b urn rahayu setyowati
TRANSCRIPT

BURN
RAHAYU SETYOWATI
http://rsetyowati31.wordpress.com

LEARNING OBJECTIVES
Describe the cause of burn injuries Describe the burn injury classification system Describe pathophysiology, clinical
manifestations, nursing and collaborative management of the three burn phases
Explain depth and TBSA in the burn case Explain nursing intervention in the emergent
phases

SKIN
SKIN Largest body organ. Much more than a
passive organ.Protects underlying tissues from injuryTemperature regulationActs as water tight seal, keeping body
fluids inSensory organcosmetic

Injuries to skin which result in loss, have problems with: Infection Inability to maintain normal water balance Inability to maintain body temperature
Epidermis Outer cells are dead Act as protection and form water tight seal
Dermis - Specialized Structures Nerve endings Blood vessels Sweat glands Oil glands - keep skin waterproof, usually
discharges around hair shafts Hair follicles - produce hair from hair root or
papilla

TYPES OF BURN INJURIES
Thermal burnSkin injury Inhalation injury
Chemical burnSkin injury Inhalation injuryMucous membrane injury
Electrical burnLightning
Radiation burn
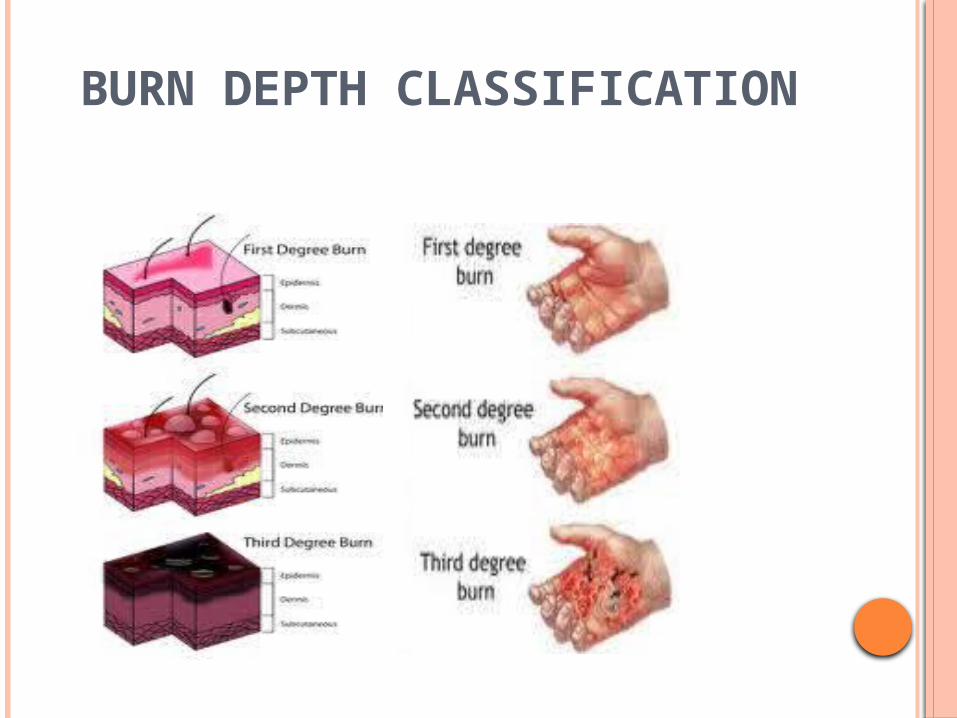
BURN DEPTH CLASSIFICATION

SUPERFICIAL (PRIMARY) BURN
1st degree (Superficial burn) Involves the epidermisCharacterized by reddeningTenderness and Pain Increased warmthEdema may occur, but no blisteringBurn blanches under pressureExample - sunburnUsually heal in ~ 7 days


PARTIAL THICKNESS (SECONDARY) BURN
2nd degreeDamage extends through the epidermis
and involves the dermis.Not enough to interfere with regeneration
of the epitheliumMoist, shiny appearanceSalmon pink to red colorPainfulhave to blister to be 2nd degreeUsually heal in ~7-21 days


FULL THICKNESS (TERTIARY) BURN
3rd degreeBoth epidermis and dermis are destroyed
with burning into SQ fatThick, dry appearancePearly gray or charred black colorPainless - nerve endings are destroyedPain is due to intermixing of 2nd degreeMay be minor bleedingCannot heal and require grafting


