behavioral and emotional aspects of tourette syndrome
TRANSCRIPT
TOURETTE SYNDROME 0733-8619 /97 $0.00 + .20
BEHAVIORAL AND EMOTIONAL ASPECTS OF
TOURETTE SYNDROME
Barbara J. Coffey, MD, and Kenneth S. Park, BA
Psychopathology has long been described in association with a variety of movement disorders, either during the course of illness or predating the onset, including Huntington’s and Sydenham’s chorea and Tourette disorder (or Tou- rette syndrome [TS]).R3 The relationship between TS and behavioral and emotional problems has received increasing attention in recent years.12,14,16~18,20,21,26,27,29,30, 37,44,64,69 Current conceptualizations of this disorder include presence of both mul- tiple tics and a variety of nontic behavioral phenomena.
Georges Gilles de la Tourette published ”La Maladies des Tics Convulsif,” the first paper on behavioral and emotional aspects of Tourette syndrome in 1899.32 He noted that fears and phobias frequently were found in association with tics. The early 20th century was characterized by an emphasis on psychoanalytic hy- potheses about the nature of the disorder; prevailing views considered the symp- tomatology such as touching and utterance of obscenities as reflections of uncon- scious conflict regarding sexual or aggressive impulses. Single case reports filled the early scientific literature, such as Frau Emmy Von N. in Sigmund Freud’s Case Studies of Hysteria, who had facial tics and nervousness and likely suffered from unrecognized TS.4 In Tics and Their Treatment by Meige and Feindel(1907), a wide variety of psychiatric symptoms were described in a patient who probably had TS, including obsessions and compulsions, depression, and i m p ~ l s i v i t y . ~ ~
Beginning in the scientific data-oriented period of the 1960s, Drs. Arthur and Elaine Shapiro and colleagues noted a significant comorbidity with attention def- icit disorder with hyperactivity in a large series of patients with TS.73-75 According to Shapiro et al, motoric hyperactivity, impulsivity, distractibility, and attentional dysfunction commonly were present in these patients. They also reported on the frequent occurrence of repetitive, ritualistic behaviors in TS patients, such as touching, tapping, rubbing, and c o ~ n t i n g . ~ ~ , ~ ~ Investigators have subsequently de- scribed these phenomena as obsessive compulsive symptoms or disorder (OCS, OCD) and have noted a frequency ranging from 20% to 60% of patient^.^",^^,^^,^'
From the Tourette’s Clinic, McLean Hospital, Belmont, Massachusetts
NEUROLOGIC CLINICS OF NORTH AMERICA
VOLUME 15 *NUMBER 2 MAY 1997 277
278 COFFEY & PARK
Others have noted emotional features, including mood and non-OCD anxiety dis- orders and aggressive dyscontro1.y,6y
The natural history of Tourette disorder reveals a typical progression of in- creasing complexity of motor and vocal tics and an elaboration of obsessive com- pulsive features over time. Some authors report a reduction of tic phenomena longitudinally and a concomitant increase in the behavioral manifestation^.^^^^^^^^
Scientific data on these long-described clinical associations between tics and emotional and behavioral symptoms has accumulated in the last decade. Recently developed neurobiologic models support theoretical relationships between move- ment and emotion, primarily through contiguous pathways in the basal ganglia, thalamus, and ~ o r t e x . ~ ~ " ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ Motor, vocal, behavioral, cognitive, and emo- tional dysfunction may represent manifestations of an underlying core disinhibi- tion problern.I2 These nontic features have an important role in the evaluation and treatment of most patients with TS. This article reviews the behavioral and emo- tional aspects of TS with a focus on behavioral phenomenology and psychiatric comorbidity.
BEHAVIORAL PHENOMENOLOGY
Recent studies of the nature and phenomenology of tics in TS have challenged the notion that the tics are involuntary. Most TS patients report at least some premonitory experiences, such as bodily or mental sensations, prior to their ti^^.^^,^^,^^,^^,^^ Patients also report that they can suppress their tics at least partially for periods of time.
Bliss first described the importance of distinct and discrete sensations preced- ing tics. He described his tics as intentional with the purpose to reduce unpleasant sensations and urges preceding the tics3 Shapiro and Shapiro later described these sensations as "sensory t i c ~ . " ~ ~ , ~ ~ These subjective experiences were defined in 1993 by the Tourette Syndrome Classification Study Group as sensory tics and included focal, localized or generalized unpleasant sensations occurring in association with and relieved by movement of the affected body region.3R Recently, several studies have reported a high prevalence of sensory phenomena or "premonitory sensa- tions" preceding tics. Lang evaluated subjective experiences of 170 patients in a specialty clinic in association with a variety of hyperkinesias. Forty-one of sixty patients with tic disorders reported that all their motor and vocal tics were inten- tionally produced, and fifteen other patients reported both intentional and unin- tentional experiences, with the intentional experiences most frequent. These find- ings were in contrast to the results in nontic patients in which 102 of 110 patients reported that their movements were ~nintent ional .~~ Similarly, Cohen and Leck- man reported on the results of a survey of 131 older children and adults with TS on subjective experiences associated with their tics; almost 90% reported some premonitory sensations (either localized or generalized, physical or mental) in relation to their tics.IO Patients reported that the premonitory sensations were usu- ally unpleasant in nature and that the tics were performed to reduce these sen- sations.
Parallels with the phenomenology of compulsions in OCD can be hypothe- sized. In OCD, compulsions are performed to reduce or eliminate anxiety in as- sociation with obsessions or repetitive thoughts and images. For example, hand- washing rituals are performed to attempt to reduce contamination fears. In theory, some tics may be performed similarly to reduce unpleasant bodily sensations and mental urges.
