best practice statement: care of the older person’s · pdf filebest practice statement:...
TRANSCRIPT

Copies of this document are available from:www.wounds-uk.comor by writing to:Wounds UKSuite 3.136 UpperkirkgateAberdeen AB10 1BA
3M is a trademark of the 3M Company. © 3M Health Care, 2006. Date of preparation: October 2006
Best Practice Statement:
Care of the Older Person’s Skin
BPS2.indd 2-3 3/11/06 12:26:11 pm

1Best Practice Statement: Care of the Older Person’s Skin
CONTENTS
Foreword 2
Development team 3
Review panel 3
Introduction 4
Dry, vulnerable tissue 4 Pressure ulcers 5 Incontinence 7 Maceration 8 Skin tears 8
Section 1: Management of dry, vulnerable tissue 9
Section 2a: Presure ulcers — risk assessment 10
Section 2b: Pressure ulcers — skin inspection 11
Section 2c: Pressure ulcers — classification 12
Section 2d: Pressure ulcers — stabilisation, positioning 13
Section 2e: Pressure ulcers — stabilisation, mattresses, chairs and cushions 14
Section 2f: Pressure ulcers — promoting healing 15
Section 3a: Skin care — incontinence 16
Section 3b: Skin care — maceration 17
Section 4: Skin tears 18
Appendix 1: Definitions of topical skin applications 19
Table 1: Quantities of dermatological preparations prescribed for specific areas of the body 19
Appendix 2: Skin examination 20
Appendix 3: Formal risk assessment scales, examples 20
Appendix 4: Pressure ulcer classification scales, examples 21
Appendix 5: Skin tear classification system 21
References 22
BPS2.indd 1 3/11/06 16:04:15

Best Practice Statement: Care of the Older Person’s Skin2
Foreword
Those charged with caring for the sick and vulnerable in the UK are faced with the challenge of ensuring that their practice is of the highest standards, while often working with heavy workloads which can be a barrier to reviewing research literature on a regular basis. Where practitioners can access the latest published research, it can often be difficult to establish what changes, if any, a practitioner should make to their practice to ensure that it is optimal. Frequently, research papers call for fur ther research to be conducted, or arrive at conclusions which can leave the practitioner unclear as to how practice should be developed.
In view of these challenges, there is a need for clear and concise guidance as to how to deliver the optimal care. One method of supporting clinicians in this aim is the provision of Best Practice Statements. These types of statements were pioneered in the area of pressure ulcers by Quality Improvement Scotland, and we are grateful to them for their permission to reproduce the relevant sections of their statements in this document. In Best Practice Statements, the relevant research is reviewed, and expert opinion and clinical guidance is provided in clear, accessible table form.
The key principles of best practice (listed below) ensure that due care and process is followed to promote the delivery of the highest standards of care across all care settings, and by all care professionals.
v Best Practice Statements (BPS) are intended to guide practice and promote a consistent and cohesive approach to care.
v BPS are primarily intended for use by registered nurses, midwives and the staff who support them, but they may also contribute to multidisciplinary working and be of guidance to other members of the healthcare team.
v Statements are derived from the best available evidence, including expert opinion at the time they are produced, recognising that levels and types of evidence vary.
v Information is gathered from a broad range of sources to identify existing or previous initiatives at local and national level, incorporate work of a qualitative and quantitative nature, and establish consensus.
v Statements are targeted at practitioners, using language that is both accessible and meaningful.
The aim of this Best Practice Statement is to provide relevant and useful information to guide those active in the clinical area, who are responsible for the management of skin care in an ageing patient population. The Best Practice Statement: Care of the Older Person’s Skin has been developed by a team of specialists, chaired by Pam Cooper. During the peer review process, practitioners from across the UK have been able to comment on the various drafts. Their expertise has been sought to cover the variety of skin issues found in the elderly. This has led to the development of a guideline to support clinicians in their decision-making, which is up-to-date at the time of printing.
BPS2.indd 2 3/11/06 16:04:15
3Best Practice Statement: Care of the Older Person’s Skin
Development team
Pam Cooper, Clinical Nurse Specialist in Tissue Viability, Department of Tissue Viability, NHS Grampian, Aberdeen
Dr Michael Clark, Senior Research Fellow, Wound Healing Research Unit, Cardiff University, Cardiff
Professor Sue Bale, Associate Director of Nursing, Gwent Healthcare NHS Trust, Gwent
Review panel
Alison Bardsley, Editor, Continence UK, Manager, Oxfordshire Continence Services, Oxford
Andrew Kingsley, Tissue Viability Nurse Specialist, North Devon District Hospital, Barnstaple
Rebecca Penzer, Editor, Dermatological Nursing, Independent Nurse Consultant, Opal Skin Solutions, Oxford
John Timmons, Tissue Viability Nurse, Department of Tissue Viability, NHS Grampian, Aberdeen
For the treatment and protectionof damaged or at-risk skin
This statement is a Wounds UK initiative, sponsored by 3M Health Care
BPS2.indd 3 3/11/06 16:04:15

Best Practice Statement: Care of the Older Person’s Skin4
Introduction
As the largest organ of the body, comprising 15% of the body’s weight, the skin reflects the individual’s emotional and physical well-being. The skin varies in thickness from 0.5–4.0 mm, depending on which part of the body is involved (Stephen-Haynes, 2005). The skin consists of three main layers; the outer epidermis, the middle dermis and the subcutaneous tissue. Combined, these three layers of tissue provide the following functions:
v Protection: the skin acts as a protective barrier, preventing damage to internal tissues from trauma, ultraviolet (UV) light, temperature, toxins and bacteria (Butcher and White, 2005).
v Barrier to infection: part of this barrier function is the physical barrier of intact skin; the other is the presence of sebum, an antibacterial substance with an acidic pH which is produced by the skin (Günnewicht and Dunford, 2004).
v Pain receptor: nerve endings within the skin respond to painful stimuli. They also act as a protective mechanism.
v Maintenance of body temperature: to warm the body, the vessels vasoconstrict (become smaller), thus retaining heat. If the vessels vasodilate (become wider), this leads to cooling (Timmons, 2006).
v Production of vitamin D in response to sunlight: this is important in bone development (Butcher and White, 2005).
v Production of melanin: this is responsible for skin colouring and protection from sunlight radiation damage.
v Communication, through touch and physical appearance: this gives clues to the individual’s state of physical well-being (Flanagan and Fletcher, 2003).
The changes in the skin that occur as an individual ages affect the integrity of the skin, making it more vulnerable to damage. The epidermis gradually becomes thinner, (Baranoski and Ayello, 2004) and thus more susceptible to the mild mechanical injury
forces of moisture, friction and trauma (pp. 6–7). In the dermis, there is a reduction in the number of sweat glands and in the production of sebum. These changes add vulnerability to the skin, and, when this is coupled with an increased necessity to cleanse the skin, damage will occur. Most soaps increase the skin’s pH to an alkaline level, thus putting the skin’s surface at risk of the effects of dehydration and altering the normal bacterial flora of the skin, which allows colonisation with more pathogenic species (Cooper and Gray, 2001).
As the skin sees a reduction in elastin fibres, it becomes more easily stretched, increasing the risk of tearing and trauma.
The most dramatic loss that the skin experiences during the ageing process is a 20% reduction in the thickness of the dermis (Bryant, 1992). This gives the skin its paper-thin appearance, commonly associated with the elderly (Kaminer and Gilchrist, 1994). This thinning of the dermis sees a reduction in the blood vessels, nerve endings and collagen, leading to a decrease in sensation, temperature control, rigidity and moisture retention (Baranoski and Ayello, 2004).
This document aims to provide clinicians with best practice guidance in five key areas of skin care for older persons, namely:
v dry, vulnerable tissuev pressure ulcersv incontinencev macerationv skin tears.
Dry, vulnerable tissue
As already said, with the ageing process, the skin undergoes a number of changes. Not only is there a significant reduction in the skin’s thickness, but because of the changes within the epidermis and dermis, there is also a reduction in the number of sweat glands, leading to dryness of the skin. Once the
BPS2.indd 4 3/11/06 16:04:15

5Best Practice Statement: Care of the Older Person’s Skin
skin becomes dry, it is more vulnerable to splitting and cracking, exposing it to bacterial contamination, and further adding to the likelihood of breakdown from infection.
Altering an individual’s position, or nursing them on an appropriate support surface in conjunction with position changes can prevent pressure damage. If the pressure is unrelieved for a long period of time, the damage will extend to the bone. A cone-shaped ulcer is created, with the widest part of the cone close to the bone, and the narrowest on the body surface. This may be seen as a non-blanching red mark, or an area of superficial skin loss on examination (Dealey, 1994). The ulcer will then appear to deteriorate rapidly, often causing alarm — however, the damage has already been present for some time. In some situations, this deep damage may have occurred in the days prior to admission to health or social care, which is a good reason for inspection within the first six hours following admission (National Institute for Clinical Excellence [NICE], 2005). Inspection Pressure ulcers
A pressure ulcer is an area of localised damage to the skin and underlying tissue, due to the occlusion of blood vessels which leads to cell death (Collier, 1996). Pressure ulcers are believed to be caused by direct pressure, shear and friction (Allman, 1997; European Pressure Ulcer Advisory Panel [EPUAP] Review, 1999). The forces of pressure are further exacerbated by moisture, and factors relating to the individual’s physical condition, such as altered mobility, poor nutritional status, medication, and underlying medical conditions. Pressure ulcers are also referred to as pressure sores, decubitus ulcers and bedsores (Beldon, 2006).
Pressure ulcers usually occur over a bony prominence, such as the sacrum, ischial tuberosity and heels. However, they can appear anywhere that tissue becomes compressed, such as under a plaster cast or splint.
Direct pressure is the major causative factor in the development of pressure ulcers. This occurs when the soft tissue of the body is compressed between a bony prominence and a hard surface. This occludes the blood supply, leading to ischaemia and tissue death.
Figure 1: Dry skin
Figure 2: Pressure ulcer body map (Bryant, 1992)
Chin 0.5%
Iliac crest 4%
Trochanter 15%
Knee 6%
Pretibial crest 2%
Malleolus 7%Heel 8%
Ischium 24%
Sacrum 23%
Elbow 3%
Spinous process 1%
Scapula 0.5%
Occiput 1%
Prone position
Supine position
Sitting position
Lateral pressure
BPS2.indd 5 3/11/06 16:04:16

