benign endometrial diseases
TRANSCRIPT

Benign Endometrial Diseases
Dr.S.Davoodi
• Normal cycle is divided into two phases: follicular
and luteal.
• The follicular phase begins with the onset of
menses and ends on the day before the luteinizing
hormone (LH) surge.{ 14 to 21 days }
• The luteal phase begins on the day of the LH surge
and ends at the onset of the next menses. { 14
days }

• Benign endometrial histology includes atrophy
(absence of a hormonal effect), proliferative
endometrium (estrogen effect), secretory
endometrium (progestin effect), disordered or dys
synchronous endometrium (implies irregular
shedding of the endometrium secondary to
unopposed estrogen), and endometritis
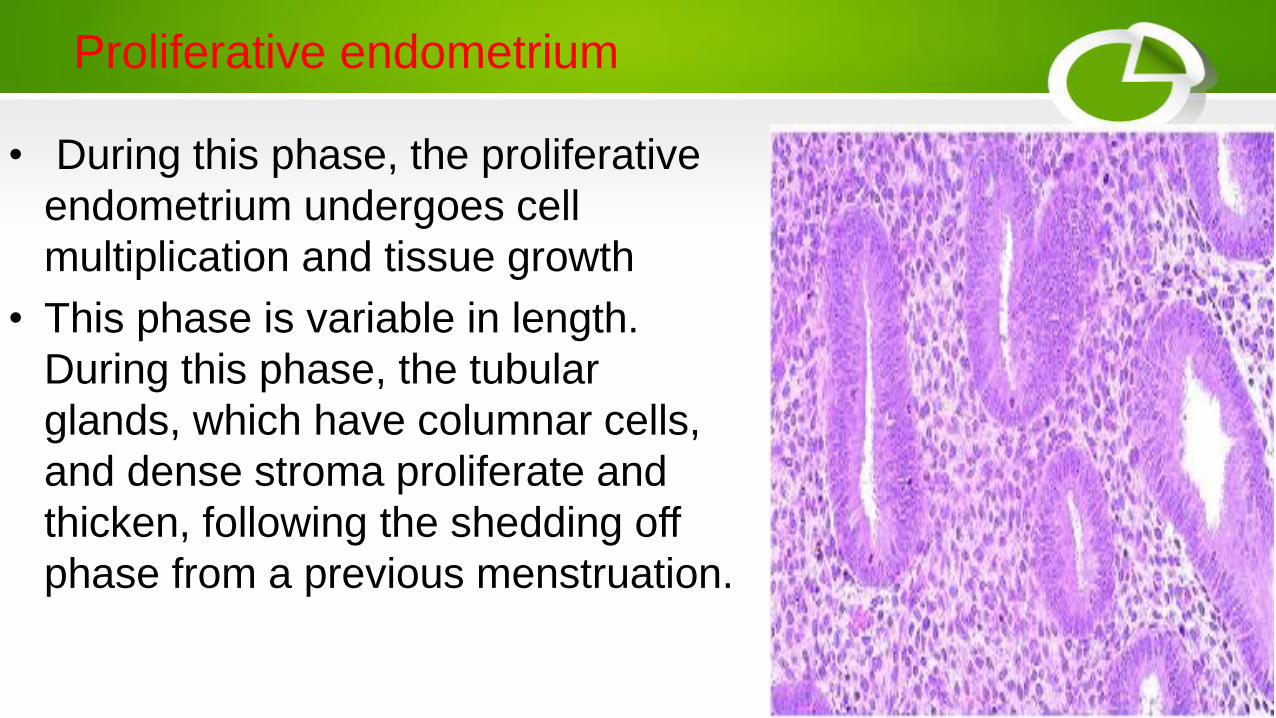
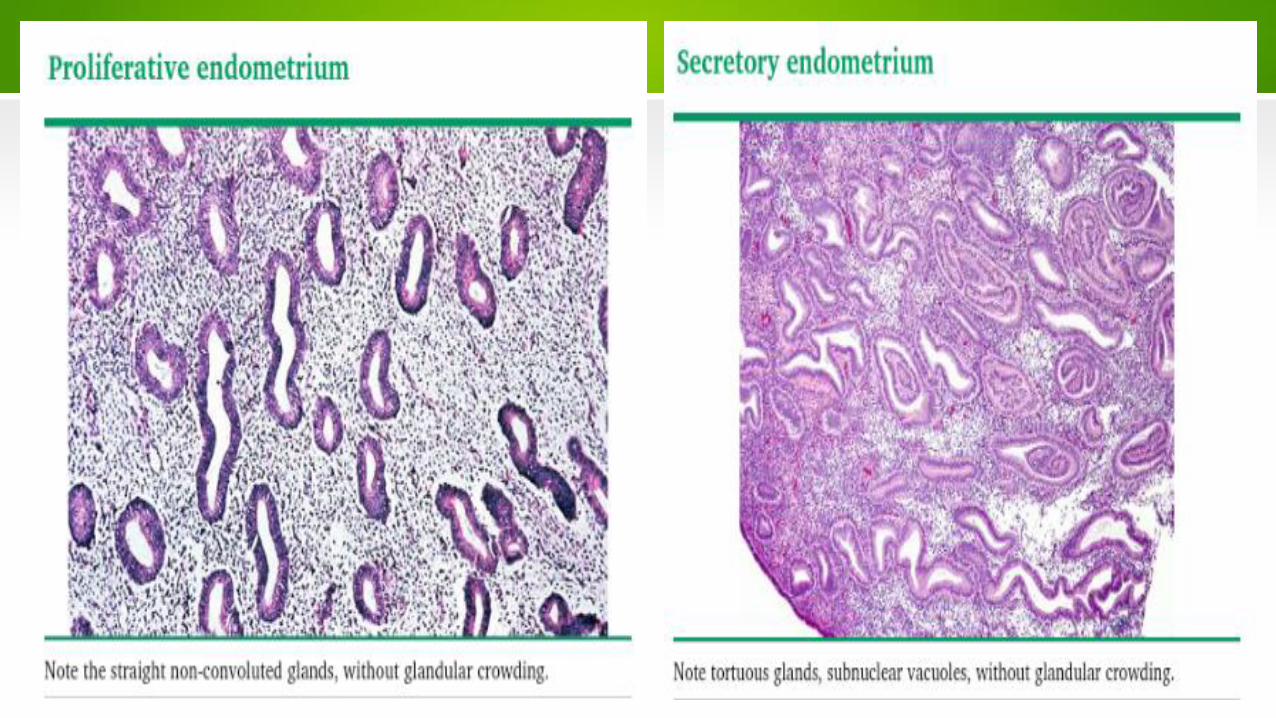
Proliferative endometrium
• During this phase, the proliferative
endometrium undergoes cell
multiplication and tissue growth
• This phase is variable in length.
During this phase, the tubular
glands, which have columnar cells,
and dense stroma proliferate and
thicken, following the shedding off
phase from a previous menstruation.

