bell's palsy: the spontaneous course of 2500 peripheral facial nerve palsies of different...
TRANSCRIPT

Acta Otolaryngol 2002; Suppl 549: 4–30
Bell’s Palsy: The Spontaneous Course of 2,500 Peripheral Facial Nerve Palsiesof Different Etiologies
ERIK PEITERSENFrom the Department of Otorhinolaryngolog y—Head & Neck Surgery, Rigshospitalet, Copenhagen , Denmark
Peitersen E. Bell’s palsy: the spontaneous course of 2,500 peripheral facial nerve palsies of different etiologies. ActaOtolaryngol 2002; Suppl 549: 000–000.
Objective—The Copenhagen Facial Nerve Study aims to explain the spontaneous course of idiopathic peripheral facialnerve palsy which occurs without any kind of treatment. In this study Bell’s palsy and idiopathic palsy are considered tobe synonymous and specify an acute, monosymptomatic, unilateral peripheral facial paresis of unknown etiology.
Material and methods—The material includes 2,570 cases of peripheral facial nerve palsy studied during a period of 25years. It includes 1,701 cases of Bell’s palsy and 869 of non-Bell’s palsy. In the total patient sample, 116 had herpes zoster,76 were diabetic, 46 were pregnant and 169 were neonates. A total of 38 different etiologies were observed. At the � rstconsultation a standard ENT examination was performed, including a thorough description of the grade and localizationof the paresis, taste, stapedius re� ex and nasolacrimal re� ex tests and acoustic-vestibular examination. Follow-up wasdone once a week during the � rst month and subsequently once a month until normal function was restored or for upto 1 year.
Results —The initial examination revealed 30% incomplete and 70% complete palsies. Follow-up showed that in 85%of patients function was returned within 3 weeks and in the remaining 15% after 3–5 months. In 71% of patients normalmimical function was obtained. Sequelae were slight in 12% of patients, mild in 13% and severe in 4%. Contracture andassociated movements were found in 17% and 16% of patients, respectively.
Conclusion —A survey of the literature showed that no kind of treatment, including prednisone, was able to give abetter prognosis. The use of prednisone raises a big ethical problem because no evidence of its ef� cacy exists and theeuphoric side-effect induces a false feeling of bene� t in the patients. Key words : Bell’s palsy, facial nerve, idiopathic facialnerve paresis, natural history, spontaneous course.
INTRODUCTION
The facial expressions of human beings fascinate mebecause they convey both the lowest, most bestialpleasures and the strongest and gentlest emotions ofthe spirit. With these words, Charles Bell de� ned theimportance of peripheral facial paralysis, which elimi-nates facial symmetry, one of the attributes of beauty,and thus creates a dis� gured and distorted face (1).
Facial nerve paralysis has been known since an-cient times by the Egyptians, Greeks, Romans, Incasand other native cultures (2, 3). The oldest artisticrepresentation of facial nerve paralysis is a clay headfrom Egypt, :4,000 years old, showing a right pe-ripheral facial nerve paralysis. A small painted earth-enware statuette of a woman with a left-sided facialparalysis from Crete, Greece, has been dated :7thto 6th century BC. A vase found in Carthage anddated :250 BC (from the third Punic war 249–246BC) depicts a peripheral facial nerve palsy on the leftside. Mochica ceramics from Peru (AD 200–700)made in clay and carefully painted represent typicalasymmetrical faces caused by facial nerve paralysis.
In the Middle Ages and during the Renaissancemany artists portrayed � gures with asymmetrical anddistorted faces. The portrait of Mona Lisa is the mostfamous and her enigmatic smile has been discussedfor many years all over the world and at several facial
nerve symposiums. There is a weakness of the cornerof the mouth, but on which side? She cannot be askedto grimace to reveal which side was affected. Leon-ardo da Vinci (1452–1519) took 4 years to paintMona Lisa but the painting was never � nished (4).The expression of a face depends to a large extent (5)on the corners of the eyes and mouth but Leonardoblurred these parts of the face very carefully, so thatit is very dif� cult to guess her mood (6). Further-more, the painting is asymmetrical (there is a lowerleft horizon), which gives the left side of the face aleaner and more erect impression (6). Attempts tointerpret the smile of Mona Lisa have been numer-ous. A guess is that it could be the smile of Leonar-do’s mother, who died before he was 5 years old (4,7, 8). The smile of Mona Lisa was used by Leonardoin some of the paintings he made after his master-piece and is called ‘‘Leonardesque’’ (4). The conclu-sion is that, from the artist’s point of view, MonaLisa did not suffer from a peripheral facial nervepalsy, as has been misdiagnosed by medical doctors(9).
The � rst medical studies of the disease should beattributed to Avicenna (10), who was the � rst torecord the differences between central and peripheralfacial paralysis. If the disease that produces paralysiscomes from the middle of the brain, one half of the
© 2002 Taylor & Francis. ISSN 0001-6489

Bell’s palsy 5
body is paralyzed. If the disease is not in the brainbut instead in the nerve, then only what depends onthis nerve is paralyzed.
The representation of facial nerve palsy in medicalpublications began in the 18th century. In 1797,Professor Niclaus A. Friedreich from Wurzburg, Ger-many treated three patients with idiopathic facialnerve paresis and documented recovery of normalfunction (11). The observation was published in theGerman medical literature in 1798 under the title‘‘Paralysis Musculorum Faciei Rheumatica’’. The� rst English review appeared in 1800 in the Annals ofMedicine published in Edinburgh and it is possiblethat Charles Bell, who was studying medicine inEdinburgh at the time, read this paper. Bell (later SirCharles Bell) described the innervation of the facialmuscles and the skin of the face and consequently thetrigeminal nerve is called Bell’s nerve. Eventually theeponym ‘‘Bell’s palsy’’ became synonymous with idio-pathic peripheral facial nerve paralysis. However,Friedreich described the syndrome 23 years beforeBell.
During the 19th century the treatment of periph-eral facial nerve palsies was anti-rheumatic . At thebeginning of the 20th century electrical stimulationwas used and some very ingenious apparatuses wereconstructed. In 1932 Balance and Duel (12) publishedthe results of inserting a free nerve graft between thecut ends of the facial nerve and also advocateddecompression of the mastoid segment of the facialnerve for Bell’s palsy when its degeneration delayedrecovery. This was the beginning of the modern eraof facial nerve surgery.
During the following three decades, the number offacial nerve decompression operations increasedrapidly. The leading experts were Cawthorne fromLondon (13), Miehlke from Germany (14), Jongkeesfrom The Netherlands (15), Fisch from Switzerland(16) and Kettel from Denmark (17), who was theorganizer of the First International Symposium onFacial Nerve Surgery held in Copenhagen in 1964(18). At that time, the surgeon’s view was that pe-ripheral facial paralysis should be treated with de-compression after 2 months in cases of continuedparalysis. The discussions at the symposium revealeda great deal of skepticism, especially from neurolo-gists and neurophysiologists , regarding the ef� cacy ofthe decompression operations. Sunderland (19, 20)described nerve injuries based on the pathology of thenerve trunk and classi� ed � ve degrees of damage(Table I). Furthermore, he combined the severity ofthe injuries with the time of recovery and was the � rstto create a pro� le of the recovery of a motoric nervepalsy.
AIM OF THE INVESTIGATION
In Copenhagen it was decided to study the naturalhistory of Bell’s palsy. The aim of this ‘‘CopenhagenFacial Nerve Study’’ was to provide a description ofthe spontaneous course of idiopathic peripheral facialpalsy, i.e. that which occurs without any kind oftreatment. The prospective study was designed toinclude a large number of patients, with no exclusionof special groups of patients, and to involve adequatefollow-up, exact descriptions of sequelae and a statis-tical analysis with signi� cant conclusions. It was de-cided not to publish the results of the investigationuntil the conclusions were statistically signi� cant.
Preliminary observations were presented in Zurichin 1976, Pittsburgh in 1977, Los Angeles in 1981,Paris and Rio de Janeiro in 1988, Cologne in 1992,Matsuyama in 1997 and Berlin in 2000.
ETIOLOGY
Theories and hypothesesThe aim of this investigation is not to list or discussall possible hypotheses or theories but to describe thespontaneous course of Bell’s palsy. Nevertheless, ashort summary of these theories is included. Forreviews, see Kettel (17), Miehlke (14) and May (21).Friedreich (11) hypothesized that the cause of facialparalysis in his three patients was ‘‘rheumatic’’ be-cause of exposure to cold often followed by fever,chills and local pain and swelling in and around theneck. Brunninghausen speculated that the paralysisarose from the nerve sheath becoming thickened andcompressed in the stylomastoid foramen. Berard in1836 repeated this hypothesis. The cold hypothesis,or paralysis e frigore, maintained that exposure todraughts produced the palsy. The ischemic hypothesismaintained that ischemia resulting from disturbedcirculation in the vasa nervorum led to nerve injury.Later on a combination with secondary ischemia wasadvocated by a number of surgeons (13–17). Theimmunological hypothesis was introduced byMcGovern and co-workers (22, 23).
During the last 25 years or more, viral infectionshave been proposed as causes of Bell’s palsy. In 1972,
Table I. Classi� cation of nerve injuries after Sunder -land (19, 20)
PathologyDegree Recovery
Neuropraxia1 CompleteAxonotmesis2 Complete
3 Neurotmesis IncompleteNon-functionalPerineurium disruption4NoneComplete disruption5

E. Peitersen6
Table II. Timetable for examinations
First examination as soon as possibleOnce a week until function returnedThereafter every second weekAfter 6 months once a monthFollow-up discontinued after function restored or after
1 year
Table III. The questionnaire administered to thepatients concerning history of Bell’s palsy
Beginning—palsy—dateRemission date—unchanged—regressionFacial palsy before—relatives with facial palsyHead trauma—systemic disease—diabetes mellitusPregnancy—infections—skin eruptionsColds—exposure to draughtOther cranial nerve symptomsHeadache—paresthesia—paresisOtitis—hearing loss—tinnitus—vertigoPostauricular painsBefore—simultaneous—afterTaste—phonophobia—tear� ow—dry eye
McCormick (24) published his hypothesis suggestingthat reactivation of herpes simplex virus type 1 (HSV-1) causes in� ammation and edema in the bonyfallopian canal and results in peripheral facial palsy.Adour et al. (25) accepted this theory. In contrast,Mulkens et al. (26) were unable to demonstrate adirect link with HSV-1. However, new molecularbiological techniques, such as polymerase chain reac-tion (PCR), have proved to be more sensitive. Mu-rakami et al. (27) studied 14 Bell’s palsy patients invivo using HSV DNA PCR. Endoneurinal � uid fromthe facial nerve and biopsies from the posterior auric-ular muscle were tested using PCR for the presence ofHSV DNA. HSV DNA was detected in samples from11:14 patients. Further experiments in the future willhopefully resolve this issue.
De� nitionThe term Bell’s palsy is accepted in many Anglo-American countries to describe a peripheral paresis ofthe facial nerve, independent of etiology. Idiopathicperipheral facial nerve paresis is an acute,monosymptomatic , peripheral facial nerve paresis ofunknown etiology. Formerly the disease was de-scribed as rheumatic or ischemic, as mentionedabove. Patients suffering from an underlying diseaseor condition, for example collagenosis, pregnancy ordiabetes mellitus, sometimes develop peripheral facialnerve palsies, but these pareses are never classi� ed asBell’s palsy. However, a reduction in future in thegroup of idiopathic pareses is anticipated on accountof better knowledge of many diseases and of thepathological conditions governing peripheral paresis.Bell’s palsy and idiopathic peripheral facial nerveparesis are considered as synonymous in this study.
MATERIAL AND METHODS
Before the start of this investigation a lot of time wastaken to work out a very speci� c plan for the study.As a result of 6 months of pilot studies it was possibleto construct a timetable for the following years. Thestudy design was as follows.
The patient was � rst examined as soon as possibleafter the onset of palsy, i.e. within 1–5 days after theonset of paresis (Table II). Follow-up examinations
were performed once a week until the returning offunction was observed. After 6 months, examinationswere conducted once a month. Follow-up was discon-tinued after restoration of function or after 1 year. Ifa patient did not attend for examination a newappointment was mailed to them. If the patient stillfailed to attend, a telephone interview was conductedor the patient was asked to complete a questionnaire.All the patients lived within a radius of 25 km of thehospital and using the Danish Central Personal Reg-ister it was easy to trace them. The majority ofpatients failed to attend the follow-up examinationsbecause normal function had been restored. Follow-up included 98% of all patients. Great importancewas attached to the date of onset of palsy as well asthe date of the � rst sign of returning of function. Thequestionnaire administered to the patients is shown inTable III. It should be stressed that patients sufferingfrom acute peripheral facial palsy were always able togive the exact date and hour of the � rst sign ofparesis.
The examination of the patient is very importantand an exact description of the paresis must be madeat the � rst examination (Table IV). Is the paresiscomplete or incomplete? Does it affect all branches oris it localized to only one or maybe two branches?Bell’s palsy usually involves all branches, althoughnot to the same degree. Patients with involvement ofonly one or perhaps two branches should arouse
Table IV. Description of the standard examination ofpatients with Bell’s palsy
Routine ENT examinationDescription of facial nerve palsyGrade and localizationCranial nerve checkTaste, stapedius re� ex and nasolacrimal re� ex testsAcoustic and vestibular function testsLaboratory tests