Research on the clinical phenomenology of TS and OCD has supported this concept. Complex motor tics in Tourette's patients and compulsions in OCD have many similar clinical features; both can be empirically described as "intentional
BEHAVIORAL AND EMOTIONAL ASPECTS OF TOURETTE SYNDROME 279
repetitive behaviors” (behaviors always performed intentionally and in a stereo- typed manner). The author and colleagues recently studied intentional repetitive behaviors (IRBs) in 15 outpatient adults with OCD (without tics) and 12 adults with TS (without OCD) that demonstrated that these behaviors could be signifi- cantly differentiated by systematic subjective measures. The author and colleagues developed a systematic rating scale to measure subjective experiences that oc- curred in association with these repetitive behaviors, including cognitive (fears and images), autonomic (somatic symptoms), and sensorimotor (generalized and local bodily sensations) experiences. Cognitive experiences (p < 0.001) and auto- nomic anxiety preceded IRBs in OCD patients, whereas sensory phenomena (p < 0.001) without cognitive or autonomic symptoms preceded these IRBs in Tou- rette’s patient^.^^ A second study of 20 adults with OCD (without tics), 20 adults with TS (without OCD), and a third group of 21 with both TS and OCD has extended these findings; patients in the group with both TS and OCD had inter- mediate levels of cognitive, autonomic anxiety and sensory experience when com- pared with patients in either of the ”pure” OCD or TS groups.ss
The author and colleagues recently have repeated this study in an outpatient group of 10 juveniles ages 8 to 17 years with OCD (without tics), 8 juveniles with TS (without OCD), and a mixed group of 11 juveniles with both TS and OCD. Significant differences were demonstrated between groups, similar to the pattern observed in the adult patients. Intentional repetitive behaviors in the juveniles with ”pure OCD” were associated with cognitive (p < 0.001) and affective phe- nomena (fears/anxiety) (p < 0.01), with specific sensorimotor phenomena in the “pure TS” group ( p < 0.01), and intermediate levels of cognitive, autonomic symp- toms, and sensorimotor phenomena in the TS plus OCD group. The phenomena examined in this study (sensory, cognitive, and physiologic) may represent valid clinical indices for differentiation of complex, stereotyped repetitive behaviors in Tourette’s and OCD.
SPECIFIC BEHAVIORAL AND EMOTIONAL FEATURES
In clinic settings up to half of Tourette’s patients have behavioral and emo- tional symptoms that would meet criteria for a comorbid psychiatric diagnosis. This finding needs to be evaluated critically, because clinic samples, particularly specialized settings, differ from community or epidemiologic populations. Ascer- tainment bias is probable in clinic settings, in that patients who are more severely ill or who may have more than one disorder are more likely to be referred for treatment. In addition, the presence of one disorder may secondarily render the other disorder more difficult to manage. Third, there may be an etiologic associ- ation between TS and other disorders at a rate higher than chance.13 Furthermore, adjustment to a chronic and potentially socially disabling illness such as TS may result in emotional reactions and vulnerability in self-esteem. Finally, pharmaco- therapy for tics can result in psychiatric syndromes. Dysphoria and separation anxiety symptoms have been reported in children with TS while they are being treated with neuroleptic agent^.^,^^,^^ Comorbid disorders, such as OCD and atten- tion deficit hyperactivity disorder (ADHD) may often be more problematic for the patient than are the tics and are frequently the target for specific intervention.
ADHD
Developmentally inappropriate hyperactivity, inattention, and impulsivity have been described in most TS patients, particularly children.15~’6~21~3~~42~50~52~s9~73~74~80 Investigators have reported that 50% to 75% of TS patients also meet criteria for
280 COFFEY & PARK
ADHD.16,73,Rc1 As many as 40% to 50% of patients may present with motoric hy- peractivity and inattention prior to the onset of tics, and it is often these symptoms that first bring patients to medical attention.h6 Neuropsychological testing findings also demonstrate difficulty in tasks requiring sustained attention over time, in focusing and shifting set between important stimuli, and in executive functions
Shapiro et a1 reported that the presence of ADHD conferred a risk for higher severity of TS and was associated with additional comorbid psych~pathology.~~,’~ In a survey of patients with TS, the Comings team also reported that higher levels of severity were associated with ADHD.1S,16 Recent studies assessing psychiatric comorbidity and tic severity in cross-sectional samples of patients with tics and TS reported greater comorbidity in those patients with higher tic s e ~ e r i t y . ’ ~ , ~ ~
Scientific debate has occurred regarding the familial association of ADHD and TS; some investigators have demonstrated a genetic link16,Z2,24 and others have not.5‘1-hl These symptoms are potentially impairing to children and older patients and can have marked effects on educational and social development. In addition, it is often the hyperactivity and impulsivity that disrupt family life as well. When this is the case, treatment intervention must be directed to the ADHD symptoms as well as the tics.
