autistic spectrum disorders - foi.nhsgrampian.org · web viewguidance on use of school age...
TRANSCRIPT

Combined Child Health Service
Autistic Spectrum Disorders
Diagnostic & Patient Care Pathways
Diagnosis to School Leaver
November 2008

Combined Child Health Service
Table of Contents
Pathway 1........................................................................................................1Pre – School Children - Diagnostic Pathway....................................1Guidance on use of Pre-School Diagnostic Patient Pathway..........2
Universal Child Health Screening...............................................2Recognition of Child’s Difficulties................................................2Clinical Assessment....................................................................3Referral to Child Development Service.......................................4Diagnostic Assessment...............................................................6Multi-Agency Case Conference..................................................6
Pathway 2........................................................................................................7Pre- School Children - Patient Care Pathway....................................7Guidance on use of Pre-School Patient Care Pathway....................8
Diagnosis of Autistic Spectrum Disorder.....................................8Information for Parents................................................................8Social Work...............................................................................10Education..................................................................................10Health........................................................................................11Personal Child Health Records (PCHR)...................................11Voluntary Agencies...................................................................11Joint Assessment of Needs / Integrated Assessment...............11Individual Educational Plan / Co-ordinated Support Plan..........12Key worker................................................................................12Regular Review.........................................................................12
Pathway 3......................................................................................................13School Age Children - Diagnostic Pathway....................................13Guidance on use of School Age Diagnostic Patient Pathway.......14
Universal Child Health Screening.............................................14Recognition of Child’s Difficulties..............................................14Clinical Assessment..................................................................15Referral to Child Development Service.....................................17Child and Family Mental Health Service...................................19Diagnostic Assessment.............................................................21Multi-Agency Case Conference................................................21
Pathway 4......................................................................................................22School Aged Children - Patient Care Pathway................................22Guidance on use of School Age Patient Care Pathway.................23
November 2008

Combined Child Health Service
Diagnosis of Autistic Spectrum Disorder...................................23Information for Parents..............................................................23Social Work...............................................................................26Health........................................................................................26Education..................................................................................26Joint Assessment of Needs / Integrated Assessment...............27Individual Educational Plan / Co-ordinated Support Plan..........27Voluntary Agencies...................................................................28Key worker................................................................................28Regular Review.........................................................................28
Annex 1...............................................................................................29THE CHAT assessment form....................................................29
Annex 2...............................................................................................31ICD-10 / DSM-IV Classification System....................................31
Documents used in the production of pathways............................35References:........................................................................................35Working Group Members.....................................................................36
November 2008

Combined Child Health Service
Pathway 1 Pre – School Children - Diagnostic Pathway
November 2008 1
Recognition of Childs DifficultiesParents, Health Visitor, General Practitioner, Nursery Staff
(Professionals listen to parents concerns)
Clinical AssessmentHealth Visitor/General Practitioner
No significant evidence of ASD(but concerns remain)
Diagnosis of ASD being considered
Follow Up with Health VisitorLiaise with Nursery, Social Work (if involved with family). Consider referral for speech & Language therapy
Refer to Child Development ServicesLiaise with Health Visitor, Nursery, Social Work, Allied Health Professionals e.g. Speech & Language, Occupational Therapist
Follow Up with Child Development Services
Liaise with Health Visitor, Nursery, Social Work, Allied Health Professionals, Educational Psychologist
Discharge
Diagnostic AssessmentMulti-disciplinary, Multi-agencyMedical AssessmentSpeech and Language AssessmentEducational AssessmentInvolvement of Social Work DepartmentConsider Mental Health Assessment and/or Autism Specific AssessmentIf indicated Occupational Therapy and Physiotherapy Assessment
Multi-Agency Case Conference
Diagnosis of ASD
Discharge
Follow Up with Child Development Services
(as above)and/or
Mental Health Service
Diagnosis of ASD not confirmed
FollowPatient Care
Pathway

Combined Child Health Service
Guidance on use of Pre-School Diagnostic Patient Pathway
Universal Child Health ScreeningThe early identification of a child requiring an assessment for health problems and developmental disorders is the aim of the child health screening and surveillance programmes. Health for all Children (Hall 4) has led to a significant change in screening and surveillance in Scotland.
Hall 4 states: -Every child and parent should have access to a universal or core programme of preventative pre-school care.Formal screening should be confined to the evidence based programmes agreed by the National Screening Committee.Health professionals must respond promptly to parental concerns.Formal universal screening for speech and language delay, global developmental delay and autism is not recommended.
Scottish Executive 2005
Early identification, early therapeutic and educational intervention, and seamless delivery of services may help a child to maximise their potential. A key aim is to minimise the delay between the initial concerns of parents, a diagnosis being made and provision of appropriate interventions and support.
Recognition of Child’s DifficultiesConcerns raised by parents should be taken seriously and responded to appropriately in all cases. Parents may say that their child is different from others of a similar age but are unable to give a clear explanation of the differences. Behaviours that may lead to concerns being raised about a child can include, failure to smile or lack of response to others smiling, slow to develop speech, loss of speech and/or language skills, does not initiate play with peers, aggression, repetitive and obsessive behaviours, inability to cope with change and appear to be “in a world of their own” Health professionals should be aware that the absence of normal development, or delayed development is as important as the presence of abnormal development in a child. Health Visitors, General Practitioner or nursery staff may have concerns about a child that the parents have not expressed, these concerns should be discussed with the parents in a sensitive manner.
November 2008 2

Combined Child Health Service
Clinical Assessment“The primary aim of clinical assessment is to examine the profile of skills and impairments of the child concerned in order to identify their specific needs. Parents or other carers are partners with the professionals in this process”
Judith Gould, 2003 (NAPC 2003)
The universal core programme for child health surveillance has an important role in the early detection of problems and includes enabling health professionals to identify children who require further assessment for autistic spectrum disorder (ASD)The use of a screening tool such as, the Checklist for Autism in Toddlers (CHAT) or the modified CHAT (M-CHAT) can be useful when considering relevant clinical features identified during an assessment. ( see Annex 1) Observation of the child for the triad of impairments should be incorporated in a developmental assessment, these are: - Social interaction, Social communication and Social imagination. SIGN guidelines have listed features, which should alert health professionals to the possibility of ASD: -
Delay or absence of spoken language Looks through people; not aware of others Not responsive other peoples facial expression/feelings Lack of pretend play; little or no imagination Does not show typical interest in or play near peers purposefully Lack of turn-taking Unable to share pleasure Qualitative impairment in non-verbal communication Does not point at an object to direct person to look at it Lack of gaze monitoring Lack of initiation of activity or social play Unusual or repetitive hand and finger mannerisms Unusual reaction, or lack of reaction, to sensory play
If after carrying out a clinical assessment, health professionals do not suspect ASD but concerns remain regular follow up by health visitor is recommended, with liaison between nursery, Allied Health Professionals and social work as required. The child can be referred to the Child Development Service at any stage for further advice.If diagnosis of ASD is being considered, the child should be referred to the Child Development Service for further assessment.
November 2008 3

