ba md wed 03 0805 saseen hypertension - cleveland … controlled if treated guidelines for...
TRANSCRIPT

1
Hypertension Pharmacotherapy
Joseph Saseen, Pharm.D., FCCP, BCPSProfessor
University of ColoradoAnschutz Medical Campus
School of Pharmacy and Medicine
American Heart Association (AHA)Heart Disease and Stroke Statistics—2011 Update
82.6 Million Americans have Cardiovascular Disease
Rogers VL, et al. Circulation. 2011;123.* Total cholesterol ≥240 mg/dL

2
National Health and Nutrition Examination Survey (NHANES) in the U.S.
Hypertension 2007;49:69-75. JAMA 2010;303:2043-2050.
72.3% Controlled if Treated
Guidelines for Hypertension
● 2003 - The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7)
● 2007 - American Heart Association Scientific Statement (AHA)
● 2011 - American Heart Association Scientific Statement (AHA)
JNC 8 (to be release in 2012)
3
Guidelines for Hypertension
http://www.nhlbi.nih.gov/guidelines/cvd_adult/background.htm
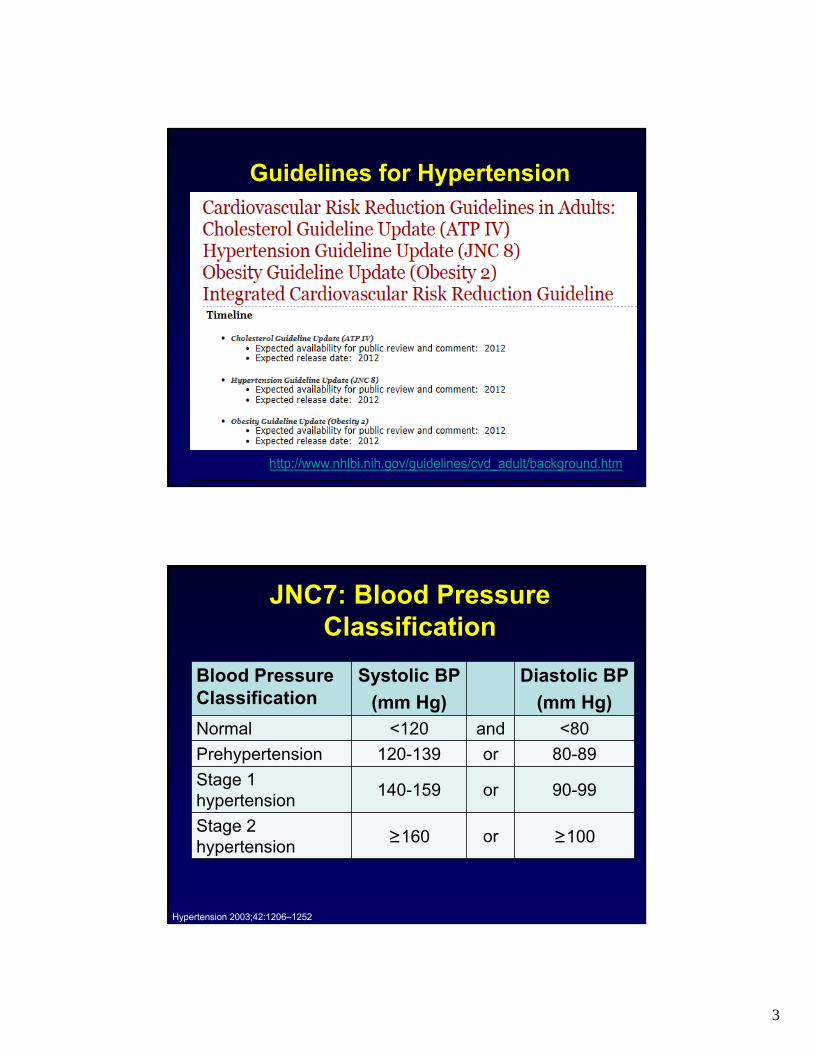
JNC7: Blood Pressure Classification
Hypertension 2003;42:1206–1252
Blood Pressure Classification
Systolic BP
(mm Hg)
Diastolic BP
(mm Hg)Normal <120 and <80
Prehypertension 120-139 or 80-89
Stage 1 hypertension
140-159 or 90-99
Stage 2 hypertension
≥160 or ≥100

4
Polling Question…
● Lower is better with regard to BP goals, with regard to reducing risk of CV events.
True
False
2003: The 7th Report of the Joint National Committee on Prevention, Detection,
Evaluation, and Treatment of High Blood Pressure (JNC7)
Primary Goal: CV morbidity & mortality
Blood Pressure Goals:
● <140/90 mm Hg for most patients
● <130/80 mm Hg for Diabetes or Chronic Kidney Disease
Hypertension 2003;42:1206–1252.