(EF).7,72
OCSs, OCD, and Spectrum Disorders
A relationship between TS and OCD is apparent in most patient ~ o h o r t s . ~ ~ ~ ~ ~ ~ ~ ~ OCSs or OCD have been reported in 20% to 60% of TS patient^.^^ Patients with OCD have about a 7% lifetime risk of TS65 and 20% risk of tics.8* Family studies indicate that OCD is found at a higher rate in close relatives than in controls, which further supports this Tourette’s and OCD share many com- mon and overlapping features, including a waxing and waning course, repetitive behaviors and complex movements or rituals, preoccupation with sexual and ag- gressive content, and partially voluntary suppressibility with subsequent buildup of tension. In a modal course, the OCD symptoms begin in early adolescence and continue or increase whereas tics may decrease.81
Repetitive counting, ordering and arranging, tapping, rubbing, touching, and ”evening up” for symmetry are among the most common OCD symptoms in TS patients; classic contamination concerns and washing rituals are less common.z George and colleagues compared 10 subjects with OCD and 15 subjects with OCD plus TS and found that the comorbid group had significantly more violent, sexual, and symmetry obsessions and more touching, blinking, counting, and self-inju- rious compulsions than did the group with OCD alone. In contrast, the OCD group had more contamination obsessions and cleaning compulsions.31 Another group of investigators studied 35 OCD patients without lifetime histories of tics and 35 OCD patients with lifetime histories of tics; the OCD plus tics group had more touching, tapping, rubbing, and blinking compulsions and fewer cleaning com- pulsions when compared to the nontic OCD group.41
OCD symptoms can interfere with functioning in school, at home, and with peers through repetitive behaviors, unusual sensitivities and intolerance, and the need to achieve symmetry or ”just right” experience^.^^
Mood and Non-OCD Anxiety Disorders
In addition to OCD, other anxiety disorders and mood disorders have been described in TS patients?,l4,l8 h4,hY Patients with TS score higher than normal con-
BEHAVIORAL AND EMOTIONAL ASPECTS OF TOURETTE SYNDROME 281
trols on psychopathology ratings for disorders such as depression.6y Non-OCD anxiety disorders may be more common in TS patients than in the general pop- ulation.'8 Robertson and colleagues administered three standardized self-reports of psychopathology (Leyton Obsessional Inventory, Beck Depression Inventory, and Spielberger State-Trait Anxiety Inventory) to 22 adults with TS, 19 with major depression (MD) and 21 normal controls (mean age 33 years). Results indicated that the groups with TS and MD scored significantly higher than the comparison group on all measures. Scores on the depression and anxiety scales were lower in the TS group than in the MD group.6g The Comings group reported on the Diag- nostic Interview Schedule70 for mood disorders that 23% of the TS patients had a clinically significant score as compared to 2% of the control g r o ~ p . ~ ~ , ~ ~ Pitman et a1 studied 16 patients with TS, 16 with OCD, and 16 controls, and reported that both the TS and OCD groups had high rates of unipolar depressive and general- ized anxiety Kerbeshian et a1 reported that bipolar disorder is over- represented in a community sample of TS patients.45
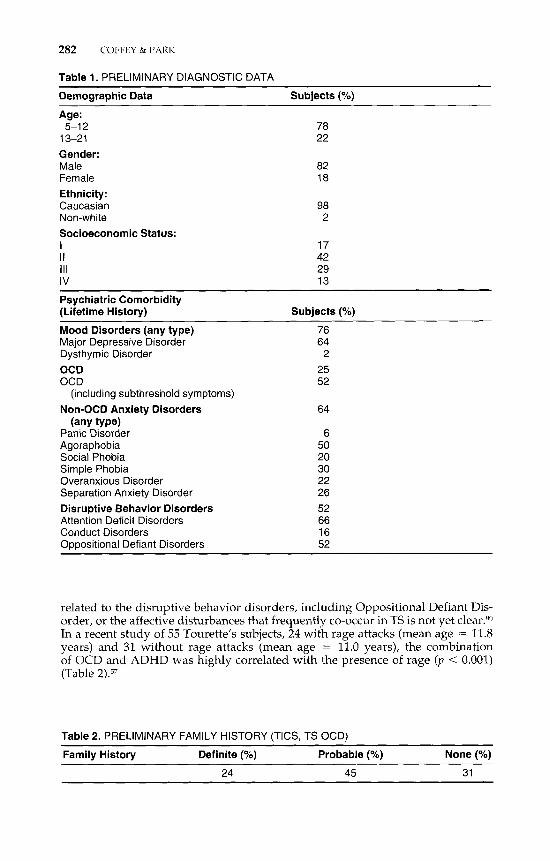
Some investigators have described an increased prevalence of panic disorder and specific phobias in TS patients when compared to normal controls. The Com- ings team reported that 26% of TS patients had more than three phobias compared to 8% of controls; 31% of the most severely afflicted TS patients had more than three panic attacks per week compared to 16% of all TS patients and none of controls.'* Additionally, a retrospective study of comorbid axis I disorders in 84 TS patients referred to a specialty clinic in a tertiary care setting. Results indicated that 16 patients (190/,) met criteria for an anxiety disorder (e.g., separation anxiety disorder, panic disorder, and simple phobia) other than OCD.9 The author and colleagues report that of the first 100 children and adolescents with TS evaluated in a specialty clinic that 76% met DSM-111-R criteria for lifetime history of mood disorder of any type, 25% met full criteria for OCD, 52% met criteria for sub- threshold OCD, and 64% met criteria for any type of non-OCD anxiety disorder (Table 1).
Scientifically it is not yet clear whether these associated conditions are etio- logically related to TS or whether they represent secondary reactions to having TS or maladaptive attempts to cope with the disorder. It is quite possible that growing up with a chronic illness would secondarily result in vulnerability to stresses associated with the illness. Additionally, the treatment itself, such as neu- roleptic medication, may result in affective d y s f u n ~ t i o n . ~ , ~ ~ , ~ ~
Psychotic Illness and Pervasive Developmental Disorders
In general the rates of comorbid psychotic illness appear to be relatively low in TS patients as compared to the aforementioned disorders. Much of the literature that exists is based on case reports. Kerbeshian and Burd described two case re- ports of children with TS who later developed childhood-onset schizophrenia. They report that for boys with TS the prevalence rate for schizophrenia is 8.7% compared to a population-based rate of 0.35 per 10,000.43
Aggressive Dyscontrol and Self Injurious Behavior
Failure of inhibition of aggression and rage attacks have been described fre- quently in TS patient^.^' Robertson et a1 reported that 33% of 90 TS patients had self-injurious behavior (SIB), includiiig four with severe eye inj~ries.~*J,~ In a more recent cohort, 44% demonstrated SIB, with head banging as the most common symptom. The etiology of this problem is not well understood. Whether this is
282 COFFEY & PARK
Table 1. PRELIMINARY DIAGNOSTIC DATA
Demographic Data Subjects (Yo)
Age: 5-1 2 78
1 3-21 22 Gender: Male 82 Female 18 Ethnicity: Caucasian 98 Non-white 2 Socioeconomic Status: I 17 II 42 111 29 IV 13
Psychiatric Comorbidity (Lifetime History) Subjects (?/.)
