avoidable reoperations for thyroid and parathyroid surgery: effect of hospital volume
TRANSCRIPT

Avoidable reoperations for thyroid andparathyroid surgery: Effect of hospitalvolumeJamie Mitchell, MD, Mira Milas, MD, German Barbosa, MD, Jazmine Sutton, BS, Eren Berber, MD,and Allan Siperstein, MD, Cleveland, Ohio
Background. Hospital volume for thyroid and parathyroid surgery inversely correlates with perioperativecomplications. This correlation has not been made regarding the need for reoperation.Methods. We retrospectively analyzed 395 reoperative thyroid (TR) and parathyroid (PR) surgeries at atertiary care hospital from 1999 to 2007. Based on current standards of care, reoperations were classifiedas avoidable or unavoidable. Public discharge data were used to classify hospitals as low-volume centers(LVC; <20 cases/yr) or high-volume centers (HVC; $20 cases/yr). The v2 test was used to determinestatistical significance.Results. Hospital data were available for 335 reoperations (85%). There were 134 avoidable (34%)and 201 unavoidable (66%) procedures. Primary hyperparathyroidism (HPT) and thyroid cancer eachaccounted for a third of cases. Of PR from LVC, 77% were avoidable compared with 22% from HVC(P < .001). Of TR from LVC, 50% were avoidable versus 14% from HVC (P < .001). Operations forboth primary HPT and thyroid cancer led to avoidable reoperations more frequently if performed at aLVC (P < .001).Conclusion. By objective criteria, many thyroid and parathyroid reoperations are avoidable. Mostoriginate from LVC. In addition to decreasing complication rates, thyroid and parathyroid surgeryperformed at HVC would decrease the need for patients to undergo reoperations. (Surgery2008;144:899-907.)
From the Endocrinology and Metabolism Institute, Section of Endocrine Surgery, The Cleveland Clinic,Cleveland, Ohio
INITIAL ATTEMPTS AT THYROID AND PARATHYROID SURGERY
resulted in significant morbidity and mortality.1,2
Improvements in our understanding of the rele-vant anatomy and pathophysiology of thyroid andparathyroid disease, as well as advances in opera-tive and anesthetic techniques, have allowed theremoval of these glands to be performed muchmore safely. Despite these advances, however, thy-roid and parathyroid operations continue to be as-sociated with potentially serious complications.3
Injury to the recurrent laryngeal nerve (RLN)can significantly affect quality of life or even belife threatening in extreme cases, with reportedrates remaining as high as 10%.4 Although the im-portance of surgeon experience in preventing
Accepted for publication July 24, 2008.
Reprint requests: Allan Siperstein, MD, Endocrinology andMetabolism Institute, Section of Endocrine Surgery, A-80, TheCleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195.E-mail: [email protected].
0039-6060/$ - see front matter
� 2008 Mosby, Inc. All rights reserved.
doi:10.1016/j.surg.2008.07.022
such complications is intuitive, only in recent yearshas this concept been documented. Severalpublished reports have demonstrated a direct corre-lation between hospital or clinician volume and clin-ical outcomes.5-9 Sosa et al10 and Pieracci et al11
showed that morbidity, mortality, and length ofstay decreased after thyroidectomy as surgeon andhospital experience increased. Stavrakis et al12
showed similar results for thyroid and parathyroidoperations.
A significant number of thyroid and parathyroidoperations performed at our institution are reoper-ative in nature (25%). Reoperations are technicallymore challenging owing to the presence of signifi-cant scar tissue, distortion of normal anatomicrelationships, and obliteration of the usual tissueplanes. This consequently increases the risk ofinadvertent injury to the RLN and parathyroidglands. Although some reoperations are unavoid-able, many times the need for reoperation was felt tobe due to inadequate or inappropriate initial treat-ment. Kouvaraki et al13 touched on this, examiningthe incidence of ‘‘preventable’’ reoperations forpapillary thyroid cancer secondary to inadequate
SURGERY 899

SurgeryDecember 2008
900 Mitchell et al
Table I. Criteria for avoidable and unavoidable reoperations*
Thyroid reoperations Parathyroid reoperations
Avoidable1. Lobectomy with known goiter in contralateral
lobe (JE)1. Missed gland during neck exploration in normal
anatomic location (TE)2. Partial lobectomy with ipsilateral recurrence of
goiter/cancer (JE)2. Persistent HPT in MEN/secondary HPT/tertiary
HPT patients after less than subtotalparathyroidectomy (JE/TE)
3. Partial thyroidectomy with known history ofionizing radiation to the neck (JE)
3. Reexploration without adequate preoperativelocalization (JE)
4. Nodal disease diagnosed by excisional biopsy (notFNA; JE)
4. Persistent HPT after focal exploration withoutlocalization/IOPTH use (JE)
5. Inadequate lymph node dissectiona. Selective lymph node excision (‘‘berry
picking’’) with recurrence in same anatomiccompartment (JE)
b. Failure to include appropriate cervicalcompartments in dissection (TE)
6. Partial thyroidectomy for known malignancyprecluding RAI therapy (JE and/or TE)
Unavoidable1. Completion thyroidectomy after lobectomy for
follicular neoplasm on FNA1. Persistent HPT after exploration with
preoperative localization and appropriate IOPTHdrop
2. Completion total thyroidectomy after lobectomyfor benign disease
2. Persistent HPT with ectopic gland not imaged onpreoperative localization
3. Interval development of new nodal disease informally dissected compartment
a. Undescended gland inaccessible throughstandard cervical incision
4. Interval development of new nodal disease inundissected compartment (no evidence oflymphadenopathy at initial operation)
b. Mediastinal gland not accessible throughstandard cervical incision
3. Persistent HPT with supernumerary gland after 4glands accounted for at initial exploration
4. Recurrent HPT
*Criteria for characterizing reoperations as avoidable or unavoidable. For avoidable reoperations, possible etiologies are included in parentheses.
