beth drolet,%md%faad%...
TRANSCRIPT

Change is Inevitable: Unlock the Secrets to Manage and Lead it
Beth Drolet, MD FAAD Professor, Dermatology and Pediatrics
Vice Chair of Dermatology Medical College of Wisconsin
Chief Experience Officer Children’s Hospital of Wisconsin
Caroline C. Kim, MD FAAD Assistant Professor, Department of Dermatology
Harvard Medical School Director, Pigmented Lesion Clinic; Associate Director, Cutaneous Oncology Program
Beth Israel Deaconess Medical Center, Boston, MA
Forum F065, March 4, 2017, 1:00PM-‐3:00PM Annual AAD MeeVng, Orlando, Florida

PHOTOGRAPHY & VIDEOTAPING ARE STRICTLY PROHIBITED IN ALL EDUCATIONAL SESSIONS
CELL PHONES MUST BE PLACED ON VIBRATE OR TURNED OFF
ViolaDons of this policy will result in removal from the session and possible revocaDon of meeDng registraDon.
Session directors will be closely monitoring such occurrences.

hWp://odevconsulVng.com/wp-‐content/uploads/2014/12/change-‐management-‐1.jpg

Changes are inevitable
“It’s not the strongest of the species that survives, nor the most intelligent, but the one most responsive to change.”
-‐-‐Charles Darwin, 1809

Changes are inevitable
• Job responsibiliVes • Staff/faculty/resident changes • Changes in support • Physical space • Problems • Insurance coverage and requirements • Paperwork • Meaningful use • Electronic Health Records • Prior authorizaVons • Financial consideraVons • Hospital mergers/ownership • Rules, regulaVons, Etc.

Overview of session
1. Group exercise -‐ Successful change 2. Basic principles of change 3. Group exercise -‐ Unsuccessful change 4. Personal side of change 5. How to navigate change 6. How to lead change
Successful change

Personal reflecVon
• Examples of successful change from group
Principles of successful change
• Different models of successful change • Three basic principles:
1. Create a climate for change 2. Engage and enable the whole organizaVon 3. Implement and sustain change

Principles of successful change
• John P. KoWer -‐-‐Professor of Leadership, Emeritus, Harvard Business School -‐-‐Studied numerous companies and organizaVons and how they restructured/ changed to adapt to environment -‐-‐Wrote seminal book on change management in 1996 “Leading Change” -‐-‐Research showed that only 30% of change programs succeeded


Principles of successful change
ADKAR® model of change
hWps://www.prosci.com/media
Example of successful change New implementaVon of new solware or electronic medical records because hospital no
longer supporVng current model
• Desire: If no desire, “I don’t want to change. What’s in it for me?” -‐-‐SoluDons: uncover personal reasons behind moVvaVon, translate into meaningfulness
• Knowledge: -‐-‐Training for specific individual job
hWps://www.prosci.com/adkar/adkar-‐model
• Awareness: If individual not aware of reason: “What a waste of ;me, old one was fine” -‐-‐If aware, reacVon may be “When does this happen, how does this affect me?”
Example of successful change New implementaVon of new solware or electronic medical records
• Ability: If no ability: “I’m not geAng this right”, “ It’s taking me twice as long” -‐-‐SoluDons: coaching, pracVce, Vme
• Reinforcement: If no reinforcement, “I’m going to keep doing it the old way” -‐-‐SoluVons: monitor if change, posiVve recogniVon, more training/coaching
hWps://www.prosci.com/adkar/adkar-‐model

Principles of successful change
ADKAR model: Goal-‐oriented change model -‐-‐helps to drive individual change for organizaVonal results
• Awareness: of reasons for change; This is goal of communicaVon from leadership • Desire: to parVcipate in change; This is goal of sponsorship and resistance management • Knowledge: of how to change; This is goal of educaVon/training and coaching • Ability: to change; This is goal of addiVonal training, pracVce and Vme
• Reinforcement: to make sure change sVcks; This is goal of adopVon measurement, correcVons and recogniVon

BIDMC case example
Beth Israel Deaconess Medical Center, Boston, MA -‐-‐In the 1990’s, affected by changing health care climate , 2 hospitals merged, Beth Israel and Deaconess
David A Garvin and Michael A. Roberto, “Change through persuasion.” HBR February 2005
-‐-‐Merger was difficult: 2 different hospitals/cultures, clinical integraVon with Beth Israel with majority of power; bad blood, mistrust, low morale
-‐-‐Business integraDon also not opDmal, as well as connecVons to feeder networks of paVents ; major losses—around $50 million a year in losses from 1997-‐2001.
-‐-‐Outside consultant issued report of dire circumstances; AWorney General of MA threatened to force BIDMC to sell to for-‐profit.