Mood Disorders (any type) 76 Major Depressive Disorder 64
OCD 25 OCD 52
Non-OCD Anxiety Disorders 64
Panic Disorder 6 Agoraphobia 50 Social Phobia 20 Simple Phobia 30 Overanxious Disorder 22 Separation Anxiety Disorder 26 Disruptive Behavior Disorders 52 Attention Deficit Disorders 66 Conduct Disorders 16 Oppositional Defiant Disorders 52
Dysthymic Disorder 2
(including subthreshold symptoms)
(any type)
related to the disruptive behavior disorders, including Oppositional Defiant Dis- order, or the affective disturbances that frequently co-occur in TS is not yet clear.8o In a recent study of 55 Tourette’s subjects, 24 with rage attacks (mean age = 11.8 years) and 31 without rage attacks (mean age = 11.0 years), the combination of OCD and ADHD was highly correlated with the presence of rage (p < 0.001) (Table 2).,,
Table 2. PRELIMINARY FAMILY HISTORY (TICS, TS OCD)
Family History Definite (“7) Probable (%) None (%)
24 45 31
BEHAVIORAL AND EMOTIONAL ASPECTS OF TOURETTE SYNDROME 283
DIAGNOSTIC EVALUATION OF BEHAVIORAL AND EMOTIONAL FEATURES
Evaluation should include a formal assessment of the behavioral and emo- tional problem areas known to cluster clinically with TS including ADHD, OCD, other anxiety disorders, mood disorders, and manifestations of impaired or dys- regulated affect (e.g., impulsivity and aggressivity). The use of structured inter- views, such as the Diagnostic Interview Schedule for Children (DISC) or the Chil- dren's Schedule for Affective Disorders and Schizophrenia (K-SADS) can improve classification and the assessment of comorbidity. Even if structured diagnostic interviews are not possible, systematic clinical psychiatric assessment should take place. Classification of the behavioral and emotional symptoms by formal diag- nostic criteria, such as the American Psychiatric Association's Diagnostic and Sta- tistical Manual, 4th Edition, is recommended.'
Rating instruments can provide quantifiable data, such as frequency and in- tensity of tics, at the time of initial assessment and following treatment. Standard- ized rating scales developed specifically for the TS population have improved diagnostic reliability in research studies and can also be useful in clinical care. The Yale-Global Tic Severity Scale (Y-GTSS);4,15 and the Tourette Syndrome Symptom List (TSSL) rate tics, compulsions, and other associated features. Specific rating scales for OCD (the Children's Yale Brown Obsessive Compulsive Scale [C- YBOCS]) and ADHD (Conners) can also be ~ ~ e d . ~ ~ ~ ~ , ~ ~ Quantifiable data on non- tic features can be helpful in the prioritization of symptom types and severity.
Auxiliary data from outside sources is essential. Pediatric and medical records document developmental and medical history, adequacy of previous medication trials and responses, hospitalization(s), and laboratory findings. Review of school records is advised, because many children and adolescents with TS manifest their difficulties while in school settings and are at risk for learning dy~funct ion.~~,~" Report cards can document academic performance; direct phone contact with teachers may provide data about attentional functioning and social and emotional competencies. Neuropsychologic or speech and language testing may be indicated for patients with impairments in school or occupational functioning. Identified areas of strength and weakness are subsequently conveyed to appropriate per- sonnel for inclusion into educational or vocational planning.
TREATMENT OF BEHAVIORAL AND EMOTIONAL SYMPTOMS IN TS
Comprehensive evaluation of the behavioral and emotional features in the patient with TS will yield an individual psychiatric diagnostic profile. The diag- nostic profile likely will include at least one comorbid psychiatric disorder in ad- dition to the multiple tics. For those uncomplicated patients with tics only (TS simplex), treatment can be directed toward the tics and is relatively straightfor- ward. The goal of treatment will be to reduce tic severity and frequency.
For patients with a clinical picture complicated by one or more psychiatric disorders (TS complex), treatment must take into account the nontic features and be individualized to the specific needs of the patient. The first task is to prioritize the symptoms in need of intervention, particularly the behavioral and emotional features. For many patients with TS, the tics are not the most distressing or im- pairing symptom and thus will not be the primary symptoms requiring treatment. In this situation, nontic target symptoms or symptom clusters should be identified for intervention. Baseline severity ratings of both tic and nontic features and doc- umentation of the patient's individual course with regard to tic type, distribution,

284 COFFEY & PARK
frequency, and nontic symptoms should be completed. Treatment planning should be initiated to address the target symptoms identified as most severe or distressing.
Pharmacotherapy
Pharmacotherapy is the cornerstone of treatment of TS and can be directed to any of the target symptoms, individually or in combination. Monotherapy with a broad-spectrum agent is recommended as the initial approach. Selection of one agent that is likely to address as many of the primary symptoms as possible is a reasonable starting point. For example, a child with TS complex with comorbid ADHD and OCD will likely have target symptoms of impulsivity, aggressive be- havior, hyperactivity, and compulsions. Monotherapy with clomipramine (Anaf- ranil) is a reasonable first-line approach in this situation, theoretically to address both the OCD and ADHD symptoms.
