author's personal copy · paradox, less skin should be excised centrally but more laterally,...
TRANSCRIPT
This article appeared in a journal published by Elsevier. The attachedcopy is furnished to the author for internal non-commercial researchand education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/copyright

Author's personal copy
High TensionAbdominoplasty 2.0Lorne King Rosenfield, MDa,b,*
The abdominoplasty can at once be deceivinglyeasy to perform and maddeningly inconsistentin its results. The plastic surgeon is challengedto excise all the anterior trunk and fat, throughthe shortest possible incision, and to ensure perprimum healing with an inconspicuous scar. Tobegin to rise to this challenge requires one tobecome a student of the abdominoplasty. Bycontinuously honing one’s surgical planning andexecution, a more ‘‘balanced’’ technique can berealized that is both reliably safe and aestheticallysuccessful. High lateral tension abdominoplasty(HLTA), with some 2.0 modifications, is sucha technique.
Traditionally, the primary goal of any abdomino-plasty has always been to excise the central lowerabdominal excess skin or pannus and plicate theabdominal fascia through a suprapubic incision.Unfortunately, this classic abdominoplasty mayoften fall short of this goal: a scar that may ridetoo high; persistent skin and lipodystrophy at thepubis, thighs, flanks, and hips; and unfortunatelya consistent incidence of midline skin necrosis orwound dehiscence.
HLTA addresses these shortfalls. It may bedefined as a more complete treatment of the trunkaesthetic unit from the abdomen to the pubis, hips,and thighs, with a greater overall aesthetic resultand margin of vascular safety. This article outlinesthe techniques and tools to accomplish thesesuperior results safely and consistently.
THE EVOLUTION OF THE MODERNABDOMINOPLASTY
The abdominoplasty technique has evolved signif-icantly in the last 4 decades. The modern abdom-inoplasty technique was developed in SouthAmerica in the 1960s.1 The basic surgical tenetshave always been to conduct a rectus plication,with maximal excision of the central skin excessby extensive undermining of the entire abdominalwall. The closure is often under some tensionand is therefore, per force, conducted with thepatient in significant flexion. When liposuctionwas introduced in the 1980s, it soon becameapparent that blithely and aggressively addingthis modality to abdominoplasty was fraught withan unacceptable incidence of flap ischemia andskin necrosis. Liposuction then evolved intoa more conservative adjuvant treatment.2
Although there were indeed less physiologic prob-lems with this technique, the aesthetic resultswere also, once again, more constrained.
Then, in the early 1990s Lockwood3 publisheda series of seminal articles that single handedlychanged the tack of the abdominoplasty tech-nique. Based on his extensive experience withbody-contouring surgery, he decisively demon-strated and definitively modified the surgical prin-ciples of abdominoplasty and reported greatersafety and improved aesthetics. He enumeratedseveral surgical tenets that were in many ways
a Division of Plastic Surgery, Department of Surgery, University of California San Francisco, 400 ParnassusAvenue, San Francisco, CA 94143, USAb Division of Plastic Surgery, Department of Surgery, Stanford University Medical Center, Stanford, 770 WelchRoad, Palo Alto, CA 94304, USA* Private Practice, 1750 El Camino Real, #405, Burlingame, CA 94010.E-mail address: [email protected]
KEYWORDS
� Abdominoplasty � High lateral tension abdominoplasty� Body contouring � Weight loss surgery
Clin Plastic Surg 37 (2010) 441–465doi:10.1016/j.cps.2010.03.0050094-1298/10/$ – see front matter ª 2010 Elsevier Inc. All rights reserved. pl
asti
csur
gery
.thec
lini
cs.c
om

Author's personal copy
diametrically opposed to those of the classic ortraditional abdominoplasty: the undermining ofonly the central skin flap to facilitate plicationwith discontinuous dissection elsewhere (toenhance vascularity and allow for judiciousconcomitant liposuction) and the initial resectionof the lateral excess skin, with more conservativeresection of the central skin flap (to accomplisha more complete and natural repair) by usinga planned and controlled high-tension closure(with the diligent use of the underlying superficialfascial system). And so HLTA was borne.
HLTA: A 2.0 VERSION
In the past 12 years, I have become a diligentstudent of these Lockwood principles and appliedthem to a large series of several hundred patients.4
The application of these principles and the criticalanalysis of the results have driven a successfulevolution of the HLTA procedure. For a result tobe called truly successful, strict standards werebalanced equally: the case had to demonstratethe greatest degree of safety (zero tolerance forcomplications), with the maximal aesthetic result(correction of all deformities) and with a consistentreliability of the technique (regardless of patientpresentation). Several important expanded princi-ples of the HLTA may be distilled from this experi-ence to define a true 2.0 advancement intechnique.
1. The abdominal procedure should not be a slaveto the otherwise arbitrary mandate that all theskin between the pubis and the umbilicusmust be excised. This approach only trulyworks in the patient with an enormous pannus.Otherwise, the excisional marking must be, perforce, placed above the pubic hairline toaccomplish wound closure, that despite theharnessing of the excess pubis, remains overlytight. That result may be an excessively highscar and superiorly retracted pubis, an unnatu-rally flat hypogastrium and more seriously, anexaggerated rate of wound dehiscense andskin necrosis. Instead, any redundant pubisshould be excised, rather than aid in the closureof harnessed. The pubis is then closed under notension and rests in a lower, more inconspic-uous location. However, except for the most‘‘redundant’’ cases, this approach often delib-erately leaves some of the skin between thepubis and umbilicus intact. This necessitatesthat the original umbilical site be closed. Thesurgeon must resist the temptation to removeeven a few centimeters of intervening
abdominal skin for fear of recreating the usualoverly tight closure.
2. Any abdominoplasty should consider not onlywhat is above the future incision (the traditionalpannus) but also what is below: that is, theexcess pubis, anterolateral and medial thighredundancy, as well as buttocks laxity. Other-wise, the tissues below the incision may bedistractingly untreated postoperatively and thefull effect of the HLTA may not be realized.This tenet underlines one of the greatest bene-fits to HLTA not normally considered possiblewith traditional abdominoplasty: one can realizea true body lift effect through an anterior inci-sion only. In essence this approach is actuallya ‘‘global’’ tension abdominoplasty, withsequential tension placed fully from lateral tomedial.
3. It is has always been important to evaluate themagnitude of excess skin to be excised. But toactually design the most efficient length anddirection of the incision, it is critical that theextent and orientation of the skin left behind isalso assessed. The surgeon must ensure thatthe remaining skin is both sufficient to closethe defect and efficiently relieved of its ownredundancy. This principle may be appliedequally to the central and lateral closure.Specifically, laterally, the excess skin at thehip and thigh is often neglected by traditionalabdominoplasty. This primarily obliquelyoriented excess tissue is efficiently removedthrough the oblique incision/vector of theHLTA. Centrally the superfluous skin at the epi-gastrium constitutes primarily horizontalexcess (that has migrated from the chest),that can neither be efficiently removed norshould be used to close a lower abdominaldefect, through the horizontal incision. Thereinlies the essence of the potential flaw in tradi-tional abdominoplasty and the efficacy of thehigh lateral tension technique. That is, an incon-gruent consequence may occur: the woundclosure may be too tight despite the apparentepigastric redundancy, which can, in turn, beleft behind and the lateral excess cannot beeffectively treated because the remainingabdominal flap has been primarily used for thecentral closure. Instead to reconcile thisparadox, less skin should be excised centrallybut more laterally, through an HTLA-orientedincision and repair. These concepts are illus-trated in Figs. 1 and 2. Using vector analysis,the lateral tissue above and below the incisionis redundant in a more oblique vector and soshould be removed through an opposing obli-que incision. Serendipitously, this matches the
Rosenfield442

