beneficial effects of a combined ... · web viewwj steinberg 99 transport for women in labour in...
TRANSCRIPT

The 21st Conference on Priorities in Perinatal Carein South Africa was held under the auspices of the
Department of Paediatrics, University of Cape Townand Department of Obstetrics and Gynaecology,
University of Stellenboschand sponsored by Abbott Laboratories SA (Pty) Ltd
i

Editor’s Note:
The articles included in these Proceedings were received electronically and have been included as submitted by the presenter/author. Some articles have been shortened. Abstracts were included where articles were not submitted.
ii

INDEX
BENEFICIAL EFFECTS OF A COMBINED MICRONUTRIENT SUPPLEMENTATION ON MATERNAL OXIDATIVE STRESS AND NEWBORN ANTHROPOMETRIC MEASUREMENTS: A RANDOMISED DOUBLE BLIND, PLACEBO-CONTROLLED TRIAL IN HEALTHY PREGNANT WOMEN. I Hininger 1
FAILURE TO DIAGNOSE IUGR: A MAJOR CAUSE OF AVOIDABLE PERINATAL DEATH IN DURBAN. NF Moran 2
CREMAPHOR VS. MIXED MICELLAR I.M. INJECTION FOR THE PREVENTION OF HAEMORRHAGIC DISEASE OF THE NEWBORN. K Bolton 7
EXPERIENCES WITH THE PERINATAL EDUCATION PROGRAMME IN THE RURAL EASTERN CAPE. D Jackson 8
THE MATERNAL CARE MANUAL OF THE PERINATAL EDUCATION PROGRAMME - NEW CURRICULUM MEDICAL STUDENTS COMPARED TO OLD CURRICULUM STUDENTS. GB Theron 11
BRINGING ABOUT CHANGE IN HEALTH CARE SERVICES: THE KALAFONG MODEL FOR NURSING STAFF ENRICHMENT. AE Pullen 15
MOWBRAY MATERNITY HOSPITAL OVER A ONE YEAR PERIOD. LL Linley 17
EARLY COMPARED WITH DELAYED ORAL FLUIDS AND FOOD AFTER CAESAREAN SECTION. L Mangesi 22
DECISION TO DELIVERY INTERVAL AT EMERGENCY CAESAREAN SECTION: UNACCEPTABLE DELAYS IN A LARGE TERTIARY HOSPITAL.
P Onyango-Okeyo 25
SEVERE ACUTE MATERNAL MORBIDITY (SAMM) IS A RAPID DIAGNOSTIC TOOL FOR EVALUATING MATERNAL CARE. L Cochet 29
EVIDENCE-BASED MEDICINE AT OBSTETRICS UNIT (KALAFONG HOSPITAL): AN AUDIT OF CURRENT PRACTICE. L Likanza 34
MANAGEMENT OF INCOMPLETE ABORTION IN SOUTH AFRICAN STATE HOSPITALS. H Brown 36
IS AN INCREASE IN CAESAREAN SECTION RATE INEVITABLE? H Van Zyl 38
EFFECT OF PRETORIA PASTEURISATION ON BACTERIAL CONTAMINATION OF EXPRESSED BREAST MILK. P Soma-Pillay 42
EARLY INTERMITTENT KANGAROO MOTHER CARE: BREASTFEEDING AT SIX WEEKS CORRECTED AGE. GF Kirsten, CL Kirsten, E Thompson 44
i

IMPLEMENTATION OF KANGAROO MOTHER CARE IN MPUMALANGA.I Pretorius 48
ASSESSING THE IMPLEMENTATION OF KANGAROO MOTHER CARE IN HEALTH CARE FACILITIES. A-M Bergh 51
THE VALUE OF A KANGAROO MOTHER CARE (KMC) UNIT AT KALAFONG HOSPITAL. E van Rooyen 56
A SURVEY OF THE SOCIAL, CULTURAL AND EDUCATIONAL BACKGROUND OF MOTHERS ADMITTED TO THE KMC UNIT AT KALAFONG HOSPITAL.
E van Rooyen 62
KANGAROO MOTHER CARE MADE EASY. E van Rooyen 65
CONTINUOUS KANGAROO MOTHER CARE AT A SECONDARY HOSPITAL IN THE WESTERN CAPE: AN UPDATE. M Franken, M Wates, G Kirsten,C Pieper 67
OXYTOCIN AND FETAL DISTRESS. H J Odendaal 69
FINDING THE CULPRIT - INTRAPARTUM HYPOXIA IN SOUTH AFRICAN HOSPITALS. E Buchmann 72
INDUCTION OF LABOUR FOR SEVERE PRE-ECLAMPSIA AFTER 34 WEEKS.P Roets 77
ECLAMPSIA: A PROSPECTIVE AUDIT OF 112 PATIENTS ADMITTED TO KING EDWARD VIII HOSPITAL OBSTETRIC HIGH CARE UNIT. F Paruk 81
ECLAMPSIA AT TYGERBERG HOSPITAL. J Pretorius 92
MATERNAL OUTCOME SIX YEARS AFTER PRESENTING WITH MILD TO MODERATE MID-TRIMESTER HYPERTENSION DURING PREGNANCY. DW Steyn 95
THE SPEED AND APPROPRIATENESS OF OBSTETRIC REFERRALS FROM A PHC FACILITY TO A SECONDARY HOSPITAL IN BLOEMFONTEIN.WJ Steinberg 99
TRANSPORT FOR WOMEN IN LABOUR IN SOWETO. T Mokaya 103
THE EFFECT OF BLOOD LOSS DURING THE INTRA-PARTUM PERIOD AND THE FIRST TWENTY FOUR HOURS AFTER THE DELIVERY ON THE HAEMOGLOBIN LEVEL VALUES OF THE PATIENT. C Gerber 107
EFFECTIVENESS OF NEVIRAPINE DELIVERY AT CORONATION HOSPITAL: AN UPDATE . L Thomas 109
ii

NEVIRAPINE: SHOULD IT BE SELF-ADMINISTERED OR ADMINISTERED BY HOSPITAL STAFF? M Chersich, L Rose, M Urban, G Gray 111
EXPANDING VOLUNTARY COUNSELLING AND TESTING (VCT) AND THE PROVISION OF INTERVENTIONS TO PREVENT VERTICAL TRANSMISSION OF HIV IN SOWETO, SOUTH AFRICA. M Chersich, A Violari, B Jivkov, B Botha, A Fiamma, JA McIntyre, GE Gray. 113
ATTITUDE OF MOTHERS WHO ARE HIV INFECTED TOWARDS INFANT FEEDING USING THEIR OWN PASTEURISED EXPRESSED BREAST MILK.KR Mokhondo 115
MTCT PROGRAMMES IN THE WESTERN CAPE. F Abdullah, NT Naledi, J Cromme,
I Cupido, E Coetzee 117
THE EFFECT OF VITAMIN A ON REDUCING MOTHER-TO-CHILD TRANSMISSION OF HIV IN BLOEMFONTEIN. WJ Steinberg 121
WHERE PARENTS PLAY A PASSIVE ROLE IN LIFE-SUPPORT DECISIONS: VLBW INFANTS AND PHYSICIAN COUNSELLING IN SOUTH AFRICA. TM Ranchod,JC Partridge, DE Ballot, AM Martinez, VA Davies 123
CASE REPORT AND LITERATURE REVIEW: FOETAL AKINESIA SEQUENCE DUE TO IN-UTERO SUBDURAL HAEMORRHAGE. J de Souza 125
SCREENING TOOLS FOR FETAL ALCOHOL SYNDROME IN THE EVALUATION OF COMMUNITIES AT HIGH RISK. D Viljoen 126
THE CONTINUED BURDEN OF POVERTY: DOES NICU CARE MAKE A DIFFERENCE. CH Pieper 128
EARLY-ONSET SEPSIS IN VERY LOW BIRTH WEIGHT INFANTS: HERE COME THE GRAM NEGATIVES? SC Velaphi 130
GROWTH AND METABOLISM OF INFANTS FED AN ACIDIFIED FORMULA WITH OR WITHOUT PROBIOTICS. PA Cooper 133
PERINATAL COUNSELLING AND LIFE-SUPPORT DECISIONS FOR EXTREMELY PREMATURE INFANTS IN SOUTH AFRICA. TM Ranchod, JC PartridgeBJ Cory, VA Davies, DE Ballot AM Martinez 136
HEALTHY BABY COMPETITION. D Tsotetsi 138
TOWARDS HUMANISATION OF CHILDBIRTH AT LOWER UMFOLOZI DISTRICT WAR MEMORIAL HOSPITAL: CREATING A VISION FOR CHANGE. D Nyasulu 140
iii

iv

HOW DO PREGNANT WOMEN EXPECT TO BE ADDRESSED BY DOCTORS? CN Mnyani 147
THE BETTER BIRTHS INITIATIVE: IMPLEMENTATION IN THE EASTERN CAPE.Z Jafta 150
ORAL FLUIDS AND FOOD DURING LABOUR: A SYSTEMATIC REVIEW.M Singata 152
OBSTACLES TO LABOUR COMPANIONSHIP AT BAMALETE LUTHERAN HOSPITAL IN RAMOTSWA-BOTSWANA. MM Mothibe 154
THE IMPORTANCE OF TOUCH. K Hansen 160
THE USE OF INHALATION ANALGESIA FOR INTRAPARUM PAIN RELIEF. EE Bekker 162
LOW-DOSE TITRATED ORAL MISOPROSTOL FOR LABOUR INDUCTION: A NEW REGIMEN. S Ferreira 164
MISOPROSTOL AND MECONIUM: CLINICAL AND LABORATORY STUDIES. BB Matonhodze 170
MISOPROSTOL FOR TREATING POSTPARTUM HAEMORRHAGE. B Maholwana 176
AN AUDIT OF THE ROLE FETAL DOPPLER ASSESSMENT CAN PLAY IN THE MANAGEMENT OF THE VERY LOW BIRTHWEIGHT COMPROMISED FETUS.JJL de Souza 180
PAIN RELIEF IN LABOUR AT MOWBRAY MATERNITY HOSPITAL: AUDIT AND INTERVENTION. S Fawcus 186
IS PRETERM LABOUR UNAVOIDABLE, BUT ARE DEATHS DUE TO PREMATURITY AVOIDABLE? RC Pattinson 188
PERINATAL PROBLEM IDENTIFICATION PROGRAM (PPIP) VERSION 2. JD Coetzee 195
AN ANALYSIS OF AVOIDABLE FACTORS IN 616 PERINATAL DEATHS IN 7 RURAL HOSPITALS. NC Mzolo 197
PERINATAL MORTALITY AT MIDWIFE OBSTETRIC UNITS: A REVIEW OF 9 YEARS: 1993-2001. DH Greenfield 202
PERINATAL MORTALITY AT LYDENBURG HOSPITAL - CHANGING PATTERNS OVER A FOUR YEAR PERIOD FROM 1996 TO 1999. NM Soodi 206
v

AUDIT OF PERINATAL MORTALITY RATE: EKOMBE HOSPITAL 1994-2000.LJ Blanco 208
SURVIVAL OF PREMATURE VERY LOW BIRTHWEIGHT INFANTS BORN AT MADADENI DISTRICT HOSPITAL - A 9 YEAR REVIEW. FS Bondi 212
SAVING BABIES: A PERINATAL CARE SURVEY OF SOUTH AFRICA 2001.RC Pattinson 215
PROCEEDINGS DATABASE: PROCEEDINGS OF THE PRIORITIES IN PERINATAL CARE CONFERENCES (1982-2001). RV Prinsloo 219
PERINATAL CHALLENGES AND OPPORTUNITIES IN HEALTH MANAGEMENT.N Bergman 220
THE EFFECT OF INVOLVING PRIVATE PRACTITIONERS ON THE QUALITY OF ANTENATAL CARE OF THE INDIGENT POPULATION OF TEMBISA.KR Mokhondo 225
A COMPARISON BETWEEN FOUR MIDWIFE OBSTETRIC UNITS IN THE PRETORIA REGION. NT Mabale 227
EXPERIENCES IN USING A MULTIDICIPLINARY APPROACH IN THE DEVELOPMENT OF QUALITY MATERNAL HEALTH SERVICES IN A DEEP RURAL AREA.S Mbambo 229
EXPERIENCES WITH COMMUNITY PARTNERSHIP IN CHANGING HEALTH SEEKING BEHAVIOUR IN DEEP RURAL AREAS. BR Ntsuntsha 232
MPUMALANGA MCWH CLINICAL SKILLS CAPACITY AUDIT (CCA) 2000 REPORT.
NP Godi 233
vi

BENEFICIAL EFFECTS OF A COMBINED MICRONUTRIENT SUPPLEMENTATION ON MATERNAL OXIDATIVE STRESS AND NEWBORN ANTHROPOMETRIC MEASUREMENTS: A RANDOMISED DOUBLE BLIND, PLACEBO-CONTROLLED TRIAL IN HEALTHY PREGNANT WOMEN
I Hininger, M Favier, J Arnaud, H Faure, JM Thoulon, E Hariveau, A Favier, A-M Roussell
During pregnancy, physiological, metabolic and hormonal changes often result in mineral, trace element and vitamin deficiencies that might be corrected by a nutrient supplementation. Beneficial effects of supplementation have been observed in pregnant women exhibiting high risks of nutritional deficiencies and in pathological pregnancies. Studies in healthy pregnant women are scarce and the question of the interest of a multivitamin and mineral supplementation in such a population is a matter of debate. To investigate the possible beneficial effects of a micronutrient supplementation during pregnancy on maternal oxidative stress and newborn anthropomorphic characteristics, we performed a randomized, double-blind, placebo-controlled trial on 100 healthy pregnant women. From 14 +/-2 weeks of gestation to delivery, 50 women received a daily combination of minerals, trace-elements and vitamins and 50 received a placebo. Plasma oxidative stress parameters (TBARs, C=O groups, SH groups) and micronutrient levels in mothers were measured at 14 and 38 weeks of gestation and anthropomorphic characteristics (weight, height, head circumference) in newborn. In the supplemented group, folic acid, vitamin C, E, B2, B6 and p-carotene levels were higher than in placebo group. There was a positive correlation between plasma SH protein groups and vitamin C concentrations in blood and a negative correlation between plasma C=O groups and Zn and vitamin C levels. Birth weights were increased by 10% and number of low newborn weights (<2700 g) decreased significantly when the mother received the supplementation.Maternal plasma Zn levels were positively correlated to the newborn heights.
1

FAILURE TO DIAGNOSE IUGR: A MAJOR CAUSE OF AVOIDABLE PERINATAL DEATH IN DURBAN
NF MoranDepartment of Obstetrics and Gynaecology, Nelson R. Mandela School of Medicine, University of Natal, Durban, Republic of South Africa
IntroductionA prospective population-based perinatal mortality audit has been conducted at Mahatma Gandhi Memorial Hospital (MGMH), in Phoenix, Durban since July 2001. Since July 2001, MGMH, (a level 2 hospital), and its satellite clinics, have provided the main obstetric service for the Northern suburbs/townships of Durban, which have a population of at least one million people. There are 15 midwife-run clinics in the area providing antenatal care, but the great majority of clinic deliveries take place at just four of these clinics, as these four are the only ones which provide a 24-hour service. The data presented is derived from the first seven months of the audit (July 2001 - January 2002). Intra-uterine growth restriction (IUGR) was identified as a major cause of avoidable death. This paper analyses these IUGR-related deaths, and identifies 3 types of error during antenatal care which resulted in failure to diagnose IUGR and therefore led to these deaths.
MethodsPerinatal deaths occurring at the hospital were identified by daily review of the hospital labour ward and neonatal nursery records, and summarised by junior doctors. Deaths occurring at the satellite clinics were summarised by clinic midwives. Deaths occurring outside a health facility, where the mother subsequently presented to the hospital or to a clinic in the immediate post-natal period were also included. For each death, the cause of the death and any avoidable factors were recorded according to the codes listed in the Perinatal Problem Identification Programme. All summaries were reviewed by a consultant (the author), referring to the case-notes when available. Where necessary, the initial
2
conclusions about the cause of death or avoidable factors were modified following the review. Deaths were labelled either as “avoidable” or not. An avoidable death was defined as one which was clearly due to an error or omission on the part of a member of the health care team. In other words, if the error or omission had not occurred, then, in all likelihood, the death would not have occurred. Deaths due to patient factors or administrative factors (e.g. lack of transport) were not included in the definition.
Results (July 2001- January 2002)
Total deliveries (500g): 6296 Total perinatal deaths (PNDs): 234 Perinatal mortality rate (PNMR): 37.2 per 1000 Avoidable PNDs: 40 (17%) Avoidable PNMR: 6.4 per 1000
CAUSES OF DEATHN0 %
Preterm labour 38 16.2No notes 37 15.8Unexplained MSB 31 13.2Labour-related hypoxia 31 13.2IUGR 28 12.0Abruptio placentae 15 6.4
PNMR due to IUGR: 4.5 per 1000
Sub-classification of PNDs due to IUGR (total 28 deaths):Idiopathic IUGR 18IUGR with pre-eclampsia 5Postmaturity 5
Avoidable PNDs due to IUGR: 2175% of all PND due to IUGR were avoidable
CAUSES OF AVOIDABLE DEATH (total of 40 avoidable deaths):N0 %
IUGR 21 52.5Labour-related hypoxia 12 30.0Abruptio placentae 2 5.0
The following recurrent errors during antenatal care were identified from the 21 cases of avoidable death due to IUGR. These errors resulted in
3

failure to diagnose IUGR. In some cases more than one of the errors occurred in the same case:
4

1. Incorrect assessment of the height of fundus, leading to overestimation of the size of the fetus. The antenatal care provider records what he or she thinks the height of fundus ought to be according to the gestational age, rather than recording the true measurement. The antenatal card therefore reveals no abnormality of growth, and no discrepancy between dates and height of fundus, whereas in fact the fetus is small for dates. IUGR is therefore missed.This error occurred in 5 (18%) cases of perinatal death due to IUGR.
2. Ignoring dates according to last menstrual period (LMP).The dates according to the LMP are simply not calculated, or not recorded on the antenatal card. This leads to problems such as failure to recognize post-dates pregnancies. It also results in failure to correlate the fundal height measurement to the gestational age according to dates, so that a discrepancy between the two, or poor growth of the height of fundus is not recognized. A common reason for the dates being ignored is that the antenatal care provider prefers to rely on the gestational age estimate provided by a late ultrasound scan, which often grossly underestimates the true gestational age, particularly when there is IUGR.This error occurred in 12 (43%) cases of perinatal death due to IUGR.
3. Failure to act when there is poor growth of the height of fundus.This danger sign is ignored, and routine antenatal care continued, and IUGR remains undetected.This error occurred in 11 (39%) cases of perinatal death due to IUGR.
DiscussionThe rate of perinatal mortality due to IUGR recorded in this study (4.5 per 1000) is much higher than that recorded in the national perinatal audit, which suggested that deaths due to IUGR occurred in only 1 in 1000
5

deliveries. Furthermore the importance of IUGR as a cause of avoidable death is not something that has been highlighted by the national report.The three recurrent errors in antenatal care identified as leading to these avoidable deaths demonstrate a lack of insight amongst antenatal care providers in Durban with regard to the diagnosis of IUGR and the role of the symphysis-to-fundal height (SFH) measurement as a screening tool for IUGR. It is possible that this is a deficiency specific to Durban, or KwaZulu-Natal (KZN), accounting for the high rate of avoidable death from IUGR identified in this study. A possible explanation for this is the fact that the standard maternity case record currently used in KZN does not include a graph for charting the growth of the SFH against gestational age. The filling of such a graph is part of routine antenatal care in many other parts of the country, and facilitates the diagnosis of IUGR.Alternatively, deaths due to IUGR may be equally common nationwide, but lower rates may be recorded because the diagnosis of IUGR is missed during perinatal audit. In the audit reported here from MGMH, of the 28 deaths eventually classified as deaths due to IUGR, only 8 were initially attributed to IUGR. The other 20 were initially classified as unexplained macerated stillbirths. However, following review by the consultant, these 20 deaths were re-classified as being due to IUGR. This diagnosis of IUGR was made according to the best judgement of the consultant, taking into account all the evidence available from the maternity case record, and from discussion directly with the patient where possible. Important information that was always considered in making the diagnosis included the best estimate of gestational age, the birth weight, and the recordings made at each antenatal visit. Neonatal assessment did not contribute to the diagnosis as all the cases in question were stillbirths.Had these 20 deaths not been re-classified as IUGR deaths, this would have reduced the percentage of deaths due to IUGR from 12% to 3.4%, and the perinatal mortality rate due to IUGR from 4.5 to 1.3 per 1000. Furthermore the percentage of deaths classified as unexplained macerated stillbirths would have been increased from 13.2 to 21.8%. The
6

20 deaths which were re-classified as IUGR would otherwise have made up 39% of the unexplained stillbirths.Unexplained intrauterine deaths have accounted for about 25% of all deaths recorded in the national perinatal audit conducted since the year 2000. Finding out what the primary pathology underlying these intrauterine deaths is has been identified as a research priority. The evidence presented in this paper suggests that at least in Durban, a significant proportion of deaths that have previously been labelled as unexplained intrauterine deaths are in fact due to IUGR. A problem in identifying IUGR as the true cause of death occurs because the people who summarise these cases often have limited insight into how to diagnose IUGR. They may even be the very same people who have made the errors in the antenatal period which have led to a failure to diagnose IUGR. The same could well be true in the rest of the country. In order to obtain a more accurate picture of the contribution of IUGR to perinatal mortality, it would be necessary for all cases of unexplained intrauterine death to be routinely reviewed by a senior maternity care worker with good insight into the diagnosis of IUGR. As a large proportion of IUGR deaths are avoidable, it would seem important to review cases of “unexplained” IUD more carefully when compiling any future national perinatal care surveys.
Conclusion and SolutionsIUGR is a major cause of avoidable perinatal death in Durban. Specific recurrent errors in antenatal care have been identified which demonstrate a lack of insight amongst those providing antenatal care about how to diagnose IUGR. At a local level one step towards improving this situation would be the introduction into routine antenatal care in the province of a graph for charting the growth of the SFH against gestational age. Introducing such a graph, however, would not in itself be a solution, unless it is accompanied by an education programme on how to use it, and an on-going monitoring programme to ensure that it is being used appropriately.
7
At a national level, closer scrutiny of unexplained intrauterine deaths, looking for evidence of IUGR, is recommended, so as to clarify whether IUGR is also a major cause of avoidable perinatal death nationwide.
8

CREMAPHOR VS. MIXED MICELLAR I.M. INJECTION FOR THE PREVENTION OF HAEMORRHAGIC DISEASE OF THE NEWBORN
K BoltonCoronation Hospital and the University of the Witwatersrand, Johannesburg.
For various reasons, the developed world has moved away from intra-muscular injection of Vit K for the prevention of haemorrhagic disease of the newborn (HDN) and repeated oral doses of the mixed micellar formulation are now preferred. Limited access to newborns in the developing world makes the “old” regime of a single i.m. dose on the first day of life an attractive alternative but the cremaphor preparation is not longer being produced. Little scientific data exists regarding the use of the new preparation given i.m. as a single dose for the prevention of HDN yet this practice has been widely adopted in South Africa.
StudyForty normal full-term babies born to mothers intending to breast-feed were randomised into two groups. Study babies received i.m. mixed micellar Vit K while controls received the i.m. cremaphor preparation. Cord serum PIVKA levels were measured, Vit K peak in babies at 2 hours post administration and Vit K & PIVKA levels at two weeks of age. The preliminary results will be presented.
9

EXPERIENCES WITH THE PERINATAL EDUCATION PROGRAMME IN THE RURAL EASTERN CAPE
D Jackson, University of the Western Cape; M Semane, B Madikizela, A Siganqwe, G Mbalo, S Masilela, Department of Health Eastern Cape Province; H de Groot, University of Cape Town; D McCoy, Health Systems Trust
The Health Systems Trust Initiative for Sub-district Support (ISDS) Obstetric Support Programme (OSP) was started in the former Region E area of the Eastern Cape. The focus of ISDS is to provide support and training for the local district health departments to improve the quality of health services.
After a situation analysis of maternity services in the region conducted during the second quarter of 2000, a planning launch was held in August 2000 with key role players in the region. Results of the situation analysis were reviewed and a way forward and programme plan for the ISDS-OSP were planned.
ISDS - Obstetric Support Programme Objectives
1) Reduce maternal and perinatal mortality
2) Improve the quality of obstetric services in Region E through the introduction of:
Perinatal audit Continuing in-service education & training Introduction of uniform maternal health guidelines Monitoring & evaluation
Continuing education and training were to be a major activity of the programme. This activity included two primary components: a) Continuing Perinatal Education (COPE) visits by a community
obstetrics specialist AND b) the Perinatal Education Programme (PEP).
10

On-site Training & Continuing Education Monthly visits by consultant obstetrician 200 total CPD hours in 2000-2001 20-25 hours per hospital Examples of Topics: CPD, PPH, Perinatal HIV, PIH,
PARTOGRAM, Mortality meetings, Ward Rounds
The focus of this report is the results from the PEP Programme in the region.
Why the Perinatal Education Programme (PEP)? Proven programme Recommended by National Maternal Care Guidelines
Selection of 1st Module – Perinatal HIV OSP Situation Analysis indicated that HIV/AIDS was a major concern
of local maternity staff NCCEMD – HIV/AIDS now leading cause of maternal death Also size & cost of module
Perinatal HIV Module supported by COPE lectures On-going lecture series as part of OSP Special lecture series by a Perinatal HIV Specialist
Maternal Care Module – 2002 COPE lecture series planned to coincide with Maternal Care Module chapters
Innovative strategy to promote registration & exam completion Registration forms in the form a contract Sisters pay ½ & HST pays ½ of registration fee If sister passes exam then gets refund of registration fee
11

Collaboration with MESAB
Participation Perinatal HIV - 9 of 11 Hospitals & CHCs HIV Round 1 – 80 sisters & 1 doctor HIV Round 2 – 30 sisters Maternal Care – Currently Registering
Examination Results HIV Round 1 56 (69%) took exam to date 100% pass with only 2 re-exam Average Score = 95% HIV Round 2 Exam schedule through May/June 2002 Maternal Care – exams late 2002 or early 2003
Lessons Learned & Success Factors Enthusiastic maternity staff Support from Administration – especially maternity matrons &
senior sisters Excellent well tested learning modules Companion lecture series Incentive programme Resources to facilitate ordering, transport of modules & exams Flexibility for exam scheduling
ConclusionPEP can be successfully implemented even in remote hospitals with a commitment by hospital management and a minimal supplementation of resources to facilitate PEP ordering and examination process“We feel empowered to provide better quality of care to our patients” - Quote from a nursing sister after passing the PEP exam
12

THE MATERNAL CARE MANUAL OF THE PERINATAL EDUCATION PROGRAMME – NEW CURRICULUM MEDICAL STUDENTS COMPARED TO OLD CURRICULUM STUDENTS
GB Theron, D GrovéDepartment of Obstetrics and Gynaecology, Faculty of Health Sciences, Stellenbosch University, Tygerberg
IntroductionA new system-based curriculum for medical students, that is horizontally and vertically integrated, was introduced in 1999. The curriculum is problem-orientated and outcome-based. While groups of students following the new curriculum rotate through obstetrics for four-week periods throughout the year, a single mid-year block provides the theoretical background for the entire class. An introduction to obstetrics is provided during the first 4 days of each rotation. Three questions were of interest: (1) Do the practical skills training and educational video requirements of the first and second semesters differ? (2) Does the equivalent performance differ? (3) How do the performances of old and new curriculum students compare? Following the introduction the students rotate for 10 days each through one of 4 regional hospitals and the tertiary hospital with its attached community antenatal clinics and midwife obstetric units.
MethodsAn introduction to clinical obstetrics is provided for the third years with hands-on skills training in a skills laboratory and educational videos. The Maternal Care Manual of the Perinatal Education Programme was the study material for both the new and old curriculum students during the clinical rotation. A questionaire was completed by each student at the end of the rotation consisting of questions using a Likert response format (0=very poor and 10=excellent) and open-ended questions for qualitative evaluation. The results of the questionaire and end of block evaluation of students doing the first two rotations (Group 1) were compared to students doing the last two rotations (Group 2). End of block student
13

evaluations were also compared to two groups of old curriculum students from 2001 and 2000.
ResultsQuestionnaires were received from 152 (96.8%) of the 157 third year medical students. The mean scores for the skills laboratory (8.4 vs 8.1; p=0.27) and videos (6.7 vs 6.3; p=0.29) for Groups 1 and 2 did not differ (Table I). However, the videos were regarded as of less value. As shown in Table II the marks of Group 2 were significantly better in 3 clinical questions (total marks = 45) during the end of block evaluation (mean: 35.8 vs 32.2, median 37 vs 32; p<0.0001). However the ability of the 2 groups to interpret antenatal cards and partograms did not differ (Table II). The mean end of block marks for clinical questions (total marks = 45) of the new curriculum students were significantly better than the old curriculum 2001 students (74.8 vs 65.3; p<0.00001) as shown in Table III. There were no differences with regards to interpretation of the antenatal card, however the new curriculum students interpreted the partogram significantly better (Table III). The mean marks of the old curriculum students of 2001 and 2000 did not differ (48.1 vs 48.9).
ConclusionsThe same introduction to clinical obstetrics can by used for third year students during both semesters. Following the midyear theory block, the ability of students to answer questions on clinical cases improved significantly. However, the ability to interpret clinical documents did not. The interpretation of the partogram by the new curriculum students was significantly better than the old curriculum students. The Maternal Care Manual was of great value as a study guide, enabling students with little theoretical knowledge to complete a clinical rotation. The problem-based new curriculum resulted in an improved performance in spite of less theoretical training.
14

Table IGroup 1 Group 2 P-value
Skills laboratory* mean (S) 8.4 (1.2) 8.1 (1.5) 0.27* median 8 8* range 5 – 10 5 – 10
Videos* mean (S) 6.7 (1.9) 6.3 (2.3) 0.28* median 7 7* range 0 – 10 0 – 10
Likert scale 0 = very poor 10 = excellent
Table IIGroup 1 Group 2 P-value
Clinical questionsTotal = 45* mean (%) 32.2 (71.6) 35.8 (79.1) 0.0002* std dev 4.4 5.9* median 32 37
Antenatal cardTotal = 15* mean (%) 9.8 (65.3) 9.7 (64.7) 0.82* std dev 2.5 3.1* median 10 10
PartogramTotal = 15* mean (%) 10.6 (70.7) 10.4 (69.3) 0.65* std dev 2.8 2.2* median 11 11
15

Table III Old and New Curriculum3rd years 4th years 4th years2001 2001 2000
Clinical questionsTotal = 45* mean (%) 33.7 (74.8) 29.4 (65.3) 29.9 (66.5)*std dev 5.7 5.7 6.3* median 33 30 30.5* p-value 0.0000 0.43
Antenatal cardTotal = 15* mean 9.1 9.2 9.7* std dev 3.3 3.1 2.8* median 10 9 10
PartogramTotal = 15* mean 10.5 9.5 9.4* std dev 2.5 2.6 2.5* median 11 10 9* p-value 0.0003
16

BRINGING ABOUT CHANGE IN HEALTH CARE SERVICES: THE KALAFONG MODEL FOR NURSING STAFF ENRICHMENT
AE PullenMRC Unit for Maternal and Infant Health Care Strategies, University of Pretoria
IntroductionDuring the last few years there has been wide spread negative reporting on the quality of care. Nurses are feeling the pressure from patients who lash out at them because of poor quality of care. A need was identified to develop an enrichment model to enable nurses to be placed back in a situation where they can fulfil their professional role and responsibilities in striving for excellence. Enrichment is viewed as building competence and self-confidence, in order to solve problems and make effective decisions to bring about change. Enrichment implies a positive affirmation of the feeling of being accepted, valued, loved, and to belong. Enrichment ensures positive motivation, excitement and commitment to strive for excellence to meet personal and professional goals. Such a model was developed at Kalafong Hospital.
The paper aims to present the model and how it can be used to bring about change in a hospital context.
Aim of the studyThe aim of the study was to describe an Enrichment Model for Nursing Staff at Kalafong Hospital. Three objectives were set: Phase 1: To explore and describe the needs and problems of nurses, which should be included in an Enrichment Model at Kalafong Hospital. Phase 2: To describe an Enrichment Model based on the empirical findings.Phase 3: To implement, validate and refine the Enrichment Model.
17
MethodDuring Phase 1 empirical data was generated through focus groups (n=20) and individual interviews (n=20). Theoretical sampling was done to determine the participants (n=300). During Phase 3, a goal directed selection of 5 units was done to implement and refine the model.
Findings
The preliminary results of the study were presented at Priorities during 2001. This model as support system for nursing staff in a hospital context may prove to be a valuable tool to bring back excellence in nursing and health care.
18

MOWBRAY MATERNITY HOSPITAL OVER A ONE YEAR PERIOD
SM Kroon, LL Linley
BackgroundMowbray Maternity Hospital (MMH) is a level 2 maternity hospital with approximately 550 deliveries per month. Most are level 2 obstetric referrals from the PMNS Midwife Obstetric Units (MOUs). There are 50 neonatal beds, and 6 ventilator spaces.A significant number of the infants born on site are critically ill requiring level 3 care. Ill neonates are also referred to the Neonatal Unit from the MOUs, other provincial hospitals and very occasionally private hospitals.From time to time, the necessity for a level 3 neonatal unit at a level 2 obstetric hospital is questioned. Our growing impression is that this level of neonatal care at such an institution is essential for an optimal perinatal service. Hence this audit.
Of secondary concern, in 1998, bilirubin measurement facilities were withdrawn from the MOUs. TSBs are now sent to MMH for processing. The new system is fraught with delays.We audited the number of admissions for neonatal jaundice (NNJ) and the number of exchange transfusions before and after the change in the NNJ surveillance system. Aim To assess the appropriateness of the neonatal service offered at a level
2 Obstetric Hospital viz Mowbray Maternity Hospital. To attempt to quantify the effect on the neonatal unit at MMH, of the
change in MOU surveillance for neonatal jaundice.
MethodsAn audit was conducted of Neonatal Unit admissions from 01/01/2000 to 31/12/2000 in terms of place of birth, birth weight category, respiratory
19

support, crude outcomes (mortality), admissions for NNJ and exchange transfusions.Information was obtained from computerised admission data, selected folders, neonatal discharge statistics, neonatal death register and neonatal death (NND) summaries.MMH mortality data was compared to national state service (PIPP & Baragwanath Hospital) and private sector neonatal admissions.The level 3 function was assessed by examining ventilation data in terms of birth weight category, duration of ventilatory support and survival. The number of ventilator days to produce 1 survivor in weight categories below 1500g was used as a crude surrogate measure of cost effectiveness of ventilation.
The number of admissions for NNJ and the number of exchange transfusions (severity indicator) up to the end of 1998 were compared with those in the three years subsequent to the changed NNJ surveillance system.
ResultsAdmissions by Place of Birth:Of 1369 babies admitted: 1029 (75,2%) were born at MMH. 282 (20,6%) were born at MOU's. 55(4%) were born at public hospitals outside the PMNS. 3 (0,2%) were born in private hospitals.
Mortality:The Overall MMH Neonatal Mortality Rate by Weight (livebirths + outborn admissions) 65 ELBW babies (500 - 999g), 47 died (72% mortality) 139 VLBW babies (1000 - 1499g), 14 died (10% mortality) 468 LBW babies (1500 - 2499g), 12 died (2,5% mortality) 697 babies >2499g, 20 died (3% mortality)
20

21

Corrected Neonatal Mortality Rate for the neonatal unit at MMH:There were 1369 admissions to the neonatal unit recorded in the annual statistics, and 93 babies died at MMH over the same time period (crude overall mortality rate 67,9/1000). However, 5 deaths recorded in the annual hospital statistics did not appear in the monthly neonatal statistics (2VLBW, 1LBW and 2>2499g). It is likely that these 'ghost' deaths were stillbirths mistakenly registered as NNDs. Five babies died after 28 days of life, and are therefore infant deaths. Corrected total NNDs are therefore 83. 17 NNDs (12 <1000g; 1 2000-2499g and 4 >2499g) were unresuscitatable in Labour Ward, and never reached the neonatal unit, but do appear in the monthly statistics, making the corrected total number of NNDs for our neonatal unit 66, and the corrected neonatal mortality rate for the neonatal unit 48.2 per 1000. Causes of death:Immaturity 45%Hypoxic Ischaemic Encephalopathy 10%Cogenital Anomaly 11%Infection 4%Preterm + perinatal hypoxia 7%MAS/PPHN 5%Other 8%
Note:2000-2499g: 9 deaths: 5 lethal congenital anomalies, 2 congenital infections, 1 MAS/PPHN and 1 massive subaponeurotic haemmorrhage
1500-1999g: 2 deaths:1 lethal congenital anomaly, 1 sudden unexplained death at 27 days of age
Ventilation:184 babies were ventilated for a total of 833 days (average 4,5 days)169 babies were supported with CPAP
22

Ventilation by Place of Birth:138 (69%) born MMH45 (22.5%) born MOUs13 (6.5%) born non-PMNS hospitals4 (2%) born before arrival
Ventilation by Weight, and Survival:26 (13%) < 1000g 14 (54%) 58 (29%) 1000-1499g 48 (83%) 26 (13%) 1500-1999g 26 (100%) 16 (28%) 2000-2499g 12 (75%) 74 (37%) >2500g 60 (82%)
Overall survival of babies offered ventilatory support is 80% (160/200)Ventilator Days to produce one survivor in infants <1000g: 15,5 daysVentilator Days to produce one survivor in infants 1000-1499g: 7,7 days
Neonatal Jaundice:Exchange transfusions and admissions for neonatal jaundice 1996-2001:Admissions 4 6 5 8 10 7Exchange transfusions 124 149 64 113 127 171 1996 1997 1998 1999 2000 2001(end October)
DiscussionMost babies requiring neonatal unit admission are referred appropriately in-utero to MMH. About half of all admissions weigh <2500g. Unfortunately, gestational age data is unreliable and has not been included in this audit.The highest mortality rate is in the ELBW babies. A significant number (14.6%) of admissions require ventilatory (excluding nCPAP) support. This audit supports the notion that level 2 obsteric referrals often result in babies requiring level 3 neonatal care. Our mortality rates are comparable with the other centres mentioned, given current resource constraints.
23

The change in neonatal jaundice surveillance at the MOUs has resulted in an increase in the number of admisssions for NNJ and an upward trend in the number of exchange transfusions done. As exchange is a procedure carrying a significant morbidity, an ongoing audit of the NNJ admissions is essential. The surveillance system for NNJ at the MOUs may need to be urgently re-examined. In conclusion, this audit primarily emphasises the essential requirement of a level 3 Neonatal Service at a level 2 Obstetric Hospital. This ensures that mothers requiring level 2 obstetric care and their ill newborn infants are not separated.An audit of neurodevelpomental outcome in weight categories is now necessary to more completely assess the quality of the level 3 service offered.
24

EARLY COMPARED WITH DELAYED ORAL FLUIDS AND FOOD AFTER CAESAREAN SECTION
L Mangesi, GJ Hofmeyr Cecilia Makiwane Hospital, East London Hospital Complex; Effective Care Research Unit; University of Witwatersrand/University of Fort Hare
BackgroundDifferent practitioners share different opinions as to when fluids and/or food should be resumed after caesarean section. Those who are for early feeding believe that caesarean section is an operation where the bowels are not tampered with or exposed and therefore should not interfere with bowel activity. The opponents of this view argue that caesarean section is a major operation with a risk of complications which may arise from giving oral fluids or food soon after surgery. This results in some practitioners withholding fluids or food for up to 24 hours and more. Some institutions allow unlimited oral fluids immediately after caesarean section and others have ‘standing orders’ of grading from oral fluids to food depending on whether the patient had bowel sounds, has passed flatus, and had bowel action. These discrepancies raise concern as to the basis of different practices.
ObjectivesThe major objective of this review is to assess the effect of early versus delayed introduction of oral fluids and food after caesarian section.
MethodsRelevant clinical trials comparing the effects of early versus delayed introduction of fluids and/or food after caesarean section were identified and evaluated for methodological quality. Trials where allocations were not random were excluded. The participants were women who were not diabetic, within the first 24 hours after caesarean section. The outcomes measured were post-operative nausea, vomiting, abdominal distension, time to passing flatus, duration of intravenous fluids, breast-feeding success, need for analgesia, women’s satisfaction and post-operative
25

hospital stay. Sub-group analysis was according to whether the type of anaesthesia was general anaesthesia, regional analgesia, or where it was mixed or not defined. Data were entered and analysed in the Review Manager (Revman) computer software.
ResultsOut of 11 studies considered, 6 were included in this review. Four were excluded and one is pending further information from trial authors. The methodological quality of the studies was not high. Of 6 studies included, three used opaque envelopes for allocation concealment and three mentioned that they practised allocation concealment but did not specify how it was done. One to three studies contributed usable data to each outcome. There is thus potential for effect of reporting bias. Three of these studies included women who had regional analgesia, one included both regional and general anaesthesia and two studies included participants where the anaesthesia was mixed or not defined. Early oral fluids and/or food, were associated with reduced time to first food intake, reduced time to return of bowel sounds, reduced post-operative stay and a trend to reduced abdominal distension.
No significant differences were identified with respect to nausea, vomiting, time to bowel action/ passing flatus, paralytic ileus and a number of analgesic doses. The outcome ‘bowel distension’ is shown in figure 1 as an example of the method of analysis.
DiscussionThe data should be interpreted in the light of the average methodological quality of the studies and the fact that data for individual outcomes were contributed by a limited number of studies. However, there was consistency in that all the outcomes which showed significant differences were in favour of the early feeding group. No disadvantages of early feeding were identified in the studies reviewed. It should be borne in mind
26

that the overall number studied was too small to exclude the possibility of rare adverse events.
ConclusionAlthough the overall number of studies was small and the methodological quality not high, no disadvantages of early feeding were identified. There was no evidence from randomised trials to justify a policy of withholding oral fluids after caesarean section.
RecommendationsFurther research is needed to confirm the findings of these small studies by larger, more methodologically sound trials.As starvation is not pleasant, oral fluids or food following caesarean section must only be restricted within the context of well-designed trials.
Figure 1 Early versus delayed fluids and/ or food after caesarean section: Abdominal distension
27