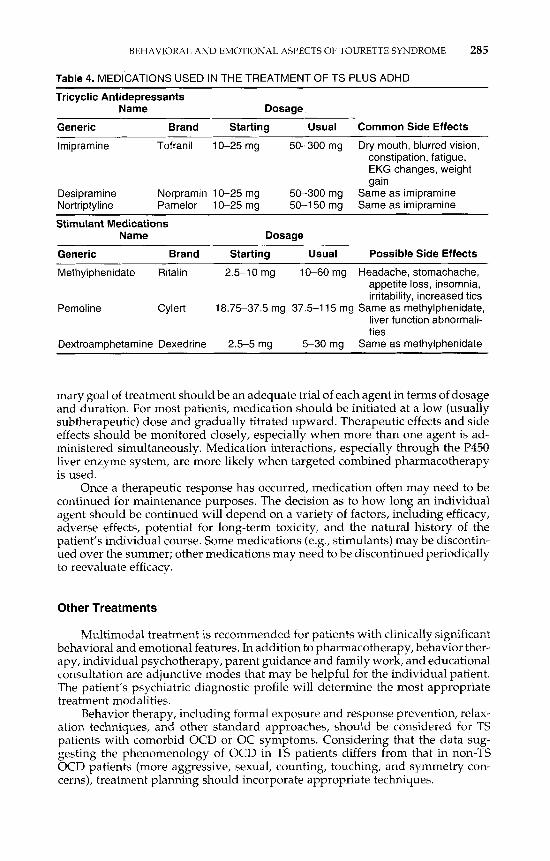
Frequently patients with TS will have several comorbid psychiatric disorders of clinical significance such as ADHD, OCD, and major depression. Intervention may be indicated for a variety of target symptoms crossing diagnostic lines. When this situation occurs, patients often require the use of more than one medication at a time to control both tics and behavioral or emotional symptoms. This ap- proach, termed targeted combined pkaumacotkevapy, involves the careful, judicious use of more than one medication simultaneously. For example, a patient may be prescribed one medication to reduce tics and a second medication to reduce some of the behavioral or emotional problems. The combined use of haloperidol (Hal- dol) and fluoxetine (Prozac) would be an example of a combination used to control both tics and OC behaviors (see Table 3). Another example is the combination of clonidine (Catapres) and dextroamphetamine (Dexedrine) to treat ADHD and TS (Table 4). This approach should be carefully monitored and periodically reeval- uated. Patients who require more than two medication types need careful ongoing evaluation because both tics and behavioral and emotional symptoms wax and wane. A patient requiring three or more major classes of medication is not nec- essarily severely ill; he or she may be noncompliant or may have developed a new-onset psychiatric disorder that is not adequately addressed by the current regimen.
Medication trials should be initiated by the introduction of one medication at a time, especially if targeted combined pharmacotherapy is necessary. The pri-
Table 3. MEDICATIONS USED IN THE TREATMENT OF TS PLUS OCD
Name Dosage
Generic Brand Starting Usual Possible Side Effects
Fluoxetine Prozac 2.5-20 mg 5-80 mg Restlessness, insomnia, gas-
Paroxetine Paxil 5-1 0 mg 10-60 mg Same as fluoxetine Clomipramine Anafranil 25 mg 50-200 mg Dry mouth, blurred vision,
trointestinal upset, sexual dysfunction
constipation, fatigue, ECG changes, weight gain
Sertraline Zoloft 12.5-25 75-300 mg Fatigue, insomnia, restless- mg ness, weight gain, sexual
dysfunction Fluvoxamine Luvox 25 mg 50-300 mg Same as fluoxetine
BEHAVIORAL AND EMOTIONAL ASPECTS OF TOURETTE SYNDROME 285
Table 4. MEDICATIONS USED IN THE TREATMENT OF TS PLUS ADHD
Tricyclic Antidepressants Name Dosage
Generic Brand Starting Usual Common Side Effects
lmipramine Tofranil 10-25 mg 50-300 mg Dry mouth, blurred vision, constipation, fatigue, EKG changes, weight gain
Desipramine Norpramin 10-25 mg 50-300 mg Same as imipramine Nortriptyline Pamelor 10-25 mg 50-1 50 mg Same as imipramine
Stimulant Medications
Generic Brand Starting Usual Possible Side Effects
Name Dosage
Methylphenidate Ritalin 2.5-10 mg 10-60 mg Headache, stomachache, appetite loss, insomnia, irritability, increased tics
Pemoline Cylert 18.75-37.5 mg 37.5-1 15 mg Same as methylphenidate, liver function abnormali- ties
Dextroamphetamine Dexedrine 2.5-5 mg 5-30 mg Same as methylphenidate
mary goal of treatment should be an adequate trial of each agent in terms of dosage and duration. For most patients, medication should be initiated at a low (usually subtherapeutic) dose and gradually titrated upward. Therapeutic effects and side effects should be monitored closely, especially when more than one agent is ad- ministered simultaneously. Medication interactions, especially through the P450 liver enzyme system, are more likely when targeted combined pharmacotherapy is used.
Once a therapeutic response has occurred, medication often may need to be continued for maintenance purposes. The decision as to how long an individual agent should be continued will depend on a variety of factors, including efficacy, adverse effects, potential for long-term toxicity, and the natural history of the patient’s individual course. Some medications (e.g., stimulants) may be discontin- ued over the summer; other medications may need to be discontinued periodically to reevaluate efficacy.
Other Treatments
Multimodal treatment is recommended for patients with clinically significant behavioral and emotional features. In addition to pharmacotherapy, behavior ther- apy, individual psychotherapy, parent guidance and family work, and educational consultation are adjunctive modes that may be helpful for the individual patient. The patient’s psychiatric diagnostic profile will determine the most appropriate treatment modalities.
