best practices in newborn care in covid-19 times: an
TRANSCRIPT

1/17
Special Section COVID-19
Texto & Contexto Enfermagem 2020, v. 29: e20200242ISSN 1980-265X DOI https://doi.org/10.1590/1980-265X-TCE-2020-0242
HOW CITED: Góes FGB, Santos AST, Lucchese I, Silva LJ, Silva LF, Silva MA. Best practices in newborn care in COVID-19 times: an integrative review. Texto Contexto Enferm [Internet]. 2020 [cited YEAR MONTH DAY]; 29:e20200242. Available from: https://doi.org/10.1590/1980-265X-TCE-2020-0242
BEST PRACTICES IN NEWBORN CARE IN COVID-19 TIMES: AN INTEGRATIVE REVIEW
Fernanda Garcia Bezerra Góes1
Andressa Silva Torres dos Santos1 Ingrid Lucchese1
Laura Johanson da Silva2 Liliane Faria da Silva3
Maria da Anunciação Silva1 1Universidade Federal Fluminense. Rio das Ostras, Rio de Janeiro, Brasil.
2Universidade Federal do Estado do Rio de Janeiro. Rio de Janeiro, Rio de Janeiro, Brasil.3Universidade Federal Fluminense. Niterói, Rio de Janeiro, Brasil.
ABSTRACT
Objective: to identify scientific evidence on best practices in newborn care, from the delivery room to the home, in COVID-19 times. Method: an integrative review conducted in April 2020 at National Library of Medicine National Institutes of Health (PubMed), Cumulative Index to Nursing and Allied Health Literature (CINAHL), and Scopus, through combinations between the controlled terms “newborn”, “coronavirus infections”, and “COVID-19”. Results: nineteen studies made up the final sample, from which five analytical categories emerged on best practices in newborn care: Pregnant women and puerperal women suspected of having COVID-19; Pregnant and puerperal women with confirmation for COVID-19; Newborns suspected of having COVID-19; Newborns with confirmation for COVID-19; and Horizontal transmission prevention of COVID-19 to newborns. Conclusion: several recommendations were divergent, due to the contemporary pandemic of COVID-19. Therefore, the role of nurses is essential for adherence to best practices, which are proven and recommended nationally and internationally, taking into account the local reality and the constant updating of the theme. Therefore, further research is needed, especially with a strong level of evidence, for formulation of assistance guidelines for this population group that contribute to reducing neonatal morbidity and mortality and healthy and harmonious child development during and post-pandemic.
DESCRIPTORS: Newborn. Pandemic. COVID-19. Coronavirus infections. Nursing.

Texto & Contexto Enfermagem 2020, v. 29: e20200242ISSN 1980-265X DOI https://doi.org/10.1590/1980-265X-TCE-2020-0242
2/17
BOAS PRÁTICAS NO CUIDADO AO RECÉM-NASCIDO EM TEMPOS DE COVID-19: REVISÃO INTEGRATIVA
RESUMO
Objetivo: identificar evidências científicas sobre boas práticas no cuidado ao recém-nascido, da sala de parto ao domicílio, em tempos de COVID-19. Método: revisão integrativa realizada em abril de 2020, nos recursos informacionais National Library of Medicine National Institutes of Health (PubMed), Cumulative Index to Nursing and Allied Health Literature (CINAHL) e Scopus, por meio de combinações entre os termos controlados “newborn”, “coronavirus infections” e “COVID-19”. Resultados: dezenove estudos compuseram a amostra final, dos quais emergiram cinco categorias analíticas sobre as boas práticas no cuidado ao recém-nascido: gestantes e puérperas com suspeita da COVID-19; gestantes e puérperas com confirmação da COVID-19; recém-nascido com suspeita da COVID-19; recém-nascido com confirmação da COVID-19; e prevenção da transmissão horizontal da COVID-19 ao recém-nascido. Conclusão: diversas recomendações foram divergentes, decorrentes da contemporaneidade da pandemia da COVID-19. Logo, é essencial o papel do enfermeiro para a adesão às boas práticas comprovadas e recomendadas nacionalmente e internacionalmente, levando em consideração a realidade local e a atualização constante na temática. Assim sendo, são necessárias novas pesquisas, especialmente com nível de evidência forte, para a formulação de diretrizes assistenciais a esse grupo populacional que contribuam para a redução da morbimortalidade neonatal e o desenvolvimento infantil saudável e harmonioso durante e pós-pandemia.
DESCRITORES: Recém-nascido. Pandemias. COVID-19. Infecções por coronavírus. Enfermagem.
BUENAS PRÁCTICAS EN EL CUIDADO DEL RECIÉN NACIDO EN COVID-19 TIMES: REVISIÓN INTEGRATIVA
RESUMEN
Objetivo: identificar evidencia científica sobre buenas prácticas en el cuidado del recién nacido, desde la sala de partos hasta el hogar, en tiempos de COVID-19. Método: revisión integradora realizada en abril de 2020, en los recursos de información National Library of Medicine National Institutes of Health (PubMed), Cumulative Index to Nursing and Allied Health Literature (CINAHL) y Scopus, a través de combinaciones entre términos controlados “newborn”, “coronavirus infections” y “COVID-19”. Resultados: diecinueve estudios constituyeron la muestra final, de la cual surgieron cinco categorías analíticas sobre buenas prácticas en el cuidado del recién nacido: Mujeres embarazadas y puerperales con sospecha de COVID-19; Mujeres embarazadas y puerperales con confirmación de COVID-19; Recién nacido con sospecha de COVID-19; Recién nacido con confirmación de COVID-19; y Prevención de la transmisión horizontal de COVID-19 al recién nacido. Conclusión: varias recomendaciones fueron divergentes, como resultado de la pandemia contemporánea de COVID-19. Por lo tanto, el papel de las enfermeras es esencial para el cumplimiento de las buenas prácticas que se prueban y recomiendan a nivel nacional e internacional, teniendo en cuenta la realidad local y la actualización constante del tema. Por lo tanto, se necesita más investigación, especialmente con un alto nivel de evidencia, para la formulación de pautas de asistencia para este grupo de población que contribuyan a la reducción de la morbilidad y mortalidad neonatal y al desarrollo infantil sano y armonioso durante y después de la pandemia.
DESCRIPTORES: Recién nacido. Pandemias. COVID-19. Infecciones por coronavirus. Enfermería.