5
2007 AHA Scientific Statement:Treatment of Hypertension in the
Prevention and Management of Ischemic Heart Disease
Circulation. 2007;115:2761-2788.
CAD, coronary artery disease
● High CAD defined by AHA as:– diabetes,
– chronic kidney disease,
– CAD equivalent (carotid artery disease, peripheral arterial disease, abdominal aortic aneurysm), or
– 10-year Framingham risk score ≥10%
AHA: Evidence-Base for BP GoalsBoth < 140/90 or <130/80 mm Hg
● Classification of Recommendation: IIa–Weight of evidence/opinion is in favor of
usefulness/efficacy
● Level of Evidence: B–Data derived from a single randomized trial or
nonrandomized studies
Circulation. 2007;115:2761-2788.

6
Current Controversy: BP Goals lower than < 140/90 mm Hg
● A 2009 Cochrane analysis:– 7 trials (22,089 subjects)
comparing different diastolic BP targets were included
– Did not demonstrate that more aggressive lowering of BP reduced mortality or morbidity better than the standard < 140/90 mm Hg
Cochrane Database of Systematic Reviews 2009, Issue 3. Art. No.: CD004349.
JAMA 2009:302(10): 1047-1048.
Systolic Blood Pressure Intervention Trial (SPRINT)
Sponsored by National Heart, Lung, and Blood Institute (NHLBI)
● Two-arm, multicenter, randomized clinical trial:– Intensive Control: SBP <120 mm Hg
– Standard BP: SBP <140 mm Hg
● 9250 patient with hypertension, ≥ 55 yrs, and at least one additional CV risk factor followed for 4-6 years
● Patients with serious comorbidities are excluded (eg, diabetes, prior stroke, left ventricular dysfunction)
● Primary outcome: First occurrence of MI, acute coronary syndrome, stroke, heart failure, or CVD death
● Anticipated completion in December 2018http://www.clinicaltrials.gov/ct2/show/NCT01206062?term=sprint&rank=2

7
AHA/ACCF Guideline: 2011 UpdateSecondary Prevention and Risk Reduction
Therapy for Patients with Coronary and other Atherosclerotic Vascular Disease
● Blood pressure control–Goal: 140/90 mm Hg
–Patients with blood pressure ≥140/90 mm Hg should be treated, as tolerated, with blood pressure medication, treating initially with beta-blockers and/or ACE inhibitors, with addition of other drugs as needed to achieve goal blood pressure.(Level of Evidence: A)
Circulation. 2011;124:2458-2473
Is Lower Better in CKD:<130/80 mm Hg vs. <140/90 mm Hg
● Systematic Review; 3 trials (MDRD, AASK, REIN-2) with 2272 participants
● Trials did not show that a lower BP target of <125/75 to 130/80 mm Hg is more beneficial than a target of less than 140/90 mm Hg
● Lower-quality evidence suggested that a low target may be beneficial in subgroups with proteinuria greater than 300 to 1000 mg/day
Upadhyay A, et al. Ann Intern Med; published online March 14, 2011

8
Reflective Question…
A BP goal of <130/80 mm Hg is recommended in patients with diabetes. Is this an evidence
based recommendation?
Hypertension Optimal Treatment (HOT) Trial: Major Cardiovascular Events at 4 yrs
All Patients n=18,790; p=NS
Lancet. 1998;351:1755-1762.
Patients with Diabetesn=1501; p=0.005

9
The Action to Control Cardiovascular Risk in Diabetes (ACCORD) Blood Pressure Trial
● Randomized, open-label, multi-center trial
● Intensive (SBP <120 mm Hg) vs. standard (SBP < 140 mm Hg) BP lowering
● 4733 patients with hypertension and:–Stable type 2 diabetes and high CVD risk
–40-79 years if established clinical CVD, or 55-79 years if ≥ 2 CV risks or subclinical CVD
● Primary Outcome: nonfatal MI, nonfatal stroke or CV death
N Engl J Med 2010;362:1575-85.
ACCORD-BP
N Engl J Med 2010;362:1575-85.

