avoiding and managing femoral access site complications · avoiding and managing femoral access...
TRANSCRIPT

Avoiding and Managing FemoralAvoiding and Managing FemoralAccess Site ComplicationsAccess Site ComplicationsAccess Site ComplicationsAccess Site Complications
Curtiss T. Stinis, M.D., F.A.C.C., F.S.C.A.I.Director, Peripheral InterventionsDirector, Peripheral Interventions
Program Director, Interventional Cardiology Fellowship
Division of Cardiology
Scripps Clinic
La Jolla, CALa Jolla, CA
SCRIPPS CLINIC

Radial Access: A Game Changer
Radial Myth vs. Radial Reality
• Radial catheterization is an important innovation incardiology and works very well for the right patientand the right anatomical situationand the right anatomical situation
• Skilled operators can probably perform around 80%of cases from the radial approach…. but what aboutthe other 20%?the other 20%? Peripheral interventions?
Impella, ECMO?
Complex cases?
TAVR?
Aberrant radial anatomy/tortuosity/spasm? Aberrant radial anatomy/tortuosity/spasm?
• Learning and maintaining proper femoral access andmanagement skills is still of critical importance!
How do we teachHow do we teachnew fellows to benew fellows to benew fellows to benew fellows to be
proficient at femoralproficient at femoralaccess when we doaccess when we do
so many radialso many radialso many radialso many radialcases now??cases now??

Femoral Access: Considerations
• Many femoral access site complicationscan be avoided by proper accesstechniquetechnique
• Always presume that the access site willbe managed by manual compressionbe managed by manual compressionalone
• DO NOT assume a closure device can/will• DO NOT assume a closure device can/willbe used and will always work
• Goal is to obtain access in a compressible• Goal is to obtain access in a compressiblesite to maximize chances of success of amanual holdmanual hold

Anatomy of the Femoral Region
External IliacDeep Circumflex Iliac
Inferior Epigastric
Common Femoral
Inguinal Ligament
Profunda Femoris
Superficial Femoral

Anatomy of the Femoral Region
Origin of IEA
Inferior border of IEA
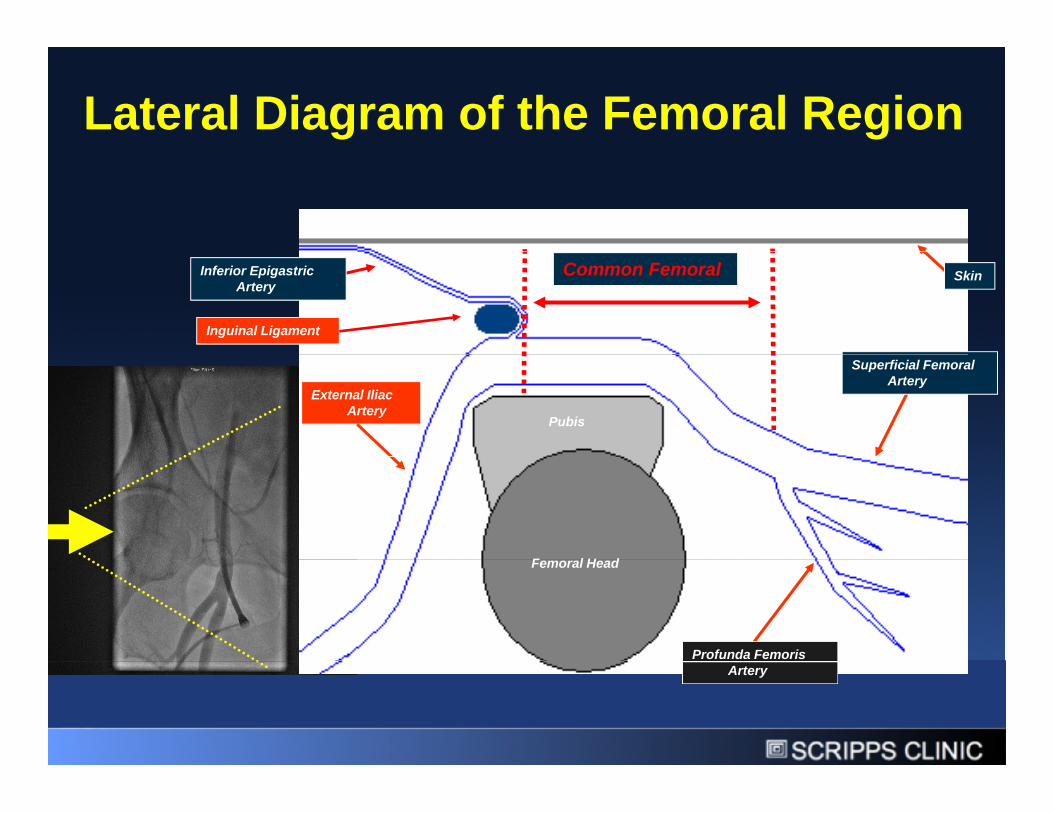
Lateral Diagram of the Femoral Region
Inguinal Ligament
Common Femoral SkinInferior EpigastricArtery
Pubis
External IliacArtery
Superficial FemoralArtery
Femoral HeadFemoral Head
Profunda FemorisArtery
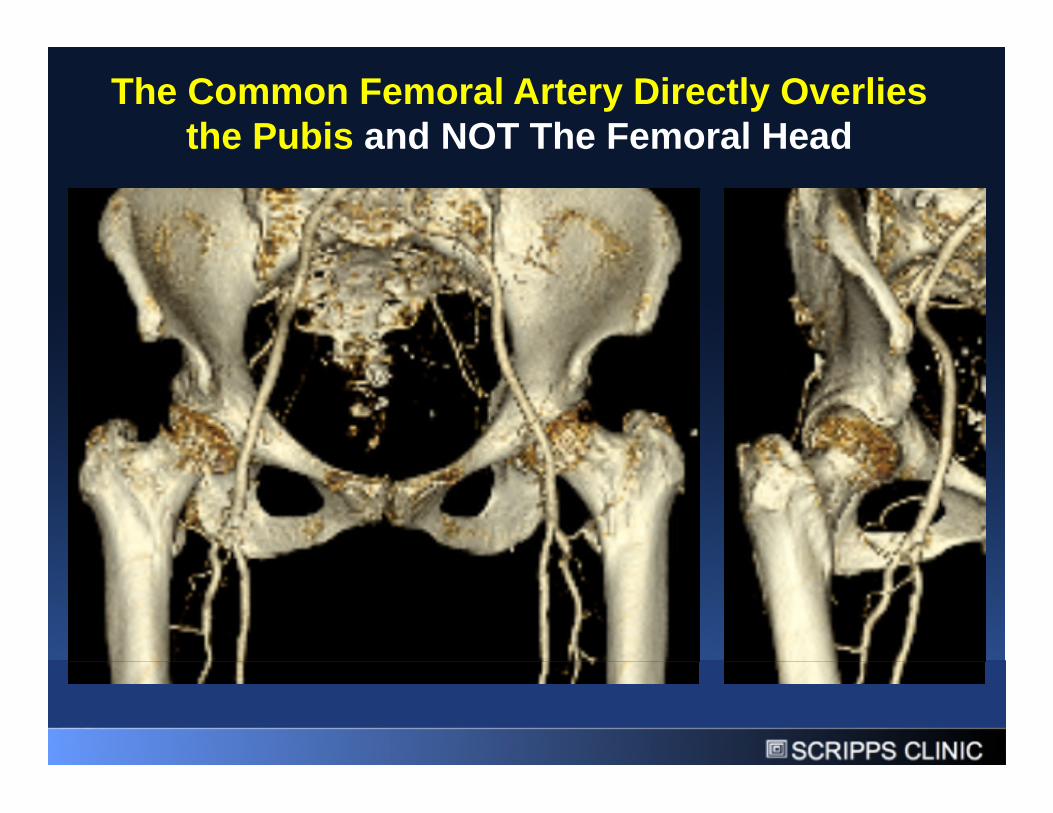
The Common Femoral Artery Directly Overliesthe Pubis and NOT The Femoral Headthe Pubis and NOT The Femoral Head