Secretory endometrium
• The secretory endometrium is a
stage of the menstrual cycle in which
a nearly mature endometrium has a
layer of grandular epithelium with
round nuclei, thickened endometrium
and curled uterine glands with
collections of glycogen within them.
This stage typically happens two days
after ovulation
• During the normal menstrual cycle, proliferative
endometrium is found during the follicular phase, and
secretory endometrium is found during the luteal phase.
Normal proliferative endometrium exhibits no crowding of
glands within the stroma (<50 percent ratio of glands to
stroma).
• Normal secretory endometrium may have >50 percent
gland to stroma ratio.
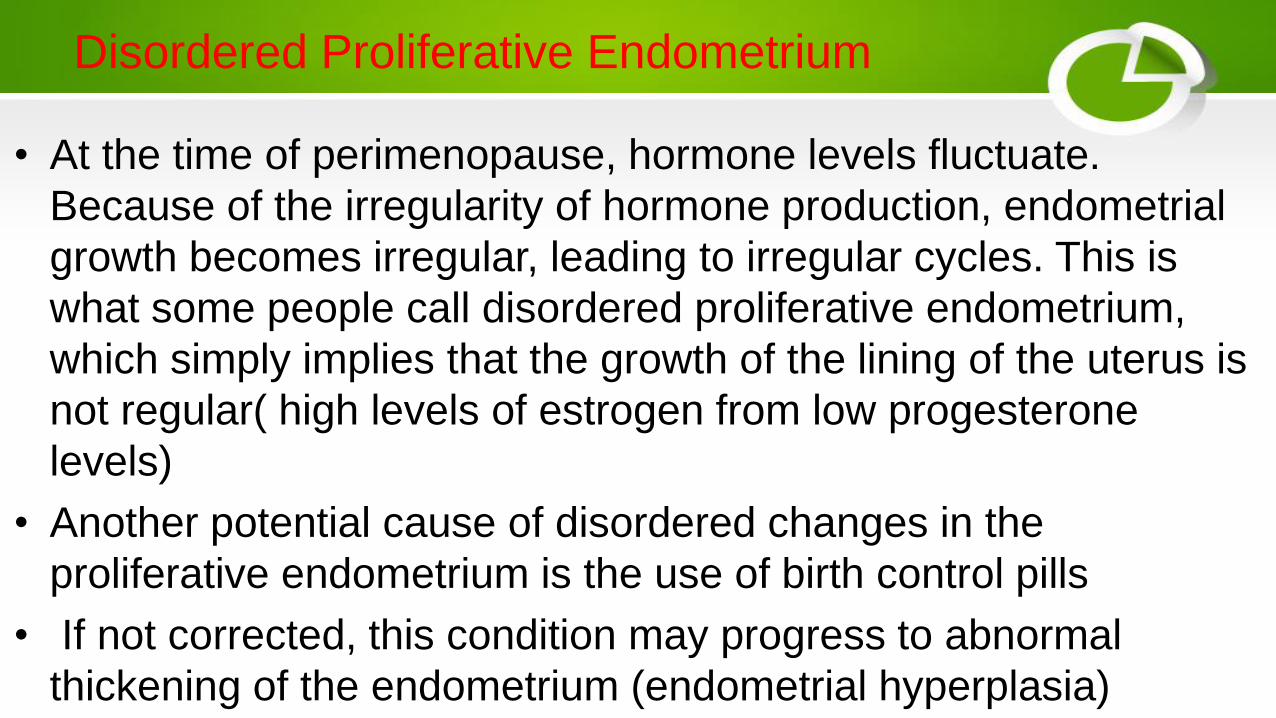
