behavioural activation: an alternative to cognitive ... · behavioural activation: an alternative...
TRANSCRIPT

Art & science depression
Behavioural activation: analternative to cognitivebehaviour therapy
Correspondence
Jessica Price ¡s a psychologicaltherapist, Solent NHS Trust,Talking Change PsychologicalServices, Portsmouth
Date of submissionJuly 11 2012
Date of acceptanceMarch 1 2013
Peer review
This articie has been subject
to double-blind review and
has been checked using
antipiagiarism software
Author guidelines
http://mhp.rcnpubiishing.com
Jessica Price explains how a client with low mood andrelationship difficulties was helped to set goals, increaseher motivation for change and re-engage in life
AbstractThis case study describes how behavioural activation
was used to treat a client with depression who
had undergone previous psychologicai treatments
including cognitive behaviour therapy. After
assessment and formulation of problems and goals,
a treatment plan was structured to increase contact
with positive activities and previously avoided
situations, people and pursuits. Collaborative
recovery-orientated work on this plan resulted in
improvements confirmed by self-rating scores and
subjective reports. Thus, the behavioural activation
sessions provided an effective alternative
evidence-based treatment of the depression.
Keywords
Behavioural activation, cognitive behaviour therapy,
depression, evidence-based practice
BEHAVIOURAL ACTIVATION (BA) is a psychosocialapproach for the treatment of depression that isrecommended by the National Institute for Healthand Care Excellence (NICE) (2009). BA is based on theidea that depression persists because of behaviouralchanges arising from the person's initial depression.Withdrawal and non-engagement can contribute to alack of positive reinforcement that would normallyresult from everyday activities, and this in turncan lead to greater feelings of depression; therebyfuelling a negative vicious cycle.
Research has indicated that behaviouralcomponents of cognitive behaviour therapy (CBT)(Beck ef al 1979) performed as well as the full
CBT package at treatment (Jacobson et al 1996).This finding promoted the development of BAas a stand-alone intervention for depression andother disorders. Sturmey (2009) conducted asystematic review of BA treatment for depression.The outcomes of BA were found to be consistentlysuperior compared with control groups.
Sturmey (2009) asserted that BA may be moreeffective than CBT in terms of lower client dropoutand could be more useful with some people forwhom CBT is less effective; these included thosewith severe, lifelong depression, people who misusesubstances and those experiencing dementia withsevere depression. BA has also been evaluated byseveral independent research groups for diverseproblems, including post-traumatic stress disorder,depression associated with cancer, obesity,addiction (Kanter and Mulick 2007) and negativesymptoms of psychosis (Mairs ef al 2011). BA hasbeen used successfully with chents of differentages, religious and ethnic backgrounds, and acrossa variety of settings (Kanter ef al 2012). In short,there is sufficient evidence to conclude that BA is aneffective, evidence-based therapy.
VariationsSeveral variants of BA have been developedand refined over the years, including that ofMartell ef al (2001, 2010) and Lejuez ef al (2011).For the treatment of depression, NICE (2009)recommends BA for 16 to 20 sessions over a three tofour-month period with subsequent foUow up, usingMarteU ef aFs (2001, 2010) model. This approachencompasses the following concepts:
MENTAL HEALTH PRACTICE October 2013 | Volume 17 | Number 2

Art & science depression
• Responses to events influence feelings - tochange how people feel you must help themto change what they do. Acting in the oppositeway to what the person feels an urge to do - forexample, doing something when they feel likedoing nothing - can help change an emotion.
• The focus of BA is on the envirormient('context') in which depression occurs andanalysis of the relationships between the context,events and mood.
• People may use various strategies to help themcope in the short term, for example, avoidance,rumination, escape. This is understandable but nothelpful since these strategies make it less likely theperson will do things differently - they are likely tocontinue feeling bad, for example, be 'stuck'.
• Basic routines are disrupted in depression butactivation can increase behaviours. Not aU clientsare inactive, but there may be subtle formsof avoidance.
• Examiaation of the function and consequence ofbehaviours is required. Which behaviours help theperson to feel better? Which are associated withbeing depressed? What happens before and aftersuch behaviours occur?
1' II Behaviours are increased when naturcdly positivelyreinforced by the environment, and activity isenhanced by making use of client values.
• Thoughts are addressed as changeable verbalbehaviours. There is focus on the context ofthinking rather than the content of thoughts.
• The therapist acts as a coach who aids clients tosolve problems and take practical steps throughgraded task assignments, shaping successivesteps toward a goal and blocking 'all or nothing'actions and attitudes.
