betel quid chewing in dagon (east) townshipeast... · 7/15/2014 3 recent epidemiological studies...
TRANSCRIPT

7/15/2014
1
Betel Quid Chewing
in Dagon (East) Township
Ko Ko Zaw1, Mya Ohnmar1, Moh Moh Hlaing1, Swe Swe Win2,
Maung Maung Than Htike 3, Phyu Phyu Aye4, Mg Mg Myint1,
Sein Shwe2 & Moe Thida Htwe2
1Department of Medical Research (Lower Myanmar), 2University of Dental Medicine (Yangon), 3International Health Division, Ministry of Health,
4Department of Health
Introduction
600 million people (10% of the world’s population)
chew betel quid worldwide.
(A review of human carcinogens–Part E. Lancet Oncol 2009;10:1033–34)
Betel quid chewing has been common in Southeast
Asia and Asia Pacific Region including Myanmar for a
long time.
Prevalence of betel quid chewing varies
from 5% in Karachi, Pakistan
through 49% in Sarawak, Indonesia
up to 80% in parts of India

7/15/2014
2
Introduction (contd.)
Betel quid use - multiple impacts on health.
Areca nut forms nitrosamines in the saliva of chewers
which induces oral pre-neoplastic disorders with a high
propensity to progress to cancer.
Areca nut, with/without added tobacco, is a cause of
oral cancer
pharyngeal cancer &
esophageal cancers
(IARC. Betel-quid and areca-nut chewing and some areca-nut derived nitrosamines. 2004.)
Areca nut with added tobacco cause pancreatic
tumours, too.
(IARC. A review of human carcinogens. 2012)
There is also limited evidence that areca nut causes
liver cancer.
(A review of human carcinogens–Part E. Lancet Oncol 2009;10:1033–34)
Introduction (contd.)

7/15/2014
3
Recent epidemiological studies show that betel quid
use is associated with a higher risk of:
obesity,
metabolic syndromes,
cardiovascular disease,
type 2 diabetes
chronic kidney disease,
low birth weight and
cirrhosis of the liver.
Introduction (contd.)
(Chien-Hung Lee et al. Intercountry prevalences and practices of betel-quid use in south, southeast and eastern
Asia regions and associated oral preneoplastic disorders .Int J Cancer, 2011 Oct 1;129(7):1741-51.)
In Myanmar, prevalence of smoking is getting lower
(22% in 2009) but that of smokeless tobacco use,
mostly in betel quid, is still high in Myanmar (30%).
The majority of these smokeless tobacco users used it
in a form of betel quid.
In Myanmar, oral cancer, a serious consequence of
betel chewing, stood at the 6th among male caners
and 10th among female cancers, contributing 3.5% of
the whole body cancers, according to cancer
registries of Yangon and Mandalay General
Hospitals.
Introduction (contd.)
7/15/2014
4
Community-based surveys on betel chewing and oral
health were scare and outdated in Myanmar and
updateted epidemiological information on these
issues is needed.
So this study tried to help fill this information gap to
some extent.
Introduction (contd.)
Objectives
The study aims to assess betel quid chewing practice
and its relation to oral pre-cancerous lesions in adult
population in Dagon (East) township.
The study has the following specific objectives:
To determine the prevalence of betel quid chewing
in adult population of Dagon (East) township.
To describe the characteristics of betel quid
chewing practice
To assess its relation to oral pre-cancerous lesions

7/15/2014
5
Methodology
Study Design: cross-sectional design
Study Place: Dagon (East) township, Yangon Region
Study Population: persons aged 18 years and above of both sexes
Excluded - very ill persons and mentally ill persons.
Methodology (contd.)
Sample Size Determination
Using the formula for one sample proportion with the following assumptions:
Alpha error is set at 5%, so, ‘z’ statistics is 1.96;
P was conservatively estimated at 50% ( the exact prevalence of betel quid chewing in Myanmar is unknown)
Margin of error (e) is 5%;
Rate of refusal to participate is10%.
Required sample size was 428 persons.

