author(s): patrick carter, daniel wachter, rockefeller ... · and adapt it. the citation key on the...
TRANSCRIPT

Author(s):PatrickCarter,DanielWachter,RockefellerOteng,CarlSeger,2009-2010.License:Unlessotherwisenoted,thismaterialismadeavailableunderthetermsoftheCreativeCommonsAttribution3.0License:http://creativecommons.org/licenses/by/3.0/
WehavereviewedthismaterialinaccordancewithU.S.CopyrightLawandhavetriedtomaximizeyourabilitytouse,share,andadaptit.Thecitationkeyonthefollowingslideprovidesinformationabouthowyoumayshareandadaptthismaterial.Copyrightholdersofcontentincludedinthismaterialshouldcontactopen.michigan@umich.eduwithanyquestions,corrections,orclarificationregardingtheuseofcontent.Formoreinformationabouthowtocitethesematerialsvisithttp://open.umich.edu/education/about/terms-of-use.Anymedicalinformationinthismaterialisintendedtoinformandeducateandisnotatoolforself-diagnosisorareplacementformedicalevaluation,advice,diagnosisortreatmentbyahealthcareprofessional.Pleasespeaktoyourphysicianifyouhavequestionsaboutyourmedicalcondition.Viewerdiscretionisadvised:Somemedicalcontentisgraphicandmaynotbesuitableforallviewers.

CitationKeyformoreinformationsee:http://open.umich.edu/wiki/CitationPolicy
Use+Share+Adapt
MakeYourOwnAssessment
CreativeCommons–AttributionLicense
CreativeCommons–AttributionShareAlikeLicense
CreativeCommons–AttributionNoncommercialLicense
CreativeCommons–AttributionNoncommercialShareAlikeLicense
GNU–FreeDocumentationLicense
CreativeCommons–ZeroWaiver
PublicDomain–Ineligible:WorksthatareineligibleforcopyrightprotectionintheU.S.(USC17§102(b))*lawsinyourjurisdictionmaydiffer
PublicDomain–Expired:Worksthatarenolongerprotectedduetoanexpiredcopyrightterm.
PublicDomain–Government:WorksthatareproducedbytheU.S.Government.(USC17§105)
PublicDomain–SelfDedicated:Worksthatacopyrightholderhasdedicatedtothepublicdomain.
FairUse:UseofworksthatisdeterminedtobeFairconsistentwiththeU.S.CopyrightAct.(USC17 § 107)*lawsinyourjurisdictionmaydifferOurdeterminationDOESNOTmeanthatallusesofthis3rd-partycontentareFairUsesandweDONOTguaranteethatyouruseofthecontentisFair.Tousethiscontentyoushoulddoyourownindependentanalysis todeterminewhetherornotyourusewillbeFair.
{Contentthecopyrightholder,author,orlawpermitsyoutouse,shareandadapt.}
{ContentOpen.Michiganbelievescanbeused,shared,andadaptedbecauseitisineligibleforcopyright.}
{ContentOpen.MichiganhasusedunderaFairUsedetermination.}

Advanced Emergency Trauma Course
GhanaEmergencyMedicineCollaborativePatrickCarter,MD∙DanielWachter,MD∙RockefellerOteng,MD∙CarlSeger,MD
GastrointestinalandGenitourinaryTrauma
Presenter:DanielWachter,MD