Best Practice Statement: Care of the Older Person’s Skin6
is necessary to check for skin blemishes, and to initiate a risk assessment and start a pressure prevention care plan to prevent further damage.
Shear can also contribute to pressure ulcer development. This usually occurs when the skeleton and underlying tissue move down the bed under gravity, but the skin on the buttocks and back remain stuck to the same point on the mattress. This twisting and dragging effect occludes blood vessels which causes ischaemia, and usually leads to the development of more extensive tissue damage. Shear force can be further exacerbated by the presence of surface moisture through incontinence or sweating (Collier, 1996), and by friction when the skin slides over the surface with which it is in contact.
Friction occurs when two surfaces move or rub across one another, leading to superficial tissue loss. Prior to the use of lift aids, patients were manually lifted up the bed and, if the sacrum and heels were not clear of the surface, they would be dragged up causing friction to these areas. The majority of pressure ulcers to the heel are caused by a combination of both pressure and friction. Initially, they present as a blister (friction), with purple discoloration to the underlying tissue (pressure).
The effects of pressure, shear and friction can be further exacerbated by the individual’s physical condition. These factors should be considered when carrying out a full assessment, including:
v general health v age v reduced mobility v nutritional status v incontinencev certain medications.
Staff and carers involved in looking after individuals at risk, or with existing pressure ulcers may use this document to support
Figure 4: Pressure ulcer to the sacrum, caused by the combined effects of pressure and shear
Figure 5: Pressure ulcer to the sacrum caused by pressure and friction. The effects of friction cause the removal of the epidermis
Figure 3: Pressure ulcer to the sacrum, which presents with exposed bone, slough and granulation tissue
BPS2.indd 6 3/11/06 16:04:17

7Best Practice Statement: Care of the Older Person’s Skin
their decision-making to ensure that best practice is provided.
Sections relating to pressure ulcers have been amended from the BPS for the prevention and treatment/management of pressure ulcers by NHS Quality Improvement Scotland (Best Practice Statement for the Prevention of Pressure Ulcers, NHS Quality Improvement Scotland, 2003 updated 2005. Best Practice statement for the Treatment/Management of Pressure Ulcers, NHS Quality Improvement Scotland, 2005).
Incontinence
Some studies have shown that older people are more prone to incontinence. In one study, 29% of older people cared for in a nursing home were incontinent of urine, 65% were doubly incontinent, and 6% were catheterised (Bale et al, 2004).
Skin has a mean pH of 5.5, which is slightly acidic. Both urine and faeces are alkaline in nature, therefore, if the individual is incontinent there is an immediate change in pH which affects the skin. Ammonia is produced when Figure 7: Incontinence skin reaction
microorganisms digest urea from the urine. Although urinary ammonia alone is not a primary irritant, urine and faeces together increase the pH around the perianal area, causing increased skin irritation (Berg, 1986; Le Lievre, 2000). This is responsible for the dermatitis excoriation seen in individuals with incontinence (Fiers, 1996).
The increase in moisture resulting from episodes of incontinence, combined with bacterial and enzymatic activity, can result in the breakdown of vulnerable skin, due to an increased friction co-efficient,
Figure 6: Thirty-degree lateral position at which pressure points are avoided (Bryant, 1992)
BPS2.indd 7 3/11/06 16:04:18

Best Practice Statement: Care of the Older Person’s Skin8
particularly in those who are very young or elderly. For those individuals experiencing incontinence and the effects of irritation from incontinence, it is important to avoid exacerbating this fur ther through inappropriate methods of cleansing the skin (Whittingham, 1998). A protective barrier spray or cream can be used to prevent sore skin from breaking down further. Advice on appropriate products to aid management of incontinence can be sought from your local continence advisor.
Maceration
It is accepted that a degree of moisture is essential for moist wound healing to occur (Winter, 1963). However, the correct moisture balance is difficult to define. The wound needs to be moist, but not too moist or too dry, as this may affect the rate of healing. Maceration of the skin may be due to any of the following factors:
v incontinence (see Section 3a, p. 16) v excess moisture from sweating in hot
environments and induced by waterproof chair and bed surfaces
v wound exudate v peri-stomal exudate.
When the skin is in contact with fluid for sustained periods of time, it becomes
Figure 9: Skin tear to a limb caused by trauma
soft and wrinkled allowing for breaks in the epidermis (White and Cutting, 2003). This softening of the tissue, along with attack from enzymes within urine, faeces and wound exudate, can cause the skin to become red, broken and painful. It is important that the skin is protected from these enzymatic onslaughts.
Skin tears
Skin tears are a common problem in the elderly because the skin becomes thin and fragile (Bryant, 1992). They usually occur on the shin and the arm, and are normally caused by trauma exacerbated by shear and friction (Morris, 2005). Due to the thin nature of the skin, skin tears tend to involve some damage to the epidermis and the dermis, and may take some time to heal. Therefore, to optimise healing, management of these wounds is best carried out at the time of injury.
Figure 8: Pressure ulcer to the heel. The surrounding white tissue indicates the presence of maceration
Each of the sections that follow, contain a table showing:
v the optimum outcomev the reason for, and how best to
succeed in reaching this outcomev how to demonstrate that best practice is
being achieved.
In addition, each section identifies key points/challenges, and is supported by appendices, a table, and references (where available).
BPS2.indd 8 3/11/06 16:04:18