7/15/2014
6
Methodology (contd.)
Sampling procedure
Four hundred and twenty two households were
selected from Ward 133: one hundred and twenty
two households were selected from Sit-Pin village.
One eligible person was selected from each
selected household.
Methodology (contd.)
Data collection
Data collection was done in April, 2013.
By using a pretested structured questionnaire, 11
trained interviewers from DMR(Lower Myanmar)
collected from the respondents the following data
on:
socioeconomic characteristics
betel quid chewing practice
alcohol drinking
smoking

7/15/2014
7
Methodology (contd.)
Data collection
Photos showing
field data collection
Methodology (contd.)
Data collection
5 oral examination teams comprising 13 dental
surgeons and 8 dental house surgeons from
University of Dental Medicine (Yangon) made oral
examination on every respondent.
Toluidine blue staining and oral brush biopsy
were done on the respondents with visible oral
lesions.
When these oral lesions were positive by Toluidine
blue stain and/or oral brush biopsy, these were
regarded as potentially malignant.

7/15/2014
8
Methodology (contd.)
Data collection
Photos showing oral examination
Methodology (contd.)
Data collection
Photo showing
Toluidine blue staining
Photo showing
oral brush biopsy specimen

7/15/2014
9
Methodology (contd.)
Data management and analysis
Prevalence of betel quid chewing was calculated
by age and sex.
Characteristics of betel quid chewing practice were
described for men and women and both sexes.
Prevalence of oral potentially malignant disorders
was determined by major health risk behaviours.
Multiple logistic regression was performed to
determine the independent effect of health risk
behaviours on oral pre-cancers, controlling for
possible confounders.
Methodology (contd.)
Ethical considerations
The proposal was approved for ethical clearance
by the Ethical Review Committee of the Department
of Medical Research (Lower Myanmar).
Informed consent was obtained from the
respondents for interview and oral examination.

7/15/2014
10
542 persons aged 18 years and above participated
in the survey.
Results
Age and sex distribution of the respondents
Age
Male Female Total
18-24 years 28 [5.17%] 31 [5.72%] 59 [10.89%]
24-44 years 92 [16.97%] 128 [23.62%] 220 [40.59%]
45-64 years 78 [14.39%] 125 [23.06%] 203 [37.45%]
65+ years
23 [4.24%]
37 [6.83%]
60 [11.09%]
Total 221 [40.77%]
321 [59.23%]
542 [100%]

7/15/2014
11
Prevalence of current betel quid chewing
among the respondents by sex and age
Sex and age Pop.
Chewers of b etel quid
without tobacco with tobacco total
Male 221 7 [3.2%]
[95%CI= 1.2 to 6.4% ]
153 [69.2%]
[95%CI=62.7 to75 .2%]
160 [72.4%]
[95%CI=66 to 78.2%]
18-24 years 28 2 [7.1%] 19 [67.9%] 21 [75%]
24-44 years 92 1 [1.1%] 74 [80.4%] 75 [81.5%]
45-64 years 78 4 [5.1%] 49 [62.8%] 53 [68.0%]
65+ years 23 0 [0%] 11 [47.8%] 11 [ 48.8%]
Female 321 37 [11.5%]
[95%CI=8.2 to 15.5%]
87 [27.1%]
[95%CI= 22.3 to 32.3% ]
124 [38.6%]
[95%CI= 33.3 to 4.2% ]
18-24 years 31 2 [6.5%] 2 [6.5%] 4 [12.9%]
24-44 years 128 13 [10.2%] 38 [29.7%] 51 [39.8%]
45-64 years 125 17 [13.6 %] 41 [32.8%] 58 [46.4%]
65+ years 37 5 [13.5%] 6 [16.2%] 11 [29.7%]
Total 542 44 [8.1%]
[95%CI= 6 to10.7% ]
240 [44.3%]
[95%CI= 40 to 48.6% ]
284 [52.4%]
[95%CI= 48 to 56.7% ]
18-24 years 59 4 [6.8%] 21 [35.6%] 25 [42.4%]
24-44 y ears 200 14 [6.4%] 112 [10.9%] 126 [57.3%]
45-64 years 203 21 [10.3%] 90 [44.3%] 111 [54.7%]
65+ years 60 5 [8.3%] 17 [28.3%] 22 [36.7%]
Prevalence of current betel quid chewing
among the respondents by sex and age
Sex and age Pop.
Chewers of b etel quid
without tobacco with tobacco total
Male 221 7 [3.2%]
[95%CI= 1.2 to 6.4% ]
153 [69.2%]
[95%CI=62.7 to75 .2%]
160 [72.4%]
[95%CI=66 to 78.2%]
18-24 years 28 2 [7.1%] 19 [67.9%] 21 [75%]
24-44 years 92 1 [1.1%] 74 [80.4%] 75 [81.5%]
45-64 years 78 4 [5.1%] 49 [62.8%] 53 [68.0%]
65+ years 23 0 [0%] 11 [47.8%] 11 [ 48.8%]
Female 321 37 [11.5%]
[95%CI=8.2 to 15.5%]
87 [27.1%]
[95%CI= 22.3 to 32.3% ]
124 [38.6%]
[95%CI= 33.3 to 4.2% ]
18-24 years 31 2 [6.5%] 2 [6.5%] 4 [12.9%]
24-44 years 128 13 [10.2%] 38 [29.7%] 51 [39.8%]
45-64 years 125 17 [13.6 %] 41 [32.8%] 58 [46.4%]
65+ years 37 5 [13.5%] 6 [16.2%] 11 [29.7%]
Total 542 44 [8.1%]
[95%CI= 6 to10.7% ]
240 [44.3%]
[95%CI= 40 to 48.6% ]
284 [52.4%]
[95%CI= 48 to 56.7% ]
18-24 years 59 4 [6.8%] 21 [35.6%] 25 [42.4%]
24-44 y ears 200 14 [6.4%] 112 [10.9%] 126 [57.3%]
45-64 years 203 21 [10.3%] 90 [44.3%] 111 [54.7%]
65+ years 60 5 [8.3%] 17 [28.3%] 22 [36.7%]
Overall prevalence = 52.4%

