bariatric surgery remission or cure for diabetes · bariatric surgery remission or cure for...
TRANSCRIPT
Dr C. Rajeswaran FRCP(UK);MSC Consultant Physician Diabetes, Obesity and Endocrinology Chair, National Diabesity Forum
Bariatric surgery Remission or Cure for Diabetes ?
Obesity .. Condition in which body fat has accumulated to such an extent that health may be adversely affected (WHO, 2000)
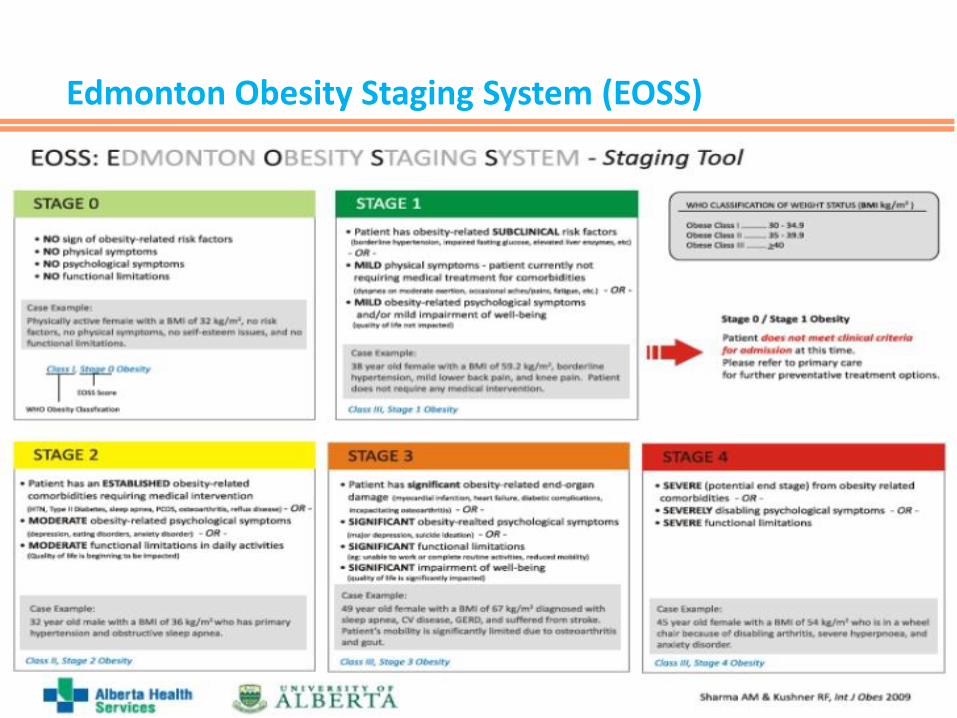
Edmonton Obesity Staging System (EOSS)
Why do people gain weight?
•Metabolic •Hormonal •Psychological •Social •Genetics •Drug induced
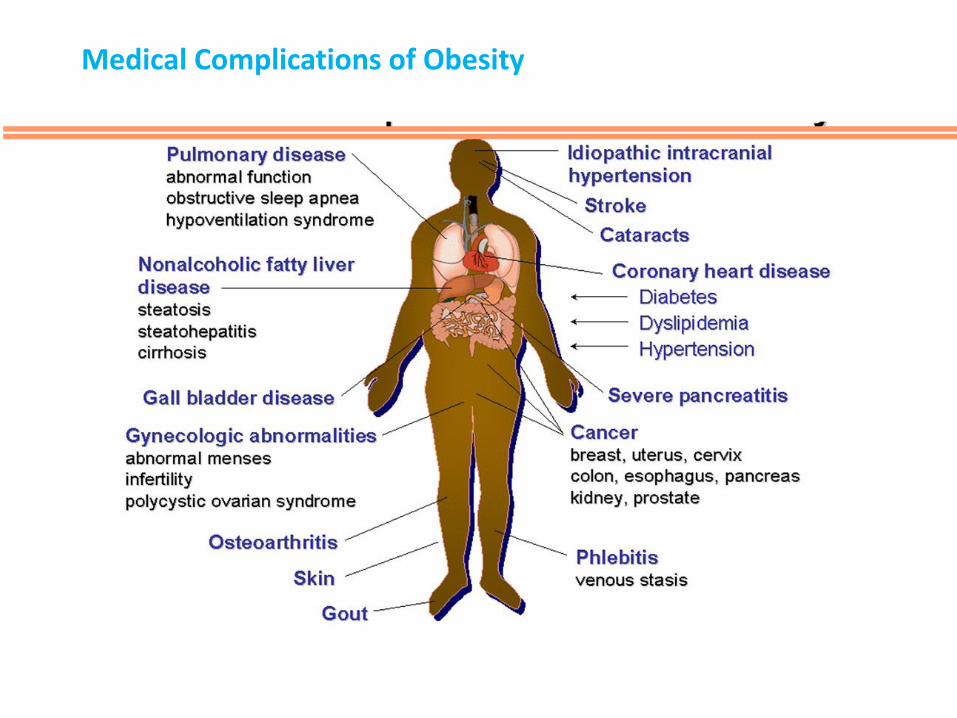
Medical Complications of Obesity
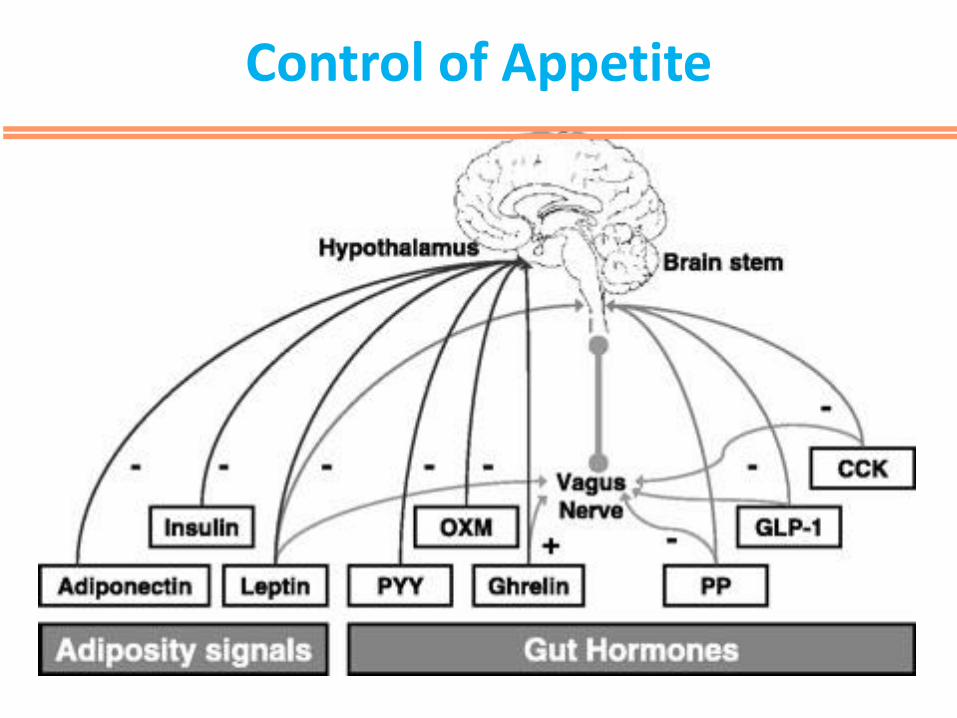
Control of Appetite
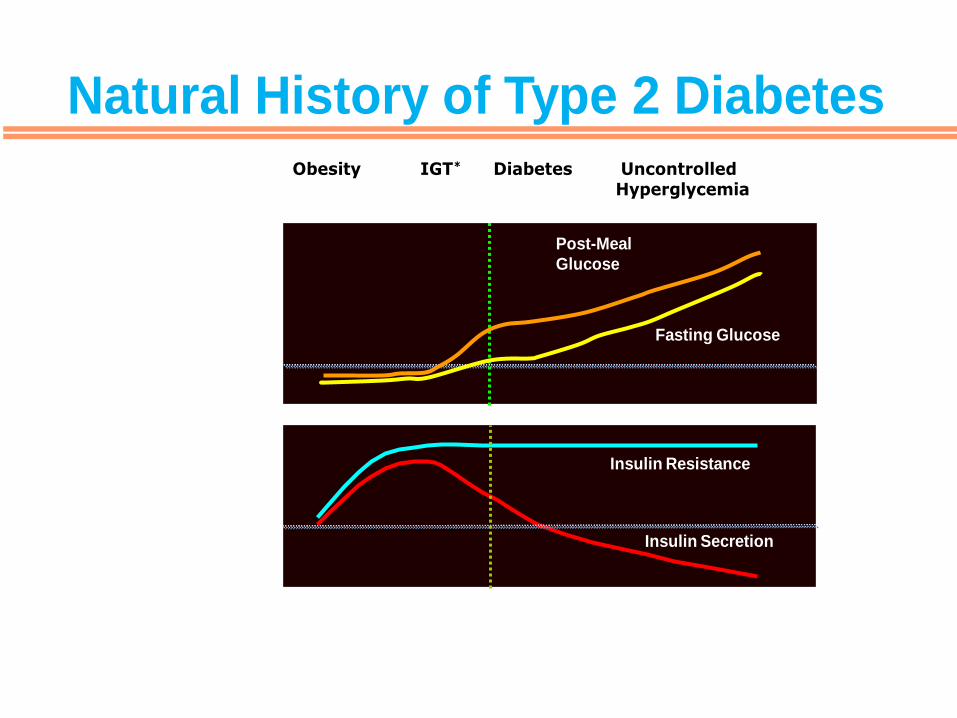
Natural History of Diabetes
Years of Diabetes
*IGT = impaired glucose tolerance.
