benefit basics€¦ · group health plans and health insurance issuers generally may not, under...
TRANSCRIPT


Floyd County Government
Service Provider Information
Health HUMANA Group #671728 1.866.427.7478 www.humana.com
Dental HUMANA Group #671728 1.800.233.4013 www.humana.com
Vision HUMANA Group #1003954 1.877.398.2980 www.humana.com Basic Life/ Voluntary Term Life and AD&D UNUM 1.800.421.0344 www.unum.com
Group Disability / Accident / Cancer / Critical Illness COLONIAL LIFE 1.800.325.4368 www.coloniallife.com Employee Assistance Program (EAP) HUMANA 1.866.440.6556 www.humana.com/eap Medical Bill Saver EAP UNUM 1.800.854.1446 www.unum.com/lifebalance
TABLE OF CONTENTS Our Commitment to You .............................................................. 2
Benefit Eligibility .......................................................................... 2
AP Assist ..................................................................................... 3
Health Insurance ......................................................................... 4
Coverage First ............................................................................. 5
Health Reimbursement Account .................................................. 6
Humana First Nurse Line ............................................................. 6
Humana Virtual Visits .................................................................. 7
Humana Go365 ...................................................................... 8-13
Dental Insurance ....................................................................... 14
Vision Insurance ........................................................................ 15
Employee Assistance Program ................................................. 16
Medical Bill Saver EAP .............................................................. 17
Basic Life / AD&D Insurance ..................................................... 18
Voluntary Term Life and AD&D ............................................ 19-20
Colonial Voluntary Benefits ....................................................... 21
Financial Education ................................................................... 22
Travel Assistance ................................................................. 23-24
Compliance Notices.............................................................. 25-31
The following information is a quick overview of the benefits plans currently provided and is not to be interpreted as a complete disclosure of plans entitlement to any benefits described. The company reserves the right to adjust, amend and revise benefits plans. In all cases of specific plan interpretations, receipt of benefits or entitlements, the actual plan document shall rule. You can contact your HR Department for the actual plan documents.

2
OUR COMMITMENT TO YOU!
Floyd County Government plans are designed to recognize the diverse needs of our workforce. In our efforts to provide enhanced benefit coverage and plan options, we continuously search for ways to make this possible.
Once again, we are able to provide competitive and comprehensive benefit options that allow you to design your own plan based on individual needs. Additionally, our plans provide long-term financial security for you and your family.
Only you can determine which benefits are the best for you and your family. We want you to understand all your options and make informed decisions.
BENEFIT BASICS
It is important that you notify Human Resources upon any life event change so that we can ensure there is no interruption or discrepancies in your benefits. Any request for coverage change or cancellation must be consistent with your Qualifying Life Event and you must have the proper supporting documentation (i.e. birth certificate, marriage license, final divorce paperwork, etc.).
Employee Portal access: We have launched an employee portal which is where you can find valuable information such as benefits, the employee handbook, policies, and newsletters.
1. https://www.floydcounty.in.gov/index.php/floyd-county-indiana-employee-portal 2. Passcode: FloydCounty47150
Eligibility
Full-time employees working 30 hours per week, are eligible to elect a variety of benefits described in this guide. New hire eligibility is the first day of the month following 30 days of employment. Dependent children may be covered until the end of the month in which they turn age 26 on the medical, dental and vision plans.
You and/or your eligible dependents must enroll within 30 days of becoming eligible. You will not be eligible to enroll until the next Open Enrollment period if you choose not to enroll for coverage within the 30-day eligibility period unless you experience a Qualifying Life Event.
Effective January 1, 2014, Floyd County Government will NO LONGER PROVIDE medical insurance to those spouses who are eligible for insurance coverage from his or her own employer. An employee will be presented a Medical Insurance Spousal Waiver during their first day of employment.
Qualifying Events
Your elections will remain in effect during the entire benefit plan year unless you experience a Qualifying Life Event. If you experience a Qualifying Life Event listed below, you may change or cancel your coverage during the benefit plan year. You must notify Human Resources within 30 days of the event to ensure there is no disruption of your coverage: Birth/Adoption Dependent Child Age Limit Divorce Marriage Death Loss of Health Coverage FMLA related Leave Eligible for Medicare You may add or drop coverage for yourself and/or dependents as a result of a qualifying event. For a complete list of Qualifying Life Events, please contact Human Resources.

3

4
HEALTH
Humana in-network physician services provide a higher benefit plan coverage and lower out-of-pocket expenses. To locate an in-network healthcare provider in your area, visit www.humana.com.
Humana PPO
Network Non-Network Benefit Allowance $500
Deductible (Single / Family) $1,000 / $2,000 $3,000 / $6,000
Out-of-Pocket Maximum (Single / Family) $6,250 / $12,500 $18,000 / $36,000
Physician Office Services $25 copay 50% *
Specialty Office Services $40 copay 50% *
Preventive Office Services No charge 50% *
Emergency Room Services copay waived if admitted
$150 copay $150 copay
Urgent Care Services $75 copay** 50% *
Inpatient & Outpatient Services 20% * 50% *
Outpatient Surgery Hospital 20% * 50% *
Retail Prescription Drugs** (tier 1 / 2 / 3 / 4) 30 day supply
$10/ $30/ $50/ 25% 30% after network copay
Mail Order** (tier 1 / 2 / 3 / 4) 90 day supply
$25/ $75/ $125/ 25% 30% after network copay
Specialty Drugs** (25% coinsurance when filled via a preferred network)
35% 50%
* After deductible has been met ** Deductible does not apply
Employee Cost Per Pay
Deferred Rates* Non-Deferred Rates
Employee $15.25 $15.25
Employee + Spouse $96.33 $113.83 Employee + Child(ren) $66.04 $83.54 Family $150.33 $167.83 *Deferred Rates are ones where your County Deferred Compensation match has been applied to the medical premium