Combined Child Health Service
Referral to Child Development ServiceThe Child Development Service is available at local clinics throughout Grampian and can be accessed by referral to:-
Community Child Health DepartmentRoyal Aberdeen Children’s Hospital
Westburn RoadAberdeenAB25 2ZG
Raeden Centre or Dr A LiebenbergMidstocket Road Ward 2Aberdeen Dr Gray’s HospitalAB15 5PD Pluscarden Road
ElginIV30 1SN
On referral, an initial assessment of the child will be arranged, including:- Pre-natal, perinatal and developmental history up to age of child at
assessment. Any social and emotional factors should be included along with evidence of any problems at home, pre-school or other social occasions.
Family history including evidence of any learning disability, speech and language problems, developmental neurological problems, psychiatric disorders, autistic spectrum disorder
Description of family and extended family members (genogram would be useful), include any family problems (parental separation/divorce, death) as this may have an affect the child’s behaviour
Description of the current problems experienced by child, parents, health visitor, early years workers
Physical and neurodevelopment examination Observation and assessment of behaviour, social and communication
skills. Observations may need to be made in areas out with the clinical setting such as home and nursery. This allows for a more comprehensive assessment. Information on how the child is functioning at home/nursery should be obtained from as many varied sources as possible.
An audiological examination may be required to exclude any underlying hearing deficit.
If after the initial assessment a diagnostic assessment is not recommended, ongoing reviews may be offered either through Child Development Services or Health Visitor. Liaison with health visitor, social work, nursery, Allied Health Professionals and educational psychology may be required to ensure the child’s care and social needs are being met.
November 2008 4

Combined Child Health Service
Referral for a multi-disciplinary, multi-agency diagnostic assessment may be offered at a later date if indicated.
After carrying out a full clinical history and assessment, if ASD is suspected the child will be referred for a multi-disciplinary, multi-agency diagnostic assessment. Parents should be informed prior to referral of its nature and purpose, to clarify the child’s difficulties and diagnosis and how best to help with their progress.
November 2008 5

Combined Child Health Service
Diagnostic AssessmentSIGN guidelines recommend that the International Classification of Diseases, version 10 (ICD-10) or the Diagnostic and Statistical Manual of Mental Disorders 4th edition (DSM-IV) classification system should be used in diagnosing ASD in children. (see Annex 2)
Undertaking a diagnostic assessment involves collecting and recording information about the development, health, education and care needs of the child and their family. Due to the assessments comprehensive nature it may take place over a period of time.
Autism Specific Assessment generally involves a number of agencies, including education and social work. This involves:-
taking a full clinical history, with detailed developmental history medical assessment; physical and neurological examination Speech and Language assessment: evaluation of speech and
language and communication skills. Occupational therapy and/or physiotherapy assessment may be
considered Specific mental health assessment may be considered Educational assessment (generally from 2 years old)
Educational Psychologists can provide key observational information Social care assessment if appropriate
Direct observation of the child in a variety of settings is recommended to help assess the current functioning level of communication, emotional development, social relationships and adaptive behaviour. Use of an ASD specific diagnostic tool may be used.
Multi-Agency Case ConferenceA multi-agency case conference involving the parents, child (if appropriate) and all relevant professionals will take place to discuss and explain the outcome of the diagnostic assessment, with the diagnosis of ASD being made explicit at this time. If ASD is not suspected a further opinion may be sought if indicated.
November 2008 6

Combined Child Health Service
Pathway 2 Pre- School Children - Patient Care Pathway
November 2008 7
Diagnosis of Autistic Spectrum Disorder
HealthDevelopmental review thorough Child Development ServicesInvolvement of other health professionals e.g. Allied health professional servicesMental Health Services
Joint Assessment of Need
EducationIdentify any Additional Support for Learning Needs.
Social WorkIdentify any Social care and Support Needs for the family.Respite care
Integrated Assessment Framework Action Plan
Key Worker Appointed(Not yet implemented)
+/- Individual Education Plan/ Coordinated Support Plan
Regular review and reassessment of needs by various professionals involved
Mainsteam NurseryDevelopmental Nursery
VoluntaryAgencies (if required)
Consider Autism specific assessments

Combined Child Health Service
Guidance on use of Pre-School Patient Care Pathway
Diagnosis of Autistic Spectrum DisorderAutistic Spectrum Disorder is a complex, lifelong developmental condition that affects individuals to different degrees, some with severe communication and social interaction difficulties, whilst others may be skilled in their use of language but still have a range of complex needs regarding social interaction and understanding the motivation of others. (Scottish Society for Autism 2006)Autistic Spectrum Disorder is more common in boys than in girls and is prevalent in all nationalities and social classes. There is no clear single underlying cause although research increasingly points to a genetic factor.
Information for ParentsParents of children diagnosed with Autistic Spectrum Disorder will require clear written and verbal information about the condition. The information should be appropriate to the child’s age, ability and include short and long term plans. Consideration should be given to informing parents that there is an increased risk of ASD in siblings of affected children. Information for parents and carers with a child or young person recently diagnosed with an autistic spectrum disorder (2006) The NHS Education for Scotland developed an information booklet, to provide information to help the family immediately after diagnosis. The booklet is available to download from: www.scottishautismnetwork.org.uk Next Steps (2006)Next Steps is an information resource produced by The National Autistic Society Scotland, to provide information and support to those who have been diagnosed with ASD their family and carers. The resource contains a directory of local services available for children, young people and their families to enable them to easily source and access relevant support. The resource manual is available to download from: www.autism.org.uk. Parents should be provided with information about training opportunities that are available to them, such as The National Autistic Society Early Bird programme.
Early Bird ProgrammeThe National Autistic Society Early Bird programme is a three month parent training programme for children under 4 years of age with Autistic Spectrum Disorder. Training involves group workshops and individual home visits, with video recording feedback. The aim of the programme is to:-
support parents between diagnosis and education to empower parents and help them with their child’s social communication
and appropriate behaviour in the home setting. to help them establish good practice in handling their child and pre-empt
inappropriate behaviour.The programme helps parents understand their child’s autism and have the opportunity to share issues with other families.
November 2008 8

Combined Child Health Service
Providing further information on local support groups and other national and local resources available will help empower parents in the care of their child. Further sources of information include:-
Grampian Autistic Society The Scottish Society for Autism33-35 Carnie Drive Hilton House Aberdeen Alloa Business ParkAB25 3AN Whins RoadTel: 01224 277900 AlloaEmail: [email protected] FK10 3SAWebsite: Under construction Website:www.autism-in-scotland.org.uk National Autistic Society Scotland The National AutisticSocietyCentral Chambers 393 City Road109 Hope Street LondonGlasgow EC1V 1NGG2 6LL Website: www.nas.org.uk Website: www.autism.org.uk
Contact a Family VSA Carers CentreCraigmillar Social Enterprise & Arts centre 24-28 Belmont Street11/9 Harewood Road AberdeenEdinburgh AB10 1JHEH16 4 NT Tel: 01224 646677Tel: 0131 659 2930 Website: www.vsa.org.uk Website: www.cafamily.org.uk
Aberdeenshire Autism Support Group (to become Aberdeenshire branch of NAS)Susan Kay 2 Broadstraik CrescentWesthill AberdeenshireTel: 01224 743475Email: [email protected]
November 2008 9