Texto & Contexto Enfermagem 2020, v. 29: e20200242ISSN 1980-265X DOI https://doi.org/10.1590/1980-265X-TCE-2020-0242
3/17
INTRODUCTION
The Coronavirus Disease 2019 (COVID-19) pandemic, caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is a serious worldwide public health problem with serious health, social, economic and political impacts. As of mid-June 2020, the World Health Organization (WHO) recorded more than 8 million cases and more than 450,000 deaths worldwide. These numbers continue to rise, including in Brazil, which, in that same period, was ranking second in number of cases worldwide.1
Many uncertainties remain about the natural history and clinical management of this disease.2 Studies on vaccines and specific treatments are still ongoing.3 However, births continue in the life cycle of humanity during this pandemic, which increases doubts about newborn care, from the delivery room to the home, during this pandemic.
A systematic review showed that children account for 1% to 5% of diagnosed cases of the disease, usually presenting milder symptoms than adults, with rare cases of death.4 To date, transplacental transmission of SARS-CoV-2 to a newborn from an infected mother in the last trimester of pregnancy has been demonstrated only once.5 This is consistent with sparse reports of positive newborns for COVID-19 on the first day of life, without any evidence of contact with infected adults.6 Therefore, most authors have described cases of newborns infected after delivery.7–8
Newborns of mothers with a positive diagnosis for SARS-CoV-2 who have had close contact with someone suspected or confirmed with the disease and/or live or traveled to areas with high numbers of cases are considered to be at high risk for COVID -19. Most of the clinical manifestations of infected newborns are not specific. When they occur, they stand out, especially in premature babies, with cardiovascular and gastrointestinal dysfunction, thermal instability and dominant respiratory problems. In severe cases, they can quickly develop Acute Respiratory Discomfort Syndrome.9–10 However, to the extent that the neonatal immune function is immature, attention should be paid to the risk of neonatal COVID-19 and the possibility of the condition becoming serious.
Carelessly performed care in the neonatal period can cause serious damage to the health of newborns, affecting healthy and harmonious child survival and development. Thus, it is imperative that nurses develop care practices and updated guidelines to ensure safe and quality postnatal care, always valuing the family and the community.11
Therefore, it is necessary to map the best evidence on the theme that support the assistance, educational and/or management actions of nurses and their teams during and after the COVID-19 pandemic, aiming at promoting health as well as reducing neonatal morbidity and mortality. Thus, this study aims to identify scientific evidence on best practices in newborn care, from the delivery room to the home, in COVID-19 times.
METHOD
This is an integrative literature review developed using six methodological steps.12 The research question was elaborated by PICo strategy that recommends as fundamental elements: P - Population; I- Interest; and Co - Context.13 Thus, the elements were defined: P - newborn; I - care; and Co - COVID-19. Therefore, the research question was: what is known so far in the scientific literature on newborn care, from the delivery room to the home, in COVID-19 times?
The stage of identification of studies involved the search for scientific evidence in different information resources, namely: National Library of Medicine National Institutes of Health (PubMed), Cumulative Index to Nursing and Allied Health Literature (CINAHL), and Scopus. They were selected due to the scope in the international context. The controlled terms were used in English, associated in pairs, using the Boolean operator “AND”: “newborn”, “coronavirus infections”, and “COVID-19”.
Texto & Contexto Enfermagem 2020, v. 29: e20200242ISSN 1980-265X DOI https://doi.org/10.1590/1980-265X-TCE-2020-0242
4/17
Based on the associations, skimming of titles and abstracts began to select articles. Data production took place at the end of April 2020.
Original articles, literature reviews, case studies, expert opinions, expert reports and editorials in full and with recommendations for newborns on the topic were included. Duplicate manuscripts (duplicate manuscripts were considered only once) were excluded. There was no time cut.
Search and selection of the studies included in the review was carried out by pairs of reviewers independently for each information resource. All doubts that arose in this process were discussed and solved in a panel among all reviewers until a consensus was reached.
In the mapping of the main information items obtained from the studies, an instrument was developed to characterize each production, including code, title, country, year, source, type of study, objective, level of evidence and recommendations, for best practices.
Level of evidence was identified based on the study design by the following criteria: I - systematic reviews and meta-analysis of randomized clinical trials; II - randomized clinical trials; III - non-randomized controlled trial; IV - case-control or cohort studies; V - systematic reviews of qualitative or descriptive studies; VI - qualitative or descriptive studies; and VII - opinion from authorities and/or reports from expert committees. This hierarchy classifies levels I and II as strong, III to V as moderate and VI and VII as weak.14
RESULTS
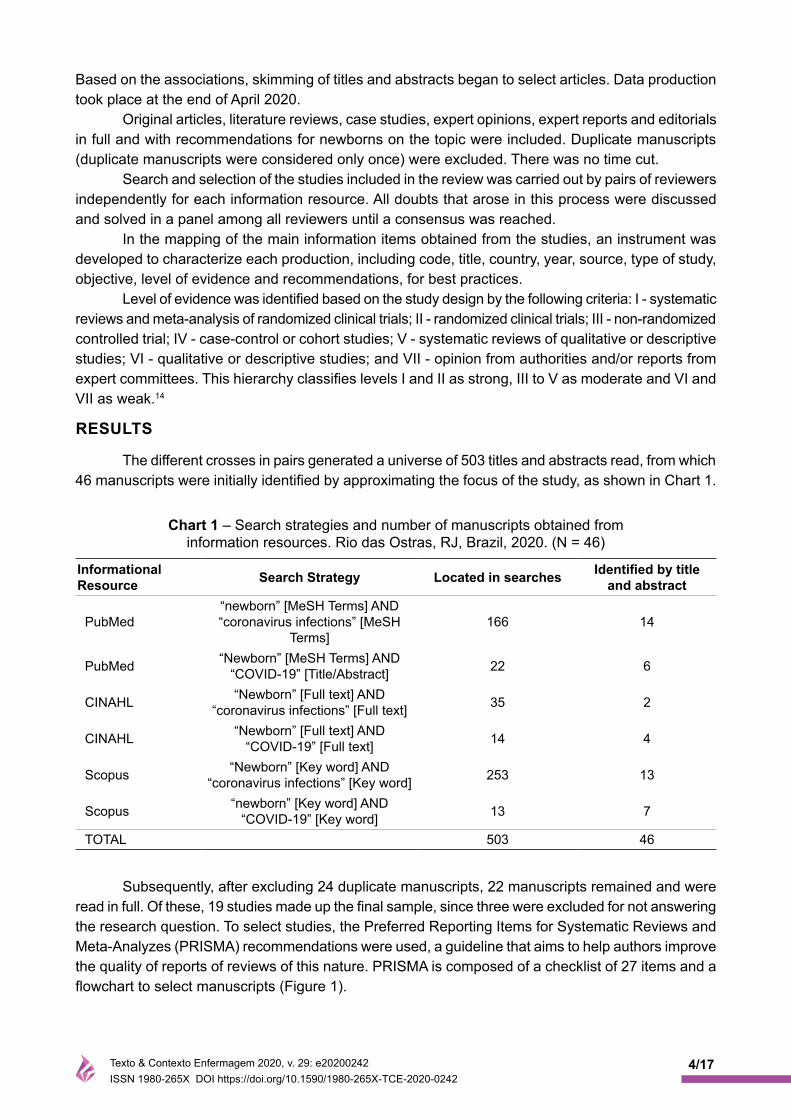
The different crosses in pairs generated a universe of 503 titles and abstracts read, from which 46 manuscripts were initially identified by approximating the focus of the study, as shown in Chart 1.
Chart 1 – Search strategies and number of manuscripts obtained from information resources. Rio das Ostras, RJ, Brazil, 2020. (N = 46)
Informational Resource Search Strategy Located in searches Identified by title
and abstract
PubMed“newborn” [MeSH Terms] AND “coronavirus infections” [MeSH
Terms]166 14
PubMed “Newborn” [MeSH Terms] AND “COVID-19” [Title/Abstract] 22 6
CINAHL “Newborn” [Full text] AND “coronavirus infections” [Full text] 35 2
CINAHL “Newborn” [Full text] AND “COVID-19” [Full text] 14 4
Scopus “Newborn” [Key word] AND “coronavirus infections” [Key word] 253 13
Scopus “newborn” [Key word] AND “COVID-19” [Key word] 13 7
TOTAL 503 46
Subsequently, after excluding 24 duplicate manuscripts, 22 manuscripts remained and were read in full. Of these, 19 studies made up the final sample, since three were excluded for not answering the research question. To select studies, the Preferred Reporting Items for Systematic Reviews and Meta-Analyzes (PRISMA) recommendations were used, a guideline that aims to help authors improve the quality of reports of reviews of this nature. PRISMA is composed of a checklist of 27 items and a flowchart to select manuscripts (Figure 1).