The Pubis: A Key Structure inFemoral Artery Access and ClosureFemoral Artery Access and Closure
PUBIS

How Does Manual CompressionReally Work?Really Work?
Vessel isVessel iscompressed tostop bleedinglong enough tolong enough toallow thestretchedarteriotomy toarteriotomy torecoil backdown tooriginal 18Gauge hole andGauge hole anddevelop a smallthrombus

External Compression of AppropriateAccess SiteAccess Site
Externalcompressioncompressioncontrols access sitedue to the presencedue to the presenceof bony structureposteriorly (pubis)
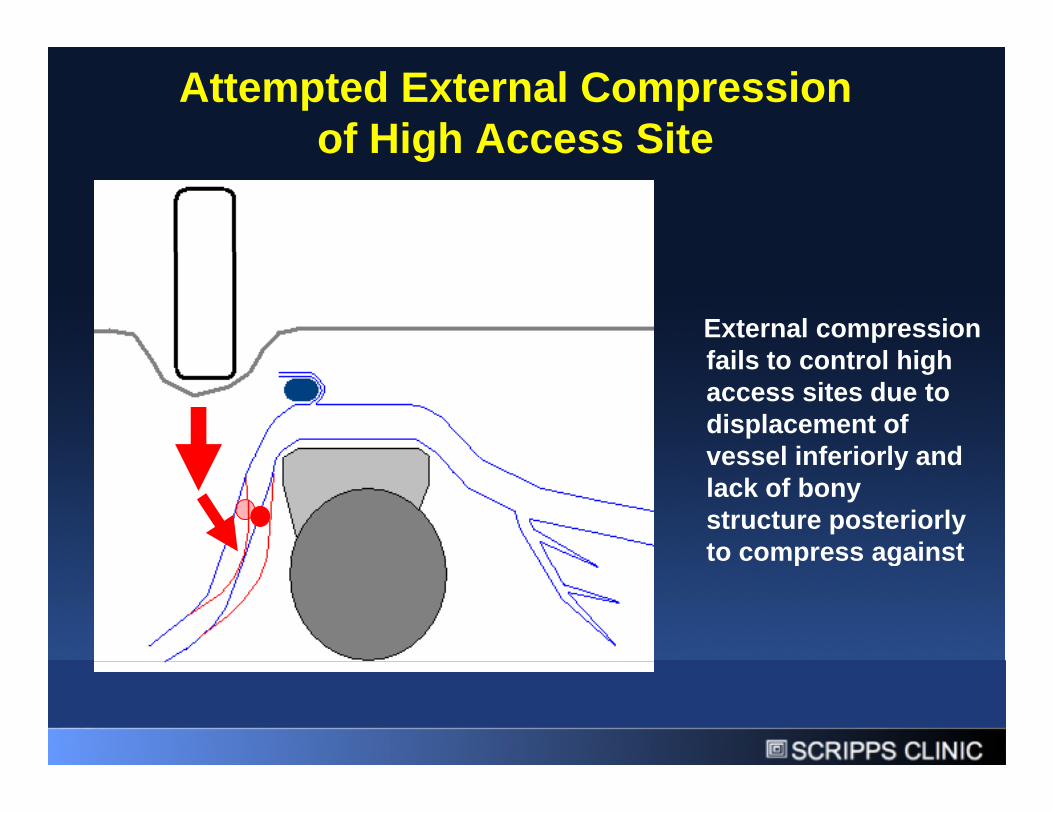