28

DECISION TO DELIVERY INTERVAL AT EMERGENCY CAESAREAN SECTION: UNACCEPTABLE DELAYS IN A LARGE TERTIARY HOSPITAL
P Onyango-Okeyo, E BuchmannChris Hani Baragwanath Hospital and University of the Witwatersrand
Access to caesarean section facilities is an essential component of obstetric care, and delay in performance of emergency caesarean section may be life-threatening for mother and baby. Chris Hani Baragwanath Hospital is the only facility performing caesarean sections for a population of about two million urban poor. The hospital delivers medium and high-risk obstetric patients, and is the referral centre for seven local midwife-run clinics. It also receives referrals of difficult patients from several other hospitals in the Gauteng Province. The annual total of hospital deliveries has increased in recent years from 15 452 in 1993 to 18959 in 2001, with numbers of caesarean sections rising from 3492 in 1993 to 4732 in 2001, an absolute increase of 36%. This has happened in the absence of any increase in operating theatre numbers, staff or equipment. We currently perform an average of 13.0 caesarean sections daily. The upper limit of elective cases is four on weekdays only. Two operating theatres are available from 08:00 to 15:00, and only one outside these hours. This has resulted in the frequent development of caesarean section queues, and delays in delivery. In 2001, 30 perinatal deaths were associated with such delays, 18 of these in term babies who died from intrapartum hypoxia. The objectives of this study were to quantify delays in performance of intrapartum caesarean section and to investigate any associations between delay, indication for operation and fetal outcome.
29

MethodsWe performed a retrospective record review of consecutive files of women who underwent intrapartum caesarean sections with live babies from February to April 2001. Information was extracted with emphasis on the indication for caesarean section and decision to delivery interval. This interval was taken from the time the doctor wrote down the intention to book a caesarean section to the time the anaesthetic was started. The latter is always reliably recorded in the notes by the theatre nursing staff. Neonatal unit records were used to ascertain details of neonatal morbidity and death. Analysis was performed using Epi-Info 6 statistical software. Differences between frequency distributions were analysed using the Wilcoxon two-sample test for nonparametric data. Differences with p values of less than 0.05 were accepted as statistically significant.
ResultsThere were 418 intrapartum caesarean sections. Decision to delivery intervals ranged from 5 to 760 minutes. The mean time delay was 116.7 minutes, with 4.8% of caesarean sections commenced within 30 minutes, 25% within 60 minutes, 50% within 90 minutes, and 75% within 150 minutes. During office hours (08:00 to 16:00, n=295) there was a median delay of 100 minutes, and out of these hours (n=124) a mean delay of 90 minutes (p=0.18). The indications for caesarean section are shown in Table 1. Table 2 shows the median decision to delivery intervals for selected indications for intrapartum caesarean section.
Table 1 Indications for intrapartum caesarean section
Indication Number of cases Per centFetal distress 176 37.5Cephalopelvic disproportion
108 23.0
‘No progress’ 72 15.3Breech 34 7.2Multiple pregnancy 16 3.4Antepartum haemorrhage 15 3.2Cord prolapse 8 1.7Eclampsia 7 1.5
30

Other 36 7.6
Table 2 Median decision to delivery intervals for selected indications for intrapartum caesarean sections. Comparisons are made between the presence and the absence of the indications.
Indication Number Median interval for indication present: absent (minutes)
P
Fetal distress 176 70:105 <0.001Cephalopelvic disproportion 108 100:85 0.037Previous caesarean section 88 90:97 0.85Antepartum haemorrhage 15 70:90 0.19Cord prolapse 8 45:90 0.040The total number of neonatal admissions was 65, 15.6% of deliveries. The reasons for neonatal admission were respiratory distress (16), mild birth asphyxia (7), non-specific observation (6), hypoxic ischaemic encephalopathy (4), phototherapy (4), meconium aspiration (3), and others (15). Neonatal admission was associated with a median decision to delivery interval of 70 minutes, compared to 95 minutes for babies who were not admitted (p=0.005). Twenty-eight (42%) of neonatal admissions followed caesarean section for fetal distress.There were 15 perinatal deaths. The decision to delivery interval for these caesarean sections ranged from 25 to 170 minutes with a median of 60 minutes, compared to a median of 95 minutes where the babies survived (p=0.07). The indications for these caesarean sections were as follows: fetal distress (7), complications of multiple pregnancy (3), cephalopelvic disproportion (2), ruptured uterus (1), abruptio placentae (1), and cord prolapse (1).
DiscussionThe average decision to delivery interval of 116.7 minutes, with a median of 90 minutes is, to our knowledge, the longest yet described. By any standards, this is unacceptably long. Internationally, a 30-minute delay is commonly adopted as the time within which an emergency caesarean section should be started. This somewhat arbitrary guideline is difficult to put into practice, even in developed countries. The South African
31

Department of Health, in its national maternity care guidelines, realistically suggests one hour as the outside limit, but even this could not be attained in our hospital. While our study did not attempt to identify the causes for delay in each case, it seems clear to us that the main reason is the development of caesarean section queues. With an average of 11 emergency caesarean sections daily, and only one theatre available for most of the day, queues are an inevitable consequence, with obvious dangers to mothers and babies. The logical answer is to have two theatres available on a 24 hour basis, but this is impossible in the short term due to a lack of funds to employ new staff. In recent years we have made some efforts to reduce the strain. For example, postpartum sterilisations are no longer done in our theatre, and we placed a ban on elective caesarean section for HIV seropositivity. This has, however, not removed the caesarean section queues; it has perhaps prevented them from becoming even longer.The decision to delivery intervals with different indications show that the more urgent the indication, the less the delay. Cord prolapse, traditionally the most pressing of indications, was associated with the most rapid response. Antepartum haemorrhage did not attain statistical significance but showed a similar trend. Previous caesarean section was seemingly not managed with any particular urgency, but this group may have included a large number of women who underwent caesarean section early in labour when the risk of uterine rupture was low. Regarding fetal outcomes, the worse the outcome in terms of neonatal admission or death, the less the decision to delivery interval. Doctors clearly selected the patients where the risk was greatest and ensured that such caesarean sections were prioritised. Our study design has limitations which make the results an underestimation of the problem of delay. We were unable to include women who were booked for caesarean section and subsequently delivered vaginally. Some of these may have been patients whose babies died while waiting for caesarean section. We also excluded all emergencies that were not in labour, such as eclampsia, placenta praevia,
32

and antepartum fetal compromise. Our decision to delivery interval does not follow that of previously published studies, as we had to use the administration of anaesthesia as our reference point for ‘delivery’. As most of our caesarean sections are done under spinal anaesthesia, the true decision to delivery intervals may have been up to 10 minutes longer.
ConclusionCaesarean section queues are likely to be a limiting factor in obstetric care in many large hospitals in South Africa and other developing countries, and, in the absence of resources to increase service levels, cannot be eradicated. Given this reality, we need to devise means of overcoming the dangers posed by caesarean section queues. Possible solutions include reducing caesarean section rates, rationalisation of procedures related to commencement of caesarean sections and triage of cases according to levels of maternal and fetal risk.
33

SEVERE ACUTE MATERNAL MORBIDITY (SAMM) IS A RAPID DIAGNOSTIC TOOL FOR EVALUATING MATERNAL CARE
L Cochet, RC Pattinson, P MacdonaldMRC Research Unit Maternal and Infant Health Care Strategies, University of Pretoria
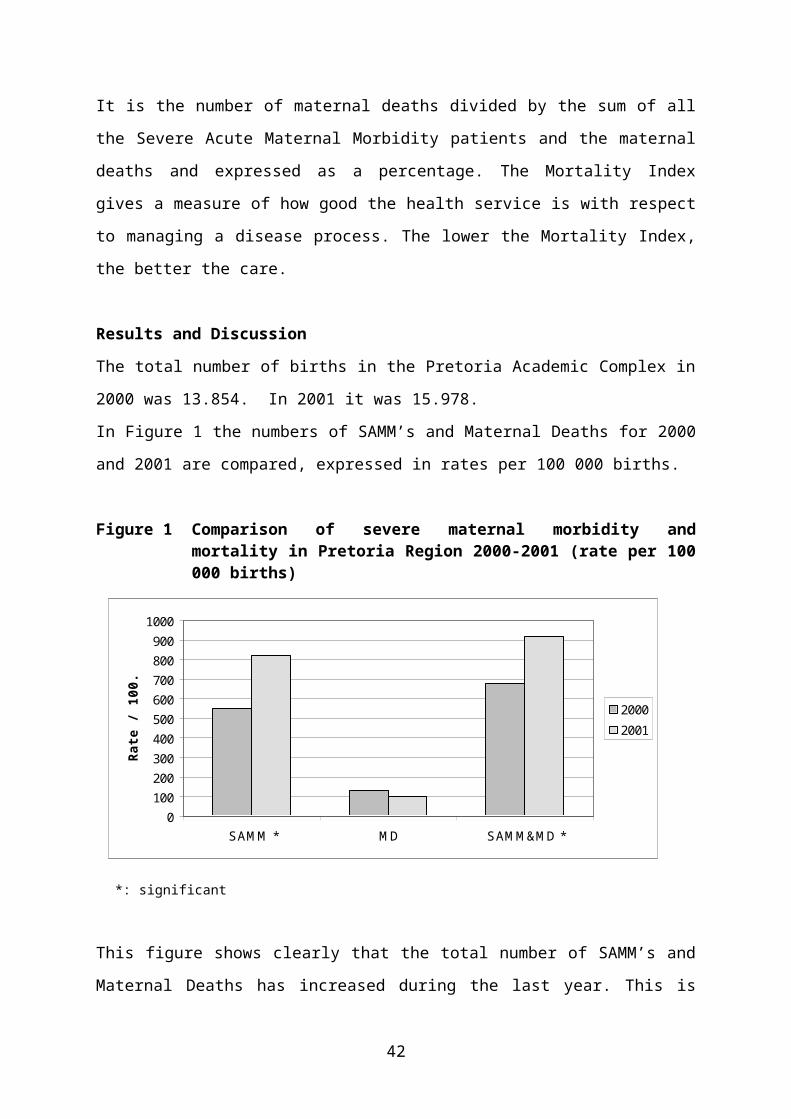
IntroductionSevere Acute Maternal Morbidity (SAMM), also known as “Near Miss”, has been defined by Mantel et al. This means a woman with severe organ dysfunction or organ failure in pregnancy, during labour or in puerperium which, if not treated appropriately, could result in maternal death. The Near Miss patient, by definition, survives. With identifying Near Misses it is possible to obtain more information about the basic disease profile of a population and of the response of the health system to the people.The aim of our study was to compare the SAMM and Maternal Mortality in the Pretoria Academic Complex for the year 2000 and 2001
Materials and MethodsSAMM’s and maternal deaths were identified at daily audit meetings in the hospitals of the Pretoria Academic Complex from 2000.01.01 until 2001.12.31. The data obtained in 2001 were compared with the data from the year 2000.The definitions for primary obstetric cause of near miss or maternal death are the same as those used for the Confidential Enquiry into Maternal Deaths in South Africa.The Mortality Index has been introduced by Vandecruys et al. It is the number of maternal deaths divided by the sum of all the Severe Acute Maternal Morbidity patients and the maternal deaths and expressed as a percentage. The Mortality Index gives a measure of how good the health service is with respect to managing a disease process. The lower the Mortality Index, the better the care.
34

Results and DiscussionThe total number of births in the Pretoria Academic Complex in 2000 was 13.854. In 2001 it was 15.978.In Figure 1 the numbers of SAMM’s and Maternal Deaths for 2000 and 2001 are compared, expressed in rates per 100 000 births.
Figure 1 Comparison of severe maternal morbidity and mortality in Pretoria Region 2000-2001 (rate per 100 000 births)
This figure shows clearly that the total number of SAMM’s and Maternal Deaths has increased during the last year. This is due to a rise in Near Misses, the number of maternal deaths has decreased. The rise in severe maternal morbidity and the rise in the sum of both, SAMM and maternal deaths have shown to be significant.
SAMMThe number of near misses related to abortions, bleeding problems, hypertension and pregnancy related sepsis is increased in 2001 compared with 2000 (Table 1).There is only a significant increase in maternal morbidity related to abortions and haemorrhages.
0100200300400500600700800900
1000
SAMM * MD SAMM&MD *
Rate
/ 10
0.00
0
2000
2001
*: significant
35

The increased number of near misses related to abortion is most likely due to a higher number of unsafe illegal abortions. There is also concern about the increase in near misses due to antepartum and postpartum haemorrhages. Our management of bleeding complications in pregnancy needs to be more aggressive
Maternal deathsOverall the number of maternal deaths has decreased in 2001 compared to the year 2000. Although we saw an increase of acute maternal morbidity related to abortions, there was no rise in maternal deaths related to this cause in 2001.The number of maternal deaths related to bleeding problems and to hypertensionhas raised during the year 2001 in comparison of these during the year 2000. These rises were not significant (Table 1).
Combination of SAMM and Maternal Death auditIn Table 1, the SAMM and Maternal Death data are combined in the last column and their primary causes are plotted in rates per 100000 births for the years 2000 and 2001.There is a rise in problems related to abortions, haemorrhages, hypertension and pregnancy related sepsis (Table 1).
Table 1 Primary obstetric cause of near miss & maternal death 2000 vs 2001 (rate/100.000 births)
Primary Obstetric Cause Near Miss Rate
Maternal Death Rate
NM+MD Rate
2000 2001 2000 2001 2000 2001No Obstetric Cause 29 25 0 6 29 31Abortion * 72 156 14 13 87 169Ectopic Pregnancy 43 25 7 0 51 25APH * 43 119 0 6 43 125PPH * 130 225 7 13 137 238Hypertension 87 106 22 31 108 138Pregnancy Related Sepsis 43 75 0 0 43 75Embolism 0 6 7 6 7 13
36

Anaesthetic Complication 29 13 7 0 36 13Acute Collapse - Cause Unknown
7 0 0 6 7 6
Non-pregnancy related infection
14 19 43 6 58 25
Pre-existing Maternal Disease
51 38 22 13 72 50
Unknown 0 13 0 0 0 13
The rises in problems related to abortions and haemorrhage have shown to be significant.By looking at maternal deaths only, we should have missed the increase in severe maternal morbidity due to abortions and haemorrhages. There is no increase in maternal deaths related to abortions. There is a slight increase in maternal deaths related to haemorrhages, but this hasn’t shown to be significant.We therefore estimate it essential to add the SAMM audit system to the already in use enquiry of maternal deaths system.The audit system we propose to use, is called MaMMAS. It stands for Maternal Morbidity And Mortality Audit System.
The Mortality IndexIn Figure 2, the Mortality Index is plotted for the different primary obstetric causes of near misses and maternal deaths in 2000 and 2001 in the Pretoria region.
37

Figure 2 Mortality Index (MI) 2000/2001 - Pretoria Region
The Mortality Index in 2001 has improved for all primary obstetric causes except for bleeding problems and hypertension. The general Mortality Index for the year 2000 was 19.1%. In 2001, the Mortality Index was decreased till 10.9%. This means that in general, our care has improved during the last year.ConclusionIn the year 2001 we had an increased number of Severe Acute Maternal Morbidity patients, but a decreased number of maternal deaths in comparison to the previous year. The general mortality index in 2001 has decreased, so we have evidence that in general our care has improved over the last year. Despite this, there is concern about the increased morbidity due to abortions and about the increased morbidity and mortality due to haemorrhage. We can conclude that the SAMM audit system has proven to be a rapid diagnostic tool for evaluating maternal care in the Pretoria Academic Complex.Looking only at maternal deaths in our hospitals, we couldn’t have been able to pick up the increasing problems related to abortions and
0%
20%
40%
60%
80%
100%
120%
Perc
enta
ge
Mortality Index 2000Mortality Index 2001
*: significant
38

haemorrhage. Therefore a combination of auditing severe maternal morbidity and mortality should be used to detect ongoing problems in maternal care at an early stage.This audit system is called MaMMAS, what stands for Maternal Morbidity And Mortality Audit System. We hope that the use of this system can be extended to other Maternity Hospitals in South Africa in the near future. By comparing the data of the different hospitals in different regions over the country we will then be able to detect regional or national problems at an early stage.
39
EVIDENCE-BASED MEDICINE AT OBSTETRICS UNIT (KALAFONG HOSPITAL). AN AUDIT OF CURRENT PRACTICE
L Likanza, RC PattinsonMRC Unit for Maternal and Infant Health Care StrategiesKalafong Hospital and University Of Pretoria
IntroductionEvidence-based medicine is rapidly gaining ground in modern medical practice. This comes after the profession has long been accused of having only about 10-20% of its practice being supported by solid scientific evidence.Recently only, in 1994, Sacket et al boldly alleged that 82% of its in-patient hospital practice was evidence-based.This study follows in those footsteps, analysing the standard of care in a busy obstetric unit at Kalafong Hospital, in South Africa. The Cochrane Library and the Better Birth Initiative have been taken as the main yardstick against which the standard and quality of care have been assessed. The proportion of the patients’ problems and solutions has been calculated.
MethodDesign: prospective, descriptive study.Setting: Kalafong Hospital (tertiary referral centre).Population: a random sample of women who delivered in the labour ward unit.Every 5th patient was selected among the total number who delivered in the unit per day. Prior to discharge every patient was interviewed and her case notes examined to have a complete picture of the management of the patient. The strength of evidence for a particular management strategy was categorised from A to G. The quality of care was assessed according to the Better Birth Initiative principles.
Results
40

One hundred and fifty three patients were randomly selected over a period of seven weeks. Forty nine obstetrics problems were identified and the evidence for the effectiveness for managing these problems was judged to be category A in 16 problems, category B in 14, category C in 4, category D in 4, and category G in 11. There was good best evidence in 41 problems (84%).
ConclusionsMore than 80% of the solutions to problems were solved by the use of the current best evidence available.The medical aspect of the standard of care was very encouraging. However, problem areas were identified, exposing mainly the quality of care which is still to be desired in many areas:- use of chromic as suture material of choice for perineal repair.- eat and drink to be offered during labour.- perineal care in general, exposed by an alarmingly high number of
either episiotomy or perineal tears.- use of routine suctioning of the neonates.
On a positive note, however, these aspects have been outstanding:- social support present (58%).- keeping patients informed about what is going on (82%).- amnioinfusion to all women with meconium staining liquor.- preparation for caesarean section.- active management of the 3rd stage of labour.- shaving (without caesarean section).- bonding between mother and baby.
41

MANAGEMENT OF INCOMPLETE ABORTION IN SOUTH AFRICAN STATE HOSPITALS
H Brown, R Jewkes, K Dickson–Tetteh, J Levin, H Rees.Reproductive Health Research Unit, Chris Hani Baragwanath and Gender and Health Group, Medical Research Council
ObjectiveTo describe the current management of incomplete abortion in South African public hospitals and discuss the extent to which management is clinically appropriate.
DesignA multicentre, prospective descriptive study.
SettingSouth African public hospitals that manage gynaecological emergencies.
Sample and Study PopulationHospitals were selected using a stratified random sampling method. All women who presented to the above sampled hospitals with incomplete abortion during the three week data collection period in 2000.
Main Outcome MeasuresDetail of medical management, detail of surgical management, use of blood products and antibiotics, methods of analgesia and anaesthesia used, use of abortifacients.
ResultsThere is a trend towards lower technology such as the use of manual vacuum aspiration and sedation anaesthesia, however this is mainly limited to the better resourced tertiary hospitals linked to academic units. The use of antibiotics and blood products has decreased but much of the use is inappropriate, as is the initial clinical assessment of women presenting with incomplete abortion, signs of sepsis and haemodynamic
42
shock often being missed. The use of abortifacients does include some use of misoprostol but merely as an adjunct to surgical evacuation.ConclusionsThe management of incomplete abortion remains a challenge in South Africa. This is a low income country that is still by and large managing a large clinical issue with costly methods. The evidence of inappropriate clinical assessment and use of blood products and antibiotics is particularly worrying as sepsis and haemorrhage are still major causes of maternal morbidity in South Africa. The limited use of misoprostol apart from as an adjunct to surgical intervention has been highlighted. This is important as recent research is indicating that misoprostol as the main method of managing incomplete abortion may be the way forward for low-income countries. It would be a method which could be used in clinics with limited resources and result in a decrease in the number of women requiring surgical intervention. The trend towards low cost technology is promising though and this study has given us information as how to best address this problem. More training in manual vacuum aspiration together with local anaesthetic techniques needs to be done, targeting in particular the regional and district level hospitals. This needs to be reinforced by skills training in the assessment of the severity of clinical cases and by ensuring that blood products and antibiotics are available. For the future, our focus should be on the undergraduate training programmes and midwife post abortion care programmes. The management of incomplete abortion that should be taught here should include good clinical assessment of women who present with incomplete abortion, signs of infection and haemodynamic status, as well as use of manual vacuum aspiration together with local anaesthesia. This will produce a new generation of appropriately trained health care providers who will be able to safely manage women who present with incomplete abortion using appropriate low cost technology.
43

IS AN INCREASE IN CAESAREAN SECTION RATE INEVITABLE?
H Van Zyl, VMC Eeckhout, SR FawcusDepartment of Obstetrics And Gynaecology, Mowbray Maternity Hospital, University of Cape Town
Introduction In developed countries, a rising trend in caesarean section rate (CSR) has been the focus of much debate. Marked differences however, exist in the rate of increase between countries, despite the World Health Organisation recommending a CSR of 10-15%. In countries like the Netherlands, Norway, Sweden and Denmark the CSR has remained low and stable at around 10%. In United Kingdom, United States of America and Canada however, rates are up to 16% in the UK and 20% in the US.
However, countries with increasing CSR, have reported no significant decreases in their perinatal mortality rates (PNMR), as compared to those with lower caesarean section rates.
In developing countries reliable data are still absent or incomplete, leading to less well documented CSRs. A few studies done in Sub Saharan Africa have shown similar increases in CSR.
Mowbray Maternity Hospital (MMH), a public maternity hospital, predominantly manages complicated cases referred from 3 Midwife Obstetric Units (MOU), as well as low risk patients, living in the neighbourhood. An average of 500 deliveries occur per month.
Routine statistics show that the absolute number of caesarean sections is increasing.
Aim1) Describe the changes in CSR at MMH from 1994 to 2001.2) Investigate the change in the various indications for CS from 1994 to
2001
44

MethodsA retrospective, descriptive audit, reviewing all deliveries from 1994 to 2001.
Our study population included patients who delivered at MMH and its catchment area, which included Gugulethu MOU, Khayelitsha MOU and Mitchell’s Plain MOU.
Labour ward and theatre registers and computerised data were obtained for November of each year, 1994 to 2001, in order to compare the number and indications for CS.
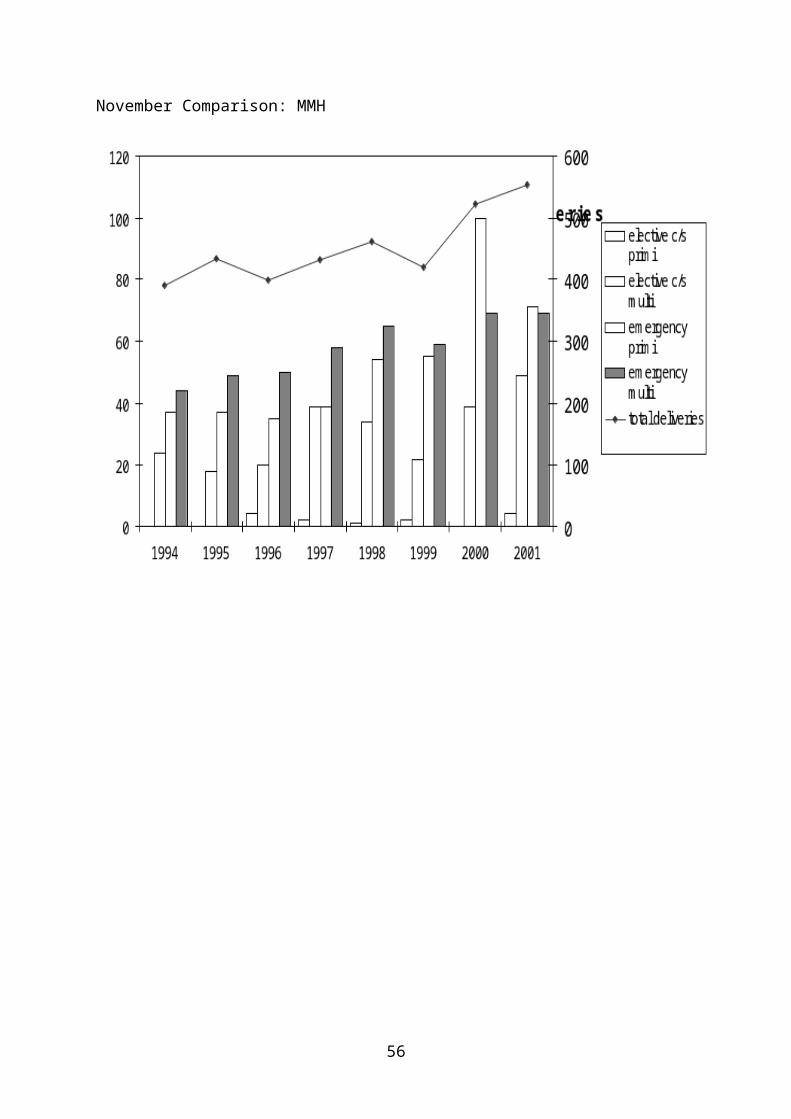
ResultsNovember Comparison: MMH
45

DiscussionThere is an obvious lack of reliable data about CSR in most developing countries. Since computerised data and delivery registers were used to obtain information for this audit, it is inevitable that some of these may be incomplete. With regard to indication of CS, we often had to prioritise when multiple indications existed, leading to assumptions that may or may not be valid.
From our data however, it is clear that the annual CSR increased significantly from 1994 to 2001 from 27.4% to 38.4% (p<0.0001), as a result of the significant increase seen in emergency CS.
When comparing November 1994 to November 2001, fetal distress contributed most to the rise in CSR. (3.6% to 8.6% of total deliveries: p<0.0011)
46

Although overall there was no significant increase in repeat CS, it became evident that significantly fewer patients were allowed to or wanted to labour after one previous CS (78.9% to 63.7% of patients with one previous CS: p<0.028). A significant decrease was also noted in the success rate (62.2% to 37.3%: p<0.0058).No significant change was noted for failure to progress/ cephalopelvic disproportion as indication for CS (9.9% to 9.8% of total deliveries: p< 0.479).CS done for malpresentation also showed a significant increase from 1% of total deliveries in 1994 to 2.5% of total deliveries in 2001 (p<0.0472).
Fetal distress will always be a difficult diagnosis. Fetal blood sampling (FBS) can successfully confirm or reject the diagnosis of fetal distress. The problem we are faced with, is the increasing prevalence of HIV. Where the status is unknown or positive, FBS is not done, leading us to diagnosis fetal distress on an abnormal or non-reassuring CTG alone.
Possible explanations for the rise in CSR at MMH could include the following:1) A new senior obstetrician that was appointed in 1996.2) Fetal blood sampling (FBS), which was done routinely until 1998, but
then discontinued, due to increased HIV prevalence.3) Screening for HIV, (MTCT program at Khayelitsha and Gugulethu),
started in 1999, leading to a lower threshold for CS in HIV positive patients.
4) The Hannah trial, which was published in 2000, recommending CS for term breech presentation.
ConclusionThe CSR increased significantly at MMH from 1994 to 2001.The HIV epidemic is having a major impact on CSR, even without an existing policy of doing routine CS in HIV positive patients. There is
47

however potential to reduce the CSR, by doing more FBS in HIV negative patients.Reasons for the decrease in VBAC needs to be explored.A prospective audit of decision making around CS is planned.It was also noted that the PNMR decreased significantly.
48

EFFECT OF PRETORIA PASTEURISATION ON BACTERIAL CONTAMINATION OF EXPRESSED BREAST MILK
P Soma-Pillay, B Jeffery, J MakinMRC Unit for Maternal and Infant Health Care Strategies, University of Pretoria and Kalafong Hospital
Introduction and ObjectivesThe Pretoria Pasteurisation (PP) method of pasteurising expressed breast milk (EBM) is a known low-cost method of heat-treatment of EBM which has been shown to inactivate HIV in the milk of infected women. This study was undertaken to:1) determine the effectiveness of PP in eliminating pathogenic bacteria in
EBM.2) determine the duration for which pasteurised milk may be kept without
refrigeration.
MethodsSixty mothers from the post-natal wards of Kalafong Hospital, who chose to breast feed were counselled and requested to donate a sample ( +/- 30ml) of breast milk in a clean jar. The sample was divided into two parts: a control portion and a PP-portion. Both samples were cultured immediately. The samples stood at room temperature and were cultured again at 4 hours, 8 hours and 12 hours.
The cultures were considered positive if the colony count was equivalent to 1000 colony-forming units per millilitre of milk for gram-positive pathogens or the presence of any gram-negative bacteria. Normal commensal organisms were considered clinically significant at a CFU count of 100 000 CFU/ml.
ResultsSixty samples were collected. Of the 60 control portions, 5 were completely sterile; 28 contained significant counts of pathogenic bacteria,
49

while 39 samples contained commensal organisms. Of these 39 samples, 3 had positive colony counts of >100 000 CFU/ml.Of the 60 pasteurised portions, 54 showed no growth up to 12 hours. Six samples had bacterial growth of which 1 contained commensal organisms. Five samples showed growth of pathogens; however for 4 of these, which were processed on the same day, there is convincing evidence that the growth was a lab contaminant.
ConclusionPretoria Pasteurisation inactivates both pathogenic and commensal bacteria in expressed breast milk. Pretoria pasteurised-EBM can be safely stored for up to 12 hours without refrigeration with an extremely low probability of bacterial contamination.
50

EARLY INTERMITTENT KANGAROO MOTHER CARE: BREASTFEEDING AT SIX WEEKS CORRECTED AGE
GF Kirsten, CL Kirsten, E ThompsonDept of Paediatrics, Tygerberg Hospital and the University of Stellenbosch
Breast milk has major short and long-term advantages for very low birth weight (VLBW) infants. These include a reduced infection, necrotising enterocolitis and mortality rates as well as an improved neurodevelopmental outcome and cost savings. Establishing and maintaining breastfeeding in VLBW infants however requires intensive support.
AimTo determine the milk feeding pattern during initial hospitalisation (Tygerberg and it’s 2 secondary hospitals) and at 6 weeks corrected age of infants <1600g who received intermittent Kangaroo Mother Care (KMC) during their hospital stay.
Study designProspective, cohort analytical.
Patients and methodsEighty non-ventilated infants (<1600g) were recruited upon admission to the KMC Unit after informed consent for participation in the study was obtained from the mothers. Infants with congenital viral infections, chromosomal disorders, major congenital abnormalities and those requiring admission to the neonatal intensive care unit were excluded from the study. Once the infants were stable and on full enteral feeding, they were transferred to KMC Units at the secondary hospitals in the Tygerberg area. Milk intake was documented daily while post-discharge milk intake was obtained through weekly telephonic interviews and at the 6-week corrected age neurodevelopmental assessment.
51
ResultsNine infants were excluded: 5 died (NEC or septicaemia) while 4 were admitted to the NICU.
Graph 1 Mean duration of hospital stay (days)
Graph 2 Duration of hospital stay (days) of the infants with birth weights above and below 1000g
*p= 0.0001
52
Graph 3 Milk feeding patterns at Tygerberg Hospital and the secondary hospitals
Graph 4 Milk feeding patterns at Tygerberg and the 2 secondary hospitals
Graph 5 Milk feeding patterns at discharge from Tygerberg, the 2 secondary hospitals and at the 6-week corrected age follow-up visit
%
%
%
53

Graph 6 Mean daily weight gain (g) at secondary hospitals and at home
Graph 7 Percentage of infants with sub-optimal weight gain (<25g/day): secondary hospitals and at home
ConclusionsAlthough some breast milk feeding still occurred in 62% of the infants at 6 weeks corrected age, full breastfeeding had decreased progressively from 75% to 18% after discharge from Tygerberg Hospital. Of concern is the dramatic decrease in breastfeeding at the one secondary hospital. A further decrease in full breastfeeding also occurred between discharge from the secondary hospital and follow-up at 6 weeks corrected age. The mean duration of hospital stay at Tygerberg Hospital (tertiary hospital) is still too long. This is probably due to the limited number of KMC beds at the secondary hospitals as well as a delay in the transfer of babies by the ambulance services. Poor mean daily weight gain at the secondary hospitals also resulted in an increased hospital stay (60% of the infants gained <25g/day). The excellent weight gain at home supports earlier discharge under close supervision. Our study confirms the importance of
%

initial and ongoing breastfeeding support of mothers of VLBW infants in hospital and post-discharge.

IMPLEMENTATION OF KANGAROO MOTHER CARE IN MPUMALANGA
I Pretorius, A-M Bergh, E Malek, RC PattinsonMRC Research Unit for Maternal and Infant Health Care StrategiesUniversity of Pretoria
IntroductionThe research project on the implementation of kangaroo mother care (KMC) in Mpumalanga is part of the larger KMC research project of the MRC Research Unit for Maternal and Infant Health Care Strategies. During the first phase, a workbook for the implementation of KMC was developed. The aim of the next phase of the project was to: test the workbook, using it in conjunction with a facilitator; refine an implementation package in preparation of the Ukugona
Outreach, an extensive KMC implementation trial in KwaZulu-Natal.
MethodsThe study was done at four hospitals in Mpumalanga. Each facility received a workbook and was visited by a facilitator (IP) five times during a six-month period in 2001 to assist them with the planning and implementation process. The facilitator wrote extensive field notes on each of the visits.
The visits were planned around the following purposes:Visit 1: To make potential role players aware of the KMC concept and
implementation programmeVisit 2: To ‘discover’ the structure and functioning of the institution
and to choose a KMC modelVisit 3: To discuss finances, items necessary in the unit and staffing
arrangementsVisit 4: To develop policies and discuss administration and record
keepingVisit 5: To review the implementation process
All the meetings were in the format of a participatory workshop of two to three hours. An independent evaluator (A-MB) assessed the outcome of the process by means of a walk-through visit.
ResultsBy the end of 2001, KMC was implemented successfully in three of the four hospitals. The fourth hospital was still in the process of implementation.
Description of the implementation processRole playersThe driving force for getting KMC implemented varied between the four hospitals and not in one of the four did the sister in charge of the neonatal ward take the lead. At one hospital no specific person was willing to take this responsibility. At the other hospitals it was the sister in charge of information management, a sister involved in the training of nurses and the MCWH coordinator respectively. In two of the four hospitals senior management was positive about implementation of KMC and in the other two the superintendents were reluctant to give permission to start the process.
Structure and staffing arrangementsThe structure of the hospital was important in determining the staffing arrangements and the space to be provided for KMC. In two hospitals, the neonatal unit was situated in a separate ward. In the other two hospitals, it was part of the paediatric or maternity ward. In the hospitals where the neonatal unit was situated in a ward, the ward comprised separate rooms and it was easy to start a KMC unit in one of the empty rooms. In one hospital a big ward was divided into smaller cubicles with 10 beds in each cubicle. It was more difficult to start a KMC unit here, because there was less privacy and it was not as homely as a smaller ward.

All new KMC units shared staff with other wards, depending on where it was situated. In two hospitals the sisters in charge of the ward did not rotate, but the rest of the staff rotated every few months, which staff perceived as being too often.
ItemsMost of the items required for a KMC unit could be obtained from in and around the hospital. In each of the hospitals “special” items were discovered during the walk-through visit, demonstrating originality and creativity. For example, in one hospital backrests obtained from the orthopaedic ward were used on the beds to get a semi-reclined position. In another hospital wrappers for holding the baby were made from old theatre gowns that were cut off and in yet another the KMC wrappers consisted of a square with straps made from an old theatre towel. Conclusion Leadership is important in driving the process. Positive attitudes are necessary. Prior knowledge or awareness is helpful. Core staff is important; this means less rotation is preferable. Visual materials and examples are preferable. Parts of the KMC workbook can be copied for use. Indicators such as the number of infants given KMC, their length of
stay and their health outcomes should be monitored closely in all institutions. This should not only reflect the savings a KMC programme produces, but also pick up problems where these may occur.

ASSESSING THE IMPLEMENTATION OF KANGAROO MOTHER CARE IN HEALTH CARE FACILITIES
A-M Bergh, I Pretorius, E Malek, RC Pattinson, E van Rooyen, A PullenMRC Research Unit for Maternal and Infant Health Care Strategies, University of Pretoria
IntroductionKangaroo mother care (KMC) is an accepted way of decreasing neonatal mortality and the cost of caring for low birth weight neonates. Some South African health authorities have also officially embraced KMC as an appropriate health care strategy. In order to get a grip on the implementation of KMC from a research perspective, the MRC Research Unit for Maternal and Infant Health Care Strategies is currently undertaking a research programme in this regard. At various points in the programme insights were gained from the assessment of implementation. This paper presents a preliminary evaluation model proposed for the institutional assessment of large-scale implementation of KMC. This model could also be used in the planning of the implementation of other health care interventions.
The research programmeOne of the special features of the KMC research programme is its emerging research design, using an adapted participatory action research approach. Figure 1 gives an overview of the evolving research programme. Apart from the main thrust that is represented by the ellipse, smaller research projects (rectangles around the ellipse) also developed over time, with some interfacing with other larger research projects impacting on the practice of KMC. Projects linked to the programme with dotted lines are those in various stages of planning. Ultimately the programme aims at stimulating individual health care practitioners to become action researchers in their own institutions with a view to improve quality of care and to develop capacity for self-reflection.
59

The initial aim of the research was merely to do action research in two hospitals to identify important implementation issues. A request by one of the provinces for guidelines for implementation led to the idea of developing a checklist for implementation. This in turn developed into the idea of an implementation workbook. This was reported on at the Priorities Conference of 2001. The workbook was tested in four hospitals in Mpumalanga by a facilitator (see “Implementation of kangaroo mother care in Mpumalanga”). This part of the research in turn contributed to the finalisation of a resource-based implementation package consisting of the workbook, a reader, two videos, a poster and other information leaflets.At the beginning of 2002, the focus shifted from researching the implementation of KMC in individual institutions to a more systematic implementation on a provincial scale. The Ukugona Outreach was launched in the province of KwaZulu-Natal. Hospitals enrolled on a voluntary basis and were randomly allocated to two different outreach strategies, with one group receiving the implementation package only and the other receiving a package as well as three regional facilitation visits. Three of the hospitals with telemedicine facilities receive regular telelearning broadcasts. For the purpose of evaluating the effectiveness of different outreach strategies, a provisional evaluation model was developed (see figure 2). The model will inform the summative evaluation of the first phase of the Ukugona Outreach.
60

FIGURE 1
The provisional evaluation modelTwo main questions guided the planning of the evaluation:- Can indicators be developed for measuring progress points in the KMC
implementation process?- How should barriers to the implementation of KMC be understood and
overcome?Three different databases from various subprojects of the research programme informed the planning and also served as triangulation:- Transcripts of interviews and field notes from the research in the two
hospitals in two provinces (1999-2000)- Responses to open-ended questions in an evaluation questionnaire
completed at the end of KMC training workshops by participants from four provinces (2000-2002)
- Observation notes from walk-through visits in the four hospitals where the workbook had been piloted (2001-2002)
The evaluation model depicted in figure 2 makes provision for three phases in the implementation process, namely pre-implementation,
61

implementation and institutionalisation. Each of these phases consists of two ‘steps’. The six steps are: awareness, conscious decision on implementation, taking ownership (mobilisation of space, equipment and human resources), visible evidence of implementation (babies in KMC position and records in use), evidence of routine and integration, and sustainable practice (accompanied by a mindset change). For each of the steps, progress markers were developed (in italics in figure 2) and an instrument was devised to measure these. The eventual aim is to compare the performance of the two randomised groups of hospitals receiving different outreach strategies with a view to determine whether one strategy has been more effective than the other. It is also envisaged to provide various forms of feedback to the participating hospitals.
FIGURE 2
62

FIGURE 3
The evaluation model is also rooted in different research principles (see figure 3). For the first two steps, evidence from the literature as well as from the other projects within the KMC research programme was used for the compilation of the implementation package and for awareness meetings. The next two steps are related to changes in behaviour and practices and can be measured quantitatively. The last two steps towards institutionalisation are also accompanied by a more qualitative approach to gauge paradigm shifts and to understand barriers to successful implementation. Whereas the first four steps are more focussed on the change process, change factors play a more prominent role during the phase of institutionalisation.
Conclusions
A number of lessons were learnt during the development of the evaluation model. Apart from the possibility of using progress markers with which to assess the progress of the implementation of KMC, the intricate interplay
63

between various factors that can either help or hinder the implementation process was also highlighted. These factors include the following:- level of awareness and exposure of health care workers to KMC.- involvement and interest of senior management in the
implementation process.- leadership of the drivers of the implementation process.- interpersonal relationships within a health care facility.- staff motivation.- management of human resources (including staff rotations). - extent of integration with related initiatives.Where implementation of KMC is unsuccessful it is necessary to investigate which of the factors act as barriers and to develop new management strategies. Further research is also needed into the complexity of the interaction between various factors or barriers. Ultimately the quality of KMC in a health care facility should be evaluated in an integrated manner together with other improvement-of-care initiatives related to KMC.
64