9Best Practice Statement: Care of the Older Person’s Skin
Sec
tio
n 1
: Man
agem
ent
of
dr
y, v
uln
erab
le t
issu
eK
ey p
oin
ts:
l If
iden
tified
as
havi
ng d
ry, v
ulne
rabl
e sk
in, t
he s
kin
shou
ld b
e fr
eque
ntly
ass
esse
d.l R
egul
ar t
reat
men
t w
ith a
moi
stur
iser
will
mai
ntai
n sk
in in
tegr
ity.
Stat
emen
tRe
ason
for s
tate
men
tH
ow to
dem
onst
rate
stat
emen
t is
bein
g ac
hiev
ed
v
All in
divid
uals
are
asse
ssed
to d
eter
mine
cond
ition
of s
kin
(dry
*, fla
ky, e
xcor
iated
, disc
olou
red,
etc)
v
Asse
ssm
ent e
nable
s the
corr
ect a
nd su
itable
pre
vent
ative
m
easu
res t
o be
initi
ated
and
main
taine
dv
Th
e he
alth
reco
rds o
f all
indi
vidua
ls ad
mitt
ed to
, or
resid
ent i
n a f
acilit
y m
ust i
nclu
de e
viden
ce o
f skin
co
nditi
on as
sess
men
t
v
Emol
lient
soap
subs
titut
es sh
ould
be
used
in in
divid
uals
with
dry
, vuln
erab
le sk
in, o
r skin
det
erm
ined
to b
e vu
lnera
ble w
hen
wash
ing/cl
eans
ing d
uring
rout
ine
pers
onal
hygie
ne
v
Was
hing s
kin w
ith an
em
ollie
nt so
ap su
bstit
ute
redu
ces
the
dryin
g effe
cts a
ssoc
iated
with
soap
and
wate
r (C
alian
no, 2
002)
v
Hea
lth re
cord
s inc
lude
evid
ence
that
the
appr
opria
te
emol
lient
is u
sed
v
Skin
shou
ld b
e th
orou
ghly
dried
to p
reve
nt fu
rthe
r de
hydr
atio
n. D
rying
shou
ld in
volve
a lig
ht p
attin
g and
not
ru
bbing
, as r
ubbin
g may
lead
to ab
rasio
n an
d/or
wea
kenin
g of
the
skin
(Brit
ton,
2003
)
v
If th
e sk
in is
left
dam
p, it
is vu
lner
able
to e
xces
s dry
ing
from
the
envir
onm
ent a
nd a
t risk
from
bac
teria
l and
fu
ngal
cont
amin
atio
n
v
Hea
lth re
cord
s hav
e ev
iden
ce th
at al
l indi
vidua
l’s sk
in is
dried
in an
appr
opria
te m
anne
r
v
All in
divid
uals
with
dry
, vuln
erab
le sk
in sh
ould
hav
e a b
land
moi
sturis
er o
r bar
rier c
ream
appli
ed at
leas
t twi
ce d
aily t
o pr
even
t the
adve
rse
effec
ts of
dry
skin
(App
endix
1, p
. 19)
v
Appli
catio
n of
a bla
nd m
oistu
riser
or b
arrie
r cre
am
rehy
drat
es th
e sk
in an
d re
duce
s the
irrit
ant e
ffect
s fro
m
perfu
mes
and
addi
tives
(Bale
, 200
4)
v
Ther
e is
evid
ence
with
in th
e he
alth
reco
rds t
hat t
he
appr
opria
te m
oist
urise
r and
am
ount
is u
sed
(see
Ap
pend
ix 1,
p. 19
)
v
Appli
catio
n of
the
moi
sturis
er o
r bar
rier c
ream
shou
ld
follo
w th
e di
rect
ion
of th
e bo
dy h
air, a
nd b
e ge
ntly
smoo
thed
into
the
skin
(am
ount
s rec
omm
ende
d by
the
Britis
h Na
tiona
l For
mula
ry [B
NF] a
re o
utlin
ed in
Table
1, p
. 19)
v
Rubb
ing th
e m
oistu
riser
or b
arrie
r cre
am in
to th
e sk
in ca
n lea
d to
irrit
atio
n
* D
ry sk
in in
the
elder
ly is
diffe
rent
to u
nder
lying
der
mat
olog
ical c
ondi
tions
such
as e
czem
a, ps
orias
is an
d un
derly
ing sk
in se
nsitiv
ities.
Indi
vidua
ls w
ith e
czem
a, ps
orias
is an
d un
derly
ing sk
in se
nsitiv
ities a
re lik
ely to
ben
efit
from
the
abov
e gu
idan
ce b
ut sh
ould
be
refe
rred
for s
pecifi
c, ap
prop
riate
trea
tmen
ts
BPS2.indd 9 3/11/06 16:04:18
Best Practice Statement: Care of the Older Person’s Skin10
Sec
tio
n 2
a: P
res
sur
e u
lcer
s —
ris
k a
sses
smen
tK
ey p
oin
ts:
l A
ll in
divi
dual
s ‘at
ris
k’, o
r w
ith e
xist
ing
pres
sure
ulc
ers
shou
ld b
e as
sess
ed.
l In
spec
tion
of id
entifi
ed in
divi
dual
s sh
ould
be
carr
ied
out
regu
larl
y an
d, in
bet
wee
n as
sess
men
ts, i
f hea
lth s
tatu
s ch
ange
s fo
r be
tter
or
wor
se.
l T
hose
indi
vidu
als
cons
ider
ed ‘a
t ri
sk’,
or t
hose
with
pre
ssur
e ul
cers
, sho
uld
rece
ive
appr
opri
ate
inte
rven
tions
.
Stat
emen
tRe
ason
for s
tate
men
tH
ow to
dem
onst
rate
stat
emen
t is
bein
g ac
hiev
ed
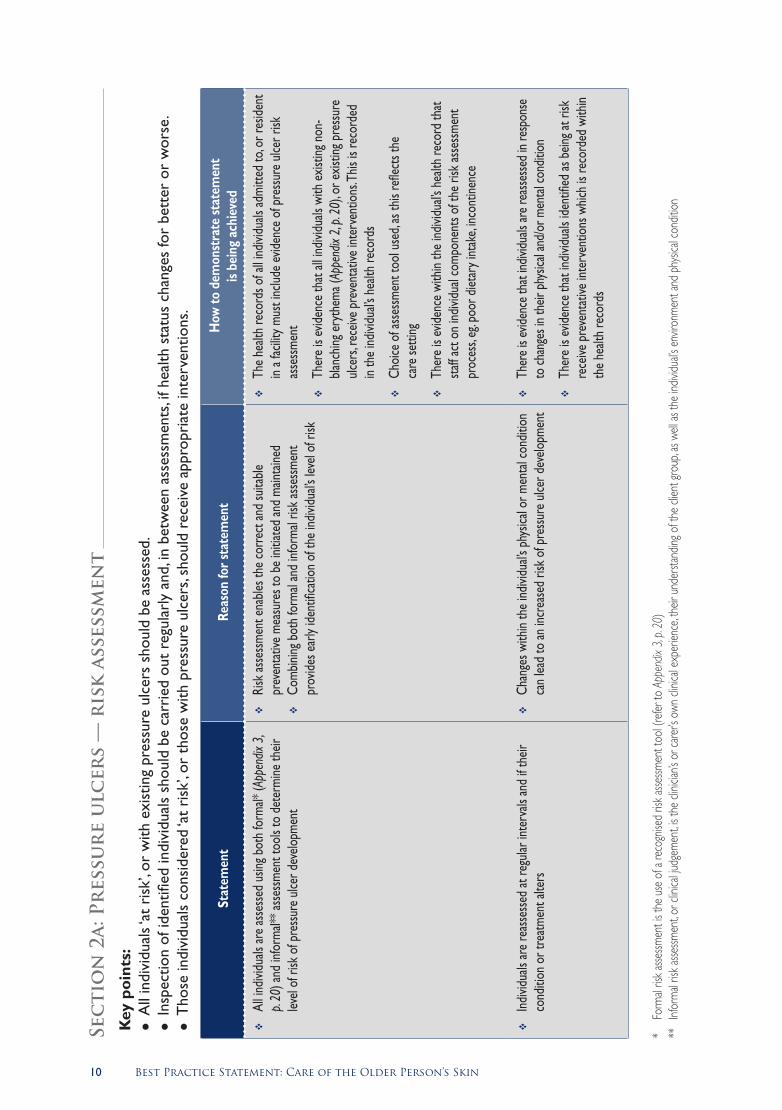
v
All in
divid
uals
are
asse
ssed
usin
g bot
h fo
rmal*
(App
endix
3,
p. 20
) and
info
rmal*
* ass
essm
ent t
ools
to d
eter
mine
their
lev
el of
risk
of p
ress
ure
ulcer
dev
elopm
ent
v
Risk
asse
ssm
ent e
nable
s the
corr
ect a
nd su
itable
pr
even
tativ
e m
easu
res t
o be
initi
ated
and
main
taine
dv
Co
mbin
ing b
oth
form
al an
d inf
orm
al ris
k as
sess
men
t pr
ovid
es e
arly
iden
tifica
tion
of th
e ind
ividu
al’s l
evel
of ri
sk
v
The
healt
h re
cord
s of a
ll ind
ividu
als ad
mitt
ed to
, or r
esid
ent
in a f
acilit
y mus
t inc
lude
evid
ence
of p
ress
ure
ulcer
risk
as
sess
men
t
v
Ther
e is
evid
ence
that
all in
divid
uals
with
exis
ting n
on-
blanc
hing e
ryth
ema (
Appe
ndix
2, p.
20), o
r exis
ting p
ress
ure
ulcer
s, re
ceive
pre
vent
ative
inte
rven
tions
. This
is re
cord
ed
in th
e ind
ividu
al’s h
ealth
reco
rds
v
Choi
ce o
f ass
essm
ent t
ool u
sed,
as th
is re
flect
s the
ca
re se
tting
v
Ther
e is
evid
ence
with
in th
e ind
ividu
al’s h
ealth
reco
rd th
at
staff
act o
n ind
ividu
al co
mpo
nent
s of t
he ri
sk as
sess
men
t pr
oces
s, eg
. poo
r diet
ary i
ntak
e, inc
ontin
ence
v
Indi
vidua
ls ar
e re
asse
ssed
at re
gular
inte
rvals
and
if th
eir
cond
ition
or t
reat
men
t alte
rsv
Ch
ange
s with
in th
e ind
ividu
al’s p
hysic
al or
men
tal c
ondi
tion
can
lead
to an
incr
ease
d ris
k of
pre
ssur
e ulc
er d
evelo
pmen
tv
Th
ere
is ev
idenc
e th
at in
dividu
als ar
e re
asse
ssed
in re
spon
se
to ch
ange
s in
their
phy
sical
and/
or m
enta
l con
ditio
n
v
Ther
e is
evid
ence
that
indi
vidua
ls id
entifi
ed as
bein
g at r
isk
rece
ive p
reve
ntat
ive in
terv
entio
ns w
hich
is re
cord
ed w
ithin
the
healt
h re
cord
s
* Fo
rmal
risk a
ssessm
ent i
s the
use
of a
reco
gnise
d ris
k asse
ssmen
t too
l (re
fer to
App
endix
3, p
. 20)
**
Infor
mal
risk a
ssessm
ent, o
r clin
ical ju
dgem
ent, i
s the
clini
cian’s
or c
arer
’s ow
n cli
nical
expe
rienc
e, th
eir u
nder
stand
ing o
f the
clien
t gro
up, a
s well
as th
e ind
ividu
al’s e
nviro
nmen
t and
phy
sical
cond
ition
BPS2.indd 10 3/11/06 16:04:19

11Best Practice Statement: Care of the Older Person’s Skin
Sec
tio
n 2
b: P
res
sur
e u
lcer
s —
sk
in i
nsp
ecti
on
Key
po
ints
: l A
ll in
divi
dual
s ‘at
ris
k’, o
r w
ith e
xist
ing
pres
sure
ulc
ers
shou
ld b
e as
sess
ed.
l In
spec
tion
of id
entifi
ed in
divi
dual
s sh
ould
be
carr
ied
out
regu
larl
y an
d, in
bet
wee
n as
sess
men
ts, i
f hea
lth s
tatu
s ch
ange
s fo
r be
tter
or
wor
se.
l T
hose
indi
vidu
als
iden
tified
sho
uld
rece
ive
appr
opri
ate
inte
rven
tions
.
Stat
emen
tRe
ason
for s
tate
men
tH
ow to
dem
onst
rate
stat
emen
t is
bein
g ac
hiev
ed
v
All in
divid
uals
at ri
sk o
f pre
ssur
e ulc
er d
evelo
pmen
t, or
wi
th e
xistin
g pre
ssur
e ulc
ers,
will h
ave
their
skin
asse
ssed
as
par
t of t
he w
hole
asse
ssm
ent p
roce
ss. F
or th
ose
with
ex
isting
pre
ssur
e ulc
ers,
a clas
sifica
tion
scor
e wi
ll be
used
(se
e Se
ction
2c o
n ‘Cl
assifi
catio
n’, p
. 12)
v
The
majo
rity o
f pre
ssur
e ulc
ers t
hat o
ccur
are
supe
rficia
l in
natu
re. E
arly
iden
tifica
tion
of sk
in ch
ange
s may
pre
vent
fu
rthe
r det
erio
ratio
n
v
Follo
wing
asse
ssm
ent o
f risk
, insp
ectio
n of
the
skin
is do
cum
ente
d wi
thin
the
indivi
dual’
s hea
lth re
cord
s
v
Gen
eral
visua
l insp
ectio
n of
all a
reas
of t
he sk
in fo
rms p
art
of th
e as
sess
men
t pro
cess
, with
spec
ial at
tent
ion
being
paid
to
bon
y pro
mine
nces
(se
e Fig
ure 2
, p. 5
).
v
The
majo
rity o
f pre
ssur
e ulc
ers t
hat o
ccur
are
loca
ted
on
the
sacr
um an
d he
els (C
lark
and W
atts,
199
4)
v
Findi
ngs f
rom
skin
inspe
ctio
n ind
icate
that
furt
her
inter
vent
ion
is re
quire
d. Th
is, alo
ng w
ith th
e su
bseq
uent
ac
tion
take
n, is
reco
rded
in th
e he
alth
reco
rds
v
Any i
nter
vent
ions
und
erta
ken,
eg. m
attre
ss, c
ushio
n, he
el pr
otec
tors
, spe
cialis
t refe
rral
mus
t be
reco
rded
in th
e he
alth
reco
rds
v
Whe
re an
area
of r
edne
ss o
r skin
disc
olor
atio
n (e
ryth
ema/
hype
raem
ia) is
not
ed, fu
rthe
r exa
mina
tion
is re
quire
d. Se
e Ap
pend
ix 2
(p. 2
0) if
dea
ling w
ith d
ark
skin
pigm
enta
tion
v
Furth
er e
xam
inatio
n wi
ll ind
icate
if th
e sk
in ch
ange
s are
the
early
stag
e of
pre
ssur
e ulc
er d
evelo
pmen
t (Ap
pend
ix 2,
p. 20
) v
Sk
in co
nditi
on an
d su
bseq
uent
exa
mina
tion
is do
cum
ente
d wi
thin
the
indivi
dual’
s hea
lth re
cord
s
BPS2.indd 11 3/11/06 16:04:19