FNA, Fine needle aspiration; HPT, hyperparathyroidism; IOPTH, intraoperative intact parathyroid hormone; JE, error in judgment; MEN, multipleendocrine neoplasia; RAI, radioactive iodine therapy; TE, technical error.
initial operative therapy. Still, no standardized set ofobjective criteria has been developed to classify thy-roid and parathyroid reoperations as preventable.In reviewing our experience with operative thyroidand parathyroid repoerations, we sought to estab-lish whether a set of objective criteria could be devel-oped to reliably characterize reoperations asavoidable or unavoidable, and whether clinical vol-ume affects the incidence of avoidable reoperations.
METHODS
All patients undergoing thyroid and parathyroidsurgery between 1999 and 2007 at the ClevelandClinic by 3 endocrine surgeons were retrospec-tively reviewed. For each reoperation, the hospitalwhere the initial operation took place wasidentified.
Preoperative imaging studies, intraoperativefindings, and histopathology reports of both theinitial and subsequent operations were analyzed toclassify each reoperation as avoidable or unavoid-able using a set of objective criteria (Table I). Thisset of criteria was created based on currently ac-cepted standards of care supported by the litera-ture.14,15 These standards were applied to eachcase at the time of the initial operation. For exam-ple, partial thyroid lobectomies for nodular goiterwith ipsilateral recurrence necessitating reopera-tion were classified as unavoidable if performedbefore 1990. Using these criteria, reoperationsclassified as avoidable were further subdividedinto 2 groups based on the nature of the error atinitial operation. These groups included technicalerrors and failure to adhere to current standards ofcare, or errors in judgment. When the same

SurgeryVolume 144, Number 6
Mitchell et al 901
patient had multiple reoperations, each was con-sidered a distinct reoperative instance and ana-lyzed separately. Additionally, when patients hadmultiple indications for reoperation (eg, persistenthyperparathyroidism and goiter), only the indica-tion related to the initial operation was used toclassify the case as avoidable or unavoidable.
For each hospital where the initial operationswere performed, publicly available hospital dis-charge data were used to determine the volume ofthyroid surgery and parathyroid surgery performedat each institution annually. Hospitals where <20operations were performed annually were classifiedas low-volume centers (LVC), and those performing$20 per year were classified as high-volume centers(HVC). Volume of thyroid operations and parathy-roid operations were considered separately in clas-sifying a center as high or low volume. For example,1 center could be high volume for thyroid opera-tions but low volume for parathyroid operations.The incidence of avoidable reoperations from LVCand HVC was determined. Statistical significancewas determined using the v2 or Fischer exact tests asappropriate (SigmaStat version 3.0; Systat Software,Inc., Chicago, Ill).
RESULTS
Study group. During the study period, 280patients underwent reoperative thyroid and para-thyroid procedures; 227 underwent 1 and 53
Table II. Summary of referring hospitals
Center typeNo. ofcenters
Annual casevolume Range
Thyroid casesHVC 10 21–50 24–49
2 51–100 52–764 >100 105–139
Total 16 81* 24–319LVC 12 <5 2–4
19 5–20 5–16Total 33 4* 1–15
Parathyroid casesHVC 1 21–50 48
2 51–100 53–671 >100 191
Total 4 90* 47–191LVC 32 <5 2–4
11 5–20 5–16Total 45 3* 1–12
Breakdown of referring hospitals by case volume, with thyroid andparathyroid volume considered separately. The cutoff for low and high-volume centers was #20 or >20 cases per year. Hospitals were furtherstratified based on volume into 5 groups.HVC, High-volume centers; LVC, low-volume centers.*Mean annual case volume.
patients underwent multiple reoperations, for atotal of 395 reoperative procedures. Reoperationsoriginating from our institution were included inthe analysis. The hospital where the initial opera-tion occurred was available for 335 (85%) of thesecases. The remaining 60 cases were excluded fromfurther analysis.
