av nodal conduction system stress test
TRANSCRIPT

Paul A. Levine MD, FHRS, FACC, CCDS
Professor of Medicine
Loma Linda University School of Medicine
Clinical Associate Professor of Medicine
University of California, Los Angeles
AV Nodal Conduction System
Stress Test
Based on: Levine PA, The AV Nodal Conduction System Stress Test, Arrhythmia
Grand Rounds, 2014: 1: ………………………….

Clinical History
63 year old male presents with repeated weak
spells and pre-syncope
Following diagnosis of sinus node
dysfunction, implantation of a dual chamber
pacing system is recommended and proceeds
in an uncomplicated manner.
The implanted pulse generator is Medtronic
Advisa™ A2DR01

Managed Ventricular Pacing
(MVP):
MVP is the default pacing mode in the Medtronic
pacemakers
It provides functional single chamber atrial pacing
in the absence of AV block
If AV block develops, there needs to be 2:1 second
degree AV block for four cycles or higher levels of
AV block before it will disable functional single
chamber atrial pacing in favor of the DDD mode
After a period of time in the DDD mode, the
algorithm withholds the ventricular output to
determine if AV block persists or has resolved

Clinical History (cont)
The patient reports that the pre-syncopal
episodes have resolved but some weak spells
persist.
At follow-up, capture and sensing thresholds
are stable, there have been no
tachyarrhythmias and there is only 1%
ventricular pacing with the system in the MVP
mode.
Questions
Can the persistent symptoms be due to the
pacing system?
How might this be evaluated?

Evaluation
The excellent capture and sensing thresholds
make an early lead problem unlikely
The baseline rhythm:

Evaluation (cont):
There is a mild first degree AV block but this
would not be expected to be symptomatic
Could there be intermittently higher levels of
AV block?
How might intermittent AV block be
evaluated?
Holter or Event Monitor
Formal EP study assessing AV conduction
Bedside AV Nodal Conduction System Stress
Test

AV Nodal Conduction System Stress test
To determine if it is safe to program the
pacemaker to the fixed or functional single
chamber atrial pacing mode (AAI), it is necessary
to assess the status of the AV conduction system.
AV Nodal Conduction Stress Test Pace AAI at progressively higher rates
Intact AV conduction to atrial paced rates of > 120 ppm
Since this test is performed at rest, there will not
be the increased circulating catecholamine levels
that are present during physical activity Hence Wenckebach AV block may occur at atrial paced rates
that would not occur during physical exercise

