barbara dale bsn rn chhn cwocn quality home health...
TRANSCRIPT
Barbara Dale BSN RN CHHN CWOCN
Quality Home Health Livingston TN

1. Describe the difference in hospice and
palliative care.
2. Discuss symptom management in palliative
care.
3. Identify practical approaches that integrate
basic wound care principles into palliative
care.

“We live in a very particular death-denying society. We isolate both the dying and the old, and it serves a purpose. They are reminders of our own mortality. We should not institutionalize people. We can give families more help with home care and visiting nurses, giving the families and the patients the spiritual, emotional, and financial help in order to facilitate the final care at home” 1972, Dr Elisabeth Kubler-Ross at a U. S. Senate special committee on aging hearing (National Hospice & Palliative Care Organization[NHPCO], n.d., p.1).
Started as a hospice movement in the 19th century, religious orders created hospices that provided care for the sick and dying in London and Ireland.
In recent years, Palliative care has become a large movement, affecting much of the population.
Began as a volunteer-led movement in the United states and has developed into a vital part of the health care system.

The goal is to improve the quality of life for
individuals who are suffering from severe
diseases.
Palliative care offers a diverse array of
assistance and care to the patient.

Palliative care:
provides relief from pain and other distressing
symptoms;
affirms life and regards dying as a normal
process;
intends neither to hasten or postpone death;
integrates the psychological and spiritual aspects
of patient care;
offers a support system to help patients live as
actively as possible until death;
offers a support system to help the family cope during the patients illness and in their own bereavement;
uses a team approach to address the needs of patients and their families, including bereavement counseling, if indicated;
will enhance quality of life, and may also positively influence the course of illness;
is applicable early in the course of illness, in conjunction with other therapies that are intended to prolong life, such as chemotherapy or radiation therapy, and includes those investigations needed to better understand and manage distressing clinical complications.
Palliative care can be provided from the time
of diagnosis.
Palliative care can be given simultaneously
with curative treatment.
Both services have foundations in the same
philosophy of reducing the severity of the
symptoms of a sickness or old age.

HOSPICE: The patient has both
• a limited life expectancy (specifically six months or
less);
• and the goals for care are exclusively to achieve and
maintain comfort, regardless of the symptom burden.
PALLIATIVE CARE: The patient has either
• a limited life expectancy (regardless of symptom burden
or goals for care),
• or a significant symptom burden (regardless of
prognosis or goals for care) or goals for care
exclusively to achieve and maintain comfort
(regardless of prognosis or symptom burden).

Division made between these two terms in
the United States
Hospice is a “type” of palliative care for
those who are at the end of their lives.
Image courtesy of
http://www.ersj.org.uk/content/32/3/796.full

Palliative
Care
Graphic by Anne Kinderman, MD; used with permission.
August 2011 Interpreting in Palliative Care 11

1. Symptom management
2. Patient/family goals
the goals of healthcare are "to cure
sometimes, relieve often, and comfort
always." Hemani, 2008.

pain from the wound
odor/smell
amount of drainage
pain from dressing changes
bleeding
appearance of the wound
Itching
Usually listed as last goals as they may be the most
difficult to modify
decreasing wound size
complete healing of the wound
Emmons, 2014

Prevention of
deterioration and
stabilization of the
wound
Promotion of a
clinically clean and
protected wound
environment
Minimization of
infection and sepsis
Control of pain, odor
and excessive exudate
Reduction in the
frequency of dressing
changes
Minimization of
bleeding
Prevention of trauma
Management of
maceration
Elimination of pruritis
Emmons, 2014

Explain and document that complete wound healing may not
be a primary outcome 2/2 (list conditions, end stage..,
arterial disease, Ca, etc). The plan of care will focus on
meeting the needs of the patient/family. By providing
excellent care, if physiologically possible, wound healing
may occur.
Ask the patient and family, what is most bothersome about
the wound.
List out of the problems and develop a plan for each issue
Prioritize each issue based on what is the worst and what
can be achieved.
Set realistic goals
Emmons, 2014

Beneficence: do good
Non-maleficence- do no harm
Autonomy-patient‟s right to decide
Justice-fairness