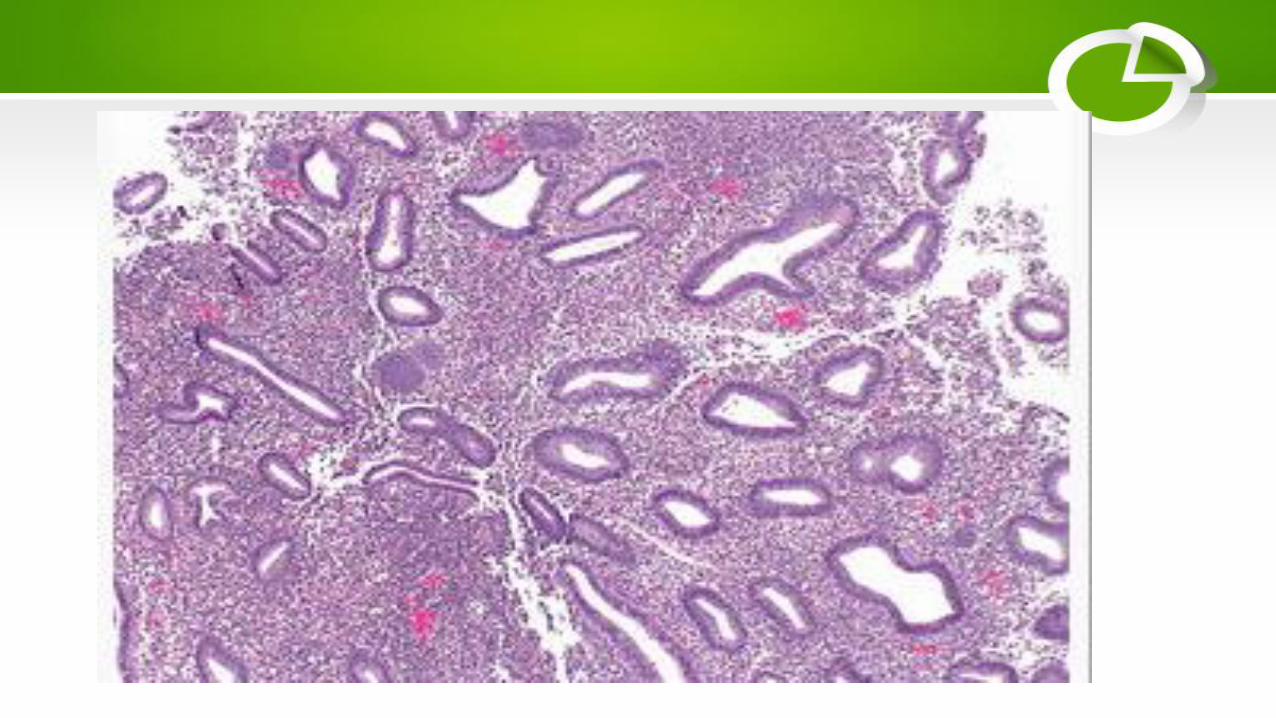
Disordered Proliferative Endometrium
• At the time of perimenopause, hormone levels fluctuate.
Because of the irregularity of hormone production, endometrial
growth becomes irregular, leading to irregular cycles. This is
what some people call disordered proliferative endometrium,
which simply implies that the growth of the lining of the uterus is
not regular( high levels of estrogen from low progesterone
levels)
• Another potential cause of disordered changes in the
proliferative endometrium is the use of birth control pills
• If not corrected, this condition may progress to abnormal
thickening of the endometrium (endometrial hyperplasia)