Author's personal copy
relative direction of the desired HTLA lateralscar placement. In addition, this oblique vectoralso treats the predominantly horizontal excessin the epigastrium. Applying this vector of
excess principle, the necessary direction ofthe most desirable HTLA central and lateralincision placement is easily understood anddefined. Thus, the more a procedure followsthe vectors of excess of both what is takenand what will remain, the more efficient thetreatment of redundant skin.
4. As a corollary of this aforementioned principle, itmay be stated that, as long as there is excesstissue, the longer the scar, the more far-reachingthe tension effect and the more dramatic theresults. In fact, as will be shown in this chapter,a ‘‘virtual’’ lower body lift can be accomplished,when indicated from this entirely ‘‘supine’’ oper-ation. Clearly, the most posterior buttocks andthighs cannot be addressed, but this approachcan and does satisfy the majority of properlyselected patients who, in fact see this effect asa significant bonus. And inherently, this, albeit,‘‘conservative’’ body lift does reduce thesurgical time and operative risks as comparedto a full truncal lift procedure.
5. Lockwood, originally, and rightfully so, empha-sized the ‘‘lateral’’ tension nature of this tech-nique. That is, that the surgeon, contrary tothe traditional approach, must begin the resec-tion from lateral and work medially. This admo-nition emanated from his original observationthat there was actually more redundancy later-ally at the hip, thigh and buttock than centrally.Indeed, if the surgeon respects and executesthis principal, they will indeed realize a superiorcorrection beyond the central abdomen. Hencethe "lateral" tension eponym. However, it ismore instructive and indeed more efficaciousto instead, consider the entire length of thewound as tension. That is, it is also possibleto accomplish as much correction centrally, atthe redundant pubic and inner and anteriorthighs, if the tension principle is honored hereas well.
6. The goal of the design and placement of thefuture scar should primarily be to hide it. Lock-wood originally described a very high (Frenchcut) lateral closure, probably because that styleof clothing was more fashionable at the timeand a more oblique vector of pull does moreefficiently treat the upper abdominal excessas described earlier. However, consideringhow fashion changes, and that a hidden scarwill usually trump some residual excess skin,the surgeon should mark the patient within theirpreferred clothing. This philosophy becomesparticularly relevant when working with thelow-cut jean fashion.
7. The location and extent of the remaining subcu-taneous fat must also be evaluated and
Fig. 1. The more a procedure follows the vectors ofexcess of both what is taken and what will remain,the more efficient the treatment of redundant skin.
Fig. 2. Applying this vector of excess principle, thenecessary direction of the most desirable HTLA centraland lateral incision placement is easily understoodand defined.
High Tension Abdominoplasty 2.0 443

Author's personal copy
respected. This assessment represents an age-old plastic surgical battle between beauty andblood. That is, at what cost to the blood supplydoes the surgeon attempt to remove all remain-ing excess subcutaneous fat? Lockwood origi-nally described a reasonable detente:liposuction should only be conducted beneathtissues that have not been undermined.However, most recently, the proverbialpendulum has swung backward: more recentpublications are giving permission once againto conduct more aggressive full truncal liposuc-tion at the time of the abdominoplasty.5 Thisrecommendation is predicated on the notionthat if one follows the original Lockwood admo-nition to restrain the flap dissection only asmuch as needed to conduct a fascial plication,then enough perforators are preserved to allowfor this aggressive liposuction. However, as hasbeen stated earlier, Lockwood did also warnthat despite this conservative undermining,liposuction of the remaining central skin flapshould not be entertained for fear of skin flapnecrosis. (And realistically, some of thesesame precious perforators are often sacrificedto repair the more protuberant abdomen.) Thisprinciple should be respected in light of Lock-wood’s prodigious experience.
8. If the premise is to preserve the central flap’sblood supply by undermining only centrally toallow for fascial plication, it may indeed beself-defeating to then disrupt the very sameflap with liposuction. Ironically, the only patientswho might be candidates for such an aggres-sive approach would be those without a signifi-cant amount of fat in the first place: that is, thepatient with a low body mass index (BMI, calcu-lated as weight in kilograms divided by thesquare of height in meters). Otherwise, in theusually higher BMI abdominoplasty patient,liposuction should be restricted to the waistand hip rolls with a planned secondary liposuc-tion centrally, some 6 to 12 months later. Onlythen, can a zero tolerance for skin flap necrosisand dehiscence be honored.
PATIENT ANATOMY
The general abdominal anatomy is well describedin this issue by Farzad Nahai. Therefore, thespecific anatomy most relevant to the under-standing and application of HLTA is highlightedin this article.
There are 3 critical anatomic points that shouldbe understood and respected when planning andperforming HLTA:
1. The superficial fascial system: This layer mustbe identified and used fully to both harnessthe maximal lift that this technique can profferand prevent wound dehiscence.
2. The perforator blood supply: The abdominalflap’s viability is predicated on the preservationof as many fascial perforators as possible.
3. The zones of adherence: These various pointsof skin attachment must be released, at leastbluntly, to realize the maximum translation ofpull of the remaining skin envelope, particularlyat the anterolateral thigh region. There is oftenalso what may be called a waist band of adher-ence at the patient’s midsection that can signif-icantly inhibit the skin’s mobility. (see laterdiscussion).
PATIENT ASSESSMENT
A comprehensive examination is mandatory toenable the surgeon to properly prepare the patientand accurately plan the surgery.
Physical
The physical examination should include evalua-tion of all layers of the abdominal wall: the skin,the subcutaneous fat, and underlying fascia/muscle (with an indirect assessment of the extentof intra-abdominal fat).
SkinThe skin examination should be much more thanjust the assessment of the classic pannus ofexcess lower abdominal skin above the pubis.
Striae Their boundaries are assessed. The extentof the striae that may not be included in the resec-tion should be duly noted and explained to thepatient (particularly those above the umbilicus).
Excess skin The extent of obvious anterior redun-dant skin (width of the pannus) is noted first. Thisevaluation most accurately defines the length ofthe incision. However, a proper assessment mustbe made beyond the obvious excess lowerabdominal pannus if a more complete correctionis to be made of the entire anterior trunk aestheticunit; that is, the extent of redundancy is evaluatednot only above the inguinal area but also below theincision, at the hips, thighs, and pubis. If there isparticular excess at the lateral thighs, then theincision will, by definition, be appreciably longer,if the HLTA approach is to be properly applied. Infact, in these patients, it may be stated that thelonger the incision made, the better the results.On the other hand, if the patient demonstratesminimal excess laterally, then significant tensionshould not be planned, to avoid making the
Rosenfield444
Author's personal copy
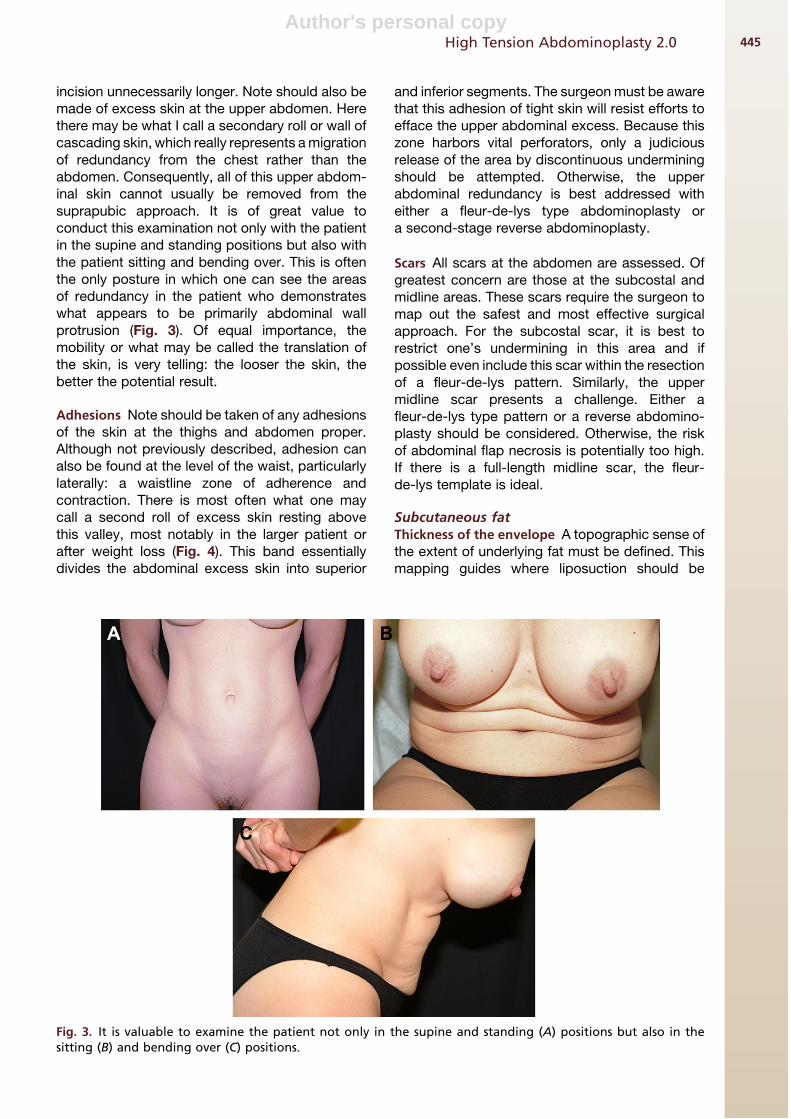
incision unnecessarily longer. Note should also bemade of excess skin at the upper abdomen. Herethere may be what I call a secondary roll or wall ofcascading skin, which really represents a migrationof redundancy from the chest rather than theabdomen. Consequently, all of this upper abdom-inal skin cannot usually be removed from thesuprapubic approach. It is of great value toconduct this examination not only with the patientin the supine and standing positions but also withthe patient sitting and bending over. This is oftenthe only posture in which one can see the areasof redundancy in the patient who demonstrateswhat appears to be primarily abdominal wallprotrusion (Fig. 3). Of equal importance, themobility or what may be called the translation ofthe skin, is very telling: the looser the skin, thebetter the potential result.
Adhesions Note should be taken of any adhesionsof the skin at the thighs and abdomen proper.Although not previously described, adhesion canalso be found at the level of the waist, particularlylaterally: a waistline zone of adherence andcontraction. There is most often what one maycall a second roll of excess skin resting abovethis valley, most notably in the larger patient orafter weight loss (Fig. 4). This band essentiallydivides the abdominal excess skin into superior
and inferior segments. The surgeon must be awarethat this adhesion of tight skin will resist efforts toefface the upper abdominal excess. Because thiszone harbors vital perforators, only a judiciousrelease of the area by discontinuous underminingshould be attempted. Otherwise, the upperabdominal redundancy is best addressed witheither a fleur-de-lys type abdominoplasty ora second-stage reverse abdominoplasty.
Scars All scars at the abdomen are assessed. Ofgreatest concern are those at the subcostal andmidline areas. These scars require the surgeon tomap out the safest and most effective surgicalapproach. For the subcostal scar, it is best torestrict one’s undermining in this area and ifpossible even include this scar within the resectionof a fleur-de-lys pattern. Similarly, the uppermidline scar presents a challenge. Either afleur-de-lys type pattern or a reverse abdomino-plasty should be considered. Otherwise, the riskof abdominal flap necrosis is potentially too high.If there is a full-length midline scar, the fleur-de-lys template is ideal.
Subcutaneous fatThickness of the envelope A topographic sense ofthe extent of underlying fat must be defined. Thismapping guides where liposuction should be
Fig. 3. It is valuable to examine the patient not only in the supine and standing (A) positions but also in thesitting (B) and bending over (C) positions.
High Tension Abdominoplasty 2.0 445