• Chents are encouraged to act towards a goal andfollow a plan regardless of feelings, thus changingpatterns of behaviour previously governed bymood. The more activity, the more possibility ofcontact with positive reward that will reinforcebehaviour. This may make the client feel better.
Case study'Shelley' (not her real name) is a 52-year-oldwoman, living with her husband of 15 years andher 12-year-old daughter. Shelley self-referred tothe Improving Access to Psychological Therapies(IAPT) service because of further deterioration inmood following a suicide attempt by her husbandthe previous year. Shelley described continuingrelationship difficulties. She perceived her motheras 'critical and manipulative... a physically violentdrinker' and her father as overly passive. Shelley'sdaughter, who experienced panic attacks and
school refusal, was the husband's confidanteand Shelley felt pushed aside by this dynamic.Shelley described becoming disillusioned with hermarriage after the first year and finally, after manyyears of unhappiness and deliberation, requestedseparation. Her husband responded by attemptingsuicide, and Shelley reluctantly agreed to stay.
Shelley's difficulties with low mood started11 years ago when returning to her job aftermaternity leave. She found it challenging to jugglework demands with parental responsibilities. Shehas had numerous long periods of sick leave dueto low mood. This led to ongoing conflict withthe company's human resources department andmanagement. When her employer made a mistakewith her pay, she struggled to make repayments. Sheresigned after the suicide attempt because she couldnot cope with work any more, nor with the difficultiesthat arose from being on sick leave.
Shelley tried many antidepressants over this 11-yearperiod. She had private psychoanalysis for four yearsand only stopped when she could no longer afford it.She did not find it useful, but kept going as she hopedthe psychoanalyst could 'fix' her. She subsequently hadhumanistic counselling for two years, but consideredthat the counsellor was 'not doing enough to help'.She gave up computerised CBT after three sessionsbecause she did not feel motivated enough tocontinue. She also dropped out of a course of face-to-face CBT with the IAPT service because, perhapsnot unexpectedly, efforts at cognitive restructuringparadoxically triggered depressive rumination. Asshe tried to monitor, evaluate and challenge negativeautomatic thoughts, her thinking spiralled downwardand generalised to other areas, reinforcing her beliefthat she was unable to improve her mood.
TreatmentStepped care refers to different levels of servicewithin mental health care. Step 1 generally refersto mental health care provided by GPs. Steps 2 and3 are delivered by ÏAPT staff. Step 2 is sometimesreferred to as 'low-intensity' interventions deliveredby psychological weUbeing practitioners (PWPs), andstep 3 as 'high-intensity' interventions delivered bypsychological therapists. These three steps are all inprimary care. If the client's level of need is deemedgreater than can safely and effectively be met inprimary care, they are likely to be referred on tomore specialist mental health services (step 4) insecondary care.Stepped care has two main principles:• Treatment should always have the best chance of
delivering positive outcomes while burdening thepatient as little as possible.
3 October 2013 Volume 17 Number 2 MENTAL HEALTH PRACTICE

A system of scheduled review to detect andact on non-improvement must be in place toenable stepping up to more intensive treatments,stepping down where a less intensive treatmentbecomes appropriate and stepping out when analternative or no treatment becomes appropriate.
There are several reasons why the author, whowas Shelley's therapist, suggested Martell ef afs(2001, 2010) high-intensity BA at Step 3 for Shelley.Shelley had previously undertaken CBT at this level ofservice, with little success. She had a long history ofdepression that indicated that she might need moretime and support than the step 2 low-intensity workthat colleagues could offer. Additionally, Martell ef aTsmodel was taught at step 3 on the IAPT course, whichthe author attended at Southampton University. Thiswas in accordance with Roth and Pilling's (2007) mapof competencies for therapists.
Therapy was complemented by Lejuez er aFs(20i i) treatment manual because of its clear andconcise forms. Although behaviour change isthe primary target of intervention, BA does notfocus on 'just doing it' and is not a 'one-size-fits-air therapy. The assumption behind BA's directbehaviour change approach is not that behaviouralissues are the only factors relevant to depression,but that depression is a multisystem disorder, andbehavioural change, in the context of a positivetherapeutic relationship, is a direct and pragmaticmethod for affecting the system (Kanter ef al 2012).Depression is understood as a series of actions andevents rather than the result of some internal causeor mechanism, and Shelley found this explanationless stigmatising than biological narratives aboutdepression. It was explained that difficulties in herlife and her avoidant behavioural responses couldreduce her ability to experience positive reward, soincreasing activation might achieve greater contactwith sources of reward and help solve problems.