5
HUMANA COVERAGE FIRST
What is CoverageFirst? With CoverageFirst, you can see any provider without a referral – but your costs are usually lower when you use in-network providers. What makes CoverageFirst unique is the $500-per-covered member “benefit allowance” that covers many services from in-network providers before you start paying toward your deductible.
Here’s how it works: 1. The plan pays the first $500 of eligible expenses from in-network providers. You just pay a copayment.
2. If you use the entire $500, you pay most additional expenses until you meet the annual deductible. The plan has a separate $500 allowance and a separate deductible for each family member; each person's costs also apply to a deductible for the entire family.
Why you might want CoverageFirst CoverageFirst offers lower premiums and a “safety net” in case of a major illness or injury.
• Your up-front costs are lower. CoverageFirst premiums are generally lower than with other plan types.
• You could have very low out-of-pocket costs. Many health plan members spend less than $500 a year on medical care.* If you’re in that group, the CoverageFirst allowance might cover all of your costs except your copayments.
• Preventive care coverage. Even if your $500 is gone, CoverageFirst covers your preventive care office visits. However, you would be responsible for special procedures billed separately, such as lab work.
• The out-of-pocket maximum provides peace of mind. If you have a serious illness or injury, your costs for covered services at in-network providers are capped.
Using your allowance The entire $500 is available on the first day of the plan year. You can use the allowance for:
• Doctor’s office visits
• Routine outpatient laboratory tests and X-rays
• Hospital services, including semiprivate room and board, emergency room services, and outpatient surgery
• Other services such as home healthcare, physical therapy, and hospice care
Your allowance isn't depleted when you fill a prescription or receive mental health services. Also, the allowance doesn't cover copayments or any services from out-of-network providers. Check the summary plan description for details about plan benefits, limitations, and exclusions.

6
FLOYD COUNTY HEALTH REIMBURSEMENT ACCOUNT (HRA)
Individuals who are covered under the Floyd County Government’s Humana Group Insurance plan are entitled to reimbursement for a portion of the deductible incurred as follows.
1. Financial Reimbursement under this plan shall be limited to allowable medical expenses which are adjudicated under the Humana Group Insurance plan as being creditable toward an insured’s deductible and which exceed $100 for an employee and their spouse and dependents. Incurred costs for procedures, treatment or expenses not covered by the Humana Group insurance plan or which are defined thereby as being “co-payments” shall not be eligible for reimbursement.
2. The reimbursement for an insured employee shall be $500; employee and spouse or employee with dependents shall be $500 to an overall maximum of $1000.
3. Allowable medical expenses exceeding the applicable amount set forth in (1), above, shall be reimbursed until the maximum reimbursement provided in (2), above has been paid.
4. A claim for reimbursement shall be submitted to the Floyd County Auditor and shall be supported by one or more Explanation of Benefits Statements issued by Humana disclosing the amount of the deductible incurred for which a claim is being made. A claim on behalf of a spouse or insured dependent shall be submitted by and paid to the employee.
5. This reimbursement may only be presented during registration at Baptist Health Floyd facilities. Please present your card, and if appropriate, Baptist Health Floyd will direct bill Floyd County for a maximum of $500.00 for services that are considered as counting towards your or family member’s Deductible, if on the County Health Plan. Patient is responsible for the first $100.00 deductible on their plan. Co-pays for office visits remain the responsibility of the employee. HRA Cards may be obtained from Human Resources.
HUMANA FIRST NURSE LINE
Free 24-hour health information, guidance and support 1-800-622-9529.
Health concerns? Give us a call.
Nurses are available around the clock for your immediate medical concerns. Our nurses can help you decide if you need to go to the ER or tell you how to change a bandage.
You can also call for longer-term health planning and support. Nurses can connect you with programs to help you lose weight or quit smoking. They can help you find out more about a health condition or help you find other support programs.
Keep this number handy—or call the Nurse Advice Line number on the back of your Humana member ID card.

7
HUMANA VIRTUAL VISITS

8
GO365

9

10

11

12

13

14
DENTAL
With Humana Dental plans, you can see any dentist. Members and their families benefit from negotiated discounts on covered services by choosing dentists in the Humana Dental PPO Network. To find a dentist in Humana Dental PPO Network, log on to www.humana.com or call 1-800-233-4013.
Plan 1- PPO 09 Plan 2-Traditional Preferred 09
In Network / Out of Network In Network / Out of Network
Deductible $50 Single
$150 Family $100 Single $300 Family
$50 Single $150 Family
$50 Single $150 Family
Annual Maximum Benefit $1,000 $2,000
Diagnostic & Preventive Services (Exams and X-rays)
100%* / 80% 100% / 100%
Basic Services (Routine fillings, space maintainers)
80% / 50% 80% / 80%
Major Services (crowns, dentures, bridges and implants)
50% / 50% 50% / 50%
Periodontics/Endodontics 50% / 50% 80% / 80%
*deductible does not apply for In network Diagnostic & Preventive services
Employee Cost Per Pay
Plan 1-PPO 09 Plan 2-Preferred 09
Employee $10.21 $15.79
Employee + Spouse $22.35 $34.53
Employee + Child(ren) $24.94 $38.53
Family $37.08 $57.30
Tips to ensure a healthy mouth
• Use a soft-bristled toothbrush
• Choose toothpaste with fluoride
• Brush for at least two minutes twice a day
• Floss daily
• Watch for signs of periodontal disease such as red,
swollen, or tender gums
• Visit a dentist regularly for exams and cleanings