Author's personal copy
conducted and just as importantly, where it shouldnot be performed. Usually the contouring of thewaist, hips, and lateral thigh assists the HLTA byfacilitating the translation of pull of the skin withits liposuction-induced discontinuous dissectionand accentuates the abdominoplasty’s shapingeffects. If the central flap is very thick with fat,then it is best to inform the patient thata second-stage liposuction surgery may be neces-sary to complete the repair safely.
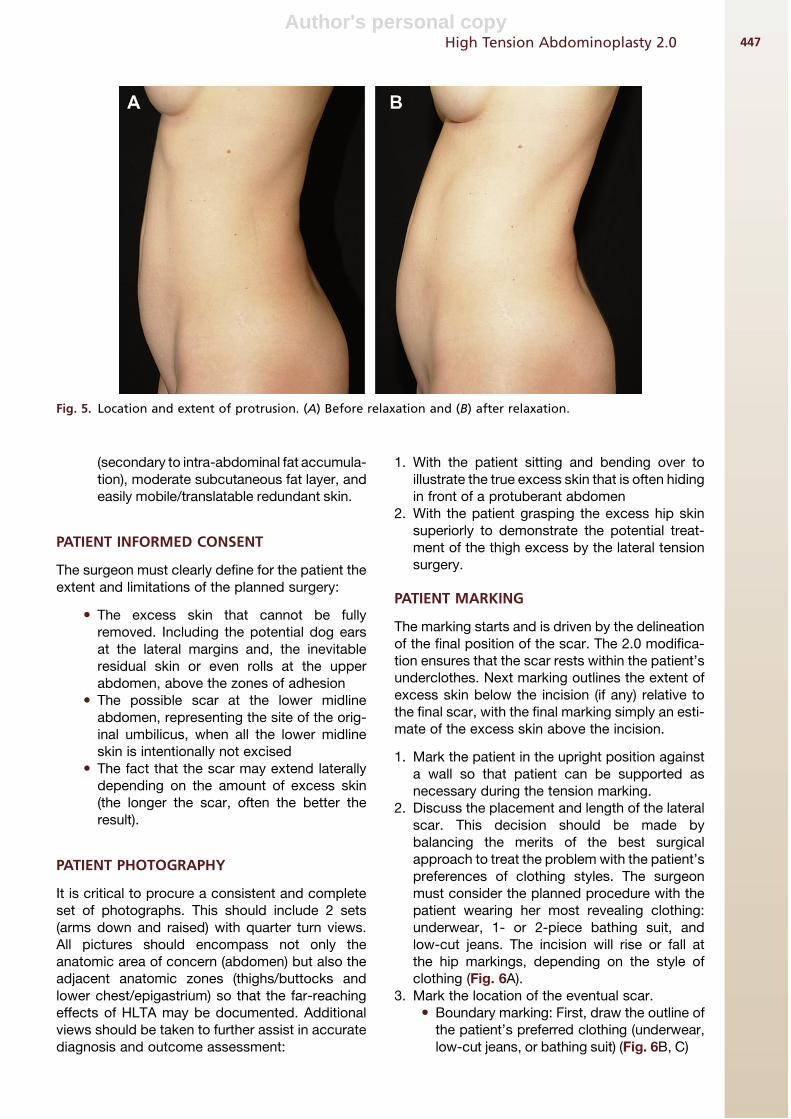
Abdominal wallThe location and extent of protrusion Assess thedegree of lower abdominal wall relaxation with thepatient lying down with knees bent, as well aswhen standing. Also ask the patient, whilestanding, to make a conscious effort to relax theabdominal wall. The additional extent of protrusionthat occurs is surprising and informative (Fig. 5). Inaddition to the obvious lower abdominal wallprotrusion, one should assess the magnitude oflaxity at the upper abdomen. Compressing thelower abdominal wall and watching for herniationof the epigastric area will accomplish this task.
The presence of hernia The examination shouldexplore for incisional, epigastric, and periumbilicalhernia. This is particularly relevant, not only so thatthe surgeon may plan to repair the defect but also
to avoid any liposuction in these areas beforeabdominal flap elevation to prevent intra-abdom-inal penetration of the cannula.
The shape of the waist If the waist is more squarewith fat blunting its shape, then an aggressive lipo-suction can be very salutary.
PATIENT SELECTION
The patient criteria to be considered must beexhaustive if the surgeon is to avoid major compli-cations or patient disappointment.
The ideal patient criteria:� Weight: not grossly overweight (BMI <30
kg/m2) and stable for more that 6 months,if significant weight lost.� Medical condition: no major medical issues
such as labile hypertension, diabetes, coro-nary disease, nutritional deficiency, and soforth.� Psychological state: well motivated and
realistic (eg, postpregnancy or gastricbypass patients).� Habits: regular exercise, reasonable diet,
no smoking or excess alcohol.� Anatomy: absence of multiple abdominal
scars, no extreme abdominal protrusion
Fig. 4. Adhesion (A, B, C).
Rosenfield446
Author's personal copy
(secondary to intra-abdominal fat accumula-tion), moderate subcutaneous fat layer, andeasily mobile/translatable redundant skin.
PATIENT INFORMED CONSENT
The surgeon must clearly define for the patient theextent and limitations of the planned surgery:
� The excess skin that cannot be fullyremoved. Including the potential dog earsat the lateral margins and, the inevitableresidual skin or even rolls at the upperabdomen, above the zones of adhesion� The possible scar at the lower midline
abdomen, representing the site of the orig-inal umbilicus, when all the lower midlineskin is intentionally not excised� The fact that the scar may extend laterally
depending on the amount of excess skin(the longer the scar, often the better theresult).
PATIENT PHOTOGRAPHY
It is critical to procure a consistent and completeset of photographs. This should include 2 sets(arms down and raised) with quarter turn views.All pictures should encompass not only theanatomic area of concern (abdomen) but also theadjacent anatomic zones (thighs/buttocks andlower chest/epigastrium) so that the far-reachingeffects of HLTA may be documented. Additionalviews should be taken to further assist in accuratediagnosis and outcome assessment:
1. With the patient sitting and bending over toillustrate the true excess skin that is often hidingin front of a protuberant abdomen
2. With the patient grasping the excess hip skinsuperiorly to demonstrate the potential treat-ment of the thigh excess by the lateral tensionsurgery.
PATIENT MARKING
The marking starts and is driven by the delineationof the final position of the scar. The 2.0 modifica-tion ensures that the scar rests within the patient’sunderclothes. Next marking outlines the extent ofexcess skin below the incision (if any) relative tothe final scar, with the final marking simply an esti-mate of the excess skin above the incision.
1. Mark the patient in the upright position againsta wall so that patient can be supported asnecessary during the tension marking.
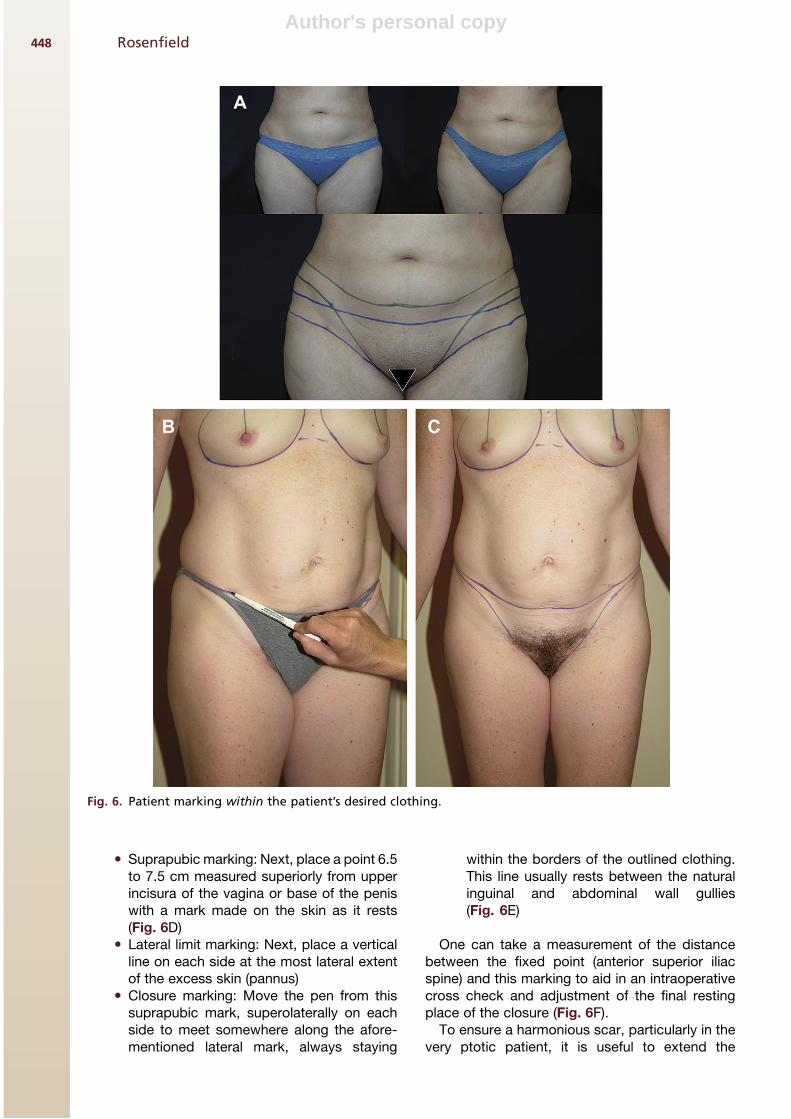
2. Discuss the placement and length of the lateralscar. This decision should be made bybalancing the merits of the best surgicalapproach to treat the problem with the patient’spreferences of clothing styles. The surgeonmust consider the planned procedure with thepatient wearing her most revealing clothing:underwear, 1- or 2-piece bathing suit, andlow-cut jeans. The incision will rise or fall atthe hip markings, depending on the style ofclothing (Fig. 6A).
3. Mark the location of the eventual scar.� Boundary marking: First, draw the outline of
the patient’s preferred clothing (underwear,low-cut jeans, or bathing suit) (Fig. 6B, C)
Fig. 5. Location and extent of protrusion. (A) Before relaxation and (B) after relaxation.
High Tension Abdominoplasty 2.0 447
Author's personal copy
� Suprapubic marking: Next, place a point 6.5to 7.5 cm measured superiorly from upperincisura of the vagina or base of the peniswith a mark made on the skin as it rests(Fig. 6D)� Lateral limit marking: Next, place a vertical
line on each side at the most lateral extentof the excess skin (pannus)� Closure marking: Move the pen from this
suprapubic mark, superolaterally on eachside to meet somewhere along the afore-mentioned lateral mark, always staying
within the borders of the outlined clothing.This line usually rests between the naturalinguinal and abdominal wall gullies(Fig. 6E)
One can take a measurement of the distancebetween the fixed point (anterior superior iliacspine) and this marking to aid in an intraoperativecross check and adjustment of the final restingplace of the closure (Fig. 6F).
To ensure a harmonious scar, particularly in thevery ptotic patient, it is useful to extend the
Fig. 6. Patient marking within the patient’s desired clothing.
Rosenfield448