Treatment
The most common treatment for endometrial hyperplasia,
which occurs when there is proliferation of the
endometrium, is progestin therapy

Endometrial Hyperplasia

Endometrial hyperplasia is characterized by a
proliferation of endometrial glands of irregular
size and shape. Compared with proliferative
endometrium, there is an increase in the
endometrial gland to stroma ratio. Endometrial
hyperplasia virtually always results from chronic
estrogen stimulation unopposed by the counter
balancing effects of progesterone

• The WHO classification of endometria hyperplasia
• is based upon two features:
• The glandular/stromal architectural pattern of the endometrium,
which is described as either simple or complex
• The presence or absence of nuclear atypia
• This results in four possible categories of endometrial
hyperplasia:
• ●Simple hyperplasia without atypia
• ●Complex hyperplasia without atypia
• ●Simple atypical hyperplasia
• ●Complex atypical hyperplasia
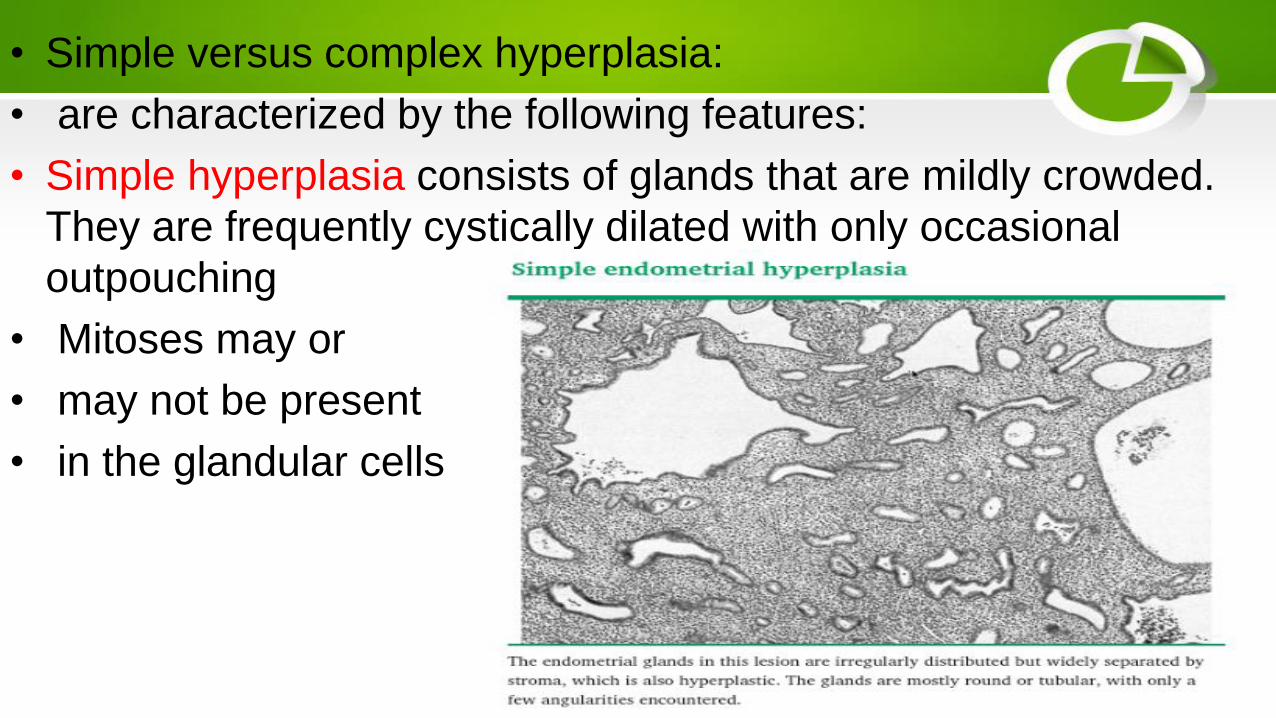
• Simple versus complex hyperplasia:
• are characterized by the following features:
• Simple hyperplasia consists of glands that are mildly crowded.
They are frequently cystically dilated with only occasional
outpouching
• Mitoses may or
• may not be present
• in the glandular cells

