autonomic dysfunction in parkinson's disease and its ...jultika.oulu.fi › files ›...
TRANSCRIPT
AUTONOMIC DYSFUNCTION IN PARKINSON'S DISEASE AND ITS CORRELATES TO MEDICATION AND DOPAMINE TRANSPORTER BINDING
TARJAHAAPANIEMI
Department of Neurology,University of Oulu
Department of Clinical Neurophysiology,University of Oulu
OULU 2001
TARJA HAAPANIEMI
AUTONOMIC DYSFUNCTION IN PARKINSON'S DISEASE AND ITS CORRELATES TO MEDICATION AND DOPAMINE TRANSPORTER BINDING
Academic Dissertation to be presented with the assent ofthe Faculty of Medicine, University of Oulu, for publicdiscussion in the Auditorium 8 of the University Hospitalof Oulu, on May 4th, 2001, at 12 noon.
OULUN YLIOPISTO, OULU 2001
Copyright © 2001University of Oulu, 2001
Manuscript received 9 April 2001Manuscript accepted 17 April 2001
Communicated byProfessor Reijo MarttilaDocent Seppo Kaakkola
ISBN 951-42-5963-7 (URL: http://herkules.oulu.fi/isbn9514259637/)
ALSO AVAILABLE IN PRINTED FORMATISBN 951-42-5962-9ISSN 0355-3221 (URL: http://herkules.oulu.fi/issn03553221/)
OULU UNIVERSITY PRESSOULU 2001


Haapaniemi, Tarja, Autonomic dysfunction in Parkinson's disease and its correlatesto medication and dopamine transporter binding Department of Neurology, University of Oulu, P.O.Box 5000, FIN-90014 University of Oulu,Finland, Department of Clinical Neurophysiology, University of Oulu, P.O.Box 5000, FIN-90014University of Oulu, Finland 2001Oulu, Finland(Manuscript received 9 April 2001)
Abstract
Patients with idiopathic Parkinson's disease (PD) may suffer from autonomic nervous systemdysfunction even in the early phase of the disease. We assessed the autonomic cardiovascular andsudomotor regulation in de novo PD patients with and without medication. We also measured thedopamine (DAT) and serotonin transporter (SERT) uptake in the PD patients using 2?-carboxymethoxy-3?-(4-iodophenyl)tropane (?-CIT) SPECT and studied the clinical correlates of theuptake. Sixty PD patients were included in the study and randomised to receive levodopa,bromocriptine or selegiline (n=20 in each) as their treatment. Thirty patients were examined with ?-CIT SPECT. The results of the patients were compared with those of healthy controls and within thesubgroups at different time points.
Cardiovascular autonomic regulation was assessed using standard cardiovascular reflex tests atbaseline, after six months' medication and following a 6-week washout period. The heart rate (HR)and blood pressure (BP) regulation was impaired in PD patients at baseline, and PD medicationsmodified the responses further. Bromocriptine and selegiline, in contrast to levodopa, increased theorthostatic BP fall and suppressed the BP response to isometric exercise. The long-termcardiovascular autonomic function was evaluated from ambulatory ECG recordings by analysis oftraditional spectral and non-spectral components of HR fluctuation together with two-dimensionalvector analysis and power-law relationship analysis of the HR dynamics. All spectral measures andthe slope of the power-law relationship demonstrated impaired tonic cardiovascular regulation in thePD patients.
Sympathetic sudomotor activity was evaluated using the sympathetic skin response (SSR). Themajor finding was suppression of the SSR amplitudes with an inverse correlation to clinical disability,whereas PD medication seemed to have only minor effects. The changes in amplitude andrepetitiveness of the SSRs with normal adaptation suggest deficits at several levels of the SSR reflexarc.
DAT uptake, assessed by ?-CIT SPECT, was diminished in the striatum and especially theputamen of the PD patients, and correlated with the results of the cardiovascular reflex tests andambulatory ECG recordings. Simultaneous measurement of SERT binding demonstrated decreasedSERT availability in the thalamic and frontal areas.
The results demonstrate disturbances of the reflectory and tonic cardiovascular autonomicregulation caused by PD itself. PD medications further modify the reflectory responses. Thedegenerative process in PD also involves the sympathetic sudomotor pathway. ?-CIT SPECTprovides a useful method for simultaneous assessment of DAT and SERT binding, demonstratingthe deficit of serotonin metabolism in PD.
Keywords: blood pressure, Parkinson disease, autonomic nervous system, heart rate, gal-vanic skin response, monoamine transporter


To my family, especially Salla

Acknowledgements
This work was carried out in the Departments of Neurology and Clinical Neurophysiology, University of Oulu, during the years 1995-2001.
I wish to express my sincere gratitude to Decane Vilho Myllylä, M.D., Head of the Faculty of Medicine, for being my teacher and supervisor both in the clinical and scientific work from the beginning of my working career in the Department of Neurology. I thank him for his excellent guidance and support throughout the years of the study. I am also deeply grateful to Docent Kyösti Sotaniemi, M.D., for his tireless support, excellent advises and constructive critic that was essential for the accomplishment of the scientific work.
My warm thanks are also due to Docent Uolevi Tolonen, M.D., for the optimistic attitude during this study and for the invaluable help in the neurophysiological assessments used in the present study. I also express my gratitude to Docent Juha Korpelainen, M.D., who provided his practical advices and encouragement when most needed to put this project forward.
I owe my thanks to Professor Aapo Ahonen, M.D., Pentti Torniainen, M.Sc. and Aki Pulkkinen, R.N., for their expert help in the SPECT imaging work and to Professor Heikki Huikuri, M.D., and Pirkko Huikuri, R.N, for their excellent guidance in the field of heart rate variability analysis. It is also a great pleasure to thank my co-writers Mika Kallio, M.D., Kalervo Suominen, M.Sc., and Ville Pursiainen, M.S., and colleagues at our research group for inspiring conversations and the good spirit for scientific work.
I’m very grateful to Professor Matti Hillbom, M.D., for placing the research facilities for the study.
I am indebted to Professor Reijo Marttila, M.D., and Docent Seppo Kaakkola, M.D., for their constructive criticism and advice during the preparation of the final manuscript. I also wish to thank Ian Morris-Wilson, M.A., Ph.D. for excellent and skilful revising of the English language of the manuscript.
I wish to thank the whole staff of the Departments of Neurology and Clinical Neurophysiology for their excellent co-operation through the years of the study. I also wish to express my sincere gratitude to the patients and their families who made this work possible.
I thank all my friends for the support that has helped me to continue this work during these years. Finally, my warmest thanks are expressed to my daughter, Salla, for her love

and patience during the years of this study, and my parents, Sanelma and Reino, and my sister, Taina for their everlasting support and interest in my work.
This study was supported by the Finnish Neurological Foundation, the Maire Taponen Foundation and the Finnish Parkinson Association. Oulu, April 2001 Tarja Haapaniemi
Abbreviations
ANS autonomic nervous system β-CIT 2β-carboxymethoxy-3β-(4-iodophenyl)tropane BP blood pressure BPI binding potential index CNS central nervous system DAT dopamine transporter ECG electrocardiogram HF high frequency HR heart rate HRV heart rate variability LF low frequency MSA multiple system atrophy OWM occipital white matter PAF pure autonomic failure PD Parkinson’s disease PET positron emission tomography RMMSD square root of the mean squares of the differences between the
successive RR intervals ROI region-of-interest SD standard deviation SD1 instantaneous beat to beat RR interval variability SD2 long-term continuous RR interval variability SERT serotonin transporter SDNN SD of all RR intervals SPECT single photon emission computed tomography SSR sympathetic skin response UPDRS Unified Parkinson’s Disease Rating Scale VLF very low frequency
List of original articles
This thesis is based on the following articles, which are referred to in the text by their Roman numerals:
I Haapaniemi TH, Kallio MA, Korpelainen JT, Suominen K, Tolonen U, Sotaniemi KA & Myllylä VV (2000) Levodopa, bromocriptine, and selegiline modify cardiovascular responses in Parkinson’s disease. Journal of Neurology 415: 868-874.
II Haapaniemi TH, Pursiainen V, Korpelainen JT, Huikuri HV, Sotaniemi KA & Myllylä VV (2001) Ambulatory ECG and analysis of heart rate variability in Parkinson’s disease. Journal of Neurology Neurosurgery and Psychiatry, 70: 305-310.
III Haapaniemi TH, Korpelainen JT, Tolonen U, Suominen K, Sotaniemi KA & Myllylä VV (2000) Suppressed sympathetic skin response in Parkinson’s disease. Clinical Autonomic Research, 10: 337-342.
IV Haapaniemi TH, Ahonen A, Torniainen P, Sotaniemi KA & Myllylä VV (2001) [123I]β-CIT SPECT demonstrates decreased brain dopamine and serotonin transporter levels in untreated parkinsonian patients. Movement Disorders, 16: 124-130.

Contents
Abstract Acknowledgements Abbreviations List of original articles 1 Introduction................................................................................................................... 15 2 Review of the literature................................................................................................. 17
2.1 Autonomic nervous system .................................................................................... 17 2.1.1 Autonomic nervous system anatomy............................................................... 17 2.1.2 Cardiovascular autonomic control................................................................... 18 2.1.3 Sudomotor regulation...................................................................................... 21
2.2 Parkinson’s disease................................................................................................. 23 2.2.1 Epidemiology, pathology and etiology............................................................ 23 2.2.2 Medication ...................................................................................................... 25
2.3 Autonomic dysfunction in Parkinson’s disease ...................................................... 26 2.3.1 Clinical aspects ............................................................................................... 26 2.3.2 Cardiovascular dysfunction............................................................................. 27 2.3.3 Sudomotor dysfunction ................................................................................... 28 2.3.4 Effects of antiparkinsonian medication on cardiovascular
and sudomotor autonomic functions ............................................................... 29 2.4 Evaluation of autonomic functions......................................................................... 30
2.4.1 General aspects ............................................................................................... 30 2.4.2 Cardiovascular autonomic reflexes ................................................................. 30 2.4.3 Ambulatory ECG and analysis of heart rate variability................................... 32 2.4.4 Sudomotor functions ....................................................................................... 33
2.5 Functional brain receptor imaging in Parkinson’s disease ..................................... 34 3 Aims of the study .......................................................................................................... 36 4 Subjects and methods.................................................................................................... 37
4.1 Subjects .................................................................................................................. 37 4.2 Methods.................................................................................................................. 39
4.2.1 Clinical examination ....................................................................................... 39 4.2.2 Cardiovascular autonomic reflex tests (Study I) ............................................. 40 4.2.3 Heart rate variability analysis (Study II) ......................................................... 41
4.2.3.1 ECG recordings........................................................................................ 41 4.2.3.2 Time domain and spectral analysis........................................................... 41 4.2.3.3 Poincaré plot analysis............................................................................... 42 4.2.3.4 Power-law relationship analysis ............................................................... 42
4.2.4 Sudomotor evaluation using the sympathetic skin response (Study III)........ 42 4.2.5 Brain receptor imaging using β-CIT SPECT (Study IV) ................................ 43 4.2.6 Statistics .......................................................................................................... 44
5 Results........................................................................................................................... 46 5.1 Clinical findings..................................................................................................... 46 5.2 Cardiovascular autonomic reflex tests (Study I) .................................................... 47 5.3 Heart rate variability measures (Study II) .............................................................. 51 5.4 Sympathetic skin response (Study III) ................................................................... 54 5.5 β-CIT SPECT (Study IV)....................................................................................... 57
6 Discussion ..................................................................................................................... 62 6.1 General aspects ...................................................................................................... 62 6.2 Clinical aspects ...................................................................................................... 63 6.3 Cardiovascular autonomic dysfunction .................................................................. 63 6.4 Sudomotor dysfunction .......................................................................................... 67 6.5 β-CIT SPECT......................................................................................................... 69
7 Conclusions................................................................................................................... 71 References
1 Introduction
The autonomic nervous system (ANS) is a complex neural network regulating the physiological functions of the body under changing internal and external conditions. As new techniques for assessing the autonomic functions have been developed, the understanding of the complexity and spectrum of the autonomic reflex responses and tonic control has expanded. Recent studies have focused on the development of new non-invasive methods for the evaluation of autonomic regulation and on the use of autonomic function measures as predictors of outcome and mortality in patients with heart diseases and in randomly selected populations.
ANS disturbances and their clinical manifestations have been found in a wide range of peripheral and central nervous system (CNS) disorders. Recently the classification of these syndromes and the nomenclature of the primary autonomic failure syndromes have been confirmed by a Consensus Panel (Consensus statement 1996). Chronic primary autonomic failure syndromes include pure autonomic failure (PAF), multiple system atrophy (MSA), and autonomic failure with Parkinson’s disease (PD) (Mathias 1997). Autonomic failure in PD has been related to abnormalities in the central and peripheral ANS, whereas there has been no peripheral involvement in MSA (Cohen et al. 1987, Yoshita 1998).
The role of autonomic failure in PD has remained controversial. James Parkinson himself described clinical autonomic dysfunction presenting itself as orthostatic hypotension, seborrhoea, excessive salivation and dysuria (Parkinson 1817). Yet, the clinical importance of autonomic dysfunction in PD has continued to be disputed, and the presence of prominent autonomic dysregulation is considered to be suggestive of diseases with more widespread involvement of the CNS like MSA (Benarroch 1997c, Bannister & Mathias 1999). However, suppression of both the sympathetic and parasympathetic regulation has been demonstrated in PD. Furthermore, as the accurate diagnosis of idiopathic PD is difficult, diseases like progressive supranuclear palsy, MSA and Alzheimer’s disease often cause differential diagnostic problems, leading to false prevalence rates of autonomic dysfunction in PD. Newly developed methods for evaluation of autonomic control, such as techniques assessing peripheral sympathetic cardiac innervation, have proved useful in the discrimination of PD patients from MSA patients (Orimo et al.1999, Reinhardt et al. 2000).

16
The effects of acute administration of levodopa and dopamine agonists on cardiovascular reflexes have been outlined, and the drugs have been associated mainly with orthostatic hypotension (Gross et al. 1972, Goetz et al. 1986). On the other hand little is known concerning the long-term effects of PD medication on cardiovascular and sudomotor autonomic control. Recently, two studies evaluating the influence of long-term selegiline treatment on cardiovascular responses have reported suppression of sympathetic functions (Churchyard et al. 1997, Turkka et al. 1997), but no effect on the mortality rate has been found (Donnan et al. 2000). Levodopa treatment has been demonstrated to suppress both blood pressure (BP) and heart rate (HR) responses in cardiovascular reflex tests (Camerlingo et al. 1990).
Since conventional structural imaging is of limited value in PD, alternative methods like positron emission tomography (PET) and single photon emission tomography (SPECT) have been used to detect changes in brain metabolism and receptor binding (Brooks 1997, Stoessl & Ruth 1998). SPECT with tracers used to monitor the dopamine transporter (DAT), e.g. 2β-carboxymethoxy-3β-(4-iodophenyl)tropane (β-CIT), have disclosed a loss of striatal binding in PD (Marek et al. 1996, Brücke et al. 1997, Müller et al. 1998, Tissingh et al. 1998). The binding to vesicular monoamine transporters (Frey et al. 1996) and postsynaptic dopamine and other receptors (Schwarz et al. 1994, Kawabata et al. 1997, Pirker et al. 1997) in PD can also be measured using PET and SPECT.
The present study was designed to elucidate the role of autonomic cardiovascular and sudomotor disturbances in untreated patients with PD. Additionally, it aimed at assessing the effects of three common PD medications, i.e. levodopa, bromocriptine and selegiline, on cardiovascular and sudomotor autonomic regulation. β-CIT SPECT was used to assess monoamine transporter availability in PD, special attention being paid to the correlation of autonomic functions with the SPECT measures.

2 Review of the literature
2.1 Autonomic nervous system
2.1.1 Autonomic nervous system anatomy
The ANS regulates multiple essential bodily functions maintaining internal physiologic homeostasis under changing internal and external conditions independently of volitional activity. The activity of the ANS is predominantly, but not exclusively, reflexive in nature. Especially cardiovascular, thermal, gastrointestinal, urinary, and sexual functions depend on autonomic regulation, and the ANS also has an important role in the control of pupillary, respiratory, renal and exocrine functions (Appenzeller 1990, Ravits 1997).
The ANS is anatomically and functionally divided into two distinct interacting divisions, the sympathetic and parasympathetic (Shields 1993, Harati & Machkhas 1997). The sympathetic preganglionic neurons lie in the spinal cord to form the intermediolateral columns extending from segments T1 to the rostral part of L3. The preganglionic myelinated axons, using acetylcholine as transmitter, synapse at the prevertebral and paravertebral ganglia. Postganglionic fibers are unmyelinated and primarily adrenergic, except for the innervation of the sweat glands, which are cholinergic (Collins 1999, Jänig & McLachlan 1999, van Zwieten 1999). The parasympathetic preganglionic neurons are situated in the brain stem and in the sacral spinal cord segments S1–S3. They leave the CNS via distinct cranial nerves, sacral ventral roots and pelvic splanchnic nerves, projecting their axons directly to the organs they supply, whereas the postganglionic neurons are located in small ganglia just outside or even within the wall of the target organ (Gibbins 1990, Reid 1990, Jänig & McLachlan 1999).
The central autonomic network is anatomically and functionally composed of several interconnected areas responsible for tonic, reflex, and adaptive control of autonomic functions (Benarroch 1993, Benarroch 1997c). It receives visceroceptive, humoral and environmental information (Loewy 1990) and contributes to autonomic (Spyer 1990), endocrine (Swanson 1991), behavioural motor (Bandler et al. 1991), emotional, attentional (Bechara et al. 2000) and pain-controlling responses (Lovick & Li 1993). The
18
structures forming the central autonomic network are distributed at the level of the cerebral cortex, basal forebrain, hypothalamus, midbrain, pons, and medulla (Loewy 1990). The insular and medial prefrontal cortices are involved at the highest level of integration of viscerosensory and visceromotor responses (Cechetto 1987, Neafsey 1990, Loewy 1991). The central nucleus of the amygdala and the bed nucleus of the stria terminalis form a unit referred to as the extended amygdala that integrates autonomic, neuroendocrine, and behavioural responses to emotions (Amaral et al. 1992, LeDoux 2000). The hypothalamus integrates autonomic with endocrine responses to maintain homeostasis (Swanson 1991, Cooper 1990). The nucleus of the solitary tract is the first relay station for various medullary reflexes controlling cardiovascular and respiratory functions (Guyenet 1990, Loewy 1990, Dampney 1994).
2.1.2 Cardiovascular autonomic control
The CNS is essential in modulating autonomic and neurohumoral influences on the cardiovascular function (Talman & Kelkar 1993). The dynamic balance of sympathetic and parasympathetic activity is critical for cardiac function including heart rate, excitability, and contractility (Guyton & Hall 1996, Benarroch 1997b). In the regulation of BP cardiovascular baroreflexes provide short-term control of arterial pressure, whereas renal regulation of blood volume is critical for long-term BP control (Benarroch 1997a).
In general, the sympathetic nervous system facilitates discharge of the sinoatrial pacemaker increasing HR, atrioventricular conduction, excitability of the ventricular conduction system, and contractility of the myocardium. The parasympathetic nerves have inhibitory effects on the heart. The influences of the cardiovagal and sympathetic nerves interact in a complex manner via prejunctional and postjunctional mechanisms, resulting in accentuated antagonism (Willette et al. 1984).
The HR control is mainly determined by the outflow from the cardiovagal motoneurons that are located in the nucleus ambiguus and the dorsal vagal nucleus (Loewy & Spyer 1990, Standish et al. 1994, Spyer 1995). The cardiovagal motoneurons in the nucleus ambiguus are excited by afferent inputs from the peripheral baroreceptors (Spyer 1995), arterial chemoreceptors and unmyelinated cardiac afferents. This excitatory effect is mediated via a direct monosynaptic projection from the nucleus tractus solitarius, which relays baroreceptor afferent inputs, and a supramedullary pathway that may involve the parabrachial nucleus and the anterior hypothalamus (Spyer 1995). Stimulation of the anterior hypothalamus inhibits the activity of cardiovagal motoneurons in the nucleus ambiguus via direct short-latency inhibition mediated by the gamma-aminobutyric acid-A receptors, disfacilitation due to inhibition of the neurons of the nucleus tractus solitarius activated by baroreceptor afferents, and an increase in inspiratory drive (Spyer 1995). Respiration affects the basic discharge of cardiovagal motoneurons and their sensitivity to central and reflex inputs (Koepchen et al. 1981), causing hyperpolarization during inspiration (Richter & Spyer 1990). It is the main determinant of respiratory sinus arrhythmia, which is an important clinical index of vagal innervation to the heart (Eckberg 1983). Individual neurons of the nucleus ambiguus and the dorsal vagal nucleus innervate either the sinoatrial or the atrioventricular node, but not
19
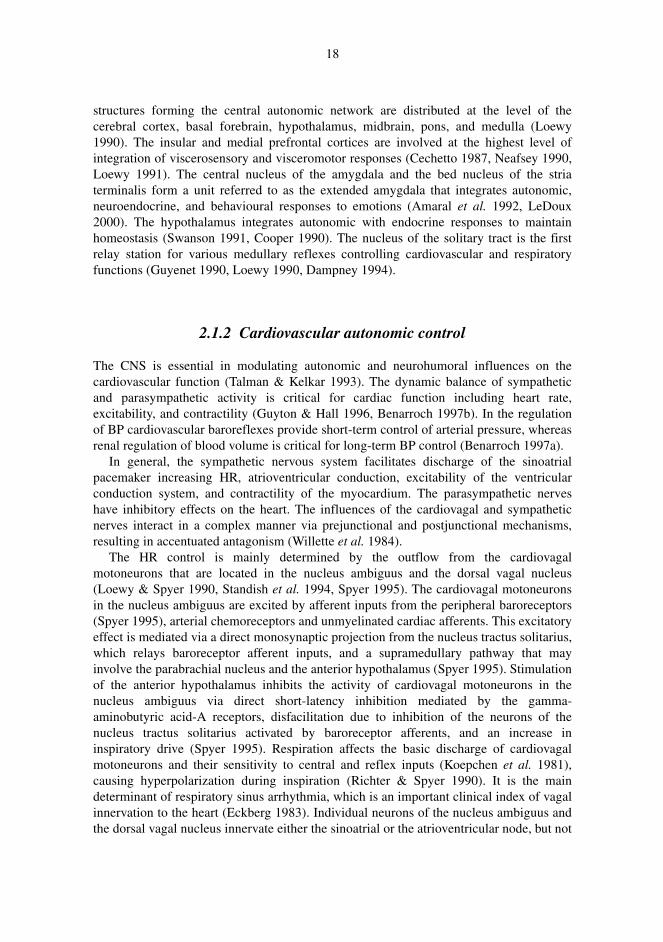
both (Richter & Spyer 1990). Therefore, the CNS may selectively influence the sinoatrial or atrioventricular node together or independently. The nucleus tractus solitarius integrates the inputs from peripheral visceral receptors with those from higher control centers like the prefrontal cortex, the central nucleus of the amygdala, the hypothalamus and the periaqueductal gray matter, and modifies the gain of baroreflexes and other cardiorespiratory responses during exercise and other adaptive conditions (Spyer 1989). Most cardiac branches of the vagal nerve separate in the thorax and innervate several cardiac ganglion cells, using acetylcholine as transmitter (Rossi 1994). The vagal inputs produce mainly fast excitatory postsynaptic potentials via nicotinic receptors and to a lesser extent slow inhibitory potentials via muscarinic receptors (Randall & Wurster 1994). Acetylcholine, activating the M2 subtype of muscarinic receptors, mediates the parasympathetic influence on the heart. The activation of these receptors leads to an increase in potassium conductance and a decrease in cyclic adenosine monophosphate via G-protein mediated mechanisms (Randall & Wurster 1994). The main neural components regulating the cardiovagal motoneurons are presented in Figure 1.
Fig. 1. Schematic diagram of the main neural components participating in the vagal control of the HR. The arrowheads indicate stimulation and the diamondheads inhibition of the cardiovagal motoneurons. (Modified after Benarroch 1997b)
The sympathetic preganglionic neurons are located in the intermediolateral column between the T2 to T5 segments of the spinal cord, the preganglionic fibers ascending in the paravertebral sympathetic chain to synapse in the cervical and upper thoracic (stellate) ganglia (Gibbins 1990). Also the sympathetic preganglionic neurons use acetylcholine as transmitter, acting mainly on nicotinic receptors. The sympathetic system acts in a lateralised manner as the right sympathetic pathways predominantly innervate the sinoatrial node, so increasing the HR, whereas the left sympathetic pathways predominantly innervate the atrioventricular node and ventricles, so increasing
20
atrioventricular conduction, excitability within the His-Purkinje system node, and increasing cardiac contractility and oxygen consumption (Cowley 1992). The influence on the heart is mediated via α and β receptors, noradrenaline acting primarily on β1
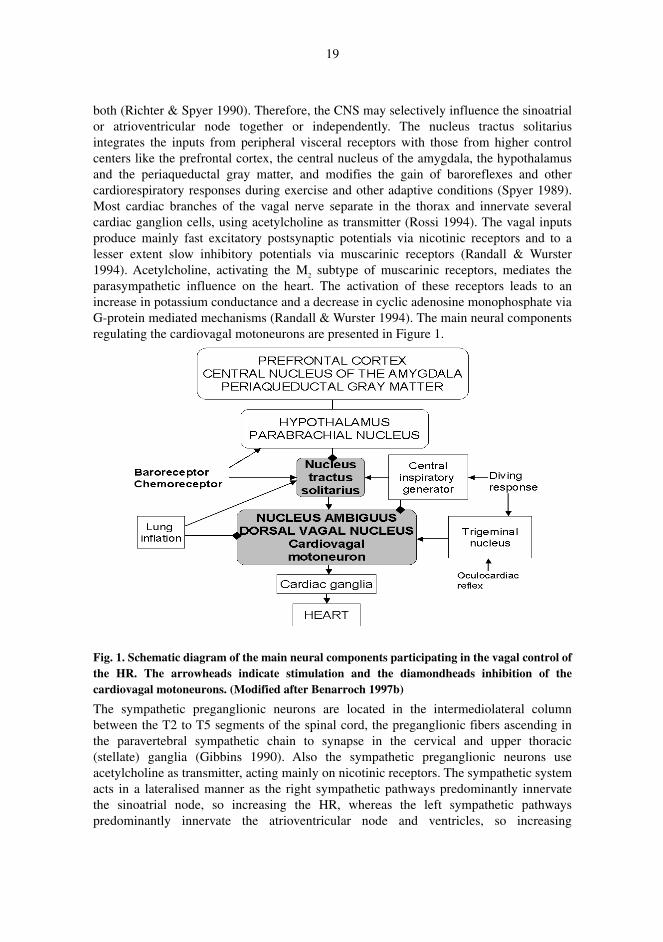
receptors (Gibbins 1990). The sympathetic preganglionic neurons receive inputs from the paraventricular nucleus and the ventrolateral medulla, as well as the lateral hypothalamic area, the zona inserta, and the periaqueductal gray matter. The main neural components participating in the sympathetic control of the HR are presented in Figure 2.
Fig. 2. Schematic diagram of the sympathetic HR control.
Medullary feedback reflexes control rapid BP changes, whereas long-term control mechanisms of arterial BP include adjustment of body fluids via pressure diuresis and the sympathetically mediated increase in arterial pressure activated by brainstem ischemia, i.e. the Cushing response. The baroreflexes are triggered by stretch of the carotid sinus and aortic arc and activation of cardiac receptors, buffering continuously the magnitude of arterial BP oscillations, via changes in cardiac output and peripheral resistance (Spyer 1981, Shepherd 1986, Ruggiero et al. 1989, Cowley 1992). The activation of arterial mechanoreceptors is mediated via branches of the IX and X cranial nerves to the nucleus tractus solitarius, leading to inhibition of sympathetic and increase of cardiovagal outflow (Spyer 1981, Ruggiero et al. 1989, Kumada et al. 1990). The neurons of the nucleus tractus solitarius generate several feedback loops, the main neuronal outputs being located in the ventral medulla and intermediate reticular formation, i.e. cardiovagal neurons of the nucleus ambiguus and the dorsal vagal nucleus, the rostral ventrolateral medulla, and the dorsal and ventral respiratory groups (Kumada et al. 1990, Richter & Spyer 1990, Spyer 1990, Dampney 1994, Standish et al. 1994, Funk & Feldman 1995,
21
Benarroch et al. 2000). Cardiac receptors monitor venous return and regulate extracellular fluid volume through sympathetic activation and inhibition of sympathetic discharges in the kidneys (Hainsworth 1991, Cowley 1992). Mechanoreceptor reflexes also control both secretion of vasopressin and renin-angiotensin II-aldosterone activation that are potent arterial vasoconstrictors and potentiate the effects of noradrenaline (Cowley 1992).
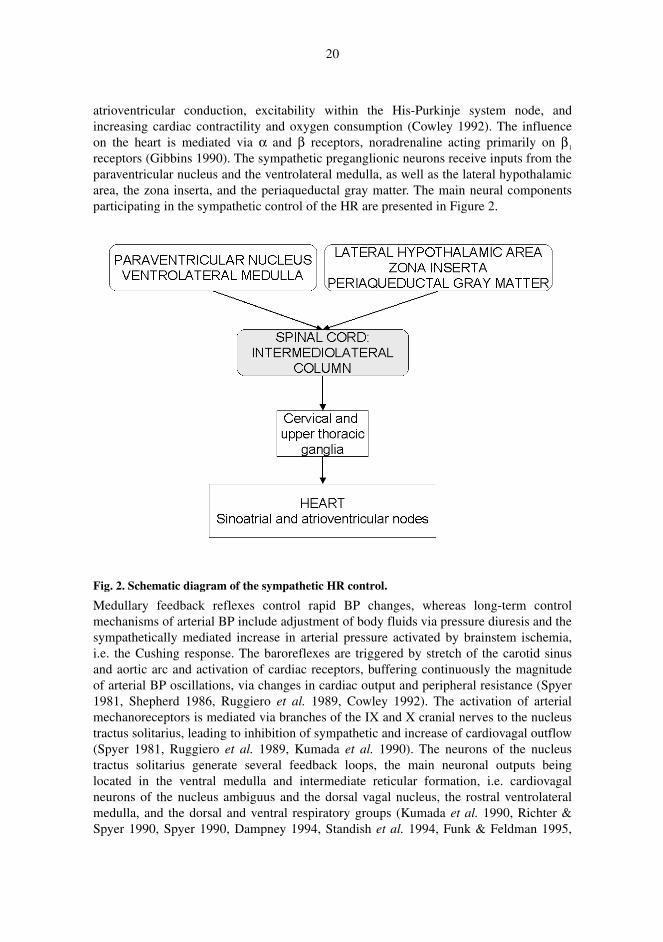
The central nucleus of the amygdala, the insular cortex and several regions of the hypothalamus play an important role in integrating responses to stress, emotional stimuli and exercise via both direct sympathoexcitation and resetting of the baroreflex (Spyer 1989, Bishop 1994). The long-term control of arterial pressure depends mainly on the pressure-diuresis volume regulation mechanism. The renal excretion of water and sodium is determined by neural (sympathetic), endocrine (vasopressin, angiotensin II, atrial natriuretic factor, aldosterone), and local factors (Cowley 1992). The sympathetically mediated Cushing response is triggered by a decrease in medullary perfusion pressure (Dickinson 1981). Figure 3 presents the components regulating arterial BP in a one-way mode of representation.
Fig. 3. Diagram of the components regulating arterial BP. (Modified after Benarroch 1997a)
2.1.3 Sudomotor regulation
The major function of sweat glands in humans is thermoregulatory, but sweat production can also be stimulated by emotional and arousal stimuli such as physiological stress (Christie 1981, Tranel & Damasio 1989, Jänig 1990, Schondorf 1993, Wallin & Elam 1993). Sudomotor neurons may be activated reflectively e.g. by visceral, noxious and
22
vibratory stimulation (Jänig 1990). An increase in the core body temperature leads to skin vasodilatation and sweating, whereas a decrease in the core temperature elicits vasoconstriction and piloerection. The sympathetic outflow to the skin regulates both vasomotor and sudomotor functions (Stolwijk 1977, Simon et al. 1986, Jänig 1990, Ogawa & Low 1993).
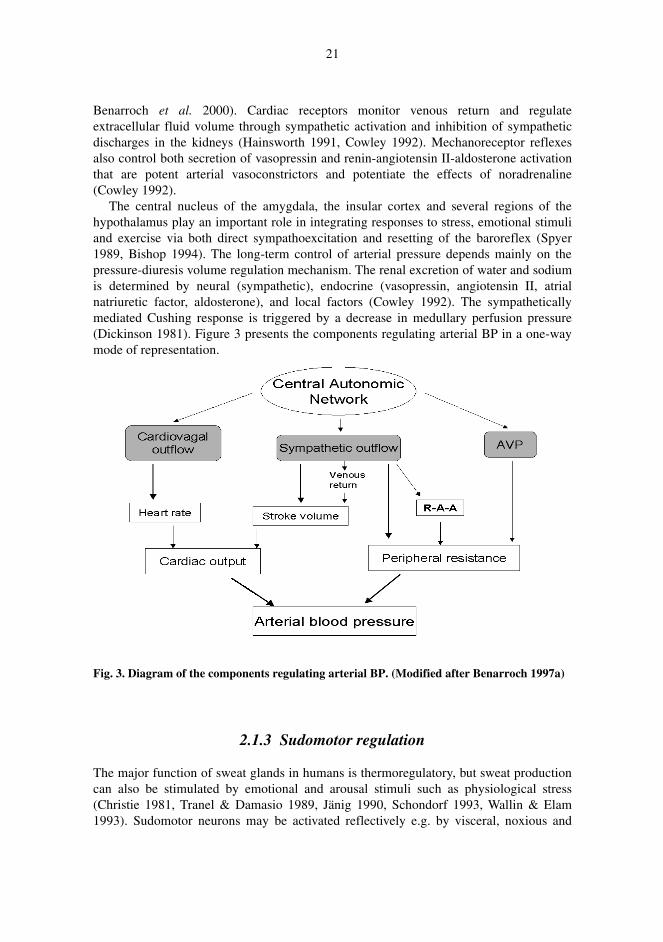
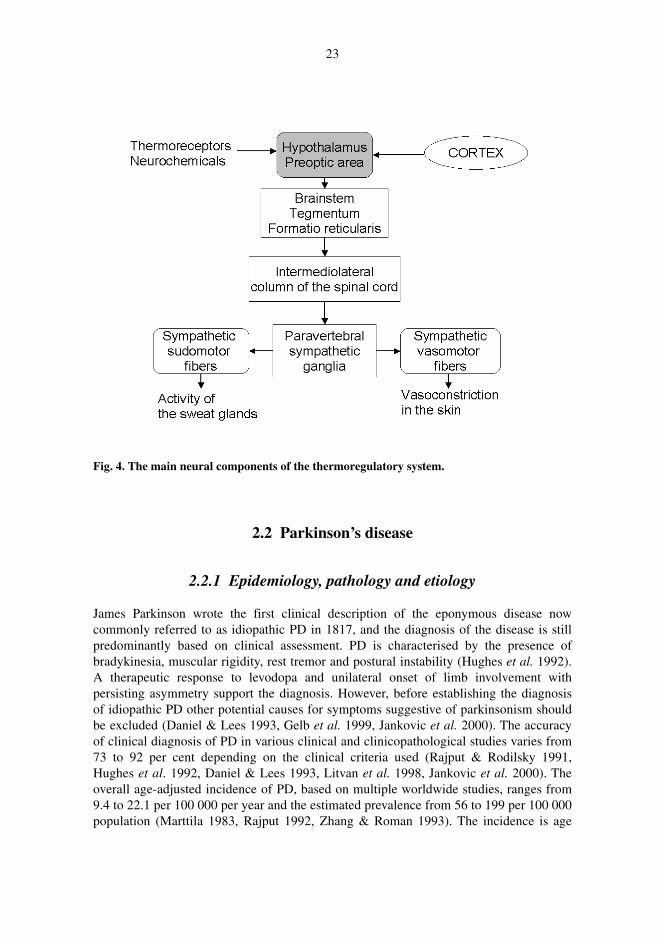
There are multiple independent thermoregulatory systems hierarchically organised at various levels of the neural axis. The thermoregulatory pathways extend from the hypothalamus and the limbic system, including cortical areas, to the lower brainstem, the reticular formation, the spinal cord, and sympathetic pathways. The medial preoptic – anterior hypothalamic region is the predominant site of intregration of the sudomotor control (Jänig 1990, Korpelainen et al. 1993, Collins 1999, Low & Fealey 1999), containing large numbers of thermoreceptors that initiate autonomic, endocrine, and motor thermoregulatory responses (Benarroch 1997d). Thermoreceptors are also present in skin, in viscera and in the spinal cord, afferent pathways ascending as multisynaptic fibres in the lateral spinal cord and in the spinothalamic tract to the reticular formation of the brainstem and finally to the hypothalamus and thalamus (Low & Fealey 1999). The output pathways from the hypothalamus that mediate thermoregulation are incompletely defined. The outflow from the hypothalamus is mainly ipsilateral, polysynaptic, and passes through the lateral tegmentum of the pons and lateral reticular substance of the medulla to the intermediolateral columns of the spinal cord (Nathan & Smith 1987, Benarroch 1997d, Low & Fealey 1999). The preganglionic cholinergic neurons synapse with paravertebral sympathetic ganglia from whence postganglionic sympathetic cholinergic sudomotor axons supply the two types of sweat glands, the eccrine and apocrine glands (Jänig 1990). Together with predominant cholinergic sympathetic neurons stimulating mainly M3 muscarinic receptors, the secretory cells have a few adrenergic terminals (Collins 1999). The sympathetic pathways mediating vasoconstriction are noradrenergic but the vasodilator pathways are still chemically undefined (Gibbins 1990, Jänig 1990). Figure 4 presents the principal neural structures of the thermoregulatory system.
The long efferent course of autonomic sudomotor fibres can be affected both by central and peripheral autonomic damage, and such disturbance may result in impairment of sweat response that can be quantified using several different techniques. Different aspects of sudomotor function, such as the electrical activity as opposed to the spontaneous electrodermal activity that is caused by different stimuli and generated in sweat glands as well as in the surrounding dermis and epidermis, i.e. the galvanic or sympathetic skin response (SSR), can be measured and quantified (Gutrecht 1994).
23
Fig. 4. The main neural components of the thermoregulatory system.
2.2 Parkinson’s disease
2.2.1 Epidemiology, pathology and etiology
James Parkinson wrote the first clinical description of the eponymous disease now commonly referred to as idiopathic PD in 1817, and the diagnosis of the disease is still predominantly based on clinical assessment. PD is characterised by the presence of bradykinesia, muscular rigidity, rest tremor and postural instability (Hughes et al. 1992). A therapeutic response to levodopa and unilateral onset of limb involvement with persisting asymmetry support the diagnosis. However, before establishing the diagnosis of idiopathic PD other potential causes for symptoms suggestive of parkinsonism should be excluded (Daniel & Lees 1993, Gelb et al. 1999, Jankovic et al. 2000). The accuracy of clinical diagnosis of PD in various clinical and clinicopathological studies varies from 73 to 92 per cent depending on the clinical criteria used (Rajput & Rodilsky 1991, Hughes et al. 1992, Daniel & Lees 1993, Litvan et al. 1998, Jankovic et al. 2000). The overall age-adjusted incidence of PD, based on multiple worldwide studies, ranges from 9.4 to 22.1 per 100 000 per year and the estimated prevalence from 56 to 199 per 100 000 population (Marttila 1983, Rajput 1992, Zhang & Roman 1993). The incidence is age
24
dependent as it shows a continuing rise with advancing age from 5 per 100 000 below 54 years of age to 254 per 100 000 at 75–84 years of age (Rajput 1984). In a recent study by Kuopio et al. (1999) the age-adjusted incidence was 14.9 and the age-adjusted prevalence 166 per 100 000 in a Finnish population. A very significant male and rural predominance was found in that study suggesting a possible environmental causative factor (Kuopio et al. 1999)
Pathologically PD is characterised by progressive neuronal loss associated with Lewy bodies in the pigmented nuclei of the midbrain, in many subcortical nuclei and in the cortex (Jellinger 1999). There is a severe depletion of melanin containing neurons and tyrosine hydroxylase positive neurons in the substantia nigra pars compacta, leading to striatal dopamine deficiency (Forno 1996, Halliday et al. 1996). It has been estimated that clinical symptoms do not appear before over 50% of the substantia nigra neurons are lost (Forno 1996). In addition to the involvement of the dopaminergic system, degeneration in PD affects the noradrenergic locus ceruleus and the dorsal motor vagal nucleus, the serotonergic raphe nuclei, the cholinergic nucleus basalis of Meynert, the pedunculopontine nucleus pars compacta, the Westphal-Edinger nucleus, and many peptidergic brainstem nuclei. Lewy bodies are also found in the thalamus, hypothalamus, substantia innominata, the mesocorticolimbic system, the intermediolateral columns of the spinal cord, the olfactory bulb, sympathetic and parasympathetic neurons, enteric nervous plexuses, and in the adrenal medulla (Den Hartog Jager & Bethlem 1960, Jellinger 1991, Wakabayashi & Takahashi 1997, Jellinger 1999). Cortical Lewy bodies are seen in the neurons of the temporal insular and cingulated regions (Braak et al. 1996). Thus the pathological process in PD involves widely the monoaminergic system and also affects the central autonomic network and peripheral parts of the ANS, resulting in a multitude of functional and clinical deficits.
Uncertainty over the etiology and pathogenesis of PD still persists despite all the recent advances in this field. The cellular degeneration in the substantia nigra is preceded by loss of neurofilament proteins, distribution of melanin, astroglial reaction and proliferation of microglia indicating functional neuronal damage, active neuron degeneration, and toxic and immunological reactions (McGeer et al.1988, Itoh et al. 1997, Joyce et al. 1997). The degeneration is also accompanied by increased nitric oxide synthase activity, that has been related to a cascade of multiple noxious factors like formation of free radicals, lipid peroxidation, oxidative stress, melanin-iron interaction with increased iron content in the substantia nigra, mitochondrial dysfunction, disorders of calcium homeostasis, functions of excitatory amino acids, and inhibition or loss of neuroprotective mechanisms (Schapira 1995, Jenner & Olanow 1996). Apoptotic nigral cell death can be induced experimentally (Jackson-Lewis et al. 1997), but nigral neurons very rarely show the morphologic signs of apoptosis (Kösel et al. 1997), suggesting that distinct mechanisms from classical apoptosis may play a role in the pathogenesis of PD. Genetic factors seem to play a role in the development of PD at least in some individuals for recent studies have shown relatively high concordance rates in twin studies (Vieregge et al. 1992, Burn et al. 1992, Tanner et al. 1999). Mutations of the genes encoding α-synuclein and parkin have been described in families with dominantly or recessively inherited PD (Golbe et al. 1990, Polymeropoulos et al. 1997, Kitada et al. 1998, Kruger et al. 1998), whereas these mutations have been excluded in pathologically verified sporadic PD (Chan et al. 1998). Among first-degree relatives of PD patients the risk is 2-