10
ACCORD-BP: Results
Intensive Events (%/yr)
StandardEvents (%/yr) HR (95% CI) P
Primary Outcome 208 (1.87) 237 (2.09) 0.88 (0.73-1.06) 0.20
Pre-specified Secondary Outcomes
Total Mortality 150 (1.28) 144 (1.19) 1.07 (0.85-1.35) 0.55
CV Death 60 (0.52) 58 (0.49) 1.06 (0.74-1.52) 0.74
Nonfatal MI 126 (1.13) 146 (1.28) 0.87 (0.68-1.10) 0.25
Nonfatal Stroke 34 (0.30) 55 (0.47) 0.63 (0.41-0.96) 0.03
Total Stroke 36 (0.32) 62 (0.53) 0.59 (0.39-0.89) 0.01
N Engl J Med 2010;362:1575-85.
ACCORD-BP: Adverse EventsIntensive
N (%)Standard
N (%)P
Serious Adverse Events 77 (3.3) 30 (1.3) <0.0001
• Hypotension 17 (0.7) 1 (0.04) <0.0001
• Syncope 12 (0.5) 5 (0.2) 0.10
• Bradycardia or Arrhythmia 12 (0.5) 3 (0.1) 0.02
• Hyperkalemia 9 (0.4) 1 (0.04) 0.01
eGFR ever <30 mL/min/1.73m2 99 (4.2) 52 (2.2) <0.001
Any Dialysis or ESRD 59 (2.5) 58 (2.4) 0.93
N Engl J Med 2010;362:1575-85.

11
JNC 7 Algorithm
Drug(s) for the compelling indications
Other drugs (diuretics, ACEI,
ARB, BB, CCB) as needed.
Stage 1 HypertensionThiazide-type
diuretics for most. May consider
ACEI, ARB, BB, CCB,
or combination.
Stage 2 Hypertension
2-drug combination for most (usually
thiazide-type diuretic and
ACEI, or ARB, or BB, or CCB)
Initial Drug Choices
With Compelling Indications
Without Compelling Indications
Hypertension 2003;42:1206–1252.
AHA Scientific Statement
Circulation. 2007;115:2761-2788.
AreaSpecific Drug Indications
General CAD Prevention
Monotherapy or combination therapy:
● ACEI (or ARB),
● CCB,
● or thiazide diuretic first-lineHigh CAD risk1
CAD2 Beta-blocker with ACEI or ARB
LVDACEI or ARB and beta-blocker and aldosterone antagonist and diuretic
CAD, coronary artery disease; LVD, left ventricular dysfunction (aka. systolic heart failure)
1= diabetes, chronic kidney disease, CAD equivalent (carotid artery disease, peripheral arterial disease, abdominal aortic aneurysm), or 10-year Framingham risk score ≥10%
2= stable angina, unstable angina/NSTEMI, or STEMI

12
Polling Question…
● The reason that beta-blockers are no longer first-line for most patients with hypertension is because they cause too many side effects (e.g., erectile dysfunction, fatigue).
True
False
A Cochrane Collaboration (2007):Beta-Blockers for Hypertension
● 13 randomized trials in 91,561 patients
Atenolol used 75% of the time
CochraneDatabase of Systematic Reviews 2007, Issue 1. Art.No.:CD002003.
Beta-blocker vs.
Relative Risk (95% CI)
CV Disease Stroke Death
Placebo0.88*
(0.79-0.97)
0.80* (0.66–0.96)
0.99 (0.88-1.11)
Thiazide1.13
(0.99-1.13)
1.17 (0.65–2.09)
1.04 (0.91-1.19)
ACEI/ARB1.00
(0.72-1.38)
1.30*(1.11-1.53)
1.10 (0.98-1.24)
CCB1.18*
(1.08-1.29)
1.24*(1.11-1.40)
1.07(1.00-1.14)

13
Comparison of Beta-BlockersDaily
Frequencyt½ (hr) Lipid
SolubilityCardio-
selectivityAlpha
Blockade
Atenolol (generic)
1-2 6-7 Low Yes No
Metoprolol Tartrate
2 3-7
Moderate to High
Yes NoMetoprolol
Succinate (Toprol XL®)
1 n/a
Carvedilol (Coreg®)
2 6-10High No Yes
Carvedilol (Coreg® CR)
1 n/a
Beta-Blocker After MI
● Systematic review of 82 randomized controlled trials, that evaluated mortality
● Long term use:–23% mortality reduction (RR 0.77; 69-0.85)
However: “Most evidence was for propranolol, timolol, metoprolol, whereas atenolol, which is commonly used, is inadequately evaluated for
long term use”
BMJ 1999;318:1730-1737.