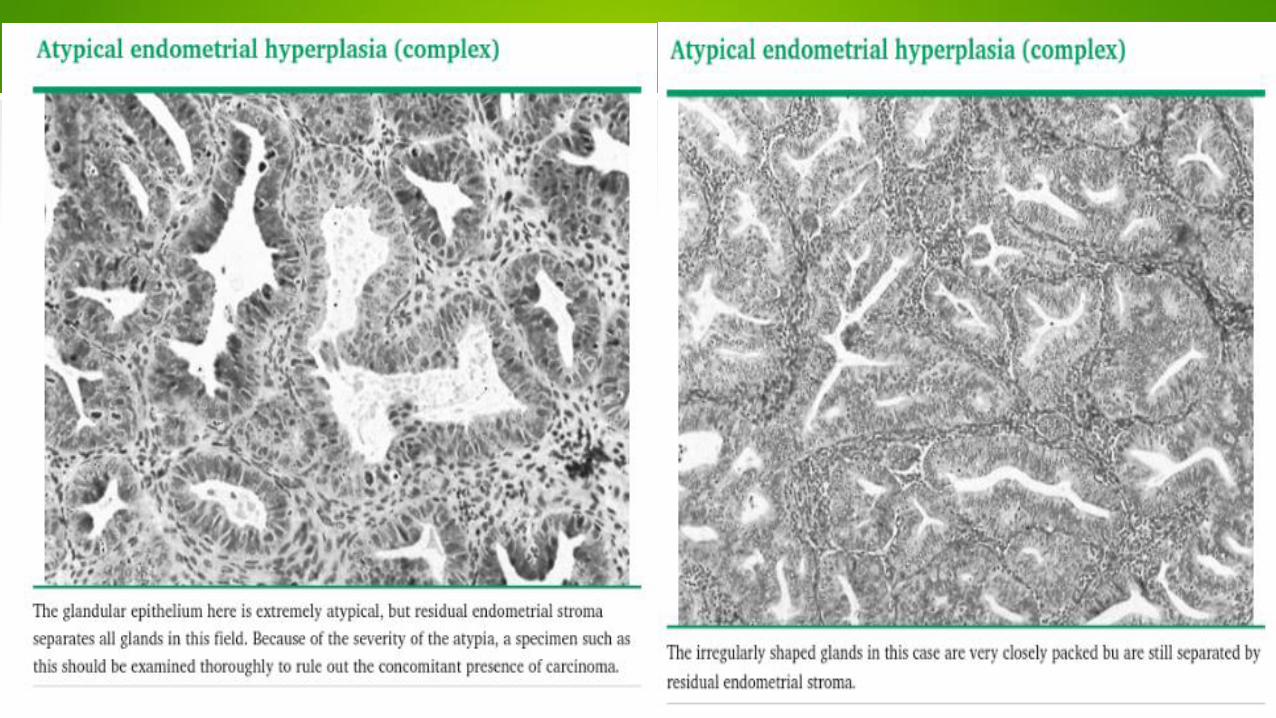
• Complex hyperplasia consists of glands that are crowded (>50
percent gland to stromal ratio)
• The glands appear disorganized and have luminal outpouching.
Mitoses are typically present

