axial changes ankylosing spondylitis - fhs. · pdf filemicrosoft powerpoint - axial changes...
TRANSCRIPT

Radiology RoundsRadiology RoundsSt. Joseph HospitalSt. Joseph Hospital
By:By:
Cyrus SalimiCyrus SalimiRheumatology FellowRheumatology Fellow
McMaster UniversityMcMaster University
Ankylosing SpondylitisAnkylosing SpondylitisAxial manifestationsAxial manifestations

Briefly about A.SBriefly about A.SSeronegative Seronegative arthropathy of arthropathy of unknown originunknown originYoung adultsYoung adultsMore severe in More severe in malesmales0.10.1--1% prevalence1% prevalenceCentral Europe Central Europe highest prevalence highest prevalence 90% HLA B2790% HLA B27


Insidious onset of low back pain Insidious onset of low back pain Early 3Early 3rdrd decade of lifedecade of lifeSacroiliitis: Sacroiliitis:
commonly seen at presentationcommonly seen at presentationBilateral symmetricBilateral symmetric
Chiefly disease of axial skeletonChiefly disease of axial skeleton

Characteristic radiographic Characteristic radiographic changes in changes in ankylosingankylosing spodylitisspodylitis
Seen first in axial skeletonSeen first in axial skeletonMore prominent in:More prominent in:
sacrosacro--iliac and iliac and discodisco--vertebral vertebral apophysealapophyseal joints joints
CostoCosto--vertebral and vertebral and costocosto--transverse transverse joints as welljoints as wellChange evolves slowly over many Change evolves slowly over many yearsyears

Time from first Time from first symptom to first symptom to first radiographic findingsradiographic findings
??

Time from first symptoms to Time from first symptoms to observing plain Xobserving plain X--ray findingsray findings
9 years9 years
Earliest radiographic findings Earliest radiographic findings SI SI jointjoint

Radiographic studiesRadiographic studies
No radiographic method ideal b/o No radiographic method ideal b/o complex individual variations of SI complex individual variations of SI jointjointInterpreteationInterpreteation of early of early sacroilitissacroilitisdifficult b/o:difficult b/o:
PresencsePresencse of of degenarativedegenarative changeschangesNot appropriate viewNot appropriate view
•• Best view with plain xBest view with plain x--rayray FergusonFerguson’’s views view(AP view, pelvis, aimed at 30(AP view, pelvis, aimed at 30°° cephaladcephalad))

XX--Ray findingsRay findingsMineralization:Mineralization:
Normal before ankylosisNormal before ankylosisGeneralized osteoporosis after ankylosisGeneralized osteoporosis after ankylosis
Subchondral bone formationSubchondral bone formationPresent before ankylosisPresent before ankylosis

SI joint xSI joint x--ray findings …ray findings …ErosionsErosions
Progressive Progressive subchondralsubchondral bone erosions bone erosions
pseudowideningpseudowideningSmall and localizedSmall and localizedNot very prominent Not very prominent
Pattern: Pattern: bilateral and symmetricbilateral and symmetricFirst on the iliac sideFirst on the iliac sideThen on sacral sideThen on sacral side
•• Appearance of Appearance of edge of postage stampedge of postage stamp•• Erosions surrounded by “bone repair” Erosions surrounded by “bone repair” sclerosissclerosis
First seen in lower 3First seen in lower 3rd (Synovial part)rd (Synovial part)

Axial XAxial X--Ray findings …Ray findings …
AnkylosisAnkylosisDistributions:Distributions:
First First SI joint and lumbarSI joint and lumbarAscending from lumbar to cervicalAscending from lumbar to cervicalInvolvement of Involvement of costovertebralcostovertebral JointsJoints
Absence of Absence of subluxationssubluxationsAbsences of cystsAbsences of cysts


Ankylosing Spondylitis: early sacroiliitisAnkylosing Spondylitis: early sacroiliitis

Ankylosing Ankylosing spondylitisspondylitis: advanced sacroiliitis : advanced sacroiliitis