Texto & Contexto Enfermagem 2020, v. 29: e20200242ISSN 1980-265X DOI https://doi.org/10.1590/1980-265X-TCE-2020-0242
5/17
Figure 1 - Flowchart of identification, selection, and study inclusion oprocesses. Adaptation of the PRISMA recommendation. Rio das Ostras, RJ, Brazil, 2020.
All manuscripts were from 2020. Most were produced exclusively by researchers from China, 11 (57.9%), followed by those in partnership with Chinese with researchers from other nationalities, 3 (15.8%). Moreover, there were studies produced by French, 2 (10.5%), Danes, 1 (5.3%), North Americans, 1 (5.3%), and Israelis with North Americans, 1 (5.3%) (Chart 2).
Through critical and interpretive analysis, five analytical categories emerged dealing with best practices in newborn care in the following situations: Pregnant women and puerperal women suspected of having COVID-19; Pregnant and puerperal women with confirmation for COVID-19; Newborns suspected of having COVID-19; Newborns with confirmation for COVID-19; and Prevention of horizontal transmission of COVID-19 to newborns.
Pregnant and puerperal women suspected of having COVID-19
Five manuscripts addressed care in cases of pregnant and puerperal women suspected of having COVID-19. P115 and P216 make the same recommendation. P216 updats P115 based on three months after clinical practice of professionals following cases of the disease. Therefore, they suggest that suspected pregnant women with high fever and hypoxemia have their newborns monitored. P922 and P1326 corroborate the need for surveillance, stipulating a period for it to occur more rigorously from 14 to 21 days after birth.
P1427 adds that pregnant women suspected of having COVID-19 should undergo lung imaging tests (chest radiography and computed tomography) and diagnostic tests for the disease as soon as possible. They should be encouraged to report symptoms, immediately examined by qualified professionals and referred to the appropriate hospital, if clinically necessary. According to this study,

Texto & Contexto Enfermagem 2020, v. 29: e20200242ISSN 1980-265X DOI https://doi.org/10.1590/1980-265X-TCE-2020-0242
6/17
Chart 2 - Characterization of the selected manuscripts for analysis according to code, title, country, source, and objective. Rio das Ostras, Rio de Janeiro, Brazil, 2020.
Code/Title Country/Source ObjectiveP1 - Perinatal and neonatal management plan for prevention and control of 2019 novel coronavirus infection (1st Edition)15
ChinaChin J Contemporary Pediatr
To propose recommendations to prevent and control transmission
of infections by 2019-nCoV in newborns.
P2 - Perinatal and Neonatal Management Plan for Prevention and Control of SARS-CoV-2 Infection (2nd Edition)16
ChinaChin J Contemporary Pediatr
To update the first version to prevent and control transmission
of infections by 2019-nCoV in newborns.
P3 - Perinatal aspects on the COVID-19 pandemic: a practical resource for perinatal-neonatal specialists17
Israel and USAJ Perinatol
To summarize the available evidence and provide
perinatologists and neonatologists with practical tools to manage
their patients.
P4 - Potential maternal and infant outcomes from (Wuhan) Coronavirus 2019-nCoV infecting pregnant women: lessons from SARS, MERS, and other human coronavirus infections18
USAViruses
To analyze published data that address the epidemiological and clinical effects of SARS, MERS and other coronavirus infections
in pregnant women and their children.
P5 - Infants Born to Mothers with a New Coronavirus (COVID-19)19
ChinaFront Pediatr
To describe the clinical course of four babies born alive to pregnant women with COVID-19 infection.
P6 - Managing neonates with respiratory failure due to SARS-CoV-220
FranceLancet Child Adolesc Health Editorial
P7 - Novel corona virus disease (COVID-19) in pregnancy: what clinical recommendations to follow?21
China, Sweden, and NorwayActa Obstet Gynecol Scand Editorial
P8 - Clinical characteristics of novel coronavirus disease 2019 (COVID-19) in newborns, infants and children8
China and TaiwanPediatr Neonatol Editorial
P9 - COVID-19 virus and children: What do we know?22
FranceArch Pediatr Editorial
P10 - Dilemmas and Priorities in the Neonatal Intensive Care Unit during the COVID-19 Pandemic23
DenmarkDan Med J Editorial
P11 - Emergency plan for inter-hospital transfer of newborns with SARS-CoV-2 infection24
ChinaChin J Contemporary Pediatr
To present the instructions for newborn transference
with COVID-19; organization management; protection
strategies for the medical team; work procedures; and methods of disinfecting transfer equipment.
P12 - Emergency response plan for the neonatal intensive care unit during epidemic of 2019 novel coronavirus25
ChinaChin J of Contemporary Pediatr
To present the emergency response plan of Neonatal
Intensive Care Units during the COVID-19 epidemic.