Best Practice Statement: Care of the Older Person’s Skin12
Sec
tio
n 2
c: P
res
sur
e u
lcer
s —
cla
ssif
icat
ion
Key
po
ints
: l A
ll in
divi
dual
s w
ith p
ress
ure
ulce
rs s
houl
d ha
ve t
he u
lcer
ass
esse
d us
ing
a re
cogn
ised
gra
ding
sca
le.
l A
sses
smen
t of
the
pre
ssur
e ul
cer
enab
les
appr
opri
ate
trea
tmen
t an
d in
terv
entio
n.
Stat
emen
tRe
ason
for s
tate
men
tH
ow to
dem
onst
rate
stat
emen
t is
bein
g ac
hiev
ed
v
All in
divid
uals
iden
tified
with
exis
ting p
ress
ure
ulcer
s sho
uld
have
their
ulce
r(s) a
sses
sed
to d
eter
mine
leve
l of t
issue
da
mag
e us
ing a
reco
gnise
d cla
ssific
atio
n to
ol, s
uch
as; t
he
EPUA
P G
uide
to P
ress
ure
Ulce
r Gra
ding
(199
9), t
he S
tirlin
g Pr
essu
re S
ore
Seve
rity S
cale
(SPS
SS) (
Reid
and
Mor
rison
, 19
94), a
nd th
e Pr
essu
re U
lcer S
cale
for H
ealin
g (PU
SH) t
ool
(Sto
tts et
al, 2
001)
v
Gra
ding
of p
ress
ure
ulcer
dam
age
enab
les co
rrec
t and
su
itable
trea
tmen
t and
inte
rven
tion
to b
e ini
tiate
d an
d m
ainta
ined
v
The
healt
h re
cord
s of a
ll ind
ividu
als id
entifi
ed as
hav
ing an
ex
isting
pre
ssur
e ulc
er(s)
will
includ
e ev
iden
ce o
f pre
ssur
e ulc
er gr
ading
from
the
initia
l iden
tifica
tion
v
Doc
umen
ted
evid
ence
with
in th
e he
alth
reco
rds o
f all
thos
e wi
th e
xistin
g pre
ssur
e ulc
ers o
f ong
oing a
ssessm
ent,
treatm
ent r
ation
ale an
d int
erve
ntion
s tak
en
v
The
pres
sure
ulce
r(s) s
hould
be
reas
sess
ed re
gular
ly, at
lea
st we
ekly,
or ac
cord
ing to
the
indivi
dual’
s con
ditio
n an
d/or
if th
e ind
ividu
al’s c
ondi
tion
chan
ges f
or b
ette
r or w
orse
v
Ong
oing
asse
ssm
ent e
nable
s an
accu
rate
and
indivi
duali
sed
treat
men
t plan
to b
e de
vised
v
Doc
umen
ted
evid
ence
that
the
indivi
dual’
s con
ditio
n an
d pr
essu
re u
lcer i
s rea
sses
sed
regu
larly,
at le
ast w
eekly
, or
mor
e fre
quen
tly ac
cord
ing to
the
indivi
dual’
s con
ditio
n
v
Whe
n as
sess
ing p
ress
ure
ulcer
s, th
e fo
llowi
ng sh
ould
be
cons
ider
ed: c
ause
, loca
tion,
grad
e (a
ccor
ding
to cl
assifi
catio
n to
ol), d
imen
sions
, wou
nd b
ed ap
pear
ance
, exu
date
, pain
, su
rrou
nding
skin
cond
ition
, and
, if in
fectio
n is
pres
ent
v
A co
mple
te h
istor
y and
phy
sical
exam
inatio
n of
the
indivi
dual
shou
ld b
e un
dert
aken
v
Early
iden
tifica
tion
of sk
in ch
ange
s and
/or t
horo
ugh
asse
ssm
ent o
f the
pre
ssur
e ulc
er(s)
shou
ld lea
d to
ap
prop
riate
trea
tmen
ts an
d int
erve
ntio
nsv
A
pres
sure
ulce
r sho
uld b
e as
sess
ed co
nside
ring t
he
indivi
dual’
s ove
rall p
hysic
al an
d ps
ycho
socia
l hea
lth
v
Evid
ence
with
in th
e ind
ividu
al’s h
ealth
reco
rds t
hat t
he
inter
vent
ions
take
n ar
e ba
sed
on fa
ctor
s ide
ntifie
d by
the
histo
ry an
d ph
ysica
l exa
mina
tion
of th
e ind
ividu
al
v
Pres
sure
ulce
rs sh
ould
be
asse
ssed
at le
ast w
eekly
, or m
ore
frequ
ently
acco
rding
to th
e ind
ividu
al’s c
ondi
tion
v
The
pres
sure
ulce
r req
uires
regu
lar as
sess
men
t to
obse
rve
for i
mpr
ovem
ent o
r det
erio
ratio
n in
cond
ition
v
Hea
lth re
cord
s con
tain
evid
ence
of r
egula
r rea
sses
smen
t, at
leas
t wee
kly, o
r mor
e of
ten
acco
rding
to th
e ind
ividu
al’s
cond
ition
BPS2.indd 12 3/11/06 16:04:19

13Best Practice Statement: Care of the Older Person’s Skin
Sec
tio
n 2
d: P
res
sur
e u
lcer
s —
sta
bili
sati
on
, po
siti
on
ing
Key
po
ints
: l In
divi
dual
s ‘at
ris
k’, o
r w
ith e
xist
ing
pres
sure
ulc
ers
are
not
left
out
of b
ed s
ittin
g fo
r lo
ng p
erio
ds.
l A
cute
ly il
l pat
ient
s ar
e re
turn
ed t
o be
d fo
r at
leas
t on
e ho
ur.
Stat
emen
tRe
ason
for s
tate
men
tH
ow to
dem
onst
rate
stat
emen
t is
bein
g ac
hiev
ed
v
Indi
vidua
ls at
risk
of p
ress
ure
ulcer
dev
elopm
ent,
or w
ith
exist
ing p
ress
ure
ulcer
s sho
uld b
e su
itably
pos
ition
ed w
hile
in be
d, or
up
sittin
g, to
mini
mise
pre
ssur
e, fri
ctio
n an
d sh
ear,
and
the
pote
ntial
for f
urth
er ti
ssue
dam
age
v
Indi
vidua
ls wh
o ca
n m
ove
indep
ende
ntly
shou
ld b
e en
cour
aged
to d
o so
v
Indi
vidua
ls wh
o re
quire
assis
tanc
e wi
th m
ovem
ent s
hould
, alo
ng w
ith as
socia
ted
care
rs, b
e ed
ucat
ed in
the
bene
fits
and
tech
nique
s of w
eight
dist
ribut
ion
v
Shor
t per
iods
(up
to tw
o ho
urs)
of su
staine
d pr
essu
re ca
n be
as d
amag
ing to
the
skin
as lo
ng p
erio
ds o
f sitt
ingv
Th
e tim
e pe
riod
betw
een
posit
ion
chan
ges i
s bas
ed o
n as
sess
men
t of e
ach
indivi
dual
and
their
cond
ition
v
Evid
ence
sugg
ests
that
indi
vidua
ls at
risk
of p
ress
ure
ulce
r dev
elopm
ent s
houl
d no
t be
posit
ione
d in
a sit
ting
posit
ion
for m
ore
than
two
hour
s with
out s
ome
form
of
repo
sitio
ning
(DeF
loor
, 200
0)v
D
evice
s to
assis
t with
the
repo
sitio
ning o
f ind
ividu
als ar
e av
ailab
le, su
ch as
elec
tric
and
non-
elect
ric p
rofili
ng b
eds,
spec
ialist
seat
ing. B
enefi
ts fro
m th
ese
have
bee
n re
cord
ed
v
Hea
lth re
cord
s sho
w ev
iden
ce o
f how
freq
uent
ly po
sitio
n ch
ange
s are
bein
g car
ried
out.
v
Hea
lth re
cord
s ind
icate
that
:
l
indivi
duals
at ri
sk o
f pre
ssur
e ulc
er d
evelo
pmen
t, or
with
exis
ting p
ress
ure
ulcer
s are
not
pos
ition
ed in
a se
at
for m
ore
than
two
hour
s, wi
thou
t bein
g rep
ositi
oned
. In
dividu
als w
ho ar
e ac
utely
ill m
ust b
e re
turn
ed to
bed
fo
r no
less t
han
one
hour
(Geb
hard
t and
Blis
s, 19
94)
l
when
pos
sible,
the
indivi
dual
and/
or ca
rer a
re in
volve
d in
the
man
agem
ent
l
for i
ndivi
duals
in b
ed, d
ifferin
g pos
ition
s suc
h as
the
30-
degr
ee ti
lt* (Y
oung
, 200
4) ar
e us
ed (F
igure
6, p
. 7)
l
hoist
sling
s and
slid
ing sh
eets
are
not l
eft u
nder
ind
ividu
als af
ter u
se**
l
skin
inspe
ctio
n sh
ould
be ca
rried
out
whe
n alt
ering
the
indivi
dual’s
pos
ition:
thes
e ins
pect
ions
can
help
guide
de
cisio
ns o
n th
e len
gth o
f tim
e bet
ween
pos
ition
chan
ges
v D
ocum
ent t
he re
sults
of s
kin in
spec
tion
and
any c
hang
es
mad
e to
the
repo
sitio
ning r
egim
e wi
thin
the
indivi
dual’
s he
alth
reco
rds
v
Indi
vidua
ls wi
th sp
ecific
mov
ing an
d ha
ndlin
g req
uirem
ents
(eg.
spina
l injur
ies) s
hould
hav
e th
eir n
eeds
asse
ssed
by t
he
prof
essio
nal w
ith th
e m
ost r
eleva
nt sk
ills
v
Mov
ing an
d ha
ndlin
g aids
can
help
repo
sitio
n ind
ividu
alsv
D
evice
s to
alter
an in
dividu
al’s p
ositi
on, s
uch
as e
lectri
c pr
ofilin
g bed
s, ar
e of
value
v
Hea
lth re
cord
s sho
w re
ferr
al to
the
appr
opria
te in
divid
ual,
ie. p
hysio
ther
apist
, occ
upat
iona
l the
rapi
st, s
pecia
list
mob
ility
serv
ices
* Th
e 30
-deg
ree
tilt is
whe
n th
e ind
ividu
al is
place
d in
the
later
ally-
inclin
ed p
ositio
n, su
ppor
ted
by p
illows
, with
their
bac
k mak
ing a
30-d
egre
e an
gle w
ith th
e su
ppor
t sur
face
**
With
asso
ciate
d m
anua
l han
dling
issu
es co
ncer
ning t
he re
mov
al of
a ho
ist o
r slin
g, eg
. pain
man
agem
ent, o
r com
fort
for t
erm
inally
ill p
atien
ts, a j
oint a
ssessm
ent b
y tiss
ue vi
abilit
y and
man
ual h
andli
ng ad
visor
s may
be
appr
opria
te
BPS2.indd 13 3/11/06 16:04:19