The SpineThe SpineInitially Initially T12T12--L1 areaL1 areaProgresses upward Progresses upward thoracic thoracic cervicalcervicalFirst finding:First finding:
•• ErosionsErosions of the of the cornerscornersSecondary reactive sclerosis Secondary reactive sclerosis ““ivoryivory”” cornerscornersSquared appearanceSquared appearance
Second finding: Second finding: •• OssificationOssification; first outer portion; ; first outer portion; anulusanulus fibrosusfibrosus
Causing lack of motion in flexion and extension Causing lack of motion in flexion and extension filmsfilms
•• Later: extension into deep layers of longitudinal Later: extension into deep layers of longitudinal ligamentsligaments
Syndesmophyte formationSyndesmophyte formation
Disc space:Disc space:Preserved before ankylosisPreserved before ankylosisCalcification possible after ankylosisCalcification possible after ankylosis
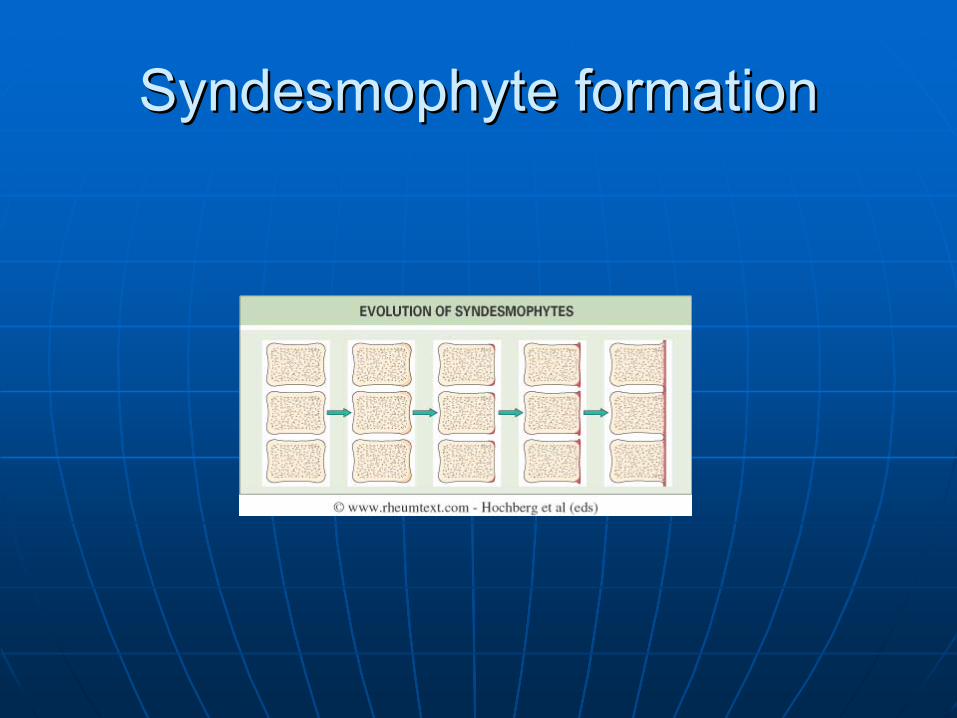
Syndesmophyte formationSyndesmophyte formation

Microscopic view of Microscopic view of syndesmophytesyndesmophyte

Ankylosing Ankylosing spondylitisspondylitis: thoracic and lumbar vertebrae "squaring," : thoracic and lumbar vertebrae "squaring," osteopeniaosteopenia, and ossification, and ossification

Ankylosing Ankylosing spondylitisspondylitis: lumbar vertebrae, bamboo spine : lumbar vertebrae, bamboo spine