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Lecture Objectives
ReviewrelevantGIandGUanatomy UnderstandpatternsandpathophysiologyoftraumaticGIandGUinjury
ExplainthediagnosticmodalitiesappropriateforparticulartraumaticGI/GUconditions
DescribeanalgorithmicapproachtoGIandGUtraumaticinjuryevaluationandmanagement
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
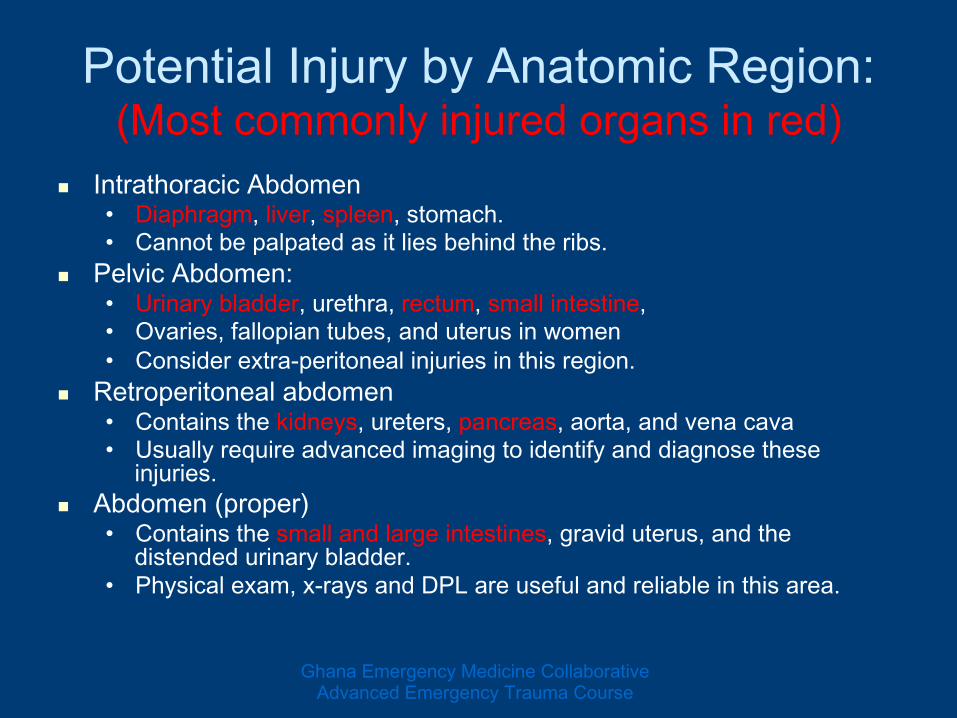
Potential Injury by Anatomic Region: (Most commonly injured organs in red)
IntrathoracicAbdomen• Diaphragm,liver,spleen,stomach.• Cannotbepalpatedasitliesbehindtheribs.
PelvicAbdomen:• Urinarybladder,urethra,rectum,smallintestine,• Ovaries,fallopiantubes,anduterusinwomen• Considerextra-peritonealinjuriesinthisregion.
Retroperitonealabdomen• Containsthekidneys,ureters,pancreas,aorta,andvenacava• Usuallyrequireadvancedimagingtoidentifyanddiagnosetheseinjuries.
Abdomen(proper)• Containsthesmallandlargeintestines,graviduterus,andthedistendedurinarybladder.
• Physicalexam,x-raysandDPLareusefulandreliableinthisarea.
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

Gastrointestinal Anatomy
LadyOfHats(Wikipedia)
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

Pathophysiology BluntTraumaticInjury:Threeinjuriespatterns• RapidDeceleration–shearinginjury
Injureshollow,solid,visceralorgansorvascularstructures• Crush
Abdominalanteriorlyandvertebraeorribsposteriorly.• ExternalCompression
Canoccurthroughouttheabdomen Maycausediaphragmaticorhollowviscousrupture
PenetratingInjury–stabsandprojectiles
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
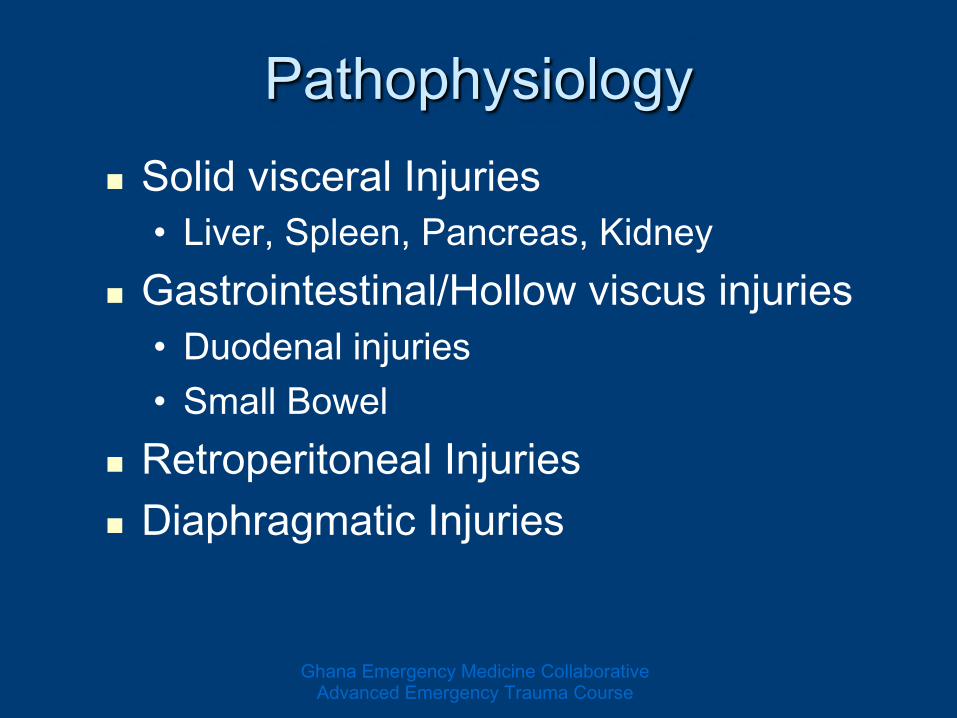
Pathophysiology of Specific Blunt Injuries
SolidvisceralInjuries• Liver,Spleen,Pancreas,Kidney
Gastrointestinal/Hollowviscusinjuries• Duodenalinjuries• SmallBowel
RetroperitonealInjuries DiaphragmaticInjuries
Pathophysiology
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