Best Practice Statement: Care of the Older Person’s Skin14
Sec
tio
n 2
e: P
res
sur
e u
lcer
s —
sta
bili
sati
on
, mat
tres
ses,
ch
air
s an
d c
ush
ion
sK
ey p
oin
ts:
l In
divi
dual
s ‘at
ris
k’, o
r w
ith a
pre
ssur
e ul
cer
mus
t be
car
ed fo
r on
an
appr
opri
ate
mat
tres
s.l In
divi
dual
req
uire
men
ts m
ay c
hang
e, b
ased
upo
n th
e co
nditi
on a
nd a
sses
smen
t.
Stat
emen
tRe
ason
for s
tate
men
tH
ow to
dem
onst
rate
stat
emen
t is
bein
g ac
hiev
ed
v
Indivi
duals
at ri
sk o
f pre
ssure
ulce
r dev
elopm
ent, o
r with
a pr
essu
re u
lcer(s
) ar
e not
care
d fo
r sole
ly on
stan
dard
NHS
ma
ttres
ses*
, or o
n ba
sic d
ivan
mattr
esse
s; at
a mini
mum,
they
ar
e pro
vided
with
a pr
essu
re-re
ducin
g foa
m ma
ttres
s or o
verla
yv
Facto
rs to
cons
ider w
hen
decid
ing o
n wh
ich p
ressu
re-re
ducin
g eq
uipme
nt to
pur
chas
e or h
ire in
clude
:
l
clini
cal e
fficac
y
l
ease
of m
ainte
nanc
e
l
impa
ct on
care
pro
cedu
res
l
patie
nt ac
cept
abilit
y
l
cost
l
ease
of u
sev
The d
ecisi
on to
pro
vide a
ny p
ressu
re-re
ducin
g equ
ipmen
t is
taken
as p
art o
f a co
mpre
hens
ive tr
eatm
ent/m
anag
emen
t str
ategy
, nev
er as
a so
le int
erve
ntion
v
Indivi
duals
bein
g car
ed fo
r on
spec
ialist
equip
ment
hav
e th
eir sk
in ins
pecte
d fre
quen
tly to
asse
ss th
e suit
abilit
y of t
he
equip
ment
; equ
ipmen
t req
uirem
ents
may c
hang
e with
chan
ges
in th
e pati
ent’s
cond
ition
v
Indivi
duals
at ri
sk, o
r with
pres
sure
ulce
rs, ar
e pro
vided
with
ap
prop
riate
pres
sure
-redu
cing e
quipm
ent w
hen s
itting
in a
chair
or
whe
elcha
ir, in
addit
ion to
whe
n the
y are
being
care
d for
in be
dv
Long
-term
whe
elcha
ir or
stati
c sea
t use
rs h
ave t
heir
need
s as
sesse
d by
thos
e with
relev
ant s
pecia
list s
kills
v
Ther
e is c
lear e
viden
ce th
at ind
ividu
als a
t risk
, or w
ith p
ressu
re
ulcer
s ben
efit f
rom
the p
rovis
ion o
f diffe
rent
/addit
ional
prod
ucts
from
the s
tanda
rd N
HS p
rovis
ion (C
ullum
et al
, 200
1; M
cInne
s, 20
04). I
ndivi
duals
with
an ex
isting
pre
ssure
ulce
r who
ar
e acu
tely
ill, o
r who
hav
e res
tricte
d mo
bility
in b
ed, a
re lik
ely
to re
quire
an ai
r-fille
d ma
ttres
s or o
verla
y (wh
ich is
comm
only,
thou
gh n
ot ex
clusiv
ely, a
ltern
ating
)
v
Ther
e is n
o cle
ar ev
idenc
e to
dete
rmine
whic
h typ
e of p
rodu
cts
are b
est t
o us
e in
any p
artic
ular s
ituati
on (C
ullum
, 200
1)
v
Indivi
duals
iden
tified
as re
quirin
g pre
ssure
-redu
cing e
quipm
ent
(matt
resse
s, sea
ting a
nd cu
shion
s) re
ceive
it as
soon
as po
ssible
, as
delay
may
resu
lt in f
urth
er tis
sue d
amag
e
v
Furth
er ti
ssue d
amag
e may
occ
ur w
hen
patie
nts a
re si
tting
in
chair
s (De
floor
, 200
0)
v
Chair
s and
/or c
ushio
ns d
esign
ed to
redu
ce th
e risk
of p
ressu
re
ulcer
dev
elopm
ent m
ust b
e suit
ed to
indiv
idual
need
s, in
relat
ion to
heig
ht, w
eight
, pos
tura
l alig
nmen
t and
foot
supp
ort
v
The s
afety
of st
atic s
eats
can
be co
mpro
mise
d du
e to
chan
ges
in he
ight, b
alanc
e and
lumb
ar su
ppor
t with
the u
se o
f cus
hions
(C
ollins
, 200
0)
v
Thes
e ind
ividu
als h
ave s
pecifi
c req
uirem
ents
base
d on
their
ov
erall
phy
sical
cond
ition,
inclu
ding t
he co
nditio
n of
their
skin
v
Ther
e is a
clea
r org
anisa
tiona
l poli
cy co
ncer
ning t
he p
rovis
ion
of sp
ecial
ist eq
uipme
nt fo
r ind
ividu
als at
risk
, or w
ith ex
isting
pr
essu
re u
lcers
v
The p
olicy
inclu
des g
uidan
ce o
n wh
en to
seek
advic
e fro
m a
spec
ialist
in th
e field
of t
issue
viab
ility
v
The d
ecisio
n to
use a
ny pr
oduc
t bey
ond a
basic
NHS
matt
ress
or
divan
is do
cume
nted
in th
e ind
ividu
al’s he
alth r
ecor
d v
Ch
airs a
nd/o
r cus
hions
desig
ned t
o re
duce
the r
isk o
f pre
ssure
ulc
er de
velop
ment
mus
t be s
uited
to in
dividu
al ne
eds, i
n rela
tion t
o th
e ind
ividu
al’s he
ight, w
eight
, pos
tura
l alig
nmen
t and
foot
supp
ort
v
The s
afety
of st
atic s
eats
can
be co
mpro
mise
d du
e to
chan
ges
in he
ight, b
alanc
e and
lumb
ar su
ppor
t with
the u
se o
f cus
hions
(C
ollins
, 200
0)v
Docu
ment
any m
easu
res b
eing i
mplem
ente
d in
addit
ion to
the
use o
f spe
cial m
attre
sses a
nd o
verla
ys
v
Docu
ment
the d
ate o
f firs
t use
of s
pecia
list e
quipm
ent
v
Re
gular
skin
inspe
ction
s, at
least
week
ly or
acco
rding
to
the i
ndivi
dual’
s con
dition
, and
any s
ubse
quen
t acti
ons t
aken
/de
cision
s mad
e are
doc
umen
ted
in th
e hea
lth re
cord
v
The i
ndivi
dual’
s hea
lth re
cord
doc
umen
ts th
e asse
ssmen
t of
their
nee
ds in
relat
ion to
whe
elcha
ir/sta
tic se
at us
ev
Lo
ng-te
rm w
heelc
hair
and
static
seat
user
s’ he
alth
reco
rds
carr
y asse
ssmen
t rec
ords
by a
suita
bly tr
ained
spec
ialist
* A
stand
ard
NH
S m
attre
ss is
one
with
out a
ny p
artic
ular p
ressu
re-re
ducin
g qua
lities
men
tione
d in
the
prod
uct l
itera
ture
. In ge
nera
l, it i
s les
s tha
n 15
cms t
hick ,
has
a sin
gle d
ensit
y foa
m th
at is
not
caste
llate
d or
cut t
o en
hanc
e pr
essu
re d
istrib
utio
n, an
d do
es n
ot h
ave
a sem
i-per
mea
ble tw
o-wa
y stre
tch
cove
r
BPS2.indd 14 3/11/06 16:04:20