14
Antihypertensive Pharmacotherapy
● Traditional First-Line Agents– Angiotensin Converting
Enzyme Inhibitor (ACEi)
– Angiotensin Receptor Blocker (ARB)
– Beta-Blocker
– Calcium Channel Blocker (CCB)
– Diuretic (typically a thiazide)
● Alternative Agents– Aldosterone Antagonist (e.g.,
spironolactone)
– Alpha Antagonist (i.e., terazosin)
– Centrally Acting Alpha Agonist (i.e., clonidine)
– Direct Arterial Vasodilator (i.e., hydralazine)
– Direct Renin Inhibitor (i.e., aliskiren)
– Loop Diuretic
– Rauwolfia Alkaloid (i.e., reserpine)
ANGIOTENSIN II
ANGIOTENSINOGEN
ANGIOTENSIN I
Vasoconstriction Aldosterone
synthesis
Sodium/Water Reabsorption
Blood Pressure
Glomerulus
Juxtaglomerular Cells
Efferent Arteriole
Afferent Arteriole
Nep
hro
n
SympatheticNerves
MaculaDensa
Renin
Converting Enzyme
AdrenalCortex
Kidney Intestine CNS Peripheral Nervous System Vascular Smooth Muscle
Heart
Contractility
Cardiac Output
Total Peripheral Resistance
Vasopressin
Sympathetic Discharge
BloodVolume
Renin Secretion
Macula densa signal Renal artery pressure/blood flow
Sympathetic stimulation
DiPiro JT, Talbert RL, Yee GC, et al, eds. Pharmacotherapy: A Pathophysiologic Approach. 7th ed. New York, NY: McGraw-Hill Companies, Inc; 2008.

15
Diuretics● Thiazide-type preferred
● Very inexpensive
● Long-term effects from decreasing peripheral vascular resistance
● Dose-dependent metabolic side effect (e.g., hypokalemia, hyperglycemia)
● Potassium sparing drugs minimize hyopkalemia but do not enhance BP lowering
Beta-Blockers
● Cardioselective agents are preferred
● Most are generic
● Decrease contractility, decrease heart rate, decrease adrenergic stimulation to lower BP
● Dose-dependent side effects (e.g., exercise intolerance, fatigue, heart block)
● Little to no role for ISA type beta-blockers

16
ACE Inhibitors
● Generic and inexpensive
● All available in fixed-dose combinations with HCTZ
● Slightly less effective in African Americans when used as monotherapy
● Most side effect (e.g., cough, angioedema) are not dose dependent
● Contraindicated in:
–Pregnancy, bilateral renal artery stenosis, history of angioedema,
ARBs
● Losartan is the only generic (valsartan, irbesartan in 2012)
● All available in fixed-dose combinations with HCTZ, some in three-drug combinations with amlodipine and HCTZ
● Slightly less effective in African Americans when used as monotherapy
● Fewest side effects of all major antihypertensive classes
● Contraindicated in:
– Pregnancy, bilateral renal artery stenosis

17
Calcium Channel BlockersDihydropyridines
– Amlodipine
– Felodipine
– Nifedipine
● Potent vasodilators
● Most common CCBs used in hypertension
● Dose dependent side effects (e.g., peripheral edema)
● Most are generic
Non-Dihydropyridines– Diltiazem
– Verapamil
● Moderate vasodilators that lower heart rate
● Dose dependent side effects (e.g., brady-cardia, constipation)
● Most are generic and extended release formulations
Combination Regimens
● Mean # of antihypertensive agents needed:–≥ 2 if goal BP is < 140/90 mm Hg
–≥ 3 if goal BP is < 130/80 mm Hg
● A diuretic is usually additive with other agents
● Many fixed-dose combinations:– Traditional: thiazide/ACEI, thiazide/ARB,
thiazide /beta-blocker, CCB/ACEI
– Newer: ARB/CCB, ARB/CCB/thiazide
● Fixed-dose combinations may decrease pill burden and costs
DiPiro JT, Talbert RL, Yee GC, et al, eds. Pharmacotherapy: A Pathophysiologic Approach. 7th ed. New York, NY: McGraw-Hill Companies, Inc; 2008.

