bengal ophthalmic - oswb.org€¦ · joyeeta das original articles ... effect of age on adult...
TRANSCRIPT


Bengal Ophthalmic
Journal of Ophthalmological Society
of West Bengal
December 2017

Advertisement

Bengal Ophthalmic Journal
Contents
December 2017
Page No. EditorialPresident’s MessageReview ArticlesOCT & Vitreo- Retinal Interface 1Lalit Verma, Arindam Chakravarti
Retinoblastoma: Diagnosis and Management 9Raksha Rao, Santosh G Honavar
Topical Anti-allergic Drugs in Ophthalmology - An Update 14Anita Ganger, Aswini Behera, Rebika Dhiman, M Vanathi
OCT angiography- A revolutionary approach for retinal imaging 19Dhrubojyoti Sarker, Rajiv Kumar Gupta
Facial nerve palsy -an ophthalmologist perspective 26Joyeeta Das
Original ArticlesEpidemiology of benign eyelid lesions in patients presenting to a teaching hospital 32Sonai Mukherjee, Nidhi Priya, Sonu Goel
A retrospective study of Outcome of repeat DCR with silicone tube intubation in a tertiary care hospital 37Prantik Maity, Kalishankar Das, Nabanita Barua
Effect of Age on Adult Stereoacuity as Measured By Distance Randot Test- 40 A Comparision Between Stereoacuity in Pre-Presbyopic and Presbyopic Age GroupsSatabdi Nanda, Anuradha Chandra
Analysis of Hess Charts and its interpretations 45Chandra Anuradha
Short CommunicationsCase Reports
Meige’s Syndrome In A Middle Aged Woman: A Case Report 49Saumen Kumar Chaudhuri, Ramarghya Kusum Chakraborty
Apert’s syndrome with optic atrophy 51Nabanita Barua, Chandana Chakraborti
Intravitreal Dexamethasone implant (Ozurdex) with PRP for Adult’s Coats Disease 54Kshitiz Kumar, Pallavi Raj, Samar Sen Gupta, Amar Agarwal

Photo Essay
Xeroderma Pigmentosum 57Chandana Chakraborti
Photo Gallery 58
Subrata Mondal
Clippings
Sabyasachi Bandyopadhay 59Chandrima Paul 59Somdutt Prasad 60Tutul Chakraborti 60
Editorial Board
Chandana ChakrabortiEditor - in - chief
Chandni ChakrabortyAssociate Editor Nabanita BaruaManaging Editor
Assistant Editors Anuradha Chandra
Jaya Biswas Krittika Pal Chowdhury
Sabyasachi Bandyopadhyay Santanu Mandal Somdutt Prasad
National Advisory Board Debasish Bhattacharya
Namrata Sharma Partha Pratim Dutta Mazumder
Santosh HonavarM. Vanathi
Zia Chowdhury
Advisory Board Asit Ranjan Banerjee
Amitava Biswas Anita Banerjee
Asim ChakrabortyAsim Dey
Chandrima Paul Tutul Chakraborti

Name Designation
Dr. Pradeep Kumar Bakshi President
Dr. Ashim Kumar Dey President Elect
Dr. Parag Mukhopadhyay Vice – President
Dr. Subhasish Nag Hony. Secretary
Dr. Aniruddha Maiti Jt. Secretary
Dr. Siddhartha Ghosh Jt. Secretary
Dr Debashis Das Hony. Treasurer
Dr. Arnav Mitra Jt. Treasurer
Dr. Ajoy Paul Chairman Sc Comm
Dr. Chandana Chakraborti Editor Journal
Dr. Indranil Bhattacharyya Member
Dr. Kakali Sen Member
Dr. Kanchan Kumar Mondal Member
Dr. Rudra Kishore Deb Member
Dr. Rupak Kanti Biswas Member
Dr. Satyam Kumar Maiti Member
Dr. Sekhar Nath Sarkar Member
Dr. Suchanda Sar Member
Dr. Sugato Paul Member
Dr. Sunil Surana Member
Dr. Supratik Bandyopadhyay Member
Dr. Tathagata De Member
Dr. Monoj Hajra Imm. Past President
Dr. Ratish Ch. Paul Imm. Past Hony. Secretary
Office Bearers of OSWB

Editorial
Greetings from the editorial desk!
The job of the Chief Editor of any journal is not only interesting but challenging.
The annual issue of Bengal Ophthalmic Journal (BOJ) brings you a bouquet of a wide variety of articles from different subspecialities.
Currently we are publishing online quarterly news letter of OSWB “OPHTHABUZZ”, which has been tremendously appreciated from various corners.
Our aim is atleast biannual publication of BOJ as well as to make it an Index Journal, but that needs lot of financial support which is really a hurdle to survive for BOJ. Collecting good quality original article is a real challenge for a non-indexed journal like us. I must admit that we have to go a long way in the field of research activities, without which we cannot expect publication of a quality journal.
I take the opportunity to acknowledge and appreciate my predecessors to keep the journal alive inspite of all odds.
I would like to request our members once again to submit good quality original articles and case reports for publications in BOJ as well as OPHTHABUZZ.
I would like to thank our contributors for their submissions and also the members of editorial board for spending their time and providing valuable suggestions for the betterment of the Journal. I am grateful to all members of OSWB for encouraging our effort constantly.
Chandana ChakrabortiEditor, Bengal Ophthalmic Journal
MD (AIIMS), Associate Professor, Dept. of OphthalmologyNorth Bengal Medical College, Darjeeling
Email: cchakoptha@yahoo. com
Dear Colleagues,
Another eventful year in the calendar is coming to an end and we are looking forward to our 48th Annual Conference at ECO PARK, New Town, Rajarhat, on 16th and 17th of December 2017.
This year has seen lot of constructive events in the OSWB Scientific and Social calendar. We had the first successful Indo Bangladesh Conference at Dhaka in the month of October 27th and 28th, 2017. This has opened out a new platform of joint meeting between two Bengals after independence. We hope to continue similar meetings in the coming years thanks to our Secretary Dr. Subhashish Nag and past Secretary Dr. Ratish Paul, with their counter parts in Bangladesh.
The recent introduction of West Bengal Clinical Establishment Act 2017 has put all of us into stress in the present day practice. The new laws are going to effect the way we look and practice pattern has to be more transparent and law abiding. The capping of doctor’s fee and the operation charges is going to effect all of us, specially those with smaller eye centres for survival.
The new generation of doctors are going to face a very uphill task to overcome all these restrictions. They have to make collective effort and be united in taking a course of action against this.
I wish everyone of you a Happy New Year 2018. May God give us strength to face the odds in the years to come.
Yours sincerely,
P. K. BakshiPresident OSWB
President’s Message

Advertisement

Review Article1
OCT & Vitreo- Retinal Interface
Lalit Verma, MD, Director, Vitreo-retinal services, Centre for Sight, Apollo Hospital, New DelhiArindam Chakravarti, MD., Centre for Sight, New Delhi
Optical coherence tomography (OCT) is a valuable tool for assessment of the vitreoretinal interface. It became commercially available in 1996. In 2006, spectral domain or Fourier domain OCT systems became commercially available. These high resolution systems are upto 65 times faster and offer double the resolution of the older systems. (Fig 1) They can identify subtle changes in photoreceptor and retinal pigment epithelium(RPE) anatomy, image the vitreo-retinal interface and confirm the presence of small amounts of intra and subretinal fluid. Before the advent of OCT, study of V-R Interface was by the means of Slit Lamp Biomicroscopy and ophthalmoscopy. Early ERM
was usually missed or misdiagnosed. After OCT came into clinical use, study of V-R Interface has become easier and more objective. Previously undiagnosed entities are now more clearly understood leading to better management5,6. Additionally by scanning a larger section of the macula, OCT enables accurate and consistent evaluation of patients with poor fixation.
OCT Levels of Vitreo-retinal pathologies
It includes conditions like macular hole, epiretinal membrane, lamellar macular hole, vitreo-macular adhesion (VMA), vitreomacular traction (VMT)1-3.
Inner Retinal Pathologies involving the middle retina between ILM – ELM: Includes macular edema due to various causes.
Outer Retinal Pathologies between ELM- RPE: Includes diseases like dry ARMD, CNVM, RPE detachments, CSR and IPCV1, 2.
Posterior Vitreous Detachment(PVD) With Age & other factors like disease and trauma, vitreous liquefaction starts, there is weakening of adhesions between posterior cortical vitreous
& ILM which allows liquid vitreous to enter retrohyaloid space through prepapillary apertures or micro-leaks in cortical vitreous initiating PVD. This is compounded by the breakdown of the inner blood retinal layer. Leakage of serum proteins may lead to proliferation of macrophages and fibroblasts leading to membrane formation. PVD begins as a localised separation from perifoveal area and slowly progresses over months to years. It is completed with vitreo-papillary separation. This early stage of Perifoveal PVD is cause / stimulus for so called Idiopathic Macular disorders`. It acts as a stimulus for glial cell formation and release of inflammatory mediators leading to ERM formation4.
Fig 1: Retinal layers depicted in SD OCT
Corresponding AuthorLalit VermaDirector, Vitreo-retinal services, Centre for Sight, Apollo Hospital, New DelhiEmail: lalitverma@yahoo. com 0-9810299934
High resolution spectral OCT

Bengal Ophthalmic Journal2
Stages of PVD
Stage 1: Perifoveal PVD with residual vitreofoveal adhesion
Stage 2: Perifoveal PVD with no vitreofoveal adhesionStage 3: Near-Complete PVD with Vitreo-Papillary adhesion
remainingStage 4: Complete PVD
Vitreo-Macular Adhesion:
Vitreous is separated from the retina throughout the peripheral fundus but remains adherent in a broad, often dumbbell-shaped region encompassing the macular area and optic nerve. There is no traction on the retina7.
Vitreoretinal adhesion patterns (VAP):Focal VAP : There is an area of foveal or parafoveal attachment with surrounding partial PVD. Multifocal VAP: Multiple areas of adhesion are interspersed with areas of vitreous separation
VMA may be both asymptomatic or cause symptoms. Usually no Intervention is required.
Vitreo-Macular Traction (VMT)
VMT is a complication of partial PVD, vitreous is adherent in a broad, often dumbbell-shaped region encompassing the macular area leading to traction. A thickened hyaloid is present with visible points of traction.
fig.2

December 2017 Bengal Ophthalmic Journal 3
Vitrectomy is usually required in cases of symptomatic vitreomacular traction. However it is important to bear in mind that the OCT picture alone should not be considered as the sole guide for treatment. The patient’s best corrected visual acuity and degree of symptoms are more important criteria. Many patients may be asymptomatic despite the presence of vitreomacular traction on OCT.
There is controversy regarding the role of internal limiting membrane (ILM) peeling during vitrectomy for VMT. Many surgeons are advocating it as it is likely to eliminate the scaffold for future regrowth of membranes. However the pathology in VMT lies in the vitreous and not in the inner retina. It is the thickened posterior hyaloid which is responsible for the macular traction. Moreover, there is always the risk of causing accidental trauma in the macula or papillomacular bundle even with highly refined instruments like the diamond dusted scraper8, 9.
MACULAR HOLE OCT helps in the study of various traction forces leading to formation of macular hole, thus aiding in understanding the pathogenesis. It further helps in monitoring status of fellow eye. It can help in the differential diagnosis between pseudocysts, pseudoholes, and lamellar holes. Additionally OCT can help assess for the presence of vitreoschisis (residual cortical vitreous on the vitreous surface despite apparent posterior vitreous separation) and associated ERM13, 14 . 9-12.
OCT Classification of Macular Hole:
Stage IA: Characterised by foveal splitting (not detachment as proposed by Gass ), a pseudocystvisible on OCT in inner layers of retina. This stage may be missed clinically.
Stage IB: Characterized by pseudocyst enlargement and extension to the outer retina, roof intact.
Stage IIA: In keeping with the Gass classification < 400 μm full thickness macular hole with posterior hyaloid face remaining attached to roof of pseudocyst.
Stage IIB:<400 μm full thickness macular hole with operculum
Stage III: This is a fully developed hole with or without operculum. Size >400 μm with surrounding thickened retina including intraretinal cystoid spaces. In addition, the perifoveal and prefoveal hyaloid is separated.
Stage IV: Stage III hole with a complete PVD. OCT is often unable to visualize the posterior hyaloid as it is too anterior.
OCT helps in prognosis by measuring the Hole Form Factor (HFF), macular hole Index (MHI) and studying the integrity of ELM & IS/OS Junction.

Bengal Ophthalmic Journal4
HFF of > 0. 9 predicts a possibility of 80 % hole closure. HFF of < 0. 5 may indicate a closure possibility of approximately 25%. For better closure, base diameter has to be less and oblique height has to be more.
Hole closure patterns after macular hole surgery can be assessed by OCT. Kang classified closed macular hole into:
Type I closure: Closed macular hole with no neurosensory retinal defect.
Type II closure: Closed macular hole with neurosensory retinal defect.
Eckardt et al used a custom rigged platform that enabled them to obtain OCT images in face down post-opeartive patients. They found that 55% of FTMHs were closed on post operative day 1 and 76% were closed by post operative day 2. Once the hole was closed, post operative positioning was stopped. No holes reopened during this regimen. However post operative OCT does not resolve the debate as to whether face down positioning is needed at all, it may offer the option of reduced duration of positioning as against the conventional advice of minimum of 1 week.
Pseudohole is characterized by a steepened foveal pit with thickened edges, reduced foveal pit diameter and normal or slightly increased central foveal thickness.
Lamellar Macular Hole They are characterized by an irregular foveal contour, a break in the inner fovea, separation of the inner and outer foveal layers and the absence of a full-thickness defect with intact photoreceptors posterior to the area of dehiscence.
Stages Of Lamellar Macular Hole Formation
Lamellar holes cause minimal loss of central visual acuity. Surgical intervention is indicated only if there is vision loss or metamorphopsia. Garretson et al reported a series of successfully repaired lamellar macular holes.
Flowchart Showing Pathogenesis of Full Thickness Macular Hole From Lamellar Hole or Pseudohole

December 2017 Bengal Ophthalmic Journal 5
Epiretinal Membrane
Epiretinal membrane (ERM) is mostly of idiopathic origin. Secondary causes of ERM include retinal detachment, branch retinal vein occlusion, diabetic retinopathy, telangiectasis and retinal artery macroaneurysm.
OCT patterns of ERM
1. ERM with Focal attachment
2. Globally attached ERM: A visible separation between the ERM and neurosensory retina is not apparent and there is loss of normal foveal depression.
Adherent ERM may be associated with macular edema.
The posterior hyaloid produces a minimally reflective greenish
signal in OCT, while an ERM generates a much thicker and stronger reddish reflection. OCT has also been helpful in confirming the relationship between PVD and ERM.
Symptomatic patients with vision drop due to ERM may require vitrectomy with ERM removal. OCT serves as a pre-operative guide by documenting the various adhesion patterns of the ERM and its relation to the posterior vitreous. It can detect changes in the RPE choriocapillary complex which may have a adverse effect on visual improvement after surgery. Post operatively OCT is helpful in documented membrane removal, relief of traction and resolution of associated macular edema.
Enzymatic Vitreolysis: A New Dimension
Ocriplasmin (Jetrea, Thrombogenics) is a recombinant proteolytic enzyme used in MIVI-TRUST study. It acts against protein components at vitreoretinal interface like laminin, fibronectin, and collagen; thereby dissolving the protein matrix responsible for vitreomacular adhesion. Dose is 0. 1mL (0. 12 mg) in diluted solution. It is provided as a single use glass vial which contains 0. 5mg in 0. 2mL solution for intravitreal injection (2. 5mg/mL). The drug is approved by the FDA for symptomatic VMA8.
Intraoperative OCT: A role in the future?
The possibility of intra-operative real time high resolution OCT images during macular surgery is an exciting but yet undefined prospect. Several reports using a handheld or microscope mounted SD OCT device intraoperatively have been published. Research is ongoing to create easily operated real time intraoperative OCT with useful displays.
Cases 1 45 years male with full thickness macular hole in RE with BCVA of FC 3 metres underwent vitrectomy + BBG assisted ILM peeling +C3F8.

Bengal Ophthalmic Journal6
FU 4 wk shows Type 2 macular hole closure with BCVA 6/18.
Case 2 70 years male presented with complaints of diminished vision(6/36) and metamorphopsia (LE). OCT shows extensive partly adherent ERM with macular thickening.
Patient underwent Vitrectomy +ERM removal. Post-op BCVA 6/18 with OCT showing decrease in the macular thickening and resolution of the ERM.

December 2017 Bengal Ophthalmic Journal 7
References:
1. S. R. Freeman, I. Kozak, L. Cheng, et al. Optical coherence tomography-raster scanning and manual segmentation in determining drusen volume in age-related macular degeneration Retina, 30 (3) (2010), pp. 431-435.
2. Sebag J, Wang MY, Nguyen D, Sadun AA. Vitreopapillary adhesion in macular diseases. Trans Am Ophthalmol Soc. 2009;107:35–44. [PubMed]
3. Forte R, Cennamo G, Pascotto F, de Crecchio G. En face optical coherence tomography of the posterior pole in high myopia. Am J Ophthalmol. 2008;145:281–8. [PubMed]
4. Ohno-Matsui K, Hayashi K, Tokoro T, Mochizuki M. Detection of paravascular retinal cysts before using OCT in a highly myopic patient. Graefes Arch Clin Exp Ophthalmol. 2006;244:642–4. [PubMed]
5. Linton KL, Klein BE, Klein R. The validity of self-reported and surrogate-reported cataract and age-related macular degeneration in the Beaver Dam Eye Study. Am J Epidemiol. 1991;134:1438–46. [PubMed]
6. Early Treatment Diabetic Retinopathy Study Research Group. Grading diabetic retinopathy from stereoscopic color fundus photographs: an extension of the modified Airlie House classification. ETDRS report number 10. Ophthalmology. 1991;98:786–806. [PubMed]
7. Duker JS, Kaiser PK, Binder S, et al. The International Vitreomacular Traction Study Group classification of vitreomacular adhesion, traction, and macular hole. Ophthalmology. 2013;120:2611–9. [PubMed]
8. Stalmans P, Benz MS, Gandorfer A, et al. Enzymatic vitreolysis with ocriplasmin for vitreomacular traction and macular holes. N Engl J Med. 2012;367:606–15. [PubMed]
9. Sigler EJ. Microcysts in the inner nuclear layer, a nonspecific SD-OCT sign of cystoid macular edema. Invest Ophthalmol Vis Sci. 2014;55:3282–4. [PubMed]
10. Duan XR, Liang YB, Friedman DS, et al. Prevalence and associations of epiretinal membranes in a rural Chinese adult population: the Handan Eye Study. Invest Ophthalmol Vis Sci. 2009;50:2018–23. [PubMed]
11. Chuo JY, Lee TY, Hollands H, et al. Risk factors for posterior vitreous detachment: a case-control study. Am J Ophthalmol. 2006;142:931–7. [PubMed]
12. Witkin AJ, Ko TH, Fujimoto JG, et al. Redefining lamellar holes and the vitreomacular interface: an ultrahigh-resolution optical coherence tomography study. Ophthalmology. 2006;113:388–97. [PubMed]
13. Sato H, Kawasaki R, Yamashita H. Observation of idiopathic full-thickness macular hole closure in early postoperative period as evaluated by optical coherence tomography. Am J Ophthalmol. 2003;136:185–7. [PubMed]
14. Chen JC, Lee LR. Clinical spectrum of lamellar macular defects including pseudoholes and pseudocysts defined by optical coherence tomography. Br J Ophthalmol. 2008;92:1342–6PMC free articlePubMed
Conflicts of Interest- None Financial disclosures- None

Review Article
Abstract: Retinoblastoma is the most common intraocular malignancy of childhood. The treatment of retinoblastoma is multimodal. Since the introduction of intravenous chemotherapy in the mid-90’s, it has been the most extensively used eye-saving modality of treatment. Periocular and intravitreal chemotherapy have emerged as treatment for recurrent seeds in retinoblastoma. Intra-arterial chemotherapy is promising alternative for advanced and refractory retinoblastoma. Radiation in the form of external beam radiotherapy and plaque radiotherapy are also use in refractory retinoblastoma. Enucleation still continues to play a role in advanced cases in eyes with no useful vision. The management of retinoblastoma is thus aimed at not only to save life, but also to preserve eye, and optimize residual vision.
Retinoblastoma: Diagnosis and Management
Raksha Rao, MS, Consultant, Orbit, Oculoplasty and Ocular Oncology, Chaithanya Eye Hospital and Research Institute, Trivandrum
Santosh G Honavar, MD, FACS, National Retinoblastoma Foundation, Ocular Oncology Service, Centre for Sight, Banjara Hills, Hyderabad, India
Corresponding AuthorSantosh G Honavar, MD, FACS Director, Ocular Oncology ServiceNational Retinoblastoma FoundationCentre for SightAshoka Capitol, Road No 2, Banjara HillsHyderabad 500034, IndiaTel: +91-98483-04001Email: santosh. honavar@gmail. com
Retinoblastoma is an ocular malignancy with a well-established genetic mutation. RB1 is a tumor suppressor gene, implicated in the genesis of retinoblastoma, that is located in the long arm of chromosome 13 (13q). Heritable retinoblastoma constitutes 30-40% of all retinoblastomas, while the rest 60-70% are non-heritable. In heritable retinoblastoma, the mutation is present in the germ cell which is carried in every cell in the body, making the patients prone for, apart from retinoblastoma, other second cancers (most commonly pinealoblastoma, osteosarcoma and soft tissue sarcomas)1. The incidence of retinoblastoma is 1 in every 15000 to 18000 live births. 2 There are an estimated 5000 new cases worldwide annually, with India alone contributing to 1500-2000 cases.
Clinical Features
Retinoblastoma is usually diagnosed at an average age of 18 months, with 95% of children diagnosed by 5 years of age. Germline retinoblastomas can present as early as first month and sporadic retinoblastomas are detected at an average age of 24 months2. Retinoblastoma can be unilateral or bilateral. The most common presenting symptom and sign is leukocoria, and strabismus is the second most common sign. The other common clinical features are as listed in Table 1.
A child with a suspicious retinoblastoma is best examined under anesthesia for a detailed fundus evaluation. Retinoblastoma typically manifests as a unifocal or multifocal, well-
Table 1: Clinical features of RetinoblastomaLeukocoriaStrabismusPoor visionRed painful eyeVitreous hemorrhagePhthisis bulbiSterile orbital cellulitisProptosis
Figure 1: Clinical presentation of retinoblastoma (A) Exophytic growth pattern with diffuse subretinal fluid (B) Endophytic growth pattern with diffuse vitreous seeds (C) Advanced retinoblastoma with neovascular glaucoma (D) Advanced retinoblastoma presenting as sterile orbital cellulitis

December 2017 Bengal Ophthalmic Journal 9
circumscribed, dome-shaped retinal mass with dilated retinal vessels. Although initially transparent and difficult to visualize, it grows to become opaque and white. In the exophytic growth pattern, the tumor causes diffuse retinal detachment (Figure 1A), and is frequently associated with small subretinal seeds. In contrast, an endophytic retinoblastoma progressively fills the vitreous cavity to cause vitreous seeding (Figure 1B). At times, the tumor maybe a combination of these two growth patterns. Diffuse infiltrating retinoblastoma is a rare pattern of presentation where there is no obvious mass, only a flat retinal infiltration, and is acalcific. It is generally seen in older children, and the incidence is less than 2%.
Patients with advanced tumor can have anterior extension of the tumor with anterior chamber cells, neovascularization of iris and glaucoma (Figure 1C), or an orbital cellulitis-like picture (Figure 1D). Retinoblastoma which has extended outside the confines of the eye is known as orbital retinoblastoma and this can occur when the tumor invades either the optic nerve, or full thickness of the sclera and beyond, and the patient generally presents with proptosis.
Grouping and Staging
The grouping system is for retinoblastomas confined to the eye, where eye salvage is the end point, whereas the staging system is for predicting survival in patients with retinoblastoma. International Classification of Retinoblastoma (ICRB) was devised in 2003 and includes both grouping and staging3. The grouping is based on the tumor size, location, severity and presence of subretinal and vitreous seeds (Table 2).
Table 2: International Classification of Retinoblastoma Grouping:Group A: Small tumor Retinoblastoma ≤3 mm in sizeGroup B: Larger tumor Rb >3 mm,
Macular location (≤3 mm to fo-veola), Juxtapapillary location (≤1. 5 mm to disc)Clear subretinal fluid ≤3 mm from margin
Group C: Focal seeds Subretinal seeds ≤3 mm from reti-nal tumorVitreous seeds ≤3 mm from retinal tumorSubretinal & Vitreous seeds ≤3 mm from retinal tumor
Group D: Diffuse seeds
Subretinal seeds >3 mm from reti-nal tumor Vitreous seeds > 3 mm from retinal tumorSubretinal & Vitreous seeds >3 mm from retinal tumor
Group E: Extensive retinoblastoma
Rb occupying 50% globe Neovas-cular glaucoma, Opaque media (from hemorrhage in anterior chamber, vitreous, or subretinal space)Invasion of postlaminar optic nerve, choroid (2 mm), sclera, orbit, ante-rior chamber
Staging:Stage 0 Unilateral or bilateral
retinoblastoma and no nucleationStage I Enucleation with complete histo-
logical resectionStage II Enucleation with microscopic tumor
residual (anterior chamber, choroid, optic nerve, sclera)
Stage III Regional extensionA. Overt orbital diseaseB. Preauricular or cervical lymph node extension
Stage IV Metastatic diseaseA. Hematogenous metastasis1. Single lesion2. Multiple lesionsB. CNS extension1. Prechiasmatic lesiom2. CNS mass3. Leptomeningeal disease
Figure 2: Standard-dose chemotherapy in retinoblastoma (A) A group B eye (B) After 6 cycles of standard-dose chemotherapy (C) A group C eye with focal vitreous seeds (D) After 6 cycles of standard-dose chemotherapy