ApophysealApophyseal jointsjoints
May or may not be involvedMay or may not be involvedOssification of ligaments of Ossification of ligaments of spinousspinousprocesses possibleprocesses possibleBamboo spineBamboo spine•• Misdiagnosed complication: Misdiagnosed complication:
•• PseudarthrosisPseudarthrosis lower lower thoracisthoracis--upper lumbarupper lumbarAround the area of true fracture Around the area of true fracture ororArea of skipped ossificationArea of skipped ossificationSingle point of motion in the spineSingle point of motion in the spineCan undergo degenerative changesCan undergo degenerative changes
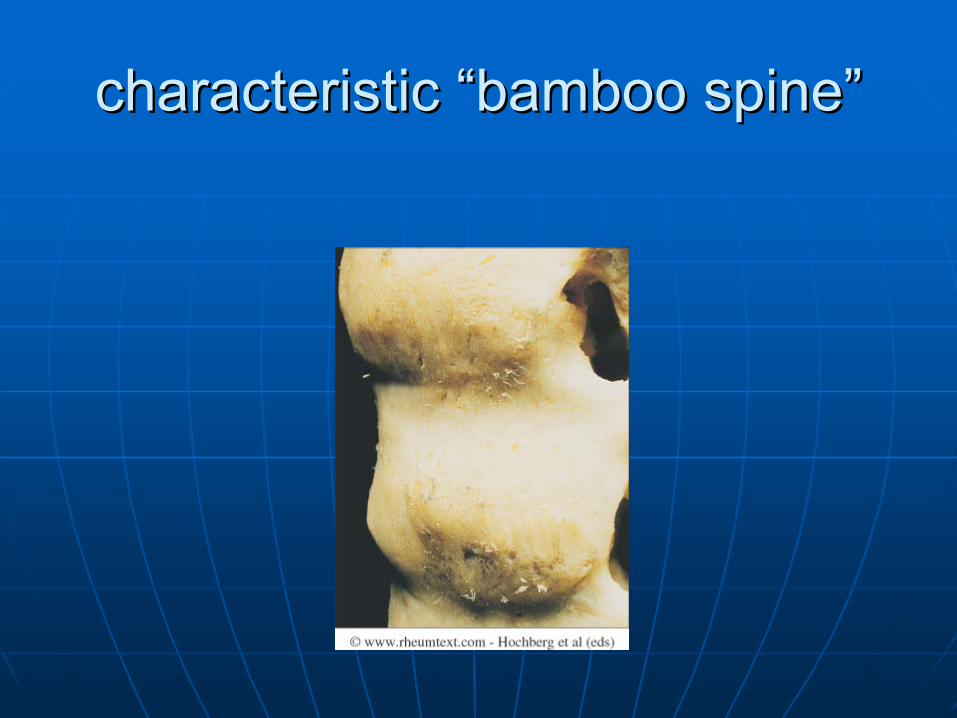
characteristic “bamboo spine”characteristic “bamboo spine”