18
Compliance, Safety, and Effectiveness of Fixed-Dose Combinations of Antihypertensive Agents
● Meta-analysis of 15 studies (n=32,331):
Fixed-Dose vs. Free Drug Combinations
P-value
Compliance 21% higher with fixed-dose 0.02
Persistence with therapy
54% better with fixed-dose (trend) 0.08
Hypertension. 2010;55:399-407.
New Antihypertensive Drugs:Fixed Dose Combination Products
Two-Drug Combinations ● Telmisartan + Amlodipine
(Twynsta)
● Amlodipine + Valsartan (Exforge)
● Amlodipine + Olmesartan (AZOR)
● Aliskiren + HCTZ (Tekturna HCT)
● Aliskiren + Amlodipine (Tekamlo)
● Aliskiren + Valsartan (Valturna)
● Azilsartan + Chlorthalidone (Edarbychlor)
Three-Drug Combinations● Amlodipine + Valsartan +
HCTZ (Exforge HCT)
● Amlodipine + Olmesartan + HCTZ (Tribenzor)
● Aliskiren + Amlodipine + HCTZ (Amturnide)

19
New Evidenceand
Clinical Controversies
Avoiding Cardiovascular Events in Combination Therapy in Patients Living with Systolic
Hypertension (ACCOMPLISH) trial
● Randomized, double-blind, controlled trial
● 11,506 patients with hypertension and:–Age ≥ 60 years; 55-59 years eligible if ≥ 2 CV
diseases or target organ damage
–SBP ≥ 160 mm Hg or on BP medication
–Evidence of CV disease, kidney disease, or target organ damage
● 1° endpoint: CV morbidity or mortality
N Engl J Med 2008;359:2417-28.

20
ACCOMPLISH Study DesignRandomization
Amlodipine/Benazepril 5/20 mg
Benazepril/HCTZ 20/12.5 mg
Amlodipine/Benazepril 5/40 mg
Benazepril/HCTZ 40/12.5 mg
Amlodipine/Benazepril 10/40 mg
Benazepril/HCTZ 40/25 mg
ForcedTitration
Free add-on other agentsN Engl J Med 2008;359:2417-28.
ACCOMPLISH: Results
● Study terminated early after a mean of 3 years
● BP Lowering:
Benazepril/ Amlodipine
Benazepril/ HCTZ
BP “control”(<140/90 mm Hg)
75.4% 72.4%
Mean BP* (mm Hg)
131.6/73.3 132.5/74.4
N Engl J Med 2008;359:2417-28.40

21
ACCOMPLISH: Primary Endpoint Results
(n=7,640)P=0.004
N Engl J Med 2008;359:2417-28.
(n=11,506)P<0.001
(n=4,560)P=0.002
Polling Question
Is it proven that high adherence with antihypertensive medications reduces risk of CV events compared with low adherence?
Yes
No

22
Adherence and CV Events● 18,806 newly diagnosed hypertensive patients ≥
35 yrs. of age (mean age 62 yrs.)
● Adherence categorized by dispensing count
Circulation. 2009;120:1598-1605.
Adherence and CV Events
● Association with First Acute CV Event
Multivariate analysis adjusted for age, gender, use of antithrombotics, 5 concurrent medications, presence of diabetes mellitus,
dyslipidemia, prior hospitalization, and weighted by the inverse estimated propensity scores. Time-dependent covariates included adherence to AHT, use of combination AHT, antithrombotics, 5 concurrent medications, presence of peripheral vascular diseases, diabetes mellitus, and dyslipidemia.
Circulation. 2009;120:1598-1605.
AdherenceHazard Ratio
(95% CI) P-value
Low 1.00 -
Intermediate0.86
(0.71-1.03)0.11
High0.62
(0.40-0.96)0.03

23
Reflective Question…
How are an ACE inhibitor, ARB, and direct renin
inhibitor (DRI) different from each other?
Vascular Resistance
Renin
Angiotensin II AT1 receptor
Angiotensinogen
Angiotensin I
Aldosterone synthesis
SodiumRetention
Nitric Oxide
Bradykinin
Inactive Products

24
Ongoing Telmisartan Alone and in Combination With Ramipril (ONTARGET)
● 25,620 patients
● Randomized, double-blind trial
● Combination vs. ramipril:– Hypotension:
• 4.8 vs. 1.7% (p<0.001)
– Renal dysfunction:• 13.5 vs. 10.2%
(p<0.001)
P=ns
N Engl J Med. 2008;358:1547-1559.
47
December 20, 2011: Novartis announces termination of the ALTITUDE study
● Study overview:–Patients with type 2 diabetes & renal
impairment randomized, double-blind, to aliskiren or placebo added to standard of care treatment (ACE inhibitor or ARB)
● Trial terminated based on independent data monitoring committee recommendation–Increased incidence of non-fatal stroke, renal
complications, hyperkalemia and hypotension in the aliskiren trial arm after 18-24 months.
www.Novartis.com