BIDMC case example
Beth Israel Deaconess Medical Center, Boston, MA Paul Levy was selected as new CEO in 2002 -‐-‐Non-‐medical background, but served in leadership roles in city: Public uVliVes and water resources, Dean of AdministraVon, Harvard Medical School
-‐-‐Set the stage on first day: email to all employees about crisis, “last chance” to save hospital or else sale to for-‐profit. Released outside consultant report and his plan for acVon.
-‐-‐Focused on core common value for all: framed changes in context of maintaining BIDMC as a warm, caring provider of top quality paVent care
• Awareness • Open, honest and
transparent • Desire, meaning

BIDMC case example
Beth Israel Deaconess Medical Center, Boston, MA Paul Levy was selected as new CEO in 2002 -‐-‐Supported and empowered others to change: Solicited suggesVons from all employees to be part of soluVon: town meeVngs, hallway chats, lunch with staff, personal response to emails, including others’ ideas
-‐-‐Reinforced short-‐term wins: lavish praise for staff, progress updates -‐-‐Prepared for next steps to conDnue changes: caring for greater paVent volume
• Knowledge • Ability, inclusivity,
empowerment and ownership
• Reinforcement
BIDMC case example
Beth Israel Deaconess Medical Center, Boston, MA Paul Levy’s leadership example:
• CommunicaDon: honest, transparent, inclusive • Framing change around core values; meaningfulness • Support and empowerment for those changing • MoDvaDon
3 years later, BIDMC reported a $37.4 million net gain Revenues rose, costs shrank, morale soared—drop in nursing turnover from 16% to 3%

Unsuccessful change

Personal reflecVon
1. When have you been part of a change that was or is unsuccessful?

Why change fails-‐it’s personal • Failure to engage
– No sponsorship or incomplete authority – Do not include people in creaVng soluVon – Do not include others on how to implement the soluVon
• Failure to communicate – Leaders talking about what’s wrong about the current – Wrong people sending the message – Leaders fail to focus on the “why” of the change
• Failure to implement – Leaders don’t invest in process improvement – Lack of training/building skills
Climate Engage Implement
Personal reflecVon
1. When have you personally resisted a change?

ResisVng change-‐it’s personal • Resistance the natural reacVon to change • Why: – Perceived loss of autonomy – Excessive uncertainty – Surprise – Failure or “loss of face” – More work – The change is not one for the beWer

ResisVng change-‐it’s personal
• Factors that affect one’s ability to absorb change include: – Personal history – Current events in their life – Current changes at work – Individual’s percepVon of the magnitude of the change

Personal moVvaVon “Drive: The Surprising Truth About What MoVvates Us”
by Daniel H Pink 1. Autonomy
1. It is our “default sepng” 2. Mastery
1. Becoming beWer at something that maWers 2. Goals must be crystal clear
3. Purpose

ResisVng change-‐it’s personal • The natural reacVon to change is resistance • Why we resist change: – Perceived loss of autonomy – Excessive uncertainty – Surprise – Failure or “loss of face” – More work – The change is not one for the beWer
Autonomy Mastery Purpose

How to navigate change

Recognize your resistance
• Why am I resisVng? • Reframe change as improvement • Engage and influence effecVvely

Influence-‐Managing up
Managing up: working with your superior to obtain the best possible results for you and your organizaVon -‐-‐relaVonship of mutual dependence