Bell’s palsy 7
suspicion of another etiology, for example a parotidgland tumor.
All topographical tests were performed during thepatient’s � rst visit. These involved examination oftaste, stapedius re� ex and nasolacrimal re� ex. Thesetests were repeated at each of the two subsequentvisits, if the result of the preceding investigation wasnot normal. Patients also underwent acoustic andvestibular tests including tympanometry, audiometry,electronystagmograph y for spontaneous and posi-tional nystagmus and a caloric test according toHallpike.
If the anamnesis and objective � ndings indicatedBell’s palsy, only a few laboratory tests were carriedout; these always included measurement of bloodpressure and a urine test for glucose. All patientswere investigated for serum antibodies against HSV,herpes zoster and borreliosis. In patients with a sec-ond episode of palsy or those in whom function wasnot restored within 4 months an extensive battery oftests was performed, including cerebrospinal � uid(CSF) cell counting, differential cell counting, deter-mination of Borrelia burghdorferi antibodies, CT andMRI scans and a variety of other tests.
Electrodiagnosis of the facial nerveDuchenne in 1855 (28) was the � rst to use contrac-tion of the facial muscles evoked by electrical stimulito the nerve as a way of predicting recovery. Incontrast to many lesions of peripheral nerves, electro-diagnosis of cranial nerves is hampered by one majordif� culty, namely that in the majority of cases it isnot possible to stimulate proximally to the site of thelesion. Thus, it is not possible to compare the re-sponse to proximal stimulation with the response tostimulation distally from the site of the lesion.
A very simple and widely-used electrical test is theso-called nerve excitability test (NET), in which thethreshold of the electrical stimulus producing visiblemuscle twitch is determined. Although the NET is avery simple test, it has limitations and its accuracy isdubious. When using a stronger stimulation to obtainmaximal contraction of the facial muscles the test isknown as the maximal stimulation test (MST). Ac-cording to Blumenthal and May (29), the NET wasnot reliable when the response was normal, as 42% oftheir patients with a normal response had residualfacial function de� cits 6 months later. Furthermore,Groves and Gibson (30) and Laumans (31) notedthat some of their patients with an abnormal re-sponse to the NET recovered full function. To thebest of my knowledge, the NET is not reliable oruseful for predicting recovery from peripheral facialnerve palsies. Langworth and Taverner (32) recom-mended conduction velocity as the best parameter forpredicting prognosis.
Electromyography is not very reliable at revealingrecent facial nerve palsies and has no prognosticsigni� cance in Bell’s palsy according to Buchthal (33).However, after :10–12 days the so-called denerva-tion potentials can be recorded and the test is alsoable to demonstrate regeneration.
Electrical tests are not routinely used in Bell’s palsypatients in my department. The Department of Clini-cal Neurophysiology performed all the electrodiag-nostic tests of the facial nerve in this study. Themajority of cases were examined by Olsen (34), whoin 1975 described the technique of electroneurogra-phy (ENoG). The method is identical to that used byEsslen in 1977 (35). ENoG is very useful for demon-strating degeneration. The principle is to compare theevoked potentials on the paretic side with those onthe healthy side. For further information, see Olsen(34) and Esslen (35).
Statistical analyses
The statistical data analyses were performed by ArneNørby Rasmussen, BScEE and Poul Aabo Osterham-mel, EE, EDA. The x2 test was used to compare databetween different groups of patients. p¾0.05 wasconsidered signi� cant. In addition, the Shapiro–Wilktest for normality was used with a signi� cance level ofp¾0.05.
PatientsThe patients in this study came from the Copenhagenarea during a 25-year period. The investigation in-cluded 2570 patients suffering from peripheral facialnerve paresis (Table V). There were 1,701 patientswith Bell’s palsy (66%) and 869 with non-Bell’s palsy(34%).
RESULTS
Incidence of Bell’s palsyIn this study ‘‘incidence’’ is de� ned as the number ofcases per year in a population of 100,000 inhabitants.Studies in the literature have shown great variationsin incidence. However, many of these studies cannotbe considered as representative, because basic criteriahave not been ful� lled. There must be a well-de� nedarea and all patients should be included. The numberof all incoming and outgoing inhabitants should beregistered, as well as the age and sex of the popula-tion; however, only a few investigations meet theserequirements. In this study the incidence of Bell’spalsy was 32.
Recurring palsies and familial Bell’s palsyA total of 6.8% of Bell’s palsy patients in the samplehad previously suffered from facial palsy on either

E. Peitersen8
Table V. Etiologies of the 2,570 study patients
Etiology n
1,701Idiopathic palsy169Neonatal age
Herpes zoster 11695Trauma76Diabetes mellitus46Pregnancy
Polyneuritis 4443Parotid tumor34Vascular (brainstem)27Hemifacial spasm21Sarcoidosis20Multiple sclerosis19Melkersson–Rosenthal syndrome18Collagenosis18Cholesteatoma of the middle ear
Children with bilateral palsy 1816Breast cancer with metastasis15Chronic otitis
Infectious mononucleosis 96Leukemia6Malignant lymphoma
Cholesteatoma of the inner ear 5Cancer of the middle ear 5
4BorreliosisAIDS 4
3Neurinoma of the VIIth extracranial nerve3Bronchial cancer with metastasis2Nephropathia2Non-de� nite paresis
Hypothyreosis 21Pemphigus1Granuloma eosinophilia1Tuberculosis1Poliomyelitis1Smallpox vaccine sequelae
Herxheimer reaction 11Paget’s disease1Hysteria
Fig. 1. Number of patients with Bell’s palsy per monthover the 25-year period of the study.
The Shapiro–Wilk test for normality revealed nosigni� cant difference from month to month (p¾0.1)and thus no seasonal variation or clustering wasfound.
Decade variationVariations from year to year or from decade todecade could not be demonstrated because the num-ber of patients with Bell’s palsy has largely remainedconstant over the study period: mean 68 (range 48–89) (Fig. 2). The Shapiro–Wilk test showed no sig-ni� cant difference from year to year (p¾0.4).
Sex distributionThe question of a gender predominance among pa-tients af� icted with idiopathic facial palsy has beendiscussed in the literature. One of the main reasonsfor the discussion has undoubtedly been the smallamount of material available. This study included1,701 patients with Bell’s palsy, 818 (48.1%) of whomwere male and 883 (51.9%) female. The underlyingpopulation comprises 47.8% males and 52.2% fe-males, clearly indicating that there is no difference insex distribution among patients with Bell’s palsy(0.8BpB0.9).
the same or the opposite site of the face. Someauthors use the term ‘‘recurrent’’ palsy exclusively todescribe paresis occurring on the same side of theface; paresis on the opposite side is termed ‘‘alternat-ing’’. Although this classi� cation is logical, the term‘‘recurrent’’ is in general use and is therefore used inthis study to describe both ipsi- and contralateralpalsies. The occurrence of familial Bell’s palsy is wellknown. In this study, 4.1% of all cases of Bell’s palsyobserved represented familial Bell’s palsy.
Seasonal variation and clusteringThe seasonal incidence of Bell’s palsy has been dis-cussed for many years. The explanation of � ndings ofseasonal variation or clustering in some samplescould be that the patient sample was too small. Inthis study the mean number of patients per monthwith Bell’s palsy was 142 (range 126–156) (Fig. 1).
Fig. 2. Number of patients with Bell’s palsy per year overthe 25-year period of the study.
Bell’s palsy 9
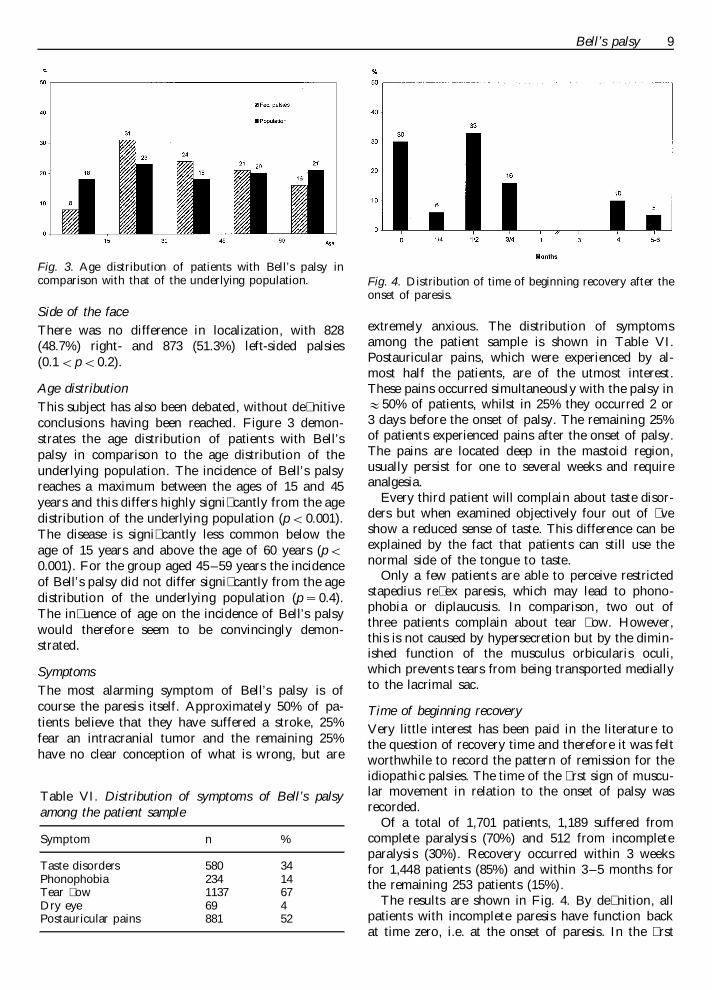
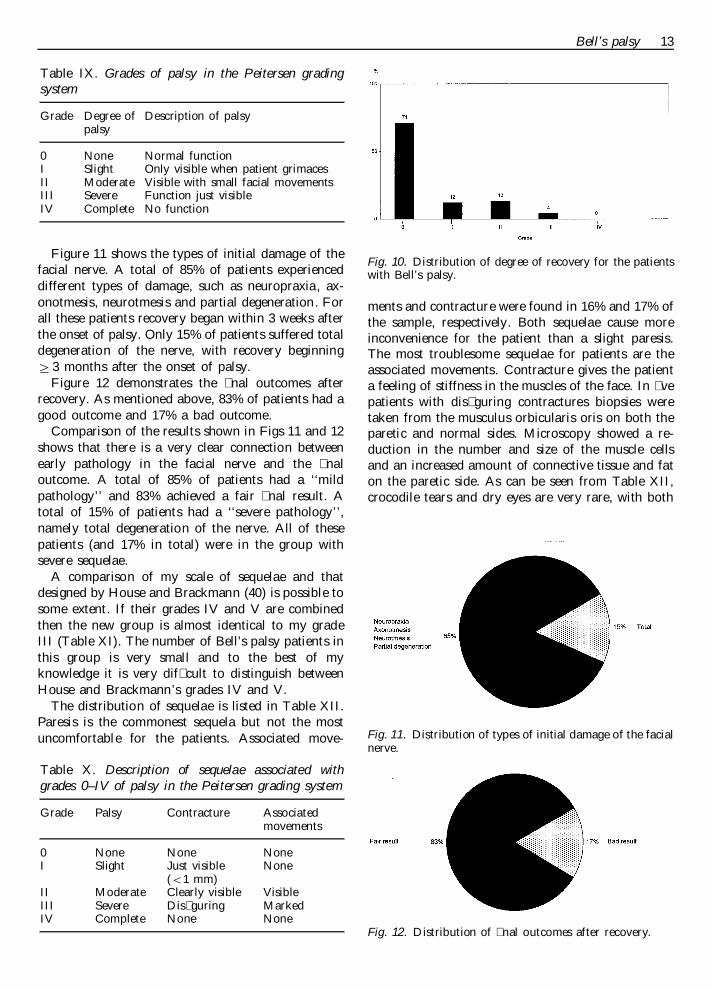
Fig. 3. Age distribution of patients with Bell’s palsy incomparison with that of the underlying population. Fig. 4. Distribution of time of beginning recovery after the
onset of paresis.
Side of the faceThere was no difference in localization, with 828(48.7%) right- and 873 (51.3%) left-sided palsies(0.1BpB0.2).
Age distributionThis subject has also been debated, without de� nitiveconclusions having been reached. Figure 3 demon-strates the age distribution of patients with Bell’spalsy in comparison to the age distribution of theunderlying population. The incidence of Bell’s palsyreaches a maximum between the ages of 15 and 45years and this differs highly signi� cantly from the agedistribution of the underlying population (pB0.001).The disease is signi� cantly less common below theage of 15 years and above the age of 60 years (pB0.001). For the group aged 45–59 years the incidenceof Bell’s palsy did not differ signi� cantly from the agedistribution of the underlying population (p¾0.4).The in� uence of age on the incidence of Bell’s palsywould therefore seem to be convincingly demon-strated.
SymptomsThe most alarming symptom of Bell’s palsy is ofcourse the paresis itself. Approximately 50% of pa-tients believe that they have suffered a stroke, 25%fear an intracranial tumor and the remaining 25%have no clear conception of what is wrong, but are
extremely anxious. The distribution of symptomsamong the patient sample is shown in Table VI.Postauricular pains, which were experienced by al-most half the patients, are of the utmost interest.These pains occurred simultaneously with the palsy in:50% of patients, whilst in 25% they occurred 2 or3 days before the onset of palsy. The remaining 25%of patients experienced pains after the onset of palsy.The pains are located deep in the mastoid region,usually persist for one to several weeks and requireanalgesia.
Every third patient will complain about taste disor-ders but when examined objectively four out of � veshow a reduced sense of taste. This difference can beexplained by the fact that patients can still use thenormal side of the tongue to taste.
Only a few patients are able to perceive restrictedstapedius re� ex paresis, which may lead to phono-phobia or diplaucusis. In comparison, two out ofthree patients complain about tear � ow. However,this is not caused by hypersecretion but by the dimin-ished function of the musculus orbicularis oculi,which prevents tears from being transported mediallyto the lacrimal sac.
Time of beginning recoveryVery little interest has been paid in the literature tothe question of recovery time and therefore it was feltworthwhile to record the pattern of remission for theidiopathic palsies. The time of the � rst sign of muscu-lar movement in relation to the onset of palsy wasrecorded.
Of a total of 1,701 patients, 1,189 suffered fromcomplete paralysis (70%) and 512 from incompleteparalysis (30%). Recovery occurred within 3 weeksfor 1,448 patients (85%) and within 3–5 months forthe remaining 253 patients (15%).
The results are shown in Fig. 4. By de� nition, allpatients with incomplete paresis have function backat time zero, i.e. at the onset of paresis. In the � rst
Table VI. Distribution of symptoms of Bell’s palsyamong the patient sample
n %Symptom
Taste disorders 3458014Phonophobia 234
Tear � ow 1137 67Dry eye 469
52Postauricular pains 881

