or CRF patients whichrestricted the use o Nespo to paediatric subjects ge
11 years o age
Fosamprenavir Telzir 2007
Extension o indication o Telzir in combination withritonavir or the treatment o Human Immunodefi-
ciency Virus Type 1 (HIV-1) inected adults in combi-nation with other antiretroviral medicinal products to
include paediatric populations
Lamivudine zidovu-
dine Combivir 2007
Extension o indication to include paediatric patients
and replacement o film-coated tablets by scored
film-coated tablets
Desloratadine Aerius 2007Extension o indication rom lsquochronic idiopathic urti-cariarsquo to lsquourticariarsquo
Insulin glulisine Apidra 2007
Extension o indication to include 6 year olds and
older children based on the results o 2 paediatricstudies
Human papilloma virusvaccine [types 6 11
16 18] (recombinantadsorbed) Gardasil 2008
Extension o indication to include the prevention ohigh-grade vaginal dysplastic lesions (VaIN 23)
Adalimumab Humira 20082011
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in adoles-cents rom 13 to 17 years o age
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in the paedi-
atric population aged rom 4 to 12 years
Caspoungin Cancidas 2008
Extension o the indication to include the paediatric
population
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2536
25
Table 5Scientific advice and protocol assistance including ollow-ups (provided by the EMA Scientific Advice Working
Party and the Committee or Human Medicinal Products per year)
259
277321
388 400 433 420
021 32
74 8057
91
0 0 0
68 8067
94
0
100
200
300
400
500
2006 2007 2008 2009 2010 2011 2012
Total number of advice (Scientific Advice and Protocol Assistance)
Sum of paediatric-only and mixed (adult and paediatric development questions)
advice
Paediatric-only or mixed advice that involved a Paediatric Committee member(s) as
expert(s)
Source EMA databases Year o advice letter
Year o start o procedure
Table 6Paediatric clinical trials by year o authorisation
2005 2006 2007 2008 2009 2010 2011 2012
Paediatric trials
(number) 254 316 355 342 404 379 334 332
Paediatric trials
that are part of anagreed PIP 2 1 2 6 16 30 76 76
Proportion of
paediatric trials
that are part of an
agreed PIP among
paediatric trials 1 0 1 2 4 8 23 23
Total number
of trials (adults
and or children) 3 350 3 979 4 749 4 512 4 445 4 026 3 809 3 698
Proportion of
paediatric trials of
all trials 8 8 7 8 9 10 9 9
Source EudraCT Data Warehouse using a predefined query on 6 March 2013 and counting the first authorised trial only in the case o more thanone Member State This partial inormation requires sponsors to use a Clinical Trial Application orm that was only available rom November 2009 or use with version 8 o EudraCT
(available rom 2011)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2636
26
Table 7Number o children to be enrolled in clinical trials
Number
of subjects 2006 2007 2008 2009 2010 2011 2012
Pretermnewborns 0 0 0 207 82 2 281 1 712
Newborns 0 0 5 64 169 1 105 1 172
Infants and
toddlers 330 21 20 59 351 2 788 3 141
Children 2 142 181 200 2 230 2 055 10 325 20 677
Adolescents 368 111 205 1 577 2 861 9 054 13 193
Sum of
above 2 840 313 430 4 137 5 517 25 553 39 895
Reference
number of paediatric
trials 316 355 342 404 379 334 332
Source EudraCT Data Warehouse using a pre-defined query on 6 March 2013 modified by excluding studies or lsquoimmunological medicinal productsrsquo
Table 8EU budget contribution to the Paediatric Regulation and the EMA expenditure
0
1
2
3
4
5
6
7
8
9
10
2006 2007 2008 2009 2010 2011 2012
EU budget contribution (in Million euro)
EMA expenditure for paediatri cs (in Mill ion euro)
EMA expenditure for paediatr ics including support (in Million euro)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2736
27
Table 9Percentage o European Medicines Agencyrsquos human resources working in the paediatric area rom 2006 (inner
circle) to 2012 (outer circle)
733 (2012)
052 (2006)
Table 10Member States acting as rapporteurs or the assessment o studies submitted in accordance with Article 46
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE SE NL FR DK IT BE PL ES NO SK FI IE RO AT HU EL CZ PT LV BG
Study included in worksharing Rapporteur appointed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2836
28
Table 11Member States acting as rapporteur or the assessment o studies submitted in accordance with Article 45
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE NL DK AT FR PL SE ES IE CZ MT IT BE SI EE FI HU NO RO BG EL LV PT IS SK
Wave 1 Wave 2 Wave 3 Wave 4 Wave 5 Wave 6 Wave 7 Wave 8 Wave 9
Wave 10 Wave 11 Wave 12 Wave 13 Wave 14 Wave 15 Wave 16 Wave 17 Wave 18
Table 12Member States acting as rapporteurspeer reviewers in EMArsquos Paediatric Committee procedures (initial PIP
waiver or modification o an agreed PIP)
0
50
100
150
200
250
300
350
400
450
500
A u s t r i a
B el gi um
B ul g a r i a
C y pr u s
C z e c h R e p u b l i c
D enm a r k
E s t oni a
F i nl a n d
F r a n c e
G er m a n y
G r e e c e
H e a l t h c a r e a n d
A c a d emi a
H un g a r y
I c el a n d
I r el a n d
I t a l y
L a t vi a
L i t h u a ni a
L ux em b o ur g
M a l t a
N or w a y
P a t i en t s Or g a ni s a t i on
P ol a n d
P or t u g a l
R om a ni a
S l ov a k i a
S l ov eni a
S p a i n
S w e d en
T h eN e t h er l a n d
s
U ni t e d K i n g d om
Initial PIP applications PIP modifications
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2936
29
ANNEX II
Detailed inventory of centrally authorised medicinalproducts for paediatric use since the entry into force
of the Paediatric Regulation
Table 13Medicinal products authorised centrally since 2007 which include a paediatric indication
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Retapamulin Altargo 2007 No Mixed
Nelarabine Atriance 2007 No Mixed
Human papillomavirus vaccine[types 16 18] Cervarix 2007 No Mixed
Hydroxocobalamin Cyanokit 2007 No Mixed
Idursulase Elaprase 2007 No Mixed
Gadoversetamide Optimark 2007 No Mixed
Betaine anhydrous Cystadane 2007 No Mixed
Stiripentol Diacomit 2007 No Paediatric only
Mecasermin Increlex 2007 No Paediatric only
Rufinamide Inovelon 2007 No Mixed
Hydroxycarbamide Siklos 2007 No Mixed
Human normal
immunoglobulin (ivig) Flebogamma DIF 2007 No Mixed
Fluticasone uroate Avamys 2008 No Mixed
Human normal immunoglobulin Privigen 2008 No Mixed
Lacosamide Vimpat 2008 No Mixed
Micaungin Mycamine 2008 No Mixed
Sapropterin Kuvan 2008 No Mixed
Sugammadex Bridion 2008 No Mixed
Tocoersonal d-alpha
tocopheryl polyethylene glycol
succinate Vedrop 2009 No Paediatric only
Miamurtide Mepact 2009 No Mixed
Rilonacept Rilonacept Regeneron 2009 No Mixed
Tacrolimus Modigra 2009 No Mixed
Pneumoccocal polysaccharideconjugate vaccine (adsorbed) Synflorix 2009 No Paediatric only
Canakinumab
Ilaris (PIP not yet
completed) 2009 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3036
30
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Pneumoccocal polysaccharide
conjugate vaccine (13-valentadsorbed)
Prevenar 13 (PIP not yetcompleted) 2009 Yes Paediatric only
Meningococcal group a c
w135 and y conjugate vaccine Menveo 2010 Yes Mixed