Diagnostic Evaluation of Penetrating Trauma: Stab Wounds
Unstablepatientsorthosewithperitonitisshouldbeconsideredemergentlyforlaparotomy.
Stablepatientscanundergolocalwoundexploration.Ifnoperitonealviolationisdetected,serialexaminationsareperformed.
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

Stab Wound Diagnosis DiagnosticPeritonealLavage(DPL)orFocusedAbdominalSonographyforTrauma(FAST)• FASTscanispreferredduetohigherpositivepredictivevalue,butbothareacceptable.• FurtherdiscussionofDPLandFASTfollows
PerformAP/LateralChestx-rayfordiaphragmatic,mediastinalorlunginjury.
CTscancanbeconsidered,butisnotalwaysmandatoryinanteriorabdominalstabwounds
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourseGhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
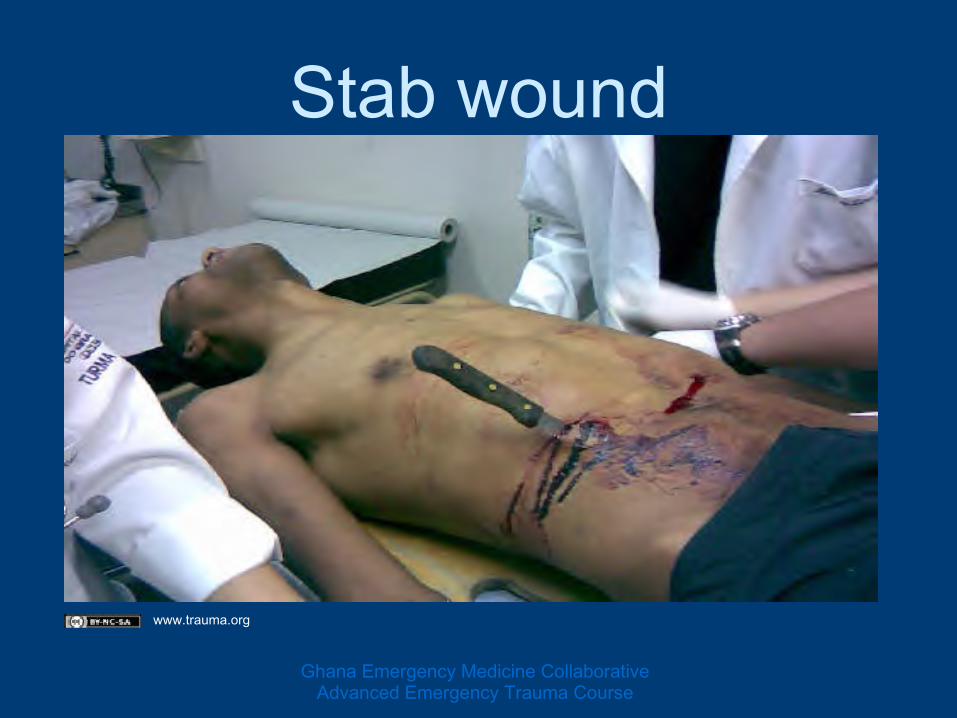
Stab wound
www.trauma.org
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