Bengal Ophthalmic Journal10
Management
The management of a child with retinoblastoma is aimed at achieving the three sequential goals of life salvage, eye salvage, and optimal vision. The management involves the identification of the tumor group and stage, decision-making regarding the appropriate therapeutic measure, and meticulous follow-up for monitoring the treatment progress and detection of any recurrence.
Imaging
While the diagnosis of retinoblastoma is mostly clinical, ancillary tests like ultrasonography, fluorescein angiography (FA), optical coherence tomography (OCT), computed tomography (CT) and magnetic resonance imaging (MRI) aid in the documentation of the disease and differentiation of pseudoretinoblastomas from retinoblastoma. CT scan also helps diagnose extraocular extension, while MRI is most appropriate to detect optic nerve invasion and to screen for pinealoblastoma in heritable retinoblastoma.
Intravenous Chemotherapy
Currently, IVC is the most widely used treatment in India (Table 3). Used as a combination triple drug therapy of vincristine, etoposide and carboplatin, chemotherapy with focal consolidation achieves excellent success rates in the primary management of retinoblastoma. Chemotherapy alone can achieve an impressive tumor control in less advanced cases, with success rates of 100%, 93% and 90% in ICRB groups A, B and C, respectively (Figures 2A-D)4, 5, 6. Rates of regression
of retinoblastoma and eye salvage with standard triple-drug chemotherapy have been suboptimal for ICRB group D and E tumors.
Periocular injection of carboplatin or topotecan injection results in higher intravitreal drug level. Transscleral penetration of posterior sub-Tenon carboplatin leads to augmented vitreous concentration. High-dose chemotherapy with concurrent periocular chemotherapy can lead to higher eye salvage in group D and E eyes.
Intra-arterial Chemotherapy
Suzuki & Kaneko described the technique of ‘selective ophthalmic artery infusion’ (SOAI) of the chemotherapeutic drugs in 2004 by the balloon technique. In 2006, Abramson and Gobin pioneered direct intra-arterial (ophthalmic artery) infusion or superselective intra-arterial chemotherapy or “chemosurgery”7. The decision to treat with IAC is undertaken in consultation with an ocular oncology team, an endovascular neurosurgeon and a paediatric oncologist. The procedure is performed under general anesthesia using a sterile technique (Figures 3A-D). Through a transfemoral approach, the ipsilateral internal carotid artery is catheterized with a 4F pediatric guide catheter. The arterial anatomy is visualized with serial angiography runs, and the ostium of the ophthalmic artery is superselectively catheterized. Each chemotherapy dose is administered in a pulsatile fashion over 30 minutes.
IAC has emerged as an effective treatment for advanced retinoblastoma. It is increasingly being used in tumors as a primary treatment, especially in unilateral retinoblastoma. It can be used as a secondary therapy for those cases which have recurred or have not responded adequately to IVC. Shields et al observed 94% globe salvage in group D eyes8, 9. IAC also seems to be more effective in eyes that have failed to respond to previous therapies.
Intravitreal Chemotherapy
Vitreous seeds are aggregates of tumor cells found in the avascular vitreous, which are relatively resistant to the effect of intravenous chemotherapy due to lack of blood supply. Intravitreal chemotherapy (IVitC) provides a high concentration of the chemotherapeutic drug in the vitreous. Melphalan is now the most extensively used drug to control the vitreous disease in retinoblastoma by a potentially safe technique to perform intravitreal injections to prevent extraocular extension of the tumor (Figure 4A-D)10. The authors have used topotecan in achieving vitreous seed regression in 36 eyes.
Radiation Therapy
Retinoblastoma is a highly radiosensitive tumor, and radiation therapy can be curative. Radiation in the form of EBRT was the
Figure 3: Intra-arterial chemotherapy: Procedure in the cath lab (A) Patient under general anesthesia with a transfemoral cathether (B) An angiography performed at the beginning of the procedure, showing a patent internal carotid artery (C) An angiography performed with the microcatheter at the ostium of the ophthalmic artery, showing a patent ophthalmic artery (D) Infusion of the chemotherapeutic drug through the transfemoral cathether

December 2017 Bengal Ophthalmic Journal 11
most popular globe-salvage therapy in retinoblastoma before the introduction of chemotherapy in 1990s. Although it is no longer the primary modality of treatment for retinoblastoma due to
Figure 4: Intravitreal chemotherapy: Safety-enhanced technique (A) Pars plana intravitreal injection of topotecan at a dose of 30 μg in 0. 15 ml with a 30-gauge needle (B) Needle is withdrawn through the first ice ball of the cryotherapy (C) Triple freeze-thaw cryotherapy at the injection site (D) Forceps-assisted jiggling of the eyeball following the injection for an even dispersion of the chemotherapeutic drug
Figure 5: Multimodal management in orbital retinoblastoma (A) External photograph of primary orbital retinoblastoma taken during examination under anesthesia (B) Axial computed tomography image displaying extraocular extension of the intraocular tumor (C) After 12 cycles of doses of high-dose chemotherapy, external beam radiotherapy and enucleation (D) Healthy child cured of orbital retinoblastoma, with a well-fitting prosthesis
the associated complications, it is used as a part of multimodal treatment for advanced retinoblastoma.
Episcleral plaque radiotherapy is a form of brachytherapy wherein the source of radiation is placed on the episclera adjacent to the tumor, and the tumor absorbs radiation, sparing other healthy ocular tissues from the ill-effects of radiation. 11 Radioisotopes like Iodine-125 and Ruthenium-106 that emit radiation are used for the treatment of small recurrent retinoblastoma.
Focal Therapy
The use of cryotherapy, TTT, and laser therapy in the treatment of retinoblastoma is for consolidation of the tumor, once it attains a considerably lower volume after chemoreduction. Transscleral cryotherapy involves freezing the tumor under visualization using indirect ophthalmoscopy. In TTT, the hyperthermia generated by infrared radiation at subphotocoagulation levels destroys the tumor. Photocoagulation using argon green laser (532 nm) delivered with an indirect laser delivery system causes tumor apoptosis.
Table 3: Intravenous ChemotherapyProcedure:IVC when given as a primary treatment for retinoblastoma causes reduction in tumor volume, and this is known as chemoreduction (CRD). Most commonly, a combination of three drugs of standard dose (SD) is used, although high dose (HD) may be necessary in advanced cases or tumors not responding to SD. Drugs:Triple drug combination therapy of vincristine, etoposide and carboplatin (VEC) is employed, generally given 4 weekly for 6 cycles. Day 1: Vincristine + Etoposide + Carboplatin Day 2: Etoposide Drug SD-VEC (≥3
years of age)SD-VEC (< 3 years of age)
HD-VEC
Vincristine*EtoposideCarboplatin
1. 5 mg/m2 150 mg/m2 560 mg/m2
0. 05 mg/kg 5 mg/kg 18. 6 mg/kg
0. 025 mg/Kg12 mg/Kg28 mg/Kg
*maximum dose < 2 mgIndications:(1) Primary tumor (2) Recurrent tumor (3) Recurrent sub-retinal seeds (4) As adjuvant therapy in post-enucleation patients with high-risk features (discussed elsewhere) (5) Orbital retinoblastoma (6) As palliative therapy in metastatic retinoblastoma
Advantages:(1) Long-term tumor control (2) Reduces incidence of pineal-oblastoma (3) Reduces incidence of second cancers (4) Reduces incidence of systemic metastasisDisadvantages:(1) Systemic side-effects including thrombocytopenia, leu-copenia and anemia (2) Allergic reactions to carboplatin and etoposide (3) Long-term effects include hearing loss, renal toxicity and secondary leukemia

Bengal Ophthalmic Journal12
Enucleation
Enucleation is the oldest form of treatment for retinoblastoma, and is still indicated in advanced cases. Unilateral disease with no salvageable vision is best treated by enucleation and the patient can be cured of the disease for life. Enucleation is a simple procedure, although special precautions need to be taken when handling an eye with retinoblastoma to avoid accidental perforation that can potentially cause orbital seeding of the tumor.
An enucleated eyeball is always submitted for pathology to assess for high risk factors (HRF). In a landmark paper by Honavar et al, the need for adjuvant chemotherapy has been emphasized to reduce the risk of secondary orbital recurrence and systemic metastasis12. The incidence of metastasis was 4% in those who received adjuvant therapy, compared with 24% in those who did not. Hence when HRF is positive, adjuvant treatment with chemotherapy and/ or EBRT is indicated (Table 4). Adjuvant chemotherapy consists of a combination of vincristine, etoposide and carboplatin given 4-weekly for 6 cycles12.
Orbital Retinoblastoma
Orbital retinoblastoma is an advanced form of retinoblastoma seen mostly in developing countries of Asia and Africa. The incidence varies among different countries, and is in the range of 18-40%13. The presence of orbital disease is generally known to carry a poor prognosis. Orbital disease increases the risk of systemic metastasis by 10-27 times and the mortality rates range from 25 to 100%13. However, with an intensive multimodal management and careful monitoring, patients with orbital disease are known to do well (Figures 5A-D).
Prenatal Genetics
To prevent transmission of the disease from parents to offspring, genetic testing for germline mutations can be done at specialized laboratories. RB1 is the only gene that is implicated in retinoblastoma. Peripheral blood lymphocytes or tumor tissue, when available, are sampled for the detection of the mutation. Preimplantation genetic testing for carriers of mutation involves the identification of RB1 mutation in a blastomere (8-cell embryo) which is obtained by in vitro fertilization (IVF) technique. The small material is amplified by polymerase chain reaction (PCR) and the blastomere without the RB1 mutation maybe implanted for a successful pregnancy.
In conclusion, the management of retinoblastoma revolves around having a sound knowledge of the disease, choosing the best treatment for the patient among the various available options and careful monitoring for recurrences. Retinoblastoma has a very high cure rate, and is best managed in an integrated retinoblastoma clinic under the watchful monitoring of an expert ocular oncologist.
References:
1. Nichols KE, Walther S, Chao E, Shields C, Ganguly A. Recent advances in retinoblastoma genetic research. Curr Opin Ophthalmol 2009;20(5):351-5.
2. Shields J, Shields C: Retinoblastoma: introduction, genetics, clinical features, classification. In Shields J, Shields C, Atlas of intraocular tumors, 3ed. Philadelphia, PA: Lippinoctt, Wolters Kluwer; 2016.
3. Chantada G, Doz F, Antoneli CB, Grundy R, Clare Stannard FF, Dunkel IJ, Grabowski E, Leal-Leal C, Rodríguez-Galindo C, Schvartzman E, Popovic MB, Kremens B, Meadows AT, Zucker JM. A proposal for an international retinoblastoma staging system. Pediatr Blood Cancer 2006; 47: 801-5.
4. Shields CL, Mashayekhi A, Au AK, Czyz C, Leahey A, Meadows AT, Shields JA. The International Classification of Retinoblastoma predicts chemoreduction success. Ophthalmology 2006;113:2276-80.
5. Shields CL, Fulco EM, Arias JD, Alarcon C, Pellegrini M, Rishi P, Kaliki S, Bianciotto CG, Shields JA. Retinoblastoma frontiers with intravenous, intra-arterial, periocular, and intravitreal chemotherapy. Eye 2012;27:253–264.
6. Shields CL, Shields JA. Retinoblastoma management: advances in enucleation, intravenous chemoreduction, and intra-arterial chemotherapy. Curr Opin Ophthalmol 2010;21:203–212.
Table 4: High-Risk Features in RetinoblastomaHigh Risk Features on pathology where adjuvant therapy is indicated• Anterior segment invasion• Ciliary body infiltration• Massive choroidal invasion (invasion ≥ 3 mm in basal
diameter or thickness)• Full thickness scleral extension• Extrascleral extension• Retrolaminar optic nerve invasion• Optic nerve invasion at line of transection• Combination of optic nerve infiltration till any level (pre-
laminar/ laminar/ retrolaminar) and choroidal infiltration (any thickness)

December 2017 Bengal Ophthalmic Journal 13
7. Abramson DH, Marr BP, Dunkel IJ, Brodie S, Zabor EC, Driscoll SJ, Gobin YP. Intra-arterial chemotherapy for retinoblastoma in eyes with vitreous and/or subretinal seeding: 2-year results. Br J Ophthalmol 2012;96(4):499-502.
8. Shields CL, Jorge R, Say EA, Magrath G, Alset A, Caywood E, Leahey AM, Jabbour P, Shields JA. Unilateral retinoblastoma managed with intravenous chemotherapy versus intra-arterial chemotherapy: outcomes based on the international classification of retinoblastoma. Asia Pac J Ophthalmol 2016;5(2):97-103.
9. Shields CL, Kaliki S, Al-Dahmash S, Rojanaporn D, Leahey A, Griffin G, Jabbour P, Shields JA. Management of advanced retinoblastoma with intravenous chemotherapy then intra-arterial chemotherapy as alternative to enucleation. Retina 2013;33(10):2103-9.
10. Munier FL, Soliman S, Moulin AP, Gaillard MC, Balmer A, Beck-Popovic M. Profiling safety of intravitreal
injections for retinoblastoma using an anti-reflux procedure and sterilisation of the needle track. Br J Ophthalmol 2012;96(8):1084-1087.
11. Shields CL, Shields JA, Cater J, Othmane I, Singh AD, Micaily B. Plaque radiotherapy for retinoblastoma: long-term tumor control and treatment complications in 208 tumors. Ophthalmology 2001;108(11):2116-21.
12. Honavar SG, Singh AD, Shields CL, Demirci H, Smith AF, Shields JA. Post-enucleation prophylactic chemotherapy in high-risk retinoblastoma. Arch Ophthalmol 2002;120:923-31.
13. Honavar SG. Orbital retinoblastoma. In Singh AD, Murphee LA, Damato BE. Clinical Ophthalmic Oncology-Retinoblastoma, 2ed. NY: Springer; 2015.
Conflicts of Interest- None Financial disclosures- None
With Best Compliments From :--
SUNWAYS ( INDIA ) PVT. LTD
MUMBAI
Advertisement

Review Article
Various types of allergic conjunctivitis are mediated by Type I and Type IV hypersensitivity reactions. Seasonal allergic conjunctivitis (SAC), perennial allergic conjunctivitis (PAC), vernal keratoconjunctivitis (VKC), atopic keratoconjunctivitis (AKC), contact lens-induced papillary conjunctivitis (CLPC) and contact dermatitis (CDC) are the main subtypes of allergic conjunctivitis1. Of these, PAC and SAC are mainly triggered by the exposure to pollens and dust mites, and mast cell mediated hypersensitivity reactions being responsible for the inflammation reaction2. Although these two conditions can not lead to significant visual disability, they interfere significantly with the patient’s quality of life3. Among various ocular allergic conditions, AKC and VKC result in significant visual loss due to the resultant chronic inflammation4.
Management of these conditions is mainly aimed at preventing ocular surface damage by controlling inflammation and by inhibiting the release of allergic mediators5. Hence before the commencement of treatment therapy, identification of the type of ocular allergy, the associated comorbidities and their long term effects is essential. Main symptoms of allergic conjunctivitis include redness, watering, itching, and burning of eye6. Before starting pharmacological therapy, adjuvant treatment with non-pharmacological intervention like cold compresses, may help in relieving mild to moderate symptoms by serving as natural decongestant. The use of cooled artificial tears especially preservative free can also be helpful5.
The pharmacological treatment of allergic conjunctivitis, includes stepwise strategy for primary, secondary and tertiary treatment as depicted in figure 11, 7. The various topical ocular medications that are commonly used in the treatment of allergic conjunctivitis (Table 1)7 are as follows.
1. Decongestants
Topical decongestants serve as a cost effective choice for mild allergies. They act as a local vasoconstrictor, temporarily reducing redness, but do not treat the symptom of “itching”. They stimulate alpha-adrenergic receptor in the arterioles of the conjunctiva, thereby decreasing hyperaemia in the eye.
There are mainly two sub groups:
Alpha agonists- Phenylephrine 0. 12% and 0. 125%
Imidazole derivatives- Naphazoline (0. 012%, 0. 05%, 0. 1%), Tetrahydrozoline (0. 05%) and Oxymetazoline (0. 025%).
All these drugs constrict superficial conjunctival vessels, but on prolonged and excessive use can cause rebound conjunctival hyperemia. These eye drops should be given with caution in patients with associated systemic diseases like hypertension, cardiovascular disease, hyperthyroidism, diabetes mellitus, arrhythmias and angle closure glaucoma8.
2. Antihistamines
There are three types of histamine receptors, of which, H1 receptors lead to vasodilatation, contraction of nonvascular smooth muscle and increased vascular permeability by effecting smooth muscles. H2 receptors mediate histamine stimulation of gastric acid secretion and H3 receptors result in feedback inhibition in CNS, lung, heart and gastrointestinal tract. In ocular therapy, mainly H1 antihistamines are relevant which prevent
Topical Anti-allergic Drugs in Ophthalmology - An Update
Anita Ganger, Aswini Behera, Rebika Dhiman, M Vanathi, Cornea and Refractive Services,
Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, New Delhi, India.
Corresponding AuthorM Vanathi, Professor of Ophthalmology, Cornea, Cataract & Refractive ServicesRajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, New Delhi, India. Telephone No. : 91-11-26593010, Email: vanathi_g@yahoo. com

December 2017 Bengal Ophthalmic Journal 15
histamine-H1 receptor interaction, and block the effects of endogenously released histamine, thus providing symptomatic relief from histamine activity9.
The various antihistamines used in topical instillation for ocular allergy are as follows:
Emedastine difumarate
Emedastine is a second generation, antihistamine (H1) with higher potency and longer duration of action. It is a relatively selective, H1 antagonist and used in the form of the difumarate. Recommended dose is one drop twice a day, for six weeks. The most common observed adverse effect is headache. Other documented minor adverse effects are asthenia, tearing, eyes dryness, burning or stinging sensation and unpleasant taste10.
Epinastine
Epinastine is a second-generation antihistamine and mast cell stabilizer. Epinastine hydrochloride ophthalmic solution is used in concentration of 0. 05%. It is highly selective for the H1 receptor and does not cross the blood-brain-barrier. Its recommended dosage is one drop, twice daily. Side effects include burning sensation in the eyes, folliculosis, hyperaemia and pruritus. Among non ocular side effect infections (cold symptoms and upper respiratory infections) are common11.
Azelastine
Azelastine is a relatively selective histamine H1 antagonist, and has some affinity to H2 receptors. It is a phthalazine derivative, acts as an antihistamine and mast cell stabilizer. Its recommended dose is one drop usually instilled twice a day. Documented side effects are bitter taste, headache, weight gain, nausea, nose bleed, drowsiness or dizziness, dry mouth and sore throat12,13.
Bepotastine besilate
Bepotastine besilate ophthalmic solution 1.5% is a histamine H1 receptor antagonist. It is a direct H1-receptor antagonist that inhibits the release of histamine from mast cells. Among side effects, eye irritation, headache, unpleasant taste, and nasopharyngitis are the common ones.
Olopatadine
Olopatadine hydrochloride is an antihistamine which also acts as an anticholinergic and mast cell stabilizer, which is relatively selective H1 receptor antagonist. Dose of 0.1% olopatadine hydrochloride twice daily, 0.2% once daily is recommended. Mild burning, stinging, irritation, itching, redness, dryness of the eyes and puffy eyelids are the reported side effects.
Ketotifen
Ketotifen fumarate is an ophthalmic solution of 0.025% in 0.01% benzalkonium chloride. It’s a non competitive H1-receptor antagonist and mast cell stabilizer, which also acts as a leukotriene antagonist and a phosphodiesterase inhibitor. Its recommended dose is one drop usually instilled twice a day. Among side effects, Irritation, pain, punctate corneal epithelial erosion and punctate keratitis are the common ones.
Alcaftadine
Alcaftadine is an H1 and H2 receptor antagonist. The recommended concentration is 0.25%. By blocking these receptors, it significantly reduces the effects of allergens. This effect on histamine receptors seems to lower itching, redness and eosinophil recruitment after exposure to an allergen. Alcaftadine inhibits release of histamine from mast cells, decreases chemotaxis, and inhibits eosinophil activation. It also exhibits modulatory action on immune cell. Alcaftadine is mainly for prevention of allergic conjunctivitis14. In reported literature, evaluation of alcaftadine 0.25% effectiveness versus placebo and olopatadine 0.1%, showed that alcaftadine 0. 25% and olopatadine 0.1% treatments exhibited significantly lower mean scores compared with placebo for ocular itching and conjunctival redness15. It’s recommended dose is one drop in each eye once a day. Mild burning, stinging sensation and irritation are the related side effects.
3. Mast Cell Stabilizers
Mast cells when exposed to specific antigen, degenerates and release mediators which are otherwise stabilized by mast cell stabilizers. These agents block calcium ions from entering the mast cell.
The various mast cell stabilisers used in topical instillation for ocular allergy are as follows:
Sodium cromoglycate
Sodium cromoglycate is the commonly used mast cell stabilizer medication and recommended dose is one drop, four times daily. Burning or stinging of the eye is the commonly associated side effect.
Lodoxamide tromethamine
Lodoxamide tromethamine is used in concentration of 0.1% and is similar to sodium cromoglycate. Its recommended dose is one drop, four times daily. Transient burning, stinging, or discomfort, dry eyes, hyperaemia, crystalline deposits ocular itching and blurred vision are the common side effects.