Author's personal copy
marking to include the design of a posterior bodylift that may be planned or desired in the future.
4. Define the lower margin of excision next. Thekey maneuver:� Place marking pen over the line of future
closure and maintain this position whilepulling the excess skin upward vigorously(this is the tension in the HTLA), until taut,then mark the skin that is now below thetip of the pen (Fig. 7A)� Perform this maneuver across the width of
the abdomen as needed to define the lowerincision (Fig. 7B, C, D)
NOTE: Because the maneuver can and shouldbe quite forceful, it is helpful to have the patientlean against a wall during the marking.
5. Estimate upper margin of excision. The keymaneuver:� Pinch the excess skin with the thumb on the
lower incision line and the fingers at thesuperior extent of the excess while tryingto maintain the premarked final closureline visible at the middle of the skin roll. Startmarking laterally and work your way medi-ally (Fig. 7E)� The resultant line will usually rest several
centimeters above the level of the umbilicus
laterally and a few centimeters below theumbilicus centrally.
6. Decide the treatment of the umbilicus. Basicprinciples:� Guiding coordinates:
- The umbilicus should be roughly 9 to 12 cmabove the superior margin of the pubis, de-pending on the patient’s habitus
- The umbilicus should rest slightly abovethe latitude of the superior margin of theiliac crests (But in the final analysis, likemany challenges in plastic surgery, one’scritical eye should ultimately drive thesurgeon’s decision.)
� The treatment of the umbilicus is deter-mined by 2 factors:
- The amount of excess skin above andbelow the umbilicus: that is, in the upperand lower poles of the abdomen and
- The location of the umbilicus in conjunc-tion with the length of the abdomen andwaist
� If there is no excess above and mild excessbelow, the excision may be conducted withthe umbilicus left intact, as a mini-abdominoplasty� If there is a moderate excess below the
umbilicus and little to no excess above,and the umbilicus appears high riding on
Fig. 6. (continued)
High Tension Abdominoplasty 2.0 449