Measures and assessment Global and clarifyingmeasures were used in Shelley's assessment. The aimwas to find out more about the difficulties she wasexperiencing.
On various rating scales (Table 1) Shelley scoredherself as follows:
Patient Health Questionnaire (PHQ-9) fordepression (Spitzer ef al 1999): 20, whichindicated severe depression.
• Generalised Anxiety Disorder (GAD-7)scale (Spitzer ef al 2006): 12, suggestingmoderate anxiety.
i3 Clinical Outcomes to Routine Evaluation (CORE-34) scale (Barkhan ef al 2005), where 0 indicatesfewest symptoms and 4 indicates most
;'s assessment rating
Measure
PHQ-9
GAD-7
CORE-34
(means)
CORE-10
WSAS
Referral
18
10
Risk=0.8Wellbeing=3.2Functioning=2.1Problems andsymptoms=2.3(Overall=2.2)
-
24
Assessment
20
12
21
22
Session 7 (present)
13
8
16
9
PHQ-9: nil = 0-9; mild = 10-14; moderate = 15-19; severe = 2 0 + .
GAD-7: nil = 0-4; mild = 5-9; moderate = 10-14; severe = 15-F.
CORE-34/10: 0 = not at all, 4 = all the time.
CORE-10 (shorter version of CORE-34): mild = 10-15; moderate = 16-20;
moderate/severe = 20-25; severe = 264-.
WSAS: five sections measuring 0 (no impairment at all) to 8 (very severely impaired).
symptoms: a mean score of 3.2 for wellbeing,2.3 for problems and symptoms, 2.1 forfunctioning and 0.8 for risk.
m Work and Social Adjustment Scale (WSAS)(Mundt ef al 2002): 22 out of 40, which indicateddefinite impairment in carrying out activities.
We revisited these brief self-rating measures atthe start of every therapy session. This providedinvaluable information about how the previous weekhad been. Discussion of the measures, as part oftherapy, helped highlight SheUey's experience ofguilt, sadness and helplessness (Table 2). Results onthe CORE-34, and subsequently on its shorter versionCORE-10, indicated low risk.
Although Shelley expressed thoughts of cuttingher face to show everyone the extent of heremotional anguish, the thought of physical painstopped her doing this. Sometimes she thought, 'Iwould be better off dead'. On further investigation,this was a desire that life could be different, anda sense of 'wanting to hide'. Strong protective
Shelley's self-rating of key symptoms
Self-rated
symptoms
Guilt
Sadness
Helplessness
Assessment
9
5
8
Session 7 (present)
6
4
5
10 = most severe, 0 = least severe, as rated on a Likert scale.
MENTAL HEALTH PRACTICE October 2013 Volume 17 Number 2
Art & science depression
factors, preventing suicide, were her daughter andher religion. We also put together a timeline thatprovided a detailed symptom history and overallview of significant life events.
Daily monitoring was used as a tool for discovery,as part of the assessment and intervention strategy.It helped assess the baseline of activity, evaluatewhether activities gave a sense of accomplishmentor enjoyment, and identify ways to increasepotential sources of positive reinforcement.Shelley's problem Ust included low mood, relationshipdifficulties, lack of social support, financial difficulties,unemployment and worries about her daughter'shealth. Shelley wanted her therapy focus to be thelow mood, as she felt this contributed to the otherproblems she was having. Consistent with a DSM-IVdiagnosis for major depressive episode, Shelley'slow mood consisted of reduced activity, rumination,tiredness, under-eating and excessive sleeping. Shehad frequent feelings of helplessness, worthlessnessand guut, isolation, tearfulness, indecisiveness,anhedonia and occasional suicidal thoughts.
Her main strategy for managing problems wasavoidance. Her problem statement read: 'When Ifeel low I do not feel Uke doing things, so I don't,and put them on my list to do. I sleep and readinstead. This helps in the short term but has long-term consequences such as never doing anythingconstructive that may help me - then I feel worse.'