Principles of managing up
Know your boss/superior -‐-‐goals, pressures -‐-‐strengths, weaknesses
Know yourself -‐-‐goals, pressures -‐-‐strengths, weaknesses, your needs
-‐-‐how you respond to being managed
• Find shared purpose -‐-‐we all want… -‐-‐how can we improve our organiza;on
Principles of managing up • InformaVon flow • Recognize, do not judge different perspecVves • Assume good intent • Build trust • Sell your issues
-‐-‐learn how to present them, frame issues in context that your superior will respond • Focus on what you can change • Include/ advocate for those you lead
Thomas Zuber and Erika James, “Managing Your Boss”, June 2001, Family PracVce Management

Recognize perspecVves The healthcare chiasm
Administrator 1. Fiscal 2. Safety 3. Heal 4. Experience
Providers 1. Safety 2. Heal 3. Experience 4. Fiscal
PaDents 1. Experience 2. Heal 3. Safety 4. Fiscal

Use Change Management
• Are there too many changes? • Do we have the skills to implement change • Is it too much work? • What can we stop doing?


How to lead change

Leading change • Why healthcare providers should lead – Perceived authority – Unique medical knowledge – Unique insight into paVents – AltruisVc-‐strong sense of purpose
• We need help overcoming obstacles – Time to be effecVve – Learn to influence-‐build relaVonships – Master leadership and change management skills

Advocate for those you lead • Debunk myths about physicians:
1. Resist change 2. Resist standardizaVon 3. Won’t change processes 4. Are financially driven 5. Don’t care about experience
• Include/involve those undergoing change • Communicate • Manage up • Talk the talk, walk the walk