Obesity IGT* Diabetes Uncontrolled Hyperglycemia
Relative -Cell Function
100 (%)
-20 -10 0 10 20 30
PlasmaGlucose
Insulin Resistance
Insulin Secretion
120 (mg/dL)
Adapted from International Diabetes Center (IDC), Minneapolis, Minnesota.
Fasting Glucose
Post-Meal
Glucose
Natural History of Type 2 Diabetes
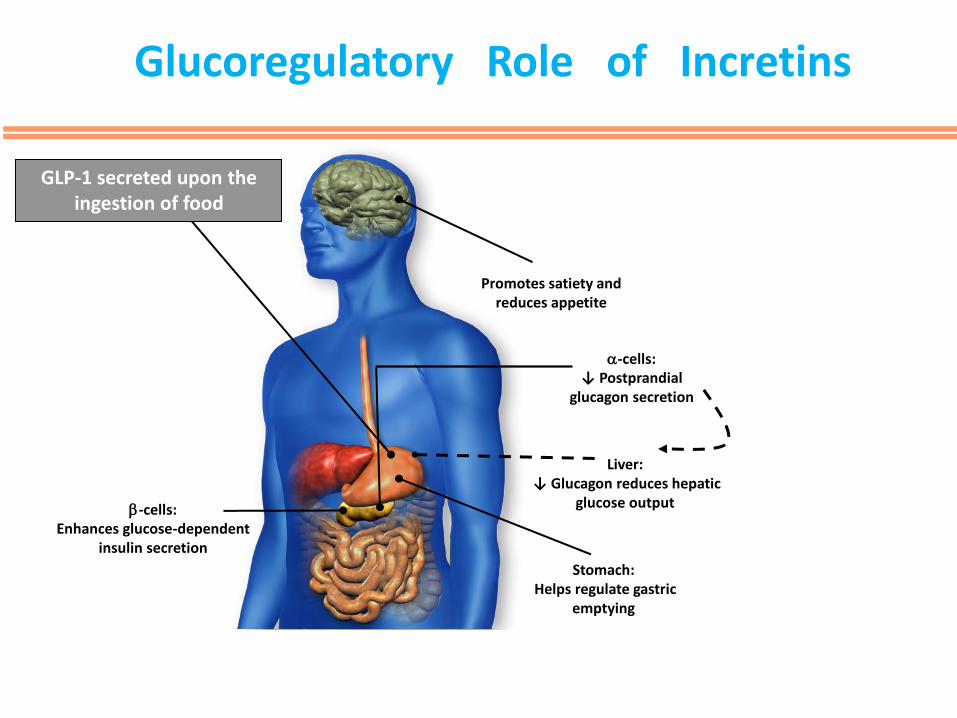
Glucoregulatory Role of Incretins
Promotes satiety and reduces appetite
-cells: Enhances glucose-dependent
insulin secretion
GLP-1: Glucagon-like peptide 1 Adapted from Flint A, et al. J Clin Invest. 1998;101:515-520; Adapted from Larsson H, et al. Acta Physiol Scand. 1997;160:413-422; Adapted from Nauck MA, et al. Diabetologia. 1996;39:1546-1553; Adapted from Drucker DJ. Diabetes. 1998;47:159-169.
Liver: ↓ Glucagon reduces hepatic
glucose output
a-cells: ↓ Postprandial
glucagon secretion
Stomach: Helps regulate gastric
emptying
GLP-1 secreted upon the ingestion of food
Types of Bariatric Surgery
• Adjustable Gastric Band
• Sleeve Gastrectomy
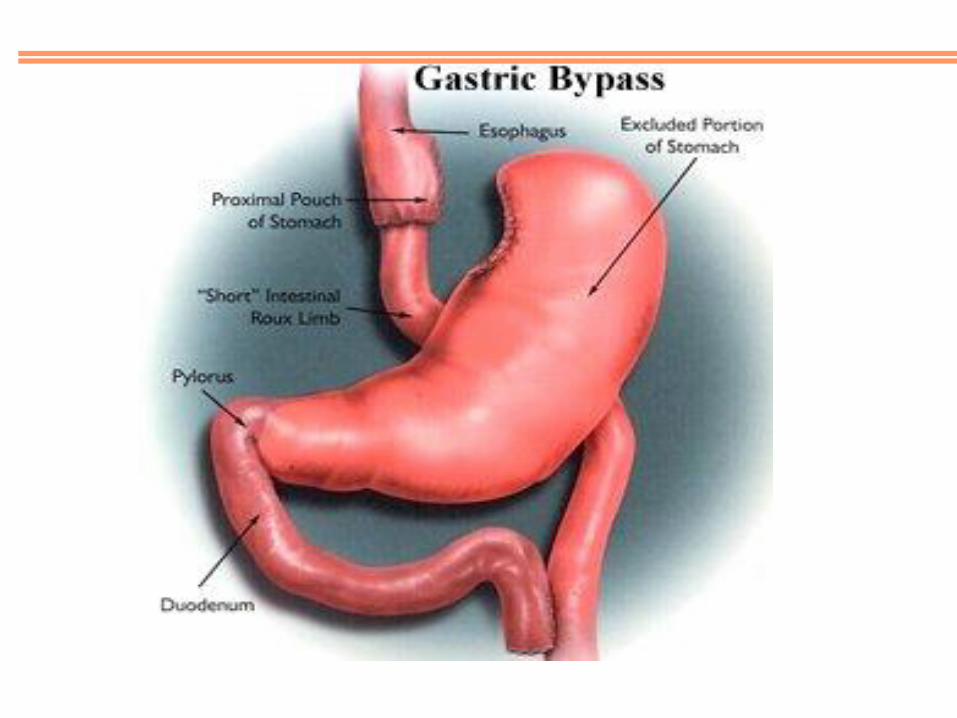
• Gastric Bypass
• Gastric balloon
• POSE
• Endobarrier
• VGBLOC
Remission of Diabetes?