Bengal Ophthalmic Journal16
Nedocromil
Nedocromil is used in strength of 2% as nedocromil sodium. It interferes with mast cell degranulation, specifically with release of leukotrienes and platelet activating factor16. Recommended dose is one drop usually instilled twice a day. On long term uses, nedocromil sodium eye drops are more efficacious than sodium cromoglycate eye drops17. When compared with 0. 1% fluoromethalone it is found to be equally efficacious18. Side effects include headache, irritation, stinging sensation, ocular burning, unpleasant taste, and nasal congestion.
4. Non-steroidal Anti-inflammatory Drugs (NSAIDs)
NSAIDS have limited role in allergic conjunctivitis, as it does not produce any inhibitional effect on allergic inflammatory mediators. These drugs act by binding to the cyclooxygenase enzymes COX-1 and COX-2, which in turn block the synthesis of prostaglandins, thromboxane as well as leukotrienes and result in reduction of itching and hyperemia19. Commonly used NSAIDS are diclofenac sodium, ketorolac and indomethacin5. In asthmatic patients, this should be given with caution to avoid the possibility of respiratory distress. Unlike steroids, NSAIDS do not lead to cataract formation and higher intraocular pressure. Most commonly used NSAID for ocular allergic conditions is ketorolac tromethamine which is a member of the pyrrole group of NSAIDs. Ocular burning, stinging and itching are the common associated side effects.
5. Corticosteroids
Corticosteroids are beneficial in allergic conjunctivitis by acting mainly on inflammation pathway. These drugs, firstly block the synthesis of prostaglandins and leukotriene from arachidonic acid by inhibiting phospholipase A. Secondly, these drugs inhibit the production of inflammatory proteins by acting at the nuclear transcription level19.
Most commonly used topical corticosteroids in ocular allergic disorders include prednisolone and dexamethasone. Although steroids are potent anti inflammatory drugs, but their use is associated with side effects like increased intraocular pressure, development of early cataracts and delayed wound healing. Hence, steroids should be used only in refractory allergic conditions and that too for the short duration only. Steroids with lower intraocular absorption like hydrocortisone, fluorometholone, loteprednol and difluprednate, can be considered in while initiating topical steroid therapy, especially if the cornea is not involved yet. Frequency and the dosage of these drugs is to be decided by the level of inflammation, and in view of various side effects, gradual tapering of these drugs is essential Strong steroids such as prednisolone, dexamethasone, or betamethasone may be chosen if the low potency steroids do not produce the required desirable therapeutic effect20.
Loteprednol etabonate
Loteprednol is a low potency, newer generation corticosteroid which is commonly used and reported to be effective for allergic disorders21. It is available as 0.5% eye drops and 0.2% or 0. 5% ophthalmic suspensions22. Main concern in prescribing corticosteroid is the requirement of constant monitoring and possibility of flaring up of ocular infections.
6. Immunosuppressants
Immunosuppressive drugs firstly help in reducing ocular inflammation by blocking Th2 lymphocyte proliferation and interleukin-2 production. Secondly these drugs reduce IL-5 production, which in turn inhibits histamine release from mast cells.
Cyclosporine A (CsA)
Cyclosporin A () is an immunomodulator that inhibits the interleukin-2 (IL-2) receptor expression, which result in inhibition of proliferation of CD4 T lymphocyte. CsA is one of the most commonly used immunosuppressants for allergic conjunctivitis. Drug concentrations of 2%, 1%, 0. 5%, and 0. 05% are reported to be effective in reducing symptomatology and have steroid sparing effect23.
Tacrolimus
Mechanism of Tacrolimus is similar to CsA. Effectiveness of tacrolimus 0.1% suspension in severe allergic conditions is reported by a multicenter, randomized, double-masked, placebo-controlled clinical trial. Ocular irritation is the most frequent reported side effect24.
A prospective study compared the efficacy of 0.1% tacrolimus ophthalmic ointment with CsA 2% and showed that both were equally effective in the treatment of VKC25.
7. Monoclonal Antibodies
Omalizumab is a monoclonal antibody, which is recombinant DNA-derived humanized IgG1κ monoclonal chimeric anti-IgE antibody, that selectively binds to the Cε3 domain of free circulating IgE26. Selective binding to IgE lowers free IgE levels, thus suppressing the activation of mast cells and subsequently IgE receptors (FcεRI) on the cells get down regulated27. Hence, the IgE-mediated reactions are less likely to occur. This is approved by the US Food and Drug Administration for treating severe vernal keratoconjunctivitis, allergic asthma and severe chronic idiopathic urticaria28-31.
8. Newer Medication
Recently FDA has approved the new topical formulation of Cetirizine (H1 receptor antagonist) for the treatment of allergic
December 2017 Bengal Ophthalmic Journal 17
conjunctivitis. This formulation is the second-generation antihistamine (H1) which reduces itching and vasodilation by binding competitively to histamine receptor sites. The recommended dose of topical cetrizine is twice instillation of one drop daily. Among documented adverse effects, ocular hyperemia, pain after instillation and blurring of visual acuity are the frequent ones.
References
1. Bielory L. Allergic and immunologic disorders of the eye Part II: ocular allergy. J Allergy Clin Immunol. 2000;106:1019-32.
2. Chowdhury B. Allergic conjunctivitis – A review. DOS Times. 2013;19:41-7.
3. Sanchez MC, Fernandez Parra B, Matheu V, et al. Allergic conjunctivitis. Conjunctivitis. J Investig Allergol Clin Immunol. 2011;21:1-19.
4. Bielory L. Ocular allergy overview. Immunol Allergy Clin North Am. 2008;28:1-23.
5. Chigbu DI. The management of allergic eye diseases in primary eye care. CLAE. 2009; 32:260-72.
6. La Rosa M, Lionetti E, Reibaldi M, Russo A, Longo A, Leonardi S, et al. Allergic conjunctivitis: a comprehensive review of the literature. Ital J Pediatr. 2013;39:18.
7. Bielory L, Meltzer EO, Nichols KK, Melton R, Thomas RK, Bartlett JD. An algorithm for the management of allergic conjunctivitis. Allergy Asthma Proc. 2013;34:408-20.
8. Van Cauwenberge P, De Belder T, Vermeiren J, Kaplan A. Global resources in allergy (GLORIA): allergic rhinitis and allergic conjunctivitis. Clin Exp All Rev. 2003;3:46-50.
9. Wade L, Bielory L, Rudner S. Ophthalmic antihistamines and H1-H4 receptors. Curr Opin Allergy Clin Immunol. 2012;12:510–6.
10. Bielory L, Lien KW, Bigelsen S. Efficacy and tolerability of newer antihistamines in the treatment of allergic conjunctivitis. Drugs. 2005;65:215–28.
11. Pradhan S, Abhishek K, Mah F. Epinastine: topical ophthalmic second generation antihistamine without significant systemic side effects. Expert Opin Drug Metab Toxicol. 2009;5:1135–40.
12. Bergmann MT, Williams JI, Gomes PJ. Treatment of allergic conjunctivitis with bepotastine besilate ophthalmic solution 1. 5%. Clin Ophthalmol Auckl NZ. 2014;8:1495–505.
13. Carr WW, Nayak AS, Ratner PH, Gow JA, McNamara TR, Williams JI, et al. Efficacy of bepotastine besilate ophthalmic solution 1.5% for seasonal allergic conjunctivitis: a randomized, placebo-controlled, natural exposure, clinical trial. Allergy Asthma Proc. 2013;34:247–54.
14. Namdar R, Valdez C. Alcaftadine: a topical antihistamine for use in allergic conjunctivitis. Drugs Today Barc Spain. 2011;47:883–90.
15. Greiner JV, Edwards-Swanson K, Ingerman A. Evaluation of alcaftadine 0.25% ophthalmic solution in acute allergic conjunctivitis at 15 minutes and 16 hours after instillation versus placebo and olopatadine 0.1%. Clin Ophthalmol Auckl NZ. 2011;5:87–93.
16. Tauber J, Alocril Community Allergy Trial Study Group. Nedocromil sodium ophthalmic solution 2% twice daily in patients with allergic conjunctivitis. Adv Ther. 2002;19:73–84.
17. Verin PH, Dicker ID, Mortemousque B. Nedocromil sodium eye drops are more effective than sodium cromoglycate eye drops for the long-term management of vernal keratoconjunctivitis. Clin Exp Allergy J Br Soc Allergy Clin Immunol. 1999;29:529–36.
18. Tabbara KF, al-Kharashi SA. Efficacy of nedocromil 2% versus fluorometholone 0. 1%: a randomised, double masked trial comparing the effects on severe vernal keratoconjunctivitis. Br J Ophthalmol. 1999;83:180–4.
19. Bielory L. Ocular allergy treatment. Immunol Allergy Clin North Am. 2008;28:189-224.
20. Druzgala P, Wu WM, Bodor N. Ocular absorption and distribution of loteprednol etabonate, a soft steroid, in rabbit eyes. Curr Eye Res 1991; 10:933.
21. Shulman DG, Lothringer LL, Rubin JM, Briggs RB, Howes J, Novack GD, et al. A randomized, double-masked, placebo controlled parallel study of loteprednol etabonate 0. 2% in patients with seasonal allergic conjunctivitis. Ophthalmology. 1999;106:362-9.
22. Mishra GP, Tamboli V, Jwala J, Mitra AK. Recent patents and emerging therapeutics in the treatment of allergic conjunctivitis. Recent Pat Inflamm Allergy Drug Discov. 2011;5:26-36.
23. Lambiase A, Leonardi A, Sacchetti M, et al. Topical cyclosporine prevents seasonal recurrences of vernal keratoconjunctivitis in a randomized, double-masked, controlled 2-year study. J Allergy Clin Immunol. 2011;128(4):896–7 e9.

Bengal Ophthalmic Journal18
24. Ohashi Y, Ebihara N, Fujishima H, et al. A randomized, placebo-controlled clinical trial of tacrolimus ophthalmic suspension 0.1% in severe allergic conjunctivitis. J Ocul Pharmacol Ther. 2010;26(2):165–174.
25. Labcharoenwongs P, Jirapongsananuruk O, Visitsunthorn N, et al. A double-masked comparison of 0. 1% tacrolimus ointment and 2% cyclosporine eye drops in the treatment of vernal keratoconjunctivitis in children. Asian Pac J Allergy Immunol. 2012;30(3):177–184.
26. Buhl R. Anti-IgE antibodies for the treatment of asthma. Curr Opin Pulm Med. 2005;11:27–34.
27. MacGlashan DW, Bochner BS, Adelman DC, Jardieu PM, Togias A, McKenzie-White J, et al. Down-regulation of Fc(epsilon)RI expression on human basophils during in vivo treatment of atopic patients with anti-IgE antibody. J Immunol Baltim Md. 1997;158:1438–45.
28. Logsdon SL, Oettgen HC. Anti-IgE therapy: clinical utility and mechanistic insights. Curr Top Microbiol Immunol. 2015;388:39-61.
29. Doan S, Amat F, Gabison E, Saf S, Cochereau I, Just J. Omalizumab in Severe Refractory Vernal Keratoconjunctivitis in Children: Case Series and Review of the Literature. Ophthalmol Ther. 2017;6:195–206.
30. Heffler E, Picardi G, Liuzzo MT, Pistorio MP, Crimi N. Omalizumab Treatment of Vernal Keratoconjunctivitis. JAMA Ophthalmol. 2016;134:461-3.
31. Mizutani N, Nabe T, Yoshino S. Topical ocular treatment with monoclonal antibody Fab fragments targeting Japanese cedar pollen Cry j 1 inhibits Japanese cedar pollen-induced allergic conjunctivitis in mice. Eur J Pharmacol. 2017;798:105-112.
Conflicts of Interest- None Financial disclosures- None
Table 1. Various Topical eye drops used in Allergic conjunctivitis
Class Examples Indications Dosage
Antihistamines Levobastine Emedastine PAC, SAC, VKC, AKC TDS-QID
Decongestants Oxymetazoline, Naphazoline
PAC, SAC TDS
Antihistamines/ Decongestants Pheniramine maleate/ naphazoline
PAC, SAC, VKC QID
Antihistamines/Mast cell stabilizers Olopatadine, Ketotifen, Epinastine, Azelastine
SAC, VKC, AKC BD
Mast cell stabilizers Sodium cromoglycate, Lodoxamide
SAC, VKC, GPC TDS-QID
NSAIDS Ketorolac tromethamine PAC, SAC, VKC TDS-QID
Corticosteroids Loteprednol etabonate, Prednisolone acetate, Dexamethasone
Severe allergic diseases BD-QID
Immunosuppressive Cyclosporin, Tacrolimus
AKC, VKC TDS
*BD - two times a day, TDS - three times a day, QID - four times a day

Review Article19
OCT angiography- A revolutionary approach for retinal imaging
Dhrubojyoti Sarker, Junior residentRajiv Kumar Gupta, Associate Professor. Department of Ophthalmology
RIO, RIMS, RANCHI
Introduction
For the last two decades’ paradigm shift of ophthalmic imaging technique is ostensibly unique. Research on Retinal imaging is continuing its yield for better modalities of quicker and reproducible methods to delineate retinal microanatomy and specifically its blood vessels. Surpassing the era of invasive two dimensional procedures like fluorescein (FA) or Indocyanine green angiography (ICGA) we embraced a no-injection, dye-free method like OCT angiography for visualizing ocular vasculature. SD- OCT can identify vessels and point out gross abnormalities (e. g. CNVM) nevertheless it sensitivity, acquisition speed, and resolution[1]have enabled volumetric imaging of ocular structures with micrometre-scale depth resolution though it offers poor contrast between small blood vessels and static tissue in most retinal layers. As a result, structural OCT is not used clinically to identify vascular changes such as capillary dropout or pathologic new vessel growth in AMD and diabetic retinopathy that can lead to vision loss.
OCT angiography is a revolutionary invention, this heavily promoted aims to contrast blood vessels from static tissue by assessing the change in the OCT signal caused by flowing blood cells. These intrinsic contrasts can be broadly classified as Doppler shift and speckle variance/decorrelation. Various quantitative metrics such as vessel density (VD) as calibre per area, length per area, and fractal dimension have been reported for the analysis of OCT-A figures. The superiority belongs to its segmental imaging in ‘en face’ manner, which mean layer by layer representation of retinal vascular network (e. g., superficial capillary plexus, deep capillary plexus, choriocapillaris) The high contrast of OCT‑A for depicting the retinal circulation lends itself for generation of quantitative data, such as capillary perfusion density.
Despite many advantages of OCT‑A, limitations do exist.[2] These limitations include motion artefact (due to eye movements or squint), attenuation artefact (due to loss of signal with depth), segmentation artefact (due to difficulties in selecting consistent
boundaries for the en face slabs), and projection artefact (due to decorrelation tails from more superficial vessels). These artefacts can dramatically confuse the interpretation of OCT‑A figures. Latest updating of software’s is going to drastically alter how ophthalmologists think about imaging. Like every investigative approach OCT-A also smooth learning curve, which sharpens clinician’s ability to locate, identify and detect vascular jeopardy perfectly. As software has improved, it is becoming clear that OCT angiography is substantially better than FFA, ICG (there was still an issue of “noise” that did not allow for the contrast we would like to have). if you’re looking at just a single frame.
The mechanism of action- demystifying finer details
The OCT technology is based on Michelson’s interferometry, which is a concept of electromagnetic theory of light. A software is employed to identify the low coherence corroborating the standard light (which reflects from the reference mirror) and the light being reflected from deeper tissues. Marely histological imaging was going to backseat as volumetric angiography was not feasible until development of the two Fourier-domain OCT implementations[3] e. g. spectral-domain (SD-OCT)[4] and swept-source.[5]. In 2006, Makita et al[6] used an 18. 7kHz SD-OCT system to perform volumetric angiography and visualization of retinal and choroidal vasculature. Further modification like optical micro angiography (OMAG) incorporated the amplitude of the OCT signal in addition to phase. An et al [7] suggested that OMAG was better able to identify the microvasculature than previous methods utilizing only phase information. OCT-A is a novel technology that rapidly and conveniently figures blood vessels in vivo without the use of exogenous dyes, providing high-resolution and three-dimensional information on the morphology of physiological and pathological blood vessels at different layers of the retina.
OCT‑A detects the motion of red blood cells as intrinsic contrast and is sensitive to both transverse and axial flow in time. Cross‑sectional OCT angiograms can superimpose color‑coded flow information on grey‑scale structural information which is already installed in the machine. Thus, both blood flow and retinal structural data can be presented together (figure 1). OCT‑A generates a data cube, segmentation, and en face presentation of vascular perfusion at various layers of the retina can summarize the flow information at relevant anatomic layers or slabs which can be up to 5 µm thin. This figures are taken in to 3×3 mm standardized perifoveal zone because this
Corresponding AuthorDhrubojyoti SarkerS-2/7 by lane, A. P. NagarPO + PS=SonarpurKolkata 700150. West bengalContact no -8013151735
Bengal Ophthalmic Journal20
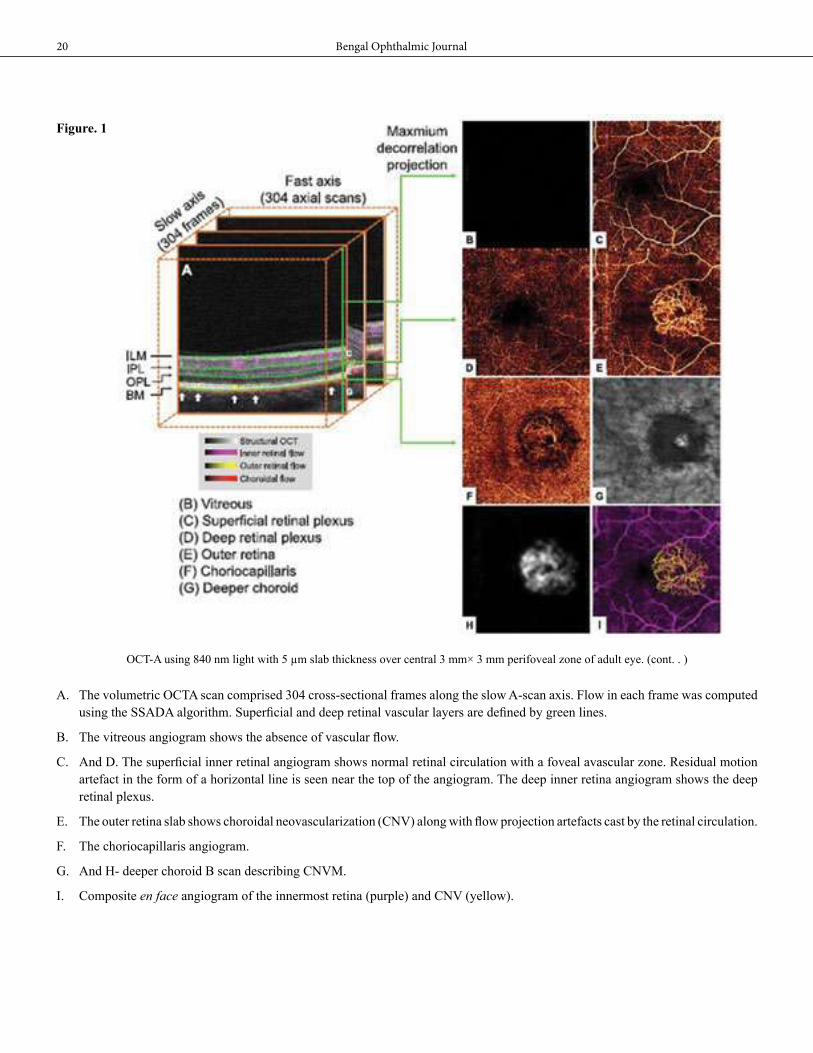
Figure. 1
OCT-A using 840 nm light with 5 µm slab thickness over central 3 mm× 3 mm perifoveal zone of adult eye. (cont. . )
A. The volumetric OCTA scan comprised 304 cross-sectional frames along the slow A-scan axis. Flow in each frame was computed using the SSADA algorithm. Superficial and deep retinal vascular layers are defined by green lines.
B. The vitreous angiogram shows the absence of vascular flow.
C. And D. The superficial inner retinal angiogram shows normal retinal circulation with a foveal avascular zone. Residual motion artefact in the form of a horizontal line is seen near the top of the angiogram. The deep inner retina angiogram shows the deep retinal plexus.
E. The outer retina slab shows choroidal neovascularization (CNV) along with flow projection artefacts cast by the retinal circulation.
F. The choriocapillaris angiogram.
G. And H- deeper choroid B scan describing CNVM.
I. Composite en face angiogram of the innermost retina (purple) and CNV (yellow).

December 2017 Bengal Ophthalmic Journal 21
plane resides perpendicularly to incidence lights so contrast and finer resolution is obvious. This OCT operates at 70, 000 A-scans per second to acquire OCT-A volumes consisting of 304 × 304 consecutive frames. Corresponding structural OCT B-scans are obtained concurrently. Wide field imaging to delineate pre equatorial and peripheral retina can be done by modifying incidence ray settings.
The latest technique of OCT-A employs several protocols such as split spectrum amplitude‑decorrelation angiography (SSADA),[8] speckle variance and phase variance have been exported[9]. The former being most efficient and informative. SSADA, was developed by David Huang, MD, PhD. This algorithm takes sequential consecutive OCT scans, and then compares each OCT scan with the subsequent scan. The SSADA algorithm also uses multiple spectrums from single B-scan to improve the figure quality( figure 2) Therefore, it reduces the number of repeat B-scans required for achieving good vascular imaging. The concept of signal and noise is imperative in SSADA because it clearly improves signal: noise ratio, signal generated from moving blood cells can be occluded by motion noise, which is unacceptable. As the SSADA utilises multiple or split spectrum that is able to figure a specific tissue by repeated
B scans, which emphasizes the brightness as well as contrast of the tissue by best finer details. SSADA’s algorithmic feature is based on-‘speckle variance’ and ‘decorrelation’, and both need to be clarified to understand the mechanism.
● Specklevariance – OCT angiography based on amplitude or intensity was initially described in 2005, when Barton et al.[10] adapted laser speckle analysis for time-domain OCT. Speckle arises as a property of the interferometric nature of OCT, the basic idea is to identify the altitudinal subtraction value and speckle variation contains information regarding the motion of scatters[11]. Specifically, the speckle pattern stays relatively constant over time for static objects while the pattern changes for objects in motion e. g. streaming blood cells and micro movements of vessel wall. In the work of by Mariampillai et al[12]. speckle variance was calculated as the variance of the OCT reflectance amplitude over three repeated B-scans at the same location. Improvising the method, the same investigators[13] noted in 2010 that the B-scan rates for repeat scans needed to be fast enough to be equivalent to OCT laser movement.
● Decorrelationmapping- intensity-based OCT-A approach was termed correlation mapping[14]. In de correlation mapping OCTA, cross-correlation of a grid on adjacent B-scans was performed to identify vasculature (weak correlation) versus static tissue (strong correlation). It is novel technique to identify different tissues with finest resolution because of different light reflectance from mobile and still tissue. The phenomenon sounds equivalent to staining a particular section of a tissue where stain will be applicable to a specific point of interest (as the congo red stains the amyloid material, when abdominal fat histopathological analysis done in a amyloidosis case)
Figure 2 – SSADA improves the image quality providing less artefact interruption.

Bengal Ophthalmic Journal22
Thus SSADA sacrificed axial resolution by splitting the OCT signal into different spectral bands to increase the number of usable figure frames without increasing scanning time or decreasing scan density. When spectrally-split amplitude-decorrelation figures were combined, the flow signal-to-noise ratio was increased and super resolution figure is generated.
Revolutionary features
1. Magnificent research tool- since last a few years OCT-A became a fabulous research tool for investigators and clinicians. The interest grown high as Optovue, Inc., who then worked quickly to implement and make OCT-A available as a research tool to the wider ophthalmic community on their commercial, SD-OCT platform. It prompted Carl-zeiss Meditec Inc. to adapt OMAG for their eye-tracking enabled SDOCT system. The following caterectristics fuelled the popularity.
2. En Face Visualization of Segmented retinal tissue- from its inception OCT-A remained struck to en face technique
describing retinal layers. Although SD-OCT could establish proper figure clarity between ILM and Bruch’s membrane, almost all OCT-A machines (discussed later) appropriate tissue layers or ‘‘slabs’’ can then be defined based on these references planes( figure 3). En face presentation of these slabs can produce angiograms similar to FA or ICGA. It’s the experience of the operator who if familiar to the gross retinal abnormality (e.g. drusen, CNVM, CMO) of the particular patient, can clearly set up desired reference slabs to pick the desired picture of the vasculature.
3. Colour coding attributing to slab level- additional information provided by the colour coding method to delineate the depth relative to a simple reference plane.[15] More often, colour was used to represent flow in different segmented tissue slabs[16]. The baseline imaging of inner retinal vascular plexus, which is drawn in the plane between ILM and OPL. This layer vessels are in red and the deep inner retinal plexus is purple. On the contrary deeper vessels presented in yellow.
OCT–A, tools available- Several manufacturers improvised OCT devices including algorithms enabling the practitioner to obtain regular highly informative OCT B-scans as well as volumetric angiographic figures. Different techniques such as Doppler shift, speckle variance/decorrelation, phase variance, optical micro-angiography and correlation mapping are employed to differentiate blood vessels by depicting the change in the OCT-signal induced by the moving blood cells[17]. Currently we have the following devices
• Angiovue optical coherence tomography angiography (Optovue RTVue XR Avanti, Optovue Inc., Fremont, CA) based on a split spectrum amplitude decorrelation angiography algorithm (SSADA)
• Zeiss AngioPlex (Cirrus HD-OCT 5000, Zeiss Meditec. Inc. ) based on micro-angiography (OMAG)
• SS-OCT Angiography employed in a Swept source OCT DRI OCT Triton (Topcon DRI OCT Triton Swept source OCT, Topcon, Japan) using the so called OCT angiography ratio analyses (OCTARA) algorithm.
In a study to compare the outcome of these OCT –A machines Marion R. Munk et al found that There was no difference in the overall vessel density (Zeiss 48. 7±4%, Optovue 47. 9±3%, Topcon 48. 3±2%, p = 0. 2). No significant difference among the devices in terms of motion artefacts were detected. However, for figure artefacts of the Superficial Capillary Plexus the Zeiss and the Topcon modules were superior compared to the other device. The FAZ border of the SCP slabs were best appreciable on the Zeiss figures, followed by the Optovue
Figure 3- superficial(a)and deep(b) vascular network as Segmented by OCT-A software.
a
b