Velaglucerase ala
Vpriv (PIP not yet
completed) 2010 Yes Mixed
Influenza vaccine (live
attenuated nasal) Fluenz (Waiver) 2011 Yes Paediatric only
C1 inhibitor human
Cinryze (PIP not yet
completed) 2011 Yes Mixed
Dihydroartemisinin
piperaquine phosphate
Eurartesim (PIP not yet
completed) 2011 Yes Mixed
Midazolam Buccolam 2011 Yes (PUMA) Paediatric only
EverolimusVotubia(PIP not yet completed) 2011 Yes Mixed
Tobramycin
Tobi Podhaler (PIP not
yet completed) 2011 Yes Mixed
Nomegestrol estradiol Ioa Zoely 2011 Yes Mixed
Colistimethate sodium Colobreathe 2012 Yes Mixed
Mercaptopurine Xaluprine 2012 No Mixed
Catridecacog NovoThirteen 2012 Yes MixedEavirenz Eavirenz Teva 2012 No Mixed
Ivacafor Kalydeco 2012 Yes Mixed
Desloratadine Desloratadine ratiopharm 2012 No Mixed
Desloratadine Desloratadine Actavis 2012 No Mixed
Perampanel Fycompa 2012 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3136
31
Table 14List o centrally authorised medicinal products or which the therapeutic indication was extended to or amend-
ed or the paediatric population
Active substance(s)
Trade
name Date Subject of the extension
Levetiracetam Keppra
2007
2009
Extension o the indication to include adjunctive ther-
apy in the treatment o primary generalised tonic-
clonic (PGTC) seizures in adults and adolescents rom
12 years o age with idiopathic generalised epilepsyExtension o indication to include the adjunctive
treatment o partial seizures with or without second-
ary generalisation in children rom 1 month to lt4
years old
Pneumococcal sac-
charide conjugated
vaccine adsorbed Prevenar 2007
Extension o the indication to include new inorma-
tion on efficacy against disease caused by Strepto-
coccus pneumoniae serotypes 4 6B 9V 14 18C 19F
and 23F in otitis mediaExtension o indication rom active immunisation
against bacteraemic pneumonia to active immunisa-
tion against pneumonia
Infliximab
Remi-
cade 2007
Extension o indication to include treatment o
severe active Crohnrsquos disease in children aged 6 to
17 years
Darbepoetin ala Aranesp 2007
Extension o indication or CRF patients whichrestricted the use o Nespo to paediatric subjects ge
11 years o age
Fosamprenavir Telzir 2007
Extension o indication o Telzir in combination withritonavir or the treatment o Human Immunodefi-
ciency Virus Type 1 (HIV-1) inected adults in combi-nation with other antiretroviral medicinal products to
include paediatric populations
Lamivudine zidovu-
dine Combivir 2007
Extension o indication to include paediatric patients
and replacement o film-coated tablets by scored
film-coated tablets
Desloratadine Aerius 2007Extension o indication rom lsquochronic idiopathic urti-cariarsquo to lsquourticariarsquo
Insulin glulisine Apidra 2007
Extension o indication to include 6 year olds and
older children based on the results o 2 paediatricstudies
Human papilloma virusvaccine [types 6 11
16 18] (recombinantadsorbed) Gardasil 2008
Extension o indication to include the prevention ohigh-grade vaginal dysplastic lesions (VaIN 23)
Adalimumab Humira 20082011
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in adoles-cents rom 13 to 17 years o age
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in the paedi-
atric population aged rom 4 to 12 years
Caspoungin Cancidas 2008
Extension o the indication to include the paediatric
population
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2536
25
Table 5Scientific advice and protocol assistance including ollow-ups (provided by the EMA Scientific Advice Working
Party and the Committee or Human Medicinal Products per year)
259
277321
388 400 433 420
021 32
74 8057
91
0 0 0
68 8067
94
0
100
200
300
400
500
2006 2007 2008 2009 2010 2011 2012
Total number of advice (Scientific Advice and Protocol Assistance)
Sum of paediatric-only and mixed (adult and paediatric development questions)
advice
Paediatric-only or mixed advice that involved a Paediatric Committee member(s) as
expert(s)
Source EMA databases Year o advice letter
Year o start o procedure
Table 6Paediatric clinical trials by year o authorisation
2005 2006 2007 2008 2009 2010 2011 2012
Paediatric trials
(number) 254 316 355 342 404 379 334 332
Paediatric trials
that are part of anagreed PIP 2 1 2 6 16 30 76 76
Proportion of
paediatric trials
that are part of an
agreed PIP among
paediatric trials 1 0 1 2 4 8 23 23
Total number
of trials (adults
and or children) 3 350 3 979 4 749 4 512 4 445 4 026 3 809 3 698
Proportion of
paediatric trials of
all trials 8 8 7 8 9 10 9 9
Source EudraCT Data Warehouse using a predefined query on 6 March 2013 and counting the first authorised trial only in the case o more thanone Member State This partial inormation requires sponsors to use a Clinical Trial Application orm that was only available rom November 2009 or use with version 8 o EudraCT
(available rom 2011)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2636
26
Table 7Number o children to be enrolled in clinical trials
Number
of subjects 2006 2007 2008 2009 2010 2011 2012
Pretermnewborns 0 0 0 207 82 2 281 1 712
Newborns 0 0 5 64 169 1 105 1 172
Infants and
toddlers 330 21 20 59 351 2 788 3 141
Children 2 142 181 200 2 230 2 055 10 325 20 677
Adolescents 368 111 205 1 577 2 861 9 054 13 193
Sum of
above 2 840 313 430 4 137 5 517 25 553 39 895
Reference
number of paediatric
trials 316 355 342 404 379 334 332
Source EudraCT Data Warehouse using a pre-defined query on 6 March 2013 modified by excluding studies or lsquoimmunological medicinal productsrsquo
Table 8EU budget contribution to the Paediatric Regulation and the EMA expenditure
0
1
2
3
4
5
6
7
8
9
10
2006 2007 2008 2009 2010 2011 2012
EU budget contribution (in Million euro)
EMA expenditure for paediatri cs (in Mill ion euro)
EMA expenditure for paediatr ics including support (in Million euro)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2736
27
Table 9Percentage o European Medicines Agencyrsquos human resources working in the paediatric area rom 2006 (inner
circle) to 2012 (outer circle)
733 (2012)
052 (2006)
Table 10Member States acting as rapporteurs or the assessment o studies submitted in accordance with Article 46
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE SE NL FR DK IT BE PL ES NO SK FI IE RO AT HU EL CZ PT LV BG
Study included in worksharing Rapporteur appointed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2836
28
Table 11Member States acting as rapporteur or the assessment o studies submitted in accordance with Article 45
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE NL DK AT FR PL SE ES IE CZ MT IT BE SI EE FI HU NO RO BG EL LV PT IS SK
Wave 1 Wave 2 Wave 3 Wave 4 Wave 5 Wave 6 Wave 7 Wave 8 Wave 9
Wave 10 Wave 11 Wave 12 Wave 13 Wave 14 Wave 15 Wave 16 Wave 17 Wave 18
Table 12Member States acting as rapporteurspeer reviewers in EMArsquos Paediatric Committee procedures (initial PIP
waiver or modification o an agreed PIP)
0
50
100
150
200
250
300
350
400
450
500
A u s t r i a
B el gi um
B ul g a r i a
C y pr u s
C z e c h R e p u b l i c
D enm a r k
E s t oni a
F i nl a n d
F r a n c e
G er m a n y
G r e e c e
H e a l t h c a r e a n d
A c a d emi a
H un g a r y
I c el a n d