Combined Child Health Service
Social WorkAn assessment of need may be carried out to determine what support and services are required by the child and their family. This may include respite care, play schemes for child or siblings and details of available financial assistance.
EducationThe Health Service may identify a child as appearing to have additional support needs arising from a disability within the meaning of the Disability Discrimination Act 1995, and bring this child to the attention of the education authority.
The educational authority will decide whether to assess the child to find out if they have additional support needs and will determine what support is required.The educational authority in partnership with the parents will decide if the child attends a mainstream nursery school or a developmental nursery or combination. The Educational Psychologists work collaboratively with parents, nurseries, medical colleagues and other agencies in diagnosis and planned intervention.All 3 and 4 year olds in Scotland are entitled to a funded part time pre-school education placement.
The Education (Additional Support for Learning) (Scotland) Act 2004 (ASL Act) introduced a new framework for providing support to children and young people who require additional help with their learning. The education authority may then, at its discretion, establish whether the child has additional support needs arising from a disability under its arrangements for identifying and providing for children with additional support needs.The Additional Support for Learning Act requires an educational authority to provide additional support to certain disabled pre-school children in their area who are under 3 years old. Once it is established by the educational authority the child has additional support needs, the authority would then have a duty to provide suitable provision to meet those needs.
The ASL Act aims to ensure that all children and young people are provided with the necessary support to help them work towards achieving their full potential. The ASL Act also promotes collaborative working among all agencies involved with supporting children.
November 2008 10

Combined Child Health Service
HealthA developmental review through Child Development Services involving other health professionals may be required to assess and manage developmental, medical and co-morbid problems.
Personal Child Health Records (PCHR) Personal Child Health Records were introduced to facilitate partnership with parents and to empower them in overseeing their child’s development and health care. It is important that health professionals use this record to allow parents to have available written information about their child’s health and development. Information on diagnosis and how to access appropriate information and support can also be recorded in the Personal Child Health Records.
Voluntary AgenciesAn Autism specific assessment of support needs by a voluntary agency e.g. Grampian Autistic Society may be useful depending on the complexity of the child’s difficulties or circumstances.
Joint Assessment of Needs / Integrated Assessment Joint assessment of needs is a co-ordinated Multi-Agency approach to gathering information and aims to avoid parents having to repeat information more than once, giving a holistic view of the child within their family and community enabling assessment of medical, social and educational needs.
Action plans are developed using the systematic assessment and analysis of the information obtained about the child. The child and their family may participate in the development of the action plan. An action plan records the needs and the professional responses and responsibilities to the child, outlining the basis for providing support, services and resources to meet the needs of the child.
An action plan should state:
what action should be taken by whom to improve the child’s circumstances
the reasons for the plan
timescales
intended outcome and future review date
The plan should be as simple as necessary and relevant to the child's needs. It should be updated or amended as needs change.
November 2008 11
Combined Child Health Service
Individual Educational Plan / Co-ordinated Support PlanAn Individual Educational Plan (IEP) describes in detail the nature of the child’s additional support needs, the ways in which these are to be met, the learning outcomes to be achieved, and specifies what additional support is required, including that required from agencies outwith education. The IEP should be reviewed and updated regularly, involving the parents and child (where possible).
A Co-ordinated support plan is prepared for children who: need support due to complex or multiple factors that have a significant
adverse affect on their education require significant involvement from one or more additional agencies
such as health and social work will need support for more than a year
The aim of a co-ordinated support plan is to ensure that the various professionals and agencies involved in providing support are working together and that the support is co-ordinated.
A Co-ordinated support plan: is an action plan for children who require significant additional support
with their education supports partnership working to help children achieve educational
targets is monitored and reviewed regularly involves the child, their family, education and additional agencies
(Enquire, 2007)
Key workerA key worker is a named person who works in partnership with the family and can provide a link between professionals and agencies involved in the child’s care. Key workers can co-ordinate access to, and delivery of services required from various agencies.
Regular Review
The child will have regular reviews carried out by the various professionals and agencies involved in their care. Their needs will be reassessed and plans updated as required.
November 2008 12

Combined Child Health Service
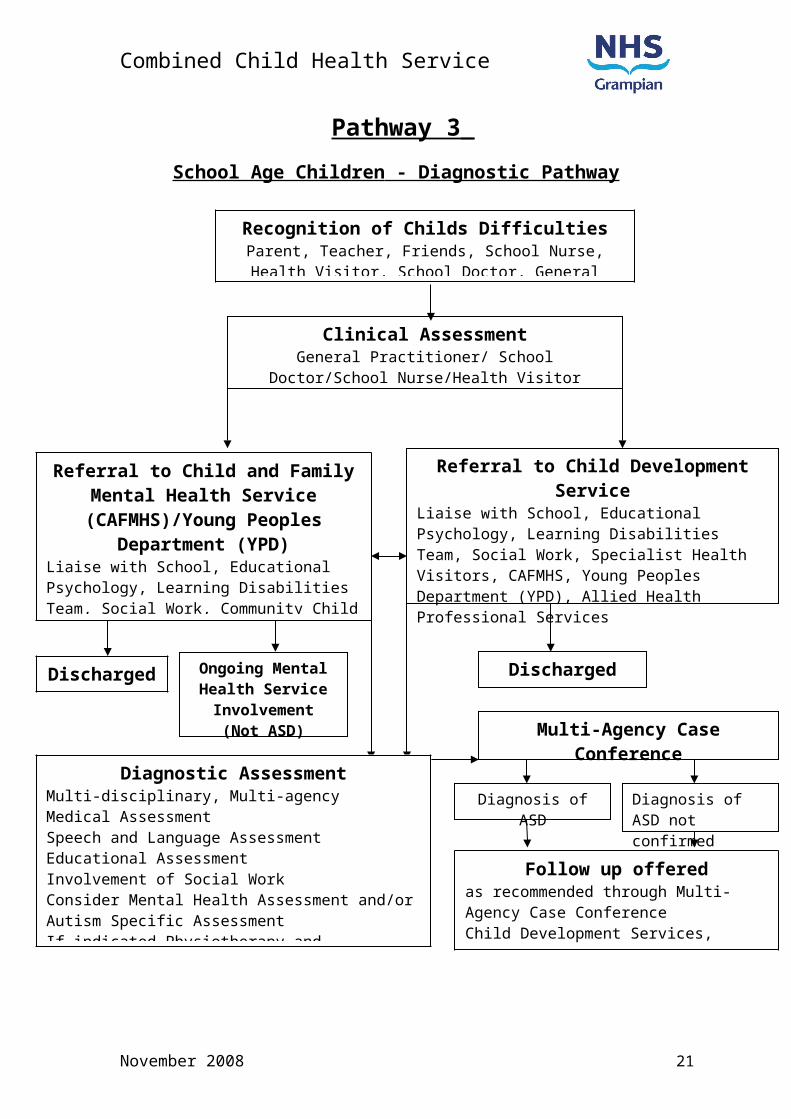
Pathway 3 School Age Children - Diagnostic Pathway
November 2008 13
Referral to Child Development ServiceLiaise with School, Educational Psychology, Learning Disabilities Team, Social Work, Specialist Health Visitors, CAFMHS, Young Peoples Department (YPD), Allied Health Professional Services
Ongoing Mental Health Service Involvement
(Not ASD)
Discharged
Multi-Agency Case Conference
Clinical AssessmentGeneral Practitioner/ School Doctor/School
Nurse/Health Visitor
Diagnosis of ASD Diagnosis of ASD not confirmed
Referral to Child and Family Mental Health Service (CAFMHS)/Young
Peoples Department (YPD)Liaise with School, Educational Psychology, Learning Disabilities Team, Social Work, Community Child Health Department (School Health Service), Specialist Health Visitors, Allied Health Professional Services
Diagnostic AssessmentMulti-disciplinary, Multi-agencyMedical AssessmentSpeech and Language AssessmentEducational AssessmentInvolvement of Social WorkConsider Mental Health Assessment and/or Autism Specific AssessmentIf indicated Physiotherapy and Occupational Therapy Assessment
Discharged
Follow up offeredas recommended through Multi-Agency Case ConferenceChild Development Services, Mental Health Services (CAFMHS/YPD)
Recognition of Childs DifficultiesParent, Teacher, Friends, School Nurse, Health Visitor,
School Doctor, General Practitioner