Defined as:
• Fasting plasma glucose below 7 mmol/L in the absence of
medical treatment for at least 3 days.
• A 2-hour plasma glucose below 11.1 mmol/L following an OGTT.
• HbA1c below 6% after 3 months of last hypoglycemic agent usage.
Hypotheses!for!Diabetic!Control!Through!Bariatric!Surgery 42 a. Foregut!exclusion!hypothesis i. Nutrient!bypass!of!proximal!gut!prevents!secretion!of!GIP!which!promotes!insulin!resistance! ii. Proven!invalid!as!vertical!sleeve!gastrectomy!does!not!bypass!proximal!gut,!yet!still!results!in! diabetes!remission!and!weight!loss!similar!to!RYGB!and!biliopancreatic!diversion b. Hindgut!hypothesis i. Increased!delivery!of!nutrients!to!distal!ileum!causes!exaggerated!GLPM1/PYY!release!through! overstimulation!of!neuroendocrine!L!cells ii. Normalization!of!blood!glucose!within!months!following!duodenal!switch!procedure!without! restrictive!gastric!surgery!in!moderately!obese!diabetic!patients!(mean!BMI!33!kg/m2 ) 43
1. Hypotheses for Diabetic Control through Bariatric Surgery
•Foregut hypothesis •Hind gut hypothesis
2. Bariatric surgery and appetite regulating hormones PYY •Increased fasting & meal stimulated PYY levels following RYGB & sleeve gastrectomy • Increased postprandial PYY in RYGB but normal in gastric banding Gherilin Mixed results on ghrelin levels post bariatric surgery Leptin Leptin levels unchanged post RYGB and sleeve!gastrectomy
Bariatric surgery and Glycaemic control
Hypotheses!for!Diabetic!Control!Through!Bariatric!Surgery 42 a. Foregut!exclusion!hypothesis i. Nutrient!bypass!of!proximal!gut!prevents!secretion!of!GIP!which!promotes!insulin!resistance! ii. Proven!invalid!as!vertical!sleeve!gastrectomy!does!not!bypass!proximal!gut,!yet!still!results!in! diabetes!remission!and!weight!loss!similar!to!RYGB!and!biliopancreatic!diversion b. Hindgut!hypothesis i. Increased!delivery!of!nutrients!to!distal!ileum!causes!exaggerated!GLPM1/PYY!release!through! overstimulation!of!neuroendocrine!L!cells ii. Normalization!of!blood!glucose!within!months!following!duodenal!switch!procedure!without! restrictive!gastric!surgery!in!moderately!obese!diabetic!patients!(mean!BMI!33!kg/m2 ) 43
3. Bariatric surgery and Incretin hormones Increased GLPM1 by a factor of 5 one month post RYGB Postprandial GLP-1 increased following RYGB but unchanged following gastric banding Persistent post prandial increases of GLP-1 20 years after duodeno-jejunal bypass
4. Glycaemic control through weight loss Achieved within days to months after operation, before major weight loss Average remission of type 2 diabetes i. Biliopancreatic diversion / duodenal switch = 95% ii. RouxMenMY gastric bypass = 80% iii. Gastric banding = 57%
Bariatric surgery and Glycaemic control
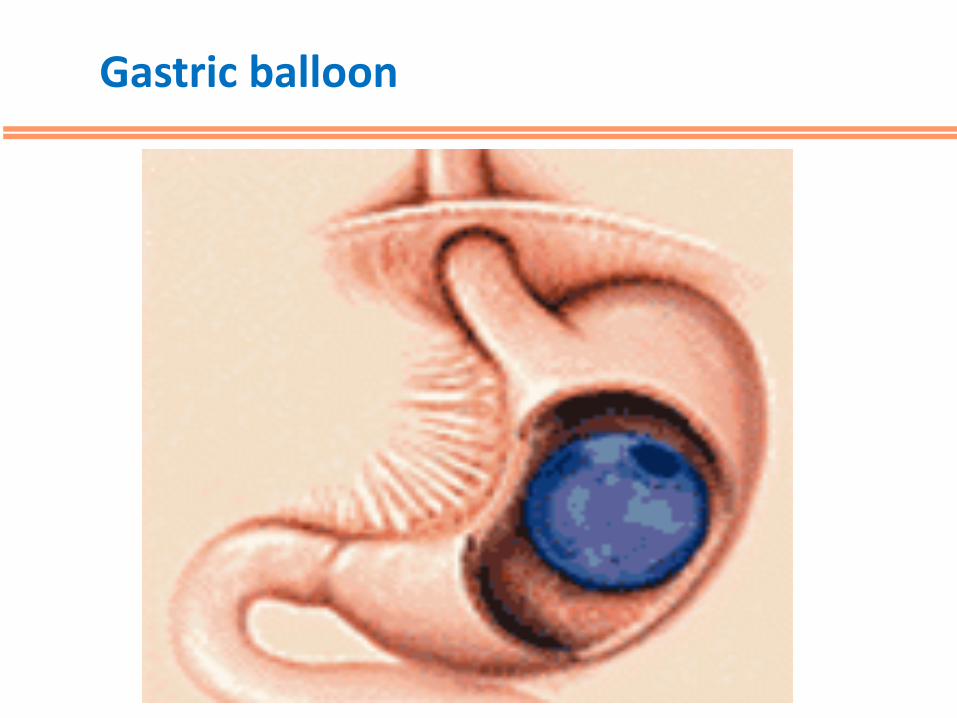
Gastric balloon
eMJA The Medical Journal of Australia
Home | Issues | Email alerts | Classifieds | Contact | More... | Topics | Search
→ Next article in this issue
→ Previous article in this issue
→ Contents list for this issue
→ More articles on Surgery
→ More articles on Gastroenterology
→ Pdf version of this article
→ Search PubMed for related articles
→ Other articles have cited this article
Abstract
•Morbid obesity (defined as having a body mass index [BMI]
> 40 kg/m2, or BMI > 35 kg/m2 with obesity-related comorbidities)
is a medical disorder associated with increased morbidity and
mortality.
•Management guidelines published by the National Health and
Medical Research Council and by similar US and UK bodies have
recommended surgery as the most effective treatment available for
selected patients with morbid obesity.
•A recent meta-analysis of obesity surgery has documented its safety
and effectiveness in resolving some of the major medical
comorbidities that occur in obese patients.
•To date, no intervention other than surgery has proven either
effective or cost-effective in treating severe obesity and its associated
medical conditions.
•Targeting patients with metabolic complications of obesity (eg, type
2 diabetes) could lead to substantial cost savings for the public health
system.
•Currently, Medicare pays for privately insured patients to undergo
obesity surgery, while uninsured patients are denied access to surgery
in public hospitals. This raises significant equity issues that should be
addressed.
Arecent review and meta-analysis by Buchwald et al1 summarises
succinctly the impact of bariatric (obesity) surgery on morbid obesity
(Box 1) and its related comorbidities. The percentage excess weight loss
in patients who have had bariatric surgery is reported to be 50%–70%,
and “cure” or significant amelioration of diabetes, hypertension,
hyperlipidaemia and obstructive sleep apnoea is experienced by over
80% of patients, on average, for each condition. The meta-analysis
confirms that bariatric surgery is a safe and effective intervention, with
positive effects persisting for years or decades. This leads us to consider
the current difficulties in providing obesity surgery for Australian
patients.
Obesity is now epidemic in the Western world, due to a complex range of
environmental and genetic factors.3 The AusDiab survey showed a
combined prevalence of overweight and obesity of about 60% in
Australian adults.4 It would be fair to assume, therefore, that overweight
and obesity are now more prevalent risk factors for disease than
smoking. Extrapolating from overseas data, the yearly number of deaths
in Australia attributable to obesity is in the order of 12 000–17 000.5,6
Over the past 20 years, the prevalence of both obesity and diabetes in
Australia has doubled,4 and the upward trend is projected to continue.