I r el a n d
I t a l y
L a t vi a
L i t h u a ni a
L ux em b o ur g
M a l t a
N or w a y
P a t i en t s Or g a ni s a t i on
P ol a n d
P or t u g a l
R om a ni a
S l ov a k i a
S l ov eni a
S p a i n
S w e d en
T h eN e t h er l a n d
s
U ni t e d K i n g d om
Initial PIP applications PIP modifications
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2936
29
ANNEX II
Detailed inventory of centrally authorised medicinalproducts for paediatric use since the entry into force
of the Paediatric Regulation
Table 13Medicinal products authorised centrally since 2007 which include a paediatric indication
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Retapamulin Altargo 2007 No Mixed
Nelarabine Atriance 2007 No Mixed
Human papillomavirus vaccine[types 16 18] Cervarix 2007 No Mixed
Hydroxocobalamin Cyanokit 2007 No Mixed
Idursulase Elaprase 2007 No Mixed
Gadoversetamide Optimark 2007 No Mixed
Betaine anhydrous Cystadane 2007 No Mixed
Stiripentol Diacomit 2007 No Paediatric only
Mecasermin Increlex 2007 No Paediatric only
Rufinamide Inovelon 2007 No Mixed
Hydroxycarbamide Siklos 2007 No Mixed
Human normal
immunoglobulin (ivig) Flebogamma DIF 2007 No Mixed
Fluticasone uroate Avamys 2008 No Mixed
Human normal immunoglobulin Privigen 2008 No Mixed
Lacosamide Vimpat 2008 No Mixed
Micaungin Mycamine 2008 No Mixed
Sapropterin Kuvan 2008 No Mixed
Sugammadex Bridion 2008 No Mixed
Tocoersonal d-alpha
tocopheryl polyethylene glycol
succinate Vedrop 2009 No Paediatric only
Miamurtide Mepact 2009 No Mixed
Rilonacept Rilonacept Regeneron 2009 No Mixed
Tacrolimus Modigra 2009 No Mixed
Pneumoccocal polysaccharideconjugate vaccine (adsorbed) Synflorix 2009 No Paediatric only
Canakinumab
Ilaris (PIP not yet
completed) 2009 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3036
30
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Pneumoccocal polysaccharide
conjugate vaccine (13-valentadsorbed)
Prevenar 13 (PIP not yetcompleted) 2009 Yes Paediatric only
Meningococcal group a c
w135 and y conjugate vaccine Menveo 2010 Yes Mixed
Velaglucerase ala
Vpriv (PIP not yet
completed) 2010 Yes Mixed
Influenza vaccine (live
attenuated nasal) Fluenz (Waiver) 2011 Yes Paediatric only
C1 inhibitor human
Cinryze (PIP not yet
completed) 2011 Yes Mixed
Dihydroartemisinin
piperaquine phosphate
Eurartesim (PIP not yet
completed) 2011 Yes Mixed
Midazolam Buccolam 2011 Yes (PUMA) Paediatric only
EverolimusVotubia(PIP not yet completed) 2011 Yes Mixed
Tobramycin
Tobi Podhaler (PIP not
yet completed) 2011 Yes Mixed
Nomegestrol estradiol Ioa Zoely 2011 Yes Mixed
Colistimethate sodium Colobreathe 2012 Yes Mixed
Mercaptopurine Xaluprine 2012 No Mixed
Catridecacog NovoThirteen 2012 Yes MixedEavirenz Eavirenz Teva 2012 No Mixed
Ivacafor Kalydeco 2012 Yes Mixed
Desloratadine Desloratadine ratiopharm 2012 No Mixed
Desloratadine Desloratadine Actavis 2012 No Mixed
Perampanel Fycompa 2012 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3136
31
Table 14List o centrally authorised medicinal products or which the therapeutic indication was extended to or amend-
ed or the paediatric population
Active substance(s)
Trade
name Date Subject of the extension
Levetiracetam Keppra
2007
2009
Extension o the indication to include adjunctive ther-
apy in the treatment o primary generalised tonic-
clonic (PGTC) seizures in adults and adolescents rom
12 years o age with idiopathic generalised epilepsyExtension o indication to include the adjunctive
treatment o partial seizures with or without second-
ary generalisation in children rom 1 month to lt4
years old
Pneumococcal sac-
charide conjugated
vaccine adsorbed Prevenar 2007
Extension o the indication to include new inorma-
tion on efficacy against disease caused by Strepto-
coccus pneumoniae serotypes 4 6B 9V 14 18C 19F
and 23F in otitis mediaExtension o indication rom active immunisation
against bacteraemic pneumonia to active immunisa-
tion against pneumonia
Infliximab
Remi-
cade 2007
Extension o indication to include treatment o
severe active Crohnrsquos disease in children aged 6 to
17 years
Darbepoetin ala Aranesp 2007
Extension o indication or CRF patients whichrestricted the use o Nespo to paediatric subjects ge
11 years o age
Fosamprenavir Telzir 2007
Extension o indication o Telzir in combination withritonavir or the treatment o Human Immunodefi-
ciency Virus Type 1 (HIV-1) inected adults in combi-nation with other antiretroviral medicinal products to
include paediatric populations
Lamivudine zidovu-
dine Combivir 2007
Extension o indication to include paediatric patients
and replacement o film-coated tablets by scored
film-coated tablets
Desloratadine Aerius 2007Extension o indication rom lsquochronic idiopathic urti-cariarsquo to lsquourticariarsquo
Insulin glulisine Apidra 2007
Extension o indication to include 6 year olds and
older children based on the results o 2 paediatricstudies
Human papilloma virusvaccine [types 6 11
16 18] (recombinantadsorbed) Gardasil 2008
Extension o indication to include the prevention ohigh-grade vaginal dysplastic lesions (VaIN 23)
Adalimumab Humira 20082011
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in adoles-cents rom 13 to 17 years o age
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in the paedi-
atric population aged rom 4 to 12 years
Caspoungin Cancidas 2008
Extension o the indication to include the paediatric
population
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2636
26
Table 7Number o children to be enrolled in clinical trials
Number
of subjects 2006 2007 2008 2009 2010 2011 2012
Pretermnewborns 0 0 0 207 82 2 281 1 712
Newborns 0 0 5 64 169 1 105 1 172
Infants and
toddlers 330 21 20 59 351 2 788 3 141
Children 2 142 181 200 2 230 2 055 10 325 20 677
Adolescents 368 111 205 1 577 2 861 9 054 13 193
Sum of
above 2 840 313 430 4 137 5 517 25 553 39 895
Reference
number of paediatric
trials 316 355 342 404 379 334 332
Source EudraCT Data Warehouse using a pre-defined query on 6 March 2013 modified by excluding studies or lsquoimmunological medicinal productsrsquo
Table 8EU budget contribution to the Paediatric Regulation and the EMA expenditure
0
1
2
3
4
5
6
7
8
9
10
2006 2007 2008 2009 2010 2011 2012
EU budget contribution (in Million euro)
EMA expenditure for paediatri cs (in Mill ion euro)
EMA expenditure for paediatr ics including support (in Million euro)
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2736
27
Table 9Percentage o European Medicines Agencyrsquos human resources working in the paediatric area rom 2006 (inner
circle) to 2012 (outer circle)
733 (2012)
052 (2006)
Table 10Member States acting as rapporteurs or the assessment o studies submitted in accordance with Article 46
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE SE NL FR DK IT BE PL ES NO SK FI IE RO AT HU EL CZ PT LV BG
Study included in worksharing Rapporteur appointed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2836
28
Table 11Member States acting as rapporteur or the assessment o studies submitted in accordance with Article 45
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE NL DK AT FR PL SE ES IE CZ MT IT BE SI EE FI HU NO RO BG EL LV PT IS SK