THE VALUE OF A KANGAROO MOTHER CARE (KMC) UNIT AT KALAFONG HOSPITAL
E van RooyenMRC Unit and Department of Paediatrics, University of Pretoria and Kalafong Hospital
IntroductionKalafong Hospital is a large regional teaching hospital serving a mainly black urban indigent population. It is also a referral hospital and manages high-risk pregnancies. A large number of high-risk LBW infants are delivered annually.Previously high-risk LBW infants were taken care of in a 15-bed High Care Unit (HCU) and a 12-bed low-care Low Birth-weight unit (LCU). The LCU functioned as a step-down facility to receive infants from the HCU. In the LCU they were cared for in incubators and bassinets in a conventional manner. During 1998 to 2000 an increasing number of high-risk LBW infants were taken care of in the HCU. During 1998 up to July 1999 all these infants could not be transferred to the LCU due to a lack of resources. Some infants had to be taken care of in the General Paediatric wards where care and conditions were not optimal. Due to the limited number of step-down beds, increased numbers of high-risk LBW infants, outbreaks of severe nosocomial infections in the HCU and the general lack of resources and equipment, it became necessary to consider an alternative method of caring for the infants.The relatively simple and novel method of KMC was considered to be the best method of resolving the demand for LBW infant care at Kalafong Hospital and a 25-bed Kangaroo Mother Care (KMC) unit was opened on 6 July 1999, which replaced the LCU. A total of 20 mother-and-baby pairs can be accommodated in the unit as well as 5 bassinets for conventional nursing care.
Subsequently an improvement has been experienced in the flow of patients between the HCU and KMC. This has relieved the pressure for
65

beds in the HCU allowing for an increased number of infants to be accommodated in the HCU during 2000.The KMC unit at Kalafong Hospital provides intermittent, continuous and conventional care to the LBW infants. The same number of nursing staff that rendered conventional care to the previous LCU, now provide care in the KMC unit. The unit is a low care facility and infants with signs of possible infection are transferred back to the HCU or one of the General Paediatric wards for further management. In order to apply the kangaroo discharge principle, namely discharge irrespective of weight, a follow-up clinic functioning within the KMC unit was established.
The KMC unit admits LBW infants as soon as the infants are in a stable condition and receive full oral feeds. There are no special weight requirements for admission to the unit. Stable infants less than 1000 grams are (have been) admitted. Oxygen- dependent infants who previously had to be admitted to the General Paediatric wards due to lack of space in the LCU are also cared for in the unit. The oxygen is administered via a nasal cannula and the mothers practice intermittent KMC.
Infants whose mothers are unavailable to take care of them, are placed in bassinets and cared for in the conventional manner. Apart from the exceptions most of the mothers practice 24-hour KMC and are empowered to become the primary care givers of their infants.
Before admission to the KMC unit most of the infants receive expressed breastmilk via an oro- or naso-gastric tube. In the unit, other feeding methods are introduced; for example cup feeding before proceeding to breastfeeding. Most infants are breastfed but formula feeds are given to infants whose mothers are HIV-infected and choose not to breastfeed.
Infants were discharged from the previous LBU as soon as they reached a weight of 1800 grams. This practice changed with the implementation of KMC and a new discharge strategy was introduced. Infants are discharged regardless of weight, as long as they breastfeed successfully and maintain
66

weight gain. After discharge all babies are seen within one week at the follow-up clinic which is held weekly in the KMC unit.
This study was undertaken to assess the effect of the KMC unit, on the care of low birth-weight infants at Kalafong Hospital.
67

Method
An audit was performed on all admissions to the KMC unit over an 18-month period from August 1999 to January 2001. An audit form was completed for each admission and provided the basis for analysis.
Data was collected on the number of infants admitted each month and the average length of stay in the unit, the admission and discharge weight of infants, breastfeeding practices of the mothers, deaths and infections that occurred, the follow-up clinic attendance rate and the average weight gain per day for each infant.
ResultsDuring the 18-month period of the study a total of 466 infants were admitted to the KMC unit with an average of 26 infants being admitted each month. The infants’ average length of stay in the unit was 13 days. The shortest stay was 2 days and the longest 71 days. The infants who stayed for a longer period were oxygen dependent due to chronic lung disease of prematurity.The Figure illustrates the admission and discharge weight categories of the infants in the KMC unit.
Overall 181 (38%) infants admitted to the unit weighed less than 1501 grams and of those, 6 (1%) weighed less than 1000 grams and, 57 (12%) less than 1001-1250 grams. With the support of the nursing and medical staff the mothers coped admirably with these small infants.
68

Also illustrated are the discharge weight categories. Of the infants discharged from the unit, 184 (39%) infants weighed less than 1751 grams and 5 (1%) infants weighed less than 1501 grams.
Under our previous policy infants were not discharged until they reached a weight of about 1800 grams. Since the implementation of KMC 184 infants could be discharged earlier resulting in a higher turnover of patients and enabling us to accommodate an increasing number of LBW infants.
Only one infant died in the unit during the 18-month study period. The possibility of infants developing a nosocomial infection in the KMC unit was the reason why 32 (7%) infants were transferred back to the HCU. No infants in the KMC unit were abandoned during the period of the study.
Breastfeeding is an important component of KMC. It was found that 396 mothers (85%) breastfed their infants. The 70 mothers (15%) who chose
69

not to breastfeed but to formula feed their infants included mainly mothers who were HIV-infected. Breastfeeding has important anti-infective properties which play an important role in the prevention of infections and necrotising enterocolitis. It is therefore heartening that such a large number, 85% of mothers breastfed their infants. This may be one of the reasons why so few infants (7%) developed possible nosocomial infections during their stay in the unit.One of the benefits of KMC is adequate weight gain (>15 grams/day). The results of the study proved that an average weight gain of 23 grams per day was achieved.
As the infants were discharged much sooner than the conventional practice, it was essential to closely monitor the progress of the infants following discharge. It was important to gather statistics of clinic attendance in order to ascertain how trustworthy the mothers will be in bringing back their infants for evaluation and growth monitoring.
The follow-up clinic was attended by 321 (69%) infants. Of those who attended, 216 (47%) attended more than once. There were 145 (31%) infants who did not attend. In previous studies conducted at Kalafong Hospital it was found that less than 50% of patients attended follow-up clinics. The audit found that more mothers than expected brought their infants for follow-up. The higher than usual follow-up rate may be due to the fact that the follow-up clinic is situated in the familiar environment of
70

the KMC unit where the mothers do not have to wait in long queues to be attended to.
Unfortunately 145 infants did not attend the follow-up clinic. This is an area of concern. Improvement of the attendance rate is needed and special attention should be given to the motivation of mothers to attend the clinic. Further investigation is needed to determine what happens to the mother and infant who do not attend the follow-up clinic.
ConclusionThe cost effectiveness of the KMC unit is considerable. The same number of nursing staff that rendered conventional care to the previous 12-bed LCU are now providing care to twice the number of infants as well as providing support to mothers.Very LBW high-risk infants were cared for successfully in the unit. A large number of infants (466) were managed in the KMC unit which relieved the accommodation pressure upon the HCU and has improved the morale of the nursing and medical staff. The mortality rate of the unit is low. Only one death occurred in the unit during the 18-month period. And no infants were abandoned. The establishment of the KMC unit is of great value and has improved the general care of LBW infants in Kalafong Hospital.
71

A SURVEY OF THE SOCIAL, CULTURAL AND EDUCATIONAL BACKGROUND OF MOTHERS ADMITTED TO THE KMC UNIT AT KALAFONG HOSPITAL
E van RooyenDepartment of Paediatrics, University of Pretoria, Kalafong HospitalMRC Unit for Maternal and Infant Health Care Strategies
I am presenting the preliminary results of an ongoing survey of the social, cultural and educational background of mothers admitted to the KMC unit at Kalafong hospital.
The information from the survey will be helpful to health care workers in order to develop personalised culturally appropriate health care and educational programs. The concept of social, cultural and educational background includes the beliefs, values and actions, which may influence the health care practices of the mother as primary care giver to her infant.
There has been no previous study of this kind in our unit. Health care workers should recognise the importance of social and cultural influences as well as specific cultural values. Understanding cultural rules allows for the interpretation of behaviour and will help the health care workers act appropriately.
Health education is a vital part of neonatal care and it is important that mothers understand the health care requirements of their new infants, especially when taking care of premature infants. Health education assists mothers and their families to deal with past, present and future health problems of their infants. This knowledge enables them to make informed decisions, to cope more effectively with alterations in their infant’s health and to assume greater responsibility for their infant’s well being. It is thus important that effective and appropriate educational health care programs are developed.
The RESEARCH problems that we identified: Mothers admitted to our unit are from a variety of social, cultural and educational backgrounds and health care workers do not always have a clear understanding of the beliefs, values and customs, which may influence the health care
72

practices of the mother and therefore they do not always render culturally appropriate care or develop effective educational health care programs.
Research Design: Descriptive study
Research MethodStudy populationMothers admitted to the KMC unit over a period of 6 months will be included in the study.
Data Collection: Data is collected from mothers by means of a structured questionnaire. The questionnaire is completed by a trained research assistant during a personal interview. A written informed consent is obtained from each participant. This is an ongoing study and 50 questionnaires have been completed. The questionnaire consists of 70 questions and it will not be possible to discuss all the details at this presentation. The ages of the mothers admitted to the unit varied. The youngest was 16 and the oldest 42 years, with a median of 26 years and a mean of 28.9 years.
Kalafong Hospital is a referral hospital and 30% of the mothers in the unit did not reside in Gauteng Province. The mothers form Gauteng was further subdivided into the greater Tshwane area. Kalafong is situated in the West and thus Western Tshwane area has the largest presentation.
The survey included the different languages spoken by the mothers. Before the survey we realized that the mothers in the unit represent a variety of language groups. Tshwane is situated in an area where most of the local people speak Northern Sotho but big metropolitan areas do not always reflect this. About 60% of mothers speak Northern Sotho but some of the other language groups are also well represented for example: Zulu. It was also noticeable how many mothers are able to understand either English or Afrikaans to some degree.
The marriage status of the mother reflect that only 32% are married while 64% are single. Only 28% mothers work while 66% of their partners work. Looking at who are the financial providers it was found that about half of
73
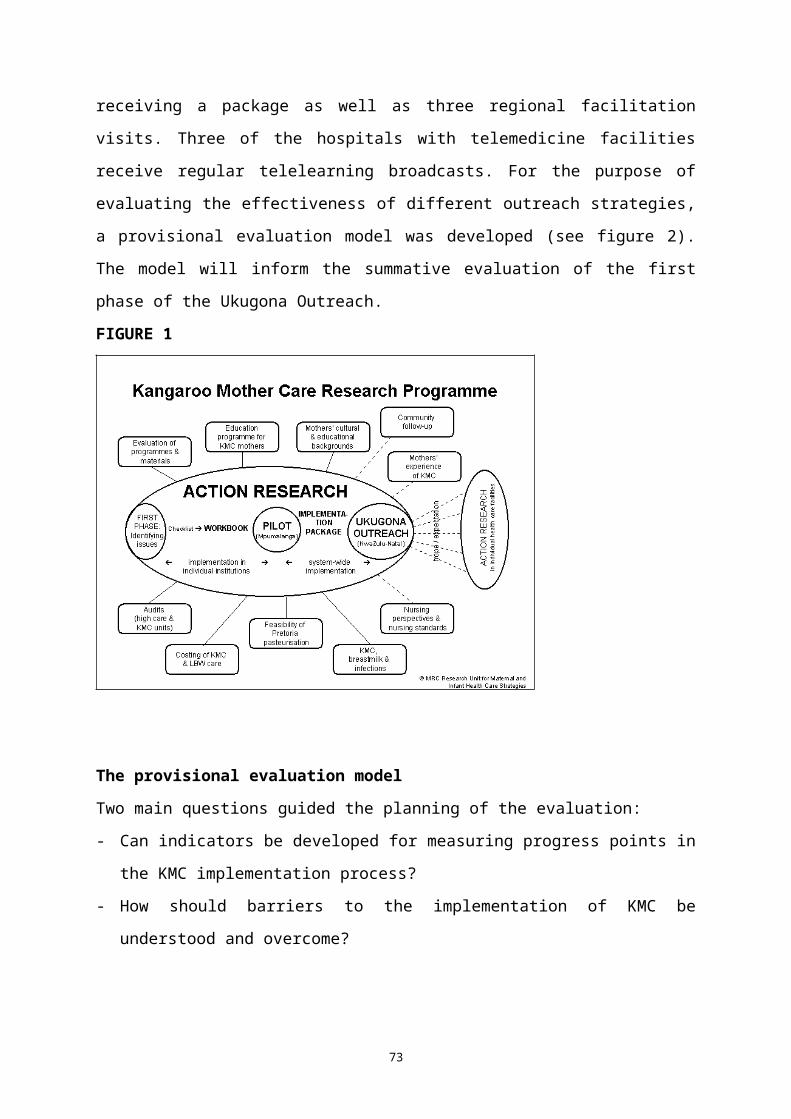
the mothers are supported by either the partner or themselves and the other half are dependent on other family members for financial support. If we look at the average monthly income 44% of the mothers have an income of less than R1000. The 20% who did not know their income may also fall into this category.
The mothers educational qualifications: 4% of mothers have no school education, 22% has a primary education, 30% Grade 8-10, 30% Grade 11-12, and 12% a higher education.
Housing and facilities at home: 66% mothers live in brick houses while 34% live in corrugated housing; 48% has water supply in the house while 52% have tap water close by, only one mother obtained water from a river; 72% of mothers have electricity and 22% have a phone in the house; 60% have flush toilets and 38% had pit toilets; 1 mother did not have any toilet facilities.
The different categories portrayed are whether mothers watch TV, listen to the radio, read a newspaper, magazine or books. TV or radio is watched and listened to most frequently. Only one mother did not have access to a radio or a TV. About 10% of mothers read regularly but more than 10% never read.
The smoking habits of the mother and partner are portrayed as follows. No mother admitted to smoking. Two said that they used snuff, 39% of their partners smoke. Only 16% of mothers admitted to drinking alcohol, namely beer and 64% of the partners drink alcohol, also mainly beer.
In the questionnaire several questions with different scenarios were asked about whether mothers will consider consulting a traditional healer. The three questions were whether they would consult a traditional healer if they have a social problem or if they have a medical problem or whether they would take their baby to a traditional healer to protect it against diseases. The majority of mothers said that they would never go to a traditional healer.
74

In conclusion the study is giving us interesting insights into the social, cultural and educational backgrounds of the mothers admitted to our unit and this information will help us develop appropriate health care and educational strategies.
A survey has limitations in that it is not possible to analyze the links between cause and effect. Some aspects are also difficult to interpret because by using a structured questionnaire one is restricted in the deductions that can be derived from different findings. A survey does enable one to recognize behaviour patterns and attitude trends and this survey may be the first step to possible further research studies.
75
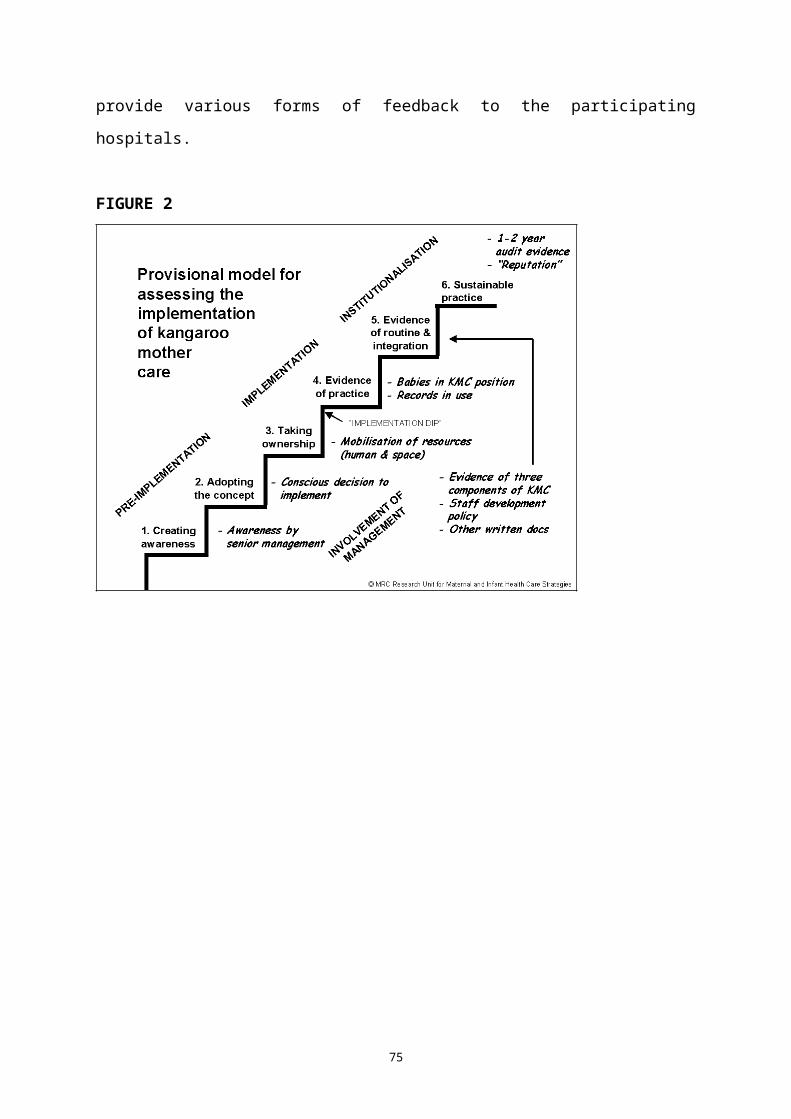
KANGAROO MOTHER CARE MADE EASY
E van Rooyen, A Pullen, A-M Bergh, RC PattinsonFaculty of Health Sciences and MRC Research Unit for Maternal and Infant Health Care Strategies, University of Pretoria
Background Because Kangaroo Mother Care (KMC) is an accepted way of decreasing neonatal mortality rates and decreasing cost of caring for low birth weight neonates, the MRC Research Unit for Maternal and Infant Health Care Strategies supports a research programme on the implementation of KMC. In informal discussions with health workers at KMC training sessions, the need for visual educational materials had been expressed from time to time. During the testing of an implementation workbook at four hospitals in Mpumalanga, health care workers identified a need for a visual educational tool for explaining the concept of KMC to mothers.
ObjectiveTo describe the development of an educational poster on KMC, which could also be used as a teaching tool.
The challengeTo develop a poster that - would appealing to the public;- could be used for educational purposes to introduce mothers to the
concept and practice of KMC.
ResultsThree people collaborated in the conceptualisation and development of the poster. After many drafts and inputs from colleagues, it was sent to KMC experts for comments.
The poster introduces kangaroo mother care by using the basic concepts accepted everywhere, namely KMC support, position, nutrition and discharge. This is done visually by means of photographs and simple text.
76

Originally a “long-life”, attractive wall poster for group education was envisaged. After the basic poster had been developed, two additional functions were added:- In some settings and under certain circumstances there was a need
for an individual bedside teaching tool and for this purpose the poster was adapted to an A4 size, printed on sturdy board and laminated.
- The text was translated into Zulu and the poster was mass produced on a lower quality paper, with English on one side and Zulu on the other. It was printed in A2 size for wall displays and in A4 size as a folded brochure.
ConclusionThe poster was included in the implementation package for the Ukugona Outreach project in Kwa-Zulu Natal to serve educational and publicity functions.It will be evaluated among users in terms of relevance, appropriateness and functionality. Other institutions and provinces could also use the basic conceptualisation in producing an educational tool for use in their health care facilities.
77

CONTINUOUS KANGAROO MOTHER CARE AT A SECONDARY HOSPITAL IN THE WESTERN CAPE: AN UPDATE
M Franken, M Wates, G Kirsten, C PieperDepartments of Paediatrics, Karl Bremer and Tygerberg Hospitals
IntroductionIntermittent Kangaroo Mother Care (KMC) is the preferred method of care for very low birth weight infants at the majority of hospitals in the Western Cape. Most institutions are, however, still reluctant to practice continuous KMC (CKMC) due to limited beds for mothers and a fear of infant death during CKMC. Some hospitals will only practice CKMC when the infant is ready for discharge. Karl Bremer Hospital (KBH) is the only secondary hospital in the Western Cape where early CKMC is practiced i.e. regardless to weight or gestation age provided the baby is stable and not receiving any supplementary oxygen or intravenous fluids.
AimTo determine the short term outcome of infants (birth weight <1800g) nursed with early CKMC.
Study DesignCohort analysis.
Patients and methodsOne hundre and seventy two infants admitted between 15 May 2000 to November 2001 to the eight-bedded KMC ward at KBH and nursed with early CKMC, were studied prospectively until discharge.
78

Results
Number of infants in CKMC 172Inborn (%) 145 (84%)Mean birth weight (g) (range)
1422 (670-1890)
Mean gestational age (wks) (range)
32 (25-40)
Mortality (%) 0Infection (%) 0Mean hospital stay (days) (range)
29.2 (4-84)
Mean daily weight gain (g) (range)
13.5 (-10-100)
ConclusionsEarly CKMC is safe as reflected by the low mortality and infection rate. The mean daily weight gain was less than the accepted 15g/day and could result in a prolonged hospital stay. Weight gain in these infants should be monitored closely and if suboptimal, corrective measures should be implemented.
79

OXYTOCIN AND FETAL DISTRESS
H J Odendaal
In recent years, several clinical incidents in which oxytocin was used in an unsafe way have been brought to my attention. The main problems were the ways in which oxytocin is used for the induction of labour and, in particular, for the augmentation of perceived poor uterine contractions.
Before augmentation of labour is discussed in more detail, it is essential to know that an unfavourable fetal position, placenta praevia, fetal distress and excessive uterine contractions are absolute contra-indications for the use of oxytocin.
In addition, oxytocin should be used with caution in cases of mild cephalopelvic disproportion, polyhydramnios, cardiac disease, suspected fetal distress, breech presentation, previous caesarean section, shortly after prostaglandin administration and coupling of uterine contractions.
Although O’Driscoll wrote his controversial article on the acceleration of slow labour many years ago, its place is still uncertain. In a meta-analysis on the active management of labour in primigravidae, Glantz and McNanley found a reduction in Caesarean section deliveries. However, Fraser et al, could not confirm the findings in another meta-analysis. It is interesting to note that the same randomised controlled trials were used in both meta-analyses, but not other articles.
O’Driscoll stated very specifically that the mother must be a primigravida, the presentation must be vertex, the fetus must be single and the membranes must be ruptured and clear amniotic fluid seen. The first three prerequisities are still accepted, but membranes are now kept intact longer to reduce HIV transmission from mother to fetus. O’Driscoll started with 6–7mU/min of oxytocin and increased it to 40mU/min. This very high dosage is no longer acceptable. For example, the Royal College of
80
Obstetricians and Gynaecologists recommends that one should start with 1–4mU/min, increasing it to a maximum of 12mU/min.I am concerned about the liberal use of oxytocin in local populations. Black patients have smaller pelvices, stronger uterine contractions, but not smaller babies. Is it safe to use more force to achieve a normal delivery? Coloured mothers have smaller babies and probably more placental insufficiency because of the high incidence of pre-eclampsia and the frequency of cigarette smoking. Is it safe or necessary to stimulate labour in all primigravidae?
In many hospitals, oxytocin is routinely used for augmentation of labour in all primigravidae. Some of them even use it in multigravidae or in mothers who have had previous Caesarean sections although there are no randomised controlled trials to support this policy or to confirm its safety.
Phillpot did most of the work on the stimulation of labour in black mothers. First of all, it needs to be stated that he limited its use to primigravidae only and that he used much less oxytocin. He started with about 2mU/min and continued no longer than 6 hours when there was no progress. In addition, he paid special attention to the meticulous clinical monitoring of the fetal heart rate by trained nursing staff in an intensive care area.
He used the partogram (cervicograph) to determine which primigravidae should receive oxytocin. It is interesting to note that only 11% of patients crossed the action line. Using this regimen, he was able to reduce the frequency of Caesarean sections from 9.9% to 2.6% and perinatal deaths from 5.8% to 0.6%. These excellent results show what can be done when oxytocin is given for specific indications and under meticulous control.
Unfortunately health care workers in many hospitals in South Africa use oxytocin for the augmentation of labour more liberally, in a higher dosage and with inadequate attention to the fetus. This is most likely one of the reasons for the very high incidence of perinatal deaths in this country, as
81

reported at previous conferences on Priorities in Perinatal Care. In a recent study, Pattinson found that 72% of deaths during labour are caused by labour-related asphyxia.Phelan and Ahn studied the perinatal observations in 48 neurologically impaired term infants and compared those with reactive fetal heart rate patterns at the beginning of labour with nonreactive patterns. Patients with reactive patterns - implying that the fetus was well at the beginning of labour - had longer use of oxytocin, more tetanic episodes and more contractions. These findings demonstrated that the liberal use of oxytocin is an important cause of cerebral palsy.
Experience in fetal heart rate monitoring has shown that frequent uterine contractions, tetanic contractions or an increase in basal tone can occur very suddenly, without any prior warning and even at a low infusion rate of oxytocin. It is therefore absolutely essential that the fetal heart rate is monitored electronically when oxytocin is used. There is no way that auscultation, even every 15 minutes, can detect alarming effects on the fetal heart rate pattern timeously.
Oxytocin is a very potent drug with many potentially harmful side effects. It should not be used for poor indications or by people who are not aware of its impact on the fetal heart rate or uterine contractions. Electronic fetal heart rate monitoring is essential to detect fetal heart rate abnormalities. Death from asphyxia during labour is totally preventable.
82

FINDING THE CULPRIT - INTRAPARTUM HYPOXIA IN SOUTH AFRICAN HOSPITALS E Buchmann, R Pattinson, M PatrickMRC Unit for Maternal and Infant Health Care Strategies, University of Pretoria
The Saving Babies report of 2000, using data from the Perinatal Problems Identification Programme (PPIP) identified intrapartum hypoxia, also known as ‘birth asphyxia’, as an important and avoidable cause of perinatal death in South Africa. In response to these findings, we undertook a more detailed study of deaths from intrapartum hypoxia, to identify the clinical and health service problems that are associated with these deaths, so as to make specific recommendations for prevention.
MethodsContributors from PPIP sites were asked to participate in this study. Those who expressed an interest were sent data sheets on which to enter detailed information from each death caused by intrapartum hypoxia according to the PPIP definition. Descriptive statistics were used for the analysis.
ResultsData sheets were returned by the following hospitals: Addington, Chris Hani Baragwanath, Kalafong, Eben Donges, Empangeni, Kimberley, Klerksdorp, Leratong, Mankweng, Lydenburg, Middelburg, Settlers, Uitenhage, Witbank, All Saint’s, Mapulaneng, Port Alfred, St Elizabeth’s, Tshilidzini. One hundred and two cases of perinatal death from intrapartum hypoxia were analysed, from 23 metropolitan, 35 city and town, 34 rural hospitals.
There were 22 stillbirths and 80 neonatal deaths. The mean birth weight was 3021g with a median gestational age of 38 weeks. Two infants had a gestational age of 41 weeks, and one of 42 weeks. There were seven breech presentations and one transverse lie. Five mothers had mild to
83

moderate hypertension in pregnancy. Four deaths followed induction of labour. The primary obstetric causes of death were intrapartum hypoxia (82), meconium aspiration (8), cord prolapse (7), trauma from breech delivery or shoulder dystocia (3) and uterine rupture (2). The median time that women were in hospital before delivery was 6.5 hours, with 24% in hospital for less than two hours before giving birth. The findings on labour length and progress are summarised in table 1.
Table 1 Labour duration and progress preceding perinatal death caused by intrapartum hypoxia
n %Latent phase >8 hours (n=82) 14 17Active phase >12 hours (n=86) 6 7Progress crossed partogram alert line (n=90) 31 34Progress crossed 2-hour partogram action line (n=90)
16 18
Progress crossed 4-hour partogram action line (n=90)
9 10
Oxytocin augmentation (n=102) 10 10Second stage >2 hours (n=66) 12 18
Fetal monitoring was noted for 80 cases. Cardiotocography was used, at least intermittently, in 41 (55%), fetal stethoscope in 24 (32%), and hand-held Doppler in 10 (13%). Findings of fetal monitoring, with modes of delivery, are shown in Table 2.
Table 2 Detection of intrapartum fetal distress and mode of delivery preceding perinatal death caused by intrapartum hypoxia (n=80, cardiotocograph used in 41)
n %Fetal heart decelerations during contractions 22 28Fetal heart decelerations after contractions 27 37All fetal heart decelerations detected 39 49Meconium staining of the liquor 50 63Thick meconium staining of the liquor 37 46Thick meconium staining with decelerations 17 21Caesarean section for fetal distress or cord prolapse
14 18
Vacuum extraction for fetal distress 2 3
84

Thirty-five infants were born by caesarean section, with the indication for operation being 11 for fetal distress and three for cord prolapse. All the other indications were maternal or obstetric, including cephalopelvic disproportion, breech presentation, previous caesarean section and transverse lie. Caesarean sections were done in 18 of the 27 women where late decelerations were detected. The time taken from decision to operate to the delivery was recorded in 28 cases. In 18 (64%) there was a delay of greater than 30 minutes, and in 14 (50%), it took more than 60 minutes for the babies to be delivered. There were 14 assisted vaginal deliveries (21% of vaginal births), including one forceps and 13 vacuum deliveries. Two of these assisted deliveries were performed for fetal distress, with the remaining 12 done for prolonged second stage or maternal exhaustion.
Eighty babies were born alive. Seventy had Apgar scores recorded, and 62 (89%) had scores less than seven at five minutes. Fifty-two newborns were intubated and 19 resuscitated with oxygen by mask. Details on the timing and circumstances of resuscitation were insufficient for meaningful analysis. Fifteen babies went on to receive intensive care ventilation. In the opinions of the persons completing the forms, 19 babies would have survived if ventilation facilities had been available at their institutions.
The time of delivery was recorded for 101 babies. Sixty were born in the night shift (19:00 to 07:00), which is 46% more than the 41 born during the day. Delay in presentation in labour was noted in 27 cases, with eight related to transport difficulties from home to the labour unit, and four caused by delays in transport from clinic to hospital. The median number of babies born during a 12 hour shift was six, with the median numbers of staff available being three midwives and one assistant nurse. Doctors were noted to be immediately available in 91% of the cases. Cardiotocographs (CTGs) were available in 98 out of the 102 cases, with the hospitals having a mean of 4.5 and a median of 2 CTGs. A mean of 3.9 CTGs were actually in working order at the time of the deaths. Basic
85

resuscitation equipment, including tubes and laryngoscopes, were available in all instances, but in only 51 (50%) was it possible to provide ventilation for newborns after initial resuscitation.
86
DiscussionIn searching for a common thread that links these deaths from intrapartum hypoxia, it was possible to reject a number of factors as possible major contributors. Post-term pregnancy, oxytocin use, breech presentation, and prolonged first stage of labour were not prominent in this sample of perinatal deaths. Labour prolongation, measured by absolute time or by crossing of lines on the partogram, was surprisingly uncommon.
Staffing and facilitiesSkilled staff and appropriate equipment were available in all of these hospitals, but it was not clear whether there was a midwifery shortage in any of these institutions. There were frequent delays in performance of caesarean sections. Cardiotocography and neonatal resuscitation equipment is available and mostly in good working order, although CTGs are probably in short supply in most of the institutions.
Transport and delay in arrivalDelay in presentation was a common problem, with transport difficulties predominating. Transport problems go beyond the health service. Poverty, distance, telephone and road infrastructure, and local administrative capacity, all play a role. In rural areas, mothers’ waiting areas in hospitals and clinics will continue to be the most effective way for women to ensure safe and supervised delivery.
Early detection of intrapartum hypoxia (fetal distress)The most striking finding in this study was the frequent failure to detect fetal distress during labour. Late decelerations were detected in only one-quarter of these cases, and operative deliveries for fetal distress were done for only a small minority. For many of these deliveries, the poor condition of the babies at birth must have been surprising to the attending midwives or doctors. It appears that insufficient care is taken with fetal monitoring and that early signs of fetal hypoxia are frequently missed.
87

The second stage of labourThe rates of prolonged second stage and assisted delivery were relatively high. Women who are pushing in the second stage of labour should not be left alone, and fetal heart auscultation must be done after each contraction. This will allow early detection of fetal bradycardia, and appropriate action can then be taken.
Neonatal careWhile most of these babies were intubated after birth, the quality of resuscitation could not be assessed. The absence of neonatal ventilation facilities is problematic as the necessary equipment and expertise are unavailable in most South African hospitals. Skills and equipment for neonatal resuscitation must be available in all obstetric units. Training of midwives and doctors remains an ongoing priority.
ConclusionIntrapartum hypoxia is a common and avoidable cause of perinatal death in South African hospitals. This study has demonstrated that the majority of these deaths occur in low-risk women with low-risk labour, with failure to detect signs of fetal distress. The single most important shift in our labour care should be close and careful monitoring of women in labour, with particular attention to detail in fetal monitoring.
88

INDUCTION OF LABOUR FOR SEVERE PRE-ECLAMPSIA AFTER 34 WEEKS
P Roets, PS Steyn, HJ OdendaalDepartment of Obstetrics and Gynaecology, Tygerberg Hospital and MRC Unit for Perinatal Mortality and University of Stellenbosch
BackgroundSevere pre-eclampsia (PE) and eclampsia are regarded by some obstetric units as an indication for emergent caesarean section, whilst other units stabilise the patient before attempting vaginal delivery through induction of labour, with good control of the maternal condition. Even in centres following the latter policy, caesarean section rates of up to 50% are obtained. There is an increased maternal morbidity associated with Caesarean sections, with the risk increasing when associated with underlying conditions like severe PE. This then serves as a reason for units to attempt vaginal delivery, as opposed to primary caesarean section. There is, however, an increased morbidity associated with emergent caesarean section should induction of labour fail, or fetal distress develops. There is also the danger that the patient’s condition can deteriorate after induction of labour, increasing her risk for morbidity. It is, therefore, important to know the caesarean section rate in patients undergoing induction of labour for severe PE, as well as the associated maternal and fetal morbidity.Currently, patients presenting with severe PE after 34 weeks gestation at Tygerberg Hospital, are stabilised before undergoing induction of labour in the absence of other obstetric contra-indications to vaginal delivery.This study reports on the outcome of patients with severe PE who undergo induction of labour in a tertiary hospital setting.
Aim of the StudyThe aim of this study was to determine the caesarean section incidence, as well as the maternal and fetal morbidity with regard to delivery
89

method, in patients undergoing induction of labour for severe PE after 34 weeks gestation.
MethodsForty-seven consecutive patients undergoing induction of labour for severe PE after 34 weeks gestation in Tygerberg Hospital’s labour ward were identified by the clinicians in the labour ward and induced according to a standard protocol. Their medical records were then used to obtain the data necessary for the study.
Inclusion criteria Severe pre-eclampsia
PE was defined as having more than 300 mg proteinuria per 24 hours or 2+ proteinuria on dipstix on 2 occasions more than four hours apart, with a diastolic blood pressure of 110 mmHg or more on 2 occasions 30 minutes apart, or a single diastolic blood pressure of 120 mmHg.
Gestational age of more than 34 weeks.
Exclusion criteria Patients with a gestation of less than 34 weeks. Patients undergoing a caesarean section primarily for another obstetric
reason. Eclampsia.
Method of induction of labourInduction of labour took place in labour ward according to a standard protocol. Patients with a Bishop count of less than 7/13 received two doses of Prepidil® 0.5mg Gel (prostaglandin E2 analogue) four hours apart intracervically. If it was technically not possible to rupture membranes after this, the patient underwent a caesarean section for failed induction.If, at any stage, it was possible to rupture the membranes (Bishop score more than 7), this was done. Oxytocin (according to the labour ward’s
90

standard protocol) was started if spontaneous contractions did not follow within two hours.The fetus was monitored for 10 minutes prior to the insertion of Prepidil®
gel, and one hour afterward, and continuously in the presence of contractions. Fetal distress was managed according to standard obstetric practice.
ResultsForty-five patients met the inclusion criteria of the study. The mean age of the patients was 27.22 years, and the median gravidity was 2, and parity 1. Eighty-four percent underwent medical induction and 16% surgical induction. The average induction to delivery time was 18.84 hours, with no difference between those delivering vaginally and those undergoing caesarean section. Twenty-three (51.11%) delivered vaginally, and 22 (48.89%) by caesarean section.
Comparative outcomesIn the vaginal delivery group, the mean induction to delivery time was 20.43 hours (minimum 2, maximum 91, SD 18.78), whilst in the caesarean section group it was 17.81 hours (minimum 0, maximum 50, SD 14.51) [p-value = 0.52].The mother’s stay in hospital postpartum was significantly (p-value = 0.000) longer in the caesarean section group, with a mean value of 4.59 days (minimum 2, maximum 9, SD deviation 1.56). In the vaginal delivery group the mean stay was 2.7 days (minimum 1, maximum 7, SD 1.52).No maternal febrile morbidity was experienced in the vaginal delivery group, whilst 2 cases were experienced in the caesarean section group (p-value = 0.139).Maternal complications were experienced in one case of the vaginal delivery group, and four cases of the caesarean section group (p-value = 0.14).No statistical difference in the masses of the babies in the two groups was found. The mean mass in the vaginal delivery group was 2532.09g
91

(minimum 1506, maximum 3860, SD 598.06), whilst the mean mass in the caesarean section group was 2190.64g (minimum 1270, maximum 3390, SD 663.34) [p-value = 0.388].No differences in the one, five, or ten-minute Apgar scores were found. The median one minute Apgar in the vaginal delivery group was nine (minimum six, maximum ten), and in the caesarean section group was eight (minimum four, maximum ten) [p-value 0.081]. The median five minute Apgar in both groups was nine (caesarean section group had a minimum of five, and a maximum of ten, whilst the vaginal delivery group had a minimum of eight, and a maximum of ten) [p-value = 0.587]. The median ten minute Apgar was ten (caesarean section group had a minimum of six, and a maximum of ten, whilst the vaginal delivery group had a minimum of eight, and a maximum of ten) [p-value = 0.554].One baby in the caesarean section group was admitted to NICU, with no admissions to NICU in the vaginal delivery group [p-value = 0.301]. Eight neonatal complications were experienced in the vaginal delivery group, compared with six in the caesarean section group [p-value = 0.586].Eight babies in the vaginal delivery group had intrauterine growth restriction, whilst thirteen babies in the caesarean section group had intrauterine growth restriction [p-value = 0.102].There was, however, a significantly [p-value = 0.031] longer hospitalisation of babies delivered by caesarean section, with a mean stay of 5.41 days (minimum 2, maximum 9, SD 2.09), compared to a mean stay in the vaginal delivery group of 3.91 days (minimum 1, maximum 9, SD 2.41).
ConclusionsInduction of labour in severe PE after 34 weeks is a viable option, with no significant increase in maternal or neonatal morbidity. It was, however, found that patients undergoing caesarean section after induction of labour had a longer maternal stay in hospital after delivery, with a longer infant stay in hospital, possibly secondary to the maternal stay. Induction of
92

labour in such patients reduces the number of high risk patients exposed to anaesthesia and surgery.This study should be continued to obtain larger numbers, which would possibly allow one to identify factors that may help predict the outcome of induction of labour in severe PE. Factors like umbilical artery Dopplers and the Bishop score should be included in the study. If predictive factors are identified, these can then be used to assign patients to induction or primary caesarean section in a randomised control trial.
93

ECLAMPSIA: A PROSPECTIVE AUDIT OF 112 PATIENTS ADMITTED TO KING EDWARD VIII HOSPITAL OBSTETRIC HIGH CARE UNIT
F Paruk, J MoodleyMRC Pregnancy Hypertension Research Unit and Department of Obstetrics and Gynaecology, Nelson R Mandela School of Medicine, University of Natal, South Africa.
IntroductionEclampsia is a multisystem disorder associated with significant fetomaternal morbidity and mortality. The incidence of eclampsia is variable but it is generally lower in well-resourced countries compared with resource scarce regions. Nonetheless the attendant morbidity is cause for equal concern in developed and developing countries. The most recent report on eclampsia at our institution (Durban, South Africa) was published in 1993. Subsequent to this, there have been various changes in health care delivery such as the provision of free antenatal care (from 1996), upward mobility of patients, improvement in patient referral patterns, the widespread acceptance and use of magnesium sulphate in the management of eclampsia (following the results of the Eclampsia Collaborative Trial and the institution of standardised management protocols for eclampsia). Furthermore, “complicated” cases of eclampsia are aggressively managed and a more liberal policy of ventilatory support has been adopted compared to the past. In addition, fluid management receives meticulous attention. This audit was performed to ascertain the impact of these changes on the maternal morbidity and mortality associated with eclampsia at our institution by comparing the current data to 1980 and 1990 data.
MethodThis prospective study was conducted in the Obstetric High Care Unit at King Edward VIII Hospital, a tertiary academic centre in Durban. The Obstetric High Care Unit comprises 2 wards (4 beds/ward) adjoining the labour ward delivery suite. All eclamptic patients are managed in this unit post delivery for a minimum period of 24 hours. The standard
94

management includes the following principles: the administration of magnesium sulphate, stabilisation of blood pressure, fluid balance monitoring (CVP), planning and effecting delivery within 12 hours of initial seizure, high care nursing and ICU therapy consideration in complicated cases. All patients admitted with the diagnosis of eclampsia from 1 January 2000 to 30 June 2000 were eligible for the study. Eclampsia was defined as follows: a diastolic blood pressure of >90mmHg, a proteinuria value of >1+mgdL and generalised seizure(s) in a gravid patient. There were no exclusions. Data captured included maternal age, gestational age, parity, number of seizures, blood pressure, timing of seizures in relation to delivery, site of diagnosis of eclampsia, maternal booking status, mode of delivery, Glasgow Coma Scale, maternal complications, haematological and biochemical abnormalities, duration of high care management, duration of intensive care and ultimate outcome. Renal dysfunction was diagnosed in the presence of oliguria (urine output below 30ml/min) or a urea level exceeding 10 mmol/l. Data are presented as actual numbers, means and percentages.
Results The incidence of eclampsia is depicted in Table 1. The total number of deliveries in 1980 and 1990 were 23 902 and 22 636 respectively. In 2000 there were 12789 deliveries in the 6-month period. The 1980 and 1990 data include King Edward VIII Hospital as well as clinic deliveries. The present study data include in addition, deliveries conducted at referring regional/district hospitals. The total number of eclamptic admissions has increased from 67 in 1980 to 135 in 1990 to 112 patients in a six month period in 2000. The incidence of eclampsia has increased from 2.8/ 1000 deliveries (1980) to 6/1000 deliveries (1990) to 8.8/1000 deliveries (2000). There were 3 maternal deaths in this series. The maternal mortality attributed to eclampsia has decreased- 11.9% (1980), 8.9% (1990) and 2.7% (2000). Figure 1 illustrates that 56.25% of seizures occurred in the antenatal period. This is lower than the previously reported incidence of 91% and
95

79.3% for 1980 and 1990 respectively. The proportion of intrapartum and postpartum eclampsia in the current series was 28.57% and 15.18% respectively. In total, 24% (27 patients) of eclamptic seizures evolved in a health care facility.As depicted in Table 2, the mean age of occurrence of eclampsia remains unchanged - 21.4 and 21.8 years for 1990 and 2000 respectively. Table 2 clearly highlights the point that in all 3 series (1980, 1990 and current data) the majority of the eclamptic patients are primigravidae. The mean gestational age was 34 weeks. In the current series, 50 patients (44.6%) had received some form of antenatal care on at least 3 occasions.
The mean duration of hospital stay was 11 days, whilst the mean duration of high care management constituted 55 hours - as depicted in Table 3. Intensive care unit (ICU) therapy was indicated in 19 patients (17%) in this series compared to 8.9% in the 1990 series. ICU therapy including ventilatory support was indicated in the scenario of extreme restlessness, inability to maintain an airway, metabolic acidosis or multiorgan dysfunction.
It is evident from Table 4 that the majority of eclamptic patients were fully conscious on admission (77 cases=68.8%). In addition, no patient had an admission Glasgow Coma Scale (GCS) below 10. In the 1980 series, 10.4% and 82% of patients were unconscious or semi-conscious respectively. In the 1990 series, 32% of cases had an admission GCS below 10. Furthermore, only 41 % of cases were fully conscious in that particular series.
The caesarean section rate among the antepartum and intrapartum eclamptic cases (n=95) was 76.8%. Regional anaesthesia was utilised in 39 patients (53.4%) undergoing a caesarean section. The postpartum eclamptic cases (n=17) exhibited a 5.9% caesarean section rate. The 1990 data reports an overall (ie. antepartum, intrapartum and postpartum cases, n=135) caesarean section rate of 78.5 %.
96