15
VISION
Humana provides vision coverage for routine eye exams, lenses and frames. In-network physician services provide a higher benefit plan coverage and lower out of pocket expenses. To locate an in-network provider in your area, visit www.humana.com
Network Out-of-Network
Routine eye exam (every 12 months) $10 copay Up to $30
Eyeglass frames (every 24 months) $100 allowance
20% off balance over $100 $50 allowance
Standard Plastic Lenses (every 12 months)
Single Vision $25 Up to $25 Bifocal $25 Up to $40 Trifocal $25 Up to $60
Lenticular $25 Up to $100
Covered Lens Options
UV coating $15 Not covered
Tint (solid and gradient) $15 Not covered
Standard scratch-resistance $15 Not covered
Standard polycarbonate – adults $40 Not covered
Standard polycarbonate - children <19 $40 Not covered
Standard anti-reflective coating $45 Not covered
Premium anti-reflective coating Premium anti-reflective coatings as follows: Premium anti-reflective coatings as follows:
- Tier 1 - Tier 2 - Tier 3
$57 $68
80% of charge
Not covered Not covered Not covered
Standard progressive (add-on to bifocal) $25 Up tp $40
Premium progressive Premium progressives as follows: Premium progressives as follows:
- Tier 1 - Tier 2 - Tier 3 - Tier 4
$110 $120 $135
$90 copay, 80% of charge less $120 allowance
Not covered Not covered Not covered Not covered
Photochromatic / plastic transitions $75 Not covered Polarized 20% off retail Not covered
Contact Lenses (every 12 months)
Contact lens exam options Standard contact lens fit and follow up Premium contact lens fit and follow up
Up to $55 10% off retail
Not covered Not covered
Elective Conventional $100 allowance,
15% off balance over $100 $80 allowance
Disposable $100 allowance $80 allowance
Medically Necessary Covered in full $200 allowance
Employee Cost Per Pay
Employee $3.26
Employee + Spouse $6.52
Employee + Child(ren) $6.20
Family $9.74

16
EMPLOYEE ASSISTANCE PROGRAM (EAP) With Humana’s EAP and Work-Life Services you can find everyday resources for things like:
• Retirement planning
• Dealing with difficult co-workers
• Conflict/anger management
• Career development
• Communicating with your boss
• Resolving legal problems
• Finding schools
• Paying for school
Life made easier Your Employee Assistance Program (EAP) and Work- Life Services help you and your household members manage everyday life issues that can affect you at home and at work. You can call the toll-free number anytime during the day or night to talk with an experienced counselor who can help you find solutions. This program is confidential, and your employer pays all costs when you and members of your household use the services. The EAP gives you:
• Assistance and counseling in-person or over the telephone
• Assessment and assistance from a Work-Life specialist who is an expert in child care, adult care, or other everyday concerns
• Free 30-minute consultations with attorneys and financial counselors
• Access to a website with articles, discounts, podcasts, webinars, assessments, live chats, and databases to help you find local resources
Advantages
• Confidential
• One call gives you access to counseling, research and referrals, and legal and financial services
• We are always here to help you
• A website that lets you find answers on your own
EAP and Work-Life are provided for all eligible employees and household members. Personal information remains confidential according to all applicable state and federal laws.
Access is easy! 24 hours a day, seven days a week. Services provided by Humana EAP and Work-Life Services.
• Care for children with special needs
• Relationship issues
• Separation/divorce
• Child care
• Parenting/discipline
• Quitting smoking
• Older adult care
• Financial issues
• Stress and anxiety
• Depression
• Addiction
• Time management
• Adoption
• Losing weight
• Grief and loss
• Nutrition
EAP and Work-Life We’re here to help with your personal, work-related, and emotional concerns.
Humana.com/eap
• username: eap3
• password: eap3
24 hours a day, seven days a week.
Free and confidential 1-866-440-6556
EAP and Work-Life are available to all eligible employees of Floyd County (including dependents) regardless of whether you are enrolled in the County’s group health plan.

17
MEDICAL BILL SAVER EAP

18
BASIC LIFE AND AD&D
Term Life with Accidental Death & Dismemberment (AD&D) Insurance can provide money for your family if you die or are diagnosed with a terminal illness.
How does it work? You keep coverage for a set period of time, or “term.” If you die during that term, the money can help your family pay for basic living expenses, final arrangements, tuition and more.
AD&D Insurance is also available, which can pay a benefit if you survive an accident but have certain serious injuries. It can pay an additional amount if you die from a covered accident.
Who can get Term Life coverage? If you are actively at work at least 30 hours per week, you can receive coverage for:
Employee: You can receive a benefit amount of $10,000.
Who can get Accidental Death & Dismemberment (AD&D) coverage?
Employee: You can receive an AD&D benefit amount of $10,000.
What else is included?
A “Living” Benefit: If you are diagnosed with a terminal illness with less than 12 months to live, you can request 100% of your life insurance benefit (up to $250,000) while you are still living. This amount will be taken out of the death benefit and may be taxable.
Waiver of premium: Your cost may be waived if you are totally disabled for a period of time
Age reduction: Coverage amounts for Life and AD&D Insurance for you and your dependents will reduce to 65% of the original amount when you reach age 70, and will reduce to 50% of the original amount when you reach age 75. Coverage may not be increased after a reduction.
.