25
14 times the risk in members of unaffected families (Wood 1998, Autere et al. 2000). Furthermore, the familial clustering of PD has extended beyond the nuclear family, providing evidence that the disease has a genetic component (Sveinbjörnsdóttir et al. 2000). The risk ratios for siblings have been higher than for offspring, indicating a role of some shared environmental factor in the development of the disease (Autere et al. 1999, Sveinbjörnsdóttir et al. 2000). There has been an extensive search for environmental risk factors of PD, factors such as living in rural areas, exposure to pesticides or herbicides and contacts with domestic animals suspected to be risk factors, whereas smoking has generally been associated with a risk reduction (Seidler et al. 1996, Kuopio et al. 1999).
2.2.2 Medication
The establishment of dopamine deficiency in the nigro-striatal system as the neurochemical basis for PD (Ehringer & Hornykiewicz 1960, Utley & Carlsson 1965) has led to the introduction of levodopa treatment and a dramatic improvement in the functional capacity and increased survival of PD patients (Cotzias et al. 1967, Uitti et al. 1993). Levodopa still remains the most effective symptomatic treatment for PD, even though it does not halt the disease progression. Long-term complications such as dyskinesias, wearing-off and motor fluctuations has been found in 50% of patients on levodopa after five years treatment (Rinne 1987, Miyawaki et al. 1997). There has also been a considerable debate over the concern that levodopa may be toxic to dopaminergic neurons (Fahn 1996). For these reasons alternative treatment options have been sought especially for young-onset PD patients.
Dopamine agonists like bromocriptine, pergolide, cabergoline, pramipexole and ropinirole have been shown to be effective in the early stages of the disease as monotherapy (Rinne et al. 1997, Shannon et al. 1997, Watts 1997, Rascol et al. 1998). Dopamine agonist monotherapy, however, is related to difficulties such as inadequate benefit, the relatively long time to attain an effective dosage, and frequent early side effects. Often encountered adverse effects are nausea and vomiting, postural hypotension and constipation (Grimes & Lang 1999). Additionally, patients on dopamine agonist monotherapy almost always require supplementary levodopa for supervening disability. The early use of dopamine agonists has been considered advantageous as they are thought to reduce the turnover of dopamine and oxidative stress and delay the development of motor complications (Rinne 1987, Grimes & Lang 1999).
Selegiline, an irreversible inhibitor of monoamine oxidase B, has unique anti-apoptotic properties that could theoretically have neuroprotective implications in addition to its symptomatic effect (Mytilineou et al. 1997). Initial reports and some further evidence have suggested that selegiline slows the progression of symptoms in idiopathic PD, but it does not seem to have substantial neuroprotective effect (The Parkinson Study Group 1993, Olanow et al. 1995). Increased mortality has been associated with the use of selegiline (Lees et al. 1996), but a recent study found no difference between the mortality rates of PD patients using selegiline and those of controls (Donnan et al. 2000). Other monoamine oxidase inhibitors are being developed and new approaches to neuroprotection are being considered aiming at retarding the course of the disease. Yet

26
none of the currently available drugs for PD have been able to stop or slow down the progression of the disease.
Symptomatic treatment is recommended for patients with mild to moderate symptoms interfering with daily activities. Age has an important impact on the treatment decisions and usually it is considered safest to begin with levodopa after the age of 70 (Grimes & Lang 1999). When disability still persists dopamine agonists or a catechol-O-methyl transferase inhibitor as adjunctive therapy should be considered (Kaakkola 2000). As motor complications related to dopamine agonists are less frequent than those associated with levodopa, the former medication may have an advantage in the early treatment of patients with PD (Ogawa 1998).
2.3 Autonomic dysfunction in Parkinson’s disease
2.3.1 Clinical aspects
PD may contribute to various autonomic manifestations but the prevalence and severity of the autonomic dysfunction is difficult to determine. In contrast to MSA and PAF, cases with severe autonomic failure preceding typical PD are uncommon and the autonomic insufficiency is generally less severe (Benarroch 1997c, Bannister & Mathias 1999).
Frequently encountered clinical manifestations of autonomic dysfunction in PD are abnormalities in the sudomotor, gastrointestinal and urinary functions, postural dizziness, hypersalivation, seborrhoea and impotence (Ludin et al. 1987, Turkka 1987, Sandroni et al. 1991, Niimi et al. 1999). Postprandial hypotension and disturbances of sleep and breathing have also been reported as signs of autonomic dysregulation (Micieli et al. 1987, Niimi et al. 1999).
Excessive sweating in the face and upper part of the body has been attributed as being compensatory to hypohidrosis in the trunk and limbs (Goetz et al. 1986). Gastrointestinal symptoms in PD include nausea, constipation and defecatory dysfunction, probably as a consequence of direct involvement of the gastrointestinal tract by the disease (Edwards et al. 1992). Constipation is one of the most frequent autonomic dysfunction symptoms in PD patients, the prevalence ranging from 44–70% (Singer et al. 1992, Magalhães et al. 1995, Martignoni et al. 1995). Bladder symptoms can be prominent in PD, high frequency and urgency of urination—manifestations of detrusor hyperreflexia verified with urodynamic studies—being common (Sotolongo 1988, Chandiramani et al. 1997). A high level of sexual dysfunction has been found with a questionnaire survey in young PD patients (Brown et al. 1990) and erectile difficulties and premature ejaculation has also been reported (Singer et al. 1989, Chandiramani et al. 1997).
The prevalence of autonomic symptoms in PD has been reported as being especially high in patients with bilateral severe bradykinesia and rigidity, and lower in patients with unilateral signs (Spiegel et al. 1969, Marttila 1974). The duration and severity of the disease have also been associated with the degree of clinical autonomic failure (Turkka 1987). The overall prevalence of autonomic symptoms varies from 76% to 93% (Spiegel et al. 1969, Turkka 1987, Singer et al. 1992, Magalhães et al. 1995).
27
2.3.2 Cardiovascular dysfunction
Among other symptoms of autonomic failure alterations of the regulation of BP have been described in PD. Several studies have detected low supine BP levels in parkinsonian patients (Barbeau et al. 1969, McDowell & Lee 1970, Aminoff & Wilcox 1971), whereas the resting BP has been found to be unaffected in other studies (Gross et al. 1972, Reid & Calne 1973, Murata et al. 1997). Some degree of orthostatic hypotension has occurred in patients with PD (Calne et al. 1970, McDowell & Lee 1970, Goetz et al. 1986, Meco et al. 1991), although not all studies have confirmed this (Appenzeller & Goss 1971, Reid & Calne 1973, Sachs et al. 1985, Ludin et al. 1987, Murata et al. 1997). Findings consistent with mild sympathetic failure also include pathological BP responses to passive tilting (Gross et al. 1972, Camerlingo et al. 1990, Meco et al. 1991, Van Dijk et al. 1991, Kallio et al. 2000) and to isometric exercise (Sachs et al. 1985, Ludin et al. 1987, Turkka et al. 1987b, Van Dijk et al. 1991, Turkka et al. 1997).
Standard cardiovascular reflex tests in PD patients have revealed changes in the HR responses to various test procedures, reflecting mainly the function of the baroreflex arc. Patients with PD have shown suppressed HR responses to normal breathing (Piha et al. 1988, Meco et al. 1991, Turkka et al. 1997), deep breathing (Sachs et al. 1985, Camerlingo et al. 1986, Ludin et al. 1987, Turkka et al. 1997, Kallio et al. 2000), and the Valsalva manoeuvre (Appenzeller & Goss 1971, Goetz et al. 1986, Turkka et al. 1987b, Piha et al. 1988, Meco et al. 1991), indicating parasympathetic dysfunction. The HR response to tilting has also been shown to be diminished in PD patients (McDowell & Lee 1970, Turkka et al. 1987b, Camerlingo et al. 1990, Meco et al. 1991, Van Dijk et al. 1993, Kallio et al. 2000). However, the frequency and amplitude of respiration or the associated BP responses which influence the values, have not been measured in most of these studies. Only a few of the previously mentioned studies have been conducted with PD patients without any antiparkinsonian medication (Camerlingo et al. 1990, Turkka et al. 1997, Kallio et al. 2000), making the evaluation of the effects of the disease itself on autonomic functions difficult. Additionally, the results in PD patients have been controversial and some studies have not been able to demonstrate abnormalities in the HR responses to cardiovascular test procedures, e.g. Ludin et al. (1987) finding normal HR responses at rest, to tilting and to the Valsalva manoeuvre. A recent follow-up study reported significant deterioration in the HR responses to deep breathing, the Valsalva manoeuvre, and the orthostatic test over a period of three years (Mesec et al. 1999), and the systolic and diastolic BP responses during the orthostatic test were also impaired (Mesec et al. 1999). Van Dijk et al. (1993) have studied the correlation of cardiovascular reflex test impairment to age, medication, disease duration and severity in PD patients. With repeated regression analysis, age explained most of the HR variability (HRV), whereas various PD medications contributed only to 7 % of the HR fluctuation.
As the standard cardiovascular tests only provide information obtained from responses to stimuli during short periods under experimental conditions, methods providing a broader view of the cardiovascular autonomic regulation have been developed. Analysis of HRV from electrocardiogram (ECG) recordings has become an important method for assessing cardiovascular autonomic regulation. A recent study, using 24-hour ECG recordings, reported diminished variability of standard RR intervals and low frequency
28
(LF) spectral measures of heart rate variability in PD, whereas the high frequency (HF) spectral component was reduced only during night time (Mastrocola et al. 1999).
The neurohumoral factors, such as secretion of catecholamines, vasopressin and renin-angiotensin-aldosterone, participate in the short- and long-term BP regulation. Aminoff and Wilcox (1971) found an increased receptor susceptibility to noradrenaline in PD, possibly due to impairment of the function of sympathetic nerve endings, a phenomenon also detected later in spinal cord lesions (Mathias et al. 1976). A recent study has confirmed the hypersensitivity of PD patients to noradrenaline infusion and has demonstrated subnormal plasma noradrenaline concentrations (Niimi et al. 1999). The response in the serum noradrenaline to standing up (Turkka et al. 1986, Koike & Takahashi 1997, Niimi et al. 1999), and the levels of 3-methoxy-4-hydroxyphenylglycol, the main metabolite of noradrenaline, in the spinal fluid is also diminished in patients with PD (Turkka et al. 1987a). However, the plasma vasopressin levels have been shown to be increased in patients with PD and autonomic failure (Koike & Takahashi 1997, Niimi et al. 1999). Plasma renin levels have been shown to be low in PD patients, and levodopa treatment further decreases the renin concentration (Barbeau et al. 1969, Martignoni et al. 1995). PD patients have also demonstrated decreased cardiac extraction of circulating [3H]norepinephrine, norepinephrine spillover, and virtual absence of venous-arterial increment in plasma levels of endogenous L-dopa and 3-methoxy-4-hydroxyphenylglycol, reflecting loss of cardiac sympathetic nerve terminals (Goldstein et al. 2000).
Hemodynamic studies of postprandial hypotension in PD have revealed a decreased vascular resistance when assessed with impedance plethysmography (Ieda et al. 1994). Cardiac scintigraphy using iodine-123 labelled metaiodobenzylguanidine and 6-[18F]fluorodopamine positron emission tomography have demonstrated low cardiac uptake of the tracer in PD patients, reflecting postganglionic cardiac sympathetic denervation (Reinhardt et al. 1999, Goldstein et al. 2000). Additionally dysfunction of the centrally mediated sympathetic vasoconstrictor responses in the muscles and skin of patients with PD has been demonstrated with the local 133-Xenon washout method (Andersen & Boesen 1997). Thus both central and peripheral sympathetic dysfunction appears to account for the abnormal orthostatic and postprandial cardiac BP responses in PD.
2.3.3 Sudomotor dysfunction
Up to 50% of patients with idiopathic PD develop clinical manifestations of disturbed thermoregulation and sweating during the course of the illness (Spiegel et al 1969, Aminoff & Wilcox 1971, Appenzeller & Goss 1971, Appenzeller 1975). Evaporimetric methods have been used with contradictory results to demonstrate that thermoregulatory sweating is reduced in the trunk and limbs and compensatorily increased in the face (Appenzeller & Goss 1971), and that sweating is increased in the upper part of the body as well (Turkka & Myllylä 1987). Impaired sweating and vasodilatation was found in PD patients when using a colorimetric method, the defect being more pronounced on the affected side (De Marinis et al. 1991),

29
The assessment of sympathetic sudomotor activity in PD patients using the SSR has revealed either a latency increase (Taly & Muthane 1992, Braune et al. 1997), or an amplitude reduction (Mano et al. 1994, Hirashima et al. 1996) or absent responses (Korczyn 1990, Taly & Muthane 1992, Wang et al. 1993). The findings have been interpreted as reflecting disturbances of both the central regulation of the sudomotor reflex arc (Wang et al. 1993) and dysfunction of the postganglionic sympathetic neurons (Hirashima et al. 1996). It has been claimed that the presence of abnormalities in the SSR increases along with the disease duration and the functional disability of the patients (Braune et al. 1997).
2.3.4 Effects of antiparkinsonian medication on cardiovascular and sudomotor autonomic functions
The question of whether antiparkinsonian drugs are the cause of orthostatic hypotension in PD patients or not has been debated for a long time. One problem is that studies on the effects of levodopa are controversial, since levodopa has variously been reported as diminishing the HR response (Camerlingo et al. 1990), enhancing the fall in BP as a result of standing up (Calne et al. 1970, McDowell & Lee 1970, Camerlingo et al. 1990), and failing to produce any such influences at all (Kuroiwa et al. 1983, Sachs et al. 1985, Goetz et al. 1986). When the influence of levodopa on autonomic function has been evaluated using microneurography, levodopa administration has been found to increase the spontaneous muscle nerve sympathetic activity and to lower systolic BP significantly (Takeuchi et al. 1993). Chronic levodopa treatment has not been shown to cause changes in sympathetic reflex mechanisms controlling blood flow when assessed with the 133-Xenon washout technique (Andersen & Boesen 1997), nor has it influenced the myocardial 6-[18F]fluorodopamine-derived radioactivity reflecting functional sympathetic nerve terminals (Goldstein et al. 2000).
The use of dopamine receptor agonists as PD medication has been associated with low resting BP (Quinn et al. 1981) and a pronounced fall in orthostatic BP (Greenacre et al. 1976, Quinn et al. 1981, Tanner et al. 1982, LeWitt et al. 1983, Kujawa et al. 2000). Although orthostatic hypotension occurred frequently in PD patients starting dopamine agonist therapy in a recent study, patients seldom considered it noteworthy, and there was no relation to the use of a specific dopamine agonist (Kujawa et al. 2000). In a recent long-term, prospective, placebo-controlled trial by Turkka et al. (1997) selegiline was shown to slightly diminish sympathetic autonomic responses. In another study by Churchyard et al. (1997) selegiline medication combined with levodopa was associated with orthostatic hypotension, and withdrawal of the drug considerably diminished the fall in orthostatic BP. Anticholinergics, that are used as a treatment for PD, including belladonna alkaloids and subsequently tertiary-amine synthetic substitutes, act more on central muscarinic and nicotinic receptors than peripheral muscarinic receptors (Weiner 1985). Despite this, these drugs have peripheral antimuscarinic effects mainly via M1 muscarinic receptors, which might theoretically increase the HR (Weiner 1985). However, anticholinergics seem not to affect the HR and BP responses to tilting and the Valsalva manoeuvre (Gross et al. 1972).