Attempted External Compressionof High Access Siteof High Access Site
External compressionfails to control highfails to control highaccess sites due todisplacement ofvessel inferiorly andvessel inferiorly andlack of bonystructure posteriorlyto compress againstto compress against
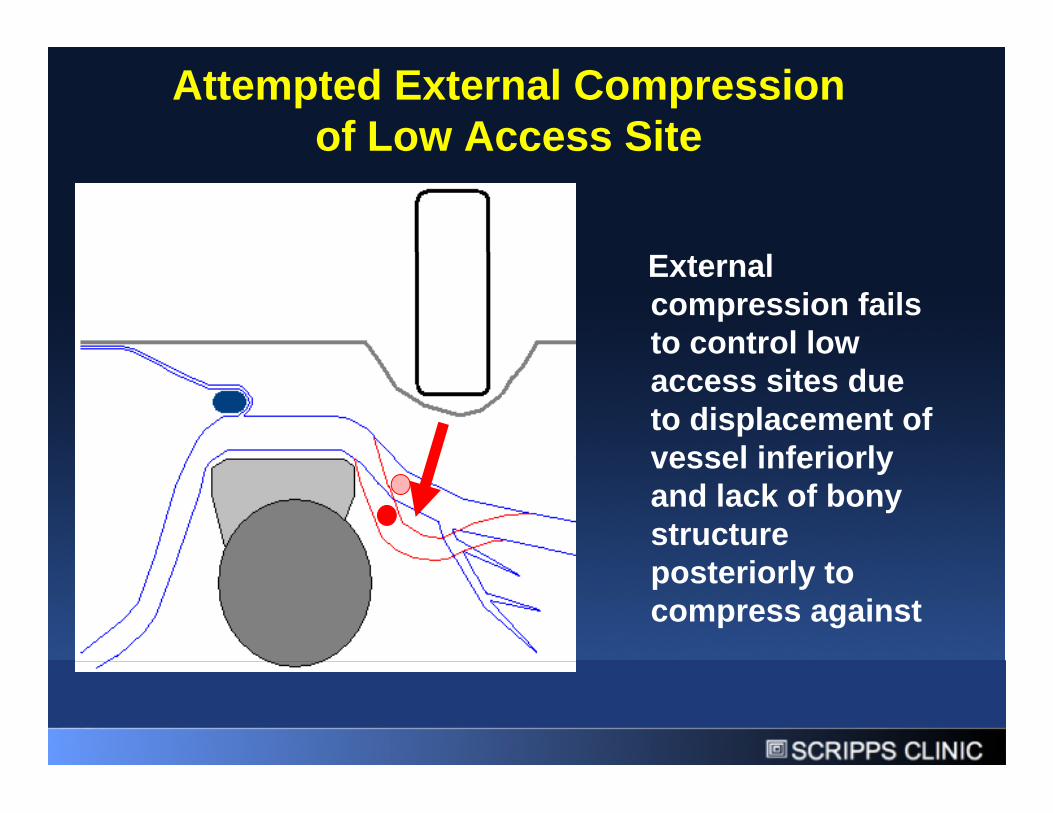
Attempted External Compressionof Low Access Siteof Low Access Site
ExternalExternalcompression failsto control lowto control lowaccess sites dueto displacement ofvessel inferiorlyvessel inferiorlyand lack of bonystructureposteriorly toposteriorly tocompress against
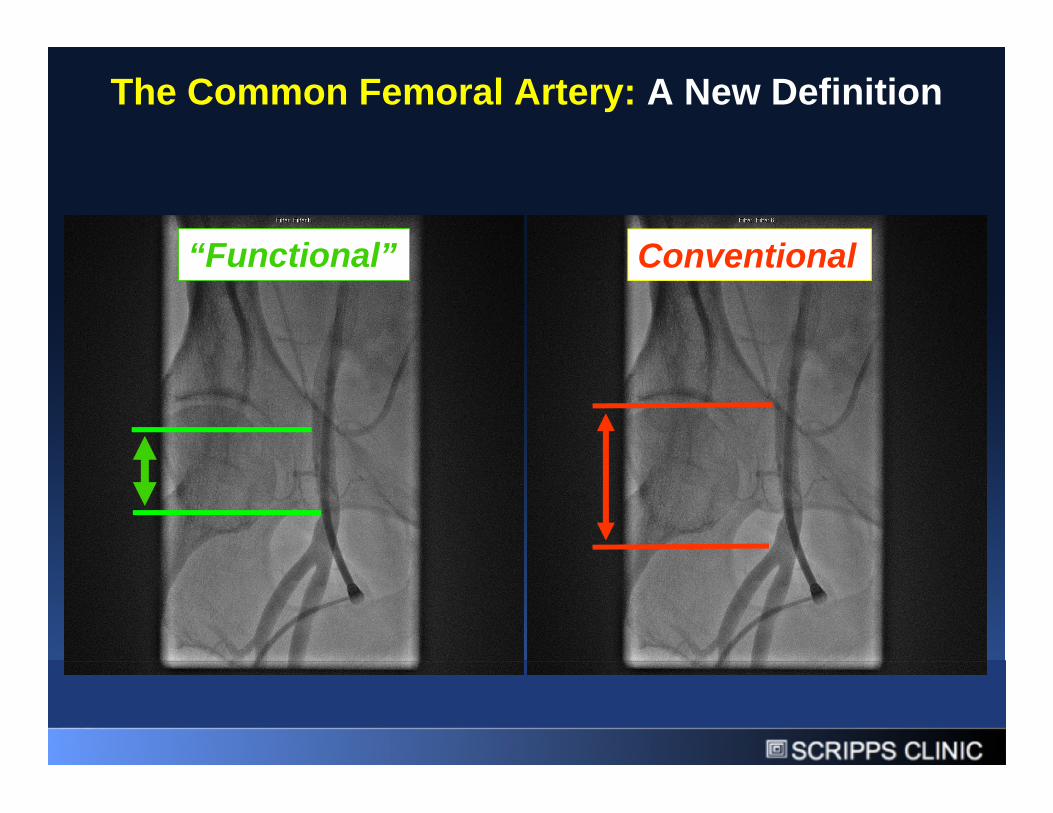