25
Polling Question…Which of the following doses of hydrochlorothiazide is the most appropriate to use in patients with hypertension?
12.5 mg daily
25 mg daily
50 mg daily
Antihypertensive Efficacy of Hydrochlorothiazide as Evaluated by
Ambulatory Blood Pressure Monitoring
● Evaluated the antihypertensive efficacy of hydrochlorothiazide (HCTZ) by 24-hour ambulatory BP monitoring (ABPM)
● Meta-analysis of randomized trials
● Trials included:–14 studies of HCTZ 12.5 to 25 mg daily (n=1,234)
–5 studies of HCTZ 50 mg daily (n=229)
J Am Coll Cardiol 2011;57:590–600.

26
Comparative 24-hr ABPM Efficacy
J Am Coll Cardiol 2011;57:590–600.
Compared with HCTZ dose 12.5 to 25 mg, p<0.001 for other antihypertensive drugs
Dose Response with HCTZ
J Am Coll Cardiol 2011;57:590–600.
p<0.0001 for 50 mg versus 12.5 or 25 mg on SBP (p=NS for all other comparisons)
4 Studies(n=129)
9 Studies(n=503)
5 Studies(n=123)

27
Polling Question…
● Hydrochlorothiazide and chlorthalidone are equally effective in the treatment of hypertension.
True
False
A Tale of Two Thiazides
Chlorthalidone Hydrochlorothiazide● Thiazide-like diuretic
● Not frequently used in U.S.
● Used in all the major landmark clinical trials
● 50-60 hr half life
● Undisputed BP lowering efficacy; twice as potent as HCTZ in 24-hr BP lowering
● Preferred over HCTZ in resistant hypertension
● Thiazide-type diuretic
● Frequently used in the U.S.
● Not used in most major landmark clinical trials
● 9-10 hr half life
● Questionable 24-hr BP lowering efficacy with 12.5 to 25 mg
● Easily available in most fixed dose combination products
N Engl J Med 2009;361:2153-64. J Am Coll Cardiol 2011;57:590–600.

28
Chlorthalidone vs. HCTZ: CV Events
● Retrospective observational cohort study from the Multiple Risk Factor Intervention Trial
● 12,866 primary prevention men 35-57 yrs; initial therapy with chlorthalidone (n=2392) or HCTZ (n=4049) started at 50 or 100 mg daily
Hypertension 2011;57:689-694.
CV EventsAdjust HR (95% CI) P-value
Chlorthalidone 0.51 (0.43-0.61) <0.0001
HCTZ 0.64 (0.55-0.75) <0.0001
Chlorthalidone vs. HCTZ 0.79 (0.68-0.92) 0.0016
Resistant Hypertension
● Defined as:– Not at goal BP on 3 or more agents
– Patient requiring 4 or more agents, even if at goal BP
● Treatment Strategies:– Rule out secondary causes and non-adherence
– Assure appropriate diuretic therapy• Preferentially use chlorthalidone instead of
hydrochlorothiazide
• An aldosterone antagonist (e.g., spironolactone) as add-on therapy is highly effective
• Consider a loop diuretic if CrCl < 30 mL/min
– Optimize combinations, prudently use alternate agents
Calhoun DA, et al. Circulation. 2008;117:e510-526

29
Antihypertensive Use in Patients with Resistant Hypertension Prescribed 4 or
More Agents
● 140,126 patients hypertension on ≥4 antihypertensive agents between May 1, 2008 and June 30, 2009
Hypertension. 2011;58:1008-1013
Reflective Question…
Should hypertension be treated differently in very
elderly patients ( 80 years)?

30
Circulation 2011, 123:2434-2506
Principles of Hypertension Treatment•Target SBP ≤140 mm Hg in patients aged 55-79•Target SBP ≤140 mm Hg in patients aged ≥80+•Achieved values <140 mm Hg for those aged ≤79 are appropriate;•But for those aged ≥80, 140 to 145 mm Hg, if tolerated, can be acceptable
Lifestyle Modifications
Not at Target Blood Pressure
Initial Drug Choices
Without Compelling Indication With Compelling Indication
Not at Target Blood Pressure
Optimize dosages or add additional drugs until goal BP is achieved. Refer to a clinical hypertension specialist if unable to achieve control.
Compelling Indication•Heart Failure
•Post myocardial infarction•CAD or High CVD risk
•Angina Pectoris•Aortopathy/Aortic Aneurysm
•Diabetes•Chronic Kidney Disease
•Recurrent Stroke Prevention•Early Dementia
Initial Therapy Options*•Thiaz, BB, ACEI, ARB, CCB,
Aldo Ant.•BB, ACEI, Aldo Ant, ARB
•Thiaz, BB, ACEi, CCB•BB, CCB
•BB, ARB, ACEi, Thiaz, CCB•ACEi, ARB, CCB, Thiaz, BB
•ACEI, ARB•Thiaz, ACEi, ARB, CCB•Blood Pressure control*Combination Therapy