Referring hospital characteristics. Initial opera-tions occurred at 49 different hospitals. Of these, 33were classified as LVC (mean annual case volume, 4;range, 1--15), and 16 were classified as HVC (meanannual case volume, 81; range, 24--319) for thyroidoperations, and 45 were classified as LVC (meanannual case volume, 3; range, 1--12) and 4 classifiedas HVC (mean annual case volume, 90; range,47--191) for parathyroid operations. LVC averaged2 referrals during the study period, and HVCaveraged 3 referrals. Of the 49 referring hospitals,11 (22%) had high thyroid volume but low para-thyroid volume. No center had high parathyroidvolume and low thyroid volume. Table II summa-rizes volume characteristics of the referringhospitals.
Hospitals were further subdivided into 5 groups:those performing <5, 5--20, 21--50, 51--100, and>100 operations per year. When looking at thenumber of referrals from each group, this showeda downward trend as volume increased above 20cases per year. However, there was a spike inreferrals from institutions performing >100 casesannually. This can be explained by the relativelylarge number of cases in which the initial opera-tion was performed at our institution. To becertain no bias occurred, once the data wereaccumulated the institution name was replaced
Table III. Summary of case distribution
Number ofcases
Percent oftotal
Hospital volumeHigh 167 50Low 168 50
Type of reoperationThyroid 189 56Parathyroid 146 44
Reoperation classificationAvoidable 134 40Unavoidable 201 60
High-volume centerAvoidable reoperation 28 17Unavoidable reoperation 139 83
Low-volume centerAvoidable reoperation 106 63*Unavoidable reoperation 62 37*
*P < .001 versus high-volume centers.
SurgeryDecember 2008
902 Mitchell et al
with either HVC or LVC before analysis. Addition-ally, analysis was performed with and without casesfrom our institution excluded and there were nosignificant differences in the outcomes.
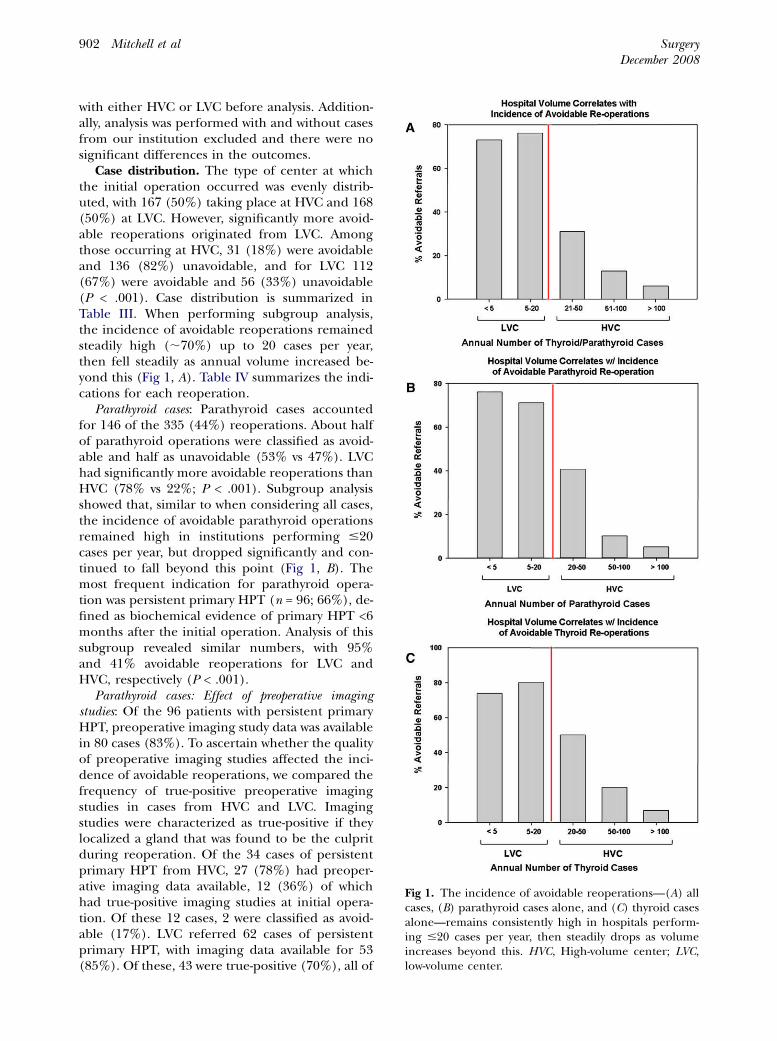
Case distribution. The type of center at whichthe initial operation occurred was evenly distrib-uted, with 167 (50%) taking place at HVC and 168(50%) at LVC. However, significantly more avoid-able reoperations originated from LVC. Amongthose occurring at HVC, 31 (18%) were avoidableand 136 (82%) unavoidable, and for LVC 112(67%) were avoidable and 56 (33%) unavoidable(P < .001). Case distribution is summarized inTable III. When performing subgroup analysis,the incidence of avoidable reoperations remainedsteadily high (;70%) up to 20 cases per year,then fell steadily as annual volume increased be-yond this (Fig 1, A). Table IV summarizes the indi-cations for each reoperation.
