behavioral correlates of self-appraised problem-solving...
TRANSCRIPT

Behavioral Correlates of Self-Appraised Problem-Solving Ability: Problem-Solving Skills
and Health-Compromising Behaviors
FRANKLIN J. GODSHALL TIMOTHY R. ELLIOTT’ United Slates Air Force Department of Physical Medicine
Aviano, Ira/]> University of Alabama-Birmingham Aviano Air Base and Rehabilitation
According to the revised social problem-solving model, problem solving skills should be associated with cognitive and behavioral attempts to solve or prevent personal problems. We reasoned that the Approach-Avoidance scale on the Problem-Solving Inventory (PSI; Heppner, 1988) measures problem-solving skills as defined in the model , and predicted that scores on this factor would be predict ive o f health-compromising behaviors among 96 undergraduate students. An aspect of the problem-orientation component would be predictive of global health perceptions. Ineffective problem-solving skills were associated with greater alcohol intake over a 2-week period, and with more sedentary leisure behavior on retrospective and prospective measures. Perceived control over emotions was predictive of health perceptions, as hypothesized. However, elements of problem solving were unrelated to tobacco use, illicit drug use, and exercise behaviors.
Contemporary models of social problem solving conceptualize problem solving into separate domains of problem orientation and problem-solving skills (D’Zurilla & Nezu, 1990). The problem orientation serves to (a) ward off negative emotions (e.g., anger, depression, anxiety) in problem-solving situations, (b) facilitate positive affects and perceptions of competency that enhance problem- solving efforts, (c) inhibit tendencies to respond impulsively and carelessly when problem solving, and (d) motivate a person toward problem-solving (D’Zurilla & Nezu, 1990; D’Zurilla & Sheedy, 1991; Nezu & D’Zurilla, 1989). The second component-problem-solving skills-involves the specific, goai- directed strategies by which individuals define problems, generate alternatives, decide on a solution, and implement and monitor problem-solving strategies. Thus, the problem orientation provides a motivational function in the model, and the problem-solving skills component entails the actual cognitive and behavioral efforts necessary to solve and cope with problems effectively.
‘Correspondence concerning this article should be addressed to Timothy R. Elliott, Department of Physical Medicine and Rehabilitation. University of Alabama at Birmingham, Spain Rehabilitation Center, 17 I7 Sixth Avenue South, Birmingham, AL 35233-7330.
929
Journal of Applied Social Psychology, 1997, 27, 1 1, pp. 929-944. Copyright 0 1997 by V. H. Winston 8 Son, Inc. All rights reserved
930 GODSHALL AND ELLIOTT
Descriptive study of self-appraised problem-solving ability has relied often on the Problem-Solving Inventory (PSI; Heppner, 1988). This instrument features empirically derived factors that lack a clear connection with contem- porary notions of social problem solving. In a recent attempt to integrate research with the PSI into current problem-solving models, Elliott and col- leagues (Elliott, Sherwin, Harkins, & Marmarosh, 1995) noted that two factors on the PSI-the personal control (PC) and problem solving confidence (PSC) factors--parallel the problem orientation component of the social problem- solving model. These factors should then be associated with emotional experi- ences and self-perceptions in a fashion congruent with the problem orientation component. In a series of a priori tests, these researchers found perceived inabilities in regulating emotional experiences when problem solving (as mea- sured by the PC factor) to be significantly predictive of state negative affect in routine and stressful situations (Elliott, Sherwin, et al., 1995) and with meas- ures of trait negative affectivity (Elliott, Herrick, MacNair, & Harkins, 1994). In these reports, problem-solving confidence was associated with state positive affect under these same conditions, and with measures of trait positive affec- tivity. I n an additional test of the presumed mood regulatory properties of the problem orientation component, Elliott and colleagues (Elliott, Shewchuk, Richeson, Pickelman, & Franklin, 1996) found that the PSC and PC contributed toward the prediction of peripartum and postpartum depression.
Elliott and colleagues (Elliott, Sherwin, et al., 1995) further propose that the third factor on the PSI-the Approach-Avoidance (AA) scale-closely resembles the problem-solving skills component of the social problem-solving model. This factor has several items that directly assess these skills (e.g., After I have solved a problem, I do not analyze what went right or what went wrong; I have a systematic method for comparing alternatives and making decisions). Thus, AA scores should be predictive of problem-solving behaviors and outcomes that have a clear behavioral pathway, and minimal relations should be observed between this factor and self-report measures of affect or adjustment. Consistent with this position, AA scores were essentially unrelated to standard measures of state positive and negative affect in the Elliott, Sherwin, et al. (1 995) studies, nor did the AA factor significantly contribute toward the prediction of trait positive and negative affect (Elliott et al., 1994) or depression associated with pregnancy and childbirth (Elliott et al., 1996). Preliminary evidence has found that AA scores are predictive of secondary complications caused by noncompliance with self-care regimens among persons with severe physical disability, as expected (Herrick, Elliott, & Crow, 1994). Nevertheless, the presumed relation of the AA factor to ongoing behaviors has yet to be tested in any a priori fashion.