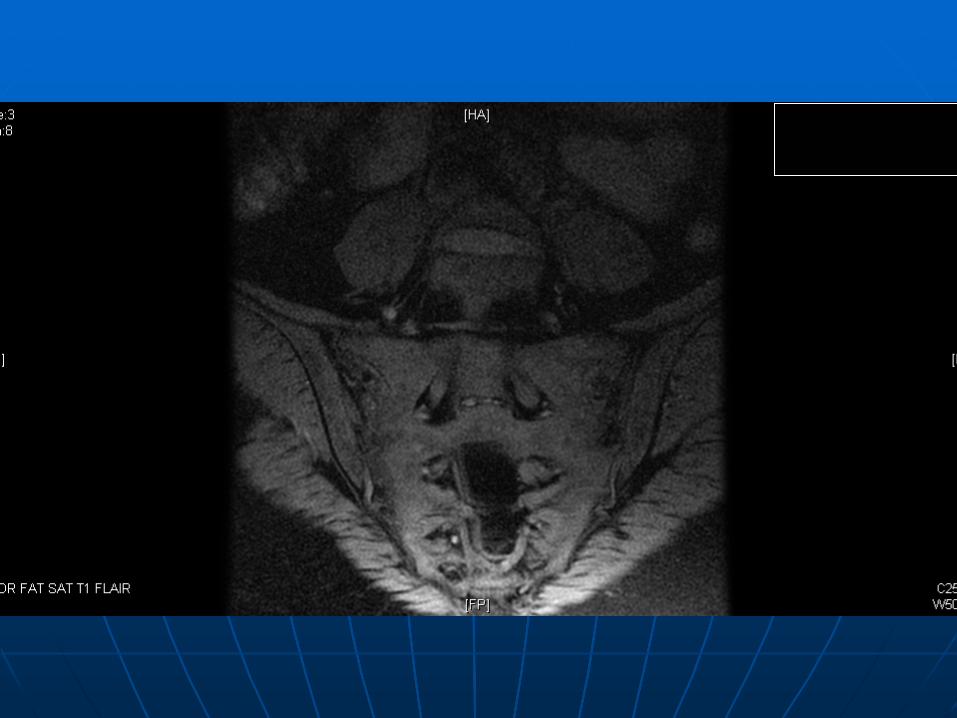
Coronal cut Coronal cut



MRI finding MRI finding
subchondralsubchondral edemaedemaBone Marrow edemaBone Marrow edema

Early detection of Early detection of sacroilitissacroilitis on MRIon MRIObjectivesObjectives
To To investgateinvestgate the diagnostic value of MRI in the detection of early the diagnostic value of MRI in the detection of early sacroiliitissacroiliitis
MethodsMethods•• Prospective longitudinal studyProspective longitudinal study
25 consecutive HLA25 consecutive HLA--B27 positive patientsB27 positive patientsInflammatory low back painInflammatory low back pain<grade 2 unilateral sacroiliitis with conventional radiography<grade 2 unilateral sacroiliitis with conventional radiographyESR and CRP followed for 3 yearsESR and CRP followed for 3 yearsClinical assessment at entry and after 3 yearsClinical assessment at entry and after 3 yearsPR and MRI of SI joint at entry and after 3 yearsPR and MRI of SI joint at entry and after 3 yearsPR and PR and MRIsMRIs interpreted independently and randomly by 2 blind interpreted independently and randomly by 2 blind investigatorsinvestigatorsThe MRI images were interpreted for BM edema as wellThe MRI images were interpreted for BM edema as well
J Rheumatol 1999; 26: 1953-8

SI joint scoring: (modified New York Criteria)SI joint scoring: (modified New York Criteria)
G1: suspiciousG1: suspiciousG2: minimal abnormality with small erosionsG2: minimal abnormality with small erosionsG3: definitive abnormality (erosion and sclerosis)G3: definitive abnormality (erosion and sclerosis)G4: total ankylosisG4: total ankylosis

Odds ratio with 95% CI used to examine relationship Odds ratio with 95% CI used to examine relationship between:between:
Inflammation (CRP>10, ESR>15, SI tenderness) and BM Inflammation (CRP>10, ESR>15, SI tenderness) and BM edemaedemaSigns of inflammation and >G2 sacroiliitis with MRISigns of inflammation and >G2 sacroiliitis with MRIPresence of BM edema on MRI and >G2 sacroiliitis on MRI Presence of BM edema on MRI and >G2 sacroiliitis on MRI at entryat entryPresence of edema on MRI at entry and >G2 sacroiliitis on Presence of edema on MRI at entry and >G2 sacroiliitis on PR after 3 yearsPR after 3 yearsPresence of >G2 sacroiliitis on MRI at entry and >G3 Presence of >G2 sacroiliitis on MRI at entry and >G3 sacroiliitis on PR after 3 yearssacroiliitis on PR after 3 years

Patient's dataPatient's data::Median age 36 Median age 36 Median duration of ILBP 4 yearsMedian duration of ILBP 4 years24 used NSAIDS24 used NSAIDS23 with alternating R and L buttock pain23 with alternating R and L buttock pain2 had uveitis9 with positive FH of AS2 had uveitis9 with positive FH of ASNo reactive A. IBD, psoriasis No reactive A. IBD, psoriasis hxhxAt entry clinical findings and MRI suggested At entry clinical findings and MRI suggested definitive AS in 16 patients, PR in 2 patientsdefinitive AS in 16 patients, PR in 2 patientsSt entry 20 patients found to have St entry 20 patients found to have subchondral edemasubchondral edema2 lost to F/U2 lost to F/U