Parathyroid cases: Parathyroid cases accountedfor 146 of the 335 (44%) reoperations. About halfof parathyroid operations were classified as avoid-able and half as unavoidable (53% vs 47%). LVChad significantly more avoidable reoperations thanHVC (78% vs 22%; P < .001). Subgroup analysisshowed that, similar to when considering all cases,the incidence of avoidable parathyroid operationsremained high in institutions performing #20cases per year, but dropped significantly and con-tinued to fall beyond this point (Fig 1, B). Themost frequent indication for parathyroid opera-tion was persistent primary HPT (n = 96; 66%), de-fined as biochemical evidence of primary HPT <6months after the initial operation. Analysis of thissubgroup revealed similar numbers, with 95%and 41% avoidable reoperations for LVC andHVC, respectively (P < .001).
Parathyroid cases: Effect of preoperative imagingstudies: Of the 96 patients with persistent primaryHPT, preoperative imaging study data was availablein 80 cases (83%). To ascertain whether the qualityof preoperative imaging studies affected the inci-dence of avoidable reoperations, we compared thefrequency of true-positive preoperative imagingstudies in cases from HVC and LVC. Imagingstudies were characterized as true-positive if theylocalized a gland that was found to be the culpritduring reoperation. Of the 34 cases of persistentprimary HPT from HVC, 27 (78%) had preoper-ative imaging data available, 12 (36%) of whichhad true-positive imaging studies at initial opera-tion. Of these 12 cases, 2 were classified as avoid-able (17%). LVC referred 62 cases of persistentprimary HPT, with imaging data available for 53(85%). Of these, 43 were true-positive (70%), all of
Fig 1. The incidence of avoidable reoperations—(A) allcases, (B) parathyroid cases alone, and (C) thyroid casesalone—remains consistently high in hospitals perform-ing #20 cases per year, then steadily drops as volumeincreases beyond this. HVC, High-volume center; LVC,low-volume center.

SurgeryVolume 144, Number 6
Mitchell et al 903
which resulted in avoidable reoperations (100%;P < .001). Results of parathyroid are summarized inTable V.
Thyroid cases: Of 335 cases, 189 were thyroidreoperations (56%), divided evenly between LVCand HVC (46% vs 54%). Malignancy was the morecommon indication (134 cases; 71%); benign dis-ease accounted for 55 cases (29%). Reoperationsfor malignancy were also evenly distributed be-tween HVC and LVC (54% vs 46%), but similarly toparathyroid reoperations, the majority of avoidablethyroid reoperations came from LVC when looking
Table IV. Summary of indications for reoperation
Indication for reoperation No. of cases
Parathyroid reoperationsPersistent primary HPT 96
Single adenoma 60Double adenoma 8Hyperplasia 27
Recurrent primary HPT 15Persistent secondary HPT 3Recurrent secondary HPT 8Persistent tertiary HPT 2Recurrent tertiary HPT 1Unrelated to initial
operation (thyroidectomy)17
Parathyroid cancer 4Total 146
Thyroid reoperationsFTC/PTC after lobectomy for follicular
neoplasm by FNA27
Recurrent goiter—ipsilateral lobe 5Recurrent goiter—contralateral lobe 22Unrelated to initial
operation (parathyroidectomy)4
Recurrent CA in lymphnodes (undissected compartment)
29
Recurrent CA in lymphnodes (formally dissected compartment)
29
Recurrent CA in lymphnodes (selectively dissectedcompartment)
18
CA after partial thyroidectomy for benigndisease
15
Goiter/CA after partial thyroidectomy withknown history of ionizing radiation
9
Thyroidectomy/neck dissectionafter excisional biopsyof neck masswithout FNA
14
Completion thyroidectomyafter incomplete resectionfor known CA
17
Total 189
CA, Cancer; FNA, fine needle aspiration; FTC, follicular thyroid cancer;HPT, hyperparathyroidism; PTC, papillary thyroid cancer.
at all thyroid cases (43 of 57 [75%];P < .001), and reoperations for malignancy (35 of43 [81%]; P < .001). There was no significant dif-ference in the incidence of avoidable thyroid reop-erations between HVC and LVC for benign disease(19% vs 33%). The distribution of thyroid reoper-ations is summarized in Table VI. Here also, avoid-able thyroid reoperations steadily declined withgreater hospital volume (Fig 1, C).