Seizure recurrence in patients on the Magnesium Sulphate regimen was 1.8%. Marked fluctuations were noted in blood pressure measurements in the first 24 hours post delivery. The difference in peak diastolic blood pressure and lowest diastolic blood pressure varied from 10 to 49 mmHg, with a mean value of 26 mmHg [SD 12.87]. A rapid acting agent (Dihydrallazine or Labetolol) was indicated in 25% of patients. Long-term antihypertensive agents were indicated in 75.9% of cases.
Maternal complications are listed in Table 5. Thrombocytopenia (32.9%), anaemia (14.3%) and the HELLP Syndrome (9.8%) comprised the common complications in this series. In comparison to the 1990 data the data from the current series illustrates a reduction in the incidence of renal failure (21% to 2.7%), abruption placentae (6% to 2.7%), coagulopathy (11% to 5%), anaemia (19% to 14.3%) and pulmonary oedema (4% to 1.8%). The incidence of thrombocytopenia was not documented in the previous series. One patient developed an intracerebral haemorrhage.
In this series, the 3 maternal deaths occurred in young patients (aged 16 to 22 years) of low parity. One death was associated with an administrative problem (lack of ICU availability) together with an iatrogenic complication. The second case exhibited marked lability of blood pressures in the scenario of the HELLP Syndrome. There was a logistic delay in procuring platelets and the patient developed an intracerebral haemorrhage. The third patient had the potentially fatal combination of eclampsia and an abruption. She required ICU therapy, but succumbed to nosocomial sepsis. In the previous report, 50% of maternal deaths occurred in patients above 31 years. In addition, 25% of maternal deaths were associated with intracerebral haemorrhages. No significant poor outcome markers were identified (viz. age, parity, booking status, Glasgow Coma Scale)
DiscussionThis audit clearly reflects an increasing trend in the incidence of eclampsia from 2.8/1000 deliveries (1980) to 6/1000 deliveries (1990) to
97
8.8/1000 deliveries in the current series. The increase is probably multifactorial in origin and related to improvements in the patient referral system as well as increase in the number of patients seeking health care. It is unlikely that it is reflective of a true increase in the incidence of the disease process. The current incidence is comparable to reports from other centres in South Africa as well as other developing countries. The incidence rates reported range from 3.6/1000 deliveries to 8.1/1000 deliveries. In stark contrast to this, the incidence of eclampsia in well-resourced regions has been drastically reduced. In a retrospective analysis spanning a 60 year period, Leitch et al (1998) from the United Kingdom have demonstrated a reduction in the disease incidence of greater than 90% from 74.1/10 000 in the 1930s to 7.2/10 000 deliveries in the 1980s. Douglas and Redman report the national incidence of eclampsia in the United Kingdom to be 4.9/10 000 maternities [95% CI: 4.5-5.4]. It is claimed that appropriate antenatal care together with timeous hospitalisation and delivery of patients with pre-eclampsia will reduce eclampsia. It is known that women in poor countries contend with problems of lack of education, gender inequality and the lack of or inaccessibility of health care. This probably explains the disparate disease incidence for different regions. In the current series, 44.6% (50 patients) had received some form of antenatal care on at least 3 occasions. The “booking” status of patients at our institution has not improved despite the provision of free antenatal services. This suggests that other specific issues such as female education, antenatal care availability, accessibility as well as acceptability need to be concomitantly assessed and appropriately addressed.
The associated maternal mortality of 2.7% (3 cases) is a reduction compared to previous rates of 8.9% and 11% for 1990 and 1980 respectively. The mortality rate in this series is low compared to 21.2% reported by Mwinyoglee et al (1996) from South Africa and 6.1% by Conde-Agudelo and Kafury-Goeta from Columbia. The low mortality rate in this series is probably largely attributed to patient related factors but also
98

to an extent associated with improved medical care. The patient related factors include upward mobility of patients and an improvement in socio–economic status as well as knowledge with respect to the availability of free maternity services. These factors have, in all likelihood, resulted in early patient presentation (as reflected by the admission neurological status of patients in this series). The point that the majority of patients in this series (68.8%) were fully conscious on admission compared to 41% and 7.6% in the 1990 and 1980 series, suggests that the patients are presenting early to a health facility following the onset of eclampsia. The reduction in the associated morbidity is thus not unexpected. From the medical care perspective, aggressive management including a more liberal policy for ventilatory support (17 % in this series compared to 8.9% in 1990), widespread acceptance on the use of magnesium sulphate (prior to 1995, either phenytoin or magnesium sulphate were indicated for further seizure prophylaxis), judicious blood pressure stabilisation, meticulous surveillance and management of fluid balance, a low rate of seizure recurrence (1.8%) on the Magnesium Sulphate regimen, and high care nursing have also contributed to the reduction in the associated morbidity and mortality. Although the proportion of intrapartum (28.57%) and postpartum cases (15.18%) has increased in this series, one cannot extrapolate that it is largely responsible for the reduction in maternal deaths – as only 24% of eclamptic seizures evolved at a health care facility. The maternal mortality in this series is however high if compared with developed countries, the most recent report on the confidential enquiry into maternal deaths in the United Kingdom quotes 2.4 eclamptic maternal deaths/1 000 000 maternities for the triennium 1997-1999. In the United States, Pritchard and Sibai have each reported 1 maternal death in two separate eclamptic series comprising 245 and 254 cases respectively.
The caesarean section rate of 76.8% among the antepartum and intrapartum cases (n=95) is high, but not unexpected. It is interesting to note that 53.4 % of the caesarean sections were conducted under regional
99
anaesthesia. The point that the majority of cases were of the uncomplicated variety, allowed for the consideration of regional anaesthesia. It must be stressed, however, that the choice of anaesthesia needs to carefully considered and individualised for each case by an experienced obstetric anaesthetist. A cause for concern is the observed lability of blood pressures in the first 24 hours post delivery (a mean value of difference in blood pressure of 26 mmHg, SD 12.87mmHg). In addition, 25 % of patients required a rapid acting agent.
This raises the issue of the potential advantages of indicating an intravenous antihypertensive agent (as standard management for at least 24 hours post delivery) in order to titrate the blood pressure and thereby prevent blood pressure fluctuations. The risk-benefit ratio assessment of this proposal certainly warrants further exploration.
Thrombocytopenia (32.9%), anaemia (14.3%) and the HELLP Syndrome (9.8%) comprised the commonest complications in this series. The increase in incidence of the HELLP Syndrome compared to the 1990 series (2%) is probably not a true increase. The incidence of the syndrome was most likely underestimated in the previous series, as it was limited by its retrospective nature. Although anaemia remains a common complication, it’s incidence has declined from the previous series (19% to 14.3%). This reduction is probably attributed to the reduction in incidence of abruption placentae (from 6% to 2.7%). The reduction in the cases of abruption placentae may also explain the lowering in the incidence of coagulopathy (from 11% to 5%). A striking observation is the marked reduction in the incidence of renal dysfunction from 21% to 2.7%. It is important to take cognisance of the point that this reduction has been achieved without a concomitant increase in the incidence of pulmonary oedema – in fact the incidence of pulmonary oedema has declined marginally from 4% to 1.8%. This result is probably related to improved understanding and care of fluid management in eclamptic patients. At our institution, all eclamptic patients are subjected to serial CVP (central venous pressure) monitoring,
100

fluid titration with colloids and meticulous attention to fluid intake and output.
In light of the fact that there were only 3 maternal deaths in this series, it is not surprising that predictors of mortality could not be identified. It is interesting to note that the maternal deaths in this series occurred in young patients aged 16-22 years. We recently reported a similar finding in a highly select cohort of 105 eclamptic patients managed in an ICU. It was clearly evident in that particular series that fatalities occurred in relatively young patients (mean age of 25 years). This is in contra-distinction to the 1980 and 1990 series, where the majority of deaths occurred in patients older than 31 years of age.
In conclusion, this audit illustrates that the incidence of eclampsia remains substantial at our institution. From a positive perspective the attendant maternal morbidity and mortality has declined, nonetheless there is room for improvement. A concerted effort is required to reduce the incidence of eclampsia. It is indeed of paramount import to ensure accessibility, availability and acceptability of antenatal services. In addition, there is a need to promote female literacy, female education and gender equality. From a medical perspective, antenatal care providers need to be appropriately trained to identify and manage pre-eclampsia adequately. The findings of the multicentre Magpie Trial (of which King Edward VIII Hospital constituted a participating centre) provides sufficient evidence for the use of prophylactic magnesium sulphate in severe pre-eclampsia in order to reduce the incidence of eclampsia. It would be prudent to practice this at our institution. Eclampsia, once diagnosed, should be managed as previously described by Moodley et al. In addition, meticulous attention needs to be focused on blood pressure control, fluid management and a careful assessment on the need for intensive care.
Table 1 Incidence of Eclampsia and the associated MortalityParameter 1980 1990 2000Duration of study (months) 12 12 6Total number of deliveries 23902 22636 12789
101

Number of eclamptics 67 135 112Eclampsia cases/1000 deliveries 2.8 6.0 8.8Number of deaths/(%) 8(11%) 12(8.9%) 3(2.7%)
Table 2 General DataParameter 1980 1990 2000Mean age [range]-years 21.4[14-40] 21.8[15-42]Primigravidae 65.7% 64.4% 64.3%Mean gestation- weeks 31.7 34
Table 3 Hospital StayParameter Mean duration [range]Total stay (n=112) 11 [5-41] daysHigh Care stay(n=112) 55 [24-120] hoursICU stay (n=19) 57.8 [12-144] hours
Table 4 Level of Consciousness on AdmissionParameter 1980
(n=67)1990(n=135)
2000*(n=112)
Fully conscious 7.6 % 41 % 68.8 %Semiconscious 82 % 47 % 31.2 %Unconscious 10.4 % 12 % -*No patient had an admission Glasgow Coma Scale below 10/15 in 2000
102

Table 5 Maternal Complications Associated with EclampsiaComplication 1990 (%) 2000 (%)HELLP Syndrome 2 9.8Coagulopathy 11 5Cerebral oedema 7 6Pneumonia 2 2.7Pulmonary oedema 4 1.8Abruption placentae 6 2.7Renal 21 2.7Anaemia 19 14.3Thrombocytopenia (< 150 /mm3) 32.9Thrombocytopenia (< 100 000/mm3) 24.9Paresis 0.9Intracerebral haemorrhage 2.2 0.9pneumothorax 0.9
103

ECLAMPSIA AT TYGERBERG HOSPITAL
J Pretorius, H Odendaal, D GrovèDepartment of Obstetrics and Gynaecology, Tygerberg Hospital, MRC Unit for Perinatal Mortality, University of Stellenbosch
Eclampsia is a serious obstetric complication associated with increased maternal and perinatal mortality and morbidity.According to the Third Interim Report on Confidential Enquiries into Maternal Deaths in South Africa, complications of hypertension in pregnancy are the most common primary direct cause of maternal death.During the past seven years, 270 cases of eclampsia have been managed at Tygerberg Hospital (TBH), a tertiary referral obstetric unit. The objective of our study was to establish a profile of the eclamptic patient and to measure the impact of eclamptic convulsions have on maternal morbidity and mortality as well as perinatal mortality at TBH.A retrospective, descriptive study was performed between the years of 1994 and 2000.Main outcome measures included: Patient demographics, manner of presentation, management, mode of delivery and maternal and perinatal complications.Eclampsia is defined as the onset of generalized convulsions during pregnancy or postpartum in a patient who has signs and symptoms of pre-eclampsia. Eighteen patients were excluded from our study (n=18), these were patients with a history of epilepsy or previous non-eclamptic seizures, current seizures attributable to other causes (for example, meningitis) and patients without a definite diagnosis of eclampsia. Patients who had attended antenatal clinics on two or more occasions were considered booked.
ResultsThe incidence of eclamptic convulsions at TBH is difficult to estimate as it is a referral hospital and cases are managed from local as well as peripheral units.
104
Patient DemographicsThe youngest patient with eclampsia was 13 years and the oldest 42 years (mean 22.6 years). One hundred and seventy eight (65.9%) were primigravid.Two hundred and five patients were considered booked and had some form of antenatal care. Sixty-five (24.1%) of patients were, therefore, unbooked. In 261 patients where gestational age could be estimated: the mean gestational age at occurrence of eclamptic convulsions was 33.3 weeks (range 20-43 weeks). One hundred and forty four (53.3%) of patients had their first eclamptic convulsion outside of a recognised medical institution. Convulsions occurred before delivery in 74.1% (200) of cases and postpartum in 14.4% (39) of cases. The blood pressure range at admission to TBH recorded therefore just before, during or soon after seizure was 100-230mmHg systolic and the diastolic range was 60-180mmHg. In general terms management of eclampsia at TBH aims to:Control and prevent further convulsions (With MgSO4 as recommended by Pritchard, this intramuscular regime is most commonly used. Of note, we wish to emphasize that patients are not given diazepam)
Stabilize the patient. (With special emphasis on blood pressure control)
Investigate for complications of eclampsia.Assess route of delivery and begin to effect delivery.
(Blood pressure control previously with IV dihydrallazine or currently oral nifedipine – diuretics and invasive haemodynamic monitoring are not used and CT scans, LP’s only if indicated. Oliguria is managed conservatively).
Method of DeliveryFifty-nine patients were in spontaneous labour. One hundred and sixty one patients were induced and 50 patients did not labour including one infant that was not delivered, as it was an intrauterine death to a patient who had died. If one excluded cases of eclampsia that occurred postpartum and therefore unlikely to influence the mode of delivery, the
105
caesarean section rate of the patients with eclampsia was 47.6%. This compared favourably to a background caesarean rate of 55.5% for severe pre-eclampsia at TBH (Hall et al). The most common indication for caesarean section in all cases was fetal distress. Women who were induced delivered vaginally in 64% of cases.Of the 209 patients monitored (excluding intrauterine deaths, non-viable pregnancies and postpartum eclampsia): forty-two fetuses (20.1%) had fetal distress on first monitoring.
Major Maternal ComplicationsComplications of eclampsia included:
HELLP syndrome that occurred in 30.5% (80) of cases.Abruptio placentae in 20.9% (53).Admission to Intensive Care Unit 6.3% (17).Acute renal failure requiring dialysis 1.5% (4).Maternal death 1.9% (5).Intracerebral haemorrhage 0.7% (2).
On discharge the blood pressure range was 90-180mmHg systolic and 40-110mmHg diastolic. Most patients were sent home on some form of anti-hypertensive therapy.
Perinatal OutcomeOf the 270 pregnancies, nine were twin pregnancies.
Outcome:Alive and well 215Miscarriages 6Termination of pregnancy (Non-viable pregnancy) 19Intrauterine death 22Neonatal death 17TOTAL 279
Perinatal mortality rate for eclampsia at TBH of 139.7/1000 deliveries.Sixty-four infants were adjudged to be light for gestational age (26.3%).
106

Forty-five infants had an Apgar score of <7 at five minutes that accounted for 11 of the 17 neonatal deaths.Further AnalysisAntenatal CareOf note in the unbooked patient, the eclamptic convulsion occurred at an earlier gestation of 30.7 weeks, which was statistically significant compared to the other groups.These patients also had a higher incidence of abruptio placentae and both unbooked patients and those referred from other institutions had a higher incidence of HELLP syndrome. The offspring to unbooked patients were lighter with a mean birth mass of 1686.7gms. They also had a statistically significant poorer perinatal outcome when compared to patients booked at TBH with a typical odds ratio of 3.45 (1.07-11.77) and when compared to other booked patients an odds ratio of 2.42 (1.2-4.8).
Occurrence of ConvulsionIn our study antepartum convulsions were associated with an increased incidence of abruptio placentae when compared to postpartum cases and an increased incidence of HELLP syndrome compared to intrapartum cases. All the maternal deaths were patients who had antepartum convulsions. The perinatal outcome was also significantly worse in this group of patients. Intrapartum patients seemed to have a relatively benign course, as there was a statistically significant decrease in the complications of eclampsia (except HELLP syndrome) as well as no perinatal losses.
Abruptio PlacentaeIn the cases complicated by abruptio placentae it was noted that the eclamptic convulsion occurred at an earlier gestation. More patients were delivered abdominally.They were associated with a statistically significant higher incidence of HELLP syndrome.
107

Neonatally they were of a lighter birth mass and the perinatal outcome was significantly poorer with 11 IUDs and 5 NNDS in this group a typical odds ratio of 2.7 (1.33-5.48) for a risk of a poor outcome. Perinatal mortality rate for abruptio placentae complicating eclampsia was 313.7/1000 deliveries.
DiscussionIn our study it was evident that unbooked status and antepartum eclampsia were the most important risk factors for developing complicated eclampsia.Maternal mortality rate at our institution is low and compares to large units in the developed world.
ConclusionsEclampsia remains a significant complication of pregnancy that carries high maternal and perinatal complication rates.However, once eclampsia does occur, proper hospital care can nevertheless give a very good maternal outcome.
108

MATERNAL OUTCOME SIX YEARS AFTER PRESENTING WITH MILD TO MODERATE MID-TRIMESTER HYPERTENSION DURING PREGNANCY.
DW Steyn, HJ OdendaalDepartment of Obstetrics and Gynaecology, Tygerberg Hospital and the University of Stellenbosch and the MRC Unit for Perinatal Mortality, Tygerberg, South Africa
Researchers in developing countries have concentrated on improving pregnancy outcome when studying hypertension during pregnancy. The long-term outcome of women who had previously presented with mild to moderate mid-trimester hypertension (MMMHT) has not been documented in an African population.
Patients and methodsWe attempted to contact 138 women who participated in a randomised controlled trial for women with MMMHT six years after delivery. The basic requirement to qualify for that study was a diastolic blood pressure persistently between 80 and 109mmHg before 20 weeks’ gestation. During the present study, participants were requested to come to the hospital. During the visit, a systematic medical history was obtained, a clinical examination performed and selected laboratory tests were done. The maternal blood pressure was measured every 30 minutes in the left arm with the Spacelabs 90207 monitor for 6 hours using an appropriately sized cuff. The mean diastolic blood pressure was calculated as the sum of all the successful measurements divided by the number of measurements. We required at least 8 (67%) successful measurements before considering the recording as adequate. The main measure of outcome was hypertension, defined as either a mean diastolic blood pressure of 90mmHg over the 6 hour period, or the need to use antihypertensive therapy.
A specific routine was followed to locate the women. These included obtaining the last known address from the hospital computer system,
109

phoning as many as three times where applicable and sending two letters. If unsuccessful, the nearest clinics and schools were phoned. Women who attended were also asked if they had contact with any other participants. If still unsuccessful, a research sister visited the last known address.
ResultsWe got information from 125 mothers (91%); the remaining 13 could not be traced. Seven women elected not to participate in the study, most commonly citing their good health as reason, while four women did not turn up for their appointments repeatedly. Three women have died due to a cerebrovascular accident (CVA), tuberculosis and breast cancer respectively.
Of the 111 (82%) survivors eventually seen, 52 (47%) were using antihypertensive medication. A further four women had previously used medication, but stopped it of their own accord (Table 1).
Table 1 Known medical problems according to whether women used antihypertensive therapy at the time of the visit to hospital.
Medical problem Antihypertensive therapy
No antihypertensive therapy
Hypertension alone 40 4Diabetes mellitus 9 0Asthma 2 1Pulmonary tuberculosis
0 2
Cardiac valve replacement
0 1
Renal stone 1 0“Spastic colon” 0 2None 0 49TOTAL 52 59
110

Twenty six women (23% of the total) not on therapy had mean diastolic blood pressure values above 90mmHg. Blood pressure control was inadequate in 23 (44%) mothers receiving antihypertensive medication (Table 2).
111

Table 2 Distribution of mean diastolic blood pressure values as determined by Spacelabs monitor over six hours
Mean diastolic blood pressure over six hours< 90 mm Hg 90 – 109.9 mm
Hg 10 mm Hg
Using antihypertensive therapy
29 20 3
Not using antihypertensive therapy
33 24 2
Thirty-two women had 41 further pregnancies since the initial study. Twenty-four (84%) of these women had 31 (76%) complicated pregnancies (Table 3). Thirty babies were born alive and one woman was still pregnant at the time we saw her. Two of the stillbirths occurred in association with abruptio placentae, while the third was due to severe placental insufficiency in a patient with early onset pre-eclampsia. Two of the miscarriages occurred during midtrimester at other institutions. The exact circumstances are unknown. The two cases of preterm labour occurred at 28 and 30 weeks’ gestation respectively, the former resulting in an early neonatal death due to severe prematurity. The two babies with congenital abnormalities were born to the same mother.
Table 3 Complications occurring in pregnancies subsequent to the initial study
ComplicationComplication NStillbirths 3Neonatal deaths 1Miscarriages 6Hypertension during pregnancy 19Pre-eclampsia 4Abruptio placentae 3Congenital abnormalities 2Spontaneous preterm labour 2Venous thrombo-embolism 1
112

Eight women had creatinine clearance values <70 ml/min repeatedly. They were referred to the Nephrology department for further follow-up. E Coli was cultured from the urine of 13 asymptomatic women. The mean body mass index (BMI) was 0.33, with 89 (80%) values above 0.27. There was a significant inverse relationship between BMI and diastolic blood pressure. (r=-0.29, p=0.03).
Conclusions
There is a high incidence of hypertension amongst women with a history of previous MMMHT when followed up six years later. These women have a high BMI, but a direct link with hypertension seems unlikely. It was difficult to locate many of the women.
113

THE SPEED AND APPROPRIATENESS OF OBSTETRIC REFERRALS FROM A PHC FACILITY TO A SECONDARY HOSPITAL IN BLOEMFONTEIN
RG Thudhope, WJ SteinbergDepartment of Family Medicine, UFS
IntroductionDuring the process of devolution of maternity services to the Primary Health Care in the Bloemfontein region, the question arose how effective and appropriate the referrals from the PHC facilities to the secondary level hospital were. It seemed that much conflict and allegations between nursing and ambulance personnel could have been prevented if the greater picture was given and each facility understood their part in the service delivery. This would also enhance the function of the maternity service for the entire district. Questions that needed to be answered were: a) Are the referrals appropriate?b) Are the referrals managed efficiently?c) Are there unnecessary delays?
Objectives of the studya) To describe reasons for referral and compare with treatment received
in receiving institution.b) To evaluate the time-lapse on transfer of a patient.
MethodA cohort of obstetric patients referred from the newly established National District Hospital maternity ward to the secondary level Pelonomi Hospital in Bloemfontein in August 2001 was followed up with respect to the speed and appropriateness of referrals. The level one facility is a newly established labour ward within a district hospital in a city setting, with secondary and tertiary services close by. This hospital does not yet provide emergency caesearian section facilities and refers mothers to the secondary facility for this operation.
114

ResultsOf the 42 mothers referred in August 2001, half (21/42) were referred for poor progress of labour, mostly caused by cephalo-pelvic disproportion (CPD). Other reasons included prolonged rupture of membranes (3/42), hypertensive proteinuria (3/42), pre-term labour (3/42), abruptio placentae, abnormal positions and a vaginal band. Of all patients referred, 62 % (26/42) had a caesarean section in the receiving hospital. See Table 1 in Appendix A.
There are two transport services that are used when referring patients from one to the other facility. The Emergency Medical Services (EMS) service is called when it is thought that there is an emergency, whereas the inter-hospital transport (IHT) is called for the more “routine” yet urgent referrals.
Inter-Hospital Transport (IHT) (n=16)30 of the patients were transported by IHT with 16 (53%) of the cases providing sufficient data. The average response time for IHT was 37 minutes.The average transfer time was 26 minutes. The average call to drop-off time was 64 minutes (Range 25 min – 115 min).
EMS –Emergency Medical Services (n=11)12 of the patients were transported by EMS and 11 (92%) provided adequate data to be included in the study. The average response time was 44 minutesThe average transport time was 30 minutesThe average call to drop-off time was 75 minutes (Range 42 min – 124 min
Combined referral times of those with sufficient data (n=28)The average response time of the ambulance services was 40 minutes.
115
Results showed the average transport time to be 30 minutes.The average call to drop off time was 72 minutes.
The average time from requesting an ambulance until the patient was picked up was 40 minutes. The average time from requesting an ambulance until the patient was delivered to the receiving hospital was 72 minutes.
The average time taken from referral (requesting an ambulance) until delivery by caesarean section was 351 minutes (5hr 51) (range 30 mins – 14hr 35), although the time of requesting an ambulance to the time of drop off at the receiving hospital of these patients was 85 minutes (1hr 25).
The times of those three patients send for foetal distress, the average response time measured 45 minutes. The referral to birth time of these patients was 3 hours and 30 minutes (range: 2hr 25–7hr). Two patients had a caesarean section whereas one ended in a vaginal delivery.
DiscussionAnalyzing the reasons for referral, it seems that the criteria of the maternal guidelines (1) are adhered to the referrals seem appropriate for the setting. This cohort does compare similarly with the referrals of other months. The time lapse on referral of these patients is disturbingly protracted, but compares with previous studies. (2) The distance between the 2 hospitals is 6.5km and takes 15 minutes to travel on a normal weekday. The fact that the EMS services took a little longer then the IHT for this travel may have to do with the fact they complete more paperwork as part of transport.
ConclusionThe reasons for referral were found to be in line with suggested referral criteria and seem appropriate for the setting. Poor progress of labour was
116

the commonest reason for referral. Foetal distress was not a common reason for referral.The average referral time has been established as 72 minutes. Delay in the management of patients requiring caesarean section at the receiving hospital has been identified. Mechanisms to shorten this time should be sought.
Table 1 Reasons for referrals and types of management August 2001
Reason referred National Hosp.
ManagementPelonomi Hosp.
Reason ReferredNational Hosp
ManagementPelonomi Hosp
1 Fetal distress NVD 21 Fetal distress C/sect for CPD, FD
2 CPD(Poor progress)
C/sect for CPD 22 Prolonged latent phase
C/sect for CPD
3 CPD (Breech) C/sect for CPD 23 Prolonged ROM C/sect for CPD4 CPD (Breech) C/sect for CPD 24 Placenta
abruptio IUDPl. abruptio, IUD
5 MEC + C/sect for CPD 25 Poor progress C/sect for CPD6 Poor progress C/sect for CPD 26 Cervical
dystociaC/sect for cerv. Dystocia
7 CPD (PROM) C/sect for CPD 27 PTB + 2o
infectionN.V.D
8 CPD (transverse)
C/sect for CPD 28 Pre-term labour
N.V.D.
9 Prolonged 1st
stageC/sect for CPD 29 CPD C/sect for CPD
10 CPD (Prolonged) C/sect for FD 30 PET IUD 5 / 9 / 200111 PET, poor
progressC/sect for CPD 31 CPD C/sect for CPD
12 Poor progress C/sect for CPD 32 CPD C/sect for CPD13 PET N.V.D. 33 Ruptured
ectopicRemoval of ectopic
14 Prolonged ROM N.V.D. 34 CPD C/sect for CPD15 Poor progress.
PROMC/sect for CPD 35 Bartholians
cystCyst drainage
16 CPD C/sect for CPD 36 Pre-term labour
N.V.D
17 Fetal distress C/sect for FD 37 Vaginal band C/sect for CPD18 Obstructed
labourVacuum. PME 38 IUGR N.V.D
19 CPD C/sect for CPD 39 CPD C/sect for CPD20 CPD NVD
117

TRANSPORT FOR WOMEN IN LABOUR IN SOWETO T Mokaya, E J BuchmannDepartment of Obstetrics and Gynaecology, Chris Hani Baragwanath Hospital
The reduction in maternal and neonatal morbidity and mortality as a result of regionalised intensive care and tertiary centres is well established. It has also been established that the referral of patients with high-risk pregnancies to tertiary centres will further improve perinatal outcome. However, this involves transporting mothers from either health facilities or from their homes to these centres. The modes of transport currently being used for this purpose include the ambulance system, privately owned vehicles or public transport. The aims of this study were to survey the modes of transport used by mothers arriving at the maternity department of the Chris Hani Baragwanath Hospital, to determine what factors influenced their choice of transport and to develop recommendations for alternative forms, methods and preparation of transport for pregnant women in labour. MethodsThe study group of one hundred postnatal women was selected using computer generated random numbers from three different delivery points i.e. labour ward, theatre and the high care area. The proportion of women was stratified for each delivery area as determined by a previous survey that showed that 66% of women delivered in labour ward; 27% in theatre by caesarean section and 8% delivered at the high care area. Women were interviewed in a language of their choice with the help of a ward midwife after obtaining consent. The inclusion criteria were women who came to hospital or clinic in labour at term and were willing to participate. Questions were aimed at obtaining the following information: demographic data, the mode of transport used, the planned mode of transport at onset of labour for day and for night, the use of the ambulance services, the time interval between decision to go to a health facility and the time of arrival, access to a telephone and the availability
118

of a car in case of an emergency. Data from the interviews was captured on a data sheet and then analysed using Epi Info 6. Comparisons of frequencies were made with the Chi-square and Fisher’s exact tests for categorical variables, while the comparisons of means were made using the Student’s t-test. P values of less than 0.05 were considered statistically significant. ResultsOne hundred women were interviewed, the ages ranged from 16 to 47 years in the study group with a mean age of 28 years. Their parity ranged from 1 to 5 with a median of 2. Fifty-four percent of women arrived at a clinic or the hospital in the twelve-hour period between 07h00 and 19h00 while 46% arrived between 18h00 and 06h00. Seventy-two of the women were from Soweto. Forty-three percent of the women or their partners were unemployed. Nine women had no formal education, while 22 had primary school education. Fifty-seven reached high school and 12 had college or university education. Seventy-four percent lived in suburbs/townships while the rest lived in informal settlements. When asked on the type of dwelling in which they stayed, 56 lived in a brick house, 30 shack, 12 in a garage or outbuilding while 2 lived in flats. In case of an emergency that required transport to hospital, 17 had a car at home, 36 could use a neighbour’s car, 21 could use a relative's car and 26 had no access to a car. Twenty-four women had a telephone at home, 15 had access to a neighbours' telephone, 27 to a public telephone, 33 had access to a mobile telephone and 1 had no access to a telephone. Table 1 shows modes of transport used to get to clinic and to hospital. Table 1 Modes of transport from home to clinic, and from home
to hospital From home to
clinicFrom home to hospital
Total
Ambulance 0 11 11Private/own 8 19 27Private/hire 12 20 32Public transport 16 9 25Walk 4 1 5
119

When asked what mode of transport they had planned to use to go to clinic/hospital during daytime, 13 had planned to use an ambulance, 47 planned to use private transport, 36 public transport, and 4 planned to walk. On enquiring what their night plan was, 28 planned on using the ambulance, 71 private transport while one planned to walk. No woman planned to use public transport at night.Of the 100 patients interviewed, 13 had called for an ambulance. Of the women who phoned, 9 received an immediate response, in 3 cases the response was delayed while in one, there was no response. Eighty of the women interviewed did not know the telephone number of the ambulance. On enquiring how long the ambulance took to arrive, in 1 case it arrived after 15 minutes; 3 took 30 minutes; 2 took 45 minutes, 4 took 60 minutes while 1 took 90 minutes, with a mean response time of 47.7 minutes In the instance when the ambulance was delayed, 4 explained that there were not enough ambulances, 2 could give no explanation while in 2 cases the ambulance staff could not find the home of the caller. The time from decision to go to a health facility to time of arrival ranged from 25 to 570 minutes with the distribution of the times shown in Table 2, with a mean of 142 minutes and median of 120 minutes. Of the 54 women who arrived during the day, the average time of decision to time of arrival was 165 minutes, while for those who arrived at night the mean time to get to hospital was 114 minutes (Students t-test P=0.006). Table 2 Time to get to a health facility Interval between decision time to arrival time (in minutes)
Frequency (N=100)
0—60 2761—120 26121—180 27181—240 12>240 8 Several factors were compared with the time it took to arrive at a health facility, and these are shown in Table 3. The only factors that were found to be associated with a reduced decision to arrival interval were going into
120

labour at night and having at one’s disposal a private car (P= 0.025). Other factors were not statistically significant. Table 3 Comparison of demographic factors and decision to
arrival interval Factors Time in minutes P valueBrick house vs. Informal 139: 145 NSSowetan vs. Non-Sowetan 151: 116 NSDay vs. night 114: 165 0.006Private car vs. no car 97: 151 0.025Own phone vs. no phone 144: 139 NSClinic arrival vs. hospital arrival
149: 136 NS
DiscussionThis is, to our knowledge, the first study in South Africa that has looked at the available modes of transport and their usage by pregnant women in labour. In this study, the factors that most influenced the time it took a woman to reach hospital was time of day and access to own transport. Women took a shorter time to reach hospital during the night. Some factors may account for this difference such as lower density of urban traffic at night and easy availability of own-private transport at night as household occupants would be back from their daytime work. This study has also shown, as might be expected, that women with access to a private car were able to reach hospital more quickly than women without such access. Interestingly, other demographic factors such as age, parity, educational level, and employment seemed to play no significant role in the length of time it took women to reach hospital. This study has certain limitations. It was a retrospective study and was dependent on patients’ recall of time, some of whom may not have had access to a timepiece. Secondly the study was done in a metropolitan area and therefore cannot necessarily be generalised to other areas. Considering the small number of women who used the ambulance services, there is a need to re-evaluate the role of ambulances especially in obstetric transport, or to consider the establishment of dedicated obstetric ambulances. Since only a minority of women knew the telephone number of the ambulance, there is need to have these numbers readily available, such as writing them in the antenatal cards. There is a need to
121

encourage pregnant women, especially during antenatal clinics visits, to prepare for labour, which is an area we often neglect. We need to encourage women to arrange their own private transport well in advance of labour, especially where the public ambulance system is weak.
122

THE EFFECT OF BLOOD LOSS DURING THE INTRA-PARTUM PERIOD AND THE FIRST TWENTY FOUR HOURS AFTER THE DELIVERY ON THE HAEMOGLOBIN LEVEL VALUES OF THE PATIENT
C GerberUniversity of the Free State
Anaemia is described as one of the most common medical condition during pregnancy, and a great deal of attention is devoted to the diagnosis and treatment of anaemia during the antepartum period. However, little information is available regarding the incidence and effect of anaemia during the post-partum period.
A descriptive study was used in the research project in order to gain more information regarding the effect of blood loss during the intrapartum period and the first 24 hours after the delivery on the haemoglobin level of the patient. The researcher collected information by means of data collecting forms.
The researcher included 65 respondents in the research project who were canvassed by means of a convenience selection. All respondents had to be 36 to 42 weeks pregnant, were to have vaginal deliveries and had to remain in the post-natal ward for at least 24 hours after the delivery.
Upon admission to the maternity ward, the aim and importance of the study were explained to the patient by the researcher. Respondents were required to give written permission for participation in the study. A venous blood sample was obtained from the patient prior to parturition and was analysed by the Haematology Department. This value was recorded on the data collecting form. The researcher determined the amount of blood lost by a respondent during the delivery. All visible, coagulated blood was collected from the bedclothes and weighed. The soiled cloths and swabs were also weighed and their mass was compared with the mass of a dry cloth and swab. The difference indicated the amount of blood absorbed by the cloths and swabs. The two quantities were added up and the
123

biostatistician converted the amount of blood weighed in gram to milliliters. A second blood sample was obtained from the respondent 24 hours after the delivery. The researcher completed the data collecting form during the post-partum period of the respondent.
The results of the research showed a positive correlation between the amount of blood lost by a patient during parturition and the first 24 hours afterwards, and the haemoglobin level value of the patient during the post-partum period. The incidence of anaemia during the post-partum period was notably higher in patients who had lost more than 350 ml of blood during the delivery, developed post-partum haemorrhage and experienced severe lochia. The incidence of anaemia during the post-partum period is considerably higher than is generally accepted.
Anaemia during the post-partum period is a reality that is being ignored by health workers at this stage. The checking of the haemoglobin level values of patients in the post-natal ward as a matter of routine recommended by the results of this research.
124

EFFECTIVENESS OF NEVIRAPINE DELIVERY AT CORONATION HOSPITAL: AN UPDATE .
L Thomas1, M Urban2, M Chersich11Perinatal HIV Research Unit, Chris Hani Baragwanath Hospital2Dept Paediatrics, Coronation Hospital
IntroductionCoronation Hospital has an antenatal program for HIV testing of consenting women and provision of nevirapine to HIV infected women and their infants perinatally. HIV-testing is by standard HIV ELISA and nevirapine is provided by midwives when women arrive in labour, and post-natally to the baby. A number of community antenatal clinics refer to Coronation Hospital, not all of which test for HIV.
AimTo assess the frequency of ante-natal HIV testing, and intrapartum provision of nevirapine before and after an intervention.
MethodsA record review was conducted post-delivery, before and after an intervention. Before the intervention, 299 records were reviewed in October 2000, and afterward 308 records were reviewed in March/April 2001. The intervention comprised a poster campaign and oral feedback to obstetric staff regarding missed opportunities for HIV testing and deficiencies in the system for obtaining HIV results and documentation of nevirapine treatment.
ResultsAfter the intervention HIV testing increased from 181(61%) to 217 (70%), chi square p=0.01. This represented 81% of cases with an opportunity for testing. The rates of syphilis testing by comparison were over 95% both before and after the intervention. Avoidable missed opportunities for testing were reduced from 82 (27%) to 43 (14%). The number of women documented to have received nevirapine increased from 14 (56%) to 38
125

(76%), chi square p=0.05. The number of infants documented to have received nevirapine increased from 4 (15%) to 28 (48%), chi square p=0.003.
DiscussionThe intervention improved both HIV testing and nevirapine usage. Improvements within the current system are still possible, as some avoidable missed opportunities remain for HIV testing and for giving nevirapine. It is possible that use of rapid ELISA tests and maternal self-administration of nevirapine will improve testing rates.
126

NEVIRAPINE: SHOULD IT BE SELF-ADMINISTERED OR ADMINISTERED BY HOSPITAL STAFF?
M Chersich1, L Rose2, M Urban3, G Gray11Perinatal HIV Research Unit, Chris Hani Baragwanath Hospital2Dept O&G, Coronation Hospital3Dept Paediatrics, Coronation Hospital
IntroductionThe administration of nevirapine to prevent mother-to-child transmission (MTCT) of HIV is a challenge in resource-constrained South African settings. Nevirapine (NVP) may be administered during labour by the health care worker. Alternatively, nevirapine may be given to the mother antenatally for self-administration at the onset of labour.
MethodsEffectiveness of delivery of the antenatal maternal dose of nevirapine was compared between Zola Clinic in Soweto, where nevirapine is self-administered, and Coronation Hospital, where nevirapine is administered by hospital staff. Nevirapine administration was considered adequate if it was given between one and 48 hours before delivery. The two sites are not directly comparable. Zola Clinic takes patients from a small area within Soweto, whereas Coronation Hospital receives patients from most of western Johannesburg and its surrounds.
ResultsSite n NVP
ingestedNVP adequate
Significance
NVP unknown
NVP > 1
Zola booked/birth 48 43(90%) 35(73%)
p=1.0 4(9%) 4(9%)
Coronation birth 47 39(83%) 32(68%)
p=0.6 1(2%) 0
Coronation birth (Coronation booked)
22 21(95%) 18(82%)
p=0.4 1(5%) 0
Coronation birth(Witkoppen booked)
16 11(69%) 9(56%) p=0.2 0 0
Discussion
127

There were no significant differences in frequency of adequate nevirapine uptake between the health care worker-administered and self-administered groups, although there was a trend for women booked at Witkoppen Clinic (3 taxi rides from Coronation Hospital) to have inadequate uptake. Self-administration appears to be associated with a likelihood of taking more than one dose (possible risk for viral resistance).
ConclusionBoth self-administration and health care worker-administration have problems. The method used should probably depend on local circumstances, or a combination of the two methods may be useful to increase uptake.
128

EXPANDING VOLUNTARY COUNSELLING AND TESTING (VCT) AND THE PROVISION OF INTERVENTIONS TO PREVENT VERTICAL TRANSMISSION OF HIV IN SOWETO, SOUTH AFRICA
M Chersich, A Violari, B Jivkov, B Botha, A Fiamma, JA McIntyre, GE Gray
BackgroundIn Soweto, the HIV epidemic has had a profound impact on child mortality. Prevalence rates of HIV in pregnant women have increased from 15.5% in 1996 to 29.7% in 2000, resulting in an increase in perinataly acquired HIV. In 2000, 38% of children admitted to Chris Hani Baragwanath Hospital (CHBH) were HIV positive. We commenced a programme to offer VCT and PMTCT services in October 2000 that was funded by International Therapeutic Solidarity Fund and EGPAF Call To Action. The aim of this programme was to assess the feasibility of delivering an intervention to reduce MTCT in a resource-constrained setting at a community level.
MethodsA programme was developed to train health care workers and lay counsellors on VCT and PMTCT in Soweto. These health care workers and lay counsellors were placed into CHBH and two midwifery units. This programme was then expanded to the remaining 9 midwifery units in Soweto.
ResultsIn the original three sites from January to December 2001, 13 313 women were offered pre-test counselling of which 12 200 (91.6%) accepted VCT. Of these, 12 009 (98.4%) were tested, of which 3 741 (31.2%) were HIV positive. The number of women receiving their results was 10 436 (86.9%) with 71.3% (8 560) receiving their results on the same day as testing. Nevirapine was dispensed to 2 924 (78.2%) of the HIV positive women constituting 90.8% of those who received their results.
129

ConclusionVCT and PMTCT interventions appear to be feasible and acceptable in our setting, an African township in South Africa. Further research is needed to identify reasons why women who accept VCT do not receive their test results or access Nevirapine prophylaxis. In addition, the impact of this programme on child survival in Soweto needs to be determined.
130