Personal habits and lifestyle choices are often the most determining etio- logic factor in personal health and well-being over the life span (Matarazzo,
PROBLEM SOLVING AND HEALTH 931
1984). Health-compromising behaviors such as smoking, alcohol abuse, seden- tary leisure activities, and lack of exercise contribute to the leading preventable causes of chronic disease and eventual death (Taylor, 1991). Mechanic and Cleary (1980) observed that a person’s lifestyle reflects individual abilities to anticipate, respond to, and cope with potential health-related problems. Thus, engaging in health-promotive behaviors and avoiding health-compromising behaviors can reflect conscious and planned responses to potential health- related problems. From this perspective, self-appraised abilities in problem solving might influence the degree to which a person is willing to engage in instrumental tasks that aid in the prevention of illness, disease, or accidents, and promote physical and emotional well-being. Other data indicate that self-appraised effective problem solving is associated with more adaptive, goal-directed, and task-relevant behaviors (Elliott, Godshall, Shrout, & Witty, 1990). Persons with effective problem-solving skills, in particular, should be more adept at generating adaptive solutions to potential health-related problems, and at rec- ognizing the hazards of certain health compromising behaviors.
Use of illicit drugs and tobacco, and excessive use of alcohol are known health-compromising behaviors. Social-cognitive models of substance use stipulate that abuse is likely when an individual possesses inadequate coping skills (Marlatt, Baer, Donovan, & Kivlahan, 1988). Subsequently, avoidant coping has been associated with alcohol use among young adults (Cooper, Russell, Skinner, & Frone, 1992; Fromme & Rivet, 1994), older problem drinkers (Moos, Brennan, Fondacaro, & Moos, 1990), and college students (Evans & Dunn, 1995). Families with adolescents who abuse substances often lack skills in family problem solving and in coping with routine problems (Hops, Tildesley, Lichtenstein, & Ary, 1990). Studies utilizing the PSI have found self-appraised ineffective problem solving to be related to retrospective accounts of substance use among undergraduates (Heppner, Hibel, Neal, We- instein, & Rabinowitz, 1982; Williams & Kleinfelter, 1989) and adult children of alcoholics (Wright & Heppner, 199 1); however, contradictory findings have been found with samples of undergraduates (Slavkin, Heimberg, Winning, & McCaffrey, 1992) and persons in an alcoholism treatment program (Larson & Heppner, 1989). All but one of these studies (Williams & Kleinfelter, 1989) relied on the PSI total score as an index of perceived problem-solving ability.
Sedentary leisure activities can constitute a health-compromising activity; appropriately strenuous exercise, however, can promote personal health. Ex- cessive television viewing has been construed as a health-compromising be- havior in light of its consistent association with obesity, poor cardiovascular fitness, inactive leisure activities, and substance use among adolescents and adults (Tucker, 1986, 1990; Tucker & Bagwell, 1991; Tucker & Friedman, 1989). Heavy viewers tend to be less imaginative and less interested in intellectual
932 GODSHALL AND ELLIOTT
pursuits, and to have fewer personal goals than light viewers (Tucker, 1987). This passive and unstructured pattern of behavior is theoretically incompatible with effective problem-solving skills. In contrast, exercise can heighten a sense of competency, personal reinforcement, and elevate positive moods. Actual engagement in exercise may necessitate active problem solving to arrange schedules and select appropriate activities. These behaviors could be related to the problem-solving skills component.
Deficiencies in problem-solving skills should represent an inadequate cop- ing repertoire and a greater proclivity for avoiding active coping with problems generally, and with one’s personal health specifically. In the present study, we predicted that a greater tendency to avoid problem solving-as measured by the AA s c a l e w o u l d be associated with a greater likelihood to use substances in everyday situations. AA scores indicative of effective problem solving have been associated with preferences for structure in one’s environment (Elliott, Herrick, Elliott, & Shrout, 1995) and with rational decision making (Chartrand, Rose, Elliott, Marmarosh, & Caldwell, 1993). Ineffective AA scores have been significantly related to greater boredom, drowsiness, and fatigue (Elliott, Sherwin, et al., 1995). Individuals who have a more sedentary, inactive leisure style appear to be less structured and less goal-oriented in regard to their personal health needs, thus they do not pursue more active physical means of leisure. Therefore, a tendency to actively engage in problem solving should be asso- ciated with more active leisure and exercise pursuits.
Finally, a negative problem orientation has been associated with health complaints and symptoms (Elliott, 1992; Elliott & Marmarosh, 1994). We predicted that factors assessing elements of the problem orientation compo- nent-the PSC and PC scales-would be unrelated to health behaviors in our sample. However, inabilities to regulate one’s emotions in problem-solving situations-as measured by the PC factor--should be significantly associated with negative subjective appraisals of personal health, consistent with prior research. We tested these hypotheses as well.
Method
Participants
Participants were recruited from upper level courses at a small private college and a large urban university. Fifty students from each site agreed to participate and completed the preparatory documentation packets. Of this number, packets from 52 women and 44 men were suitable for use. The sample was predominantly single ( N = 89) and predominantly Caucasian ( N = 85). The average participant was 2 1.6 years of age (SD = 4.5, range = 18-48 years).
PROBLEM SOLVING AND HEALTH 933
Predictor Variables
The PSI-Form A (Heppner, 1988) was used to measure self-appraised problem-solving ability. The PSI contains 32 items which are rated on a 6-point Likert-type scale ranging from 1 (strongly agree) to 6 (strongly disagree). The PSI contains three factors described earlier: problem-solving confidence, ap- proach-avoidance, and personal control (Heppner, 1988). Reliability estimates revealed that these constructs are internally consistent (alpha coefficients from .72 to .90) and stable over a 2-week period (test-retest correlations from .83 to .89; Heppner, 1988). Validity estimates indicated that the PSI subscales are significantly related in predicted directions with a variety of self-report and observational measures (Heppner, 1988). Higher scores indicate negative per- ceptions of one’s problem-solving ability.
