best practice treatment for opioid use disorders practices oud powerpoint handout-dr....
TRANSCRIPT

7/24/2018
1
Best Practice Treatment for Opioid Use Disorders
Leslie Hulvershorn, MD
Medical Director
Indiana Division of Mental Health and Addiction
Director, Adolescent Dual Diagnosis Program, Riley Hospital for Children
Associate Professor of Psychiatry
Indiana University School of Medicine
Opioid Use Disorder Treatment
• History of Opioid Use
• Why do we have this epidemic?
• What are opioid use disorders?
• Evidence based treatments: Adults and Adolescents

7/24/2018
2
What is the best that we can do to promote recovery?

7/24/2018
3
Opium History
• First cultivation of opium poppies was in Mesopotamia, approximately 3400 B.C., plant called Hul Gil, the "joy plant”
• The Greek gods Hypnos (Sleep), Nyx (Night), and Thanatos(Death) were depicted wreathed in poppies
• The Persian physician, al-Razi (845-930 A.D.) made use of opium in anesthesia and recommended its use for the treatment of melancholy.
Opium History
• Between 400 and 1200 AD, Arab traders introduced opium to China.
• 14th century Ottoman Empire-opium used to treat headache and back pain.
• 15th century China- first officially recorded use of opium as a recreational drug.
• 1874- heroin developed
• 1898-heroin marketed by Bayer as safe pediatric cough suppressant

7/24/2018
4
Opiates & Opioids
Opiates = naturally present in opium • e.g. morphine, codeine, thebaine
Opioids = manufactured• Semisynthetics are derived from an opiate
• heroin from morphine
• buprenorphine from thebaine
• Synthetics are completely man‐made to work like opiates
• methadone
Opioid Use Disorders: DSM‐5“Opioid Addiction”
• Take more than intended
• Desire/unsuccessful efforts to cut back or quit
• Time spent using, obtaining or recovering
• Craving
• Failure to fulfill work, school, home obligations
• Continued use despite problems (social, psychological, physical)
• Activities given up
• Use in hazardous situations
• Tolerance
• Withdrawal

7/24/2018
5
THE PROBLEM:Emergency room mentions of opioid use
95,000
88 89 90 91 92 93 94 95 96 97 99 00 019830,000
40,000
50,000
60,000
70,000
80,000
90,000
DAWN, 2002
7/24/2018
6
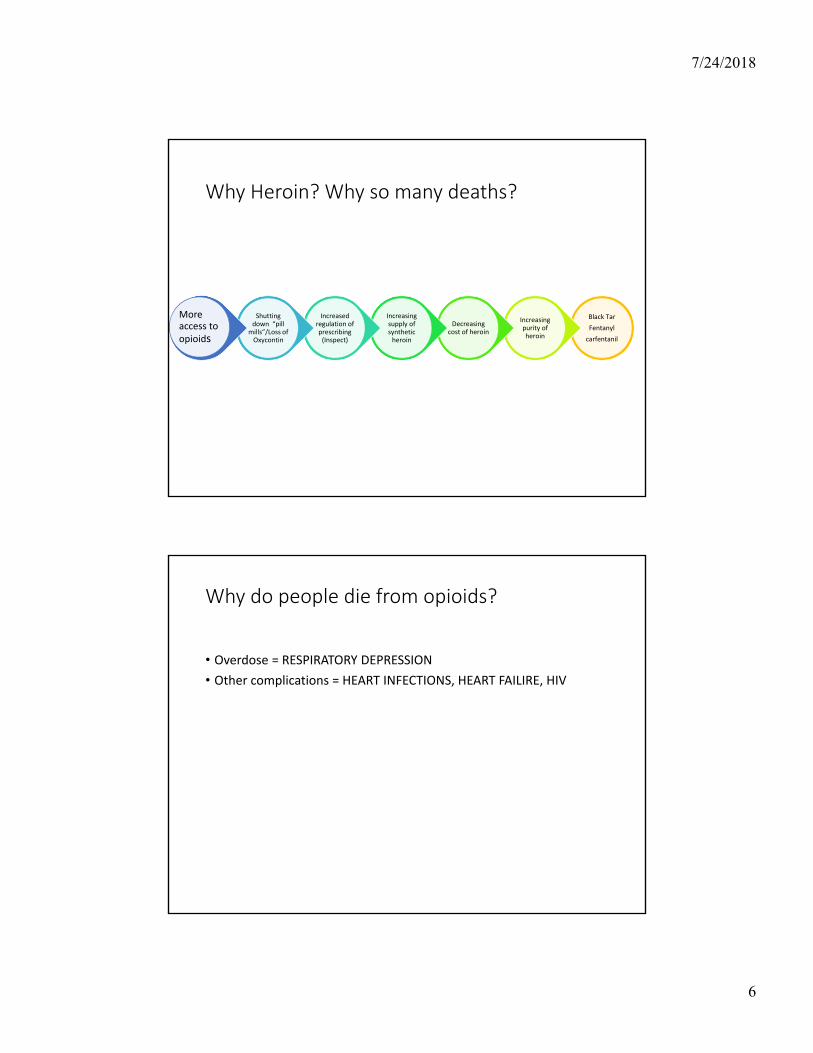
Why Heroin? Why so many deaths?
Black Tar
Fentanyl
carfentanil
Increasing purity of heroin
Decreasing cost of heroin
Increasing supply of synthetic heroin
Increased regulation of prescribing (Inspect)
Shutting down “pill
mills”/Loss of Oxycontin
More access to opioids
Why do people die from opioids?
• Overdose = RESPIRATORY DEPRESSION
• Other complications = HEART INFECTIONS, HEART FAILIRE, HIV