Activity
Walking
Pilâtes
Swimming
Shopping with daughter
Church, holy days
Awake on daughter's return
from school
Church, Sundays
Behaviour towards a part-time job
Sit with daughter at meal times
Healthier diet
Assertive behaviour with mother
(for example, say 'no')
Actions toward leaving marriage
Rank (l=least difficult to 10=most difficult)
1
3
4
5
6
6
6.5
7
8
8
10
10
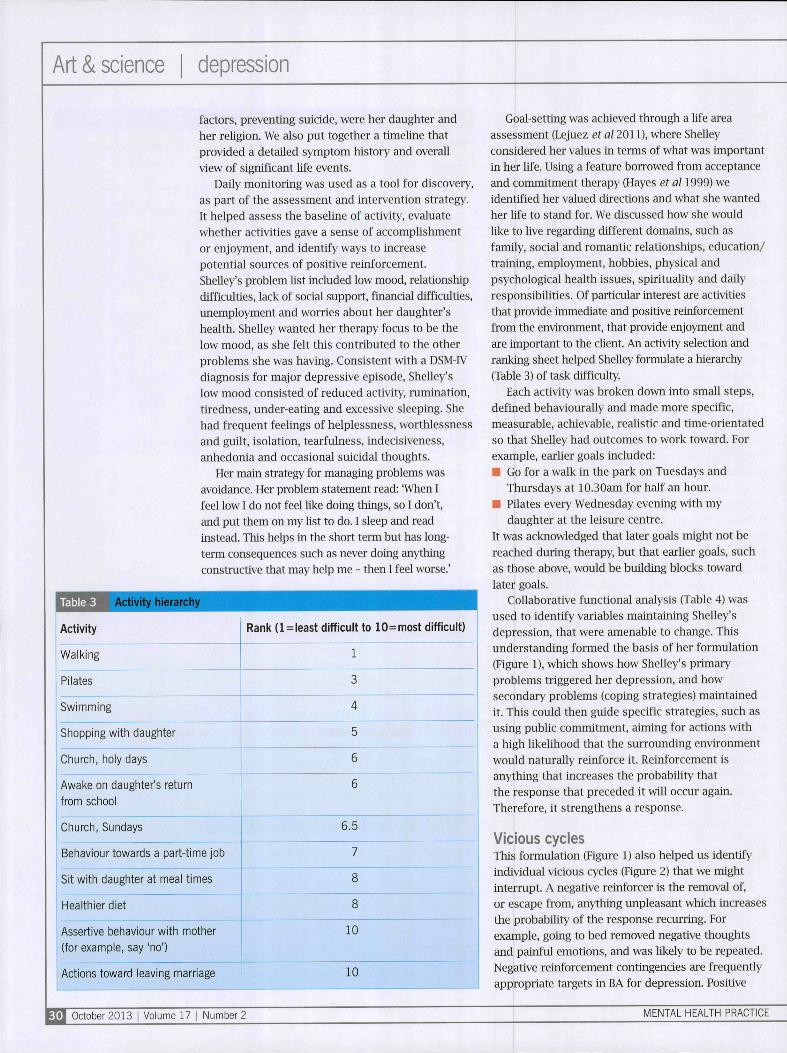
Goal-setting was achieved through a life areaassessment (Lejuez ef al 2011), where Shelleyconsidered her values in terms of what was importantin her Ufe. Using a feature borrowed from acceptanceand commitment therapy (Hayes ef al 1999) weidentified her valued directions and what she wantedher Ufe to stand for. We discussed how she wouldlike to Uve regarding different domains, such asfamily, social and romantic relationships, education/training, employment, hobbies, physical andpsychological health issues, spirituality and dailyresponsibilities. Of particular interest are activitiesthat provide immediate and positive reinforcementfrom the environment, that provide enjoyment andare important to the cUent. An activity selection andranking sheet helped SheUey formulate a hierarchy(Table 3) of task difficulty.
Each activity was broken down into small steps,defined behaviourally and made more specific,measurable, achievable, realistic and time-orientatedso that Shelley had outcomes to work toward. Forexample, earher goals included:• Go for a walk in the park on Tuesdays and
Thursdays at 10.30am for half an hour.• PUates every Wednesday evening with my
daughter at the leisure centre.It was acknowledged that later goals might not bereached during therapy, but that earUer goals, suchas those above, would be building blocks towardlater goals.
Collaborative functional analysis (Table 4) wasused to identify variables maintaining Shelley'sdepression, that were amenable to change. Thisunderstanding formed the basis of her formulation(Figure 1), which shows how Shelley's primaryproblems triggered her depression, and howsecondary problems (coping strategies) maintainedit. This could then guide specific strategies, such asusing pubhc commitment, aiming for actions witha high likelihood that the surrounding environmentwould naturally reinforce it. Reinforcement isanything that increases the probabiUty thatthe response that preceded it will occur again.Therefore, it strengthens a response.