Texto & Contexto Enfermagem 2020, v. 29: e20200242ISSN 1980-265X DOI https://doi.org/10.1590/1980-265X-TCE-2020-0242
7/17
newborns of mothers with suspicion should be isolated for 14 days after birth and closely monitored for infection clinical manifestation.
Pregnant and puerperal women confirmed by COVID-19
Nine manuscripts discussed the care to be performed before pregnant women and puerperal women with confirmation for COVID-19.15–17,21–22,24,27,30,32 According to a consensus issued by the Chinese Medical Association, COVID-19 infection is not an absolute indication for termination of pregnancy or for early delivery. Each case should be assessed,30,32 taking into account, mainly, the progression of maternal disease, gestational age and intrauterine situation of the fetus.32 In general, transplacental transmission is unlikely as the virus was not identified in the amniotic fluid, placenta, and breast milk of these mothers or in the nasal secretions of their newborns;21 however, it is still necessary to maintain a high surveillance level of newborns during 14-21 days after birth.22,27
Pregnant women diagnosed with SARS-CoV-2 should be examined immediately by qualified professionals and referred to an appropriate hospital, if clinically necessary. These patients should be admitted, preferably, to isolation rooms or wards with negative pressure. Routine prenatal care should be maintained and performed, if possible, in isolation rooms.27
Code/Title Country/Source ObjectiveP13 - Experience of Clinical Management for Pregnant Women and Newborns with Novel Coronavirus Pneumonia in Tongji Hospital, China26
ChinaCurr Med Sci
To present updated clinical management for pregnant women
and newborns with pneumonia due to COVID-19.
P14 - Expert consensus for managing pregnant women and neonates born to mothers with suspected or confirmed novel coronavirus (COVID-19) infection27
ChinaInt J Gynaecol Obstet
To provide clinical management guidelines in pregnancy for
COVID-19.
P15 - A contingency plan for the management of the 2019 novel coronavirus outbreak in neonatal intensive care units28
ChinaLancet Child Adolesc Health
To obtain a contingency plan for the COVID-19 outbreak in
Neonatal Intensive Care Units.
P16 - An interpretation on perinatal and neonatal management plan for prevention and control of SARS-CoV-2 infection (2nd Edition)29
ChinaChin J Contemporary Pediatr
To interpret the perinatal and neonatal management plan to
prevent and control SARS-CoV-2 infection (2nd Edition).
P17 - Systematic perinatal management of the pregnant women and neonates during the epidemic of COVID-1930
ChinaChin J Obstet Gynecol
To present targeted suggestions on all prevention and control of
the perinatal period.
P18 - Response plan in the Neonatal intensive care unit during epidemic of SARS-CoV-2 infection (2nd Edition)31
ChinaChin J Contemporary Pediatr
To update a response plan in NICUs unit during the SARS CoV-
2 epidemic.
P19 - Safe delivery for pregnancies affected by COVID-1932
China and UK.Int J Gynaecol Obstet Editorial
Chart 2 - Char

Texto & Contexto Enfermagem 2020, v. 29: e20200242ISSN 1980-265X DOI https://doi.org/10.1590/1980-265X-TCE-2020-0242
8/17
Delivery time should be individualized, based on routine obstetric indications and the mothers’ clinical condition. Therefore, vaginal delivery is allowed when possible and cesarean delivery when necessary obstetrically.27 Delivery should take place with negative pressure isolation in a ward or operating room, both isolating from infection. Unnecessary items must be removed from the room and the number of health professionals must be minimized. Professionals must have strict protection against infections, using appropriate personal protective equipment (PPE) throughout the delivery process, including disposable caps and protective clothing, shoe covers, N95 masks, glasses, two-layer gloves, and hand hygiene.17,27,32
During delivery, patients with non-general anesthesia should wear surgical masks.32 Moreover, it is important to strengthen perinatal monitoring of obstetric complications.30 Immediately after birth in China, it is recommended to clamp the umbilical cord as soon as possible, immediate collection of umbilical cord blood, amniotic fluid and neonatal pharyngeal swabs, sputum, secretions from the lower respiratory tract, blood and others test samples to determine if newborns are infected with COVID-19.30 Newborns should be transferred to neonatal isolation immediately after being assessed by the neonatologist17,21,24,27,32 and carefully monitored for any signs of infection.21
In cases of maternal diagnosis after delivery, newborns should be treated as a suspicious case, being immediately isolated and monitored in the neonatal ward, with a PCR test, and it is recommended that it be quarantined for 14 days to minimize the risk of viral transmission pending further clinical outcome data.15–17,21,24,27,32 P1932 points out that after two consecutive negative tests for maternal nucleic acid newborns can be transferred from the isolation ward to mother care.
Newborns suspicted of having COVID-19
Fifteen studies showed precautionary measures when newborns infected with SARS-CoV-2 are suspected. In most of them, in cases of mothers with suspected or confirmed diagnosis, 14 days before delivery or 28 days after, or who had close contact with possibly infected people, newborns were considered suspicious cases and placed in isolation in the neonatal ward and under observation for at least 14 days.8,15–16,20,22,24–26,28–32 P216 still adds that this neonatal isolation ward must have negative pressure.
Furthermore, two articles mentioned that newborns with a history of contact with wild animals in the past two weeks would also be suspected.8,25 In these suspects with or without symptoms such as fever, cough, or respiratory discomfort, confirmatory diagnostic tests, such as PCR and nasopharyngeal smears should be performed, combined with epidemiological history, clinical manifestations, chest tomography, acid test nucleic acid and other methods of etiological testing. Attention should also be paid to the method, sample collection location, kit stability, experimental operation and other factors so as not to generate false negatives.15–17,20,29
When mothers have tested negative for SARS-CoV-2 with two consecutive nucleic acids (one day apart) and with informed consent, they may care for their children.26,32 Three manuscripts recommended that if babies with SARS-CoV-2 infection are suspected, they should immediately consult a hospital designated for infection or the infection department of the referral hospital for transport and additional diagnosis and treatment.24–25,29
P1831 reported the importance of differentiating neonatal SARS-CoV-2 infection from other causes such as neonatal pneumonia, premature infantile respiratory distress syndrome (RDS), severe asphyxia, neonatal sepsis, and meconium aspiration. A study also recommended team multidisciplinary management with neonatologists for newborns from mothers with COVID-19 pneumonia.27

Texto & Contexto Enfermagem 2020, v. 29: e20200242ISSN 1980-265X DOI https://doi.org/10.1590/1980-265X-TCE-2020-0242
9/17
Newborns with confirmation for COVID-19
Ten studies made up this category. P216 highlights that COVID-19 diagnosis in newborns can be confirmed by means of samples from the respiratory tract or blood, for the detection of SARS-CoV-2 nucleic acid, detected by fluorescent RT-PCR. Regarding the management of newborns positive for SARS-CoV-2, seven publications highlight the imperative need for immediate application of standard and additional precautionary measures, with guarantee of contact isolation, droplets and air, when aerosols are easily generated.16,20,23,26,28,30–31
P88 and P1528 recommended that suspected or laboratory confirmed cases be admitted to the Neonatal Intensive Care Unit (NICU). However, P317 points out that only symptomatic newborns need care in NICU. Meanwhile, P620 states that monitoring of positive neonates does not necessarily require admission to NICU, and can be done in a single room, without full NICU resources, according to local settings. Other studies, such as P13,26 P17,30 and P18,31 also claim that assessment and follow-up in a single room or neonatal isolation ward are necessary, with a quarantine period of at least 14 days.
Only P1023 outlined considerations about family management with COVID-19 at NICUs. It proposes that parents be assessed regarding presentation of symptoms and adherence to local preventive measures, especially with regard to strict compliance with precautions. But it is necessary to consider the children’s maturity, challenges of treatment, severity of the disease, expected duration of the stay as well as family capacity and resources and network, especially if parents are very affected by COVID-19 to be at NICUs.
The general clinical treatment of newborns positive for SARS-CoV-2 is symptomatic and supportive, involving maintenance of homeostasis, close blood test monitoring, chest radiography, prevention and treatment of complications and initial respiratory support, if necessary.15–16,28 In this regard, one of the priorities is detecting neonatal acute respiratory disorders in order to classify the clinical severity and offer ventilatory support following the guidelines and best available evidence.20
In newborns with severe acute RDS, manifested by opacification of the lungs (white lungs), studies refer to considering administration of pulmonary surfactant in high doses, inhalation of nitric oxide, and high-frequency oscillatory ventilation.8,15–16,20,28,31 Antimicrobial drugs are prescribed only for patients with probable or confirmed bacterial infection.28,31 Critical cases may require intravenous administration of glucocorticoids or immunoglobulins, continuous renal replacement therapy or extracorporeal membrane oxygenation (ECMO) treatment.8,15–16,28,31 Concerning the antiviral drugs used in adults, all manuscripts reinforce that it is uncertain as to safety and efficacy, requiring careful consideration of the risk-benefit ratio and technical issues.20,31
Concerning the clinical criteria for hospital discharge, it is recommended to consider asymptomatic infections two negative samples from the upper respiratory tract (nasal and oropharyngeal smear), consecutively (at least 24 hours apart). In cases of infections of the upper respiratory tract, return of normal body temperature for more than three days and the improvement of respiratory symptoms are added as criteria. In turn, in cases of pneumonia, in addition to the previous criteria, negative tests of lower respiratory tract samples are also added, improvement of the pulmonary image showing inflammation absorption and normal blood gas analysis without supplemental oxygen.15–16 On the other hand, it is emphasized that if babies are positive but asymptomatic, they may be discharged, but requiring quarantine at home. If possible, uninfected individuals over the age of 60 or with comorbidities should not care for these babies.
Preventing horizontal transmission of COVID-19 to newborns
Thirteen manuscripts addressed measures to prevent horizontal transmission of COVID-19 to newborns. Furthermore, to prevent newborn exposure to COVID-19, in cases of mothers with