Etiology of avoidable reoperations. Whenconsidering all cases, avoidable reoperations atHVC were due to errors in judgment (68%)more frequently than technical errors (32%),whereas at LVC errors in judgment (51%) andtechnique (49%) were equally responsible (P =.166). When looking at parathyroid reoperationsalone, technical errors were responsible for themajority of avoidable reoperations from bothHVC and LVC (64% and 76%, respectively),whereas judgment errors were responsible formost avoidable thyroid reoperations from bothcenters (100% and 91%, respectively; P < .001;Table VII).
To examine whether thyroid volume affectedthe incidence of avoidable parathyroid reopera-tions, we analyzed the 18 referrals from hospitalswith high thyroid volume but low parathyroidvolume. Of these, 14 (78%) were classified asavoidable, and 4 (22%) as unavoidable. Thesenumbers were similar to those obtained whenconsidering all parathyroid.
Complications. Because all thyroid and parathy-roid reoperations at our institution are precededby direct laryngoscopy to assess vocal cord func-tion, we were able to compare the incidence ofRLN injury after initial operations from HVC andLVC. Operations performed at LVC resulted inRLN injury in 15 patients (9%). This was signifi-cantly higher than seen after operations per-formed at HVC, where 5 patients suffered RLNinjuries (3%; P < .05; Fig 2). The overall complica-tion rate after reoperations was 4%, with the spe-cific complications summarized in Table VIII.This was significantly higher than the rest of ourpatient population with a complication rate of 1%.
DISCUSSION
To our knowledge, this is the first study lookingat the incidence of avoidable reoperations inthyroid and parathyroid surgery and how it relatesto hospital volume. It is also the first study topropose a set of objective criteria with which toclassify thyroid and parathyroid operations asavoidable or unavoidable. Although it may seem

SurgeryDecember 2008
904 Mitchell et al
as though the indications for parathyroid andthyroid reoperations may be widely variable, theset of 10 criteria for parathyroid cases and 8 forthyroid cases developed here encompassed all ofthe thyroid and parathyroid reoperations per-formed at this institution over a 9-year period,allowing us to objectively and reliably determinewhether or not such cases were avoidable. Addi-tionally, although the ability to objectively classifycases in this manner may not have practical clinicalutility for a particular patient, the existence of thistype of classification system allows such an analysisto be performed. This, in turn, provides objectivedata, which speak to where patients needing sur-gical care for thyroid and parathyroid disease will
Table V. Distribution of parathyroid reoperations
Type of case HVC LVC Difference
All cases 64 (100%) 82 (100%)Avoidable 14 (22%) 63 (78%)
TE 9 (64%) 48 (76%)JE 5 (36%) 15 (24%)
Unavoidable 50 (78%) 19 (22%) 56%*Persistent primary
HPT34 (100%) 62 (100%)
Avoidable 14 (41%) 59 (95%)TE 9 (64%) 47 (80%)JE 5 (36%) 12 (20%)
Unavoidable 20 (59%) 3 (5%) 54%*TP imaging 12 (36%) 43 (70%) 34%y
HPT, Hyperparathyroidism; HVC, high-volume center; JE, error in judg-ment; LVC, low-volume center; TE, technical error; TP, true positive imag-ing study.*P < .001.yP < .01.
Table VI. Distribution of thyroid reoperations
Type of case HVC LVC Difference
All cases 103 86Avoidable 14 (14%) 43 (50%)
TE 0 (0%) 4 (9%)JE 14 (100%) 39 (91%)
Unavoidable 89 (86%) 43 (50%) 36%*Malignancy 72 62
Avoidable 8 (11%) 35 (56%)TE 0 (0%) 3 (9%)JE 8 (100%) 32 (91%)
Unavoidable 64 (89%) 27 (44%) 55%*Benign disease 31 24
Avoidable 6 (19%) 8 (33%)TE 0 (0%) 1 (12%)JE 6 (100%) 7 (88%)
Unavoidable 25 (81%) 16 (67%) 14%NS
JE, Error in judgment; NS, not significant; TE, technical error.*P < .001.
best be served. It can also serve to guide qualitycontrol assessments, and a hospital can identifyspecific targets for improvement.
It is important to note that, although our directmeasure of outcome is by hospital experience witha particular operation, this likely reflects surgeonexperience as well, indirectly. Such an assumptionhas limitations; surgeons who perform high-vol-ume thyroid surgery may perform only a few ofthese cases per year at a particular low-volumehospital, creating a false perception. However, it isa reasonable assumption that most cases per-formed at LVC are by surgeons who perform fewof these cases, and vice versa. Data to support thisassumption has been recently presented at anational surgical meeting (Sosa et al, unpublisheddata from the Annual Meeting of the AmericanAssociation of Endocrine Surgeons, Monterey,California, April 6--8, 2008. Paper entitled ‘‘Pedi-atric endocrine surgery: Who is operating on ourchildern?’’). Additionally, such a scenario where asingle surgeon might perform 18 operations at aLVC versus 5 surgeons performing 23 operationsat a HVC could only exist near the 20 case-per-year cutoff. This is not a realistic scenario inHVC performing >100 cases per year, where themost significant difference in outcomes are seen(Fig 1, A–C).