December 2017 Bengal Ophthalmic Journal 23
device, whereas the FAZ of the DCP was best discernible on the Optovue device [pone]
Clinical applications
Measurement of Retinal and choroidal blood flow is a fascinating issue for several decades. Initially colour Doppler imaging (CDI)[18], laser Doppler velocimetry (LDV)[19], laser speckle technique[20], laser Doppler flowmetry (LDF)[21], retinal vessel analyser (RVA)[22], retinal oximetry[23], and blue field entoptic technique.[24] were employed but had had limitations, furthermore scanning laser ophthalmoscopy angiography with fluorescein FFA, an invasive technique which lack perfect quantification which considered to be highly demanding in
terms of early diagnosis and pointing characteristic changes of vessels that can be only found in textbook drawings previously.
OCT-A in normal eye - (figure 3) the number and thickness of plexuses depend on the thickness of retina. Parapapillary and perifoveal area being the thickest where 3–4 layers may be distinguished. the existence of separate vascular networks in the inner retina (nerve fibre layer and the ganglion cell layer) and the deep retina (outer plexiform layer) and both these networks were interconnected with numerous vertical vessels. Fingler et al. also described the use of OCT‑A and FAZ area, they reported the FAZ area was significantly larger in deep plexus as compared to superficial plexus [25]
OCT-A in diabetic retinopathy - DR cases are always at risk for aggravation of vascular homeostasis. Changes that take place subtle way are extremely difficult to identify. Patients who are classified in early or mild NPDR, might have changes suggestive of moderate to severe NPDR. Retinal micro aneurysms and ischemic zones are identifiable at ease, eventually help to institute early therapeutic intervention. de Carlo et al. reported that OCT‑A was able to figure foveal microvascular changes not detected by clinical examination. Foveal Avascular Zone (FAZ)area was 0. 348 mm2 in diabetic eyes and 0. 288 mm2 in the control eye. also capillary non perfusion observed with OCT‑A was more severe in diabetic eyes (21%) compared to 4% in control eyes [26]. So enlargement of FAZ is indeed an early prognostic factor for better diagnosis and management. (figure 4)
OCT-A in retinal vaso occlusive disorders - Vaso occlusive disorders like BRVO, CRVO, CRAO are quite common in diabetic or hypertensive individuals. Filho et al. first highlighted the benefit of OCT‑A to define areas on non perfusion in ischemic RVOs[27]. Kashani et al. reported OCT‑A is highly efficient delineating areas of impaired vascular perfusion, retinal atrophy, vascular dilation, and forms of intraretinal edema[28].
OCT-A in chroidal neovascularisation(CNV) - wet ARMD, clinico pathologically identified as CNV is a potential threat to central vision most of the time. Due to its growth in subretinal space penetrating through Bruch’s membrane, CNV should be always early diagnosed to obviate risk of sub macular bleed and sub foveal fibrosis. Jia et al. first described the ability of a prototype SS‑OCT‑A system to visualize and qualify CNV. de Carlo et al. described the sensitivity of detection of CNV on OCT‑A was high (91%) compared to FA (91%), though the specificity was 50%[29]. Lumbroso et al. noted morphological changes of new vessels and discovered the loss of smaller vessels after intravitreal anti VEGF injection.
OCT-A in glaucoma - the persistently elevated IOP is unarguably the most important risk factor. But perfusion analysis by OCT-A
Figure 4- superficial and deep vascular zones are delineated in a case of NPDR. Microanurysm and tortuous capillery
bed and enlarged FAZ well documented

Bengal Ophthalmic Journal24
of optic nerve head and lamina cribrosa region, both of which have rich vascular network around them, yields superior outcomes. Parapapillary microvasculature is normally attenuated in both the superficial disc vasculature and deeper lamina cribrosa in glaucomatous eyes. Liu et al. describe the mean vascular density of glaucomatous eyes versus healthy ones to be 80. 55% to 93%, respectively[30]. Ghasemi Falavarjani et al. evaluated ONH microvasculature of acute and chronic neuropathies using OCT‑A, they observed a reduction in the visibility of the parapapillary microvasculature which corresponded to retinal nerve fibre layer atrophy observed in OCT[31]
OCT-A in anterior segment imaging- defining the abnormal fine vessels in cornea is a path breaking success attained by OCT-A. till now the slit lamp is being employed to identify neo vascularisation of cornea in any disease procedures like-herptitic eye disease, graft rejection, chronic non healed corneal ulcer and limbal stem cell deficiency[32]. OCT-A assessment, however, may be of benefit for identifying subtle vascular features, particularly when there may be other corneal opacity which can interfere with typical clinical assessments. Ange et al. were able to visualize corneal vessels invading a corneal graft and corneal NV in pterygium using OCT‑A.
Diagnostic pearls and Future directions of OCT-A imaging
OCT-A is a highly efficient, fast, reproducible, potential functional extension of OCT. Despite its recent introduction, the potential clinical impact of OCT-A can already be felt. In the world of quicker and promising diagnostic machine it has strengthened ophthalmologist’s armamentarium with advanced discovery of diseases like occult CNV, subtle NPDR changes, ischemic zones in RVO, RAO etc. which usually evading FFA technique. Optical coherence tomography angiography is also able to visualize the closure of branch CNV vessels after anti-VEGF injection and their reopening/remodelling over time[33] Rebound of CNV vessel area can precede fluid reaccumulation[34] and may be helpful for guiding the timing of therapy. In central serous chorio retinopathy, OCTA can more reliably determine the presence of CNV, which can be difficult to assess with FA[35].
Furthermore, the depth-resolved nature of OCT-A improves visualization and localization of pathologic features in specific plane. Because of dye free investigation it does not visualize leakage, so vascular integrity is identified by only morphological changes unlike FFA.
The innovative designs of OCT-A undergoing metamorphosis to overcome its previous limitations. Going forward, we expect to see continued advances in hardware and software, which should expand the field of view of OCT-A. It’s a continuous endeavour to visualize a lesion in a single frame, which is going to happen by the latest updated soft wares, that efficiently negate blurring
and yield best quality figures. A recent study suggested that the usage of the FS-ADA algorithm, which is implemented in the Heidelberg module, would cause less projection artefacts compared to the SSADA algorithm.[36] Heidelberg prototype uses a full-spectrum amplitude decorrelation algorithm (FS-ADA) to evaluate motion contrast, which allows the evaluation of blood flow without sacrificing depth resolution.[37] The prototype acquired an A-scan rate of 85kHz with an axial resolution of 7μm and a lateral resolution of 14μm.[38].
Technological advancement continues to be in focal research to reduce motion artefacts, localising the perfect plane, quantification of OCT-A figures need experience and skill. The improvised software will guide to get high resolution picture. Finally, the OCT-A should be introduced in teaching curriculum to understand the in vivo retinal microenvironment, and making diagnosis in a better way.
Conclusion
OCT-A is fast, reproducible, non-invasive, and does not even require the use of bright visible light, it can be used more frequently than traditional angiography, which requires intravenous dye injection. Thus, we expect that OCT-A could be used for high-volume applications such as the routine screening of diabetic retinopathy and regular follow-up of AMD. A few limitations (expense, no leakage/velocity, and artefacts), which may make interpretation of OCT‑A figures a challenge in a developing country. Large scale clinical trials and technological advancement always be promoted for a bright angiographic future in retinal horizon.
References
1. Drexler W, Liu M, Kumar A, Kamali T, Unterhuber A, Leitgeb RA. Optical coherence tomography today: speed, contrast, and multimodality. J Biomed Opt. 2014;19:071412.
2. Spaide RF, Fujimoto JG, Waheed NK. Figure artifacts in optical coherence tomography angiography. Retina 2015;35:2163‑80.
3. Leitgeb R, Hitzenberger C, Fercher A. Performance of Fourier domain vs. time domain optical coherence tomography. Opt Express. 2003;11:889–894.
4. Wojtkowski M, Leitgeb R, Kowalczyk A, Bajraszewski T, Fercher AF. In vivo human retinal imaging by Fourier domain optical coherence tomography. J Biomed Opt. 2002;7:457– 463.
5. Yun S, Tearney G, de Boer J, Iftimia N, Bouma B. High-speed optical frequency-domain imaging. Opt Express. 2003;11: 2953–2963.

December 2017 Bengal Ophthalmic Journal 25
6. Makita S, Hong Y, Yamanari M, Yatagai T, Yasuno Y. Optical coherence angiography. Opt Express. 2006;14:7821–7840.
7. An L, Wang RK. In vivo volumetric imaging of vascular perfusion within human retina and choroids with optical micro-angiography. Opt Express. 2008;16:11438–11452.
8. Bonini Filho MA, Adhi M, de Carlo TE, et al. Optical coherence tomography angiography in retinal artery occlusion. Retina. 2015;35:2339–2346.
9. Barton J, Stromski S. Flow measurement without phase information in optical coherence tomography figures. Opt Express. 2005;13:5234–5239.
10. Mariampillai A, Standish BA, Moriyama EH, et al. Speckle variance detection of microvasculature using swept-source optical coherence tomography. Opt Lett. 2008;33:1530– 1532.
11. Mariampillai A, Leung MK, Jarvi M, et al. Optimized speckle variance OCT imaging of microvasculature. Opt Lett. 2010; 35:1257–1259.
12. Kim DY, Fingler J, Werner JS, Schwartz DM, Fraser SE, Zawadzki RJ. In vivo volumetric imaging of human retinal circulation with phase-variance optical coherence tomography. Biomed Opt Express. 2011;2:1504–1513.
13. Miura M, Makita S, Iwasaki T, Yasuno Y. Three-dimensional visualization of ocular vascular pathology by optical coherence angiography in vivo. Invest Ophthalmol Vis Sci. 2011; 52:2689–2695.
14. Zhang A, Zhang Q, Chen CL, Wang RK Methods and algorithms for optical coherence tomography based angiography: a review and comparison. J Biomed Opt. 2015; 20:100901. https://doi. org/10. 1117/ 1. JBO. 20. 10. 100901 PMID: 26473588.
15. Munk MR, Giannakaki-Zimmermann H, Berger L, Huf W, Ebneter A, Wolf S, et al. (2017) OCT-angiography: A qualitative and quantitative comparison of 4 OCT-A devices. PLoS ONE 12(5): e0177059.
16. Schmetterer L, Garhofer G. How can blood flow be measured ? Surv Ophthalmol 2007;52 Suppl 2:S134‑8.
17. Dimitrova G, Kato S. Color Doppler imaging of retinal diseases. Surv Ophthalmol 2010;55:193‑214.
18. Garhofer G, Bek T, Boehm AG, Gherghel D, Grunwald J, Jeppesen P, et al. Use of the retinal vessel analyzer in ocular blood flow research. Acta Ophthalmol 2010;88:717‑22.
19. Hardarson SH. Retinal oximetry. Acta Ophthalmol 2013;91 Thesis 2:1‑47.
20. Schmetterer L, Garhofer G. How can blood flow be measured ? Surv Ophthalmol 2007;52 Suppl 2:S134‑8.
21. Fingler J, Zawadzki RJ, Werner JS, Schwartz D, Fraser SE. Volumetric microvascular imaging of human retina using optical coherence tomography with a novel motion contrast technique. Opt Express 2009;17:22190‑200.
22. de Carlo TE, Romano A, Waheed NK, Duker JS. A review of optical coherence tomography angiography (OCTA). Int J Retina Vitreous 2015;1:5.
Conflicts of Interest- None Financial disclosures- None

Review Article
Facial Nerve Palsy -An Ophthalmologist Perspective Joyeeta Das, Consultant, orbit and oculoplasty services, Disha Hospital
Abstract: An ophthalmologist plays a crucial role in the management of patients with facial nerve palsy. It is important to recognize and treat the potentially life-threatening underlying causes. An ophthalmologist’s first priority is to ensure adequate corneal protection. Long-term management consists of surgical treatment of corneal exposure due to lagophthalmos and lid laxity. This review aims to provide a guide to the management of this complex condition
Keywords: Facial nerve palsy, Lagophthalmos, Gold weight lid loading
Introduction
Facial nerve or the 7th cranial nerve is the most commonly paralysed nerve of the body which leads to significant visual as well as psychosocial disabilities. An ophthalmologist may be the first clinician to encounter a case of facial palsy who plays a pivotal role in proper diagnosis, treatment and rehabilitation of such cases. Prompt ocular support which specifically aimed at prevention of corneal exposure due to lagophthalmos. This review article aimed at providing a brief outline of anatomy of the facial nerve, common aetiologies and management of facial nerve palsy from ophthalmologist’s perspective
Anatomy
The facial nerve has combined motor, sensory and secretomotor (parasympathetic) components.
FIG:1 Anatomy of the facial nerve roots and peripheral branches
The muscles of facial expression, scalp and stapedeous are supplied by the motor nerve. Its nucleus lies within the Pons and receives cortico-nuclear fibre input from cerebral hemisphere. The area of the motor nucleus that supplies the upper face (forehead) gets cortico-nuclear fibres from precentral gyri of both right and left hemisphere and that is why in upper motor neuron (UMN) palsy the forehead movement are spared but in peripheral or LMN palsy the whole half of the face is affected. (FIG 2)
The sensory nucleus of the facial nerve (Nucleus tractus solitorious) receives fibres carrying taste sensation from anterior 2/3rd of tongue and trigeminal sensory nucleus supplying small part of ear (Chorda tympani).
The superior salivatory nucleus of Facial nerve sends secretomotor fibres to lacrimal gland and salivary secretion. The facial nerve leaves the Cerebellopontine angle and enters the internal auditory canal of the temporal bone to runs a 30-mm long course through the temporal bone which makes it vulnerable to compression.
Within the temporal bone it leaves three branches. First branch is greater superficial petrosal nerve (GSPN) supplies the lacrimal and palatine secretomotor fibres to the pterygopalatine ganglion. Other two branches are Nerve to stapedeus and chorda tympani.
FIG: 2The facial motor fibres exit at the stylomastoid foramen to supply the facial musculature through five main branches: the temporal, zygomatic, buccal, mandibular, and cervical branches
Facial nerve lesion above the geniculate ganglia causes more ocular symptoms as it affects both lacrimal gland secretion and orbicularis muscle tone.
Corresponding AuthorJoyeeta DasConsultant Orbit and Oculoplasty surgeonDisha Eye Hospitals, Barrackpore, Email: drjoey2007@gmail. com

December 2017 Bengal Ophthalmic Journal 27
Etiology of facial palsy
The main causes of facial palsy can be broadly divided into (a) Idiopathic (b) Infection (c) Traumatic (d) Neoplastic and (e) miscellaneous
a) Idiopathic
Bells’ palsy or idiopathic facial palsy is the most common cause of facial palsy which is a diagnosis of exclusion. Although considered idiopathic some evidence suggests that an underlying herpes simplex infection as probable cause. It accounts for more than half of all cause of facial palsy[1]. All ages can be affected but the incidence is highest between 15 to 45 years of age. Onset of Bells palsy is sudden unilateral facial palsy affecting all branches in equal fashion, whose deficits are fully evolved within 72 hours.
Recovery typically begins within 3 weeks however it may be delayed up to 6 months. If there is no improvement of muscle function by 6 months the clinician should suspect alternate pathology. Without treatment, 70% of patients with Bell’s palsy will recover to completely normal function, while 13% will recover with minor degrees of synkinesis, and 16% will recover with severe facial synkinesis with significant impairment of facial expression[2].
Oral corticosteroids are the mainstay of treatment in acute phase and should be started within 72 hours of onset of symptom. Corticosteroid with antiviral therapy promotes rapid recovery but only antiviral monotherapy is strongly not recommended.
b) Infections
Herpes zoster virus infection is a relatively common cause of facial palsy. Involvement of geniculate ganglion [Ramsey Hunt syndrome] characterized by vesicle in tympanic membrane and auditory canal with associated severe dermatomal pain. It is treated with high dose oral Acyclovir and corticosteroids.
Other infective causes are Lymes disease (Borelia burgdorferi), cytomegalovirus, mumps HIV, Leprosy etc.
c) Traumatic
Trauma is the second most common etiology of facial nerve paralysis, comprising 8–22% of cases[1]. A significant percentage of cases occur during delivery both in birth canal and during forceps delivery. Other causes of traumatic nerve injuries are surgical trauma, penetrating parotid or middle ear trauma, barotraumas, facial fractures, and temporal bone fractures. Primary end-to-end neurorrhaphy is the preferred management for transection injuries.
d) Neoplastic
Facial nerve palsy can result from direct compression, stretching of the nerve or infiltration tumor. Cerebello-pontine angle tumor causes multiple cranial nerve palsies. The most common intracranial tumors affecting facial nerve are acoustic neuroma meningioma. In case of children leukaemia should be rule out.
e) Miscellaneous
Other less common causes are CVA particularly basilar artery as well as brain stem. Myotonic dystrophy and Myasthenia, Sarcoidosis also causes facial palsy.
Examination
The assessment of a patient with facial nerve palsy begins with a thorough history. History of the onset, progress, and associated symptoms of newly acquired facial nerve palsy is extremely helpful in determining the potential cause of the palsy and serves as a guide for prognosis and timing of any necessary surgical intervention. History of herpes zoster, trauma, previous surgery and other systemic illness like diabetes mellitus etc should be asked.
Clinical features of facial palsy:
• Deviation of face to one side [FIG 3]• Weakness of both upper and lower facial muscles of
the affected side in LMN Palsy and only lower face [sparing the forehead] in UMN palsy
• Inability to close the eye -Lagophthalmos • Dry eye • Excessive tearing of the eye (epiphora)• Drooping of the corner of the mouth• Ipsilateral loss of taste sensation• Difficulty with eating due to ipsilateral muscle weakness• Increased sensitivity to sound (hyperacusis) on
affected side if stapedius muscle is involved
Examinations
i Upper eyelid
Evaluate upper eyelid retraction it contributes to lagophthalmos due to the unopposed action and tone of the levator and Muller’s muscles.
ii. Corneal sensation and Blink reflex
It should be carefully tested and compared to the normal side. Acute loss of corneal sensation indicates a severely guarded

Bengal Ophthalmic Journal28
prognosis for patients with facial palsy and demands aggressive treatment.
iii. Eyelid closure
Evaluate lagophthalmos on gentle and forced closure. This will dictate the extent and timing of medical and surgical intervention to protect the eye.
iv. Bell’s phenomenon
Patients with good Bell’s phenomenon may tolerate poor closure much better than those with poor Bell’s.
v. Lower eyelid
Evaluate paralytic ectropion particularly medial canthal tendon laxity.
vi. Midface
Evaluate midface position, nasolabial fold, cheek tone and elevation. Evaluate mouth symmetry, ability to drink and eat.
vii. Tear function
A Schirmer’s test is performed to determine tear production. Tearing may be decreased with facial nerve palsy or may be increased with aberrant regeneration or reflex tearing from ocular irritation secondary to exposure
viii. Synkinesis
Spontaneous twitching or cross innervations due to aberrant regeneration may occur in longstanding or recovering facial nerve palsy. The most noticeable areas of synkinesis involve the orbicularis oculi, nasolabial fold area, and mouth.
Indications for MRI in facial palsy1. Upper motor neuron palsy2. recurrent facial nerve palsy3. involvement of other cranial nerve4. no signs or recovery after 6 weeks5. children under 18 years
Facial nerve grading systems have been proposed by various Otolaryngology and neurology society for the assessment, quantification and monitoring of improvement of facial nerve function in clinical setup. Most widely used system is House-Brackmann Grading system endorsed by the American Academy of Otolaryngology in 1985. It has some limitations like poor inter-observer reliability, unable to reflect regional facial weakness in final grading and secondary complications inadequately defined. To overcome these pitfalls Facial Nerve Grading System 2. 0 has been proposed which can quantify regional nerve deficit and synkinesis more accurately. Another useful facial nerve grading system is SunnyBrook facial nerve grading.
House--Brackmann Grading System for Facial Palsy
Grade 1 Normal functionGrade 2 Mild dysfunctionGrade 3 Reduced forehead movement, noticeable
synkinesis and contractureGrade 4 No forehead movement, incomplete eye
closure, asymmetric mouth, disfiguring asymmetry
Grade 5 Minimal movement
Grade 6 No movement
Management
The management starts with thorough clinical history, followed by a comprehensive examination. The clinician should ascertain whether the paralysis is acute or chronic in onset, unilateral or bilateral, exclude secondary causes of facial palsy, and differentiate between UMN and LMN lesion. Ophthalmologist’s major concerns in facial palsy patient are poor eyelid closure and resultant corneal exposure.
The aim of management of Facial nerve palsy is protecting globe integrity using minimal intervention and maximizing convenience for the patient and maintaining good visual acuity. Treatment is undertaken in stages.
Acute stage facial palsy
In acute stage is the treatment aimed at
corneal protection
medical treatment to speed up recovery
a) Corneal protection
corneal protection options are depends on the predicted prognosis of return of nerve function and the degree of risk to the cornea based on the amount of lagophthalmos, the quality of Bell’s phenomenon, corneal reflex and the presence or absence of paralytic ectropion.
Intensive lubrication with preservative-free methylcellulose preparations is the mainstay of treatment in the early phases during the day and a more viscous petroleum based ointment overnight.
i. In case of poor Bells phenomenon where risk of corneal exposure is high attempts should made to close the eye and cover the cornea. Lid taping may be advised but should be done very carefully otherwise the tape may rub the cornea itself. To avoid this ‘X’ taping is better option. Moisture chamber is better option. In western world it is commercially as Protective eye bubble and

December 2017 Bengal Ophthalmic Journal 29
moisture Goggles [FIG 5]. Alternatively simple taping of cellophane paper over periocular area with tape is a low-cost readymade option. [FIG 4]
FIG 4: Moisture chamber with cellophane paper
FIG 5: Moisture goggle
ii. Inj Botulinum toxin A 5 units to temporally paralyse the LPS muscle and produce temporary ptosis to cover cornea is an option but disadvantage is obstruction of vision. It is also not recommended in cases where there is loss corneal sensation.
iii. Temporary tarsorraphy is another option to protect cornea but is kept as last option in acute stage management where Bells phenomenon is poor with associated loss of corneal reflex
(b) Medical Treatment
Oral corticosteroids within 72 hours of symptom onset in all patients with Bell’s palsy shorten the recovery time and improve long-term outcome. Oral prednisolone 60 mg per day [1mg per Kg body weight] for 5 days followed by 10 mg tapering every day over 5days is a standard protocol. Caution should be taken in case of uncontrolled diabetes mellitus.
Studies have found that combination of an antiviral and a corticosteroid reduces long-term sequelae of Bell’s palsy compared with a corticosteroid alone, especially in patients who initially present with complete facial palsy. The recommended antiviral doses are Oral Valacyclovir 500-1000 mg twice daily for 7 days or Acyclovir 400 mg 5 times a day for 10 days along with corticosteroid as above mentioned dose.
Late Stage Facial palsy
After acute phase is over when the chances of facial nerve recovery is low and in iatrogenic surgical transection of the nerve [in acoustic neuroma] where there is evidence of corneal damage, more permanent surgical management option are considered. Various forms of lid surgeries are advocated according to the degree of involvement of upper and lower lid which are divided into static and dynamic procedure. Dynamic procedures typically restore the movement to some extent where as static procedures improve lid position. All the surgical procedures are aimed to narrow the palpebral aperture which can be approached by
1. Lowering the upper lid
2. Elevation of lower lid
3. Medial or lateral canthal shortening
4. Temporalis muscle transfer and nerve grafting
1) Lowering the upper lid
Upper eye lid loading procedure is the most popular reanimation surgery first described by Illig in 1958 which become very popular worldwide over the years. Upper lid weight results in increased gravitational pull on the lid and levator palpebrae relaxation that passively help the paralyzed eyelid to close and reduce lagophthalmos, improve corneal coverage and decrease lubricant-dependence. Lid loading with 99. 9% pure gold is the most commonly performed surgery for Facial nerve palsy of any etiology. The advantages of the procedure are it is safe, has lower complication rate and equally effective in both early and later stages. It is reversible procedure, if the nerve function improves it can be taken out easily6. It has advantages over permanent tarsorrhaphy as it results better cosmesis, maintained binocular field of vision and improved blink amplitude. In case of gold intolerance platinum weights can be used as an alternative. [FIGURE 6]
Palpebral spring implantation[7, 9] is another option for closure of paralysed lid. A custom-made stainless steel spring is implanted and secured to the superior orbital rim and pretarsal area. When the opposite eye closes, the levator muscle relaxes and the spring actively pushes the eyelid down. An advantage of spring is the eyelid movement is rapid. but the major

Bengal Ophthalmic Journal30
disadvantages are that the procedure is technically difficult and complications like erosion and spontaneous extrusion may arise.
Lid retraction is another common phenomenon in facial nerve palsy which adds to lagophthalmos. Transconjunctival Muller’s muscle recession, anterior or posterior LPS recession and Mullerectomy are the surgical options which can be done alone or along with lid loading procedure according to the severity of lagophthalmos.
2) Elevation of lower lid
Late phase of facial nerve palsy is associated with lower lid laxity, ectropion, and lower lid retraction. The choice of surgical procedure will depend on the degree of laxity or ectropion and state of the medial and lateral canthal tendons. Increased support to raise the lower lid can be achieved by combining medial and lateral canthoplasties. The lateral tarsal strip has been the most commonly performed procedure for this purpose and frequently
works well. When there is significant lower lid retraction, it can be combined with insertion of a spacer (scleral graft or autologus hard palate). In cases of marked tissue atrophy, an autologus fascial sling can be sutured through the entire length of the lid and fixed to the medial canthal tendon and periosteum of lateral orbital rim [8, 9]
3) Medial or lateral canthal shortening
Laxity of the medial canthal tendon and punctal ectropion can be treated with a medial canthoplasty. In significant tendon laxity, a deep periosteal Royce-Johnston suture or medial wedge excision could be used.
4) Temporalis muscle transfer and nerve grafting
These are dynamic procedures done for restoration of facial movements and expression. It needs multidisciplinary participation of neurosurgeon, maxillofacial surgeon, and micro vascular surgeon.
Figure 6: [A]63 years old gentleman presented with left sided LMN facial nerve palsy post- Acuastic neuroma surgery 1 year back. [B] On presentation he had LE lagophthalmos with corneal exposure and lower lid ectropion. LE upper lid Gold weight (1. 42 gm) loading with lower lid lateral tarsal strip surgery done. [C, D] Post operative 6 months -LE no lagophthalmos and lid ectropion
A C
DB