E. Peitersen10
week 6% of patients achieved remission, in the secondweek 33% and in the third week 16%. No patientsachieved remission between 3 weeks and 3–5 monthsafter the onset of paresis. This is because patientswho showed improvement in the � rst 3 weeks hadonly partial degeneration and blocking of nerve con-duction whilst patients who showed improvementafter 3–5 months had total degeneration. After 3–5months 10% of patients experienced remission andafter 5–6 months an additional 5% experienced re-mission. This investigation shows that all patientsdiagnosed with Bell’s palsy achieve some degree ofmuscular function. However, this does not imply thatall patients achieve normal function. The period be-tween the � rst 3 weeks without remission and afterthe third month without remission is one character-ized by ‘‘hibernation of the facial nerve’’. Althoughthe nerve seems to be dead it is in fact still alive andin the process of repairing the damage.
Complete recoveryThe next question is naturally how many patients willachieve complete remission? In this study, of a totalof 1,701 patients, 1,202 (71%) achieved normal facialnerve function. The second question is how long doesit take before patients achieve normal function?
Prospects are decidedly better for the group withsome remission within the � rst 3 weeks (Table VII).Patients with the poorest prognosis are of coursethose with total degeneration and late return of func-tion. This group does not regain normal mimicalfunction. Normal function is regained as early aswithin 2 months for the majority (58%) of all patients(Fig. 5). The possibility of normalization is very smallafter 3 months, at which time 64% of patients haveregained normal function, and beyond 6 months nopatients regained normal mimical function (Fig. 6).As noted before (Table VII), the incomplete Bell’spalsy patients have a very good prognosis for fullrecovery (481:512; 94%). Of the patients with com-plete Bell’s palsy, 721:1,189 (61%) regained normalfacial muscle function. The difference between thetwo groups in terms of the number of patients who
Fig. 5. Distribution of time of complete recovery after theonset of paresis.
achieved full recovery was highly signi� cant (pB0.001).
Gender and recoveryThe numbers of males and females who experiencedfull recovery were 564 (69%) and 638 (72%), respec-tively. There was no statistically signi� cant differencebetween the two groups (p\2).
Factors in� uencing the � nal resulsTime of beginning remission. The number of days
between the onset of paresis and the beginning ofremission is a very decisive factor in the degree ofrecovery (Fig. 7). A total of 94% of patients withincomplete paresis regained normal function. Of pa-tients who showed remission in the � rst week, 88%regained normal function, as opposed to 83% ofthose who showed remission in the second week and61% of those who showed remission in the thirdweek. The prognosis for patients with incompleteparesis was signi� cantly better than that for thegroup who recovered in the � rst week (p¾0.03).There was no signi� cant difference in prognosis be-tween patients who recovered in the � rst and secondweeks (p¾0.2) but patients who recovered in the
Fig. 6. Distribution of time of complete recovery (cumula-tive) after the onset of paresis.
Table VII. Distribution of patients with initial incom-plete and complete paresis who make a full recoveryfrom Bell’s palsy
Initial FinalParesis withfull recovery
n% %n
Incomplete 9448130512721701189Complete 61

Bell’s palsy 11
Fig. 7. Proportion of patients who achieve complete recov-ery as a function of time of beginning recovery after theonset of paresis.
VIII) should be performed very carefully and alwaysin exactly the same way or else the comparison ofresults is meaningless. The results should not dependon the person performing the tests.
Taste. The taste test according to Boernstein (36) issemiquantitative and based on recognition of fourbasic tastes—sweet, salt, sour and bitter—at threedifferent concentrations. Initial taste examinationshowed that 83% of patients had partially reduced orabolished taste while 12% had normal taste. Finaltaste examination showed that 80% of patients hadregained normal taste function. Taste function andthe muscular function of the face normalized at ap-proximately the same time.
Stapedius re� ex. The stapedius re� ex is an acousticfacial re� ex provoked on both sides by one-sidedsound stimulation (37). Initially, 72% of patients hada reduced or abolished re� ex and only 22% had anormal re� ex. When remission occurs, stapediusre� ex will usually return 1–2 weeks before visualfunction of the facial muscles can be con� rmed.Normal function was restored in 86% of patients.
Tearing or nasolacrimal re� ex. The nasolacrimalre� ex passes from the nasal mucosa to the superiorsalivary nucleus and thence to the secretory � bers,with the facial nerve ending in the lacrimal gland. Inthis study a modi� cation of Schirmer’s test II (38)was used, which is based on measurement of tear � owfor 1 min. Stimulation with benzene is carried out for30 s and measurement is performed by using � lterpaper placed in the lower fornix. At the end of thetest the length of the soaked strip of � lter paper ismeasured on both sides. The difference between the 2sides is B20% in 95% of normal persons. Initially,11% of patients had partially reduced or abolishedtearing. The � nal result showed that 97% of patientsachieved normal tearing. In comparison with tasteand stapedius re� ex testing, tearing became normal ina surprisingly high proportion of patients.
Figure 9 shows the prognostic value of the threetopographical tests. The patients were divided intotwo groups: one group with normal facial musclefunction and the other with muscular sequelae. Com-parison of the results of the initial taste tests for thegroups with and without sequelae showed that 91%and 80% of patients, respectively had partially re-duced or abolished taste (pB0.001). Concerning thestapedius re� ex, it was found that 91% and 63% ofpatients, respectively had a reduced or abolishedre� ex (pB0.001). The nasolacrimal re� ex is also areliable prognostic indicator because 27% and 5% ofpatients, respectively had abolished or reducedlacrimal function (pB0.001). In conclusion, all threeof the topographical tests provide reliable prognosticinformation.
third week had a signi� cantly worse outcome (pB0.001). It is clear that the time of beginning remissionis highly signi� cant to the prognosis.
Age of patients. Age is another parameter thatin� uences the � nal result (Fig. 8). Children aged 514years had the most favorable prognosis, with 90%achieving full recovery. Patients aged 15–29 yearshad a fairly good chance of recovery (84%). Thechance of a full recovery was reduced for patientsaged between 30 and 44 years (75%). Above the ageof 45 years, the chances of recovery diminished sig-ni� cantly (64%). Above the age of 60 years, onlyabout one-third of patients will experience the returnof normal function. The in� uence of age on the � naloutcome is therefore highly signi� cant (pB0.001).
Postauricular pains. As noted above, postauricularpains were registered in 52% of all cases of Bell’spalsy. A total of 78% of patients with no pain re-gained normal function, as opposed to only 64% ofpatients with pain (pB0.001).
The prognostic value of topographical tests. It mustbe stressed that the examination of taste, stapediusre� ex and tear � ow or nasolacrimal re� ex (Table
Fig. 8. Age distribution of patients who achieve completerecovery.

E. Peitersen12
Table VIII. Results of the initial and � nal examinations of taste, stapedius re� ex and nasolacrimal re� ex
None assessible Normal functionReduced or abolished functionTest
% n % n %n
Taste83 111Initial 7 171 101,41914 111 7 1,354 80236Final
Stapedius re� ex72 108 6 372Initial 221,2217 122 7 1,471 86122Final
Nasolacrimal re� ex11 27 2Initial 1,482 871922 27 129 1,645 97Final
Sequelae. As mentioned before, 71% of patientsregain normal function of their facial muscles after anidiopathic paresis. The remaining 29% of patientssuffer from varying degrees of sequelae. It is extremelydif� cult to describe the sequelae accurately and togroup the degree of sequelae; however, it should beborne in mind that the daily discomfort of sequelae isa signi� cant problem for the patients. Today, thereare at least 10 systems available for facial nervegrading but none of these systems is ideal (39, 40).
The existing systems include gross scales, regionalsystems and speci� c scales. One of the biggest prob-lems with grading systems is � nding a balance be-tween an exact description of the sequelae andminimizing the number of groups into which thepatients are classi� ed. The scale should combine themain parameters (paresis, contracture and associatedmovements) based on speci� c de� nitions. An idealsystem is one with high speci� city and an acceptablesensitivity. Before proposing my gross scale the � rst200 of the patients in this study were examined 3times. The scale emerged from an examination ofthese 200 patients who suffered from peripheral facialnerve palsy with different grades of reduced functionand other sequelae. It should be stressed that the scaleincludes all types of motoric dysfunction. Other sec-ondary defects, such as crocodile tears, decreasedtearing, taste disturbances and stapedius muscle prob-lems, are registered and should be added to the othersequelae to � nd the total number of sequelae. Myscale is a modi� cation of that of Botman and Jong-kees (41).
The factors determining the degree of sequelae areparesis, contracture and associated movements (alsoknown as mass movements or synkinesis). The de� ni-tion of synkinesis is an involuntary movement accom-panying a voluntary one. The � nal cosmetic resultdepends on a combination of these three elements.
Table IX shows the grade of palsy. De� nitions ofgrades 0–IV are given in Table X. Contracture causesa narrowed palpebral � ssure on the involved sidewhen the face is in repose. The corner of the mouthoccurs higher on the affected side and the folds of theface are abnormally deep; in particular the nasal labialfold is very marked. Associated movements are foundin the muscles of the eye, cheek and mouth and moreseldom in the forehead. Associated movements arevisible when the patient tries to close his:her eye andsmiles involuntarily or vice versa. Associated move-ments often cause more cosmetic inconvenience to apatient than a slight paresis or contracture. The threeparameters should be combined to give an accuratedescription of sequelae.
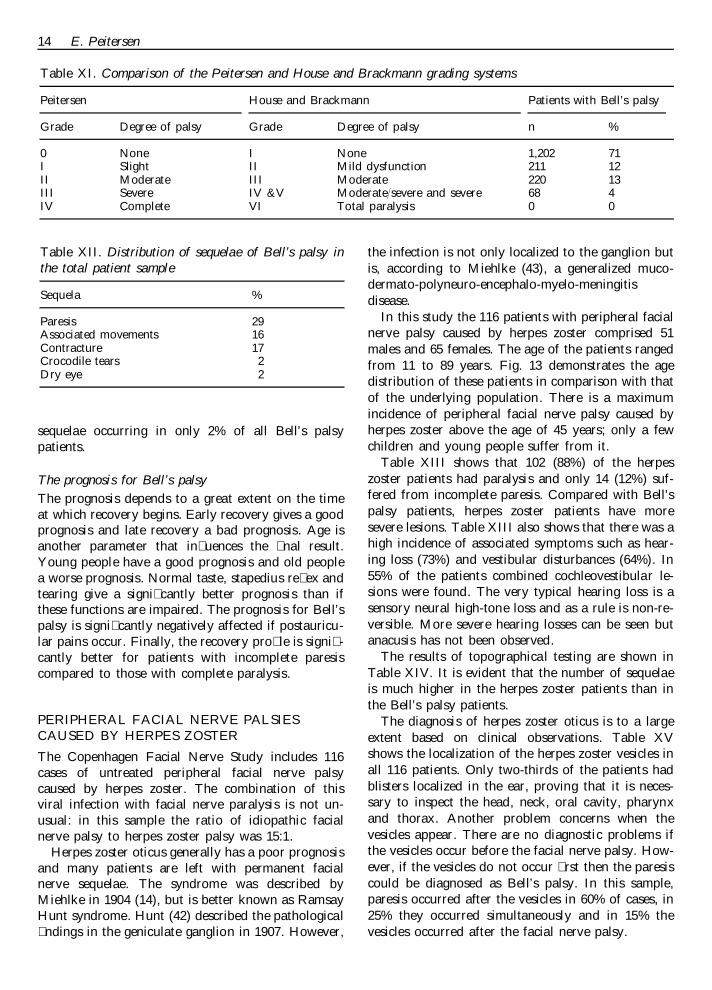
The degree of recovery for all patients is demon-strated in Fig. 10, which shows that 71% recoveredcompletely, 12% had slight sequelae, 13% had moder-ate sequelae and only 4% had severe sequelae. Itshould be stressed that no patients became paralyzed.In summary, 83% of patients had a good recovery and17% a bad recovery without any kind of treatment.
Fig. 9. Proportions of patients with and without muscularsequelae who had reduced or abolished function in thethree topographical tests.
Bell’s palsy 13
Table IX. Grades of palsy in the Peitersen gradingsystem
Grade Description of palsyDegree ofpalsy
Normal function0 NoneOnly visible when patient grimacesI SlightVisible with small facial movementsModerateII
SevereIII Function just visibleNo functionCompleteIV
Fig. 10. Distribution of degree of recovery for the patientswith Bell’s palsy.
Figure 11 shows the types of initial damage of thefacial nerve. A total of 85% of patients experienceddifferent types of damage, such as neuropraxia, ax-onotmesis, neurotmesis and partial degeneration. Forall these patients recovery began within 3 weeks afterthe onset of palsy. Only 15% of patients suffered totaldegeneration of the nerve, with recovery beginning]3 months after the onset of palsy.
Figure 12 demonstrates the � nal outcomes afterrecovery. As mentioned above, 83% of patients had agood outcome and 17% a bad outcome.
Comparison of the results shown in Figs 11 and 12shows that there is a very clear connection betweenearly pathology in the facial nerve and the � naloutcome. A total of 85% of patients had a ‘‘mildpathology’’ and 83% achieved a fair � nal result. Atotal of 15% of patients had a ‘‘severe pathology’’,namely total degeneration of the nerve. All of thesepatients (and 17% in total) were in the group withsevere sequelae.
A comparison of my scale of sequelae and thatdesigned by House and Brackmann (40) is possible tosome extent. If their grades IV and V are combinedthen the new group is almost identical to my gradeIII (Table XI). The number of Bell’s palsy patients inthis group is very small and to the best of myknowledge it is very dif� cult to distinguish betweenHouse and Brackmann’s grades IV and V.
The distribution of sequelae is listed in Table XII.Paresis is the commonest sequela but not the mostuncomfortable for the patients. Associated move-
ments and contracture were found in 16% and 17% ofthe sample, respectively. Both sequelae cause moreinconvenience for the patient than a slight paresis.The most troublesome sequelae for patients are theassociated movements. Contracture gives the patienta feeling of stiffness in the muscles of the face. In � vepatients with dis� guring contractures biopsies weretaken from the musculus orbicularis oris on both theparetic and normal sides. Microscopy showed a re-duction in the number and size of the muscle cellsand an increased amount of connective tissue and faton the paretic side. As can be seen from Table XII,crocodile tears and dry eyes are very rare, with both
Fig. 11. Distribution of types of initial damage of the facialnerve.
Table X. Description of sequelae associated withgrades 0–IV of palsy in the Peitersen grading system
Contracture AssociatedGrade Palsymovements
None None0 NoneNoneI Just visibleSlight
(B1 mm)Clearly visible VisibleII Moderate
MarkedIII Dis� guringSevereNoneNoneCompleteIV
Fig. 12. Distribution of � nal outcomes after recovery.
E. Peitersen14
Table XI. Comparison of the Peitersen and House and Brackmann grading systems
Patients with Bell’s palsyPeitersen House and Brackmann
Grade Degree of palsy nDegree of palsy %Grade
None I None 1,202 710II Mild dysfunction 211 12I SlightIII Moderate 220Moderate 13II
SevereIII IV &V Moderate:severe and severe 68 4VI Total paralysis 0 0IV Complete
Table XII. Distribution of sequelae of Bell’s palsy inthe total patient sample
%Sequela
29Paresis16Associated movements17Contracture
Crocodile tears 2Dry eye 2
the infection is not only localized to the ganglion butis, according to Miehlke (43), a generalized muco-dermato-polyneuro-encephalo-myelo-meningitisdisease.
In this study the 116 patients with peripheral facialnerve palsy caused by herpes zoster comprised 51males and 65 females. The age of the patients rangedfrom 11 to 89 years. Fig. 13 demonstrates the agedistribution of these patients in comparison with thatof the underlying population. There is a maximumincidence of peripheral facial nerve palsy caused byherpes zoster above the age of 45 years; only a fewchildren and young people suffer from it.
Table XIII shows that 102 (88%) of the herpeszoster patients had paralysis and only 14 (12%) suf-fered from incomplete paresis. Compared with Bell’spalsy patients, herpes zoster patients have moresevere lesions. Table XIII also shows that there was ahigh incidence of associated symptoms such as hear-ing loss (73%) and vestibular disturbances (64%). In55% of the patients combined cochleovestibular le-sions were found. The very typical hearing loss is asensory neural high-tone loss and as a rule is non-re-versible. More severe hearing losses can be seen butanacusis has not been observed.
The results of topographical testing are shown inTable XIV. It is evident that the number of sequelaeis much higher in the herpes zoster patients than inthe Bell’s palsy patients.
The diagnosis of herpes zoster oticus is to a largeextent based on clinical observations. Table XVshows the localization of the herpes zoster vesicles inall 116 patients. Only two-thirds of the patients hadblisters localized in the ear, proving that it is neces-sary to inspect the head, neck, oral cavity, pharynxand thorax. Another problem concerns when thevesicles appear. There are no diagnostic problems ifthe vesicles occur before the facial nerve palsy. How-ever, if the vesicles do not occur � rst then the paresiscould be diagnosed as Bell’s palsy. In this sample,paresis occurred after the vesicles in 60% of cases, in25% they occurred simultaneously and in 15% thevesicles occurred after the facial nerve palsy.
sequelae occurring in only 2% of all Bell’s palsypatients.
The prognosis for Bell’s palsyThe prognosis depends to a great extent on the timeat which recovery begins. Early recovery gives a goodprognosis and late recovery a bad prognosis. Age isanother parameter that in� uences the � nal result.Young people have a good prognosis and old peoplea worse prognosis. Normal taste, stapedius re� ex andtearing give a signi� cantly better prognosis than ifthese functions are impaired. The prognosis for Bell’spalsy is signi� cantly negatively affected if postauricu-lar pains occur. Finally, the recovery pro� le is signi� -cantly better for patients with incomplete paresiscompared to those with complete paralysis.
PERIPHERAL FACIAL NERVE PALSIESCAUSED BY HERPES ZOSTER
The Copenhagen Facial Nerve Study includes 116cases of untreated peripheral facial nerve palsycaused by herpes zoster. The combination of thisviral infection with facial nerve paralysis is not un-usual: in this sample the ratio of idiopathic facialnerve palsy to herpes zoster palsy was 15:1.
Herpes zoster oticus generally has a poor prognosisand many patients are left with permanent facialnerve sequelae. The syndrome was described byMiehlke in 1904 (14), but is better known as RamsayHunt syndrome. Hunt (42) described the pathological� ndings in the geniculate ganglion in 1907. However,