Unfortunately, poor results of non-surgical intervention mean that there
is rarely an exit for patients entering the obese cohort.
Treatment strategies for obesity have been exhaustively evaluated, both
at a primary-care level and as intensive medical therapies instituted for
high-risk patients. Primary-care interventions have either been
ineffective or of insufficient duration to assess long-term results.7-9 The
National Health and Medical Research Council (NHMRC), after an
extensive evaluation of available therapies,10 concluded that obesity is
associated with significant morbidity and mortality and that medical
treatments for obesity generally result in weight loss of less than 10 kg of
variable duration. While a sustained 3–5 kg weight loss may be
acceptable for an “overweight” or “Class I” obese patient (Box 1),
recommending non-surgical therapy to morbidly obese patients needing
more significant weight loss is unsupported by evidence. Surgery is
documented as the only consistently effective therapeutic intervention for
the morbidly obese.1,10,11
The fact that surgery is not widely advocated by clinicians managing
severely obese patients may, in part, be explained by the chequered
history of some procedures that have been introduced with enthusiasm,
rapidly disseminated, then later abandoned because of either dangerous
side effects (eg, jejuno-ileal bypass) or ineffective weight loss (eg,
gastroplasty). The number of patients happy to undergo often untested
procedures with unknown long-term consequences is testament to the
desperation faced by those afflicted with obesity.
Current bariatric surgical techniques have evolved to produce highly safe
and effective treatments for obesity and are now considered mainstream.
Perhaps no other type of surgical procedure has been as extensively
scrutinised. Multiple studies have shown that bariatric surgery leads to
long-term weight loss with low morbidity and mortality. Indeed, obesity
surgery has become one of the most frequently performed major surgical
procedures in the United States (with over 120 000 projected cases for
2004), and is the second most frequent upper gastrointestinal surgical
procedure (after cholecystectomy) performed in Australia (unpublished
Health Insurance Commission data).
Bariatric surgery has been evaluated by the NHMRC,10 the UK National
Institute for Clinical Excellence (NICE)11,12 and the US National
Institutes of Health (NIH).13 These three agencies have explicitly
recommended that surgery be made available to selected morbidly obese
patients (Box 2). On the basis of a cost-effectiveness analysis of gastric
bypass surgery, the NICE has recommended that National Health Service
trusts actively promote bariatric surgery. Similar analyses in the United
States are prompting the US government to consider more widespread
payment, through Medicare, to allow surgery in uninsured patients.
Worldwide, about 65% of bariatric surgical procedures performed each
year are variations of the gastric bypass (Box 3), with the laparoscopic
band (Box 4) being the second most common procedure. The latter
procedure is the most common performed outside the United States.14
In Australia, we have an unusual situation in which Medicare pays for
bariatric surgery and postsurgical care for privately insured patients,
while non-insured patients are denied the same services in public
hospitals. As the prevalence of obesity is significantly greater in lower
socioeconomic classes, there are obviously a significant number of obese
people excluded from treatment that has been recommended by the
NHMRC.10 A surgical approach to obesity treatment is also supported
by the Australian Safety and Efficacy Register of New Interventional
Procedures — Surgical (ASERNIP-S)15 and the Medical Services
Advisory Committee (MSAC).16 The recommendations of the
ASERNIP-S and the MSAC were to continue provision of funding for
gastric banding in particular, but bariatric surgery in general was also
supported.
The reason bariatric surgery was allowed to proceed in the UK National
Health Service was a cost analysis showing that gastric bypass was
cheaper than other interventions on a quality-adjusted-life-year (QALY)
basis.
Gastric bypass surgery is the only intervention, to date, that has been
shown to be cost-effective for treating severe obesity.17,18 It results in
lower morbidity, mortality and cost in operated compared with non-
operated patients.19,20 Although laparoscopic gastric banding did not
appear as cost-effective as gastric bypass when evaluated by the
NICE,11,12 modelling analysis suggests it could be cost-effective.21
This seems likely, given the good weight control and comorbidity
resolution observed in Australian studies of gastric banding.22 The
MSAC report16 costed gastric banding at just over $9000 and gastric
bypass at just over $8000 per procedure — figures that accord fairly well
with our own estimates (unpublished data), except that our bypass costs
were $1000–$2000 higher than banding costs because they included
hospital and intensive care unit/high-dependency unit stays. These
figures do not take into account the apparent high rate of band
removal/replacement,23-25 also reported in Health Insurance
Commission data, that would need to be included in cost calculations
(Box 5).
Patients with diabetes are of particular interest as a potential target
population for bariatric surgery. All studies to date have shown a cure
rate of at least 80% for type 2 diabetes after gastric bypass surgery.27-30
There are currently over 900 000 Australians with type 2 diabetes, with
the number projected to rise to over 1.2 million by 2010.31 The yearly
cost of managing each patient with diabetes averages $10 900 (ranging
from $9095 to $15 850, depending on the presence of complications).32
This means that a patient with diabetes having bariatric surgery in a
public hospital is likely to have the procedure pay for itself within a year.
Existing federal–state funding arrangements are not conducive to
promoting obesity surgery as a cost-saving measure. While most of the
costs of managing people with diabetes and serious obesity-related
comorbidities are borne by the federal government, state-government-
funded hospitals bear the costs of surgery. It is unlikely that state
governments, without benefiting from the overall savings, would be
swayed by cost-effectiveness arguments. The current inequities may,
therefore, continue.
Currently, Australia is far behind many Western countries in developing
strategies to reduce the future burden of obesity and treat people who are
severely afflicted. We have had no open-forum discussions between
stakeholders and government of the kind that produced the recent UK
House of Commons report on obesity.33 We have no primary-care
equivalent of the UK Counterweight Project,8 and no effective
treatments available to those who can not afford either drug therapy or
surgery. Surgery for obesity is regarded by many people, including
clinicians, to be akin to cosmetic surgery, a perception that is likely to
persist while it remains solely in the domain of the private system.
Although managing obesity is going to be a problem of major
proportions, the longer we wait, the more difficult it will be to find
solutions that suit the Australian population. The first step will be to
acknowledge the severity of the problem and to offer treatment for the
morbidly obese based on best available evidence. To do otherwise is to
either ignore the evidence or simply discriminate against the obese.
1 Obesity definitions*2
Competing interests
Drs Talbot and Jorgensen received travel assistance from Johnson and
Johnson Medical to attend an obesity surgery meeting in 2004. All three
authors are bariatric surgeons with public hospital appointments.
References
1.Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a
systematic review and meta-analysis. JAMA 2004; 292: 1724-1737.
<PubMed>
2.World Health Organization. Obesity: preventing and managing the
global epidemic. Report of a WHO consultation. World Health Organ
Tech Rep Ser 2000; 894: i–xii, 1–253. <PubMed>
3.Swinburn B, Egger G. The runaway weight gain train: too many
accelerators, not enough brakes. BMJ 2004; 329: 736-739.
<PubMed>
4.Cameron AJ, Welborn TA, Zimmet PZ, et al. Overweight and
obesity in Australia: the 1999–2000 Australian Diabetes, Obesity and
Lifestyle Study (AusDiab). Med J Aust 2003; 178: 427–432.
<eMJA full text> <PubMed>
5.Allison DB, Fontaine R, Manson JE, et al. Annual deaths
attributable to obesity in the United States. JAMA 1999; 282: 1530-
1538. <PubMed>
6.Banegas JR, Lopez-Garca E, Gutierrez-Fisac JL, et al. A simple
estimate of mortality attributable to excess weight in the European
Union. Eur J Clin Nutr 2003; 57: 201–208. <PubMed>
7.Moore H, Summerbell CD, Greenwood DC, et al. Improving
management of obesity in primary care: cluster randomised trial.
BMJ 2003; 327: 1085-1089. <PubMed>
8.The Counterweight Project Team. A new evidence-based model for
weight management in primary care: the Counterweight Programme.