December 2017 Bengal Ophthalmic Journal 31
Late Sequelae of Facial palsy
During regeneration of nerve, some aberrant nerves regenerate causing various synkinetic movements. These are Marin-Amat syndrome (lid closure on chewing movement), ‘Crocodile tears’ (tearing while chewing food) or Frey’s syndrome (sweating on cheek while chewing).
This can be managed by chemodenervation by injection Botulinum toxin, physiotherapy or surgery.
Summary
Facial nerve palsy may result devastating effect on visual function, if not properly managed. Prompt treatment should include detection of underlying cause(s), instillation of copious lubricants, and early intervention to protect cornea from exposure. Management of facial nerve palsy should be of multidisciplinary approach and should include inputs from other specialties to provide maximum benefit of the patient.
References
1. May M, Klein SR. Differential diagnosis of facial nerve palsy. Otolaryngol Clin North Am. 1991; 24:613–645
2. Peitersen E. The natural history of Bell palsy. Am J Otol. 1982;4:107-111
3. Gronseth GS, Paduga R; American Academy of Neurology. Evidence-based guideline update: steroids and antiviral for Bell palsy. Neurology. 2012;79:2209-2213
4. Sullivan FM, Swan IR, et al. Early treatment with prednisolone or acyclovir in Bell’s palsy. N Engl J Med. 2007;357:1598–1607.
5. Seiff SR, Chang Jr JS. The staged management of ophthalmic complications of facial nerve palsy. Ophthal Plast Reconstr Surg 1993;9:241–249.
6. Levine RE, Pulec JL. Eyelid reanimation with the palpebral spring after facial nerve graft surgery: an interdisciplinary approach. Ear Nose Throat J 1993;72:686–691
7. Rahman I, Sadiq SA. Ophthalmic management of facial nerve palsy: a review. Surv Ophthalmol 2007;52(2):121–44.
8. Lee V, Currie Z, Collin JR. Ophthalmic management of facial nerve palsy. Eye (Lond) 2004;18(12):1225–34.
9. Mavrikakis I. Facial nerve palsy: anatomy, etiology, evaluation, and management. Orbit 2008;27(6)

Original Article
Epidemiology of Benign Eyelid Lesions in Patients Presenting to A Teaching Hospital
Sonai Mukherjee DNB, Nidhi Priya MD, Sonu Goel DNB, MNAMSOrbit and Oculoplasty Services Anand Eye Centre, Jaipur, India
Introduction
Wide varieties of lesions affecting the eyelid are encountered within routine ophthalmology practice. These lesions are numerous due to the unique anatomical features of the eyelid as the whole skin structures, appendages, muscle, modified glands, and conjunctival mucous membrane are represented in the eyelid. Eyelid lesions can be divided into congenital, inflammatory, traumatic, or neoplastic (benign or malignant). Neoplastic lesions can be further classified according to their anatomical origin. A tentative clinical diagnosis based on the characteristic features is given then routinely confirmed by histopathological examination of the tissue specimen. The concern is the off chance histopathologic investigation which identifies a diagnosis different than the suspected clinical diagnosis with some diagnoses coming with deleterious
implications. Histopathologic evaluation enforces our clinical diagnostic skills and is extremely important in early detection of tumors, particularly in masquerade syndromes1, 2.
The relative frequencies of different benign eyelid lesions are variable from different locations in the world and are widely reported in the literatures. Therefore, this study was aimed at evaluating the relative frequency of benign eyelid lesions presented to a teaching hospital help clinicians prioritizing their presumed clinical diagnoses according to the commonly presented lesions in the community. We also highlighted the most characteristic clinical features helped the attending physician to catch up the exact diagnosis and the most likely alarming sign raised the possibility of unusual lid lesion.
Patients and methods
The histopathological reports of specimens obtained from patients with presumed benign eyelid lesions who were seen in a teaching hospital between January 2015 and December 2015 were reviewed. Patient age, gender, clinical features, indication for biopsy, surgical findings, and pre-excision clinical diagnosis (PECD) were retrieved. Special attention was focused on the
Corresponding AuthorSonai MukherjeeSenior Resident Oculoplasty Services, Anand Eye Hospital. Jaipur, IndiaEmail: sonaimarch1@gmail. com
Abstract
PurposeThis study evaluates the relative frequency of benign eyelid lesions presented to a teaching hospital in Rajasthan, India.
Patients and methodsCharts of patients with benign eyelid lesions were retrospectively reviewed from January 2015 to December 2015. Clinical details included demographic data, symptoms and signs, surgical findings, primary diagnosis, and indication for biopsy were analyzed in a histopathologically confirmed benign eyelid lesions. Eyelid lesions were arranged according to their order of frequencies.
ResultsA total of 87 biopsies were evaluated from 87 patients (male 39. 2% and female 60. 8%). The age of the patient at the time of biopsy ranged from 2 to 87 years old. The most common benign eyelid lesion encountered in our practice was sweat gland hidrocystoma followed by chalazion, skin tag, epidermal cyst, nevus, seborrheic keratosis, xanthelasma, and molluscum contagiosum respectively. Histopathological studies confirmed the clinical diagnosis in 95. 9% of specimens and was different from the clinical diagnosis in 4. 1% of the lesions which included seborrheic keratosis (n = 3), pilomatrixoma, steatocystoma, hemangioendothelioma, juvenile xanthogranuloma.
ConclusionSweat gland hidrocystoma with classical clinical features and straightforward diagnosis is the most frequent lesion in our series which could be due to characteristic dry climate. Keywords: Epidemiology, Eyelid, Benign, Lesions
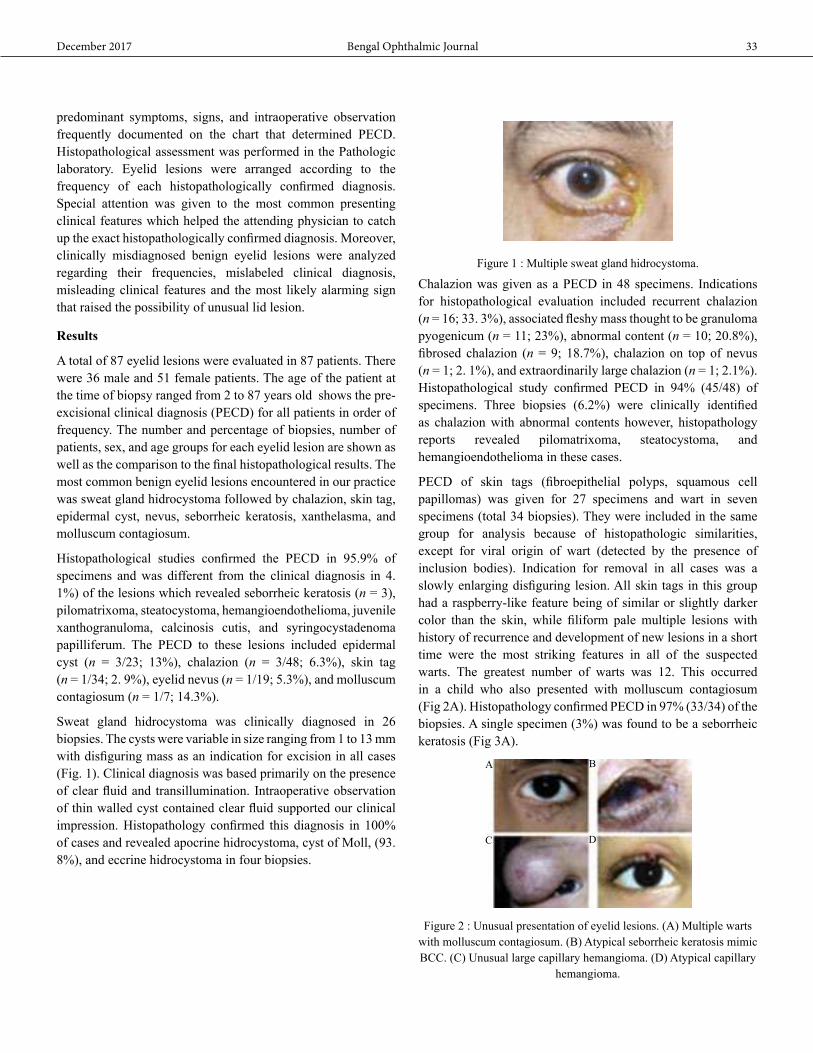
December 2017 Bengal Ophthalmic Journal 33
predominant symptoms, signs, and intraoperative observation frequently documented on the chart that determined PECD. Histopathological assessment was performed in the Pathologic laboratory. Eyelid lesions were arranged according to the frequency of each histopathologically confirmed diagnosis. Special attention was given to the most common presenting clinical features which helped the attending physician to catch up the exact histopathologically confirmed diagnosis. Moreover, clinically misdiagnosed benign eyelid lesions were analyzed regarding their frequencies, mislabeled clinical diagnosis, misleading clinical features and the most likely alarming sign that raised the possibility of unusual lid lesion.
Results
A total of 87 eyelid lesions were evaluated in 87 patients. There were 36 male and 51 female patients. The age of the patient at the time of biopsy ranged from 2 to 87 years old shows the pre-excisional clinical diagnosis (PECD) for all patients in order of frequency. The number and percentage of biopsies, number of patients, sex, and age groups for each eyelid lesion are shown as well as the comparison to the final histopathological results. The most common benign eyelid lesions encountered in our practice was sweat gland hidrocystoma followed by chalazion, skin tag, epidermal cyst, nevus, seborrheic keratosis, xanthelasma, and molluscum contagiosum.
Histopathological studies confirmed the PECD in 95.9% of specimens and was different from the clinical diagnosis in 4. 1%) of the lesions which revealed seborrheic keratosis (n = 3), pilomatrixoma, steatocystoma, hemangioendothelioma, juvenile xanthogranuloma, calcinosis cutis, and syringocystadenoma papilliferum. The PECD to these lesions included epidermal cyst (n = 3/23; 13%), chalazion (n = 3/48; 6.3%), skin tag (n = 1/34; 2. 9%), eyelid nevus (n = 1/19; 5.3%), and molluscum contagiosum (n = 1/7; 14.3%).
Sweat gland hidrocystoma was clinically diagnosed in 26 biopsies. The cysts were variable in size ranging from 1 to 13 mm with disfiguring mass as an indication for excision in all cases (Fig. 1). Clinical diagnosis was based primarily on the presence of clear fluid and transillumination. Intraoperative observation of thin walled cyst contained clear fluid supported our clinical impression. Histopathology confirmed this diagnosis in 100% of cases and revealed apocrine hidrocystoma, cyst of Moll, (93. 8%), and eccrine hidrocystoma in four biopsies.
Figure 1 : Multiple sweat gland hidrocystoma.
Chalazion was given as a PECD in 48 specimens. Indications for histopathological evaluation included recurrent chalazion (n = 16; 33. 3%), associated fleshy mass thought to be granuloma pyogenicum (n = 11; 23%), abnormal content (n = 10; 20.8%), fibrosed chalazion (n = 9; 18.7%), chalazion on top of nevus (n = 1; 2. 1%), and extraordinarily large chalazion (n = 1; 2.1%). Histopathological study confirmed PECD in 94% (45/48) of specimens. Three biopsies (6.2%) were clinically identified as chalazion with abnormal contents however, histopathology reports revealed pilomatrixoma, steatocystoma, and hemangioendothelioma in these cases.
PECD of skin tags (fibroepithelial polyps, squamous cell papillomas) was given for 27 specimens and wart in seven specimens (total 34 biopsies). They were included in the same group for analysis because of histopathologic similarities, except for viral origin of wart (detected by the presence of inclusion bodies). Indication for removal in all cases was a slowly enlarging disfiguring lesion. All skin tags in this group had a raspberry-like feature being of similar or slightly darker color than the skin, while filiform pale multiple lesions with history of recurrence and development of new lesions in a short time were the most striking features in all of the suspected warts. The greatest number of warts was 12. This occurred in a child who also presented with molluscum contagiosum (Fig 2A). Histopathology confirmed PECD in 97% (33/34) of the biopsies. A single specimen (3%) was found to be a seborrheic keratosis (Fig 3A).
Figure 2 : Unusual presentation of eyelid lesions. (A) Multiple warts with molluscum contagiosum. (B) Atypical seborrheic keratosis mimic BCC. (C) Unusual large capillary hemangioma. (D) Atypical capillary
hemangioma.
A
C
B
D

Bengal Ophthalmic Journal34
Figure 3 : Unexpected diagnosis. (A) Seborrheic keratosis misdiagnosed as fibroepithelial polyp. (B) Juvenile xanthogranuloma
misdiagnosed as epidermal cyst.
PECD of epidermal and epidermal inclusion cysts were postulated in 23 specimens. History of trauma was given in three patients which raised the possibility of epidermal inclusion cyst. Histopathology confirmed the PECD in 87% (20/23) of the lesions with typical yellowish, well circumscribed lesion with intraoperative observation of clear line of cleavage between the cyst and surrounding tissue and yellowish sequestrated content. Three specimens (13%) were histopathologically different from PECD that included juvenile xanthogranuloma involving the eyelid margin in a 43-year-old female (Fig 3B), calcinosis cutis in a 12-year-old girl, and seborrheic keratosis in a 63-year-old female.
PECD of eyelid nevi was given in 19 specimens; five of these were non-pigmented. Indications for excision included cosmetic reasons (n = 13), increase of lesion size (n = 3), inflamed nevus (n = 2), and itching with bleeding (n = 1). Histopathology reports revealed 16 intradermal nevi (84.2%) and two junctional nevi while seborrheic keratosis was reported in one biopsy (5. 3%) from a female patient age 43 years old with right upper and lower eyelid non-pigmented lesions, one of which proved to be an intradermal nevus.
PECD of seborrheic keratosis was given in 11 specimens. An isolated lesion was present in six patients and multiple in two. The clinical presentation was variable. Nine lesions were non-pigmented. Most lesions were cauliflower-like greasy masses (n = 7), others were sessile lesions (Fig 2B) mimicking basal cell carcinoma (n = 3), or rarely painless yellowish dome-shaped swelling mimicking an epidermal cyst (n = 1). Histopathological examinations confirmed the PECD in 100% of the lesions with two lesions confirmed as a variant of seborrheic keratosis (Inverted Follicular Keratosis, IFK).
Xanthelasma was a suspected PECD in eight patients. All eyelids were involved in four patients with upper lids being more severely affected. Three patients had only bilateral upper lid involvement and one had unilateral upper lid involvement with a history of surgical trauma. Histopathological studies confirmed the PECD in 100% of the lesions.
Molluscum contagiosum was suspected clinically in seven biopsies from three pediatric patients and one adult. Multiple
lesions were present in two children. Histopathology confirmed the clinical diagnosis in six biopsies with one biopsy which revealed syringocystadenoma papilliferum in the lone adult patient.
Excisional biopsy was performed in two children with a PECD of capillary hemangioma. This was done because of large lesion in one patient with severe ptosis (Fig 2C), the other had an atypical presentation of a pedunculated, rapidly enlarging lesion with bleeding (Fig 2D). Histopathology findings confirmed the clinical diagnosis of lobular capillary hemangioma in both cases.
PECD of foreign body granuloma (n = 2), eyelid coloboma (n = 1), traumatic eyelid notch (n = 1), and local lid margin fibrosis after radiofrequency electrolysis (n = 1) were each confirmed histologically.
Discussion
In clinical practice, we encounter different lesions affecting the eyelid, mostly are benign but some have malignant potentials or frank malignant features. The incidence of such lesions has been widely reported by different previous studies. 3, 7, 10, 16 In our study, none of the clinically expected benign lesion was proved to be malignant or premalignant, which is different from previous studies, however high index of suspicious and relatively low incidence of malignant lesions could explain such a difference5, 7, 10, 12. Nevertheless, nine benign eyelid lesions (4.1%) were misdiagnosed clinically and proved by histopathology study to be another entity of benign lesions which is higher than Kersten (2.3%) and less than Özdal (6.4%) studies10, 17. The result of this study revealed sweat gland hidrocystoma as the most common benign eyelid lesion encountered in our practice followed by chalazion, squamous papilloma, epidermal cyst, and eyelid nevus respectively. The most common benign eyelid lesion was variably reported in previous literatures from different countries; Kersten (United State) and Ni (China) reported papilloma (43.9% and 27.9%, respectively), Chi and Beak (South Korea) found nevus (57.1%), while Hsu and Lin (Taiwan) documented epidermal cyst as the most common benign eyelid lesion (23.1%)3, 7, 10, 16.
Sweat gland hidrocystoma was the most common lesion in this series (29. 3%). Dry climate in the central province in North western part of India leaves open the question whether excessive stimulation of the sweat gland may play a role in having higher frequency of hidrocystoma in our study. Histopathologic study confirmed PECD in all cases due to classical presentation of a clear cystic lesion along the lid margin, making the clinical diagnosis straightforward13, 20, 22. Nevertheless, some eccrine variety is confusing and the value of the histopathology study comes out to differentiate it from epidermal cyst which is another entity of benign lesion with no malignant potential22.
A B

December 2017 Bengal Ophthalmic Journal 35
Chalazion is the most common lid lesion faced by the ophthalmologist13, 24, 27, but it was the second most common benign lesion in our series (21.6%) due to referral nature of our tertiary hospital. Recurrent chalazion was the most common indication for chalazion biopsy as sebaceous cell carcinoma (SGC) was always included as a differential diagnosis as some cases of SGC can mimic this lesion17. One study reported as much as 20% of sebaceous carcinomas were initially misdiagnosed as recurrent chalazion21. Having mentioned that, any abnormal content or tissue proliferation is an alarming sign which necessitates histopathologic evaluation. In this series, intraoperative observation of abnormal content raised the possibility of differential diagnosis and actually all cases of rare eyelid tumors namely pilomatrixoma, steatocystoma, and hemangioendothelioma were included in this category.
Papillomatous skin lesions is a wide descriptive name rather than a true clinical diagnosis that makes them very tricky. The lack of clear clinical sub-classification may lead to misdiagnosis or even mislabel malignant lesions as benign ones10. In this study, skin tags, warts and seborrheic keratosis were specifically mentioned clinically and clearly evaluated as separate subgroups of the papillomatous lesions, therefore no malignant lesion has been unexpectedly diagnosed. Despite differentiation between subgroups, altogether (45 biopsies; 20.3%) were the third frequent lesions in this series. Skin tags represented 15. 3% of all biopsied lesions. The presence of the characteristic raspberry-like surface with almost the same or slightly darker color as the skin was the most common pathognomonic sign, and when present, always had a confirmatory histopathological diagnosis9, 13, 14, 27. This clinical feature was absent in one case which was histopathologically proved to be seborrheic keratosis. Histopathologic evaluation of wart (verruca) is important in terms of eradication of the disease and prevention of spreading of this papillomatous lesion as it has viral origin27. Seborrheic keratosis(basal cell papilloma) is another papillomatous lesion which can mimic other benign and malignant lid lesions10, 14. Three cases of histopathologically confirmed seborrheic keratosis were clinically felt to be a skin tag, an epidermal cyst, and an eyelid nevus. Therefore given its clinical variability in this series, histopathological study is extremely helpful any time this diagnosis is considered.
Nevus was not that common in our series due to the tertiary service nature of our hospital and referral policy. Ni reported pigmented nevi as the second leading lesions in his series (24. 4%)16. In our study, intradermal nevi were reported in the vast majority of eyelid nevi that have no malignant potential (n = 16; 84. 2%), while junctional nevus, which has low malignant potential, was reported in two biopsies (10. 5%). Chi and Beak
reported same frequencies, while compound nevus was the most common one reported by Hsu and Lin3, 7.
Xanthelasma has a typical presentation and very rarely requires consideration for a differential diagnosis and yet omitted from most of the studies dealing with eyelid lesions6, 18. In this series, there was only one case in which presumed xanthelasma was part of a differential diagnosis as it was a unilateral lesion with a history of previous surgical trauma that raised the possibility of necrobiotic xanthogranuloma which has been reported before28.
Molluscum contagiosum has peculiar clinical feature with high accuracy of clinical diagnosis9, 19, 27. All our cases were reported in the pediatric age group, occurring in otherwise normal children, with the exception of the unexpectedly diagnosed syringocystadenoma papilliferum that occurred in the middle aged female.
Capillary hemangioma is frequently seen in pediatric population but rarely treated by surgical excision which explains the rarity of such a lesion in our study4, 23. However, one of our cases was large, localized and amenable to excision with meticulous hemostasis. The other one was a rapidly growing, pedunculated, red lesion with bleeding, which placed keratoacanthoma in the differential diagnosis. Biopsy was essential to confirm the diagnosis and to exclude other vascular lesions with recurrence potential such as a hemangioendothelioma or tufted angioma8, 11, 25.
Foreign body granuloma, coloboma, traumatic eyelid notch, and post-electrolysis fibrosis were rarely reported in this series as well as others.
Conflicts of Interest- NoneFinancial disclosures- None
References
1. Al-Malki S., Al-Faky Y. H., Al-Rikabi A. C. Bilateral subepidermal calcified nodule of the eyelid. Saudi J Ophthalmol. 2011;25(1):81–83. [PMC free article] [PubMed]
2. Chalfin S., Lloyd W. C., 3rd Juvenile xanthogranuloma of the eyelid in an adult. Arch Ophthalmol. 1998;116(11):1546–1547. [PubMed]
3. Chi M. J., Beak S. H. Clinical analysis of benign eyelid and conjunctival tumors. Ophthalmologica. 2006;220:43–51. [PubMed]
4. Deans R. M., Harris G. J., Kivlin J. D. Surgical dissection of capillary hemangiomas. An alternative to intralesional corticosteroids. Arch Ophthalmol. 1992;110(12):1743–1747. [PubMed]

Bengal Ophthalmic Journal36
5. Glatt H. J., Olson J. J., Putterman A. M. Conventional frozen sections in periocular basal-cell carcinoma: a review of 236 cases. Ophthalmic Surg. 1992;23(1):6–9. [PubMed]
6. Harry J., Misson G. Clinical ophthalmic pathology: principles of diseases of the eye and associated structures. Butterworth–Heinemann. 2001;4:205.
7. Hsu H. C., Lin H. F. Eyelid tumors in children: a clinicopathologic study of a 10-year review in southern Taiwan. Ophthalmologica. 2004;218:274–277. [PubMed]
8. Jones E. W., Orkin M. Tufted angioma (angioblastoma). A benign progressive angioma, not to be confused with Kaposi’s sarcoma or low-grade angiosarcoma. J Am Acad Dermatol. 1989;20:214–225. [PubMed]
9. Kanski J. J. 4th ed. Butterworth–Heinemann; Oxford: 1999. Clinical ophthalmology a systematic approach. p. 15, 62–3.
10. Kersten R. C., Ewing-Chow D., Kulwin D. R., Gallon M. Accuracy of clinical diagnosis of cutaneous eyelid lesions. Ophthalmology. 1997;104(3):479–484. [PubMed]
11. Lee B., Chiu M., Soriano T., Craft N. Adult-onset tufted angioma: a case report and review of the literature. Cutis. 2006;78(5):341–345. [PubMed]
12. Lin H. Y., Cheng C. Y., Hsu W. M., Kao W. H., Chou P. Incidence of eyelid cancers in Taiwan: a 21-year review. Ophthalmology. 2006;113(11):2101–2107. [PubMed]
13. Nerad J. A. vol. 10. C. V. Mosby Co. ; St. Louis: 2005. (Oculoplastic surgery: the requisites in ophthalmology). p. 271–72.
14. Nesi F. A., Lishman R. D., Levine M. R. 2nd ed. vol. 27. Mosby-Year Book Inc. ; 1998. (Ophthalmic plastic and reconstructive surgery). p. 498–9 (848, 494)
15. Nguyen J., Jakobiec F. A., Hanna E., Fay A. Subepidermal calcified nodule of the eyelid. Ophthal Plast Reconstr Surg. 2008;24(6):494–495. [PubMed]
16. Ni Z. Histopathological classification of 3510 cases with eyelid tumor. Zhonghua Yan Ke Za Zhi. 1996;32(6):435–437. [PubMed]
17. Özdal PÇ, Codère F. Accuracy of the clinical diagnosis of chalazion. Eye. 2004;18:135–138. [PubMed]
18. Rayner S. A., Duncombe A. S., Keefe M., Theaker J., Manners R. M. Necrobiotic xanthogranuloma occurring in an eyelid scar. Orbit. 2008;27(3):191–194. [PubMed]
19. Redmond R. M. Molluscum contagiosum is not always benign. BMJ. 2004;329(7462):403. [PMC free article] [PubMed]
20. Shields J. A., Eagle R. C. Apocrine hidrocystoma of the eyelid. Arch Ophthalmol. 1993;111:866–867. [PubMed]
21. Shields J. A., Demirci H. Sebaceous carcinoma of the eyelids, personal experience with 60 cases. Ophthalmology. 2004;111:2151–2157. [PubMed]
22. Singh A. D., McCloskey L. Eccrine hidrocystoma of the eyelid. Eye. 2005;19:77–79. [PubMed]
23. Slaughter K., Sullivan T., Boulton J. Early surgical intervention as definitive treatment for ocular adnexal capillary haemangioma. Clin Exp Ophthalmol. 2003;31(5):418–423. [PubMed]
24. Tran D. T., Wolgamot G. M., Olerud J., Hurst S., Argenyi Z. An ‘eruptive’ variant of juvenile xanthogranuloma associated with langerhans cell histiocytosis. J Cutan Pathol. 2008;35(Suppl. 1):50–54. [PubMed]
25. Vanhooteghem O., André J., Bruderer P., Touma D., Benkirane F., Song M. Tufted angioma, a particular form of angioma. Dermatology. 1997;194(4):402–404. [PubMed]
26. Vick V. L., Wilson M. W., Fleming J. C., Haik B. G. Orbital and eyelid manifestations of xanthogranulomatous diseases. Orbit. 2006;25(3):221–225. [PubMed]
27. Yanoff M., Fine B. S. Ocular pathology. 5th ed. vol. 17. Mosby Inc. ; 2002. (Ocular melanocytic tumors). p. 641–51 (6 (185), p. 193–4)
28. Zoumalan C. I., Erb M. H., Rao N. A., See R., Bernstine M. A., Shah S. B. Periorbital. Xanthogranuloma after blepharoplasty. Br J Ophthalmol. 2007;91(8):1088–1089. [PMC free article] [PubMed]