Bell’s palsy 15
Fig. 13. Age distribution of patients with herpes zoster incomparison with that of the underlying population.
Table XV. Localization of herpes zoster vesicles in the116 patients with herpes zoster
Nerve:skin innervation %
66Concha and external canalTrigeminal 15Glossopharyngeal 5Vagus 4Cervical nerves 2 and 3 7
3ThoraxTotal 100
Fig. 14. Distribution of degree of recovery for herpes zosterpatients.
The diagnosis of herpes zoster was based on clini-cal observations and determination of speci� c anti-bodies in serum and CSF. A lumbar puncture wasperformed in 20 consecutive patients. CSF showed araised protein level of 0.8–1.8 g:l and pleocytosis of40–300½106 leukocytes:l. (Normal protein levels arede� ned as B0.5 g:l for young and middle-aged pa-tients and B0.7 g:l for elderly patients. Pleocytosis isde� ned as \3½106 leukocytes:l.) Positive antibodieswere also found in all patients. Re-examination wasperformed in six patients 3–6 months after the initialexamination. All patients still had raised protein lev-els and pleocytosis but the degree of abnormality haddecreased.
The prognosis for restoration of facial nerve func-tion in herpes zoster patients is poor (Fig. 14). Only
21% achieve normal function, 25% have mild seque-lae only, 26% have moderate sequelae, 24% severesequelae and 4% no function at all. The recoverypro� le is fair for 46% of patients and bad for 54%.
When this study was � nished, treatment of herpeszoster palsies was started. Only 28 patients wereincluded in this program. A 6-day treatment withacyclovir, 10 mg:kg i.v. every 8 h, was used (44). Theresults were not encouraging. The recovery for thetreated group did not differ signi� cantly from that forthe untreated group. No effect could be demonstratedon hearing loss, but it was obvious that tinnitus andvertigo decreased within a few days. However, thepatient sample was too small for de� nitive conclu-sions to be drawn.
PERIPHERAL FACIAL NERVE PALSIES ANDDIABETES MELLITUS
Diabetes mellitus is a generalized metabolic disordercharacterized by elevation of the blood glucose level.The disease causes damage to the vascular system andthis insuf� ciency produces very common central andperipheral nervous system disorders. The nerves in-nervating the eye muscles are the most frequentlyaffected, followed by the facial nerve. The paresis isunilateral and recurrent paresis is common; however,bilateral peripheral facial nerve palsies have also been
Table XIII. Distribution of herpes zoster palsies
%Paresis n
88Complete 102Incomplete 14 12Hearing loss 85 73Vestibular lesions 74 64Combined cochleovestibular disturbances 64 55
Table XIV. Final results of topographical tests forBell’s palsy patients and herpes zoster patients. Valuesshown represent percentages of patients with normalfunction in the tests
Patients withTest Bell’s palsyherpes zoster patients
Taste 43 79Stapedius re� ex 46 87Nasolacrimal re� ex 9687

E. Peitersen16
described. This study included 76 diabetics (42%male; 58% female) with peripheral facial nerve pare-sis. The patients were aged between 21 and 82 yearsand all were treated with insulin. The ratio of idio-pathic palsy to palsy in diabetics was 22:1.
Of the 76 patients, 47 (62%) suffered from incom-plete paresis and 29 (38%) from complete paralysis. Itwas a surprise that the majority of these patients(almost two-thirds of them) had incomplete paresisand an even greater surprise that the recovery forthese patients was very poor, with only 25% achievingnormal facial muscle function. The explanation forthe poorer degree of recovery of facial nerve functionin these patients is undoubtedly the underlying dis-ease of diabetic polyneuropathia . In Denmark dia-betes is estimated to affect 3–4% of the population.
PERIPHERAL FACIAL NERVE PALSIES INCHILDREN
Of a total of 2570 patients with peripheral facial palsy,349 were aged B15 years. The etiology of thesepatients is shown in Table XVI; for a review see May(21). It can be seen that Bell’s palsy, which includesidiopathic palsy, comprises about one-third of thecases and that the largest group of patients comprisesneonates. The group of multiple malformations in-cludes the real congenital palsies (neonatal age n¾169). The subject of congenital versus birth traumaticpalsies will be discussed later. There are very fewpatients in the other groups, with the exception ofbilateral palsies, which are probably caused by viralinfections. Eight of these cases occurred during thesame month. A slight fever, headache and, in � ve ofthe cases, vomiting were reported before the facialparesis occurred. Three of the patients showed bilateralparesis within 24 h. Lumbar puncture was performedin � ve cases but CSF was normal and Echo andCoxsackie virus investigations were negative. In theother three cases there were intervals of 3–8 days
Table XVI. Etiology of peripheral facial nerve palsiesin children (B15 years)
Etiology n
Bell’s palsy 138169Neonatal age16Bilateral palsy
Acute otitis 7Temporal bone fracture 6
2Herpes zoster2Chronic otitis
Infectious mononucleosis 22Leukemia1Cholesteatoma of the middle ear
Melkersson–Rosenthal syndrome 1Malignant lymphoma 1Pemphigus 1
1Smallpox vaccine sequelaeTotal 349
between the occurrence of paresis on both sides. All thechildren regained normal facial function.
Table XVII illustrates that neonates with presumedbirth trauma are the largest group. In 33 patients allbranches were affected and in 68 only the marginalmandibular branch of the facial nerve was affected.The marginal mandibular branch is the most vulnera-ble of all branches. This branch innervates the depres-sor muscle group of the lower lip and in cases of paresisthis will result in a straight lip on the paretic side.
This particular group of patients is continuallyunder discussion with regard to whether paresis iscongenital, due presumably to aplasia of the facialnucleus, or is perhaps due to birth trauma. Forseveral reasons many supporters of the � rst theoryhave now abandoned it. The primary reason beingthat, if the theory of congenital paresis holds, thenfunction would not be likely to improve. Improve-ment has, however, been seen in a certain number ofcases. Second, from surgical experience and fromknowledge of Bell’s palsy it is known that the mar-
Table XVII. Localization of facial nerve paresis in neonates with presumed birth injuries and distribution of degreeof recovery as a function of localization of paresis
000 RecoveryParesisn Branches
NormalNo Yesn
033 All Complete 7 5 29251Incomplete 26
9 3 144 \1 Complete 1214311Incomplete 32
39 2 068 M.m.br. Complete 4111234Incomplete 27
59 86 35Total 145
M.m.br.¾marginal mandibular branch.

Bell’s palsy 17
Table XVIII. Congenital abnormalities and facialnerve palsies in neonates
Abnormality n
Treacher Collins syndrome 162Moebius syndrome113-trisomy (Patau’s syndrome)
18-trisomy (Edward’s syndrome) 14Multiple defects
24Total
Fig. 15. Proportions of patients who achieved completerecovery from facial nerve palsies of different etiologies.
ginal mandibular branch is the most vulnerable andthat its regeneration is the poorest in Bell’s palsypatients, with :10% never recovering function ofthis branch. Third, the number of birth traumaticpalsies has decreased to :15% during the last 25years as a result of improved obstetric techniques.Finally, electrical tests, such as electromyography andEnoG, allow one to distinguish between peripheraland central lesions. However, babies untouched byhands and forceps in utero can still have paralysis ofthe marginal mandibular branch. Experience showsthat if the marginal mandibular branch is paralyzedthen function will never be restored. Details areshown in Table XVII. Table XVIII shows somecongenital abnormalities and facial nerve palsies inneonates. The majority of cases suffer from TreacherCollins syndrome. The other children had multipledefects or chromosomal abnormalities with one-sidedor bilateral palsies.
Figure 3 demonstrates the age distribution of pa-tients with Bell’s palsy in comparison with that of theunderlying population. The disease is signi� cantlyless common below the age of 15 years (pB0.001).Furthermore, children have the most favorable prog-nosis, with 90% achieving full recovery (Fig. 8).
PERIPHERAL FACIAL NERVE PALSIESIN PREGNANCY
Peripheral facial nerve palsy is uncommon in preg-nant women. The ratio of idiopathic facial nervepalsy in women to palsy in pregnancy was 19:1 in thisstudy. A comparison of recovery between non-preg-nant females aged 15–44 years and pregnant womenshowed that normal function was obtained in 80%and 61%, respectively. The prognosis of peripheralfacial nerve palsy for pregnant women is signi� cantlyworse than that for non-pregnant women of the sameage (pB0.001).
PERIPHERAL FACIAL NERVE PALSIES OFDIFFERENT ETIOLOGIES
Figure 15 shows a comparison of the � nal results offacial nerve palsies of different etiologies. It can be
seen that 71% of the idiopathic group, 61% of preg-nant women, 21% of herpes zoster patients, 25% ofdiabetes mellitus patients and 24% of polyneuritispatients recovered completely. The majority of pa-tients suffering from B. burghdorferi infection wereincluded in the polyneuritis group. These � gures leadto the conclusion that idiopathic palsy has the bestprognosis of all the types of peripheral facial nerveparalysis.
AN EVALUATION OF TREATMENT OFBELL’S PALSY
Can Bell’s palsy be treated?As mentioned in the Introduction, Friedreich was the� rst doctor to attempt to treat patients suffering fromidiopathic peripheral facial nerve palsies. During thelast two centuries an unknown, but large, number ofthese patients have been treated with almost everykind of medicine, physiotherapy, electrical stimula-tion and surgery. More than 1,000 papers have beenpublished and the conclusions, with very few excep-tions, have been that the patients bene� ted from thetreatment and that the authors were convinced of itsef� cacy, even though there was no real proof.
Fortunately, reviews of the literature on the treat-ment of facial paralysis exist. Cleveland gave a reviewcovering the period 1932–38 (45) and Ghiora andWinter (45) reviewed the literature on conservativetreatment of Bell’s palsy between 1939 and 1960.These reviews make very interesting reading and it isstressed that the evaluation of therapy is madedif� cult by the usually high percentage of sponta-neous and complete recovery. Many patients showsigns of returning function as early as 10 days afteronset, even without treatment. Conservative treat-ment is of course designed to reduce edema, ischemia,congestion and compression, and thus to preventtotal degeneration. In the following sections a shortoverview of treatment methods will be presented.