Combined Child Health Service
Guidance on use of School Age Diagnostic Patient Pathway
Universal Child Health ScreeningThe early identification of a child requiring an assessment for health problems and developmental disorders is the aim of the child health screening and surveillance programmes. Health for all Children (Hall 4) has led to a significant change in screening and surveillance in Scotland. All children receive a health check when starting primary school, with little formal child health surveillance after that. In school age children detection of problems should be part of mainstream school life.
Hall 4 states: -Formal screening should be confined to the evidence based programmes agreed by the National Screening Committee.Health professionals must respond promptly to parental concerns.Formal universal screening for speech and language delay, global developmental delay and autism is not recommended.Children starting school should receive the agreed screening programmes.Health care of school-age children should include support for children with problems and special needs.
Scottish Executive 2005
Early identification, early therapeutic and educational intervention, and seamless delivery of services may help a child to maximise their potential. A key aim is to minimise the delay between the initial concerns of parents, a diagnosis being made and provision of appropriate interventions and support.
Recognition of Child’s DifficultiesConcerns raised by parents should be taken seriously and responded to appropriately in all cases. Parents may say that their child is different from others of a similar age but are unable to give a clear explanation of the differences. Behaviours that may lead to concerns being raised about a child can include, loss of speech and/or language skills, inappropriate reaction to teacher’s instructions, school refusal, poor concentration, does not initiate play with peers, aggression, repetitive and obsessive behaviours, inability to cope with change and appear to be “in a world of their own”. Times of change or transition between schools or other services are periods when difficulties can be recognised, this can include first years of primary school, move to secondary school or in adolescence.Health professionals should be aware that the absence of normal development, or delayed development is as important as the presence of abnormal development in a child. General Practitioner, school doctor, school nurse or school teacher may have concerns about a child that the parents have not expressed, these concerns should be discussed with the parents.
November 2008 14

Combined Child Health Service
Clinical Assessment“The primary aim of clinical assessment is to examine the profile of skills and impairments of the child concerned in order to identify their specific needs. Parents or other carers are partners with the professionals in this process”
Judith Gould, 2003 (NAPC 2003)
The universal core programme for child health surveillance involves partnership working between children, parents and health professionals and may assist in the early recognition of Autistic Spectrum Disorder (ASD)Observation of the child for the triad of impairments should be incorporated in a developmental assessment, these are: - Social interaction, Social communication and Social imagination.
SIGN guidelines have listed features, which should alert health professionals to the possibility of ASD in school aged children:-
Communication impairment abnormalities in language development including muteness odd or inappropriate prosody persistent echolalia referral of self as “you” or “he” beyond three years unusual vocabulary for child’s age/social group limited use of language for communication and/or tendency to talk
freely only about specific topics
Social impairment inability to join in play of other children or inappropriate attempts at joint
play (may manifest as aggressive or disruptive behaviour) lack of awareness of classroom “norms” (criticising teachers, overt
unwillingness to cooperate in classroom activities, inability to appreciate or follow current trends)
easily overwhelmed by social or other stimulation failure to relate normally to adults (too intense/no relationship) showing extreme reactions to invasion of personal space and
resistance to being hurried
Impairments of interest, activities and/or behaviours lack of flexible cooperative imaginative play/creativity difficulty in organising self in relation to unstructured space ( hugging
the perimeter of playgrounds and halls) inability to cope with change or unstructured situations, even ones that
other children enjoy (school trips, teacher away etc)
Other factors unusual profile of skills/deficits any other evidence of odd behaviours including unusual responses to
sensory stimuli
November 2008 15

Combined Child Health Service
SIGN guidelines have also listed features, which should alert health professionals to the possibility of ASD in adolescents:-General Picture
long standing difficulty in social behaviours, communication and coping with change, which are obvious at times of transition (change of school, leaving school)
significant discrepancy between academic ability and “social” intelligence, most difficulties in unstructured social situations (in school, work breaks)
socially “naïve”, lack common sense, not as independent as peers
Language, non-verbal skills and social communication problems with communication, even if wide vocabulary and normal use
of grammar. May be unduly quiet, may talk at others rather than hold a to and fro conversation, or may provide excessive information on topics of own interest
unable to adapt style of communication to social situations, may sound like “a little professor” (overly formal), or be inappropriately familiar
may have speech peculiarities including “flat”, unmodulated speech, repetitiveness, use of stereotyped phrases
may take things literally and fail to understand sarcasm or metaphor unusual use of timing of non-verbal interaction (eye contact, gesture
and facial expression)
Social problems difficulty making and maintaining peer friendships, though may find it
easier with adults or younger children can appear unaware or uninterested in peer group “norms”, may
alienate by behaviours which transgress “unwritten rules” may lack awareness of personal space, or be intolerant of intrusions
on own space
Rigidity in thinking and behaviour preference of highly specific, narrow interests or hobbies, or may enjoy
collecting, numbering or listing strong preferences for familiar routines, may have repetitive behaviours
or intrusive rituals problems using imagination (in writing, future planning) may have unusual reactions to sensory stimuli (sounds, tastes, smell,
touch, hot or cold)
If a diagnosis of ASD is being considered, the child may be referred to the Child Development Service or Mental Health Services - Child and Family Mental Health Service (CAFMHS) up to the age of 13 years, (young people with learning disabilities are seen up to school leaving age) or The Young Persons Department (YPD) from 13-18 years for further assessment. Alternatively when concerns are identified in school, an Educational Psychology consultation may clarify issues and support onward referral.
November 2008 16