Original Article
Introduction: External DCR is a widely acceptable and common surgical procedure for primary acquired nasolacrimal duct obstruction in which a communication between the lacrimal sac mucosa and nasal mucosa is created[1]. Despite meticulous surgery, failures are often met with. The two most common causes of DCR failure are common canalicular obstruction and obstruction at the rhinostomy site[2]. Besides poor surgical technique, non-opening of the lacrimal sac (very rare), also contributes significantly to its failures. Some studies in the literature report failed External DCR rates of 5–10%[3-5] to 35–40%[6-8]. Placement of stents at the osteotomy site are thought to increase the success of the procedure. Use of silicone tube is a useful adjunct for performing repeat DCR in failed cases. Here, we tried to find out the efficacy of silicone tube intubation in failed DCR cases.
Material and methods: Records of 24 patients who underwent re-DCR procedures during march 2015 to december 2015 were gathered from our department files, retrospectively. All patients were operated on by the same surgeon under local anesthesia. All patients were suffering from epiphora. There was no trauma history in any of the patients before the epiphora occurred and no ocular abnormalities. Preoperatively, after a standard ocular examination including visual acuity, biomicroscopic anterior segment and fundus examination, to confirm nasolacrimal duct obstruction, nasolacrimal duct irrigation and dacryocystogram
was done, and obstruction seen in all patients. All patients consulted an ear, nose and throat (ENT) specialist to detect any nasal pathology.
During surgery a J-shaped skin incision was made with a surgical knife over the sac area. The periosteum overlying the lacrimal fossa and the area above were elevated with a periosteum elevator. Full exposure of lacrimal sac area was done and previously made bony ostium enlarged (Image 1). The site was cleared of any fibrous scar etc. After that silicone tube was introduced through both the puncta and ends are sutured within nostril (Image 2 and 3). After controlling hemorrhage, the subcutaneous tissue and skin were sutured using 6. 0 vicryl in a continuous fashion. Injection triamcinolone acetate was used particularly in patients who had excessive granulation tissue at the surgical area, especially surrounding the sac and previous flaps. A nasal pack with antibiotic ointment was placed at the end of the surgery. Postoperatively, patients were given amoxicillin-clavulanate and NSAID for 7 days and local gentamycin-dexamethasone and ketorolac eye drops for 2 weeks. The skin sutures were removed after 7 days. The silicone tube was removed at least after 6 months. The patients were followed up at the 1st week and 1, 3, 6 and 12 months. The patients who were followed up less than 3 months were excluded from the study.
Successful re-DCR was defined as relief of symptoms and an open passage at nasolacrimal syringing.
Results
Among 24 patients 15 are female (62. 5%), 9 are male (37. 5%). Age varies from 23 to 57 years. In 14 cases procedure performed in right side and rest in left side.
A Retrospective Study of Outcome of Repeat DCR with Silicone Tube Intubation in A Tertiary Care Hospital
Prantik Maity. MS, Kalishankar Das. MS, Nabanita Barua. DO, DNB, FICO Orbit and Oculoplasty Services, Department of Ophthalmology
Nilratan Sircar Medical College & Hospital, Kolkata
Corresponding AuthorNabanita BaruaRMO cum Clinical tutor, Nilratan Sircar Medical College & Hospital, KolkataE-mail: nabanita_br@yahoo. co. in
Abstract: Use of silicone tube is an useful adjunct for performing repeat dacryocystorhinostomy(DCR) in failed DCR cases. Records of Twenty four patients of chronic dacryocystitis who were operated(external DCR) during a period of six months to two years were studied. Repeat DCR with silicone tube intubation was performed in all the patients. Post-operative follow-up for a period of 12 months revealed asymptomatic 20 patients while 2 patients persisted with watering and discharge despite uncomplicated surgical procedure. One patient had spontaneous extrusion and 1 had medial migration of tube. Repeat DCR with silicone tube intubation is a very safe and can be used in day to day practice.
Key Words
Failed dacryocystorhinostomy (DCR), Silicone tube intubation

Bengal Ophthalmic Journal38
No complain of epiphora, discharge or regurgitation was found postoperatively in 20 patients (83.33%). 1 patient (4.2%) had persistent discharge and had to undergo premature tube removal. In 2 patients (8.3%), there was spontaneous extrusion of tube but the patient was found to be asymptomatic. 1 patient (4. 2%) had medial migration of tube due to punctual splitting.
Discussion
DCR with silicone tube intubation has been accepted as a highly successful procedure in patients with history of epiphora and discharge following chronic dacryocystitis. A review of literature reveals a success rate of 90 - 95%[9-11].
Failure of DCR may be attributed mainly to anastomosis, failure due to defective identification and apposition, sagging down of flap anastomosis, closure between two flap complex, ostium closure and common canalicular closure.
Mc Pherson and Egelston noted that 3 out of 7 patients in their study who underwent a second operation were found to have a dense scar tissue present at the osteotomy site[12]. In our study however, 17 out of 24 patients were found to have a dense fibrous scar closure of the bony ostium. This stresses upon the need of making a comparatively big osteotomy hole. Linberg and colleagues documented that surgically created ostia (average 11. 84 mm diameter) undergo dramatic narrowing during the first few months of healing (average 1.80 mm diameter post-operatively)[13]. Thus complete ostium closure remains a frequent concern among DCR failures. Pico stated that in every instance, the cause of failure was found at the second surgery to be an obstruction of the new drainage channel by an occluding membrane, which on histologic examination was shown to be composed of organized granulation tissue[14] .
In our study, obstruction of the common canalicular end was the cause of primary DCR failure in 7 patients. Mc Lachlan et. al. also proposed the higher incidence of common canalicular obstruction as a cause of DCR failure[15].
Conclusion
Repeat DCR with silicone tube intubation is a very safe and effective procedure for failed DCR and can be used in day to day practice.
Conflicts of Interest- NoneFinancial disclosures- None
References
1. Go Y, Park J, Kim K, Lee S. Comparison of nonlaser endoscopic endonasal revision surgery and diode laser transcanalicular revision surgery for failed dacryocystorhinostomy. J
Craniofac Surg. 2015;26(3):863–866.
2. Welham RAN, Henderson PH. Results of DCR analysis of causes of failure. Trans Ophthalmol Soc UK 1973 ; 93: 601
3. McMurray CJ, McNab AA, Selva D. Late failure of dacryocystorhinostomy. Ophthal Plast Reconstr Surg. 2011;27(2):99–101.
4. Hartikainen J, Antila J, Varpula M, Puuka P, Seppa H, Grenman R. Prospective randomized comparison of endonasal endoscopic dacryocystorhinostomy and external dacryocystorhinostomy. Laryngoscope. 1998;108:1861–1866.
5. Hartikainen J, Grenman R, Puukka P, Seppa H. Prospective randomized comparison of endonasal endoscopic dacryocystorhinostomy and external dacryocystorhinostomy. Ophthalmology. 1998;105:1106–1113.
6. Tarbet KJ, Custer PL. External dacryocystorhinostomy: surgical success, patient satisfaction and economic cost. Ophthalmology. 1995;102:1065–1070.
7. Yung MW, Hardman-Lea S. Analysis of the results of surgical endoscopic dacryocystorhinostomy: effect of the level of obstruction. Br J Ophthalmol. 2002;86(7):792–794.
8. Durvasula V, Gatland DJ. Endoscopic dacryocystorhinostomy: long-term results and evolution of surgical technique. J Laryngol Otol. 2004;118:628–632.
9. Tarbet KJ, Custer PL. External DCR : surgical causes, patient satisfaction and economic cost. Ophthalmology 1995;102 : 1065-67
10. Wallant MJ, Rose JE. Factors affecting the success rate of open lacrimal surgery. Br J Ophthalmol 1994; 78: 888-91.
11. Becker BB. DCR without flaps. Ophthalmic Surg 1988 ;19 : 419-27
12. Mc Pherson SD, Egelston D. DCR: a review of 106 operations. Am J Ophthalmol 1959; 47: 328-31
13. Linberg JV, Anderson RL, Bumsted RM et al. Study of intranasal ostium external dacryocystorhinostomy. Arch Ophthalmol 1982 ; 100 : 1758-62.
14. Pico GA. Modified technique of external DCR. Am J Ophthalmol 1972; 72: 679-90.
15. Mclachlan DL, Shannon GM, Flanagan JC. Results of DCR analysis of the re-operation. Ophthalmic Surg 1980;11: 427-30.

December 2017 Bengal Ophthalmic Journal 39
Figure 2: Intubation set passed through lower punctum
Figure 1: Bony osteum enlarged and remnant of nasal mucosa
Figure 3: Bicanalicular intubation and suturing of soft tissue and muscle over tube

Original Article
Effect of Age on Adult Stereoacuity as Measured By Distance Randot Test- A Comparision Between Stereoacuity in
Pre-Presbyopic and Presbyopic Age Groups
Satabdi Nanda, MBBS, DNB 2ND YEAR RESIDENTAnuradha Chandra, MBBS, M. S., FAICO
Introduction
Stereopsis implies the ability to obtain an impression of depth by superimposition of two pictures of the same object taken from different angles. It is measures in seconds of arc. Lower the value, better the stereoscopic vision.
Purpose
To observe the change in stereoscopic acuity over a age span of 20-80 years in patients with vision better than or equal to 6/12. We aimed at finding normative data for Distant Randot stereoacuity in 3 age groups, 20-40, 40-60, 60-80 yrs and look for age related depression of values. Also, effect of presbyopia on stereopsis was observed. Comparision of stereoacuity in early cataractous and pseudophakic patients was done.
Setting
Cross-sectional study at a tertiary care hospital
Methods
The Distant Randot is a Polaroid vectographic book, presenting 2 shapes each of 4 disparities- 400, 200, 100 and 60 secs of arc viewed at 3m through polarizing glasses. The smallest disparity level at which the patient identifies the shapes is recorded as stereoacuity.
We administered the test to 125 patients with good vision (>=6/9), 50 in 20-40yrs, 50 in 40-60 yrs, 25 in 60-80yrs, and tabulated the results.
Results
Distance Randotscores from normal subjects have low variability within each age group. In the 20-40 age group, 54% had stereoacuity of 60”, 28% had 100” whereas in 40-60 age group, 46% had 60”, 24% had 100”, and 20% had 200”. Above 60yrs, stereoacuity declined to 200” in 60% patients.
Conclusion
Age-related deterioration in stereoacuity is reflected not only by a linear correlation between age and threshold but also by a catastrophic factor that produces more marked deterioration after age 60. Both factors are probably cerebral. The Distance Randot Stereotest is a sensitive measurement of binocular sensory status that may be useful in monitoring progression of strabismus and/or recovery following strabismus surgery. Due to lack of any normative data for distance stereopsis in the Indian population, this study can be taken forward with a larger sample.
Corresponding AuthorSatabdi Nanda Fellow Pediatric ophthalmologistInstitution: Dept of pediatric ophthalmology and strabismus, Susrut Eye foundation and Research centre. HB36A/1 Saltlake, sector 3, Kolkata 700109Email: docanu. oph@gmail. com

December 2017 Bengal Ophthalmic Journal 41
Introduction
Many studies have been conducted in the past to describe the stereopsis in the elderly, using a variety of tests like the TNO test, Frisby Davis test etc. A high incidence of deficient stereopsis has been described in population studies of elderly subjects, but this was often associated with poor vision in one eye1. These studies have not generally measured stereopsis across the full adult age range in normal subjects.
The Distant Randot is a Polaroid vectographic book with 8 pages, presenting 2 shapes each of 4 disparities- 400, 200, 100 and 60 secs of arc viewed at 3m through polarizing glasses. The smallest disparity level at which the patient identifies the shapes is recorded as stereoacuity. The advantages of the Distant Randot over the Frisby-Davis Distance test is that it doesn’t offer any monocular clues discouraging guessing. The FD2 is also large is size and cumbersome to handle.
A number of studies have described reduced stereoscopic function in older people, with one study describing a ‘‘catastrophic’’ drop in stereoacuity in some subjects over the age of 60 years. 2 This study aims at procuring normative data for distance stereopsis for age group 20-80 along with observing if there is any such rapid depletion of stereoscopy due to presbyopia or cataractous changes in the lens.
Aims and Objectives
● AIM- To study the Distant Randot Stereoacuity values in 100 patients of 20-60 years.
● Primary Objective To obtain normative data for 20-60yr olds in Distant Randot
Test To compare stereopsis values in pre-presbyopic and
presbyopic population. ● Secondary Objective To compare stereopsis values in phakic and pseudophakic
population. Method
It is a cross-sectional study of observational type with the entire data collected over the span of 2 months from 1st of March to 1st of May 2017. Sample size initially taken as 200 including patients with vision better than 6/12 which was later trimmed to 125 because the minimum visual acuity as brought down to 6/9. There are 50 patients each in 20-40, 41-60 yr agegroups and 25 in 61-80 yrs age group. The study as conducted at a tertiary eye care hospital. The study parameter taken is distance stereoacuity measured in seconds of an arc, by the standard Distant Randot Stereotest.
Distance Randot Stereotest Protocol
The Distance Randot Stereotest3 is a Polaroid vectographic book (21×17 cm), presenting 2 geometric shapes at each of 4 disparities: 400, 200, 100, and 60 arcsec. Subjects viewed the books at 3 meters in a normally illuminated room while wearing polarizing glasses (Stereo Optical Polarized Viewer). If the subject wore corrective spectacles, polarizing glasses were worn over his/her corrective lenses.
Pretest—The subject was asked to identify black-and-white pictures of the 4 geometric shapes (circle, triangle, square, and star) to confirm that they were able to name or match the shapes used in the test. The test proceeded only if the subject was able to name or match the shapes.
Test—Testing always began with the 400 arcsec level. If the subject passed the pretest but could not identify or match both shapes at the 400 arcsec level, the test was scored as nil. If both responses were correct, testing proceeded to 200 arcsec, and so on, untilthe subject made an error. The smallest disparity atwhich the subject identified or matchedboth shapes correctly was recorded as stereoacuity.
Patient Selection
Inclusion Criteria
1. Age 20-80yrs
2. BCVA >= 6/9
Exclusion Criteria
1. No ocular surgery other than cataract surgery
Data Tabulation
The data was tabulated basing upon the following-
• 3 age groups -20-40yrs, 41-60yrs, 61-80yrs
• Lens status- phakic, cataractous or pseudophakic
• Presbyopic correction whether or not needed
• Distant Randot Stereoacuity value
• Any other significant existing ocular pathology
Statistical Analysis
In the 20-40 age group, the mean value was found to be 86. 4 arcsec with standard error(SE) of 6. 45 arcsec. 95% of values range from 73. 75 to 99. 04 arcsec. There was 1 outlier.
In the 41-60 age group, the mean was 103. 90 arcsec with SE of 7. 56”.95% values lie between 84. 56-114. 12 arcsec with 3 nil values.

Bengal Ophthalmic Journal42
In the 61-80 age group, the mean was calculated to be 140. 13 arcsec with SE of 13. 25 arcsec. 95% values lie between 119. 10- 162. 71” with 2 nil values.
Discussion
Stereopsis is the ability to fuse images that have horizontally disparate retinal elements within Pannum’s fusional area resulting in binocular appreciation of object in depth. It implies the ability to obtain an impression of depth by super imposition of two pictures of the same object which have been taken from different angles4. It is measured in seconds of an arc. Stereopsis emerges early on in development at 3 to 6 months of life, continues to mature until about 10 years of age and declines in later life5.
Distance stereoscopy, the central topic of the study has been found to be sensitive to refractive error changes, hetereophoria and strabismus6. It is particularly important clinically, because clinical groups such as intermittent exotropes are more impaired on distance than near stereoacuity7. There are various tests for its measurement, Frisby- Davis test and Distant Randot test being the most commonly used. There is no use of monocular clues in Distant randot like in Frisby Davis test, hence the false positives are reduced. AO Vectographic method and Mentor B-VAT II video acuity tester are no longer put to use. 8
Stereopsis test for distance Equipment Stereopsis grade tested1. AO vectographic
project O-chart slidePhoropter with polarizing lenses 480-30 seconds of arc
2. Mentor B-Vat II Sag video acuity tester
Video system with monitor using Random dot E(BVRDE) and Contour circles (BVC)
240-15 seconds of arc
3. Frisby Davis Distance Stereotest (FD2 test)
Box with four translucent objects at varying distances
5-50 seconds of arc at 6 m
4. Distance Randot stereotest
3-dimensional polaroid vectograph and polaroid spectacles
400-60 seconds of arc
In the light of the currently undergoing demographic shift in the Indian population, there will be a growing proportion of the middle aged to elderly individuals. Also, in the present age, the levels of activity in these age groups has considerably increased because of greater consciousness. The elderly now have many more options for outdoor activities for which stereopsis and accurate depth perception is of prime concern.

December 2017 Bengal Ophthalmic Journal 43
Other than that, the Distant Randot stereoacuity test is a relatively new test which is underutilized in our country. No normative data is available for the indian population. No such
study has been found to have been conducted in West Bengal. So, lack of normative data makes it difficult to put the test to use. There are a few studies for normative data in children, but hardly any for adults across all age groups. Also, most of the previous studies fail to control for vision, considering that low vision will undeniably cause a drop in stereoacuity. For this reason, age-related changes in depth discrimination could reflect either ocular optical changes, changes in general neural pathways mediating many aspects of vision, or brain mechanisms restricted to depth discrimination or possibly just stereopsis.
In one of the earliest studies on stereopsis and ageing conducted by Wright and Wormald9, it was concluded that of 728 individuals over the age of 65, only 27% has full stereopsis and 29% had
no stereopsis, even without any significant ocular morbidity as measured by Frisby stereotest. The prevalence of decreased stereopsis increased with age.
In a study published in 2006, Garnham and Sloper10 compared various stereoacuity test (TNO, Frisby Near, Frisby Davis Distance, Titmus) values to check for variability. In all tests, results showed mild decline of stereoacuity with age, with more marked reduction in subjects above 55(only TNO test). Wang et. al11 published a study on normative data based on Distant Randot Test considering 156 volunteers(6-40yrs) and 77 strabismic patients (<65yrs). They opined that 96% of normal population had a stereoacuity of less than 100 arcsec, hereas in strabismic patients, 62. 3% had abnormal values. Also, there seemed to be low variability of stereoacuity within each group.
In our study, 125 subjects have been considered, 50 each in 20-40 and 40-60 yrs age group, and 25 in 60-80years age group. It is a cross sectional study of an observational nature. In the study, we consider subjects of acuity better than or equal to 6/9, hence controlling for vision. All patients who have been taken as subjects have never undergone any ocular surgery other than cataract surgery. Presbyopia has also been considered as a factor to compare stereoscopy. The lens status of the patient as noted as early cataract, normal or pseudophakic.
In our sample, 23 patients has early cataract (nuclear sclerosis grade 1 and/or cortical cataract), 19 patients were pseudophakic and 83 had completely normal lens status. Subjects with early cataractous lens has a slight decrease in the stereoacuity, mean being 127” as compared to early and pseudophakic population, which had nearly similar mean stereoacuity values. (98-102”)
14%
30%
27%
6%
0 PLATE 164
3 PLATES 197
INVALID 43
1 PLATE 104
2 PLATES 220
23%
Fig. 1. Crude prevalence of stereopsis grades in 728 individuals over 65 of age.
Fig. 2. Relative frequency of stereopsis grade by age group for those with N6 both eyes
65-69 70-74 75-79 80+ TOTAL
TOTAL 120 126 103 68 4173 PLATES 59 53 29 16 1572 PLATES 49 45 55 21 1701 PLATES 8 18 10 18 54NO PLATES 4 10 9 13 36
NO PLATES 1 PLATES 2 PLATES 3 PLATES
AGE GROUP
FREQUENCY
100%
75%
50%
25%
0%

Bengal Ophthalmic Journal44
Similarily, the entire group was divivded into presbyopes (86) and pre-presbyopes(39). Mean value of stereoacuity as measured in presbyopes was 122 “, which was almost 25-30% below the mean of the other group(82”).
Conclusion
In 20-40 age group, 84% had Stereoacuity <100 arcsec. There was a gradual but mild decline in older age, but still enough to be called as sufficient for daily work (most values<200). Presbyopes show a small fall in stereopsis. Early cataract with good vision causes a fall in stereopsis (~25%), but pseudophakia doesnt affect stereopsis. The normal distance stereopsis in Indian population >40 can be considered to lie between 100-200”.
The study also has a few limitations. One major limitation is the small sample size because of which the values show larger degree of variability. Had the sample size been larger, there
could have been lesser variability. Also, our study doesn’t take into consideration the near stereoacuity.
References
1 Fawcett, S., Stager, D. and Felius, J. Factors influencing stereoacuity outcomes in adults with acquired strabismus. American Journal of Ophthalmology 2004;138(6), pp. 931-935.
2 Jani SN. The age factor in stereopsis screening. Am J Optom Arch Am Acad Optom 1966;43:653–7.
3 WANG, J. The Final Version of the Distance Randot Stereotest: Normative data, reliability, and validity. JAAPOS 2010 ;14(2), p. 1.
4 Bhola, R. Binocular Vision. 2006. [online] Available at: http://webeye. ophth. uiowa. edu/eyeforum/tutorials/Bhola-BinocularVision. htm [Accessed 16 Nov. 2017].
5 Bohr I, Read JCA Stereoacuity with Frisby and Revised FD2 Stereo Tests. PLoS ONE 2013;8(12): e82999. doi:10. 1371/journal. pone. 0082999
6 Bohr, I. and Read, J. Stereoacuity with Frisby and Revised FD2 Stereo Tests. PLOS, 2013;p. 2.
7 Sharma, P. Strabismus simplified. New Delhi: CBS Publishers & Distributors. 2008.
8 Sharma, P. Strabismus simplified. New Delhi: CBS Publishers & Distributors 2008.
9 Wright, L. and Wormald, R. Stereopsis And Ageing. 1992;p. 1.
10 Garnham, L. and Sloper, J. Effect of Age on Stereoacuity. Br J Ophthalmology. 2006
11 Wang, J. The Final Version of the Distance Randot Stereotest: Normative data, reliability, and validity. JAAPOS 2010;14(2), p. 1.
Conflicts of Interest- NoneFinancial disclosures- None