Behavior therapy, including formal exposure and response prevention, relax- ation techniques, and other standard approaches, should be considered for TS patients with comorbid OCD or OC symptoms. Considering that the data sug- gesting the phenomenology of OCD in TS patients differs from that in non-TS OCD patients (more aggressive, sexual, counting, touching, and symmetry con- cerns), treatment planning should incorporate appropriate techniques.

286 COFFEY & PARK
Individual psychotherapy using verbal or play techniques may be helpful for the TS complex patient with coexisting mood or anxiety symptoms. A primary goal for the psychotherapy would be to reduce anxiety or mood symptoms; tics may be reduced secondarily because they are frequently exacerbated by stress. Another goal for psychotherapy is to provide emotional support for the patient and to promote the development of more adaptive coping capacities.
Parent support, education and family work is essential. Referral to the na- tional and local Tourette Syndrome Association network is fundamental for par- ents and families. Education of parents regarding the nature of the behavioral and emotional symptoms, and the interface with normal developmental issues is a key component of the work. Support and advice about the special developmental con- siderations of the child with TS is necessary, such as appropriate limit-setting techniques and peer issues. Often neglected is the emotional response and ad- justment of the siblings in the family. Siblings may be both genetically and emo- tionally at risk and need education and support.
Educational evaluation is indicated for most children and adolescents with TS because they are at risk for learning diffi~ulties.~~ Neuropsychological evalua- tion is the first step in assessment of cognitive strengths and weaknesses and can be utilized to develop an individual educational plan. Consultation with the teacher often will be necessary to provide education and monitor the child’s pro- gress.
CONCLUSION
TS is a complex neuropsychiatric disorder characterized by disinhibition and dysregulation of motor, cognitive, affective, and behavioral functions. Although multiple motor and vocal tics are the key diagnostic phenomena, hyperactivity, impulsivity, inattention, obsessive compulsive, and emotional symptoms are com- mon in many patients. Evaluation and treatment should take into account the behavioral and emotional symptoms as well as the tics. Treatment should incor- porate multimodal strategies so as to address both the tics and nontic symptoms.
References
1. American Psychiatric Association: Association: Diagnostic and Statistical Manual of
2. Baer L: Factor analysis of symptom subtypes of obsessive compulsive disorder and their
3. Bliss J: Sensory experiences of Gilles de la Tourette syndrome. Arch Gen Psychiatry
4. Breuer, JF: Case studies in hysteria. In Freud S (eds): Complete Psychological Works.
5. Bruun RD: Dysphoric phenomena associated with haloperidol treatment of Tourette
6. Bruun RD: Subtle and underrecognized side effects of neuroleptic treatment in children
7. Channon SF, Robertson, M . Attentional deficits in Gilles de la Tourette Syndrome. Neu-
8. Coffey B, Miguel E, Savage C, et al: Tourette’s disorder and related problems: A review
9. Coffey B, Frazier J, Chen S Comorbidity, Tourette syndrome, and anxiety disorders.
Mental Disorders. Washington, D.C., American Psychiatric Press, Inc., 1995
relation to personality and tic disorders. J Clin Psychiatry 55 (3 Suppl):lR, 1994
37:1343, 1980
Standard ed, Vo12 (1893-96). London, Hogarth Press, 1955, p 48
syndrome. Adv Neurol35:433,1982
with Tourette’s disorder. Am J Psychiatry 145:621, 1988
ropsychiatry Neuropsychol Behav Neurol5:170,1992
and update. Harvard Rev Psychiatry 2:121, 1994
[review]. Adv Neurol58:95, 1992
BEHAVIORAL AND EMOTIONAL ASPECTS OF TOURETTE SYNDROME 287
10. Cohen AJ, Leckmaii JF: Sensory phenomena associated with Gilles de la Tourette’s syn- drome. J Clin Psychiatry 53:319, 1992
11. Cohen DJ, Friedhoff AJ, Leckman JF, et al: Tourette syndrome: Extending basic research to clinical care [review]. Adv Neurol58:341, 1992
12. Cohen DJ, Leckman JF: Developmental psychopathology and neurobiology of Tourette‘s syndrome [review]. J Am Acad Child Adolesc Psychiatry 332, 1994
13. Cohen DJ, Riddle MA, Leckman JF: Pharmacotherapy of Tourette’s syndrome and as- sociated disorders [review]. Psychiatr Clin North Am 15109, 1992
14. Comings BG, Comings DE: A controlled study of Tourette syndrome. V. Depression and mania. Am J Hum Genet 41:804, 1987
15. Comings D: ADHD in Tourette syndrome. I n Comings D, (ed): Tourette Syndrome and Human Behavior. Duarte, CA, Hope Press, 1990, p 99
16. Comings DE, Comings BG: A controlled study of Tourette syndrome. I. Attention-deficit disorder, learning disorders, and school problems. Am J Hum Genet 41:701,1987
17. Comings DE, Comings BG: A controlled study of Tourette syndrome. 11. Conduct. Am J Hum Genet 41:742, 7987