BODY SURFACE AREA
Rule of nine


INFANT

CHILD

Lund-Browder chart


FACTORS TO DETERMINE THE SERIOUSNESS OF BURN
The depth The extent to the affected body surface area Location of the burn
burn on the face, hands, feet, and genital are more severe than on other body parts.
Victim’s age and medical conditionpre-existing medical problem, elderly (over 55 yr) or very young (under 5 yr)

SYSTEMIC RESPON
Cardiovascular response- cardiac output decreases- vascular volume decreases
burn shock
- increase in pulse rate and BP low- first 24 – 36 hours after the burn, peaking by 6-8 hours

Effects of fluids, elektrolytes, and blood volume- during burn shock : hyponatremia- immediately after burn injury : hyperkalemia (massive cell destruction)- after fluids shifts : hypokalemia (inadequate potassium replacement)
Pulmonary response- hypoxia- upper airway injury edema obstruction- atelectasis (collapse of alveoli)
Urinary System hypovolemia blood flow ischemiadestruction of red blood cell hematuria anemia

Immunologic systemhigh risk for infection and sepsis
o Theroregulatory hypotermic
o Gastrointestinal system- paralitic ileus - gastric or duodenal erosion (curling’s ulcer)

EMERGENT / RESUSCITATIVE PHASE OF BURN CARE
First Aid: COOL, COVER & CALL
Immediate care of a burn injury should always include:
Cooling all burns with tepid to cool water, regardless of degree. Continue flushing the area for up to 10 minutes. Do not apply ice, ointments, butter or other “home remedies”. Remove all clothing or garments to reduce the contact time with hot items.
Cover affected areas with a clean dry cloth, towel or blanket to protect the burn and minimize pain.
Seek medical attention if burn is larger than the victim’s hand size, if the victim is a child or elderly person.

BASIC CARE
1. Stop the Burning Process (Thermal Burn):Remove clothing and jewelry. Flush all burns with water, NOT ice for approximately 10 minutes. Cover burns with a clean, dry sheet. Keep blisters intact. Do not apply dressings.
2. Chemical Burns: irrigate profusely with running water for 20 minutes. Brush away dry powders first. Cover whith dry dressing. If it in the eye, flood it for ±20 minutes using low pressure. Monitor for hypothermia while irrigating. Transport victim’s clothing for analysis.

3. Electrical Burns- unplug, disconnect, or turn off the power or call the power company- check ABC or CPR if necessary- if the victim fell, check for spinal
injury- treat the victim for shock- seek medical attention immediately

4. ABCDE’s of Care
Assess the airway, respiratory rate and rhythm. Note chest wall expansion, especially if full thickness burns are circumferential to the trunk. Administer 100% (humidified) oxygen by non-rebreather mask.
For a compromised airway:- consider Chin Lift - Jaw Thrust - Oral Pharyngeal Airway (for the unconscious patient)
Assess circulation, blood pressure, pulse rate and skin color. Fluid shifting in burn patients’ causes edema and volume loss. Elevate extremities.

Burn patients should be initially alert and oriented. If not, consider trauma or other associated injuries. Determine level of consciousness by AVPU method; Alert, Verbal/Painful stimuli, Unresponsive
Obtain a complete history of the events, time, open or enclosed space, last meal, medications, allergies, past medical history and any other pertinent data.

Conduct a thorough head-to-toe examination of the patient, noting any deformities, irregularities, as well as calculating out the total burn surface area (Refer to Rule of 9’s Chart)
If the patient requires advance burn care, contact paramedics or transport to the nearest medical facility.

ADVANCED CARE
Airway Management:Administer 100% (humidified) oxygen by non-rebreather mask. Symptoms of smoke inhalation may have a delayed onset. If there is any suspicion or history of airway injury, check arterial blood gases and carboxyhemoglobin level. Consider endotracheal intubation. (Nasotracheal intubation is preferred.) Be sure the ET tube is secure and in good position.