We also included gender as a second predictor variable. Undergraduate men tend to use more substances than do women (Schall, Kemeny, & Maltzman, 1992), so gender differences were anticipated on measures of alcohol, tobacco, and drug use. Gender was coded for use in correlational analyses (1 =female, 2 = male).
Criterion Variables
Perceived health status. Perceived health was measured by a Likert-type question (Speake, Cowart, & Pellet,.] 989): Generally speaking, would you describe your health as: poor ( I ) , fair ( 2 ) , good (3), e.rcellent (4).
Retrospective measures of health behaviors. Five items assessing substance use, television viewing, and exercise were embedded in an 1 8-item questionnaire administered at the initial assessment. Respondents were instructed to report the number of times within the past 7 days certain behaviors were performed. Specifi- cally, respondents were to report the number of alcoholic beverages consumed (12 oz beer, 4 oz wine, 1 oz liquor = 1 beverage) on the following scale: 0, 1 (1-3 drinks), 2 (4-6), 3 (7-10), 4 (11-19), or 5 (20 or more). Similar items using the same response categories required respondents to indicate frequency of illicit drug use and the number of hours spent watching television or programs on VCRs. An item assessing frequency of tobacco use employed the following response set: 0, 1 (1-5 times), 2 (6-15), 3 (16-40), 4 (41-80), and 5 (81 or more). A final item measured the number of times a respondent engaged in strenuous physical activity (in which sweating or hard breathing occurred for at least 20 min; i.e., brisk walk, aerobics, run, bike, dance, swim, gardening, etc.) on the following scale: 0, 1 (1-2 times), 2 ( 3 - 4 , 3 (5-7),4 (8-10), and 5 ( I 1 or more).
Daily log of health behaviors. A daily log was used to measure health behaviors during the previous 24-hr period. The daily log required participants to indicate the occurrence of selected behaviors during the previous 24-hr period, three days a week, for 2 weeks. Participants reported use of tobacco
934 GODSHALL AND ELLIOTT
(cigarettes, cigars, pipes, and chewing tobacco), alcohol (beer, wine, and distilled liquor), and other drugs (drugs used for recreational purposes and not under direction of appropriate authority); strenuous physical exercise; and sedentary leisure activity (television/VCR viewing). The item format for sub- stance use and television viewing behaviors was the same as the retrospective items. Responses were averaged to obtain separate indices of daily alcohol, tobacco, and drug uses. Similarly, log entries concerning time viewing televi- sion were averaged to obtain a single index of this activity.
To assess quantity and quality of exercise behavior, participants were asked to indicate the number of times they engaged in strenuous physical activity causing them to sweat or breathe hard for at least 20 min. They were also asked to indicate the length of time engaged in this activity and to specify the activity. Trained judges unfamiliar with the study rated logged accounts of exercise. Guidelines for sufficient physical activity came primarily from the American College of Sports Medicine (199 1 ) and Feist and Brannon (1988). Strenuous activity was defined as activity that would elevate the heart rate to between 60% and 80% of maximum heart rate and last at least 20 min. Less than 20 min of strenuous activity was considered insufficient, but for activities lasting longer than 20 min, duration and intensity were taken into account. Longer duration activity required less intensity to qualify as strenuous physical activity, or exercise. Responses indicating engagement in appropriate strenuous physical activity were coded by raters as a I , othknvise the response received a code of 2. Adequate agreement was observed between raters ( r = .87).
Procediire
A monetary lottery was offered as an incentive for complete participation, and individual classroom instructors were able to award extra credit (if made available in some equivalent manner to all class participants) to completed participants. During the first class, the nature, purpose, and procedure for the study were explained to potential student participants by a trained assistant. Prospective participants were asked to read and sign a consent form detailing the conditions of participation; confidentiality was assured in this form.
Once the consent form was signed, volunteers completed a demographic data sheet (age, marital status, race, occupation, education), the retrospective measures of health behaviors, the PSI, and the measure of perceived health status. The log of daily health-related behaviors was then completed for the first day. Participants were required to pick up and fill out separate logs at class time on Wednesday and Friday of that initial week, and on Monday, Wednesday, and Friday of the following week. Each participant was given two extra logs in case they missed class for some reason. However, the logs had to be turned in that day to assigned
PROBLEM SOLVING AND HEALTH 935
locations. The purpose for these restrictions was to protect and maximize the accu- racy of the daily logs. Similar reasoning guided the determination to use a 3-day period as opposed to 5 or 7. Using this procedure, the participants were required to complete the daily logs immediately following the 24-hr period covered.
Data Analysis
Responses to the retrospective measures of alcohol, drug, and tobacco use, television viewing, and exercise were treated as separate criterion variables. Incomplete responses reduced the number of usable data points to 93 for the activity variables and the alcohol- and drug-use variables; 92 participants completed the tobacco use item. Individuals who failed to return daily logs as instructed, or who did not complete certain measures on the logs were deleted from analyses on these variables. Thus, 78 participants had usable data on the daily logs for the exercise, drug-use, and television-viewing variables; 79 partici- pants had usable data on the alcohol- and tobacco-consumption variables.