Our data show that, although the number ofreferrals for thyroid reoperations and parathyroidoriginated from HVC and LVC in equal numbersin our patient population, the vast majority ofavoidable reoperations came from the LVC, sug-gesting a clear association between volume ofsurgery and outcome. This study lends support tothe data by Sosa et al10 and Pieracci et al,11 show-ing that, although only for thyroidectomy, lengthof stay, morbidity, and mortality decreased with
Table VII. Etiology of avoidable reoperations
Reason for reoperation
Type of center Error in judgment Technical error
All casesHVC 68% 32%LVC 51% 49%
Parathyroid casesHVC 36%* 64%LVC 24%y 76%
Thyroid casesHVC 100% 0%LVC 91% 9%
HVC, High-volume centers; LVC, low-volume centers.*P < .05 versus thyroid cases.yP < .001 versus thyroid cases.

SurgeryVolume 144, Number 6
Mitchell et al 905
increasing surgeon and hospital experience. Ourcurrent work addresses all types of cervical endo-crine surgery from the novel perspective of utiliz-ing the incidence of avoidable reoperation as ameasure of outcome, but our data contribute fur-ther tangible evidence to suggest that thyroidand parathyroid surgery should be performed atHVC.
Because nationwide diseases and surgery of thethyroid are more prevalent than of the parathy-roid, this may be reflected by a difference inavoidable reoperation rates. This was not the casein our patient population, however. LVC hadsignificantly more avoidable reoperations thanHVC among both thyroid and parathyroid opera-tions, and the mean annual volume at LVC wasequally low for thyroid and parathyroid operations(4 and 3 cases per year, respectively). Even moresignificantly, our data show that experience withthyroid surgery does not affect outcomes in para-thyroid operations, because centers performinghigh-volume thyroid surgery but low-volume para-thyroid surgery still had a significantly higherincidence of avoidable parathyroid reoperations.When LVC perform very few cases annually, thisrelative lack of experience translates into signifi-cantly poorer outcomes for both thyroid andparathyroid operations. They also suggest thatsurgical experience is disease specific with respectto this particular outcome measure.
Lack of experience may lead to avoidablereoperations by several mechanisms. One is dimin-ished or poorly developed technical skills, andanother is lack of familiarity with current standardsof care for more specialized diseases. The few
Fig 2. The incidence of recurrent laryngeal nerve(RLN) injury after initial operations at high- (HVC)and low-volume centers (LVC) in patients undergoingthyroid and parathyroid reoperations.
thyroid or parathyroid operations that a typicalgeneral surgeon performs annually represents arelatively small fraction of an overall busy practice.It may be more challenging for those with ageneralized practice to stay current in a particularsubspecialty area, which might contribute to errorsin technique or judgment, leading to reoperation.Our series hints at this concept because avoidablereoperations from LVC were due equally to errorsin judgment and technique, whereas those fromHVC were primarily judgment errors. However,when looking at thyroid and parathyroid casesseparately, avoidable thyroid reoperations weredue mainly to errors in judgment and avoidableparathyroid were due primarily to technical errorsfrom both centers. It may be the case that first-timethyroid surgery is more challenging in terms ofpreoperative decision making and first-time para-thyroid surgery is more technically challenging,and that level of experience dictates how fre-quently those challenges will be successfully met.
Although lower than LVC, the incidence ofavoidable reoperations for persistent primaryHPT was higher than expected. In an attempt toexplain these findings, we looked at the preoper-ative imaging studies of these cases. LVC had initialtrue-positive localizing studies much more oftenthan HVC. This disparity may reflect more com-plex patients seen at HVC, as cases of multiglanddisease are more likely to have negative sestamibiscans. Additionally, the HVC performing the fewestcases (21--50) were responsible for the majority ofthe avoidable parathyroid reoperations.
Table VIII. Summary of complications afterreoperation
Complication No. of cases
Readmission for hypocalcemia 6Hypoxia/MS changes
requiring ICU admission1
Infected hematomarequiring reoperation
1
Hematoma requiringoffice drainage
1
Lymphatic leakrequiring re-operation
3
Hypoglossal nerve palsy 1Upper extremity DVT 1Seroma requiring
office drainage 321
Recurrent laryngealnerve injury
1
Total 16
DVT, Deep venous thrombosis; ICU, intensive care unit; MS, mentalstatus.