Author's personal copy
the abdomen, then it could be maintained insitu and stretched on its stalk for a couple ofcentimeters� If there is moderate excess of skin below
and above and the umbilicus is relativelyhigh riding, the umbilicus may be floatedinferiorly with release of its stalk, again fora few centimeters� If there is a large excess, above and/or
below the umbilicus, then it must be cir-cumscribed and translocated.
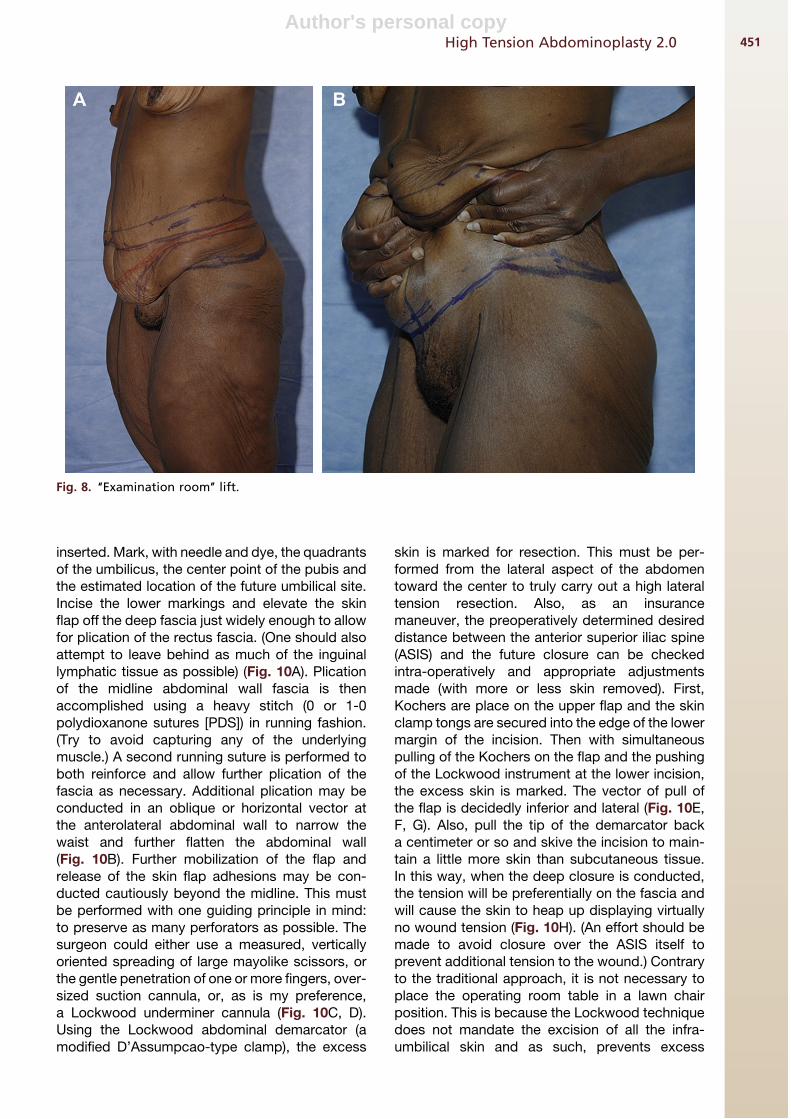
7. Mark the areas for liposuction as neededincluding the hips, waist, pubis, and thighs. Tocheck your surgical plan (markings) and recon-cile the patient’s expectations, simply instruct
the patient to reproduce the desired result byperforming an examination room ‘‘lift’’. Thismaneuver is particularly valuable with thepatient who presents with voluminous skinexcess (Fig. 8).
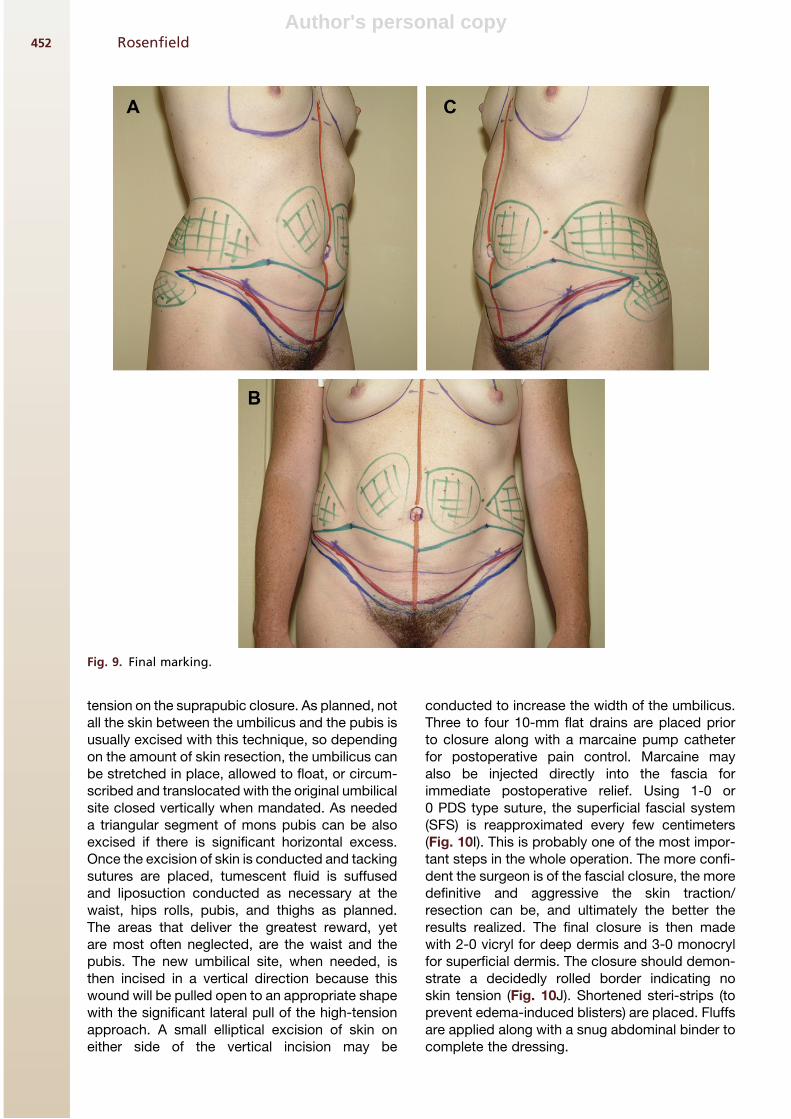
8. Final marking represented in Fig. 9. Greenline: estimated upper incision; red line: definedlocation of final closure; blue line: marked lowerincision.
HLTA: SURGICAL TECHNIQUEProcedure
Place patient supine on warmer, with antiemboliccompression device applied, and Foley catheter
Fig. 7. (A–D) Marking the lower margin of excision. (E) Marking for upper margin of excision.
Rosenfield450
Author's personal copy
inserted. Mark, with needle and dye, the quadrantsof the umbilicus, the center point of the pubis andthe estimated location of the future umbilical site.Incise the lower markings and elevate the skinflap off the deep fascia just widely enough to allowfor plication of the rectus fascia. (One should alsoattempt to leave behind as much of the inguinallymphatic tissue as possible) (Fig. 10A). Plicationof the midline abdominal wall fascia is thenaccomplished using a heavy stitch (0 or 1-0polydioxanone sutures [PDS]) in running fashion.(Try to avoid capturing any of the underlyingmuscle.) A second running suture is performed toboth reinforce and allow further plication of thefascia as necessary. Additional plication may beconducted in an oblique or horizontal vector atthe anterolateral abdominal wall to narrow thewaist and further flatten the abdominal wall(Fig. 10B). Further mobilization of the flap andrelease of the skin flap adhesions may be con-ducted cautiously beyond the midline. This mustbe performed with one guiding principle in mind:to preserve as many perforators as possible. Thesurgeon could either use a measured, verticallyoriented spreading of large mayolike scissors, orthe gentle penetration of one or more fingers, over-sized suction cannula, or, as is my preference,a Lockwood underminer cannula (Fig. 10C, D).Using the Lockwood abdominal demarcator (amodified D’Assumpcao-type clamp), the excess
skin is marked for resection. This must be per-formed from the lateral aspect of the abdomentoward the center to truly carry out a high lateraltension resection. Also, as an insurancemaneuver, the preoperatively determined desireddistance between the anterior superior iliac spine(ASIS) and the future closure can be checkedintra-operatively and appropriate adjustmentsmade (with more or less skin removed). First,Kochers are place on the upper flap and the skinclamp tongs are secured into the edge of the lowermargin of the incision. Then with simultaneouspulling of the Kochers on the flap and the pushingof the Lockwood instrument at the lower incision,the excess skin is marked. The vector of pull ofthe flap is decidedly inferior and lateral (Fig. 10E,F, G). Also, pull the tip of the demarcator backa centimeter or so and skive the incision to main-tain a little more skin than subcutaneous tissue.In this way, when the deep closure is conducted,the tension will be preferentially on the fascia andwill cause the skin to heap up displaying virtuallyno wound tension (Fig. 10H). (An effort should bemade to avoid closure over the ASIS itself toprevent additional tension to the wound.) Contraryto the traditional approach, it is not necessary toplace the operating room table in a lawn chairposition. This is because the Lockwood techniquedoes not mandate the excision of all the infra-umbilical skin and as such, prevents excess
Fig. 8. ‘‘Examination room’’ lift.
High Tension Abdominoplasty 2.0 451
Author's personal copy
tension on the suprapubic closure. As planned, notall the skin between the umbilicus and the pubis isusually excised with this technique, so dependingon the amount of skin resection, the umbilicus canbe stretched in place, allowed to float, or circum-scribed and translocated with the original umbilicalsite closed vertically when mandated. As neededa triangular segment of mons pubis can be alsoexcised if there is significant horizontal excess.Once the excision of skin is conducted and tackingsutures are placed, tumescent fluid is suffusedand liposuction conducted as necessary at thewaist, hips rolls, pubis, and thighs as planned.The areas that deliver the greatest reward, yetare most often neglected, are the waist and thepubis. The new umbilical site, when needed, isthen incised in a vertical direction because thiswound will be pulled open to an appropriate shapewith the significant lateral pull of the high-tensionapproach. A small elliptical excision of skin oneither side of the vertical incision may be
conducted to increase the width of the umbilicus.Three to four 10-mm flat drains are placed priorto closure along with a marcaine pump catheterfor postoperative pain control. Marcaine mayalso be injected directly into the fascia forimmediate postoperative relief. Using 1-0 or0 PDS type suture, the superficial fascial system(SFS) is reapproximated every few centimeters(Fig. 10I). This is probably one of the most impor-tant steps in the whole operation. The more confi-dent the surgeon is of the fascial closure, the moredefinitive and aggressive the skin traction/resection can be, and ultimately the better theresults realized. The final closure is then madewith 2-0 vicryl for deep dermis and 3-0 monocrylfor superficial dermis. The closure should demon-strate a decidedly rolled border indicating noskin tension (Fig. 10J). Shortened steri-strips (toprevent edema-induced blisters) are placed. Fluffsare applied along with a snug abdominal binder tocomplete the dressing.
Fig. 9. Final marking.
Rosenfield452