Combined Child Health Service
Referral to Child Development ServiceThe Child Development Service is available at local clinics throughout Grampian and can be accessed by referral to:-
Community Child Health Department or Dr A LiebenbergRoyal Aberdeen Children’s Hospital Ward 2Westburn Road Dr Gray’s HospitalAberdeen Pluscarden RoadAB25 2ZG Elgin
IV30 1SN
On referral, an initial assessment of the child will be arranged, including:- Pre-natal, perinatal and developmental history up to age of child at
assessment. Any social and emotional factors should be included along with evidence of any problems at home, school or other social occasions.
Family history including evidence of any learning disability, speech and language problems, developmental neurological problems, psychiatric disorders, autistic spectrum disorder
Description of family and extended family members (genogram would be useful), include any family problems (parental separation/divorce, death) as this may have an affect the child’s behaviour
Description of the current problems experienced by child, parents, teacher
Physical and neurodevelopment examination Observation and assessment of behaviour, social and communication
skills. Observations may need to be made in areas out with the clinical setting such as home and school. This allows for a more comprehensive assessment. Information on how the child is functioning at home/school should be obtained from as many varied sources as possible.
An audiological examination may be required to exclude any underlying hearing deficit.
If after the initial assessment a diagnostic assessment is not recommended, ongoing reviews may be offered through Child Development Services, or the child may be discharged from Child Development Services. Liaison with specialist health visitors, social work, school, Allied Health Professionals, CAFMHS, YPD and educational psychology may be required to ensure the child’s care and social needs are being met. If comorbid mental health problems are identified during the initial assessment, the child may be referral to CAFMHS, YPD or Learning Disabilities Team for further assessment, diagnosis and management of the problems.
November 2008 17

Combined Child Health Service
Referral for a multi-disciplinary, multi-agency diagnostic assessment may be offered at a later date if indicated.After carrying out a full clinical history and assessment, if ASD is suspected the child will be referred for a multi-disciplinary, multi-agency diagnostic assessment. Parents should be informed prior to referral of its nature and purpose, to clarify the child’s difficulties and diagnosis and how best to help with their progress.
November 2008 18

Combined Child Health Service
Child and Family Mental Health ServiceChildren up to the age of 13 years may be referred directly to Child and Family Mental Health Service (CAFMHS), young people with learning disabilities may be seen up to school leaving age or young people from 13-18 years to the Young Persons Department (YPD) from Community Child Health Services or General Practitioner.
The Child and Family Mental Health Service are available throughout Grampian and can be accessed by referral to:-
Child and Family Mental Health ServiceLower Ground Floor
Royal Aberdeen Children’s HospitalWestburn Road
AberdeenAB25 2ZG
Young Persons Department Child and Family Mental Health ServiceLower Garden Villa The Rowan CentreRoyal Cornhill Hospital Maryhill Cornhill Road High StreetAberdeen ElginAB25 2ZH IV30 1AT
On referral, an initial assessment of the child will be arranged, including:- Pre-natal, perinatal and developmental history up to age of child at
assessment. Any social and emotional factors should be included along with evidence of any problems at home, school or other social occasions.
Family history including evidence of any learning disability, speech and language problems, developmental neurological problems, psychiatric disorders, autistic spectrum disorder
Description of family and extended family members (genogram would be useful), include any family problems (parental separation/divorce, death) as this may have an affect the child’s behaviour
Description of the current problems experienced by child, parents, teacher
Physical and neurodevelopment examination Observation and assessment of behaviour, social and communication
skills. Observations may need to be made in areas out with the clinical setting such as home and school. This allows for a more comprehensive assessment. Information on how the child is functioning at home/school should be obtained from as many varied sources as possible.
November 2008 19

Combined Child Health Service
If after the initial assessment a diagnostic assessment is not recommended, the child may be discharged from Child and Family Mental Health Services. Liaison with Community Child Health Department, specialist health visitors, social work, school, Allied Health Professionals, educational psychology may be required to ensure the child’s care and social needs are being met. If comorbid problems such as anxiety disorder, behavioural problems, Obsessive Compulsive disorder (OCD), depression, Attention Deficit hyperactivity Disorder (ADHD) are identified during the initial assessment, the child may have ongoing involvement with CAFMHS, YPD or Learning Disabilities Team for further assessment, diagnosis and management of the problems. Referral for a multi-disciplinary, multi-agency diagnostic assessment may be offered at a later date if indicated.
After carrying out a full clinical history and assessment, if ASD is suspected the child will be referred for a multi-disciplinary, multi-agency diagnostic assessment. Parents should be informed prior to referral of its nature and purpose, to clarify the child’s difficulties and diagnosis and how best to help with their progress.
November 2008 20
Combined Child Health Service
Diagnostic AssessmentSIGN guidelines recommend that the International Classification of Diseases, version 10 (ICD-10) or the Diagnostic and Statistical Manual of Mental Disorders 4th edition (DSM-IV) classification system should be used in diagnosing ASD in children. (See annex 2)
Undertaking a diagnostic assessment involves collecting and recording information about the development, health, education and care needs of the child and their family. Due to the assessments comprehensive nature it may take place over a period of time.
Autism Specific Assessment generally involves a number of agencies, including education and social work. This involves:-
taking a full clinical history, with detailed developmental history medical assessment; physical and neurological examination Speech and Language assessment: evaluation of speech and
language and communication skills. assessment of functioning within the school cognitive assessment may be considered to assess child’s intellectual
development Occupational therapy and/or physiotherapy assessment may be
considered specific mental health assessment may be considered Educational assessment
Educational Psychologists (through their consultation model) can provide information that is key to helpful intervention.
Social care assessment if appropriate
Direct observation of the child in a variety of settings is recommended to help assess the current functioning level of communication, emotional development, social relationships and adaptive behaviour. An ASD specific diagnostic tool may be used.
Multi-Agency Case ConferenceA multi-agency case conference involving the parents, child (if appropriate) and all relevant professionals will take place to discuss and explain the outcome of the diagnostic assessment, with the diagnosis of ASD being made explicit at this time. If ASD is not confirmed a further opinion may be sought if indicated.
November 2008 21

Combined Child Health Service
Pathway 4
School Aged Children - Patient Care Pathway
November 2008 22
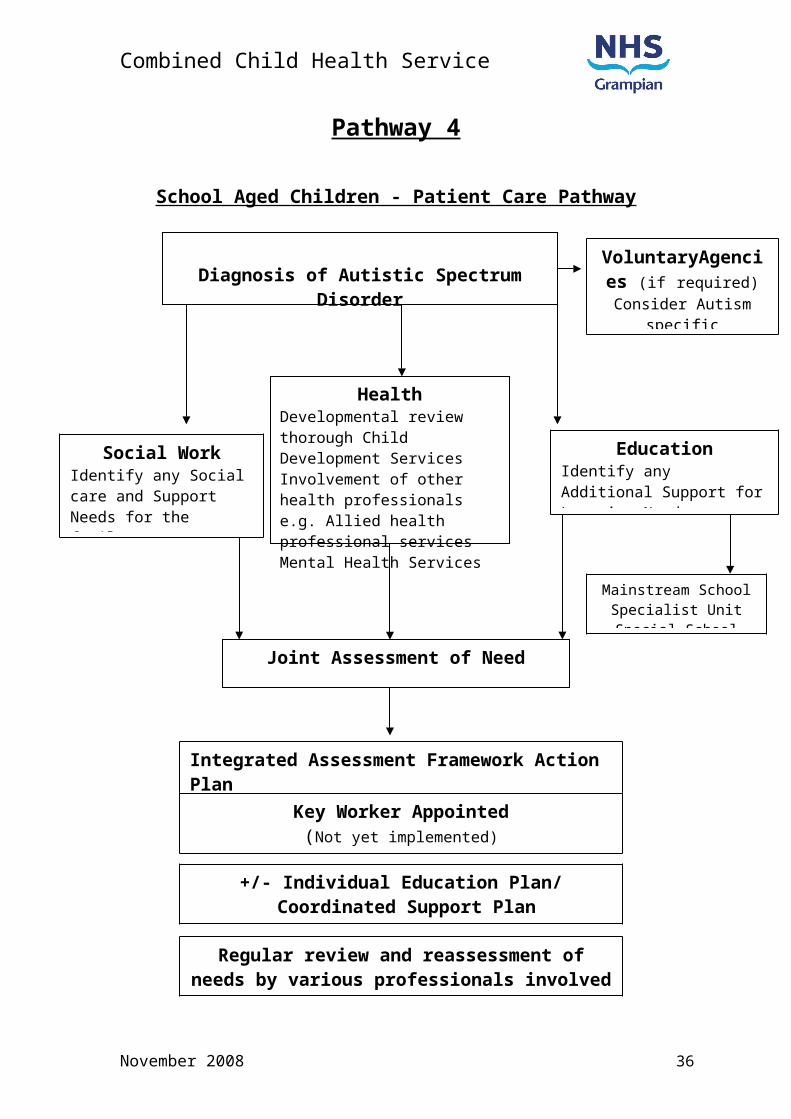
Diagnosis of Autistic Spectrum Disorder
HealthDevelopmental review thorough Child Development ServicesInvolvement of other health professionals e.g. Allied health professional servicesMental Health Services
Joint Assessment of Need
EducationIdentify any Additional Support for Learning Needs.
Social WorkIdentify any Social care and Support Needs for the family.Respite care
Integrated Assessment Framework Action Plan
Key Worker Appointed (Not yet implemented)
+/- Individual Education Plan/ Coordinated Support Plan
Regular review and reassessment of needs by various professionals involved
VoluntaryAgencies (if required)
Consider Autism specific assessments
Mainstream SchoolSpecialist UnitSpecial School