E. Peitersen18
Thermal methodsIn the older literature the majority of authors advocateconductive, radiative and convective heat transfer inorder to achieve vasodilatation. Vasodilatation may beboth local and re� ex in nature and it is logical toattempt vasodilatation in view of the acceptance ofvasoconstriction as the major pathogenic factor. Fur-thermore, experience has shown the soothing effect ofheat treatment in patients with Bell’s palsy. However,some authors assert that heat treatment may increaseedema and thus is inadvisable. Instead of heat treat-ment, some patients were treated by applying ice overthe mastoid region with the aim of relieving edema.However, according to the ischemia theory, suchtreatment would increase vasoconstriction and workagainst the intention of vasodilatation (45). No con-trolled clinical trials have been published in this areaand heat therapy may be considered to be a form ofpsychotherapy.
ElectrotherapyElectrotherapy is one of the most controversial sub-jects in the treatment of peripheral facial nerve paral-ysis. Some authors have advocated electrotherapy butothers have criticized it. According to Ghiora andWinter it is useless and possibly even dangerous,because it may cause contractures (45). Mosforth andTaverner (46) reported a controlled trial of the valueof galvanic stimulation in the management of 86 Bell’spalsy patients. The authors concluded that althoughno signi� cant advantage could be demonstrated by theuse of galvanic stimulation the presence of contracturewas not related to the mild electrical treatment. How-ever, Williams (47) cautioned against exaggeratedforms of physiotherapy, especially electrical stimula-tion, as this kind of therapy may lead to permanentcontractures. As electromyography has demonstratedthat even a denervated muscle will preserve its func-tion for at least a year, it is dif� cult to see whatphysiotherapy will contribute to recovery. If reinner-vation takes place it will occur within a year and theinnervated muscles will recover their function regard-less of physiotherapy. On the other hand, if denerva-tion is permanent, no amount of physiotherapy willprevent muscular degeneration.
Different electrical stimulation apparatuses, some ofthem very sophisticated, were constructed during thelast century. Galvanic and faradic stimulation wereused.
This study included 28 patients with recurrent pare-sis on the opposite side. The � rst paresis in thesepatients had been treated with intensive electricalstimulation. The second paresis was not treated butwas followed until normal function was obtained orfor up to 1 year. A comparison of the 2 sides of the
face showed that 23 patients had more marked con-tractures on the treated side. The grade of sequelaewas II–III on the treated side and I–II on theuntreated side but, as stressed by Langworth andTaverner (32), the development of contractures re-quires degeneration.
MassageThe value of massage is to produce hyperemia andmaintain tonus of the facial muscles. Different opin-ions exist concerning the ef� cacy of massage, but againno signi� cant studies have been published. Massagemay be considered to be a form of psychotherapy (45).
Facial exercise
For many years facial exercises have been recom-mended for peripheral facial nerve palsy patients withboth complete and incomplete paresis. The patientshould stand in front of a mirror and watch the facewhile raising the eyebrows, gently closing the eyes,wrinkling the nose, whistling, blowing out the cheeksand grinning. These facial exercises should be per-formed twice a day (21, 45, 48). Although the effect offacial exercises has not been statistically evaluated,patients appreciate the exercises to a very great extent.However, they should be considered a form of psy-chotherapy according to Wolferman (49).
Cervical sympathetic blockBlocking of sympathetic pathways may relieve vasodi-latation of the vasa nervorum to the facial nerve. Thismay be applied to the stellate ganglion using procaine.Korkis (50) claimed satisfactory results, but no con-trolled trials have been reported. Fearnley et al. (51)found no signi� cant bene� t from the use of thismethod.
SurgeryIn 1932 Balance and Duel (12) advocated a transmas-toid decompression operation in patients with Bell’spalsy. In the years that followed the number ofoperations increased dramatically, but the well-knowndecompression surgeons Cawthorne (13), Jongkees(15), Miehlke (14) and Kettel (17) did not try toexplain their treatment results. According to Jongkees(52), Kettel (53) and Miehlke (14) the indication forsurgery was paralysis lasting 2 months. In their expe-rience patients achieved function :1 month after theoperation. However, this study has documented thatthe operation is useless and that spontaneous regener-ation results in regained function. As mentioned be-fore, indication for surgery was based on a mechanicalway of thinking and furthermore there is not suf� cientmaterial to prove the ef� cacy of decompressionsurgery for Bell’s palsy.

Bell’s palsy 19
Fisch (16, 54) recommended total decompressionof the facial nerve from the styloid foramen to theinternal ear canal if the electroneurographic degener-ation exceeded 90% within 6 days after the onset ofpalsy. This indication is based on his so-called ‘‘bot-tleneck theory’’. The present patient sample is toosmall to ful� ll the requirements for randomization(55, 56).
Yanagihara et al. (57), who believe in transmastoiddecompression, have sought to prove the ef� cacy ofthe operation. Their patient sample included 101Bell’s palsy patients initially treated with steroid butwith denervation exceeding 95% and, at early exami-nation, a function equivalent to House and Brack-mann’s grade V or VI. Surgery was performed duringthree different periods from the onset of palsy: (i)within 1 month; (ii) during the second month; or (iii)after 2–4 months. The best results were obtained inthe � rst group, i.e. those with the earliest surgery.Unfortunately, information about the time from theonset of palsy to the � rst sign of recovery is notavailable. This study shows that patients with nofunction after 3 weeks undergo total degenerationand begin recovery after 3–5 months. The time ofoperation and the time of spontaneous recovery coin-cide. Information about the period between the oper-ation and the beginning of recovery would have beenvaluable but is also not available. There was an agedifference between the surgery and control groupsand furthermore the number of patients was toosmall to permit signi� cant statistical evaluation. It isimpossible to explain how decompression can help apatient 2–4 months after the onset of palsy, when thefacial nerve is undergoing regeneration. The trial ofYanagihara et al. does not provide evidence of theef� cacy of the decompression operation in Bell’spalsy patients who were initially treated unsuccess-fully with steroids.
Drug therapy
Despite the appearance of many publications on drugtherapy during the period 1930–60, there were fewadequate therapeutic trials. Initially, vasodilatorswere mainly used, based on the etiologic factor ofischemia of the vasa nervorum of the facial nerve.Later on steroids were introduced in an attempt toin� uence a possible non-speci� c acute in� ammatoryreaction.
Vasodilators
Different authors have used a variety of vasodilatordrugs. Despite pharmacological observations in nor-mal persons and animals, the actual value of manydrugs in peripheral vascular disorders is uncertain.The drugs used were histamine, procaine, nicotinic
acid, nitrites and papaverine (45). Alarming side-ef-fects associated with histamine and i.v. procaine werenot unusual and � ushing resulted from the adminis-tration of large doses of nicotinic acid. Korkis (50)concluded that it was possible that the vasodilatedvessels leading to the affected nerve caused furtherswelling of the nerve within the bony canal, therebyaggravating compression and secondary ischemia. Inview of the danger and doubtful bene� t of many ofthese drugs in many peripheral vascular disorders,there seems little basis for recommendingvasodilators.
PrednisoneTaverner (58) in 1954 was the � rst to design a con-trolled treatment trial of steroids but unfortunatelythe number of patients was too small to permit asigni� cant statistical evaluation. Attempts to treatBell’s palsy with steroids changed in the 1970s. Thepublication of Adour et al. (59) in 1972 concerningprednisone treatment for idiopathic facial paralysiswas a milestone in the treatment of Bell’s palsy butunfortunately the double-blind protocol was aban-doned in 1970, because the placebo-treated patientsdemanded steroids. What these patients were reallyseeking was the euphoric side-effect of prednisone.The trial included 194 treated and 110 untreatedBell’s palsy patients. The controls were retrospectiveand the study was not blind or randomized. TheNET was used to demonstrate the absence of com-plete nerve denervation in all treated patients but, asstressed by Blumenthal (29), Groves and Gibson (30),Laumans (31) and Wolferman (49), this test is notreliable. The description of sequelae was not exact,because patients with only 76% function of the facialmuscles obtained a maximum points score of 10, sothat it is impossible to � nd out how many patientsregained normal function. However, the conclusionwas that the treated group experienced fuller recoveryand less severe complications.
After the initial publication of Adour et al. (59),several series of treatments with prednisone for Bell’spalsy were designed, but almost all of them were ofunsatisfactory quality. Nevertheless, the majority ofauthors claimed that they had shown steroids to bebene� cial to a statistically signi� cant degree. Oneexception was the report of May et al. (60) in 1976.They concluded that there was no proven ef� cacioustreatment for Bell’s palsy. Unfortunately the materialwas too small to permit a valid statistical analysis.Burgess et al. (61) described the problems in 1984,but more recently designed trials do not ful� ll therequirements for a clinical study (Table XIX). In acomprehensive review of the literature in 1987,Stankiewicz (62) concluded that ‘‘A de� nitive statisti-

E. Peitersen20
cally valid study considering the bene� t of steroids inthe treatment of idiopathic facial nerve palsy has yetto be performed’’. Prescott (63) in 1988 could notdemonstrate any effect of prednisone treatment in879 patients.
Based on the conclusion of Stankiewicz, Austin etal. (64) in 1993 concluded that a randomized con-trolled study to evaluate the ef� cacy of oral steroidsin the treatment of idiopathic facial nerve palsy wasnecessary. They published a well-designed study com-paring the use of oral prednisone versus placebo inthe treatment of idiopathic facial nerve palsies. It wasobvious that only one objection could be raisedagainst the trial, albeit a very serious one. There weretoo few patients in the study (n¾76) to enablestatistically signi� cant conclusions to be drawn (61).Nevertheless the conclusion was that patients treatedwith prednisone had less denervation and a signi� -cant improvement in the facial grade of recovery thanthe placebo-treated patients. No differences werefound between the two groups in terms of the timeperiod for recovery, the percentage of patients withsynkinesis and the percentage of patients withcrocodile tears. Both synkinesis and crocodile tearsare caused by degeneration and so it is not easy to seehow the treatment could help when the time ofrecovery and the percentage of patients with synkine-sis were the same in the prednisone- and placebo-treated groups.
Shafshak et al. (65) performed a prospective studyon 160 unilateral non-recurrent Bell’s palsy patientstreated with prednisone at suggested suf� cient doses.The study was randomized, but there was a malepredominance (129 males, 31 females) and placebowas not used. The number of patients was less thanhalf that required to draw statistically signi� cantconclusions (61). Statistical comparison between thecontrol group and the steroid subgroups revealed thatpatients who started prednisone intake within 24 h ofonset had a signi� cantly better recovery than those inthe control group, but only 23 patients bene� ted in
this way. Furthermore, there was no signi� cant dif-ference in outcome between patients in the controlgroup and those who started prednisone intake \24h after onset. The study showed that only 23:93patients treated bene� ted from the medication.
Ramsey et al. (66) in 2000 conducted a meta-analy-sis to evaluate facial recovery in patients with com-plete idiopathic facial nerve paralysis by comparingoutcomes of those treated with prednisone therapywith outcomes of those treated with placebo or withno treatment. A total of 47 trials were identi� ed; 20of these trials were excluded because they were retro-spective and 24 prospective studies were excluded fora variety of reasons such as lack of outcome, multiplemedical or surgical treatments or a steroid dose thatdid not meet the inclusion criteria. Therefore onlythree trials were assessed to meet the inclusion crite-ria, namely those by May et al. (60), Austin et al. (64)and Shafshak et al. (65). The meta-analysis of Ram-sey et al. (66) is a considerable piece of work butseems to contain some illogical statements. Althoughthe statistical analysis is extremely thorough, the datawere manipulated: initially three trials (60, 64, 65)were included but later the trial of May et al. (60)was excluded because of the small sample size thatshowed a worse outcome with the use of steroidtreatment. Consequently, a pooled analysis from theother two trials was presented. A minor problem withthe meta-analysis is the incorrect number of subjectsmentioned by May et al. (60) and by Austin et al.(64). A more serious problem is that the numbers ofpatients in all three trials are too small and even acombination of the three samples does not give asuf� cient number of patients, according to Burgess etal. (61).
The meta-analysis of Ramsey et al. (66) concludesthat ‘‘Corticosteroid treatment provides a clinicallyand statistically signi� cant improvement in recoveryof function in complete idiopathic facial nerve paraly-sis’’. This conclusion is based on what is called ‘‘mar-ginal signi� cance’’ in the trial of Austin et al. (64) and‘‘signi� cance’’ in the study of Shafshak et al. (65).However, Shafshak et al. showed only a better recov-ery for the subgroup of 23 patients who began steroidintake within 24 h after the onset of palsy. Thereforeonly 23:93 patients treated bene� ted from the medi-cation. To the best of my knowledge I cannot see thatthe conclusion of the meta-analysis is correct becausethere is a marked discrepancy between the data ana-lyzed and the conclusion in the abstract.
Antiviral drugsIn 1996 Adour et al. (67) reported that combinedtreatment with prednisone»acyclovir restored 92%of patients to normal function but, as in these au-
Table XIX. Requirements for documentation of ther-apy for peripheral facial nerve palsies
Prospective studySuf� cient number of patientsNo selection of patientsClear inclusion and exclusion criteriaRandomized studyDouble-blind placebo studyFollow-up until restoration of normal function or for
1 yearExact description of sequelaeAdequate statistical analysisConclusions based on the results

Bell’s palsy 21
thors’ prednisone study from 1972 (59), a specialgrading system was used. Furthermore, 13% of pa-tients developed contracture and synkinesis, so thatthe proportion of patients who achieved a fair resultshould be reduced to 87%; again it is impossible tosee how many patients obtained full recovery. Fur-thermore, the patients in the study of Adour et al.were highly selected, with 80% having incompleteparesis. It should be stressed that :95% of initiallyincomplete paresis patients obtain normal functionwithout treatment. The follow-up used in this study(4 months) was too short. After 4 months it is notpossible to assess sequelae because contracture andsynkinesis have not developed to their full extent. Asmentioned above it is necessary to follow these pa-tients for 12 months until a steady state is attained.The number of patients in the study was also toosmall to permit statistical signi� cance (61). Adour etal. (67) found contracture and synkinesis in 13% ofthe acyclovir »prednisone-treated group and in 28%of the placebo (prednisone-treated) group. In 1972Adour et al. (59) had found contracture and synkine-sis in 15% of the prednisone-treated group and 21%of the untreated group. It is dif� cult to explain thedifference between the prednisone-treated groups in1972 and 1996. The placebo (prednisone-treated)group in the 1996 study had a worse outcome (28%)than the untreated group in 1972 (21%) and thisdiscrepancy is inexplicable. Despite this Adour et al.emphasized that the NET did not show degenerationin the steroid-treated group; they described contrac-ture and synkinesis in 15% of patients and as amatter of fact development of contracture as well assynkinesis requires severe degeneration (68).
A comparison between the present study, in whichpatients were not treated, and that of Adour et al.(67) shows no difference in the proportion of patientsachieving a fair outcome: 83% and 87%, respectively.As stressed above, the proportion of patients withincomplete paresis in the 2 studies was 30% and 80%,respectively.
Combined therapySome authors regard Bell’s palsy as an emergencythat should be treated using all available measuresagainst possible multiple factors. Therefore a combi-nation of medicine, electrical stimulation, physicaltherapy and sometimes even decompression opera-tion has been used. Sittel et al. (69) published aretrospective trial in 2000 that included 334 patientssuffering from sudden facial paralysis of unknowncause. Only 239 patients were recorded as havingbeen treated with a drug cocktail consisted of pred-nisone, dextran and pentoxifylline. The term an-tiphlogistic–rheologic infusion therapy (ARIT) has
been coined to describe this regimen. The majority ofpatients 173 (72%) had incomplete palsy and only 66(28%) had complete paralysis. Patients with incom-plete palsy obtained full recovery in 98% of cases, aresult which does not differ from the result (94%)obtained without treatment in this study. Patientswith complete paralysis regained normal function in77% of cases, as opposed to 61% of patients in thisstudy. It is surprising that in the study of Sittel et al.(69) diabetics obtained the same � nal outcome asnormal persons. In the present study it was foundthat only 25% of diabetics regained normal functionand, furthermore, they had recurrences more often.
When comparing trials of treatment of facialpalsies it is generally considered that treatmentshould start within 5 days after the onset of palsy.Most authors consider that treatment should last fora maximum of 10 days (18 days for ARIT). Thismeans that patients can be treated for up to 4 weeksafter the onset of palsy. The majority of trials (64, 65,67) require that treatment should start as early aspossible to prevent damage of the nerve; however,Sittel et al. (69) instead used a later start but a longertreatment period. It should be stressed that the trialof Sittel et al. did not use double blinding withplacebo and that it was a retrospective study with adrop-out rate of almost 30% and a high proportion(72%) of patients with incomplete paresis.
Conclusions
A review of the literature of the last century regard-ing the treatment of peripheral facial nerve paresisreveals three major problems:
1. The etiology of Bell’s palsy is unclear and, conse-quently, treatment options vary widely.
2. The spontaneous course of Bell’s palsy has notbeen systematically examined, so that it has beenimpossible to compare the effect of treatment withthe outcome of the natural history of the palsy.
3. Trials designed to prove the ef� cacy of a giventreatment are inadequate and do not ful� ll therequirements for a rigorous clinical study.
Although thermal methods, massage and facial ex-ercises are appreciated to a very large extent by thepatients, no controlled clinical trials have been pub-lished. These therapies may be considered to be formsof psychotherapy. Electrotherapy is not useful; inten-sive electrical stimulation may increase the risk ofcontractures and should be abandoned. Vasodilatorsare of doubtful value and no documentation of theireffect exists. In terms of surgery, there is no docu-mentation that any kind of surgery proves a betteroutcome for patients with idiopathic peripheral facialnerve palsies. No signi� cant ef� cacy could be demon-