31
Initiation of Antihypertensive Drug Therapy in the Elderly
● Initial drug should be started at the lowest dose and gradually increased, depending on BP response, to the maximum tolerated dose– If BP response is inadequate after reaching “full dose”,
add a second drug from another class
– If response is inadequate after reaching “full doses” of 2 drugs, add a third drug from another class
● When BP is 20/10 mm Hg above goal, therapy should be initiated with 2 drugs. However, treatment must be individualized.– Orthostatic hypotension (SBP decrease of > 20 mm Hg
after 3 minutes of standing) may occurCirculation 2011, 123:2434-2506
Hypertension in the Very Elderly Trial (HYVET)
● 3845 patients age 80 years or older with hypertension
● Randomized, double-blind, to:– Placebo or
– Perindopril +/-Indapamide
● Trial stopped early after 1.8 years
P=0.06 P=0.02
N Engl J Med 2008;358:1887-98.

32
70
80
90
100
110
120
130
140
150
160
170
180
0 1 2 3 4 5
Blo
od P
ress
ure
(m
mH
g)
Follow-up (years)
Placebo
Indapamide SR +/-perindopril
15 mmHg
6 mmHg
N Engl J Med 2008;358:1887-98.
Target BP = 150/80 mm Hg
HYVET – Results
BP goals in Patients ≥ 80yrs
● Data suggest SBP of 150 mm Hg as the diagnostic criterion for hypertension and the treatment target
● When SBP <150 mm Hg is readily and safely obtained with 1 or 2 drugs, further treatment intensification to <140 mm Hg could be considered
● The lowest safely achieved SBP ≥150 mm Hg is acceptable for patients under 3 circumstances:1) despite taking a regimen of 4 well-selected and appropriately
dosed drugs, goal has not been achieved;
2) prescribed therapy is causing unacceptable side effects
3) in attempting to reach the SBP target, the DBP is being reduced to a potentially dangerous level <65 mm Hg
Circulation 2011, 123:2434-2506

33
BP and outcomes in very old hypertensive CAD patients: an INVEST substudy
(Am J Med. 2010;123:719 –26)
Circulation 2011, 123:2434-2506
Renal Disease and Hypertension
Stage 5CKD
Stage 4 CKDHypertensive
Nephrosclerosis
DiabeticNephropathy
Stage 3 CKD
Micro-albuminuria
Proteinuria(>1 gm/d)

34
Effect of Inhibitors of the Renin-Angiotensin System and Other Antihypertensive Drugs
on Renal Outcomes
Systematic review and meta-analysis
● ACEi or ARB vs. other antihypertensive drugs – Doubling serum creat. RR = 0·71 (0·49–1·04)
– ESRD RR = 0·87 (0·75–0·99)
● Placebo-controlled trials of ACEi or ARBs showed greater benefits than comparative trials, but were accompanied by BP reductions
Lancet 2005; 366: 2026–33
Effect of Combination ACEi and ARB for Proteinuria in CKD
● 49 studies including 6181 patients
● The combination of ARB with ACEi further reduced proteinuria more than either alone:–Ratio of means (95% CI) over 5 to 12 months:
• ACEi + ARB vs. ARB 0.75 (0.61 to 0.92)
• ACEi + ARB vs. ACEi 0.82 (0.67 to 1.01)
Ann Intern Med. 2008;148:30-48.