The Common Femoral Artery: A New Definition
“Functional” Conventional“Functional” Conventional
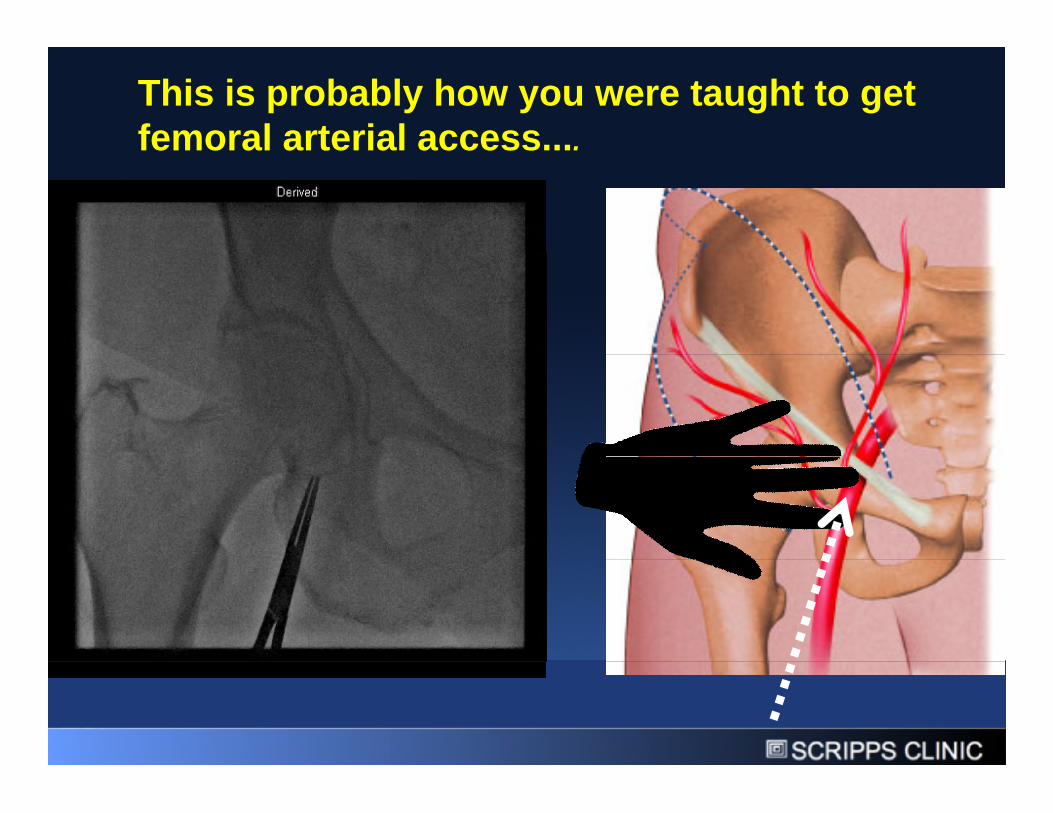
This is probably how you were taught to getfemoral arterial access....femoral arterial access....
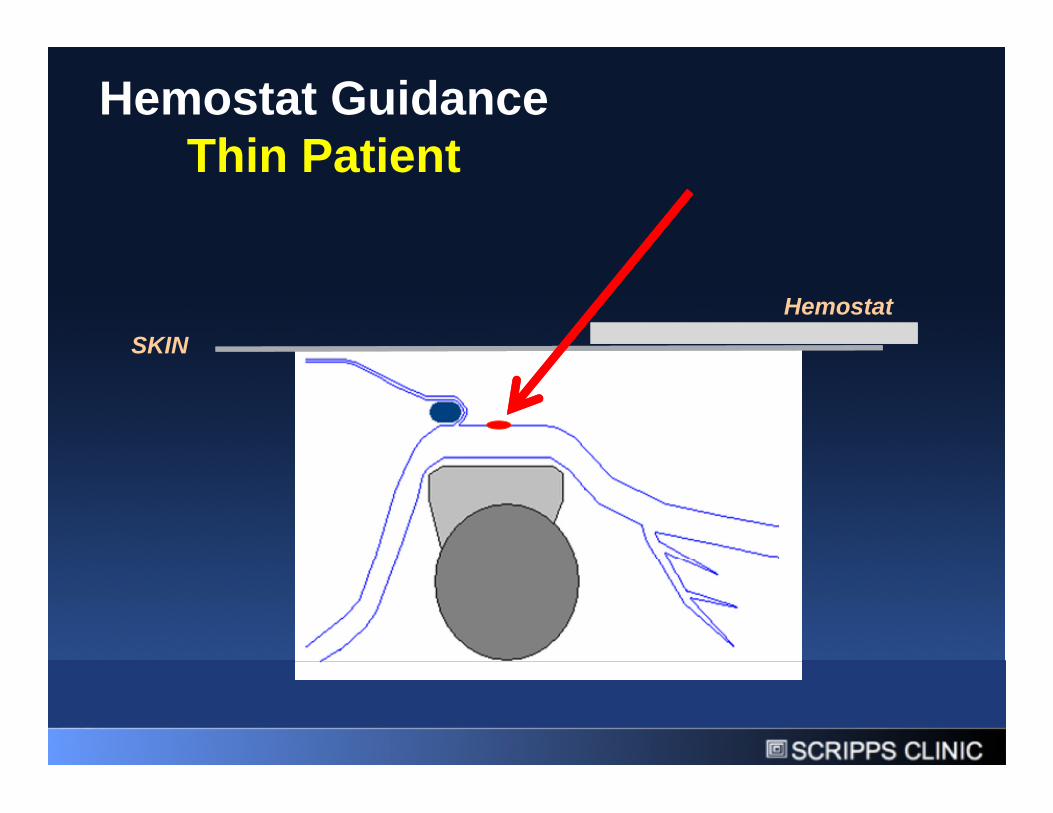
Hemostat GuidanceThin PatientThin Patient
SKIN
Hemostat
SKIN
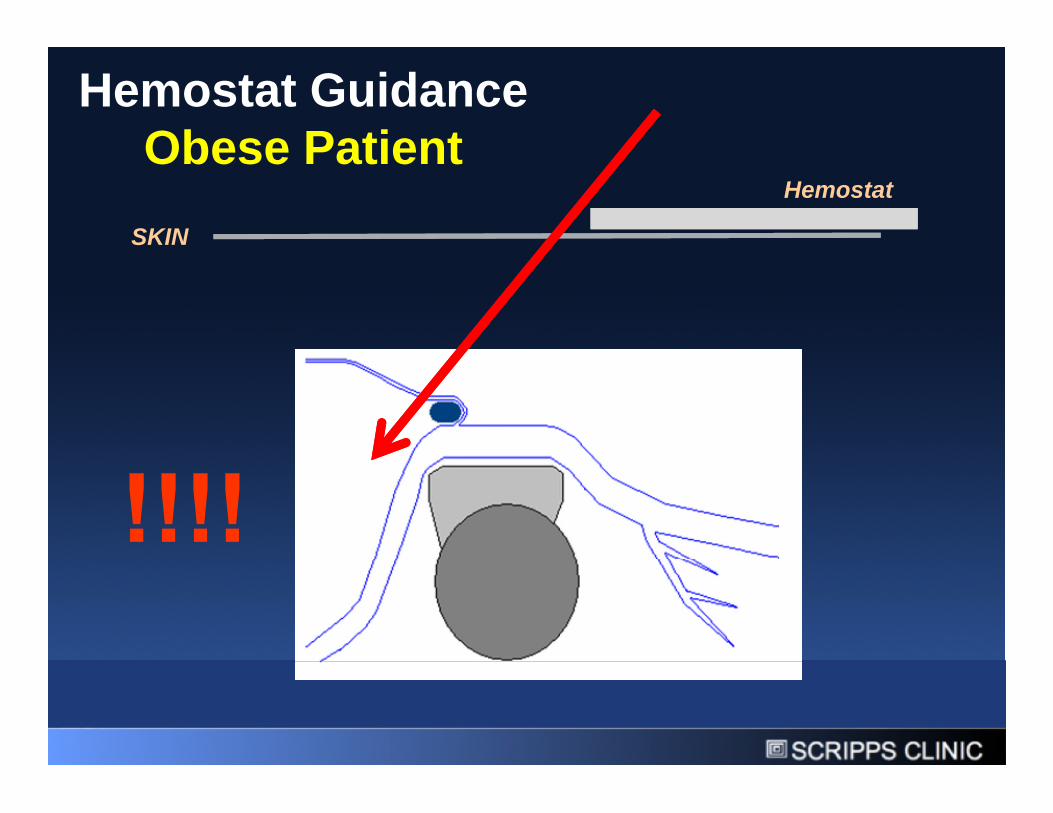
Hemostat GuidanceObese PatientObese Patient
SKIN
Hemostat
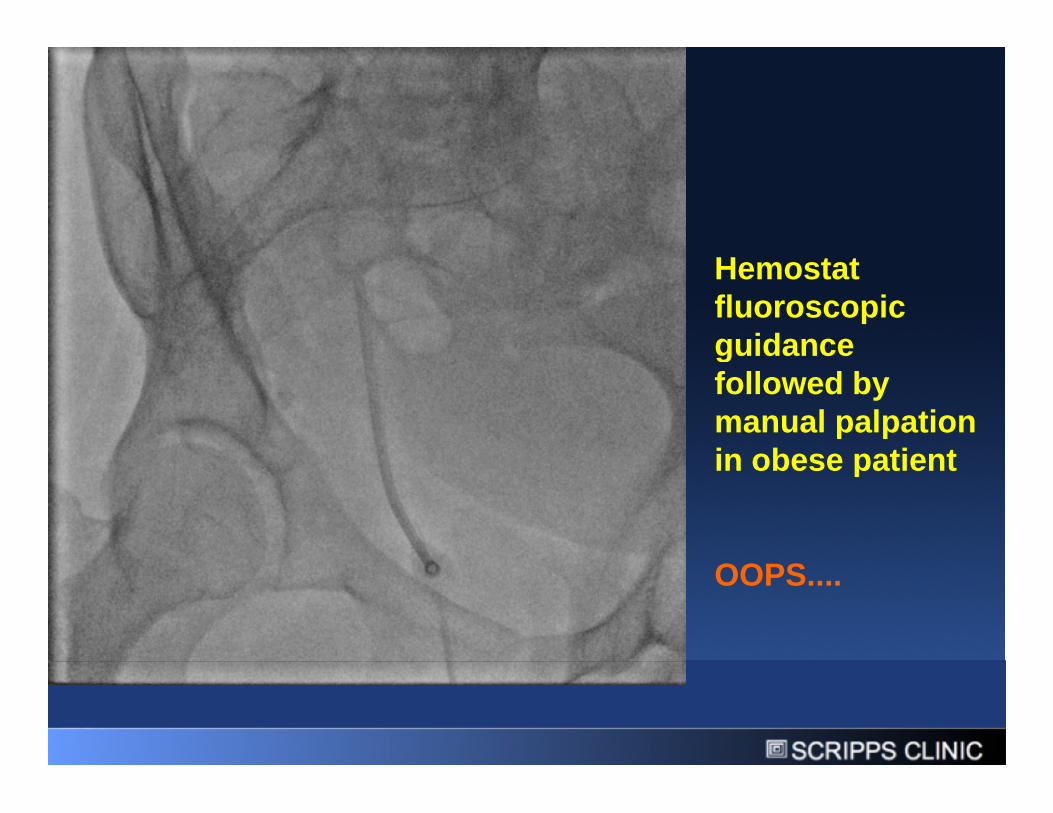
HemostatHemostatfluoroscopicguidanceguidancefollowed bymanual palpationin obese patientin obese patient
OOPS....OOPS....