7/24/2018
7
What increases risk for death in opioid users?
• Tainted supply: Fentanyl and Carfentanil
• Co‐administration with benzodiazepines and alcohol
• Intermittent use decreasing tolerance
Lethal Dose

7/24/2018
8

7/24/2018
9
What the heroin user feels…
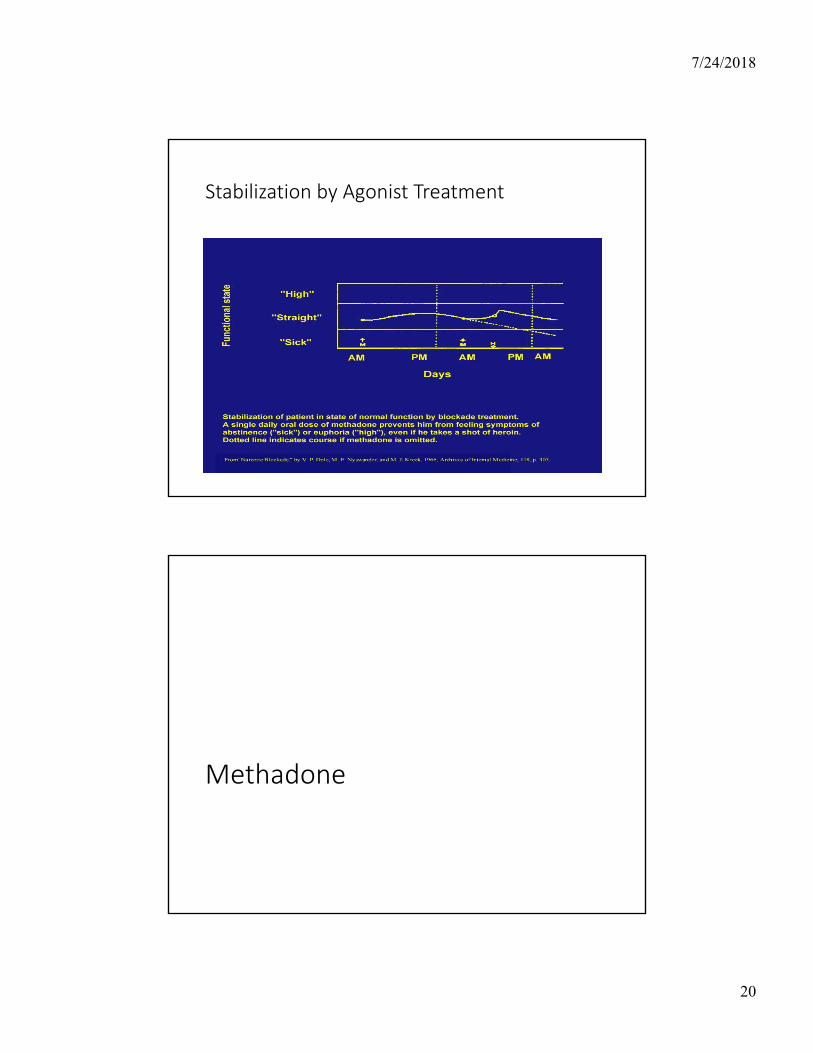
Dole, Arch Int Med, 1966
Behavioral Interventions

7/24/2018
10
Psychotherapies for Adults
• CBT
• Contingency Management
• Motivational Enhancement Therapy
• 12 step models
• Can be co‐located (ideal) in methadone/bup program or separate (more common)
(SAMHSA)
Cognitive Behavior Therapy (CBT)
• Individual
• Group Based
• Recognize and stop negative patterns of behavior
• Become aware of how stressors, feelings, situations lead to substance use
• Learn to avoid situations
• Reframe thoughts
• Cope with cravings
• Inpatient or outpatient
• Requires some degree of cognitive abilities

7/24/2018
11
Contingency Management
• Provides incentives to reinforce positive behaviors (e.g., abstinence, compliance with treatment)
• Very effective intervention
• Not therapy in a traditional sense
• Rewards can be provided by the clinic or family or patient
• Can be stand alone or in combination with CBT/12 step
Motivational Interviewing Techniques
•Be supportive of their need for autonomy
•Collaborative: confidential sessions•Avoid righting reflex: correction/advice giving/data
•Express empathy
•Develop discrepancy: “change talk”•Roll with resistance•Support self‐efficacy: goal setting, positive focus