ATTITUDE OF MOTHERS WHO ARE HIV INFECTED TOWARDS INFANT FEEDING USING THEIR OWN PASTEURISED EXPRESSED BREAST MILK
KR Mokhondo, AE Pullen, B Jeffery, RC Pattinson, SD Delport.MRC Unit for Maternal and Infant Health Care Strategies, University of Pretoria
IntroductionBreastfeeding provides substantial benefits to both the mother and child. There is evidence that HIV is transmitted through breastfeeding in 10%-16% of infants born to mothers infected with HIV. Affordable forms of infant feeding are needed, which minimizes the risk of mother to child transmission.
One such a method is the Pretoria Pasteurisation method where mothers express and pasteurize their breastmilk for their own infant feeding. This is an inexpensive and simple technique that can be used in any domestic setting. Culture and customs in any society are important. The decision to breastfeed is affected by customs and traditions and the socio-economic vulnerability of woman in society.
AimThe aim of the study was to explore the attitudes of HIV infected mothers towards infant feeding using their own pasteurised expressed breast milk.
Research design A qualitative, descriptive and contextual was conducted.
Study populationTen women of seropositive status were recruited post-delivery including mothers of high-risk low birth weight infants.
131

Research methodIndividual interviews were held with mothers using a structured-open ended questionnaire. All interviews were taped and transcribed. Data analysis was done by means of text analyses.
ConclusionThe results of the study will be presented. During the study, five participants requested immediate assistance to start with pasteurisation of their breastmilk.
132

MTCT PROGRAMMES IN THE WESTERN CAPE
F Abdullah, NT Naledi, J Cromme, I Cupido (PAWC), E Coetzee (UCT
BackgroundThe Western Cape Province started a pilot MTCT programme in Khayelitsha in January 1999. Khayelitsha is a peri-urban, poorly resourced area approximately 30km from Cape Town. The programme is offered at two Midwife Obstetric Units (MOU’s) and eight surrounding baby clinics. This programme follows the Thai regime where HIV pregnant women are given AZT antenatally from 34 weeks gestation and also receive 3 hourly AZT during labour. The mothers are given information of the benefits and risks of breastfeeding and formula feeding and are asked to make an informed choice on a feeding method. Exclusive feeding is encouraged. Women opting to formula feed are provided free formula for 9 months. The babies are tested using rapid testing at 9 months and if positive are tested again at 18 months.
Table 1 shows that from January 1999 to December 2000 there were 14139 antenatal bookings in Khayelitsha, 71% of which accepted voluntary counselling and testing. From a record review of 962 records from this period, it was shown that 87% of women received any dose of AZT during the antenatal period or labour, 52% received at least 2 weeks of antenatal AZT and 76% received at least one dose in labour. 41% of women self administered AZT. From these results, the programme was assessed as being operationally feasible to implement at a primary level care. With the publishing of the HIVNET012 data showing the efficacy of Nevaripine in MTCT, the relative ease with which this programme could be implemented and at a cheaper price than AZT, the Province decided to roll out the programme using Nevirapine.
133

Table1 Khayelitsha MTCT results Jan 1999 – Dec 2000
Antenatal bookings 14 139 Accepted VCT 71%HIV Positive: 16% (1999)
20% (2000)Any AZT dose 87% Received ≥2 weeks supply 52%Received 4 weeks supply 25%Received at least 1 dose in labour 76% Self administered AZT 41%
The First Phase Roll-OutThe first phase roll-out started in January 2001 in Gugulethu, a poorly resourced township in Cape Town. In May 2001, the programme rolled out to Vanguard - another poorly resourced township in Cape Town, Paarl - a peri-urban/rural area and George - a rural area. In June 2001 the programme rolled out further to Worcester, another rural area. The service is also largely provided at primary level care. Gugulethu and Paarl are also two of the 18 national MTCT pilot sites for operational research.
Table 2 shows the results of the first phase roll-out from January 2001 to December 2001. During this phase roll out there were 11846 bookings, 86,4% of which accepted voluntary testing and counselling. The average HIV positivity rate at these sites was 14.6% with a range of 7.9% in Worcester to 21.3% in Gugulethu. 456 women on the programme delivered and 61.8% of whom self-administered Nevirapine and 98.7% of the babies were administered Nevirapine. All the women who had not self-administered Nevirapine received it in the labour ward. Almost 90% of the women chose formula feeding and 63.5% of the babies were compliant to formula, defined as having been dispensed 8 tins of formula per month. The vast majority of women who choose formula feeding opt for the formula provided for free.
134

First Phase Roll Out
Table 2 First Phase roll out results Jan 2001 - Dec 2001
Gugulethu
Paarl Vanguard
Worcester
George TOTAL
Total Bookings
4528 2185 2594 1069 1470 11846
Accepting VCT
81.7% 98.4%
86.2% 69.7% 91.5% 86.4%
HIV Positivity Rate
21.3% 8.4% 14.5% 7.9% 8.3% 14.6%
Deliveries 210 82 65 37 62 456Self admin NVP in labour
68.1% 57.3%
64.6% 43.2% 54.8% 61.8%
Babies admin NVP
98.6% 100% 93.9% 102.7%* 100% 98.7%
Babies Dispensed formula (postnatally)
95.2% 70.7%
100% 97.3% 82.3% 89.9%
Babies on follow up
324** 64 101** Nil 38 526**
Formula compliance^
61.1% 68.8%
64.4% Nil 71% 63.5%
* This includes babies born on arrival (BBA’s) **This includes babies from other MTCT sites in the province^Formula compliance is when the baby has been dispensed 8 tins of formula per
month.
The Weaknesses of the programme
Human resource problems such as not matching the speed of roll out with increasing staff numbers have been one the programme’s weaknesses.
Infrastructural problems have also resulted in sub-optimal space and privacy for counselling in some areas.
Inadequate psychological support for staff and mothers and inadequate support around infant feeding are also issues of concern.
The inadequate measure of outcome in terms of measuring HIV transmission rates and baby morbidity and mortality is also another weakness in the programme.
135
The Strengths of the programme The Health Park Forum
This is a strategic forum assisting the Provincial Department of Health in implementing the programme. This forum consists of Provincial, Regional, District and Local authority managers, specialists in Obstetrics & Gynaecology, Neonatology, Paediatrics and Public Health and NGO’s
Earmarked funding provided to the regions specifically for MTCT programmes.
Identifying “MTCT Champions” at district level who are service managers or district managers or district co-coordinators. These “champions” become the drivers of the programme at district level.
Real time monitoring of programme processes & outputs
ConclusionThe MTCT programme in the Western Cape has been operational since 1999. The lessons learnt at the Khayelitsha pilot programme have been used to help implement MTCT roll-out in the Province. First phase roll-out occurred from January 2001 to June 2001 and included both urban and rural sites. Second phase roll-out occurred from September 2001 to March 2002. Third phase roll-out is expected to start April 2002 to June 2002 and the last phase roll-out is expected from July 2002 to March 2003. To date the programme is offered to 60% of all women attending public sector antenatal care in the Province and we expect to have 100% roll out by March 2003.
136

THE EFFECT OF VITAMIN A ON REDUCING MOTHER-TO-CHILD TRANSMISSION OF HIV IN BLOEMFONTEIN.
P Chikobvu1, G Joubert1, R Schall6, WJ Steinberg2, JI Viljoen3, M Kotze4, J Kriel5, E van der Ryst3
Departments of 1Biostatistics, 2Obstetrics and Gynecology and Family Medicine, 3Virology, 4Haematology and Cell Biology, and 5Pediatrics and Child Health; University of the Orange Free State, 6Quintiles ClinData in Bloemfontein.
Introduction and purposePaediatric HIV infection remains a fatal disease in Africa and prevention is important. The overall mother-to-child HIV transmission has been reported to be between 20 and 40% in Africa compared to 10-20% in the USA and Europe with breast-feeding reported to contribute an additional 14%. Although it has been shown that AZT can reduce vertical transmission of HIV significantly, it is still largely unaffordable in Africa. Clinical data has shown that vitamin A deficiency is associated with increased vertical transmission of HIV in Africa. A randomized controlled trial to assess the effect of vitamin A supplementation on vertical transmission of HIV-1 was launched in 1997. This paper describes the differences in the characteristics of babies in vitamin A and placebo as well as the transmission rates.
MethodsInfants were seen at 1 month old, then 3 monthly till they were 18 months old. Condition at birth, physical examination, medical history, demographic data, infant illness and feeding methods were recorded at 1 month and follow-up visits. Blood samples were obtained at 3, 6, 12 and 18 months. Infant HIV status was determined using PCR, P-24 antigen test and confirmed by ELISA test at 18 months.
ResultsOf the 158 babies whose HIV status is known 73 were in vitamin A and 85 in placebo. The average change in baby characteristics did not differ significantly from 1 months to 18 months. Of the 104 infants whose HIV
137

status was known at 3 months, 50 were in vitamin A and 54 were in placebo group. The transmission rates at 3 months were 20% in vitamin A group and 22.2% in placebo group. At three months, 72% of patients were formula feeding their babies and this group had a transmission rate of 23%, whereas 23% of mothers were exclusively breast-feeding and had a transmission rate of 13% at three months. Only 4% of mother reported to mixed feed at three months, and this group had a transmission rate of 40%. These groups, however, were small and show wide confidence intervals and no statistically significant differences.Looking at the total transmission rates there was no significant difference between the two groups either, with transmission rates of 19.2% in the vitamin A group and 21.2% in placebo the group. Considering the mortality rate of this study sample, a perinatal mortality rate (PNMR) of 46/1000 was calculated (14/303), which is similar to that of the community these patients come from. However the infant mortality rate (IMR) of the study sample was 86/1000 (26/303) slightly higher than that of the community where these patients come from. This is the best possible scenario as some patients were lost for follow-up. All babies that have died and we have results of, were PCR positive for HIV.
ConclusionVitamin A supplementation does not reduce the transmission rates in this population. However, the transmission rate in the placebo group at 21.2% was lower than expected.
138

WHERE PARENTS PLAY A PASSIVE ROLE IN LIFE-SUPPORT DECISIONS: VLBW INFANTS AND PHYSICIAN COUNSELLING IN SOUTH AFRICA.
TM Ranchod, JC Partridge, DE Ballot, AM Martinez, VA DaviesPediatrics, University of California, San Francisco, CA; Paediatrics, Univ. of Witwatersrand, Johannesburg, South Africa.
BackgroundEconomic realities may restrict treatment options for premature infants born in developing countries with available intensive care technology.
ObjectivesTo characterize physician counselling and parental decision-making roles for very low birthweight (VLBW) infants <1501g in South Africa.
MethodsWe interviewed 51 parents whose VLBW infants received care in 3 university hospitals providing tertiary care for urban, low socioeconomic patients in South Africa. After nursery discharge, parents were interviewed using a structured standardized questionnaire (translated by NICU nurses as needed).
ResultsAt birth, the infants were 1163g (+ 187) BW and 30 (+ 2) wks GA (median). Mothers had a mean age of 27.9 (+ 6.3) yrs. Parents recalled that physicians infrequently discussed overall survival (39%) or options for withholding life support (20%); <50% of parents believed physicians adequately discussed disability, pain, finances, religion, or family wishes. Parents (75%) reported understanding treatment plans after counselling; nurses were more often perceived helpful in communications than were physicians (47% vs 37%). After counselling, two-thirds of parents feared death in the nursery; 26% still feared death after hospital discharge. Few factors affected life-support (LS) decisions: only pain and physician recommendations affected decisions for >50% of parents. Most parents
139
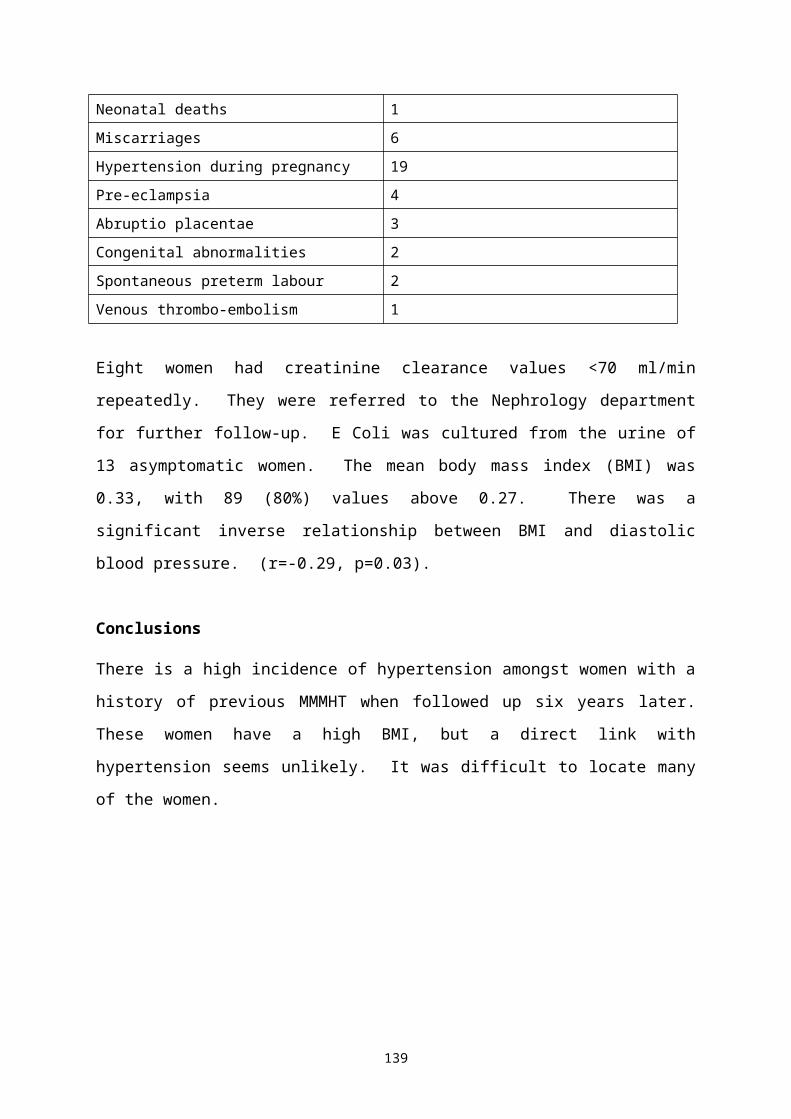
(45/51) agreed with physician recommendations. Joint decision-making between parents and physicians was uncommon: 14% before and after birth; 59% of parents stated that physicians had played primary roles in LS decisions. Asked the optimal process for LS decisions, 49% of parents preferred joint decision-making, while 45% stated physicians should still play the dominant role. Fifty seven percent of parents of surviving infants felt satisfied with communications and NICU care.
ConclusionsIn South African hospitals, where limited resources restrict availability of treatment,, physicians may incompletely inform parents of VLBW infants. Incomplete disclosure of care options may stem from time constraints, language barriers, or physician judgements that some options are too costly for infants at high risk of death or severe sequelae. Limited by poverty, educational disadvantage, or cultural disparities, some mothers may cede decision-making capacity to physicians.
140

CASE REPORT AND LITERATURE REVIEW: FOETAL AKINESIA SEQUENCE DUE TO IN-UTERO SUBDURAL HAEMORRHAGE.
I Erasmus1, K Bolton2, J de Souza1, M. Urban21Dept Obstetrics, Coronation Hospital2Dept Paediatrics, Coronation Hospital
BackgroundFoetal akinesia sequence comprises multiple joint contractures (arthrogryposis multiplex congenita) and pulmonary hypoplasia due to prolonged foetal immobility. This sequence of deformations may occur secondary to physical constraint or foetal neuro-muscular disorder.
Case reportA 24 year old primiparous woman had a normal clinical and ultrasound examination at 26 weeks gestation. On repeat abdominal ultrasound examination at 32 weeks gestation, a notable increase in liquor volume was detected. A foetal anomaly scan showed a large subdural haemorrhage, fixed flexion deformities of both hands and a protuberant tongue with poor sucking movements. On questioning, the mother gave a history of a fall two weeks previously, followed by decreased foetal movements. The baby was born at 37 weeks gestation with a birth weight of 2390g and head circumference of 33cm. The baby was in severe respiratory distress and had a small chest. Other features were: “floppy” baby with absent moro and suck reflexes, poor bulk of limb and abdominal wall muscles, undescended testes and bilateral recent humeral fractures. Head ultrasound showed no obvious evidence of the subdural haemorrhage. It was decided not to ventilate the baby, and the baby died two hours after birth. Post-mortem examination confirmed a subdural haemorrhage and bilateral pulmonary hypoplasia.
DiscussionA case of subdural haemorrhage at approximately 30 weeks of gestation, causing foetal akinesia sequence with pulmonary hypoplasia, is described.
141
The subdural haemorrhage was “occult” at birth. A literature review on foetal akinesia will be presented.
142

SCREENING TOOLS FOR FETAL ALCOHOL SYNDROME IN THE EVALUATION OF COMMUNITIES AT HIGH RISK
D ViljoenNational Health Laboratory Service (NHLS) and Faculty of Health Sciences, University of the Witwatersrand
IntroductionFetal alcohol syndrome (FAS) is the most common preventable cause of mental retardation worldwide. In certain underprivileged communities in the Western Cape, Gauteng and Northern Cape Provinces, the prevalence amongst grade I school-entry children is the highest reported anywhere in the world. Due to the lack of biomedical markers, the diagnosis of FAS can only be achieved by a combination of clinical evaluation, maternal history of alcohol-abuse during pregnancy and neurodevelopmental testing of the child. The current epidemiological evaluation of communities at-risk for FAS are dependent on these costly ascertainment procedures. Screening modalities for the ascertainment of FAS amongst school children are therefore, urgently required.
MethodsSeveral methods have been developed during the past 5 years of screening for FAS in order to minimise cost and time in the evaluations of at-risk communities. These include :-(a) At-risk anthropometric screening measurements for grade 1 school children.(b) A stereo–photogrammetric method to measure the facial dysmorphology.(c) Use of “weighted” scores for dysmorphological features.(d) Use of “weighted” scores for neurodevelopmental testing.(e) Use of a shortened maternal questionnaire for ascertaining alcohol abuse.
143

ResultsThe use of these modalities have high specificity and sensitivity in the clinical diagnosis of FAS in school-entry children. The findings of epidemiological studies amongst communities in the Western Cape, Gauteng and Northern Cape Provinces using these methods will be discussed.ConclusionsThe costs and labour involved in the epidemiological appraisal of large communities can be reduced to approximately 25 percent with marginal loss of accuracy in the ascertainment of FAS using these methods. They will form the basis of future surveillance of trends in FAS prevalence in high-risk populations.
144

THE CONTINUED BURDEN OF POVERTY: DOES NICU CARE MAKE A DIFFERENCE
C H PieperNeonatal Service, Tygerberg Children’s Hospital, University of Stellenbosch.
IntroductionCertain factors associated with the birth of premature babies have been associated with poor outcome. The birthweight and gestational age of the baby are time-honored examples where there is a direct correlation between increased mortality with increasing lower birthweight or gestational age.
AimThe aim of this study was to determine other factors which may influence the outcome as measured by mortality.
SettingA prospective study was done on all admissions to the Tygerberg NICU during 1992 to 1996. All babies weighing less than 1500 grams or less than 33 weeks gestational age were studied.
ResultsDuring this period 455 babies were admitted, of whom 116 died (26%).Means All
(n=455)Survivors (n=336)
Non-survivors (n=119)
Birth-weight ( grams) 1198 1229 1129Gestational age ( weeks) 30.3 30.4 29.9Age of mother ( years) 27 27 27.2Income 892 958 706IPPV duration 8.5 8 9.8Days oxygen 20.9 21.3 19.8Apgar 1 min 5 5 4.9Apgar 5 min 7.2 7.2 7.1p<0.05
145

Family incomes (mean) :Income per month (Rands)
All Survivors Non-survivors
%
Nil 124 92 32 261-500 107 76 31 29501-1500 140 97 43 31>1500 82 69 13 13Total 453* 334 119 100* 2 excluded
Income (mean) per racial group and sexIncome ( Rands)*
Survivor Non-survivors %
Black (n=48) 441 (n=31) 637 (n=17) 35Mixed (n=382) 901 (n=288) 634 (n=96) 25White (n=23) 2869 (n=17) 2047 (n=6) 26Male 1086 (n=166) 630 (n=72) 30Female 833 (n=170) 821 (n=47) 21
Discussion:In this study, the income of the family correlated with outcome, except in black families. The difference seems to matter more in males, who also have a much higher chance of death because of their sex. NICU care does not seem to make a difference. The reasons may be poor nutrition, less care or later admission warranting a further study.
146

EARLY-ONSET SEPSIS IN VERY LOW BIRTH WEIGHT INFANTS: HERE COME THE GRAM NEGATIVES?
SC Velaphi, JD Siegel, NB Cushion, PJ SanchezUniversity of Texas, Southwestern Med. Center, Dallas, TX
IntroductionThe Centers for Disease Control and Prevention (CDC) in 1996 published consensus guidelines for prevention of perinatal GBS disease that recommended a risk-based or screening-based approach to identify women for intrapartum chemoprophylaxis. Implementation of these guidelines has led to 65% reduction in early-onset sepsis due to GBS. It also has been associated with a reduction in early-onset sepsis (EOS) due to pathogens other than GBS. However, in preterm infants, concern exists with regard to a possible increase in EOS due to Gram-negative bacteria especially ampicillin-resistant Gram-negatives including E. coli. In January 1995 and continuing to date (2001), a combined obstetric (risk-based approach: intrapartum ampicillin given to mothers with risk factors) and neonatal protocol for prevention of early-onset GBS disease has been implemented at Parkland Memorial Hospital (PMH), Dallas, USA. The paediatric component consists of a single intramuscular dose of penicillin administered within one hour of birth to all infants with no signs suggestive of infection.
ObjectivesThe objectives of this study were to compare the rates of EOS due to GBS, Gram- negative bacteria and ampicillin-resistant bacteria in very low birth weight (VLBW) infants before and after implementation of this combined (obstetric and neonatal) GBS chemoprophylaxis strategy.
Methods Infants with EOS were identified by active laboratory-based surveillance at PMH from 1987 to 1999. Maternal and infant medical records were reviewed and a case was defined by the isolation of a bacterial pathogen from blood or cerebrospinal fluid in the first 3 days of age. Ampicillin
147
resistance was defined using organism-specific minimal inhibitory concentrations. EOS rates were compared between the period from 1987 to 1994 when no chemoprophylaxis was provided, to the period from 1995 to 1999 when the combined obstetric and neonatal GBS chemoprophylaxis strategy was in place.
ResultsThe rate of EOS due to GBS was significantly reduced after the implementation of the combined GBS chemoprophylaxis strategy but the rates of EOS due to other Gram-positive organisms, Gram-negative organisms and E. coli specifically did not change significantly between the two periods (Table). There were no significant differences in the rate of early-onset sepsis due to ampicillin resistant Gram-negative organisms and ampicillin-resistant E. coli. The case fatality rates for GBS, Gram-negative organisms and E. coli were significantly reduced after the implementation of our GBS chemoprophylaxis strategy.
ConclusionA combined obstetric and neonatal GBS chemoprophylaxis strategy significantly reduced the rates of GBS infection in VLBW infants. The rates of EOS due to Gram-negative organisms, ampicillin-resistant Gram-negative organisms, E. coli and ampicillin-resistant E. coli did not change significantly in VLBW infants after implementation of GBS prophylaxis. Implementation of our combined GBS chemoprophylaxis strategy was associated with significant reduction in case-fatality rates of GBS, Gram-negative bacteria and E. coli. And finally continued surveillance for changes in both the etiologic agents of neonatal sepsis and antibiotic resistance remains an important component of a GBS prophylaxis strategy.
148

Table 1 Number of deliveries, VLBW infants and rates of early-onset sepsis due to Gram positive and Gram negative organisms.
1987-1994No Prophylaxis
1994-1999Prophylaxis
P-value
Number of livebirths 117 478 67 869Number of VLBW infants 1923 (1.6%) 973 (1.4%)EOS in VLBW infants due to:- Group B Streptococcus
(GBS)- Other Gram Positive
Bacteria- All Gram Negative
Bacteria- E. coli
EOS in VLBW infants due to Ampicillin resistant organisms:- Gram negative bacteria
(All)- E. coli
23 (12.0)*8 ( 4.2)11 ( 5.7)2 ( 1.0)
4 (2.1) 1 (0.5)
2 (2.1)07 (7.2) 3 (3.1)
4 (4.1) 1 (1.0)
0.010.100.820.43
0.54 0.80
* - Numbers in parenthesis are rates per 1000 livebirths
149

GROWTH AND METABOLISM OF INFANTS FED AN ACIDIFIED FORMULA WITH OR WITHOUT PROBIOTICS
PA Cooper, KD Bolton, M Urban, M Mokhachane.Department of Paediatrics, University of the Witwatersrand, Johannesburg, South Africa.
ObjectivesWhere socio-economic conditions permit, formula feeding is the preferred method for HIV positive mothers. The development of a formula which will provide good nutrition coupled with the potential for limiting infections was the rationale for the current study. Acidified formulas have been shown to inhibit bacterial growth in vitro, while addition of probiotics to formulas will result in colonization of the infant’s gastrointestinal tract with lactobacilli. Both of these modifications to infant formulas therefore have the potential to reduce the number of gastrointestinal infections.
Methods:A randomised, double-blind trial of 3 infant formulas (whey adapted starter formula (WASF), biological acidified WASF, and biological acidified WASF with probiotics [Lactobacillus bifidis]) was performed on a cohort of 131 infants born to HIV positive mothers in 3 teaching hospitals sites. Mothers had opted for formula feeding antenatally prior to recruitment. Subjects were normal term infants of birth weight > 2500g and exclusively formula fed. Exclusions were for major illness or congenital anomaly. Babies were followed for 6 months (4 months to be exclusive formula feeding) and evaluated for growth, gastro-intestinal and other potential side effects, infections and HIV transmission which was evaluated by PCR testing at 6 weeks and 6 months of age. Groups were analysed for growth using z-scores according to Eurogrowth standards and by Chi-square test for tolerance and side effects.
Results:There were 33 drop outs of 131 enrolled babies leaving 98 for analysis. 4/45 (8.8%) infants who received Nevirapine vs 13/63 (20.6%) were
150

subsequently shown to have became infected with HIV. Where infant HIV status was known, the drop-out rate was much higher in those babies who became positive (50% vs 15%). Anthropometric data from the HIV negative group showed normal growth parameters for all three formulas with the acidified formula groups showing significantly greater weight gain than the non-acidified group. The weight for age Z scores are shown below.
Severe adverse effects occurred in 9/93 (9.7%) HIV negative vs 5/17 (29%) of HIV positive infants. None of these adverse effects was attributed to the milk formula. There were no differences in gastro-intestinal symptoms between the 3 formulas. It was also noted that the mothers in the study developed a group identity which resulted in greater self confidence and significant personal growth due to the informal support systems that developed within groups of mothers in the study. Some subsequently found employment and/or became HIV/AIDS counsellors themselves
DiscussionInfants born to HIV positive mothers fed exclusively on acidified whey adapted formulas, with or without added probiotics results in excellent
151

growth which was significantly greater than those fed non-acidified whey-adapted formula. The reasons for the increased weight gain in the acidified formula groups were not clear, but results of the biochemical monitoring of these infants are still awaited. Their rates of growth were similar to Eurogrowth standards and, under the conditions of a study such as this, were able to be formula fed safely. No differences in the number of adverse events and gastrointestinal infections could be demonstrated, but it is likely that a study involving much larger numbers would be required to show this.
152

PERINATAL COUNSELLING AND LIFE-SUPPORT DECISIONS FOR EXTREMELY PREMATURE INFANTS IN SOUTH AFRICA.
TM Ranchod, JC Partridge, BJ Cory, VA Davies, DE Ballot AM MartinezPediatrics, University of California, San Francisco, CA; and Paediatrics, University of Witwatersrand, Johannesburg, South Africa.
BackgroundObjectiveTo characterize counselling and life-sustaining treatments (LSMT) where economic restrict neonatal intensive care for extremely premature infants. Cultural, educational and demographic variables affect physician attitudes about limiting the use of life-support for premature infants with poor prognoses. We characterised demographic correlates of physician attitudes on limiting life-support in South Africa, where access to health care differs between private and public sectors.
Design/MethodsIn August 2001, we mailed surveys to 394 pediatricians in South Africa, asking parent counselling practices, resuscitation thresholds, limits to use of LSMT, type of medical practice, and demographics.
ResultsWe report 93 surveys analysed (response rate 24%). Physicians were mostly male (71%), 46 yrs old and 15 yrs in practice (means); 68% were Christian, 42% trained in neonatology, 20% worked in state hospitals. Frequency of antenatal counselling increases at higher gestational ages [GA] (7% at 23 wks to 23% at 30 wks). In counselling parents of fetuses <800gm or <26 wks, most physicians discuss morbidity and mortality (97%, 93%); 67% discuss death despite resuscitation, and 55% discuss limiting LSMT. Expected outcome affect LSMT decisions: anomalies (95% of physicians), mortality (82%), and quality of life (68%). Physicians less commonly consider parents’ wishes (38%) and resources (40%), cost of care (33%), or pain (25%). Proportions believing parents should have a role in non-resuscitation decisions decreased from 76% at 23 wks to 33%
153

at 30wks. Some physicians exclude parents from LSMT decisions fearing that parents might change their minds or fail to understand options (57% and 54%, respectively). Resuscitation thresholds range for 400-1200gm and 20-30 wks. Mean birthweight thresholds vary by LSMT: intubation (665gm), cardiac massage (678gm), and drug resuscitation (661gm) [+185 gm]. GA thresholds also vary little: intubation (25 0/7 wks, cardiac massage (25 3/7 wks), and drug resuscitation (25 3/7 wks) [+13d, SD]. 68% of physicians agree with state-hospital practice of not instituting mechanical ventilation for infants <1000 gm if facilities are limited.
ConclusionsIn South Africa, variations in resuscitation thresholds reflect disparities in available technology and economic resources. Physicians choose to restrict LSMT to infants with higher GA and BW who are more likely to survive. Consideration of parent preferences is less relevant where economics constrain care options.
154

HEALTHY BABY COMPETITION
D Tsotetsi
Aims1. To implement MBFHI as national objective.2. To promote breastfeeding in reducing IMR.3. To encourage bonding between mother and baby.4. To empower mothers re-care of their babies which will assist to
reduce malnutrition in children under five years.5. To stimulate community participation and encourage parents
responsibility on health issues e.g. RTH programme.
Activities1. Pilot study was conducted at Sedibeng region in 1998; 310 clinics
were selected as pilot sites including Local and Provincial clinics as well as Rural Mobile points.
2. Due to recommendation after evaluation by Healthy Baby competition committee, the resolution was taken to continue the project yearly until 2001.
3. The above mentioned committee was to perform the following duties: Arrangements for mini and final Healthy Baby competition; Coordinate and facilitate the event; Allocate and control budgets; Set standards and conduct the project; Set standards, monitor and evaluate the programme; Review and give recommendations.
Outcomei. increased utilization of well baby clinics;ii. reduction of referral cases to hospitalization;iii. improvement of RTH card-carrying – produced at clinic when in
need;
155

iv. improved breastfeeding skills among mothers;v. reduced malnutrition in children;vi. eradication of common conditions among children e.g. diarrhoea.
ConclusionIn conclusion, we would like to expand our project to other conuntries on how we manage to motivate mothers, parents, families, community and other health workers in maintaining a healthy baby to reduce infant mortality rate, especially from birth to 2 years.
156
TOWARDS HUMANISATION OF CHILDBIRTH AT LOWER UMFOLOZI DISTRICT WAR MEMORIAL HOSPITAL: CREATING A VISION FOR CHANGE.
D Nyasulu, KwaZulu Natal MCWH SubdirectorateF Ndlovu & Midwives at Lower Umfolozi District War Memorial Hospital
Humanised maternity care has become the key focus in recent times. The KZN MCWH Sub directorate has identified evidence-based midwifery care as a priority and has taken a firm stand in promoting Better Birth Practices including – Kangaroo Mother Care; social support in pregnancy and childbirth, childbirth education, and ongoing perinatal reviewHumanised maternity care seeks to accomplish three things, viz: - providing women centred maternity care;- ensuring maternal and child wellbeing;- enabling the mother and her supporters to assume responsibility
throughout the perinatal period and thus ensure client provider partnership.
Humanization of childbirth pilot project was introduced at Lower Umfolozi District War Memorial Hospital (LUDWMH) in April 2001. This is a 252 bed hospital with an average of 800 deliveries per month. It is a referral hospital for all the level 1 hospitals in northern KwaZulu Natal. Although it is a level 2 hospital, it has some specialists and intensive care facilities. The labour ward has 14 cubicles with one labour bed each. Five of these are used for monitoring latent phase of labour. The physical lay out of the labour ward allows for adequate patients’ privacy however, up to the time of implementing the pilot intervention project, companionship in labour was not allowed.
The AimTo develop, implement and monitor application of a humane maternity care model based on currently available evidence, using an organized audit model.
157

The Pilot Intervention ProjectThe project involved a combination of the following approaches: - Better Births Initiative, Social Support in pregnancy and childbirth, KMC, Childbirth Education ongoing Perinatal Care Audit. It was introduced in 5 phases with phase 3 & 4 running concurrently
Phase 1: Initiation and orientation of health care providers.The aim during this phase was to ensure ownership of the project and also to update health care providers. This was done in recognition of the fact that apart from adequate institutional infrastructure, obstetric care of good quality requires well-trained staff with continuously updated information along with hospital protocols that incorporate the best scientific evidence available.The main focus was on orientation of midwives to a humanistic approach in maternity care with special emphasis evidence based midwifery practice. The major elements of the orientation programme were: midwife-patient relationship, midwife-doctor relationship, communication process, better birth practices, social support during pregnancy and childbirth, KMC and perinatal review.
Phase 2: Health Education to clients & communityThis was done to stimulate active participation of women and their significant others. Women who feel empowered to be active and informed players during labour and delivery enjoy a better experience during pregnancy and delivery. It is also a fact that empowering women and improving providers’ skills should be complementary actions.
Phase 3: Auditing patients’ recordsA review of 102 records of women who delivered at LUDWM before implementation of the intervention project was conducted to identify indicators for use as baseline in monitoring and evaluation of changes in perinatal care.
158

Phase 4: Implementation, Monitoring & Assessment
Implementing change and re-assessing practices in maternity. Introduction of companionship system, these were significant
others since the Doula system was already in operation. Introduction of better birth practices. Introduction of intermittent KMC. Exit interviews to assess client perceptions. On-going in-service education for staff members and health
education sessions for client and significant others. Perinatal Review - Although perinatal audit and perinatal review
meetings have been a standard in this hospital, it became necessary to stimulate, encourage and motivate midwives to be pro-active and active participants in these activities.
The Johnson & Johnson Company offered to sponsor the doulas. There are 5 volunteers who act as doulas and they are only available during the day.
Phase 5: Evaluation: Recommendations & Roll out of the programme in the district.In the evaluation phase the sources of data were: Patients’ records Exit interviews to assess client satisfaction with the implemented
changes
Assessment and evaluation of this project is on-going and although not all objectives have been met, preliminary results show some improvement in the care as shown below:
Monitoring and evaluation of progressFindings on base line data from record review (n=102)Parity Nulliparas = (48) 47% Multiparas = (54) 53%Use of pain relief in labour: 45%
159
Use of IV fluids: 59%Position during delivery-Dorsal: 100% Episiotomy: 34%**Average duration of labour: 16hrs** poor recording made it difficult to assess duration of labour and second stage of labour There was no indication of whether there has been accompaniment or not in all cases reviewed.
Findings during Implementation: ( May-December 2001)Only 374 records have already been reviewed and 10 women were interviewed on discharge.
Table 2 Parity (n=374)
Parity No %Nulliparas 189 51Multiparty 185 49Total 374 100
Table 3 Care during labour: (n=374)
Indicator No %Use of Analgesics in Pain Relief 87 23IV Fluids 73 19Oral Fluids 248 66Position during delivery:Sitting up (on the bed)SquattingDorsalNot Recorded
201 72 70 31
541919 8
Episiotomy 79 21Companionship:DoulaSignificant otherNo companion
84 28 262
22 7 70
160

The average duration of labour in this group was 11hrs.
Analysis of IndicatorsThe indicators are presented as preliminary findings. The project is ongoing and will be reassessed later. Thus only basic statistics are presented and the significance of findings have not as yet been analysed.
161

The positive benefits of the introduction of humanised care are already indicated on the bar graphs and thus should encourage all midwifery units to implement and support this care.Client Responses to Interviews and Suggestion Box with regards to standard of care.Although the intention was to interview all 374 women whose records were reviewed, only 10 were interviewed on discharge. This was because of staff shortages and time constraints. Data was also collected from a large suggestion box in the postnatal ward. This data is still being processed but some preliminary findings from both the interview schedule and the suggestion box are included.
Comments:Women suggested that companionship in labour should be continued and more companions should be available even at night. They mentioned that although they would prefer their significant others to provide companionship, it was not always easy for them to be present due to cost of transport and other family commitments. Women who had previously delivered at LUDWM said that care they received had improved. The following interesting comments were made:-
Request to be “attended immediately on arrival in the labour ward”Squatting position “gives more strength to push and makes things go fast”Companion is a “distracter of the pain”“I missed the drip, it helped me a lot in the previous labour, it gives me strength to push”
ConclusionThere are still many challenges and obstacles hindering implementation of humanised maternity care, however, a step forward has been taken to implement better birth initiatives and effort should be made to keep moving forward.
162

The concept of companionship appears to be accepted but there are still problems in involving significant others as companions in labour.The role of health education during antenatal clinic is critical in preparing women, especially those who have had previous deliveries for labour. The introduction of the project coincided with the outbreak of the cholera epidemic and clinic sisters became more involved in prevention and care or cholera cases than in maternity cases as a result clinics did not participate in the project.The high incidence of staff turnover coupled with frequent staff rotation also affects implementation and sustainability of changes.Midwives’ comments were positive about the project. They, however, voiced their concerns regarding shortage of staff and time spent on assisting students allocated in the wards.
163

HOW DO PREGNANT WOMEN EXPECT TO BE ADDRESSED BY DOCTORS?
CN Mnyani, EJ BuchmannDepartment of Obstetrics and Gynaecology, Chris Hani Baragwanath Hospital and University of the Witwatersrand, Johannesburg.
IntroductionDoctor-patient interactions in many South African state hospitals are typically brief and impersonal. This problem may aggravated by differences of class, race, nationality, and gender between doctors and patients. In the obstetric consultation, the history and examination contain intimate elements that make it necessary for the doctor to gain the confidence and preserve the dignity of the woman. A good starting point is that of introduction. The doctor should know and use the name of the patient, and should introduce him or herself. Whether to use the first name or surname depends on the cultural and local context. We undertook this study to determine how pregnant women in our institution prefer to be addressed and to ascertain what their experiences were of recent consultations with doctors.
MethodsThis was a descriptive prospective study of pregnant in-patients at Chris Hani Baragwanath maternity hospital. Occupied beds in the antenatal ward were numbered and subjects chosen from a random number list. The author (CNM) interviewed the patients in the languages of their choice (Zulu, Xhosa, Sotho, or English) after identifying herself as a doctor. Simple demographic data were asked, followed by questions on the patients’ preferences for forms of address, including their opinions on being addressed by first name, surname, and commonly used terms such as ‘sweety’, ‘darling’, ‘mama’ etc. The patients were also asked whether they knew the names of the doctors who had last seen them, and their recommendations on how doctors should introduce themselves.
164

ResultsFifty women were interviewed. The mean age was 28.1 years, with a range of 18 to 39. Forty (80%) considered themselves to be of urban origin, and 40 (80%) had attended high school. Forty-two (84%) lived in formal housing, 18 (36%) were currently employed and 16 (32%) were married. Forty nine (98%) preferred to be addressed by first name, rather than surname. Two (4%) thought it insulting if a doctor younger than themselves addressed them by first name. Thirty-three (66%) felt that they would receive better care if they were addressed by name. Twenty-seven (54%) said they would be offended if they were not addressed by name. Regarding casual forms of address, the terms ‘aunty’, ‘darling’, and ‘sweety’ were disliked by 31 (62%), 24 (48%) and 24 (48%) of women respectively. The terms ‘mama’ and ‘sisi’ were liked by 32 (64%) and 30 (60%) and disliked by 6 (12%) and 9 (18%) of women respectively. This is shown in figure 1.
When asked about their last consultations with doctors, 35 women (70%) reported that they had been addressed by name, 11 (22%) had received no form of address, and 4 (8%) were addressed by other terms. Seventeen (34%) could name the last doctor who had seen them. Forty-three (86%) felt that doctors should introduce themselves by name and the same number agreed with the suggestion that doctors wear name badges.
Figure 1 Pregnant women’s opinions on being addressed by certain casual terms (n=50)
165
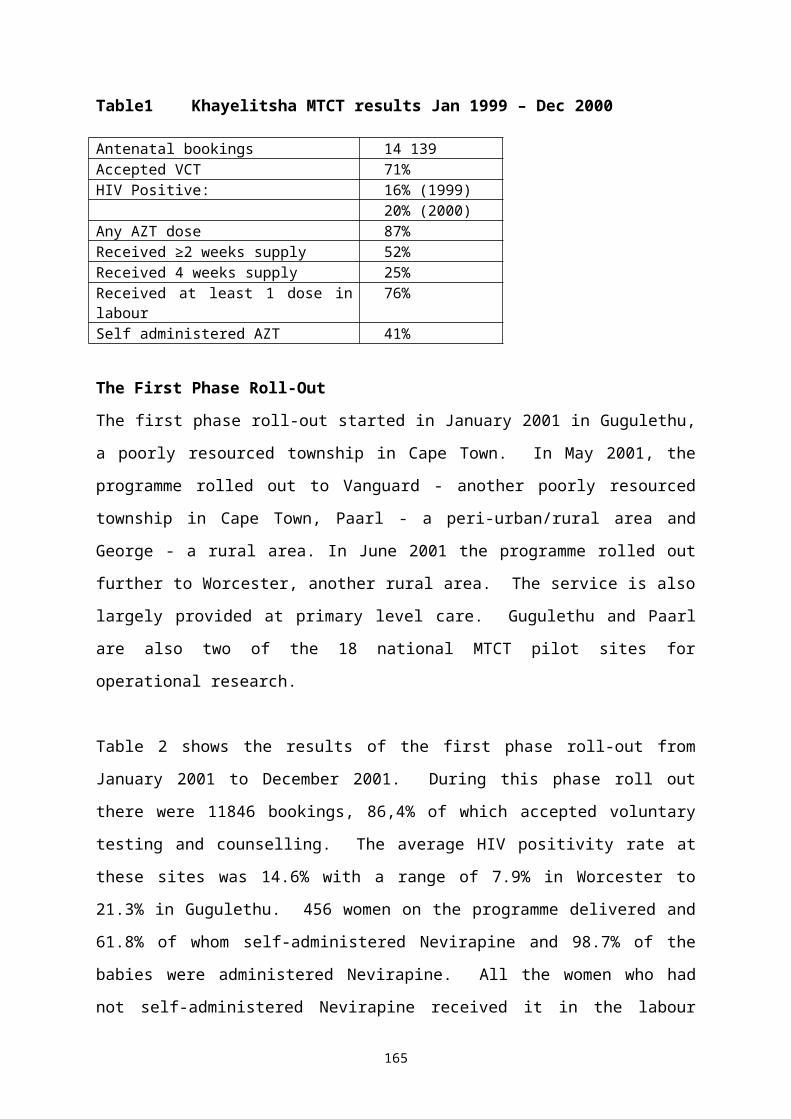
DiscussionThe results show that first name address is acceptable to the vast majority of women in our institution, and that the formality of using surnames is unnecessary. A majority of women found it insulting not be addressed by name. Casual forms of address were not popular, with ‘aunty’, ‘darling’ and ‘sweety’ being the most objectionable. Most women, however, liked the terms ‘mama’ and ‘sisi’, but a significant minority did not want to be addressed in this fashion. The simple courtesy of addressing pregnant women by name costs nothing, is preferred by a majority of women, and is likely to enhance the quality of the consultation. Studies in the United Kingdom and the USA have shown that general practice patients prefer to be addressed by first name. Our study is the first, to our knowledge, that has been done in Africa and on pregnant women.
Most women in the sample did not know the names of the doctors who last saw them, and there was overwhelming agreement with the suggestion that doctors should introduce themselves and wear name badges. This practice needs to be encouraged among all doctors who work in our obstetric department, and perhaps enforced by departmental regulations. Patients’ knowledge of their caregivers’ names has been described as a ‘crucial element in establishing the high-priority patient-provider relationship’.
The study has limitations that relate mainly to generalisability of the results. The sample is representative mainly of urban working class pregnant women who use state hospitals. We cannot speculate on the possible opinions of rural women, wealthy women, non-pregnant women, and users of private health care facilities. It is possible that surnames or other appellations that may imply respect for the individual are more appropriate in other environments.
166