18. Comings DE, Comings BG: A controlled study of Tourette syndrome. 111. Phobias and panic attacks. Am J Hum Genet 41:761, 1987
19. Comings DE, Comings BG: A controlled study of Tourette syndrome. IV. Obsessions, compulsions, and schizoid behaviors. Am J Hum Genet 41:782, 1987
20. Comings DE, Comings BG: A controlled study of Tourette syndrome. IV. Obsessions, compulsions, and schizoid behaviors. Am J Hum Genet 41:782, 1987
21. Comings DE, Comings BG: Tourette’s syndrome and attention deficit disorder with hy- peractivity [letter]. Arch Gen Psychiatry 44:1023, 1987
22. Comings DE, Comings BG: A controlled family history study of Tourette’s syndrome, I: Attention-deficit hyperactivity disorder and learning disorders. J Clin Psychiatry 51275, 1990
23. Comings DE, Comings BG: A controlled family history study of Tourette’s syndrome, 111: Affective and other disorders. J Clin Psychiatry 51:288, 1990
24. Comings DE, Comings BG, Knell E: Hypothesis: Homozygosity in Tourette syndrome. Am J Med Genet 34:413, 1989
25. Conners C: Conners’ Continuous Performance Test. Canada, Multi-Health Systems, 1992 26. de Groot CM, Bornstein RA: Obsessive characteristics in subjects with Tourette’s syn-
drome are related to symptoms of their parents. Comprehen Psychiatry 35948, 1994 27. DeGroot C, Bornstein, R, Spetier L et al: The course of tics In Tourette’s syndrome: A 5
year followup study. Ann Clin Psychiatry 6927, 1994 28. Demeter S Structural imaging in Tourette syndrome [review]. Adv Neurol58:201,1992 29. Erenberg G, Cruse RP, and Rothner AD: The natural history of Tourette syndrome: A
30. Frankel M, Cummings JL, Robertson MM, et al: Obsessions and compulsions in Gilles
31. George MS, Trimble MR, Ring HA, et a1 Obsessions in obsessive-compulsive disorder
32. Gilles de la Tourette G: La maladie des tics convulsifs. La Semaine Medicale 19:153,1899 33. Golden G S Psychologic and neuropsychologic aspects of Tourette’s syndrome. Neuro-
34. Goodman WK, Price LH, Rasmussen SA, et al: The Yale-Brown obsessive compulsive
35. Goodman WK, Price LH, Rasmussen SA, et al: The Yale-Brown Obsessive Compulsive
36. Grad LR, Pelcovits D, Olson M: Obsessive-compulsive symptomatology in children with
37. Grad LR, Pelcovitz D, Olson, M, et al: Obsessive-compulsive symptomatology in chil-
38. Group TTSCS: Definiti0r.s and classifications of tic disorders. Arch Neurol50:1013,1993 39. Hagin RA, Beecher R, Pagano G, et al: Effects of Tourette syndrome on learning. Adv
Neurol35:323, 1982 40. Harcherik DF, Carbonari CM, Shaywitz SE, et al: Attentional and perceptual distur-
bances in children with Tourette’s syndrome, attention deficit disorder, and epilepsy. Schizophren Bull 8:356,1982
follow-up study. Ann Neurol 22383, 1987
de la Tourette’s syndrome. Neurology 36:378, 1986
with and without Gilles de la Tourette’s syndrome. Am J Psychiatry 150:93, 1993
logic Clin 291, 1984
scale (YBOCS). Part I: Development, use and reliability. Arch Gen Psych 46:1006, 1989
Scale 11. Validity. Arch Gen Psychiatry 46:1012, 1989
Tourette’s Syndrome. Am Acad Child Adolesc Psychiatry 26:69, 1987
dren with Tourette’s syndrome. J Am Acad Child Adolesc Psychiatry 26:69, 1987
288 COFFEY & PARK
41. Holzer JC, Goodman WK, McDougle CJ, et al: Obsessive-compulsive disorder with and without a chronic tic disorder: A comparison of symptoms in 70 patients. Br J Psychiatry 164:469, 1994
42. Jankovic J: Deprenyl in attention deficit associated with Tourette’s syndrome. Arch Neu- rol50:286, 1993
43. Kerbeshian J, Burd L: Tourette disorder and schizophrenia in children. Neurosci Bio- behav Rev 12:267, 1988
44. Kerbeshian J, Burd L: Epidemiology and comorbidity: The North Dakota prevalence studies of Tourette syndrome and other developmental disorders. Adv Neurol 58:67, 1992
45. Kerbeshian JB, Burd L, Klug M: Comorbid Tourette’s disorder and bipolar disorder: An etiologic perspective. Am J Psychiatry 152:11:1646, 1995
46. Lang A: Patient perception of tics and other movement disorders. Neurology 41:223, 1991
47. Leckman J, Walker D, Goodman W, et al: ”Just right” perceptions associated with com- pulsive behavior in Tourette’s syndrome. Am J Psychiatry 151:675, 1995
48. Leckman JF, Walker DE, Cohen DJ: Premonitory urges in Tourette’s syndrome. Am J Psychiatry 15098, 1993
49. Linet LS: Tourette syndrome, pimozide, and school phobia: The neuroleptic separation. Am J Psychiatry 142:613, 1985
50. Linet LS: Tourette’s syndrome with symptoms of attention deficit disorder treated with desipramine [letter]. J Clin Psychiatry 48:1987
51. Lowe TL, Cohen DJ, Detlor J, et al: Stimulant medications precipitate Tourette’s syn- drome. JAMA 247:1168,1982
52. Matthews WS: Attention deficits and learning disabilities in children with Tourette’s syndrome. Pediatr Ann 17410,1988
53. Meige Feindel E: Tics and their treatment [Trans: Wilson SKI. New York, William Wood & Co, 1907
54. Miguel EC, Coffey BJ, Baer L, et a 1 Phenomenology of intentional repetitive behaviors in obsessive compulsive disorder and Tourette‘s disorder. J Clin Psych 56:246, 1995