SurgeryDecember 2008
906 Mitchell et al
We did not calculate the specific costs to thepatient, but one can appreciate the impact ofpotentially avoidable surgery on many areas. Theseinclude financial costs, the emotional impact ofreoperation, and the additional risk exposure tosignificant complications impacting quality of life.Complication rates in our reoperation patientswere significantly higher than our other patientsduring the study period. The rate of RLN injuryafter initial operations from LVC was also muchhigher than those from HVC. These costs add upto a significant burden both on the patient andsociety in general in terms of unnecessary utiliza-tion of health care resources.
In conclusion, an objective set of criteria canreliably be used to classify thyroid and parathyroidreoperations as avoidable or unavoidable. Usingsuch a classification system, we have shown thatsignificantly more thyroid and parathyroid reoper-ations originating from LVC are avoidable com-pared with those performed at HVC. Suchavoidable reoperations impose a significant bur-den on both the patient and society in general,and any means to minimize this would be of greatbenefit. This study provides additional evidence toadvocate the practice of concentrating surgicaltreatment of such detail-oriented specialties asthyroid and parathyroid disease to HVC. Theimplications for future practice patterns with re-spect to surgeons, referring physicians, hospitals,insurers, and patients are enormous.
REFERENCES
1. Becker WF. Presidential address: pioneers in thyroidsurgery. Ann Surg 1977;185:493-504.
2. Dubose J, Ragsdale T, Morvant J. ‘‘Bodies so tiny’’: the his-tory of parathyroid surgery. Curr Surg 2005;62:91-5.
3. Edis AJ. Prevention and management of complications asso-ciated with thyroid and parathyroid surgery. Surg ClinNorth Am 1979;59:83-92.
4. Harness JK, Fung L, Thompson NW, et al. Total thyroidec-tomy: complications and technique. World J Surg 1986;10:781-6.
5. Gordon TA, Burleyson GP, Tielsch JM, Cameron JL. The ef-fects of regionalization on cost and outcome for one gen-eral high-risk surgical procedure. Ann Surg 1995;221:43-9.
6. Hannan EL, O’Donnell JF, Kilburn H Jr, et al. Investigationof the relationship between volume and mortality for surgi-cal procedures performed in New York State hospitals.JAMA 1989;262:503-10.
7. Lieberman MD, Kilburn H, Lindsey M, Brennan MF. Rela-tion of perioperative deaths to hospital volume among pa-tients undergoing pancreatic resection for malignancy.Ann Surg 1995;222:638-45.
8. Jollis JG, Peterson ED, DeLong ER, et al. The relation be-tween the volume of coronary angioplasty procedures athospitals treating Medicare beneficiaries and short-termmortality. N Engl J Med 1994;331:1625-9.
9. Lavernia CJ, Guzman JF. Relationship of surgical volumeto short-term mortality, morbidity, and hospital charges inarthroplasty. J Arthroplasty 1995;10:133-40.
10. Sosa JA, Bowman HM, Tielsch JM, et al. The importance ofsurgeon experience for clinical and economic outcomesfrom thyroidectomy. Ann Surg 1998;228:320-30.
11. Pieracci FM, Fahey III TJ. Effect of hospital volume of thy-roidectomies on outcomes following substernal thyroidec-tomy. World J Surg 2008;32:740-6.
12. Stavrakis AI, Ituarte PH, Ko CY, Yeh MW. Surgeon volume asa predictor of outcomes in inpatient and outpatient endo-crine surgery. Surgery 2007;142:887-99.
13. Kouvaraki MA, Lee JE, Shapiro SE, et al. Preventable reop-erations for persistent and recurrent papillary thyroid carci-noma. Surgery 2004;136:1183-91.
14. Cooper DS, Doherty GM, Haugen BR, et al. Managementguidelines for patients with thyroid nodules and differenti-ated thyroid cancer. Thyroid 2006;16:109-42.
15. The American Association of Clinical Endocrinologists andthe American Association of Endocrine Surgeons positionstatement on the diagnosis and management of primaryhyperparathyroidism. Endocr Pract 2005;11:49-54.
DISCUSSION
Dr Richard A. Hodin (Boston, Mass): I guess it may bean obvious point, but there clearly could be selectionbias here. And your conclusion may be absolutely true,but, on the other hand, it is possible that the high vol-ume centers keep their avoidable operations and redothem there and they don’t come to the Cleveland Clinic,and that would explain the differences. Is that not true?
Dr Jamie C. Mitchell (Cleveland, Ohio): Thank youfor your question, Dr Hodin. Analyzing reoperations asavoidable or unavoidable is a form of outcomes measure-ment that has not yet been looked at in endocrine sur-gery. I think you are correct that there is some degreeof referral bias inherent in this type of analysis. Thereis no way to know the status of the reoperations thatare not referred to us, as you point out. It is possiblethat all avoidable reoperations from high-volume centersare not referred to other institutions, whereas thosefrom low-volume centers are referred out more fre-quently, thus skewing the data. It is more likely, I think,that in general high-volume centers manage their ownreoperations, avoidable or unavoidable, themselves.The patients we are seeing are referred to us for a varietyof reasons from high-volume centers, such as changes ininsurance, patient preference, patient relocation, pri-mary care physician or endocrinologist recommenda-tions, and so on, and are, I think, a representativegroup of patients from high-volume centers, and there-fore a valid population with which to perform thisanalysis.