Combined Child Health Service
Guidance on use of School Age Patient Care Pathway
Diagnosis of Autistic Spectrum DisorderAutistic Spectrum Disorder is a complex, lifelong developmental condition that affects individuals to different degrees, some with severe communication and social interaction difficulties, whilst others may be skilled in their use of language but still have a range of complex needs regarding social interaction and understanding the motivation of others. (Scottish Society for Autism, 2006)Autistic Spectrum Disorder is more common in boys than in girls and is prevalent in all nationalities and social classes. There is no clear single underlying cause although research increasingly points to a genetic factor.
Information for ParentsParents of children diagnosed with an Autistic Spectrum Disorder (ASD) will require clear written and verbal information about the condition. The information should be appropriate to the child’s age, ability and include short and long term plans. Consideration should be taken on informing parents that there is an increased risk of ASD in siblings of affected children.
Information for parents and carers with a child or young person recently diagnosed with an autistic spectrum disorder (2006) The NHS Education for Scotland developed an information booklet, to provide information to help the family immediately after diagnosis. The booklet is available to download from: www.scottishautismnetwork.org.uk
Next Steps (2006)Next Steps is an information resource produced by The National Autistic Society Scotland, to provide information and support to those who have been diagnosed with ASD their family and carers. The resource contains a directory of local services available for children, young people and their families to enable them to easily source and access relevant support. The resource manual is available to download from: www.autism.org.uk.
Parents should be provided with information about training opportunities that are available to them, such as The National Autistic Society Early Bird Plus programme and help! Programme.
Early Bird Plus ProgrammeThe National Autistic Society Early Bird Plus programme is a three month training programme for parents and professionals of children aged 4-8 years with an Autistic Spectrum Disorder. The Early Bird Plus programme addresses the child’s needs at home and at school. Training involves eight group workshops and two individual home visits. The aim of the programme is to:-
to empower parents and help them with their child’s social communication and appropriate behaviour.
to help them establish good practice in handling their child and pre-empt inappropriate behaviour.
November 2008 23

Combined Child Health Service
to encourage a consistent approach between home and school by training parents and professionals together
improve communication between parent and child
help! Programme The National Autistic Society help! programme offers information and support for parents and carers of school age children 5-11years old, young people 11-16 years old and adults, who have been diagnosed with ASD in the last 12-18 months. There are different types of programmes available, these include the 20 hour, 1day or 2day programmes, consisting of presentations, group discussions, DVD material and a help! parent manual. The aim of the programme is to:-
to develop knowledge and understanding of ASD provide positive management strategies provide information on local support services
These programmes help parents understand their child’s autism and have the opportunity to share issues with other families.
Providing further information on local support groups and other national and local resources available will help empower parents in the care of their child.Further sources of information include:-
Grampian Autistic Society National Autistic Society Scotland33-35 Carnie Drive Central ChambersAberdeen 109 Hope StreetAB25 3AN GlasgowTel: 01224 277900 G2 6LLEmail: [email protected] Website: www.autism.org.uk
The Scottish Society for Autism National Autistic SocietyHilton House 393 City RoadAlloa Business Park LondonWhins Road EC1V 1NGAlloa Website: www.nas.org.uk FK10 3SAWebsite: www.autism-in-scotland.org.uk
Aberdeenshire Autism Support Group(to become Aberdeenshire branch of NAS)Susan Kay 2 Broadstraik CrescentWesthill AberdeenshireTel: 01224 743475Email: [email protected]
November 2008 24

Combined Child Health Service
Contact a Family Scotland VSA Carers CentreCraigmillar Social Enterprise & Arts Centre 24-28 Belmont Street11/9 Harewood Road AberdeenEdinburgh AB10 1JHEH16 4NT Tel: 01224 646677Tel: 0131 659 2930 Website: www.vsa.org.uk Website: www.cafamily.org.uk
November 2008 25

Combined Child Health Service
Social WorkAn assessment of need may be carried out to determine what support and services are required by the child and their family. This may include family support services, mainstream or specialist childcare, respite care, leisure and recreational facilities and details of available financial assistance.
HealthChildren and young people with ASD may also have medical or emotional problems and require access to the same health care as other children.A developmental review through Child Development Services involving other health professionals may be required to assess and manage developmental,medical and mental health problems.
EducationThe Health Service may identify a child as appearing to have additional support needs arising from a disability and bring this child to the attention of the education authority.
The educational authority will decide whether to assess the child to find out if they have additional support needs and will determine what support is required.The educational authority in partnership with the parents will decide if the child attends a mainstream school, a specialist unit attached to a mainstream school or a special school.The Educational Psychologists work collaboratively with parents, schools, medical colleagues and other agencies in diagnosis and planned intervention.
The Education (Additional Support for Learning) (Scotland) Act 2004 (ASL Act) introduced a new framework, based on the idea of additional support needs, to provide for children and young people who require additional help with their learning. The education authority may then, at its discretion, establish whether the child has additional support needs arising from a disability under its arrangements for identifying and providing for children with additional support needs. Once it is established by the educational authority the child has additional support needs, the authority would then have a duty to provide suitable provision to meet those needs.
The ASL Act aims to ensure that all children and young people are provided with the necessary support to help them work towards achieving their full potential.The ASL Act also promotes collaborative working among all agencies involved with supporting children.
November 2008 26
Combined Child Health Service
Joint Assessment of Needs / Integrated AssessmentJoint assessment of needs is a co-ordinated Multi-Agency approach to gathering information and aims to avoid parents having to repeat information more than once, giving a holistic view of the child within their family and community enabling assessment of medical, social and educational needs.
Action plans are developed using the systematic assessment and analysis of the information obtained about the child. The child and their family may participate in the development of the action plan.An action plan records the needs and the professional responses and responsibilities to the child, outlining the basis for providing support, services and resources to meet the needs of the child.An action plan should state:
what action should be taken by whom to improve the child’s circumstances the reasons for the plan timescales intended outcome and future review date
The plan should be as simple as necessary and relevant to the child's needs. It should be updated or amended as needs change.
Individual Educational Plan / Co-ordinated Support PlanAn Individual Educational Plan (IEP) describes in detail the nature of the child’s additional support needs, the ways in which these are to be met, the learning outcomes to be achieved, and specifies what additional support is required, including that required from agencies outwith education. The IEP should be reviewed and updated regularly, involving the parents and child (where possible).
A Co-ordinated support plan is prepared for children who: need support due to complex or multiple factors that have a significant
adverse affect on their education require significant involvement from one or more additional agencies
such as health and social work will need support for more than a year
The aim of a co-ordinated support plan (CSP) is to ensure that the various professionals and agencies involved in providing support are working together and that the support is co-ordinatedA Co-ordinated support plan:
is an action plan for children who require significant additional support with their education
supports partnership working to help children achieve educational targets
is monitored and reviewed regularly involves the child, their family, education and additional agencies
(Enquire, 2007)
November 2008 27