30
There are no prospective studies on the effects of PD medication on sudomotor function assessed by using SSR. Even though anticholinergics are known to inhibit the activity of sweat glands (Weiner 1985), it has been postulated that levodopa and anticholinergic medications have no influence on the SSR (Braune et al. 1997).
2.4 Evaluation of autonomic functions
2.4.1 General aspects
The clinical evaluation of autonomic dysfunction has proved laborious due to the large normal individual variations in ANS functions. The major aims of investigations has been to determine the normality of autonomic function, to assess the degree of autonomic dysfunction, and to ascertain whether any abnormality is primary or secondary. A range of investigations has been conducted, with the emphasis on the cardiovascular system, and there have been numerous advances, especially in the field of non-invasive measurements. The information of each test should be considered in relation to the clinical picture as a whole, since the assessment is dependent not only on reflex arcs and afferent nerve activity, but also on end-organ responsiveness and the individual characteristics of subjects.
In most centres pursuing autonomic investigations routine evaluation of ANS functions includes cardiovascular autonomic function assessment based on physiological, biochemical and pharmacological measurements (Mathias & Bannister 1999). Quantitative investigation procedures have also been developed for the evaluation of sudomotor, gastrointestinal, renal, urinary, sexual, respiratory and pupil functions. New methods, like scintigraphy with iodine-123 labelled metaiodobenzylguanidine and 6-[18F]fluorodopamine positron emission tomography, have been introduced to assess cardiac postganglionic adrenergic innervation (Goldstein et al. 1997, Orimo et al. 1999, Reinhardt et al. 2000). Percutaneous microneurographic techniques have provided information about sympathetic activity in the skin and muscle in polyneuropathies, traumatic spinal cord injury, PAF and PD (Fagius 1982, Stjernberg et al. 1986, Dotson et al. 1990, Ishida et al. 1990, Fagius 1991).
2.4.2 Cardiovascular autonomic reflexes
Examination of the standard cardiovascular reflexes has established itself as the most commonly used method for assessing the autonomic function. These reflexes provide information about both the sympathetic and parasympathetic cardiovascular autonomic regulation (Mathias & Bannister 1999). The test procedures require continuous HR, BP and breathing monitoring to define circulatory responses under standardised conditions.
The variation of HR with respiration, known as sinus arrhythmia, is generated by autonomic brainstem reflexes and primarily mediated by vagal innervation of the heart
31
(Wheeler & Watkins 1973). Inspiration causes an increase in HR and expiration results in a reduced HR. Transection of the vagal nerve or parasympathetic blockage with atropine abolishes sinus arrhythmia, while sympathetic blockade has little effect. This cyclic HR fluctuation increases in a supine position, whereas it decreases with ageing, hyperventilation, and hypocapnia (Bennet et al. 1977, Ewing et al. 1981, Wieling et al. 1982, Low et al. 1990). The respiratory sinus arrhythmia is evaluated at rest and during deep breathing at a rate of 6 breaths per minute that produces the maximum sinus arrhythmia (Angelone & Coulter 1964, Borgdorff 1975, Hirsch & Bishop 1981, Piha et al. 1988). Registration of HR fluctuation during normal and deep breathing is a sensitive detector of autonomic dysfunction (Mackay et al. 1980).
In the Valsalva manoeuvre the respiratory strain increases the intra-thoracic and intra-abdominal pressure, altering hemodynamic and cardiac functions (Nishimura & Tajik 1986, Benarroch 1991). The most commonly used test parameter is the Valsalva ratio that calculates the ratio of the longest RR interval after the blowing to the shortest RR interval during the blowing (Levin 1966). A bradycardia reaction is caused by a baroreflex response to a BP rise secondary both to the return of cardiac output and venous return to normal while peripheral vasoconstriction is continued. Thus both the sympathetic and parasympathetic nervous system control the autonomic responses during the Valsalva manoeuvre (Sandroni et al. 1991). Continuous BP monitoring increases the sensitivity of the test and non-invasive devices for easier evaluation of the beat to beat BP have been developed (Ravits 1997).
The HR increases immediately upon standing or passive tilting due to an exercise reflex that decreases parasympathetic tone, and continues to rise due to the influence of sympathetic activity. Thereafter a relative bradycardia follows due to vagal reflexes (Ewing et al. 1978, Borst et al. 1982). The HR changes as a result of standing are expressed as the 30:15 ratio (Ewing et al. 1980). Tilting, on the other hand, shifts the venous blood to the peripheral compartments, resulting in a decreased cardiac filling pressure and stroke volume. This in turn leads to decreased baroreceptor activity and withdrawal of parasympathetic activity with increasing sympathetic activity. As a consequence of the increased vascular tone and peripheral vascular resistance, the BP is largely maintained (Ravits 1997). The BP is monitored during the test continuously or serially and the largest drop (or lowest increase) is quantified. Orthostatic hypotension is signalled by a reduction of systolic BP of at least 20 mmHg or of diastolic BP of at least 10 mmHg within 3 minutes (Consensus Statement 1996). Other diagnostic criteria for orthostatic hypotension have also been used (Schatz 1984). Even though the physiological responses to passive tilting are not identical to those to standing up, the pulse response is seen if the tilting is performed quickly and extended up to 90° (Sundquist et al. 1980, Myllylä et al. 2000).
The isometric work test measures the BP reaction to a sustained handgrip. The mechanism involves the exercise reflex that withdraws parasympathetic activity and increases the sympathetic tone. Normally the diastolic BP rises more than 15 mmHg. Age does not affect the BP response to isometric exercises (Goldstraw & Warren 1985) but the responses are greater in men than women (Piha 1993, Khurana & Setty 1996).
The cardiovascular reflex parameters based on HR fluctuation have been shown to be age and HR dependent and must therefore be adjusted for age and the baseline RR interval. A result of two subtests outside the 95% confidence limits of the control subjects

32
has been considered as a clinically abnormal finding, though a marked decrease of BP with fainting after either standing or tilting, as a sole finding, is enough for the diagnosis of clinical abnormality. Abnormalities in the cardiovascular reflexes have been detected in 80–85% of patients with MSA and PAF (Cohen et al. 1987, Ravits et al. 1995). Cardiovascular responses have also been used to evaluate autonomic dysfunction in diabetic, uremic and hereditary neuropathies (Bennet et al. 1977, Low et al. 1986, Wang et al. 1994, Shahani et al. 1990), pulmonary diseases (Pagani et al. 1996), amyotrophic lateral sclerosis (Pisano et al. 1995), cerebellar and extrapyramidal disorders (Sandroni et al. 1991), stroke (Korpelainen et al. 1994), migraine (Havanka-Kanniainen et al. 1988) and multiple sclerosis (Senaratne et al. 1984, Vita et al. 1993).
2.4.3 Ambulatory ECG and analysis of heart rate variability
Cardiovascular variables like HR and BP fluctuate from one beat to another under autonomic control. Temporal fluctuations related to respiration (i.e. respiratory sinus arrhythmia) were first noticed by Hales in 1733 (Singer & Underwood 1962), but more subtle beat to beat fluctuations have received attention only after the development of high resolution ECG recordings and digital computers with adequate capacity. Analysis of HRV from ambulatory ECG recordings has now become an important method for assessment of cardiovascular autonomic regulation. The time and frequency domain analysis based on linear fluctuations of HR provide useful information about tonic autonomic effects on the heart (Huikuri et al. 1995). However, as the heart is not a periodic oscillator under normal physiological conditions, these measures are insufficient for outlining the changes in HR dynamics (Kaplan & Goldberger 1991, Goldberger 1996). Therefore, other methods based on non-linear dynamics and fractal analysis have been introduced to quantify complex HR dynamics and to complement conventional HRV measures (Goldberger & West 1987, Denton et al. 1990, Pincus & Goldberger 1994).
The time domain analysis of HR fluctuation is conventionally based on indices drawn from statistical operations applied to measures of the RR intervals. The most widely used index is the standard deviation of all normal to normal RR intervals (SDNN) over a 24-hour period, that reflects primarily the very low frequency (VLF) fluctuation in HR behaviour, possibly associated with the peripheral vascular resistance and thermoregulation (Rosenbaum & Race 1968). Low SDNN has been used as a predictor of increased mortality in post myocardial infarction patients (Kleiger et al. 1987).
Spectral analysis of HRV studies the frequency-specific oscillations of HR fluctuation and decomposes series of sequential RR intervals into a sum of sinusoidal functions of different amplitudes and frequencies (Akselrod et al. 1981). The amplitude of the HR fluctuations at different oscillation frequencies is presented as a power spectrum. The most commonly used methods for the transformation of signals to the frequency domain are Fast Fourier transformation and autoregressive analysis. The power spectrum is usually divided into three or four frequency bands, the boundaries of which are as follows: ultra low frequency <0.0033 Hz, VLF from 0.0033–0.04 Hz, LF from 0.04–0.15 Hz and HF 0.15–0.4 Hz (Task Force 1996). The HF fluctuation of RR intervals mainly reflects the cardiovagal modulation and the inspiratory inhibition of vagal tone, whereas
33
the LF and VLF bands are affected by sympathetic excitation, sympathovagal balance and arterial BP oscillations (Dwain & Eckberg 1997, Pagani et al. 1997).
The Poincaré plot, a geometrical method of HRV analysis, is a diagram (scattergram) plotting each RR interval as a function of the previous RR interval. These plots can be interpreted visually and quantitatively, where the SD of the continuous long-term RR interval variability (SD2) and the instantaneous beat to beat RR interval variability (SD1) are analysed (Huikuri et al. 1996, Tulppo et al. 1996). SD1 describes the magnitude of beat to beat RR interval variability reflecting vagal modulation of the HR and has a relatively strong correlation with the HF spectral component; SD2 describes the long-term RR interval fluctuations and reflects the magnitude of both the VLF and LF spectral components. One potential advantage of the Poincaré method over spectral analysis techniques is that it is not affected by stationary irregularities and trends in the RR intervals, thus being more suitable for HRV analysis from uncontrolled ambulatory ECG recordings (Tulppo et al. 1996).
Analytic methods derived from non-linear dynamics based in chaos theory and fractal mathematics have opened new approaches for studying and understanding the characteristics of HR behaviour (Goldberger & West 1987, Goldberger 1996). These methods estimate the correlation properties and complexity of the HRV. Methods analysing fractal-like properties have been used to detect abnormalities in RR interval dynamics in various cardiovascular disorders (Bigger et al. 1996, Huikuri et al. 1998, Mäkikallio et al. 1998, Mäkikallio et al. 1999a, Mäkikallio et al. 1999b). Analysis of 1/f characteristics, i.e. the inverse power-law slope, has been a more useful predictor of survival than the traditional risk markers both in elderly people and in patients with impaired left ventricular dysfunction (Brouwer et al. 1996, Ho et al. 1997, Huikuri et al. 1998). The physiological background of this method is not known exactly, but it is influenced by the autonomic input to the heart, for the slope of the power law relation is especially deep in denervated, transplanted hearts (Bigger et al. 1996). Approximate entropy is a parameter that quantifies the regularity or predictability of time series data. HR dynamics have been found to display reduced dynamics in sick neonates and in patients with postoperative complications after cardiac surgery (Pincus & Viscarello 1992, Fleisher et al. 1993). Low approximate entropy values have also been reported in patients with chronic liver disease (Fleisher et al. 2000).
2.4.4 Sudomotor functions
The sympathetic nervous system plays a major role in thermoregulation. Sympathetic sudomotor fibers innervate sweat glands to regulate evaporative heat loss. Vasoconstriction of cutaneous vessels to reduce convective heat loss is caused by vasomotor fibers, though the pilomotor function in humans is rudimentary (Ravits 1997). Sudomotor dysfunction has been measured by the SSR, the quantitative sudomotor axon reflex test, the thermoregulatory sweat test, the acetylcholine sweatpot test, the silastic mold test, and the evaporimetric method. The sensitivity of the quantitative sudomotor axon reflex test is comparable with the SSR for the detection of autonomic dysfunction, and there is concordance between the two (Maselli et al. 1989). A qualitative assessment

34
of thermoregulatory sweating can also be made using chemicals, e.g. quinizarin powder and starch-iodine for the detection of large anhidrotic areas.
The SSR, based on changes in skin conductance levels in response to various internal or external stimuli, has long been used to assess the integrity of the sympathetic sudomotor function (Fagius & Wallin 1980, Uncini et al. 1988, Elie & Guiheneuc 1990). The early fast change in skin potential has been related to sweating, but the later changes are due to skin potential changes (Low & Fealey 1999). The afferent part of this reflex arc includes large myelinated sensory fibers, the auditory nerves and the optic pathways, and the efferent sympathetic pre- and postganglionic nerve fibers activate the eccrine sweat glands in the skin (Uncini et al. 1988, Elie & Guiheneuc 1990). The central parts mediating the SSR in man are incompletely known, reports being based mainly on ischemic lesion studies (Schondorf 1993, Korpelainen et al. 1993). However, these centres, including the orbitofrontal cortex, the caudate nucleus, the anterior lobe of the cerebellum, the dorsal thalamus, the posterior hypothalamic nuclei, the ventrolateral and ventromedial substantia reticularis and the intermediolateral nucleus, have been identified in the cat (Wilcott 1969, Schondorf 1993).
There is general agreement that loss of the SSR is abnormal (Shahani et al. 1984, Korczyn 1990, Shahani et al. 1990, Taly & Muthane 1992, Bordet et al. 1996), but some controversy exists as to whether a reduction of the SSR amplitude or prolonged latencies are reliable abnormalities (Fusina et al. 1999), since the SSR amplitudes show great individual variability and many factors can modify the responses. SSRs have been used to assess autonomic dysfunction in diabetic and other peripheral neuropathies, and also of diseases affecting the central pathways (Yokota et al. 1991, Schondorf 1993, Wang et al. 1993, Yokota et al. 1993, Elie & Louboutin 1995), although a recent study showed limitations in the use of SSR as an indicator of autonomic dysfunction in diabetic polyneuropathy (Bril et al. 2000). SSRs may be helpful in distinguishing idiopathic PD from other extrapyramidal syndromes such as MSA, since abnormal SSRs are found more often in MSA (69%) than in PD (8%) (Bordet et al. 1996).
2.5 Functional brain receptor imaging in Parkinson’s disease
Structural imaging provides limited information in extrapyramidal disorders, since patients with PD have normal brain computed tomography though they may show abnormal signals in the substantia nigra in magnetic resonance imaging (Duguid et al. 1986, Gorell et al. 1995). Functional imaging, on the other hand, has provided a sensitive means of detecting brain abnormalities in parkinsonian syndromes, characterising regional changes in brain metabolism and dopamine receptor binding (Brooks 1997).
Various cocaine analogues have been introduced to assess mainly dopamine but also serotonin transporter (DAT and SERT, respectively) activity in PD. β-CIT is the most widely used SPECT tracer that has a high affinity for presynaptic DAT. It is characterised by high striatal uptake and slow binding kinetics, equilibrium being reached between 20 to 30 hours after injection (Laruelle et al. 1994). Recently developed new tracers allow imaging of the DAT earlier than β-CIT, even as early as 1 to 2 hours post injection, but
35
their affinity to DAT is lower (Abi-Dargham et al. 1996, Booij et al. 1997, Tatsch et al. 1997).
In PD, the use of SPECT with these tracers has revealed a reduction of DATs in the striatum, particularly in the putamen (Seibyl et al. 1995, Abi-Dargham et al. 1996, Marek et al. 1996, Asenbaum et al. 1997, Booij et al. 1997, Sjøholm et al. 1997, Tatsch et al. 1997, Müller et al. 1998). The uptake of the tracers has been affected bilaterally in patients with hemiparkinsonism and the reduction of striatal uptake has been approximately 45–65% contralateral to the affected side (Tissingh et al. 1998). Striatal, particularly putaminal, binding of these ligands has reliably discriminated early PD patients from healthy subjects and the uptake has correlated inversely with the degree of motor disability measured with the Unified Parkinson’s Disease Rating Scale (UPDRS) subscores and the Hoehn and Yahr stages (Seibyl et al. 1995, Marek et al. 1996, Booij et al. 1997, Brücke et al. 1997, Tatsch et al. 1997, Tissingh et al. 1998). Levodopa/carbidopa, selegiline and dopamine agonist therapy has not been shown to influence the DAT levels in the striatum significantly (Ahlskog et al. 1999, Innis et al. 1999).
β-CIT has also been reported to have high affinity for SERTs in the hypothalamic/midbrain regions (Laruelle et al. 1993). The peak activities in these regions have been observed earlier than the striatal activity, at about 4 hours post-injection (Brücke et al. 1993). In a preliminary study by Brücke et al. (1993) the hypothalamus/midbrain activity reflecting SERT binding was mildly diminished in PD patients, but Kim et al (1997) could not verify this in the early stages of PD.
3 Aims of the study
The main purposes of the present study were to identify and quantitatively evaluate autonomic dysfunction in de novo PD and to assess the effects of PD medications on autonomic regulation. The more specific aims of the individual studies were:
I To evaluate cardiovascular autonomic regulation disturbances in untreated PD patients, and to assess the effect of levodopa, bromocriptine and selegiline monotherapy on the cardiovascular functions by measuring cardiovascular autonomic reflexes.
II To evaluate dynamic measures of HR behaviour in PD by using 24-hour ambulatory ECG recordings as indicators of tonic cardiovascular autonomic dysfunction.
III To study the sudomotor dysfunction in PD with special reference to PD medication by analysing the SSR.
IV To assess the dopamine and serotonin transporter binding in PD with β-CIT SPECT and to correlate the findings with autonomic dysfunction.

4 Subjects and methods
4.1 Subjects
The study was carried out in the Departments of Neurology and Clinical Neurophysiology, University of Oulu, during the years 1995–2001. The study was approved by the Ethics Committee of the Medical Faculty, University of Oulu, and carried out according to the principles of the Declaration of Helsinki. All patients and control subjects gave their informed consent before their inclusion in the study. Sixty consecutive patients with idiopathic PD fulfilling the Parkinson’s Disease Society Brain Bank clinical criteria (Daniel & Lees 1993), referred to the Department of Neurology, Oulu University Hospital, because of extrapyramidal symptoms, were included in the study. Patients with manifestations of other central or peripheral nervous system disorders and patients with any other disease or medication known to affect the ANS were excluded. None of the patients had received any antiparkinsonian medication or used drugs affecting the dopaminergic or serotonergic systems.
The patients were randomly assigned into three groups (n=20 in each) to commence levodopa/carbidopa (100/25 mg), bromocriptine or selegiline medication (random sampling using closed envelopes). The doses of levodopa and bromocriptine were individually adjusted to reach the therapeutic level, the mean daily doses being 280 mg (range 200-300 mg) and 9 mg (range 7.5-10 mg), respectively. The daily dose of selegiline was 10 mg. The treatment period was 6 months (the dose of the medication was kept stable during the last 3 months) and was followed by a 6-week washout period. There were no statistical differences in disease duration and age between the three medication groups, but there were more women in the bromocriptine medication group than in the other medication groups.
There were six dropouts due to insufficient therapeutic response (one patient receiving selegiline) or to adverse effects of the treatment (two patients receiving levodopa and three receiving bromocriptine). Additionally one patient (receiving levodopa) discontinued the medication during the study. These patients were excluded from Study III. One patient was excluded because of recurrent supraventricular arrhythmias during the recording of cardiovascular (I) and ECG (II) responses, which made the data ineligible for analysis. Two further patients were excluded due to technical reasons in the

38
cardiovascular reflex recordings (I) and three patients in the ECG recordings (II). The clinical follow up of the patients was continued after the study trial period, the mean follow up time being 3 years (range 1.3-4.6 years). This post-trial follow up disclosed one case of progressive supranuclear palsy and one case of MSA, both of which were therefore also excluded from all studies.
The clinical characteristics of the patients and control subjects in the individual studies are presented in Table 1. The mean age of the control subjects and PD patients in the individual studies did not differ significantly. In Study III the heights and weights of the PD patients were equal, and in the other studies considerably overweighed subjects were not included in the study. All control groups consisted of healthy volunteers with no medication affecting the ANS, dopaminergic and serotonergic systems. Altogether 117 controls participated in the studies. In Studies I, III and IV the control subjects were recruited from relatives and acquaintances of the PD patients and hospital staff. In Study II the control group consisted of some of the healthy people who were participating in a trial comparing the characteristics of hypertensive and normotensive subjects randomly selected by their social security code from the population of the city of Oulu. They all underwent a thorough physical examination.

39
Table 1. Characteristics of the subjects in the individual studies.
Study No. of subjects
____________
women men
Age, mean years
(SD, range)
Duration of
disease,
mean years
(SD)
Hoehn and
Yahr stage,
median
(range)
UPDRS total
score, mean
(SD)
Study I
All PD patients
Levodopa
Bromocriptine
Selegiline
Control subjects
Study II
PD patients
Control subjects
Study III
All PD patients
Levodopa
Bromocriptine
Selegiline
Control subjects
Study IV
PD patients
Control subjects
23
6
12
5
18
22
15
18
4
9
5
5
14
8
35
13
8
14
10
32
32
33
12
8
13
15
15
13
61.7 (12.5, 38-75)
64.5 (10.1, 48-75)
59.7 (9.9, 38-71)
61.0 (12.8, 39-75)
57.1 (16.4, 38-85)
61.4 (10.9, 38-75)
59.6 (9.4, 42-81)
61.6 (11.0, 38-75)
65.1 (10.1, 48-75)
59.3 (9.8, 38-71)
60.6 (12.8, 39-75)
59.0 (10.0, 44-82)
57.1 (10.2, 38-73)
54.3 (11.7, 33-73)
1.9 (1.9)
1.8 (1.2)
1.9 (2.3)
2.0 (2.2)
1.7 (1.6)
1.9 (1.9)
1.7 (1.1)
1.9 (2.3)
2.0 (2.2)
1.5 (1.2)
1.75 (1-3)
1.5 (1-3)
2.0 (1-3)
1.5 (1-2.5)
1.5 (1-3)
1.75 (1-3)
1.5 (1-3)
2.0 (1-3)
1.5 (1-2.5)
1.5 (1-3)
31.6 (14.7)
33.6 (15.8)
32.1 (15.7)
29.4 (12.5)
31.7 (14.3)
30.8 (14.6)
31.9 (15.8)
31.8 (15.7)
28.8 (12.6)
28.3 (13.3)
4.2 Methods
4.2.1 Clinical examination
The author examined all the PD patients with special attention being paid to neurological deficits caused by PD, and to symptoms and signs referring to autonomic dysfunction. The clinical examination was performed before starting the PD medication, after six months on medication and after a 6-week washout period. The clinical disability caused by PD was graded using the Hoehn and Yahr stages (Hoehn & Yahr 1967) and the UPDRS (Fahn et al. 1987).
The clinical severity of the autonomic failure was presented as the sum of scores obtained on 3-point rating scales used to assess 11 different modalities of ANS measures (postural dizziness, disturbances of sweating, urinary function, bowel function, sexual function, HR regulation, salivation, breathing, signs of peripheral circulation disturbances, sluggish pupillary reactions and seborrhoea), the dysfunction being graded from 0 to 2 (0 = absent, 1 = mild, 2 = moderate to severe) (Turkka 1987). Orthostatic

40
hypotension was evaluated in a test where patients stood up after a 30-minute rest taken in a supine position and stood still in an upright position for 10 minutes. The BP was recorded just before and immediately after standing up, as well as at 1-minute intervals during the standing. Orthostatic hypotension was defined as a reduction of systolic BP of at least 20 mmHg or of diastolic BP of at least 10 mmHg within 3 minutes of standing (Consensus statement 1996).
4.2.2 Cardiovascular autonomic reflex tests (Study I)
Cardiovascular autonomic function tests, based on HR and BP responses at rest and after various stimuli, were performed on all patients included in the study and on 28 control subjects under standardised environmental conditions between 8 and 9 a.m. before breakfast. The patients were allowed to take their regular drugs before the test. The tests were performed before PD medication, six months after starting the medication and after a 6-week washout period. First, with the patient in a supine position on the tilt table, the maximum contraction power (handgrip) of the patient’s dominant hand was measured three times with a dynamometer for the isometric work test. At the end of a 30-minute resting period, the baseline BP was measured three times using an automatic arm sphygmomanometer. Thereafter, the following five tests were performed: normal breathing, paced breathing at six breaths per minute, the Valsalva manoeuvre, upright tilting and isometric work. The interval between these tests was standardised so that the next test was not begun until HR and BP had returned to the rest level.
In the analyses of the deep breathing test the thermistor signal ascertained that the paced deep but not maximum breathing was evenly performed. In the Valsalva manoeuvre the blowing pressure was monitored and only steadily maintained blowings were accepted. In the isometric work test the contraction power on the dynamometer was monitored graphically and thereby maintained at the optimal level.
The ECG and nasal thermistor signals were conveyed through a 12-bit A/D converter with a sampling frequency of 320 Hz to a PC and were analysed after visual off-line checking of the raw ECG and breathing signal. Test performances in deep breathing, the Valsalva manoeuvre and the isometric work tests were checked on-line and off-line and only adequately accomplished test performances were accepted for analysis (Turkka et al. 1987b, Havanka-Kanniainen et al. 1988, Suominen 1997).
In the normal breathing test, the consecutive RR intervals for a period of 10 minutes were measured from the ECG, and the standard deviation (SD) of the RR intervals was used as a variable. Successive RR intervals were measured and the square root of the mean squares of the differences between successive intervals (rMSSD) was calculated, so reflecting the true beat-to-beat variation.
In the deep breathing test, the ratios of the longest (expiration) to the shortest (inspiration) RR interval of five consecutive breathing cycles was calculated. The test was performed twice, and the higher median RR interval ratio of the tests was used as the ”maximum-minimum (max-min) ratio”.
In the Valsalva manoeuvre, the ratio on the longest RR interval after blowing (at 40 mm Hg or at least 50% of the subject’s maximum blowing power for 15 seconds) to the
41
shortest one during blowing was calculated. The highest ratio of three manoeuvres was used as the ”Valsalva ratio”.
In the tilting test, the ratio of the longest RR interval at approximately beat 30 (between beats 20 to 40) to the shortest RR interval at approximately beat 15 (between beats 10 to 20) after quick passive upright tilting (2 seconds, 80°) was used as the ”30:15 ratio”. The systolic and diastolic BP responses to passive upright tilt were measured immediately and at 2 and 5 minutes after tilting. The largest drop (or lowest increase) in systolic and diastolic BP was also quantified. The largest increase in systolic and diastolic BP during a 5-minute period of sustained handgrip with a dynamometer at 30% of the maximum voluntary force was also noted (the isometric work test).
4.2.3 Heart rate variability analysis (Study II)
4.2.3.1 ECG recordings
All the subjects were monitored for 24 hours with an ambulatory two-channel ECG recorder (Electrocardiocorder Del Mar Avionics, California). The PD patients were encouraged to continue their daily activities during the recording in a hospital ward.
The ECG data from the recordings were sampled digitally and transferred from the Oxford Medilog scanner to a microcomputer for analysis of HRV. All the RR interval time series were first edited automatically, after which careful manual editing was performed by visual inspection of the RR intervals. Each RR interval time series was passed through a filter that eliminates premature beats and artefacts and deletes the filling gaps (Korpelainen et al. 1999). In the final analysis of the linear and non-linear components of HRV, 24-hour measurements were divided into segments of 8000 RR intervals, and only segments with >85% sinus beats were included.
4.2.3.2 Time domain and spectral analysis
The mean duration of all RR intervals and the standard deviation of the RR intervals (SDNN) in the whole epoch were computed as time domain measures. An autoregressive model was used to estimate the power spectrum densities of the HRV (Kay & Marple 1981). The size of 20 was used as the model order in the analysis of the RR interval data. The power spectra were quantified by measuring the area in three frequency bands: 0.005 to 0.04 Hz (VLF), 0.04 to 0.15 Hz (LF) and 0.15 to 0.4 Hz (HF).