Retroperitoneal bleeding due to lacerationof the inferior epigastric artery
Usingfluoroscopicguidance of the
of the inferior epigastric artery
guidance of thefemoral headfollowed byfollowed bymanualpalpation canlead tolead tolaceration ofadjacentstructuresstructures

LESSON:LESSON:
Using thefemoral headas a markerfollowed bymanualmanualpalpation isfraught withproblems!problems!

1004 patients randomized 1:1 to femoral access using fluroscopy alone1004 patients randomized 1:1 to femoral access using fluroscopy alonevs. ultrasound guidance
Ultrasound Use Associated with:• Lower vascular complication rates• Lower vascular complication rates• Improved first pass success rate• Reduced number of access attempts• Reduced risk of inadvertent venopuncture• Reduced risk of inadvertent venopuncture• Reduced time to access
JACC INTERV., VOL. 3, NO. 7, 2010 JULY 2010:751– 8
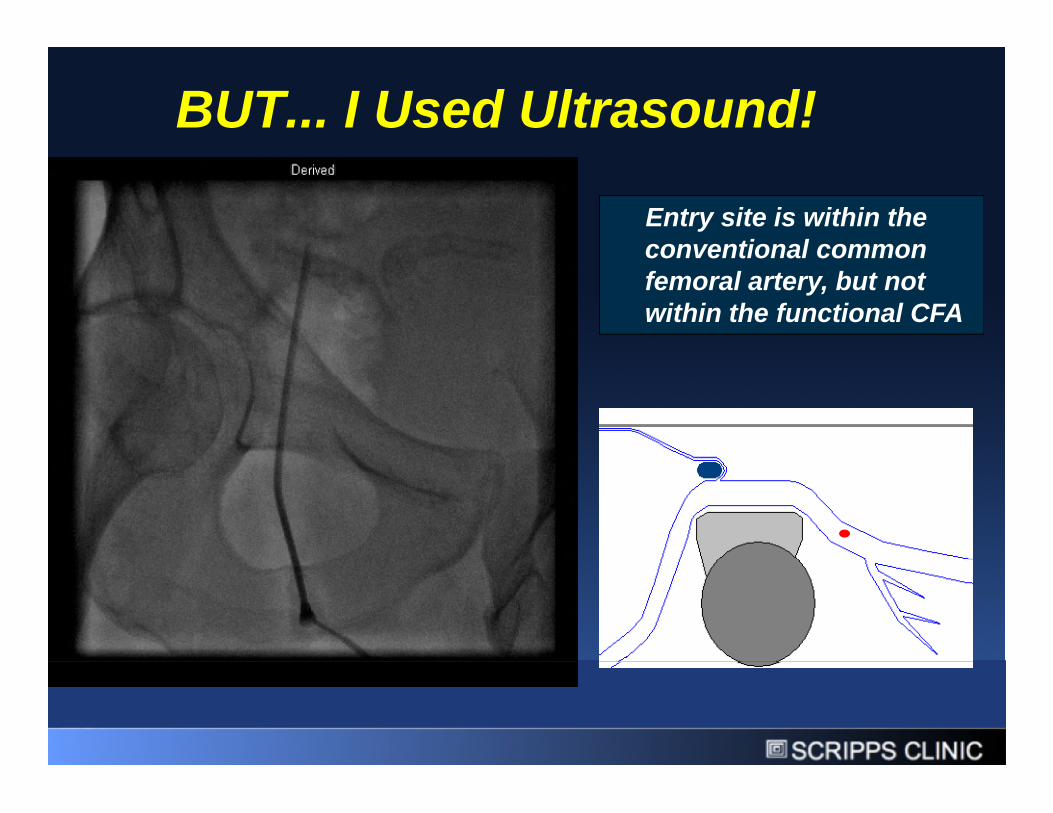
BUT... I Used Ultrasound!
Entry site is within theconventional commonconventional commonfemoral artery, but notwithin the functional CFA

• Use fluoroscopy toposition ultrasoundprobe over the pubisprobe over the pubis
• Then use ultrasoundto visualize needleentering arteryentering artery
• Insert needle intoartery at 45 degreeartery at 45 degreeangle

Optimal Femoral Access:Ultrasound AND FluoroscopyUltrasound AND Fluoroscopy
•• Ultrasound gets you into the vessel
Assures single puncture of the center ofAssures single puncture of the center ofthe artery, avoids inadvertent injury ofunwanted structures
• Fluoroscopy gets you into the vessel inthe right place
Assures entry into the artery over thepubis

“Lets take anangiogram atangiogram atthe end of thecase to see ifwe can use awe can use aclosure device”
LESSON:
Take angiogramBEFOREproceeding withproceeding withcase and givinganticoagulationanticoagulation

Correct Technique Incorrect Technique
Wire Insertion Technique
Correct Technique Incorrect Technique
Needle bevel notfully insertedthrough vesselwall, but insertedenough to getflash
Wire advancedinto subintimalspace leading
Needle inserted fullyinto vessel (but NOT space leading
to dissectioninto vessel (but NOTthrough posterior wall)at 45 degree angle

Glidewire usedGlidewire usedand advanced“easily” butguide wontguide wontadvance…
LESSON:
Use soft tipshapeable wire(ie: Wholey(ie: Wholeywire) if J wirewont advancewont advance

Complications Associated WithFemoral AccessFemoral Access
• Hematoma• Hematoma
• Pseudoaneurysm
• Arterial-Venous Fistula• Arterial-Venous Fistula
• Retroperitoneal Hemorrhage
• Dissection
• Endarteritis
• Acute Closure/Vascular Compromise
• Distal Embolization• Distal Embolization
• Nerve Injury
SCRIPPS CLINIC

Complications Associated WithFemoral AccessFemoral Access
• Hematoma• HematomaMultiple punctures
Back wall/through and through puncture
Poor hemostasis with closure device or manual holdPoor hemostasis with closure device or manual hold
Laceration of femoral artery
Laceration/puncture of adjacent vessels
Kinked sheath at arteriotomy replace with braided sheathKinked sheath at arteriotomy replace with braided sheath
Access site not over bony structures cant adequatelycontrol bleeding with compression
Any of the above with anticoagulationAny of the above with anticoagulation
SCRIPPS CLINIC

• 78yo morbidlyobese femaleobese female
• PCI via left groin
• Manual hold in• Manual hold inrecovery area
• During hold processlarge hematomaforms and isforms and isexpanding
• Multiple people“pressing down” ongroin sitegroin site
• Hypotensiveresponds to fluidsresponds to fluids
• Hypotensiveagaintaken back tocath lab..
SCRIPPS CLINIC

• Alternate accessrapidly obtainedrapidly obtained
• Balloon insertedand inflated
• Hemostasis• Hemostasisachieved
• Blood pressureimmediatelyimmediatelyimproves
• Taken to OR: leftfemoral arteryrepaired, large leftthigh hematomathigh hematomaevacuated
SCRIPPS CLINIC

• Small hematomas can be stabilized and resolvedwith good manual pressurewith good manual pressure
• Large hematomas are nearly impossible to managewith external compression alone- impossible to getwith external compression alone- impossible to getpoint pressure on the artery just above the puncturesite
• Often pressure is distributed too widely and can• Often pressure is distributed too widely and canlead to injury of adjacent femoral nerve orcompression of vessel distal to bleeding siteaccentuates bleedingaccentuates bleeding
• These are best managed by rapid internaltamponade technique, +/- surgery or covered stent
SCRIPPS CLINIC
tamponade technique, +/- surgery or covered stentplacement along with supportive measures
Complications Associated WithFemoral AccessFemoral Access
• Pseudoaneurysm• PseudoaneurysmSite of access below pubis cant compress adequately
Use of Femostop for primary hemostasis
Poor manual hold technique/weak hands
Multiple punctures in close proximity
Late/delayed failure of closure deviceLate/delayed failure of closure device
SCRIPPS CLINIC