Texto & Contexto Enfermagem 2020, v. 29: e20200242ISSN 1980-265X DOI https://doi.org/10.1590/1980-265X-TCE-2020-0242
10/17
COVID-19, there is recommendation for early clamping of the umbilical cord21,27,30 and temporary separation of newborns and their mothers for 14 days to minimize viral transmission risk.15–17,21,27,29
If rooming-in occurs due to facility limitations or maternal wishes, newborns should be kept about 2 meters away from the mother. If mothers with COVID-19 take care of babies, they should wear a face mask and practice hand hygiene before each feeding or other close contact with newborns.17
Direct breastfeeding was not recommended during the mother’s infection period by nine studies.15–16,21,25–30 However, two studies had a favorable position on breastfeeding, as long as preventive measures are taken, for instance, mother wearing a face mask and practicing hand hygiene before each feeding.17,22 Studies mention that a possible option is for sick mothers to pump breast milk, which can be offered to their baby by a healthy caregiver.17,21–22 Another recurrent aspect in all studies was that mothers should be encouraged to empty their breasts,15–17,22,25–27,29–30 thus guaranteeing lactation. However, P216 recommends that breastfeeding should only be reestablished after 14 days of negative breast milk testing.
Neonatal infection can occur after delivery by inhaling SARS-CoV-2 through aerosols produced by the cough of mothers, relatives, or healthcare professionals.18,31 Thus, at home, babies should be avoided with people at high risk of contamination, such as those with fever or respiratory symptoms;15–16 people should avoid going out and prohibiting the visit of relatives and friends, but when they happen, visitors must wear appropriate protective equipment;17,23,29 the number of caregivers should be limited; good ventilation, frequent hand hygiene should be provided when caring for babies; and daily disinfection of newborns’ utensils should be performed.26,29
DISCUSSION
Based on the findings, it is noted that the vast majority of studies have a low level of evidence, which is expected due to the contemporary COVID-19 pandemic. Furthermore, there was a predominance of investigations carried out by Chinese researchers. This fact is also justified, considering that in December 2019 the SARS-CoV-2 coronavirus was discovered in the city of Wuhan, a province in that country, which led to search for answers and immediate actions in the face of this disease.2
However, best practices that were previously recommended are still based on expert opinion, since no clinical trials and case-control or cohort studies were found. Recommendations have been treated as provisional and may be modified as new evidence becomes available. In addition, it was found that some recommendations vary according to the local context, which sometimes converge and sometimes diverge, especially with regard to breastfeeding in COVID-19 times.
Concerning newborns of mothers suspected of having COVID-19, studies recommend that babies whose mothers have high fever and hypoxemia be monitored between 14 and 21 days after birth. To date, most studies suggest that there is no mother-to-child vertical transmission. Therefore, the concern with newborn care has as its main focus, until now, the prevention of infection in babies after birth. This fact corroborates the Brazilian Society of Pediatrics (Sociedade Brasileira de Pediatria, abbreviated SBP) recommendations.6
Vaginal delivery is allowed whenever possible and cesarean delivery upon clinical indication but both should take place in hospital units with isolated areas with negative pressure; however, in Brazil, this availability is reduced.6 The Brazilian Federation of Gynecology and Obstetrics Associations also advises that the time and route of delivery, in most cases, should not be determined by maternal SARS-CoV-2 infection. Therefore, in pregnant women with good clinical conditions, mild symptoms and a fetus with good vitality, vaginal delivery is recommended.33
Such Federation indicates that suspected or confirmed patients for COVID-19 should be admitted to hospitals with a higher level of complexity for possible cases of maternal and/or fetal decompensation.

Texto & Contexto Enfermagem 2020, v. 29: e20200242ISSN 1980-265X DOI https://doi.org/10.1590/1980-265X-TCE-2020-0242
11/17
Therefore, delivery by suspected or confirmed women for COVID-19 is not recommended in households or in Childbirth Centers,33 which is also agreed with the studies in this review.
Transmission of SARS-CoV-2 occurs predominantly from person to person through respiratory droplets transmitted when an infected person coughs, sneezes, or speaks close to other people. Contaminated surfaces, or objects can also be sources of transmission.34 Therefore, the findings of the review reinforce that professionals during childbirth, regardless of route, are wearing PPE for contact precautions, droplets and aerosols, as Brazilian literature also recommends.6.33 An additional precaution would be for the team to dress in a room adjacent to the delivery room, wait and enter the delivery room shortly before birth.6
As for clamping of the umbilical cord, the publications indicated that for both suspected and confirmed cases, the recommendation is for early clamping. This recommendation differs from the WHO35 and Brazilian recommendations regarding COVID-19, which indicate timely clamping for newborns with gestational age ≥ 34 weeks with adequate breathing and muscle tone in flexion at birth. However, newborns should not be positioned in the mother’s abdomen or thorax during this period, which is an important modification in COVID-19 times. In newborns with gestational age <34 weeks of gestation, it is indicated to wait 30-60 seconds before clamping the umbilical cord, following what is already established. If placental circulation is not intact or if babies do not start breathing or do not show muscle tone in flexion, immediate clamping is recommended.6,33
Studies have indicated that newborns from mothers with COVID-19 confirmation should be transferred to neonatal isolation after delivery and monitored. However, SBP recommends that the choice of location to keep newborns after initial care and before admission to rooming-in, or neonatal unit depends on the local conditions of each maternity hospital. Whenever possible, first care for newborns should be provided in a separate room from the mothers. If this is not possible, a minimum distance of 2 meters must be maintained between the mother and the neonatal resuscitation table.6
Moreover, in Brazil, it is recommended that babies not be placed in skin-to-skin contact with mothers in the delivery room, according to the manuscripts found. Therefore, it may be necessary to remain in an incubator until transfer to the neonatal unit or until mothers and babies are transferred to rooming-in. Breastfeeding and skin-to-skin contact of newborns of mothers with suspected or confirmed COVID-19 should be postponed until measures to prevent contamination of babies can be adopted; this includes puerperal bath, change of mask, cap, nightgown, and sheets. Newborn bath in the first hour of life should be individualized according to the conditions of each institution.6
After birth, the need to perform specific tests to establish the diagnosis of infection in suspected newborns for COVID-19 was indicated. They must be placed in isolation in the neonatal ward. SBP meets these recommendations, stating that this investigation is indicated among newborns with acute onset respiratory symptoms, up to seven days, with suspected infection (mothers with a history of suspected or confirmed SARS-CoV-2 infection between 14 days before delivery and 28 days after delivery or newborns exposed to infected people - family members, caregivers, health professionals, or visitors) or confirmed by RT-PCR test on respiratory tract samples. It is noteworthy that the respiratory condition must not result from RDS, Transient Tachypnea of the Newborn (TTN), or congenital malformation.6
The studies in this review pointed out that the clinical treatment of newborns positive for SARS-CoV-2 is symptomatic and supportive. Furthermore, those with RDS or other conditions that show clinical severity may require NICU admission. Thus, administration of pulmonary surfactant, intravenous glucocorticoid or immunoglobulin medication as well as antimicrobials, nitric oxide inhalation, high-frequency oscillatory ventilation and continuous renal replacement and extracorporeal membrane oxygenation (ECMO) treatment may be necessary. The Brazilian Ministry of Health advises that the handling of cases should be carried out according to national protocols in force.36