15Best Practice Statement: Care of the Older Person’s Skin
Sec
tio
n 2
f: P
res
sur
e u
lcer
s —
pr
om
oti
ng
hea
lin
gK
ey p
oin
ts:
l Ex
tens
ive
supe
rfici
al p
ress
ure
ulce
rs, o
r an
y se
vere
pre
ssur
e ul
cers
, req
uire
spe
cial
ist
refe
rral
. l Pr
essu
re u
lcer
s ca
n be
life
-thr
eate
ning
.
Stat
emen
tRe
ason
for s
tate
men
tH
ow to
dem
onst
rate
stat
emen
t is
bein
g ac
hiev
ed
v
Exte
nsive
supe
rficia
l pre
ssure
ulce
rs, o
r any
seve
re p
ressu
re
ulcer
s, sh
ould
be co
nside
red
for r
eferr
al on
to sp
ecial
ist se
rvice
s, ie.
tissu
e viab
ility s
pecia
list n
urse
s (TV
Ns)
or p
lastic
surg
eon
v
Alwa
ys en
sure
that
the m
edica
l staf
f in ch
arge
of
an in
dividu
al’s
care
are n
otifie
d of t
he ex
isten
ce an
d ext
ent o
f pre
ssure
dama
ge
v
The m
anag
emen
t of in
dividu
als w
ith la
rge a
reas
of s
uper
ficial
ulc
ers,
or an
y sev
ere u
lcers
, requ
ires s
pecia
list i
nput
due
to th
e po
tent
ial fo
r the
dev
elopm
ent o
f life-
thre
atenin
g com
plica
tions
, eg
. sep
ticae
mia
v
Healt
h re
cord
s sho
w th
at ind
ividu
als w
ith ex
tens
ive su
perfi
cial
pres
sure
ulce
ratio
n ha
ve b
een
refer
red
for a
spec
ialist
revie
w,
unles
s the
indiv
idual’
s con
dition
dict
ates o
ther
wise
v
Healt
h re
cord
s sho
w th
at ind
ividu
als w
ith se
vere
pre
ssure
ulc
erati
on h
ave b
een
refer
red
for a
spec
ialist
revie
w un
less t
he
indivi
dual’
s con
dition
dict
ates o
ther
wise
v
Healt
h re
cord
s of t
he in
dividu
al re
ferre
d fo
r spe
cialis
t rev
iew
shou
ld re
flect
the n
ature
of r
eferr
al, eg
. telep
hone
or l
ette
r, an
d th
e out
come
of t
he re
ferra
l, eg.
telep
hone
advic
e or d
irect
cons
ultati
on
v
Each
indiv
idual
with
a pr
essu
re u
lcer s
hould
hav
e a cl
ear p
lan o
f ma
nage
ment
out
lined
in th
eir h
ealth
reco
rd, in
cludin
g:
l
full in
dividu
al as
sessm
ent
l
any i
nter
vent
ions,
eg. s
pecia
list m
attre
sses,
cush
ions o
r ot
her d
evice
s
l
full a
ssessm
ent o
f the
pre
ssure
ulce
r, cau
se, lo
catio
n, cla
ssific
ation
, des
cript
ion o
f the
wou
nd, tr
eatm
ent a
ims a
nd
objec
tives
, revie
w da
te
v
Pres
sure
ulce
rs ar
e like
ly to
requ
ire a
numb
er o
f wee
ks o
r mo
nths
to he
al, de
pend
ing o
n the
ir se
verit
y and
the i
ndivi
dual’s
co
re m
orbid
ity, p
artic
ularly
ambu
lator
y cap
acity
and t
heir
abilit
y to
chan
ge th
eir o
wn po
sition
v
Healt
h re
cord
s inc
lude e
viden
ce th
at a f
ull as
sessm
ent o
f th
e pre
ssure
ulce
r has
bee
n un
derta
ken,
along
with
a pla
n of
ma
nage
ment
: this
shou
ld inc
lude s
teps
to en
sure
cont
inuity
of
care
bet
ween
care
setti
ngs. T
he h
ealth
reco
rd sh
ould
includ
e all
form
al re
ferra
ls, or
info
rmal
discu
ssion
s with
spec
ialist
s re
gard
ing th
e man
agem
ent o
f the
indiv
idual
v
Evide
nce o
f initia
l and
ong
oing m
anag
emen
t to
prev
ent f
urth
er
tissu
e dam
age s
hould
be e
viden
t
v
The m
anag
emen
t of t
he w
ound
bed
of a
pre
ssure
ulce
r sho
uld
adhe
re to
the p
rincip
les o
f mois
t wou
nd m
anag
emen
t unle
ss th
e ind
ividu
al’s c
ondit
ion d
ictate
s oth
erwi
se (t
his m
ay b
e co
ntra
indica
ted
when
an in
dividu
al is
term
inal a
nd d
ebrid
emen
t of
the p
ressu
re u
lcer i
s not
appr
opria
te). T
he d
ressi
ngs u
sed
will
not c
ause
trau
ma to
the w
ound
bed
v
Wou
nds m
anag
ed us
ing pr
oduc
ts wh
ich pr
omot
e mois
t wou
nd
heali
ng re
sult
in en
hanc
ed he
aling
rate
s and
redu
ced i
nfecti
on
v
Using
pro
ducts
whic
h pr
omot
e a m
oist w
ound
envir
onme
nt,
unles
s con
traind
icate
d by
the i
ndivi
dual’
s con
dition
, and
then
do
cume
nting
them
in th
e hea
lth re
cord
sv
Do n
ot u
se d
ressi
ng m
ateria
ls wh
ich ad
here
to th
e wou
nd b
ed
and/
or ca
use t
raum
a to
the w
ound
bed
BPS2.indd 15 3/11/06 16:04:20

Best Practice Statement: Care of the Older Person’s Skin16
Sec
tio
n 3
a: S
kin
car
e —
in
co
nti
nen
ce
Key
po
ints
: l In
cont
inen
ce c
an in
crea
se t
he r
isk
of s
kin
brea
kdow
n.
l C
lean
sing
with
soa
p an
d w
ater
can
incr
ease
the
ris
k of
ski
n br
eakd
own.
l A
ppro
pria
te m
easu
res
shou
ld b
e ta
ken
to p
reve
nt s
kin
brea
kdow
n.
Stat
emen
tRe
ason
for s
tate
men
tH
ow to
dem
onst
rate
stat
emen
t is
bein
g ac
hiev
ed
v
Indivi
duals
with
inco
ntine
nce s
hould
und
ergo
a ho
listic
nurs
ing
asse
ssmen
t, whic
h inc
ludes
que
stion
s reg
ardin
g blad
der a
nd/o
r bo
wel fu
nctio
n/ha
bit
v
Indivi
duals
with
inco
ntine
nce h
ave t
heir
cont
inenc
e stat
us
reas
sesse
d re
gular
ly, or
acco
rding
to th
e ind
ividu
al’s c
ondit
ion
v
Cont
inenc
e man
agem
ent s
hould
be r
eview
ed re
gular
ly
v
Soap
and
wate
r sho
uld n
ot b
e use
d wh
en cl
eans
ing fo
llowi
ng
episo
des o
f inco
ntine
nce
v
The u
se o
f foam
clea
nser
s is r
ecog
nised
as a
clean
sing r
egim
e fo
r ind
ividu
als w
ith in
cont
inenc
e
v
If sk
in is
exco
riate
d or
bro
ken,
prod
ucts
which
pro
mote
a mo
ist
woun
d en
viron
ment
shou
ld be
use
d. Un
less c
ontra
indica
ted
by
the i
ndivi
dual’
s phy
sical
cond
ition,
a full
asse
ssmen
t to
asce
rtain
th
e cau
se o
f the
inco
ntine
nce i
s req
uired
v
Urina
ry in
cont
inenc
e is a
comm
on p
roble
m aff
ectin
g up
to 1
0%
of th
e pop
ulatio
n (R
oe et
al, 1
996)
. Inco
ntine
nce i
s a sy
mpto
m,
not a
diag
nosis
. Asse
ssmen
t is c
rucia
l, as e
ffecti
ve m
anag
emen
t is
dete
rmine
d by
accu
rate
diag
nosis
of t
he ty
pe o
f inco
ntine
nce
(Che
ater e
t al, 1
992)
v
Incon
tinen
ce ca
n inc
reas
e an
indivi
dual’
s risk
of s
kin d
amag
e due
to
chem
ical ir
ritati
on fr
om b
oth
urine
, and
faec
es an
d/or
the
inapp
ropr
iate s
kin cl
eans
ing re
gime
v
Chan
ges i
n inc
ontin
ence
(inc
ontin
ence
patt
ern,
clean
sing r
egim
e us
ed, c
ontin
ence
aids
) can
cont
ribut
e to
the d
evelo
pmen
t of
skin
brea
kdow
n
v
Clea
nsing
with
soap
and
wate
r can
cont
ribut
e to
the
deve
lopme
nt o
f pre
ssure
ulce
rs (C
oope
r and
Gra
y, 200
1)
v
Barr
ier cr
eams
and
barr
ier fi
lms c
an b
e use
d on
intac
t and
/or
brok
en sk
in to
act a
s a b
arrie
r aga
inst f
urth
er ir
ritati
on fr
om
incon
tinen
ce. R
eapp
licati
on an
d us
e sho
uld b
e in
acco
rdan
ce
with
man
ufactu
rers
’ instr
uctio
ns
v
Reco
rds o
f all h
olisti
c nur
sing a
ssessm
ents
includ
e refe
renc
e to
cont
inenc
e stat
us an
d an
y cur
rent
trea
tmen
t
v
All n
urse
s hav
e acc
ess t
o inf
orma
tion
on as
sessi
ng
incon
tinen
ce an
d as
socia
ted
cont
inenc
e car
e plan
ning
v
All n
urse
s hav
e acc
ess t
o an
asse
ssmen
t too
l
v
Healt
h re
cord
s inc
lude e
viden
ce th
at re
gular
skin
inspe
ction
tak
es p
lace a
t opp
ortu
ne ti
mes,
eg. d
uring
assis
tance
with
pe
rson
al hy
giene
v
Findin
gs fr
om sk
in ins
pecti
on in
dicati
ng th
at fur
ther
actio
n is
requ
ired,
along
with
subs
eque
nt ac
tion
taken
, are
reco
rded
in
the i
ndivi
dual’
s hea
lth re
cord
s
v
The h
ealth
reco
rds d
ocum
ent e
pisod
es o
f inco
ntine
nce a
nd
indica
te ac
tion
taken
, inclu
ding s
kin cl
eans
ing p
rodu
cts u
sed
v
The a
dvice
of a
cont
inenc
e adv
isor i
s sou
ght w
here
cont
inenc
e ma
nage
ment
pro
ducts
are c
ompr
omise
d by
the i
ndivi
dual’
s co
nditio
n, or
oth
er in
terv
entio
ns af
fectin
g qua
lity o
f life,
ie.
pres
sure
-redu
cing m
attre
sses
v
The i
ndivi
dual’
s hea
lth re
cord
s con
tain
evide
nce o
f ong
oing
asse
ssmen
t, tre
atmen
t rati
onale
and
inter
vent
ions t
aken
BPS2.indd 16 3/11/06 16:04:20