7/24/2018
12
12‐step
• Most widely used treatment model
• Provides long term support
• My personal bias: I prefer it in addition to other treatment (particularly in the recovery support phase)
Recovery Supports
• Augment treatment both during, but particularly after a treatment episode
• Transportation
• Employment support
• Specialized living
• Peer‐to‐peer supports (12 step or other)
• Support groups
• Drop in centers
• Respite
• Wellness coaching
7/24/2018
13
Peer Supports
• Peers=individuals in recovery who can use their own experiences to help others work toward recovery
• “lived experience”
• Majority are 12 step
• Other curricula exist (NAMI)
• Can be a paid job!
What about adolescents?
7/24/2018
14
Existing Models
•Separate treatment programs for psychiatric disorders and addictions
•Group Treatments: 12 step, CBT• Inpatient•Residential “Rehab”•ENCOMPASS: outpatient co‐occurring model•Family Therapy: Multidimensional Family Therapy, Functional Family Therapy, SOFT, Adolescent Community Reinforcement Approach (A‐CRA)
•Non evidence based practices
Goals of family/parenting interventions
• Parent training
• Improve Family Functioning
• Reduce/Eliminate Substance Use
• Increase Problem Solving Skills
• Develop (Nurture Existing) Future Orientation
• Address Ecology of the Problem
28

7/24/2018
15
http://www.drugabuse.gov/family‐checkup
Adolescent Treatment
• Medication Management• Comorbidities
• Depression and Anxiety have clear pharmacologic targets
• ADHD: Stimulants (controversial), Bupropion
• SUDs• Small literature for use in adolescents but wealth of adult research in treatment for SUDs

7/24/2018
16
Medication Assisted Treatments for Opioid Use Disorders
Medication Assisted Treatment (MAT) actually means
medication + other psychosocial treatments together

7/24/2018
17
Phases of Substance Use that are Targets for Pharmacotherapy
• intoxication/overdose: Narcan (naloxone)
•withdrawal/detoxification (clonidine, bup, methadone)
• abstinence initiation/use reduction (methadone, bup)
• relapse prevention (methadone, bup, naltrexone)
• sequelae (psychosis, agitation, etc.): antipsychotics? Antidepressants?

7/24/2018
18
OUD Maintenance Treatment Options
Opiate Addiction
Buprenorphine
Detox/Maintenance
Program
Naltrexone
(Vivitrol)
Program
Methadone
Detox/Maintenance Program
36
Pharmacology Terminology
• agonist (replacement/substitution)
• antagonist (blockade)
• aversive (negative reinforcement)
• correction of underlying/associated disorders (such as depression, etc.)

7/24/2018
19
Rationale for Opioid Replacement/Agonist Therapy
• Traditional treatment has been to provide opioid agonist therapy• Methadone (Dolophine®)
• Levo‐Alpha Acetyl Methadol (LAAM) – not available
• Buprenorphine
• Stabilize neuronal circuitry• Mu occupation/blockade
• Cross‐tolerant, long‐acting, oral
• Prevent withdrawal and craving
• Extinguish compulsive behavior
• Prevent spread of HIV and HCV
• Prevent criminal activity
MarkedAbsentEuphoria
3-6 hours24-36 hoursDuration
Immediate30 minutesOnset
IV, INOral or SL
Route
HeroinMethadone
Buprenorphine
Treatment vs. OUD
7/24/2018
20
Stabilization by Agonist Treatment
Methadone
7/24/2018
21
History of Methadone
Synthesized in Germany:
Less addictive than
morphine
1930s
Used in US for pain
1947
Research demonstrated efficacy for heroin
addiction
1964
Federal regulations
developed for methadone maintenance treatment
1971
Federal regulations updated to allow more effective and consistent use
2001
http://www.cesar.umd.edu/cesar/drugs/methadone.asp
Methadone Maintenance
• Maintenance=help avoid negative consequences of illicit opiate misuse
• Dosed once daily
• <80‐100 mg daily
• When properly managed, reduce narcotics related deaths, users' involvement in crime, the spread of AIDS, and helps users gain control of their lives
• If used correctly, few side effects, no high
7/24/2018
22
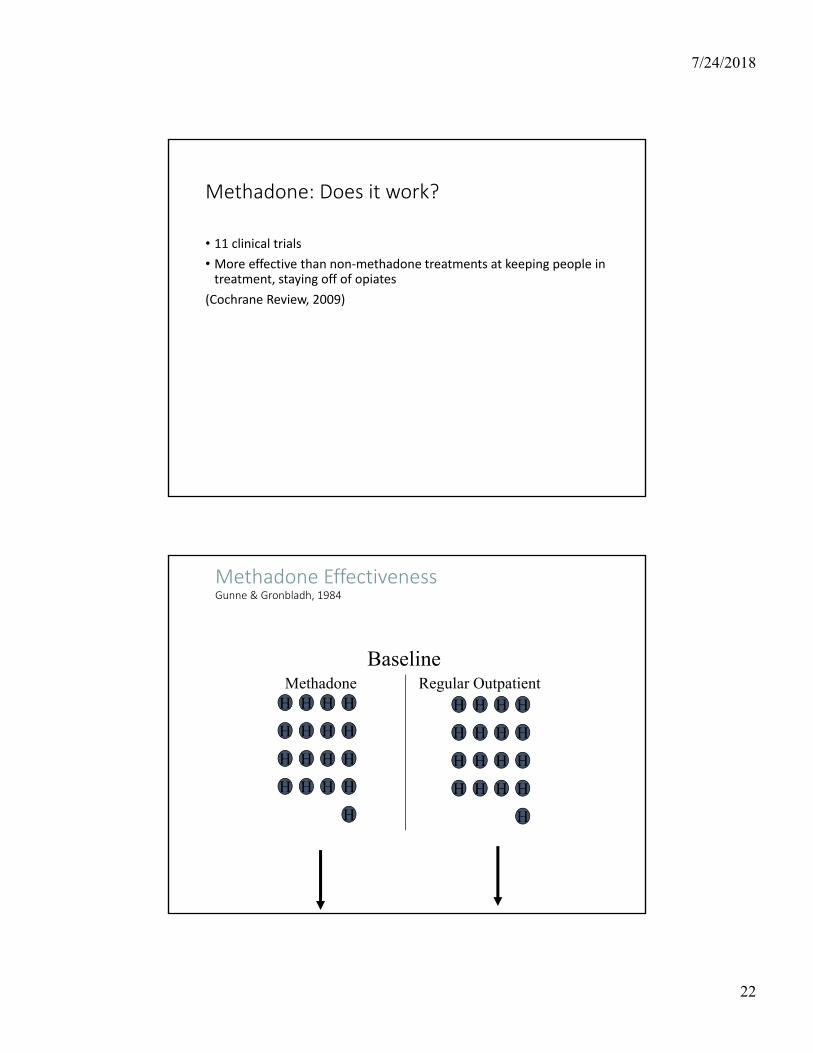
Methadone: Does it work?
• 11 clinical trials
• More effective than non‐methadone treatments at keeping people in treatment, staying off of opiates
(Cochrane Review, 2009)
Methadone EffectivenessGunne & Gronbladh, 1984
H H HH
H H HH
H H HH
H H HH
H
H H HH
H H HH
H H HH
H H HH
H
Methadone Regular Outpatient
Baseline