ConclusionPatients must be addressed by name, and the use of casual terms like ‘darling’ should be condemned. This study gives clear support to policies which dictate that doctors should introduce themselves at the beginning of a consultation and wear name badges.
167
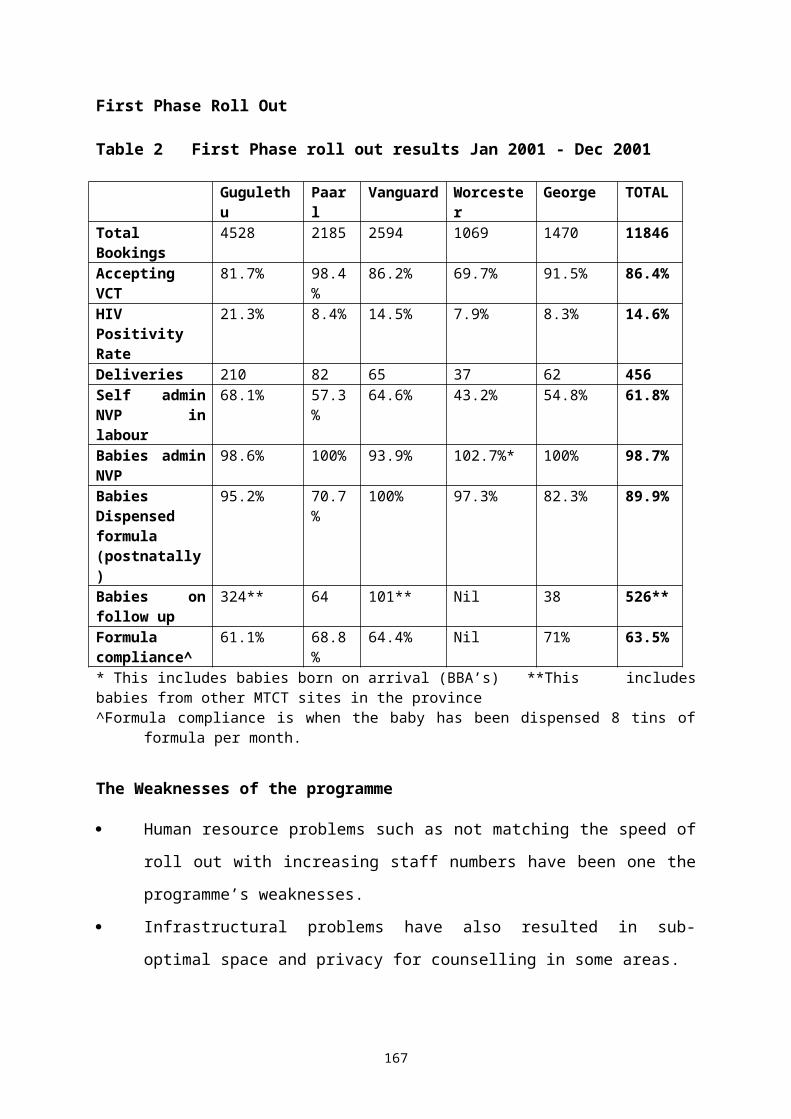
THE BETTER BIRTH INITIATIVE: IMPLEMENTATION IN THE EASTERN CAPE
Z Jafta, B Maholwana, S Masilela*, G J HofmeyrEffective Care Research Unit, East London Hospital Complex/University of Witwatersrand and * E. Cape Dept. of Health
IntroductionThe Better Births Initiative is a global initiative to promote humane, evidence-based childbirth care. Care should be humane and comfortable for women. An added advantage is that this will enhance the reputation of the service and encourage women to attend. Greater use of services is a key step in reducing the half a million maternal deaths in developing countries each year.A workshop format is used for labour ward staff to explore current practice and the need for change. Support for groups who undertake to implement change includes a self-audit process to track improvements. The principles of the initiative are Humanity, Benefit, Commitment and Action. The program materials are available electronically on the internet (http://www.liv.ac.uk/lstm/EHCP.html), and some are included in the 2002 version of the WHO Reproductive Health Library. The program was developed through research by collaborators including the Effective Care and Reproductive Health Research Units (University of the Witwatersrand) and University of Liverpool. The program has the support of the SA National Directorate for Maternal and Child Health. Following pilot studies in Gauteng, it is being implemented in Kwazulu-Natal.
ObjectivesTo implement the Better Births Initiative in Eastern Cape Province.
MethodsA partnership is being formed between the Effective Care Research Unit, Eastern Cape Department of Health (Maternal and Child Health), Fort Hare University and other institutions. During 2001, introductory meetings were held with the Provincial Maternal and Child Health task team, and
168
the Maternal and Child Health regional managers, all of whom have expressed support for the initiative. Workshops will be held in all 24 regions during 2002. Contact will be maintained with maternity units throughout the province, and the effects of the program will be evaluated.
ResultsFeedback from the initial district workshops will be presented at the conference.
169
ORAL FLUIDS AND FOOD DURING LABOUR: A SYSTEMATIC REVIEW
M Singata, JE Tranmer*, GJ HofmeyrEffective Care Research Unit, Frere and Cecilia Makiwane Hospitals and University of the Witwatersrand; *Kingston General Hospital, Ontario
BackgroundRestricting the oral fluid and food intake of women in active labour in hospitals is a strongly held obstetric tradition. A survey of labour ward policies in England in 1985 showed that over a third of consultant maternity units allowed no oral fluids whatsoever during labour.Restriction of oral intake is not a common practice in home births or birth centers, nor is the practice consistent across hospital sites. It is generally believed that withholding oral fluids and food during labour decreases the risk of maternal morbidity from Mendelson’s syndrome if a general anaesthetic is required, as fasting is thought to ensure small volumes of gastric contents. Recent reviews suggest that there is no evidence to support this belief. Interventions to reduce stomach contents or the acidity of the content, both by pharmacological means and by restriction of oral intake, have not proved successful. Irrespective of whether a woman has been starved or not during labour, anaesthetic precautions are necessary to reduce the risk of gastric content aspiration.Despite the risks and lack of evidence of benefits, restriction of oral fluids and food in labour is widely practised.
ObjectiveTo determine the benefits and risks of oral fluid or food restriction during labour.
MethodsStudies comparing policies of starvation; allowing food and/or oral fluids; allowing only carbohydrate-based oral fluids; or allowing only water, and using random group allocation with reasonable allocation concealment (e.g. opaque, numbered, sealed allocation envelopes) will be included. Predefined maternal and fetal outcomes will be sought. The search
170

strategy developed for the Pregnancy and Childbirth Group as a whole will be used. All studies will be assessed for eligibility criteria. Data will be analyzed using RevMan software. For dichotomous data, relative risks and 95% confidence intervals will be calculated. For continuous data, weighted mean differences and 95% confidence intervals. In the absence of heterogeneity, results will be pooled using a fixed effects model. The following subgroups will be analyzed: Intravenous fluids used routinely for women not receiving oral fluids; Intravenous fluids not routinely used.
ResultsResults and recommendations will be presented.
171

OBSTACLES TO LABOUR COMPANIONSHIP AT BAMALETE LUTHERAN HOSPITAL IN RAMOTSWA-BOTSWANA
MM Mothibe, AGW Nolte*Bamalete Lutheran Hospital, Botswana, *Rand Afrikaans University, Johannesburg
Introduction and BackgroundThe common feature of the maternity units at BLH is that women go through labour and delivery without continuous support during the worst moments of pain, exertion, fatigue, anxiety, doubt, vulnerability, strange surroundings and unfamiliar people. The long hours of uterine contractions often render the woman helpless and sometimes frustrated.There is under-utilisation of labour companionship at BLH despite several efforts that have been made to introduce labour companionship. Labour companionship is a rare exception in the BLH labour ward.
A randomised controlled trial of primigravidae in Botswana was conducted to determine the effectiveness of the presence of a female relative as a labour companion on labour outcomes. This study revealed that the presence of a female relative is associated with fewer interventions and higher frequency of normal deliveries compared to the outcomes of those without family member support.
At BLH, a pilot study was conducted on labour companionship and pain relief. The study revealed that the patients’ wish for a labour companion was not granted. More than 60% wished to have a companion but only 12% had companionship during labour and delivery. Almost all the women who had had a companion wished to have one in future deliveries. The person most mentioned as a companion was the mother.
The primary health care delivery system advocates involvement of the traditional birth attendants (TBAs) in the mother and child health care. In 1994, the Ministry of Health in collaboration with the WHO published three studies on determinants of home deliveries and traditional maternity care
172

in Botswana. TBAs were identified to provide supportive care to the mothers. On the other hand, TBAs are seriously handicapped as far as the current concepts of management of labour are concerned, both in approach and specific skills. Problem StatementStaff shortages force midwives to concentrate on “delivering” the woman instead of going through the labour process with the woman. This situation calls for a labour companion who can offer the woman consistent emotional and physical support during labour and delivery. Labour companionship remains underutilized in the Bamalete Lutheran Hospital (BLH) maternity ward despite its proven benefits.
Purpose and ObjectivesThe overall purpose of this research was to improve maternity care.The specific objectives were to explore and describe obstacles to the utilization of labour companionship and to identify the need for the utilization of labour companions. To develop and recommend strategies to overcome the obstacles to labour companionship at BLH.
Research Design and MethodAn explorative, descriptive qualitative contextual and multiple case study was conducted to gain insight into, and understanding of, obstacles to labour companionship at Bamalete Lutheran Hospital.
The target population was mothers who delivered at Bamalete Lutheran Hospital.The sample consisted of five primigravidae who were unaccompanied during labour and delivery, the attending midwives, and any person of the primigravidae’s choice willing to participate in the study.
Data was collected in three stages.
173

Stage oneThis stage consisted of five unaccompanied primigravidae who were at least eight hours post-delivery. Face-to-face semi-structured interviews were conducted. Stage twoThis stage consisted of participants selected by the primigravidae as their ideal labour companions. Face-to-face semi-structured audiotaped interviews with open-ended questions were used to ensure free sharing of information and to explain the underlying meaning of their responses. Stage three This stage consisted of naive sketches by the midwife who attended the first and/or the second stage of labour. The researcher requested the midwives to write the naive sketches immediately after the delivery while the experiences were still clear.
Data analysisData analysis was done using four cognitive processes of qualitative methods which are comprehending, synthesizing, theorizing and contextually. An analysis was done after verbatim transcriptions of the interviews and translation from Setswana into English.
Findings and ConclusionThis study identified six themes and categories under stage one, five themes and categories under stage two, and four themes and their categories under stage three. The results of each stage were discussed and utilized to develop a model of the findings, which was used to guide the conclusions (see Figure 1).
174

Figure 1 A Model for Obstacles to Labour Companionship at Bamalete Lutheran Hospital
Obstacle 1Lack of knowledge on the concept of labour companinoship and it's availability as a service at BLH
Stage One PrimigravidaeFindings revealed that lack of knowledge about labour companionship among primigravidae was found to be the reason why labour companionship was under-utilised. Primigravidae not only lacked knowledge on the concept of labour companionship, but also lacked knowledge that it is a service offered at BLH. These findings revealed the need for extensive education of the Ramotswa community about the concept of labour companionship and how it is implemented at BLH. Utilisation of labour companionship can improve if women are well informed about the availability of the service.
Stage Two Labour companionFindings revealed that ideal companions who were mostly primigravidae’s mothers had sufficient knowledge about labour companionship from a traditional view point. The study was also able to reveal that labour companions’ lack of knowledge on how labour companionship can be implemented in a hospital setting and lack of knowledge about labour
Obstacle 4Reluctance to
implement labour
companionship by midwives
Labour companionship at BLH
Obstacle 3Obstacle 3Lack of privacy
in the unit
Obstacle 2Obstacle 2Lack of knowledge on how to practise labour
companionship in a hospital setting by an ideal labour companion
175

companionship as a service, were the reasons for the under-utilisation of labour companionship at BLH.
These findings showed that labour companionship must be marketed extensively in order to inform the community about the available service. Education and information about labour companionship must include mechanisms of modifying traditional labour companionship to fit into the hospital setting.
Stage Three Midwives naive sketchesFindings revealed that the midwives’ reluctance to implement labour companionship and lack of privacy in the unit were the reasons for under-utilisation of labour companionship at BLH.
Extensive in-service training for midwives on how to modify and incorporate traditionally known labour companionship in a hospital setting is required. Training on communication, interpersonal and counselling skills should also be offered to improve labour companionship implementation at BLH.
Promotion StrategiesThis study utilised the Sexual Reproductive Health (SRH) and Information, Education and Communication (IEC) approach as a guide. Identified obstacles to labour companionship were used to develop the promotion strategies for labour companionship at BLH.The aim of the programme is to improve knowledge about labour companionship and to promote utilisation of labour companionship at BLH.
Promotion strategy 1 is to overcome reluctance by midwives to implement labour companionship.Development of an in-service training programme to improve the skills of midwives on: support skills of women in labour and their labour companions.
176

implementation of labour companionship in a hospital setting. interpersonal and communication skills. counselling skills.Promotion strategy 2+3 is to overcome the following obstacles Primigravidae’s lack of knowledge of the concept of labour
companionship and it’s availability as a service at BLH. Labour companions’ lack of knowledge on how to practise labour
companionship in a hospital setting.
The promotion strategy 4 is to overcome the lack of privacy in the unitLack of privacy was found to be due to the construction of the ward, which if privacy is to be ensured would require major structural changes and has financial implications for BLH management. Labour companionship at BLH is a service essential to the SRH and therefore need to be incorporated into the programmes and activities of the hospital hence lack of privacy will be addressed using both the short and the long-term strategies. Short-term strategies include: Modification of the existing labour cubicles by erecting mobile
partitioning to replace curtains. Information orientation of relatives regarding the ward and which items
to bring to the hospital to facilitate optimal use of the available resources.
Long-term strategies will include:Strategic planning by BLH management on how to secure funds and plan for the reconstruction of the maternity ward should be done.The SRH personnel will have to be involved in the planning of the maternity ward for practical input with special attention to the following: Increase in the number of labour rooms Increase in the number of post-natal wards. Provision for a waiting room for relatives. Provision of a counselling room.
177
Provision of a secured nurses station and a rest room. Secure funds for on-going in-service training for midwives.
178

THE IMPORTANCE OF TOUCH
Karen HansenJohnson and Johnson Professional Education Division (SA); Touch Research Institute (TRI), University of Miami School of Medicine
ObjectivesTo motivate and assist Health Care Professionals in implementing consistently proven cost-effective interventions such as Touch Therapy.
IntroductionTouch Therapy is as old as mankind and its benefits have been documented as far back as the 16th century. It has been practiced by many cultures and found to be beneficial in many medical conditions from pre-birth to the elderly. Modern day research continues to prove the physiological, emotional and intellectual benefits. Detailed information on 63 various studies available at poster presentation e.g. HIV, colic, disturbed sleep patterns, childbirth companion, kangaroo care.
Tactile deprivation is known to have negative effects on individuals and society e.g. violence, abuse etc.
179

Outcomes
BIOLOGICAL/PHYSIOLOGICAL INFLUENCES OF TOUCH
PHYSICAL, EMOTIONAL AND INTELLECTUAL BENEFITS
Stimulation of the vagus nerve results in increased food absorption
Increased weight gain in premature infants resulting in early discharge – cost saving
Increased levels of serotonin - depression
symptoms of depression (PND), enhanced relationships, positive emotions and a greater sense of wellbeing
Reduced levels of stress hormones – cortisol and catecholamines
Besides reduced levels of anxiety and stress, decrease in clinical symptoms in certain medical conditions e.g. asthma, eating disorders and arthritis, and results in quicker healing time
Increased secretion of hormones e.g. prolactin
Assists milk production, helps relax the mother and advances infant-mother bonding
Increases natural killer cells HIV studies show improvement in immune systems and reduced risk of infection
Shifts brain wave activity from the right side to the left
Improved productivity and mental alertness in the workplace
Stimulates sustaining systems e.g. circulation, heart rate, breathing and digestion
Advances general health in people of all ages
Develops body awareness and advances communication
Assists emotional and mental development, improves trust, increases bonding, promotes self esteem and builds confidence
ConclusionHealth Care Professionals have long understood the importance of touch in parent-infant bonding. In recent decades, they have restructured their clinical settings and standards of care to facilitate early contact. These practices have, in turn, instilled a common wisdom among patients about the ciritical role of touch.Touch should not be considered “alternate medicine”. Studies have clearly demonstrated that touch therapies – such as doula support during labour, kangaroo care and infant massage have a place in the contemporary settings.Ultimately, tactile stimulation may well be recognised as an approach to wellness: just as we see lifestyle factors such as diet and exercise as critical to maintaining our daily health, we need to think about touch in the same way.
180

THE USE OF INHALATION ANALGESIA FOR INTRAPARUM PAIN RELIEF
EE BekkerUniversity of the Orange Free State.
The birth of a baby is usually associated with pain. Intelligent and creative methods of pain relief have been developed to address this problem. In labour wards in Bloemfontein only two methods of pain relief are used: opoid analgesics and epidural block. Inhalation analgesia is not utilised.
The study was undertaken in order to determine possible reasons why inhalation analgesia is not commonly used as a method of intrapartum pain relief. The following goals were set: to determine which methods of intrapartum analgesia are used and
preferred by midwifes; to carry out an evaluation of the knowledge and attitude of midwifes
regarding inhalation analgesia; and to formulate recommendations relating to the increased use of
inhalation analgesia.
The participants in the study were selected from the population, namely the registered professional nurses/midwives working in four hospitals in Bloemfontein with maternity sections. A total of 33 out of the possible 54 respondents completed the questionnaire.
A descriptive research design was used; the particular methodology was a survey study. Questionnaires were distributed and collected. A data analysis was done and frequencies and percentages were obtained.
Most midwifes preferred using pharmacological methods of pain relief. They had limited knowledge of inhalation analgesia (Entonox®). Those who do use Entonox® were generally satisfied with it. The basic and continued training of midwifes in intrapartum pain relief should also receive attention in order to establish a more balanced approach to
181
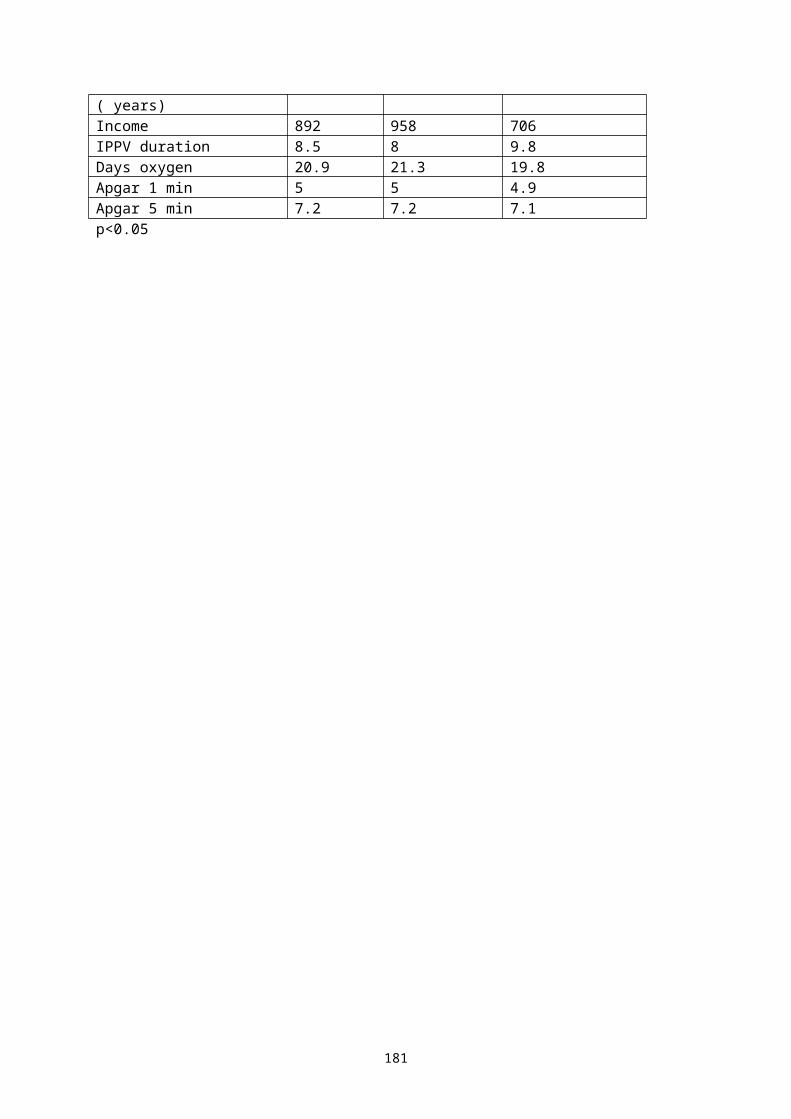
intrapartum analgesia. Entonox® deserves a rightful place in the balanced spectrum of methods of intrapartum analgesia. The possibilities for use in the practise of a midwife outside the hospital environment are very high. Entonox® is a save, effective and client-friendly method to relief pain and could help some of our mothers to enjoy a pleasant birth experience.
182

LOW-DOSE TITRATED ORAL MISOPROSTOL FOR LABOUR INDUCTION: A NEW REGIMEN
S Ferreira, C Grieve, L Mangesi, GJ HofmeyrEffective Care Research Unit, East London Hospital Complex/University of the Witwatersrand
IntroductionThe medical and surgical induction of labour involves both the ripening of the cervix and the initiation and/or augmentation of uterine contraction. Induction is commonly indicated in labour management affecting up to 16% of pregnancies. Pre-induction cervical ripening can be achieved by inserting a trans-cervical Foley catheter and by the use of prostaglandin (PG) E2 (dinoprostone) and PGE1 (misoprostol; Cytotec, Searle). Both methods improve the Bishops score in women with unripe cervices. Uterine myometrial contractions can be stimulated surgically by amniotomy and medically by intravenous oxytocin and prostaglandins.
Misoprostol, a PGE1 analogue, is indicated and licensed for the protection of the gastric mucosa against ulceration. It has also been used in labour induction. Misoprostol has many advantages: it causes both cervical ripening and uterine contraction, it is inexpensive, it is rapidly absorbed orally and vaginally and has a short biological half-life when given orally, it is stable at room temperature, and has few systemic side effects.
Numerous controlled trials have proven the efficacy of Misoprostol for labour induction. In these trials, vaginally- and orally-administered misoprostol was evaluated to be successful in labour induction. The vaginal route of administration results in a prolonged biological half-life when compared to oral administration. A longer bio-availability may provide greater effect but possibly also lead to increased complications and adverse drug effects. The shorter half-life of orally administered misoprostol may be an advantage with regard to complications. Previous randomised trials of oral misoprostol have reported fixed misoprostol regimens with a range of dosages, from 50μg 4-hourly to 200μg 6-hourly.
183

Lower oral doses of misoprostol given more frequently have been shown to be efficacious and minimise the risk of adverse drug effects, notably uterine hyper-stimulation and rupture. In these studies, orally administered clinically titrated doses of 20-50μg were given 2-hourly. Following these studies, it is thought that a further option would be the use of a single small dose of misoprostol vaginally for locally mediated effects on the cervix, followed by titrated low dose oral misoprostol for fine tuning of uterine contractions.
In an effort to reduce the exposure of the patient in labour to risks of misoprostol-induced adverse effects, the lowest dosage regimens clinically acceptable need to be assessed. This study compares the advantageous and adverse effects of titrated low-dose oral misoprostol given after a single small vaginal dose, to currently accepted dosage and frequency regimens used for labour induction.
MethodsA quantitative retrospective descriptive survey of patient records was undertaken on women who delivered following a predetermined protocol of labour induction using misoprostol. The details of the induction protocol are described below. The women included in the study were pregnant with a clinical indication for induction from the East London Hospital Complex. Data was collected and analysed using Epi-Info 6 and MS Excel.The study was approved by the Committee for Research on Human subjects, University of the Witwatersrand, and the Ethics Committee, East London Hospital Complex.
The following is the protocol using titrated oral misoprostol for labour induction:
184

1. Before the commencement of induction, fetal condition was assessed by cardiotocograph (CTG), fetal movement or acoustic stimulation.
2. Once in labour, fetal condition was monitored by CTG or careful auscultation before each misoprostol treatment.
3. Women with unfavourable cervices were given misoprostol (25μg) per vaginum inserted deeply into the posterior vaginal fornix. After 4 hours the cervix was re-assessed and they were then started on the titrated oral misoprostol regime.
4. Women with favourable cervices were given a stat dose of misoprostol 25μg per os. Two hours later they started 2-hourly titrated oral misoprostol.
5. Titrated oral misoprostol (2 hourly) was commenced as follows: Uterine Contractions Oral MisoprostolAdequate (3+ per 10 minutes lasting 45+ seconds)
Nil
Inadequate 25μgNone, or remain inadequate 2 hours after 25 or 60μg
50μg
6. Vaginal examination was performed once at the onset of labour, every 4 hours during the latent phase, and every 2 hours during active labour.
7. Oxytocin (Syntocinon) was not used within 2 hours of oral or within 6 hours of vaginal misoprostol.
8. If the woman was not progressing after 24 hours, the management options were reviewed (cease induction, increased doses of misoprostol, amniotomy, syntocinon, PGE2, or Foley Catheter).
The primary outcomes of labour that were assessed follow those described by Hofmeyr, namely:1. Vaginal delivery achieved within 24 hours.
185

2. Rate of uterine hyper-stimulation (either uterine hypertonus – a single contraction lasting more than 2 minutes, or uterine tachysystole – more than 5 uterine contractions in 10 minutes for 2 consecutive periods) associated with an abnormal fetal heart rate pattern.
3. Caesarean section rate.4. Serious neonatal morbidity (documented as admission to
neonatal ICU or high care) or perinatal death.5. Maternal side effect profile, serious morbidity or death.
The assessed outcomes in this study were compared to those obtained in other similar low-dose oral misoprostol (LDOM) and those obtained in standard-dose oral misoprostol (SDOM) trails.ResultsRecords from 101 women (68 from Frere Hospital, 33 from Cecilia Makiwane Hospital) were analysed in this study. The mean (standard deviation) age of the mothers was 28.42 (7.16) years. Fifty percent were primiparous and 1 was grand multiparous. Sixty five percent of the women had a favourable cervix (modified Bishop’s score >6) at admission. The mean (standard deviation) weight of the delivered neonates was 2820g (722).
Gestational proteinuric hypertension (GPH) was the most common reason for induction, accounting for 79/101. Other reasons (n/101) were intra-uterine demise = 9, post-dates = 7, twin pregnancy = 1, eclampsia = 2, anencephaly = 1, maternal diabetes mellitus = 5, and premature rupture of membranes = 6.
The median dose of oral misoprostol was 300μg, ranging from 25 to 3800μg. The patient receiving 3800μg was in labour for 76 hours. Nine women received more than 1000μg of oral misoprostol during the course of their labour.
186

The induction-delivery interval was less than 12 hours in 17/69 (24.6%) patients, and less than 24 hours in 42/69 (60.9%) patients. The mean induction-delivery interval was 26.03 + 21.91 hours. Headache was reported in 2/101 patients, nausea in 3/101 patients and ascites in 3/101 patients. No other adverse maternal effects were documented.
The five minute APGAR score was less than 7 in a total of 16 neonates. This includes 11 stillbirths. The stillbirths were due to 9 intra-uterine deaths, 1 anencephaly and 1 peripartum fetal demise in a mother with severe gestational proteinuric hypertension and HELLP syndrome. Sixteen fetal distress patterns on CTG were noted during labour, meconium-stained liquor was seen in 9/101, and 30 infants were admitted to either neonatal ICU or a high care facility.
187

Table 1 Results comparing labour induction using titrated low-dose oral misoprostol after a single vaginal dose to other studies of oral misoprostol
Outcome LDOM+Vb SDOMc LDOMd
Vaginal delivery >24 hours 39.1 (31.2-44.9)
9.2 38-65
Caesarean section 31.7 (27.8-41.7)
7.7-21.0 16-21.5
Uterine hyper-stimulation 1 (0.0-5.7) 2.6 0-12Oxytocin augmentation
a Results given as % (95% CI) b LDOM+V low dose oral misoprostol after single vaginal dose (this study)c SDOM standard dose oral misoprostold LDOM low dose oral misoprostol
DiscussionThe demographics and other characteristics of women in this study were similar, in most regards, to those reported in other studies. One notable difference is the high incidence of gestational proteinuric hypertesion seen in women from the East London Hospital Complex requiring induction.
This study shows a general increase in the number of women delivering within 24 hours (60.9%) when compared to using low dose oral misoprostol (LDOM) alone (35-62%). These numbers are far less than those reported in a single trial using ‘standard’ or high dose oral misoprostol (SDOM) where 90.8% of 76 women delivered within 24 hours. This higher dose oral misoprostol may have resulted in this accelerated, if not precipitous, time to delivery. The complication risk in this high dose trial was significantly greater. Although we used the standard 24-hour comparison point (61% delivering by this time), it should be noted that the mean induction to delivery interval in our study was 26 hours, and 72.4% of patients had delivered within 32 hours. This would indicate a reasonably efficient form of labour induction without tending towards precipitous labour. Nine of the documented labours were prolonged, requiring increased doses of misoprostol and possibly oxytocin supplementation. This shows misoprostol to be reasonably effective as an induction agent.
188

Perhaps the most important adverse outcome is possible uterine hyper-stimulation and rupture. Our results showing 0.99% uterine hyper-stimulation are significantly lower than the 2.6% seen in the SDOM and up to 12% in the LDOM studies. We documented no cases of uterine rupture. It would seem that the use of oral misoprostol combined with vaginal misoprostol is decreasing the risk of adverse uterine effects.
Our study did show a particularly high rate of caesarean sections performed (31.7%) as well as increased numbers of neonatal admissions to either ICU or high care wards (33%). We cannot comment whether this is due to misoprostol being used in induction, but suspect the high rates are due to the complicated nature of the obstetric patients seen – many presenting with gestational proteinuric hypertension (GPH). Many GPH patients were caesarean sectioned. It could be debated that these patients should not be induced in the first place and that they should be surgically managed on admission, but unfavourable circumstances, resources and diagnosis make this difficult.
Other known side effects of misoprostol such as fever, shivering, headache and GIT disorders were notably few in our study (2 women complaining of headache and 3 complaining of nausea). This would probably be due to the low doses used.
On the basis of these results it could be cautiously suggested that the use of a single small dose of misoprostal vaginally for locally mediated effects on the cervix, followed by titrated low-dose oral misoprostol solution for fine-tuning of uterine contractions, improves the clinical effect and safety profile of using misoprostol in labour induction.
189

MISOPROSTOL AND MECONIUM: CLINICAL AND LABORATORY STUDIES
GJ Hofmeyr, BB Matonhodze, *L Katsoulis.Effective Care Research Unit, Frere and Cecilia MakiwaneHospitals, and * Department of Pharmacy and Pharmacology, University of the Witwatersrand, Parktown, Johannesburg, South Africa.
BackgroundWe have previously shown a trend to increased meconium passage in women taking castor oil or herbal remedies (isihlambezo), and that in-vitro individual constituents of isihlambezo stimulate both rat myometrium and ileum. We postulated that there may be a direct effect on fetal bowel action of substances ingested by the mother which cross the placenta to the fetus.Systematic reviews of labor induction trials have shown increased meconium passage with vaginal misoprostol use versus intracervical dinoprostone use, with oral versus vaginal misoprostol and a trend to more meconium passage with prostaglandin use than with oxytocin for prelabor rupture of membranes at term.
ObjectiveTo determine the in-vitro contractile activities of dinoprostone, misoprostol and oxytocin on myometrial and ileal smooth muscle.
Experimental hypotheses1. Misoprostol and dinoprostone stimulate both bowel smooth muscle and
myometrium.2. The relative stimulatory effect of misoprostol on bowel smooth muscle
compared with myometrium is greater than that of dinoprostone.
MethodsVirgin Spraque-Dawley rats weighing approximately 250g were oestrogenised by injection with stilbestrol (10g/100g) (Maybaker (SA)) i.p. 24 hours before being euthanased with CO2. Uterine and ileal tissue was
190
dissected out and mounted in Tyrode’s solution. Organs were allowed to equilibrate in the organ baths for at least 30 min during which time the baths were rinsed frequently. Isotonic contractions of the organs were measured against 1g resistance and recorded electronically using potentiometer recorders. The organs were challenged with cumulative doses of either reference agonists or study medications. Standard curves using the relevant reference agonist alone were run at the start of each experiment and between each test challenge. Repeat experiments were carried out using tissues from different rats. The response to each concentration of drug was expressed as a percentage of the maximal response to acetylcholine tested prior to the test challenge.
ResultsOxytocinThe maximal uterine response to oxytocin and acetylcholine are equivalent (Figure 1a), whereas oxytocin has no measurable effect on the ileum for the concentrations used (Figure 1b). The uterus tissue returned to baseline lengths more quickly after being challenged with acetylcholine than when challenged with oxytocin (data not shown). For the above three reasons, acetylcholine was used as the reference drug for the comparison between dinoprostone and misoprostol.
DinoprostoneThe uterine response to dinoprostone was significantly larger than the ileal response (P<0.05) for the concentrations 1.6M to 0.4Mm (Figure 2). The mean maximal response of the uterus to dinoprostone relative to the uterine response to acetylcholine was 91.3 whereas the maximal response of the ileum relative to the maximum response of the ileum to acetylcholine was 70.3 (Table 1). The EC50 was an order of magnitude lower in the uterus than in the ileum.
Misoprostol
191

The contractile response to misoprostol was significantly larger in the uterus then in the ileum (P<0.05) for the dinoprostone concentrations 0.1Nm to 32Nm (Figure 3). The maximal response of the uterus to misoprostol relative to the uterine response to acetylcholine was 79.8 whereas the maximal response of the ileum to misoprostol relative to the maximum response of the ileum to acetylcholine was 61.8 (Table I). As for dinoprostone, misoprostol is more potent on the uterus than the ileum (Table I).
Misoprostol and dinoprostoneFor each drug, the response (expressed as a fraction of the acetylcholine Emax) to the maximal concentrations for the ileal tissue was calculated as a proportion of that for the uterine tissue from the same animal. The mean results were 70.2% for misoprostol and 70.5% for dinoprostone. These values are equivalent (DF=8; P=0.980).
DiscussionThese results support the hypothesis that prostaglandin analogues but not oxytocin may stimulate fetal meconium passage. They infer that pharmacodynamic differences in contractile activity do not contribute towards the higher incidence of meconium passage with vaginal misoprostol use versus intracervical dinoprostone use. It is more likely that the resistance of misoprostolic acid to placental PGDH enables the misoprostolic acid to enter the foetal circulation more readily than does dinoprostone.
ConclusionThese results provide a pharmacological basis for the increased rate of maternal gastrointestinal complaints and meconium passage with labour induction using dinoprostone and misoprostol compared to oxytocin.
192

Figure 1 Comparison of contractile response to oxytocin of rat uterus a) compared with rat ileum b) muscle. There was no measurable ileal response to oxytocin within the concentration range studied.
Log concentration (M)
% m
axim
al r
espo
nse
toac
etyl
chol
ine
-13 -12 -11 -10 -9 -8 -7 -6 -5 -4
0
20
40
60
80
100
Acetylcholine (n=14)Oxytocin (n=7)
a) uterus
Log concentration (M)
% m
axim
al r
espo
nse
toac
etyl
chol
ine
-13 -12 -11 -10 -9 -8 -7 -6 -5 -4
0
20
40
60
80
100
Acetylcholine (n=14)Oxytocin (n=7)
b) ileum
193

Figure 2 Comparison of contractile response to dinoprostone of rat uterus compared with rat ileum muscle. The plots represent the mean with the SEM and the asterisks indicate the concentrations at which the uterine and ileal responses to dinoprostone are significantly different (p<0.05).
Figure 3 Comparison of contractile response to misoprostol of rat uterus compared with rat ileum muscle. The asterisks indicate the concentrations of misoprostol at which the differences between the uterine and ileal responses to misoprostol are statistically significant
(p<0.05).
Log concentration (M)
% m
axim
al r
espo
nse
toac
etyl
chol
ine
-11 -10 -9 -8 -7 -6 -5 -4 -3 -2
0
20
40
60
80
100
ACh ileum (n=14)
Dinoprostone
Ileum (n=11)Uterus (n=12)
ACh uterus (n=14)
**
** *
*
Log concentration (M)
% m
axim
al r
espo
nse
toac
etyl
chol
ine
-13 -12 -11 -10 -9 -8 -7 -6 -5 -4
0
20
40
60
80
100
ACh ileum (n=14)
Misoprostol
ACh uterus (n=14)
Uterus (n=10)
Ileum (n=8)
**
** *
*
194

Table I Maximal responses to dinoprostone and misoprostol relative to their maximal responses to acetylcholine
Uterus IleumMaximal response Maximal response
DinoprostoneDinoprostone 91.381.3 –101.1
70.395% CI 46.1 – 94.4MisoprostolMisoprostol 79.8
66.1 – 93.461.6
95% CI 35.0 – 88.7
195
MISOPROSTOL FOR TREATING POSTPARTUM HAEMORRHAGE
B Maholwana, GJ Hofmeyr, C Nikodem, S Ferreira, M Singata, L Mangesi, Z Jafta, Z MlokotiEffective Care Research Unit – East London Hospital Complex and Tembisa Hospitals, University of Witwatersrand
BackgroundPostpartum haemorrhage is a major cause of maternal mortality, particularly in resource-poor countries of the developing world. The most recent report of Confidential Enquiries into Maternal Deaths in South Africa identified postpartum haemorrhage as one of the top three contributors to maternal mortality. The incidence of postpartum haemorrhage is successfully reduced by the judicious use of routine oxytocics.
Misoprostol has now well-documented uterotonic properties as it is a potent myometrial stimulant of the pregnant uterus. This is more relevant for developing countries as misoprostol is a thermostable drug that does not require refrigeration. It is administered with ease and remains relatively inexpensive.
Prostaglandins for the Prevention of Postpartum Haemorrhage(Cochrane Review )A Cochrane review done on Prostaglandins for the Prevention of Postpartum haemorrhage was done recently. The main results showed that oral misoprostol at the dose of 600mcg was found to be less effective than conventional injectable uterotonics in reducing blood loss >1000 mls (RR 1.36; 95% CI: 1.17 – 1.58). Shivering and elevated body temperature were identified as the main side-effects of misoprostol and are dose-related.
The main contribution to this review was the WHO mega-trial involving over 18000 women. The primary outcome, blood loss exceeding 1000ml was significantly higher in the misoprostol group. However, there was a
196

trend to less blood transfusions in the misoprostol group. Subsequent, unpublished analysis showed a trend to fewer women in the misoprostol group with haemorrhage exceeding 1750ml and 2000ml. One possibility is that misoprostol does have an effect, perhaps delayed, in preventing massive blood loss. This suggests an opportunity for the evaluation of misoprostol as adjunctive therapy for the treatment of postpartum haemorrhage.
Uncontrolled ReportsUncontrolled trials of misoprostol for treating postpartum haemorrhage have claimed impressive results, but these are difficult to interpret because of the lack of a control group. The results show a promising role for misoprostol in the treatment of postpartum haemorrhage not responsive to conventional uterotonics. The primary outcome measure used in all these studies was prompt cessation of haemorrhage and sustained uterine contraction.
Misoprostol For Treating Postpartum Haemorrhage – A Systematic ReviewWe have conducted a systematic review of misoprostol for treating postpartum haemorrhage, using Cochrane methodology. A literature search was done using the Cochrane controlled trial register, the WHO Reproductive Health Library and Medline. One controlled trial was identified, conducted in Durban – South Africa, which showed fewer women who had received misoprostol, failing to respond clinically to the treatment. The study yielded a 28.1% difference between the misoprostol arm and the syntocinon plus syntometrine arm, when measuring cessation of haemorrhage within twenty minutes. However, the interpretation is limited by the fact that the clinicians were not blinded, and the randomisation was not successful in producing comparable groups. There remains, thus, a need for a larger confirmatory trial.
197