Relationship between signs of inflammation and BM edema Relationship between signs of inflammation and BM edema on MRI at study entryon MRI at study entry
0.060.06--0.920.920.230.23SI tenderness SI tenderness
0.360.36--12.3212.322.092.09ESR>15ESR>15
0.30.3--10.9410.942.082.08CRP>10CRP>10
95% CI95% CIOdds RatioOdds Ratio

Relationship between signs of inflammation and >G2 Relationship between signs of inflammation and >G2 sacroiliitis on MRI at study entrysacroiliitis on MRI at study entry
0.300.30--4.794.791.21.2SI tendernessSI tenderness
0.480.48--48.4648.464.84.8ESR>15ESR>15
0.780.78--79.6679.6688CRP>10CRP>10
95% CI95% CIOdds RatioOdds Ratio

Relationship between presence of BM edema on MRI at Relationship between presence of BM edema on MRI at study entry and presence of >G2 sacroiliitis on MRI at entry study entry and presence of >G2 sacroiliitis on MRI at entry
and presence of >G2 sacroiliitis on PR after 3 yearsand presence of >G2 sacroiliitis on PR after 3 years
0.720.72--10.0510.052.72.7>G2 >G2 SiSi--tistis on on PR after 3 yrsPR after 3 yrs
1.171.17--30.7230.7266>G2 >G2 SiSi--tistis on on MRI at entryMRI at entry
95% CI95% CIOROR
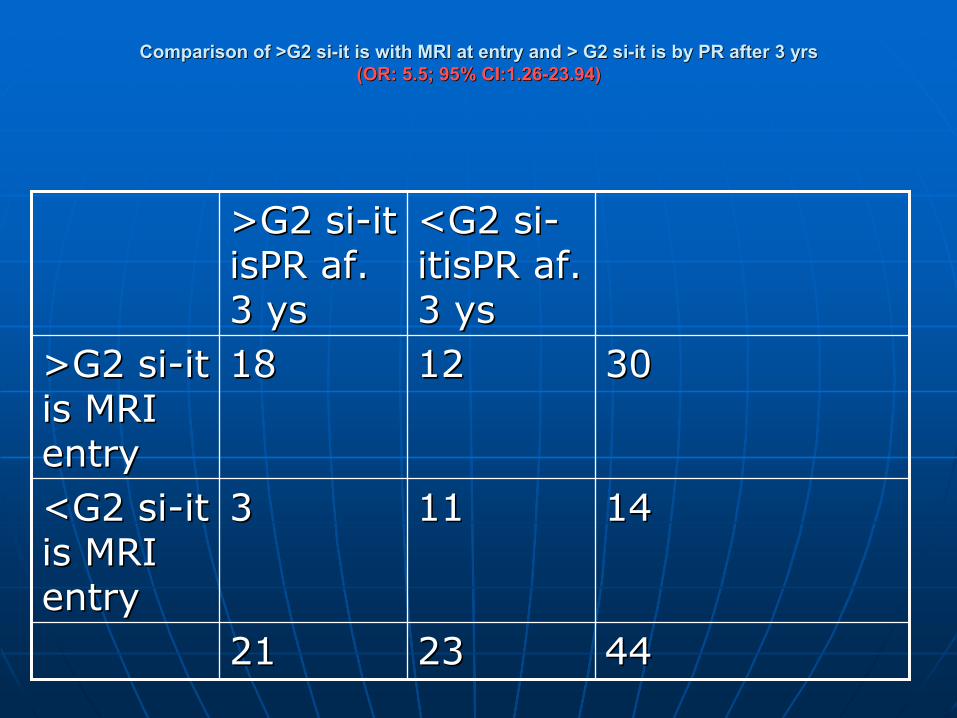
Comparison of >G2 Comparison of >G2 sisi--it is with MRI at entry and > G2 it is with MRI at entry and > G2 sisi--it is by PR after 3 yrsit is by PR after 3 yrs(OR: 5.5; 95% CI:1.26(OR: 5.5; 95% CI:1.26--23.94)23.94)
444423232121
1414111133<G2 <G2 sisi--it it is MRI is MRI entryentry
303012121818>G2 >G2 sisi--it it is MRIis MRIentryentry
<G2 <G2 sisi--itisPRitisPR afaf. . 3 3 ysys
>G2 >G2 sisi--it it isPRisPR afaf. . 3 3 ysys