17Best Practice Statement: Care of the Older Person’s Skin
Sec
tio
n 3
b: S
kin
car
e —
mac
erat
ion
Key
po
ints
: l M
acer
atio
n of
the
ski
n ca
n ca
use
skin
bre
akdo
wn.
l A
ppro
pria
te m
easu
res
shou
ld b
e ta
ken
to p
reve
nt s
kin
brea
kdow
n.
Stat
emen
tRe
ason
for s
tate
men
tH
ow to
dem
onst
rate
stat
emen
t is
bein
g ac
hiev
ed
v
Asse
ssmen
t sho
uld b
e car
ried
out t
o de
term
ine th
e cau
se o
f ma
cera
tion
of sk
in as
it m
ay b
e due
to an
y of t
he fo
llowi
ng
facto
rs: in
cont
inenc
e (se
e Sec
tion 3
a), e
xces
s mois
ture
, wou
nd
exud
ate, p
eri-s
toma
l exu
date
v
Early
det
ectio
n of
skin
mace
ratio
n th
roug
h ide
ntific
ation
of t
he
caus
e may
pre
vent
skin
brea
kdow
nv
He
alth
reco
rds h
ave e
viden
ce th
at as
sessm
ent h
as b
een
carr
ied
out t
o de
term
ine ca
use o
f mac
erati
on
v
Area
s of m
acer
ation
may
ben
efit f
rom
the a
pplic
ation
of a
ba
rrier
film
or c
ream
to p
reve
nt fu
rther
det
erior
ation
of
skin
cond
ition
v
Mace
ratio
n is l
ikely
to o
ccur
arou
nd w
ound
s and
with
in sk
in fol
ds
which
are i
n con
tact w
ith ea
ch o
ther
v
Appli
catio
n of a
barri
er ag
ent, e
g. ba
rrier
film
or cr
eam
may h
elp
redu
ce th
e irri
tant e
ffects
of m
acer
ation
of h
ealth
y tiss
ue
(Bale
, 200
4)
v
Asse
ssmen
t sho
uld in
clude
exam
inatio
n of
area
s at r
isk o
f ma
cera
tion
which
is re
cord
ed in
the i
ndivi
dual’
s hea
lth re
cord
s
v
Whe
n se
lectin
g a b
arrie
r film
or c
ream
, ens
ure t
hat i
t doe
s no
t affe
ct th
e pro
perti
es o
f oth
er in
terv
entio
ns, e
g. th
e stic
king
abilit
y of a
n ad
hesiv
e dre
ssing
v
Some
barri
er cr
eams
will
redu
ce th
e adh
esion
of a
dhes
ive
dres
sings
, or r
educ
e the
abso
rben
cy o
f con
tinen
ce ai
dsv
Healt
h re
cord
s sho
w wh
ich b
arrie
r age
nt h
as b
een
used
and
reco
rd fr
eque
ncy o
f rea
pplic
ation
v
The m
anag
emen
t of t
he w
ound
shou
ld be
bas
ed o
n a f
ull
asse
ssmen
t to
dete
rmine
why
exud
ate is
pre
sent
, ie. p
art o
f no
rmal
heali
ng o
r an
infec
tion
is pr
esen
t
v
Trea
tmen
t int
erve
ntion
s will
be ba
sed u
pon e
arly
ident
ificati
on
of th
e cau
se o
f wou
nd ex
udate
v
Evide
nce o
f initia
l and
ong
oing m
anag
emen
t to
prev
ent f
urth
er
tissu
e dam
age s
hould
be p
rese
nt, a
nd re
cord
ed w
ithin
the
indivi
dual’
s hea
lth re
cord
s
v
Reco
rd o
f th
e volu
me an
d vis
cosit
y of e
xuda
te an
d its
qua
lity,
eg. h
aemo
puru
lent, s
eros
angu
inous
, etc
., alon
g with
not
es to
ind
icate
the r
easo
n fo
r its
pres
ence
, eg.
infec
tion,
card
iac fa
ilure
, lim
b sw
elling
, etc
. are
reco
rded
in th
e not
es o
f pati
ents
with
ma
cera
tion
BPS2.indd 17 3/11/06 16:04:20

Best Practice Statement: Care of the Older Person’s Skin18
Sec
tio
n 4
: Sk
in t
ear
sK
ey p
oin
ts:
l If
trea
ted
quic
kly,
re-la
ying
a s
kin
tear
flap
can
enc
oura
ge w
ound
hea
ling.
l A
ppro
pria
te m
easu
res
shou
ld b
e ta
ken
to m
anag
e sk
in t
ears
.
Stat
emen
tRe
ason
for s
tate
men
tH
ow to
dem
onst
rate
stat
emen
t is
bein
g ac
hiev
ed
v
Asse
ssmen
t sho
uld be
carri
ed o
ut to
dete
rmine
the c
ause
of t
he
skin
tear
and t
his sh
ould
be re
move
d to
prev
ent f
urth
er in
jury
v
Early
det
ectio
n of
skin
traum
a thr
ough
iden
tifica
tion
of th
e ca
use m
ay p
reve
nt fu
rther
skin
brea
kdow
n (B
aron
oski,
200
3)v
He
alth
reco
rds h
ave e
viden
ce th
at as
sessm
ent h
as b
een
carr
ied
out t
o de
term
ine th
e cau
se o
f the
skin
tear,
and
that
this
has
been
remo
ved
v
The s
kin te
ar sh
ould
be cl
assifi
ed (A
ppen
dix 4
, p. 2
1) ac
cord
ing
to th
e deg
ree o
f tiss
ue d
amag
ev
Cl
assifi
catio
n of t
he da
mage
enab
les co
rrect
and s
uitab
le tre
atmen
t and
inte
rven
tion t
o be
initia
ted a
nd m
aintai
ned
v
Healt
h re
cord
s sho
w th
at ind
ividu
als w
ith a
skin
tear
hav
e ha
d a f
ull as
sessm
ent a
nd th
at a p
lan o
f man
agem
ent h
as b
een
deve
loped
, whic
h inc
orpo
rate
s rev
iew o
f the
wou
nd an
d co
ntinu
ity o
f car
e bet
ween
diffe
rent
care
setti
ngs
v
Man
agem
ent o
f skin
tear
s sho
uld co
nside
r:
l
stopp
ing b
leedin
g if it
is p
ersis
tent
l
prev
entin
g infe
ction
l
minim
ising
pain
and
disco
mfor
t
l
reco
verin
g skin
inte
grity
v
Wou
nds w
hich a
re m
anag
ed fo
llowi
ng th
e prin
ciples
of m
oist
woun
d hea
ling,
resu
lt in
enha
nced
heali
ng ra
tes a
nd re
duce
d inf
ectio
n rate
s
v
Evide
nce
of in
itial
and
ongo
ing m
anag
emen
t to
prev
ent f
urth
er
tissu
e da
mag
e sh
ould
be re
cord
ed w
ithin
the
indivi
dual’
s he
alth
reco
rds
v
Man
agem
ent o
f wou
nds i
nvolv
es m
aintai
ning s
kin in
tegr
ity:
l
if the
skin
tear
has
drie
d ou
t, it s
hould
be r
emov
ed u
sing
a ste
rile t
echn
ique
l
if the
skin
flap
is sti
ll viab
le, cl
eans
e with
war
m, sa
line o
r tap
wa
ter, a
nd ro
ll the
flap
bac
k int
o pla
ce to
obt
ain o
ptim
um
skin
cove
r
l
if the
skin
tear
is vi
able,
secu
re u
sing o
ne o
f the
sugg
este
d
me
thod
s: ad
hesiv
e wou
nd cl
osur
e stri
ps, s
kin gl
ue, s
ilicon
e
on-ad
hesiv
e dre
ssing
s. Ho
weve
r, the
met
hod
of sk
in
appli
catio
n wi
ll still
requ
ire th
e app
licati
on o
f an
appr
opria
te
se
cond
ary d
ressi
ng to
pro
vide f
urth
er p
rote
ction
v
Trea
tmen
t int
erve
ntion
s and
a pla
n of c
are sh
ould
be ev
ident
wi
thin
the i
ndivi
dual’s
healt
h rec
ords
BPS2.indd 18 3/11/06 16:04:21

19Best Practice Statement: Care of the Older Person’s Skin
Appendix 1: Definitions of topical skin applications
Emollients: also known as moisturisers. These are grease-based substances which, when applied to the skin, either trap water in or allow water to be pulled from the dermis to the epidermis (Loden, 2003). Emollients can be used as wash products in the form of soap substitutes and bath oils. Once washing is complete, emollients can be applied to the skin in the form of lotions, creams or ointments to seal water into the skin (Penzer and Burr, 2005).
Lotions: these are the lightest and least greasy emollients. They are less effective as they contain less oil.
Creams: these have a higher oil content than lotions, allowing the oil to sink into the skin. They are good for daytime use.
Ointments: these have the highest oil content and are very greasy. They can leave the skin looking shiny and clothes greasy. However, if the skin is very dry, ointments should be used and may be best applied at night.
Table 1: Quantities of dermatological preparationsprescribed for specific areas of the body
Creams and ointments Lotions
Face 15–30 g 100 ml
Both hands 25–5 g 200 ml
Scalp 50–100 g 200 ml
Both arms or legs 100–200 g 200 ml
Trunk 400 g 500 ml
Groins and genitalia 15–25 g 100 ml
BPS2.indd 19 3/11/06 16:04:21