Original Article
Introduction
Diplopia is a subjective complaint of seeing two images of a viewed object. It can arise from neurologic, ocular, or extraocular muscle disorders. Monocular diplopia is usually caused by a disorder in one eye, whereas binocular diplopia arises from ocular misalignment caused by either neurologic or ophthalmic disorders. The Hess test is a gold standard test evaluating patients with diplopia1.
It aids in the diagnosis of ocular motility defects. It measures the deviation and the amount of underaction and overaction of muscles. It is a repeatable and reliable record of the condition and is therefore a good way to show improvement or deterioration of the condition. The principleof Hess Chart is foveal projection. The chart is plotted based on the Hering’s and Sherrington’s law of innervation. The dissociation of two eyes is by the means of red green dissociative glasses and foster torches are used for projection of target. It helps in diagnosis of cause of diplopia. It differentiates between paralytic and restrictive squint. It also helps to assess the change over time. Management decisions like when to operate, which muscle to be touched and expected effect of treatment can be complemented by Hess Chart findings2, 3, 4.
Purpose
The aim of this study was to retrospectively analyse the hess charts and their interpretations and their clinical diagnoses. The purpose was to find the frequency of a particular diagnoses in the strabismus clinic.
Materials and methods
The study was conducted in the strabismus and pediatric ophthalmology clinic of tertiary eye hospital. The number of hess charts done at the clinic from may 2017 to july 2017 were collected. The data from the MRD number was collected and the diagnosis of each hess chart was corroborated with the clinical findings.
The test is performed with each eye fixating in turn. It is done at 50 cms. Patient wears red and green glasses. Left eye is tested first followed by right eye. The red glasses are placed on the right eye first (Red for right, R for R). The chart has electronically operated board with small red lights. The red lights can be illuminated as needed separately. The foster torch is of green light and is in patient’s hand. Patient is asked to place the green light in each of the points on the red light as illuminated on the chart. Next the goggles are changed and the left eye has red goggles and the eye to be tested is right eye. The recording is done first with the red glass over the red eye and repeated with red over the left eye. The eye that has the red glass is the fixing eye. The eye with the green glass is the eye being tested. The required points are joined to form an inner and the outer square. The patient’s head must remain straight through out the procedure/ test. Occasionally, it becomes necessary to hold the head in the correct position. The fovea of both eyes should have common visual direction.
Corresponding AuthorDr. Anuradha Chandra, Pediatric ophthalmologistInstitution: Dept of pediatric ophthalmology and strabismus, Susrut Eye foundation and Research centre. HB36A/1 Saltlake, sector 3, Kolkata 700109Email: docanu. oph@gmail. com
Abstract : Background: Hess chart helps in diagnosis of cause of diplopia. It differentiates between paralytic and restrictive squint. It also helps to assess the change over time. However often there is a lot of interobserver variability in interpretation of hess charts.
Purpose:The aim of this study was to retrospectively analyse the hess charts and their interpretations and their clinical diagnoses. The purpose was to find the frequency of a particular diagnoses in the strabismus clinic.
Methods: After the hess chart was done they were collected and retrospectively asked to be analysed by two different observers. Both the observers were blinded to te clinical findings and were asked to interpret the hess charts independently.
Interobserver variability was determined by taking the clinical diagnosis in the file as the true diagnosis.
Results: The nerve palsies were most commonly diagnosed cases of hess charts. There were large interobserver variability when restrictive squints were charted.
Conclusions: In our retrospective analysis of hess charts it was found that the typical presentations of paralytic squints can be easily interpreted by observing the pattern of hess chart only but when it comes to restrictive squints without clinical findings hess chart itself is of no value.
Analysis of Hess Charts and its interpretations
Chandra Anuradha M. B. B. S, M. S, F. A. I. C. O, Deshpande Vrushali M. B. B. S

Bengal Ophthalmic Journal46
The basic principle of Hess chart is foveal projection therefore the higher field belongs to the higher eye. This is opposite of diplopia charting where the higher image is of the lower eye. Position of the central dot indicates whether the deviation is in primary position or not. The position of the central dot is to be seen both fixing right eye and fixing left eye. The variation in the size of the Hess chart of each eye is due to the Hering’s law. Small field belongs to the eye with primary limitation of movement. Underaction can be seen with the inward movement of the dots and therefore the whole curve. Maximum displacement occurs in the direction of the affected muscle if the patient has presented early before the spread of comitance. Overaction can be seen by noting the outward displacement of the dots. Maximum displacement occurs in the direction of the main action of the overacting contralateral synergist in the larger field. Overaction can be seen by noting the outward displacement of the dots. Maximum displacement of the dots occurs in the direction of the main action of the overacting contralateral synergist in the larger field. If the inward and outward displacement is less marked, secondary underactions and overactions are present as a result of the development of muscle sequel. Outer field should be examined for small underactions and overactions which may not be apparent on the inner field. A narrow field restricted in opposing directions of movement denotes a mechanical restriction of ocular movement. Equal sized field denote either symmetrical limitation of movement in both eyes or a non paralytic strabismus. Each small square on the grid subtends 5 degrees at the working distance of 50 cm, therefore the amount of deviation can be calculated. In primary position, the amount could be calculated by fixing either eye by the displacement of the pointer from the centre dots. The amount of underaction and overaction can be calculated in the various positions and hence the amount of excursions can also be calculated. 5, 6
After the hess chart was done they were collected and retrospectively asked to be analysed by two different observers. Both the observers were blinded to the clinical findings and were asked to interpret the hess charts independently.
Interobserver variability was determined by taking the clinical diagnosis in the file as the true diagnosis.
Results
Total 39 hess charts were used for the study. The diagnoses were as follows:
Diagnoses Number Sixth nerve palsy 8Fourth nerve palsy 6Third nerve palsy 7Concomitant squint(acute) 6Thyroid ophthalmopathy 2Post cataract surgery inferior rectus paresis 2Post vr surgery restrictive squint 2Post trauma restrictive squint 3Internuclear ophthalmoplegia 3
Intraobserver variability
Diagnoses Number Observer 1
Observer 2
Sixth nerve palsy 8 8 7Fourth nerve palsy 6 5 3Third nerve palsy 7 7 7Concomitant squint(acute) 6 5 5Thyroid ophthalmopathy 2 0 0Post cataract surgery inferior rectus paresis
2 1 0
Post vr surgery restrictive squint
2 0 0
Post trauma restrictive squint
3 0 1
Internuclear ophthalmo-plegia
3 1 0

December 2017 Bengal Ophthalmic Journal 47
Discussion
General rules for interpretation of hess chart
1. Comparision of spaces between the two plotted fixation points indicates underaction of a muscle acting in that direction.
2. Expansion indicates overaction.
3. Smaller fields belongs to eye with paretic muscle. ws
4. Unaffected eye shows larger field expressing the overaction of the contralateral synergist.
5. Fields of similar shape and size seen in comitant deviation, while dissimilar shape and size indicate incomitance.
Hess chart in third Nerve palsy:
In general the eye affected shows underaction of medial rectus, superior rectus, inferior rectus and inferior oblique muscle and other eye will show overaction of all the muscles except medial rectus and inferior rectus.
For e. g. if the patient is having right sided third nerve palsy the hess chart will show the following characteristic findings:
• Contraction of right chart and expansion of left
• Right chart - underactions of all muscles except lateral rectus and superior oblique
• Left chart - overactions of all muscles except medial rectus and inferior oblique
Hess chart in fourth Nerve palsy
In this case Hess chart will show no significant difference in chart size. The chart will be seen tilted on one side. The affected side will show upward deviation due to underaction of superior oblique and overaction of inferior oblique muscle and other side will show downward deviation due to overaction of inferior rectus and underaction of superior rectus muscle.
For e. g. if the patient is having right side fourth nerve palsy the hess chart will show the following characteristic findings:
• Upward deviation of right fixation spot on inner chart (hypertropia)
• Downward deviation of left fixation spot on inner chart
• Right chart - underaction of superior oblique and overaction of inferior oblique
• Left chart - overaction of inferior rectus and underaction of superior rectus
Hess chart in sixth Nerve palsy
In sixth nerve palsy the hess chart will show underaction of lateral rectus muscle on that side and other side will show overaction of medial rectus muscle
For e. g. if the patient is having right side sixth nerve palsy the hess chart will show the following characteristic findings:
• Contraction of right chart and expansion of left
• Right chart - marked underaction of lateral rectus and mild overaction of medial rectus
• Left chart - marked overaction of medial rectus.
The nerve palsies in their acute state have very characteristic findings as innumerated above which helps the observer to clinch the diagnosis very easily and accurately. But once the nerve palsy is chronic there will be spread of comitance which leads to the muscle actions getting averaged and therefore the characteristic findings are lost. In these cases without observing the ductions and versions of the patient it is difficult to interpret the hess chart.
In restrictive squints the hess chart becomes more cumbersome to interpret. Though we know in thyroid ophthalmopathy the medial rectus and inferior rectus is involved, there are frequent instances the hess chart may not have characteristic findings. A post vitreoretinal surgery with bands often present with hess chart similar to thyroid ophthalmopathy. The duanes and congenital fibrosis syndromes again present with variable hess chart findings differing from case to case.
Therefore independent interpretation of hess charts are often not corroborating with the diagnosis.
Conclusion
All the nerve palsies were most frequent cases seen in Strabismus clinic.
In our retrospective analysis of hess charts it was found that the typical presentations of paralytic squints can be easily interpreted by observing the pattern of hess chart only but when it comes to restrictive squints without clinical findings hess chart itself is of no value.
Conflicts of Interest- NoneFinancial disclosures- None
References
1. Hess, W. Eine neue Untersuchungsmethode bei Doppelbildern. Arch Augenheilk. 1909;62:233–238
2. Roper-Hall, G. The Hess screen test. Am Orthopt J. 2006;56:166–174.
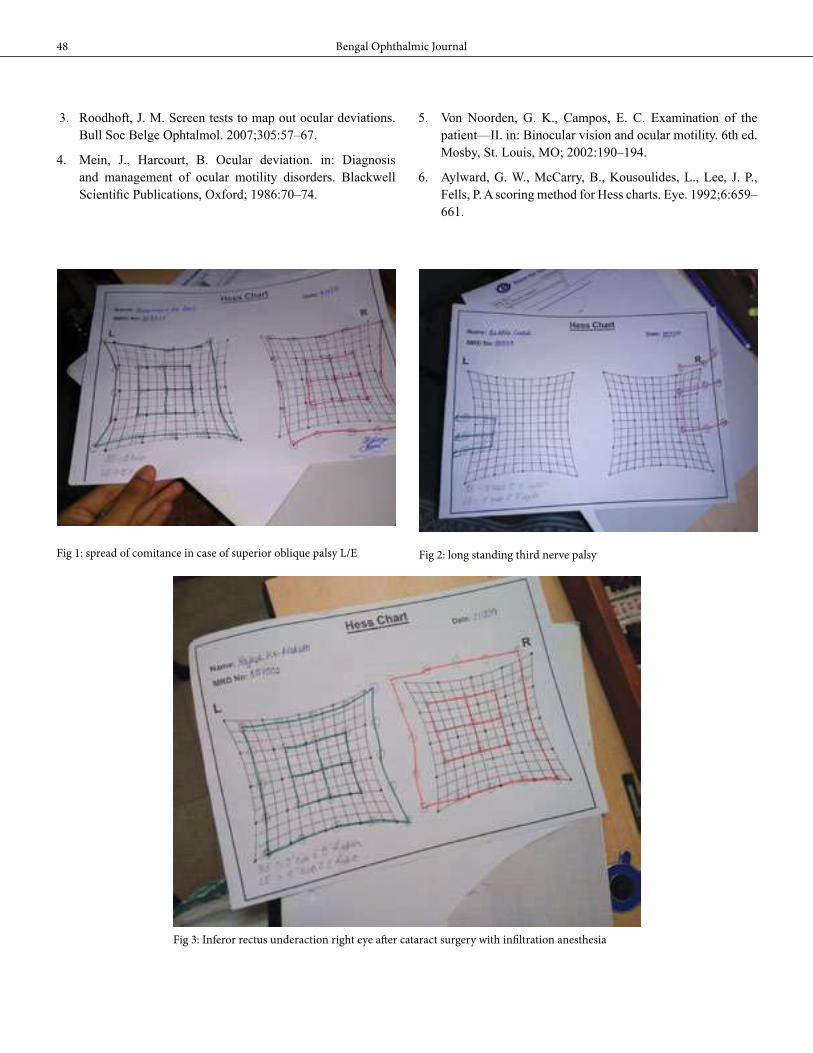
Bengal Ophthalmic Journal48
3. Roodhoft, J. M. Screen tests to map out ocular deviations. Bull Soc Belge Ophtalmol. 2007;305:57–67.
4. Mein, J., Harcourt, B. Ocular deviation. in: Diagnosis and management of ocular motility disorders. Blackwell Scientific Publications, Oxford; 1986:70–74.
Fig 1: spread of comitance in case of superior oblique palsy L/E Fig 2: long standing third nerve palsy
Fig 3: Inferor rectus underaction right eye after cataract surgery with infiltration anesthesia
5. Von Noorden, G. K., Campos, E. C. Examination of the patient—II. in: Binocular vision and ocular motility. 6th ed. Mosby, St. Louis, MO; 2002:190–194.
6. Aylward, G. W., McCarry, B., Kousoulides, L., Lee, J. P., Fells, P. A scoring method for Hess charts. Eye. 1992;6:659–661.
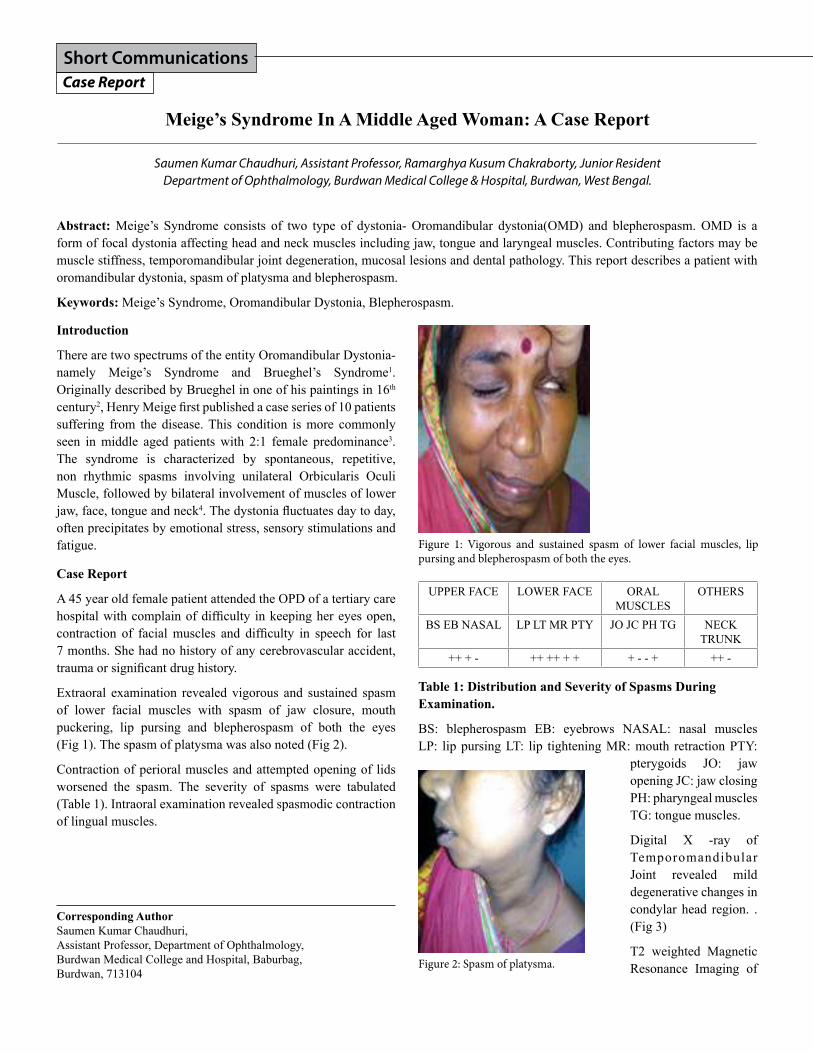
Short CommunicationsCase Report
Introduction
There are two spectrums of the entity Oromandibular Dystonia- namely Meige’s Syndrome and Brueghel’s Syndrome1. Originally described by Brueghel in one of his paintings in 16th century2, Henry Meige first published a case series of 10 patients suffering from the disease. This condition is more commonly seen in middle aged patients with 2:1 female predominance3. The syndrome is characterized by spontaneous, repetitive, non rhythmic spasms involving unilateral Orbicularis Oculi Muscle, followed by bilateral involvement of muscles of lower jaw, face, tongue and neck4. The dystonia fluctuates day to day, often precipitates by emotional stress, sensory stimulations and fatigue.
Case Report
A 45 year old female patient attended the OPD of a tertiary care hospital with complain of difficulty in keeping her eyes open, contraction of facial muscles and difficulty in speech for last 7 months. She had no history of any cerebrovascular accident, trauma or significant drug history.
Extraoral examination revealed vigorous and sustained spasm of lower facial muscles with spasm of jaw closure, mouth puckering, lip pursing and blepherospasm of both the eyes (Fig 1). The spasm of platysma was also noted (Fig 2).
Contraction of perioral muscles and attempted opening of lids worsened the spasm. The severity of spasms were tabulated (Table 1). Intraoral examination revealed spasmodic contraction of lingual muscles.
UPPER FACE LOWER FACE ORAL MUSCLES
OTHERS
BS EB NASAL LP LT MR PTY JO JC PH TG NECK TRUNK
++ + - ++ ++ + + + - - + ++ -
Table 1: Distribution and Severity of Spasms During Examination.
BS: blepherospasm EB: eyebrows NASAL: nasal muscles LP: lip pursing LT: lip tightening MR: mouth retraction PTY:
pterygoids JO: jaw opening JC: jaw closing PH: pharyngeal muscles TG: tongue muscles.
Digital X -ray of Temporomandibular Joint revealed mild degenerative changes in condylar head region. . (Fig 3)
T2 weighted Magnetic Resonance Imaging of
Abstract: Meige’s Syndrome consists of two type of dystonia- Oromandibular dystonia(OMD) and blepherospasm. OMD is a form of focal dystonia affecting head and neck muscles including jaw, tongue and laryngeal muscles. Contributing factors may be muscle stiffness, temporomandibular joint degeneration, mucosal lesions and dental pathology. This report describes a patient with oromandibular dystonia, spasm of platysma and blepherospasm.
Keywords: Meige’s Syndrome, Oromandibular Dystonia, Blepherospasm.
Meige’s Syndrome In A Middle Aged Woman: A Case Report
Saumen Kumar Chaudhuri, Assistant Professor, Ramarghya Kusum Chakraborty, Junior ResidentDepartment of Ophthalmology, Burdwan Medical College & Hospital, Burdwan, West Bengal.
Corresponding AuthorSaumen Kumar Chaudhuri, Assistant Professor, Department of Ophthalmology, Burdwan Medical College and Hospital, Baburbag, Burdwan, 713104
Figure 1: Vigorous and sustained spasm of lower facial muscles, lip pursing and blepherospasm of both the eyes.
Figure 2: Spasm of platysma.

Bengal Ophthalmic Journal50
the brain revealed diffuse cerebral atrophy (Fig 4). Digital X-ray of cervical spine was within Normal Limits. Vertebral bodies showed mild degenerative changes.
It was diagnosed as Meige’s Syndrome and as adviced by Neurologist, the treatment has been started with Baclofen and Clonazepam.
Discussion
Meige’s Syndrome consists of two forms of dystonia- Blepherospasm and Oromandibular dystonia. Blepherospasm presents as uncontrollable closing of eyes, photophobia, and involuntary closure of lids during speech. Oromandibular dystonic symptoms include facial muscle spasm, difficulty in
opening and closing of jaws, dysarthria, dysphagia and lingual dystonia.
The cause of this syndrome is little known. In the adult form mutation of chromosome 14q22 in the GCH1 gene has been identified5. Defective inhibitory control of the Basal Ganglia, Thalamus and Medulla Oblongata has been suggested6.
The syndrome can be due to acute or delayed adverse drug reaction of some Antipsychotic medications7. It is often misdiagnosed as familial Cranial Dystonia, Parkinsonism or temporomandibular joint disorders and can progress upto a point of continuous spasm8.
The diagnosis is mainly clinical. MRI helps in ruling out any
structural anomalies. Surface Electromyography is helpful to document the spasms in a precise manner.
The syndrome is incurable. Medications like Anticholinergics, Baclofen, Benzodiazepines may provide some symptomatic reliefs but their success rate is variable. Botox injections may help with blepherospasm and to suppress the dystonia but the results are not very assuring9.
Conclusion
Without any definite identifiable causative factors, the treatment results are often disappointing.
References
1. Marsden C. D Blepherospasm oromandibular dystonia syndrome ( Brueghel’s syndrome). A variant of adult onset dystonia? Journal of Neurology, Neurosurgery, and Psychiatry 1976;39:1204-09.
2. Meige H. Les convulsions de la face, une forme clinique de convulsion faciale, bilaterale et mediane. Revue Neurologique(Paris) 1910;20:437-43.
3. Tolosa ES, Klawans HL. Meige’s disease: A clinical form of facial convulsion, bilateral and medial. Arch Neurol 1979;36:635-37.
4. Paulson GW. Meige’s syndrome. Geriatrics 1972:27(18):69-73.
5. Steinberger D, et al. GCH! Mutation in a patient with adult onset oromandibular dystonia. Journal of Neurology 1999; 52:877-79.
6. Jones M, Hunter R, Abnormal movements in patients with chronic psychiatric illness. In: Crane GE and Gardener R (Eds). Psychotropic drugs and dysfunction of the basal ganglia. Washington DC, US Government Printing Office 1969.
7. Rosenbaum AH, Niven RG, Hanson NP, et al. Tardive dyskinesia: Relationship with a primary affective disorder. Journal of Disease and Nervous System 1977;38:423-27.
8. Tolosa ES, Lai C. Clinical featuresof Meige’s disease (Idiopathic Orofacial Dystonia). Arch Neurol 1981;38:147-51.
9. Challas G, Chapel J, Jenkins R. Meige’s disease: Control of symptoms and its clinical course. Int J Neuropsychit (suppl 1) 1967;3:95-104
Conflicts of Interest- NoneFinancial disclosures- None
Figure 3: Mild degenerative changes in Right Temporomandibular joint on Digital XRay.
Figure 4: T2W MRI showing Prominent Sulci and Dilatation of Ventricles suggestive of Diffuse Cerebral Atrophy.