55. Miguel EC, Baer L, Coffey BJ, et al: Phenomenological differences of repetitive behaviors in obsessive-compulsive disorder and Tourette’s Syndrome. Br J Psychiatry, in press
56. Mikkelsen EJ, Detlor J, Cohen DJ: School avoidance and social phobia triggered by halo- peridol in patients with Tourette’s disorder. Am J Psychiatry 138:1572, 1981
57. Park KS, Budman CL, Bruun RD, et al: Rage attacks in children and adolescents with Tourette’s disorder. Sci Proc Am Acad Child Adolesc Psychiatry 12:110, 1996
58. Pauls DL: The genetics of obsessive compulsive disorder and Gilles de la Tourette’s syndrome [review]. Psychiatr Clin North Am 15:759,1992
59. Pauls DL, Hurst CR, Kruger SD, et a1 Gilles de la Tourette’s syndrome and attention deficit disorder with hyperactivity: Evidence against a genetic relationship. Arch Gen Psychiatry 43:1177,1986
60. Pauls DL, Leckman J F The inheritance of Gilles de la Tourette’s syndrome and associ- ated behaviors. Evidence for autosomal dominant transmission. N Engl J Med 315:993, 1986
61. Pauls DL, Leckman JF, Cohen, DJ: Familial relationship between Gilles de la Tourette’s syndrome, attention deficit disorder, learning disabilities, speech disorders, and stutter- ing. J Am Acad Child Adolesc Psychiatry 32:1044, 1993
62. Pauls DL, Raymond CL, Stevenson JM, et al: A family study of Gilles de la Tourette syndrome. Am J Hum Genet 48:154, 1991
63. Pauls DL, Towbin KE, Leckman JF, et al: Gilles de la Tourette‘s syndrome and obsessive- compulsive disorder. Evidence supporting a genetic relationship. Arch Gen Psychiatry 43:1180, 1986
64. Pitman RK, Green RC, Jenike MA, et al: Clinical comparison of Tourette’s disorder and obsessive-compulsive disorder. Am J Psychiatry 144:1166, 1987
65. Rasmussen SA, Eisen JL: Epidemiology and clinical features of obsessive-compulsive disorder. In Jenike MB, Minichiello W (eds): Obsessive Compulsive Disorder: Theory and Management. Chicago, Year Book Medical, 1990, p 10
66. Robertson M: The Gilles de la Tourette syndrome: The current status. Br J Psychiatry 154:147, 1989
BEHAVIORAL AND EMOTIONAL ASPECTS OF TOURETTE SYNDROME 289
67. Robertson MM: The Gilles de la Tourette syndrome and obsessional disorder [review]. Int Clin Psychopharmacol3:69,1991
68. Robertson MM: Self-injurious behavior and Tourette syndrome [review]. Adv Neurol- ogy 58:105, 1992
69. Robertson MM, Channon S, Baker J, et al: The psychopathology of Gilles de la Tourette’s syndrome: A controlled study. Br J Psychiatry 162:114,1993
70. Robins LN, Helzer JE, Croughan J: The National Institute of Mental Health (NIMH) Diagnostic Interview Schedule, Version 111. Rockville, MD, National Institute of Mental Health, 1981
71. Santangelo S, Pauls D, Goldstein J, et al: Tourette’s syndrome: What are the influences of gender and comorbid obsessive compulsive disorder? J Am Acad Child Adolesc Psy- chiatry 33:795, 1994
72. Schuerholz LJ, Baumgardner TL, Singer HS, et al: Neuropsychological status of children with Tourette’s syndrome with and without attention deficit hyperactivity disorder. Neurology 46:958, 1996
73. Shapiro A, Shapiro E, Young J, et al: Psychology, Psychopathology, and Neuropsychol- ogy. In Shapiro A, Shapiro E, Young J, et a1 (eds): Gilles de la Tourette Syndrome. New York, Raven Press, 1988, p 195
74. Shapiro A: Signs, Symptoms, and Clinical Course. In Shapiro A, Shapiro E, Feinberg T, et a1 (eds): Gilles de la Tourette Syndrome. 1988, p 169
75. Shapiro AK, Shapiro E: Tourette’ syndrome: History and present status. Adv Neurol 35:17. 1982
76. Shapiro AK, Shapiro E: Evaluation of the reported association of obsessive-compulsive symptoms or disorder with Tourette’s disorder [review]. Comprehen Psychiatry 33:152, 1992
77. Singer HS, Hahn IH, Moran TH: Abnormal dopamine uptake sites in postmortem stria- tum from patients with Tourette’s syndrome. Ann Neurol30:558, 1991
78. Singer HS, Rosenberg LA: Development of behavioral and emotional problems in Tou- rette syndrome. Pediatr Neurol5:41, 1989
79. Singer HS, Walkup JT: Tourette syndrome and other tic disorders: Diagnosis, patho- physiology, and treatment [review]. Medicine 7015, 1991
80. Spencer T, Biederman J, Harding M, et al: The relationship between tic disorders and Tourette’s syndrome revisited. J Am Acad Child Adolesc Psychiatry 34:1133, 1995
81. Steingard R, Dillon-Stout D: Tourette’s syndrome and obsessive compulsive disorder: Clinical aspects [review]. Psychiatr Clin North Am 15:849, 1992
82. Swedo SE, Rapoport JL, Leonard H, et al: Obsessive compulsive disorder in children and adolescents. Arch Gen Psychiatry 46:335,1989
83. Trimble M: Psychopathology and movement disorders: a new perspective on the Gilles de la Tourette syndrome [review]. J Neurol, Neurosurg Psychiatry [Suppl] 90-95, 1989
84. Wolf SS, Jones DW, Knable MB, et al: Tourette syndrome: Prediction of phenotypic variation in monozygotic twins by caudate nucleus D2 receptor binding. Science 273:1225,1996
Address reprint requests to Barbara J. Coffey, MD
Tourette’s Clinic McLean Hospital
Higginson 112 115 Mill Street
Belmont. MA 02178