Combined Child Health Service
Voluntary AgenciesAn Autism specific assessment of support needs by a voluntary agency e.g. Autistic society may be useful depending on the complexity of the child’s difficulties or circumstances.
Key workerA key worker is a named person who works in partnership with the family and can provide a link between professionals and agencies involved in the child’s care. Key workers can co-ordinate access to, and delivery of services required from various agencies.
Regular Review
The child will have regular reviews carried out by the various professionals and agencies involved in their care. Their needs will be reassessed and plans updated as required.
November 2008 28

Combined Child Health Service
Annex 1
THE CHAT assessment form. (The National Autistic Society, www.nas.org.uk accessed July 2007)
THE CHATTo be used by GPs or Health Visitors during the 18 month developmental
check-up.
Child’s name:................................. Date of birth:............... Age:................
Child’s address:................................................. Phone number: ................
SECTION A: ASK PARENT:
1. Does your child enjoy being swung, bounced on your
knee, etc?
YES NO
2. Does your child take an interest in other children? YES NO
3. Does your child like climbing on things, such as up stairs? YES NO
4. Does your child enjoy playing peek-a-boo/hide-and-seek? YES NO
5. Does your child ever PRETEND, for example, to make a
cup of tea using a toy cup and teapot, or pretend other
things?
YES NO
6. Does your child ever use his/her index finger to point, to
ASK for something?
YES NO
7. Does your child ever use his/her index finger to point, to
indicate INTEREST in something?
YES NO
8. Can your child play properly with small toys (e.g. cars or
bricks) without just mouthing, fiddling or dropping them?
YES NO
9. Does your child ever bring objects over to you (parent) to
SHOW you something?
YES NO
November 2008 29

Combined Child Health Service
SECTION B: GP OR HV OBSERVATION:i. During the appointment, has the child made eye contact
with you?
YES NO
ii. Get child’s attention, then point across the room at an
interesting object and say “Oh look! There’s a (name of toy)!”
Watch child’s face. Does the child look across to see what
you are pointing at?
YES NO*
iii. Get the child’s attention, then give child a miniature toy
cup and teapot and say “Can you make a cup of tea?” Does
the child pretend to pour out tea, drink it, etc?
YES NO**
iv. Say to the child “Where’s the light?”, or “Show me the
light”. Does the child POINT with his/her index finger at the
light?
YES NO***
v. Can the child build a tower of bricks? (If so how many?)
(Number of bricks:.............)
YES NO
* (To record YES on this item, ensure the child has not simply looked at your
hand, but has actually looked at the object you are pointing at.)
** (If you can elicit an example of pretending in some other game, score a
YES on this item.)
*** (Repeat this with “Where’s the teddy?” or some other unreachable object, if child does not understand the word “light”. To record YES on this item, the child must have looked up at your face around the time of pointing.)
MRC/SBC 1995
November 2008 30

Combined Child Health Service
Annex 2
ICD-10 / DSM-IV Classification SystemInternational Classification of Diseases, version 10 (ICD-10) and the Diagnostic and Statistical Manual of Mental Disorders 4 th edition (DSM-IV) definition of Autism. (SIGN Guidelines 2007) ICD-10 Classification System DSM-IV Classification SystemF84.0 Childhood Autism
A. Presence of abnormal or impaired development before the age of three years, in at least one of the following areas:
receptive or expressive language as used in social communication
the development of selective social attachment or of reciprocal social interactions
functional or symbolic playB. Qualitative abnormalities in
reciprocal social interaction, manifest in at least one of the following areas:
failure to adequately use eye-to-eye gaze, facial expression, body posture and gesture to regulate social interaction
failure to develop (in a manner appropriate mental age, and despite ample opportunities) peer relationships that involve a mutual sharing of interests, activities and emotions
a lack of socio-emotional reciprocity as shown by an impaired or deviant response to other peoples emotions; or a lack of modulation of behaviour according to social context, or a weak integration of emotional and communicative behaviours
C. Qualitative abnormalities in communication, manifests in at least two of the following areas:
a delay in, or total lack of development of spoken language that is not
299.00 AutismA total of six or more from 1, 2 and 3, with at least two from 1 and one each from 2 and3.
1. Qualitative impairment in social interaction, as manifested by at least two of the following:
marked impairment in the use of multiple nonverbal behaviours such as eye-to--eye gaze, facial expression, body posture and gestures to regulate social interactions
failure to develop peer relationships appropriate to development level
a lack of spontaneous seeking to share enjoyment, interest or achievements with other people (by a lack of showing, bringing or pointing out objects of interest)
lack of social or emotional reciprocity
2. Qualitative impairment in communication as manifested by at least one of the following:
delay in or total lack of the development of the spoken language (not accompanied by an attempt to compensate through alternative modes of communication such as gesture or mime)
in individuals with adequate speech, marked impairment in the ability to initiate or sustain a conversation with others
stereotyped and repetitive use of language or idiosyncratic language
lack of varied, spontaneous make-believe play or social
November 2008 31