7/15/2014
12
Prevalence of current betel quid chewing by sex
72.4%
38.6%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
Male (n=221) Female (n=321)
Curr
en
t b
ete
l ch
ew
ers
Prevalence of current betel quid chewing by age
75.0%
81.5%
68.0%
48.8%
12.9%
39.8%
46.4%
29.7%
Male 18-24years
(n=28)
24-44years
(n=92)
45-64years
(n=78)
65+years
(n=23)
Female 18-24years
(n=31)
24-44years
(n=128)
45-64years
(n=128)
65+years
(n=37)

7/15/2014
13
Prevalence of current betel quid chewing by age
75.0%
81.5%
68.0%
48.8%
12.9%
39.8%
46.4%
29.7%
Male 18-24years
(n=28)
24-44years
(n=92)
45-64years
(n=78)
65+years
(n=23)
Female 18-24years
(n=31)
24-44years
(n=128)
45-64years
(n=128)
65+years
(n=37)
Addition of tobacco to betel quid
Among 284 current chewers,
240 (85%) added tobacco to
betel quid.

7/15/2014
14
62.9%
30.8%
19.6%15.4%
7.5% 7.1%4.2% 3.3% 2.1%
Kinds of tobacco consumed with betel quids among chewers of betel quid with tobacco (n=240) *
*Multiple responses
Photo showing some kinds of tobacco
added to betel quids
7/15/2014
15
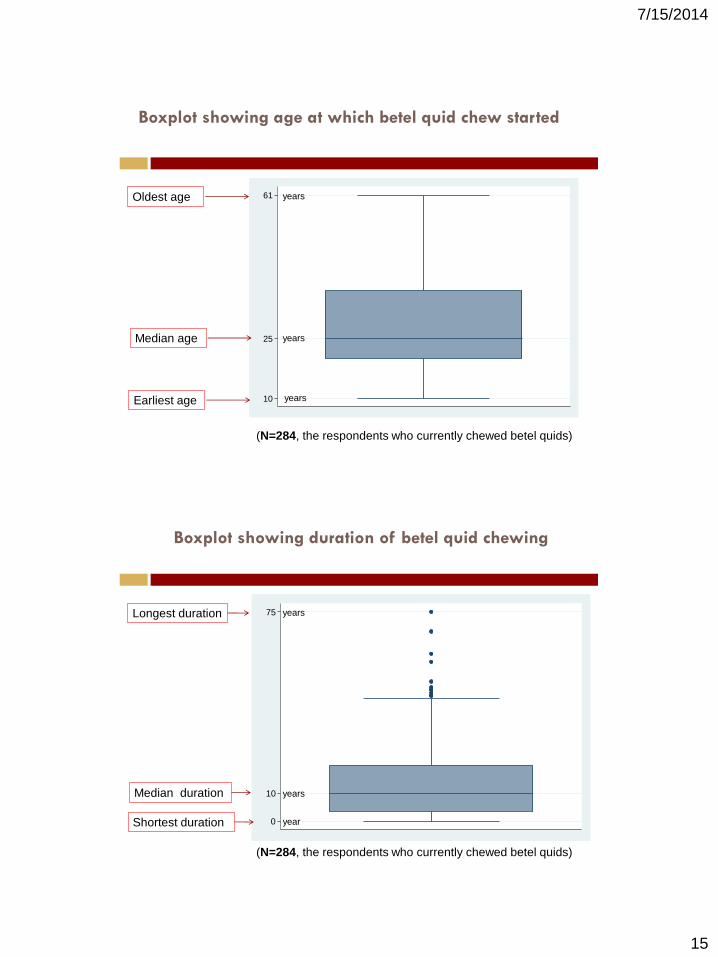
Boxplot showing age at which betel quid chew started
10
25
61Oldest age
Median age
Earliest age
(N=284, the respondents who currently chewed betel quids)
years
years
years
0
10
75
Boxplot showing duration of betel quid chewing
Longest duration
Median duration
Shortest duration
years
years
year
(N=284, the respondents who currently chewed betel quids)