Correlational procedures were used to test the presumed relation of problem solving to each criterion variable. In order to provide adequate tests of our hypotheses, we used hierarchical multiple regression equations in the manner employed in earlier tests of the integrated social problem-solving model (e.g., Elliott, Sherwin, et al., 1995). For each regression equation, gender was entered at the initial step to account for any variance attributable to gender differences. In the equations to predict the separate substance use and activity variables, the problem-orientation factors were then entered at the second step to control for any variance in the criterion variable unique to these predictors. AA scores were then entered at the third step of each equation. This method tested the hypothesized relation of problem-solving skills to each health behavior after controlling for gender differences and problem orientation. This procedure has the added advantage of testing our prediction that problem orientation would not be associated with health behaviors.
In the prediction of perceived health, PSC and AA scores were entered at the second step of the equation after controlling for possible gender effects. PC scores were then entered at the final step of the equation. This method tested the presumed relation of this problem-orientation component to health perceptions. One-tailed tests of significance were used in all regression equations to test the relation of the problem-solving variables to each respective criterion variable.
Results
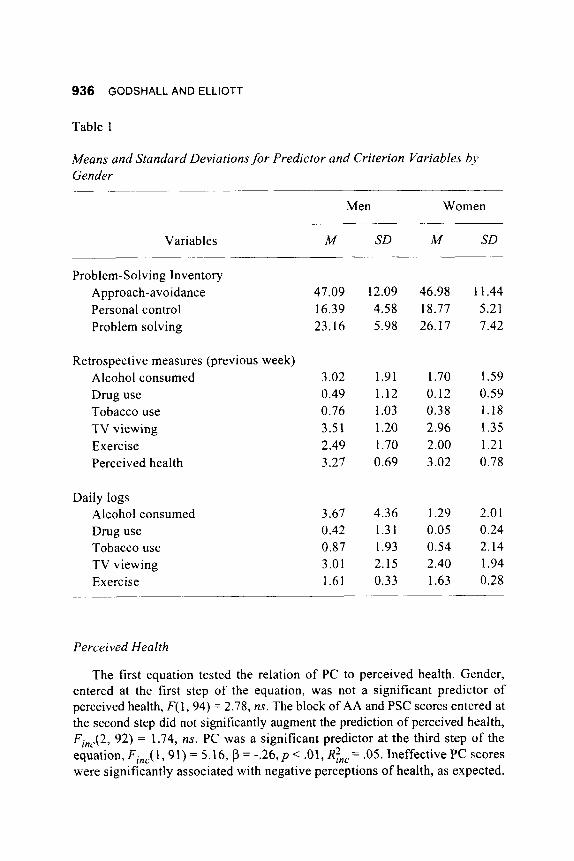
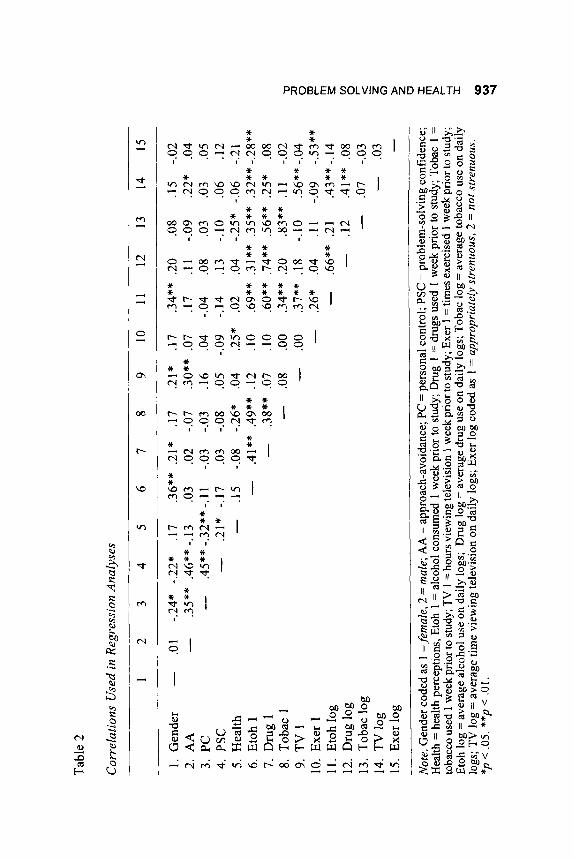
Means and standard deviations for all variables are displayed by gender in Table 1. Correlations between all variables subsequently employed in regression analyses are contained in Table 2.
936 GODSHALL AND ELLIOTT
Table 1
Means and Standard Deviations f o r Predictor and Criterion Variables bj> Gender
Variables
Problem-Solving Inventory Approac h-avoidance Personal control Problem solving
Retrospective measures (previous week) Alcohol consumed Drug use Tobacco use TV viewing Exercise Perceived health
Daily logs Alcohol consumed Drug use Tobacco use TV viewing Exercise
Men Women
M SD M SD
47.09 16.39 23.16
3.02 0.49 0.76 3.51 2.49 3.27
3.67 0.42 0.87 3.01 1.61
12.09 4.58 5.98
1.91 1.12 1.03 1.20 1.70 0.69
4.36 1.31 1.93 2.15 0.33
46.98 18.77 26.17
1.70 0.12 0.38 2.96 2.00 3.02
1.29 0.05 0.54 2.40 1.63
11.44 5.21 7.42
1.59 0.59 1.18 1.35 1.21 0.78
2.0 1 0.24 2.14 1.94 0.28
Perceived Health
The first equation tested the relation of PC to perceived health. Gender, entered at the first step of the equation, was not a significant predictor of perceived health, F( 1,94) = 2.78, ns. The block of AA and PSC scores entered at the second step did not significantly augment the prediction of perceived health, Fi,,(2, 92) = 1.74, ns. PC was a significant predictor at the third step of the equation, Fi,J 1, 9 1) = 5.16, p = -.26, p < .01, RBc = .05. Ineffective PC scores were significantly associated with negative perceptions of health, as expected.