Wave 1 Wave 2 Wave 3 Wave 4 Wave 5 Wave 6 Wave 7 Wave 8 Wave 9
Wave 10 Wave 11 Wave 12 Wave 13 Wave 14 Wave 15 Wave 16 Wave 17 Wave 18
Table 12Member States acting as rapporteurspeer reviewers in EMArsquos Paediatric Committee procedures (initial PIP
waiver or modification o an agreed PIP)
0
50
100
150
200
250
300
350
400
450
500
A u s t r i a
B el gi um
B ul g a r i a
C y pr u s
C z e c h R e p u b l i c
D enm a r k
E s t oni a
F i nl a n d
F r a n c e
G er m a n y
G r e e c e
H e a l t h c a r e a n d
A c a d emi a
H un g a r y
I c el a n d
I r el a n d
I t a l y
L a t vi a
L i t h u a ni a
L ux em b o ur g
M a l t a
N or w a y
P a t i en t s Or g a ni s a t i on
P ol a n d
P or t u g a l
R om a ni a
S l ov a k i a
S l ov eni a
S p a i n
S w e d en
T h eN e t h er l a n d
s
U ni t e d K i n g d om
Initial PIP applications PIP modifications
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2936
29
ANNEX II
Detailed inventory of centrally authorised medicinalproducts for paediatric use since the entry into force
of the Paediatric Regulation
Table 13Medicinal products authorised centrally since 2007 which include a paediatric indication
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Retapamulin Altargo 2007 No Mixed
Nelarabine Atriance 2007 No Mixed
Human papillomavirus vaccine[types 16 18] Cervarix 2007 No Mixed
Hydroxocobalamin Cyanokit 2007 No Mixed
Idursulase Elaprase 2007 No Mixed
Gadoversetamide Optimark 2007 No Mixed
Betaine anhydrous Cystadane 2007 No Mixed
Stiripentol Diacomit 2007 No Paediatric only
Mecasermin Increlex 2007 No Paediatric only
Rufinamide Inovelon 2007 No Mixed
Hydroxycarbamide Siklos 2007 No Mixed
Human normal
immunoglobulin (ivig) Flebogamma DIF 2007 No Mixed
Fluticasone uroate Avamys 2008 No Mixed
Human normal immunoglobulin Privigen 2008 No Mixed
Lacosamide Vimpat 2008 No Mixed
Micaungin Mycamine 2008 No Mixed
Sapropterin Kuvan 2008 No Mixed
Sugammadex Bridion 2008 No Mixed
Tocoersonal d-alpha
tocopheryl polyethylene glycol
succinate Vedrop 2009 No Paediatric only
Miamurtide Mepact 2009 No Mixed
Rilonacept Rilonacept Regeneron 2009 No Mixed
Tacrolimus Modigra 2009 No Mixed
Pneumoccocal polysaccharideconjugate vaccine (adsorbed) Synflorix 2009 No Paediatric only
Canakinumab
Ilaris (PIP not yet
completed) 2009 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3036
30
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Pneumoccocal polysaccharide
conjugate vaccine (13-valentadsorbed)
Prevenar 13 (PIP not yetcompleted) 2009 Yes Paediatric only
Meningococcal group a c
w135 and y conjugate vaccine Menveo 2010 Yes Mixed
Velaglucerase ala
Vpriv (PIP not yet
completed) 2010 Yes Mixed
Influenza vaccine (live
attenuated nasal) Fluenz (Waiver) 2011 Yes Paediatric only
C1 inhibitor human
Cinryze (PIP not yet
completed) 2011 Yes Mixed
Dihydroartemisinin
piperaquine phosphate
Eurartesim (PIP not yet
completed) 2011 Yes Mixed
Midazolam Buccolam 2011 Yes (PUMA) Paediatric only
EverolimusVotubia(PIP not yet completed) 2011 Yes Mixed
Tobramycin
Tobi Podhaler (PIP not
yet completed) 2011 Yes Mixed
Nomegestrol estradiol Ioa Zoely 2011 Yes Mixed
Colistimethate sodium Colobreathe 2012 Yes Mixed
Mercaptopurine Xaluprine 2012 No Mixed
Catridecacog NovoThirteen 2012 Yes MixedEavirenz Eavirenz Teva 2012 No Mixed
Ivacafor Kalydeco 2012 Yes Mixed
Desloratadine Desloratadine ratiopharm 2012 No Mixed
Desloratadine Desloratadine Actavis 2012 No Mixed
Perampanel Fycompa 2012 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3136
31
Table 14List o centrally authorised medicinal products or which the therapeutic indication was extended to or amend-
ed or the paediatric population
Active substance(s)
Trade
name Date Subject of the extension
Levetiracetam Keppra
2007
2009
Extension o the indication to include adjunctive ther-
apy in the treatment o primary generalised tonic-
clonic (PGTC) seizures in adults and adolescents rom
12 years o age with idiopathic generalised epilepsyExtension o indication to include the adjunctive
treatment o partial seizures with or without second-
ary generalisation in children rom 1 month to lt4
years old
Pneumococcal sac-
charide conjugated
vaccine adsorbed Prevenar 2007
Extension o the indication to include new inorma-
tion on efficacy against disease caused by Strepto-
coccus pneumoniae serotypes 4 6B 9V 14 18C 19F
and 23F in otitis mediaExtension o indication rom active immunisation
against bacteraemic pneumonia to active immunisa-
tion against pneumonia
Infliximab
Remi-
cade 2007
Extension o indication to include treatment o
severe active Crohnrsquos disease in children aged 6 to
17 years
Darbepoetin ala Aranesp 2007
Extension o indication or CRF patients whichrestricted the use o Nespo to paediatric subjects ge
11 years o age
Fosamprenavir Telzir 2007
Extension o indication o Telzir in combination withritonavir or the treatment o Human Immunodefi-
ciency Virus Type 1 (HIV-1) inected adults in combi-nation with other antiretroviral medicinal products to
include paediatric populations
Lamivudine zidovu-
dine Combivir 2007
Extension o indication to include paediatric patients
and replacement o film-coated tablets by scored
film-coated tablets
Desloratadine Aerius 2007Extension o indication rom lsquochronic idiopathic urti-cariarsquo to lsquourticariarsquo
Insulin glulisine Apidra 2007
Extension o indication to include 6 year olds and
older children based on the results o 2 paediatricstudies
Human papilloma virusvaccine [types 6 11
16 18] (recombinantadsorbed) Gardasil 2008
Extension o indication to include the prevention ohigh-grade vaginal dysplastic lesions (VaIN 23)
Adalimumab Humira 20082011
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in adoles-cents rom 13 to 17 years o age
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in the paedi-
atric population aged rom 4 to 12 years
Caspoungin Cancidas 2008
Extension o the indication to include the paediatric
population
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2736
27
Table 9Percentage o European Medicines Agencyrsquos human resources working in the paediatric area rom 2006 (inner
circle) to 2012 (outer circle)
733 (2012)
052 (2006)
Table 10Member States acting as rapporteurs or the assessment o studies submitted in accordance with Article 46
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE SE NL FR DK IT BE PL ES NO SK FI IE RO AT HU EL CZ PT LV BG
Study included in worksharing Rapporteur appointed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2836
28
Table 11Member States acting as rapporteur or the assessment o studies submitted in accordance with Article 45
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE NL DK AT FR PL SE ES IE CZ MT IT BE SI EE FI HU NO RO BG EL LV PT IS SK
Wave 1 Wave 2 Wave 3 Wave 4 Wave 5 Wave 6 Wave 7 Wave 8 Wave 9
Wave 10 Wave 11 Wave 12 Wave 13 Wave 14 Wave 15 Wave 16 Wave 17 Wave 18
Table 12Member States acting as rapporteurspeer reviewers in EMArsquos Paediatric Committee procedures (initial PIP
waiver or modification o an agreed PIP)
0
50
100
150
200
250
300
350
400
450
500
A u s t r i a
B el gi um