Vicious cyclesThis formulation (Figure 1) also helped us identifyindividual vicious cycles (Figure 2) that we mightinterrupt. A negative reinforcer is the removal of,or escape from, anything impleasant which increasesthe probabihty of the response recurring. Forexample, going to bed removed negative thoughtsand painful emotions, and was Ukely to be repeated.Negative reinforcement contingencies are frequentlyappropriate targets in BA for depression. Positive
* 1 October 2013 Volume 17 I Number 2 MENTAL HEALTH PRACTICE
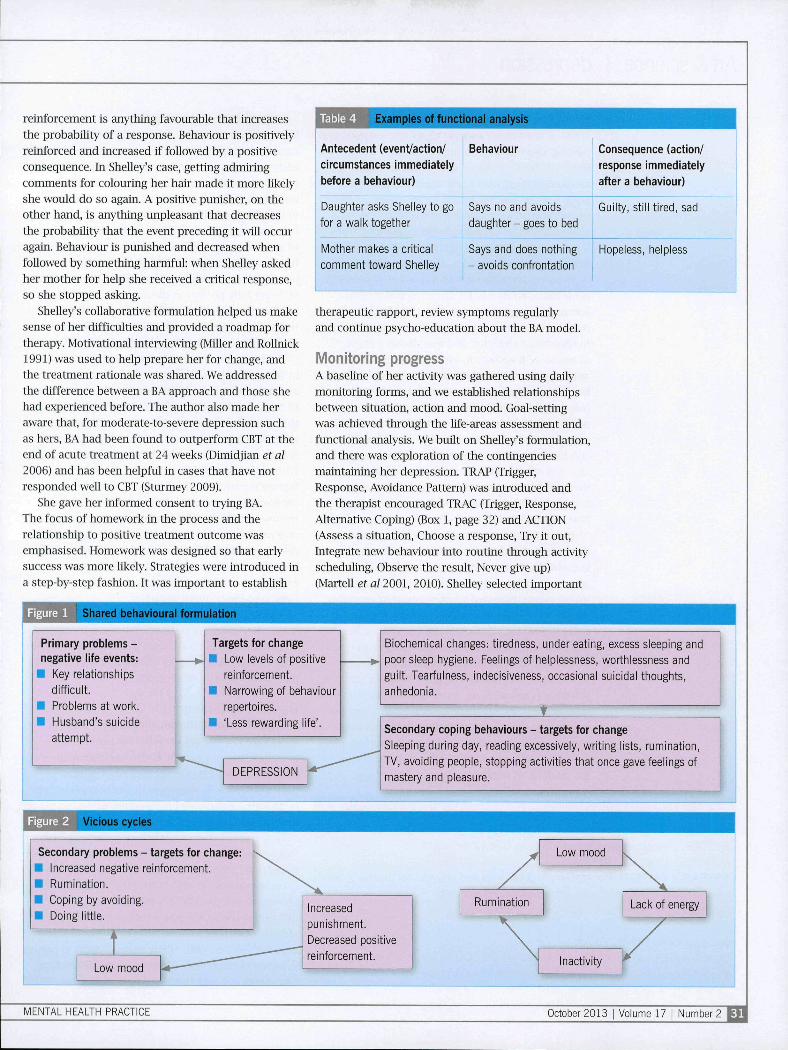
reinforcement is anything favourable that Increasesthe probability of a response. Behaviour is positivelyreinforced etnd increased if followed by a positiveconsequence. In SheUey's case, getting admiringcomments for colouring her hair made it more likelyshe would do so again. A positive punisher, on theother hand, is anything unpleasant that decreasesthe probability that the event preceding it will occuragain. Behaviour is punished and decreased whenfollowed by something harmful: when Shelley askedher mother for help she received a critical response,so she stopped asking.
Shelley's collaborative formulation helped us makesense of her difficulties and provided a roadmap fortherapy. Motivational interviewing (Miller and RoUnick1991) was used to help prepare her for change, andthe treatment rationale was shared. We addressedthe difference between a BA approach and those shehad experienced before. The author also made heraware that, for moderate-to-severe depression suchas hers, BA had been found to outperform CBT at theend of acute treatment at 24 weeks (Dümdjian et al2006) and has been helpful in cases that have notresponded well to CBT (Sturmey 2009).