AAI pacing at 100 bpm
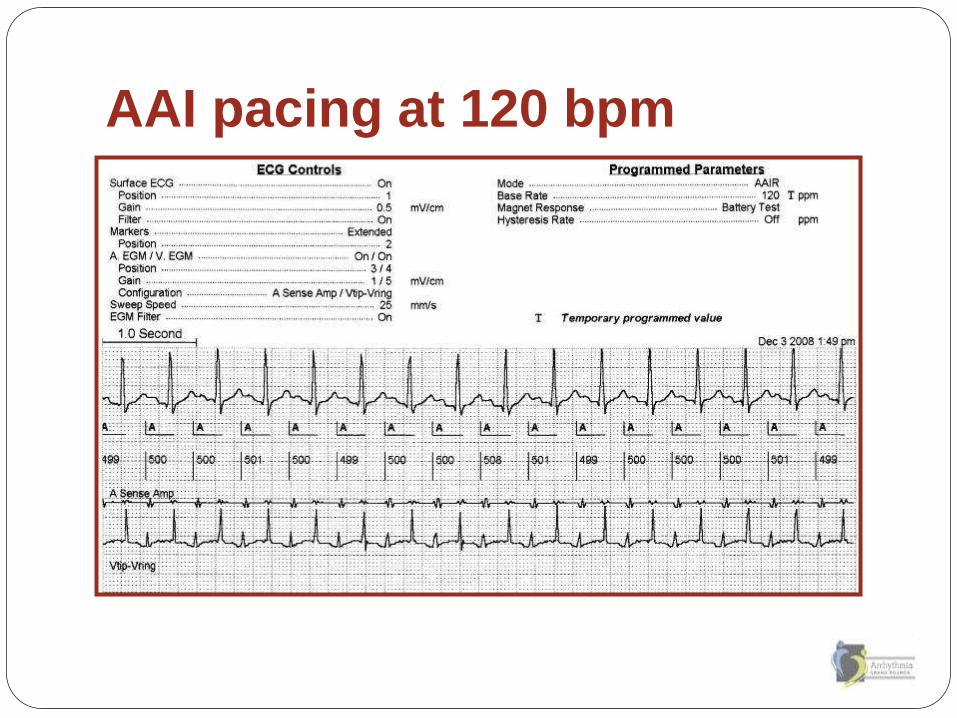
AAI pacing at 120 bpm
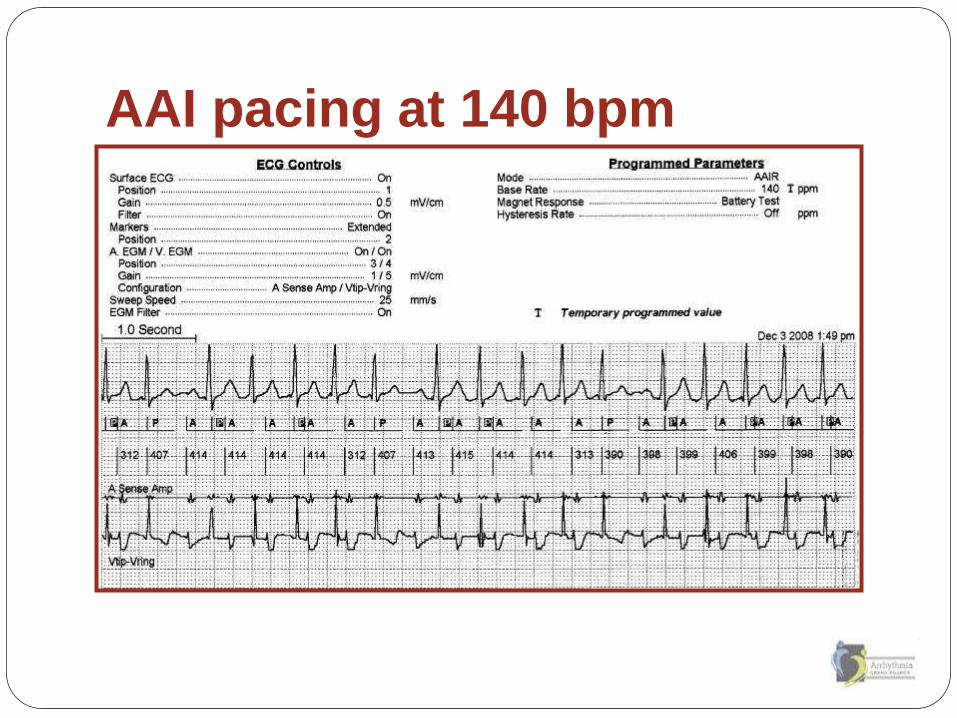
AAI pacing at 140 bpm

Question
What is the cause of the pause during AAI
pacing at 140 ppm?
A. Wenckebach 2nd degree AV block
B. First degree AV block
C. First degree AV block with FFRW sensing
D. Atrial oversensing
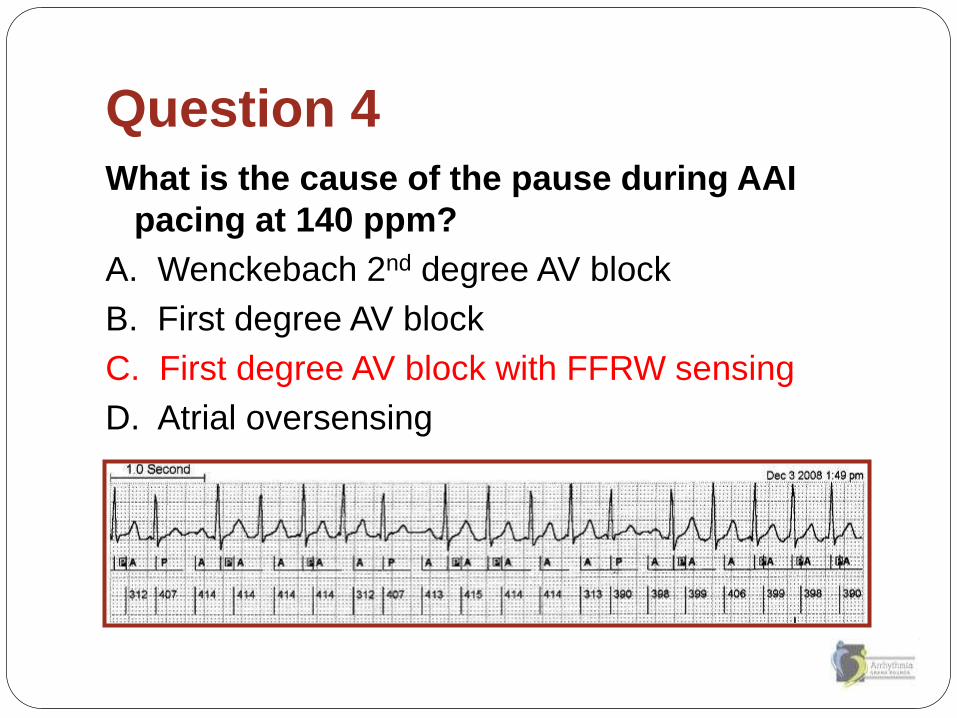
Question 4
What is the cause of the pause during AAI
pacing at 140 ppm?
A. Wenckebach 2nd degree AV block
B. First degree AV block
C. First degree AV block with FFRW sensing
D. Atrial oversensing