Unstablepatientssufferingprojectilewoundstotheabdomenshouldproceedemergentlytotheoperatingtheater.
Thespecificlocationofprojectilefragmentscanbeinvestigatedafterstabilizationisachieved.
StablepatientssufferingprojectilewoundstotheabdomenshouldundergoCTscanningandserialexaminations.
Diagnostic Evaluation of Penetrating Trauma: Projectile Wounds
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

GSW to RUQ
www.trauma.org
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

www.Trauma.org
Blunt Traumatic Injury
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

Evaluation after Blunt Abdominal/Pelvic Injury
PhysicalExamination DiagnosticImaging• Plainradiography• Ultrasound• CTscan
DiagnosticProcedures
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

Physical Exam: Abdomen
Observefordistension Listenforbowelsounds Palpatefortenderness “GrayTurner”signisecchymosisofflankfromretroperitonealinjury
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

Grey-Turner Sign
http://en.wikipedia.org/wiki/File:Hemorrhagic_pancreatitis_-_Grey_Turner%27s_sign.jpg
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

Physical examination: Pelvis
CompresstheAnteriorSuperiorIliacCreststoassessforpainormovementonPAcompression.
CompresstheAnteriorSuperiorIliacCrestslaterallyforpainormovement.
Palpateatthepubicsymphisisfortenderness,step-offorcrepitance.
Pelvicfracturearepainfulandusuallydemonstratetenderness. GhanaEmergencyMedicineCollaborative
AdvancedEmergencyTraumaCourse

Check the Back/Rectal Log-rollthepatientwhileobservingspinalprecautions.
Lookandpalpateforstep-offs,abrasions• Bulletholesorstabwounds
Performrectalexamforgrossbloodbonypelvicfragmentsor“high-riding”prostate.
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

www.Trauma.org
CXR – Diaphragmatic Rupture
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

http://ejournal.afpm.org.my/Assets/factory_worker_chest_radiograph2.jpg
CXR – Viscus Rupture FreeAirbelowthediaphragm
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

FAST Exam FocusedAbdominalSonographyinTrauma
4viewsoftheabdomentolookforfluid.• RUQ/Morrison’spouch• Subxiphoid–viewofheart• LUQ–viewofsplenorenaljunction• Bladder–viewofpelvis
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

FAST Haslargelyreplaceddeepperitoneallavage(DPL)
Bedsideultrasoundlookingforbloodcollectioninanunstablepatient.
Ifthepatientisunstableandabloodcollectionisfound,proceedemergentlytotheoperatingtheater.
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

FAST Sensitivityof94.6% Specificityof95.1% Overallaccuracyof94.9%inidentifyingthepresenceofintraabdominalinjuries.• Yoshil:JTrauma1998;45
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

FAST Right Upper Quadrant -Morrison’s Pouch
BetweentheliverandkidneyinRUQ. Firstplacethatfluidcollectsinsupinepatient.
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

FAST Exam - RUQ
Source: University of Louisville ED website www.louisville.edu/medschool/emergmed/ultrasoundfast.htm
Source: University of Louisville ED website www.louisville.edu/medschool/emergmed/ultrasoundfast.htm
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

FAST - Subxiphoid
Evaluateforpericardialfluid Viewthroughliver• TranshepaticorParasternal
Searchesforfluidbetweenheartandpericardium
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

FAST - Subxiphoid
Source: University of Louisville ED website www.louisville.edu/medschool/emergmed/ultrasoundfast.htm
Source: University of Louisville ED website www.louisville.edu/medschool/emergmed/ultrasoundfast.htm
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

FAST – Left Upper Quadrant
Viewbetweenthespleenandkidney Anotherdependentplacethatfluidcollects Alsoseediaphragminthisview
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

FAST - LUQ
Source: University of Louisville ED website www.louisville.edu/medschool/emergmed/ultrasoundfast.htm
Source: University of Louisville ED website www.louisville.edu/medschool/emergmed/ultrasoundfast.htm
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