RISK FACTORS
• The risk factors for endometrial hyperplasia are the same as
those for endometrial carcinoma

CLINICAL PRESENTATION
• Endometrial hyperplasia typically presents with
abnormal uterine bleeding and is most common in
women who are postmenopausal, and with
increasing age in premenopausal women.
Occasionally, women with no abnormal uterine
bleeding present with abnormal findings on cervical
cytology.

DIAGNOSTIC EVALUATION
Women with a clinical presentation suspicious for
endometrial hyperplasia are evaluated initially with
physical examination.
Pelvic sonography may also be performed to
evaluate for other etiologies of abnormal uterine
bleeding or to assess endometrial thickness in
postmenopausal women.

DIAGNOSIS
• Endometrial hyperplasia is a histologic
diagnosis made based upon the results of
evaluation of an endometrial biopsy, curettage
sample, or hysterectomy specimen.

FURTHER EVALUATION AFTER ENDOMETRIAL SAMPLING
• Negative endometrial sampling
• Insufficient cells on endometrial biopsy :
• Women with an endometrial biopsy result that has insufficient
endometrial cells should have sampling repeated with an office
biopsy or dilation and curettage (D&C).
• If two office endometrial biopsies have been unsuccessful, a
D&C should be performed.
• Cervical stenosis, a common cause of an unsuccessful biopsy,
can be managed with preprocedure cervical preparation or
dilation.

Evaluation of the endometrium
• The Pipelle device was more sensitive for the detection of
endometrial cancer and atypical hyperplasia than all other
sampling devices.

• Hystroscopy
• its use should be reserved for women at low risk of endometrial
cancer, and in whom the value of hysteroscopic resection of a
lesion is clear
• Transvaginal ultrasound
• In women with postmenopausal bleeding and not on hormonal
replacement therapy, an endometrial thickness of less than or
equal to 4 or 5 mm is associated with a low risk of endometrial
disease

• Persistent bleeding is worrisome even when the
• endometrial thickness is <4 mm, particularly if there are other
risk factors for endometrial cancer .
• Endometrial cancer can still occur in this setting since serous
carcinoma of the endometrium may arise from atrophic
endometrium. Therefore, further diagnostic evaluation is
indicated.
• Asymptomatic women with endometrial thickening or fluid
• we suggest sampling the endometrium of postmenopausal
women without uterine bleeding who have an endometrial
thickness >11 mm

• If curettage D&C is performed as a follow-up to
• endometrial biopsy, if the results are atypical endometrial
hyperplasia or carcinoma, the patient is managed as
appropriate.
• If the results are less severe or negative, the patient should be
managed based upon the results of the initial sample.
• Persistent or recurrent bleeding — If bleeding persists or recurs
after endometrial sampling with benign findings, further
evaluation is required.
• reevaluate such cases after three to six months.

• Premenopausal women
• TVUS should be performed on day 4, 5, or 6 of the
bleeding cycle, when the endometrium is expected to be
its thinnest (in reproductive-age women, normal
endometrial thickness in the proliferative phase is 4 to 8
mm and in the secretory phase 8 to 14 mm
• In asymptomatic premenopausal women, endometrial thickness
alone is not an indication for biopsy.
• Endometrial evaluation should be based on a combination of
factors , including cervical cytology results showing glandular
abnormalities or endometrial cells, a chronic history of estrogen
excess or anovulation (polycystic ovary syndrome),
• Women on tamoxifen
• women should have an endometrial biopsy if any abnormal
bleeding occurs
MANAGEMENT
• The choice of treatment of endometrial hyperplasia is based primarily
upon two factors: 1) nuclear atypia, and 2) the desire for fertility.
• The presence or absence of nuclear atypia is the primary factor in
determining whether treatment is needed.
• Options for the management of endometrial hyperplasia include:
• ●Hysterectomy.
• ●Hormonal management – Progestins are the usual therapy, since
they oppose the effect of estrogen on the endometrium. In a minority
of cases, treatment includes removal of the intrinsic or extrinsic
source of unopposed estrogen (eg, an estrogen-producing neoplasm).
• ●Surveillance with serial endometrial sampling.