19
VOLUNTARY TERM LIFE AND AD&D
A simple, economical way to plan for your and your family’s future.
How does it work? You choose the amount of coverage that’s right for you, and you keep coverage for a set period of time, or “term.” If you die during that term, the money can help your family pay for basic living expenses, final arrangements, tuition and more.
AD&D Insurance is also available, which pays a benefit if you survive an accident but have certain serious injuries. It pays an additional amount if you die from a covered accident.
Who can get Term Life coverage?
If you are actively at work at least 30 hours per week, you may apply for coverage for:
Employee: Choose from $10,000 to $500,000 in $10,000 increments, up to 5 times your earnings. You can get up to $110,000 with no health questions during your initial enrollment.
Spouse: Get up to $500,000 of coverage in $5,000 increments. Spouse coverage cannot exceed 100% of the coverage amount you purchase for yourself. Your spouse can get up to $25,000 with no health questions, if eligible, during the initial enrollment.
Dependent: - Get up to $10,000 of coverage in $2,000 increments if eligible. One policy covers all of your children until their 19th birthday − or until their 26th birthday if they are full-time students. The maximum benefit for children live birth to 6 months is $1,000.
Who can get Accidental Death & Dismemberment (AD&D) coverage?
Employee: Get up to $500,000 of AD&D coverage for yourself in $10,000 increments to a maximum of 5 times your earnings.
Spouse: Get up to $500,000 of AD&D coverage for your spouse in $5,000 increments, if eligible.
Dependent: - Get up to $10,000 of coverage for your children in $2,000 increments if eligible.
What else is included?
A “Living” Benefit: If you are diagnosed with a terminal illness with less than 12 months to live, you can request 50% of your life insurance benefit (up to $750,000) while you are still living. This amount will be taken out of the death benefit, and may be taxable.
Waiver of premium: Your cost may be waived if you are totally disabled for a period of time. Portability: You may be able to keep coverage if you leave the company, retire or change the number of hours you work.
Age reduction: Coverage amounts for Life and AD&D Insurance for you and your dependents will reduce to 65% of the original amount when you reach age 70, and will reduce to 50% of the original amount when you reach age 75. Coverage may not be increased after a reduction.
Why is this coverage so valuable? If you buy a minimum of $10,000 of coverage during your initial enrollment, you can increase your coverage in the future up to
$110,000 to meet your growing needs. You won’t have to answer any health questions or take a health exam.
20
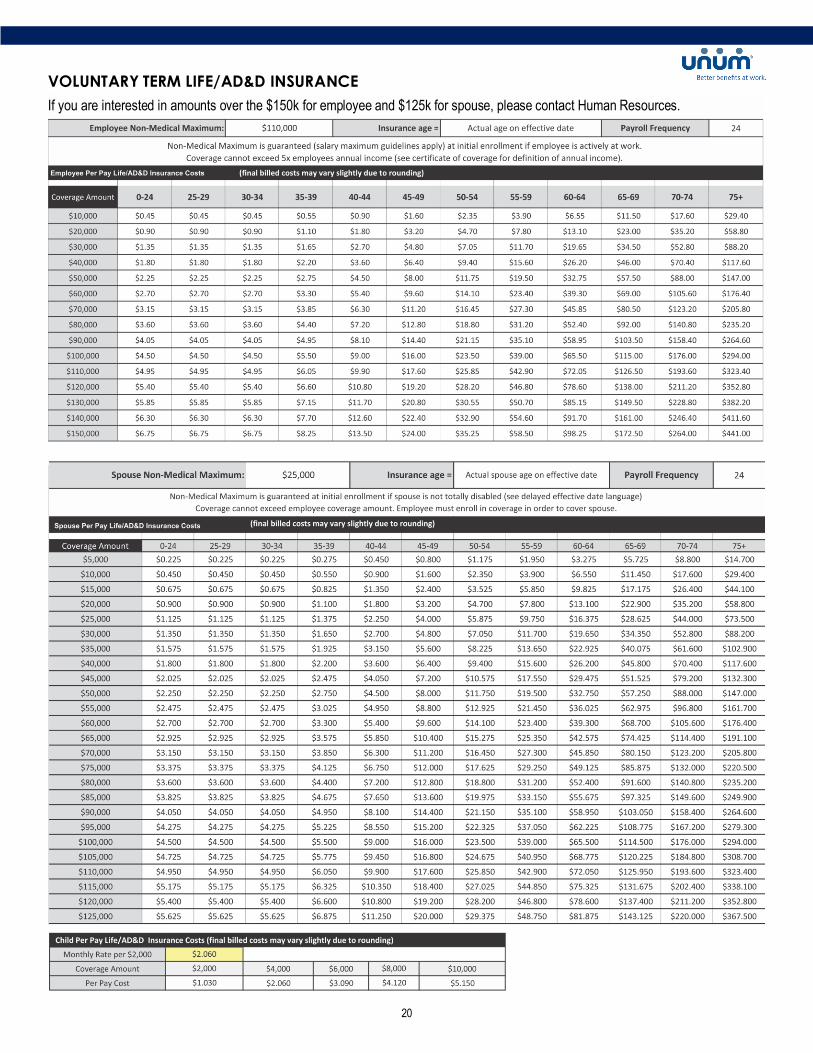
VOLUNTARY TERM LIFE/AD&D INSURANCE
If you are interested in amounts over the $150k for employee and $125k for spouse, please contact Human Resources.

21
COLONIAL VOLUNTARY BENEFITS
Group Disability Insurance You never know when a disability could impact your way of life. Fortunately, there’s a way to help protect your income. If a covered accident or sickness prevents you from earning a paycheck, Colonial’s group disability insurance can provide a monthly benefit for off-the-job disabilities to help you cover your ongoing expenses. Group Accident Insurance Colonial’s group accident insurance can help with medical or other costs associated with a covered accident or injury that your health insurance may not cover. Accident can include insect bite, poison ivy, cuts, burns, broken bones, etc. With Colonial’s group accident coverage, you may not need to use your savings or secure a loan to help pay those unexpected out-pf-pocket expenses. Coverage options are available for you, your spouse and eligible dependent children. This benefit is guarantee issue and helps with out-of-pocket expenses such as co-pays and deductibles when there is an accidental injury.
There is a $50 annual health screening benefit included with this benefit. Group Cancer Insurance Colonial’s cancer insurance helps provide financial protection through a variety of benefits. These benefits are not only for you but also for your covered family members. This product pays indemnity-based benefits to help cover medical and non-medical expenses related to cancer diagnosis and treatment. This includes initial diagnosis benefit and a choice of 2 levels of coverage.
There is a $100 health screening benefit included with this benefit. Group Critical Illness Insurance If you’re diagnosed with a covered critical illness, group critical illness insurance from Colonial can help with your expenses. This product provides a lump-sum benefit when a covered critical illness is diagnosed. Covered illnesses are heart attack, stroke, end stage
renal failure, permanent paralysis, blindness, coma and cardio by-pass surgery.
To learn more about the benefits available through Colonial, please contact your Human Resource department or visit the Employee Portal.