E. Peitersen22
strated with either prednisone or combined pred-nisone »acyclovir treatment. Combined therapy withARIT does not improve the � nal outcome.
DISCUSSION
EtiologyThe aim of this study, as mentioned above, is not todiscuss all possible theories but instead to describe thenatural history of Bell’s palsy. For reviews, see Mieh-lke (14) and May (21). The original cold hypothesishas been improved to an edema theory, which indi-cated the necessity of surgery. However, is the edemaessential? It is in no way speci� c and can, in humans,be caused by many insults. Trauma, burns, infections,bacteria, viruses and irradiation can also cause edemain tissue. The edema is a result of damage to thenormal tissue structure and is not a disease. Thetemporal bone contains a narrow canal with the facialnerve inside and pressure from the edema will damagethe nerve. However, the edema is a secondary effectcaused by several known and unknown factors, whichshould be considered as the primary effect. To date noproof has been given of the importance or conse-quence of the edema. During parotidectomia the facialnerve swelled to twice its normal diameter as a resultof manipulation in dif� cult cases; however, no paresisdeveloped. Steroids have been given to counteract thein� ammatory edema, but their effect has not yet beenproven.
Peripheral facial nerve paresis occurs in patientswith many different diseases and can also be caused byinfections, such as herpes zoster (21). Some idiopathicpalsies may resemble an infectious disease (70) or areactivation of HSV-1 (27) or other viruses, such asEpstein–Barr virus or cytomegalovirus (71). Recently,Vrabec and Payne (72), using a PCR assay, detectedHSV and varicella-zoster virus in 42% and 44%,respectively of cases of cranial nerve ganglia. Thetrigeminal, geniculate, vestibular, spinal and vagalganglia were examined. Vrabec and Payne concludedthat ‘‘In order to con� rm a viral etiology for variouscranial nerve disorders, demonstration of a signi� cantdifference in prevalence of the viruses in specimensfrom af� icted individuals will be necessary’’. This is alogical and thought-provoking conclusion; however, a� nal conclusion has yet to be drawn.
Natural historyThe aim of this study was to describe the spontaneouscourse of peripheral facial nerve palsies of unknownetiology. In addition to exposing the recovery pro� leof Bell’s palsy, insight was also gained into many otheraspects of the disease. One of the most important wasthat in order to draw statistically signi� cant conclu-
sions one requires a large number of patients; as aresult the number of sophisticated statistical calcula-tions required can automatically be reduced. When500 patients were collected no signi� cant conclusionscould be drawn for the subgroups. When the numberof patients reached 750 the situation looked better, butin some subgroups there was still no signi� cance.Having collecting 1,000 patients the conclusions weresigni� cant and did not change after reaching 1,700patients. The foolproof conclusion that can be drawnis that studies involving only a small number ofpatients are useless.
IncidenceInvestigators from the Mayo Clinic, Rochester, MNhave performed very careful analyses regarding theincidence of Bell’s palsy: Hauser et al. (73), in 1971,found the incidence to be 22 and Katusic et al. (74),in 1986, found an incidence of 25; however, the patientsamples in these two studies were small. Adour et al.(75), in 1978, found an incidence of 17–19 based ona sample of 1,048 patients. Devriese et al. (76), in 1990,based on a survey of :1,000 patients, found theincidence to be 20. In the present study the incidencewas estimated to be 32. I do not have de� nitiveknowledge of geographical and demographic differ-ences in the incidence of Bell’s palsy and thereforefurther investigations must be considered necessary inorder to solve this problem.
Recurring and familial Bell’s palsyThis sample includes 6.8% of Bell’s palsy patients whohad previously suffered from facial palsy on the sameor opposite side of the face. Ghiora and Winter (45),in a review of the literature between 1939 and 1960,reported recurrence rates of 4.5–15%. Park andWatkins (48) found a 7% recurrence rate in a sampleof 440 patients. Adour et al. (75) described previousparalysis in 9.3% of a group of 1,000 patients. Devrieseet al. (76) found an 8.6% recurrence rate in a sampleof 1,235 patients.
Several case reports of familial Bell’s palsy haveappeared in the literature, e.g. Knudstrup (77). DeSanto and Schubert (78) observed 10 cases in a familyand Willbrand et al. (79) reported 29 cases in a singlefamily. The familial incidence of Bell’s palsy in thisstudy was 4.1% and in 1 family 18 cases were observedover 3 generations during a 58-year period.
Both the recurrence rate and familial incidence ofBell’s palsy are surprisingly high. Genetics may play arole, but knowledge of which factors are actuallyinherited remains unknown. The association betweenhuman leukocyte antigen and Bell’s palsy is stillunclear (80). Further genetic studies are needed toresolve these problems.

Bell’s palsy 23
Seasonal variation and clusteringNo seasonal variation or clustering was evident inthis sample and furthermore no variation from yearto year or from one decade to another could bedemonstrated (Fig. 1). Adour et al. (75) did notobserve signi� cant differences in the number of casesoccurring during the cold and warm seasons andneither did they report any epidemic incidence. De-vriese et al. (76) reported that far more cases of Bell’spalsy were seen during the last 3 months of the year.Parry and King (81), in a 25-year study including 516patients, found a slight, but non-signi� cant, tendencyfor the condition to be more common during thewinter months. Park and Watkins (48) found nostatistically signi� cant seasonal variation in a sampleof 500 cases. Leibowitz (82) analyzed the time distri-bution of 499 consecutive cases of Bell’s palsy andfound it to be statistically different from the distribu-tion of independent cases, because the cases appearedin clusters. The explanation for the � nding of sea-sonal variation or clustering in some samples couldbe that the number of patients was too small. Thelack of seasonal variation must be noted but exertsno in� uence on the etiology, even if it de� nitelyeliminates any possibility of epidemic viral infections.
Sex distributionThe question of a gender predominance among pa-tients af� icted with idiopathic facial palsy has beendiscussed in the literature, without any conclusionsbeing drawn. One of the main reasons for the discus-sion has again undoubtedly been the small amount ofmaterial available. This investigation included 1,701patients with Bell’s palsy, 818 of whom were maleand 883 female, a gender ratio equal to that in thegeneral population. In almost all trials no compari-son has been made between the sex distributions inthe patients and in the general population. Adour etal. (75) found the proportions of males and femaleswith Bell’s palsy to be about equal. Devriese et al.(76) reported more men than women in their samplebut the difference was not signi� cant and no com-parison was made with the general population. Incontrast, Park and Watkins (48) found palsy to bemore frequent in women than in men; however, againthe sex distribution was not compared to that in thegeneral population and the study included only 450patients.
Side of the face
There is no disagreement in the literature about thisaspect of Bell’s palsy. The largest patient samples (75,76, this study) show no signi� cant difference in thenumber of palsies of the right and left sides of theface.
Age distributionThis study showed that the incidence of Bell’s palsyreaches a maximum between the ages of 15 and 45years and that the disease is signi� cantly less commonbelow the age of 15 years and above 60 years of age.It should be stressed that it is very important tocompare the age distribution of the patients with thatof the underlying population, because the differentage groups are not of equal size. In spite of this, thelargest series (48, 63, 75, 76) showed the highestfrequencies of Bell’s palsy in the second, third andfourth decades.
Time of beginning recovery and � nal outcomeThe number of days between the onset of paresis andthe beginning of remission of function is a verycrucial time, during which the fate of the nerve isdetermined (Fig. 7). In this study, 94% of patientswith incomplete paresis experienced full recovery. Ofthose who showed signs of remission in the � rst andsecond weeks, 88% and 83%, respectively experiencedfull recovery. There was no signi� cant difference inoutcome between patients who showed signs of re-mission in the � rst and second weeks, but remissionin the third week was associated with a signi� cantlyworse outcome (61%). After 3 weeks a period withoutremission occurred which lasted until :3 monthsafter the onset of the palsy and this is referred to as‘‘the hibernation of the facial nerve’’. These patientsunderwent total degeneration and did not regainnormal function, as previously stressed by Taverner(68) in 1965.
Ramsey et al. (66) concluded that the literatureclearly shows that virtually all patients with clinicallyincomplete paresis have excellent recovery of facialfunction, independent of treatment: in this study arate of 94% was found, Parry and King (81) found arate of 96% and Sittel et al. (69) a rate of 98%. In thegroup with initially complete Bell’s palsy in thisstudy, 61% regained normal facial muscle function.In contrast, Ramsey et al. (66) did not ‘‘expect’’ toobserve full recovery in \40% of the patients withparalysis. Steroid treatment was ‘‘expected’’ to im-prove the recovery rate to :57%. Therefore thereseems to be no difference between the percentage ofrecovery observed in the present study and in thesteroid-treated patients.
Age-dependent recoveryAge is another parameter that in� uences the � nalresult (Fig. 8). Children have the most favorableprognosis, with 90% experiencing full recovery.Above the age of 60 years, only about one-third ofpatients will experience the return of normal func-tion. Adour and Wingerd (83) described a worse

E. Peitersen24
outcome for patients aged \60 years. Prescott (63)and Devriese et al. (76) emphasized that the age ofthe patients was an important factor determiningrecovery. Katusic et al. (74) reported that those aged]55 years had a signi� cantly higher rate of incom-plete recovery. The in� uence of age on the � naloutcome is therefore highly signi� cant.
Postauricular painsIn this study, postauricular pains were registered in52% of all Bell’s palsy patients. Patients with painshave a signi� cantly worse prognosis than those with-out pains. Katusic et al. (74) evaluated prognosticfactors and reported that pain other than in the earhad a signi� cant relationship with incompleterecovery.
The prognostic value of topographica l testsFigure 9 shows the prognostic value of the threetopographical tests: taste, stapedius re� ex and naso-lacrimal re� ex. In the literature a dry eye has alwaysbeen associated with a bad � nal outcome. Adour andWingerd (83), May et al. (60) and Katusic et al. (74)found a worse outcome in patients with dry eyes.
HypertensionThe in� uence of hypertension on the outcome ofBell’s palsy is controversial. Adour and Wingerd (83),in a sample of 446 patients with Bell’s palsy, found 55(12%) with hypertension and demonstrated a signi� -cantly higher risk of a worse outcome in these pa-tients. Devriese et al. (76), in a sample of 1,235patients with Bell’s palsy, diagnosed 145 patients(13%) with hypertension. They attributed the worseoutcome for the patients with hypertension to thehigher age of those patients.
In this study, 134:1,701 patients (8%) suffered fromhypertension. A total of 264 patients were aged \60years and 37 of these patients (14%) had hyperten-sion. Bell’s palsy did not occur at a higher frequencythan expected in patients with hypertension. Thefrequency of sequelae in patients with hypertensiondid not differ from that in the group with normalblood pressure. Katusic et al. (74) con� rmed thehypothesis that hypertension is a risk factor for Bell’spalsy and also concluded that increasing age resultedin a greater frequency of incomplete recovery. Theimportance of comparing hypertensive patients withnon-hypertensive patients of equal age should beemphasized.
This study (Fig. 8) shows that recovery depends toa very large extent on age, as also stressed by De-vriese et al. (76), so the connection between advancedage and hypertension would seem to be a coinci-dence. Another explanation for this � nding may be
misdiagnosis of an incomplete central paresis as aperipheral paresis.
SequelaeThe factors determining the degree of sequelae areparesis, contracture and associated movements (Ta-bles IX and X). The mechanism that causes contrac-ture is not known in detail, but some degree ofregeneration is necessary. Contracture is almost al-ways combined with associated movements or synki-nesis caused by misdirection of the nerve � bersduring regeneration. It is necessary to follow thesepatients for 1 year, until a steady state is attained.
In this study, associated movements and contrac-ture were found in 16% and 17% of patients, respec-tively. Adour and co-workers (59, 67) foundcontracture and synkinesis in 15% of prednisone-treated patients and 21% of untreated patients, re-spectively in 1972 and in 28% of prednisone(placebo)-treated patients and 13% of acyclovir»prednisone-treated patients, respectively in 1996.Austin et al. (64) described synkinesis in 13% of bothsteroid-treated and untreated patients. Therefore,prednisone does not seem to prevent sequelae.
How to avoid misdiagnosis of Bell’s palsy?Although Bell’s palsy is the commonest form ofperipheral nerve palsy, care should be taken not tomisdiagnose any palsy as idiopathic. Although someworkers try to determine the etiology by using a widerange of tests, this approach is not always successful.The symptomatology of Bell’s palsy is not speci� cand if the acute phase of the palsy does not affect allbranches it is important to consider another etiologybecause a partial palsy of one or two branchesstrongly suggests disease localized distally from thestylomastoid foramen, and may indicate a cancer inthe parotid gland.
If symptoms from other cranial nerves are ob-served an obvious supposition would be viral infec-tion or neoplastic disease. In 75% of cases aperipheral facial palsy caused by herpes zoster showsacoustic and:or vestibular disturbances. The diagno-sis can be veri� ed by CSF or serological tests iftypical vesicles are not seen. If endocrinopathic dis-eases are suspected, diabetes mellitus is a possibilityand can be veri� ed by a glucose tolerance test. If theparotid gland is enlarged and eye symptoms areobserved, sarcoidosis is a possibility and can be ver-i� ed by lung X-ray and possibly by mediastinoscopywith gland biopsy. A recurrent palsy should be exam-ined using standard investigations and, in addition,eye and neurological examinations should be per-formed. CT scans of the facial nerve canal should bemade even if pathology seldom occurs. Of 69 patients