The question this review also hoped to answer was the best route of administration of misoprostol for this indication. Oral misoprostol in the third stage of labour had significant side-effects, particularly shivering and pyrexia. These appear to be less with the rectal route. Further, extrapolation from studies of labour induction suggest that dose for dose, misoprostol is clinically more effective when administered vaginally or buccally. The rectal route is assumed to be similar to the vaginal or buccal route because of muco-cutaneous and local properties.ECRU Pilot Study and ProtocolWe are conducting a double-blind placebo-controlled randomised trial comparing misoprostol by multiple routes with placebo in women with postpartum haemorrhage who have received all the standard therapy. Included are women aged 18 or more who present with bleeding that is qualitatively more than expected, at least 10 minutes post delivery, who were willing and able to give consent.
Intervention – Routine treatment for postpartum haemorrhage will be administered as per hospital protocol and eligible women will be randomised by drawing the next in designated treatment packs with five tablets containing either misoprostol 200mcg or placebo. In addition to routine management, misoprostol or placebo tablets will be given as one orally, two sublingually and two rectally.
Primary outcome measures – Blood loss >500ml measured one hour after enrolment, median blood loss, median haemoglobin level on the first day post-delivery and the side-effects one hour after enrolment.
A sample size of 334 will give an 80% chance of detecting reduction from 25% - 12.5%. Recruitment started in September 2001 and we are targeting 134 enrolments a year. The expected duration of the trial is three years.
198

Current Blinded Data from ECRU TrialIn this paper, we have compiled preliminary results in the form of blinded data from our trial. We have recruited 37 women in three centers to date and have looked only at our primary outcome measures. Blood loss of >500ml one hour after enrolment was found in 0.11% and an elevated temperature of >38 in 13.5%. Shivering was noted in 38%, graded as mild to moderate in 21% and severe in the remaining 17%. A large 59% of the sample had a day 1 mean haemoglobin of <9.5 g/dl and 40% of this subset required blood transfusion. Only two patients had surgical complications; requiring examination under anaesthesia.
Thus far, the primary outcome event rate is less than the sample size calculation. In order to obtain sound estimates on more substantive outcomes, the sample size will need to be increased to about 500 per group. We shall require multicentre participation to speed up recruitment.
Results will be expressed as relative risks or weighted mean difference with 95% confidence intervals, using Epi Info 6 and Revman software. Dummy results tables will be prepared prior to the data analysis.
ConclusionsMisoprostol, if proved effective, may impact on maternal mortality in low income countries. This method has, in fact, entered clinical use particularly in developing countries but this is without systematic research to document the optimal dosages, effectiveness or risks. It remains essential, therefore, to evaluate its effectiveness objectively and systematically.
199

AN AUDIT OF THE ROLE FETAL DOPPLER ASSESSMENT CAN PLAY IN THE MANAGEMENT OF THE VERY LOW BIRTHWEIGHT COMPROMISED FETUS.
JJL de Souza, I Erasmus, K ApenDepartment of Obstetrics and Gynaecology, Coronation Hospital, University of the Witwatersrand
According to established guidelines on the use of umbilical artery Doppler, delivery of the compromised growth retarded pre-term fetus should take place when the following criteria apply at the POG given:
1. Absent flow without oligohydramnios – deliver at 32 weeks.2. Absent flow with oligohydramnios – deliver from 28 weeks.3. Reversed flow – deliver as soon as possible if the fetus is viable.
In the South African setting, the problem with the above can be that there is limited access to neonatal intensive care stations. As far as the uncompromised premature fetus is concerned, criteria for acceptance into most units include a fetal mass category of at least 1000gms, while in others 900gms would qualify. Generally there is a shortage of neonatal ICU stations – academic hospitals have an ICU station ratio of 0.5 – 1.0 per 1000 deliveries, much lower than elsewhere. Along with the fact that it is cheaper to keep the fetus in utero under surveillance in a high care unit rather than in a neonatal ICU once born, there is virtue in the selective delay beyond the criteria fulfilling the guidelines, as long as irreversible damage to the fetus through waiting too long does not take place. Postponing delivery could have implications regarding reduced need to ventilate and shorter length of stay in the neonatal ICU. The ultimate stage of deterioration before fetal serious intellectual and neurological damage has not been clearly identified, some believe it will be shortly after CTG changes denoting hypoxia appear, while others believe that this stage can be too late. Hecher and Hackeloer and Stewart Campbell have suggested that reduced flow in the Ductus venosus is a sign that serious irreversible damage is just beginning, and if this point is reached, timeous delivery will denote a good outcome. They also believe in not waiting for CTG changes to appear and disregard a normal CTG. Gudmundson, on the
200
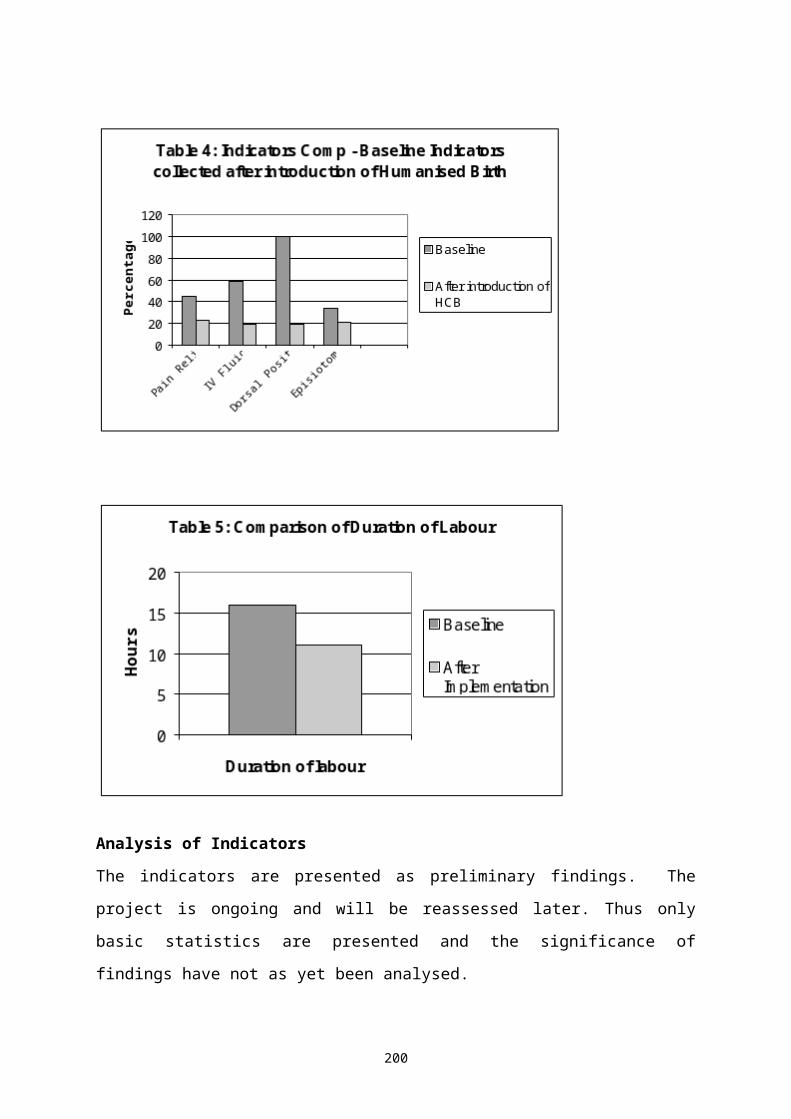
other hand, believes that pulsation in the umbilical vein is a marker for ominous outcome, especially if such a pulsation takes on a double wave form. Whichever way, there has been a tendency to discount the CTG. Materials and MethodsSince May 1999, IUGR pregnancies managed at Coronation Hospital with umbilical artery changes denoting vascular impairment have undergone additional fetal Dopper assessment of vessels in the fetus, including vessels such as the middle cerebral artery, the aorta and inferior vena cava, and have also been assessed for signs of cardiac enlargement and cardiac failure. Parameters denoting abnormality were derived from graphs supplied by the Maternal Fetal Foundation, London.Decision to deliver lay entirely with the consultant in charge of the case. However, if advice was sought we encouraged delivery of a viable fetus once REDF became evident. This was often delayed due to unavailability of an ICU station. Some cases were terminated before the reversed flow stage was reached due to the advent of fulminating pre-eclampsia or the discovery of the HELLP syndrome. All case records of pregnancies undergoing Doppler assessment between May 1999 and March 2001 were reviewed and categorised into the following groups:
GROUP 1 Reduced or absent umbilical artery end diastolic flow + arterial redistribution in the fetal brain denoted by reduced PI, >32 weeks.
GROUP 2 AEGF, redistribution, <32 weeks. GROUP 3 AEDF, abnormal EDF in the Ductus venosus,
no pulsation in umbilical vein. GROUP 4 All fetal Dopplers abnormal, pulsation in the
umbilical vein present. GROUP 5 Abnormal Doppler in twins.
Adverse outcome parameters included intrauterine death, 5 minute Apgar scores <7, length of stay in hospital, fetal morbidity, neonatal ventilation, neonatal death, abnormal or pre-terminal CTG tracings, and cardiac effects. The data is displayed in the tables.
201

202

Group 1 Reduced or absent Umbil art ED flow, redistribution to brain but other parameters either normal or abnormal >32 weeks.
FetalCase No Age POG High BP Pre eclamp Umb art Dop MCA CTG Wt Apgar 5min Outcome. . 1. 35y 35w - - absent flow N flat+decel 1459 g 9 NVD well 2. 24y 34w + - absent flow redis normal 1570 g 5 NVD well 3. 37y 34w + - absent flow redis normal 1600 g 8 NVD well. 4. 36y 33w - - absent 2days redis pathol 1400 g 3 .
Group 2 Reduced or absent UA flow, idem but at <32 weeks.Case No Age POG High BP Pre eclamp Umb art Dop MCA CTG Wt Apgar 5 min OutcomeCase No Age POG High BP Pre eclamp Umb art Dop MCA CTG Wt Apgar 5 min Outcome. . 5. 29y 28w + + + absent flow redis flat 60 min 1459 g 9 CS well HELLP vol expan bcu 42 days 6. 33y 29w - - absent flow redis N 1570 g 5 CS died day 5 7. 34y 29w + ++ absent flow redis N 990 g 7 CS ICU 210 days 8. 21y 28w + + absent flow redis decel 1060 g 8 CS well tachy 9. 35y 28w + + absent flow redis N 952 g 7 CS well ABRUPTION bcu 52 days
Group 3 Reversed Umbil art EDF, abnor Ductus Venosus (reduced or absent ED flow) no pulsation in the umbilical vein.
Case No Age POG High BP Pre ecl UA Dop MCA DV UV Heart CTG Wt Apgar 5 min Outcome
. . 10. 35y 30w + - Rev flow redis abn N dilat N 1120 g 8 CS well ICU 11. 35y 29w + + Rev flow redis abn N N equiv 900 g 9 CS well bcu 12. 28y 32w + + Rev flow redis abn N dilat decel 1100 g 7 well bcu 26d 13. 22y 26w - - Rev flow redis abn + IUD IUD 520 g IUD IUD 14. 31y 29w - - Rev flow redis abn N N flat 860 g 8 CS well 60 min 15. 24y 28w + - Rev flow redis abn N N N 1300 g 9 well 7 days 7 days 16. 28y 30w - - Rev flow redis abn N N N 700 g 9 NVD well 17. 33y 26w + - Rev flow redis abn N N IUD 1040 g IUD IUD . .
Group 4 Reversed Umb art EDF, Ductus ven reduced or absent, with pulsation in the Umbilical vein
FetalCase No Age POG High BP Pre ecl UA Dop MCA DV UV Heart CTG Wt Apgar 5 min Outcome
. . 18. 26y 30w + - Rev flow redis abn puls N decel 850 g 9 died 6 days 19. 38y 33w + - Rev flow redis abn puls pericard N 1100 g 8 well ICU effusion 43 days 20. 24y 32w + + Rev flow redis abn puls dilat flat 1480 g 6 well ICU HELLP ++ decel 20 days 21. 26y 30w + + Rev flow redis abn puls N N 830 g 7 well bcu +++ 22. 26y 29w - - Rev flow redis abn puls N flat 1280 g 8 well ICU
60 min 39 days 23. 25y 29w + + Rev flow redis abn puls N N. 900 g 9 died 5 days . +++ ++ . 24. 26y 30w + + Rev flow redis abn puls dilat IUD 780 g IUD IUD
>24 hrs effusion pericardium
25. 17y 26w + + Rev flow redis abn puls N TOP 716 g TOP TOP >24 hrs 26. 41y 27w + - Rev flow redis abn puls N IUD 900 g IUD IUD
1. 24hrs
203

Group 5 Twins
Case No Age POG High BP Pre ecl UA Dop MCA DV UV CTG Wt Apgar 5 min Outcome . . 27. 30y 27w + + A. Rev flow redis abn puls - 720 g 4 Ph <7.0
CS delayed…… ……..7 day died day 3B. Abs flow redis N N - 1040 g 9 well
28. 31y 30w + + A. N - N N - 1220 g 6 well B. Rev flow redis abn puls IUD 510 g IUD IUD
.
Group 6 Referred too late with fetus in abject state when Ist US done.Case No Age POG High BP Pre ecl UA Dop MCA DV UV CTG Wt Apgar 5 min Outcome . . 29. 31y 30+ - - reversed - reversal flat 1760 8 Encephalopathy
+++ puls double
US findings - severe oligohydramnios, cardiomegaly, echogenic bowel, pleural effusion. Absent flow aorta, “a” wave in IVC. .
An audit of this series was performed to assess how Doppler can be used to determine optimisation of delivery matching degree of deterioration with outcome. We exclude cases where the outcome was bad due to default - cases 24, 25 and 26. Case 24 refused admission and returned with an IUD, case 26 refused to allow termination without her family’s permission and 36 hours delay in an effort to summon them resulted in the discovery of an IUD as well. Case 25 was terminated due to mis-assessment and inexperience of the clinicians involved but might have been saved had they been prepared to act in the baby’s interest. Despite adequate surveillance, no attempt was made to salvage one previable fetus (case no 13- birthweight 520gms). An interesting case was number 16, a 700g baby which was unexpectedly born in the admission ward without anyone being aware that she was in labour. Excluding these 4 cases as well as an additional case (no 17) which defaulted due to miscommunication, 22 of the 27 singleton pregnancies managed in hospital could be audited. There were 16 survivors.
Group 3 consisted of cases with abnormal ductus flow but no pulsation in the umbilical vein. Six of the eight babies in this group survived, and ¾ of these with fetal mass <1kg survived. Only one of the survivors needed to
204

be ventilated – case no 10. The two deaths were cases that were not subjected to intense serial Doppler surveillance – no’s 13 and 17. At least 2 cases definitely had ECG changes at time of delivery and did well. The respective weights of the survivors were 900, 860, 700, 1120*, 1100, 1300 grams. Remarkably only one these, the 1120* baby required ventilation.
Twenty cases had abnormal flow in the ductus alone or combined with venous pulsation, and 9/13 that had potential to survive did so.
Twelve cases developed umbilical venous pulsation. In only 6 were the criteria for audit met based on compliance by the patients, salvageable size or willingness to deliver with 24 hours of pulsations appearing. There were 4 survivors. The 4 survivors had remained under daily Doppler surveillance for 1, 2, 5 and 6 days respectively. Only one of the survivors had an abnormal CTG, and another with an abnormal CTG did well. Two cases with simple pulsation in unbilical vein had severe abnormality in the ductus, either absent or reversed flow in diastoly. Both these cases did well. The one case with a double pulsation in the umbilical vein also had the severest abnormality in the ductus – reverse flow. This fetus had a normal reactive CTG, and was born with an Apgar of 9/10. The baby did not survive and died on day 5.
Neonates stay in hospital was a mean of 63 days, median 40 days. The 90th centile was 52 days.
Results in tiny babies were as follows:There were 12 neonates between 700g and 1000g. Four were clearly managed inappropriately. Of the remaining 8 there were 6 survivors. Their respective weights were 700g, 830 g, 860g*, 900g, 952g* and 990g.* The three that were ventilated are marked *.
205

ConclusionIt would seem that reversed flow is inevitably associated with some change in the ductus venosus. No conclusions can be drawn about CTG changes and their role either on their own or in association with Doppler in ascertaining optimised timing of delivery. It would seem that it is indeed worth readiness to deliver tiny IUGR babies with an estimated fetal mass of below 1000g and Doppler surveillance helps to identify the fetus which is still salvageable. It would seem to be unwise not to react immediately once pulsation in the umbilical vein appears. Whether widespread availability of this technology will produce improved results is yet to be determined.
206

PAIN RELIEF IN LABOUR AT MOWBRAY MATERNITY HOSPITAL: AUDIT AND INTERVENTION
S Fawcus, P Rode, F Ibach, R DyerMowbray Maternity Hospital. Departments of Obstetrics and Anaesthetics
IntroductionPain relief in labour is often neglected in public maternity facilities. Mowbray Maternity Hospital (MMH) is a public secondary level maternity hospital, which receives complicated maternity cases from 3 midwife obstetric units (Mitchells Plain, Khayelitsha and Guguletu) and a few low risk women from the area. Deliveries per year average 5500 with a 35% caesarean section rate.
MethodsIn 1999, a survey of recently delivered mothers was conducted by an obstetric registrar. Using a questionnaire, information was elicited about (1) the consumer’s views about labour pain and analgesic methods; (2) analgesic methods received or required and their efficacy; and (3) consumer’s views on their pain relief in labour.
ResultsEighty eight recently delivered mothers were interviewed (47 primipara and 41 multipara). Sixty five (73%) had been referred from midwife units with complicated labour. Forty five percent required augmentation, 17.1% required induction of labour, 3.4% had vacuum deliveries and 34% required emergency caesarean sections.Knowledge: Ten (21.3%) of primipara had absolutely no knowledge about labour pains. Forty five (51.1%) of the total sample had no knowledge of any analgesic method.Companionship: Fifty three (60.2%) had no labour companion.Analgesia: Thirty two (35.4%) had had no method of pain relief. Of these, 65.5% did not ask for a method and 34.5% asked but did not receive. All would have like help. Of the 56 (63.6%) who had analgesia, 50 (89.2%)
207

had morphine intramuscularly, 2 (3.6%) had inhalational entonox, 2 (3.6%) had an epidural, and 2 had a combination of methods.ConclusionThere were serious shortcomings in both antenatal education and preparation of pregnant women for labour and actual pain relief management in labour. This was particularly serious given the high percentage of women with complicated labours and extra analgesic requirements. Problems identified to explain the above findings included lack of sufficient midwifery staff, lack of adequate epidural service and problems with staff attitudes.
208
IS PRETERM LABOUR UNAVOIDABLE, BUT ARE DEATHS DUE TO PREMATURITY AVOIDABLE?
RC PattinsonMRC Unit for Maternal and Infant Health Care StrategiesUniversity of Pretoria
IntroductionTo make an impact on the unacceptably high perinatal mortality rate (PNMR) in South Africa, strategies have to be developed that will tackle the major causes of the high PNMR in the country. Since the beginning of the new millennium a perinatal care survey has been conducted in South Africa. The survey is conducted in sentinel sites where a detailed audit has been performed on each perinatal death. At each site the causes and avoidable factors related to perinatal death are recorded on PPIPWIN, a Windows based computer programme. The data from each site is amalgamated and a representative picture of perinatal care is obtained.
Spontaneous preterm labour is second to unexplained intrauterine death as the most common cause of perinatal death. There is a marked difference between the neonatal death rate (NNDR) in the metropolitan areas and the NNDR in the city and towns and in the rural areas (Figure 1). This difference is most apparent between the birthweights 1000g and 2000g. Spontaneous preterm birth is by far the most common primary cause of perinatal death for births in this birthweight category (Table 1 and Figure 2).
Table 1 Proportion of the primary obstetric causes of perinatal deaths between 999g and 2000g per area for 2001
Primary obstetric cause Metropolitan%
City and Town%
Rural%
Spontaneous preterm labour 22.2 29.4 49.7Unexplained intrauterine death 29.5 22.6 21.1Hypertension 18.0 16.7 7.5Antepartum haemorrhage 17.6 16.8 9.5Ideopathic intrauterine growth restriction
1.2 1.3 2.0
Intrapartum asphyxia and birth trauma
1.6 3.8 3.4
209

Infections 1.8 5.3 1.4Congenital abnormalities 4.8 2.1 2.0Pre-existing maternal disease 2.0 0.6 -Other 1.0 0.2 2.7
210

This study was undertaken to determine what the avoidable factors, missed opportunities and substandard care are related to spontaneous preterm labour. With this information, it was felt that rational health care strategies could be developed such that a decrease in the perinatal mortality rate (PNMR) due to spontaneous preterm labour could be achieved, thus effectively reducing the overall PNMR.
MethodsData was collated from the 44 PPIP sentinel sites spread throughout South Africa. Every perinatal death in these sites was analysed and the primary obstetric cause of death and where applicable the final neonatal cause of death allocated. Also avoidable factors, missed opportunities and substandard care were sought for each death. This data was entered on PPIPWIN, a Windows based perinatal audit system. All the deaths whose primary obstetric cause of death was categorised as being due to spontaneous preterm labour were separated and the avoidable factors, missed opportunities and substandard care analysed. This is a function of the PPIPWIN programme.
ResultsThe Perinatal Care Survey of 2001 analysed the causes and avoidable factors associated with 3045 perinatal deaths in 78 343 births of 1000g or more. There were 518 perinatal deaths whose primary obstetric cause of death was due to spontaneous preterm labour. This comprised 17% of all perinatal deaths. The PNMR was of 7.48/1000 births.
Spontaneous preterm labour as a primary obstetric cause of death is divided into a number of sub-categories and this is shown in Table 2. Idiopathic preterm labour was the most common sub-category being responsible for 77% of deaths in the whole group.
211

Table 2Table 2 Sub-category causes of spontaneous preterm labourSub-category causes of spontaneous preterm labourSub-category cause Number
(518)%
Idiopathic preterm labour 399 77.0Preterm premature rupture of membranes (PPROM) 83 16.0PPROM with chorioamnionitis 20 3.9Cervical incompetence 7 1.4Preterm labour with chorioamnionitis with intact membranes
2 0.4
Other 7 1.4
The specific avoidable factors, missed opportunities and substandard care related to spontaneous preterm labour are shown in Table 3. The most common factors allocated were lack of antenatal care (32,6%), delay in seeking help during labour (14.7%), lack of neonatal facilities (10.0%), lack of transport (7.3%) and inappropriate response to premature rupture of membranes (4.6%). There were only 16 cases reported where the management in the antenatal period or intrapartum care in hospital could have been better.
Table 3 Specific avoidable factors, missed opportunities and substandard care for perinatal deaths due to spontaneous preterm labour – 2001
FactorNo.518
%SPL deaths
Lack of antenatal care 169 32.6Delay in seeking attention during labour 76 14.7Lack of transport 38 7.3Inappropriate response to rupture of membranes 24 4.6Inadequate neonatal facilities 52 10.0Multiple pregnancy not diagnosed 18 3.5Incorrect management of preterm labour 12 2.3Antenatal steroids not given 4 0.8Delay in referral 18 3.5
SPL – Spontaneous preterm labour. Note a case may have more than one factor.
Table 4 gives the factors associated with spontaneous preterm labour per designated area. Inadequate neonatal facilities were most marked in the rural areas being associated with 20.5% of perinatal deaths. Undiagnosed twins were also a frequent problem in the rural areas.
212

Table 4 Specific factors involved in perinatal deaths due to spontaneous preterm labour per area.
Factor Metropolitan(N=121)%
City & Town(N=314)%
Rural(N=83)%
Lack of antenatal care 34 (28.1) 115 (36.6) 20 (24.1)
Delay in seeking attention during labour
12 (9.9) 52 (16.6) 12 (14.5)
Lack of transport 7 (5.8) 27 (8.6) 4 (4.8)Inappropriate response to rupture of membranes
3 (2.5) 17 (5.4) 4 (4.8)
Inadequate neonatal facilities 3 (2.5) 32 (10.2) 17 (20.5)
Multiple pregnancy not diagnosed 1 (0.8) 9 (2.9) 8 (9.6)Incorrect management of preterm labour
- 12 (3.8) -
Antenatal steroids not given - 2 (0.6) 2 (2.4)Delay in referral 3 (2.5) 10 (3.2) 5 (6.0)
DiscussionThe major problem of deaths due spontaneous preterm labour is outside of metropolitan areas, more especially in rural areas and this is clearly reflected in the higher neonatal death rates in the cities and towns and rural areas.In allocating the avoidable factors the clinicians are restricted by the information available to them. If a history was not taken at the time of admission on why the patient, for example, presented late in labour, problems relating to transport or the rapidity of preterm labour will not be detected. All that will be documented is the patient arrived late in labour. It is suspected that this will mostly be due to transport problems from the patients’ home to the institution and rapidly progressing preterm labour. Hence the factor ‘delay in seeking attention during labour’ probably includes a large number of transport problems and that factor coupled with directly recorded transport problems probably reflects the real magnitude of transport problems. Transport problems are probably present in between one in four and one in six cases of perinatal death. Analysis of the avoidable factors, missed opportunities and substandard care has nevertheless clearly indicated where the major problems lie. They are mostly related to transport problems, lack of neonatal facilities
213
and the rapidity of preterm labour. In most cases, the health institutions did not have time to stop the labour and administer corticosteroids. This is not an uncommon finding. Doubelaere et al, recorded in only 2.4% of women delivering low birthweight infants was prevention of labour attempted of the 550 low birth weight infants delivering in a tertiary hospital over a six-month period. They concluded that hospital staff could do little to prevent delivery of low birthweight babies. The net result is health institutions are faced with having to manage live premature infants. The infants’ survival is dependant on the neonatal care they receive. The neonatal death rate (NNDR) was significantly lower in the metropolitan areas. Had the cities and towns and rural areas the facilities and expertise available in the metropolitan areas the NNDR could be significantly reduced. The low rate of delay in referral recorded probably reflects the advanced stage of labour many of the women arrive in, making in-utero transfer inappropriate. It also reflects delay in transfer of the premature infants. It is surprising that this was not recorded much more frequently. There are two possible explanations, firstly the infants died rapidly in the institutions, making referral impossible. The second more likely explanation is that the doctors know from experience that the neonatal intensive care units in the tertiary hospitals are “always full” and have got tired of trying to refer the infants who would normally qualify for referral. The shortage of neonatal intensive care facilities is well documented. In one metropolitan area, lack of neonatal intensive care facilities was documented as being closely associated with 20% of infants born within that institution. Refusal of requests from outside institutions was not documented and one can safely assume the rate was high. What is surprising is that no attendance for antenatal care is regarded as a major avoidable factor in these patients, given our inability to predict or prevent preterm labour in general. Also Ndiweni and Buchmann have previously demonstrated that the high perinatal mortality related to lack of antenatal care is normally associated with preterm labour and that the labour intervened before the woman had intended to start antenatal care.
214

These women are usually women of lower risk than those who initiate antenatal care early. There is probably a large element of victim blaming in this circumstance. The major issue related to antenatal care is promoting early attendance at antenatal care and not waiting until the third trimester, which unfortunately is still a common practice. Efforts must continue to bring down the gestational age at which antenatal care is started. The initiation of antenatal care at pregnancy confirmation would clearly facilitate this process. It is in no way certain that early initiation of antenatal care will reduce the rate of spontaneous preterm labour.In looking for health care strategies to improve the PNMR in South Africa, transport and neonatal care facilities and management skills are the major problems in the health system that need to be overcome. It would be unreasonable to suggest a large increase in neonatal intensive care facilities in the metropolitan areas, given the expense and the already existing transport problems. It seems the sensible approach would be to look for easily implementable neonatal care strategies that could be applied to institutions outside of metropolitan areas. Fortunately there are two strategies that seem tailor-made for this. The first could be the introduction of nasal continuous positive airway pressure (CPAP) to stabilise premature infants with respiratory difficulties. Nasal CPAP is a non-invasive, inexpensive method of supporting the neonates’ respiration. It does not require intubation or mechanical ventilation. The second strategy would be the use of kangaroo mother care. Both interventions have been extensively studied and are ideal to fill the current need in South Africa. Lack of transport is a problem that is experienced throughout the health service. It is being addressed at a national level and more ambulances have been ordered. Negotiations with the emergency services in each area should, in the meantime, be initiated so that the principle is established that the highest priority rating is given to pregnant woman in labour.
215

ConclusionImproving neonatal care for premature infants outside of the metropolitan areas is the area where there is the greatest potential to rapidly decrease perinatal mortality rate in South Africa. Two interventions stand out in their potential to immediately address this need, namely the introduction of nasal CPAP and secondly kangaroo mother care. The introduction of these strategies is both inexpensive and the intervention of proven benefit. It is a matter of urgency that these strategies be implemented. More intractable problems such as late initiation of antenatal care and poor transport still need to be addressed.
216

PERINATAL PROBLEM IDENTIFICATION PROGRAM (PPIP) VERSION 2
JD CoetzeeMRC Unit for Maternal and Infant Health Care StrategiesUniversity of Pretoria
The third version of PPIP (the second for Windows) will be introduced. The aim with the program is unchanged: to provide an instrument which health care providers can use to give structure to the audit programs they institute in their units. It provides a complete data analysis, making it possible for units at all levels to enter and analyze their own data. PPIP also makes it possible to include every piece of information entered at any level to automatically be included in data analysis at higher levels.
The main changes to the program include the following: Technical: Now 32-bit, higher resolution graphs, requires more disk
space and RAM. A few more data fields have been included with the basic delivery
entries in order to accommodate the Dept. of Health basic data set. Data analysis has been expanded to allow a more customized look at
the data. The user is allowed to include only specific birth weight categories, causes of death or similar groups in most analyses to get down to exactly the answer that is needed.
New data analysis methods have been introduced and current ones updated as requested by current PPIP users.
Allows the user to view and print ‘raw’ data from the data files. This means that you can actually get a look at the complete data file without any type of manipulation.
All the data displayed in graphs can also be displayed as a table, which makes it easier to see the actual values of the data points in the graphs.
Allows export of the data files to the commonly used data formats, including DBASE, ASCII and Excel.
217

The administrative functions of the program have been simplified – getting data into or out of PPIP is more straightforward.
A few button clicks will import your data from the current version of PPIP, ready for use in version two.
For Internet users the program will allow direct access to the PPIP Web site to search for updates of the program or code lists.
It will be possible to automatically send a copy of the data file as an email attachment to the PPIP Web site.
218

AN ANALYSIS OF AVOIDABLE FACTORS IN 616 PERINATAL DEATHS IN 7 RURAL HOSPITALS
M Ross, NC Mzolo, SM RossCentre for Rural Health, (formerly CHESS) University of Natal, Durban
IntroductionAs part of a programme funded by the MCWH sub-directorate of KwaZulu-Natal, we have been attending perinatal review meetings (PRM) at 7 level one hospitals in rural areas of the province for the past 22 months. Much of the obstetric care is provided by Community Service doctors with minimal obstetric experience. All the hospitals have at least one advanced midwife. At each PRM the staff were encouraged to analyse each perinatal death for avoidable factors. We reviewed 616 perinatal deaths from the seven hospitals for avoidable factors using the PPIP codes (with a few additional ones) and the results were discussed with the maternity staff at 6 out of 7 seven hospitals.
ResultsIn the months under review, there were almost 19 500 deliveries in the 7 hospitals and the overall PNMR was 37/1000 deliveries. The PNMR varied from 23 to 51/1000 deliveries over the time the data was collected, with a range of month by month 7 to 83 and the average number of deliveries in each hospital varied from 111 to 254 per month. The lowest PNMRs were in the hospitals where there was considerable support and supervision from senior medical staff.
The percentage of patient- and health personnel-associated avoidable factors was the same (42%).Administrative avoidable factors accounted for 16% of the total.
219

Patient avoidable factors The commonest problem was late booking (237) which we
defined as being after 20 weeks. However, it is very likely that many women had successful pregnancy outcomes also booked late.
Much more serious, was the number of women (92) who delayed seeking help in labour and many of them arrived in hospital with the cervix fully dilated.
There are likely to be many reasons for women not acting when fetal movements are decreased (71) including lack of transport especially during the night.
Not initiating antenatal care (47) was not common but it was noted that the hospital with the lowest PNMR had the least number of unbooked patients.
Infrequent attenders (45). Along with failure to return on the correct date, we included
delay in going to hospital after referral from a clinic e.g. for ultrasound or hypertension (43). This could be due to not understanding the urgency of action (e.g. gestational aging being only accurate with an early ultrasound or the dangers of hypertension or the lack of resources to get to hospital.)
Administrative avoidable factors Non-availability of transport (63) especially from clinic to hospital
was the main problem. In one clinic, the ambulance was called at 09h00 for a primip with a cervix which was almost fully dilated – eventually it arrived at 20h30 by which time the baby was dead and the patient gave a history suggestive of a vesico-vaginal fistula. Hiring private transport at night can cost up to R300; in the rural areas under discussion, distances are long and transport is often not readily available even during the day.
Shortage of nursing staff (58) is becoming an increasing problem in rural areas. This is partly because of the lure of higher salaries overseas, as well a fairly high death and retirement rate. It is
220

impossible to provide optimal care for sick antenatal patients where staff-nurses provide most of the care and are rotated to different wards on a monthly basis. Monitoring patients in labour requires an adequate number of skilled and experienced staff.
It was disappointing that lack of RPR results is still occurring (38) though fortunately syphilis is not a common problem in pregnancy in the areas served by these hospitals. On-site testing by midwives in clinics has been suggested but at the moment a suitable method is not available.
Many of the neonates who died (20) were transferred from clinics and were cold when they arrived at the hospital. The increased use of kangaroo mother care should considerably improve this situation.
Lack of equipment and drugs (20) included sphygmomanometer and means of inducing labour.
Commonest health personnel avoidable factors Undetected fetal distress was the commonest finding (84). This
included babies born covered with meconium, or with an Apgar score of <3 at 5 minutes and where there was no indication of any problem prior to delivery.
Poor management of hypertension (69) is a problem at both hospital and clinic level. Problems found varied from a primip with a BP of 140/200 being asked to return after a month, patients with severe PIH being allowed to go post dates as well as poor intrapartum management of hypertensive patients.
Problems with the use of the partogram (61) have been grouped together. Diagnosing labour and deciding when to start the partogram create difficulty but correct plotting and interpretation are major problems. Sometimes a partogram was started in the clinic then ignored on admission to hospital.
No response to history (46) applied not only to previous perinatal loss but also to patients with previous C/S who were often not
221

referred to the High Risk Clinic or were not identified as high risk on admission to hospital.
Poor neonatal care (43) included poor resuscitation, poor management after delivery (one baby was left on a wet towel on the Resuscitaire and no one noticed he was no longer breathing) and poor management planning.
Incorrect use of CTG (35) included a CTG not being done for high-risk patients on admission or during labour as well as incorrect interpretation and lack of action on abnormalities on the trace.
No response to poor symphysis fundal growth (30). SFH is not always recorded, or if recorded there may be no referral or consultation about poor growth.
Delay in calling the MO or ADM (29) we found to be much commoner than no response to the call.
Incorrect use of ultrasound (25) refers to an ultrasound being done before 20 weeks then ignored in calculating gestational age as well as no action on significant finings (e.g. decreased liquor).
No action on prolonged second stage (17). Incorrect management of trial of scar (TOS) (15). This included
poor monitoring in labour or no action taken when the action line was crossed. During the study period, three patients having a TOS had a ruptured uterus.
Conclusion and recommendation1. PATIENT
With regard to patient related avoidable factors, the occurrence of late booking, delay in seeking help and delayed response to decreased fetal movements is influenced by the fact that rural women are disempowered in decision making and have many barriers that prevent access to resources. In order to reduce these problems community structures have been involved. e.g. Traditional Birth Attendants (TBA), Community Health Workers (CHW), Community Health Committees (CHC) and forums, as well as
222

men as partners in childbirth. It is hoped that these linkages between the health-workers and the community will improve communication of these concerns. In a focus group discussion held with men in one of the districts, they cited their role in childbirth as financial providers to meet expenses incurred including visits to clinics/hospitals, and provision of transport and of clothes for the newborn.
223

2. ADMINISTRATIVE FACTORSThe most important avoidable factor was delay in getting emergency transport. The problem of delays in ambulance services must be tackled in 3 ways:a. Convince the ambulance services that some obstetrical
emergencies are red code.b. Ensure that the clients and their families take some
responsibility in planning for labour during the 9-month pregnancy period.
c. The community responsibility is to make sure that transport can have accessed without fear of hijackings and that it is available at reasonable cost
Staffing problems are also a very important administrative contribution to avoidable perinatal death. Is it possible for the Priorities in Perinatal Care forum to play an advocacy role for better working conditions for staff in rural hospitals?
3. HEALTH-WORKER FACTORS Some of the health-worker related factors are being attended to with the help of the MCWH sub-directorate in our province using tools such as PEP, protocols in each facility, appropriate manuals, and perinatal mortality audit meetings using PPIP. Appropriate training programmes for midwives are being supported e.g. DEPAM, PEP, the safe-motherhood initiative and kangaroo mother care.Community service doctors are making an important contribution but they need to be better prepared for the responsibility awaiting them in the rural hospitals.
224

PERINATAL MORTALITY AT MIDWIFE OBSTETRIC UNITS: A REVIEW OF 9 YEARS: 1993 – 2001.
DH GreenfieldNeonatal Medicine, UCT
IntroductionThe Midwife Obstetric Units (MOUs) are the primary care arm of the Peninsula Maternal and Neonatal Service (PMNS). They were established in 1972. Medical input by doctors is on once or twice weekly visits to provide a clinical service, and in regular audit, educational and support activities.
MethodsReasonably accurate data is available on perinatal deaths at the MOUs since 1993. All the perinatal deaths from 1993 to 2001 were assessed. Perinatal and neonatal mortality rates were calculated, and the primary obstetric and neonatal causes and avoidable factors recorded. All perinatal deaths occurring at the MOU, or in infants arriving at the MOU having been born at home, were evaluated.
Results
Table 1 Perinatal Mortality Rates
Annual Deliveries: 11164 to 13379 ( total = 122 657)
BW > 499g BW > 999gMean SB Rate 7.2 / 1000 4.2 / 1000Mean NND Rate 3.7 / 1000 2.1 / 1000Mean PNM Rate 10.9 / 1000 6.3 / 1000
The perinatal and neonatal mortality rates are low and did not change significantly over this time period.
225

Table 2 Primary Obstetric Causes of Death
Cause BW > 499g BW > 999gn % n %
Spontaneous preterm labour 539 33 185 15Intrapartum hypoxia 243 15 266 22Infection 224 14 188 15 Syphilis 132 8 118 10Intrauterine growth restriction
196 12 141 12
Unexplained intrauterine death
178 11 135 11
The main cause of perinatal death in infants, with a birth weight of 1000g or more, is intrapartum hypoxia. This is a matter of concern as it should be largely preventable. Most of the hypoxia was labour-related. It appeared that there was a decline in the numbers until 1997, after which they increased again. (see graph below: Perinatal Deaths – Intrapartum Hypoxia) It was about this time that vigorous recruiting for South African nurses to work overseas was started. There was a significant drop in the numbers of deaths due to infections, this being mainly due to the improvement in the management of syphilis in pregnancy (see below: Neonatal Deaths – Syphilis).
226

Table 3 Final Neonatal Cause of Death
Cause BW > 499g BW > 999gn % n %
Immaturity 281 40 81 17Hypoxia 214 31 207 43Infection 74 11 71 15Syphilis 29 4 34 7Congenital Abnormality
69 10 60 12
The commonest cause of neonatal death in infants over 1000g during this period was hypoxia, accounting for 43% of the deaths. This occurred in spite of on-going in-service training, which dealt with the use of the partogram and resuscitation of the newborn. The upturn in the numbers of deaths due to this cause could be related, to some extent, to the loss of numbers of midwives, many of them experienced, to places overseas.
There was a dramatic drop in the number of neonatal deaths due to syphilis after 1993. This was due to the introduction of a system of getting VDRL results back to the MOU on the same day that the patient booked, and before she went home. Subsequent to this, there has not been a neonatal death from syphilis in a patient who has booked.
Table 4 Avoidable Factors
NPatient Related 221Inadequate antenatal care 124Delay in coming in labour 76Inappropriate response to decr. FM 16
Health Worker Related 90Monitoring in labour 35
Administrative 21Transport 15
227

The patient-related avoidable factors may well be a reflection of socio-economic and other conditions in the community rather than the “patients fault”.
Health worker related factors were often associated with “hands-on” clinical skills not being up to standard. Inadequate monitoring in labour, in whatever form, was the most common problem.
ConclusionsTimely availability of the results of syphilis testing have resulted in a significant reduction in deaths due to this disease. Many of the deaths from intrapartum hypoxia and immaturity should be prevented by careful antenatal and intrapartum care and improved resuscitation, and care of the low birth weight baby. Many of these interventions are simple, but do require the acquisition of a few basic skills.
228

PERINATAL MORTALITY AT LYDENBURG HOSPITAL – CHANGING PATTERNS OVER A FOUR YEAR PERIOD FROM 1996 TO 1999
NM Soodi*, NP Godi#* MCWH Co-ordinator, Lydenburg Sub-district, #Mpumalanga MCWH Programme Manager, Nelspruit
IntroductionThe Perinatal Problem Identification Programme (PPIP) was started in Lydenburg in 1996. There has been an ongoing perinatal audit since then. There have been weekly perinatal mortality meetings held at this hospital. Regular feedback was given to the service providers (referring clinics). This was done during the monthly Primary Health Care meetings. A referral system for high-risk pregnancies and neonates was established between Lydenburg and Middelburg/Witbank Hospitals. There has been an obvious change in trend in the perinatal mortality and PPIP statistics over the years. We are looking at the PPIP data from 1996 to 1999 to highlight the changing patterns.
MethodA review of Lydenburg Hospital PPIP data forms and statistics from 1996 to 1999 was done. We looked at the following parameters for our analysis and comparison: Total deliveries and PPIP classification of final causes of deaths and avoidable factors (medical personnel, infections, unbooked patients, RPR not done, low birth weight, fresh stillborn, macerated stillborn, administrative problems, missing files and Asphyxia and birth trauma and the WHO perinatal mortality rates >1000g).
ResultsThere has been a gradual increase in the total number of deliveries and a gradual decrease in the perinatal causes of deaths as classified by PPIP. The perinatal mortality rates for >1000g for the four year period are as follows:
WHO PNMR>1000g 1996 44.7/10001997 28.2/1000
229