Author's personal copy
HLTA: RESULTSAssessment of Results
1. The essential advantage of this technique is theability to deliver consistently superior and saferresults:
� The incision is maintained low and hiddenwithin the patient’s clothing.
� More skin can be removed below the inci-sion laterally (which, in effect results ina significant lift of the anterolateral thighs)and centrally (which promotes a lift of thepubis and anteromedial thighs). In effect,a ‘‘virtual’’ posterio-lateral body lift can beaccomplished through an extended anteriorincision (from ‘‘beside to beside’’).
Fig. 10. HTLA surgical technique.
High Tension Abdominoplasty 2.0 453

Author's personal copy
� There is little opportunity for flap ischemiabecause of the maintenance of maximumblood supply: local perforators arepreserved with judicious and discontinuousundermining and its integrity is respectedwith the restraining of any liposuction ordirect fat removal from the flap itself.
� There is less tension at the lower centralabdomen, resulting in a lower incidence offlap ischemia, and a more aestheticallypleasing mild convexity at thehypogastrium.� The excess skin in the horizontal plane of
the abdomen, particularly in the upper
Fig. 11. HTLA with liposuction of the hips and lateral thighs with breast reduction after gastric bypass surgery.
Rosenfield454

Author's personal copy
poles, is more effectively treated with theoblique vector of excision.
2. Any residual fat, particularly within the abdom-inal flap itself, can be treated aggressively, withrelative impunity and equanimity, as a second-stage procedure within 6 to 12 months of theabdominoplasty.
3. Any residual skin resting laterally and posteri-orly can be addressed at a second stage witha posterior extension of the abdominal incisionfor a completion posterior body lift.
4. The residual skin resting at the upper epigastricand subcostal areas can be treated later witheither excision through submammary incisionsor with a proper reverse abdominoplasty.
5. Should the lateral scar rest slightly outside thepatient’s preferred clothing; thescar, under localanesthesia, can be easily moved up or down byexcising the appropriate amount of skin.
Photographic Results
Fig. 11 shows a 46-year-old, gravida 0, para0 woman who was seen after losing 66 kg (145lb) following a gastric bypass. She preferred toavoid a midline scar, but still desired as muchimprovement as possible. She underwent HLTAwith liposuction of the hips and lateral thighs. Amastopexy was accomplished at the samesurgery. Note the presence of the supraumbilicalline of demarcation buttressing the more redun-dant skin above. Therefore, dissection was
deliberately discontinuous in this area and thepatient was informed of the likelihood of someresidual epigastric excess postoperatively. Shehealed without complications. These photographswere taken at about 8 months postoperatively.Note the correction of the abdominal deformity,even in the epigastric area on account of the afore-mentioned oblique vector of its excision. Also, byextending the incision postero-laterally, theHTLA’s body lift effect is realized in the anterolat-eral thigh and buttock areas.
Fig. 12 shows a 57-year-old woman, gravida 2,para 2, who lost about 45 kg (100 lb). She under-went HLTA with liposuction of the hips and thighsand breast reduction. Note the reconstitution of anaesthetic abdomen and how far posteriorly theincision can be extended to realize a rewardingbuttock lift with the patient.
Fig. 13 show a 39-year-old woman, gravida 0,para 0, who lost 90 kg (200 lb) by diet and exercisealone. She demonstrated the most desirable skinenvelope: thin and mobile. The patient underwentHLTA with an extended posterior incision to realizethe more complete excision and lift of the lateraltrunk, while still properly treating the centraltissues. Liposuction of the hips and lateral thighsas well as mastopexy with implantation were alsoaccomplished.
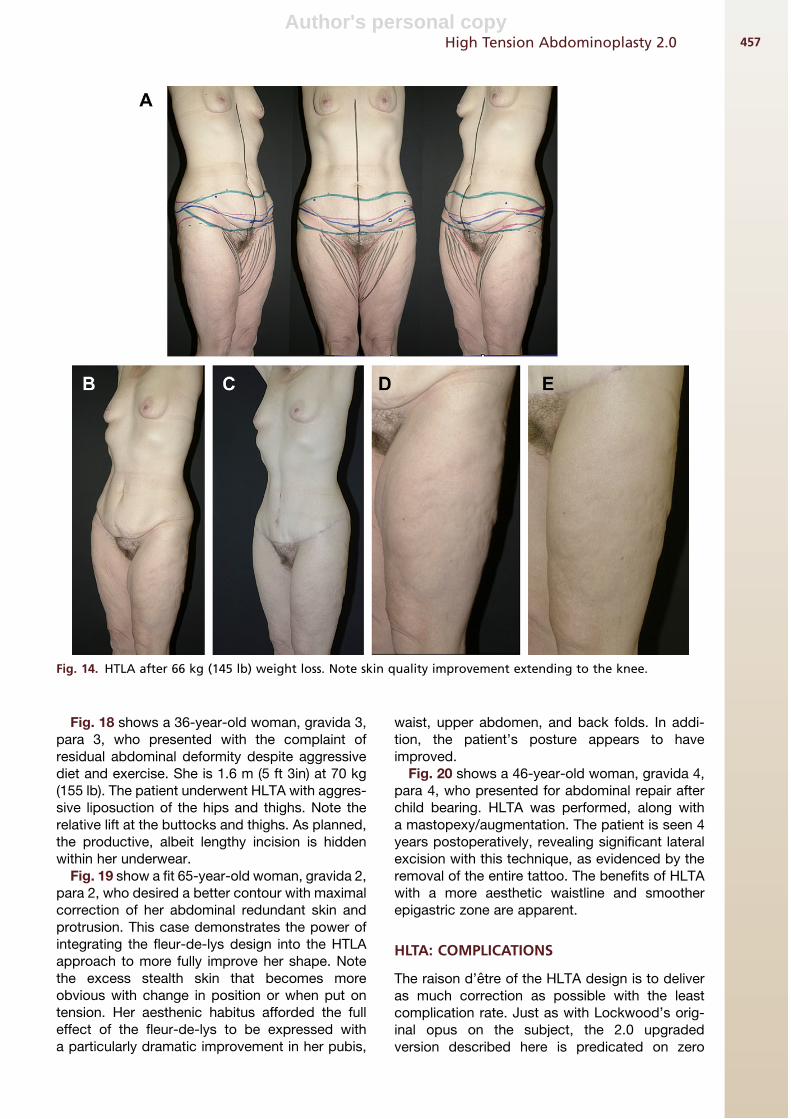
Fig. 14A, B, C, D shows a 43-year-old woman,gravida 0, para 0, who lost 66 kg (145 lb) aftergastric bypass. She subsequently underwentHLTA and is seen here 9 months postoperatively.
Fig. 12. HLTA with liposuction of the hips and thighs and breast reduction.
High Tension Abdominoplasty 2.0 455