7/15/2014
16
1
8
100
Boxplot showing number of betel quids chewed per day
Highest number
Median number
Lowest number
quids
quids
quid
(N=284, the respondents who currently chewed betel quids)
Ways of dealing with betel quid juice among the
respondents who currently chewed betel quids
Swallow (2.8%)
Spit out (88.7%)
Both swallow and spit
out (8.5%)
(N=284, the respondents who currently chewed betel quids)
7/15/2014
17
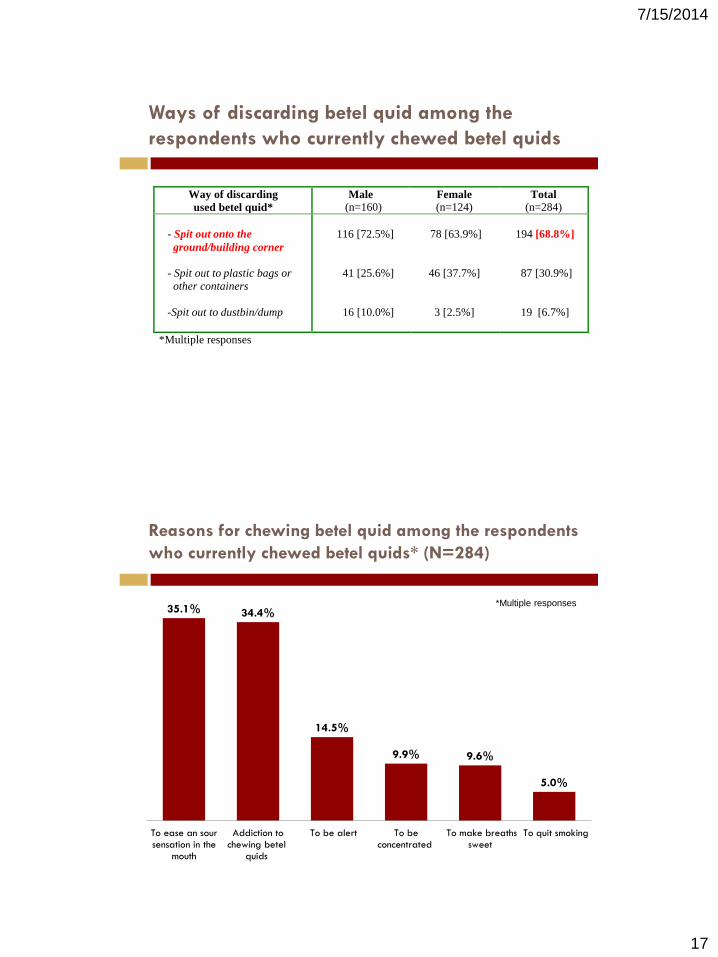
Ways of discarding betel quid among the
respondents who currently chewed betel quids
Way of discarding
used betel quid*
Male
(n=160) Female
(n=124) Total
(n=284)
- Spit out onto the
ground/building corner
- Spit out to plastic bags or
other containers
-Spit out to dustbin/dump
116 [72.5%]
41 [25.6%]
16 [10.0%]
78 [63.9%]
46 [37.7%]
3 [2.5%]
194 [68.8%]
87 [30.9%]
19 [6.7%]
*Multiple responses
Reasons for chewing betel quid among the respondents
who currently chewed betel quids* (N=284)
35.1% 34.4%
14.5%
9.9% 9.6%
5.0%
To ease an soursensation in the
mouth
Addiction tochewing betel
quids
To be alert To beconcentrated
To make breathssweet
To quit smoking
*Multiple responses