B ul g a r i a
C y pr u s
C z e c h R e p u b l i c
D enm a r k
E s t oni a
F i nl a n d
F r a n c e
G er m a n y
G r e e c e
H e a l t h c a r e a n d
A c a d emi a
H un g a r y
I c el a n d
I r el a n d
I t a l y
L a t vi a
L i t h u a ni a
L ux em b o ur g
M a l t a
N or w a y
P a t i en t s Or g a ni s a t i on
P ol a n d
P or t u g a l
R om a ni a
S l ov a k i a
S l ov eni a
S p a i n
S w e d en
T h eN e t h er l a n d
s
U ni t e d K i n g d om
Initial PIP applications PIP modifications
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2936
29
ANNEX II
Detailed inventory of centrally authorised medicinalproducts for paediatric use since the entry into force
of the Paediatric Regulation
Table 13Medicinal products authorised centrally since 2007 which include a paediatric indication
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Retapamulin Altargo 2007 No Mixed
Nelarabine Atriance 2007 No Mixed
Human papillomavirus vaccine[types 16 18] Cervarix 2007 No Mixed
Hydroxocobalamin Cyanokit 2007 No Mixed
Idursulase Elaprase 2007 No Mixed
Gadoversetamide Optimark 2007 No Mixed
Betaine anhydrous Cystadane 2007 No Mixed
Stiripentol Diacomit 2007 No Paediatric only
Mecasermin Increlex 2007 No Paediatric only
Rufinamide Inovelon 2007 No Mixed
Hydroxycarbamide Siklos 2007 No Mixed
Human normal
immunoglobulin (ivig) Flebogamma DIF 2007 No Mixed
Fluticasone uroate Avamys 2008 No Mixed
Human normal immunoglobulin Privigen 2008 No Mixed
Lacosamide Vimpat 2008 No Mixed
Micaungin Mycamine 2008 No Mixed
Sapropterin Kuvan 2008 No Mixed
Sugammadex Bridion 2008 No Mixed
Tocoersonal d-alpha
tocopheryl polyethylene glycol
succinate Vedrop 2009 No Paediatric only
Miamurtide Mepact 2009 No Mixed
Rilonacept Rilonacept Regeneron 2009 No Mixed
Tacrolimus Modigra 2009 No Mixed
Pneumoccocal polysaccharideconjugate vaccine (adsorbed) Synflorix 2009 No Paediatric only
Canakinumab
Ilaris (PIP not yet
completed) 2009 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3036
30
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Pneumoccocal polysaccharide
conjugate vaccine (13-valentadsorbed)
Prevenar 13 (PIP not yetcompleted) 2009 Yes Paediatric only
Meningococcal group a c
w135 and y conjugate vaccine Menveo 2010 Yes Mixed
Velaglucerase ala
Vpriv (PIP not yet
completed) 2010 Yes Mixed
Influenza vaccine (live
attenuated nasal) Fluenz (Waiver) 2011 Yes Paediatric only
C1 inhibitor human
Cinryze (PIP not yet
completed) 2011 Yes Mixed
Dihydroartemisinin
piperaquine phosphate
Eurartesim (PIP not yet
completed) 2011 Yes Mixed
Midazolam Buccolam 2011 Yes (PUMA) Paediatric only
EverolimusVotubia(PIP not yet completed) 2011 Yes Mixed
Tobramycin
Tobi Podhaler (PIP not
yet completed) 2011 Yes Mixed
Nomegestrol estradiol Ioa Zoely 2011 Yes Mixed
Colistimethate sodium Colobreathe 2012 Yes Mixed
Mercaptopurine Xaluprine 2012 No Mixed
Catridecacog NovoThirteen 2012 Yes MixedEavirenz Eavirenz Teva 2012 No Mixed
Ivacafor Kalydeco 2012 Yes Mixed
Desloratadine Desloratadine ratiopharm 2012 No Mixed
Desloratadine Desloratadine Actavis 2012 No Mixed
Perampanel Fycompa 2012 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3136
31
Table 14List o centrally authorised medicinal products or which the therapeutic indication was extended to or amend-
ed or the paediatric population
Active substance(s)
Trade
name Date Subject of the extension
Levetiracetam Keppra
2007
2009
Extension o the indication to include adjunctive ther-
apy in the treatment o primary generalised tonic-
clonic (PGTC) seizures in adults and adolescents rom
12 years o age with idiopathic generalised epilepsyExtension o indication to include the adjunctive
treatment o partial seizures with or without second-
ary generalisation in children rom 1 month to lt4
years old
Pneumococcal sac-
charide conjugated
vaccine adsorbed Prevenar 2007
Extension o the indication to include new inorma-
tion on efficacy against disease caused by Strepto-
coccus pneumoniae serotypes 4 6B 9V 14 18C 19F
and 23F in otitis mediaExtension o indication rom active immunisation
against bacteraemic pneumonia to active immunisa-
tion against pneumonia
Infliximab
Remi-
cade 2007
Extension o indication to include treatment o
severe active Crohnrsquos disease in children aged 6 to
17 years
Darbepoetin ala Aranesp 2007
Extension o indication or CRF patients whichrestricted the use o Nespo to paediatric subjects ge
11 years o age
Fosamprenavir Telzir 2007
Extension o indication o Telzir in combination withritonavir or the treatment o Human Immunodefi-
ciency Virus Type 1 (HIV-1) inected adults in combi-nation with other antiretroviral medicinal products to
include paediatric populations
Lamivudine zidovu-
dine Combivir 2007
Extension o indication to include paediatric patients
and replacement o film-coated tablets by scored
film-coated tablets
Desloratadine Aerius 2007Extension o indication rom lsquochronic idiopathic urti-cariarsquo to lsquourticariarsquo
Insulin glulisine Apidra 2007
Extension o indication to include 6 year olds and
older children based on the results o 2 paediatricstudies
Human papilloma virusvaccine [types 6 11
16 18] (recombinantadsorbed) Gardasil 2008
Extension o indication to include the prevention ohigh-grade vaginal dysplastic lesions (VaIN 23)
Adalimumab Humira 20082011
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in adoles-cents rom 13 to 17 years o age
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in the paedi-
atric population aged rom 4 to 12 years
Caspoungin Cancidas 2008
Extension o the indication to include the paediatric
population
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2836
28
Table 11Member States acting as rapporteur or the assessment o studies submitted in accordance with Article 45
(paediatric work-sharing procedures)
0
10
20
30
40
50
60
UK DE NL DK AT FR PL SE ES IE CZ MT IT BE SI EE FI HU NO RO BG EL LV PT IS SK
Wave 1 Wave 2 Wave 3 Wave 4 Wave 5 Wave 6 Wave 7 Wave 8 Wave 9
Wave 10 Wave 11 Wave 12 Wave 13 Wave 14 Wave 15 Wave 16 Wave 17 Wave 18
Table 12Member States acting as rapporteurspeer reviewers in EMArsquos Paediatric Committee procedures (initial PIP
waiver or modification o an agreed PIP)
0
50
100
150
200
250
300
350
400
450
500
A u s t r i a
B el gi um
B ul g a r i a
C y pr u s
C z e c h R e p u b l i c
D enm a r k
E s t oni a
F i nl a n d
F r a n c e
G er m a n y
G r e e c e
H e a l t h c a r e a n d
A c a d emi a
H un g a r y
I c el a n d
I r el a n d
I t a l y
L a t vi a
L i t h u a ni a
L ux em b o ur g
M a l t a
N or w a y
P a t i en t s Or g a ni s a t i on
P ol a n d
P or t u g a l
R om a ni a
S l ov a k i a
S l ov eni a
S p a i n
S w e d en
T h eN e t h er l a n d
s
U ni t e d K i n g d om
Initial PIP applications PIP modifications
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2936
29
ANNEX II
Detailed inventory of centrally authorised medicinalproducts for paediatric use since the entry into force
of the Paediatric Regulation
Table 13Medicinal products authorised centrally since 2007 which include a paediatric indication
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Retapamulin Altargo 2007 No Mixed