Texto & Contexto Enfermagem 2020, v. 29: e20200242ISSN 1980-265X DOI https://doi.org/10.1590/1980-265X-TCE-2020-0242
12/17
Considering the clinical fragility and the potential for virus transmission at NICUs, Brazilian guidelines indicate some additional care, such as suspension of chatting at the bedside by the team that provides assistance as well as any and all collective activities carried out at NICUs.36
A study listed in this research outlined considerations about family and NICU management. Guidelines we have in Brazil deal with the suspension of entry, in this sector, of anyone other than father or mother. Only as an exception, such as death and prolonged hospitalization, can the family appoint another caregiver to follow newborns, as long as asymptomatic, with legal age and without home contact with people with flu syndrome or respiratory infection proven by SARS-CoV-2.36 WHO recommends that mothers should have free access to neonatal units in the face of the pandemic, with appropriate measures to prevent and control infections.35
Among the criteria for hospital discharge of newborns are improvement of symptoms, negative samples of the upper respiratory tract and improvement of the pulmonary image. Therefore, when planning discharge, the family should be guided as to the warning signs of illness of newborns and seek assistance according to the flow established by the assistance protocols validated by the Ministry of Health of Brazil. It is also important to guarantee safe transportation to home, avoiding the crowding of public public transport. Concerning follow-up of elective consultations at the follow-up clinic for asymptomatic preterm infants in hospitals, a temporary postponement is suggested.36
Breastfeeding was the most controversial point in the review. Some articles contraindicated this practice during the mother’s infection period and others were favorable as long as preventive measures are taken, such as using facial mask and hand hygiene by mothers. For WHO, infant feeding standard guidelines should also be maintained under COVID-19. Promotion of breastmilk substitutes and artificial nipples (bottles or pacifiers) should not occur in maternity hospitals.35 In Brazil, for now, the Ministry of Health recommends that breastfeeding be maintained in case of infection by SARS-CoV-2 as long as mothers wish to breastfeed and are in adequate clinical conditions.37
To protect newborns, some alternatives can be considered, such as using incubators instead of cribs, or using physical barriers between mother and baby, such as curtains. At NICUs, skin-to-skin contact should only be encouraged by the asymptomatic mother who does not maintain home contact with a person with influenza syndrome or respiratory infection proven by SARS-CoV-2, in the last 14 days.38
It is worth mentioning that milk should not be donated by women with symptoms compatible with flu-like syndrome, respiratory infection or confirmation of a SARS-Cov-2 case. Contraindication is extended to women with home contacts of cases with influenza syndrome or confirmed case for SARS-Cov-2.38
Finally, the studies listed care to be taken at home after hospital discharge in times of pandemic. Among them is avoiding the babies’ contact with people at high risk for contamination, unnecessary outings and visits, in addition to reinforcing hygiene measures. However, it is important to maintain elective follow-up appointments, routine immunization and growth and development surveillance.36
Health professionals, including nurses, must combine technical care with relational technologies to involve mothers and family members in care and decision-making related to babies. Thus, it will be able to encourage the formation of bonds and prepare them for discharge,39 especially in COVID-19 times, which imposes new challenges for home care of newborns.
This study has as limitation absence of strong or moderate scientific evidence in the literature, making it difficult to compare the findings and imposing the need to update this review later.
CONCLUSION
A review of different care practices directed at newborns in the time of COVID-19 emerged, whose recommendations were divergent, resulting from the contemporary pandemic of COVID-19; however,

Texto & Contexto Enfermagem 2020, v. 29: e20200242ISSN 1980-265X DOI https://doi.org/10.1590/1980-265X-TCE-2020-0242
13/17
they were discussed and contextualized, taking into account the official Brazilian recommendations. Nurses are important in care, educational and/or managerial practice to collaborate in adhering to best practices that are proven and recommended nationally and internationally, considering the local reality and the constant updating of the theme. Further research is needed, especially with a strong level of evidence, to develop assistance guidelines for this population group that contribute to reducing neonatal morbidity and mortality and healthy and harmonious child development during and post-pandemic.
REFERENCES
1. World Health Organization. Novel Coronavírus (COVID-19) Situation [Internet]. Geneva (CH); 2020 [cited 2020 Apr 29]. Available from: https://experience.arcgis.com/experience/685d0ace521648f8a5beeeee1b9125cd
2. McIntosh K, Hirsch MS, Bloom A. Coronavirus Disease 2019 (COVID-19): epidemiology, virology, clinical features, diagnosis, and prevention. Up to Date [Internet]. 2020 [cited 2020 Apr 29]. Available from: https://www.uptodate.com/contents/coronavirus-disease-2019-covid-19-epidemiology-virology-clinical-features-diagnosis-and-prevention
3. Adams JG, Walls RM. Supporting the health care workforce during the covid-19 global epidemic. JAMA [Internet]. 2020 [cited 2020 Apr 29];323(15):1439-40. Available from: https://dx.doi.org/10.1001/jama.2020.3972
4. Ludvigsson JF. Systematic review of COVID‐19 in children shows milder cases and a better prognosis than adults. Acta Paediatr [Internet]. 2020 [cited 2020 Apr 29];109:1088-95. Available from: https://doi.org/10.1111/apa.15270
5. Vivanti A, Vauloup-Fellous C, Prevot S, Zupan V, Suffee C, Cao JD, et al. Transplacental transmission of SARS-CoV-2 infection. J Matern-Fetal Med [Internet]. 2020 [cited 2020 May 24]. Available from: https://dx.doi.org/10.21203/rs.3.rs-28884/v1
6. Sociedade Brasileira de Pediatria. Recomendações para Assistência ao Recém-Nascido na sala de parto de mãe com COVID-19 suspeita ou confirmada – Atualização 2 – [Internet]. 2020 [cited 2020 May 24]. Available from: https://www.sbp.com.br/fileadmin/user_upload/22499c-NA-Assist_RN_SalaParto_de_mae_com_COVID-19.pdf
7. Lu Q, Shi Y. Coronavirus disease (COVID-19) and neonate: What neonatologist need to know. J Med Virol [Internet]. 2020 [cited 2020 Apr 29];92:564-7. Available from: https://doi.org/10.1002/jmv.25740
8. Hong H, Wang Y, Chung HT, Chen CJ. Clinical characteristics of novel coronavirus disease 2019 (COVID-19) in newborns, infants and children. Pediatr Neonatol [Internet]. 2020 [cited 2020 Apr 29];61(2):131-2. Available from: https://doi.org/10.1016/j.pedneo.2020.03.001
9. Li F, Feng ZC, Shi Y. Proposal for prevention and control of the 2019 novel coronavirus disease in newborn infants. Arch Dis Child Fetal Neonatal [Internet]. 2020 [cited 2020 May 2]; 0(0):1. Available from: http://dx.doi.org/10.1136/archdischild-2020-318996
10. Centers for Disease Control and Prevention. Interim clinical guidance for management of patients with confirmed Coronavirus Disease (COVID-19) [Internet]. 2020 [cited 2020 May 2]. Available from: https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-guidance-management-patients.html
11. Leandro JS, Christoffel MM. Cuidado familial de recém-nascidos no domicílio: um estudo de caso etnográfico. Texto Contexto Enferm [Internet]. 2011 [cited 2020 Apr 29];20(spe):223-31. Available from: https://doi.org/10.1590/S0104-07072011000500028