7/15/2014
18
Out of 542 persons, 25 persons (4.6%) turned out to
have visible oral lesions (ulcer or patch) which tested
positive for Toludine blue staining and/or oral brush
biopsy (95%CI=3.0 to 6.7).
These oral lesions were regarded as potentially
malignant (precancerous).
Prevalence of oral potentially malignant lesions
Prevalence and unadjusted risk of oral precancer
by three major lifestyles
Pop. Oral potentially malignant lesions
Number Percent [95% CI] Crude Odds Ratio
Betel quid chewing habit
Non-chewers (Ref. group) 258 1 0.4 [0 to 2.1] 1
Chewers without tobacco 44 1 2.3 [0.06 to 12] 6 [2 to 17]
Chewers with tobacco 240 23 9.6 [6.2 to 14] 27 [12 to 62]
Smoking habit
Non-smoker (Ref. group) 371 17 4.6 [2.7 to 7.2] 1
Smoker 171 8 4.7 [2.0 to 9.0] 1.02 [0.4 to 2.6]
Alcohol drinking habit
Non-drinker (Ref. group) 451 17 3.8 [2.2 to 6.0] 1
Drinker 91 8 8.8 [3.9 to 16.6] 2.5 [1.1 to 5.7]
7/15/2014
19
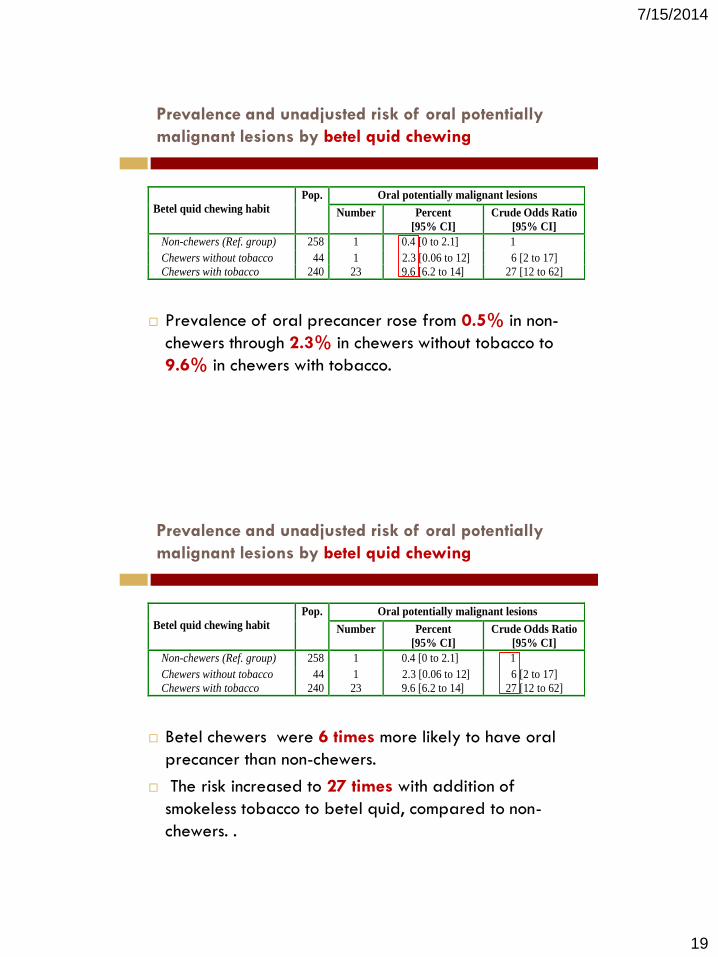
Prevalence and unadjusted risk of oral potentially
malignant lesions by betel quid chewing
Prevalence of oral precancer rose from 0.5% in non-
chewers through 2.3% in chewers without tobacco to
9.6% in chewers with tobacco.
Betel quid chewing habit
Pop. Oral potentially malignant lesions
Number Percent
[95% CI]
Crude Odds Ratio
[95% CI]
Non-chewers (Ref. group) 258 1 0.4 [0 to 2.1] 1
Chewers without tobacco 44 1 2.3 [0.06 to 12] 6 [2 to 17]
Chewers with tobacco 240 23 9.6 [6.2 to 14] 27 [12 to 62]
Prevalence and unadjusted risk of oral potentially
malignant lesions by betel quid chewing
Betel chewers were 6 times more likely to have oral
precancer than non-chewers.
The risk increased to 27 times with addition of
smokeless tobacco to betel quid, compared to non-
chewers. .
Betel quid chewing habit
Pop. Oral potentially malignant lesions
Number Percent
[95% CI]
Crude Odds Ratio
[95% CI]
Non-chewers (Ref. group) 258 1 0.4 [0 to 2.1] 1
Chewers without tobacco 44 1 2.3 [0.06 to 12] 6 [2 to 17]
Chewers with tobacco 240 23 9.6 [6.2 to 14] 27 [12 to 62]
7/15/2014
20
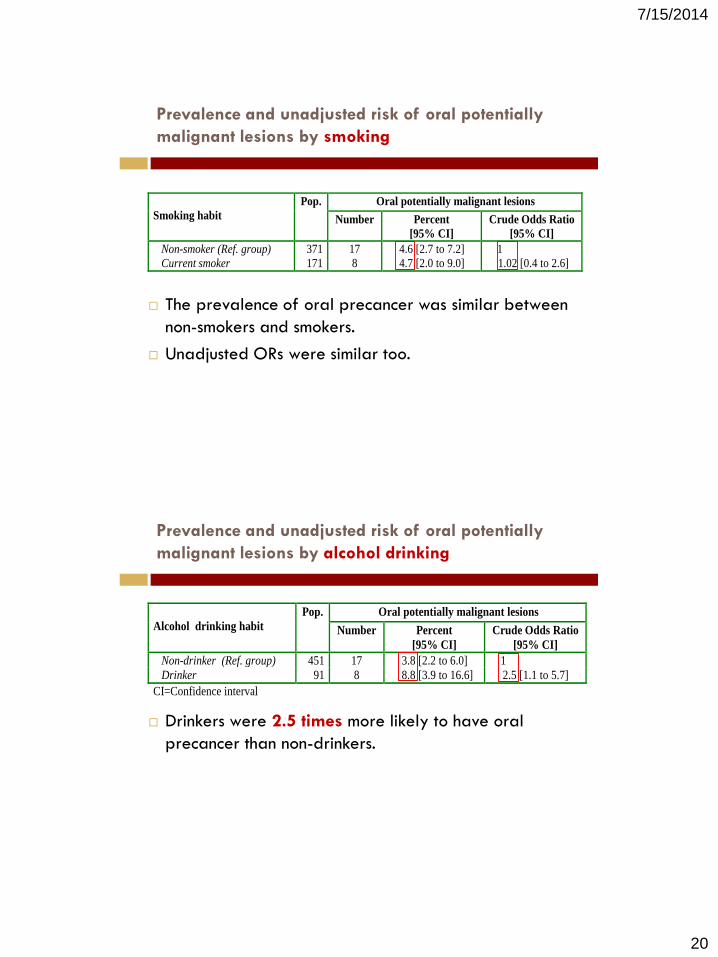
The prevalence of oral precancer was similar between
non-smokers and smokers.
Unadjusted ORs were similar too.
Prevalence and unadjusted risk of oral potentially
malignant lesions by smoking
Smoking habit
Pop. Oral potentially malignant lesions
Number Percent
[95% CI]
Crude Odds Ratio
[95% CI]
Non-smoker (Ref. group) 371 17 4.6 [2.7 to 7.2] 1
Current smoker 171 8 4.7 [2.0 to 9.0] 1.02 [0.4 to 2.6]
Alcohol drinking habit
Pop. Oral potentially malignant lesions
Number Percent
[95% CI]
Crude Odds Ratio
[95% CI]
Non-drinker (Ref. group) 451 17 3.8 [2.2 to 6.0] 1
Drinker 91 8 8.8 [3.9 to 16.6] 2.5 [1.1 to 5.7]
CI=Confidence interval
Drinkers were 2.5 times more likely to have oral
precancer than non-drinkers.
Prevalence and unadjusted risk of oral potentially
malignant lesions by alcohol drinking