Pressure ulcers,
Skin tears,
Venous and/or arterial leg ulcers,
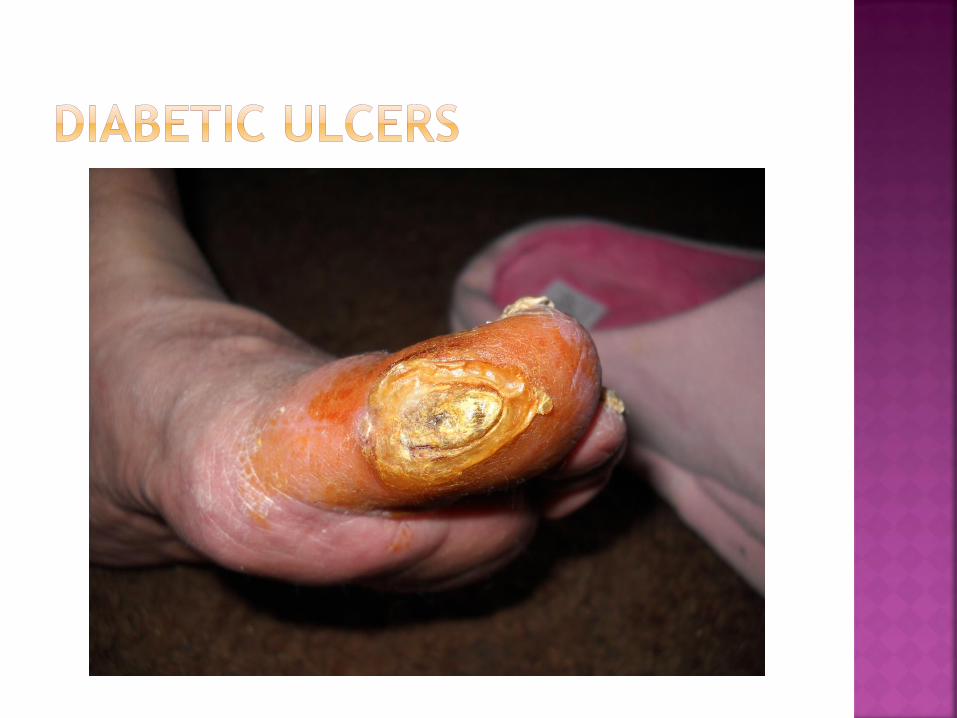
DFiabetic ulcers,
Fungating/malignant wounds.

Happy wounds are
healing wounds

3 requirements for wound healing
Etiology-what “caused” the wound. Try to
correct or manage the cause.
Systemic- is the pt „able” to heal? Education to
pt to improve healing ability.
Topical- what is done to the wound to make the
wound happy. Happy wounds are healing wounds.
Based on DIPAMOPI.

Determine the cause
Correct or manage the cause
Pressure-support surfaces, turning, etc
Venous stasis-compression
Arterial-vascular consult
Surgical-NA
Diabetic-glucose control, offloading
Atypical-varies, referral to dermatology (?)
Skin tears-improve skin integrity, pad items

Nutrition-protein 1.2-1.5g/kg/d & calories 30cc/kg/d
Perfusion-decrease reducible factors
BMI-appropriate wt/ht
Activity-
Glucose management
Hydration-30cc/kg/d typical
Immune system
Manage co-morbidities

D Debride any non viable tissue
I Infection
P Pack dead space
A Absorb exudate
M Maintain moist environment
O Open closed wound edges
P Protect from trauma
I Insulate
Addressing ALL of these components make for a
happy wound.

Soupy wet or dried out.
Cold (frequent changes)
Lots of necrotic tissue
Infection
Pressure
Moist
Warm
Protected from trauma
Controlled bacteria (bioburden)
Free: http://www.epuap.org/wp-
content/uploads/2012/07/SCALE-Final-
Version-2009.pdf
Statement 9: The probable skin change etiology and
goals of care should be determined. Consider the 5 Ps
for determining appropriate intervention strategies:
Prevention
Prescription (may heal with appropriate treatment)
Preservation (maintenance without deterioration)
Palliation (provide comfort and care)
Preference (patient desires)

Braden
Norton
Hunters Hill (specifically for Palliative Care)



Pressure Ulcers
Although risk can be assessed to develop
individual care plans, all palliative patients are
high risk and should be treated the same. The
three ingredients of a successful prevention
program5 include 1) pressure
relief/redistribution for bed and chair, 2)
pressure relief/redistribution for heels, and 3)
lubricating the skin with aggressive emollient
therapy.(Tippett 2012)



Most bothersome symptoms: Drainage and itching
Itching---lanolin and topical abx can exacerbate eczema and actually
cause itching
Venous Hypertension: Back pressure on the venous system exerted either
from central or pulmonary sources, or from extrinsic compression
syndrome. Example, a mass, tumor or tight girdle.
Venous Insufficiency: An obstruction which blocks outflow, valvular
incompetence, which permits retrograde flow, or muscle pump failure,
resulting in incomplete emptying of the venous system in the lower leg.
Venous Leg Ulcers: Wounds that usually occur on the lower leg in people
with venous insufficiency disease. Venous Leg Ulcers are also known by
such terms as venous stasis ulcer and venous insufficiency. Ulcers result
from chronic venous hypertension caused by the failure of the calf
muscle pump.