Best Practice Statement: Care of the Older Person’s Skin20
Appendix 2: Skin examination
Further examination of erythema or skin discoloration should include the following steps:
v Apply light finger pressure to the area of erythema or discoloration for 10 seconds.
v Release the pressure. If the area is white and then returns to its original colour, the area probably has an adequate blood supply. Observation should continue and preventative strategies should be employed.
v If, on release of pressure, the area remains the same colour as before pressure was applied, it is an indication of the beginning of pressure ulcer development and preventative strategies should be employed immediately.
v If there is an alteration in the skin colour (redness, purple or black), increased heat or swelling, it may imply underlying tissue breakdown. Frequency of assessment should be increased and preventative strategies should be employed.
v With dark skin pigmentation, pressure ulcer development will be indicated by areas where there is localised heat, or where there is damage, coolness, purple/black discoloration, localised oedema and induration.
Appendix 3: Formal Risk Assessment Scales, Examples
Braden Scale Bergstrom N, Braden BJ, Laguzza A, Holman V (1987) The Braden scale for predicting pressure sore risk. Nurs Res 36(4): 205–10
Knoll scale Towey AP, Erland SM (1988) Validity and reliability of an assessment tool for pressure ulcer risk. Decubitus 1(2): 40–8
Norton Scale Norton D, Mclaren R, Exton-Smith AN (1962) An investigation of geriatric nursing problems in hospital. The National Corporation for the Care of Old People, London
Pressure Sore Prediction Score Lowthian P (1989) Identifying and protecting patients who may get pressure sores. Nurs Standard 4(4): 26–9
Waterlow Risk Assessment Score Waterlow J (1988) The Waterlow card for the prevention and management of pressure sores: towards a pocket policy. Care Science and Practice 6(1): 8–12
Pressure Ulcer Risk Assessment Tool (PURAT)
Wicks G (2006) PURAT: is clinical judgement an effective alternative? Wounds UK 2(2): 14–24
Pressure ulcer risk assessment scales for children: Bedi, Cockett, Garvin, Braden Q, Pickersgill, the Pattoid pressure scoring system, the paediatric pressure sore/skin damage risk assessment (Waterlow)
Wilcock J (2006) Pressure ulcer risk assessment in children. In: White R, Denyer J, eds. Paediatric Skin and Wound Care. Wounds UK, Aberdeen: 79–86
BPS2.indd 20 3/11/06 16:04:21

21Best Practice Statement: Care of the Older Person’s Skin
Appendix 4: Pressure ulcer Classification Scales,Examples
European Pressure Ulcer Advisory Panel (EPUAP)
The management of pressure ulcers in primary and secondary care. NICE Clinical Guidelines, September 2005
Pressure ulcers Best Practice Statement for Treatment/Management of Pressure Ulcers. NHS Quality Improvement Scotland, March 2005
Stirling Pressure Sore Severity Scale(SPSSS)
Reid J, Morrison M (1994) Towards a consensus classification of pressure sores.J Wound Care 3(3): 157–60
Pressure Ulcer Scale for Healing(PUSH)
Stotts NA, Rodeheaver GT, Thomas DR, Frantz RA et al (2001) An instrument to measure healing in pressure ulcers: development and validation of the pressure ulcer scale for healing (PUSH).Journals of Gerontology Series: A Biological Sciences and Medical Sciences 56(12): 795
Appendix 5: Skin Tear Classification System
Category 1 Without tissue loss In a linear or flap type skin tear. The epidermis and dermis have been pulled apart, as if an incision has been made
Category 11 Partial skin loss 25% or less25% or more
Where part of the epidermis is lost. This can be categorised as less than 25% or more than 25% tissue loss
Category 111 Full-thickness skin loss The epidermal flap or tissue is absent in this type of skin tear
(Source: Payne and Martin, 1993)
BPS2.indd 21 3/11/06 16:04:21

Best Practice Statement: Care of the Older Person’s Skin22
References
Allman RM (1997) Pressure ulcer prevalence, incidence, risk factors, and impact. Clin Geriatr Med 13(3): 421–36
Bale S, Tebble N, Jones VJ, Price PE (2004) The benefits of introducing a new skin care protocol in patients cared for in nursing homes. J Tissue Viability 14(2): 44–50
Baranoski S (2003) Skin Tears: Staying on guard against the enemy of frail skin. Nursing 33(10): 14–20
Baranoski S, Ayello EA (2004) Wound Care Essentials, Practice Principles. Lippincott, Williams and Wilkins, Springhouse, PA
Beldon P (2006) Pressure Ulcers: prevention and management. Wound Essentials 1: 68–81
Berg RW (1986) Etiology and pathophysiology of diameter dermatitis. Adv Dermatol 3: 102–6
British National Formulary (2006) British National Formulary, No 51. British Medical Association and the Royal Pharmaceutical Society of Great Britain, London
Britton J (2003) Eczema. Prescribing and using topical treatments for all types of eczema. Available online at: www.dermatology.co.uk
Britton J (2003) The use of emollients and their correct application. J Community Nurs 17(9): 22–5
Bryant R (1992) Acute and Chronic Wounds: Nursing Management. Mosby Year book, St Louis
Buckingham KW, Berg RW (1986) Etiologic factors in diaper dermatitis: the role of feces. Pediatr Dermatol 3(2): 107–12
Butcher M, White R (2005) The structure and functions of the skin. In: White R, ed. Skin Care in Wound Management: Assessment, prevention and treatment. Wounds UK, Aberdeen: 1–16
Calianno C (2002) Patient hygiene, Part 2 – skin care: keeping the outside healthy. Nursing. 29(12): suppl 1–11; quiz 12–3
Cheater F, Lakhani M, Cawood C (1999) Assessment of patients with urinary incontinence: evidence-based audit protocol for primary healthcare teams. Department of General Practice and Primary health Care, University of Leicester. Protocol CT15. Available online at: www.leac.uk/cgrdu/protocol.html
Clark M, Watts S (1994) The incidence of pressure sores within a National Health Service Trust Hospital during 1991. J Adv Nurs 20(1): 33–6
Collier M (1996) Pressure-reducing mattresses. J Wound Care 5(5): 207–11
Collins F (2000) Selecting the most appropriate armchair for patients. J Wound Care 9(2): 73–6
Cooper P, Gray D (2001) Comparison of two skin care regimes for incontinence. Br J Nurs (Supplement) 10(6): 6–20
Cullum N, Deeks J, Sheldon T et al (2001) Beds, mattresses and cushions for pressure ulcer prevention and treatment. Cochrane Database of Systematic Reviews (2): (CD001735) (last substantive update May 2004 )
Dealey C (1994) The Care of Wounds. Blackwell Science, Oxford
Defloor T (2000) The effect of position and mattress on interface pressure. Appl Nurs Res 13(1): 2–11
European Pressure Ulcer Advisory Panel (1999) Guide to Pressure Ulcer Grading. EPUAP Rev 3(3): 75
Fiers SA (1996) Breaking the cycle: The etiology of incontinence dermatitis and evaluating and using skin care products. Ostomy/Wound Management 42(3): 33–43
BPS2.indd 22 3/11/06 16:04:21
23Best Practice Statement: Care of the Older Person’s Skin
Flanagan M, Fletcher J (2003) Tissue Viability: Managing chronic wounds. In: Booker C, Nicol M, eds. Nursing Adults: The Practice of Caring. Mosby, St Louis
Gebhardt K, Bliss MR (1994) Preventing pressure sores in orthopaedic patients — is prolonged chair nursing detrimental? J Tissue Viability 4(2): 51–4
Günnewicht B, Dunford C (2004) Fundamental Aspects of Tissue Viability Nursing. Quay Books, MA Healthcare, London
Kaminer M, Gilchrist B (1994) Aging of the skin. In: Hazzard W, ed. Principles of Geriatric Medicine and Gerontology. McGraw-Hill Book Co, New York
Le Lievre S (2000) Care of the incontinent client’s skin. J Community Nurs 14(2): 26–32
Leyden JJ, Katz S, Stewart R, Kligman AM (1977) Urinary ammonia and ammonia producing micro-organisms in infants with and without diaper dermatitis. Arch Dermatol 113: 1678–80
Loden M (2003) Role of topical emollients and moisturisers in the treatment of dry skin barrier disorders. Am J Clin Dermatol 4(11): 771–88
McInnes E (2004) The use of pressure-relieving devices (beds, mattresses and overlays) for the prevention of pressure ulcers in primary and secondary care. J Tissue Viability 14(1): 4–6, 8, 10 passim
Morris C (2005) Skin Trauma. In: White R, ed. Skin Care in Wound Management: Assessment, prevention and treatment. Wounds UK, Aberdeen: 74–86
NHS Quality Improvement Scotland (2005) Best Practice statement for the Treatment/Management of Pressure Ulcers. NHS Quality Improvement Scotland
National Institute for Clinical Excellence (2005) CG29 Pressure ulcer management: Quick reference guide. NICE, London. Available online at: www.nice.org.uk/download.aspx?o=CG029quickrefguide
Payne RL, Martin MC (1993) Defining and classifying skin tears: need for a common language. Ostomy/Wound Management 39(5): 16–26
Penzer R, Burr S (2005) Promoting skin health. Nurs Standard 19(36): 57–65
Reid J, Morrison M (1994) Towards a consensus: classification of pressure sores. J Wound Care 3(3): 157–60
Roe B, Wilson K, Doll H, Brooks P (1996) An evaluation of health interventions by primary health care teams and continence advisory services on patient outcomes related to incontinence. Department of Public Health and Primary Care, University of Oxford. (Summary volume available from the Continence Foundation)
Stephen Haynes J (2005) Essential Skin Care: Protection and Maintenance. 3M Health Care Limited, Loughborough
Stotts NA, Rodeheaver GT, Thomas DR, Frantz RA et al (2001) An instrument to measure healing in pressure ulcers: development and validation of the pressure ulcer scale for healing (PUSH). J Gerontology Series: A Biological Sciences and Medical Sciences 56(1): 795
Timmons J (2006) Skin function and wound healing physiology. Wound Essentials 1: 8–17
White RJ, Cutting KF (2003) Interventions to avoid maceration of the skin and wound bed. Br J Nurs 12(20): 1186–1203
Whittingham K (1998) Cleansing regimes for continence care. Prof Nurse 14(3): 167–72
Winter GD (1963) Formation of the scab and the rate of epithelialisation of superficial wounds in the skin of the young domestic pig. Nature 193(4812): 293–4
Young T (2004) The 30-degree tilt position vs the 90-degree lateral and supine positions in reducing the incidence of non-blanching erythema in a hospital inpatient population: a randomised controlled trial. J Tissue Viability 14(3): 88, 90, 92–6
BPS2.indd 23 3/11/06 16:04:22

Best Practice Statement: Care of the Older Person’s Skin24
Notes
BPS2.indd 24 3/11/06 16:04:22