I think that is possible. As we had talked about withprevious studies and previous presentations, as you haveseen today, there have been studies that have looked atmore traditional outcome measures in endocrine sur-gery, meaning length of stay, costs, complication rate,and so on. And again, given our personal practice, Ithought this would be an interesting way to look at

SurgeryVolume 144, Number 6
Mitchell et al 907
another outcomes measure. But you make a good point,there could definitely be referral selection bias here.
Dr Keith S. Heller (New York, NY): I wonder if youcould be more specific about the types of things you clas-sified as avoidable. ‘‘Avoidable’’ implies to me at least amistake. Is a recurrence in the central compartment af-ter an operation for a known thyroid cancer an avoid-able recurrence? Because that is not necessarily amistake of inexperience, that is a treatment decision. Isrecurrent or persistent hyperparathyroidism after a fo-cused exploration where the focused exploration wasdone properly and the PTH dropped, is that avoidableor unavoidable?
Dr Jamie C. Mitchell (Cleveland, Ohio): Thank youfor your question, Dr Heller. In the interest of time, Idid not show a full list of our criteria for classifying oper-ations as avoidable or unavoidable. To answer your spe-cific questions, a recurrence in the centralcompartment after total thyroidectomy in the absenceof clinically apparent adenopathy would represent anunavoidable reoperation. Persistent hyperparathyroid-ism after a focused exploration based on preoperativeimaging with an appropriate drop in intraoperativePTH measurements would also represent an unavoid-able reoperation. Although there may be certain situa-tions where different surgeons may take exception tosome of the criteria we used, I feel we avoided classifyingreoperations as avoidable where there currently existssignificant controversy in management. A figure listingall these criteria will be included in the manuscript(Table I).
That is a great question. I didn’t list all of ourcriteria. Could I have slides back up? I have a slidethat shows those criteria. I suspect that people mightwant to see those. But to answer your question ofspecific situations that you gave, no, those would nothave been classified as avoidable. For example, if youhave done a formal dissection, formal anatomic lymphnode dissection for cancer, for example, and still hada nodal recurrence, that would not be classified as anavoidable reoperation. I guess I can’t show you thatentire list. It would take some time to run throughthem all. But it would be interesting for people to seeexactly what we use; I just didn’t feel we could showthem all. And I am sorry that I can’t show them to youon the slides.
Dr Julie Ann Sosa (New Haven, Conn): Three briefquestions. First of all, to follow-up on Dr Heller’s ques-tion, I think a lot of us in the audience hear ‘‘avoidable’’and take that to mean that there was an error in judg-ment or technique made, which has obvious medicolegalimplications. So I wonder, first of all, what are the med-icolegal implications of your study and are these findingsdiscoverable? Second, in follow-up to that point, I guess,you talked a lot about hospital volume. Did you look atsurgeon volume? Because what you are looking at wasavoidable and unavoidable findings are actually deci-sions that are being made in the operating room andthey are not really proxies for hospital and system-widemeasures. A third question is, was there a consensus de-cision made across 1, 2, or 3 expert surgeons about whatconstituted an avoidable or unavoidable mistake?
Dr Jamie C. Mitchell (Cleveland, Ohio): Thank youfor your questions, Dr Sosa. I do not feel these findingsare in any way discoverable. As far as the medicolegal im-plications, I think there are more important implicationsfor insurers, as again, this study lends support to previ-ous studies already mentioned, suggesting that the man-agement of these highly specialized diseases should beconcentrated at high-volume centers where high-vol-ume, experienced surgeons practice.
There certainly are previous papers, such as your ownfrom 2004 looking at outcomes after thyroidectomy, thathave shown that surgeon volume but not hospital volumeaffected outcomes. Again, the outcome measures ana-lyzed were more traditional, such as cost, length of stay,and complications. Certainly in this study, which usesincidence of avoidable reoperations as an outcome mea-sure, the important variable is the surgeon. So why did weuse hospital volume? We did not have the volume of theindividual referring surgeons available to us, so we usedhospital volume as an indirect measure of surgeon vol-ume. This is an assumption, obviously, but we feel it to be avalid one. It is intuitive that high-volume surgeons arerarely going to perform a few operations at a low-volumecenter. There are actually data to support that in aprevious presentation today, that most high-volume sur-geons are operating at high-volume centers. But again, it isan assumption that is being made. To answer the firstquestion, the initial analysis was performed by 1 personand then was reviewed by multiple members of the team ofexpert surgeons and a consensus was arrived at.