• HYPERPLASIA WITHOUT ATYPIA
• The risk of progression to endometrial cancer is low for hyperplasia without atypia (<1 to 3 percent)
• . The goal of treatment is to prevent progression to cancer in a small number of women and to control abnormal uterine bleeding.
• Medroxyprogesterone acetate (MPA) has typically been first-line therapy for non-atypical endometrial hyperplasia. However, other options include estrogen-progestin contraceptives or the levonorgestrel-releasing intrauterine device, 20 mcg/day (LNg20; Mirena).

• The LNg20 appears to be more effective than oral progestins
for the treatment of non-atypical endometrial hyperplasia.
• For women treated with MPA, we prescribe 10 mg daily for
three to six months. Most women find this continuous dosing
schedule more acceptable than a cyclic regimen because
they do not have cyclic vaginal bleeding during treatment.
• A cyclic regimen of MPA (eg, 10 mg daily for 12 to 14 days each
month) may also be used.
• Micronized progesterone (100 to 200 mg) in a vaginal cream – In
one study, use of this agent from the 10th to the 25th day of the
menstrual cycle for three to six months resulted in regression of
endometrial hyperplasia without atypia to normal endometrium
• If regression to normal endometrium does not occur after three
to six months, the progestin dose may be increased, or a
combination of a systemic progestin and the LNg20 may be
used.

• ATYPICAL HYPERPLASIA
• Hysterectomy is the treatment of choice for women with
endometrial hyperplasia with atypia who are not planning future
pregnancy.
• Progestin therapy is an option for women who wish to preserve
fertility or who cannot tolerate surgery.
• The recommendation for hysterectomy is based upon the high
risk endometrial cancer in women with atypical endometrial
hyperplasia. Many women with atypical endometrial hyperplasia
diagnosed with endometrial sampling are found to have
concurrent foci of endometrial cancer

• Supracervical hysterectomy is not a valid option for
• these patients, since the potential for local extension of
the endometrial neoplasia into the cervix outweighs any
purported benefits of this surgical approach.
• Postmenopausal women
• For postmenopausal women with atypical endometrial
hyperplasia, we suggest hysterectomy with concomitant
bilateral salpingo-oophorectomy (BSO) rather than
hysterectomy alone

• Women with atypical endometrial hyperplasia who desire
future childbearing or are not appropriate for surgery may
be treated with progestin therapy. These women must be
able to comply with medical therapy and follow-up
endometrial sampling.
• Megestrol acetate is typically the oral progestin used for
atypical hyperplasia
• We often treat patients in this population with oral
megestrol acetate 80 mg twice per day .
• This may be increased to 160 mg twice per day
• if there is no regression of the hyperplasia on
• follow-up endometrial sampling.
• Alternatively, a 20 mcg/day levonorgestrel-releasing intrauterine device
(LNg20; Mirena)
• Other options for progestin therapy have been described and include
• ●MPA (oral) 10 to 20 mg daily
• ●Depot medroxyprogesterone (intramuscular) 150 mg every three months
• ●Micronized progesterone (vaginal) 100 to 200 mg daily
• For patients on maintenance progestin therapy, we repeat an endometrial
biopsy every 6 to 12 months initially.

• Danazol
• Gonadotropin-releasing hormone (GnRH) agonists or
antagonists may be given to produce a
pseudomenopausal state
• Aromatase inhibitors