42
4.2.3.3 Poincaré plot analysis
For quantitative two-dimensional vector analysis, the standard deviation of the continuous long-term RR interval variability (SD2) and the instantaneous beat to beat RR interval variability (SD1) were analysed, and visually presented as Poincaré plot scatter grams in which each RR interval is plotted as a function of the previous one (Tulppo et al. 1996, Korpelainen et al. 1999). In the computerised analysis, the Poincaré plot was first turned 45° clockwise, and the standard deviation of the plot data was then computed around the horizontal axis, passing through the data centre (SD1). The standard deviation of the continuous long-term RR intervals was quantified by turning the plot 45° counterclockwise (SD2) and by computing the data points around the horizontal axis, passing through the centre of the data.
4.2.3.4 Power-law relationship analysis
The power-law relationship of the RR interval variability, a spectral measure reflecting the distribution of the spectral characteristics of the RR interval oscillations, was calculated from the frequency range of 10-4 to 10-2 by a previously described method (Bigger et al. 1992). The point power spectrum was logarithmically smoothed in the frequency domain, and the power was integrated into bins spaced 0.0167 log(Hz) apart. A robust line-fitting algorithm of log(power) on log(frequency) was then applied to the power spectrum between 10-4 to 10-2, and the slope of this line was calculated. This frequency band was chosen on the basis of previous observations regarding the linear relationship between log(power) and log(frequency) in the frequency band (Saul et al. 1991, Bigger et al. 1996).
4.2.4 Sudomotor evaluation using the sympathetic skin response (Study III)
SSRs to various stimuli were used to assess the sympathetic sudomotor activity in 51 untreated PD patients and 20 age-matched controls. The SSR recordings of the PD patients were performed before PD medication, six months after starting the medication and after a 6-week washout period. The experiment was performed under standard conditions in an illuminated and silent room with ambient temperature at 22°C to 24°C. The subject was awake and relaxed in a lying position.
Recordings were carried out using an electromyograph (Counterpoint®, Dantec, Skovlunde, Denmark) with an amplifier gain of 0.1–2 mV per division and filter settings at 0.2–50 Hz. The SSRs were provoked by using two types of stimulation separately: an auditory click (0.1 ms, 120 dB) delivered to both ears, and an electric single square pulse (0.5 ms, intensity adjusted to 20% to 30% above the motor threshold) for stimulating the median nerve at the wrist. Both types of stimulation were performed two times and given at irregular rates after intervals of at least 60 seconds. The electrodes (discs) connected to
43
the negative input of the amplifier were attached to the palms of the hands and soles of the feet, and the electrodes connected to the positive input of the amplifier were attached to the dorsum of the hands and feet. Skin temperatures on the recording areas were measured in all the recording sessions. There were no skin temperature differences between the PD patients and the controls and between the recording sessions, and there was no difference between the left and right body sides of the subjects.
The data were sampled digitally with a sampling frequency of 34 Hz, and transferred to a computer for the off-line analysis of the SSR. SSR signals were recorded simultaneously on both hands and feet and the recording continued for two minutes after each stimulus, and the mean peak-to-peak amplitudes and latencies of the right and the left side of the recording that showed greater responses were included in the analysis. The number of SSRs after a single stimulus was analysed. Only the SSR waves showing the same morphology and having a minimum of 25 % of the amplitude of the primary response were considered. The response adaptation (an amplitude decrease of 30% in a repeated procedure) from the two successive stimuli was calculated.
4.2.5 Brain receptor imaging using ββββ-CIT SPECT (Study IV)
Striatal dopamine transporters (DATs) were evaluated in 29 and serotonin transporters (SERTs) in 27 of the PD patients included in the study and compared to 21 and 16 healthy control subjects, respectively. SPECT studies were performed using a dual head gamma camera (ADAC Vertex) equipped with high-resolution fan beam collimators. SPECT scans were done 4 and 24 hours after the slow (30 s) intravenous injection of 120-185 Mbq high specific activity [123I]β-CIT (MAP, Medical Technologies Inc., Tikkakoski, Finland). The ligand was synthesized according to a method described previously (Hiltunen et al. 1998). Thyroid uptake was blocked with 400 mg potassium perchlorate taken orally 30 min before tracer injection.
The investigator performing the region-of-interest (ROI) analyses was unaware of the subject demographics. Transaxial slices oriented along the orbitomeatal line were reconstructed and the two slices corresponding to the highest striatal uptake were summed, yielding a final slice of thickness of 9.2 mm (Laine et al. 1999). The ROIs were drawn over the right and left striata using a colour scale with about 60% isocontour cutoff boundaries for delineation. The size of the average striatal ROI was about 20 pixels. Occipital white matter (OWM) ROIs were drawn as a reference (nondisplaceable activity) because postmortem studies have shown a very low density of DAT and SERT in cerebral cortices and the cerebellum (Laruelle et al. 1988, Palacios et al. 1988, De Keyser et al. 1989). The cerebellar region was not taken as a reference for nondisplaceable activity since this region is situated close to the bed surface and could cause interference for raw SPECT data. In addition to the whole striatal areas the putamen and caudate ROIs were determined. Average templates for the putamen and caudate nuclei in 6 controls were determined using magnetic resonance imaging. These average templates were placed individually into the putamen and caudate areas. The average ROI areas for the putamen and caudate were 10 and 9 pixels, respectively. In addition to the striatal dopamine areas ROIs for monoamine transporters, mainly reflecting SERT (Laruelle et al. 1988), were
44
visually positioned on the summed transversal slices of the hypothalamus/midbrain (including the raphe nuclei, substantia nigra and colliculi; average size 9 pixels), the thalamus (average size 11 pixels) and the medial prefrontal area at the striatal level (average size 15 pixels). The hypothalamus/midbrain activity was consistently detected on the midline about 12 mm below the level of the striatal transversal slice. These areas were identified by reference to the Talairach and Tournoux stereotactic atlas (1988) and magnetic resonance imaging scans were performed in 6 controls.
Specific striatal DAT binding was calculated as the ratio of the total binding in the striatum minus the nondisplaceable binding in the OWM divided by the OWM, i.e. (STRIATUM-OWM)/ OWM, reflecting the specific-to-nondisplaceable binding. As it has been shown that a state of equilibrium in the striatal and occipital areas exists at 20–24 hours after the injection, the ratio at this time point was used as an estimate of the Binding Potential (Abi-Dargham et al. 1996). This estimate, the binding potential index (BPI), reflects the equilibrium partition coefficient described by Salmon et al. (1990). A caudate to putamen uptake ratio was calculated as the ratio of the BPI of the caudate to the BPI of the putamen.
4.2.6 Statistics
The demographic data between the PD patients and controls, and between the medication groups were analysed with the Mann-Whitney U two-sample test (continuous data) and the χ2 test (rate and proportional data). The results of the clinical evaluation of the disease severity and autonomic dysfunction were correlated with Spearman’s correlation coefficients, as were the results of the autonomic disability grading and the β-CIT SPECT measurements. The values of the HR responses (after logarithmic transformation) of the PD patients and the control subjects in Study I were compared with each other using covariance analysis with age and baseline HR as covariants, since cardiovascular autonomic responses have been shown to be dependent on both age and HR (Wieling & Karemaker 1999). Covariance analysis was also used to compare the BP responses in the PD patients and the control subjects with age as covariant. The BP responses were normalised to the baseline BP by expressing BP change as a percentage of the baseline BP. For the isometric work the genders were analysed separately as the BP responses are greater in males than females (Piha 1993, Khurana & Setty 1996), while other parameters were analysed without separation of the genders (Matthews 1988, Braune et al. 1996). Within the patient groups the comparisons between the cardiovascular responses at different time points were performed using the general linear model with repeated measures analysis. Friedman’s test was used to evaluate the prevalence of orthostatic hypotension at different time points.
The Mann-Whitney U two-sample test was used for comparing the HRV values (II) and the SSR amplitudes and latencies (III) of the PD patients with those of the control subjects. The correlation between the clinical parameters of PD and the various measures of HRV was analysed with Spearman’s correlation coefficient (II). The Wilcoxon matched pairs test was used to compare the SSR amplitudes and latencies at different time points and to compare the responses of the affected limbs with those of the

45
contralateral limbs in patients with hemiparkinsonian syndrome (III). The number of PD patients and control subjects showing repetitive responses and adaptation was compared with the χ2 test.
Comparisons of the regional SPECT data of the PD patients and controls were made utilizing unpaired two-tailed t tests since the results of the measurements were normally distributed (IV). ANOVA with age as covariant was used to factor out age in the comparisons between the groups. Relationships between variables were calculated with Pearson’s correlation coefficient. The equality of age was tested with the Mann-Whitney U-test. Bonferroni correction was not used since it is highly conservative for large numbers of comparisons (Altman 1991). All analyses were made on observed cases and calculated using the SPSS Windows version 7.0.

5 Results
5.1 Clinical findings
Most of the 58 PD patients (87%) had subjective symptoms referring to ANS dysfunction. The most common complaints were about disturbances of sweating (51%), urinary function (48%), bowel function (41%) and postural dizziness (40%). The male patients frequently suffered from impotence (52%). In the clinical examination signs of autonomic disturbances could be found in 85% of the PD patients, the most common finding being peripheral circulation disturbances (60%). The autonomic symptoms and signs were mild in most cases as only 10% of the PD patients had moderate or severe clinical autonomic manifestations. In the orthostatic test one third of the patients had orthostatic hypotension (at least a 20 mmHg reduction in systolic BP within 3 minutes of standing).
The severity of clinical autonomic dysfunction correlated with the Hoehn and Yahr stage, with the UPDRS total score, and with the degree of hypokinesia and rigidity but not of tremor of the major motor signs. Of the individual autonomic symptoms the severity of constipation and urinary disturbances correlated with the Hoehn and Yahr stage, the UPDRS total score, rigidity and hypokinesia. Furthermore, the degree of impotence correlated strongly with hypokinesia and rigidity. The correlation coefficients of clinical autonomic symptoms and clinical measures of PD are presented in Table 2.
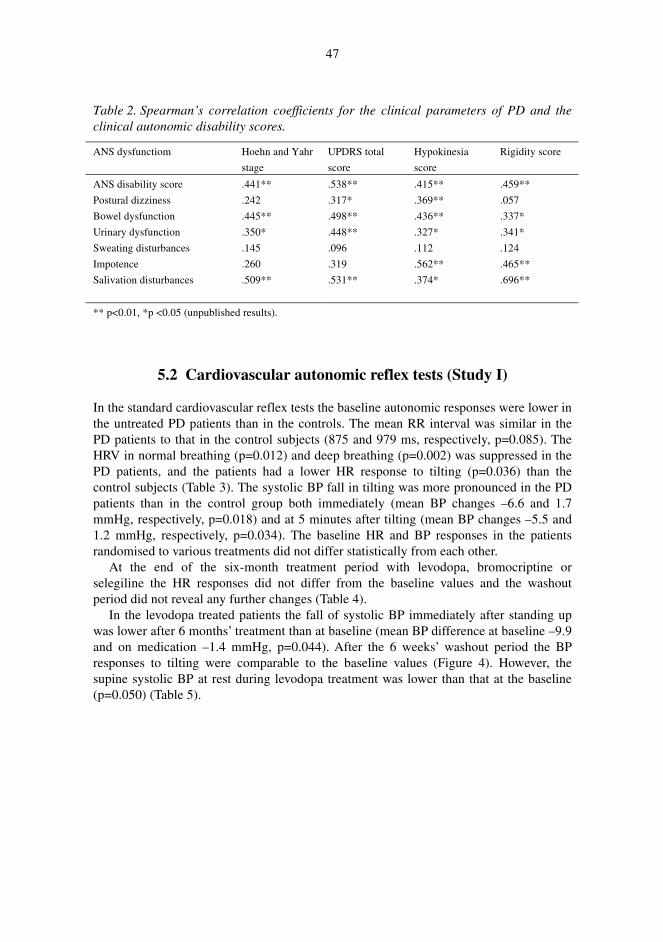
47
Table 2. Spearman’s correlation coefficients for the clinical parameters of PD and the clinical autonomic disability scores.
ANS dysfunctiom Hoehn and Yahr
stage
UPDRS total
score
Hypokinesia
score
Rigidity score
ANS disability score
Postural dizziness
Bowel dysfunction
Urinary dysfunction
Sweating disturbances
Impotence
Salivation disturbances
.441**
.242
.445**
.350*
.145
.260
.509**
.538**
.317*
.498**
.448**
.096
.319
.531**
.415**
.369**
.436**
.327*
.112
.562**
.374*
.459**
.057
.337*
.341*
.124
.465**
.696**
** p<0.01, *p <0.05 (unpublished results).
5.2 Cardiovascular autonomic reflex tests (Study I)
In the standard cardiovascular reflex tests the baseline autonomic responses were lower in the untreated PD patients than in the controls. The mean RR interval was similar in the PD patients to that in the control subjects (875 and 979 ms, respectively, p=0.085). The HRV in normal breathing (p=0.012) and deep breathing (p=0.002) was suppressed in the PD patients, and the patients had a lower HR response to tilting (p=0.036) than the control subjects (Table 3). The systolic BP fall in tilting was more pronounced in the PD patients than in the control group both immediately (mean BP changes –6.6 and 1.7 mmHg, respectively, p=0.018) and at 5 minutes after tilting (mean BP changes –5.5 and 1.2 mmHg, respectively, p=0.034). The baseline HR and BP responses in the patients randomised to various treatments did not differ statistically from each other.
At the end of the six-month treatment period with levodopa, bromocriptine or selegiline the HR responses did not differ from the baseline values and the washout period did not reveal any further changes (Table 4).
In the levodopa treated patients the fall of systolic BP immediately after standing up was lower after 6 months’ treatment than at baseline (mean BP difference at baseline –9.9 and on medication –1.4 mmHg, p=0.044). After the 6 weeks’ washout period the BP responses to tilting were comparable to the baseline values (Figure 4). However, the supine systolic BP at rest during levodopa treatment was lower than that at the baseline (p=0.050) (Table 5).

48
Table 3. HR responses in PD patients at baseline and in the control subjects.
Variable Control subjects
PD patients at baseline
SD of RR intervals
rMSSD of RR intervals
Max-min ratio
Valsalva ratio
30:15 ratio
35.3 (29.2-40.5)
27.9 (22.7-33.2)
1.26 (1.22- 1.31)
1.81 (1.68-1.93)
1.12 (1.09-1.16)
26.4 (23.4-29.4)*
20.9 (17.1-24.7)*
1.16 (1.14-1.18)**
1.67 (1.59-1.76)
1.07 (1.06-1.09)*
* p<0.05, ** p<0.01. HR variables of the PD patients and control subjects compared using covariance analysis.
The values, mean (95% CI), are age and baseline RR interval corrected (data from Study I).
Table 4. HR responses in PD medication groups at baseline, after 6 months’ medication and after a 6 weeks’ the washout period.
SD of RR intervals
Max-min ratio Valsalva ratio 30:15 ratio
Levodopa (n=15)
Baseline
On medication
Washout
Bromocriptine (n=17)
Baseline
On medication
Washout
Selegiline (n=17)
Baseline
On medication
Washout
26.4 (19.6-33.2)
22.6 (17.2-28.1)
24.3 (19.9-28.7)
27.5 (21.2-33.1)
27.3 (20.5-34.0)
26.9 (23.7-35.5)
26.2 (20.8-31.6)
26.0 (22.2-29.8)
30.7 (23.0-38.4)
1.16 (1.10-1.21)
1.18 (1.11-1.25)
1.14 (1.09-1.20)
1.18 (1.11-1.23)
1.17 (1.11-1.23)
1.18 (1.13-1.22)
1.16 (1.14-1.19)
1.14 (1.11-1.17)
1.16 (1.13-1.19)
1.60 (1.45-1.74)
1.66 (1.52-1.80)
1.63 (1.49-1.77)
1.82 (1.63-2.01)
1.88 (1.66-2.10)
1.94 (1.74-2.14)
1.65 (1.50-1.80)
1.70 (1.57-1.84)
1.72 (1.59-1.84)
1.07 (1.04-1.11)
1.07 (1.04-1.11)
1.06 (1.03-1.14)
1.09 (1.05-1.13)
1.07 (1.02-1.13)
1.07 (1.03-1.14)
1.07 (1.02-1.12)
1.09 (1.04-1.14)
1.08 (1.06-1.10)
The values are mean (95% CI), age and baseline RR interval adjusted (data from Study I).
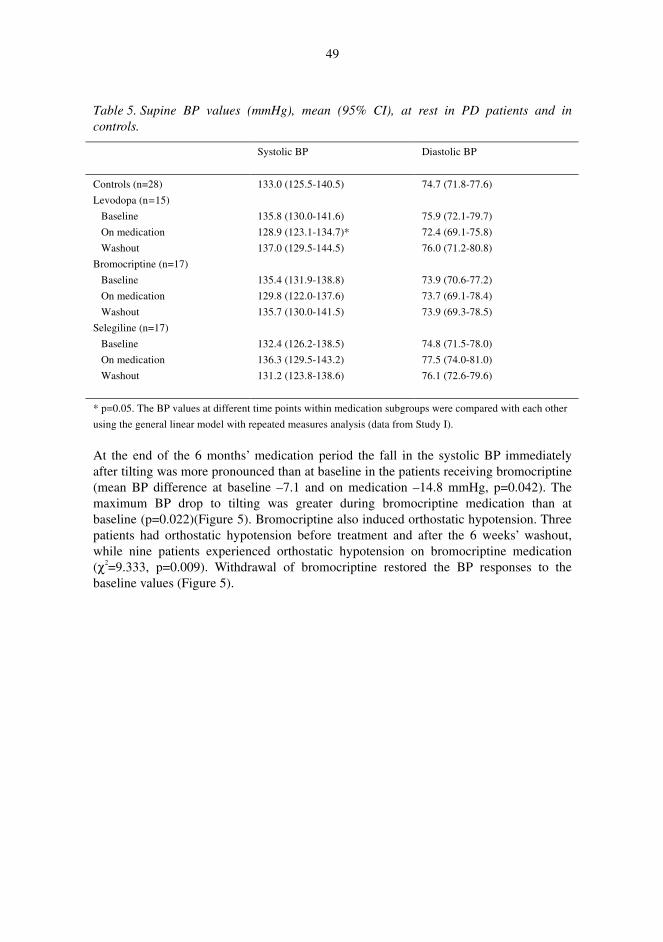
49
Table 5. Supine BP values (mmHg), mean (95% CI), at rest in PD patients and in controls.
Systolic BP
Diastolic BP
Controls (n=28)
Levodopa (n=15)
Baseline
On medication
Washout
Bromocriptine (n=17)
Baseline
On medication
Washout
Selegiline (n=17)
Baseline
On medication
Washout
133.0 (125.5-140.5)
135.8 (130.0-141.6)
128.9 (123.1-134.7)*
137.0 (129.5-144.5)
135.4 (131.9-138.8)
129.8 (122.0-137.6)
135.7 (130.0-141.5)
132.4 (126.2-138.5)
136.3 (129.5-143.2)
131.2 (123.8-138.6)
74.7 (71.8-77.6)
75.9 (72.1-79.7)
72.4 (69.1-75.8)
76.0 (71.2-80.8)
73.9 (70.6-77.2)
73.7 (69.1-78.4)
73.9 (69.3-78.5)
74.8 (71.5-78.0)
77.5 (74.0-81.0)
76.1 (72.6-79.6)
* p=0.05. The BP values at different time points within medication subgroups were compared with each other
using the general linear model with repeated measures analysis (data from Study I).
At the end of the 6 months’ medication period the fall in the systolic BP immediately after tilting was more pronounced than at baseline in the patients receiving bromocriptine (mean BP difference at baseline –7.1 and on medication –14.8 mmHg, p=0.042). The maximum BP drop to tilting was greater during bromocriptine medication than at baseline (p=0.022)(Figure 5). Bromocriptine also induced orthostatic hypotension. Three patients had orthostatic hypotension before treatment and after the 6 weeks’ washout, while nine patients experienced orthostatic hypotension on bromocriptine medication (χ2=9.333, p=0.009). Withdrawal of bromocriptine restored the BP responses to the baseline values (Figure 5).

50
Fig. 5. Mean (+SEM) systolic BP change immediately after tilting (a), and the maximum systolic BP fall after tilting (b), in PD patients randomised to levodopa, bromocriptine or selegiline at baseline, during medication and after the washout period. The results on medication and after washout are compared to the baseline values using the Wilcoxon Signed Ranks test, * p<0.05 (data from Study I).

51
Selegiline increased the fall in systolic BP immediately after tilting compared to the baseline results (mean BP change at baseline -0.6 and on medication-12.6 mmHg, p=0.030). The BP responses to tilting returned to the baseline level after the washout period. The supine systolic BP at rest was higher during the selegiline treatment than at baseline (p=0.049) (Table 5).
In the male patients the systolic BP reaction to the isometric work test increased during the levodopa treatment, but this increase over the baseline values did not reach statistical significance (mean BP change at baseline 48.4 and on medication 56.4 mmHg, p=0.100). In men receiving bromocriptine the systolic responses to the isometric work test were diminished (mean BP change at baseline 47.7 and on medication 35.4 mmHg, p=0.076), and the selegiline treatment also diminished the systolic BP responses of men to the isometric work (mean BP change at baseline 51.7 and on medication 42.1 mmHg, p=0.038). The BP responses to the isometric work in all the treatment groups returned to the baseline values after the washout period. Medication caused no significant changes in the BP responses to the isometric work in women, but the number of women was too small for reliable statistical analysis.
5.3 Heart rate variability measures (Study II)
The conventional linear time and frequency domain measures of HRV were lower in patients with PD than in the healthy control subjects. The SDNN values (p=0.024) and the VLF (p=0.001), LF (p=0.009) and HF (p=0.004) spectral components were lower in the PD patients than in the control subjects. The RR interval did not differ (p=0.905) between the patients and control subjects. The SD1 and SD2 of the Poincaré measures in the patients did not differ from the values of the control group (p=0.053 and p=0.186). The slope of the power-law relation of the HRV was deeper (p=0.002) in the patient group than in the control subjects. The values of the various measures of HRV in the patients and the control subjects are presented in Table 6. Figures 6, 7, and 8 present examples of the power spectrum analyses of HRV, Poincaré plots and power-law relation slopes from a PD patient whose values represent the median for the spectral parameters and from a healthy subject.
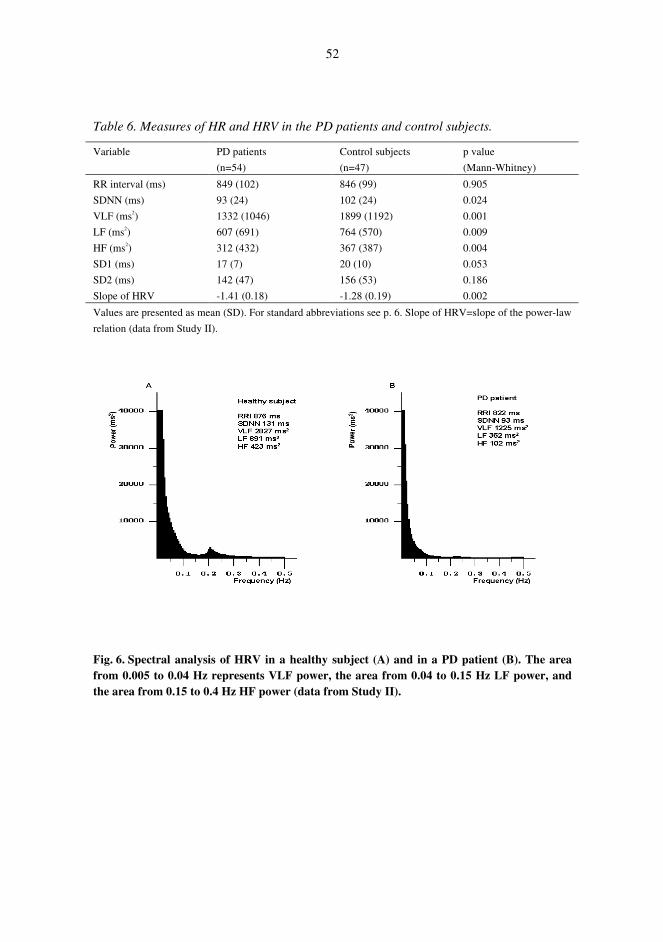
52
Table 6. Measures of HR and HRV in the PD patients and control subjects.
Variable PD patients
(n=54)
Control subjects
(n=47)
p value
(Mann-Whitney)
RR interval (ms)
SDNN (ms)
VLF (ms2)
LF (ms2)
HF (ms2)
SD1 (ms)
SD2 (ms)
Slope of HRV
849 (102)
93 (24)
1332 (1046)
607 (691)
312 (432)
17 (7)
142 (47)
-1.41 (0.18)
846 (99)
102 (24)
1899 (1192)
764 (570)
367 (387)
20 (10)
156 (53)
-1.28 (0.19)
0.905
0.024
0.001
0.009
0.004
0.053
0.186
0.002
Values are presented as mean (SD). For standard abbreviations see p. 6. Slope of HRV=slope of the power-law
relation (data from Study II).
Fig. 6. Spectral analysis of HRV in a healthy subject (A) and in a PD patient (B). The area from 0.005 to 0.04 Hz represents VLF power, the area from 0.04 to 0.15 Hz LF power, and the area from 0.15 to 0.4 Hz HF power (data from Study II).