Texto & Contexto Enfermagem 2020, v. 29: e20200242ISSN 1980-265X DOI https://doi.org/10.1590/1980-265X-TCE-2020-0242
14/17
12. Souza LMM, Marques-Vieira CMA, Severino SSP, Antunes AV. Metodologia de revisão integrativa da literatura em enfermagem. Rev Invest Enferm [Internet]. 2017 [cited 2020 May 2];2(21):17-26. Available from: http://hdl.handle.net/20.500.12253/1311
13. Peters MDJ, Godfrey CM, McInerney P, Soares CB, Khalil H, Parker D. The Joanna Briggs Institute reviewers’ manual 2015: methodology for JBI scoping reviews [Internet]. 2015 [cited 2020 May 2]. Available from: http://joannabriggs.org/assets/docs/sumari/Reviewers-Manual_Methodology-for-JBI-Scoping-Reviews_2015_v2.pdf
14. Melnyk BM, Fineout-Overholt E. Evidence-based practice in nursing & healthcare. A guide to best practice. China: Wolters Kluwer/Lippincott Williams & Wilkins; 2011.
15. Working Group for the Prevention and Control of Neonatal 2019-nCoV Infection in the Perinatal Period of the Editorial Committee of Chinese Journal of Contemporary Pediatrics. Perinatal and neonatal management plan for prevention and control of 2019 novel coronavirus infection (1st Edition). Chin J Contemporary Pediatr [Internet]. 2020 [cited 2020 May 5];22(2):87-90. Available from: https://doi.org/10.7499/j.issn.1008-8830.2020.02.001
16. Working Group for the Prevention and Control of Neonatal 2019-nCoV Infection in the Perinatal Period of the Editorial Committee of Chinese Journal of Contemporary Pediatrics. Perinatal and neonatal management plan for prevention and control of 2019 novel coronavirus infection (2st Edition). Chin J Contemporary Pediatr [Internet]. 2020 [cited 2020 May 5];22(3):195-8. Available from: https://doi.org/10.7499/j.issn.1008-8830.2020.03.003
17. Mimouni F, Lakshminrusimha S, Pearlman SA, Raju T, Gallagher PG, Mendlovic J. Perinatal aspects on the covid-19 pandemic: a practical resource for perinatal–neonatal specialists. J Perinatol [Internet]. 2020 [cited 2020 May 5];40:820-6. Available from: https://doi.org/10.1038/s41372-020-0665-6
18. Schwartz DA, Graham AL. Potential maternal and infant outcomes from coronavirus 2019-nCoV (SARS-CoV-2) infecting pregnant women: lessons from SARS, MERS, and other human coronavirus infections. Viruses [Internet]. 2020 [cited 2020 May 5];12(2):194. Available from: https://doi.org/10.3390/v12020194
19. Chen Y, Peng H, Wang L, Zhao Y, Zeng L, Gao H, et al. Infants born to mothers with a new coronavirus (COVID-19). Front Pediatr [Internet]. 2020 [cited 2020 May 5];9(104):1-5. Available from: https://doi.org/10.3389/fped.2020.00104
20. Luca DD. Managing neonates with respiratory failure due to SARS-CoV-2. Child Adolesc Health [Internet]. 2020 [cited 2020 May 5];4(4):e8. Available from: https://doi.org/10.1016/S2352-4642(20)30073-0
21. Liang H, Acharya G. Novel corona virus disease (COVID-19) in pregnancy: what clinical recommendations to follow? Acta Obstet Gynecol Scand [Internet]. 2020 [cited 2020 May 5];99:439-42. Available from: https://doi.org/10.1111/aogs.13836
22. Morand A, Fabre A, Minodier P, Boutin A, Vanel N, Bosdure E, et al. COVID-19 virus and children: what do we know? Arch Pediatr [Internet]. 2020 [cited 2020 May 5];27(3):117-8. Available from: https://doi.org/10.1016/j.arcped.2020.03.001
23. Breindahl M, Zachariassen G, Christensen PS, Henriksen TB. dilemmas and priorities in the neonatal intensive care unit during the COVID-19 pandemic. Dan Med J [Internet]. 2020 [cited 2020 May 5];67(4):A205021. Available from: https://ugeskriftet.dk/files/scientific_article_files/2020-04/a205021_web.pdf
24. Chen Z, Du LZ, Fu JF, Shu Q, Chen ZM, Shi LP, et al. Emergency plan for inter-hospital transfer of newborns with SARS-CoV-2 infection. Chin J Contemporary Pediatr [Internet]. 2020 [cited 2020 May 5];22(3):226-30. Available from: https://doi.org/10.7499/j.issn.1008-8830.2020.03.009