Nelarabine Atriance 2007 No Mixed
Human papillomavirus vaccine[types 16 18] Cervarix 2007 No Mixed
Hydroxocobalamin Cyanokit 2007 No Mixed
Idursulase Elaprase 2007 No Mixed
Gadoversetamide Optimark 2007 No Mixed
Betaine anhydrous Cystadane 2007 No Mixed
Stiripentol Diacomit 2007 No Paediatric only
Mecasermin Increlex 2007 No Paediatric only
Rufinamide Inovelon 2007 No Mixed
Hydroxycarbamide Siklos 2007 No Mixed
Human normal
immunoglobulin (ivig) Flebogamma DIF 2007 No Mixed
Fluticasone uroate Avamys 2008 No Mixed
Human normal immunoglobulin Privigen 2008 No Mixed
Lacosamide Vimpat 2008 No Mixed
Micaungin Mycamine 2008 No Mixed
Sapropterin Kuvan 2008 No Mixed
Sugammadex Bridion 2008 No Mixed
Tocoersonal d-alpha
tocopheryl polyethylene glycol
succinate Vedrop 2009 No Paediatric only
Miamurtide Mepact 2009 No Mixed
Rilonacept Rilonacept Regeneron 2009 No Mixed
Tacrolimus Modigra 2009 No Mixed
Pneumoccocal polysaccharideconjugate vaccine (adsorbed) Synflorix 2009 No Paediatric only
Canakinumab
Ilaris (PIP not yet
completed) 2009 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3036
30
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Pneumoccocal polysaccharide
conjugate vaccine (13-valentadsorbed)
Prevenar 13 (PIP not yetcompleted) 2009 Yes Paediatric only
Meningococcal group a c
w135 and y conjugate vaccine Menveo 2010 Yes Mixed
Velaglucerase ala
Vpriv (PIP not yet
completed) 2010 Yes Mixed
Influenza vaccine (live
attenuated nasal) Fluenz (Waiver) 2011 Yes Paediatric only
C1 inhibitor human
Cinryze (PIP not yet
completed) 2011 Yes Mixed
Dihydroartemisinin
piperaquine phosphate
Eurartesim (PIP not yet
completed) 2011 Yes Mixed
Midazolam Buccolam 2011 Yes (PUMA) Paediatric only
EverolimusVotubia(PIP not yet completed) 2011 Yes Mixed
Tobramycin
Tobi Podhaler (PIP not
yet completed) 2011 Yes Mixed
Nomegestrol estradiol Ioa Zoely 2011 Yes Mixed
Colistimethate sodium Colobreathe 2012 Yes Mixed
Mercaptopurine Xaluprine 2012 No Mixed
Catridecacog NovoThirteen 2012 Yes MixedEavirenz Eavirenz Teva 2012 No Mixed
Ivacafor Kalydeco 2012 Yes Mixed
Desloratadine Desloratadine ratiopharm 2012 No Mixed
Desloratadine Desloratadine Actavis 2012 No Mixed
Perampanel Fycompa 2012 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3136
31
Table 14List o centrally authorised medicinal products or which the therapeutic indication was extended to or amend-
ed or the paediatric population
Active substance(s)
Trade
name Date Subject of the extension
Levetiracetam Keppra
2007
2009
Extension o the indication to include adjunctive ther-
apy in the treatment o primary generalised tonic-
clonic (PGTC) seizures in adults and adolescents rom
12 years o age with idiopathic generalised epilepsyExtension o indication to include the adjunctive
treatment o partial seizures with or without second-
ary generalisation in children rom 1 month to lt4
years old
Pneumococcal sac-
charide conjugated
vaccine adsorbed Prevenar 2007
Extension o the indication to include new inorma-
tion on efficacy against disease caused by Strepto-
coccus pneumoniae serotypes 4 6B 9V 14 18C 19F
and 23F in otitis mediaExtension o indication rom active immunisation
against bacteraemic pneumonia to active immunisa-
tion against pneumonia
Infliximab
Remi-
cade 2007
Extension o indication to include treatment o
severe active Crohnrsquos disease in children aged 6 to
17 years
Darbepoetin ala Aranesp 2007
Extension o indication or CRF patients whichrestricted the use o Nespo to paediatric subjects ge
11 years o age
Fosamprenavir Telzir 2007
Extension o indication o Telzir in combination withritonavir or the treatment o Human Immunodefi-
ciency Virus Type 1 (HIV-1) inected adults in combi-nation with other antiretroviral medicinal products to
include paediatric populations
Lamivudine zidovu-
dine Combivir 2007
Extension o indication to include paediatric patients
and replacement o film-coated tablets by scored
film-coated tablets
Desloratadine Aerius 2007Extension o indication rom lsquochronic idiopathic urti-cariarsquo to lsquourticariarsquo
Insulin glulisine Apidra 2007
Extension o indication to include 6 year olds and
older children based on the results o 2 paediatricstudies
Human papilloma virusvaccine [types 6 11
16 18] (recombinantadsorbed) Gardasil 2008
Extension o indication to include the prevention ohigh-grade vaginal dysplastic lesions (VaIN 23)
Adalimumab Humira 20082011
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in adoles-cents rom 13 to 17 years o age
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in the paedi-
atric population aged rom 4 to 12 years
Caspoungin Cancidas 2008
Extension o the indication to include the paediatric
population
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 2936
29
ANNEX II
Detailed inventory of centrally authorised medicinalproducts for paediatric use since the entry into force
of the Paediatric Regulation
Table 13Medicinal products authorised centrally since 2007 which include a paediatric indication
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Retapamulin Altargo 2007 No Mixed
Nelarabine Atriance 2007 No Mixed
Human papillomavirus vaccine[types 16 18] Cervarix 2007 No Mixed
Hydroxocobalamin Cyanokit 2007 No Mixed
Idursulase Elaprase 2007 No Mixed
Gadoversetamide Optimark 2007 No Mixed
Betaine anhydrous Cystadane 2007 No Mixed
Stiripentol Diacomit 2007 No Paediatric only
Mecasermin Increlex 2007 No Paediatric only
Rufinamide Inovelon 2007 No Mixed
Hydroxycarbamide Siklos 2007 No Mixed
Human normal
immunoglobulin (ivig) Flebogamma DIF 2007 No Mixed
Fluticasone uroate Avamys 2008 No Mixed
Human normal immunoglobulin Privigen 2008 No Mixed
Lacosamide Vimpat 2008 No Mixed
Micaungin Mycamine 2008 No Mixed
Sapropterin Kuvan 2008 No Mixed
Sugammadex Bridion 2008 No Mixed
Tocoersonal d-alpha
tocopheryl polyethylene glycol
succinate Vedrop 2009 No Paediatric only
Miamurtide Mepact 2009 No Mixed
Rilonacept Rilonacept Regeneron 2009 No Mixed
Tacrolimus Modigra 2009 No Mixed
Pneumoccocal polysaccharideconjugate vaccine (adsorbed) Synflorix 2009 No Paediatric only
Canakinumab
Ilaris (PIP not yet
completed) 2009 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3036
30
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Pneumoccocal polysaccharide
conjugate vaccine (13-valentadsorbed)
Prevenar 13 (PIP not yetcompleted) 2009 Yes Paediatric only
Meningococcal group a c
w135 and y conjugate vaccine Menveo 2010 Yes Mixed
Velaglucerase ala
Vpriv (PIP not yet
completed) 2010 Yes Mixed
Influenza vaccine (live
attenuated nasal) Fluenz (Waiver) 2011 Yes Paediatric only
C1 inhibitor human
Cinryze (PIP not yet
completed) 2011 Yes Mixed
Dihydroartemisinin
piperaquine phosphate
Eurartesim (PIP not yet
completed) 2011 Yes Mixed
Midazolam Buccolam 2011 Yes (PUMA) Paediatric only
EverolimusVotubia(PIP not yet completed) 2011 Yes Mixed
Tobramycin
Tobi Podhaler (PIP not
yet completed) 2011 Yes Mixed
Nomegestrol estradiol Ioa Zoely 2011 Yes Mixed
Colistimethate sodium Colobreathe 2012 Yes Mixed
Mercaptopurine Xaluprine 2012 No Mixed
Catridecacog NovoThirteen 2012 Yes MixedEavirenz Eavirenz Teva 2012 No Mixed
Ivacafor Kalydeco 2012 Yes Mixed