She gave her informed consent to trying BA.The focus of homework in the process and therelationship to positive treatment outcome wasemphasised. Homework was designed so that earlysuccess was more likely. Strategies were introduced ina step-by-step fashion. It was important to establish
Shared behavioural formulation
Examples of functional analysis
Antecedent (event/action/ Behaviour
circumstances immediately
before a behaviour)
Daughter asks Shelley to go
for a walk together
Mother makes a critical
comment toward Shelley
Says no and avoids
daughter - goes to bed
Consequence (action/
response immediately
after a behaviour)
Guilty, still tired, sad
Says and does nothing
- avoids confrontation
Hopeless, helpless
therapeutic rapport, review symptoms regularlyand continue psycho-education about the BA model.
Monitoring progressA baseline of her activity was gathered using dauymonitoring forms, and we established relationshipsbetween situation, action and mood. Goal-settingwas achieved through the Mfe-areas assessment andfunctional analysis. We built on SheUey's formulation,and there was exploration of the contingenciesmaintaining her depression. TRAP (Trigger,Response, Avoidance Pattern) was introduced andthe therapist encouraged TRAC (Trigger, Response,Alternative Coping) (Box 1, page 32) and ACTION(Assess a situation. Choose a response. Try it out.Integrate new behaviour into routine through activityscheduling. Observe the result, Never give up)(Martell et al 2001, 2OiO). Shelley selected important
Primary problems -negative life events:
• Key relationships
difficult.
• Problems at work.
• Husband's suicide
attempt.
Targets for change
• Low levels of positive
reinforcement.
• Narrowing of behaviour
repertoires.
• 'Less rewarding life'.
Biochemical changes: tiredness, under eating, excess sleeping and
poor sleep hygiene. Feelings of helplessness, worthlessness and
guilt. Tearfulness, indecisiveness, occasional suicidal thoughts,
anhedonia.
DEPRESSION
Secondary coping behaviours - targets for change
Sleeping during day, reading excessively, writing lists, rumination,
TV, avoiding people, stopping activities that once gave feelings of
mastery and pleasure.
Figure 2 l/îcious cycles
Secondary problems - targets for change:• Increased negative reinforcement.
• Rumination.
• Coping by avoiding.
• Doing little.
Low mood
Increased
punishment.
Decreased positive
reinforcement.
MENTAL HEALTH PRACTICE October 2013

Art & science | depression
activities of various degrees of difficulty to bring asense of enjoyment, completed activity selection andranking sheets, and then built an activity hierarchy(Table 3). These activities were scheduled onto themonitoring chart with a star alongside them, tomake it clear which activities (or intermediate stepstowards them) were plarmed. If the activity wasachieved, Shelley circled it on the monitoring form.If not, she put a line through it and wrote what shehad done instead.
We considered barriers to activation, consideredbehavioural strategies for targeting ruminationand promoted problem-solving skills. Shelleycompleted an activity level graph to show numbersof completed activities, and was shown a graphof her score measures to visualise change andnotice patterns. She continuously reviewedher goals, formulations, activity hierarchy androutines, encouraging introduction of activities,building on daily monitoring sheets, TRAP, TRACand ACTION. Self-coaching (in place of therapistcoaching) was built into her life and BA expandedinto new Ufe contexts. Towards the end of therapy,we endeavour to cover relapse prevention andmanagement, including a therapy blueprint andpost-therapy goals.
When considering homework between sessions,the goal was not to complete all parts of anyhomework activity - rather, to get started, increaseactivation and disrupt avoidance. Possible and actualbarriers were discussed when planning or reviewinghomework. Shelley now routinely completes herwalking task and Püates lessons. She approachessecondary problems and experiences a domino effect- doing activities propels her to do other things.TRAP, TRAC and ACTION help her to notice that it isoften her response to an environmental cue that leadsto avoidance. She is generating new alternatives andrecognising that she has a choice whether to avoid oractivate, as demonstrated in Box 1. We chart progresson dauy monitoring forms, and socialising SheUey tothe model is a continual process.
Example of Shelley getting out of getting
The TRAP:TRIGGER: Tried on a pair of trousers in shop. Size 12 did not fit.
RESPONSE: Upset and despondent.
AVOIDANCE PATTERN: Rumination about being fat and ugly and not deserving new
trousers (despite need for them). Eat chocolate. Home to bed.
PASSIVE APPROACH: Not solved problem and feel worse.
Getting back on TRAC:
Same TRIGGER and RESPONSE but ALTERNATIVE COPING: Try a different size
and/or different shop. This is an active rather than avoidant response.