7/24/2018
23
Methadone EffectivenessGunne & Gronbladh, 1984
P H HH
H
P HP
H H HH
H H HH
H H H
Methadone No Methadone
After 2 Years
1
32
1- Sepsis & endocarditis2- Leg amputation3- SepsisPurple=expelled from txP=prisonH=heroin
Methadone EffectivenessGunne & Gronbladh, 1984
P H H
H
P P
P
Methadone No Methadone
After 5 Years

7/24/2018
24
Myth: There Isn’t Any Proof That MAT Is Better Than Abstinence
FACT: MAT is evidence-based (many, many clinical trials in 1970s-2000s) and is the recommended course of treatment for OUDs. The National Institute on Drug Abuse, Substance Abuse and Mental Health Services Administration, National Institute on Alcohol Abuse and Alcoholism, Centers for Disease Control and Prevention, and other agencies emphasize MAT as first line treatment.

7/24/2018
25
Myth: MAT Is Only For The Short Term
•FACT: Research shows that patients on MAT for at least 1‐2 years have the greatest rates of long‐term success. There is currently no evidence to support benefits from cessation.
•FACT: Patients with long‐term abstinence can follow a slow taper schedule under a physician’s direction, when free of stressors, to attempt dose reduction or total cessation.
7/24/2018
26
Myth: Many Patients’ OUDs Are Not Severe Enough to Require MAT
•FACT: MAT utilizes a multitude of different medication options (agonists, partial agonists and antagonists) that can be tailored to fit the unique needs of the patient.
Myth: It is best to take the lowest possible dose of methadone.
• Fact: The appropriate dose of methadone should be determined by cessation of cravings for each individual.
• Fact: Too low of a dose has been shown to result in cravings and relapse.