Desloratadine Desloratadine ratiopharm 2012 No Mixed
Desloratadine Desloratadine Actavis 2012 No Mixed
Perampanel Fycompa 2012 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3136
31
Table 14List o centrally authorised medicinal products or which the therapeutic indication was extended to or amend-
ed or the paediatric population
Active substance(s)
Trade
name Date Subject of the extension
Levetiracetam Keppra
2007
2009
Extension o the indication to include adjunctive ther-
apy in the treatment o primary generalised tonic-
clonic (PGTC) seizures in adults and adolescents rom
12 years o age with idiopathic generalised epilepsyExtension o indication to include the adjunctive
treatment o partial seizures with or without second-
ary generalisation in children rom 1 month to lt4
years old
Pneumococcal sac-
charide conjugated
vaccine adsorbed Prevenar 2007
Extension o the indication to include new inorma-
tion on efficacy against disease caused by Strepto-
coccus pneumoniae serotypes 4 6B 9V 14 18C 19F
and 23F in otitis mediaExtension o indication rom active immunisation
against bacteraemic pneumonia to active immunisa-
tion against pneumonia
Infliximab
Remi-
cade 2007
Extension o indication to include treatment o
severe active Crohnrsquos disease in children aged 6 to
17 years
Darbepoetin ala Aranesp 2007
Extension o indication or CRF patients whichrestricted the use o Nespo to paediatric subjects ge
11 years o age
Fosamprenavir Telzir 2007
Extension o indication o Telzir in combination withritonavir or the treatment o Human Immunodefi-
ciency Virus Type 1 (HIV-1) inected adults in combi-nation with other antiretroviral medicinal products to
include paediatric populations
Lamivudine zidovu-
dine Combivir 2007
Extension o indication to include paediatric patients
and replacement o film-coated tablets by scored
film-coated tablets
Desloratadine Aerius 2007Extension o indication rom lsquochronic idiopathic urti-cariarsquo to lsquourticariarsquo
Insulin glulisine Apidra 2007
Extension o indication to include 6 year olds and
older children based on the results o 2 paediatricstudies
Human papilloma virusvaccine [types 6 11
16 18] (recombinantadsorbed) Gardasil 2008
Extension o indication to include the prevention ohigh-grade vaginal dysplastic lesions (VaIN 23)
Adalimumab Humira 20082011
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in adoles-cents rom 13 to 17 years o age
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in the paedi-
atric population aged rom 4 to 12 years
Caspoungin Cancidas 2008
Extension o the indication to include the paediatric
population
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3036
30
Active
substance(s)
Trade
name
Year
of
authorisation
Requirement
to fulfil
Paediatric
Regulation
at first
authorisation
Indication is
paediatric-only
or lsquomixedrsquo (adult
and paediatric)
Pneumoccocal polysaccharide
conjugate vaccine (13-valentadsorbed)
Prevenar 13 (PIP not yetcompleted) 2009 Yes Paediatric only
Meningococcal group a c
w135 and y conjugate vaccine Menveo 2010 Yes Mixed
Velaglucerase ala
Vpriv (PIP not yet
completed) 2010 Yes Mixed
Influenza vaccine (live
attenuated nasal) Fluenz (Waiver) 2011 Yes Paediatric only
C1 inhibitor human
Cinryze (PIP not yet
completed) 2011 Yes Mixed
Dihydroartemisinin
piperaquine phosphate
Eurartesim (PIP not yet
completed) 2011 Yes Mixed
Midazolam Buccolam 2011 Yes (PUMA) Paediatric only
EverolimusVotubia(PIP not yet completed) 2011 Yes Mixed
Tobramycin
Tobi Podhaler (PIP not
yet completed) 2011 Yes Mixed
Nomegestrol estradiol Ioa Zoely 2011 Yes Mixed
Colistimethate sodium Colobreathe 2012 Yes Mixed
Mercaptopurine Xaluprine 2012 No Mixed
Catridecacog NovoThirteen 2012 Yes MixedEavirenz Eavirenz Teva 2012 No Mixed
Ivacafor Kalydeco 2012 Yes Mixed
Desloratadine Desloratadine ratiopharm 2012 No Mixed
Desloratadine Desloratadine Actavis 2012 No Mixed
Perampanel Fycompa 2012 Yes Mixed
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3136
31
Table 14List o centrally authorised medicinal products or which the therapeutic indication was extended to or amend-
ed or the paediatric population
Active substance(s)
Trade
name Date Subject of the extension
Levetiracetam Keppra
2007
2009
Extension o the indication to include adjunctive ther-
apy in the treatment o primary generalised tonic-
clonic (PGTC) seizures in adults and adolescents rom
12 years o age with idiopathic generalised epilepsyExtension o indication to include the adjunctive
treatment o partial seizures with or without second-
ary generalisation in children rom 1 month to lt4
years old
Pneumococcal sac-
charide conjugated
vaccine adsorbed Prevenar 2007
Extension o the indication to include new inorma-
tion on efficacy against disease caused by Strepto-
coccus pneumoniae serotypes 4 6B 9V 14 18C 19F
and 23F in otitis mediaExtension o indication rom active immunisation
against bacteraemic pneumonia to active immunisa-
tion against pneumonia
Infliximab
Remi-
cade 2007
Extension o indication to include treatment o
severe active Crohnrsquos disease in children aged 6 to
17 years
Darbepoetin ala Aranesp 2007
Extension o indication or CRF patients whichrestricted the use o Nespo to paediatric subjects ge
11 years o age
Fosamprenavir Telzir 2007
Extension o indication o Telzir in combination withritonavir or the treatment o Human Immunodefi-
ciency Virus Type 1 (HIV-1) inected adults in combi-nation with other antiretroviral medicinal products to
include paediatric populations
Lamivudine zidovu-
dine Combivir 2007
Extension o indication to include paediatric patients
and replacement o film-coated tablets by scored
film-coated tablets
Desloratadine Aerius 2007Extension o indication rom lsquochronic idiopathic urti-cariarsquo to lsquourticariarsquo
Insulin glulisine Apidra 2007
Extension o indication to include 6 year olds and
older children based on the results o 2 paediatricstudies
Human papilloma virusvaccine [types 6 11
16 18] (recombinantadsorbed) Gardasil 2008
Extension o indication to include the prevention ohigh-grade vaginal dysplastic lesions (VaIN 23)
Adalimumab Humira 20082011
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in adoles-cents rom 13 to 17 years o age
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in the paedi-
atric population aged rom 4 to 12 years
Caspoungin Cancidas 2008
Extension o the indication to include the paediatric
population
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3136
31
Table 14List o centrally authorised medicinal products or which the therapeutic indication was extended to or amend-
ed or the paediatric population
Active substance(s)
Trade
name Date Subject of the extension
Levetiracetam Keppra
2007
2009
Extension o the indication to include adjunctive ther-
apy in the treatment o primary generalised tonic-
clonic (PGTC) seizures in adults and adolescents rom
12 years o age with idiopathic generalised epilepsyExtension o indication to include the adjunctive
treatment o partial seizures with or without second-
ary generalisation in children rom 1 month to lt4
years old
Pneumococcal sac-
charide conjugated