FAST – Bladder View
EvaluatesforfluidinthepouchofDouglas• Posteriortobladder.
Dependentpotentialspace.
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

FAST – Bladder View
Source: University of Louisville ED website www.louisville.edu/medschool/emergmed/ultrasoundfast.htm
Source: University of Louisville ED website www.louisville.edu/medschool/emergmed/ultrasoundfast.htm
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

Interpret this FAST Image:
Source: University of Louisville ED website www.louisville.edu/medschool/emergmed/ultrasoundfast.htm
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

Diagnostic Procedures Diagnostic peritoneal lavage
• Bedside test for expeditious discovery of free peritoneal blood.
• Used in multiply injured, altered mentation or to more closely investigate those whose exam is confounded by pelvic or thoracic injuries.
• Semi-open technique is preferable to percutaneous technique
• Performed at infraumbilical site unless the patient is pregnant or a large pelvic hematoma is suspected.
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

Diagnostic Peritoneal Lavage
DPLmustnotdelaytransporttotheoperatingtheaterwhenemergentlaparotomyisneededregardlessofDPLfindings.
ComplicationsofDPLinclude:• Bleeding,• Infection• Intra-abdominalinjuries• False-positiveleadingtounnecessaryexploratorylaparotomy.
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

DPL: Findings Mandating Surgery
Greaterthan10mLgrossbloodoncatheterinsertion,orgreaterthan15-20mLonaspiration
Followingperitoneallavagewithoneliter(1L)crystalloid:• Greaterthan100,000RBC/mm3,or• Greaterthan500WBC/mm3,or• Bile,foodmatter,highamylase,bacteria
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

Pelvic Fractures Canbestableorunstable. Ifunstable,theymustberepairedbyorthopedics.
Mayhavesignificantbleedingfromvesselsonpelvicfloor.
Pelvicfracturesshouldbestabilizedwithasheetwrappedtightlyaroundthepelvis.
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

Pelvic Fracture PelvicRingFractureshaveahighassociationwithabdominal/pelvicinjuries
PelvicFracture–“OpenBook”
http://emedicine.medscape.com/article/394515-overview
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

www.Trauma.org
Pelvic Fracture
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

Improvised Pelvic Binder
Maximalcompressionisattheheightofthegreatertrochanters
http://www.aaos.org/news/aaosnow/jul09/clinical8-3.gif
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

After Binder Application
www.trauma.org
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
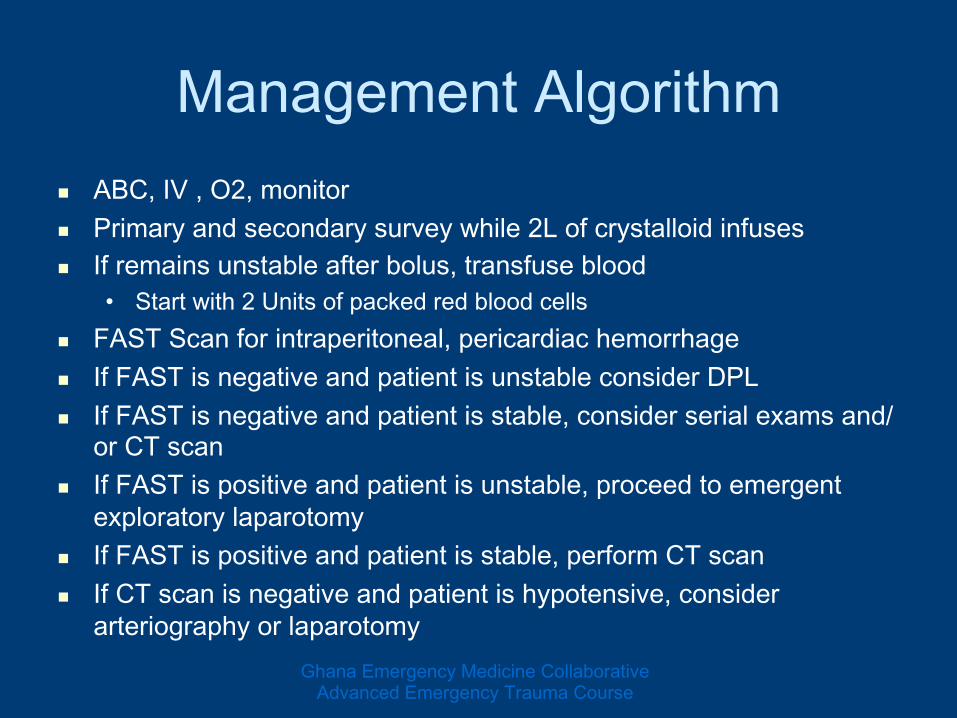
Management Algorithm ABC,IV,O2,monitor Primaryandsecondarysurveywhile2Lofcrystalloidinfuses Ifremainsunstableafterbolus,transfuseblood• Startwith2Unitsofpackedredbloodcells
FASTScanforintraperitoneal,pericardiachemorrhage IfFASTisnegativeandpatientisunstableconsiderDPL IfFASTisnegativeandpatientisstable,considerserialexamsand/orCTscan
IfFASTispositiveandpatientisunstable,proceedtoemergentexploratorylaparotomy
IfFASTispositiveandpatientisstable,performCTscan IfCTscanisnegativeandpatientishypotensive,considerarteriographyorlaparotomy
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