Author's personal copy
The hallmarks of the HLTA effects are evident: thescar rests in a hidden position, the suprapubic skinis not overly tight, and the thigh and hip regionshave been lifted. The closeup picture of the thighreveals the qualitative improvement in the skin ex-tending practically to the knee.
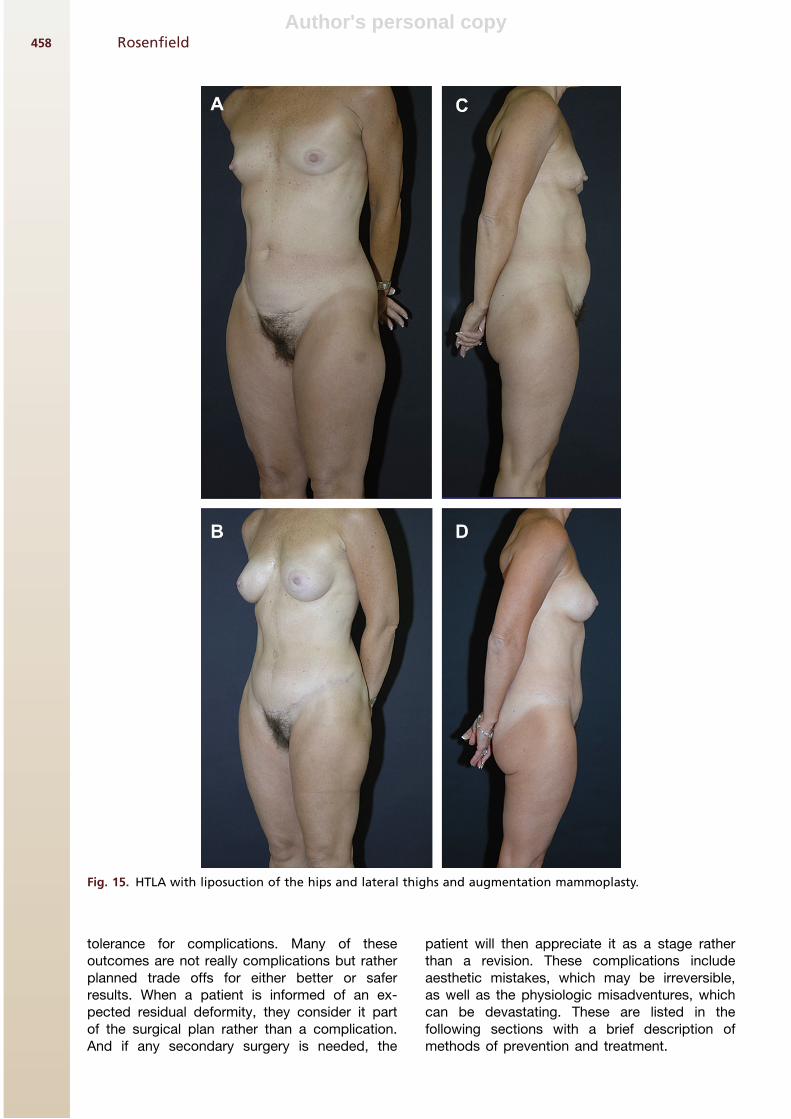
Fig. 15 shows a 50-year-old woman, gravida 1,para 1, who desired rejuvenation of herabdomen. She underwent HTLA with liposuctionof the hips and lateral thighs and augmentationmammoplasty. The pleasing aesthetic of theabdominal repair is realized with a well-placedscar, a not overly tight suprapubic region, andan improved hip/thigh contour. Note the‘‘stealth’’ skin redundancy, visible when thepatient is sitting and bending, and its repair post-operatively. And yet, as can be preordained,
there is residual skin persists in the epigastricarea postoperatively.
Fig. 16 shows a 35-year-old woman, gravida 1,para 1, who presented for correction of herabdominal protrusion. She demonstrated a similarexcess of skin when bending or sitting. HLTA wasperformed with liposuction of the hips and thighs.The benefits of this technique are demonstratedwith the return of a prepregnancy contour. Asplanned, the scar is properly hidden within thepatient’s underclothes.
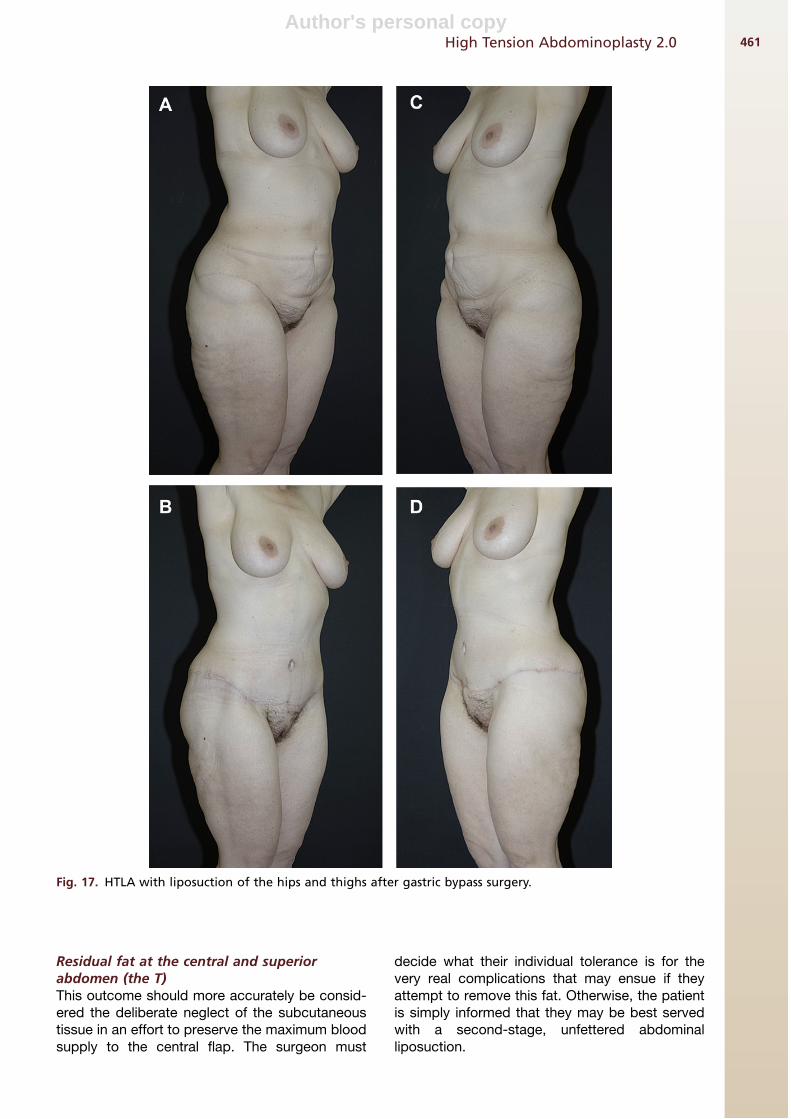
Fig. 17 shows a 43-year-old woman, gravida 0,para 0, who lost more than 45 kg (100 lb) aftera gastric bypass. She elected to have HTLA withliposuction of the hips and thighs. Again note thelift and correction of the lateral thigh/buttockregion through a well-placed scar.
Fig. 13. HTLA with liposuction of the hips and lateral thighs as well as mastopexy with implantation.
Rosenfield456
Author's personal copy
Fig. 18 shows a 36-year-old woman, gravida 3,para 3, who presented with the complaint ofresidual abdominal deformity despite aggressivediet and exercise. She is 1.6 m (5 ft 3in) at 70 kg(155 lb). The patient underwent HLTA with aggres-sive liposuction of the hips and thighs. Note therelative lift at the buttocks and thighs. As planned,the productive, albeit lengthy incision is hiddenwithin her underwear.
Fig. 19 show a fit 65-year-old woman, gravida 2,para 2, who desired a better contour with maximalcorrection of her abdominal redundant skin andprotrusion. This case demonstrates the power ofintegrating the fleur-de-lys design into the HTLAapproach to more fully improve her shape. Notethe excess stealth skin that becomes moreobvious with change in position or when put ontension. Her aesthenic habitus afforded the fulleffect of the fleur-de-lys to be expressed witha particularly dramatic improvement in her pubis,
waist, upper abdomen, and back folds. In addi-tion, the patient’s posture appears to haveimproved.
Fig. 20 shows a 46-year-old woman, gravida 4,para 4, who presented for abdominal repair afterchild bearing. HLTA was performed, along witha mastopexy/augmentation. The patient is seen 4years postoperatively, revealing significant lateralexcision with this technique, as evidenced by theremoval of the entire tattoo. The benefits of HLTAwith a more aesthetic waistline and smootherepigastric zone are apparent.
HLTA: COMPLICATIONS
The raison d’etre of the HLTA design is to deliveras much correction as possible with the leastcomplication rate. Just as with Lockwood’s orig-inal opus on the subject, the 2.0 upgradedversion described here is predicated on zero
Fig. 14. HTLA after 66 kg (145 lb) weight loss. Note skin quality improvement extending to the knee.
High Tension Abdominoplasty 2.0 457
Author's personal copy
tolerance for complications. Many of theseoutcomes are not really complications but ratherplanned trade offs for either better or saferresults. When a patient is informed of an ex-pected residual deformity, they consider it partof the surgical plan rather than a complication.And if any secondary surgery is needed, the
patient will then appreciate it as a stage ratherthan a revision. These complications includeaesthetic mistakes, which may be irreversible,as well as the physiologic misadventures, whichcan be devastating. These are listed in thefollowing sections with a brief description ofmethods of prevention and treatment.
Fig. 15. HTLA with liposuction of the hips and lateral thighs and augmentation mammoplasty.
Rosenfield458