Tab
le 2
Cor
rela
tions
Use
d in
Reg
ress
ion
Ana
lyse
s
1 2
3 4
5 6
7 8
91
01
11
21
31
41
5
1. G
ende
r -
.01
-.24*
-.2
2*
.17
.36*
* .2
1*
.17
.21*
.1
7 .3
4**
.20
.08
.15
-.02
2. A
A
-
.35*
* .4
6**
-.13
.03
.02
-.07
.30*
* .0
7 .1
7 .1
1 -.0
9 .2
2*
.04
3. PC
-
.45*
* -.3
2**
-.11
-.03
-.03
.16
.04
-.04
.08
.03
.03
.05
4. P
SC
-
.21*
-.1
7 .0
3 -.0
8 .0
5 -.0
9 -.1
4 .1
3 -.
lo
.06
.12
5. H
ealt
h -
.15
-.08
-.26*
.0
4 .2
5*
.02
.04
-.25*
-.0
6 -.2
1 6.
Eto
h 1
-
.4 1 *
* .4
9**
.12
. 10
.69*
* .3
1 **
.35*
* .3
2**
-.28*
* 7.
Dru
g1
-
.38*
* .0
7 .1
0 .6
0**
.74*
* .5
6**
.25*
.0
8 8.
Tob
ac 1
-
9. T
V 1
-
.OO
.37*
* .1
8 -.
lo
.56*
* -.0
4 .0
8 .O
O .3
4**
.20
.83*
* .1
1 -.0
2 -0
-
.26*
.0
4 .l
l -.0
9 -.5
3**
I- m
11.
Eto
h lo
g -
.66*
* .2
1 .4
3**-
.14
z P JJ
10.
Exe
r 1
.12
.41*
* .0
8 12
. D
rug
log
14.
TV lo
g -
.03
15. E
xer l
og
Not
e. G
ende
r cod
ed a
s 1 =
fem
ale,
2 =
mal
e; A
A =
appr
oach
-avo
idan
ce;
PC =
per
sona
l con
trol
; PSC
= p
robl
em-s
olvi
ng co
nfid
ence
; H
ealth
= h
ealth
per
cept
ions
, Eto
h 1
= a
lcoh
ol c
onsu
med
1 w
eek
prio
r to
stud
y; D
rug
1 =
dru
gs u
sed
1 w
eek
prio
r to
stud
y; T
obac
1 =
to
bacc
o us
ed 1
wee
k pr
ior t
o st
udy;
TV
1 =
hour
s vie
win
g te
levi
sion
1 w
eek
prio
r to
stud
y; E
xer 1
= ti
mes
exer
cise
d 1 w
eek
prio
r to
stud
y;
Etoh
log
= a
vera
ge a
lcoh
ol u
se o
n da
ily lo
gs;
Dru
g lo
g =
aver
age
drug
use
on
daily
logs
; Tob
ac lo
g =
aver
age
toba
cco
use
on d
aily
lo
gs; T
V lo
g =
ave
rage
tim
e vi
ewin
g te
levi
sion
on
daily
logs
; Exe
r log
cod
ed a
s 1
= a
ppro
pria
tely
str
enuo
us, 2
= n
ot s
tren
uous
.
v) C z 0
>
z 0
X F
-
- 13
. T
obac
log
-
.07
-.03 -
(0
0
*p <
.05.
**p
< .0
1.

938 GODSHALL AND ELLIOTT
Retrospective Measures of Substance Use
Gender was significantly predictive of alcohol use over the week prior to assessment, F(1, 91) = 13.28, p = .36,p < .001, R’ = .13. Men reported more alcohol consumed than did women. The problem-orientation variables, added at the second step of the equation, were not significantly predictive of alcohol use, Fin, (2,89) < I , ns. Finally, AA scores did not significantly augment equation at the third step, contrary to our expectations, F,,,( 1, 88) < 1, ns. Similarly, gender was a significant predictor of prior drug use, F( I , 9 1 ) = 4.08, p = .2 1, p < .05, R’ = .04. Men reported more drug use than did women. The problem- orientation variables were not significantly associated with drug use at the second step, F,,,(2, 89) < I , ns. AA scores were not significantly predictive of drug use when entered at the third step. Fill,( 1, 88) < 1, ns. Neither gender, nor problem orientation, nor AA scores significantly predicted prior tobacco use.
Retrospective Measures of Activity Patterns
Gender was significantly predictive of hours spent watching television, F( 1 , 91) = 4.24, p = .21, p < .05, R’ = .05. Men reported more television viewing than did women. The addition of the problem-orientation variables at the second step significantly augmented the equation, Fi,,(2, 89) = 2 . 4 2 , ~ < .05, R i , = .05. Inspection of beta weights revealed that ineffective PC scores were significantly associated with greater television viewing (p = .23, p < .05). AA scores, entered at the third step, were significantly predictive of television viewing, Fin,( I , 88) = 6.53, p = .29, p < .01, R!,,, = .06. Ineffective problem- solving skills were significantly associated with greater television viewing, as expected. Gender was not significantly predictive of prior exercise behavior, nor were any of the problem-solving variables associated with exercise.