vaccine adsorbed Prevenar 2007
Extension o the indication to include new inorma-
tion on efficacy against disease caused by Strepto-
coccus pneumoniae serotypes 4 6B 9V 14 18C 19F
and 23F in otitis mediaExtension o indication rom active immunisation
against bacteraemic pneumonia to active immunisa-
tion against pneumonia
Infliximab
Remi-
cade 2007
Extension o indication to include treatment o
severe active Crohnrsquos disease in children aged 6 to
17 years
Darbepoetin ala Aranesp 2007
Extension o indication or CRF patients whichrestricted the use o Nespo to paediatric subjects ge
11 years o age
Fosamprenavir Telzir 2007
Extension o indication o Telzir in combination withritonavir or the treatment o Human Immunodefi-
ciency Virus Type 1 (HIV-1) inected adults in combi-nation with other antiretroviral medicinal products to
include paediatric populations
Lamivudine zidovu-
dine Combivir 2007
Extension o indication to include paediatric patients
and replacement o film-coated tablets by scored
film-coated tablets
Desloratadine Aerius 2007Extension o indication rom lsquochronic idiopathic urti-cariarsquo to lsquourticariarsquo
Insulin glulisine Apidra 2007
Extension o indication to include 6 year olds and
older children based on the results o 2 paediatricstudies
Human papilloma virusvaccine [types 6 11
16 18] (recombinantadsorbed) Gardasil 2008
Extension o indication to include the prevention ohigh-grade vaginal dysplastic lesions (VaIN 23)
Adalimumab Humira 20082011
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in adoles-cents rom 13 to 17 years o age
Extension o indication to include treatment o active
polyarticular juvenile idiopathic arthritis in the paedi-
atric population aged rom 4 to 12 years
Caspoungin Cancidas 2008
Extension o the indication to include the paediatric
population
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3236
32
Active substance(s)
Trade
name Date Subject of the extension
Etanercept Enbrel 20082011
Extension o indication to include the treatment
o chronic severe plaque psoriasis in children and
adolescents rom the age o 6 years who areinadequately controlled by or are intolerant to other
systemic therapies or phototherapies
Extension o indication to include lower age range
or polyarticular juvenile idiopathic arthritis lsquorom the
age o 4 yearsrsquo to lsquorom the age o 2 yearsrsquo
Miglustat Zavesca 2009
Extension o indication to include the treatment o
progressive neurological maniestations in adult
patients and paediatric patients with Niemann-Pick
type-C disease
Tacrolimus Protopic 2009
Extension o indication to lsquomaintenance treatmentrsquo
urther to completion o one study in adult patients
and one in paediatric patients
Tipranavir Aptivus 2009
Extension o indication to include the treatment o
HIV-1 inection in highly pre-treated adolescents 12years o age or older with virus resistant to multiple
protease inhibitors
Omalizumab Xolair 2009
Extension o indication to children rom 6 to lt12
years o age as add-on therapy to improve allergic
asthma control
Aripiprazole Abiliy 2009
Extension o indication to include treatment o
schizophrenia in adolescents 15 years and older
Pegintereron ala-2b
PegIn-
tron 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Ribavirin Rebetol 2009
Extension o indication o the combination therapypegintereron ala-2b and ribavirin to include treat-
ment o the paediatric population
Abatacept Orencia 2010
Extension o indication to include the treatment o
moderate to severe active polyarticular juvenile idio-pathic arthritis in paediatric patients 6 years o age
and older who have had an insufficient response to
other DMARDs including at least one TNF inhibitor
Atazanavir sulphate Reyataz 2010
Extension o indication or Reyataz capsules toinclude the treatment o HIV-inected children and
adolescents above the age o 6 in combination with
other antiretroviral medicinal products
Measles mumps andrubella vaccine (live)
M-M-RVAXPRO 2010
Extension o indication to include administration tohealthy children rom 9 months o age
Nitric oxide Inomax 2011
Extension o indication to include the treatment o
pulmonary hypertension peri- and post heart surgeryin children
Tenoovir disoproxilumarate Viread 2011
Amendment o indication based on the results o a
saety and efficacy study in treatment-experiencedadolescents aged 12 to 18 years old
Paliperidone Invega 2011
Extension o indication to include treatment o psy-
chotic or manic symptoms o schizoaffective disorder
Sildenafil Revatio 2011
Extension o indication in paediatric patients aged
1 year to 17 years old with pulmonary arterial hyper-tension
Human normal immu-
noglobulin (ivig) Kiovig 2011
Extension o indication to include treatment o multi-
ocal motor neuropathy and hypogammaglobulinae-
mia in patients afer allogeneic haematopoietic stem
cell transplantation in adults and children
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3336
33
Active substance(s)
Trade
name Date Subject of the extension
Tocilizumab
Ro-
actemra 2011
Extension o indication to include treatment o ac-
tive systemic juvenile idiopathic arthritis in patients
2 years o age and older who have respondedinadequately to previous therapy with NSAIDs and
systemic corticosteroids
Pneumococcal polysac-
charide conjugatevaccine (adsorbed) Synflorix 2011
Extension o indication to increase the upper agelimit o inants and children rom 2 years to 5 years
Insulin detemir Levemir 2011
Extension o indication as add-on therapy to liraglu-
tide treatment
Extension o indication to children aged 2-5 years
Eculizumab Soliris 2011
Extension o indication to include atypical haemolytic
uremic syndrome (aHUS) Additional vaccination and
antibiotic prophylaxis recommendation have alsobeen added in section 42 or treatment o aHUS in
adults and children
Human papillomavirus
vaccine [types 16 18](recombinant adju-
vanted adsorbed) Cervarix 2011 Extension o indication to children rom 9 years
Etanercept Enbrel 2012
Extension o the Juvenile idiopathic arthritis (JIA)indication to include children and adolescents with
extended oligoarticular JIA rom the age o 2 years
children and adolescents with enthesitis-related
arthritis rom the age o 12 years and children and
adolescents with psoriatic arthritis rom the age o12 years
Measles mumps
rubella and varicellavaccine (live) Proquad 2012
Extension o the age range in the indication to chil-
dren rom 9 months o age onwards under specialcircumstances ie outbreak control
For a more detailed inventory including inormation on nationally authorised products and new routes o
administration or new pharmaceutical orms please reer to Annex II o the lsquo5-year Report to the European
Commissionrsquo o the EMA
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636
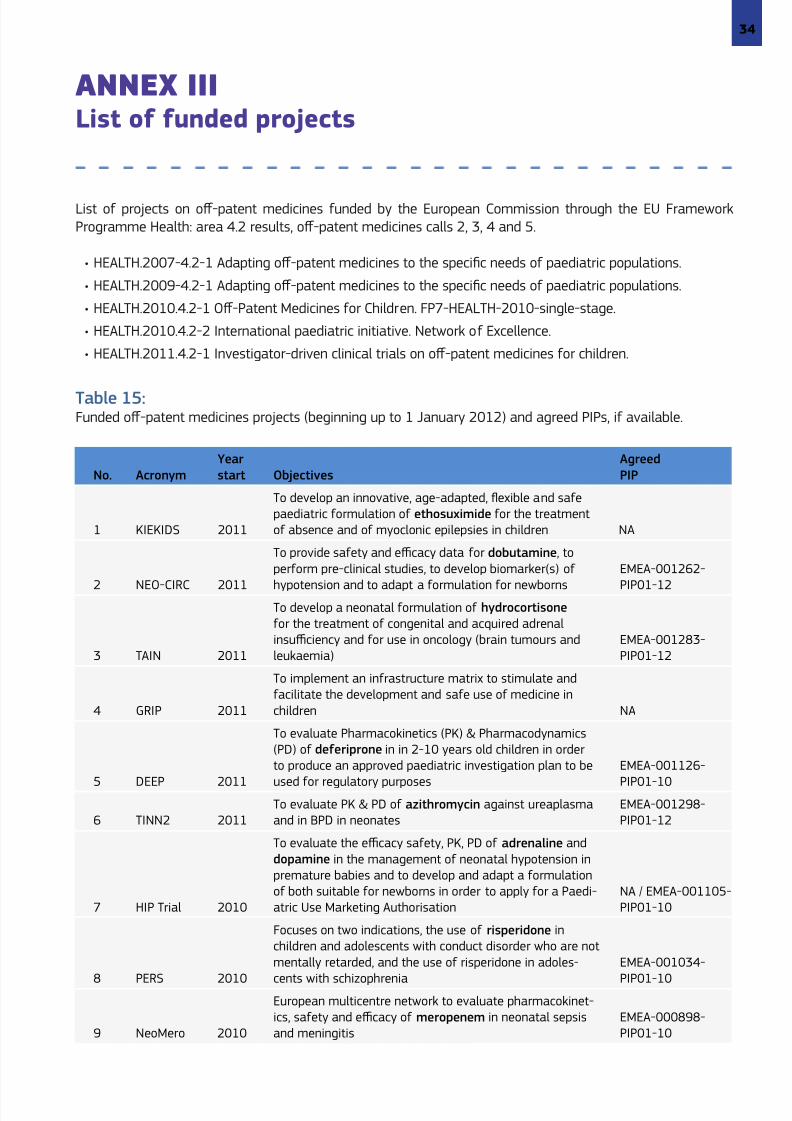
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3436
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3536
8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636

8102019 Better Medicines for children From Concept to Reality
httpslidepdfcomreaderfullbetter-medicines-for-children-from-concept-to-reality 3636