Leading change • Change management science
1. John KoWer 2. Prosci-‐ADKAR
• Recognize change is not linear • Recognize personal side of change
¡ “Drive”, Daniel H. Pink • Assume good intent • Expect resistance
Climate Engage Implement
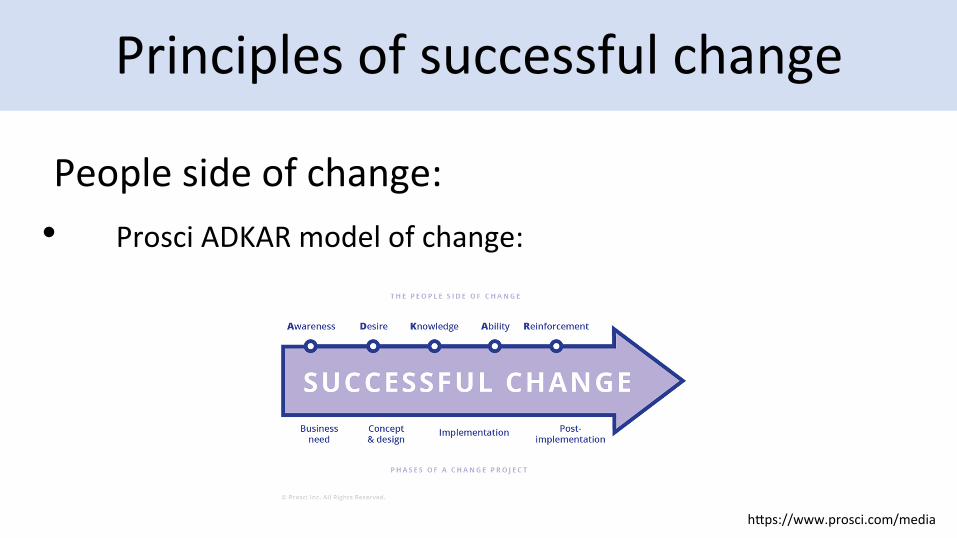
Principles of successful change
People side of change: • Prosci ADKAR model of change:
hWps://www.prosci.com/media
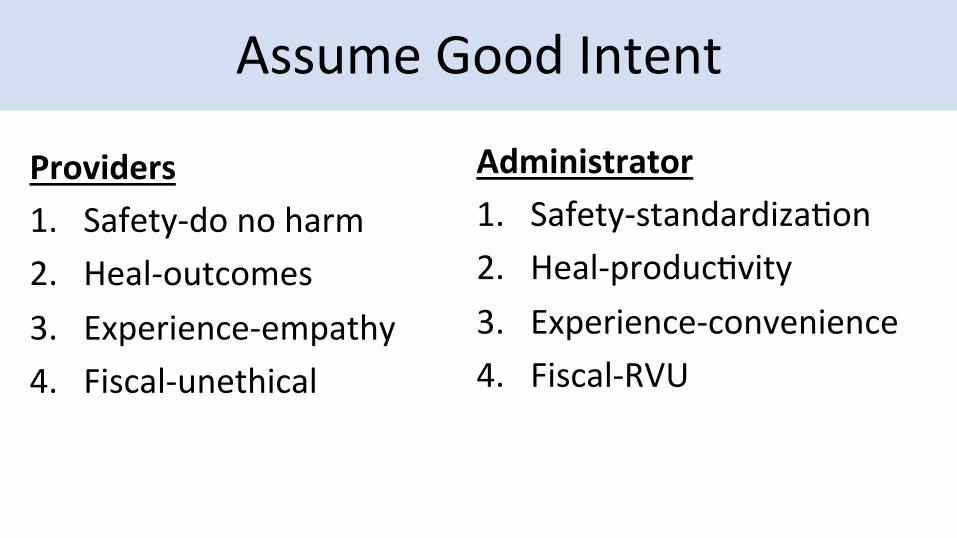
Assume Good Intent
Providers 1. Safety-‐do no harm 2. Heal-‐outcomes 3. Experience-‐empathy 4. Fiscal-‐unethical
Administrator 1. Safety-‐standardizaVon 2. Heal-‐producVvity 3. Experience-‐convenience 4. Fiscal-‐RVU
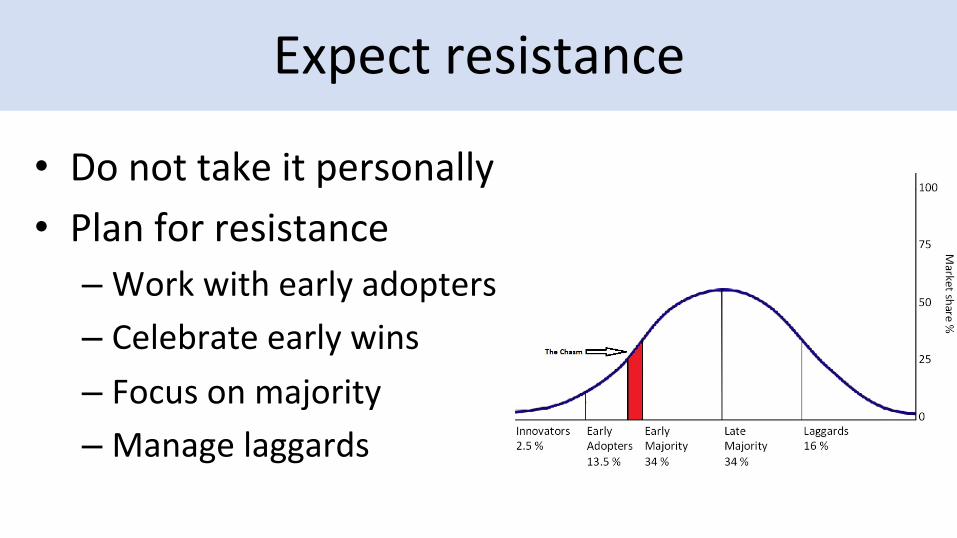
Expect resistance
• Do not take it personally • Plan for resistance – Work with early adopters – Celebrate early wins – Focus on majority – Manage laggards
Summary and Discussion
1. Basic principles of change 2. Personal side of change 3. How to navigate change 4. How to lead change

Change is Inevitable: Unlock the Secrets to Manage and Lead it
Thank you!
Beth Drolet,MD FAAD Professor Of Dermatology and Pediatrics
Interim Chairman of Dermatology Medical College of Wisconsin
Chief Experience Officer Children’s Hospital of Wisconsin
Caroline C. Kim, MD FAAD Assistant Professor, Department of Dermatology
Harvard Medical School Director, Pigmented Lesion Clinic; Associate Director, Cutaneous Oncology Program
Beth Israel Deaconess Medical Center, Boston, MA