7/24/2018
27
Why is methadone so tightly regulated?• Complex pharmacokinetics: blood levels build quickly (non‐linear) as dose increases, thus there is risk of overdose
• Very dangerous when combined with benzodiazepines, especially early in treatment
• Can interact with many commonly used medications Decreased methadone concentrations:
• Pentazocine• Phenytoin• Carbamazepine • Rifampin • Efavirenz• Nevirapine• Lopinavir (Kaletra)
• Opiate withdrawal syndrome
• Increased methadone concentrations:• Ciprofloxacin• Fluvoxamine• Discontinuation of inducing drug
• Cognitive impairment• Respiratory depression• QTc prolongation; Torsade de Pointes
McCance‐Katz et al. 2009
Federal and State Rules for OTPs
7/24/2018
28
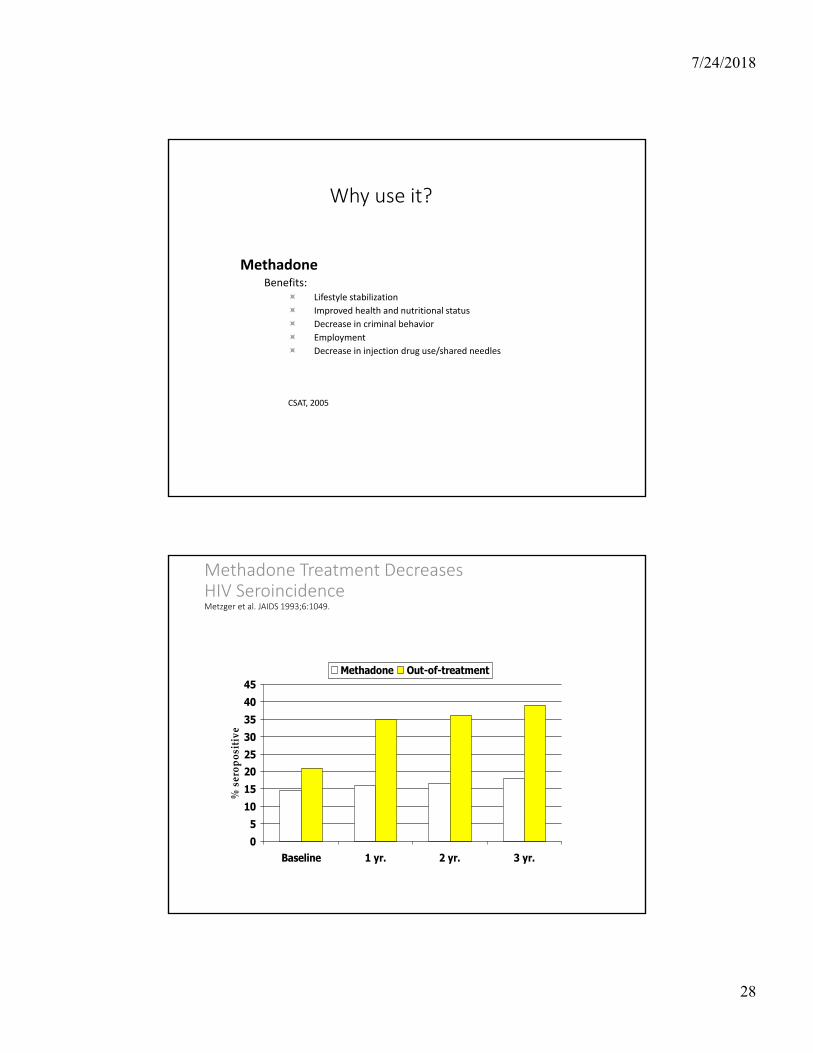
Why use it?
MethadoneBenefits:
Lifestyle stabilization
Improved health and nutritional status
Decrease in criminal behavior
Employment
Decrease in injection drug use/shared needles
CSAT, 2005
Methadone Treatment Decreases HIV SeroincidenceMetzger et al. JAIDS 1993;6:1049.
05
1015202530354045
Baseline 1 yr. 2 yr. 3 yr.
% s
erop
osit
ive
Methadone Out-of-treatment
7/24/2018
29
Where do you get it?
OUDs ‐>Opioid Treatment Programs (OTPs)
Pain ‐> Any prescriber can write a script that can be filled at traditional pharmacies
Opioid Treatment Programs (OTPs)
• Only source of methadone for maintenance
• Provide a multi‐modal approach including medication, counseling, and other supportive services, to treat opioid addiction
• Heavily regulated by state and federal agencies
• Historically 13 clinics (3 CMHCs) + 5 new (Plus VA)
• Serve approximately 15,000 people
• Can also administer buprenorphine
• Opioid use disorders are widespread and Indiana is still underserved

7/24/2018
30
“Take Homes”
• Privilege earned through clean drug screens
• Incentive for “good behavior”
• Improves compliance, sobriety from other drugs
7/24/2018
31
Methadone PROS CONS
• Close supervision: daily dosing
• Enforce therapy
• Incentivize “take homes”
• Most effective treatment
• Hassle: interfere with employment, parenting, etc.
• Expensive
• Societal consequences for take homes
Treatment Options
Opiate Addiction
Buprenorphine
Maintenance
Program
Naltrexone
(Vivitrol)
Program
Methadone
Maintenance Program

7/24/2018
32
BuprenorphineSuboxone, Subutex, etc
Buprenorphine/Naloxone
• Semi‐synthetic partial agonist (limited effects) + antagonist
• Does not require daily dispensing
• Safer in overdose = much less regulation
• Easier to stop than methadone, milder withdrawal

7/24/2018
33
Sublingual Film or Tab
Buprenorphine treatment is evidence based
• Many clinical trials have shown that it is superior to placebo.
• Outcomes are similar to methadone, if patients are able to comply with less structured buprenorphine in Office Based Outpatient Treatment (OBOT) settings.

7/24/2018
34
Drug Abuse Treatment Act (DATA) of 2000
• Allowed “Qualified” physicians to treat opioid dependence outside methadone facilities1. Addiction certification from approved organization, or
2. Physician in clinical trial of qualifying medication, or
3. Complete 8‐hour course from approved organization
• DEA issues (free) to qualifying physicians a new DEA number to use medication for opioid dependence
• As of today, only one medication formulation is approved for this use
Buprenorphine’s Properties
• Modest agonist activity with ceiling
• Long half life
• Precipitated withdrawal if taken after full agonist
• Decreased risk of respiratory, CNS depression
• Sublingual route of administration
• “Combo” tablet with naloxone limits abuse by injection
7/24/2018
35
Buprenorphine Safety• No alteration of cognitive functioning
• feel “normal”
• No organ damage• Early concern of hepatic toxicity unconfirmed• No evidence of QT prolongation
• Ceiling prevents respiratory depression, OD(Overdose reports with combining use with benzodiazepines)
• No clinically significant interactions with other drugs
Appropriateness for Office-based Treatment
• Patient is less likely to be an appropriate candidate for office-based treatment:
• Dependence on high doses of benzodiazepines, alcohol, or other CNS depressants
• Significant psychiatric co-morbidity• Multiple previous treatments (methadone) and relapses