22
\

23
TRAVEL ASSISTANCE

24
TRAVEL ASSISTANCE

25
Compliance Notices
Premium Assistance Under Medicaid and the Children’s Health Insurance Program (CHIP)
If you or your children are eligible for Medicaid or CHIP and you’re eligible for hea lth coverage from your employer, your state may have a premium assistance program that can help pay for coverage, using funds from their Medicaid or CHIP programs. If you or your children aren’t eligible for Medicaid or CHIP, you won’t be eligible for these premium assistance programs but you may be able to buy individual insurance coverage through the Health Insurance Marketplace. For more information, visit . If you or your dependents are already enrolled in Medicaid or CHIP and you live in a State listed below, contact your State Medicaid or CHIP office to find out if premium assistance is available. If you or your dependents are NOT currently enrolled in Medicaid or CHIP, and you think you or any of your dependents might be eligible for either of these programs, contact your State Medicaid or CHIP office or dial 1-877-KIDS NOW or www.insurekidsnow.gov to find out how to apply. If you qualify, ask your state if it has a program that might help you pay the premiums for an employer-sponsored plan. If you or your dependents are eligible for premium assistance under Medicaid or CHIP, as well as eligible under your employer plan, your employer must allow you to enroll in your employer plan if you aren’t already enrolled. This is called a “special enrollment” opportunity, and you must request coverage within 60 days of being determined eligible for premium assistance. If you have questions about enrolling in your employer plan, contact the Department of Labor at www.askebsa.dol.gov or call 1-866-444-EBSA (3272). If you live in one of the following states, you may be eligible for assistance paying your employer health plan premiums. The following list of states is current as of July 31, 2018. Contact your State for more information on eligibility –
KENTUCKY – Medicaid INDIANA – Medicaid Website: https://chfs.ky.gov
Phone: 1-800-635-2570 Healthy Indiana Plan for low-income adults 19-64
Website: http://www.in.gov/fssa/hip/
Phone: 1-877-438-4479
All other Medicaid
Website: http://www.indianamedicaid.com
Phone 1-800-403-0864
To see if any other states have added a premium assistance program since July 31, 2018, or for more information on special enrollment rights, contact either:
U.S. Department of Labor U.S. Department of Health and Human Services Employee Benefits Security Administration Centers for Medicare & Medicaid Services www.dol.gov/agencies/ebsa www.cms.hhs.gov 1-866-444-EBSA (3272) 1-877-267-2323, Menu Option 4, Ext. 61565
Paperwork Reduction Act Statement According to the Paperwork Reduction Act of 1995 (Pub. L. 104-13) (PRA), no persons are required to respond to a collection of information unless such collection displays a valid Office of Management and Budget (OMB) control number. The Department notes that a Federal agency cannot conduct or sponsor a collection of information unless it is approved by OMB under the PRA, and displays a currently valid OMB control number, and the public is not required to respond to a collection of information unless it displays a currently valid OMB control number. See 44 U.S.C. 3507. Also, notwithstanding any other provisions of law, no person shall be subject to penalty for failing to comply with a collection of information if the collection of information does not display a currently valid OMB control number. See 44 U.S.C. 3512. The public reporting burden for this collection of information is estimated to average approximately seven minutes per respondent. Interested parties are encouraged to send comments regarding the burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden, to the U.S. Department of Labor, Employee Benefits Security Administration, Office of Policy and Research, Attention: PRA Clearance Officer, 200 Constitution Avenue, N.W., Room N-5718, Washington, DC 20210 or email [email protected] and reference the OMB Control Number 1210-0137.
OMB Control Number 1210-0137 (expires 12/31/2019)