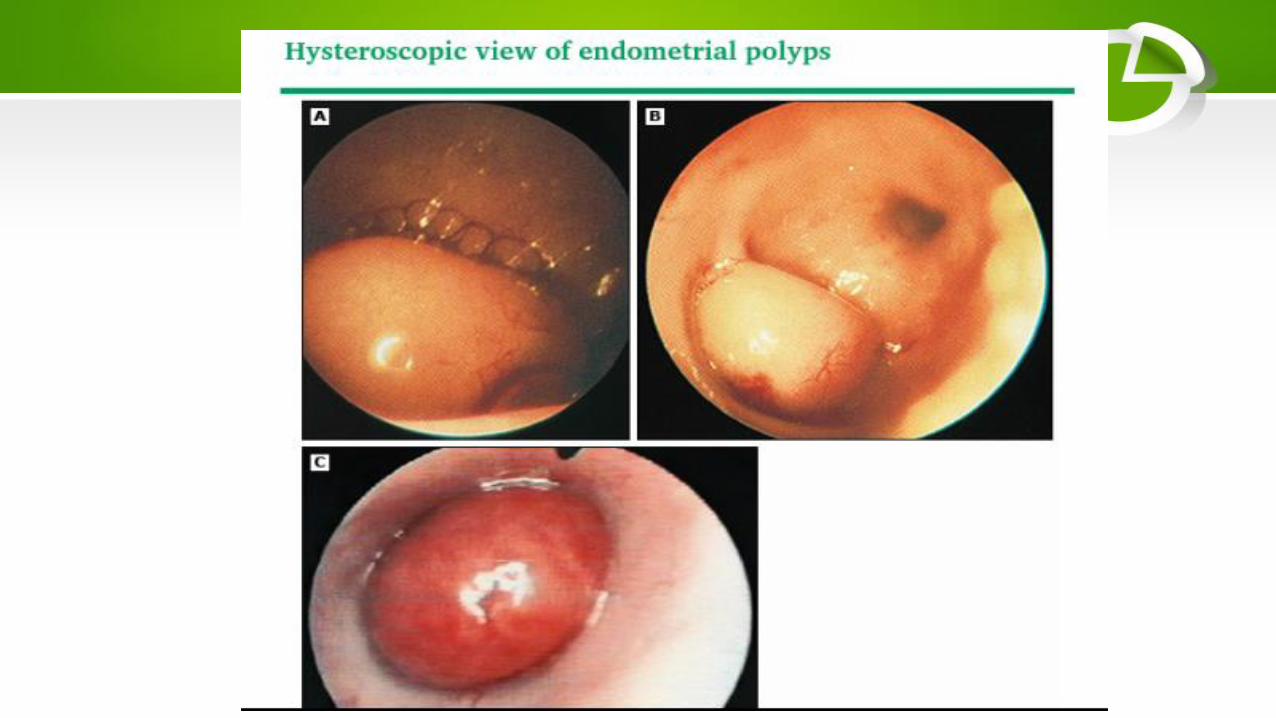
Endometrial polyp

• Endometrial polyps are one of the most common
etiologies of abnormal genital bleeding in both
premenopausal and postmenopausal women .
• They are hyperplastic overgrowths of endometrial
glands and stroma that form a projection from the
surface of the endometrium (lining of the uterus).
They may also be asymptomatic. The great majority
of endometrial polyps are benign, but malignancy
occurs in some women

• Polyps can develop anywhere in the uterine cavity.
• Most risk factors for endometrial polyps involve increased levels or
activity of endogenous or exogenous estrogen.
• Tamoxifen :Polyps in these women may be large (>2 cm), multiple,
or show molecular alterations
• Obesity:those with a BMI ≥30 had a significantly higher rate of
polyps than other women
• Hereditary nonpolyposis colorectal cancer
• CLINICAL PRESENTATION
• Abnormal uterine bleeding
• Intermenstrual bleeding is the most frequent symptom in
premenopausal women with endometrial polyps
• Postmenopausal bleeding is another common presentation
• Incidental finding on imaging or hysteroscopy
• Endometrial cells on cervical cytology
• Prolapsed polyp

• DIAGNOSTIC EVALUATION
• Pelvic ultrasound and hysteroscopy
• sonohysterography
• CLINICAL COURSE
• Continued growth or regression
• Risk of malignancy — Approximately 95 percent of endometrial polyps are benign .
• malignant or hyperplastic was significantly higher in postmenopausal compared with premenopausal women and those with bleeding compared to those without bleeding
• polyps greater than 1.5 cm in diameter
• Tamoxifen

• CHOOSING A MANAGEMENT APPROACH
• Symptomatic endometrial polyps should be removed in all
women
• For other asymptomatic women, we perform polypectomy if the
following characteristics are present:
• ●Polyp >1.5 cm in diameter
• ●Multiple polyps
• ●Polyp prolapsed through the cervix
• ●Infertility
• Postmenopausal women — For postmenopausal women, we
recommend removal of all endometrial polyps

• Thank you