7/24/2018
36
Most often heard quotes with Buprenorphine
“Doc, I feel normal”
“I wake up not sick”
“I have my life back”
• Treatment in normal medical settings:• Encourages continuity of medical/specialty care
• Encourages relationship building with clinicians
• Legitimize opioid dependence as a normal, treatable, chronic illness
Buprenorphine: Reduces Other Drug Use
Fudala, NEJM 2003
7/24/2018
37
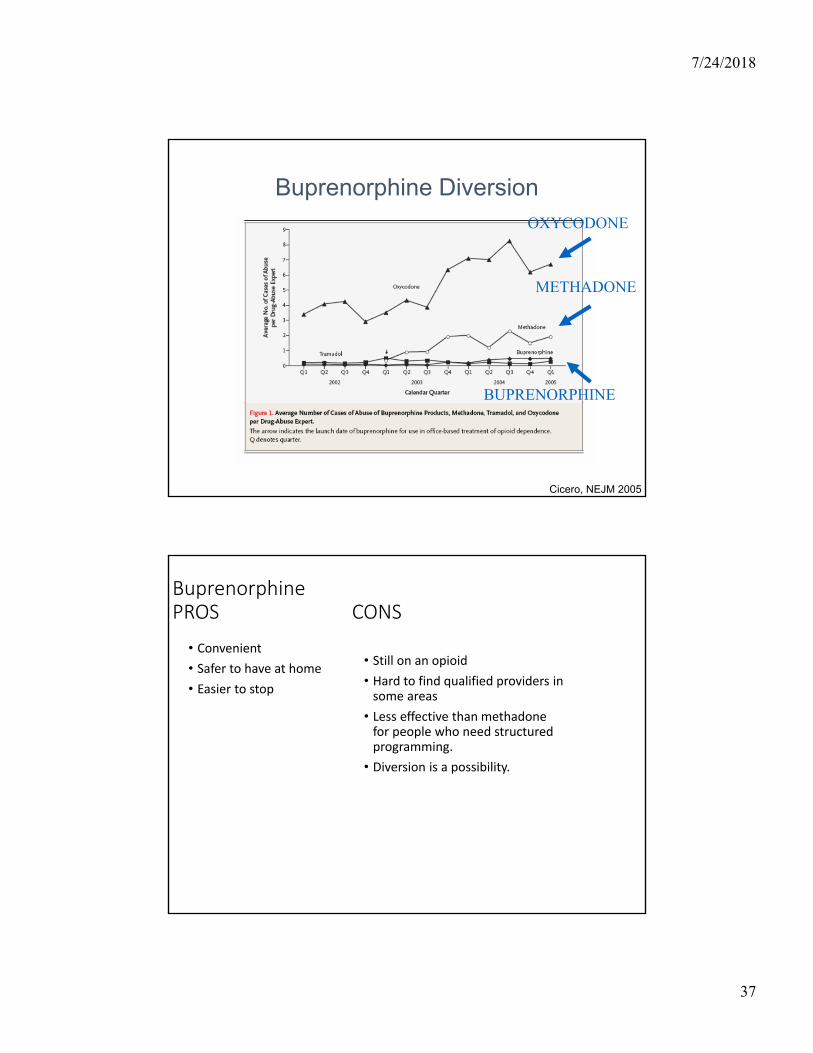
Buprenorphine Diversion
Cicero, NEJM 2005
OXYCODONE
METHADONE
BUPRENORPHINE
BuprenorphinePROS CONS
• Convenient
• Safer to have at home
• Easier to stop
• Still on an opioid
• Hard to find qualified providers in some areas
• Less effective than methadone for people who need structured programming.
• Diversion is a possibility.

7/24/2018
38
BIG NEWS: Long Acting Injectable Buprenorphine
• 2 Formulations: Sublocade (single dose available) and another formulation pending FDA approval
• Sublocade: subcutaneous, requires 7 days of oral bup, two monthly initial doses of 300 mg followed by 100 mg monthly maintenance doses
• NOW COVERED BY IN MEDICAID
Opiate Use Disorders and Pregnancy
• Detoxification is associated with high rates of spontaneous abortions in the first trimester and premature delivery in the third trimester
• Babies exposed to heroin have lower birth weights
• Babies exposed to heroin were more likely to require morphine than those with methadone treated mothers (40% vs. 19%)
• Current recommendations: Treat with Methadone or Buprenorphine

7/24/2018
39
Neonatal Abstinence Syndrome
• “Neonatal abstinence syndrome is an expected and treatable condition that follows prenatal exposure to opioid agonists.”
‐American College of Obstetricians and Gynecologists
Naltrexone (Vivitrol)