Combined Child Health Service
ICD-10 Classification System DSM-IV Classification Systemaccompanied by an attempt to compensate through the use of gesture or mime as alternative modes of communication (often preceded by a lack of communicative babbling);
relative failure to initiate or sustain conversation interchange (at whatever level of language skills are present) in which there is reciprocal to and from responsiveness to the communications of the other person;
stereotyping and repetitive use of language or idiosyncratic use of wards or phrases;
abnormalities in pitch, stress, rate, rhythm and intonation of speech;
D. Restricted, repetitive, and stereotyped patterns of behaviour, interests and activities manifests in at least two of the following areas:
an encompassing preoccupation with one or more stereotyped and restricted patterns of interest that are abnormal in content and focus; or one or more interests that are abnormal in their intensity and circumscribed nature although not abnormal in their content or focus,
apparently compulsive adherence to specific, non-functional, routines or rituals;
stereotyped and repetitive motor mannerisms that involve either hand or finger flapping or twisting, or complex whole body movements;
preoccupation with part-objects or non-functional
imitative play appropriate to developmental level
3. Restricted repetitive and stereotyped patterns of behaviour, interest and activities, as manifested by at least one of the following:
encompassing preoccupation with one or more stereotyped and restricted patterns of interest that is abnormal either in intensity or focus
apparently inflexible adherence to specific, non-functional routines or rituals
stereotyped and repetitive motor mannerisms (hand or finger flapping or twisting, or complex whole body movements)
persistent preoccupation with parts of objects
4. Delay or abnormal functioning in at least one of the following areas, with onset prior to the age of three years:
Social interaction Language as used in social
communication Symbolic or imaginative play5. The disturbance is not better
accounted for by Rett’s Disorder or childhood Disintegrative Disorder.
299.80 Pervasive Development Disorder nor otherwise specified (including Atypical Autism)This category should be used when there is a severe and pervasive impairment in the development of reciprocal social interactions associated with impairment in either verbal or nonverbal communication skills or with the presence of stereotyped behaviour, interests and activities, but the criteria are not met for a specific Pervasive Development Disorder, Schizophrenia, Schizotypal Personality Disorder, or Avoidant
November 2008 32

Combined Child Health Service
ICD-10 Classification System DSM-IV Classification Systemelements of play materials (such as their odour ,the feel of their surface, or the noise or vibration that they generate);
distress over changes in small, non-functional, details of the environment;
E. The clinical picture is not attributable to the other varieties of pervasive development disorder.
F84.1 Atypical autismA. Presence of abnormal or
impaired development at or after age three years(criteria as for autism expected age of manifestation)
B. Qualitative abnormalities in reciprocal social interactions or in communication, or restricted, repetitive and stereotyped patterns of behaviour, interests and activities (criteria as for autism except that it is not necessary to meet the criteria in terms of numbers of areas of abnormality).
C. The disorder does not meet the diagnostic criteria for autism (F84.0)
Autism may be atypical in either age of onset (F84.11) or phenomenology (F84.12), these two types being differentiated with a fifth character for research purposes.Syndromes that are atypical in both respects should be coded F84.12 F84.10 Atypicality in age of onset
A. Does not meet criterion A for autism. That is, abnormal or impaired development is evident only at or after age three years.
B. Meets criteria B, C, D and E for autism (F84.0)
F84.11 Atypicality in symptomatology
A. Meets criterion A for autism.
Personality Disorder. For example, this category includes *atypical autism*- presentations that do not meet the criteria for autistic Disorder because of late age of onset, atypical symptomatology, or sub threshold symptomatology, or all of these. 229.80 Aspergers Disorder
1. Qualitative impairment in social interaction, as manifested by at least two of the following:
marked impairment in the use of multiple nonverbal behaviours such as eye-to-eye gaze, facial expression, body postures, and gestures to regulate social interaction
failure to develop peer relationships appropriate to developmental level
a lack of spontaneous seeking to share enjoyment, interest, or achievements with other people(e.g. by a lack of showing, brining, or pointing out objects of interest to other people)
lack of social or emotional reciprocity
2. Restricted repetitive and stereotyped patterns of behaviour, interests, and activities, as manifested by a least one of the following:
encompassing preoccupation with one or more stereotyped and restricted patterns of interest that is abnormal either in intensity or focus
apparently inflexible adherence to specific, non-functional routines or rituals
stereotyped and repetitive motor mannerisms (e.g. hand or finger flapping or twisting, or complex whole-body movements)
persistent preoccupation with parts of objects
November 2008 33

Combined Child Health Service
ICD-10 Classification System DSM-IV Classification System(i.e. presence of abnormal or impaired development is evident only at or after age three years).
B. Qualitative abnormalities in reciprocal social interactions or in communication, or restricted, repetitive and stereotyped patterns of behaviour, interests and activities (criteria as for autism except that it is not necessary to meet the criteria in terms of numbers of areas of abnormality).
C. Meets criterion E for autism. D. Does not meets the full criteria
B, C and D for autism (F84.0)F84.12 Atypicality in both age of onset and symptomatology
A. Does not meet criterion A for autism. That is, abnormal or impaired development is evident only at or after age three years.
B. Qualitative abnormalities in reciprocal social interactions or in communication, or restricted, repetitive and stereotyped patterns of behaviour, interests and activities (criteria as for autism except that it is not necessary to meet the criteria in terms of numbers of areas of abnormality).
C. Meets criterion E for autism. Does not meets the full criteria B, C and D for autism (F84.0)
3. The disturbance causes clinically significant impairment in social, occupation, or other important areas of functioning.
4. There is no clinically significant general delay in language (e.g. single words used by age 2 years, communicative phrases used by age 3 years)
5. There is no clinically significant delay in cognitive development or in the development of age-appropriate self-help skills, adaptive behaviour (other than in social interaction), and curiosity about the environment in childhood.
6. Criteria are not met for another specific Pervasive development disorder or Schizophrenia.
November 2008 34

Combined Child Health Service
Documents used in the production of pathways
Assessment, diagnosis and clinical interventions for children and young people with autism spectrum disorder. SIGN Guideline 2007
Autistic Spectrum Disorders, Needs Assessment Report. Public Health
Institute of Scotland (PHIS) 2001
Autistic Spectrum Disorders Needs Assessment Report (2001), Scottish Executive Report on Implementation and Next Steps. Scottish Executive 2006
National Autism Plan for Children (NAPC) National Initiative for Autism: Screening and Assessment (NIASA) 2003
References:
Enquire, Planning children’s and young people’s learning, www.enquire.co.uk (accessed 2007)
Scottish Society for Autism (2006), What is Autism? www.autism-in-scotland.org.uk (accessed 2007)
Scottish Executive, Education (Additional Support for Learning) (Scotland) Act 2004
Scottish Executive (2006), Getting it Right for Every Child
National Autistic Society, Early Bird Plus Programme, www.nas.org.uk (accessed 2007)
National Autistic Society, help programme, www.nas.org.uk (accessed 2007)
National Autistic Society Scotland (2006), Scottish autism information resource Next Steps, working with parents, working with professionals, working together
NHS Scotland (2006), Information for parents and carers with a child or young person recently diagnosed with an Autism Spectrum Disorder
November 2008 35
Combined Child Health Service
Working Group Members
Jackie Crum (chair) Consultant Paediatrician
Elaine Bremner Team Manager, Aberdeenshire Social Work
Christine Bruce Staff Grade Paediatrician
Lynn Buntin Clinical Psychologist
Donella Clark Senior Practioner,Aberdeenshire Social Work
Ena Cromar Project Co-Ordinator, Children with Disabilities
Suleman Daud Consultant Paediatrician
John Forrester Training & Assessment Consultant(Grampian Autistic Society)
Janette Fotheringham Educational Psychologist Aberdeenshire
Anne Gilchrist Consultant Psychiatrist
Andre Liebenberg Consultant Paediatrician
Izy McDonald Health Visitor Aberdeenshire
Gail McKeitch Parent Representative
Elma Stephen Consultant Paediatrician
Gail Thomson Service Manager Royal Aberdeen Children’s Hospital
Donald Todd Clinical Nurse Manager
November 2008 36