7/15/2014
21
Odds ratios of oral precancer from multiple logistic
regression according to demographic and major
lifestyles characteristics
Multiple logistic regression was performed to determine
the independent effect of demographic and life style
factors on oral pre-cancer.
Initially, 5 variables (age, sex, betel chewing, smoking
and alcohol drinking, , all of which were defined as
categorical, were included in the model.
In the final model, only 4 variables (age, sex, betel
chewing and alcohol drinking) remained: smoking was
omitted because it was multicollinear with alcohol
drinking.
Odds ratios of oral potentially malignant lesions
from multiple logistic regression according to four
demographic and major lifestyles characteristics
Variable Adjusted Odds Ratio 95% Confidence Interval
Age
<=40 years (Ref. group) 1.0
40-60 years 1.5 0.6 to 4.2
60+ years 2.0 0.7 to 5.7
Sex
Female (Ref. group) 1.0
Male 0.7 0.3 to 1.7
Betel quid chewing habit
Non-chewers (Ref. group) 1.0
Chewers without tobacco 5.7* 1.4 to 22.9
Chewers with tobacco 28.6* 9.8 to 83.6
Alcohol drinking habit
Non-drinker (Ref. group) 1.0
Drinker 1.6 0.7 to 4.0
*Significant at 0.05 level