Programming High Rates in the
Medtronic Pacemakers
Program to the AAI mode and a high rate
When evaluation completed, need to reprogram
the pacemaker to the desired parameters
Utilize the Capture Threshold test
This is performed in a temporary mode such
that when ended, the mode and rate go back to
the baseline
In DDD mode, highest allowed rate is 120 bpm
In AAI mode, highest allowed rate is 175 bpm
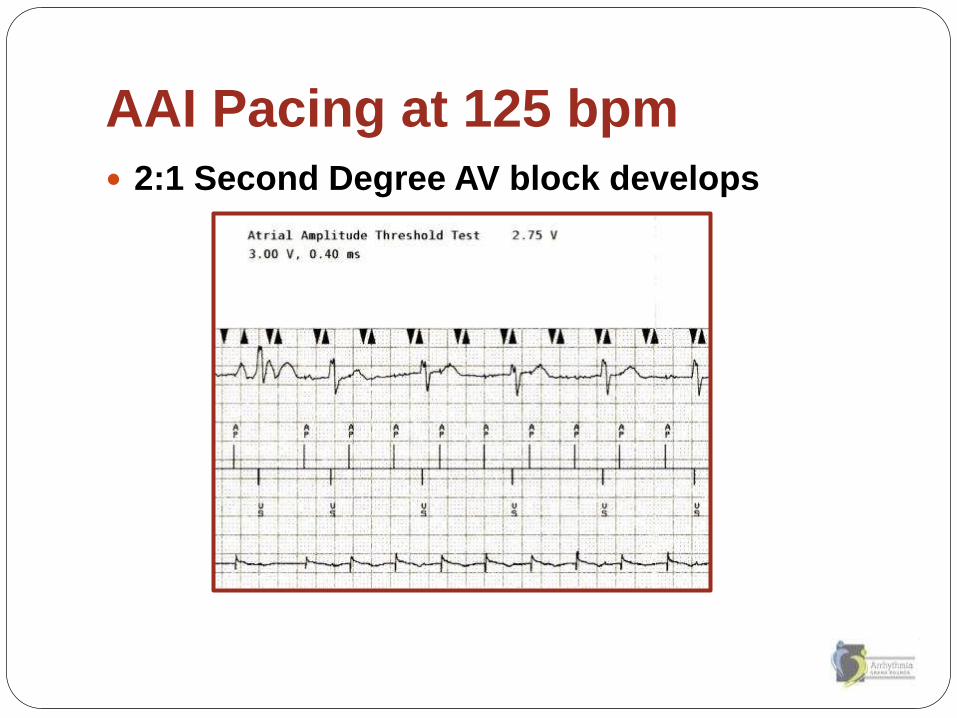
AAI Pacing at 125 bpm
2:1 Second Degree AV block develops

Management
Intermittent low grade AV block could explain
his continued weak spells
Disable MVP mode in favor of DDDR
combined with the Search AV+ hysteresis
algorithm
Reassess in 1 to 3 months
If symptoms resolved, patient has intermittent
AV block in addition to sinus node dysfunction
If symptoms persist, need to continue to
evaluate

Management
When ever programming to the fixed AAI
mode or the functional AAI mode, it is prudent
to assess the status of the AV nodal
conduction system at each follow-up visit.
This patient called the office two weeks after
having been seen and his pacemaker
programmed to report total resolution of his
intermittent weak spells.