26
NEWBORNS' AND MOTHERS' HEALTH PROTECTION ACT NOTICE Group health plans and health insurance issuers generally may not, under Federal law, restrict benefits for any hospital length of stay in connection with
childbirth for the mother or newborn child to less than 48 hours following a vaginal delivery, or less than 96 hours following a cesarean section. However,
Federal law generally does not prohibit the mother’s or newborn’s attending provider, after consulting with the mother, from discharging the mother o r her newborn earlier than 48 hours (or 96 hours as applicable). In any case, plans and issuers may not, under Federal law, require that a provider obtain
authorization from the plan or the insurance issuer for prescribing a length of stay not in excess of 48 hours (or 96 hours).
NOTICE OF PATIENT PROTECTIONS
generally allows the designation of a primary care provider. You have the right to designate any primary care provider who participates in our network and
who is available to accept you or your family members. For information on how to select a primary care provider, and for a list of the participating primary
care providers, contact Human Resources.
For children, you may designate a pediatrician as the primary care provider.
You do not need prior authorization from or from any other person (including a primary care provider) in order to obtain access to obstetrical or
gynecological care from a health care professional in our network who specializes in obstetrics or gynecology. The health care pro fessional, however, may
be required to comply with certain procedures, including obtaining prior authorization for certain services, following a pre-approved treatment plan, or
procedures for making referrals. For a list of participating health care professionals who specialize in obstetrics or gyneco logy, contact Human Resources.
NOTICE OF SPECIAL ENROLLMENT RIGHTS
If you are declining enrollment for yourself or your dependents (including your spouse) because of other health insurance or group health plan coverage, you may be able to enroll yourself and your dependents in this plan if you or your dependents lose eligibility for that other
coverage (or if the employer stops contributing toward your or your dependents’ other coverage). However, you must request enrollment
within 31 days after your or your dependents’ other coverage ends (or after the employer stops contributing toward the other coverage).
In addition, if you have a new dependent as a result of marriage, birth, adoption, or placement for adoption, you may be able to enroll yourself and your
dependents. However, you must request enrollment within 31 days after the marriage, birth, adoption, or placement for adoption.
To request special enrollment or obtain more information, contact Human Resources.
WOMEN'S HEALTH AND CANCER RIGHTS ACT NOTICES
If you have had or are going to have a mastectomy, you may be entitled to certain benefits under the Women’s Health and Cancer Rights Act of 1998
(WHCRA). For individuals receiving mastectomy-related benefits, coverage will be provided in a manner determined in consultation with the attending
physician and the patient for:
• All stages of reconstruction of the breast on which the mastectomy was performed;
• Surgery and reconstruction of the other breast to produce a symmetrical appearance;
• Prostheses; and
• Treatment of physical complications of the mastectomy, including lymphedema.
These benefits will be provided subject to the same deductibles and coinsurance applicable to other medical and surgical benefits provided under this
plan. Therefore, the following deductibles and coinsurance apply:
• $5,000 individual deductible, then 25% coinsurance
If you would like more information on WHCRA benefits, call your plan administrator.
Protections from Disclosure of Medical Information
We are required by law to maintain the privacy and security of your personally identifiable health information. may use aggregate information to design
a program based on identified health risks in the workplace. Your physician and the vendors who administer and provide screenings will not disclose
any of your personal information either publicly or to the employer, except as expressly permitted by law. Medical information that personally identifies you that is provided in connection with the wellness program will not be provided to your supervisors or managers and may never be used to make
decisions regarding your employment. In addition, all health information obtained through the wellness program will be maintained separately from your personnel records, stored electronically and encrypted, and not be used in making any employment decision. Appropriate precautions will be taken to
avoid any data breach, and in the event a data breach occurs involving information you provide in connection with the wellnes s program, we will notify you immediately. You will not be discriminated against in employment because of the medical information you provide as part of participating in the
wellness program, nor will you be subjected to retaliation if you choose not to participate.
Your health information will not be sold, exchanged, transferred, or otherwise disclosed except to the extent permitted by law to carry out specific
activities related to the wellness program, and you will not be asked or required to waive the confidentiality of your health information as a condition of participating in the wellness program or receiving a reward. Anyone who receives your information for purposes of providing you services as part of the
wellness program will abide by the same confidentiality requirements. may be provided with an aggregate report (summary of results with no identifying information) or a list of names of participants for programs where participation is tracked for the purposes of distributing rewards.
If you have questions or concerns regarding this notice, or about protections against discrimination and retaliation, please contact Human Resources.

27
GENERAL NOTICE OF COBRA RIGHTS
** Continuation Coverage Rights Under COBRA**
Introduction
You’re receiving this notice because you recently gained coverage under a group health plan (the Plan). This notice has important information about your right to COBRA continuation coverage, which is a temporary extension of coverage under the Plan. This notice explains COBRA continuation
coverage, when it may become available to you and your family, and what you need to do to protect your right to get it. When you become
eligible for COBRA, you may also become eligible for other coverage options that may cost less than COBRA continuation coverage.
The right to COBRA continuation coverage was created by a federal law, the Consolidated Omnibus Budget Reconciliation Act of 1985 (COBRA).
COBRA continuation coverage can become available to you and other members of your family when group health coverage would otherwise end. For more information about your rights and obligations under the Plan and under federal law, you should review the Plan’s Summary Plan Description or
contact the Plan Administrator.
You may have other options available to you when you lose group health coverage. For example, you may be eligible to buy an individual plan
through the Health Insurance Marketplace. By enrolling in coverage through the Marketplace, you may qualify for lower costs on your monthly premiums and lower out-of-pocket costs. Additionally, you may qualify for a 30-day special enrollment period for another group health plan for which you are
eligible (such as a spouse’s plan), even if that plan generally doesn’t accept late enrollees.
What is COBRA continuation coverage?
COBRA continuation coverage is a continuation of Plan coverage when it would otherwise end because of a life event. This is also called a “qualifying
event.” Specific qualifying events are listed later in this notice. After a qualifying event, COBRA continuation coverage must be offered to each person who is a “qualified beneficiary.” You, your spouse, and your dependent children could become qualified beneficiaries if coverage under the Plan is lost
because of the qualifying event. Under the Plan, qualified beneficiaries who elect COBRA continuation coverage must pay for COBRA continuation
coverage.
If you’re an employee, you’ll become a qualified beneficiary if you lose your coverage under the Plan because of the following qualifying events:
• Your hours of employment are reduced, or
• Your employment ends for any reason other than your gross misconduct.
If you’re the spouse of an employee, you’ll become a qualified beneficiary if you lose your coverage under the Plan because o f the following qualifying
events:
• Your spouse dies;
• Your spouse’s hours of employment are reduced;
• Your spouse’s employment ends for any reason other than his or her gross misconduct;
• Your spouse becomes entitled to Medicare benefits (under Part A, Part B, or both); or
• You become divorced or legally separated from your spouse.
Your dependent children will become qualified beneficiaries if they lose coverage under the Plan because of the following qualifying events:
• The parent-employee dies;
• The parent-employee’s hours of employment are reduced;
• The parent-employee’s employment ends for any reason other than his or her gross misconduct;
• The parent-employee becomes entitled to Medicare benefits (Part A, Part B, or both);
• The parents become divorced or legally separated; or
• The child stops being eligible for coverage under the Plan as a “dependent child.”
When is COBRA continuation coverage available?
The Plan will offer COBRA continuation coverage to qualified beneficiaries only after the Plan Administrator has been notified that a qualifying event has
occurred. The employer must notify the Plan Administrator of the following qualifying events:
• The end of employment or reduction of hours of employment;
• Death of the employee; or
• The employee’s becoming entitled to Medicare benefits (under Part A, Part B, or both).
For all other qualifying events (divorce or legal separation of the employee and spouse or a dependent child’s losing eligibility for coverage
as a dependent child), you must notify the Plan Administrator w ithin 60 days after the qualifying event occurs. You must provide this notice to your, Human Resources Department. The notice must include a description of the qualifying event and the date the qualifying event
occurred.
How is COBRA continuation coverage provided?
Once the Plan Administrator receives notice that a qualifying event has occurred, COBRA continuation coverage will be offered to each of the qualified
beneficiaries. Each qualified beneficiary will have an independent right to elect COBRA continuation coverage. Covered employees may elect COBRA
continuation coverage on behalf of their spouses, and parents may elect COBRA continuation coverage on behalf of their children.
COBRA continuation coverage is a temporary continuation of coverage that generally lasts for 18 months due to employment termination or reduction of hours of work. Certain qualifying events, or a second qualifying event during the initial period of coverage, may permit a beneficiary to receive a
maximum of 36 months of coverage.