The problem of ruminationShelley has noticed that, for her, the function ofrumination is avoidance. She now considers the prosand cons of rumination versus accepting what is outof her personal control, making room for painfulfeelings, urges and sensations, and allowing themto come and go without a struggle. This is whuecommitting to action that wiU improve her quality'of Ufe. A Ust was made of ways Shelley could spendtime more productively. She has been trying tomindfuUy notice, label and step back from thoughts.By being fully present in the moment, she finds itharder to engage in repetitive self-talk. Attentiontraining has helped her attend to environmentaldetails and focus away from rumination.
Following the 'what if?' experiment documentedin Wells (2008), Shelley discovered that using worryand rumination to solve problems or cope, or tryingto reason váih worry, can be counterproductive. Thetherapist played the role of her 'what if?' worryingstyle for a specific worry, and she was required toreason with and answer each 'what if?' question.With each response, the therapist presented afurther negative 'what if?' possibiUty representingthe worst case scenario. This demonstrated thatthe use of a 'what if?' worrying style generates itsown problems and how trying to reason with worryprolongs rumination. Shelley subsequently trainedherself to limit worrying to a 30-minute 'worry time'each day and has found it helpful to use worry andrumination as a cue to get active.
Problem-solving has taught Shelley to chooseaction over passivity by looking at the relevant facts,brainstorming solutions, selecting and implementingone of these, observing its effects and continuing topractise alternative behaviours.
Barriers to treatmentThere have been obstacles to treatment. Some ofthese could be predicted on the basis of SheUey'sformulation. One obstacle is that her environmentdoes not support healthy behaviour. Attemptshave been made to overcome this by analysing herbehavioural response to her mother, using ftmcuonalanalysis and problem solving.
A second obstacle is avoidance stemming from'not feeUng Uke' doing things, which is commonin depression and indeed other disorders. SheUeyis encouraged to revisit her BA knowledge andidiosyncratic formulation, whue vaUdaüng thedifficulties of change. Interventions have beenstructured to help her engage in activities despitenegative feeUngs, particularly as motivation to engagein anything can be low. There has been discussionconcerning her perceptions of how motivation
October 2013 1 Volume 17 1 Number 2 MENTAL HEALTH PRACTICE

develops ('It's just something you have - it's eitherthere or it's not') versus trying to begm a task to seeif this increases motivation.
A 'five-minute rule' has been devised - she mustbegin a task, check in with how she feels afterfive minutes and then make an informed decisionwhether or not to carry on. Commitment to time,place and person, and explicitly linking tolong-term goals and values, increases the Ukehboodthat she will foUow through with the behaviour.A helpful question has been, 'if you were not low,what would you do?' Looking at the advEintages ofbehaviour, such as role-modeUmg behaviour to herdaughter, and the disadvantages - she would dolittle or nothing otherwise - has also helped her toactivate. Tables 1 and 2 summarise her progress.
The author is mindful of her own tendency totry to progress too quickly with clients. Attemptsto overcome this have been made by attending toShelley's understanding, feeding back progress,giving validation and being warm and genuine whueremaining non-judgemental and matter-of-fact.There have been interpersonal issues in therelationship (Safran and Segal 1990): Shelley'sthought, 'I am helpless' pulls from the therapistthe willingness to work very hard and take a moredirective, persuasive stance stemming from a desireto fix things. However, acting like this towardShelley could potentially confirm her beliefs abouthelplessness and lack of self-efficacy.
Labelling what is happening in the relationship,pausing and stepping back have helped increasetherapist objectivity. Self-coaching has been assistedby adopting a team approach to Shelley's difficulties,staying alert to her active involvement in therapy,using Socratic dialogue, direct suggestions and
problem-solving. Physically sitting alongside her hasreinforced this collaborative team approach.
Reflecting on the sessionsIt was challenging to simultaneously learn and applythe approach as a trainee psychological therapist,and a difficult model to sell, given Shelley's lowmotivation. An analogy to medication was used: thatis BA is like taking medication (doing the behaviour)whue waiting for benefits.
Enjoyment from activity may not be immediateand clients can experience a lag between doingthings differently and feeling different. However, itis hoped 'what the hands do, the head wul foUow' -and if not, at least the client is working toward theirvalues to improve their Uves.
Working with Shelley, the therapist has becomeincreasingly aware that what clients want at a givenmoment is not necessarily what they need. Whenreviewing therapy, Shelley shared a desire to analyseher thoughts more in sessions. We discussed howshe has done this in other therapies, and she noticedthat excessive talking and intellectualising has fedher avoidance of doing things differently.