7/15/2014
22
Odds ratios of oral potentially malignant lesions
from multiple logistic regression according to four
demographic and major lifestyles characteristics
Betel chewing is significantly associated with risk of oral pre-cancer.
Chewers of betel quid alone has 6-fold increase and chewers of
betel quid with tobacco 29-fold increase in risk of oral precancer,
compared to non-chewers.
Variable Adjusted Odds Ratio 95% Confidence Interval
Age
<=40 years (Ref. group) 1.0
40-60 years 1.5 0.6 to 4.2
60+ years 2.0 0.7 to 5.7
Sex
Female (Ref. group) 1.0
Male 0.7 0.3 to 1.7
Betel quid chewing habit
Non-chewers (Ref. group) 1.0
Chewers without tobacco 5.7* 1.4 to 22.9
Chewers with tobacco 28.6* 9.8 to 83.6
Alcohol drinking habit
Non-drinker (Ref. group) 1.0
Drinker 1.6 0.7 to 4.0
*Significant at 0.05 level
Odds ratios of oral potentially malignant lesions
from multiple logistic regression according to four
demographic and major lifestyles characteristics
Old age, female sex and alcohol drinking were also
associated with increased risk of oral pre-cancer but their
relationship was not significant.
Variable Adjusted Odds Ratio 95% Confidence Interval
Age
<=40 years (Ref. group) 1.0
40-60 years 1.5 0.6 to 4.2
60+ years 2.0 0.7 to 5.7
Sex
Female (Ref. group) 1.0
Male 0.7 0.3 to 1.7
Betel quid chewing habit
Non-chewers (Ref. group) 1.0
Chewers without tobacco 5.7* 1.4 to 22.9
Chewers with tobacco 28.6* 9.8 to 83.6
Alcohol drinking habit
Non-drinker (Ref. group) 1.0
Drinker 1.6 0.7 to 4.0
*Significant at 0.05 level

7/15/2014
23
Discussion
Half of this population were currently chewing betel
quids.
This prevalence of betel chewing is quite high given
the global estimate of 10-20% and regional
estimates of 20%-40% in India, Pakistan and Nepal
over the last two decades.
Discussion(contd.)
In the current study, 85% of the betel quid chewers
added tobacco, comparable to levels for Dhaka,
Bangladesh (85.2%) (Rahman et al.).
Current betel quid chewing in men was highest (81%)
in the most productive age group (24-44 years).
Betel quid chewers mostly started betel chewing
practice around 25 years of age, chewed 8 betel
quids per day for 10 years or more.