28
There are also ways in which this 18-month period of COBRA continuation coverage can be extended:
Disability extension of 18-month period of COBRA continuation coverage
If you or anyone in your family covered under the Plan is determined by Social Security to be disabled and you notify the Plan Administrator in a timely fashion, you and your entire family may be entitled to get up to an additional 11 months of COBRA continuation coverage, for a
maximum of 29 months. The disability would have to have started at some time before the 60th day of COBRA continuation coverage and
must last at least until the end of the 18-month period of COBRA continuation coverage. Contact the Human Resources Department.
Second qualifying event extension of 18-month period of continuation coverage
If your family experiences another qualifying event during the 18 months of COBRA continuation coverage, the spouse and dependent
children in your family can get up to 18 additional months of COBRA continuation coverage, for a maximum of 36 months, if the Plan is properly notified about the second qualifying event. This extension may be available to the spouse and any dependent children getting
COBRA continuation coverage if the employee or former employee dies; becomes entitled to Medicare benefits (under Part A, Part B, or both);
gets divorced or legally separated; or if the dependent child stops being eligible under the Plan as a dependent child. This extension is only available if the second qualifying event would have caused the spouse or dependent child to lose coverage under the Plan had the f irst
qualifying event not occurred.
Are there other coverage options besides COBRA Continuation Coverage?
Yes. Instead of enrolling in COBRA continuation coverage, there may be other coverage options for you and your family through the Health Insurance
Marketplace, Medicaid, or other group health plan coverage options (such as a spouse’s plan) through what is called a “special enrollment period.” Some of these options may cost less than COBRA continuation coverage. You can learn more about many of these options at www.healthcare.gov.
If you have questions
Questions concerning your Plan or your COBRA continuation coverage rights should be addressed to the contact or contacts identified below. For more information about your rights under the Employee Retirement Income Security Act (ERISA), including COBRA, the Patient Protection and Affordable
Care Act, and other laws affecting group health plans, contact the nearest Regional or District Office of the U.S. Department of Labor’s Employee Benefits Security Administration (EBSA) in your area or visit www.dol.gov/ebsa. (Addresses and phone numbers of Regional and District EBSA Offices
are available through EBSA’s website.) For more information about the Marketplace, visit www.HealthCare.gov.
Keep your Plan informed of address changes
To protect your family’s rights, let the Plan Administrator know about any changes in the addresses of family members. You should also keep a copy,
for your records, of any notices you send to the Plan Administrator.

29
GENERAL FMLA NOTICE EMPLOYEE RIGHTS UNDER THE FAMILY AND MEDICAL LEAVE ACT THE UNITED STATES DEPARTMENT OF LABOR WAGE AND HOUR DIVISION
Leave Entitlements
Eligible employees who work for a covered employer can take up to 12 weeks of unpaid, job-protected leave in a 12-month period for the following
reasons:
• The birth of a child or placement of a child for adoption or foster care;
• To bond with a child (leave must be taken within 1 year of the child’s birth or placement);
• To care for the employee’s spouse, child, or parent who has a qualifying serious health condition;
• For the employee’s own qualifying serious health condition that makes the employee unable to perform the employee’s job;
• For qualifying exigencies related to the foreign deployment of a military member who is the employee’s spouse, child, or parent.
An eligible employee who is a covered servicemember’s spouse, child, parent, or next of kin may also take up to 26 weeks of FMLA leave in a single 12-
month period to care for the servicemember with a serious injury or illness.
An employee does not need to use leave in one block. When it is medically necessary or otherwise permitted, employees may take leave intermittently
or on a reduced schedule.
Employees may choose, or an employer may require, use of accrued paid leave while taking FMLA leave. If an employee substitutes accrued paid leave
for FMLA leave, the employee must comply with the employer’s normal paid leave policies.
Benefits & Protections
While employees are on FMLA leave, employers must continue health insurance coverage as if the employees were not on leave.
Upon return from FMLA leave, most employees must be restored to the same job or one nearly identical to it with equivalent pay, benefits, and other
employment terms and conditions.
An employer may not interfere with an individual’s FMLA rights or retaliate against someone for using or trying to use FMLA leave, opposing any practice
made unlawful by the FMLA, or being involved in any proceeding under or related to the FMLA.
Eligibility Requirements
An employee who works for a covered employer must meet three criteria in order to be eligible for FMLA leave. The employee must:
• Have worked for the employer for at least 12 months;
• Have at least 1,250 hours of service in the 12 months before taking leave;* and
• Work at a location where the employer has at least 50 employees within 75 miles of the employee’s worksite.
* Special “hours of service” requirements apply to airline flight crew employees.
Requesting Leave
Generally, employees must give 30-days’ advance notice of the need for FMLA leave. If it is not possible to give 30-days’ notice, an employee must
notify the employer as soon as possible and, generally, follow the employer’s usual procedures.
Employees do not have to share a medical diagnosis but must provide enough information to the employer so it can determine if the leave qualifies for FMLA protection. Sufficient information could include informing an employer that the employee is or will be unable to perform his or her job functions,
that a family member cannot perform daily activities, or that hospitalization or continuing medical treatment is necessary. Employees must inform the
employer if the need for leave is for a reason for which FMLA leave was previously taken or certified.
Employers can require a certification or periodic recertification supporting the need for leave. If the employer determines that the certification is
incomplete, it must provide a written notice indicating what additional information is required.
Employer Responsibilities
Once an employer becomes aware that an employee’s need for leave is for a reason that may qualify under the FMLA, the employer must notify the employee if he or she is eligible for FMLA leave and, if eligible, must also provide a notice of rights and responsibilities under the FMLA. If the employee
is not eligible, the employer must provide a reason for ineligibility.
Employers must notify its employees if leave will be designated as FMLA leave, and if so, how much leave will be designated as FMLA leave.
Enforcement
Employees may file a complaint with the U.S. Department of Labor, Wage and Hour Division, or may bring a private lawsuit against an employer.
The FMLA does not affect any federal or state law prohibiting discrimination or supersede any state or local law or collective bargaining agreement that
provides greater family or medical leave rights.
For additional information or to file a complaint: 1-866-4-USWAGE (1-866-487-9243) TTY: 1-877-889-5627 www.dol.gov/whd
U.S. Department of Labor | Wage and Hour Division