Logged Accoirnts of Substance Use
Gender was a significant predictor of average daily alcohol use over the next 2 weeks, F(1, 77) = 10.06, p = .36, p < .01, R2 = .12. Consistent with retrospective data, men reported greater alcohol consumption. At the second step, the block of problem-orientation variables did not significantly contribute to the equation, F,,?,(2, 75) < 1 , ns. AA scores, entered at the third step, significantly augmented the prediction of average alcohol use, Fin,( 1, 74) =
5.41, p = .28, p < .05, R;,, = .06. Ineffective problem-solving skills were significantly associated with greater alcohol consumption, as expected. Neither gender nor any of the problem-solving variables were significantly predictive of average tobacco use over the 2-week period. Gender was significantly

PROBLEM SOLVING AND HEALTH 939
predictive of average drug use, F( I , 76) = 3.12, R2 = .04, p < .05; men reported greater drug use over the 2-week period. However, the problem-solving vari- ables did not significantly contribute to the equation.
Logged Accounts of Activity Patterns
Gender was not significantly predictive of television viewing over the next 2 weeks, F(1, 76) = 1.77, ns. At the second step, the problem-orientation variables did not significantly augment the equation, Fi,,(2, 74) < 1, 11s. However, AA scores, added at the second step of the equation, were signifi- cantly predictive of television viewing, Fj,,( l , 73) = 3.68, p = .25, p < .05, Rinc = .05. Ineffective problem-solving skills were significantly associated with more time spent viewing television over the 2-week period, as predicted. Gender was not significantly predictive of exercise behavior over the 2-week period; similarly, none of the problem-solving variables contributed to the prediction of exercise.
Discussion
These data provide some support for the presumed relation of problem solving skills to health-compromising behaviors. Problem-solving skills, as measured by the AA factor, were unrelated to retrospective accounts of sub- stance use. This trend continued with the prospective data, in that AA was unrelated to drug or tobacco use. However, AA scores were significantly predictive of time spent viewing television on both retrospective and prospec- tive measures; AA scores were also significantly predictive of alcohol con- sumption over the 2-week period. No element of problem solving was related to exercise behavior. As expected, the problem-orientation variables were not significantly associated with any substance-use variable.
The mixed results concerning problem-solving skills and substance use may be caused by several factors. Available data suggest that the relationship between problem solving and substance use may vary as a function of familial models (Slavkin et al., 1992) or substance-specific expectancies (Williams & Kleinfelter, 1989). Measurement methods might obfuscate possible relations between problem solving and alcohol use. No relation was observed between AA skills and retrospective accounts of consumption, but the hypothesized relation was found when prospective data were analyzed. Furthermore, this relation was observed after gender differences were taken into consideration. These data indicate that effects may be sensitive to assessment methods, and analyses need to take gender differences into account. Notably, the most consistent support for our hypotheses was found in relation to sedentary leisure
940 GODSHALL AND ELLIOTT
behavior. Effective AA scores were associated with less time spent viewing television on retrospective and prospective measures. We argued that persons with a greater tendency to approach rather than to avoid problems in general would be more goal oriented, would prefer more structured activities, and would thus be less likely to engage in a high degree of television viewing. These data support this logic. Ineffective AA scores may reflect a general tendency toward procrastination, passivity, and shirking responsibilities and decision making (Maydeu-Olivares & D’Zurilla, 1996).
Converging evidence now depicts several behaviors that might characterize those with ineffective problem-solving skills as measured by the AA factor. Individuals with ineffective AA scores might be prone to experience lethargy (Elliott, Sherwin, et al., 1995) and have a more unstructured approach in dealing with their environment (Elliott, Herrick, et al., 1995). These persons might also be less likely to be assertive in tense situations (Elliott, Godshall, Herrick, Witty, & Spruell, 1991); they may not readily employ rational decision-making strategies (Chartrand et al., 1993). The present study suggests that ineffective AA scores are associated with increased alcohol intake and a greater amount of time spent watching television. This might explain, in part. why previous research has associated ineffective problem-solving skills with skin breakdown and pressure sores among persons with varying levels of paralysis (Herrick et al., 1994). Ineffective AA scores are associated with a generalized passivity and a tendency to avoid active problem solving under routine and specific conditions. Thus, individuals with these characteristics may engage in more sedentary leisure pursuits at the expense of more health-promoting behaviors.
The present study also replicates and extends prior findings concerning the relation of the PC factor to negative self-perceptions. This factor-which evinces a strong association with state and trait negative affectivity (Elliott et al., 1994; Elliott, Sherwin, et al., 1995)-seems to regulate the expression of negative affect and perceptions of the self. A negative problem orientation is related to negative emotional experiences, psychological distress, and pessi- mistic interpretations and expectancies (Chang & D’Zurilla, 1996). Health perceptions are influenced considerably by pessimistic appraisal processes and negative affectivity (Anderson & Lobel, 1995). Thus, a negative problem orientation will likely be associated with negative health perceptions, regard- less of actual health status. Although the PC factor was related to retrospective accounts of television viewing, this association was unanticipated and not replicated in the prediction of logged accounts of viewing.
Our data also lend insight into unresolved discrepancies between problem solving appraisals and actual behavior. Research has consistently documented associations between perceived problem-solving ability and indices o f psycho- logical adjustment (D’Zurilla & Maydeu-Olivares, 1995; Heppner, 1988).