Mechanism of PseudoaneurysmFormationFormation
SCRIPPS CLINIC

Pseudoaneurysm from low access and poor hold technique
SCRIPPS CLINIC
Management of Pseudoaneurysm
• If less than 2cm in size and assymptomatic, may not• If less than 2cm in size and assymptomatic, may notrequire intervention
• If 2cm or greater in size and with narrow neck,ultrasound guided compression or thrombininjection is very effective
• Wide neck pseudoaneurysms are not ideal for• Wide neck pseudoaneurysms are not ideal forthrombin injection, and may require surgicalintervention
SCRIPPS CLINIC
Complications Associated WithFemoral AccessFemoral Access
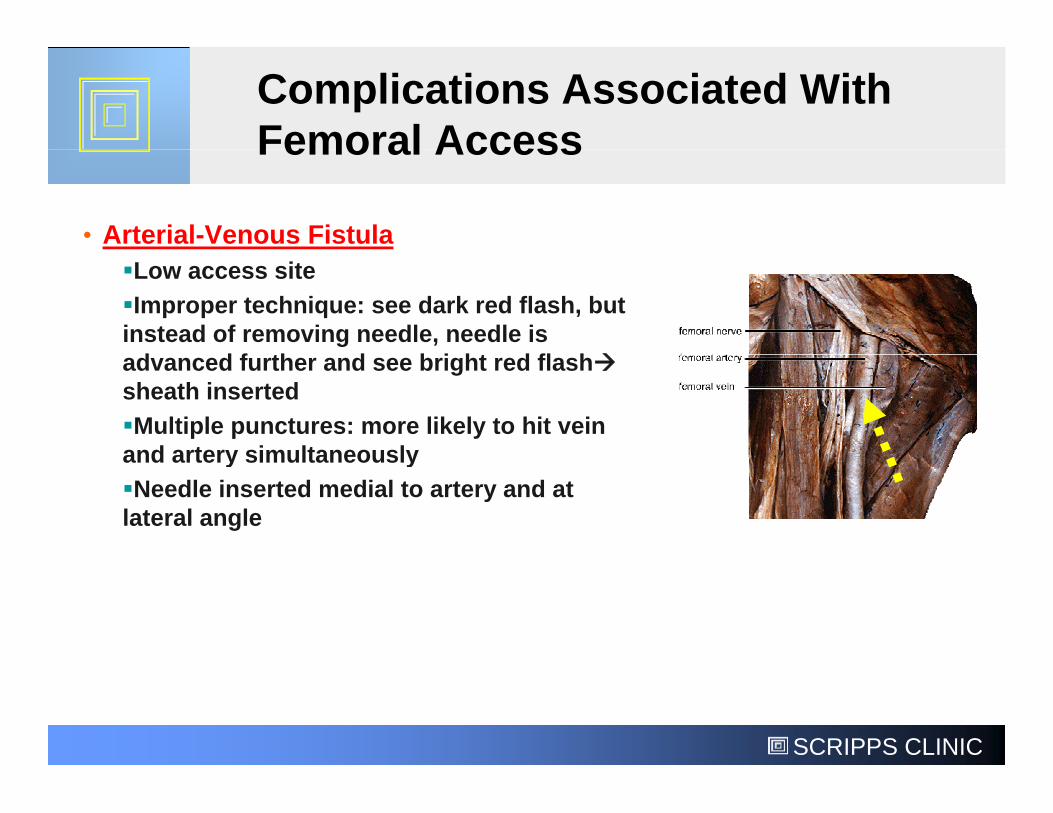
• Arterial-Venous Fistula
Low access site
Improper technique: see dark red flash, butinstead of removing needle, needle isadvanced further and see bright red flashadvanced further and see bright red flashsheath inserted
Multiple punctures: more likely to hit veinand artery simultaneouslyand artery simultaneously
Needle inserted medial to artery and atlateral angle
SCRIPPS CLINIC
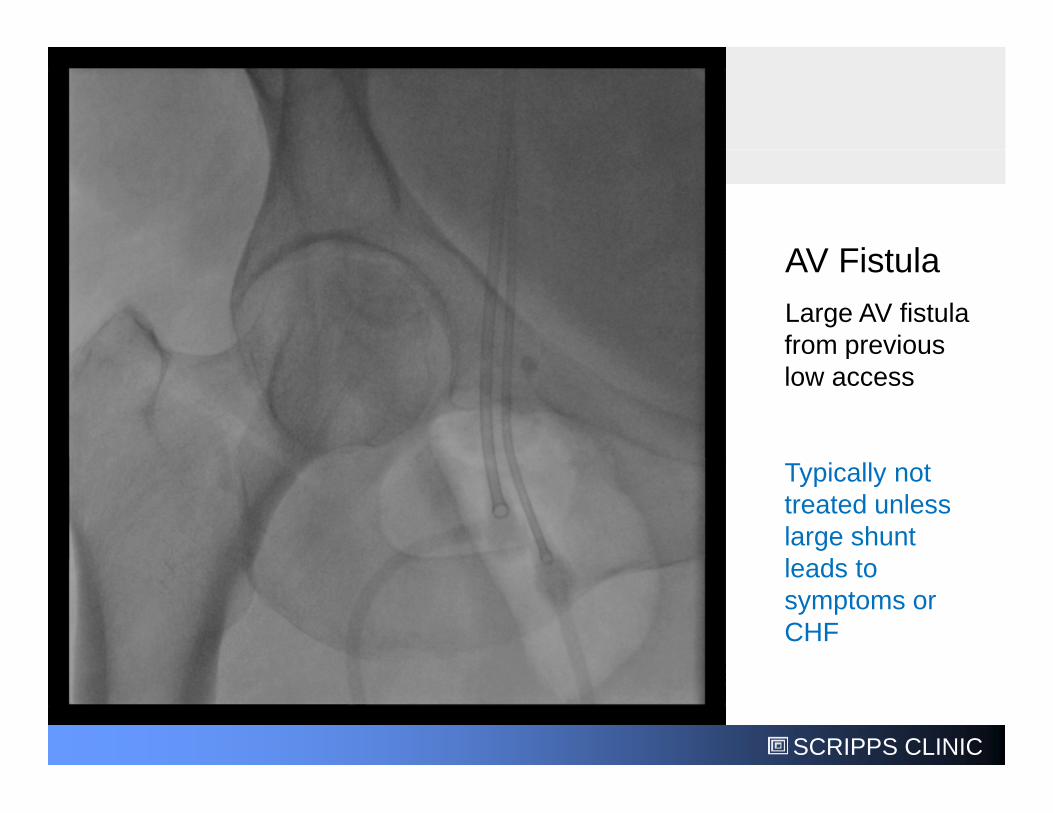
AV FistulaAV Fistula
Large AV fistulafrom previousfrom previouslow access
Typically nottreated unlesslarge shuntleads toleads tosymptoms orCHF
SCRIPPS CLINIC
Complications Associated WithFemoral AccessFemoral Access
• Retroperitoneal Hemorrhage
High access site/non-compressible access site
Use of Femostop or poor manual hold in obese patientslarge pannus leads to pressure being applied DISTAL toarteriotomy blood then tracks upwards through femoralcanal into abdomen instead of into thigh because Femostop ormanual pressure is creating a physical barriermanual pressure is creating a physical barrier
Laceration of adjacent vessels
Wire perforation of small branches in pelvis use ofGlidewire/non J-tipped wires
SCRIPPS CLINIC
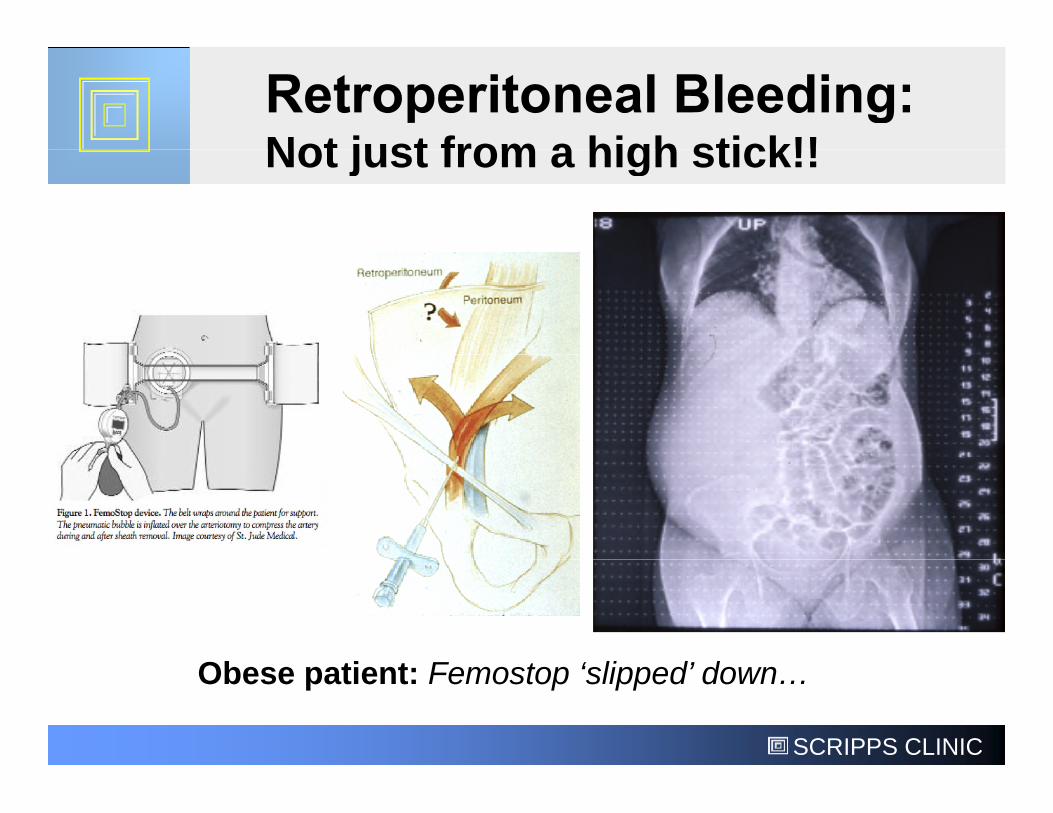
Not just from a high stick!!Not just from a high stick!!
Obese patient: Femostop ‘slipped’ down…
SCRIPPS CLINIC
Obese patient: Femostop ‘slipped’ down…