53
Fig. 7. Poincaré plots from a healthy subject (A) and a PD patient (B). SD1 indicates SD of instantaneous RR interval variability measured from axis 1, and SD2 indicates SD of long-term continuous RR interval variability measured from axis 2 (data from Study II).
Fig. 8. Slopes of power-law relation of a healthy subject (A) and a PD patient (B) (data from Study II).
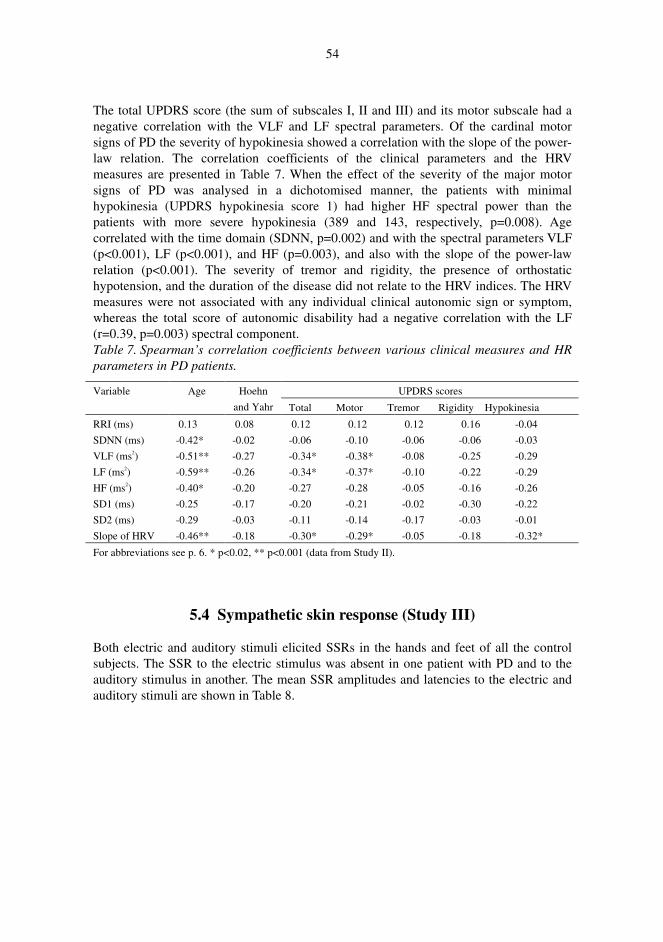
54
The total UPDRS score (the sum of subscales I, II and III) and its motor subscale had a negative correlation with the VLF and LF spectral parameters. Of the cardinal motor signs of PD the severity of hypokinesia showed a correlation with the slope of the power-law relation. The correlation coefficients of the clinical parameters and the HRV measures are presented in Table 7. When the effect of the severity of the major motor signs of PD was analysed in a dichotomised manner, the patients with minimal hypokinesia (UPDRS hypokinesia score 1) had higher HF spectral power than the patients with more severe hypokinesia (389 and 143, respectively, p=0.008). Age correlated with the time domain (SDNN, p=0.002) and with the spectral parameters VLF (p<0.001), LF (p<0.001), and HF (p=0.003), and also with the slope of the power-law relation (p<0.001). The severity of tremor and rigidity, the presence of orthostatic hypotension, and the duration of the disease did not relate to the HRV indices. The HRV measures were not associated with any individual clinical autonomic sign or symptom, whereas the total score of autonomic disability had a negative correlation with the LF (r=0.39, p=0.003) spectral component. Table 7. Spearman’s correlation coefficients between various clinical measures and HR parameters in PD patients.
UPDRS scores Variable Age Hoehn
and Yahr Total Motor Tremor Rigidity Hypokinesia
RRI (ms)
SDNN (ms)
VLF (ms2)
LF (ms2)
HF (ms2)
SD1 (ms)
SD2 (ms)
Slope of HRV
0.13
-0.42*
-0.51**
-0.59**
-0.40*
-0.25
-0.29
-0.46**
0.08
-0.02
-0.27
-0.26
-0.20
-0.17
-0.03
-0.18
0.12
-0.06
-0.34*
-0.34*
-0.27
-0.20
-0.11
-0.30*
0.12
-0.10
-0.38*
-0.37*
-0.28
-0.21
-0.14
-0.29*
0.12
-0.06
-0.08
-0.10
-0.05
-0.02
-0.17
-0.05
0.16
-0.06
-0.25
-0.22
-0.16
-0.30
-0.03
-0.18
-0.04
-0.03
-0.29
-0.29
-0.26
-0.22
-0.01
-0.32*
For abbreviations see p. 6. * p<0.02, ** p<0.001 (data from Study II).
5.4 Sympathetic skin response (Study III)
Both electric and auditory stimuli elicited SSRs in the hands and feet of all the control subjects. The SSR to the electric stimulus was absent in one patient with PD and to the auditory stimulus in another. The mean SSR amplitudes and latencies to the electric and auditory stimuli are shown in Table 8.
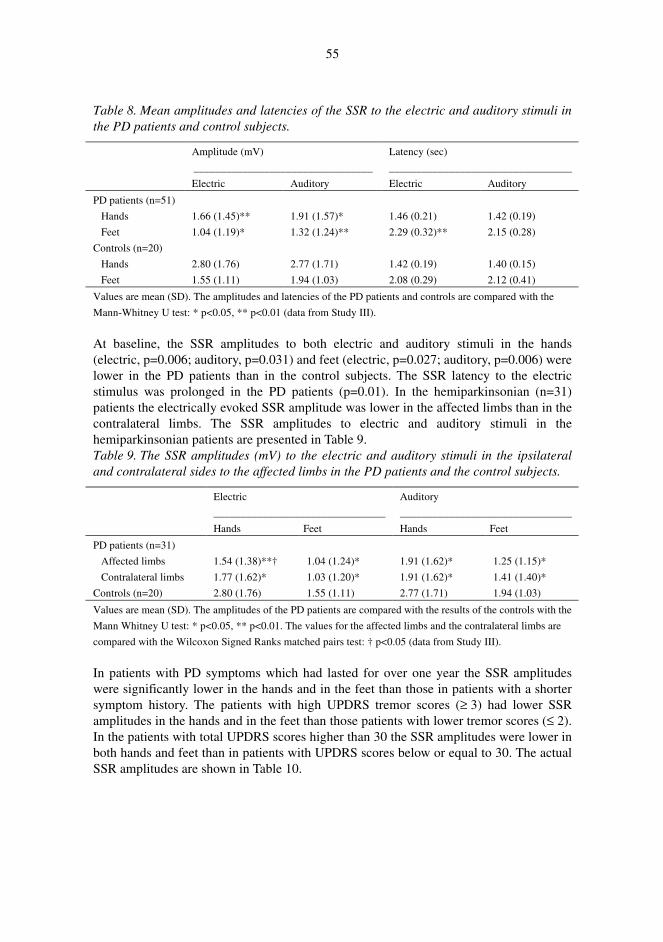
55
Table 8. Mean amplitudes and latencies of the SSR to the electric and auditory stimuli in the PD patients and control subjects.
Amplitude (mV)
_________________________________
Latency (sec)
__________________________________
Electric Auditory Electric Auditory
PD patients (n=51)
Hands
Feet
Controls (n=20)
Hands
Feet
1.66 (1.45)**
1.04 (1.19)*
2.80 (1.76)
1.55 (1.11)
1.91 (1.57)*
1.32 (1.24)**
2.77 (1.71)
1.94 (1.03)
1.46 (0.21)
2.29 (0.32)**
1.42 (0.19)
2.08 (0.29)
1.42 (0.19)
2.15 (0.28)
1.40 (0.15)
2.12 (0.41)
Values are mean (SD). The amplitudes and latencies of the PD patients and controls are compared with the
Mann-Whitney U test: * p<0.05, ** p<0.01 (data from Study III).
At baseline, the SSR amplitudes to both electric and auditory stimuli in the hands (electric, p=0.006; auditory, p=0.031) and feet (electric, p=0.027; auditory, p=0.006) were lower in the PD patients than in the control subjects. The SSR latency to the electric stimulus was prolonged in the PD patients (p=0.01). In the hemiparkinsonian (n=31) patients the electrically evoked SSR amplitude was lower in the affected limbs than in the contralateral limbs. The SSR amplitudes to electric and auditory stimuli in the hemiparkinsonian patients are presented in Table 9. Table 9. The SSR amplitudes (mV) to the electric and auditory stimuli in the ipsilateral and contralateral sides to the affected limbs in the PD patients and the control subjects.
Electric
________________________________
Hands Feet
Auditory
________________________________
Hands Feet
PD patients (n=31)
Affected limbs
Contralateral limbs
Controls (n=20)
1.54 (1.38)**†
1.77 (1.62)*
2.80 (1.76)
1.04 (1.24)*
1.03 (1.20)*
1.55 (1.11)
1.91 (1.62)*
1.91 (1.62)*
2.77 (1.71)
1.25 (1.15)*
1.41 (1.40)*
1.94 (1.03)
Values are mean (SD). The amplitudes of the PD patients are compared with the results of the controls with the
Mann Whitney U test: * p<0.05, ** p<0.01. The values for the affected limbs and the contralateral limbs are
compared with the Wilcoxon Signed Ranks matched pairs test: † p<0.05 (data from Study III).
In patients with PD symptoms which had lasted for over one year the SSR amplitudes were significantly lower in the hands and in the feet than those in patients with a shorter symptom history. The patients with high UPDRS tremor scores (≥ 3) had lower SSR amplitudes in the hands and in the feet than those patients with lower tremor scores (≤ 2). In the patients with total UPDRS scores higher than 30 the SSR amplitudes were lower in both hands and feet than in patients with UPDRS scores below or equal to 30. The actual SSR amplitudes are shown in Table 10.
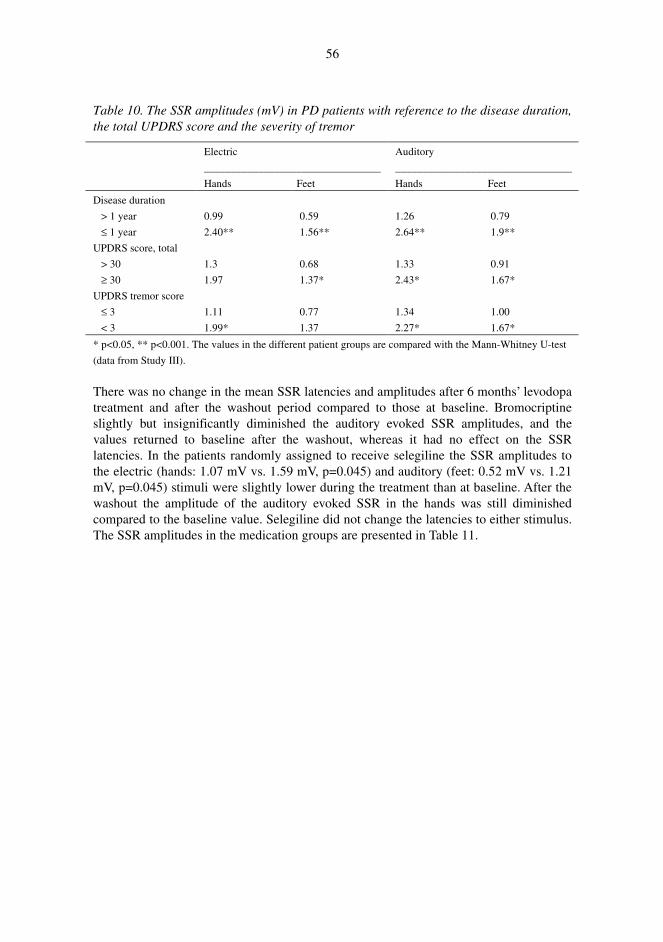
56
Table 10. The SSR amplitudes (mV) in PD patients with reference to the disease duration, the total UPDRS score and the severity of tremor
Electric
_________________________________
Hands Feet
Auditory
_________________________________
Hands Feet
Disease duration
> 1 year
≤ 1 year
UPDRS score, total
> 30
≥ 30
UPDRS tremor score
≤ 3
< 3
0.99
2.40**
1.3
1.97
1.11
1.99*
0.59
1.56**
0.68
1.37*
0.77
1.37
1.26
2.64**
1.33
2.43*
1.34
2.27*
0.79
1.9**
0.91
1.67*
1.00
1.67*
* p<0.05, ** p<0.001. The values in the different patient groups are compared with the Mann-Whitney U-test
(data from Study III).
There was no change in the mean SSR latencies and amplitudes after 6 months’ levodopa treatment and after the washout period compared to those at baseline. Bromocriptine slightly but insignificantly diminished the auditory evoked SSR amplitudes, and the values returned to baseline after the washout, whereas it had no effect on the SSR latencies. In the patients randomly assigned to receive selegiline the SSR amplitudes to the electric (hands: 1.07 mV vs. 1.59 mV, p=0.045) and auditory (feet: 0.52 mV vs. 1.21 mV, p=0.045) stimuli were slightly lower during the treatment than at baseline. After the washout the amplitude of the auditory evoked SSR in the hands was still diminished compared to the baseline value. Selegiline did not change the latencies to either stimulus. The SSR amplitudes in the medication groups are presented in Table 11.
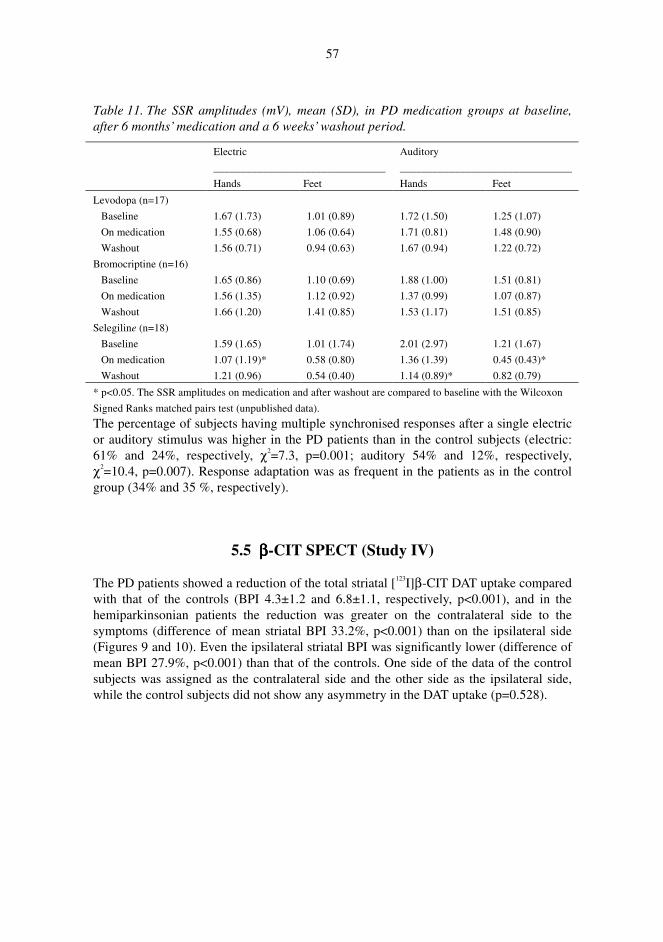
57
Table 11. The SSR amplitudes (mV), mean (SD), in PD medication groups at baseline, after 6 months’ medication and a 6 weeks’ washout period.
Electric
________________________________
Hands Feet
Auditory
________________________________
Hands Feet
Levodopa (n=17)
Baseline
On medication
Washout
Bromocriptine (n=16)
Baseline
On medication
Washout
Selegiline (n=18)
Baseline
On medication
Washout
1.67 (1.73)
1.55 (0.68)
1.56 (0.71)
1.65 (0.86)
1.56 (1.35)
1.66 (1.20)
1.59 (1.65)
1.07 (1.19)*
1.21 (0.96)
1.01 (0.89)
1.06 (0.64)
0.94 (0.63)
1.10 (0.69)
1.12 (0.92)
1.41 (0.85)
1.01 (1.74)
0.58 (0.80)
0.54 (0.40)
1.72 (1.50)
1.71 (0.81)
1.67 (0.94)
1.88 (1.00)
1.37 (0.99)
1.53 (1.17)
2.01 (2.97)
1.36 (1.39)
1.14 (0.89)*
1.25 (1.07)
1.48 (0.90)
1.22 (0.72)
1.51 (0.81)
1.07 (0.87)
1.51 (0.85)
1.21 (1.67)
0.45 (0.43)*
0.82 (0.79)
* p<0.05. The SSR amplitudes on medication and after washout are compared to baseline with the Wilcoxon
Signed Ranks matched pairs test (unpublished data).
The percentage of subjects having multiple synchronised responses after a single electric or auditory stimulus was higher in the PD patients than in the control subjects (electric: 61% and 24%, respectively, χ2=7.3, p=0.001; auditory 54% and 12%, respectively, χ2=10.4, p=0.007). Response adaptation was as frequent in the patients as in the control group (34% and 35 %, respectively).
5.5 ββββ-CIT SPECT (Study IV)
The PD patients showed a reduction of the total striatal [123I]β-CIT DAT uptake compared with that of the controls (BPI 4.3±1.2 and 6.8±1.1, respectively, p<0.001), and in the hemiparkinsonian patients the reduction was greater on the contralateral side to the symptoms (difference of mean striatal BPI 33.2%, p<0.001) than on the ipsilateral side (Figures 9 and 10). Even the ipsilateral striatal BPI was significantly lower (difference of mean BPI 27.9%, p<0.001) than that of the controls. One side of the data of the control subjects was assigned as the contralateral side and the other side as the ipsilateral side, while the control subjects did not show any asymmetry in the DAT uptake (p=0.528).

58
Fig. 9. The DAT BPI of the striatum and contralateral putamen of the affected extremities in PD patients and controls plotted against age (data from Study IV).
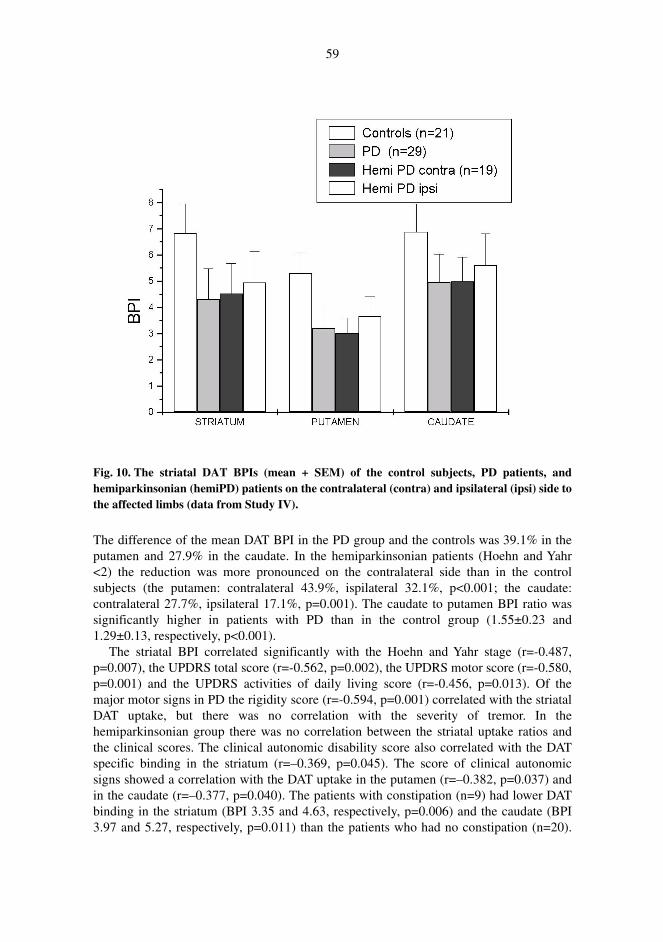
59
Fig. 10. The striatal DAT BPIs (mean + SEM) of the control subjects, PD patients, and hemiparkinsonian (hemiPD) patients on the contralateral (contra) and ipsilateral (ipsi) side to the affected limbs (data from Study IV).
The difference of the mean DAT BPI in the PD group and the controls was 39.1% in the putamen and 27.9% in the caudate. In the hemiparkinsonian patients (Hoehn and Yahr <2) the reduction was more pronounced on the contralateral side than in the control subjects (the putamen: contralateral 43.9%, ispilateral 32.1%, p<0.001; the caudate: contralateral 27.7%, ipsilateral 17.1%, p=0.001). The caudate to putamen BPI ratio was significantly higher in patients with PD than in the control group (1.55±0.23 and 1.29±0.13, respectively, p<0.001).
The striatal BPI correlated significantly with the Hoehn and Yahr stage (r=-0.487, p=0.007), the UPDRS total score (r=-0.562, p=0.002), the UPDRS motor score (r=-0.580, p=0.001) and the UPDRS activities of daily living score (r=-0.456, p=0.013). Of the major motor signs in PD the rigidity score (r=-0.594, p=0.001) correlated with the striatal DAT uptake, but there was no correlation with the severity of tremor. In the hemiparkinsonian group there was no correlation between the striatal uptake ratios and the clinical scores. The clinical autonomic disability score also correlated with the DAT specific binding in the striatum (r=–0.369, p=0.045). The score of clinical autonomic signs showed a correlation with the DAT uptake in the putamen (r=–0.382, p=0.037) and in the caudate (r=–0.377, p=0.040). The patients with constipation (n=9) had lower DAT binding in the striatum (BPI 3.35 and 4.63, respectively, p=0.006) and the caudate (BPI 3.97 and 5.27, respectively, p=0.011) than the patients who had no constipation (n=20).
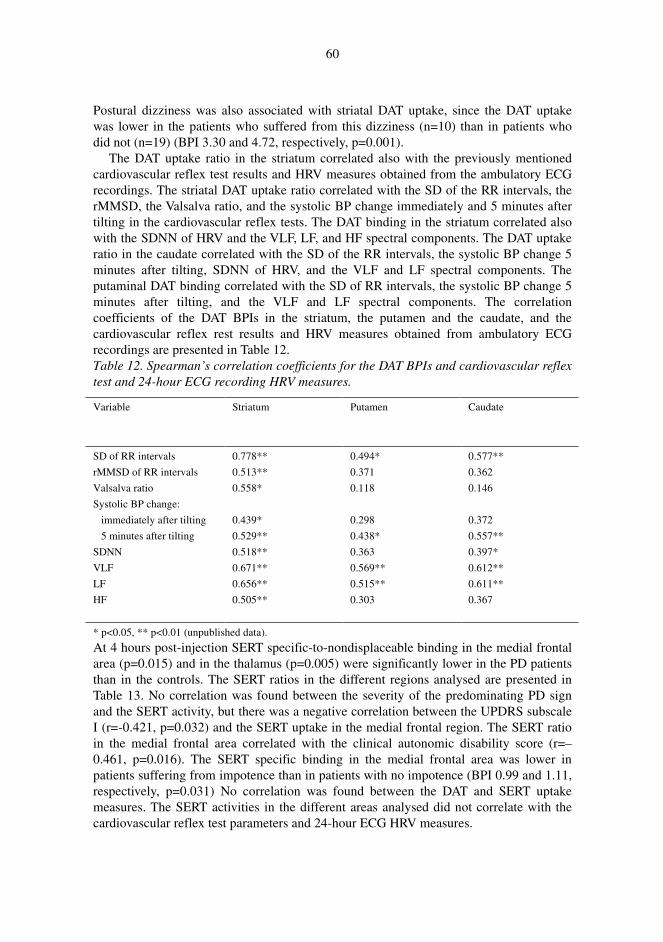
60
Postural dizziness was also associated with striatal DAT uptake, since the DAT uptake was lower in the patients who suffered from this dizziness (n=10) than in patients who did not (n=19) (BPI 3.30 and 4.72, respectively, p=0.001).
The DAT uptake ratio in the striatum correlated also with the previously mentioned cardiovascular reflex test results and HRV measures obtained from the ambulatory ECG recordings. The striatal DAT uptake ratio correlated with the SD of the RR intervals, the rMMSD, the Valsalva ratio, and the systolic BP change immediately and 5 minutes after tilting in the cardiovascular reflex tests. The DAT binding in the striatum correlated also with the SDNN of HRV and the VLF, LF, and HF spectral components. The DAT uptake ratio in the caudate correlated with the SD of the RR intervals, the systolic BP change 5 minutes after tilting, SDNN of HRV, and the VLF and LF spectral components. The putaminal DAT binding correlated with the SD of RR intervals, the systolic BP change 5 minutes after tilting, and the VLF and LF spectral components. The correlation coefficients of the DAT BPIs in the striatum, the putamen and the caudate, and the cardiovascular reflex rest results and HRV measures obtained from ambulatory ECG recordings are presented in Table 12. Table 12. Spearman’s correlation coefficients for the DAT BPIs and cardiovascular reflex test and 24-hour ECG recording HRV measures.
Variable Striatum Putamen Caudate
SD of RR intervals
rMMSD of RR intervals
Valsalva ratio
Systolic BP change:
immediately after tilting
5 minutes after tilting
SDNN
VLF
LF
HF
0.778**
0.513**
0.558*
0.439*
0.529**
0.518**
0.671**
0.656**
0.505**
0.494*
0.371
0.118
0.298
0.438*
0.363
0.569**
0.515**
0.303
0.577**
0.362
0.146
0.372
0.557**
0.397*
0.612**
0.611**
0.367
* p<0.05, ** p<0.01 (unpublished data).
At 4 hours post-injection SERT specific-to-nondisplaceable binding in the medial frontal area (p=0.015) and in the thalamus (p=0.005) were significantly lower in the PD patients than in the controls. The SERT ratios in the different regions analysed are presented in Table 13. No correlation was found between the severity of the predominating PD sign and the SERT activity, but there was a negative correlation between the UPDRS subscale I (r=-0.421, p=0.032) and the SERT uptake in the medial frontal region. The SERT ratio in the medial frontal area correlated with the clinical autonomic disability score (r=–0.461, p=0.016). The SERT specific binding in the medial frontal area was lower in patients suffering from impotence than in patients with no impotence (BPI 0.99 and 1.11, respectively, p=0.031) No correlation was found between the DAT and SERT uptake measures. The SERT activities in the different areas analysed did not correlate with the cardiovascular reflex test parameters and 24-hour ECG HRV measures.
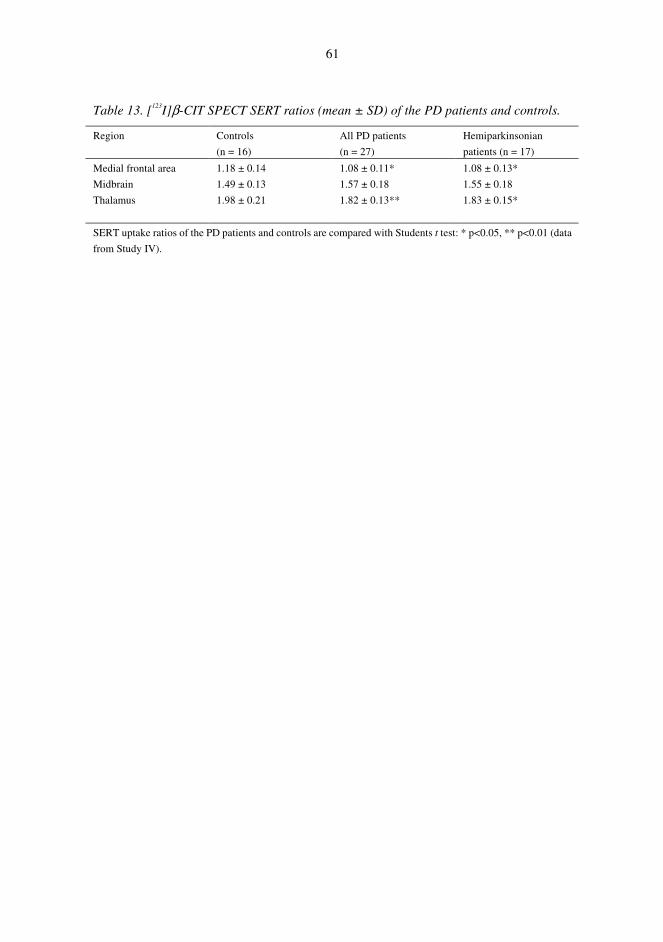
61
Table 13. [123I]β-CIT SPECT SERT ratios (mean ± SD) of the PD patients and controls.
Region Controls
(n = 16)
All PD patients
(n = 27)
Hemiparkinsonian
patients (n = 17)
Medial frontal area
Midbrain
Thalamus
1.18 ± 0.14
1.49 ± 0.13
1.98 ± 0.21
1.08 ± 0.11*
1.57 ± 0.18
1.82 ± 0.13**
1.08 ± 0.13*
1.55 ± 0.18
1.83 ± 0.15*
SERT uptake ratios of the PD patients and controls are compared with Students t test: * p<0.05, ** p<0.01 (data
from Study IV).
6 Discussion
6.1 General aspects
Previous evaluation of autonomic symptoms and quantitative measurements assessing the autonomic cardiovascular and sudomotor regulation have provided data that suggest manifold ANS involvement in patients with PD. There are, however, several pitfalls when the occurrence and severity of autonomic dysfunction in PD is considered. Despite the use of uniform clinical criteria (Daniel & Lees 1993), MSA and other degenerative cerebral disorders are occasionally diagnosed incorrectly as idiopathic PD. Moreover, the abnormal results of PD patients in the cardiovascular function test may be misinterpreted because the effects of baseline HR, age, disease stage and medications are not adequately encountered. Furthermore, the cardiovascular reflex tests provide only a limited view of the cardiovascular autonomic control, since the responses are recorded under experimental conditions and for only a short time period. Therefore, HR analysis using ambulatory ECG recordings presumably reveal new aspects of the cardiovascular control mechanisms and the pathophysiology which lead to autonomic dysfunction in PD.
The present study was designed to assess quantitatively the reflectory cardiac control with standard cardiovascular reflex tests, and the tonic autonomic cardiac regulation with HR fluctuation analysis from 24-hour ECG recording in de novo PD patients who had not received any antiparkinsonian medication. The HR variation parameters in the standard cardiovascular reflex tests were adjusted for baseline RR interval, and the effect of age was taken into account in the statistical analyses. For the first time the influence of three different antiparkinsonian drugs, i.e. levodopa, bromocriptine and selegiline, on cardiovascular reflex responses and sympathetic sudomotor function was investigated prospectively. In spite of the use of widely accepted clinical criteria the clinical follow-up of the PD patients after the study trial period disclosed one case of progressive supranuclear palsy and one case of MSA, and these two patients were excluded from the study. The accuracy of the diagnosis is in accordance with other studies that confirm the diagnosis of PD with a pathological examination (Daniel & Lees 1993, Hughes et al. 1992, Rajput & Rodzilsky 1991).
Examination of presynaptic DAT specific binding in the striatum with β-CIT SPECT has proved useful in the diagnostic procedure of PD. Thus, we evaluated the striatal DAT
63
uptake in 30 of the total 60 PD patients to further confirm the diagnosis. In addition we assessed the SERT availability in the midbrain, thalamus and medial frontal cortex to see whether this SPECT technique could reveal a serotonin deficiency in de novo PD patients.
6.2 Clinical aspects
Most patients with advanced PD are known to suffer from autonomic symptoms (Turkka. 1987), but our findings showed that even newly diagnosed untreated patients have symptoms and signs referring to autonomic dysfunction nearly as often as the earlier reports suggest. The most often reported symptoms of autonomic dysfunction have been postural dizziness (Aminoff & Wilcox 1971, Turkka 1987), gastrointestinal disorders (Singer et al. 1992, Magalhães et al. 1995, Martignoni et al. 1995) and micturition problems (Sotolongo et al. 1988, Chandiramani et al. 1997). Accordingly, nearly 50% of our patients suffered from these manifestations, but they also complained of sweating disorders and the male patients very often had sexual disturbances. However, only in 10% of the patients was the severity of the autonomic symptoms or signs considered moderate or severe. Thus the disability caused by the clinical autonomic symptoms seems to be mild and consistent with the general presumption that autonomic insufficiency is usually modest in PD.
The severity of the clinical autonomic dysfunction was associated with the disability caused by the disease as evaluated with the UPDRS score and the Hoehn and Yahr stage, thus confirming earlier reports (Turkka 1987, Van Dijk et al. 1993). The degree of hypokinesia and rigidity, of the cardinal motor signs, also correlated with the clinical autonomic scores, whereas there was no correlation to the severity of tremor. The severity of hypokinesia and rigidity correlated with the severity of constipation and urinary disturbances of the individual autonomic symptoms and signs as well. Thus development of the akinetic-rigid type of PD and autonomic insufficiency may share common pathophysiological mechanisms in distinction to the tremor onset type of PD.
6.3 Cardiovascular autonomic dysfunction
The results of this study displayed that PD interferes not only with the cardiovascular HR and BP reflexes, but also with the tonic autonomic regulation of HRV. In addition, PD medications were found to modify the reflectory autonomic responses in a reversible manner in this early phase of the disease. Bromocriptine and selegiline increased the orthostatic BP fall while levodopa diminished it. Furthermore, the rise of BP as a sympathetic reaction to isometric contraction decreased during bromocriptine and selegiline therapies. By contrast, these drugs had no effects on the HR responses in the cardiovascular tests. Evaluation of the possible effects of these antiparkinsonian drugs on the HRV measures analysed from ambulatory ECG recordings is under way.
In previous studies with cardiovascular reflex tests PD patients have demonstrated reduced HR variation in normal breathing (Piha et al. 1988, Meco et al. 1991, Turkka et
64
al. 1997), in deep breathing (Sachs et al. 1985, Camerlingo et al. 1987, Ludin et al. 1987, Turkka et al. 1997), after the Valsalva manoeuvre (Appenzeller & Goss 1971, Gross et al. 1972, Goetz et al. 1986, Meco et al. 1991, Piha et al. 1993, Turkka et al. 1997), and after standing up (McDowell & Lee 1970, Meco et al. 1991, Van Dijk et al. 1993, Turkka et al. 1997). The BP responses during tilting (Gross et al. 1972, Piha et al. 1988, Camerlingo et al. 1990, Meco et al. 1991, Van Dijk et al. 1993) and the isometric handgrip (Sachs et al. 1985, Ludin et al. 1987, Turkka et al. 1987b, Meco et al. 1991, Van Dijk et al. 1993, Sénard et al. 1995, Turkka et al. 1997) are also abnormal in parkinsonian patients, and our findings are consistent with these earlier reports even though few of these studies were conducted on drug-naïve patients and designed to evaluate the effects of PD medication prospectively. Therefore it has been difficult to differentiate between the effects of the disease and its medication on the ANS function.
Recently Mastrocola et al. (1999) discovered abnormalities in the diurnal HRV in PD patients on levodopa treatment. The SDNN and the LF spectral power were lower in parkinsonian patients than healthy control subjects during the day and night, whereas the HF spectral power was lower only during the night. We also found suppression in the SDNN values and all the power spectral measurements even in untreated PD patients, suggesting involvement of the ANS early in the course of the disease. In addition, the cardiac autonomic dysregulation associated with PD affected the slope of the power- law relation.
Even though the precise role of the sympathetic and parasympathetic nervous systems in the reflectory and tonic autonomic cardiac regulation is not yet understood, these two systems appear to be involved in the cardiovascular dysfunction of PD patients. Since both the HR and BP responses of the cardiovascular reflex tests were influenced by the disease, it is apparent that both sympathetic and parasympathetic insufficiency occurs in parkinsonian patients. This conclusion is supported by the results of the ambulatory ECG HRV analysis. Of the different power spectrum frequency bands the HF band is thought to reflect the parasympathetic activity mediated by the vagus nerve, whereas the LF band is believed to be dependent on negative feedback from the baroreflex arc mediated both by sympathetic and parasympathetic activity in an upright position and mainly by vagal activity in a supine position (Pomeranz et al. 1985, Ori et al. 1992). As the slope of the power-law relation is especially deep in transplanted hearts that are denervated (Bigger et al. 1996), the findings in our patients may indicate abnormal postganglionic adrenergic innervation of the heart. This agrees with the results of several studies using [123I]-metaiodobenzylguanidine myocardial scintigraphy or 6-[18F]fluorodopamine PET where the tracer uptake has been reduced in patients with PD in contrast to patients with MSA (Yoshita et al. 1998, Reinhardt et al. 2000). Furthermore, concerning peripheral autonomic effector mechanisms, -adrenoceptor reactivity has been reported to correlate inversely with the duration of PD (Milon et al. 1991), but others have reported the -adrenergic sensitivity to be unaffected by the disease and levodopa treatment (Durrieu et al. 1990). PD patients with orthostatic hypotension have also had low concentrations of endogenous catecholamines associated with an upregulation of 2-adrenoreptors (Galinier et al. 1994).
In systematic neuropathological studies of the ANS in PD patients, Lewy bodies have been widely distributed in the hypothalamus, the sympathetic system (the intermediolateral nucleus of the thoracic cord and sympathetic ganglia) and the
65
parasympathetic system (the dorsal vagal and sacral parasympathetic system) (Jellinger 1991, Wakabayashi & Takahashi 1997). Lewy bodies have also been found in the enteric nervous system of the alimentary tract, the cardiac plexus, the pelvic plexus and the adrenal medulla (Qualman et al. 1984, Wakabayashi et al. 1988, Wakabayashi & Takahashi 1997). The number of neurons in the intermediolateral nucleus of the thoracic cord is reduced in PD patients (Wakabayashi & Takahashi 1997), especially in patients with autonomic failure (Oppenheimer 1980). Therefore, involvement of both the central and peripheral ANS is evident. Our results also suggest multidimensional affection of the ANS in the PD disease process, since both reflex HR and BP adaptation mechanisms and tonic HRV regulation are involved. Furthermore, the steep power law relation slopes refers to pathology of the peripheral sympathetic cardiac innervation.
The knowledge of the influence of PD medication on autonomic regulation has based mainly on the assessment of the effects of the acute administration of a drug, of the effects of short-time medication withdrawals, or of correlations of autonomic dysfunction to medication. In several reports, acute administration of levodopa has not been shown to affect cardiovascular reflexes (Goetz et al. 1972, Kuroiwa et al. 1983, Sachs et al. 1985, Turkka et al. 1987b, Sénard et al. 1995) whereas some have shown that levodopa produces mild orthostatic hypotension (Calne et al. 1970, McDowell & Lee 1970, Appenzeller & Goss 1971) and lowers the resting BP (Calne et al. 1970, Iwasaki et al. 1990). Camerlingo et al. (1990) studied the long-term effect of levodopa in de novo PD patients and found a more pronounced BP fall after tilting and a lower HR response to tilting after two years’ of levodopa medication than before treatment. Although we found the BP level at rest to be lower during levodopa treatment, levodopa did not suppress the autonomic cardiovascular responses and the sympathetic BP response to tilting. The discrepancy between our results and the previous study may be explained by the progression in the severity of the disease in the previous study, whereas the motor functions improved during medication in our patients. Furthermore, cardiovascular reflexes have been reported as deteriorating with the progression of the disease over a three-year follow-up period (Mesec et al. 1999).
Some studies have suggested that dopamine receptor agonists cause an orthostatic BP fall in PD (Tanner et al. 1982, Le Witt et al. 1983, Kujawa et al. 2000). However, the orthostatic hypotension has not been related to any specific dopamine agonist and has seldom been appreciated by the patients (Kujawa et al. 2000). The marked fall of systolic BP in response to tilting in our study was in accordance with the clinical experience that dopamine agonists induce orthostatic hypotension. Sympathetic dysfunction was further supported by the suppressed BP responses to isometric contraction in patients on bromocriptine. Our finding that selegiline increased the orthostatic BP fall also agrees with the results of two earlier studies (Churchyard et al. 1997, Turkka et. al. 1997) in which selegiline combined with levodopa caused an increase in the fall of systolic BP after tilting while withdrawal of selegiline abolished the orthostatic BP fall (Churchyard et al. 1997). The present study demonstrated for the first time a reversibly diminished sympathetic response to isometric contraction in PD patients on selegiline monotherapy.
The pathophysiological mechanisms behind the influence of PD medication on the ANS regulation have remained unsettled. The renin levels in PD patients are low and levodopa causes a further decrease in the renin concentration and this might be responsible for the mild postural hypotension reported in the early stages of levodopa
66
treatment (Barbeau et al. 1969, Martignoni et al. 1995). Though there is a deficit in the baroreflex activity leading to sympathetically mediated constriction of resistance and capacitance vessels during tilting in PD patients (Gross et al. 1972, Piha et al. 1988, Meco et al. 1991, Van Dijk et al. 1993), levodopa doesn’t seem to aggravate this deficit (Appenzeller & Goss 1971). Levodopa might have a direct sympathetic vasoconstrictor effect on peripheral resistance vessels via α1-receptors as sympathetic nerve terminals produce noradrenaline from tyrosine via the precursors dopa and dopamine (Guyton & Hall 1996) even though the use of dopa decarboxylase inhibitors probably inhibits most of the dopamine and noradrenaline production (Bianchine 1985). Levodopa administration also increases the spontaneous muscle sympathetic nerve activity when assessed by microneurography (Takeuchi et al. 1993). This may explain why BP responses to tilting were not diminished in our patients on levodopa. Furthermore, levodopa may increase the cardiac output by increasing the skeletal muscle contraction and venous return towards the heart. On the other hand, dopamine is thought to act as an inhibitor on the sympathetic nerve terminals (Korczyn 1990) and have a β2-adrenergic effect decreasing the systemic vascular resistance (Bianchine 1985), possibly leading to lower BP levels at rest as was found in our study.
The use of bromocriptine alone or in combination with levodopa/carbidopa has been associated with a sustained reduction of systolic and diastolic BP not blocked by peripheral dopamine receptor antagonists, suggesting a central mechanism (Quinn et al. 1981, Montastruc et al. 1985). Bromocriptine is also assumed to cause arterial and venous relaxation (Mehta & Tolis 1979), which in turn, could weaken the baroreflex during tilting and account for the pronounced orthostatic hypotension found in the present study. In rats bromocriptine has been reported to act on the peripheral sympathetic nervous system as an agonist of presynaptic dopamine receptors and α2-receptors and as an antagonist of postsynaptic α1-adrenoceptors leading to impaired pressor responses (Vila et al. 1985). Selegiline is likely to act neuropharmacologically through the inhibition of monoamine oxidase B, which in turn leads to changes in catecholamine turnover, possibly resulting in sympathetic hypofunction (Churchyard et al. 1997). This hypothesis is supported by the decreased cerebrospinal fluid concentrations of 3-methoxy-4-hydroxyphenyl glycol, the main brain metabolite of noradrenaline, in samples of selegiline-treated patients (Heinonen et al. 1993). Selegiline may also have peripheral effects since it appears to be a weak α 1-receptor antagonist (Nedergaard & Moller 1994) and to exert postganglionic sympatholytic effects attenuating the increase in plasma noradrenaline and decrease in baroreceptor sensitivity in rabbits with heart failure (Shite et al. 2000).
The present study was the first to show suppressed diurnal HRV in untreated PD patients using HRV analysis of ambulatory ECG, using both conventional spectral and non-spectral dynamic methods of HRV. The advantages of 24-hour ambulatory ECG recordings are good reproducibility and the information concerning the LF bands of the spectral HRV gathered over longer time periods than the standard cardiovascular reflex tests can provide (Kleiger et al. 1987, Ori et al. 1992, Huikuri et al. 1990). The results of the standard cardiovascular reflex tests agree well with those of the ambulatory ECG recordings, both demonstrating parasympathetic and sympathetic dysfunction early in the course of PD. Because of a great interindividual variation in the HRV measures used in this study, these parameters can only be used to assess autonomic dysfunction at a group