Intravenous Fluid Resuscitation:- Infuse Lactated Ringer’s solution
@Parkland (Baxter) 4 ml RL x Kg x %TBSA (total fluid requirements for first 24hr after burn). @Brooke 1.5 ml RL/kg/%TBSA + 0.5 ml colloid/kg/%TBSA + 2000 ml D5W@Brooke (modified) 2 ml RL x Kg x %TBSA
- Application : - ½ of total in first 8 hrs- ½ of total in second 16 hrs
- Maintain urine output 0,5 - 1 ml/kg/hrs (30 to 50 ml/hrs)
- Monitor Hematocrit, hemoglobin and serum sodium level
- Insert Foley Catheter.

example :
for a 70 kg patient with a 50% TBSA burn :
4 ml x 70 kg x 50% TBSA burn = 14.000 ml = 14 L per 24hr
½ of total in first 8 hrs = 7000 ml = 875 ml/h
½ of total in second 16 hrs = 7000 ml
= 437 ml/h
- colloid may be given in the third or fourth 8-hour period after the burn
- for the client extensive burns CVP.
- in the second 24-hour period, 5% dextrose replace RL as the crystalloid solution of choice.

Nutritional Therapy
Emergent no food or fluid by mount, prevent aspiration of vomitus.
Large burn paralytic ileus gastric tube
(to low intermitten suction)
bowel sound (+) after 48 – 72
hours oral intake (liquid)
hypermetabolic high calories and protein
Drug Therapy :
- analgesia; I.V. Morphine Sulphate (1mg/10Kg).
- Infection prophylaxis: tetanus immunization.
- Antibiotics (sulvadiazin, sulfamylon, bacitracin, mupirocin).

NURSING PROCESSBURN CARE DURING THE EMERGENT / RESUSCITATIVE
PHASE
Assessment- data by prehospital providers- vital signs are checked frequently- cardiac monitoring (cardiac diseases, respiratory problem, electrical injury)- monitor urine output hourly- high voltage electrical injury : suspect myglobinuria or hemoglobinuria- head to toe assessment- neurologic assessment- monitor distal circulation

Nursing Diagnoses and Intervention Impaired gas exchange related to carbon
monoxide poisoning and upper airway obstruction Inneffective airway clereance releated to edema
Intervention :
- O2
- monitor respiratory (rate, depth, quality)
- auscultation lungs sound
- monitor ABG
- incentive spirometry
- encouraging coughing and deep breathing
- suctioning if need
- positioning

Fluid volume deficit releated to increased capillary permeability and evaporative fluid loss from the burn wound- assess vital sign every 1-2 hrs - monitor urinary output- give fluids according to patient needs- monitor lab test (Na & K)
Hypotermia releated to loss of skin and open wound- keep patient warm- cover with dry and cotton blankets
Pain releated to tissue and nerve injury - i.v morphine or other opioid analgesic- administer medication for pain 30 min before interventions

Imbalanced nutrition : less than body requirements releated to increases calori demand- maintain patient NPO with NG tube to low intermitten suction- assess return of bowel sounds- institute progressive diet - chart calori diet
Risk for infection releated to impaired skin integrity- use good hand washing technique- use sterile technique - applay sterile dessing - give tetanus - observe wound daily - monitor vital sign and temperature- give antibiotic

REFERENCES
1. Smeltzer & Bare. 2010. Texbook of Medical Surgical Nursing. Twelfth edition. USA : Wolters Kluwer.
2. Oman,Kathleen S. 2007. Emergency Nursing Secrets. Second Edition. USA : Mosby.
3. John MA. 2004. Emergency Medicine. USA : McGraw-Hill.-
4. Heitkemper, Lewis. 2004. Medical Surgical Nursing. USA : Mosby.
5. www.nygsh.org/medicalemergencyteam1met1
LETS EXERCISE ……….. berat badan 50 kg, dibawa ke IGD karena
mengalami kebakaran pada bagian leher depan, dada, abdomen, daerah genitalia, keseluruhan tangan kanan dan keseluruhan kaki kanan.
Hitung kebutuhan cecair 24 jam pertama(8 jam pertama dan 16 jam berikutnya).

LETS EXERCISE ……….. berat badan 40 kg, dibawa ke ugd karena
mengalami kebakaran pada kaki kanan keseluruhan bagian depan , kaki kiri bawah bagian depan.
Hitung kebutuhan cairan 24 jam pertama(8 jam pertama dan 16 jam berikutnya).