Author's personal copy
Aesthetic Complications
Abdominal scar too longThe scar can only be considered too long if thepatient was not clearly informed of its often requi-site length. The lateral scar is the primary literal‘‘foot print’’ of HLTA. If any tension lifting is attemp-ted at the lateral thigh and hip area, the incision willper force, grow longer. Therefore, the surgeonshould critically evaluate this anatomy preopera-tively and decide, with the patient’s input, whetherthere is enough laxity to warrant extending the inci-sion. Otherwise, experience would indicate that aslong as a scar is of good quality, corrects the defor-mities, and most importantly is hidden, a patient willalways be accepting of a lengthier repair.
Lateral scar too high or too lowIn general, the greater the excess skin present, themore unpredictable the scar placement can be.This outcome is usually caused by poor markingdesign: that is, an over- or underestimation of themagnitude of skin redundancy below the incision.There are several ways to help avoid this problemdepending on the magnitude of redundant skin:
� If there is significant excess below the inci-sion, then there is a real danger of an unpre-dictable scar placement (usually riding toohigh) and the surgeon must be sure duringthe marking, to place the skin on maximumtension and like any good tailor, measure
twice and cut once. That is, recheck yourmarkings, and test them by having thepatient recreate the lift by pulling up theexcess tissues to their desired location.� If there is not a notable excess below the
incision (usually in the thicker, less mobileskin envelope), then the scar could bepredictably too low if too much inferiorskin is removed. The surgeon should there-fore place the skin on less tension whenmarking.� Also, intra-operatively, the aforementioned
preoperative measurement of the distancebetween the fixed ASIS and the desiredlevel of the final wound may be used asa guide. It is best to be conservative withany additional resection (especially in thethicker patient), because the thigh skinbelow may drift inferiorly postoperatively.
Pubis disproportionateThis is usually caused by an inaccurate estimationof the true redundancy of the pubic area. Thesurgeon must put the pubis on maximum stretchduring marking but leave at least 6.5 cm of pubicheight to avoid creating a too tall or short pubis.The pubis can also be left too wide, with thetension surgery potentially worsening thisaesthetic. If necessary, to prevent this appear-ance, a wedge resection of the pubis can be con-ducted simultaneously to the HTLA or at a later
Fig. 15. (continued)
High Tension Abdominoplasty 2.0 459

Author's personal copy
stage. However, overcorrection must be avoidedby maintained a pubic width of at least 6.5 cm.
Poor umbilical closure scarThis problem is often most feared (more by thesurgeon than the patient), but least realized. These
scars uniformly resolve into short, thin, white lines.Rarely, a steroid injection or revision will be neces-sary. Even so, as the patient is made aware, this2.5-cm scar is a small price to pay for the alterna-tive: an ectopic abdominoplasty scar residing toohigh pulling the pubis along with it.
Fig. 16. HLTA with liposuction of the hips and thighs.
Rosenfield460
Author's personal copy
Residual fat at the central and superiorabdomen (the T)This outcome should more accurately be consid-ered the deliberate neglect of the subcutaneoustissue in an effort to preserve the maximum bloodsupply to the central flap. The surgeon must
decide what their individual tolerance is for thevery real complications that may ensue if theyattempt to remove this fat. Otherwise, the patientis simply informed that they may be best servedwith a second-stage, unfettered abdominalliposuction.
Fig. 17. HTLA with liposuction of the hips and thighs after gastric bypass surgery.
High Tension Abdominoplasty 2.0 461

Author's personal copy
Residual skin at upper abdomenThis is really not a unique complication of HLTA.There is a good argument that because this tech-nique delivers a more oblique vector of pull, moreof this redundancy can actually be effaced.
However, the patient with a significant upperabdominal excess (a ‘‘second’’ pannus) should beinformed of its probable persistence postopera-tively. Otherwise, only a fleur-de-lys or reverse ab-dominoplasty can treat this zone definitively.
Fig. 18. HLTA with aggressive liposuction of the hips and thighs.
Rosenfield462

Author's personal copy
Lateral dog earsThe best way to avoid this problem is to fully lipo-suction this area and to intrepidly extend the inci-sion as much necessary.
Epigastric recurrent/residual protrusionOn account of the deliberatly more conservativedissection in the upper abdomen with HLTA, inthe very protuberant patient, an commensuratelymore constrained plication is necessary. Conse-quently, there can be a degree of epigastric recur-rence/residual deformity postoperatively.
Physiologic Complications
SFS stitch abscessesThe stitches used for the tension closure of thefascia are, per force, of large caliber with abundantknots. Therefore, stitch abscesses may arise post-operatively often (surprisingly late) if permanentsuture is used. This problem is far less likely if anabsorbable suture is utilized.
SeromaBecause far less dissection and no central liposuc-tion is conducted with the HLTA, this annoyingproblem should be rare. For the same reason,the concept of flap adhesion stitches is not really
applicable to HLTA. However, when a seromadoes occur, a consistent set of aspirations usuallysolves the problem within a couple of weeks. Theprimary modes of prevention otherwise includemaintaining the web of lymphatic-containingtissue overlying the fascia when elevating theflap and placing multiple drains at least (3).
Deep vein thrombosis and pulmonaryembolismTomes of analysis and advice have been written onthis subject, particularly in the last few years.Clearly, with good patient selection, consistentuse of antiembolism pumps, and early mobilization,the incidence of this problem should remain rare. Asfor chemical prophylaxis, considering thestill unset-tled status of this modality, the surgeon should referto the latest recommendations in the literature.
Skin necrosisThis dreaded complication can occur if thesurgeon goes too far during the surgery: overlyaggressive flap mobilization in an effort to removethe maximum amount of redundant skin (particu-larly from the upper half of the abdomen) and exces-sively zealous flap fat removal (by liposuction ordirect excision) to thin the flap as much as possible.
Fig. 19. HTLA with mastopexy/augmentation.
High Tension Abdominoplasty 2.0 463

Author's personal copy
Unfortunately, the patients who would rightfullyneed these extreme measures to be taken are alsooften the riskiest candidates (high BMI or massiveexcessive skin). And, for all other patients there isno reliable metric to accurately stratify those whowill do well with these more invasive techniques;the surgeon must decide between the proverbialconflicting forces of blood and beauty.
CONCLUDING PRINCIPLES
The key principles with HLTA:
1. HLTA is driven by the concerted effort totreat not only the tissues above the incisionbut also those below. This treatment is asmuch excision of redundancy as it is a far-reachingbodylift throughanalbeitextended
Fig. 20. Fleur-de-lys abdominoplasty with a marriage to the high lateral tension principle.
Rosenfield464

Author's personal copy
anterior incision. The pubis and anterome-dial thighs as well as the hips and anterolat-eral thighs and even buttocks can beaesthetically improved by this technique.
2. This procedure is fundamentally and philo-sophically different in that the skin isconsidered more redundant at the lateraltrunk than in the midline. Therefore, the an-terolateral thigh is treated more effectively.In addition, the redundant upper abdom-inal skin is seen as emanating more fromthe chest and demonstrating more ofa horizontal laxity in opposition to thevertical laxity of the lower pannus. Assuch, the relatively oblique pull of HLTAcan treat this epigastric excess moreeffectively.
3. This approach, in contradistinction to thetraditional abdominoplasty, is not drivenby the usually mandatory excision of allthe skin between the pubis and umbilicus.Therefore, the pubic/median portion ofthe incision can be naturally lower andmore hidden and the closure under lesstension, improving the chances for perprimum healing and a more natural-look-ing result.
4. HLTA often mandates that the incision belonger laterally. However, it is also truethat the longer the lateral incision, thebetter the result. This approach allowsthe excision of a greater extent of skinand more importantly, affords an impres-sive body lift of the surrounding tissues.This balance between scar length andresult must be negotiated with thepatient.
5. As a corollary, if there is a less redundantskin envelope at the lateral thigh, thenHLTA should be tempered and the scarcan and should be shorter.
6. This technique, although often more effec-tive at treating the upper abdominal skinexcess, should still be supplemented bya second-stage reverse abdominoplastyprocedure, when necessary.
7. HLTA is predicated on the preservation offlap blood supply first and foremost. Aspart of this philosophy, for the patientwith a medium to high BMI, the surgeonshould seriously consider a staged lipo-suction of the central and superior abdom-inal flap instead of either liposuction ordirect excision. Only then can a zero toler-ance for skin necrosis be truly practiced.
REFERENCES
1. Pitanguy I. Abdominal lipectomy: an approach to it
through an analysis of 300 consecutive cases. Plast
Reconstr Surg 1967;40:384.
2. Matarasso A. Abdominolipoplasty: a system of classi-
fication and treatment for combined abdominoplasty
and suction-assisted lipectomy. Aesthetic Plast Surg
1991;15:111–21.
3. Lockwood T. High-lateral-tension abdominoplasty
with superficial fascial system suspension. Plast
Reconstr Surg 1995;96:603–15.
4. Gradinger GP, Rosenfield LK, Nahai FR. The art of
aesthetic surgery. St Louis (MO): Quality Medical
Publishing; 2005. p. 2355.
5. Saldanha OR, Pinto EBDS, Mattos WN, et al. Lipoab-
dominoplasty with selective and safe undermining.
Aesthetic Plast Surg 2003;27:322.
High Tension Abdominoplasty 2.0 465