67
level, as is also often the case with standard cardiovascular reflex tests in PD patients (Bannister & Mathias 1999). Our finding that the slope of the power-law relationship of 24-hour HRV is steeper in PD patients than in healthy subjects raises the question of whether these measures could be used as predictors of mortality in patients with PD, since the power-law relationship has been proved on one hand to be a more powerful predictor of death than traditional risk markers both in elderly subjects (Saul et al. 1991) and in patients with recent myocardial infarction (Bigger et al. 1996), and on the other hand to be an even better prognostic indicator than the spectral parameters that are independent predictors of outcome in patients with coronary heart disease and after acute myocardial infarction (Bigger et al. 1996).
6.4 Sudomotor dysfunction
The present study established a clearly abnormal SSR pattern in untreated patients with PD. The disease was associated with suppression of SSR amplitudes to both electric and auditory stimuli, the decrease being more pronounced on the side of the affected limbs than contralaterally in hemiparkinsonian patients. As a novel observation PD patients had more often repetitive synchronous SSRs after a single stimulus than the control group. This phenomenon has also been reported in alcoholic patients with palmoplantar hyperhidrosis (Tugnoli et al. 1999) and it could be related to hyperhidrosis in PD although we could not demonstrate any association between clinical sweating disturbances and the SSR results.
The SSR has been widely used to evaluate autonomic dysfunction in peripheral nervous disorders like diabetec polyneuropathy, but some inconsistency of its reliability as an index of autonomic dysfunction in diabetics with peripheral polyneuropathy exists (Bril et al. 2000). Impairment of sympathetic sudomotor activity evaluated with the SSR has also been reported in several diseases, such as stroke, progressive autonomic failure syndromes, and multiple sclerosis, affecting the central pathways that participate in the reflex arc. In earlier studies with PD patients SSR responses have been absent (Shahani et al. 1984, Korczyn 1990, Taly & Muthane 1992, Bordet et al. 1996), or SSR latencies have been prolonged or amplitudes suppressed (Taly & Muthane 1992, Mano et al. 1994, Hirashima et al. 1996, Braune et al. 1997, Fusina et al. 1999). The present study showed an inverse correlation between the suppressed SSR amplitudes and the duration of the disease, the disease severity and the tremor score. Our finding that higher UPDRS tremor scores were related to suppression of the SSR amplitude contrasts with the results of Braune et al. (1997) which show no correlation between the predominant PD signs and the SSRs. The possible mechanism by which tremor interferes with the SSR may be tremor acting as an internal stimulation, like deep breathing, causing adaptation of the SSR (Shahani et al. 1984, Schondorf et al. 1993, Fusina et al. 1999). Furthermore, according to the interpretation of Lin et al. (1995), if the system is already active (e.g. following an internal trigger such as tremor) it cannot show a maximum response after a stimulus because of other factors than adaptation, such as gland fatigue or temperature change. On the other hand, any attempts made by the patient to suppress the tremor may interfere with the responses.

68
Our knowledge of the central structures mediating SSRs in man is mainly based on ischemic brain lesion studies (Korpelainen et al. 1993, Schondorf 1993). However, in the cat those centers that belong to the central autonomic network have been identified: the orbitofrontal cortex, the caudate nucleus, the anterior lobe of the cerebellum, the dorsal thalamus, the posterior hypothalamic nuclei, the ventrolateral and ventromedial substantia reticularis and the intermediolateral nucleus (Wilcott 1969, Schondorf 1993). Correspondingly, the pathology in PD also involves the sympathetic nervous system: Lewy bodies have been found in the hypothalamus, in the intermediolateral cell columns of the spinal cord and in the sympathetic ganglia (Rajput & Rodzilsky 1976, Langston & Forno 1978, Wakabayashi & Takahashi 1997). The topographically close relationship of the pathways controlling SSRs at the CNS level to the long motor tracts (Linden & Berlit 1995) could explain the asymmetry of the SSR amplitudes in our hemiparkinsonian patients. The amplitude reduction of SSRs is often considered to be linked to peripheral sympathetic lesions, but as Lin et al. (1995) suggested it may also be due to central causes. A decreased number of excitable sweat glands and low sweat volume in response to intradermal asetylcholine injections when the density of total unmyelinated and acetylcholine positive fibers is normal has been related to dysfunction of the postganglionic sympathetic fibers (Hirashima et al. 1996). Central mechanisms such as loss of inhibition explain best the increased number of symmetrical synchronous repetitive SSRs after a single stimulation found in our PD patients, whereas the normal adaptation that is a physiological central phenomenon in subjects responding to repetitive stimuli suggests peripheral deficits in our patients (Elie & Guiheneuc 1990).
This was the first study to assess prospectively the possible effects of PD medication on the sympathetic sudomotor function by quantification of SSR amplitudes and latencies. It has been postulated that levodopa and anticholinergic medications have no influence on the SSR (Braune et al. 1997). Indeed we could not find any change in the SSR amplitudes or latencies after six months on levodopa/carbidopa or bromocriptine medication, whereas selegiline seemed to decrease the amplitude of the responses. No change in the local skin temperature that could explain the SSR amplitude decrease (Bini et al. 1980) was found between the recording sessions. However, one should be cautious in drawing conclusions concerning the effects of selegiline on SSRs, since the responses did not return to baseline after the washout period.
The PD process causes a sympathetic sudomotor dysfunction presenting itself as suppressed SSRs, amplitudes showing a negative correlation with the disease duration, the severity of the disease and especially the magnitude of tremor. Of the investigated PD medications only selegiline would seem to diminish the SSR amplitudes, though only slightly, whereas levodopa and bromocriptine have no such effect. The observed changes in SSR amplitude and repetitiveness of the SSRs with normal adaptation suggest that the disturbed sudomotor function in PD is caused by damage at multiple levels along the neural axis.
69
6.5 ββββ-CIT SPECT
The use of β-CIT SPECT in this work disclosed significantly low DAT specific binding in the striatum of untreated patients with early PD. Marek et al. (1996) studied the dopamine transporters in 8 de novo hemiparkinsonian patients and reported a 53% (contralateral) and 37% (ipsilateral) decrease in striatal DAT uptake when compared to age matched controls. In another study the reduction in DAT specific binding in 29 hemiparkinsonian patients was 41% in the contralateral striatum and 30% in the ipsilateral striatum when compared to age adjusted control values (Brücke et al. 1997). Our corresponding values were somewhat smaller, being 34% and 28%, respectively, revealing a bilateral reduction of DAT availability in patients with unilateral symptoms. The difference of DAT uptake ratios in our study compared with earlier studies (Brücke et al. 1993, Asenbaum et al. 1997) can be explained both by the early phase of the disease of our patients, and by better age-matching of the PD and control groups in our study compared to previous reports (Asenbaum et al. 1997, Brücke 1997, Müller et al. 1998). The striatal DAT BPIs were expectedly higher in the hemiparkinsonian PD patients than those in the whole group, since the disease was less disabling in the former.
In SPECT studies using 123I-FP-CIT and 123I-IPT as tracer the reduction of the specific to non-specific DAT uptake ratios has been comparable with the studies using β-CIT. In two recent studies the DAT uptake ratio of PD patients on medication presented as a percentage of the uptake ratio found in healthy controls ranged from 36–43% on the contralateral side to the affected limbs and from 42–56% on the ipsilateral side (Booij et al. 1997, Tissingh et al. 1998). The specific to non-specific uptake ratio of 123I-FP-CIT was approximately 50% in the contralateral striatum and 60% in the ipsilateral striatum of the uptake found in healthy controls in a study with 5 de novo PD patients (Booij et al. 1997).
Pathological findings have indicated relatively selective loss of dopamine in the posterior putamen (Nahmias et al. 1985, Fearnley et al. 1991), the loss being 30-50% in the putamen and 20-25% in the caudate based on PET studies (Brooks et al. 1990, Leenders et al. 1990, Otsuka et al. 1991, Morrish et al. 1995). Both putamen and caudate DAT uptake ratios were lower in our PD patients than in the controls, but the loss was more pronounced in the putamen. The contralateral putamen value has demonstrated the strongest loading in discriminant function analysis and has accounted for most of the difference between the PD patients and the controls in previous reports (Seibyl et al. 1995, Tissingh et al. 1998). Recently Tissingh et al. (1998) reported a 57% reduction of 123I-FP-CIT binding in the putamen and a 29% reduction in the caudate nucleus of the control mean binding in early drug-naïve PD patients. In the present study there was some overlap in the mean putamen DAT uptake ratios of the PD patients and the controls while the contralateral putamen DAT activity almost distinguished the PD patients from the control subjects.
The clinical autonomic disability score showed an inverse correlation to the DAT specific binding in the striatum which was also related to the degree of hypokinesia and rigidity but not to that of tremor. However, partial correlation analyses showed that the severity of rigidity and hypokinesia, and the overall severity of the disease were confounding factors explaining most of this correlation. The DAT activity in the striatum, the caudate, and the putamen also correlated with the HR responses during normal
70
breathing and BP responses after tilting in the cardiovascular reflex tests, and the SDNN and spectral components analysed from 24-hour ambulatory ECG recordings. No confounding factors were found with partial correlation analysis, thus suggesting that the dopaminergic deficit in the striatum is associated with autonomic cardiovascular dysfunction in PD patients.
As has been found in earlier reports, the caudate to putamen uptake ratios were significantly higher in the present PD patient group than in the control group, but the DAT uptake ratio did not differ from the control values as clearly as in some earlier studies (Marek et al. 1996). However, it must be kept in mind that the SPECT method may carry some inadequacy in the quantification of very small ROIs such as the putamen and the caudate. Despite this, the caudate to putamen DAT uptake ratio may be useful in the differential diagnosis of PD and other extrapyramidal syndromes (Brooks 1997).
To our knowledge, the present study was the first one to use β-CIT SPECT to evaluate SERT activity simultaneously with DAT activity in PD patients and to compare the result with healthy controls. Clinical examinations have shown that 25% of PD patients experience depression before the diagnosis of PD is made (Mayeux 1992) and eventually 40% of PD patients experience depression (Lieberman 1998). Some studies have suggested a correlation between serotonin loss and depression in PD (Mayeux et al. 1988) and serotonin depletion has been reported in the basal ganglia and neocortex of PD patients (Jellinger 1991). β-CIT SPECT has been useful for quantifying the SERT availability in depression (Malison et al. 1998), and the capability of antidepressants, e.g. citalopram, to block specifically β-CIT uptake in SERT areas has been documented (Pirker et al. 1995). One preliminary β-CIT SPECT study has shown a slight decrease in the SERT uptake ratios in the midbrain of PD patients (Brücke et al. 1993), whereas the β-CIT uptake in the midbrain and thalamus regions, using PET, did not differ between PD patients and controls (Laihinen et al. 1995). Recently both DAT and SERT binding were assessed in the hypothalamic/midbrain region at 20-24 hours post-injection, but no correlation between the SERT uptake and the UPDRS scores was found (Kim et al. 1999). The significant deficit of SERT activity in the medial frontal area and in the thalamus in the present study agrees with the clinical knowledge of depression in PD and the pathological findings concerning the serotonin metabolism. The SERT activity in the medial frontal area showed a negative correlation with the UPDRS subscore I that was used to evaluate parameters like mentation, behaviour and mood that might be associated with depression. However, further studies are needed to demonstrate the clinical correlation between specific depression scale results and SERT activity measured with β-CIT SPECT in PD. Interestingly, the SERT binding in the medial frontal area correlated also with impotence, suggesting that serotonin depletion may be involved in the development of sexual disturbances reported in PD patients.
The influence of the serotonin metabolism on the motor symptoms of PD remains speculative. It has been claimed that it has an inhibitory effect on dopaminergic neuronal activity (Ugedo et al. 1989), a hypothesis supported by observations that serotonin re-uptake inhibitors like fluoxetine may aggravate parkinsonian symptoms (Jansen Steur 1983). Moreover, it is thought that reduced serotonin contributes to the pathogenesis of resting tremor (Friedman & Lannon 1990), but we found no correlation between SERT activity and tremor or any other cardinal PD sign.

7 Conclusions
Clinical symptoms and signs of autonomic dysfunction are common but usually mild in PD. The most often complained autonomic manifestations in our parkinsonian patients (n=58) were sweating disturbances (51%), urinary dysfunction (48%), bowel dysfunction (42%) and postural dizziness (40%). The severity of the disease, the rigidity and the hypokinesia of the major motor PD signs correlated with the degree of dysautonomia. I PD itself causes autonomic dysfunction leading to abnormalities in
cardiovascular regulation and the PD medication seems to further modify the ANS responses. Bromocriptine and selegiline, in contrast to levodopa, increased the orthostatic BP fall and suppressed the BP response to isometric exercise, reflecting mainly impairment of the sympathetic regulation.
II In addition to impairment of reflectory cardiovascular regulation, PD causes extensive dysfunction of the tonic autonomic cardiovascular regulatory system. The conventional spectral and dynamic HRV measures showed a negative correlation with the disease severity and hypokinesia. Of the dynamic measures the slope of the power-law relation especially seemed to be a sensitive indicator of abnormalities in the HR fluctuation of PD.
III The degenerative process in PD involves the sudomotor system as reflected by the progressive suppression of SSR amplitudes with a correlation to the PD symptom duration and clinical disability. PD medications seemed to have only minor effects on the SSRs. The observed changes in SSR amplitude together with increased repetitiveness of the SSRs with normal adaptation suggest that the disturbed sudomotor function in PD is caused by damage at multiple levels of the neural axis.
IV β-CIT SPECT provides a useful method for simultaneous assessment of both DAT and SERT activity in PD patients. In addition to decreased DAT uptake PD patients seemed to have reduced SERT binding in the thalamic and frontal areas. The clinical signs and symptoms of autonomic dysfunction, and the results of cardiovascular autonomic regulation showed a correlation with DAT availability.

References
Abi-Dargham A, Gandelman MS, DeErausquin GA, Zea-Ponce Y, Zoghbi SS, Baldwin RM, Laruelle M, Charney DS, Hoffer PB, Neumeyer JL & Innis RB (1996) SPECT imaging of dopamine transporters in human brain with iodine-123-fluoroalkyl analogs of β-CIT. J Nucl Med 37: 1129-1133.
Ahlskog JE, Uitti RJ, O’Connor MK, Maraganore DM, Matsumoto JY, Stark KF, Turk MF & Burnett OL (1999) The effect of dopamine agonist therapy on dopamine transporter imaging in Parkinson’s disease. Mov Disord 14: 940-946.
Akselrod S, Gordon D, Ubel FA, Shannon DC, Barger MA & Cohen RJ (1981) Power spectrum analysis of heart rate fluctuation: a quantitative probe of beat-to-beat cardiovascular control. Science 213: 220-222.
Altman DG (ed) (1991) Practical Statistics for Medical Research. Chapman and Hall, London, p 210-212.
Amaral DG, Price JL, Pitkänen A, Carmichael ST (1992) Anatomical organization of the primate amygdaloid complex. In: Aggleton JP (ed) The Amygdala: Neurobiological Aspects of Emotion, Memory, and Mental Dysfunction. Wiley-Liss, New York, p 1-66.
Aminoff MJ & Wilcox CS (1971) Assessment of autonomic function in patients with parkinsonian syndrome. Br Med J 4: 80-84.
Andersen EB & Boesen F (1997) Sympathetic vasoconstrictor reflexes in Parkinson’s disease with autonomic dysfunction. Clin Auton Res 7: 5-11.
Angelone A & Coulter NA (1964) Respiratory sinus arrhythmia: a frequency dependent phenomenon. J App Physiol 19: 479-482.
Appenzeller O (1975) Baroreceptor and vasomotor function in neurological disease. Int J Neurol 9: 247-261.
Appenzeller O (1990) Anatomy and histology. In: Appenzeller O (ed) The Autonomic Nervous System, 4th ed. Elsevier Science Publishes B.V., Amsterdam, p 1-33.
Appenzeller O & Goss JE (1971) Autonomic deficits in Parkinson’s syndrome. Arch Neurol 24: 50-57.
Asenbaum S, Brücke T, Pirker W, Podreka I, Angelberger P, Wenger S, Wöber C, Müller C & Deecke L (1997) Imaging of dopamine transporters with iodine-123-β-CIT and SPECT in Parkinson’s disease J Nucl Med 38: 1-6.
Autere JM, Moilanen JS, Myllylä VV & Majamaa K (2000) Familial aggregation of Parkinson’s disease in a Finnish population. J Neurol Neurosurg Psychiatry 69: 107-109.
Bandler R, Carrive P & Zhang SP (1991) Integration of somatic and autonomic reactions within the midbrain periaquaductal grey: viscerotopic, somatotopic, and functional organization. Prog Brain Res 87: 269-305.
73
Bannister R & Mathias CJ (1999) Clinical features and evaluation of the primary chronic autonomic failure syndromes. In: Mathias CJ, Bannister R (eds) Autonomic failure: A Textbook of Clinical Disorders of the Autonomic Nervous System, 4th ed. Oxford University Press, New York, p 307-316.
Barbeau A, Gillo-Joffrey L, Boucher R, Nowaczynski W & Genest J (1969) Renin-aldosterone system in Parkinson’s disease. Science 165: 291-292.
Bechara A, Damasio H & Damasio AR (2000) Emotion, decision-making and the orbitofrontal cortex. Cereb Cortex 10: 295-307.
Benarroch EE (1993) The central autonomic network: functional organization, dysfunction, and perspective. Mayo Clin Proc 68: 988-1001.
Benarroch EE (1997a) Arterial pressure. In: Benarroch EE (ed) Central Autonomic network: Functional Organization and Clinical Correlations. Futura Publishing Company, Inc., Armonk, NY, p 197-229.
Benarroch EE (1997b) Cardiac rhythm. In: Benarroch EE (ed) Central Autonomic Network: Functional Organization and Clinical Correlations. Futura Publishing Company, Inc., Armonk, NY, p 169-196.
Benarroch EE (1997c) Overview of the organization of the central autonomic network. In: Benarroch EE (ed) Central Autonomic Network: Functional Organization and Clinical Correlations. Futura Publishing Company, Inc., Armonk, NY, p 3-28.
Benarroch EE (1997d) Postganglionic sympathetic outflow. In: Benarroch EE (ed) Central Autonomic Network: Functional Organization and Clinical Correlations. Futura Publishing Company, Inc., Armonk, NY, p 139-168.
Benarroch EE, Opfer-Gehrking TL & Low PA (1991) Use of the photoplethysmographic technique to analyze the Valsalva maneuver in normal man. Muscle Nerve 14: 1165-1172.
Benarroch EE, Schmeichel AM & Parisi JE (2000) Involvement of the ventrolateral medulla in parkinsonism with autonomic failure. Neurology 54: 963-968.
Bennet T, Fentem PH, Fitton D, Hampton JR, Hosking DJ & Riggot PA (1977) Assessment of vagal control of the heart in diabetes: measures of R-R interval variation under different conditions. Br Heart J 39: 25-28.
Bianchine JR (1985) Drugs for Parkinson’s disease, spasticity, and acute muscle spasms. In: Goodman Gilman A, Goodman LS, Rall TW & Murod F (eds) Goodman and Gilman’s The Pharmacological Basis of Therapeutics, 7th edition. Macmillan Publishing Company, New York, p 473-490.
Bigger JT Jr, Fleiss JL, Steinman RC, Rolnitzky LM, Kleiger RE & Rottman JN (1992) Frequency domain measures of heart period variability and mortality after myocardial infarction. Circulation 85: 164-172.
Bigger JT, Jr, Steinman RC, Rolnitzky LM, Rolnitzky LM, Fleiss JL, Albrecht P & Cohen RJ (1996) Power law behavior of RR-interval variability in healthy middle-aged persons, patients with recent acute myocardial infarction, and patients with heart transplants. Circulation 93: 2142-2151.
Bini G, Hagbarth KE, Hynninen P & Wallin BG (1980) Thermoregulatory and rhythm-generating mechanisms governing the sudomotor and vasoconstrictor outflow in human cutaneous nerves. J Physiol 306: 537-552.
Bishop VS (1994) Carotid baroreflex control of blood pressure and heart rate during dynamic exercise. J Appl Physiol 77: 491-492.
Booij J, Tissingh G, Boer GJ, Speelman JD, Stoof JC, Janssen AGM, Wolter Ech & van Royen EA (1997) [123I]FP-CIT SPECT shows a pronounced decline of striatal dopamine transporter labelling in early and advanced Parkinson’s disease. J Neurol Neurosurg Psychiatry 62: 133-140.
Bordet R, Benhadjali J, Destee A, Hurtevent JF, Bourriez JL & Guieu JD (1996) Sympathetic skin response and R-R interval variability in multiple system atrophy and idiopathic Parkinson’s disease. Mov Disord 11: 268-272.
Borgdorff P (1975) Respiratory fluctuation in pupil size. Am J Physiol 228: 1094-1102. Borst C, Wieling W, Van Brederode JF, Hind A, De Rijk LG & Dunning AJ (1982) Mechanisms of
initial heart rate response to postural change. Am J Physiol 243: H676-681.

74
Braak H, Braak E, Yilmazer D, de Vos RA, Jansen EN & Bohl J (1996) Pattern of brain destruction in Parkinson’s and Alzheimer’s diseases. J Neural Transm 103: 455-490.
Braune HJ, Korchounov AM & Schipper HI (1997) Autonomic dysfunction in Parkinson’s disease assessed by sympathetic skin response: a prospective clinical and neurophysiological trial on 50 patients. Acta Neurol Scand 95: 293-297.
Braune S, Auer A, Schulte-Mönting J, Schwerbrock S & Lücking CH (1996) Cardiovascular parameters: sensitivity to detect autonomic dysfunction and influence of age and sex in normal subjects. Clin Autonom Res 6: 3-15.
Bril V, Nyunt M, Ngo M (2000) Limits of the sympathetic skin response in patients with diabetic polyneuropathy. Muscle Nerve 23: 1427-1430.
Brooks DJ (1997) Advances in imaging Parkinson’s disease. Curr Opin Neurol 10: 327-331. Brooks DJ, Ibanez V, Sawle GV, Quinn N, Lees AJ, Mathias CJ, Bannister R & Frackowiak RSJ
(1990) Differing patterns on 18F-Dopa uptake in Parkinson’s disease, multiple system atrophy and progressive supranuclear palsy. Ann Neurol 28: 547-555.
Brouwer J, van Veldhuisen DJ, Man in ´t Veld AJ, Haaksma J, Dijk WA, Visser KR, Boomsma F & Dunselman PH (1996) Prognostic value of heart rate variability during long-term follow-up in patients with mild to moderate heart failure. J Am Coll Cardiol 28: 1183-1189.
Brown RG, Jahanshahi M, Quinn N & Marsden CD (1990) Sexual function in patients with Parkinson’s disease and their partners. J Neurol Neurosurg Psychiatry 53: 480-486.
Brücke T, Asenbaum S, Pirker W, Djamshidian S, Wenger S, Wöber Ch, Müller Ch & Podreka I (1997) Measurement of dopaminergic degeneration in Parkinson’s disease with [123I]β-CIT and SPECT. Correlation with clinical findings and comparison with multiple system atrophy and progressive supranuclear palsy. J Neural Transm 50(Suppl):S9-24.
Brücke T, Kornhuber J, Angelberger P, Asenbaum S, Frassine H & Podreka I (1993) SPECT imaging of dopamine and serotonin transporters with [123I]β-CIT. Binding kinetics in the human brain. J Neural Transm 94: 137-146.
Burn DJ, Mark MH, Playford RD, Maraganore DM, Zimmerman TR Jr, Duvoisin RC, Harding AE, Marsden CD & Brooks DJ (1992) Parkinson’s disease in twins with 18F-dopa and positron emission tomography. Neurology 42: 1894-1900.
Calne DB, Brennan J, Spiers ASD & Stern GM (1970) Hypotension caused by L-dopa. Brit Med J 1: 474-475
Camerlingo M, Aillon C, Bottacchi E, Gambaro P, D’Alessandro G, Franceschi M, Denoti G & Mamoli A (1986) Parasympathetic assessment in Parkinson’s disease. In: Yahr MD & Bergmann J (eds.) Advances in Neurology. Raven Press, New York 45: 267-269.
Camerlingo M, Ferraro B, Gazzaniga GC, Casto L, Cesana BM & Mamoli A (1990) Cardiovascular reflexes in Parkinson’s disease: long-term effects of levodopa treatment on de novo patients. Acta Neurol Scand 81: 346-348.
Cechetto DF (1987) Central representation of visceral function. Fed Proc 46: 17-23. Chan P, Jiang X, Forno LS, Di Monte DA, Tanner CM & Langston JW (1998) Absence of
mutations in the coding region of the alpha-synuclein gene in pathologically proven Parkinson’s disease. Neurology 50: 1136-1137.
Chandiramani V, Palace J & Fowler C (1997) How to recognise patients with parkinsonism who should not have urological surgery. Br J Urol 80: 100-104.
Christie MJ (1981) Electrodermal activity in the 1980s: a review. J R Soc Med 74: 616-622. Churchyard A, Mathias CJ, Boonkongchuen P & Lees AJ (1997) Autonomic effects of selegiline:
possible cardiovascular toxicity on Parkinson�s disease. J Neurol Neurosurg Psychiatry 63: 228-234.
Cohen J, Low P & Fealey RD (1987) Somatic and autonomic function in progressive autonomic failure and multiple system atrophy. Ann Neurol 22: 692-699.
Collins KJ (1999) Temperature regulation and the autonomic nervous system. In: Mathias CJ & Bannister R (eds) Autonomic Failure: A Textbook of Clinical Disorders of the Autonomic Nervous System, 4th ed. Oxford University Press, Inc., New York, p 92-98.
Concensus statement on the definition of orthostatic hypotension, pure autonomic failure, and multiple system atrophy (1996) Clin Auton Res 6: 125-126.