Bell’s palsy 25
with recurrent Bell’s palsy in this study, only one hada pathology of the facial nerve canal, a bi� d canalanswering to the third part which shows that this typeof pathology is very rare.
Among 13 other patients with recurrent palsy ofdifferent etiologies 1 patient with ear cholesteatomawas found. Another had pronounced destruction ofthe second part of the bony canal involving thegeniculate ganglion region. Upon surgery a tumor wasfound and histology revealed the same picture as thatof a breast cancer for which the patient had beentreated 27 years earlier. Another patient with radiolog-ically demonstrable destruction of the temporal bonesuffered from Paget’s disease.
As mentioned before, Bell’s palsy is an acute,monosymptomatic , peripheral facial palsy of un-known etiology. A monosymptomati c diagnosis isrequired in order to distinguish the paresis fromtick-borne B. burghdorferi infection, collagenosis andpolyneuritis, for which the symptoms are polysymp-tomatic. Speci� c laboratory tests are required in orderto differentiate between many of these diseases.
Table II shows the timetable for examinations ofperipheral facial nerve palsies. Using a follow-uptimetable with short intervals between visits providesmany chances for assessing and reassessing the diagno-sis. Furthermore, supplementary tests can also beperformed. In this study the preliminary diagnosis waschanged during follow-up in :2% of all patients.
Side -effectsSurprisingly, very few of the publications that havetried to prove the effect of steroids have revealed thefrequency and severity of side-effects. Elderly patientsare excluded from many trials because the treatmentcould cause severe side-effects. It is obvious that theresults of such studies would be over-exaggerated ,because age is a very important factor determiningrecovery (63, 74, 76, 83; Fig. 8).
A drug as potent as prednisone, given in high doses,is estimated to produce side-effects in :10% ofpatients. Adour et al. (59) used one of these side-effectsas a indication for treatment: the treated patients wereeuphoric and the untreated patients asked for treat-ment.
PsychotherapyAll patients with acute peripheral facial nerve palsycomplain of anxiety. The best way to help thesepatients is to explain that the symptoms are caused notby a stroke but by a lesion of the peripheral facialnerve, maybe of unknown etiology. The patient shouldbe informed that 85% of patients begin recovery within2–3 weeks and that in the other 15% beginningfunction is obtained within 3–5 months. All patients
are tested according to the scheme shown in Table IV.Patients should be told that 3:4 patients achieve fullrecovery with normal mimical facial function within3–4 months.
Follow-up of patients should occur once a weekinitially. It is essential that patients feel better, are lessdepressed after the consultation and are looking for-ward to beginning recovery. Many patients feel com-fortable with moderate heat applied to the paretic sideof face. Facial exercises have a great psychologicaleffect: when function starts to return the patient cansee the improvement. In my experience giving thepatient information and repeating follow-up is the bestway to help them; however, it should be stressed thatthere is no documentation of the ef� cacy of any kindof treatment.
EthicsThe Third International Nerve Symposium was held inZurich in 1976. The Swedish professor Hamberger (84)participated in a panel discussion and stressed theimportance of thorough examinations, frequent fol-low-up and the provision of detailed information forpatients with peripheral facial nerve palsies. No treat-ment was given by Hamberger with the exception ofpsychotherapy, which included mild physiotherapy.This seems to me to be a honest way to managepatients with peripheral facial palsies. Nevertheless,Katusic et al. (74) from the Mayo Clinic expressed ina publication from 1986 that ‘‘The extreme attitude,according to Hamberger, is that of the Scandinavianphysicians who only treat patients with Bell’s palsywith physiotherapy or massage as a ‘psychologicaltreatment’ ’’ and continued: ‘‘Our results suggest thatindividual differences in patients may in� uence thetype of therapy chosen’’. A close reading of thepublication revealed a retrospective study of a smallsample without randomization. The trial was notdouble-blind or placebo-controlled and no indicationwas given as to how individual differences in patientsmay in� uence the type of therapy. Nevertheless, theauthors recommended treatment with prednisone. Us-ing high-dose prednisone is risky and, without docu-mentation of the � nal outcome, may be unethical.
It is time, after two to three decades, to requirevalid documentation before using prednisone. Thisraises an ethical problem: how can such a high-po-tency drug with marked side-effects have been used athigh doses for such a long time without documenta-tion? It is unbelievable and must raise a huge ethicaldilemma for those doctors who prescribe prednisonefor Bell’s palsy patients. Now we are back to theaccusation of Hamberger (84) by Katusic et al. (74).Hamberger does not have an ethical problem becausehe was honest. Katusic et al. do not have any basis

E. Peitersen26
for their accusation and treatment; this is an ethicalproblem of large dimensions and they are still usingthe drug without proof of its ef� cacy and whilst onlyinforming the patients of the bene� ts. Even worse isthe fact that the euphoric side-effect is used as anindication for the use of the drug (59), which is veryunethical.
Final remarksEvaluation of therapy for Bell’s palsy is madedif� cult by the spontaneous and usually completerecovery observed in the majority of patients. In thisstudy, 71% of all patients regained normal facialmuscle function.
In a trial of treatment only :20% of patients needthe treatment, meaning that a large number of pa-tients are required in order for the trial to be valid.According to Burgess et al. (61) at least 200 patientsare required in both the treated and placebo groups.The most striking � aw of many trials is the insuf� -cient number of patients enrolled. In many trials theaim seems to be to show the effect of a given treat-ment rather than to make an objective evaluation ofthe data and a statistical analysis. It seems obviousthat bias is unavoidable (85). Furthermore, dis-crepancies are often found between the results of thedata analyzed and the conclusions. Careful reading iscrucial.
As mentioned above, no documentation of theef� cacy of physiotherapy, electrotherapy or surgeryhas been given. In a review of the literature in 1987,Stankievicz (62) concluded that a de� nitive and statis-tically valid study considering the bene� t of steroidsin the treatment of Bell’s palsy had yet to be per-formed. Even today the situation remains unchanged,because no valid study to prove the effectiveness ofpredisone has been published.
Maybe it is time to investigate new directions in thetreatment of Bell’s palsy. A parallel can be drawnwith Guillain–Barre syndrome (86), an acute im-mune-mediated polyradiculoneuropathy preceded byan infection with Campylobacter jejuni, mycoplasma,cytomegalovirus or Epstein–Barr virus. Today’streatment is i.v. immunoglobulin in high doses (87).Steroids do not help these patients, but were used formany years.
It would be most logical to � rst prove the etiologyof Bell’s palsy, as it is obvious that the best treatmentfor a disease can be given when its etiology is known.Bell’s palsy is not a disease sui generis but a paresiscaused by several known and unknown generatingfactors. When is the optimal time to start treatment?Generally, all kinds of treatment should be started assoon as possible, as long as the diagnosis is con� -rmed. The electrophysiological examinations per-
formed by Langworth and Taverner (32), Olsen (34)and Esslen (35) showed that degeneration occurredwithin 7–10 days. Based on these results, the ten-dency was to start treatment, either surgery or pred-nisone treatment, as early as possible. Pulec (88, 89)advocated early decompression. Brown (90), Austinet al. (64) and Shafshak et al. (65) recommendedearly prednisone treatment. As stressed by Adour etal. (67), no electrical test is able to predict the out-come in all patients but ENoG seems to be the mostvaluable (91). When Wallerian degeneration hasstarted, it takes up to 3 days before the nerve isinexcitable; this means that one is always about 3days behind the progression of degeneration. The � rstweek seems to be the crucial time for the nerve tosurvive and if any treatment could help it is obviousthat it should be started as early as possible.
It is recommended that prospective investigatorsshould read the paper by Schulz et al. (85). Theconclusion is ‘‘This study provides empirical evidencethat inadequate methodological approaches in con-trolled trials, particularly those representing poor al-location concealment, are associated with bias.Readers of trial reports should be wary of thesepitfalls, and investigators must improve their design,execution, and reporting of trials’’. The tutorials byNeely and co-workers (92–95) are also highlyrecommended.
CONCLUSIONS
The Copenhagen Facial Nerve Study collected a largeamount of data and, based on an analysis of thesedata, the following statistically signi� cant conclusionscan be drawn.
Time of beginning recovery of function: early re-covery leads to excellent function and late recoveryimplies sequelae.Age of the patient: young patients have a goodprognosis and elderly patients a worse outcome.Topographical tests: a dry eye and abolished tasteand stapedius re� ex affect the prognosisnegatively.Postauricular pains: patients without pains faresigni� cantly better than those with pains.The incidence of Bell’s palsy is estimated to be 32per 100,000 population per year.Recurrent palsies were found in 7% of Bell’s palsypatients and 4% of all cases of Bell’s palsy repre-sented familial Bell’s palsy.Seasonal variation and clustering were not foundand variations from year to year or from decade todecade could not be demonstrated because thein� ux of Bell’s palsy patients remained constantover the 25-year period of the study.

Bell’s palsy 27
The investigation clearly indicates that there is nodifference in the sex distribution of Bell’s palsypatients.There is no difference regarding left or right local-ization of Bell’s palsy.The age distribution of Bell’s palsy patients shouldbe compared with that of the underlying popula-tion. The incidence reaches a maximum betweenthe ages of 15 and 45 years. It is signi� cantly lesscommon below the age of 15 years and above theage of 60 years.Complete recovery was observed in 71% of allpatients. Males and females recovered in the sameproportions.Patients with incomplete paresis regained normalfunction in 94% of cases and those with completeparalysis regained normal function in 61% ofcases.All Bell’s palsy patients recovered to some extent:83% of all patients recovered with a fair result; 5%of patients were left with an unacceptably highdegree of sequelae.Normal function was regained within 3 months inabout two-thirds of all patients; after 6 months noadditional patients regained normal mimicalfunction.Sequelae were found as follows: residual paresis,29%; contracture, 17%; associated movements orsynkinesis, 16%; dry eye and crocodile tears, 2%.Bell’s palsy is not more frequent in hypertensivepatients and the prognosis in these patients is notworse than that in non-hypertensive patients; theconnection between advanced age and hyperten-sion would seem to be a coincidence.Pregnant women with peripheral facial nerve palsyregained normal function in 61% of cases.Paresis caused by herpes zoster was complete in88% of cases and incomplete in 12%. The progno-sis for these patients is bad, with normal recoveryin 21% and no recovery in 4%.Facial nerve palsy in diabetics was incomplete in62% of cases and complete in 38%. In spite of thehigh proportion of mild pareses the � nal outcome,as a result of polyneuropathy, was poor, with only25% regaining normal function.Bell’s palsy in children is uncommon and theprognosis is excellent, with 90% regaining normalfunction. The non-Bell’s palsy group had differentetiologies determining the prognosis. The incidenceof birth trauma facial nerve paresis has decreaseddramatically during the last 25 years, as a result ofimprovements in obstetrical techniques.Bell’s palsy has the best prognosis of all peripheralfacial nerve palsies.
Based on the experience of this investigation itshould be emphasized that clinical trials require alarge number of patients in order to be valid.
The facial nerve surgeon from London Sir TerenceCawthorne advised his assistants to examine facialnerve patients properly. It would be a catastrophe todiagnose facial palsy as idiopathic if the patient suf-fered from a severe disease:
‘‘All that glitters is not gold’’ (William Shakespeare)
‘‘All that palsies is not Bell’’ (Cawthorne)
For more than 35 years I have studied facial nerveparalysis and have learned that close reading of theliterature is crucial:
‘‘To be or not to be’’ (William Shakespeare)
‘‘To be skeptical’’ (Peitersen)
FUTURE DIRECTIONS
Regarding idiopathic peripheral facial nerve paraly-sis: where are we and where are we going? The focusshould be on the treatment. Today’s problems aresimilar to those encountered in the 1950s and 1960s,when facial nerve surgeons believed in decompressionoperations but never provided signi� cant documenta-tion of its ef� cacy. Prednisone treatment began in the1970s and increased dramatically in the 1980s and1990s, especially in the USA but less so Europe andhas never really been accepted in Scandinavia. Asurvey of the literature today reveals at least 100trials that have reported the effectiveness of pred-nisone treatment. Nevertheless no trial has ful� lledthe requirement for a clinical, randomized, double-blind study with a suf� cient number of patients andwith exact descriptions of the time of recovery andsequelae, including residual paresis, associated move-ments and contracture, graded after 1 year. This is avery depressing statement to make but nevertheless itis the truth.
Simple electrical tests have been used to predict thedegree of denervation. Based on these results the � naloutcome was predicted, but this was not based on aclinical examination after 1 year. The value of electri-cal tests has been overestimated. If the nerve isinexcitable then Wallerian degeneration must havebegun 3 days previously and the denervation has tobe accepted. There is no test available that can tell usearly enough what has happened to the nerve. Fromthis point of view any viable treatment should bebegun as early as possible. But is there a drug ofchoice? Not yet is the correct answer. Early treatmentraises another problem: :80% of Bell’s palsy pa-tients do not need treatment and it may be unethicalto treat this group, given the chance of side-effects.