CHF- dyspnea

Venous stasis ulcers
Other:
Rheumatoid arthritis
PVD/Arterial wounds/gangrene















Clean – Free of bacterial proliferation eliciting no response from the host.
Contamination – The presence of bacteria on the wound surface without proliferation.
Colonization – Presence and proliferation of bacteria eliciting no response from the host.
Infection – Invasion of bacteria which proliferates and elicits a response from the host e.g.,erythema, pain, warmth, edema, exudates
Bacterial balance describes the bacterial level present in a wound and their ability to cause damage or infection. All chronic wounds contain bacteria. However, the impact of these bacteria on healing is dependent on several factors, including the number of organisms, the virulence of these organisms and host resistance (Sibbald, Woo, & Ayello, 2006).


Special shout out to Dr Emmons for
sharing your wisdom and resources!

Hemani, S. & Letizia, M.(2008) Providing Palliative Care in End-stage
Heart Failure. Journal of Hospice and Palliative Nursing,10(2):100-
105.
McDonald, A. & Lesage, P. (2006). Palliative management of pressure
ulcers in malignant wound inpatients with advanced illness. Journal
of Palliative Medicine, 9(2):285-296.
National Hospice & Palliative Care Organization. (n.d.). History of
Hospice Care. Retrieved April 20, 2013, from
http://www.nhpco.org/history-hospice-care
Kunimoto, B., Cooling, M., Gulliver, W., Houghton, P., Orsted, H., &
Sibbald, R. G. (2001). Best Practices in the Prevention and
Treatement of Venous Leg Ulcers. Ostomy Wound Management,
47(2), 34-50.
Jerant, A. F., Azari, R. S., Nesbitt, T. S., & Meyers, F. J. (2004). The
TLC Model of Palliative Care in the Elderly: Preliminary Application in
the Assisted Living Setting. Annals of Family Medicine, 2, 54-60.
doi:10.1370/afm.29

Lipsky, B., Berendt, A. R., Cornia, P. B., Pile, J. C., Peters, E. J.,
Armstrong, D. G., . . . Senneville, E. (2012, March 22). ISDA Guidelines.
2012 Infectious Diseases Society of America Clinical Practice Guideline
for the Diagnosis and Treatment of Diabetic Foot Infections. Oxford
University Press. Retrieved May 14, 2013, from
http://www.idsociety.org/uploadedFiles/IDSA/Guidelines-
Patient_Care/PDF_Library/2012%20Diabetic%20Foot%20Infections%20Guid
eline.pdf
Resnick, B. (2012). Differentiating programs versus philosophies of care:
Palliative care and hospice care are not equal. Geriatric Nursing, 33(6),
427-429. doi:10.1016/j.gerinurse.2012.09.008.
Williams, R. (2009). Cadexomer iodine: An effective palliative dressing in
chronic critical limb ischemia. WOUNDS, 21(11).
Roat, C., Kinderman, A., & Fernandez, A. (2011) Interpreting in Palliative
Care: A continuing education workshop. Available from http:
//www.chef.org/publications/2011/11/interpreting-palliative-care-
curriculum

Grocott, P. Gethin, G., & Probst, S. (2013). Malignant wound management
in advanced illness: new insights. Current Opinions in Supportive and
Palliative Care, 7(1), 101-5.
Letizia, M., Uebelhor, J., & Paddack, E. (2010). Providing palliative care
to seriously ill patients with nonhealing wounds, Journal of Wound
Ostomy Continence Nursing, 37(3), 277-82.
McManus, J. (2007). Principles of skin and wound care: the palliative
approach. End of Life Care, 1(1), 8-17.
McCusker M, Ceronsky L, Crone C, Epstein H, Greene B, Halvorson J,
Kephart K, Mallen E, Nosan B, Rohr M, Rosenberg E, Ruff R, Schlecht K,
Setterlund L. Institute for Clinical Systems Improvement. Palliative Care
for Adults. Updated November 2013. Available from:
https://www.icsi.org/_asset/k056ab/PalliativeCare.pdf
Clinical Practice Guidelines for Quality Palliative Care, Third Edition.
(2013). National Concensus Project for Quality Palliative Care. Available
from :
http://www.nationalconsensusproject.org/Guidelines_Download2.aspx

F.R.A.I.L. (2002). F.R.A.I.L. Supplement Report, WOUNDS, 14(8).
Supplement; October 2002.
Emflorgo, C. (1998) Controlling Bleeding in Fungating Wounds. Journal of
Wound Care, 7(5).
Emmons, KR & Lachman VD. (2010). Palliative Wound Care. A concept
analysis. JWOCN 37(6):639-644
Sibbald RG, Krasner DL, Lutz JB, et al. The SCALE Expert Panel: Skin
Changes At Life’s End. Final Consensus Document. October 1, 2009.
Available from: http://www.epuap.org/wp-
content/uploads/2012/07/SCALE-Final-Version-2009.pdf
National Hospice & Palliative Care Organization. (n.d.). History of
Hospice Care. Available from http://www.nhpco.org/history-hospice-care
Lo, S. F., Hayler, M., Hu, W. Y., Hsu, M. Y., & Li, Y. F. (2012). Symptom
burden and quality of life in patients with malignant fungating wounds.
Journal of Advanced Nursing, 68(6).