1998 44.6/10001999 30.7/1000
230

1996 1997 1998 1999Total Deliveries 1034 1177 1211 1698Medical Personnel 80.0% 65.3% 51.8% 45.5%Infection 21.1% 12.1% 8.0% 8.0%Unbooked patient 12.2% 11.1% 8.9% 16.4%RPR not done 90.7% 33.3% 66.1% 32.7%Low birthweight 13.3% 13.2% 12.0% 11.6%Fresh SB 24.0% 40.0% 37.5% 33.3%Macerated SB 76.9% 60.0% 62.5% 58.5%Administrative problems 14.5% 8.3% 7.1% 10.9%Missing files 25.5% 13.9% 3.6% 1.8%Asphyxia & birth trauma 36.8% 33.3% 41.7% 33.3%
ConclusionThe introduction of PPIP at Lydenburg Hospital has brought about improvement in the final causes of perinatal deaths and avoidable factors. The perinatal mortality rates >1000g seem to be fluctuating, a cause for this needs to be looked at.
231

AUDIT OF PERINATAL MORTALITY RATE: EKOMBE HOSPITAL 1994-2000
FA Gonzalez, LJ Blanco
The Perinatal Mortality Rate (PNMR) has being always been a very important indicator to show the advance of any country. In our Hospital we achieved a reduction of the PNMR from 50.9 per 1000 in 1995 to 25.0 per 1000 in 2000. This was possible after the introduction of not very sophisticate or very expensive actions. The early initiation of the antenatal care, early diagnosis of the problem, strong Primary Health Care follow-up of the high-risk patient, ultrasound, early admission in the ward or in the Waiting Mothers area especially for multiple pregnancies as early as 28 weeks, reduction of home deliveries, and others that we will explain later has made possible such a huge reduction of the PNMR in our very isolated rural hospital.
The objective of the study1. To show the reduction of the PNMR at Ekombe Rural Hospital during
5 years (1996-2000) as compared with previous years.2. To analyse the results of the different components of the PNMR.3. To identify Perinatal Mortality in relation to birthweight.4. To show the number of the newborn per year, for the last 7 years.
MethodsA prospective and retrospective study was done about the Perinatal Mortality Rate (PNMR) occurred in Ekombe Hospital during a period of 5 years (1996-2000). We also look at two years before (1994-1995) with the purpose of making some comparison to the reduction of the PNMR.The primary data was taken from the Ekombe Hospital birth and death registers and placed in a data sheet created specifically for this study.All the data collected were analysed in tables and graphics. The results are shown as well as the conclusion and recommendations.
232

DiscussionThere has been a huge but gradual reduction in PNMR at Ekombe Rural Hospital in the last five years, from 50.9 per 1000 newborns in 1994 to 25.0 per 1000 newborns in the year 2000. The best years were 1997 with 24.4/1000; 1998 with 22.0/1000 and 1999 with 23.8/1000.One study was performed in the Josini Health District in KZN where the PNMR was also audited in 4 different hospitals. The highest PNMR was found at Bethesda Hosp with 41/1000 and the lowest at Mosvold Hospital with 24/1000.The main causes of deaths found in the above-mentioned study were similar to our environment (asphyxia and births trauma, prematurity, congenital abnormality and sepsis) although we are not given any data about these.According to Dr Larsen a PNMR less than 25/1000 newborns for small and isolated rural hospital is a very good indicator of the work done.Beside the all difficulties found to achieve those results (e.g. very poor condition of the roads; long distances to the hospital, lack of transport; lack of health education, poverty, malnutrition, etc) the results obtained were possibly due to the following aspects:1. Commitment and dedication in the daily obstetric work and also
good team spirit.2. Better use of the hospital beds for early admission of the high-risk
patients as well as better use of the waiting mother area for low risk and for those at term but with transport problem.
3. The use of the ultrasound for the early diagnosis of obstetric problems as well as congenital malformation.
4. Early admission of all multiple pregnancies as early as 28 weeks.5. The reduction of the home deliveries.6. Huge improvement in antenatal clinic attendance.7. Improvement in the number of patient who starts early antenatal
care during the pregnancy.
233

Conclusion1. There was an increaset in the number of newborn as from 1996.2. There was a reduction of the absolute number of stillbirths and
neonatal deaths.3. More than 50% of the stillbirths weighed more than 2500grs and
majority were Macerated Stillbirths.4. The PNMR has being gradually decreasing since 1994 (50.9/1000) to
(25.0/1000) in the year 2000.
RecommendationWe have the opinion that the PNMR can see further reduction in this rural hospital, if we consider the following aspects:1. Early detection of pregnancy and early initiation of antenatal
care.2. To achieve at least 8 antenatal clinic visit in every patient.3. Early diagnosis of congenital malformation between 19-24 weeks
of pregnancy using ultrasound.4. Early admission to the hospital of the multi-pregnancy (28 weeks).5. Strict control of the high-risk patient and also early admission to
the hospital for waiting mothers (36 weeks)
Table 1 Maternity Statistic Ekombe Hospital.1996-2000 Year 1994 1995 1996 1997 1998 1999 2000N.V.Ds 870 711 933 881 938 891 760New Born 873 716 1005 967 1028 987 820Twin 15 8 11 18 17 13 12L.B.W. 114 80 105 78 89 98 93M.S.B 12 8 22 8 12 14 9F.S.B. 12 10 9 10 4 5 9N.N.D. 21 10 9 6 7 5 3Total Death 45 28 40 24 23 24 21P.M.R. 50.0 43.9 38.6 24.4 22 23.8 25L.W.B. (Index) 13 11.2 10.4 8 8.6 9.9 11.3/S 64 74 77 99 60
Table 2 Fresh Stillbirths, Macerated Stillbirths and Total Stillbirths at Ekombe Hospital.1994-2000
234

Year 1994 1995 1996 1997 1998 1999 2000M.S.B 10.00 7.00 22.00 8.00 12.00 14.00 9.00F.S.B 11.00 10.00 9.00 10.00 4.00 5.00 9.00T.S.B 21.00 17.00 31.00 18.00 16.00 19.00 18.00
Table 3 Weight of the foetus and Neonatal Death at Ekombe Hospital. 1994-2000
Weight in gm 1994 1995 1996 1997 1998 1999 20001000-1499 7 (16%) 9 (28%) 5 (12%) 1 (4%) 3 (13%) 5 (21%) 1 (5%)1500-1999 5 (11%) 3 (9%) 7 (17%) 2 (8%) 4 (17%) 5 (21%) 4 (19%)2000-2499 3 (7%) 3 (9%) 5 (12%) 6 (25.5%) 4 (17%) 4 (17%) 3 (14%)2500-2999 11 (25%) 7 (22%) 9 (23%) 3 (12%) 4 (17%) 3 (12%) 3 (14%)3000 and + 12 (27%) 7 (22%) 12 (30%) 12 (50%) 8 (35%) 7 (29%) 10 (48%)Unknown 6 (14%) 3 (9%) 2 (5%) 0 0 0 0
Total44 (100%)
32 (100%)
40 (100%)
24 (100%)
23 (100%)
24 (100%)
21 (100%)
Table 4 Neonatal Death Weight <2499 grs and >2500 grs at Ekombe Hospital. 1994-2000
Year1994
1995
1996
1997
1998
1999
2000
Weight < 2499 grs 15 15 17 9 11 14 8Weight > 2500 grs 29 17 23 15 12 10 13Total Neonatal Death 44 32 40 24 23 24 21
235
SURVIVAL OF PREMATURE VERY LOW BIRTHWEIGHT INFANTS BORN AT MADADENI DISTRICT HOSPITAL – A 9 YEAR REVIEW
FS Bondi
IntroductionFewer than a third of all infants born outside the private sector in South Africa have access to NICU. Also, in the public service, NICUs are largely limited to academic hospitals and regional referral centers. Since most babies are delivered outside these areas, we found it necessary to provide information on the survival rate of the more immature infants (below 1.5kg) in a peripheral hospital. This category of babies was chosen because they are more likely to require ventilation and other forms of intensive therapy. Our primary objective was to determine the outcome (survived or died) of babies weighing 1499g or less in the absence of a NICU.
Subjects and MethodsThis study is based on 758 infants weighing less than 1.5kg, who were delivered in our facility or were sent from the adjoining clinics (BBAs). Data was obtained retrospectively and manually, from the admission records of our nursery covering the period 1993-2001 (nine years). Earlier information was poorly kept and was thus excluded from this series. The information abstracted from the notes included, birth weight, duration of admission (up to the time of discharge or demise) and whether the infant survived or died. No effort was, however, made to unravel the causes of deaths, as no postmortems were performed and for various reasons, the records of laboratory investigations were unreliable.
ResultsOverall AdmissionsThere were 22 262 admissions into our nursery during the study period, of which 2152 (9.7%), 758 (3.4%) and 191 (0.9%) were babies weighing <2.5kg (LBW), <1.5kg (VLBW) and <1.0kg (ELBW) respectively. This
236

study focuses on the 758 VLBW babies. Figure 1 depicts the birthweight-specific distribution of these cases. There were 321 boys and 437 girls (M:F=1.0:1.4). One hundred and twenty-five were BBAs while the remaining 633 or 83.5% were inborn. There were 75 sets of twins and a lone set of quadruplets. In 16 of the 75 sets of twins, the other twin weighed 1.5kg and above and were thus excluded from this analyses.
From 1999, low apgar (<6) and respiratory distress were documented in 93 (37.3%) of the 249 VLBW babies.
DeathsOf the 22 262 admissions into the nursery from 1993 to 2001, 1061 (4.8%) died and 598 (56.4%) of the fatal cases were VLBW. Thus, despite the fact that VLBW infants accounted for only about 3% of the entire admissions they were responsible for over half of the deaths. A majority of the fatalities occurred within 24 hours of birth (380 of 598, 63.5%). Of note, also, is that 108 of the 125 (86.4%) VLBW who were BBAs died.
SurvivalsOnly 160 (21.1%) of the 758 VLBW infants in this report survived. Also, while there were no survivals for babies below 0.8kg, survival in those weighing between 1.4 and 1.499kg was about 40%. When the yearly survival was examined, it varied between 17.1% and 30.2% with our best results being 1995 (28.6%) and 2001 (30.2%). Another interesting finding was that 46 babies survived for over a week before dying. With respect to the infants who survived long enough to be discharged at 2.0kg, their hospital stay varied between 17 and 110 days, with only 23 of the 160 (14.4%) survivals staying for less than 28 days.
DiscussionRecent reports from South Africa indicate that the survival rate (SR) of very low birth weight infants is good. In some series, 9 in 10 of these babies have survived. However, these studies were based on babies
237
cared for in sophisticated NICU and little attention has been given to the fate of similar infants in circumstances of sparse resources. This study is an attempt to provide a broad overview of the SR of 758 babies in a level 2 nursery, without ICU facilities. Only 160 of the 758 (21%) cases involved in this report survived. This contrasts sharply with SR of up to 90% in the national series. Deaths in this investigation occurred particularly soon, as 60% were within 24 hours of birth. It is likely that this subgroup of babies would have benefited from artificial ventilation and other forms of intensive care. Our contention is supported by the fact that the more immature babies (ELBW) are the least likely to survive.BBAs were another vulnerable group. Only 17 of the 125 (23.6%) outborn babies survived and this we have attributed largely to problems of hypothermia and sepsis. At best, BBAs reach our nursery wrapped in cotton wool and aluminium foil and it is not uncommon for such infants to be delivered in the taxi en route to our unit.There were 46 babies who survived well beyond the first week of life but subsequently demised. Whilst it is difficult to explain these ‘late’ deaths, it is not unlikely that accelerated HIV infection has a role to play. Also, we have noted that in our nursery, some of these deaths are due to aspiration of feeds.
The findings in this study suggest that the survival of VLBW infants in remote hospitals is poor and this probably reflects the picture in a large majority of our public institutions. There is need for some form of decentralization of neonatal services. However, in the short term, the use of anti-retroviral therapy for the PMTCT of HIV and the implementation of the kangaroo mother care programme are being actively pursued in KZN.
238

SAVING BABIES: A PERINATAL CARE SURVEY OF SOUTH AFRICA 2001
RC Pattinson and PPIP UsersMRC Unit for Maternal and Infant Health Care Strategies, University of Pretoria
Aim1. To estimate a national perinatal mortality rate (PNMR) and to identify
the major causes of perinatal mortality and related avoidable factors, missed opportunities and substandard care in South Africa.
2. Recommend strategies to reduce the PNMR based on this information. SettingAll provinces in South Africa gave input, where possible, into the PNMR in their particular provinces. Furthermore, 44 state hospitals throughout South Africa representing metropolitan areas, cities and towns, and rural areas were the sentinel sites for the documentation of the causes of perinatal death and the avoidable factors associated with the deaths.
MethodThe Provincial Health Information Sections and the Maternal, Child and Women’s Health units of the provinces presented their available data. Users of the Perinatal Problem Identification Programme (PPIP) amalgamated their data to provide descriptive data on the causes of perinatal death and the avoidable factors, missed opportunities and substandard care in South Africa and comprised the sentinel sites. The sentinel sites were grouped into metropolitan, city and town, and rural areas. The metropolitan grouping reflects urban areas and a fully functioning tiered health care system with ready access to tertiary care. The city and town grouping reflects functioning primary and secondary levels of care, with limited access to tertiary care, and the rural grouping reflects primary care, with less accessibility to secondary and tertiary care.
239

ResultsSome provinces have developed effective data collection systems at the time of the workshop and were able to provide accurate data for their whole province regarding births and perinatal deaths within state institutions. Accurate data was available for Gauteng and the Western Cape. The PNMR for Gauteng was reported as being 32.1/1000 births and for Western Cape reported as 18.4/1000 births.
A total of 3045 perinatal deaths of 1000g or more were reported from 78 343 births at the sentinel sites. The perinatal mortality rates for the metropolitan, city and town and rural groupings were 38.4, 43.4 and 25.5/1000 births, respectively. The neonatal death rate was highest in the City and Town groups (16.5/1000 live births) followed by the Rural and Metropolitan groups (11.1 and 10.7/1000 live births respectively). The low birth weight rate was highest in the Metropolitan group (21.4%), followed by the City and Town group (18.6%) and the Rural group (13.7%).
Unexplained intrauterine deaths were a common grouping of primary cause of death in all groups. The most common primary cause of perinatal death in the Rural group was intrapartum asphyxia and birth trauma (rate 6.28/1000 births) followed by spontaneous preterm delivery (6.07/1000 births). The most common primary cause of death in the City and Town group was spontaneous preterm delivery (7.48/1000 births) followed by antepartum haemorrhage (7.0/1000 births) and intrapartum asphyxia and birth trauma (6.8/1000 births). The Metropolitan group’s most common primary causes were antepartum haemorrhage (6.82/1000 births), spontaneous preterm labour (5.33/1000 births) and complications of hypertension in pregnancy (5.19/1000 births). Neonatal deaths due to complications of prematurity and hypoxia were the most common final neonatal causes of death in all groups.
240
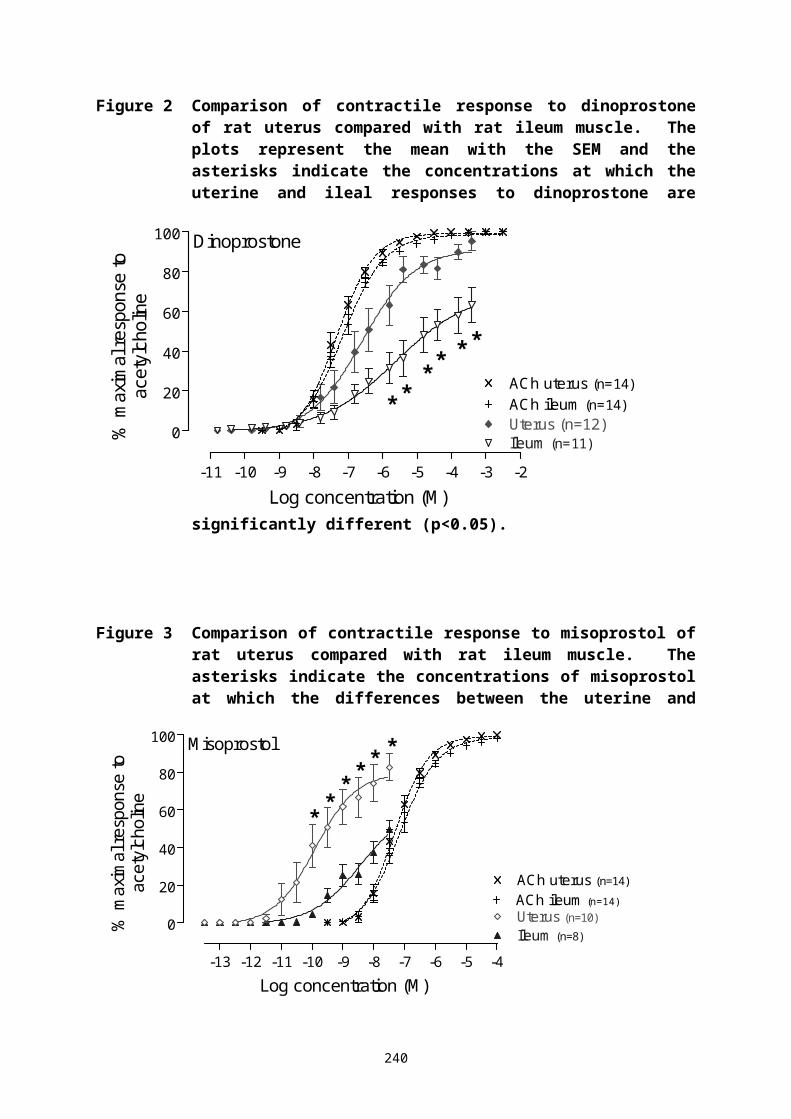
Patient-related avoidable factors were reported to be present in 39.3% of perinatal deaths, followed by health worker-related (24.6%) and administrative (14.0%). Lack of sufficient information to evaluate the case was present in 5.1% of cases. No, late initiation or infrequent attendance for antenatal care (present in 688 cases) was the most common avoidable factor. This was followed by an inappropriate responses by health workers to problems identified during antenatal care (305 occasions); inappropriate response by patients to poor fetal movements (227 occasions); delays in seeking medical attention during labour (177 occasions); delays in referring patients or calling for assistance (173 occasions); transport delays (162 occasions) and problems of monitoring the fetus during labour (106 occasions).
ConclusionsThe current data is sufficient to state that the PNMR in South Africa is probably in the order of 40/1000 births, and some readily remedial problems have been identified. These are in the structure of antenatal care, management of labour, resuscitation of the asphyxiated neonate and care of the premature neonate. Focusing attention on these readily remedial priority problems, by ensuring that equipment, protocols and trained health workers are always available and by specifically introducing kangaroo mother care for the care of the premature infants, makes the reduction of perinatal mortality in South Africa feasible and inexpensive.
RecommendationsSolutions for improving pregnant women and their baby’s care and reducing the PNMR rate at institutions1. Ensure each site conducting births has the necessary equipment and
protocols and that the staff are appropriately trained to manage labour and are especially trained in the use of the partogram. Introduce a quality assurance tool to assess the success of the training.
241

2. Ensure each site conducting births has the necessary equipment and protocols and appropriately trained staff to manage asphyxiated neonates. See that training programmes in neonatal resuscitation are accessible to all staff involved in conducting childbirth.
3. Ensure each site caring for premature infants has the necessary equipment and protocols and that the staff are appropriately trained in kangaroo mother care. See that implementation programmes are available to the staff.
4. Ensure each site performing antenatal care has protocols in place for where to and when to refer patients and the staff is appropriately trained therein. Introduce a quality assurance tool to assess the success of the training.
5. Move to a system where the time and point at which the woman confirms she is pregnant also becomes the woman’s first antenatal visit where she can be classified according to risk and where her further antenatal care is specifically planned. If this is not practice, establish what barriers there are and attempt to overcome them.
Improve the process1. Continue to establish more PPIP sentinel sites.2. Hold regular Provincial MCWH – PPIP sentinel site meetings.
Research priorities 1. What are the barriers to implementing on-site screening for syphilis?2. What is the primary pathology related to unexplained IUDs?3. What is the feasibility of introducing nasal CPAP for managing
premature infants in cities and towns and rural areas?
Advocacy Valuable information obtained from the Perinatal Care Survey must be conveyed to the appropriate bodies.
242

243

PROCEEDINGS DATABASE: PROCEEDINGS OF THE PRIORITIES IN PERINATAL CARE CONFERENCES (1982-2001)
RV Prinsloo, RC PattinsonMRC Unit for Maternal and Infant Health Care Strategies, University of Pretoria
The Proceedings of the Priorities in Perinatal Care Conferences (1982-2001, including IAMANEH 2000) are available on CD-Rom.
All articles have been indexed and allocated keywords in the Proceedings database (Access 2000). The database is updated annually as the latest Proceedings are published.
Searches can be performed by author, keywords, title (or portion thereof) and by year. These searches can be printed. There are links from the database to the relevant Proceedings. Links can be accessed in the main table of the database.
Articles can then be viewed and/or printed.
The Proceedings will also be available on the Priorities website: www.perinatalpriorities.co.za. Individual Proceedings or the entire database and all the Proceedings can be downloaded from the website. Alternatively searches can be run for people not wishing to download the database by e-mailing the MRC Unit your request.
CDs are available from: MRC Unit for Maternal and Infant Health Care Strategies
Klinikala Building, Kalafong HospitalPrivate Bag x396PRETORIA, 0001Tel/Fax: (012) 373-0825E-mail: [email protected]
244

PERINATAL CHALLENGES AND OPPORTUNITIES IN HEALTH MANAGEMENT
N BergmanMowbray Maternity Hospital, Cape Town.
IntroductionPerinatal care ranks as a priority with our new Government and Health Department, but the resources required do not always match the priority. There is also considerable inequity between the public and private health sectors in South Africa.
Expenditure on health Proportion population PRIVATE 60 % 20%PUBLIC 40% 80%Spending proportion PRIVATE : PUBLIC 6 : 1
Though government policy may say that health is a priority, in reality many health services have seen decreased allocation of resources, in particular formerly “favoured” provinces. The reality in the WC has been a unprecedented/unparalleled decrease in the health sector work force, the loss of manpower experience and expertise, poor morale, falling standards, and aging equipment that is difficult to replace or repair. A medical manager has a formidable challenge maintaining any kind of standard, never mind making improvements. Nevertheless, the political changes have seen policy changes which present opportunities. Revenue retention and decentralized management have become a reality, a major shift in bureaucracy. Following this the Western Cape has encouraged “revenue generating projects”, as a counter to national cuts in budget.
MethodDespite the gloomy picture above, perinatal care in the Western Cape has some strengths. It represents a Primary Health Care system with well-functioning levels of care, it has written protocols under regular review, a well-functioning audit system, and with a perinatal mortality rate possibly
245

the best in Africa. The innovative “method” has been to apply standard business principles to our local context, using existing public hospital space for private patients. OPPORTUNITY is described above, in addition Mowbray Maternity had an unused nurses’ residence. The PRODUCTS are, inter alia, our excellence in terms of clinical protocols, and our 24-hour doctor cover. Our CLIENTS are mothers and babies, and also private midwives. Our MARKET is a clientele disillusioned with exorbitant costs of private care, and the over-medicalised nature of that care (high Caesar rate). THREATS we have to address are primarily related to the client perception of the Quality of Care. WEAKNESSES include our administrative ability to generate and collect fees, and the “perceived poor state” of the hospital should clients need to be transferred for secondary care. The main STRATEGY has been two-fold. The ACTIVE BIRTH UNIT is a facility designed for the use of private midwives to deliver their private clients, with a charge for the use of the facility. The “P” MIDWIFE OBSTETRIC UNIT provides perinatal care to paying patients by public midwives, initially using the ABU facility, but in time in its own space. Both projects function under a DISPENSATION, allowing that we deliver “one tier health care, and temporarily two tier hotel care”. The Province has invested just under two million rand in seed money to launch the above, and the hospital will undergo major renovation in the coming year.
In addition, there has been a conscious consideration and application of a holistic definition of “Quality of care” (lifted from Hulton LA et al, University of Southampton)
QUALITY OF CAREPROVISION OF CARE EXPERIENCE OF CARE
1 Human and physical resources 7 Human and physical resources2 Referral system 8 Understanding of care3 Maternity information systems 9 Attitudes (respect, dignity,
equity)4 Use of appropriate technologies 10 Emotional support5 Internationally recognised good practice
246

6 Management of emergenciesConsiderable time and effort was spent ensuring that all aspects of quality were addressed. In particular, protocols and referral criteria were negotiated with the private midwives, and a Board established to ensure a high standard of practice in the ABU. The actual facility was designed by the same private midwives, to their own requirements. The ABU has three suites, each with double beds, big baths, birthing balls and birthing mats, CD player, candles, and a discrete cupboard with medical equipment for use when needed.The term “Active birth” is variously defined, but is here taken to mean that the facility encourages mothers’ choices and positions, a woman’s control over her own birthing experience (“the primitive brain process”), family participation and celebration in the event, (“de-medicalisation” of birth).Clients pay the Hospital for use of facility, and separately pay the private midwife. The ABU requires no dedicated staffing, and is thus a low-risk operation. It’s success depends entirely on the private midwives using it, and therefore on good relationships. A carrot: obstetric cover for home births and emergencies is provided by the hospital and its medical staff.The MOU section is staffed by state-employed midwives, and clients are charged UPFS (Uniform Patient Fee Schedule), which is lower than private sector fees. Innovative and varied employment mechanisms have been adopted, to meet individual needs of nurses. Extensive use of agencies and flexible contracts allows the workforce to be closely matched to the workload.
The ABU and the MOU provide only primary level care. ABU clients may elect to have secondary care at other hospitals, or use Mowbray, MOU clients are referred to Mowbray. Charges are raised for this secondary care according to the UPFS also.
247

ResultsThe units were operational by September 2001, they are both located in the same section of the old Nurses Home, and can be managed as a single cost center. There had been considerable delays and frustrations, this meant that there were initial delays in the utilisation of the ABU. The use of the MOU increased according to the projections made at the beginning, there being a private client-base within the hospital, and a market that had been identified beforehand.“Critical success factors” that have been attended to include a focus on the role and status of the midwife, ensuring job satisfaction and development, and autonomy within the clinical management protocols of the PMNS. There has been ongoing advertising and marketing, working with various media and with medical schemes. Fees and income procedures have been improved, and the income generated has been recycled on an ongoing basis, with some amounts being used for ongoing improvements of infrastructure and equipment. By matching workforce to workload, there has, at no stage, been an operational deficit after the launch phase.
Improvement in quality of care has been an objective from the beginning. With private midwives following their clients when referred for secondary care, numerous issues with respect to patient perception of care have been highlighted and have been remedied or improved. For every private patient admitted, an agency nurse was allowed to be called in, which cost half of what the client paid, but allowed improved care for the public patients, and took the pressure off the hospital midwives. Morale rapidly improved as a result, with further gains in quality of care in the main hospital.
Conclusions (perinatal health management priorities)The specific context of Cape Town and the service provided by the hospital has to a large extent determined the solutions that have been made. Replicating the above in another context may not work at all. Using
248

the above purely as an example, some general principles that might be extracted as generally applicable could include:
# Aim at bigger pie, and a bigger slice of the pie (the national allocation to health).Maternal and Child health is a priority, and deserves more funding!
# Supplement the size of the slice Example - ABU and PMOUidentify the strengths that exist, invest in their optimal use to make
revenue.# Focus on the human resource Example - status of midwife
midwives and nurses have been neglected, their job satisfaction is paramount.Apply flexibility and innovation with respect to working hours,
schedules.# Use all resources actively, efficiently and effectively
Immediate use of income decentralization and revenue retention are practical and possible, and give rapid returns in all sorts of respects, deserve full support of Provincial Governments.
# Continue development of excellence Protocols and innovations
Clinicians, midwives and medical managers need to work closely together, not just to overcome the major challenges that are there, but to develop and improve our care.
249

THE EFFECT OF INVOLVING PRIVATE PRACTITIONERS ON THE QUALITY OF ANTENATAL CARE OF THE INDIGENT POPULATION OF TEMBISA
KR Mokhondo, RC Pattinson, AE Pullen, AK Tshabalala, T Chaane, R van der Walt, M ModiseMRC Unit for Maternal and Infant Health Care Strategies, University of PretoriaKhayalami Independent Practitioners AssociationGauteng Department of Health
IntroductionThe perinatal mortality rate in Tembisa is unacceptably high at 50/1000 deliveries. Private practitioners are evenly distributed throughout the township of Tembisa whereas the public sector has only one clinic in the settlement and one in the hospital performing antenatal care. The majority of women confirm their pregnancies with General Practitioners (GPs). The earlier the intervention is started the better the outcome of pregnancy. New initiatives are required to address this problem in order to save the lives of mothers and babies. Incorporation of the GPs might achieve this. A public-private health partnership was created to investigate the accessibility and quality of care of pregnant women.
Study design A cohort analytical study.
Preparation for the studyThe Gauteng Provincial Antenatal Care Policy Guidelines were distributed to the GPs, hospital doctors and midwives. Study PopulationTwo hundred pregnant women of the indigent population of Tembisa were included in the study. The women were divided into two groups: Group A included women in GP care and Group B women in Standard Clinic care.
250
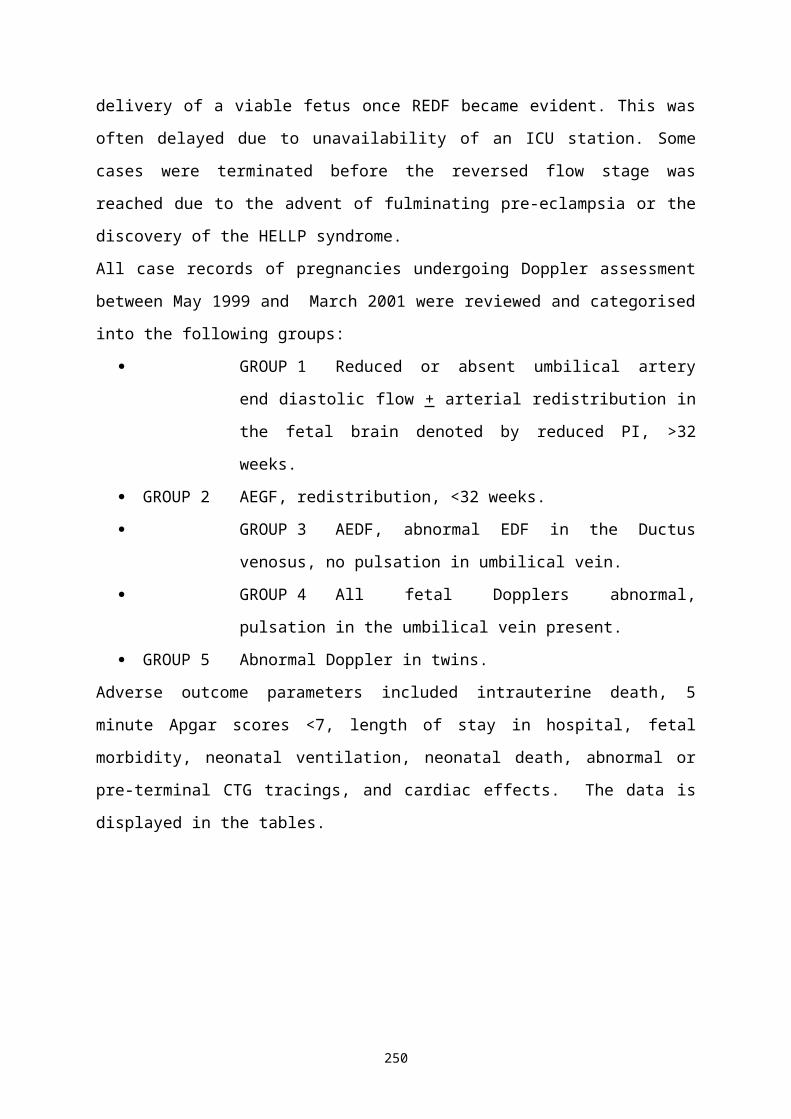
Data CollectionAll motherhood cards were collected upon delivery at Tembisa Hospital and the pregnancy outcome recorded and evaluated.Outcome Measures: The gestational age at the initiation of antenatal care. The quality of antenatal care.
ConclusionThe results of the study will be presented.
251

A COMPARISON BETWEEN FOUR MIDWIFE OBSTETRIC UNITS IN THE PRETORIA REGION
NT Mabale, C van der Westhuizen, RC Pattinson,MRC University for Maternal and Infant Health Care Strategies, Kalafong Hospital and University of Pretoria
IntroductionMidwifery obstetric units (MOUs) have been established in South Africa in response to the health needs of pregnant women. Although various types of MOU’s currently exist, the function of the MOU and the quality of midwifery care rendered, have never been documented. This study, aimed at describing and comparing four different types of MOU’s in the Pretoria region, will contribute toward providing an evidence base needed for effective policy-making. We believe that MOUs should play an important role in the reduction of material mortality and morbidity.
Methods and proceduresA comparative descriptive design is followed to reach the aim of the study. Triangulation of data collection methods are used to ensure a rich description of the functioning of MOU's and quality of midwifery care rendered. The checklists and interview guides used, are the following: checklist for ward statistics (current formats used in the units, together with Guidelines for Maternity Care in South Africa [Department of Health 1999]); interview guide (Unit managers); interview guide (patient satisfaction and reasons for by-passing MOU's); and analysis of partogram.
A sample of four MOU's in the Pretoria Region is chosen purposively because of their unique characteristics resembling four different types of MOU's. Systematic random sampling is used to select patient records with a total of 50 records needed from each MOU. Admission books and delivery records, MOU's guidelines, procedural/protocol documents, inventories of facility's equipment, stock and supply records are audited. To determine patient satisfaction, patients are selected at random in the
252

postnatal wards. Patients by-passing the MOU are identified at the nearest hospital and interviewed in a non-random fashion, because of the problems of following-up these patients.The content validity of the checklist for ward statistics is based on the current format used in the units as well as on the Guidelines for Maternity Care in South Africa (Department of Health) and was tested during a pilot study. The interview guide (unit managers) is structured according to the study objective and was tested during the pilot study. The interview guide (patients) is based on an instrument developed by Steyn (1998) to access patient satisfaction with antenatal care, has been adapted for the purpose of the study and was tested during the pilot study. Analysis of partogram: an instrument developed by the MRC Unit for Maternal and Child Health Strategies is used. Strategies to ensure trustworthiness of data collection on and analysis are based on the model of Guba and Lincoln.
Descriptive and inferential statistics, as well as Tesch's approach towards the analysis of qualitative data is used to examine differences between the four MOU's. Within the scope of this study the researcher does not intend to generalise the findings.
ConclusionA preliminary report of the study was presented at Priorities in March 2001. The findings and recommendations will be presented.
253

EXPERIENCES IN USING A MULTIDICIPLINARY APPROACH IN THE DEVELOPMENT OF QUALITY MATERNAL HEALTH SERVICES IN A DEEP RURAL AREA.
S MbamboDistrict Co-ordinator For Maternal Child and Women’s Health in DC 26, KZN.
IntroductionThe aim was to set and provide a sustainable health service system that would address the needs of the people that would then result in reduced maternal and Perinatal Mortality rate in the district.
Special attention was paid to: Antenatal care, Intrapartum care, Neonatal care, Post-natal care, Competence of health care workers.
Problems encounteredFragmentation within the health service leading to: Incomplete/faulty data was collected. Poor team spirit among health professionals e.g. midwives, doctors,
laboratory technicians, pharmacists, transport officers, clinic staff, hospital staff, etc.
Limited supervision at all levels. Frequent staff turnover. Inadequate numbers of personnel due to brain drain (especially
professional nurses). Lack of critical thinking and decision making by health workers due
to lack of vision and leadership.
254

Partners in service delivery: Policy makers, Health managers, Health professionals, Academic institutions, Communities.
Strategy One partner not mentioned above is NGO’s e.g. CHESS, who was
involved in the facilitation of the programme in our district. A women’s Health Management Team was built in each area and
key role players are seen in the organisational structure of the Maternal Health Care programme.
These teams worked with Community Health Workers as a means of community involvement.
The Chess facilitators and the MCWH co-ordinator visit each area to assist in running Perinatal review meetings and to conduct workshops. These workshops take place monthly.
Available resources like guidelines and protocols, PEP and the introduction of the ANC package were all used in order to improve efficiency in staff performance.
Sessions of perinatal and professional development during monthly workshops helped in boosting confidence and self esteem especially among midwives.
Women’s health teams from each area were linked to form a sub-district team. Sub-district teams were also linked to form a District Women’s Health Management Team. This was made possible by choosing a district co-ordinator for Maternal, Child and Women’s Health. In this way, the district programme was strengthened.
General practitioners and private sector were also included, therefore our PMR include:
o Hospital deliveries,o Clinic deliveries,
255

o Private hospital deliveries,o Home deliveries, ando Babies born before arrival at health centres.
Results The building of women’s health temas has helped to improve
the team spirit among health workers. In one of the sub-districts an AGM has been tasked to visit
clinic midwives on a regular basis to support them, do on the spot training and to act as a consultant if there are high-risk clients.
Twenty three midwives in the district have registered for PEP, none have completed the programme though.
In all 5 sub-district hospitals, PPIP has been installed and is used to find the causes of each perinatal death and to deal with avoidable factors.
Women’s health teams are working with CHWs, TBAs and clinic committees as these are community representatives and they know what the community needs.
The district information system has improved since each sub-district has a sub-district information officer and they all send their statistics to the district information officer who sends it to the province.
Training of trainers for on-site RPR testing will start on 17 March 2002 and this will help in getting the blood results on the 1st
visit and if necessary treatment will be commenced on the same day.
ConclusionIn 1999 the PMR was 66/1000. In 2001, the cumulative for the district is 36/1000 that is almost a 50% decrease in the PMR in 2 years.
256

EXPERIENCES WITH COMMUNITY PARTNERSHIP IN CHANGING HEALTH SEEKING BEHAVIOUR IN DEEP RURAL AREAS
BR NtsuntshaNkonjeni Hospital Mahlabathini – Ulundi
IntroductionPerinatal review identified hypertension as a major cause of perinatal deaths. Data showed that only 3,2% of ANC clients attended ANC before 20 weeks of pregnancy. A community partnership approach was agreed upon with an objective of reducing P. I. H. related perinatal deaths, by increasing the number of women attending ANC for the first visit before 20 weeks of pregnancy.
Method• Mobilization of the Community Health Workers (CHWs) to motivate
the traditional birth attendants (TBAs) to come forward and work with health workers.
• Meetings and workshop with the traditional birth attendants for strategic and operational plans to achieve the objective.
• Empowerment of the community on health seeking behaviour through house–to–house visits, presenting talks in community meetings, church and community gatherings as well as in schools on the importance of antenatal visits before the 20th week of pregnancy.
• Feedback was provided to CHWs and TBAs on community-response based on ANC attendance in each clinic from the very first month of the programme.
• Provision of positive feedback to the people who performed well. ResultsANC booking before the 20th week of pregnancy has improved by 14.8% in the first 5 months of the programme.
257

ConclusionThe projected improvement over one year is 35,5%. The positive results are increasing commitment and motivation within the team.
258

MPUMALANGA MCWH CLINICAL SKILLS CAPACITY AUDIT(CCA) 2000 REPORT
NP Godi Mpumalanga Provincial MCWH Programme, Nelspruit
IntroductionAn audit of clinical skills capacity was done in all the 27 public hospitals in the province. The maternal and women’s health unit of the maternal child and women’s health team audited those skills which the team deemed essential and necessary for the rendering of basic, safe and standard obstetrics, perinatal and gynaecological care services. This audit was an attempt to identify problem areas in the rendering of the above-mentioned health care services. The audit team was expected to come up with recommendations to be implemented in order to address and improve the health care service delivery as referred to above. The audit took place from the 08/02/2000 to 13/04/2000. The hospitals visits took 13 days to complete.
MethodA questionnaire was used to interview maternity, neonatal and gynaecology unit staff and to make personal observations on site during the interview visits. The questionnaire tried to address some of the following: antenatal care practice, obstetric procedures and some equipment, labour management, audit processes, personnel/staffing of unit, obstetric anaesthesia and anaelgesia, women’s health services and the referral network.
Findings/ResultsSome of the results are presented.Eleven hospitals had antenatal care clinics on site. Three of these had a high risk obstetrics clinic. None of the hospitals had medical obstetrics clinics. There were only 7 hospitals where syphilis testing and treatment was done on the same day.
259
Perinatal and maternal morbidity and mortality meetings and audit were taking place in 15 and 11 hospitals respectively. There were only 4 hospitals which were implementing the PPIP programme.Cardiotocograph (CTG) machine availability was as follows, 17 hospitals had all their machines in a working order (6 of these had one each, included here is the province’s main referral hospital, the remaining hospitals number of machines ranged from 2 to 8). Four hospitals had half their machines in working order (they had 2 CTG machines). There were 2 hospitals with all their machines out of order and 3 hospitals with no CTG machines at all.
There were three types of labour graphs in use in the different regions/districts. We did not scientifically assess the correct use of the labour graphs but the overall impression was that of a general lack of the skills or willingness to complete the labor graph properly.
Spinal anaesthesia was utilised in 17 hospitals. No epidural anaesthesia services were available in the public service hospitals. Caesarean sections and vacuum extractions could be done in 21 hospitals. Almost all the hospitals had emergency blood available. Manual vacuum aspiration for the treatment of incomplete abortions was practised in 8 hospitals. There were only 6 hospitals which were implementing the Choice on Termination of Pregnancy (TOP) Act, with only 2 of these doing second trimester TOP’s. Emergency hysterectomy could be done in half of the provincial hospitals.
The province had 6 obstetricians & gynaecologists.Advanced midwives (ADM’s) were available in 16 of our hospitals (the number of ADM’s ranged from 1 in 7 hospitals to 5 in 2 hospitals). Three other hospitals had one student ADM in training. PEP training was done in 12 of our hospitals. Eighteen hospitals had PEP trained midwives.
There were more than half of our hospitals which experienced problems with the referral system, ranging from lack/shortage of
260

transport/ambulances, communication problems and unavailability of beds at the referral centre.
261

Conclusions* Most of our hospitals do not have Antenatal Care Clinics. * Hospitals use different types of partograms and there were
problems with the completion/plotting of the labourgraphs. * There is no equity in the distribution of staff - obstetricians,
advanced midwives & PEP trained nurses.* There is unequal distribution of CTGs * Syphillis screening results and treatment is not provided same day
in most hospitals* At least half the hospitals could perform an emergency hysterectomy* Spinal anaesthesia is not utilised in 9 institutions. * The referral network and process was a problem in half the
provincial hospitals.* Recommendations based on the findings above, were made to the
provincial management.
262