J Hum Nutr Diet 2004; 17: 191-208. <PubMed>
9.James J, Thomas P, Cavan D, Kerr D. Preventing childhood obesity
by reducing consumption of carbonated drinks: cluster randomised
controlled trial. BMJ 2004; 328: 1237. <PubMed>
10.National Health and Medical Research Council. Clinical practice
guidelines for the management of overweight and obesity in adults.
Canberra: NHMRC, September 2003. Available at:
www.health.gov.au/internet/wcms/publishing.nsf/Content/obesitygui
delines-guidelines-adults.htm/$FILE/adults.pdf (accessed Feb 2005).
11.Clegg A, Sidhu MK, Colquitt J, et al. Clinical and cost
effectiveness of surgery for people with morbid obesity.
Southampton: National Institute for Clinical Excellence, 2001.
Available at: www.nice.org.uk/pdf/AssessmentReport-
Surgeryforobesity.pdf (accessed Mar 2005).
12.NHS National Institute for Clinical Excellence. Guidance on the
use of surgery to aid weight reduction for people with morbid
obesity. Technology Appraisal Guidance No. 46. London: NICE, July
2002. Available at: www.nice.org.uk/pdf/Fullguidance-PDF-
morbid.pdf (accessed Feb 2005).
13.US National Heart, Lung, and Blood Institute. Clinical guidelines
on the identification, evaluation, and treatment of overweight and
obesity in adults. Bethesda, MD: NHLBI, 1998. Available at:
www.nhlbi.nih.gov/guidelines/obesity/ob_home.htm (accessed Feb
2005).
14.Buchwald H. 50 years of bariatric surgery. Obes Surg 2004; 14:
898.
15.Chapman A, Game P, O’Brien P, et al. Systematic review of
laparoscopic adjustable gastric banding in the treatment of obesity.
Update and re-appraisal. Adelaide: Australian Safety and Efficacy
Register of New Interventional Procedures — Surgical, Royal
Australasian College of Surgeons, June 2002. Available at:
www.surgeons.org/asernip-
s/systematic_review/LAGBreviewUp0602.pdf (accessed Feb 2005).
16.Medical Services Advisory Committee, Australian Department of
Health and Ageing. Laparoscopic adjustable gastric banding for
morbid obesity. MSAC reference 14. Assessment report. Canberra:
DHA, 2003. Available at:
www.msac.gov.au/pdfs/reports/msacref14.pdf (accessed Feb 2005).
17.Gallagher SF, Banasiak M, Gonzalvo JP, et al. The impact of
bariatric surgery on the Veterans Administration healthcare system: a
cost analysis. Obes Surg 2003; 13: 245-248. <PubMed>
18.Craig BM, Teng DS. Cost-effectiveness of gastric bypass for
severe obesity. Am J Med 2002; 113: 491-498. <PubMed>
19.Christou NV, Sampalis JS, Liberman M, et al. Surgery decreases
long-term mortality, morbidity, and health care use in morbidly obese
patients. Ann Surg 2004; 240: 416–424. <PubMed>
20.Sampalis JS, Liberman M, Auger S, Christou NV. The impact of
weight reduction surgery on health-care costs in morbidly obese
patients. Obes Surg 2004; 14: 939-947. <PubMed>
21.Clegg A, Colquitt J, Sidhu M, et al. Clinical and cost effectiveness
of surgery for morbid obesity: a systematic review and economic
evaluation. Int J Obes 2003; 27: 1167-1177.
22.Dixon JB, O’Brien PE. Changes in comorbidities and
improvements in quality of life after LAP-BAND placement. Am J
Surg 2002; 184(6B): 51S-54S. <PubMed>
23.Biertho L, Steffen R, Branson R, et al. Management of failed
adjustable gastric banding. Surgery 2005; 137: 33-41. <PubMed>
24.Tweddle EA, Woods S, Blamey S. Laparoscopic gastric banding:
safe and modestly successful. ANZ J Surg 2004; 74: 191-194.
<PubMed>
25.Camerini G, Adami G, Marinari GM, et al. Thirteen years of
follow-up in patients with adjustable silicone gastric banding for
obesity: weight loss and constant rate of late specific complications.
Obes Surg 2004; 14: 1343-1348. <PubMed>
26.O’Brien P, Brown W, Dixon J. Revisional surgery for morbid
obesity – conversion to the Lap-Band system. Obes Surg 2000; 10:
557-563. <PubMed>
27.Hickey MS, Pories WJ, MacDonald KG, et al. A new paradigm
for type 2 diabetes mellitus: could it be a disease of the foregut? Ann
Surg 1998; 227: 637-644. <PubMed>
28.Schauer PR, Burguera B, Ikramuddin S, et al. Effect of
laparoscopic Roux-en-Y gastric bypass on type 2 diabetes mellitus.
Ann Surg 2003; 238: 467-485. <PubMed>
29.MacDonald KG, Long SD, Swanson MS, et al. The gastric bypass
operation reduces the progression and mortality of non-insulin
dependent diabetes mellitus. J Gastrointest Surg 1997; 1: 213–220.
<PubMed>
30.Scopinaro N, Adami GF, Marinari GM, et al. Biliary pancreatic
diversion. World J Surg 1998; 22: 936-946. <PubMed>
31.McCarty DJ, Zimmet P, Dalton A, et al. The rise and rise of
diabetes in Australia, 1996: a review of statistics, trends and costs.
Canberra: Department of Health and Family Services, 1996.
32.Colagiuri S, Colagiuri R, Conway B, et al. DiabCo$t Australia:
assessing the burden of type 2 diabetes in Australia. Canberra:
Diabetes Australia, 2003.
33.House of Commons Health Committee. Obesity. Third report of
session 2003–04. London: Stationery Office, 2004. Available at:
www.publications.parliament.uk/pa/cm200304/cmselect/cmhealth/23
/23.pdf (accessed Feb 2005).
(Received 28 Oct 2004, accepted 15 Feb 2005)
Department of Surgery, University of New South Wales at St George
Hospital, Kogarah, NSW.
Michael L Talbot, MB ChB, FRACS, Senior Lecturer; John O Jorgensen,
MB BS, FRACS, Visiting Surgeon; Ken W Loi, MB BS, FRACS,
Lecturer.
Correspondence: Dr Michael L Talbot, Department of Surgery,
University of New South Wales, Level 3, Pitney Building, St George
Hospital, Kogarah, NSW 2217. m.talbotATunsw.edu.au
AntiSpam note: To avoid spam, authors' email addresses are written
with AT in place of the usual symbol, and we have removed "mail to"
links. Replace AT with the correct symbol to get a valid address.