7/15/2014
24
4.6% of study population had oral precancer as
determined by rapid screening tests (Toludine blue
staining and oral brush biopsy).
Prevalence of oral precancer in current chewers of
betel quid without tobacco (2.3%) increased to
nearly 10% with addition of smokeless tobacco to
betel quid.
This finding provides additional evidence for
formulating policy on control of smokeless tobacco
use in Myanmar.
Discussion(contd.)
Multiple logistic regression indicated that older age,
betel chewing, especially with tobacco and
consumption of alcohol were associated with risk of
oral pre-cancer.
These findings are consistent with the internationally
established risk factors for oral pre-cancer.
Discussion(contd.)

7/15/2014
25
Conclusion
Betel quid chewing was found to be a common habit
in both men and women of the study population
Because betel quid chewing have serious health
consequences, an anti-betel quid chewing programme
is warranted for current chewers.
Health risks of betel quid chewing should be
emphasized in the health education to the public and
especially betel chewers.
Regular oral examination of betel quid chewers may
help prevent avoidable oral cancers in the future.
Conclusion
As the habit is rooted in Myanmar tradition and
culture, anthropological studies are indicated for
designing appropriate educational campaigns.
7/15/2014
26
Utilization of research findings
The findings were provided to the tobacco control
program of Department of Health for future
programming and policy formulation.
The persons who tested positive for Toluidine blue
stain and oral brush biopsy were referred to
University of Dental Medicine for further
investigation, regular follow-up and necessary
treatment.
Acknowledgements
We wish to thank all respondents who gave up their time
to be interviewed and examined and who welcomed
interviewers into their homes.
We thank local health staff from Urban Health Center in
Ward 133 and from Sitpin RHC, Dagon (East) Township.
We would also like to appreciate the commitment and
professionalism of the interviewers from Department of
Medical Research (Lower Myanmar) and oral
examination teams from University of Dental Medicine
(Yangon).
7/15/2014
27
References
IARC Monographs Program. A review of human carcinogens–Part E. Lancet Oncol
2009;10:1033–34.
Gupta PC, Ray CS. Epidemiology of betel quid usage. Ann Acad Med Singapore
2004; 33:31–6.
Gupta PC, Warnakulasuriya S. Global epidemiology of areca nut usage. Addict
Biol 2002;7:77–83.
Ministry of Information. Myanmar Encyclopaedia. CD-ROM; Myanmar 2005.
IARC. Tobacco habits other than smoking; betel quid and areca-nut chewing and
some related nitrosamines. IARC Monograph on the Evaluation of Carcinogenic Risk
of Chemicals to Humans, Vol 37. Lyon: International Agency for Research on Cancer;
1985.
IARC. Betel-quid and areca-nut chewing and some areca-nut derived nitrosamines.
IARC Monograph on the Evaluation of Carcinogenic Risk of Chemicals to Humans, Vol
58. Lyon: International Agency for Research on Cancer; 2004.
References (contd.)
IARC. A review of human carcinogens. IARC Monograph on the Evaluation of
Carcinogenic Risk of Chemicals to Humans, Vol 100. Lyon: International Agency for
Research on Cancer; 2012.
Chien-Hung Lee1, Albert Min-Shan Ko, Saman Warnakulasuriya. Intercountry
prevalences and practices of betel-quid use in south, southeast and eastern Asia
regions and associated oral preneoplastic disorders: An international collaborative
study by Asian betel-quid consortium of south and east asia. Int J Cancer. 2011 Oct
1;129(7):1741-51.
World Health Organization. Non-communicable Disease Risk Factor Survey
Myanmar 2009. New Delhi : WHO Regional Office for South-East Asia; 2011.
Mazahir S, Malik R, Maqsood M, Merchant KA, Malik F, Majeed A, et al. Socio-
demographic correlates of betel, areca and smokeless tobacco use as a high risk
behaviour for head and neck cancers in a squatter settlement of Karachi, Pakistan.
Subst Abuse Treat Prev Policy. 2006; 26: 10-15.
7/15/2014
28
References
Rahman M, Rahman M, Flora MS, Akter SFU, Hossain S, Mascie-Taylor CGN.
Behavioural risk factors of non-communicable diseases in Bangladesh. Dhaka:
National Institute of Preventive and Social Medicine, 2006.
Meerjady S F, Christopher GN M-T, Mahmudur R. Betel quid chewing and its risk
factors in Bangladeshi adults. WHO South-East Asia Journal of Public Health
2012;1(2):169-181.
Thank you for the kind attention!