Likewise, the therapist (being a reflectivist/theorist) has experienced an urge to unpick Shelley'sthoughts in therapy, so encouraging a pragmatic/activist approach and maintaining an activationfocus has been chaUengmg. However, followingMartell ef aFs (2001, 2010) model and Lejuez ef aTs(2011) manual, understanding and structure forsessions have been achieved which, combined withtherapist flexibility and clinical judgement andShelley's hard work, have provided an effective,alternative evidence-based treatment. This appearsto be working well for Shelley.
Online archiveFor related information, visit
our online arciiive and search
using tiie keywords
Conflict of interest
None declared
Aci<nowiedgementThe author would like toacknowledge the training shereceived in Martell ei a/'sbehavioural activationapproach whiie she was atrainee psychological therapiston the Improving Access toPsychological Therapies courseat Southampton University
References
Barkham M, Gilbert N, Connell J (2005)Suitability and utility of the CORE-ÜM andCORE-A for assessing severity of presentingproblems in psychological therapy servicesbased in primary and secondary' care settings.British Journal of Psychiatr)'. 186, 239-246.
Beck A, Rush A, Shaw B et a/ (1979) CognitiveTherapy of Depression. Guilford. New York NY.
Dimidjian S, Hollon S, Dobson K et al (2006).Randomi¿ed trial of behavioural activation,cognitive therapy, and antidepressantmedication in the acute treatment of adultswith major depression. Joumal of Consultingand Clinical Psychology. 74, 4, 658-670.
Hayes S, Strosahl K, Wilson K ( 1999)Acceptance and Commitment Therapy. Guilford,New York NY.
Jacobson N, Dobson K, Traux P et al (1996) Acomponent analysis of cognitive behaviouraltreatment for depression. Joumal of Consulting& Clinical Psychology. 64. 2, 295-304.
Kanter J, Mulick P (2007) Basic ScienceFoundations and New .Applications of BehaviouralActivation. Symposium presented at the annualmeeting of the Association of Behavioural andCognitive Therapies, Philadelphia PA.
Kanter J, Puspitasari A, Santos M eraI(2012)Behavioural activation: histor)', evidenceand promise. British Journal of Psychiatry.200,5,361-363.
Lejuez C, Hopko D, Ademo R eta/(2011)Ten year revision of the Brief BehavioralActivation Treatment for Depression (BATD):Revised Treatment Manual (BATD-R). BehaviorModification. 35, 2, 111-161.
Mairs H, LoveD K, CampbeU et al (2011)Development and pilot investigation ofbehavioral activation for negative symptoms.Behavior Modification. 35, 5, 486-S06.
Martell C, Addis M, Jacobson N (2001)Depression in Context; Strategies for GuidedAction. Norton. New York NY.
Martell C, Dimidjian S, Hermann-Dunn R(2010) Behavioral Activation for Depression.Guilford. New York NY.
Miller W, Rollnick S (1991) MotivationalInterviewing: Preparing People for Change.Guiidford Press, New York NY.
Mundt J. Marks I, Shear K et a¡ (2002) TheWork and Social Adjustment Scale: a simplemeasure of impairment in functioning,British Journal of Psychiatry. 180, 461-464.
National Institute for Health and CareExcellence (2009) Depression. Treatment andManagement of Depression in Adults, IncludingAdults With Chronic Physical Health Problems.NICE, London.
Roth AD, Pilling S (2007) The CompetenciesRequired to Deliver Effective Cognitiveand Behavioural Therapy to People withDepression and with Anxiety Disorder.";. London.Department of Health.
Safran J, Segal Z (1990) Interpersonal Processesin Cognitive Therapy. Basic Books, New YorkNY.
Spitzer R, Kroenke K, Williams J (1999)Validation and utility' of a self-report versionof PRIME-MD: the PHQ Primary Care Study.The Journal of the American MedicalAssociation. 282, 18, 1737-1744.
Spitzer R, Kroenke K, Williams J et a/ (2006) Abrief measure for assessing Generalized AnxietyDisorder: the GAD-7. Archives of InternationalMedicine. 166, 10, 1092-1097.
Sturmey P (2009) Behanoral activation is anevidence-based treatment for depression.Behaviour Modification. 33, 6, 818-829.
Wells A (2008) Cognitive Therapy of AnxietyDisorders. A Practice Manual and ConceptualGuide. Wiley, Chichester.
MENTAL HEALTH PRACTICE October 2013 Volume 17

Copyright of Mental Health Practice is the property of RCN Publishing Company and itscontent may not be copied or emailed to multiple sites or posted to a listserv without thecopyright holder's express written permission. However, users may print, download, or emailarticles for individual use.