Retroperitonealbleeding with“Bladder Sign”
SCRIPPS CLINIC
Complications Associated WithFemoral AccessFemoral Access
• Dissection• DissectionMost often due to poor access technique- “partial needleinsertion” or simply forcing J wire to go if resistance felt
Use of Glidewire or other hydrophillic and/or stiff wiresUse of Glidewire or other hydrophillic and/or stiff wires
Advancing wire without fluoro imaging
SCRIPPS CLINIC
• Most dissections are retrograde, and simply• Most dissections are retrograde, and simplyremoving wires/equipment will allow them to healover time
• Antegrade dissections can occur upon withdrawl ofshaped catheters or bulky devices (ie: valvuloplastyballoons, large diameter sheaths, etc.) and shouldballoons, large diameter sheaths, etc.) and shouldbe treated to prevent propagation and subsequentflow limitation
• Antegrade dissections typically can be managed• Antegrade dissections typically can be managedwith a combination of balloon angioplasty and stentplacement
SCRIPPS CLINIC
placement

Complications Associated WithFemoral AccessFemoral Access
EndarteritisEndarteritis
• Can occur withclosure devices,closure devices,especially in very thinor very obese
• Don’t discharge• Don’t dischargepatients withtegaderm-typedressings in place!
• Don’t use closuredevices inimmunocompromised
SCRIPPS CLINIC
immunocompromisedpatients

Complications Associated WithFemoral Access
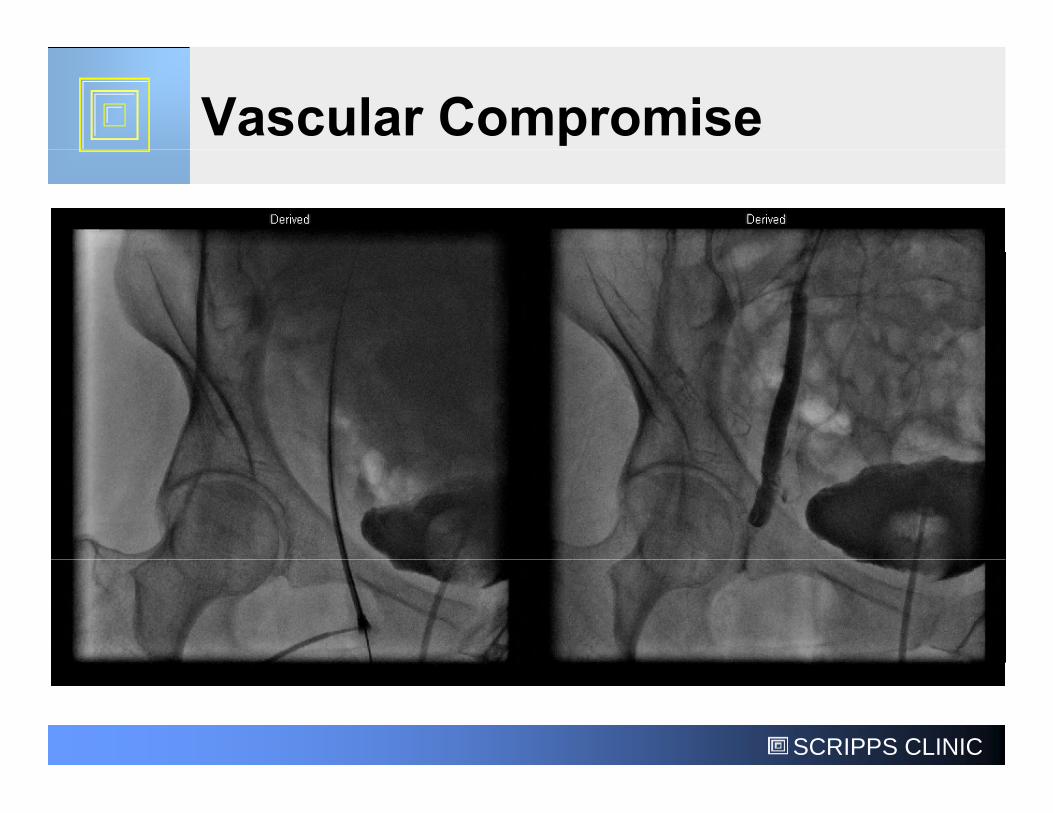
Acute Vessel Closure
• DO NOT hold fully occlusive pressure on a severely
Femoral Access
• DO NOT hold fully occlusive pressure on a severelydiseased artery for more than 10 minutes
• Do not deploy closure devices in a significantly• Do not deploy closure devices in a significantlydiseased or dissected femoral artery
• Assess distal pulses before and immediately afterhemostasis is complete to assure no newcompromise has occurred
• If patient complains of foot/leg pain or numbness• If patient complains of foot/leg pain or numbnessconsider acute vascular compromise this is anEMERGENCY
SCRIPPS CLINIC
SCRIPPS CLINIC
Complications Associated WithFemoral Access
Distal Embolization
Femoral Access
Distal Embolization
• Can occur due to disruption of plaque bycatheters/wires, or thrombus formation aroundcatheters/wires, or thrombus formation aroundsheath, catheters.
• Critically important to assess distal pulses before• Critically important to assess distal pulses beforeand after procedure to assess for any change.
SCRIPPS CLINIC

• Aspirate 2-4 cc of blood• Aspirate 2-4 cc of bloodfrom indwelling sheathbefore removing it
• DON’T flush sheath by• DON’T flush sheath byflushing saline intopatient may embolizea clot
• DON’T aspirate 2-3 ccand then flush it rightback into the patient!
• DON’T leave a sheath ina patient for longer thanreally necessary
SCRIPPS CLINIC