When to Consult Surgery Following Abdominal Trauma
Clinicallyunstable• Abnormalvitalsignsorpoorgeneralappearancewithoutexternalhemorrhagetoaccountforinstability
Peritonealfindingsonexam• Severetenderness,reboundorguarding
Highriskofassociatedsignsandinjuries• Pelvicfractures,lumbarspinefractures,lowerribfractures,“Grey-Turner”or“Cullen”Sign,Seat-BeltSign
Patientcannotbeadequatelyevaluated:• Alteredmentalstatus,languagebarrier,age(youngoradvanced),significantheadorneckinjury.
PositiveDPL,FASTscanorfree-aironplainradiographs
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

Penetrating Abdominal Trauma Miscellaneous Points
Evisceration• Proceedtotheoperatingtheaterorreducetheomentumwithemergentsurgicalconsultation.
Penetratingobjectsshouldnotberemovedexceptinproximitytodefinitivecare.• Pre-maturelyremovingtheobjectmayleadtoexsanguinationifitistamponadingapotentialvasculardisaster.
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

Genitourinary Trauma
GeneralAnatomyReview• UpperGU:kidneys,pelvocalicealsystem,andureters• LowerGU:bladder,urethra,externalgenitalia
PathophysiologyofTraumaticInjury• BluntTraumaticInjury
RapidDecelerationConsideration PediatricConsiderations
• PenetratingInjuryGhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

GU Trauma Physical Examination
Examineforbloodattheurethralmeatus. Bloodpresentshouldraiseconcernforpelvicfracture.
Foleyshouldnotbeplaceduntilaretrogradeurethrogramhasbeenperformed.
Aretrogradeurethrogramorcystograminastablepatientwhohasbloodattheurethralmeatusorevidenceofurethralorbladderinjuryfrompenetration.
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

Evaluation for Traumatic GU Injury PhysicalexamforGUinjuriesisoflimitedvalueinobtainingdetailedoroperative-planninginformation• Urinedipandmicroscopy• RectalExamforbonyprotrusion,tenderness,high-ridingprostate,boggyprostate
• Examineforbloodattheurethralmeatus,scrotalhematomaandperinealecchymosis
Indicationsforimaging• Grosshematuria• Microscopichematuriawithhemodynamicinstability• Persistentmicroscopichematuria(serialurineanalysis)• Hemodynamicinstabilitywithhistoryofsignificantdecelerationmechanism• However,microscopichematuriainaclinicallystablepatientisrarelyassociatedwithfindingsonimaging.
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

CT Scanning in GU Trauma CTscanoftheabdomenandpelviswithIVcontrast• CTscanispreferredoverintravenouspyelogram(IVP)inrenalinjuries• Imagingismoredetailed,sensitiveandmaydetectotherintraabdominalinjuriesorurinecollections
InthepresenceofpenetratingflanktraumaIV/PO/PR,“triplecontrast”CTscanisthepreferredmodality
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourseGhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