Texto & Contexto Enfermagem 2020, v. 29: e20200242ISSN 1980-265X DOI https://doi.org/10.1590/1980-265X-TCE-2020-0242
15/17
25. Pediatric Committee, Medical Association of Chinese People′s Liberation Army; Editorial Committee of Chinese Journal of Contemporary Pediatrics. Emergency response plan for the neonatal intensive care unit during epidemic of 2019 novel coronavirus. Chin J of Contemporary Pediatr [Internet]. 2020 [cited 2020 May 5];22(2):91-5. Available from: https://doi.org/10.7499/j.issn.1008-8830.2020.02.002
26. Wang SS, Zhou X, Lin XG, Liu YY, Wu JL, Sharifu LM, et al. Experience of clinical management for pregnant women and newborns with novel coronavirus pneumonia in Tongji Hospital, China. Curr Med Sci [Internet]. 2020 [cited 2020 May 5];40(2):285-9. Available from: https://doi.org/10.1007/s11596-020-2174-4
27. Chen D, Yang H, Cao Y, Cheng W, Duan T, Fan C, et al. Expert consensus for managing pregnant women and neonates born to mothers with suspected or confirmed novel coronavirus (COVID-19) infection. Int J Gynaecol Obstet [Internet]. 2020 [cited 2020 May 5];149(2):130-6. Available from: https://doi.org/10.1002/ijgo.13146
28. Whan J, Qi H, Bao L, Li F, Shi Y. A contingency plan for the management of the 2019 novel coronavirus outbreak in neonatal intensive care units. Lancet Child Adolesc Health [Internet]. 2020 [cited 2020 May 5];4(4):258-9. Available from: https://doi.org/10.1016/S2352-4642(20)30040-7
29. Wang LS, Hu XJ, Zhou WH. An interpretation on perinatal and neonatal management plan for prevention and control of SARS-CoV-2 infection (2nd Edition). Chin J Contemporary Pediatr [Internet]. 2020 [cited 2020 May 5];22(3):199-204. Available from: https://doi.org/10.7499/j.issn.1008-8830.2020.03.004
30. Pu J, Liu XX. Systematic perinatal management of the pregnant women and neonates during the epidemic of COVID-19. Chin J Obstet Gynecol [Internet]. 2020 [cited 2020 May 5];55(3):153-6. Available from: https://doi.org/10.3760/cma.j.cn112141-20200221-00123
31. Medical Association of Chinese People′s Liberation Army; Editorial Committee of Chinese Journal of Contemporary Pediatrics; Preparatory Group of Pediatric Disaster, Pediatric Society, Chinese Medical Association. Response plan in the neonatal intensive care unit during epidemic of SARS-CoV-2 infection (2nd Edition). Chin J Contemporary Pediatr [Internet]. 2020 [cited 2020 May 5];22(3):205-10. Available from: https://doi.org/10.7499/j.issn.1008-8830.2020.03.005
32. Qi H, Luo X, Zheng Y, Zhang H, Li J, Zou L, et al. Safe delivery for pregnancies affected by COVID-19. Int J Gynaecol Obstet [Internet]. 2020 [cited 2020 May 5];0:1-3. Available from: https://doi.org/10.1111/1471-0528.16231
33. Federação Brasileira das Associações de Ginecologia e Obstetrícia. COVID-19: orientações da Febrasgo para atendimento na gestação, parto, puerpério e abortamento [Internet]. 2020 [cited 2020 May 24]. Available from: https://portaldeboaspraticas.iff.fiocruz.br/atencao-mulher/covid-19-orientacoes-da-febrasgo-para-avaliacao-e-tratamento-ambulatorial-de-gestantes/
34. Zou L, Ruan F, Huang M, Liang L, Huang H, Hong Z, et al. SARS-CoV-2 viral load in upper respiratory specimens of infected patients. N Engl J Med [Internet]. 2020 [cited 2020 May 24]; 382:1177-9. Available from: https://doi.org/10.1056/NEJMc2001737
35. Word Health Organization. Clinical management of COVID-19: Interim guidance [Internet]. Geneva (CH); 2020 [cited 2020 May 24]. Available from: https://cdn1.redemc.net/campus/wp-content/uploads/2020/04/2020-WHO-Clinical-Management-of-covid19-Interim-Guidance-May-18.pdf
36. Ministério Da Saúde, Secretaria de Atenção Primária à Saúde (BR). Nota técnica COCAM/CGCIVI/DAPES/SAPS/MS nº 10/2020: atenção à saúde do recém-nascido no contexto da infecção pelo novo coronavírus (SARS-CoV-2) [Internet]. Brasília, DF (BR); 2020 [cited 2020 May 25]. Available from: http://189.28.128.100/dab/docs/portaldab/documentos/notatecnica102020COCAMCGCIVIDAPESSAPSMS_003.pdf

Texto & Contexto Enfermagem 2020, v. 29: e20200242ISSN 1980-265X DOI https://doi.org/10.1590/1980-265X-TCE-2020-0242
16/17
37. Ministério da Saúde (BR). Nota Técnica DAPES/SAPS/MS nº 9/2020: orientações direcionadas ao Centro de Operações de Emergências para o Coronavírus (COE COVID-19), a serem adotadas pelo Sistema Único de Saúde (SUS) para a amamentação em eventuais contextos de transmissão de síndromes gripais [Internet]. Brasília, DF (BR); 2020 [cited 2020 May 24]. Available from: http://189.28.128.100/dab/docs/portaldab/documentos/notatecnicaamamentacao92020DAPESSAPSMS03abr2020COVID-19.pdf
38. Sociedade Brasileira de Pediatria. Aleitamento Materno em tempos de COVID-19 – recomendações na maternidade e após a alta [Internet]. 2020 [cited 2020 May 24]. Available from: https://www.sbp.com.br/fileadmin/user_upload/22467f-NA_-_AleitMat_tempos_COVID-19-_na_matern_e_apos_alta.pdf
39. Santos AS, Rodrigues LN, Santos MSN, Sousa GJB, Viana MCA, Chaves EMC. Papel materno durante a hospitalização do filho na unidade de terapia intensiva neonatal. Texto & contexto enferm [Internet]. 2019 [cited 2020 Jun 03]; 28: e20180394. Available from: https://doi.org/10.1590/1980-265x-tce-2018-0394

Texto & Contexto Enfermagem 2020, v. 29: e20200242ISSN 1980-265X DOI https://doi.org/10.1590/1980-265X-TCE-2020-0242
17/17
NOTES
CONTRIBUTION OF AUTHORITYStudy design: Góes FGB, Santos AST, Lucchese I, Silva LJ, Silva LF, Silva MA.Data collection: Góes FGB, Santos AST, Lucchese I, Silva LJ, Silva LF, Silva MA.Analysis and interpretation of data: Góes FGB, Santos AST, Lucchese I, Silva LJ, Silva LF, Silva MA.Discussion of results: Góes FGB, Santos AST, Lucchese I, Silva LJ, Silva LF, Silva MA.Writing and/or critical review of content: Góes FGB, Santos AST, Lucchese I, Silva LJ, Silva LF, Silva MA.Final review and approval of the final version: Góes FGB, Santos AST, Lucchese I, Silva LJ, Silva LF, Silva MA.
CONFLICT OF INTERESTThere is no conflict of interest.
EDITORSAssociated Editors: Gisele Cristina Manfrini Fernandes, Mara Ambrosina de Oliveira Vargas, Monica Motta LinoEditor-in-chief: Roberta Costa
HISTORICAL Received: June 03, 2020.Approved: June 24, 2020.
CORRESPONDING AUTHORFernanda Garcia Bezerra Gó[email protected]