7/24/2018
40
Antagonist Treatment
Naltrexone
Why antagonist therapy?
• Block effects of a dose of opiate (Walsh et al. 1996)
• Prevent impulsive use of drug
• Dose (oral): 50 mg daily, 100 mg every 2 days, 150 mg every third day
• Blocks agonist effects
• Side effects: hepatotoxicity, monitor liver function tests every 3 months
• Biggest issue is lack of compliance; but those who “test” naltrexone by taking a dose of opioid and experiencing no effect do better with the medication (Cornish JW, et al. 1997)
7/24/2018
41
Who is a Candidate for Naltrexone?
• The patient is opioid free for 7‐10 days (DIFFICULT IN OUTPATIENT SETTINGS)
• The patient does not have severe or active liver or kidney problems (Typical guidelines suggest liver function tests no greater than 3 times the upper limits of normal, and bilirubin normal)
Risks: side effects, costs, take home
doses
Benefits: Decrease drug use, improve health, reduce high
risk behaviors, increase employment
7/24/2018
42
MYTH : Providing MAT Will Only Disrupt and Hinder a Patient’s Recovery Process
• FACT: MAT has been shown to assist patients in recovery by improving quality of life, level of functioning and the ability to handle stress. Above all, MAT helps reduce mortality while patients begin recovery.
National Council for Behavioral Health
MAT Summary
• Studies have shown that MAT reduces illicit drug use, disease rates, and related harmful behaviors, including criminal activity.
• People in MAT are up to 75% less likely to die from a cause related to their addiction.
• Despite what the National Institute of Health says is “unequivocal” evidence of MAT’s effectiveness and safety, many myths persist about MAT. As a result, people are denied potentially life saving addiction treatment.
7/24/2018
43
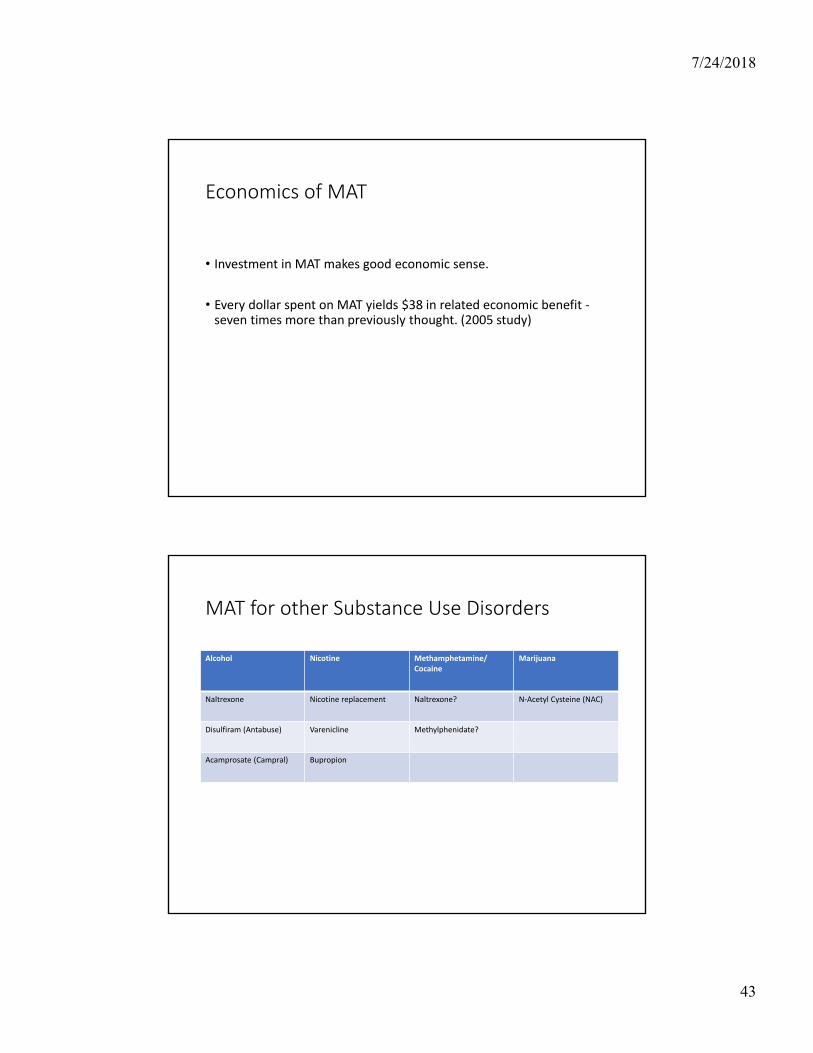
Economics of MAT
• Investment in MAT makes good economic sense.
• Every dollar spent on MAT yields $38 in related economic benefit ‐seven times more than previously thought. (2005 study)
MAT for other Substance Use Disorders
Alcohol Nicotine Methamphetamine/Cocaine
Marijuana
Naltrexone Nicotine replacement Naltrexone? N‐Acetyl Cysteine (NAC)
Disulfiram (Antabuse) Varenicline Methylphenidate?
Acamprosate (Campral) Bupropion

7/24/2018
44
We need to advocate for a full continuum of care
What to do if you are concerned about care being provided to people with OUDs?
• FSSA’s Division of Mental Health and Addiction licenses and certifies addiction providers.
• Please report concerns to DMHA’s consumer service line at: 1-800-901-1133