Further GU Trauma Imaging Intravenouspyelogram(IVP)• Contrastdyeclearedviathekidneysprovidesagoodindicationofbilateralrenalfunctionifureteralinjuryisconsidered.
• CanbeusedwhenrenalinjuryissuspectedandCTscanisnotavailable,buttestcharacteristicsareinferiortoCTscanning.
• AbnormalIVPisanindicationforCTscan,angiographyorsurgery. Ultrasonography• UltrasonographyisoftenreadilyavailablebutdoesnotofferthesensitivityofCTscanning
• RenalimagingisperformedroughlybytheFASTexaminationbutmightdetectrenallacerationswithhematomaformationorurinomas.
Radionuclideimagingisnotindicatedintheinitialevaluationforrenaldamage.
Retrogradeureterogramisnotperformedintheemergencysetting.
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

Normal Bladder vs. Ruptured Bladder
http://img.medscape.com/pi/emed/ckb/emergency_medicine/756148-821994-828251-1375001.jpg
http://img.medscape.com/pi/emed/ckb/emergency_medicine/756148-821994-828251-1374998.jpg
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Genitourinary Injuries UrethralInjuries• Almostexclusivelyinmales• Anteriorurethrainjuryusuallycausedbystraddleinjury• Posteriorurethrainjuryusuallycausedbypelvicfracture• Urologyconsultation,bladderdrainagewithsuprapubiccatheteranddelayedrepair
TesticularandScrotalInjuries–radionuclidestudyfortesticularviability.Considersurgicalexploration
PenileInjuries–associatedwithurethralinjuries,causedbyrupturedBucks’fasciaandcorpuscallosumfromtraumaduringerection• 90%resolvespontaneously• 10%requiresurgeryforhematomaevacuation
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

Genitourinary injuries RenalInjuries–frequentlydiagnosedbyCTandlikelynotanisolatedinjury• Managementinvolvessurgery,urologyandangiography• RenalContusion• RenalLaceration• PedicleInjury• RenalRupture• RenalPelvicRupture
UreteralInjuries–rareduetowell-protectedlocation
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

Bladder Injuries Ifimagingisunavailable,canbesuspectedbyinabilitytoaspirateafterbladderirrigation• CTcystoscopyisreplacingtraditionalcystoscopyastheimagingmodalityofchoice• Usuallytheresultofbluntabdominaltrauma• Bladdercontusion–conservativemanagementashematuriaresolves
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

Bladder Rupture Intraperitoneal• Lesscommon• Notusuallyassociatedwithpelvicfractures• Requiressurgicalrepair
Extraperitoneal• Morecommon• Associatedwithpelvicfractures• Initialconservativemanagementisacceptable• Delayedcystogramin7-10daysaslongaspatientisabletovoidwithorwithoutfoleycatheter Unlesshematuriacontinuesorpelvichematomaforms
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

Key Points of GU Trauma GUinjuriesarehighlyassociatedwithadditionalabdominal/pelvicinjuries
Lookforlowerabdominal/flank/genital/backecchymosisoredema
Elicitahistoryofinabilitytovoidfollowinginjury Exploreforhematuria Consideradvancedimaging Involvegeneralandspecialistsurgeonsfordefinitivemanagementandtoguidethediagnosticevaluation
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

Special Cases PenetratingTraumatotheFlank• Scapulartiptoiliaccrest,betweenanteriorandposteriorAxillarylines• Pathophysiology–canviolateretro-andintra-peritonealspaces• ClinicalFeatures–
Flankecchymosis,hematuria,abdominaltenderness,CVAtenderness,orUNDIFFERENTIATEDHYPOTENSION
• Diagnosis–triplecontrastCT(IV/PO/PRcontrast)• Treatment–
Surgery,angiographyorconservativemeasureareallpossible.
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

Special Cases PenetratingTraumatotheButtocks• Pathophysiology
Canviolateretro-,intra-andextra-peritonealspacesandstructures
GI/GU,vascular,neurologicalandmusculoskeletalstructuresareallatrisk
• Diagnosis–Negativerectalexamdoesnotexcludethediagnosis
CTscanshouldbestronglyconsidered Endoscopyshouldbeavoidedduetopossiblehollowviscusinjuryworseninginthefaceofinsufflation
• Management– Surgicalconsultation Angiographymayalsoberequired.
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Questions?
Dkscully(flickr)