35
ACCOMPLISH: Renal Outcomes
● Pre-specified secondary analysis– CKD progression defined as doubling of serum
creatinine or end-stage renal• Benazepril/amlodipine 113 (2·0%)
• Benazepril/HCTZ 215 (3·7%) p<0·0001
● 1093 patients had CKD at baseline:– CV and total mortality higher than in non-CKD
– About half had diabetes; did not influence results
– CKD progression slower in benazepril/amlodipine than benazepril/HCTZ (p=0.001)
Lancet 2010; 375: 1173–81
The Eighth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 8)
● Staring with evidence models and a set of prioritized critical questions important for clinical practice
● Critical questions are being answered by conducting systematic reviews of the scientific evidence using a rigorous and standardized approached
Status Report on the NHLBI-Sponsored CVD Prevention Guidelines presented in
November 2011 at the AHA Meeting
http://www.nhlbi.nih.gov/guidelines/cvd_adult/background.htm

36
Evidence-Based Clinical Practice Guidelines for CVD PreventionEvidence-Based Clinical Practice Guidelines for CVD Prevention
How the Process Has Evolved
Strictly evidence-based
Focus only on randomized controlled trials assessing important health outcomes (no use of intermediate/surrogate measures)
Every included study is rated for quality by two independent reviewers using standardized tools
Evidence statements graded for quality using prespecified criteria
Separate grading for recommendations
Independent methodology team to ensure objectivity of the review
Initial set of recommendations focused on 3 key questions
71
Evidence-Based Clinical Practice Guidelines for CVD PreventionEvidence-Based Clinical Practice Guidelines for CVD Prevention
Rationale for the Questions
Interest in assessing the evidence to support 140/90 mm Hg as a treatment threshold or goal
Should the treatment threshold / goal be lower in populations with diabetes, chronic kidney disease, coronary artery disease, stroke, and other co-morbidities or characteristics?
Should the treatment threshold / goal be different in older adults?
Use of different treatment thresholds and goals is confusing
Is there evidence that treatment to lower BP with a particular drug or drug class improves outcomes compared to another?
72

37
Evidence-Based Clinical Practice Guidelines for CVD PreventionEvidence-Based Clinical Practice Guidelines for CVD Prevention
Question 1
Among adults with hypertension, does initiating antihypertensive pharmacological therapy at specific BP thresholds improve health outcomes?− When to initiate drug treatment?
73
Evidence-Based Clinical Practice Guidelines for CVD PreventionEvidence-Based Clinical Practice Guidelines for CVD Prevention
Question 2
Among adults, does treatment with antihypertensive pharmacological therapy to a specified BP goal lead to improvements in health outcomes?− How low should you go?
74

38
Evidence-Based Clinical Practice Guidelines for CVD PreventionEvidence-Based Clinical Practice Guidelines for CVD Prevention
Question 3
In adults with hypertension, do various antihypertensive drugs or drug classes differ in comparative benefits and harms on specific health outcomes? − How do you get there?
75
Evidence-Based Clinical Practice Guidelines for CVD PreventionEvidence-Based Clinical Practice Guidelines for CVD Prevention
Inclusion/Exclusion Criteria
Randomized Controlled Trials
RCTs are subject to less bias and represent the gold standard for determining efficacy and effectiveness1
Search dates: 1966 to present
Minimum one-year follow-up period
Studies with sample sizes less than 100 excluded
1 Institute of Medicine. 2011. Finding What Works In Health Care. Standards For Systematic Reviews. Washington, DC: The National Academies Press.
76

39
Evidence-Based Clinical Practice Guidelines for CVD PreventionEvidence-Based Clinical Practice Guidelines for CVD Prevention
Populations Included
77
Evidence-Based Clinical Practice Guidelines for CVD Prevention
Articles Screened = 2662
Good = 15
Included = 101
Total Abstracted = 66
Excluded = 2561
(Did not meet prespecified
inclusion criteria)Poor = 35Fair = 51
Question 3: In adults with hypertension, do various antihypertensive drugs or drug classes differ in comparative
benefits and harms on specific health outcomes?
78

40
Evidence-Based Clinical Practice Guidelines for CVD PreventionEvidence-Based Clinical Practice Guidelines for CVD Prevention
Next Steps
Evidence statements and recommendations (in progress)
Draft report (in progress)
Review of the draft report by:
Other federal agencies (CDC, CMS, AHRQ, HRSA, VA, etc.)
Invited organizations and individuals
Public
Revisions based on comments received
Final report
79
Predictions for the JNC 8
● Role of beta-blockers will be second-line or for patients with a compelling indication
● Goal SBP of <140 mm Hg for all, with lower goal on an individual basis
● Address HCTZ vs. chlorthalidone
● ACEI or ARB with CCB might be the preferred first-combination therapy
● Tailored recommendations for the “Very Elderly”

41
Pirates of the Caribbean: The Curse of the Black Pearl
● Philosophy of Guidelines
the code is more what you'd call "guidelines" than actual rules
http://www.imdb.com/title/tt0325980/quotes
Conclusions