E. Peitersen28
The enormous use of prednisone over the last twodecades is a huge problem. To use a potent drug witha high risk of side-effects, but without documentedef� cacy, is unethical. Although patients bene� t fromthe euphoric side-effect they do not have the chanceto differentiate between the effect and the side-effect.In my opinion this seems to represent a real ethicalproblem for doctors. The time has come to stop theuse or misuse of prednisone, to be honest with thepatients and to accept that there is no effective treat-ment for Bell’s palsy.
Future etiologic studies should be expanded toreveal the pathogenesis of Bell’s palsy. Obtainingadditional knowledge may open the door for a spe-ci� c treatment. Last but not least, how can the effectof all kinds of treatment be explained? Only byfollowing the spontaneous course of idiopathic pe-ripheral facial nerve palsy.
ACKNOWLEDGMENTS
I wish to express my sincere gratitude to the following: mycolleagues, for their support and for supplying me with thepatients for the study; Mr. Arne Nørby Rasmussen andMr. Poul Aabo Osterhammel, for performing the statisticaldata analyses; my secretary, Bente Rasmussen, for typingthe manuscript with great accuracy; my daughter, Anette,for helping me with the translation and for correcting thelanguage; and the board of the Danish Society of Otolaryn-gology—Head & Neck Surgery for providing � nancialsupport from Oda Pedersen’s Research Fund.
REFERENCES
1. Bell C. On the nerves: giving an account of someexperiments on their structure and functions whichleads to a new arrangement of the systems. PhilosTrans R Soc London 1821; 111: 398–424.
2. Resende LAL. Peripheral facial paralysis in history. In:Castro D, ed. The facial nerve. Amsterdam: Kugler &Ghedini, 1988: 65–75.
3. Kindler W. Die Fazialislahmungen in der Darstellender Kunst seit mehr als vier Jahntausenden. Z LaryngolRhinol Otol 1969; 48: 135–9.
4. Freud S. The standard edition of the complete psycho-logical works. London: Hogarth Press, 1973.
5. Hjortso CH. Manniskans ansikte ock mimiska spraÊ ket.Malmo, Sweden: Studenterlitteratur Forlagshuset Nor-den AB, 1969.
6. Gombrich EH. Kunstens historie. Copenhagen: SteenHasselbalch’s Forlag, 1960.
7. Lange-Eichbaum W, Wolfram K. Irrsinn und Ruhm.Munich: Ernst Reinhardt Verlag, 1967.
8. Marcus Aa. Leonardo da Vinci. Copenhagen: Gylden-dals Uglebøger, 1964.
9. Nielsen SJ. Mona Lisa’s gaÊ defulde smil. Ugeskr Laeger1975; 137: 1668–9.
10. Kataye S. La paralysic faciale selon Avicenne. AnnOtolaryngol Chir Cervicofac 1975; 92: 79–82.
11. Bird TD. Nicolaus A. Friedreich’s description of pe-ripheral facial nerve paralysis in 1798. J Neurol Neuro-surg Psychiatry 1979; 42: 56–8.
12. Balance C, Duel AB. The operative treatment of facialpalsy. Arch Otolaryngol 1932; 15: 1–70.
13. Cawthorne T. Pathology and surgical treatment ofBell’s palsy. J Laryngol Otol 1951; 65: 792–804.
14. Miehlke A. Surgery of the facial nerve. Munich: Urban& Schwarzenberg, 1973.
15. Jongkees LBW. Treatment of Bell’s palsy. Neurology1957; 7: 697–702.
16. Fisch U. Total intratemporal exposure of the facialnerve. Arch Otolaryngol 1972; 95: 335–41.
17. Kettel K. Peripheral facial palsy, pathology andsurgery. Copenhagen: Munksgaard, 1959.
18. Danish Otolaryngological Society. Management of pe-ripheral facial palsies. Arch Otolaryngol 1965; 81: 441–546.
19. Sunderland S. A classi� cation of peripheral nerve in-juries producing loss of function. Brain 1951; 74: 491–516.
20. Sunderland S. Some anatomical and pathophysiologi-cal data relevant to facial nerve injury and repair. In:Fisch U, ed. Facial nerve surgery. Amstelveen:Birming-ham: Kugler:Aesculapius, 1977: 47–61.
21. May M. The facial nerve. New York: Thieme Inc,1986.
22. McGovern FH, Konigsmark BW, Sydnon JB. An im-munological concept for Bell’s palsy. Experimentalstudy. Laryngoscope 1972; 82: 1594–601.
23. McGovern FH, Estevez J, Jackson R. Immunologicalconcept for Bell’s palsy. Further experimental study.Ann Otol Rhinol Laryngol 1977; 86: 300–5.
24. McCormick DP. Herpes simplex virus as cause of Bell’spalsy. Lancet 1972; 1: 937–9.
25. Adour KK, Bell DN, Hilsinger RL Jr. Herpes simplexvirus in idiopathic facial paralysis (Bell’s palsy). JAMA1975; 233: 527–30.
26. Mulkens PSJZ, Bleeker JD, Schroder FP. Acute facialparalysis: a virological study. Clin Otolaryngol 1980; 5:303 –10.
27. Murakami S, Mizobuchi M, Nakashiro Y, Doi T,Hato N, Yanagihara N. Bell’s palsy and herpes simplexvirus: identi� cation of viral DNA in endoneurinal � uidand muscle. Ann Intern Med 1996; 124: 27–30.
28. Duchenne GB. De L’electrisation Localisee. Paris: Bail-liere, 1855: 372–401.
29. Blumenthal F, May M. Electrodiagnosis. In: May M,ed. The facial nerve. New York: Thieme Inc, 1986:241 –63.
30. Groves J, Gibson WPR. Bell’s (idiopathic facial) palsy.The nerve excitability test in selection of cases for earlytreatment. J Laryngol Otol 1974; 88: 851–4.
31. Laumans EPJ. Nerve excitability tests in facial paraly-sis. Arch Otolaryngol 1965; 81: 478–85.
32. Langworth EP, Taverner D. The prognosis in facialpalsy. Brain 1963; 86: 465–80.
33. Buchthal F. Electromyography in paralysis of the facialnerve. Arch Otolaryngol 1965; 81: 463–9.
34. Olsen PZ. Prediction of recovery in Bell’s palsy.Copenhagen: Munksgaard, 1975.
35. Esslen E. The acute facial palsies. Berlin: SpringerVerlag, 1977.
36. Boernstein WS. Cortical representation of taste in manand monkey. II. The localization of the cortical taste inman and a method of measuring impairment of taste inman. Yale J Biol Med 1949; 13: 133–48.
37. Jepsen O. Studies on the acoustic impedance of thetympanic membrane in normal individuals and in pa-

Bell’s palsy 29
tients with peripheral facial palsy. Aarhus, Denmark:Universitetsforlaget, 1955.
38. Zilstorff K. Modern oto-neurology. The progress fromacoustic-vestibular studies to cranial nerve diagnosis. JLaryngol Otol 1962; 76: 45–54.
39. House JW. Facial nerve grading systems. Laryngo-scope 1983; 93: 1056–69.
40. House JW, Brackmann DE. Facial nerve grading sys-tem. Otolaryngol Head Neck Surg 1985; 93: 146–7.
41. Botman JWM, Jonkees LBW. The result of intratem-poral treatment of facial palsy. Pract Otorhinolaryngol1955; 17: 80–100.
42. Hunt JR. A further contribution to herpetic in� amma-tions of the geniculate ganglion. Am J Med Sci 1908;136: 226–32.
43. Miehlke A. Die Chirurgie des Nervus facialis. Munich:Urban & Schwarzenberg, 1960.
44. Dickins JR, Smith JT, Graham SS. Herpes zosteroticus: treatment with intravenous acyclovir. Laryngo-scope 1988; 98: 776–9.
45. Ghiora A, Winter ST. The conservative treatment ofBell’s palsy. A review of the literature, 1939–1960. AmJ Phys Med 1962; 41: 213–27.
46. Mosforth J, Taverner D. Physiotherapy for Bell’spalsy. BMJ 1958; ii: 675–7.
47. Williams HL. Bell’s palsy. Arch Otolaryngol 1959; 70:436–43.
48. Park HW, Watkins AL. Facial paralysis. Analysis of500 cases. Arch Phys Med 1949; 30: 749–61.
49. Wolferman A. The present status of therapy of Bell’sparalysis: a critical evaluation. Ann Otol Rhinol Laryn-gol Suppl 1974; 12: 1–15.
50. Korkis FB. A treatment of recent Bell’s palsy on arational etiological basis. Arch Otolaryngol 1959; 70:562–9.
51. Fearnley ME, Rainer EH, Taverner D, Boyle T McM,Miles DW. Cervical sympathetic block in treatment ofBell’s palsy. Lancet 1964; i: 725–7.
52. Jongkees LBW. On the histology of Bell’s palsy. ActaOtolaryngol (Stockh) 1954; 44: 336–43.
53. Kettel K. Danish Otolaryngological Society Sympo-sium. Management of peripheral facial palsies. ArchOtolaryngol 1964; 81: 462.
54. Fisch U. Surgery for Bell’s palsy. Arch Otolaryngol1981; 107: 1–11.
55. Linder T. Facial nerve decompression: still justi� ed?Laryngorhinootologie 2000; 79 (Suppl 1): 174.
56. Gantz BJ, Rubinstein JT, Gidley P, Woodworth GG.Surgical management of Bell’s palsy. Laryngoscope1999; 109: 1177–88.
57. Yanagihara N, Hato N, Murakami S, Honda N.Transmastoid decompression as a treatment of Bellpalsy. Otolaryngol Head Neck Surg 2001; 124: 182–6.
58. Taverner D. Cortisone treatment of Bell’s palsy. Lancet1954; ii: 1052–4.
59. Adour KK, Wingerd J, Bell DN, Manhing JJ, HurleyJP. Prednisone treatment for idiopathic facial paralysis(Bell’s palsy). N Engl J Med 1972; 287: 1268–72.
60. May M, Wette R, Hardin WB Jr, Sullivan J. The use ofsteroids in Bell’s palsy: a prospective controlled study.Laryngoscope 1976; 86: 1111–22.
61. Burgess LPA, Yim DWS, Lepore ML. Bell’s palsy: thesteroid controversy revisited. Laryngoscope 1984; 94:1472 –6.
62. Stankiewicz JA. A review of the published data onsteroids and idiopathic facial paralysis. OtolaryngolHead Neck Surg 1987; 97: 481–6.
63. Prescott CAJ. Idiopathic facial nerve palsy (the effectof treatment with steroids). J Laryngol Otol 1988; 102:403 –7.
64. Austin JR, Peskind SP, Austin SG, Rice DH. Idio-pathic facial nerve paralysis: a randomized doubleblind controlled study of placebo versus prednisone.Laryngoscope 1993; 103: 1326–33.
65. Shafshak TS, Essa AY, Bakey FA. The possible con-tributing factors for the success of steroid therapy inBell’s palsy: a clinical and electrophysiological study. JLaryngol Otol 1994; 108: 940–3.
66. Ramsey MJ, Der Simonian R, Holtel MR, BurgessLPA. Corticosteroid treatment for idiopathic facialnerve paralysis: a meta-analysis. Laryngoscope 2000;110: 335–41.
67. Adour KK, Ruboyianes JM, von Dorrsten PG, et al.Bell’s palsy treatment with acyclovir and prednisonecompared with prednisone alone: a double-blind, ran-domized, controlled trial. Ann Otol Rhinol Laryngol1996; 105: 371–8.
68. Taverner D. Treatment of facial palsy. Arch Otolaryn-gol 1965; 81: 489–93.
69. Sittel C, Sittel A, Guntinas-Lichius O, Eckel HE, Sten-ners E. Bell’s palsy: a 10-year experience with antiphlo-gistic-rheologic infusion therapy. Am J Otol 2000; 21:425 –32.
70. Jonsson L. On the etiology of Bell’s palsy. Immunolog-ical and magnetic resonance imaging abnormalities.Uppsala, Sweden: Acta Universitatis Upsaliensis, 1987.
71. Hyden D, Roberg M, Forsberg P, et al. Acute ‘‘idio-pathic’’ peripheral facial palsy. Clinical, serological andcerebrospinal � uid � ndings and effects of corticos-teroids. Am J Otol 1993; 14: 179–86.
72. Vrabec JT, Payne DA. Prevalence of herpes viruses incranial nerve ganglia. Acta Otolaryngol 2001; 121:831 –5.
73. Hauser WA, Karnes WE, Annis J, Kurland LT. Inci-dence and prognosis of Bell’s palsy in the population ofRochester, Minnesota. Mayo Clin Proc 1971; 46: 258–64.
74. Katusic SK, Beard CM, Wiederholt WC, BergstralhEJ, Kurland LT. Incidence, clinical features, and prog-nosis in Bell’s palsy, Rochester, Minnesota 1968–1982.Ann Neurol 1986; 20: 622–7.
75. Adour KK, Byl FM, Hilsinger RL Jr, Kahn ZM,Sheldon MI. The true nature of Bell’s palsy: analysis of1000 consecutive patients. Laryngoscope 1978; 88:787 –801.
76. Devriese PP, Schumacher T, Scheide A, De jonge RH,Houtkooper JM. Incidence, prognosis and recovery ofBell’s palsy. A survey of about 1000 patients (1974–1983). Clin Otolaryngol 1990; 15: 15–27.
77. Knudstrup P. Familial peripheral facial palsy. DanMed Bull 1964; 11: 224–6.
78. De Santo LW, Schubert HA. Bell’s palsy: ten cases ina family. Arch Otolaryngol 1969; 89: 700–2.
79. Willbrand JW, Blumhagen JD, May M. Inherited Bell’spalsy. Ann Otol Rhinol Laryngol 1974; 83: 343–6.
80. Shibahara T, Okamura H, Yanagihara N. A possibleassociation of HLA with Bell’s palsy as an etiologicalgenetic factor. In: Castro D, ed. The facial nerve.Amsterdam: Kugler & Ghedini, 1988: 323–5.
81. Parry CBW, King PF. Results of treatment in periph-eral facial paralysis. J Laryngol Otol 1977; 91: 551–64.
82. Leibowitz U. Epidemic incidence of Bell’s palsy. Brain1969; 92: 109–14.

E. Peitersen30
83. Adour KK, Wingerd MA. Idiopathic facial paralysis(Bell’s palsy): factors affecting severity and outcome in446 patients. Neurology 1974; 24: 1112–6.
84. Hamberger C-A. Panel discussion no. 9: incidence andmanagement of Bell’s palsy according to geographicdistribution. In: Fisch U, ed. Facial nerve surgery.Amstelveen:Birmingham: Kugler:Aesculapius, 1977:334.
85. Schulz KF, Chalmers I, Hayes RJ, Altman DG. Empir-ical evidence of bias. Dimensions of methodologicalquality associated with estimates of treatment effects incontrolled trials. JAMA 1995; 273: 408–12.
86. Ropper AH. The Guillain-Barre syndrome. N Engl JMed 1992; 17: 1130–6.
87. Van der Meche FGA. Intravenous immuneglobulin inthe Guillain-Barre syndrome. Clin Exp Immunol 1994;97 (Suppl 1): 43–7.
88. Pulec JL. Bell’s palsy: diagnosis, management and re-sults of treatment. Laryngoscope 1974; 39: 185–94.
89. Pulec JL. Early decompression of the facial nerve inBell’s palsy. Ann Otol Rhinol Laryngol 1981; 90: 570–7.
90. Brown JS. Bell’s palsy: a 5 year review of 174 consecu-tive cases: an attempted double blind study. Laryngo-scope 1982; 92: 1369–73.
91. Engstrom M. Magnetic resonance imaging, electroneu-rographic, and clinical � ndings in Bell’s palsy. Uppsala,Sweden: Acta Universitatis Upsaliensis, 1998.
92. Neely JG, Hartman JM, Wallace MS. Building thepowerful 10-minute of� ce visit. Part I: introductionto the new section. Laryngoscope 2000; 110: 1595–601.
93. Neely JG, Hartman JM, Wallace MS. Building thepowerful 10-minute of� ce visit. Part II: beginning acritical literature review. Laryngoscope 2001; 111: 70–6.
94. Neely JG, Hartman JM, Wallace MS, Forsen JW Jr.Tutorials in clinical research: Part III: selecting a re-search approach to best answer a clinical question.Laryngoscope 2001; 111: 821–31.
95. Hartman JM, Forsen JW Jr, Wallace MS, Neely JG.Tutorials in clinical research: Part IV: recognizing andcontrolling bias. Laryngoscope 2002; 112: 23–31.
Address for correspondence:Erik Peitersen, MD, DMScDepartment of Otorhinolaryngology
Head & Neck SurgeryRigshospitaletBlegdamsvej 9DK-2100 Copenhagen ØDenmarkTel.: »45 35 45 23 77Fax.: »45 35 45 26 90E-mail: [email protected]