Other articles have cited this article:
Anna Peeters, Reannan L Cashen and Paul E O’Brien. Inequalities in the provision of bariatric surgery for morbid obesity in Australia Med J Aust
2005; 182 (11): 598-599. [Letters] <http://www.mja.com.au/public/issues/182_11_060605/letters_060605_fm-7.html>
Paul E O’Brien, Wendy A Brown and John B Dixon. Obesity, weight loss and bariatric surgery Med J Aust 2005; 183 (6): 310-314. [Clinical
Update] <http://www.mja.com.au/public/issues/183_06_190905/obr10369_fm.html>
Home | Issues | Email alerts | Classifieds | More... | Contact | Topics | Search
The Medical Journal of Australia eMJA
©The Medical Journal of Australia 2005 www.mja.com.au PRINT ISSN:
0025-729X ONLINE ISSN: 1326-5377
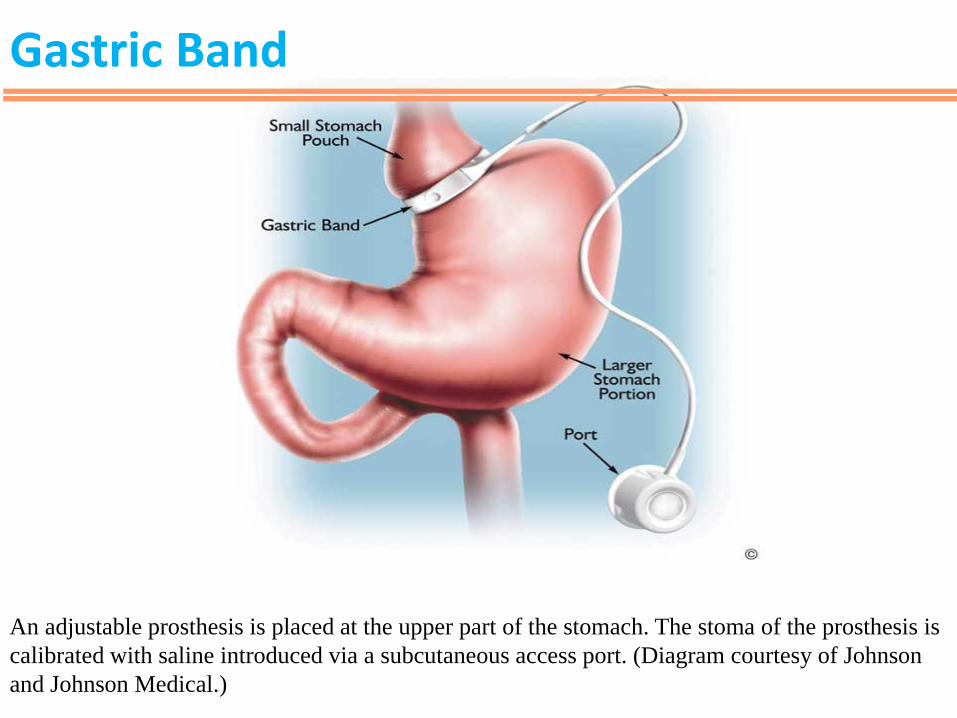
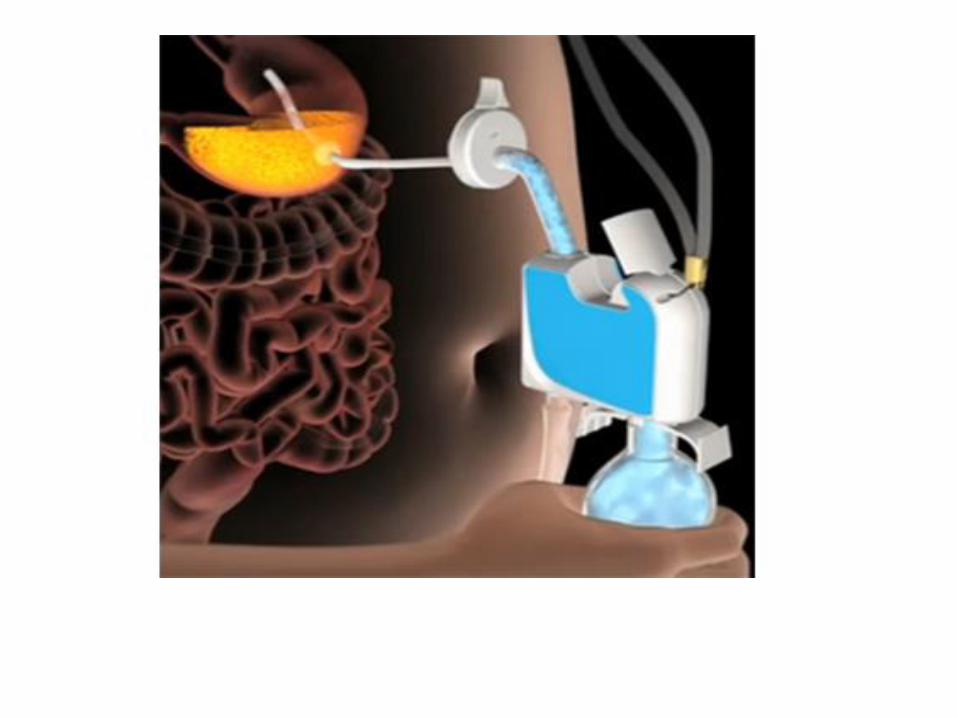
An adjustable prosthesis is placed at the upper part of the stomach. The stoma of the prosthesis is
calibrated with saline introduced via a subcutaneous access port. (Diagram courtesy of Johnson
and Johnson Medical.)
Gastric Band
Mode of action of Gastric banding
• Band is placed at top of stomach which creates a small pouch
• Reduction in intake, quicker and longer satiety
• Proposed that compression of vagal afferent nerves in band area mediates satiety effect (O’Brien, 2010)
• Activation of peripheral satiety mechanism without
physically restricting meal size (Burton& Brown, 2011)
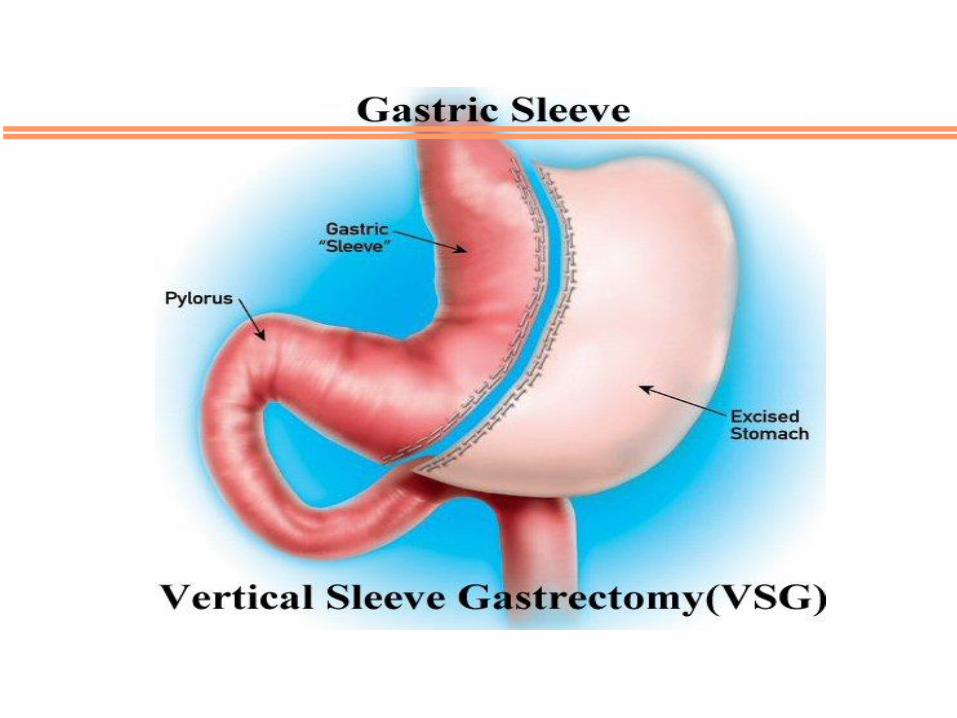
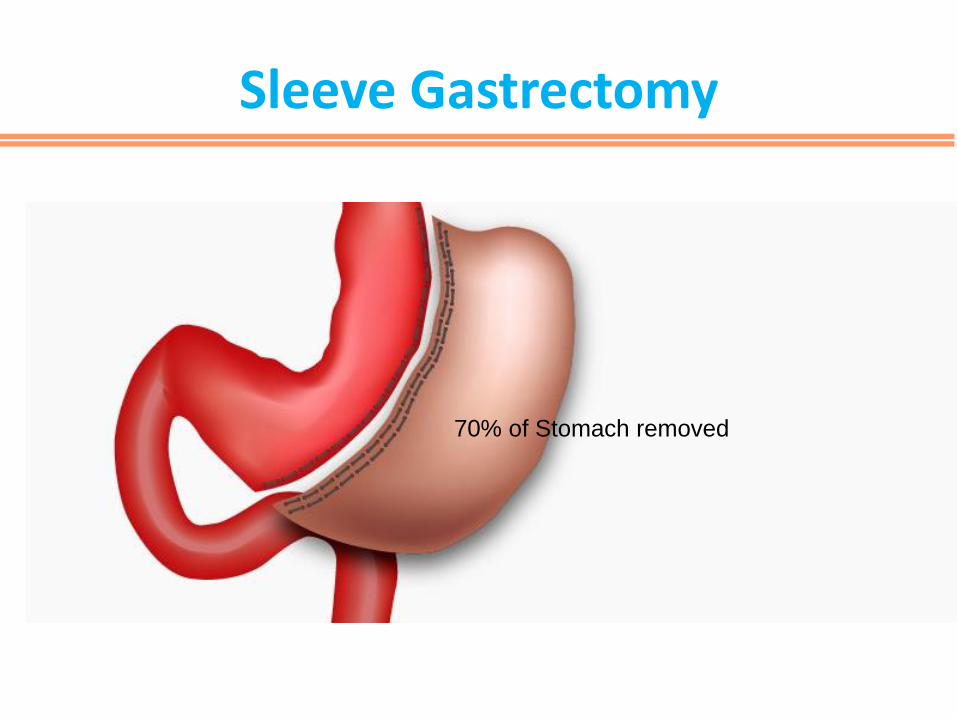
Sleeve Gastrectomy
70% of Stomach removed
Mode of Action of Sleeve
• Restrictive
• Alters hormone signals from stomach to
brain
IFSO/NICE Obesity Guidelines
• BMI >40kg/m2 or BMI >35kg/m2 with co-morbidities that could be improved with weight loss