Short CommunicationsCase Report
Introduction
Apert syndrome is a rare type of acrocephalosyndactyly syndrome. It was first described by a French physician, Apert in 19061. It is characterized by craniosynostosis, severe syndactyly of the hands and feet and facial dysmorphism1-3. It is an autosomal dominant disorder due to mutation of fibroblast growth factor receptors (FGFR-2) gene at locus 10q262, 4 which plays a key role in cranial development. It is usually inherited from father with prevalence of 1:65, 000 with no sex predilection2, 6, 3, 5.
Case Report
A 10 year old boy, presented to eye OPD of a tertiary care Hospital with complaint of diminution of vision both eyes for last 2 months. He was mentally retarded with history of delayed developmental milestones, could not manage daily activities without assistance till date. He was unable to close mouth completely with frequent attacks of upper respiratory infections. He developed headache, vomiting 2 months ago necessitating hospital admission in neurology department and referred to ophthalmology.
On examination, he was irritable and un-cooperative. His best corrected visual acuity was counting finger close to face in both eyes. Ocular examination revealed exophthalmos, down slanting of palpebral fissures(Fig1, 2). Rest of the anterior sement examination was within normal limit Pupils were sluggishly reacting, dilated fundus evaluation showed bilateral optic atrophy (Fig 3).
Systemic examination revealed boat shaped head (oxycephaly), flat midface, syndactyly of middle 3 fingers and toes (Fig 4, 5), crowding of tooth, pseudoprognathism, byzantine-arch palate,
mental retardation. Mouth was constantly open with protruded teethes.
Magnetic resonance tomography of brain revealed mega cysterna magna suggesting mass effect compressing cerebellum and brainstem anteriorly with supratentorial ventriculomegaly (Fig 6). Maxillary sinus had mucosal thickening. Based on clinical finding and neuro-imaging, ventriculoperitoneal shunt was planned in neurosurgical department.
Discussion
Apert’s syndrome is most severe form of craniosynostosis( acrocephaly/ oxycephaly ). Premature fusion of coronal or any other suture (e. g. lambdoid ) leads to cone shaped head.
Apert’s syndrome with optic atrophy : A case report
Nabanita Barua. DO, DNB. FICO, Chandana Chakraborti. MD.
Corresponding AuthorChandana ChakrabortiAssociate Professor, Dept. of OphthalmologyNorth Bengal Medical College, DarjeelingE-mail: cchakoptha@yahoo. com
Abstract: A 10 year old boy presented with oxycephaly, retruded midface, syndactyly, hydrocephalus, crowding of tooth, pseudoprognathism, byzantine-arch palate, mental retardation. Presenting visual acuity was counting finger close to face both eyes. He had exophthalmos, down slanting palpebral fissures, bilateral sluggishly pupillary reaction. Fundoscopy revealed bilateral secondary optic atrophy. In today’s era of improved neurosurgical intervention optic atrophy is rare in case of Apert’s syndrome. Early diagnosis is the key factor and an integrated approach should involve dentists, neurosurgeons, plastic surgeons, ophthalmologists and radiologist for the effective planning and treatment of these patients.
Key words: Apert’s syndrome, optic atrophy
Figure1: Lateral view showing conical head, proptosis and flat mid face

Bengal Ophthalmic Journal52
Facial abnormalities hypoplastic midface (maxilla is hypoplastic with a high-arched palate) with normal sized mandible leads to crowding of tooth and pseudoprognathism which was present in our case. Other dental problems may be impacted teeth, delayed eruption, ectopic eruption, supernumerary teeth, thick gingiva etc. Respiratory abnnormalities include, short and wide nose with depressed nasal bridge (1, 2, 5, 7), cleft soft palate, bifid uvula, Byzantine-arch palate ( incomplete fusion of the palatal process with the nasal spine), anterior open bite of maxilla, choanal stenosis, and anomalies of the tracheal cartilage (8).
Systemic features include syndactyly of the hands and feet (partial or complete fusion of second and fourth finger) are present. Patients may also have impaired mental function, various anomalies of the viscera, elbows and shoulders, skeleton. CNS features may include prominent forehead, enlarged anterior frontanelle6, abnormalities of the corpus callosum (CC), hypoplasia or absence of the septum pellucidum, hippocampal hypoplasia or dysplasia and cerebral cortex dysplasia, ventriculomegaly, megaloencephaly and gyral malformation.
Ocular features are hypertelorism, proptosis, down slanting palpebral fissures, ptosis, antimongoloid slant, strabismus, amblyopia, optic atrophy, and occasionally papilledema. Apert’s closely resembles Crouzon’s syndrome; both having proptosis and hypertelorism though cause of dystopia is quite different. Proptosis in crouzon is due to retrusion of lateral and inferior wall in an extremely short orbital floor. Lateral orbital margin is indeed markedly protruded in Apert’s syndrome, resulting
Figure 3: Secondary optic atrophy
in protrusion of eyeball. Type of squint is also different in these two diseases, exotropia being common in Crouzon and V pattern (exotropic upgaze and esotropic downgaze) in Apert. Some structural abnormalities of extraocular muscles are also noted in Apert’s which may also lead to strabismus. Subluxation of eyeball, vision threatening complications like exposure keratitis, chronic papilledema, optic atrophy (in around 20% cases) is more common in Crouzon10.
A multidisciplinary approach should be undertaken while dealing with this disorder. An integrated approach should include dentists, neurosurgeons, plastic surgeons, ophthalmologists and radiologist for the effective planning and treatment of these patients.
References
1. Harper JI. Genetics and genodermatoses. In: Champion RH, Burton JL, Burns D, Breathnach SM (editors): Rook/ Wilkinson/ Ebling, Text book of dermatology. 6th ed. Oxford: Black Well Science; 1998:425-6.
2. Mukhopadhyay AK, Mukherjee D. Apert’s syndrome. Indian J Dermatol Venereol Leprol 2004;70:105-7.
3. Cohen MM Jr, Kreiborg S. New indirect method for estimating the birth prevalence of the Apert’s syndrome. Int J Oral Maxillofac Surg 1992;21:107-9.
Figure 5: Fused feet
Figure 4: Fused fingers

December 2017 Bengal Ophthalmic Journal 53
4. Sohi BK, Sohi AS. Apert’s syndrome. Indian J Dermatol Venereol Leprol 1980;46:169-72.
5. Cohen MM Jr, Kreiborg S. An updated pediatric perspective on the Apert syndrome. Am J Dis Child 1993;147:989-93.
6. Wilkie AO, Wall SA. Craniosynostosis- Novel insights into the pathogenesis and treatment. Curr Opin Neurol 1996;9:146-52.
7. Chen L, Li D, Li C, Engel A, Deng CX. Ser250trp substitution in mouse fibroblast growth factor receptor 2 (FGFR2) results in craniosynostosis. Bone 2003;33:169-78.
8. Kaplan LC. Clinical assessment and multispecialty management of Apert syndrome. Clin Plast Surg 1991;18:217-25.
9. Upton J. Apert Syndrome. Classification and pathologic anatomy of limb anomalies. Clin Plast Surg 1991;18:321-55.
10. Arroyo Carrera I, Martínez-Frías ML, Marco Pérez JJ, et al. Apert syndrome: clinico-epidemiological analysis of a series of consecutive cases in Spain. An Esp Pediatr 1999;51:667-72.
Conflicts of Interest- NoneFinancial disclosures- None
Figure 6: MRI brain showing dilated ventricle and normal orbit

Short CommunicationsCase Report
Introduction
Coats’ disease is a unilateral (95%), idiopathic retinal vascular abnormality characterized by telangiectatic retinal vessels in association with lipid exudation[1]. Although most cases are diagnosed before the age of 20 years (75%), Coats’ disease may also manifest in adult patients[2]. Conventional therapeutic strategies involve observation, photocoagulation or cryotherapy for retinal telengiectasias and surgical intervention for retinal detachment. Adjunctive treatment modalities such as intravitreal anti-VEGF agents and/or traimcinolone may be employed to improve anatomic and visual outcome in cases with a significant amount of subretinal fluid but with inconclusive outcomes[3-6]. High efficacy of dexamethasone intravitreal implant in the initial management of Coats’ disease has been reported recently [7, 8].
Here, we report a case of Adult onset Coats disease with retinal vasoproliferative tumor (RVT) managed with dexamethasone intravitreal implant Ozurdex(®) (Allergan, Inc., Irvine, Calif., USA).
Intravitreal Dexamethasone implant (Ozurdex) with PRP for Adult’s Coats Disease
Kshitiz Kumar, Pallavi Raj, Samar Sen Gupta, Amar AgarwalDr. Agarwal’s Eye Hospital jointly with Peerless Hospitex and B K Roy Research Centre, Kolkata, India
Case Report
A 41-year-old female was referred to our department with a 6month history of progressive vision loss in her left eye. BCVA was 20/20 in RE and CF1M in LE. Anterior segment examination was unremarkable.
Whereas the RE fundus did not show any significant change, in the LE massive exudation within the inferior-temporal quadrant of the retina was evident, with posterior pole involvement and intraretinal lipid accumulation. In addition, a yellowish mass
with overlying haemorrhages and neo-vessels was observed in temporal peripheral retina (Fig. 1). SD-OCT confirmed the presence of exudative retinal detachment with macular involvement with numerous hyperreflective intraretinal lesions corresponding to lipids were evident (Fig. 2). USG-B scan showed an intraretinal mass located in the temporal periphery, associated with the exudative retinal detachment. FFA (Fig. 3) confirmed the presence of telangiectatic vessels with peripheral capillary non perfusion areas; the peripheral temporal mass was identified as a retinal vasoproliferative tumor (RVT). Patient was treated with an intravitreal injection of the sustained-release dexamethasone implant Ozurdex® (Allergan, Inc., Irvine, Calif., USA). One month later, BCVA improved to 20/120 and SD-OCT revealed complete resolution of the exudative retinal detachment with persistent macular edema (CFT 513 microns). PRP was done to CNP areas along with telangiectatic vessels (Fig. 4). At 3 months, macular edema had resolved (CFT 253 microns) with BCVA 20/60. The volume of the RVT decreased progressively. Through the follow-up of 4 months, no further recurrences of the exudation was noted, and the extensive lipid accumulation progressively regressed with stable vision (Fig. 5). Corresponding author/Address for reprints:
Saumen Kumar Chaudhuri, Assistant Professor, Department of Ophthalmology, Burdwan Medical College and Hospital, Baburbag, Burdwan, 713104
Fig. 2 SD-OCT image of Left Eye. At presentation showing massive neurosensory detachment, retinal edema and intra retinal and sub retinal lipid exudation
Fig. 1 Fundus photos of Left Eye. A, B, C. Massive intaretinal lipid accumulation in retina. D. Temporal periphery showing a mass lesion with overlying new vessels and hemorrhages suggestive of secondary retinal vasoproliferativhe tumor (RVT).
A
C
B
D

December 2017 Bengal Ophthalmic Journal 55
Discussion
Coats’ disease affects men 3 times as often as women, in the first or second decade of life, with no racial predilection and is usually unilateral (bilateral in 5% of cases) Retinal vasoproliferative tumors can occur secondarily to preexisting conditions (26%) such as inflammatory, vascular, traumatic or degenerative retinal diseases as evidenced in our patient who had associated Coats’s disease as the primary pathology.[9,10] This unique presentation in a female patient in fourth decade of life makes an interesting case study.
Coats’s disease may have a possible underlying inflammatory component, though uncommon[11]. And the fact that intravitreal corticosteroid treatment is known to attenuate leukostasis and vascular leakage along with suppression of inflammation[12], dexamethasone implant has come up as a latest tool in the management of this complex disorder. Intravitreal triamcinolone acetonide injection is another alternative but with a poor safety profile compared to dexamethasone implant in Coats disease. Castillo et. al.[7] demonstrated complete resolution of exudation and closure of telengiectasias with photocoagulation as evidenced in this study also. Similar results were seen in case study of Saatci et. al [8] but in paediatric patients.
Some investigators have demonstrated an increased level of VEGF in eyes with Coats’ disease and a significant decrease in VEGF after the injection of anti-VEGF agents[13]. Ray et al.[14] compared their results with bevacizumab in-jections to those
Fig. 3 Funds fluorescein angiography images at presentation. A. Posterior pole showing pinpoint leakages. B, C. Early and late films showing Capillary non perfusion areas with leakages from telengiectasias. D. Extreme temporal periphery with telangiectatic bulbs.
Fig. 4 A. Anterior segment photo of LE showing Ozurdex implant in anterior vitreous. B, C, D. Red-free funds photos showing discrete panretinal photocoagulation burns in the retina. E. SD-OCT of LE 1month post intravitreal ozurdex, macular edema with resolved sub retinal fluid.
Fig. 5 Fundus photos 3 months post intravitreal ozurdex injection. A. Resolution of retinal exudation with clearing of intraretinal lipids. B. Fibrosed retinal vasoproliferativhe tumor with regression. C. SD-OCT 3months post injection, showing completely flat macula with resolved macular edema.
A
A
A
C
C
C
B
B
B
D
D
E

Bengal Ophthalmic Journal56
achieved with triamcinolone acetonide injections as an addi-tional treatment modality to ablative therapy in eyes with Coats’ disease. They argued that rapid resorption of subretinal fluid was seen after treatment with intravitreal triamcinolone, but this was not the case after bevacizumab injection. Therefore with the proven efficacy of corticosteroids in reducing exudation before ablative therapy can be rendered to retina, intravitreal dexamethasone implant (Ozurdex) administered in this case helped in the overall management.
Conclusion
Coats disease can be a rare presentation in an adult female patient. Secondary retinal vasoproliferative tumors are frequently associated finding in such cases. Intravitreal dexamethasone implant (Ozurdex) adds to the armamentarium of Coats disease management and can be offered as a first line of treatment with high degree of efficacy.
References
1. Shields JA, Shields CL, Honavar SG, Demirci H: Clinical variations and complications of Coats’ disease in 150 cases: the 2000 Sanford Gifford Memorial Lecture. Am J Ophthalmol 2001;131:561–571.
2. Smithen LM, Brown GC, Brucker AJ, Yannuzzi LA, Klais CM, Spaide RF. Coats’ disease diagnosed in adulthood. Ophthalmology. 2005;112:1072–1078.
3. Bergstrom CS, Hubbard GB 3rd: Combination intravitreal triamcinolone injection and cryotherapy for exudative retinal detachments in severe Coats disease. Retina 2008;28(3 suppl):S33–S37.
4. Othman IS, Moussa M, Bouhaimed M: Management of lipid exudates in Coats disease by adjuvant intravitreal triamcinolone: effects and complications. Br J Ophthalmol 2010;94:606–610.
5. Venkatesh P, Mandal S, Garg S: Management of Coats disease with bevacizumab in 2 patients. Can J Ophthalmol 2008;43:245–246.
6. Goel N, Kumar V, Seth A, Raina UK, Ghosh B: Role of intravitreal bevacizumab in adult onset Coats’ disease. Int Ophthalmol 2011;31:183–190.
7. Martinez-Castillo S, Gallego-Pinazo R, Dolz-Marco R, Marin-Lambíes C, Diaz-Llopis M: Adult Coats’ disease successfully managed with the dexamethasone intravitreal implant (ozurdex®) combined with retinal photocoagulation. Case Rep Ophthalmol 2012;3:123–127.
8. Saatci AO, Doruk HC, Yaman A. Intravitreal dexamethasone implant (ozurdex) in coats’ disease. Case Rep Ophthalmol. 2013 Sep 21;4(3):122-8.
9. Shields JA, Shields CL: Coats’ disease: the 2001 Lu Esther T. Mertz lecture. Retina 2002; 22:80–91.
10. Shields CL, Shields JA, Barrett J, De Potter P: Vasoproliferative tumors of the ocular fun- dus. Classification and clinical manifesta- tions in 103 patients. Arch Ophthalmol 1995; 113:615–623.
11. Lim WK, Nussenblatt RB, Chan CC: Immunopathologic features of inflammatory coats disease. Arch Ophthalmol 2005;123:279–281. 10.
12. Tamura H, Miyamoto K, Kiryu J, Miyahara S, Katsuta H, Hirose F, Musashi K, Yoshimura N: Intravitreal injection of corticosteroid attenuates leukostasis and vascular leakage in experimental diabetic retina. Invest Ophthalmol Vis Sci 2005;46:1440–1444.
13. He YG, Wang H, Zhao B, Lee J, Bahl D, McCluskey K: Elevated vascular endothelial growth factor level in Coats’ disease and possible therapeutic role of bevacizumab. Graefes Arch Clin Exp Ophthalmol 2010;248:1519–1521.
14. Ray R, Barañano DE, Hubbard GB: Treatment of Coats’ disease with intravitreal bevacizumab. Br J Ophthalmol 2013;97:272–277.

Photo Essay
A 6- year–old female child presented to us with red eye, photophobia and foreign body sensation in both eyes. On ophthalmic examination her visual acuity was 6/24 in right eye and 6/36 in the left eye. There was conjunctival congestion, perilimbic pigmentation and punctate keratitis in both eyes. In left eye, there was pterygium nasally (Fig 1). ‘Salt and pepper’ pigmentory changes was found all over her body and face (Fig. 2 & 3). Buccal mucosa and lips were also affected along with cheilitis. Appearance of skin hyperpigmentation started at 1 year of age, ocular lesions started at 3 years of age. Family history
symblepharon, corneal opacity, neovascularization, pterygia, band keratopathy, keratitis and corneal oedema. Squamous cell carcinomas, malignant melanomas and limbal stem cell deficiency have been also reported. Fundus involvement is rare as the posterior segment is protected from UV damage by the cornea and lens[3].
The impression cytology is helpful for early diagnosis of XP. There is no definitive cure for the disease. Methyl cellulose or quinodine-containing eye drops and bland ointment at night are advised. Avoidance of UVradiation, use of protective
clothing, sunscreens, oral retinoids, 5-fluorouracil and topical application of 5-fluorouracil or imiquimod are advocated for premalignant lesions. For malignant neoplasms of the skin, tongue, eyelids, conjunctiva and cornea surgical excision is indicated[4, 5]. In spite of early detection and management, 2/3 of the cases die before third decade of the life. Regular consultations with dermatologists,
ophthalmologists, neurologists and dentists are a must for timely detection of premalignant and malignant lesions.
References
1. Kraemer KH, Slor H. Xeroderma pigmentosum. Clin Dermatol 1985;3: 33-69.
2 Hebra F, Kaposi M. On disease of the skin including exanthemata. New Sydenham Soc 1874;61: 252-8.
3. Kaposi M. Xeroderma pigmentosa. Ann Dermatol Venereol 1874;4: 29-38.
4. L. Feller, N. H. Wood, M. H. Motswaledi, R. A. G. Khammissa, M. Meyer, J. Lemmer. Xerodermapigmentosum: a case report and review of the literature. J Prev med hyg 2010; 51: 87-91.
5. Hasan S, Saeed S. XerodermaPigmentosum-A Rare Genodermatosis: Overview of Literature. Pigmentary Disorders 2: 2015;230.
Conflicts of Interest- NoneFinancial disclosures- None
Xeroderma Pigmentosum
Chandana Chakraborti, MD. Associate Professor, Dept. of OphthalmologyNorth Bengal Medical College, Darjeeling
Corresponding AuthorChandana Chakraborti, MBBS, MD (AIIMS)Associate Professor, Dept. of OphthalmologyNorth Bengal Medical College, DarjeelingE-mail: cchakoptha@yahoo. com
Fig 1. Punctate keratitis in both eyes with nasal pterygium
Fig 2. Salt and pepper pigmentory skin changes
disclosed similar disease in her 4years old younger sister. The child was advised to avoid sunlight. Ocular lesions were treated with topical antibiotics and lubricating eye drops and ointment. The mother was asked to bring the sibling for consultation but unfortunately they did not turn up.
Discussion: The term xeroderma pigmentosum(XP) was coined in 1882 by Kaposi. It is a rare autosomal recessive genetic disorder in which the ability to repair damaged DNA caused by ultraviolet (UV) light is deficient[1, 2]. The condition is characterized by photosensitivity, dry pigmented skin, premature skin aging, and skin malignancies like multiple basal cell carcinomas, metastatic malignant melanoma and squamous cell carcinoma[1] [3]. The disease occurs in both genders and in all races. Consanguinity has been implicated as an etiological factor. Approximately 40% -80% of XP patients present with ocular lesions like photophobia, blepharospasm, lower lid ectropion,
Fig 3 Pigmentory changes over body and face

Photo Gallery
Croroidal melanoma
DUSN with macular hole and worm
Vitelliform dystrophy
Cysticercosis
Dropped cataractous lens adhered to disc with CRVO
Subhyaloid hge with RBC WBC Layer

Clippings
Sabyasachi BandyopadhayMS, Associate Professor. RG Kar Medical College.
Pueyo V et al (BJO 2017; Vol 101: issue 9) performed a study to identify differences in neuronal tissue from retinal and brain structures in children born small for gestational age (SGA) with no abnormality in neonatal brain ultrasonography and no previous neurological impairment, and to evaluate the relationship between retinal structure and brain changes in school-age children born SGA.
They recruited two cohorts of children: 25 children born SGA and 25 children born with an appropriate birth weight according to gestational age. All the children underwent an ophthalmic examination, which included retinal imaging using spectral-domain optical coherence tomography, and a brain MRI. MRI
images were automatically segmented and global and regional brain volumes were obtained.
It was observed that although visual function did not differ between both groups, the complex ganglion cell and inner plexiform layers (GCL-IPL) was thinner in SGA children. Total intracranial volume, and global grey and white matter volumes in brain and cerebellum were correlated with birthweight centile, as were certain regional volumes (temporal and parietal lobes, hippocampus and putamen). Abnormal GCL-IPL measurements accurately identified SGA children with the most severe grey and white matter changes in the brain.
They concluded that SGA children, both preterm and term born, showed evidence of structural abnormalities in the retina, which may be an accurate and non-invasive biomarker of neuronal damage in brain tissue.
Pediatric Ophthalmology
Chandrima PaulPhD (Ophthalmology)B B Eye Foundation, 2/5 Sarat Bose Road, Kolkata 700 020. Email : drchandrimapaul@gmail. com
Tham YC et al (Ophthalmology 2014; Vol 121:issue11. Pages 2081-90) studied Global prevalence of glaucoma and projections of glaucoma burden through 2040. It was a systematic review and meta-analysis. The authors systematically examined the global prevalence of primary open-angle glaucoma (POAG) and primary angle-closure glaucoma (PACG), and projected the number of affected people in 2020 and 2040.
Data from 50 population-based studies (3770 POAG cases among 140, 496 examined individuals and 786 PACG cases among 112 398 examined individuals) were used for analysis and review.
The authors searched PubMed, Medline, and Web of Science for population-based studies of glaucoma prevalence published up to March 25, 2013. They used hierarchical Bayesian approach to estimate the pooled glaucoma prevalence of the population aged 40-80 years along with 95% credible intervals (CrIs). The authors estimated the projections of glaucoma based on the United Nations World Population Prospects and to assess the association between the prevalence of POAG and the relevant factors Bayesian meta-regression models were performed.
They observed that the global prevalence of glaucoma for population aged 40-80 years were 3.54% (95% CrI, 2. 09-5. 82). The prevalence of POAG was highest in Africa (4.20%; 95% CrI, 2. 08-7.35) while the prevalence of PACG was highest in Asia (1. 09%; 95% CrI, 0. 43-2.32). The number of people in the age group of 40-80 years with glaucoma was estimated to be 64.3 million worldwide in 2013. The projected number of affected people is 76.0 million in 2020 and 111. 8 million in 2040. They also observed that men were more likely to have POAG than women (odds ratio [OR], 1. 36; 95% CrI, 1. 23-1. 52) in the Bayesian meta-regression model. After adjusting for age, gender, habitation type, response rate, and year of study, people of African ancestry were found to have POAG than people of European ancestry (OR, 2.80; 95% CrI, 1.83-4. 06), and people living in urban areas were more likely to have POAG than those in rural areas (OR, 1. 58; 95% CrI, 1. 19-2. 04).
The authors concluded that the projected number of people with glaucoma worldwide will be 111. 8 million in 2040 and it will affect people residing in Asia and Africa disproportionally and the meta- analysis will have important role in guiding the designs of glaucoma screening, treatment and related public health strategies.
Glaucoma

Bengal Ophthalmic Journal60
Glaucoma
Somdutt PrasadMS, FRCSEd, FRCOphth, FACS, Consultant of Ophthalmologist AMRI & Fortis Hospitals, Kolkata
Koch DD, Hill W, Abulafia A, Li W. Journal of Cataract and Refractive Surgery. Pursuing perfection in intraocular lens calculations: Logical approach for classifying IOL calculation formulas. June 2017, Volume 43, Issue 6, Pages 717–718
It has been 50 years since Fyodorov published his paper describing the first theoretical intraocular lens (IOL) power calculation formula. A multitude of formulae have emerged since then that have their uses and limitations.
The authors have stated that IOL calculations comprise a complex scientific and therapeutic measure that necessitates some preoperative, intraoperative and postoperative steps to be followed meticulously. They have suggested that formulas should be classified by their method of calculating IOL power and the data they use for these calculations. They have proposed classification of IOL calculation formulas under the following headings:
1. Historical/refraction based: These were the first attempts at calculating IOL power. Obviously, this approach is obsolete.
2. Regression: These formulas are derived from an analysis of previous data and do not rely on theoretical optics:
• SRK and SRK II: Linear regression
3. Vergence: based on Gaussian optics that can be subclassified as
• 2 variable formulas: – Holladay 1
– SRK/T – Hoffer Q• 3-variable formulas: – Haigis
– Ladas Super Formula (which combines Haigis and the 2-variable formulas)
• 5-variable formulas: – Barrett Universal II• 7-variable formulas: – Holladay 2
4. Artificial intelligence. It is a sophisticated engineering-based statistical model to find relationships not otherwise evident in theoretical approaches:- Clarke neural network- Hill-RBF (radial basis function)
5. Ray tracing. - Okulix- Phacooptics (Olsen)
The authors concluded that “Newer” is often, but not always, better and the fact remains that there are limits to how far we can accurately predict post operative outcomes. Complex eyes often require new formulas or modifications of the existing ones. We might have hit a temporary ceiling for IOL calculation accuracy for normal eyes at approximately 90% of eyes within ±0. 50 D of target and, of course, lower for more complex eyes. With the increased availability of optical biometry machines in our practices which have any of the newer formulae built in, it is essential to understand them to get the best outcome for our patients.
Refractive Surgery
Tutul ChakravartiDO, DNBAssistant ProfessorVivekananda Mission Institute, KolkataThe prevalence of myopia in eyes with angle closureJ Glaucoma in 2007 Oct-Nov;16(7):642-3Tutul Chakravarti, George L Spaeth
Narrowing of the anterior chamber angle and angle closure glaucoma are typically associated with hyperopia. Hyperopic eyes are frequently having short axial length, small corneal diameter, and a shallow anterior chamber. They are at a increase
risk of Primary angle closure (PAC) and Primary Angle Closure Glaucoma (PACG). In myopic eyes, the axial length is usually longer than average and the anterior chamber is usually deep; PAC is rarely observed in these eyes. Because angle closure in myopic patients is unusual; gonioscopy in these patients are not performed routinely.
However, Dr. Tutul Chakravarti and Professor George L Spaeth studied 322 cases of PAC. In this retrospective chart review of 322 cases of PAC, 6 PAC cases occurred in myopic eyes. All cases were diagnosed by the use of indentation gonioscopy. . This study emphasizes the importance of gonioscopy to detect PAC, even in myopic eyes.