75
Cooper PE (1990) Disorders of the hypothalamus and the pituitary gland. In: Joynt RJ (ed) Clinical Neurology, vol. 3. J.B. Lippincot Company, Philadelphia, p 1-88.
Cotzias GC, van Woert MH, & Schiffer LM (1967) Aromatic amino acids and modification of parkinsonism. N Engl J Med 276: 374-379.
Cowley AW Jr (1992) Long-term control of arterial blood pressure. Physiol Rev 72: 231-300. Dampney RAL (1994) Functional organization of central pathways regulating the cardiovascular
system. Physiol Rev 74: 323-364. Daniel SE & Lees AJ (1993) Parkinson’s Disease Society Brain Bank, London: overview and
research. J Neural Transm 39(Suppl): S165-172. De Keyser J, DeBacker J-P, Ebinger G & Vauquelin G (1989) Hydrogen-3-GBR-12935 binding to
dopamine uptake sites in the human brain. J Neurochem 53: 1400-1404. DeMarinis M, Stocchi F, Testa SR, deOandis F & Agnoli A (1991) Alterations of thermoregulation
in Parkinson’s disease. Funct Neurol 6: 279-283. Den Hartog Jager WA & Bethlem J (1960) The distribution of Lewy bodies in the central and
autonomic nervous system in idiopathic paralysis agitans. J Neurol Neurosurg Psychiatry 23: 283-290.
Denton TA, Diamond GA, Helfant RH, Khan S & Karagueuzian H (1990) Fascinating rhythm: a primer on chaos theory and its applications to cardiology. Am Heart J 120: 1419-1439.
Dickinson CJ (1981) Neurogenic hypertension revisited. Clin Sci (Colch) 60: 471-477. Donnan PT, Steinke DT, Stubbings C, Davey PG & MacDonald TM (2000) Selegiline and
mortality in subjects with Parkinson�s disease. Neurology 55: 1785-1789. Dotson R, Ochoa J, Marchettini P & Cline M (1990) Sympathetic neural outflow directly recorded
in patients with primary autonomic failure: clinical observations, microneurography, and histopathology. Neurology 40: 1079-1085.
Duguid JR, De La Paz R & De Groot J (1986) Magnetic resonance imaging of the midbrain in Parkinson�s disease. Ann Neurol 20: 744-747.
Durrieu G, Rispail Y, Chatelut E, Berlan M, Rascol A, Montastruc JL, Montastruc P (1990) Beta-adrenergic sensitivity in Parkinson�s disease: effect of levodopa treatment. Clin Neuropharmacol 13: 492-499.
Dwain L, & Eckberg DL (1997) Sympathovagal balance; a critical appraisal. Circulation 96: 3224-3232.
Eckberg DL (1983) Human sinus arrhythmia as an index of vagal cardiac outflow. J Appl Physiol 54: 961-966.
Edwards LL, Quigley EM & Pfeiffer RF (1992) Gastrointestinal dysfunction in Parkinson�s disease: frequency and pathophysiology. Neurology 42: 726-732.
Ehringer H & Hornykiewicz O (1960) Verteilung von Noradrenalin und Dopamin (3-Hydroxytyramin) im Gehirn des Menschen und ihr Verhalten bei Erkrankungen des Extrapyramidalen Systems. Klin Wschr 38: 1236-1239.
Elie B & Guiheneuc P (1990) Sympathetic skin response: normal results in different experimental conditions. Electroencephalogr Clin Neurophysiol 76: 258-267.
Elie B & Louboutin JP (1995) Sympathetic skin response is abnormal in multiple sclerosis. Muscle & Nerve 18: 185-189.
Ewing DJ, Borsey DQ, Bellavere F & Clarke BF (1981) Cardiac autonomic neuropathy in diabetes: comparison of measures of R-R interval variation. Diabetologia 21: 18-24.
Ewing DJ, Campbell IW, Murray H, Neilson JM & Clarke BF (1978) Immediate heart-rate response to standing: simple test for autonomic neuropathy in diabetes. BMJ 1: 145-147.
Ewing DJ, Hume L, Campbell IW, Murray H, Neilson JM & Clarke BF (1980) Autonomic mechanisms in the initial heart rate response to standing. J Appl Physiol 49: 809-814.
Fagius J (1982) Microneurographic findings in diabetic polyneuropathy with special reference to sympathetic activity. Diabetologia 23: 415-420.
Fagius J (1991) Aspects of autonomic neurophysiology in diabetic polyneuropathy. Diabet Med 8: S58-62.
Fagius J & Wallin BG (1980) Sympathetic reflex latencies and conduction velocities in normal man. J Neurol Sci 47: 433-448.
Fahn S (1996) Is levodopa toxic? Neurology 47(Suppl.): S184-195.

76
Fahn S, Elton RL, and the members of the UPDRS Development Committee (1987) UPDRS: Unified Parkinson�s Disease Rating Scale. In: Fahn S, Marsden CD, Calne DB & Goldstein (eds) Recent Developments in Parkinson�s Disease. Macmillan Health Care Information, Florham Park, NJ, p 153-164.
Fearnley JM & Lees AJ (1991) Ageing and Parkinson’s disease: substantia nigra regional selectivity. Brain 114: 2283-2301.
Fleisher LA, Fleckenstein JF, Frank SM & Thuluvath PJ (2000) Heart rate variability as a predictor of autonomic dysfunction in patients awaiting liver transplants. Dig Dis Sci 45: 340-344.
Fleisher LA, Pincus SM & Rosenbaum SH (1993) Approximate entropy of heart rate as a correlate of postoperative ventricular dysfunction. Anesthesiology 78: 683-692.
Forno LS (1996) Neuropathology of Parkinson’s disease. J Neuropathol Exp Neurol 55: 259-272. Frey KA, Koeppe RA, Kilbourn MR, Vander Borght TM, Albin RL, Gilman S & Kuhl DE (1996)
Presynaptic monoaminergic vesicles in Parkinson’s disease and normal aging. Ann Neurol 40: 873-884.
Friedman JH & Lannon MC (1990) Clozapine responsive tremor in Parkinson’s disease. Mov Disord 5: 225-229.
Funk GD & Feldman JL (1995) Generation of respiratory rhythm and pattern in mammals: insight from developmental studies. Curr Opin Neurobiol 5: 778-785.
Fusina S, Conte L, Bertolasi E, Fincati E, Nardelli E & Bongiovanni LG (1999) Sympathetic skin response in early stage idiopathic Parkinson’s disease. Clin Neurophysiol 110: 358-366.
Galinier M, Senard JM, Valet P, Doazan JP, Durrieu G, Tran MA, Montastruc JL, Bounhoure JP (1994) Relationship between arterial blood pressure disturbances and alpha adrenoceptor density. Clin Experiment Hypert 16: 373-389.
Gelb DJ, Oliver E & Gilman S (1999) Diagnostic criteria for Parkinson disease. Arch Neurol 56: 33-39.
Gibbins I (1990) Peripheral autonomic nervous system. In: Paxinos G (ed) The Human Nervous System. Academic Pres, San Diego, p 93-123.
Goetz CG, Lutge W & Tanner CM (1986) Autonomic dysfunction in Parkinson’s disease. Neurology 36: 73-75.
Golbe LI, Di Iorio G, Bonavita, Miller DC & Duvoisin RC (1990) A large kindred with autosomal dominant Parkinson’s disease. Ann Neurol 27: 276-282.
Goldberger AL (1996) Non-linear dynamics for clinicians: chaos theory, fractals, and complexity at the bedside. Lancet 347: 1312-1314.
Goldberger AL & West BJ (1987) Applications of nonlinear dynamics to clinical cardiology. Ann New York Acad Sci 504: 155-212.
Goldstein DS, Holmes C, Cannon III RO, Eisenhofer G & Kopin IJ (1997) Sympathetic cardioneuropathy in dysautonomias. N Engl J Med 336: 696-702.
Goldstein DS, Holmes C, Li ST, Bruce S, Metman L Verhagen & Cannon III RO (2000) Cardiac sympathetic denervation in Parkinson disease. Ann Intern Med 133: 338-347.
Goldstraw PW & Warren DJ (1985) The effect of age on the cardiovascular responses to isometric exercise: a test of autonomic function. Gerontology 31: 54-58.
Gorell JM, Ordidge RJ, Brown GG, Deniau JC, Buderer NM & Helpern JA (1995) Increased iron-related MRI contrast in the substantia nigra in Parkinson’s disease. Neurology 45: 1138-1143.
Goto S, Hirano A & Matsumoto S (1989) Subdivisional involvement of nigrostriatal loop in idiopathic Parkinson’s disease and striatonigral degeneration. Ann Neurol 26: 766-770.
Greenacre JK, Teychenne PF, Petrie A, Calne DB, Leigh N & Reid JL (1976) The cardiovascular effects of bromocriptine in parkinsonism. Br J Clin Pharmacol 3: 571-574.
Grimes DA & Lang AE (1999) Treatment of early Parkinson’s disease. Can J Neurol Sci 26(Suppl. 2): S39-44.
Gross M, Bannister R & Godwin-Austen R (1972) Orthostatic hypotension in Parkinson’s disease. Lancet 1: 174-176.
Gutrecht JA (1994) Sympathetic skin response. J Clin Neurophysiol 11: 519-524. Guynet PG (1990) Role of the ventral medulla oblongata in blood pressure regulation. In: Loewy
AD & Spyer KM (eds) Central Regulation of Autonomic Functions. Oxford University Press, New York, p 145-167.

77
Guyton AC & Hall JE (1996) Nervous regulation of the circulation, and rapid control of arterial pressure. In: Guyton AC & Hall JE, (eds) Textbook of Medical Physiology, 9th edition. Philadelphia: W.B. Saunders Company, p 209-220.
Hainsworth R (1991) Reflexes from the heart. Physiol Rev 71: 617-658. Halliday GM, McRitchie DA, Cartwright HR, Pamphlett R, Hely MA & Morris JGL (1996)
Midbrain neuropathology in idiopathic Parkinson’s disease and diffuse Lewy body disease. J Clin Neurosci 3:52-60.
Harati Y & Machkhas H (1997) Spinal cord and peripheral nervous system. In: Low PA (ed) Clinical Autonomic Disorders, 2nd ed. Lippincott-Raven Publishers, Philadelphia, p 25-45.
Havanka-Kanniainen H, Tolonen U & Myllylä VV (1988) Autonomic dysfunction in migraine: a survey of 188 patients. Headache 28: 465-470.
Heinonen EH, Savijärvi M, Kotila M, Hajba A & Scheinin M (1993) Effects of monoamine oxidase inhibition by selegiline on concentrations of noradrenaline and monoamine metabolites in CSF of patients with Alzheimer’s disease. J Neural Transm 5: 193-202.
Hiltunen J, Åkerman KK, Kuikka JT, Bergström KA, Halldin C, Nikula T, Räsänen P, Tiihonen J, Vauhkonen M, Karhu J, Kupila J, Länsimies E & Farde L (1998) Iodine-123 labelled nor-β-CIT as a potential tracer for serotonin transporter imaging in the human brain with single-photon emission tomography. Eur J Nucl Med 25: 19-23.
Hirashima F, Yokota T & Hayashi M (1996) Sympathetic skin response in Parkinson’s disease. Acta Neurol Scand 93: 127-132.
Hirsch JA & Bishop B (1981) Respiratory sinus arrhythmia in humans: how breathing pattern modulates heart rate. Am J Physiol 241: 620-629.
Ho KKL, Moody GB, Peng CK, Mietus JE, Larson MG, Levy D & Goldberger AL (1997) Predicting survival in heart failure cases and control subjects by use of fully automated methods for deriving nonlinear and conventional indices of heart rate dynamics. Circulation 96: 842-848.
Hoehn MM & Yahr MD (1967) Parkinsonism: onset, progression, and mortality. Neurology 17: 427-442.
Hughes AJ, Daniel SE, Kilford L & Lees AJ (1992) The accuracy of the clinical diagnosis of Parkinson’s disease: A clinicopathological study of 100 cases. J Neurol Neurosurg Psychiatry 55: 181-184.
Huikuri HV, Kessler KM, Terracall E, Castellanos A, Linnaluoto MK & Myerburg RJ (1990) Reproducibility and circadian rhythm of heart rate variability in healthy subjects. Am J Cardiol 65: 391-395.
Huikuri HV, Koistinen MJ, Yli-Mäyry S, Airaksinen KEJ, Seppänen T, Ikäheimo MJ & Myerburg RJ (1995) Impaired low frequency oscillations of heart rate in patients with prior acute myocardial infarction and life-threatening arrhythmias. Am J Cardiol 76: 56-60.
Huikuri HV, Mäkikallio TH, Airaksinen KEJ, Seppänen T, Puukka P, Räihä IJ & Sourander LB (1998) Power law relationship of heart rate variability as a predictor of mortality in the elderly. Circulation 97: 2031-2036.
Huikuri HV, Seppänen T, Koistinen MJ, Airaksinen J, Ikäheimo MJ, Castellanos A & Myerburg RJ (1996) Abnormalities in beat-to-beat dynamics of heart rate before the spontaneous onset of life-threatening ventricular tachyarrhythmias in patients with prior myocardial infarction. Circulation 93: 1836-1844.
Ieda T, Hirayama M, Koike Y, Hasegawa Y, Hakusui S & Takahashi A (1994) Hemodynamic study on postprandial hypotension in patients with Parkinson’s disease having autonomic failure (abstract). In: 11th Int Symp Parkinson’s Disease, Rome p 157A.
Innis RB, Marek KL, Sheff K, Zoghbi S, Castronuovo J, Feigin A & Seibyl JP (1999) Effect of treatment with L-dopa/carbidopa or L-selegiline on striatal dopamine transporter SPECT imaging with [123I]beta-CIT. Mov Disord 14: 436-442.
Ishida G, Nakashima K & Takahashi K (1990) Skin nerve sympathetic activity reflex latency in Parkinson’s disease. Acta Neurol Scand 81: 121-124.
Isojärvi JI, Ansakorpi H, Suominen K, Tolonen U, Repo M & Myllylä VV (1998) Interictal cardiovascular autonomic responses in patients with epilepsy. Epilepsia 39: 420-426.
78
Itoh K, Weis S, Mehraein P & Müller-Höcker J (1997) Defects of cytochrome c-oxidase in the substantia nigra of Parkinson’s disease: An immunohistochemical and morphometric study. Mov Disord 12: 9-16.
Iwasaki S, Hamguchi K, Iwasaki A, Takagusaki M & Narabayashi Y (1990) Hypotensive effect of long-term levodopa in patients with Parkinson’s disease. Eur Neurol 30: 194-199.
Jackson-Lewis V, Donaldson D & Przedborski S (1997) Apoptosis and Parkinson’s disease. Neurology 48: A323.
Jankovic J, Rajput AH, McDermott MP, Perl DP, for the Parkinson Study Group (2000) The evolution of diagnosis in early Parkinson Disease. Arch Neurol 57: 369-372.
Jansen Steur ENH (1983) Increase of Parkinson disability after fluoxetine medication. Neurology 42: 211-213.
Jellinger KA (1999) Post mortem studies in Parkinson’s disease – is it possible to detect brain areas for specific symptoms? J Neural Transm 56 (Suppl.): S1-29.
Jellinger KA (1991) Pathology of Parkinson’s disease. Changes other than the nigrostriatal pathway. Mol Chem Neuropathol 14: 153-197.
Jenner O & Olanow CW (1996) Oxidative stress and the pathogenesis of Parkinson’s disease. Neurology 56 (Suppl. 3): S161-170.
Joyce JN, Smutzer G, Whitty CJ, Myers A & Bannon MJ (1997) Differential modification of dopamine transporter and tyrosine hydroxylase mRNAs in midbrain of subjects with Parkinson’s, Alzheimer’s with parkinsonism, and Alzheimer’s disease. Mov Disord 12: 885-897.
Jänig W (1990) Functions of the sympathetic innervation of the skin. In: Loewy AD & Spyer KM (eds) Central Regulation of Autonomic Functions. Oxford University Press, New York, p 334-348.
Jänig W & McLachlan EM (1999) Neurobiology of the autonomic nervous system. In: Mathias CJ & Bannister R (eds) Autonomic Failure: a Textbook of Clinical Disorders of the Autonomic Nervous System, 4th ed. Oxford University Press, New York, p 3-15.
Kaakkola S (2000) Clinical pharmacology, therapeutic use and potential of COMT inhibitors in Parkinson’s disease. Drugs 59: 1233-1250.
Kallio M, Haapaniemi T, Turkka J, Suominen K, Tolonen U, Sotaniemi K, Heikkilä V-P, Myllylä V (2000) Heart rate variability in patients with untreated Parkinson’s disease. Eur J Neurol 7: 667-672.
Kaplan DT & Goldberger AL (1991) Chaos in cardiology. J Cardiovasc Electrophysiol 2: 342-354. Kawabata T & Tachibana H (1997) Evaluation of benzodiazepine receptors in the cerebral cortex
of Parkinson’s disease using 123I-iomazenil SPECT. Nippon Rinsho 55: 244-248. Kay SM & Marple SL Jr (1981) Spectrum analysis: a modern perspective. Proc IEEE, 69: 1380-
1419. Khurana RK & Setty A (1996) The value of the isometric handgrip test – studies in various
autonomic disorders. Clin Autonom Res 6: 211-218. Kim SE, Choi JY, Choe YS, Lee WY, Choi Y, Lee KH, Lim BT (1997) Serotonin transporters in
Parkinson’s disease studied with [I-123]β-CIT SPECT (abstract). J Nucl Med 38 (Suppl.): 280A.
Kim SE, Lee WY, Choe YS & Kim JH (1999) SPECT measurement of iodine-123-β-CIT binding to dopamine and serotonin transporters in Parkinson’s disease: Correlation with symptom severity. Neurol Res 21: 255-261.
Kitada T, Asakawa S, Hattori N, Matsumine H, Yamamura Y, Minoshima S, Yokochi M, Mizuno Y & Shimizu N (1998) Mutations in the parkin gene cause autosomal recessive juvenile parkinsonism. Nature 392: 605-608.
Kleiger RE, Miller JP, Bigger JT, Moss AJ, for the Multicenter Post-infarction Research Group (1987) Decreased heart rate variability and its association with increased mortality after acute myocardial infarction. Am J Cardiol 59: 256-262.
Koepchen HP, Klussendorf D & Sommer D (1981) Neurophysiological background of central neural cardiovascular-respiratory coordination: basic remarks and experimental approach. J Auton Nerv Syst 3: 335-368.

79
Koike Y & Takahashi A (1997) Autonomic dysfunction in Parkinson’s disease. Eur Neurol 38 (Suppl. 2): S8-12.
Korczyn AD (1990) Autonomic nervous system disturbances in Parkinson’s disease. In: Streifler MB, Korczyn AD, Melamed E & Youdim MBH (eds.) Advances in Neurology. New York: Raven Press, 53: 463-468.
Korpelainen JT, Sotaniemi KA, Mäkikallio A, Huikuri HV & Myllylä VV (1999) Dynamic behavior of heart rate in ischemic stroke. Stroke 30: 1008-1012.
Korpelainen JT, Sotaniemi KA, Suominen K, Tolonen U & Myllylä VV (1994) Cardiovascular autonomic reflexes in brain infarction. Stroke 25: 787-792.
Korpelainen JT, Tolonen U, Sotaniemi KA & Myllylä VV (1993) Suppressed sympathetic skin response in brain infarction. Stroke 24: 1389-1392.
Kruger R, Kuhn W, Muller T, Woitalla D, Graeber M, Kosel S, Przuntek H, Epplen JT, Schols L & Riess O (1998) Ala30Pro mutation in the gene encoding alpha-synuclein in Parkinson’s disease. Nature Genetics 18: 106-108.
Kujawa K, Leurgans S, Raman R, Blasucci L & Goetz CG (2000) Acute orthostatic hypotension when starting dopamine agonists in Parkinson’s disease. Arch Neurol 57: 1461-1463.
Kumada M, Terui N & Kuwaki T (1990) Arterial baroreceptor reflex: its central and peripheral neural mechanisms. Prog Neurobiol 35: 331-361.
Kuopio A-M, Marttila RJ, Helenius H & Rinne UK (1999) Changing epidemiology of Parkinson’s disease in southwestern Finland. Neurology 52: 302-308.
Kuopio A-M, Marttila RJ, Helenius H & Rinne UK (1999) Environmental risk factors in Parkinson’s disease. Mov Disorord 14: 928-939.
Kuroiwa Y, Shimada Y & Toukura Y (1983) Postural hypotension and low R-R interval variability in parkinsonism, spinocerebellar degeneration, and Shy-Drager syndrome. Neurology 33: 463-467.
Kösel S, Egensperger R, von Eitzen U, Mehraein P & Graeber MP (1997) On the question of apoptosis in the parkinsonian substantia nigra. Acta Neuropathol 93: 105-109.
Laihinen AO, Rinne JO, Nagren KA, Lehikoinen PK, Oikonen VJ, Ruotsalainen UH, Ruottinen HM, Rinne UK (1995) PET studies on brain monoamine transporters with carbon-11-beta-CIT in Parkinson’s disease. J Nucl Med 36: 1263-1267.
Laine TPJ, Ahonen A, Torniainen P, Heikkilä J, Pyhtinen J, Räsänen P, Niemelä O & Hillbom M (1999) Dopamine transporters increase in human brain after alcohol withdrawal. Molecular Psychiatry 4: 189-191.
Langston JW & Forno LS (1978) The hypothalamus in Parkinson’s disease. Ann Neurol 3: 129-133.
Laruelle M, Balwin RM, Malison RT, Zea-Ponce Y, Zoghbi SS, Al-Tikriti MS, Sybirska EH, Zimmerman RC, Wisniewski G, Neumeyer JL, Milius RA, Wang S, Smith EO, Roth RH, Charney DS, Hoffer PB & Innis RB (1993) SPECT imaging of dopamine and serotonin transporters with [123I]β-CIT: Pharmacological characterization of brain uptake in nonhuman primates. Synapse 13: 295-309.
Laruelle M, Vanisberg M-A & Maloteaux J-M (1988) Regional and subcellular localization in human brain of [3H]paroxetine binding, a marker of serotonin uptake sites. Biol Psychiatry 24: 299-309.
Laruelle M, Wallace E, Seibyl JP, Baldwin RM, Zea-Ponce Y, Zoghbi SS, Neumeyer JL, Charney DS, Hoffer PB & Innis RB (1994) Graphical, kinetic and equilibrium analyses in vivo [123I]β-CIT binding to dopamine transporters in healthy human subjects. J Cereb Blood Flow Metab 14: 982-994.
LeDoux JE (2000) Emotion circuits in the brain. Annu Rev Neurosci 23: 155-184. Leenders K, Salmon EP, Tyrrell P, Perani D, Brooks DJ, Sager H, Jones T, Marsden CD &
Frackowiak RS (1990) The nigrostriatal dopaminergic system assessed in vivo by positron emission tomography in healthy volunteer subjects and patients with Parkinson’s disease. Arch Neurol 47: 1290-1298.
Lees AJ on behalf of the Parkinson’s Disease Research Group of the UK. (1996) Comparison of therapeutic effects and mortality data of levodopa and levodopa combined with selegiline in patients with early, mild Parkinson’s disease. BMJ 311: 1602-1607.

80
Levy MN (1984) Cardiac sympathetic-parasympathetic interactions. Fed Proc 43: 2598-2602. LeWitt PA, Ward CD, Larsen TA, Raphaelson MI, Newman RP, Foster N, Dambrosia JM & Calne
DB (1983) Comparison of pergolide and bromocriptine therapy in parkinsonism. Neurology 33: 1009-1014.
Lieberman A (1998) Managing the neuropsychiatric symptoms of Parkinson’s disease. Neurology 50(Suppl 6): S33-38.
Lin TK, Chee EC, Chen HJ & Cheng MH (1995) Abnormal sympathetic skin response in patients with palmar hyperhidrosis. Muscle Nerve 18: 917-919.
Linden D & Berlit P (1995) Sympathetic skin response (SSRs) in monophocal brain lesions: topographical aspects of central sympathetic pathways. Acta Neurol Scand 91: 372-376.
Litvan I, MacIntyre A, Goetz CG, Wenning GK, Jellinger K, Verny M, Bartko JJ, Jankovic J, McKee A, Brandel JP, Chaudhuri KR, Lai EC, D’Olhaberriague L, Pearce RK & Agid Y(1998) Accuracy of the clinical diagnosis of Lewy body disease, Parkinson disease, and dementia with Lewy bodies: a clinicopathologic sudy. Arch Neurol 55: 969-978.
Loewy AD (1990) Central autonomic pathways. In: Loewy AD & Spyer KM (eds) Central Regulation of Autonomic Functions. Oxford University Press, New York, p 88-103.
Loewy AD (1991) Forebrain nuclei involved in autonomic control. Prog Brain Res 87: 253-268. Loewy AD & Spyer KM (1990) Vagal preganglionic neurons. In: Loewy AD & Spyer KM (eds)
Central Regulation of Autonomic Functions. Oxford University Press, New York, p 68-87. Lovick TA & Li P (1993) Integrated function of neurones in the rostral ventrolateral medulla. Prog
Brain Res 81: 223-232. Low PA & Fealey RD (1999) Evaluation of sudomotor function. In: Autonomic failure: A
Textbook of Clinical Disorders of the Autonomic Nervous System 4th ed. Oxford University Press, New York, p 263-270.
Low PA, Offer-Gehrking TL, Proper CJ & Zimmerman I (1990) The effect of ageing on cardiac autonomic and postganglionic sudomotor function. Muscle Nerve 13: 152-157.
Low PA, Zimmerman BR & Dyck PJ (1986) Comparison of distal sympathetic with vagal function in diabetic neuropathy. Muscle Nerve 9: 592.596.
Ludin SM, Steiger UH & Ludin HP (1987) Autonomic disturbances and cardiovascular reflexes in idiopathic Parkinson�s disease. J Neurol 235: 10-15.
Mackay JD, Page M, Cambridge J & Watkins PJ (1980) Diabetic autonomic neuropathy. The diagnostic value of heart rate monitoring. Diabetologia 18: 471-478.
Magalhães M, Wenning GK, Daniel SE & Quinn NP (1995) Autonomic dysfunction in pathologically confirmed multiple system atrophy and idiopathic Parkinson�s disease: A retrospective comparison. Acta Neurol Scand 91: 98-102.
Malison RT, Price LH, Berman R, van Dyck CH, Pelton GH, Carpenter L, Sanacora G, Owens MJ, Nemeroff CB, Rajeevan N, Baldwin RM, Seibyl JP, Innis RB & Charney DS (1998) Reduced brain serotonin transporter availability in major depression measured by [123I]2β-carboxymethoxy-3β-(4-iodophenyl)tropane and single photon emission computed tomography. Biol Psychiatry 44: 1090-1098.
Mano Y, Nakamuro T, Takayanagi T & Mayer RF (1994) Sweat function in Parkinson’s disease. J Neurol 241: 573-576.
Marek KL, Seibyl JP, Zoghbi SS, Zea-Ponce Y, Baldwin RM, Fussell B, Charney DS, van Dyck C, Hoffer PB & Innis RB (1996) [123I]β-CIT/SPECT imaging demonstrates bilateral loss of dopamine transporters in hemi-Parkinson’s disease. Neurology 46: 231-237.
Martignoni E, Pacchetti C, Godi L, Micieli G & Nappi G (1995) Autonomic disorders in Parkinson’s disease. J Neural Transm 45(Suppl.): S11-19.
Marttila R (1974) Epidemiological, clinical, and virus serological studies of Parkinson’s disease. Doctoral thesis, Turku.
Marttila RJ (1983) Diagnosis and epidemiology of Parkinson’s disease. Acta Neurol Scand 95(Suppl.): S9-17.
Maselli RA, Jaspan JB, Soliven BC, Green AJ, Spire JP & Arnason BG (1989) Comparison of sympathetic skin response with quantitative sudomotor axon reflex test in diabetic neuropathy. Muscle Nerve 12: 429-423.