• All appropriate non surgical measures have failed to achieve clinically significant weight loss
• Intensive management in specialist obesity service
• Commit to the need for long term follow up
• Fast track for people with BMI >50kg/m2
No alcoholism or major psychiatric illness
• Need to be abstinent
• Consult a psychiatrist if necessary
– Schizophrenia, borderline personality, active suicidal ideation, uncontrolled depression (?absolute contraindications)
Evidence
• Swedish Obese Subjects - Mortality: up to 40% lower risk over 10years
(Sjöström et al.,2007)
• Diabetes: >70% remission after 2 years (in recently diagnosed)
(Sjöström et al.,2004) (Dixon et al., 2008)

Bariatric Surgery and Diabetes
• Meta-analysis (Buchwald et al – 2009)
Overall remission rate of 78%
• < 2 years since surgery 80%
• >2 years since surgery 75%
• Results seen with all operations, yet most dramatic with the gastric bypass
If treated within 5 years of Diabetes diagnosis—higher long term remission rates (Brethauer et al, 2013)
Bypass and Diabetes
• Bypass shows more promising resolution of diabetes than the sleeve or band.
• Parikh et al (2013)—Meta-analysis (1389pts)
– Remission rates (1 year):
• 33% Lap band
• 54% Sleeve
• 64% Gastric Bypass
• Buchwald et al (2009)
– Resolution of T2DM
• 57% Lap band patients
• 80% Gastric bypass patients
Bypass and Diabetes
• Unique to bypass—Diabetes resolution can come before weight loss
• Rubino et al (2006) – animal studies
– Bypassing a short segment of proximal intestine directly ameliorates T2DM, independent of food intake, body weight, etc.
– Potentially undiscovered factors from proximal small bowel contributing to pathophysiology of DM
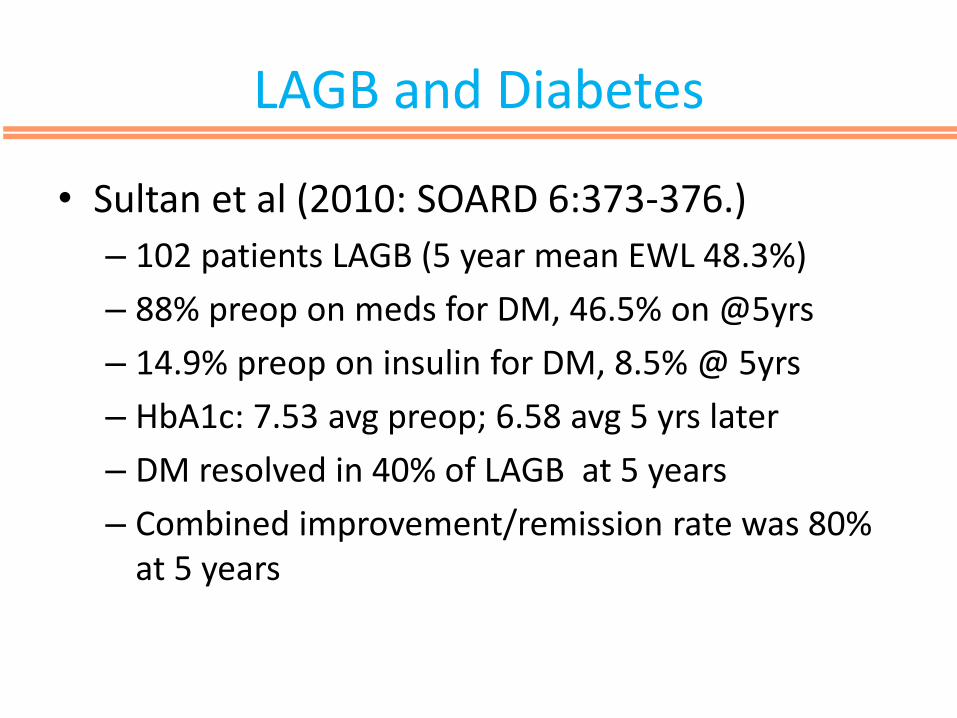
LAGB and Diabetes
• Sultan et al (2010: SOARD 6:373-376.)