PROBLEM SOLVING AND HEALTH 941
Problem-solving appraisals have also been related to behaviorally based outcomes such as grade point averages (D’Zurilla & Sheedy, 1991; Elliott et al., 1990) and secondary complications due to medical noncompliance (Herrick et al.. 1994). Nevertheless, problem-solving appraisals have not been consistently associated with problem-solving performance in simulated situations (e.g., Larson, Potenza, Wennstedt, & Sailors, 1995). This discrepancy may be ex- plained in part by the lack of multiple and precise measures of different problem-solving components in experimental situations, and the possible lack of generalizability from experimental to field settings (D’Zurilla & Maydeu-Olivares, 1995). Our findings suggest that behaviorally based mea- sures such as daily logs may be useful in elucidating possible appraisal-behavior linkages that affect adjustment.
It should be noted that a constellation of health-compromising behaviors appeared within our sample. Intake of alcohol and drugs was associated with greater time spent viewing television (Table 2). These correlations corroborate other research implicating heavy television viewing with substance use (Tucker, 1987). Substance use among undergraduates is apparently associated with engagement in sedentary leisure activities. Unstructured activities and environments that offer few contingencies for substance use contribute to the development and maintenance of substance abuse (Newton, Elliott, & Meyer, 1988). Interventions and programs designed to address substance abuse on campus may benefit from an integration of self-management (Thoreson & Mahoney, 1974). problem-solving (D’Zurilla & Goldfried, 197 I ) , and social- cognitive (Marlatt et al., 1988) principles to promote more goal-oriented, structured activities incompatible with substance use.
Certain limitations of our study should be noted. Our single-item measures of retrospective substance use and activity may be rather unreliable indices of these behaviors. These single-item measures exhibited moderate to high corre- lations with corresponding items on the daily logs, suggesting that these items were sufficient for our purposes. Furthermore, inspection of variance statistics indicates that elements of problem solving accounted for relatively low amounts of variance in the criterion variables. Although several of these relations were theoretically consistent, the degree to which our findings are replicable and generalizable is unknown. It is possible that these relations were attenuated by the general nature of the items in the PSI; these items are embedded in a broad context, and they are not specific to any health concern such as substance use or exercise. Additionally, our analyses examined direct relations between problem-solving and criterion variables. Other social-cognitive (e.g., expectancies) or affective constructs might mediate the relation between elements of problem-solving and health behaviors. These possibilities should be considered in future research.

942 GODSHALL AND ELLIOTT
References
American College of Sports Medicine. (199 I ) . Guidelines,for exercise testing and prescription (4th ed.). Philadelphia, PA: Lea & Febiger.
Anderson. M., & Lobel, M. ( 1 995). Predictors of health self-appraisal: What’s involved in feeling healthy? Basic and Applied Social Psychologv, 16,
Chang, E. C., & D’Zurilla, T. J. (1996). Relations between problem orientation and optimism, pessimism, and trait affectivity: A construct validation study. Behaviozir Research and Therapy, 34, 185- 194.
Chartrand, J., Rose, M., Elliott, T., Marmarosh, C., & Caldwell, S. ( I 993). Peeling back the onion: Personality, problem solving, and decision mak- ing correlates. Joiirnal of Career Assessnient, 1, 66-82.
Cooper, M. L.. Russell, M., Skinner, J . B., & Frone, M. R. (1992). Stress and alcohol use: Moderating effects of gender, coping, and alcohol expectan- cies. Jozirnal ofAbnornta1 Psycholog?., 101, 139-152.
D’Zurilla, T. J., & Goldfried, M. R. (1971). Problem solving and behavior modification. Jozirnal of Abnornial Psycholog?,, 78, 107- 126.
D’Zurilla, T. J., & Maydeu-Olivares, A. (1995). Conceptual and methodologi- cal issues in social problem solving assessment. Behavior Therap),, 26,
D’Zurilla, T. J., & Nezu, A. (1990). Development and preliminary evaluation of the social problem solving inventory. Psychological Assessnient, 2,
D’Zurilla, T. J., & Sheedy, C. (1991). Relation between social problem-solving ability and subsequent level of psychological stress in college students. Joiirnal ofPersonality and Social Psychology. 61, 84 1-846.
Elliott, T. ( 1 992). Problem-solving appraisal, oral contraceptive use, and men- strual pain. Journal of Applied Social Ps~lchology, 22, 286-297.
Elliott, T., Godshall, F., Herrick, S., Witty, T., & Spruell, M. (1991). Problem- solving appraisal and psychological adjustment following spinal cord in- jury. Cognitive Therap), and Research, 15, 387-398.
Elliott, T., Godshall, F., Shrout, J. R., & Witty, T. (1990). Problem-solving appraisal, self-reported study habits, and performance of academically at-risk college students. Journal of Coirnseling Psychology, 37, 203-207.
Elliott, T., Herrick, S., Elliott, A,, & Shrout, J . R. (1995). Personality correlates of self-appraised problem solving abilities. Counseling Psvchologi. Quar- ferlji, 8, 163- 17 1 .
Elliott, T., Herrick, S., MacNair, R., & Harkins, S. (1994). Personality corre- lates of self-appraised problem solving ability: Problem orientation and trait affectivity. Journal o f Personality Assessment, 63, 489-505.
121- 136.
409-43 2.
156-1 63.
PROBLEM SOLVING AND HEALTH 943
Elliott, T., & Marmarosh, C. (1994). Problem solving appraisal, health com- plaints, and health-related expectancies. Journal of Counseling and Devel- opment, 72. 53 1-537.
Elliott, T., Sherwin, E., Harkins, S., & Marmarosh, C. (1995). Self-appraised problem solving ability, affective states, and psychological distress. Jour- nal of Counseling Psychology, 42, 105-1 15.