81
Mastrocola C, Vanacore N, Giovani A, Locuratolo N, Vella C, Alessandri A, Baratta L, Tubani L & Meco G (1999) Twenty-four-hour heart rate variability to assess autonomic function in Parkinson’s disease. Acta Neurol Scand 99: 245-247.
Mathias CJ (1997) Autonomic disorders and their recognition. N Engl J Med 10: 721-724. Mathias CJ & Bannister R (1999) Investigation of autonomic disorders. In: Mathias CJ & Bannister
R (eds) Autonomic failure: A Textbook of Clinical Disorders of the Autonomic Nervous System, 4th ed. Oxford University Press, New York, p 169-195.
Mathias CJ, Frankel HL, Christensen NJ & Spalding JM (1976) Enhanced pressor response to noradrenaline in patients with cervical spinal cord transection. Brain 99: 757-770.
Matthews KA & Stoney CM (1988) Influences of sex and age on cardiovascular responses during stress. Psychosom Med 50: 46-56.
Matthews MR (1999) Autonomic ganglia and preganglionic neurones in autonomic failure. In: Mathias CJ & Bannister R, (eds) Autonomic failure: A Textbook of Clinical Disorders of the Autonomic Nervous System. Fourth edition. New York: Oxford University Press, p 329-339.
Mayeux R (1992) The mental state in Parkinson’s disease. In: Koller WC (ed) Handbook of Parkinson’s Disease. Marcel Decker Inc., New York, p 159-184.
Mayeux R, Stern Y, Sano M, Williams JB & Cote LJ (1988) The relationship of serotonin to depression in Parkinson’s disease. Mov Disord 3: 237-244.
McDowell FH & Lee JE (1970) Levodopa, Parkinson’s disease, and hypotension. Ann Intern Med 72: 751-752.
McGeer PL, Itagaki S, Akiyama H & McGeer EG (1988) Rate of cell death in parkinsonism indicates active neuropathological process. Ann Neurol 24: 574-576.
Meco G, Pratesi L & Bonifati V (1991) Cardiovascular reflexes and autonomic dysfunction in Parkinson’s disease. J Neurol 238: 195-199.
Mehta AE & Tolis G (1979) Pharmacology of bromocriptine in health and disease. Drugs 17: 313-325.
Mesec A, �ega S, Tro�t M & Pogačnik T (1999) The deterioration of cardiovascular reflexes in Parkinson�s disease. Acta Neurol Scand 100: 269-299.
Michelakis AM & Robertson D (1970) Plasma renin activity and levodopa in Parkinson’s disease. JAMA 213: 83-85.
Micieli G, Martignoni E, Cavallini A, Sandrini G & Nappi G (1987) Postprandial and orthostatic hypotension in Parkinson’s disease. Neurology 37: 386-393.
Milon D, Allain H, Bentue-Ferrer D, Martinet JP, Lemaitre MH, Decombe R (1991) Cardiac beta-adrenoceptor sensitivity and Parkinson’s disease. Fundam Clin Pharmacol 5: 539-548.
Miyawaki E, Lyons K, Pahwa R, Troster AI, Hubble J, Smith D, Busenbark K, McGuire D, Michalek D & Koller WC (1997) Motor complications of chronic levodopa therapy in Parkinson’s disease. Clin Neuropharmacol 20: 523-530.
Montagna P, Salvi F & Liguori R (1988) Sympathetic skin response in familial amyloid polyneuropathy, letter. Muscle Nerve 11: 183-184.
Montastruc JL, Chamontin B & Rascol A (1985) Parkinson’s disease and hypertension: Chronic bromocriptine treatment. Neurology 35: 1644-1647.
Morrish PK, Sawle GV & Brooks DJ (1995) Clinical and [18F]dopa-PET findings in early Parkinson’s disease. J Neurol Neurosurg Psychiatry 59: 597-600.
Murata Y, Harada T, Ishizaki F, Izumi Y & Nakamura S (1997) Autonomic dysfunction in Parkinson’s disease and vascular parkinsonism. Acta Neurol Scand 96: 359-365.
Müller T, Farahati J, Kuhn W, Eising EG, Przuntek H, Reiners C & Coenen HH (1998) [123I]β-CIT SPECT visualizes dopamine transporter loss in de novo parkinsonian patients. Eur Neurol 39: 44-48.
Myllylä VV, Korpelainen JT, Tolonen U, Havanka H & Saari A (2000) Neuropathology and cardiovascular regulation. In: Ter Horst GJ (ed) The Nervous System and the Heart. Humana Press Inc., New York, p 181- 237.
Mytilineou C, Radcliffe PM & Olanow CW (1997) L-(-)-desmethylselegiline, a metabolite of selegiline [L-(-)-deprenyl], protects mesencephalic dopamine neurons from excitotoxity in vitro. J Neurochem 68: 434-436.

82
Mäkikallio TH, Høiber S, Køber L, Torp-Pedersen C, Peng C-K, Goldberger AL & Huikuri HV (1999) Fractal analysis of heart rate dynamics as a predictor of mortality in patients with depressed left ventricular function after acute myocardial infarction. Am J Cardiol 83: 836-839.
Mäkikallio TH, Koistinen MJ, Jordaens L, Tulppo MP, Wood N, Golosarsky B, Peng CK, Goldberger AL & Huikuri HV (1999) Heart rate dynamics before spontaneous onset of ventricular fibrillation in patients with healed myocardial infarcts. Am J Cardiol 83: 880-884.
Mäkikallio TH, Ristimäe T, Airaksinen KE, Peng CK, Goldberger AL & Huikuri HV (1998) Heart rate dynamics in patients with stable angina pectoris and utility of fractal and complexity measures. Am J Cardiol 81: 27-31.
Nahmias C, Garnett ES, Firnau G & Lang A (1985) Striatal dopamine distribution in Parkinsonian patients during life. J Neurol Sci 69: 223-230.
Nathan PW & Smith MC (1987) The location of descending fibres to sympathetic preganglionic vasomotor and sudomotor neurons in man. J Neurol Neurosurg Psychiatry 50: 1253-1262.
Neafsey EJ (1990) Prefrontal cortical control of the autonomic nervous system: anatomical and physiological observations. Prog Brain Res 85: 147-165.
Nedergaard OA, Moller J (1994) Inhibition by (-)-deprenyl of agonist-evoked contractions in rabbit aorta. Pharmacol Toxicol 75: 377-383.
Niimi Y, Ieda T, Hirayama M, Koike Y, Sobue G, Hasegawa Y & Takahashi A (1999) Clinical and physiological characteristics of autonomic failure with Parkinson’s disease. Clin Auton Res 9: 139-144.
Nishimura RA & Tajik AJ (1986) Valsalva maneuver and response revisited. Mayo Clin Proc 61: 211-217.
Ogawa N (1998) Early introduction of dopamine agonists in the long-term treatment of Parkinson’s disease. Neurology 51(Suppl. 2): S13-20.
Ogawa T & Low PA (1993) Autonomic regulation of temperature and sweating. In: Low PA (ed) Clinical Autonomic Disorders: Evaluation and Management. Little, Brown and company, Boston, p 79-91.
Olanow CW, Hauser RA, Gauger L, Malapira T, Koller W, Hubble J, Bushenbark K, Lilienfeld D & Esterlitz J (1995) The effect of deprenyl and levodopa on the progression of Parkinson’s disease. Ann Neurol 38: 771-777.
Oppenheimer DR (1980) Lateral horn cells in progressive autonomic failure. J Neurol Sci 46: 393-404.
Ori Z, Monir G, Weiss J, Sayhouni X & Singer DH (1992) Heart rate variability. Frequency domain analysis. Cardiol Clin 10: 499-537.
Orimo S, Ozawa E, Nakade S, Sugimoto S & Mizysawa H (1999) 123I-metaiodobenzylguanidine myocardial scintigraphy in Parkinson’s disease. J Neurol Neurosurg Psychiatry 67: 189-194.
Otsuka M, Ichiya Y, Hosokawa S, Kuwabara Y, Tahara T, Fukumura T, Kato M, Masuda K & Goto I (1991) Striatal blood flow, glucose metabolism, and 18F-dopa uptake: difference in Parkinson’s disease and atypical parkinsonism. J Neurol Neurosurg Psychiatry 54: 898-904.
Pagani M, Lucini D, Pizzinelli P, Sergi M, Bosisio E, Sandro MG & Malliani A (1996) Effect of aging and of chronic obstructive pulmonary disease on RR interval variability. J Auton Nerv Sys 59: 125-132.
Pagani M, Montano N, Porta A, Malliani A, Abboud FM, Birkett C & Somers VK (1997) Relationship between spectral components of cardiovascular variabilities and direct measures of muscle sympathetic nerve activity in humans. Circulation 95: 1441-1448.
Palacios JM, Camps M, Cortes R & Probst A (1988) Mapping dopamine receptors in the human brain. J Neural Transm 27(Suppl.): S227-235.
Parkinson J (1817) An Essay on the Shaking Palsy. Sherwood, Neely, and Jones, London. Piha SJ (1993) Cardiovascular responses to various autonomic tests in males and females. Clin
Autonom Res 3: 15-20. Piha SJ, Rinne JO, Rinne UK & Seppänen A (1988) Autonomic dysfunction in recent onset and
advanced Parkinson’s disease. Clin Neurol Neurosurg 90: 221-226. Pincus SM & Goldberger AL (1994) Physiologic time series analysis: what does regularity
quantify? Am J Physiol 226: H1643-1656.

83
Pincus SM & Viscarello RR (1992) Approximate entropy: statistical properties and applications. Commun Stat Theory Meth 21: 3061-3077.
Pirker W, Asenbaum S, Kasper S, Walter H, Angelberger P, Koch G, Pozzera A, Deecke L, Podreka I & Brücke T (1995) Beta-CIT SPECT demonstrates blockage of 5HT-uptake sites by citalopram in the human brain in vivo. J Neural Transm 100: 247-256.
Pirker W, Asenbaum S, Wenger S, Kornhuber J, Angelberger P, Deecke L, Podreka I & Brücke T (1997) Iodine-123-epidepride-SPECT: studies in Parkinson’s disease, multiple system atrophy and Huntington’s disease. J Nucl Med 38: 1711-1717.
Pisano F, Miscio G, Mazzuero G, Lantranchi P, Colombo R & Pinelli P (1995) Decreased heart rate variability in amyotrophic lateral sclerosis. Muscle Nerve 18: 1225-1231.
Polymeropoulos MH, Lavedan C, Leroy E, Ide SE, Dehejia A, Dutra A, Pike B, Root H, Rubenstein J, Boyer R, Stenroos ES, Chandrasekharappa S, Athanassiadou A, Papapetropoulos T, Johnson WG, Lazzarini AM, Duvoisin RC, Di Iorio G, Golbe LI & Nussbaum RL (1997) Mutation in the -synuclein gene identified in families with Parkinson’s disease. Science 276: 2045-2047.
Pomeranz B, Macauley RJB, Caudill MA, Kutz I, Adam D, Gordon D, Kilborn KM, Barger AC, Shannon DC & Cohen RJ (1985) Assessment of autonomic function in humans by heart rate spectral analysis. Am J Physiol 248: H151-153.
Qualman SJ, Haupt HM, Yang P & Hamilton SR (1984) Esophageal Lewy bodies associated with ganglion cell loss in achalasia. Similarity to Parkinson’s disease. Gastroenterology 87: 848-856.
Quinn N, Illas A, Lhermitte F & Agid Y (1981) Bromocriptine in Parkinson’s disease: a study of cardiovascular effects. J Neurol Neurosurg Psychiatry 44: 426-429.
Rajput AH (1984) Epidemiology of Parkinson’s disease. Can J Neurol Sci 11 (Suppl. 1): S156-159. Rajput AH (1992) Frequency and cause of Parkinson’s disease. Can J Neurol Sci 19 (Suppl. 1):
S103-107. Rajput AH & Rodzilsky B (1976) Dysautonomia in parkinsonism: a clinicopathological study. J
Neurol Neurosurg Psychiatry 39: 1092-1100. Rajput AH & Rodzilsky B (1991) Accuracy of clinical diagnosis in Parkinsonism — a prospective
study. Can J Neurol Sci 18: 275-278. Randall WC, Wurster RD (1994) Peripheral innervation of the heart. In: Levy MN, Schwartz PJ
(eds) Vagal Control of the Heart: Experimental Basis and Clinical Implications. Futura Publishing Company, Armonk, NY, p 21-32.
Rascol O, Brooks DJ, Brunt ER, Korczyn AD, Poewe WH & Stocchi F (1998) Ropinirole in the treatment of early Parkinson’s disease: a 6-month interim report of 5-year levodopa-controlled study. 056 Study Group. Mov Disord 13: 39-45.
Ravits J, Hallet M, Nilsson J, Polinsky R & Dambrosia J (1995) Electrophysiological tests of autonomic function in patients with idiopathic autonomic failure syndromes. Muscle Nerve 19: 758-763.
Ravits JM (1997) Autonomic nervous system testing. Muscle Nerve 48: 919-937. Reid JL (1990) Central and peripheral autonomic control mechanisms. In: Bannister R (ed)
Autonomic Failure: A Textbook of Clinical Disorders of the Autonomic Nervous System. Oxford University Press, New York, p 44-55.
Reid JL & Calne DB (1973) Cardiovascular effects of levodopa in parkinsonism. In: Calne DB (ed) Advances in Neurology. Raven Press, New York, p 223-232.
Reinhardt MJ, Jüngling FD, Krause TM & Braune S (2000) Scintigraphic differentiation between two forms of primary dysautonomia early after onset of autonomic dysfunction: value of cardiac and pulmonary iodine-123 MIBG uptake. Eur J Nucl Med 27: 595-600.
Richter DW & Spyer KM (1990) Cardiorespiratory control. In: Loewy AD & Spyer KM (eds) Central Regulation of Autonomic Functions. Oxford University Press, Oxford, p 189-207.
Rinne JO, Rummukainen J, Paljärvi L & Rinne UK (1989) Dementia in Parkinson’s disease is related to neuronal loss in the medial substantia nigra. Ann Neurol 26: 47-50.
Rinne UK (1987) Early combination of bromocriptine and levodopa in the treatment of Parkinson’s disease: a 5-year follow-up. Neurology 37: 826-828.
84
Rinne UK, Bracco F, Chouza C, Dupont E, Gershanik O, Marti Masso JF, Montastruc JL, Marsden CD, Dubini A, Orlando N & Grimaldi R (1997) Cabergoline in the treatment of early Parkinson’s disease: results of the first year of treatment in a double-blind comparison of cabergoline and levodopa. Neurology 48: 363-368.
Rosenbaum M & Race D (1968) Frequency-response characteristics of vascular resistance vessels. Am J Physiol 1397-1402.
Rossi L (1994) Histology of cardial vagal innervation in man. In: Levy MN & Schwartz PJ (eds) Vagal Control of the Heart: Experimental Basis and Clinical Implications. Futura Publishing Company, Armonk, NY, p 3-20.
Ruggiero DA, Cravo SL, Arango V & Reis GJ (1989) Central control of the circulation by the rostral ventrolateral reticular nucleus: anatomical substrates. Progr Brain Res 81: 49-79.
Sachs C, Berglund B & Kaijser L (1985) Autonomic cardiovascular responses in parkinsonism: effect of levodopa with dopa-decarboxylase inhibition. Acta Neurol Scand 71: 37-42.
Salmon E, Brooks DJ, Leenders KL, Turton DR, Hume SP, Cremer JE, Jones T & Frackowiak RS (1990) A two-compartment description and kinetic procedure for measuring regional cerebral [11C]nomifensine uptake using positron emission tomography. J Cereb Blood Flow Metab 10: 307-316.
Sandroni P, Ahlskog JE, Fealey RD & Low PA (1991) Autonomic involvement in extrapyramidal and cerebellar disorders. Clin Auton Res 1: 147-155.
Saul JP, Berger PD, Albrecht P, Stein SP, Chen MH & Cohen RJ (1991) Transfer function analysis of the circulation: unique insights into cardiovascular regulation. Am J Physiol 261: H1231-1245.
Schapira AHV (1995) Oxidative stress in Parkinson’s disease. Neuropathol Appl Neurobiol 21: 3-9.
Schatz J (1984) Orthostatic hypotension: II. Clinical diagnosis and treatment. Arch Intern Med 144: 1037.
Schondorf R (1993) The role of the sympathetic skin response in the assessment of autonomic function. In: Low PA (ed) Clinical Autonomic Disorders: Evaluation and Management. Little, Brown and company, Boston, p 231-241.
Schwarz J, Antonini A, Tatsch K, Kirsch CM, Oertel WH & Leenders KL (1994) Comparison of 123I-IBZM SPECT and 11C-raclopride PET findings in patients with parkinsonism. Nucl Med Commun 15: 806-813.
Seibyl JP, Marek KL, Quinlan D, Sheff K, Zoghbi S, Zea-Ponce Y, Baldwin RM, Fussell B, Smith EO, Charney DS, Hoffer PB & Innis RB (1995) Decreased single-photon emission computed tomographic [123I] -CIT striatal uptake correlates with symptom severity in Parkinson’s disease. Ann Neurol 38: 589-598.
Seidler A, Hellenbrand W, Robra BP, Vieregge P, Nischan P, Joerg J, Oertel WH, Ulm G & Schneider E (1996) Possible environmental, occupational, and other etiologic factors for Parkinson’s disease: a case-control study in Germany. Neurology 46: 1275-1284.
Senaratne MP, Carrol D, Warren KG & Kappagoda T (1984) Evidence for cardiovascular autonomic nerve dysfunction in multiple sclerosis. J Neurol Neurosurg Psychiatry 47: 947-952.
Sénard J-M, Verwaerde P, Rascol O & Montastruc JL (1995) Effects of acute levodopa administration on blood pressure and heart variability in never treated parkinsonians. Hypertens Res 18 (Suppl 1): S175-177.
Shahani BT, Day TJ, Cros D, Khalil N & Kneebone CS (1990) RR interval variation and the sympathetic skin response in the assessment of autonomic function in peripheral neuropathy. Arch Neurol 47: 659-664.
Shahani BT, Halperin JJ, Boulu P & Cohen G (1984) Sympathetic skin response a method assessing unmyelinated axon dysfunction in peripheral neuropathies. J Neurol Neurosurg Psychiatry 47: 536-542.
Shannon KM, Bennett JP Jr & Friedman JH (1997) Efficacy of pramipexole, a novel dopamine agonist, as monotherapy in mild to moderate Parkinson’s disease. Neurology 49: 724-728.
Shepherd JT & Mancia G (1986) Reflex control of the human cardiovascular system. Rev Physiol Biochem Pharmacol 105: 1-99.
85
Shields RW (1993) Functional anatomy of the autonomic nervous system. J Clin Neurophysiol 10: 2-16.
Shite J, Dong E, Kawai H, Stevens SY, Liang CS (2000) Selegiline improves cardiac sympathetic terminal function and beta-adtnergic reponsiveness in heart failure. Am J Physiol – Heart & Circulatory Physiology 279: H1283-1290.
Simon E, Oierau FK & Taylor DCM (1986) Central and peripheral thermal control of effectors in homeothermic temperature regulation. Physiol Rev 66: 235-300.
Singer C & Underwood EA (1962) Some physiological advances. In: Singer C & Underwood EA (eds) A Short History of Medicine. Clarendon Press, Oxford, p 154-161.
Singer C, Weiner WJ & Sanchez-Ramos JR (1992) Autonomic dysfunction in men with Parkinson’s disease. Eur Neurol 32: 134-140.
Singer C, Weiner WJ, Sanchez-Ramos JR & Ackerman M (1989) Sexual dysfunction in men with Parkinson’s disease. J Neurol Rehab 3: 199-204.
Sjøholm H, Mellgren SI & Sundsfjord J (1997) Nigrostriatal degeneration demonstrated in parkinsonian patients with iodine-123-beta-CIT SPECT: Methods of quantitation. Acta Neurol Scand 96: 91-96.
Sotolongo JR Jr (1988) Voiding dysfunction in Parkinson’s disease. Semin Neurol 8: 166-169. Spiegel EA, Wycis HT, Schor S, Schwartz HA & Fabioni FR (1969) The incidence of vegetative
symptoms in Parkinson patients with or without bradykinesia. In: Gillingham FJ & Donaldson TMC (eds) Third Symposium on Parkinson’s Disease. Livingston, Edinburgh, p 200.
Spyer KM (1981) Neural organisation and control of the baroreceptor reflex. Rev Physiol Biochem Pharmacol 88: 24-124.
Spyer KM (1989) Neural mechanisms involved in cardiovascular control during affective behaviour. Trends Neurosci 12: 506-513.
Spyer KM (1990) The central nervous organization of reflex circulatory control. In: Loewy AD & Spyer KM (eds) Central Regulation of Autonomic Functions. Oxford University Press, New York, p 168-188.
Spyer KM (1995) Central nervous mechanisms responsible for cardio-respiratory homeostasis. Adv Exp Med Biol 381: 73-79.
Standish A, Enquist LW & Schwaber JS (1994) Innervation of the heart and its central medullary origin defined by viral tracing. Science 263: 232-234.
Stjernberg L, Blumberg H & Wallin BG (1986) Sympathetic activity in man after spinal cord injury. Outflow to muscle below the lesion. Brain 109: 695-715.
Stoessl AJ & Ruth TJ (1998) Neuroreceptor imaging: new developments in PET and SPECT imaging of neuroreceptor binding (including dopamine transporters, vesicle transporters and post synaptic receptor sites). Curr Opin Neur 11: 327-333.
Stolwijk JA (1977) Responses to thermal environment. Fed Proc 36: 1655-1658. Sundquist G, Lilja B & Almer LO (1980) Abnormal diastolic blood pressure and heart rate
reactions to tilting in diabetes mellitus. Diabetologia 19: 433-438. Suominen K (1997) Design and implementation of a PC-based data acquisition measuring ECG
and respiratory signals. Int J Clin Monitoring and Computing 14: 225-230. Sveinbjörnsdóttir S, Hicks AA, Jónsson T, Pétursson H, Guðmundsson G, Frigge ML, Kong A,
Gulcher JR & Stefánsson K (2000) Familial aggregation of Parkinson’s disease in Iceland. N Engl J Med 343: 1765-1770.
Swanson LW (1991) Biochemical switching in hypothalamic circuits mediating responses to stress. Prog Brain Res 87: 181-200.
Takeuchi S, Sugiyama Y, Mano T, Iwase S & Matukawa T (1993) Effect of L-dopa on human muscle sympathetic nerve activity. Environ Med 37: 99-102.
Talairach J & Tournoux P (eds) (1988) Coplanar Stereotaxic Atlas of the Human Brain. George Thieme Verlag, New York.
Talman WT & Benarrhoc EE (1993) Neural control of cardiac function. In: Dyck PJ, Thomas PK, Griffin JW, Low PA & Poduslo JF (eds) Peripheral Neuropathy, 3rd ed. WB Saunders Company, Philadelphia, p 177-186.
Talman WT & Kelkar P (1993) Neural control of the heart. Central and peripheral. Neurol Clin 11: 239-256.
86
Taly AB & Muthane UB (1992) Involvement of peripheral nervous system in juvenile Parkinson’s disease. Acta Neurol Scand 85: 272-275.
Tanner CM, Goetz CG, Glantz RH, Glatt SL & Klawans HL (1982) Pergolide mesylate and idiopathic Parkinson disease. Neurology 32: 1175-1179.
Tanner CM, Ottman R, Goldman SM, Ellenberg J, Chan P, Mayeux R & Langston JW (1999) Parkinson’s disease in twins: an etiologic study. JAMA 281: 341-346.
Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology (1996) Heart rate variability: standards of measurement, physiological interpretation, and clinical use. Circulation 93: 1043-1065.
Tatsch K, Schwarz J, Mozley PD, Linke R, Pogarell O, Oertel WH, Fieber RS, Hahn K & Kung HF (1997) Relationship between clinical features of Parkinson’s disease and presynaptic dopamine transporter binding assessed with [123I]IPT and single-photon emission tomography. Eur J Nucl Med 24: 415-421.
The Parkinson study Group (1993) Effects of tocopherol and deprenyl on the progression of disability in early Parkinson’s disease. N Engl J Med 328: 176-183.
Tissingh G, Bergmans P, Booij J, Winogrodzka A, van Royen EA, Stoof JC & Wolters EC (1998) Drug-naive patients with Parkinson’s disease in Hoehn and Yahr stages I and II show a bilateral decrease in striatal dopamine transporters as revealed by [123I]β-CIT SPECT. J Neurol 245: 14-20.
Tranel D & Damasio H (1989) Intact electrodermal skin conductance responses after bilateral amygdala damage. Neuropsychologia 27: 381-390.
Tugnoli V, Eleopra R & De Grandis D (1999) Hyperhidrosis and sympathetic skin response in chronic alcoholic patients. Clin Autonom Res 9: 17-22.
Tulppo MP, Mäkikallio TH, Takala TES, Seppänen T & Huikuri HV (1996) Quantitative beat-to-beat analysis of heart rate dynamics during exercise. Am J Physiol 271: H1573-1579.
Turkka JT (1987) Correlation of the severity of autonomic dysfunction to cardiovascular reflexes and to plasma noradrenaline levels in Parkinson’s disease. Eur Neurol 26: 203-210.
Turkka JT, Juujärvi KK, Lapinlampi TO & Myllylä VV (1986) Serum noradrenaline response to standing up in patients with Parkinson’s disease. Eur Neurol 25: 355-361.
Turkka JT, Juujärvi KK & Myllylä VV (1987a) Correlation of autonomic dysfunction to CSF concentrations of noradrenaline and 3-methoxy-4-hydroxyphenylglycol in Parkinson’s disease. Eur Neurol 26: 29-34.
Turkka JT & Myllylä VV (1987) Sweating dysfunction in Parkinson’s disease. Eur Neurol 26, 1-7. Turkka JT, Suominen K, Tolonen U, Sotaniemi KA, Myllylä VV (1997) Selegiline diminishes
cardiovascular autonomic responses in Parkinson’s disease. Neurology 48: 662-667. Turkka JT, Tolonen U & Myllylä VV (1987b) Cardiovascular reflexes in Parkinson’s disease. Eur
Neurol 26: 104-112. Ugedo L, Grenhoff J & Svensson TH (1989) Ritanserin, a 5-HT2 receptor antagonist, activates
midbrain dopamine neurons by blocking serotonergic inhibition. Psychopharmacology 98: 45-50.
Uitti RJ, Ahlskog JE, Maragamore DM, Muenter MD, Atkinson EJ, Cha RH & O’Brien PC (1993) Levodopa therapy and survival in idiopathic Parkinson’s disease: Olmstead County Project. Neurology 43: 1918-1926.
Uncini A, Pullman SL, Lovelace RE & Gambi D (1988) The sympathetic skin response: normal values, elucidation of afferent components and application limits. J Neurol Sci 87: 299-306.
Utley JD & Carlsson A (1965) Relative effects of L-dopa and its methyl ester given orally or intraperitoneally to reserpine-treated mice. Acta Pharmacol Toxicol (Copenh) 23: 189-193.
Van Dijk JG, Haan J, Koenderink M & Roos RAC (1991) Autonomic nervous function in progressive supranuclear palsy. Arch Neurol 48: 1083-1084.
Van Dijk JG, Haan J, Zwinderman K, Kremer B, van Hilten BJ & Roos RAC (1993) Autonomic nervous system dysfunction in Parkinson’s disease: Relationship with age, medication, duration, and severity. J Neurol Neurosurg Psychiatry 56: 1090-1095.
Van Zwieten PA (1999) Adrenergic and cholinergic receptors. In: Mathias CJ & Bannister R (eds) Autonomic Failure: A Textbook of Clinical Disorders of the Autonomic Nervous System, 4th ed. Oxford University Press, New York, p 56-62.
87
Vieregge P, Schiffke KA, Friedrich HJ, Muller B & Ludin HP (1992) Parkinson’s disease in twins. Neurology 42: 1453-1461.
Vila E, Badia A, Jane F (1985) Effects of bromocriptine on catecholamine receptors mediating cardiovascular responses in the pithed rat. J Auton Pharmcol 5: 125-130.
Vita G, Fazio MC, Milone S, Blandino A, Salvi L & Messina C (1993) Cardiovascular autonomic dysfunction in multiple sclerosis is likely related to brainstem lesions. J Neurol Sci 120. 82-86.
Wakabayashi K & Takahashi H (1997) Neuropathology of autonomic nervous system in Parkinson’s disease. Eur Neurol 38 (Suppl. 2): S2-7.
Wakabayashi K, Takahashi H, Takeda S, Ohama E & Ikuta F (1988) Parkinson’s disease: The presence of Lewy bodies in the Auerbach’s and Meissner’s plexuses. Acta Neuropathol 76: 217-221.
Wallin BG & Elam M (1993) Microneurography and autonomic dysfunction. In: Low PA (ed) Clinical Autonomic Disorders: Evaluation and Management. Little, Brown and company, Boston, p 243-252.
Wang SJ, Fuh JL, Shan DE, Liao KK, Lin KP, Tsai CP & Wu ZA (1993) Sympathetic skin response and R-R interval variation in Parkinson’s disease. Mov Disord 2: 151-157.
Wang SJ, Liao KK, Liou HH, Lee SS, Tsai CP, Lin P, Kao KP & Wu ZA (1994) Sympathetic skin response and R-R interval variation in chronic uremic patients. Muscle Nerve 17: 411-418.
Watahiki Y, Baba, M, Matsunaga M, Takebe K & Onuma T (1989) Sympathetic skin response in diabetic neuropathy. Electromyogr Clin Neurophysiol 29: 155-159.
Watts RL (1997) The role of dopamine agonists in early Parkinson’s disease. Neurology 49(Suppl.): S34-S48.
Wheeler T & Watkins PH (1973) Cardiac denervation in diabetes. BMJ 4: 584-586. Weiner N (1985) Atropine, scopolamine, and related antimuscarinic drugs. In: Goodman Gilman A,
Goodman LS, Rall TW, Murad F (eds) Goodman and Gilman’s: The Pharmacological Basis of Therapeutics 7th ed. Macmillan Publishing Company, New York, p 130-144.
Wieling W & Karemaker JM (1999) Measurement of heart rate and blood pressure to evaluate disturbances in neurocardiovascular control. In: Mathias CJ & Bannister R (eds) Autonomic Failure: A Textbook of Clinical Disorders of the Autonomic Nervous System. 4th ed. Oxford University Press, New York, p 196-210.
Wieling W, van Brederode JF, de Rijk LG, Borst C & Dunning AJ (1982) Reflex control of heart rate in normal subjects in relation to age: a data base for cardial vagal neuropathy. Diabetologia 22: 163-166.
Wilcott RC (1969) Electrical stimulation of the anterior cortex and skin potential responses in cat. J Comp Physiol Psychol 69: 465-472.
Willette RN, Punnen S, Krieger AJ & Sapru HN (1984) Interdependence of rostral and caudal ventrolateral medullary areas in the control of blood pressure. Brain Res 321: 169-174.
Wood NV (1998) Genetic risk factors in Parkinson’s disease. Ann Neurol 44(Suppl.1): S58-62. Yokota T, Hayashi M, Tanabe H & Tsukagoshi H (1993) Sympathetic skin response in patients
with cerebellar degeneration. Arch Neurol 50: 422-427. Yokota T, Matsunaga T, Okiyama R, Hirose K, Tanabe H, Furukawa T & Tsukagoshi H (1991)
Sympathetic skin response in patients with multiple sclerosis compared with patients with spinal cord transection and normal controls. Brain 114: 1381-1394.
Yoshita M (1998) Differentiation of idiopathic Parkinson’s disease from striatonigral degeneration and progressive supranuclear palsy using iodine-123 metaiodobenzylguanidine myocardial scintigraphy. J Neurol Sci 155: 60-67.
Zhang Z-X & Román GC (1993) Worldwide occurrence of Parkinson’s disease: an updated review. Neuroepidemiology 12: 195-208.