SCRIPPS CLINIC
Complications Associated WithFemoral Access
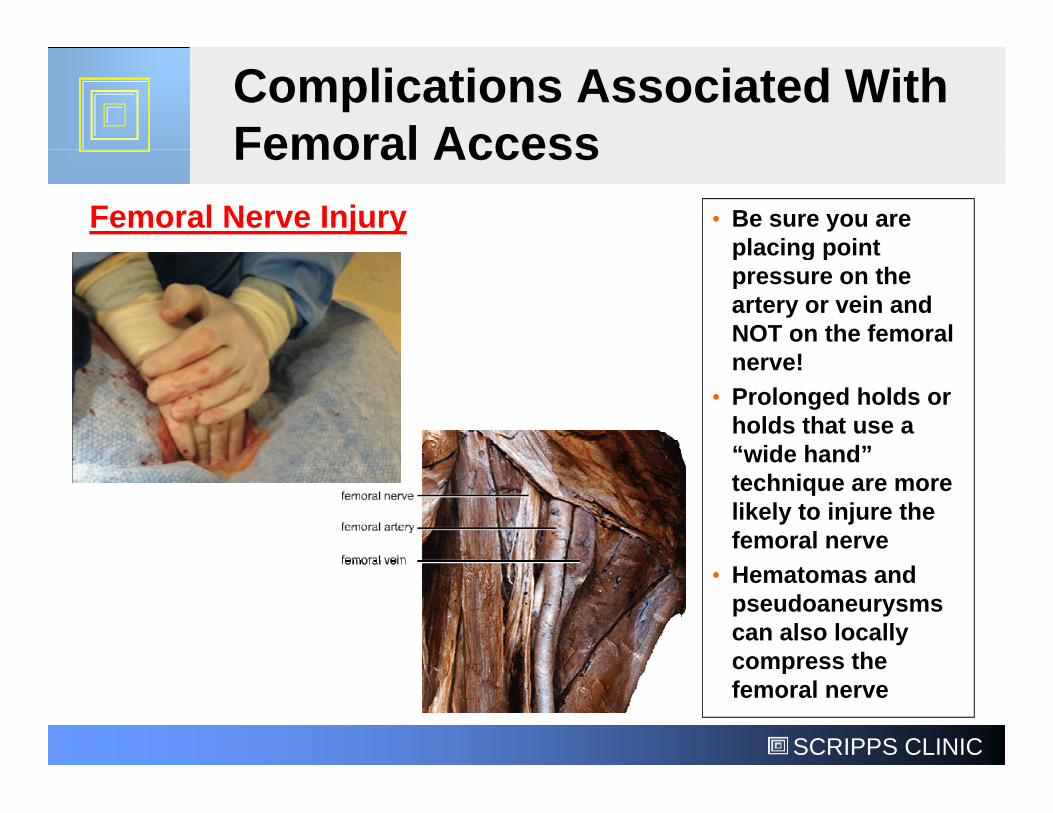
• Be sure you areplacing point
Femoral Nerve Injury
Femoral Access
placing pointpressure on theartery or vein andNOT on the femoralnerve!nerve!
• Prolonged holds orholds that use a“wide hand”“wide hand”technique are morelikely to injure thefemoral nerve
• Hematomas andpseudoaneurysmscan also locallycompress the
SCRIPPS CLINIC
compress thefemoral nerve

Stinis’ RuleStinis’ Rule
• First episode: Could be vaso-vagal (if getting• First episode: Could be vaso-vagal (if gettingmanual pressure)Fluids, Atropine
• Second episode: Retroperitoneal bleeding until• Second episode: Retroperitoneal bleeding untilproven otherwise!Fluids, call for blood, vasopressors, Trandelenberg,consider immediate return to cath lab for furtherinvestigation and internal tamponade and/or covered stentplacement
DO NOT send a suspected retroperitoneal bleedingpatient to the CT scanner! CT is not an actual therapy
SCRIPPS CLINIC
patient to the CT scanner! CT is not an actual therapyfor hypotension or retroperitoneal bleeding!!

• It’s July at ateachingteachinginstitution.....
• What to do?Call surgeons
Pull and hold (andPull and hold (and
pray)
Closure device?
SCRIPPS CLINIC

• Contralateralfemoral accessobtainedobtained
• Be sure secondaccess is not toohigh!
SCRIPPS CLINIC
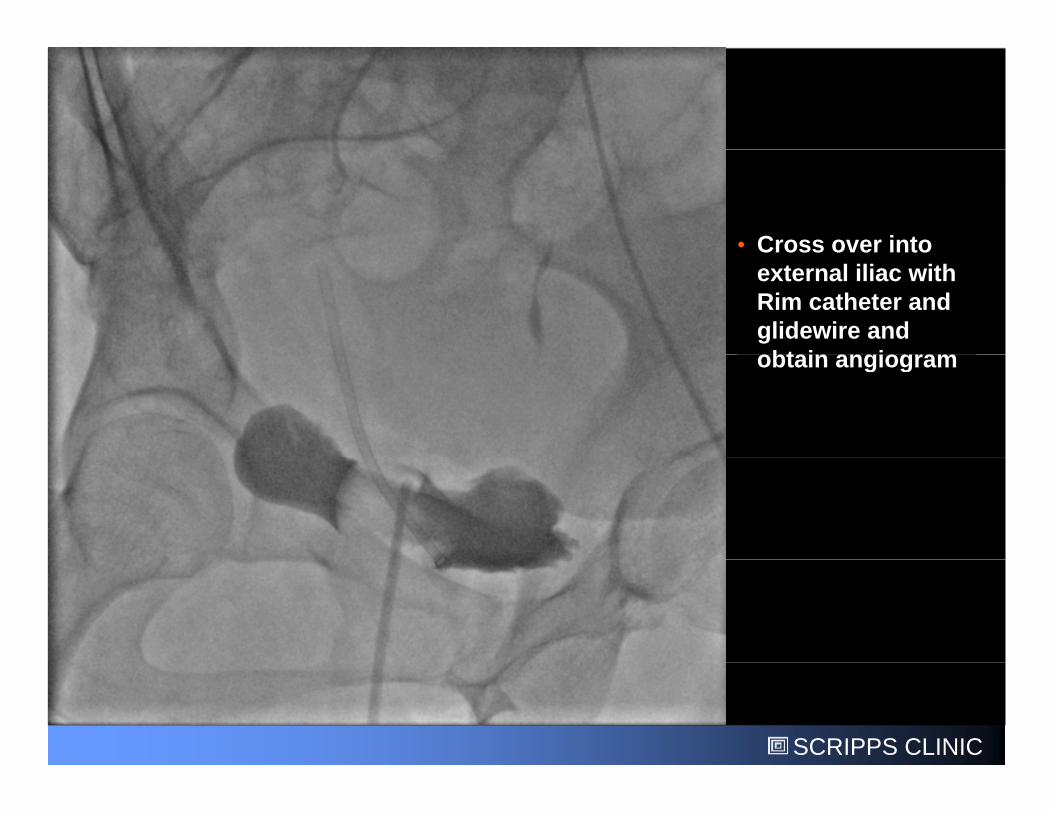
• Cross over into• Cross over intoexternal iliac withRim catheter andglidewire andobtain angiogramobtain angiogram
SCRIPPS CLINIC

• Remove sheath,close high accessclose high accesssite with Perclosedevice and re-insert guidewire toinsert guidewire tomaintain vesselaccess
• Angiogram takento assess forextravasation
SCRIPPS CLINIC

• Wire removed• Wire removed
• Sutures secured inplace
• Completion• Completionangiogramperformed toassure noevidence ofevidence ofbleeding
SCRIPPS CLINIC

Important to take• Important to takeangiograms inmultiple views
• Mild vessel spasm• Mild vessel spasmnoted, but noextravasation
SCRIPPS CLINIC

Management of Inadvertent HighAccess SiteAccess Site
• DO NOT send the patient for a manual hold!
• DO NOT blindly close the access site and assumethe patient is OK because you don’t see anybleeding and they seem stable.... You wont see thebleeding and they seem stable.... You wont see thebleeding- its going into the retroperitoneal space!
• DO obtain alternative access and close the highaccess with a Perclose device and directly visualizeby angiography that it is indeed closed- DO NOT useby angiography that it is indeed closed- DO NOT useany other closure device!
• DO have an appropriately sized balloon ready to go
SCRIPPS CLINIC
• DO have an appropriately sized balloon ready to goin case internal tamponade is needed
• Most femoral access site complications can beavoided by obtaining proper access of the vesselavoided by obtaining proper access of the vesselAccess should be iin the “functional CFA” over the pubis
Use ultrasound AND fluoroscopy: neither by itself
Avoid “high” and “low” sticks
Single anterior wall puncture at 45 degrees
Perform femoral angiogram at the BEGINNING of the casePerform femoral angiogram at the BEGINNING of the case
• Don’t attempt to perform a manual hold on any siteof access in the vicinity of or above the inguinalligamentligament
• Large or expanding hematomas are best managedby urgent internal tamponade, followed by surgical
SCRIPPS CLINIC
by urgent internal tamponade, followed by surgicalintervention or covered stent placement