30
Important Notice from Floyd County Government About
Your Prescription Drug Coverage and Medicare
Please read this notice carefully and keep it where you can find it. This notice has
information about your current prescription drug coverage with Floyd County Government and about your options under Medicare’s prescription drug coverage. This information can help you decide whether or not you want to join a Medicare drug plan. If you are considering joining, you should compare your current coverage, including which drugs are covered at what cost, with the coverage and costs of the plans offering Medicare prescription drug coverage in your area. Information about where you can get help to make decisions about your prescription drug coverage is at the end of this notice. There are two important things you need to know about your current coverage and Medicare’s prescription drug coverage:
1. Medicare prescription drug coverage became available in 2006 to everyone with Medicare. You can get this coverage if you join a Medicare Prescription Drug Plan or join a Medicare Advantage Plan (like an HMO or PPO) that offers prescription drug coverage. All Medicare drug plans provide at least a standard level of coverage set by Medicare. Some plans may also offer more coverage for a higher monthly premium.
2. Floyd County Government has determined that the prescription drug coverage offered by the Floyd County Government Health and Welfare Plan is, on average for all plan participants, expected to pay out as much as standard Medicare prescription drug coverage pays and is, therefore, considered Creditable Coverage. Because your existing coverage is Creditable Coverage, you can keep this coverage and not pay a higher premium (a penalty) if you later decide to join a Medicare drug plan.
When Can You Join A Medicare Drug Plan?
You can join a Medicare drug plan when you first become eligible for Medicare and each year from October 15th
to
December 7th
.
However, if you lose your current creditable prescription drug coverage, through no fault of your own, you will also be eligible for a two (2) month Special Enrollment Period (SEP) to join a Medicare drug plan.
What Happens To Your Current Coverage If You Decide to Join A Medicare Drug Plan?
If you decide to join a Medicare drug plan, your current Floyd County Government coverage will not be affected. You can keep this coverage if you elect Part D as this plan will coordinate with Part D coverage.
If you do decide to join a Medicare drug plan and drop your current Floyd County Government coverage, be aware that you and your dependents will not be able to get this coverage back except for during the next annual open enrollment period or if you experience a qualifying event.
When Will You Pay A Higher Premium (Penalty) To Join A Medicare Drug
Plan?
You should also know that if you drop or lose your current coverage with Floyd County Government and don’t join a Medicare drug plan within 63 continuous days after your current coverage ends, you may pay a higher premium (a penalty) to join a Medicare drug plan later. If you go 63 continuous days or longer without creditable prescription drug coverage, your monthly premium may go up by at least 1% of the Medicare base beneficiary premium per month for every month that you did not have that coverage. For example, if you go nineteen months without creditable coverage, your premium may consistently be at least 19% higher than the Medicare base beneficiary premium. You may have to pay this higher premium (a penalty) as long as you have Medicare prescription drug coverage. In addition, you may have to wait until the following October to join.

31
For More Information About This Notice Or Your Current Prescription Drug Coverage…
Contact the person listed below for further information. NOTE: You’ll get this notice each year. You will also get it before the next period you can join a Medicare drug plan, and if this coverage through Floyd County Government changes. You also may request a copy of this notice at any time.
For More Information About Your Options Under Medicare Prescription
Drug Coverage…
More detailed information about Medicare plans that offer prescription drug coverage is in the “Medicare & You”
handbook. You’ll get a copy of the handbook in the mail every year from Medicare. You may also be contacted directly
by Medicare drug plans.
For more information about Medicare prescription drug coverage: Visit
Call your State Health Insurance Assistance Program (see the inside back cover of your copy of the “Medicare & You” handbook for their telephone number) for personalized help
Call 1-800-MEDICARE (1-800-633-4227). TTY users should call 1-877-486-2048.
If you have limited income and resources, extra help paying for Medicare prescription drug coverage is available. For information about this extra help, visit Social Security on the web at www.socialsecurity.gov, or call them at 1-800-772-1213 (TTY 1-800-325-0778).
Remember: Keep this Creditable Coverage notice. If you decide to join one of the Medicare
drug plans, you may be required to provide a copy of this notice when you join to show whether or not you have maintained creditable coverage and, therefore, whether or not you
are required to pay a higher premium (a penalty).