7/24/2018
45
Summit Resources
• IN.gov/recovery
• IN OBOT Guidelines
• Benchcard
References• Max Bayard M, Mcintyre J, Hill KR, Woodside J: Alcohol Withdrawal Syndrome. Am Fam Physician 2004;69:1443–50
• Grant BF, Stinson FS, Dawson DA et al.: Prevalence and co‐occurrence of substance use disorders and independent mood and anxiety disorders: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Arch Gen Psychiatry 2004; 61: 807‐816.
• Kessler RC, Berglund P, Demler O, et al.: Lifetime prevalence and age‐of‐onset distributions of DSM‐IV disorders in the National Comorbidity Survey replication. Arch Gen Psychiatry 2005; 62: 593‐602.
• American Psychiatric Association. Practice guidelines for the treatment of psychiatric disorders. Treatment of alcohol use disorders. Pp 377‐391, 2006.
• Fleming MF, Mihic SJ, Harris RA: Ethanol, in Goodman and Gilman’s The Pharmacological Basis of Therapeutics, 10 ed. Edited by Hardman JG, Limbird LE, Gilman AG, New Your, McGraw‐Hill, 2001, pp 429‐446.
• Fuller RK, Williford WO, Lee KK, Derman R.: Veterans Administration cooperative study of disulfiram in the treatment of alcoholism: study design and methodological considerations. Control Clin Trials. 1984 Sep;5(3):263‐73
• O'Farrell TJ, Allen JP, Litten RZ: Disulfiram (antabuse) contracts in treatment of alcoholism. NIDA Res Monogr., 150:65‐91, 1995.
• Garbutt JC, Kranzler HR, O’Malley SS, Gastfriend DR, Pettinati HM, Silverman BL, Loewy JW, Ehrich EW: Efficacy and tolerability of long‐acting injectable naltrexone for alcohol dependence: a randomized controlled trial. JAMA 2005; 293: 1617‐1625.
• Streeton C, Whelan G: Naltrexone, a relapse prevention maintenance treatment of alcohol dpendence: a meta‐analysis of randomized controlled trialss. Alcohol Alcohol 2001; 36: 544‐552.
• Littleton J: Acamprosate in alcohol dependence: how does it work? Addiction 1995; 90: 1179‐1188.
• Naltrexone Information Sheet http://familydoctor.org/online/famdocen/home/common/addictions/alcohol/130.html
• Acamprosate Information: http://kap.samhsa.gov/products/brochures/advisory/text/Acamprosate‐Advisory.doc
• Johnson BA, Rosenthal N, Capece JA, Wiegand F, Mao L, Beyers K, McKay A, Ait‐Daoud N, Anton RF, Ciraulo DA, Kranzler HR, Mann K, O'Malley SS, Swift RM; Topiramate for Alcoholism Advisory Board; Alcohol Study Group: Topiramate for treating alcohol dependence: a randomized controlled trial. JAMA. 2007; 10: 298: 1641‐51.
• Walsh SL, Sullivan JT, Preston KL, Garner JE, Begelow GE: Effects of naltrexone on response to intravenous cociane hydromorphone, and their combination in humans. J Pharmacol Exp Ther 1996; 279‐524‐528.
• Cornish JW, Metzger D, Woody GE, Wilson D, McLellan AT, Vandergrift B, O’Brien CP: Naltrexone pharmacotherapy for opioid dpendet federal probationers. J Subst Abuse Treat 1997; 14:529‐534.
• Naloxone challenge: http://www.rxlist.com/revia‐drug.htm
• Center for Substance Abuse Treatment. Medication‐Assisted Treatment for Opioid Addiction in Opioid Treatment Programs. Treatment Improvement Protocol (TIP) Series 43. DHHS Publication No. (SMA) 05‐4048. Rockville, MD: Substance Abuse and Mental Health Services Administration, 2005.
• Strain EC, Bigelow GE, Liebson IA, Stitzer ML: Moderate vs. high dose methadone in the treatment of opioid dependence: a randomized trial. JAMA 1999; 281: 1000‐1005.
• McCance‐Katz EF, Sullivan LS, Nallani S: Drug interactions of clinical importance between the opioids, methadone and buprenorphine, and frequently prescribed medications: A review. Am J Addictions, in press.
• McCance‐Katz EF: Office based treatment of opioid dependence with buprenorphine. Harvard Review of Psychiatry, 12: 321‐338, 2004.
• McNicholas, L. Clinical guidelines for the use of buprenorphine in the treatment of opioid addiction: A treatment improvement protocol (TIP 40). Rockville, MD: US Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Substance Abuse Treatment, 2004.
• Center for Substance Abuse Treatment. Medication‐Assisted Treatment for Opioid Addiction in Opioid Treatment Programs. Treatment Improvement Protocol (TIP) Series 43. DHHS Publication No. (SMA) 05‐4048. Rockville, MD: Substance Abuse and Mental Health Services Administration, 2005.
• Baker JR, Jin C, McCance‐Katz EF: Cocaine Use Disorders. In Psychiatry 3rd edition, A Tasman, J. Kay,M. First, J.A.Lieberman (eds.) Wiley Blackwell Co., Chichester, England, pp. 1058‐1089, 2008.

7/24/2018
46
Acknowledgements
• Michael Fingerhood MD (NIDA CTN)
• Steve Batki, MD (UCSF)
• Donna Shelly, MD (Columbia)
• Kari Franson, PharmD, PhD