ResultResultAt study entryAt study entry::
•• MRI detected >G2 MRI detected >G2 sisi--itisitis of 36 out of 50 SI of 36 out of 50 SI joints without any PR evidence of joints without any PR evidence of sisi--it isit is
•• MRI + clinical findingsMRI + clinical findings suggested suggested definitive definitive DxDx of As in 16 patientsof As in 16 patients
•• PR detected 2 cases of unilateral >G3 PR detected 2 cases of unilateral >G3 sisi--it isit is
After 3 yrsAfter 3 yrs::•• Definitive Definitive DxDx of AS made in remaining 10/22 of AS made in remaining 10/22
ptspts•• 8 of these 8 of these had had bilbil. . SiSi--iltisiltis >G2 on MRI at >G2 on MRI at
entryentry

Conclusion Conclusion
MRIMRI can reveal definitive evidence of can reveal definitive evidence of sacroiliitis in HLAsacroiliitis in HLA--B27 + patientsB27 + patientswith ILBP at anwith ILBP at an earlier stageearlier stagecompared to plain Xcompared to plain X--ray.ray.

Advantages:Advantages:•• Prevention of progression of disease at early Prevention of progression of disease at early
stagesstages
Disadvantage:Disadvantage:•• Very expensiveVery expensive

MRI of normal SI jointMRI of normal SI joint

Abnormal SI joint Abnormal SI joint By MRI (sacroiliitis) By MRI (sacroiliitis)




Clinical radiology 2004;59,400-413


Clinical radiology 2004;59,400-413

Clinical radiology 2004;59,400-413

Clinical radiology 2004;59,400-413

Clinical radiology 2004;59,400-413


Ankylosing Ankylosing spondylitisspondylitis: : thoracolumbarthoracolumbar spine, spine, pseudarthrosispseudarthrosis (CT scan(CT scan))

Differential DiagnosisDifferential Diagnosis
DISHDISHOsteitisOsteitis CondencenceCondencenceReactive arthritisReactive arthritisSAPHOSAPHOPsoriatic spondyloarthropathyPsoriatic spondyloarthropathyIBD arthropathy IBD arthropathy

Do the radiological changes of classic Do the radiological changes of classic ankylosingankylosingspondylitisspondylitis differ from the changes found in the differ from the changes found in the spondylitisspondylitis associated with inflammatory bowel associated with inflammatory bowel
disease, psoriasis, and reactive arthritis?disease, psoriasis, and reactive arthritis?
Ann Rheum Dis 1998;57:135-140






Reactive arthritis: sacroiliitis Reactive arthritis: sacroiliitis

OsteitisOsteitis condensanscondensans iliiilii: pelvis : pelvis

Diffuse idiopathic skeletal hyperostosisDiffuse idiopathic skeletal hyperostosis

SAPHOSAPHO
Skeletal Radiology (2003), 32Skeletal Radiology (2003), 32

SAPHO
MRI

ConclusionConclusion
The role of MRI in imaging of AS has The role of MRI in imaging of AS has greatly expandedgreatly expandedWith MRI the disease can be With MRI the disease can be detected much earlier detected much earlier early early treatment treatment early prevention of early prevention of disabilitydisabilityWhen high suspicion When high suspicion do not delay do not delay MRI imagingMRI imaging