– 102 patients LAGB (5 year mean EWL 48.3%)
– 88% preop on meds for DM, 46.5% on @5yrs
– 14.9% preop on insulin for DM, 8.5% @ 5yrs
– HbA1c: 7.53 avg preop; 6.58 avg 5 yrs later
– DM resolved in 40% of LAGB at 5 years
– Combined improvement/remission rate was 80% at 5 years
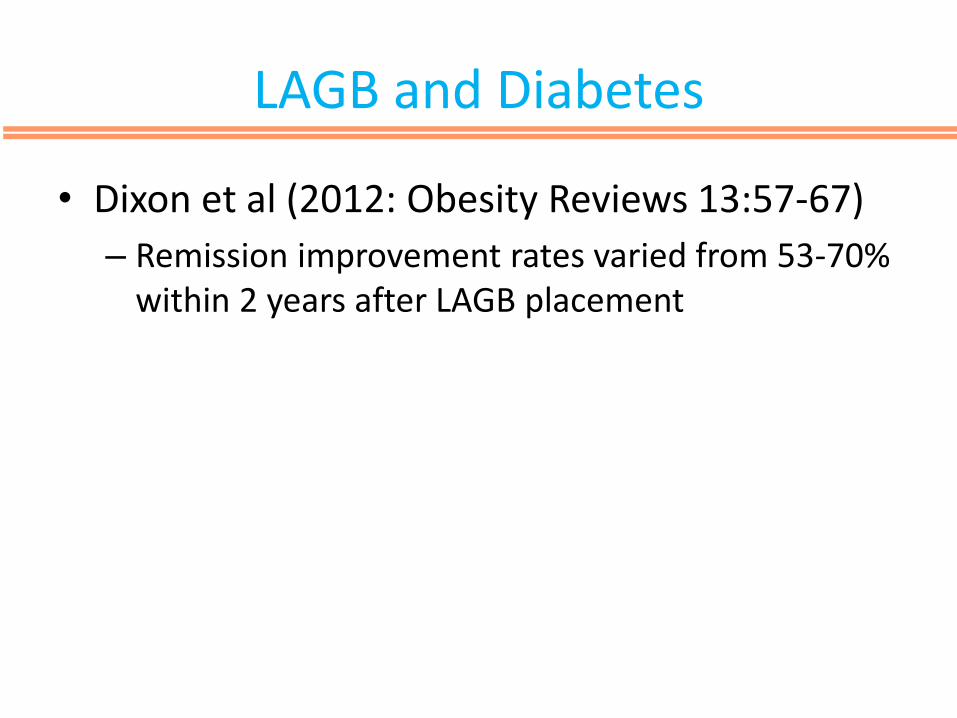
LAGB and Diabetes
• Dixon et al (2012: Obesity Reviews 13:57-67)
– Remission improvement rates varied from 53-70% within 2 years after LAGB placement
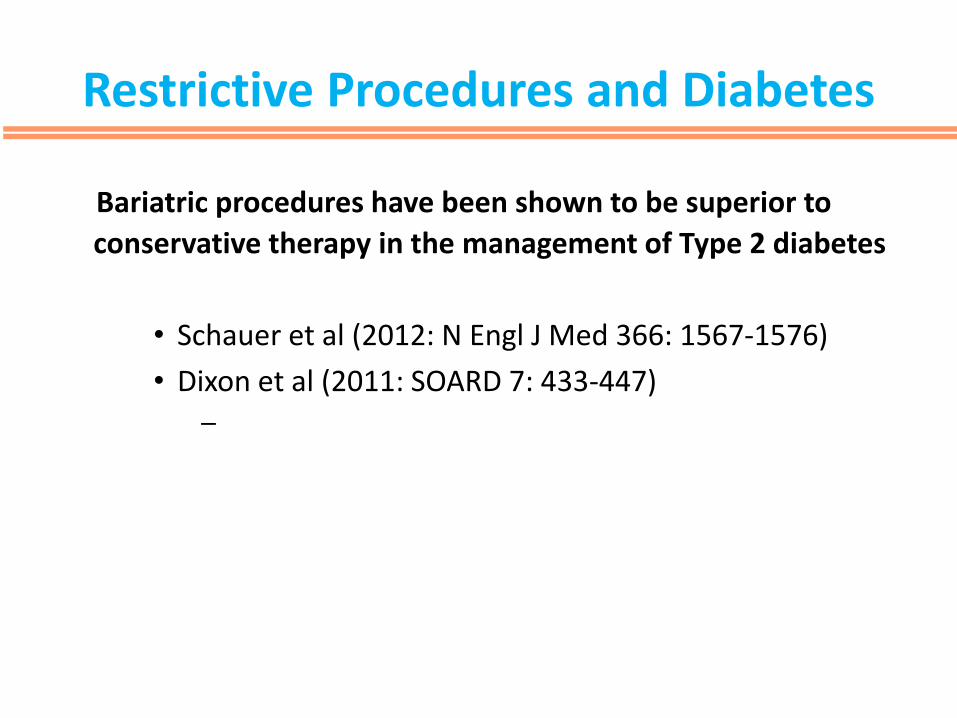
Restrictive Procedures and Diabetes
Bariatric procedures have been shown to be superior to
conservative therapy in the management of Type 2 diabetes
• Schauer et al (2012: N Engl J Med 366: 1567-1576)
• Dixon et al (2011: SOARD 7: 433-447) –

Long term Remission
Association of Bariatric Surgery With Long-term Remission of Type 2 Diabetes and With Microvascular and Macrovascular Complications
Lars Sjöström et al
JAMA. 2014;311(22):2297-2304.
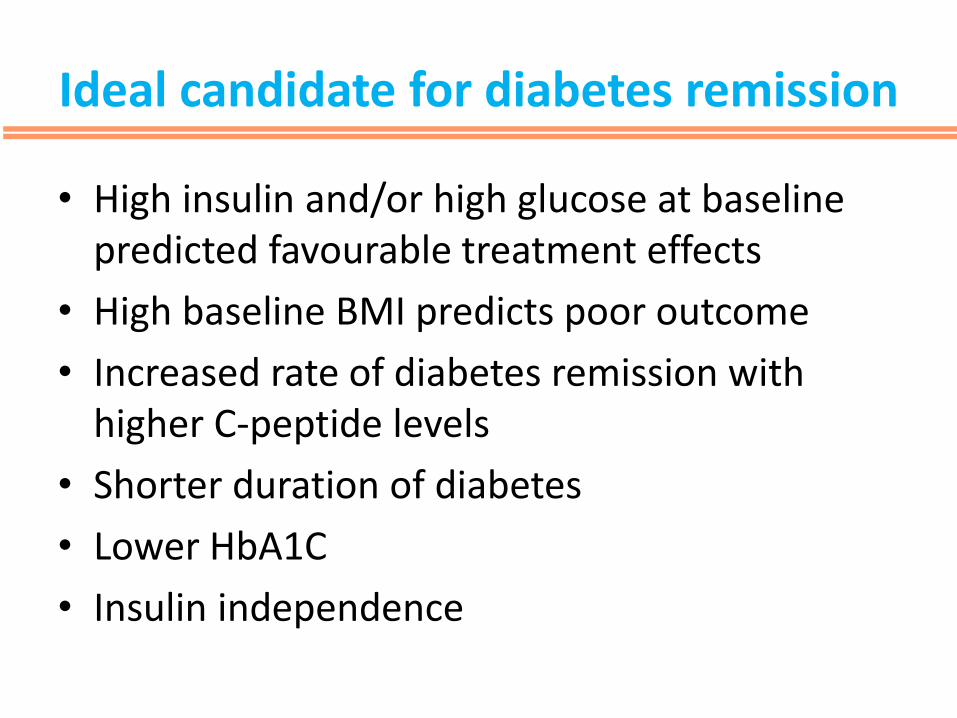
Ideal candidate for diabetes remission
• High insulin and/or high glucose at baseline predicted favourable treatment effects
• High baseline BMI predicts poor outcome
• Increased rate of diabetes remission with higher C-peptide levels
• Shorter duration of diabetes
• Lower HbA1C
• Insulin independence
Benefits of Bariatric surgery
•BP reduction
•Reduced risk of cancer
•Improved quality of life
•Improved exercise tolerance
•Reduced cardio vascular risk
•Improvement in sleep apnoea
•Improvement in fertility
•Increased confidence and self esteem

Metabolic complications of bariatric surgery
1. Acid-base disorder 2. Bacterial overgrowth (primarily with BPD, BPD/DS) 3. Pseudo-obstruction 4. Nocturnal diarrhea 5. Proctitis 6. Acute arthralgia 7. Electrolyte abnormalities (primarily with BPD, BPD/DS) Low
Ca, K, Mg, Na, P 8. Arrhythmia, myopathy 9. Enteral or parenteral repletion 10. Fat-soluble vitamin deficiency Vitamin A—night vision 11. Vitamin D—osteomalacia 12. Vitamin E—rash, neurologic 13. Vitamin K—coagulopathy 14. Folic acid deficiency Hyperhomocysteinemia
15. Anaemia 16. Foetal neural tube defects 17. Osteoporosis Fractures 18. Oxalosis Kidney stones 19. Secondary hyperparathyroidism 20. Vitamin D deficiency 21. Thiamine deficiency Wernicke–Korsakoff encephalopathy 22. Beriberi 23. Vitamin B12 deficiency Neuropathy 24. Zinc deficiency 25. Selenium deficiency
Metabolic complications of bariatric surgery
•Post operative worsening of retinopathy
•Recurrent hypoglycaemia leading to cognitive impairment
•Nesidioblastoma
Other complications
Spot the difference
Summary
• Remission of Type 2 and not Type 1 diabetes can be expected with Bariatric surgery.
• Prolonged duration of disease has been associated with poorer remission rates of diabetes after bariatric surgery
• Even if Type 2 diabetes remission is achieved patients should be followed yearly with HbA1C and should have retinal screening done