Elliott, T., Shewchuk, R., Richeson, C., Pickelman, H., & Franklin, K. (1996). Self-appraised problem solving abilities and depression during pregnancy and the post-partum period. Journal of Counseling andDevelopment, 74, 645-65 1 .
Evans, D. M., & Dunn, N. J. (1995). Alcohol expectancies, coping responses and self-efficacy judgments: A replication and extension of Cooper et al.’s 1988 study in a college sample. Journal of Studies in Alcohol, 56, 186- 193.
Feist, J., & Brannon, L. (1988). Healthpsychology: An introduction to behav- ior and health. Belmont, CA: Wadsworth.
Fromme, K., & Rivet, K. (1 994). Young adults’ coping style as a predictor of their alcohol use and response to daily events. Journal of Youth and Adolescence, 23, 85-97.
Heppner, P. P. (1988). The Problem-Solving Inventory: Manual. Palo Alto, CA: Consulting Psychologists Press.
Heppner, P. P., Hibel, J., Neal, G., Weinstein, C., & Rabinowitz, F. (1982). Personal problem solving: A descriptive study of individual differences. Journal of Counseling Psychology, 29, 580-590.
Herrick, S., Elliott, T., & Crow, F. (1994). Self-appraised problem solving skills and the prediction of secondary complications among persons with spinal cord injury. Journal of Clinical Psychology in Medical Settings, 1,
Hops, H., Tildesley, E., Lichtenstein, E., & Ary, D. (1990). Parent-adolescent problem solving interactions and drug use. American Journal of Drug & Alcohol Abuse, 16, 239-258.
Larson, L. M., & Heppner, P. P. (1989). Problem-solving appraisal in an alcoholic population. Journal of Counseling Psychology, 36, 73-78.
Larson, L. M., Potenza, M. T., Wennstedt, L. W., & Sailors, P. J. (1995). Personal problem solving in a simulated setting: Do perceptions accu- rately reflect behavior? Cognitive Therapy and Research, 19, 241 -257.
Marlatt, G . A., Baer, J. S., Donovan, D. M., & Kivlahan, D. R. (1988). Addictive behaviors: Etiology and treatment. Annual Review of Psychol-
Matarazzo, J. D. (1984). Behavioral health: A 1990 challenge for the health professions. In J. D. Matarazzo, J. A. Herd, N. E. Miller, & S. M. Weiss (Eds.), Behavioral health: A handbook of health enhancement and disease prevention (pp. 3-40). New York, NY: John Wiley & Sons.
269-283.
ogy, 39,223-252.
944 GODSHALL AND ELLIOTT
Maydeu-Olivares, A., & D’Zurilla, T. J . (1996). A factor-analytic study of the social problem solving inventory: An integration of theory and data. Cog- nitive Therapy andResearch, 20, 115-133.
Mechanic, D., & Cleary, P. D. ( 1 980). Factors associated with the maintenance of positive health behavior. Preventive Medicine, 9, 805-8 14.
Moos, R. H., Brennan, P. L., Fondacaro, M. R., & Moos, B. S. (1990). Approach and avoidance coping responses among older problem and non- problem drinkers. PsycholoBi and Aging, 5, 3 1-40.
Newton, R. M., Elliott, T., & Meyer, A. (1988). The role of structured work in alcoholism rehabilitation. Journal of Rehabilitation, 54(4), 63-67.
Nezu, A. M., & D’Zurilla, T. J . (1989). Social problem solving and negative affect. In P. Kendall & D. Watson (Eds.), Anxiety and depression: Distinc- tive and overlapping features (pp. 285-3 15). San Diego, CA: Academic.
Schall, M., Kemeny, A,, & Maltzman, I. (1992). Factors associated with alcohol use in university students. Journal of Studies on Alcohol, 53,
Slavkin, S. L., Heimberg, R. G., Winning, C. D., & McCaffrey, R. J. (1992). Personal and parental problem solving: Effects of problem solving per- formance and self-appraisal. Addictive Behaviors, 17, 19 1 - 199.
Speake, D. L., Cowart, M. E., & Pellet, K. (1989). Health perceptions and lifestyles of the elderly. Research in Nursing & Health, 12, 93-100.
Taylor, S. E. (1991). Health psychology (2nd ed.). New York, NY: McGraw- Hill.
Thoreson, C. E., & Mahoney, M. J . (1974). Behavioralself-control. New York, NY: Holt, Rinehart, & Winston.
Tucker, L. A. ( 1 986). The relationship of television viewing to physical fitness and obesity. Adolescence, 84, 797-806.
Tucker, L. A. (1987). Television, teenagers, and health. Journal of Youth and Adolescence, 16,415-425.
Tucker, L. A. (1990). Television viewing and physical fitness in adults. Re- search Quarterly in Exercise and Sport, 61, 315-320.
Tucker, L. A., & Bagwell, M. (1991). Television viewing and obesity in adult females. American Joztrnal of Public Health, 81, 908-91 1.
Tucker, L. A., & Friedman, G. (1989). Television viewing and obesity in adult males. American Journal of Public Health, 79, 5 16-5 18.
Williams, J . G., & Kleinfelter, K. J. (1989). Perceived problem solving skills and drinking patterns among college students. Psychological Reports, 65,
Wright, D. M., & Heppner, P. P. (1991). Coping among nonclinical college age
122- 136.
1235-1244.
children of alcoholics. Journal of Counseling Psychology, 38,465-472.