autacoids : receptor- and non receptor-mediated
DESCRIPTION
AUTACOIDS : Receptor- and Non Receptor-Mediated. Therapeutics 201, Learning Unit IV Semester 1, AY 2009-2010 Department of Pharmacology & Toxicology UP College of Medicine July 13, 2009. Autacoids : Agonists, Antagonists. Objectives: At the end of the session, students are expected to: - PowerPoint PPT PresentationTRANSCRIPT
AUTACOIDS : Receptor- and Non Receptor-Mediated
Therapeutics 201, Learning Unit IV Semester 1, AY 2009-2010
Department of Pharmacology & ToxicologyUP College of Medicine
July 13, 2009

Autacoids : Agonists, AntagonistsObjectives:At the end of the session, students are expected to:• Review concepts pertaining to the inflammatory process• Define an autacoid • Describe the different autacoids in terms of
(emphasis on histamine, serotonin, eicosanoids)
1. Distribution/site in the body2. Synthesis/storage/release/metabolism3. Factors that stimulate synthesis, release4. Specific receptors5. Pharmacologic action/effect of agonists, antagonists and
enzyme inhibitors6. Clinical applications
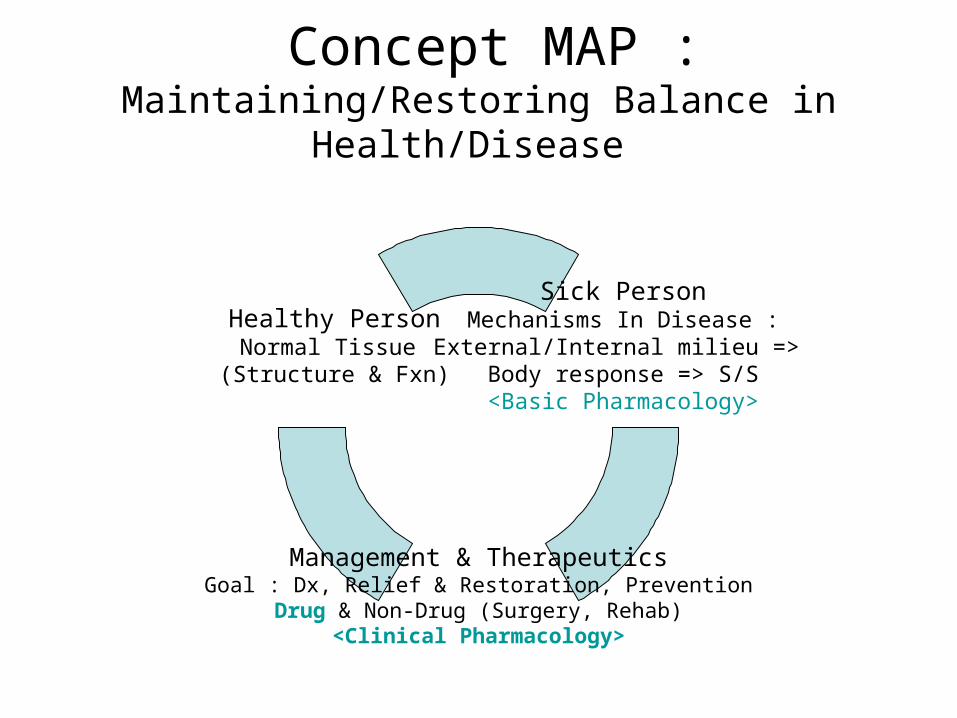
Concept MAP : Maintaining/Restoring Balance in Health/Disease
Sick Person Mechanisms In Disease : External/Internal milieu =>
Body response => S/S<Basic Pharmacology>
Management & TherapeuticsGoal : Dx, Relief & Restoration, Prevention
Drug & Non-Drug (Surgery, Rehab)<Clinical Pharmacology>
Healthy PersonNormal Tissue
(Structure & Fxn)

Clinical illness is produced by:Direct invasion of tissueToxic compounds liberated by the organismThe body’s response to the organism
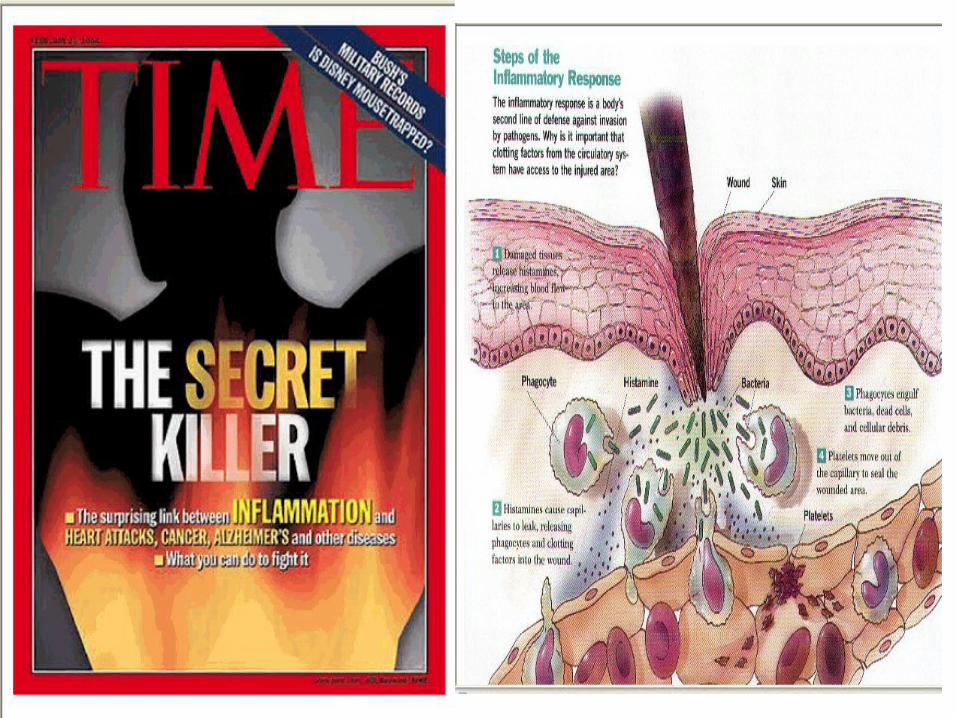

The manifestations of disease are usually produced by various inflammatory mediators produced by:•the initiating organism or•the host
The resulting inflammation may be:•helpful in localising the causative infection or•harmful

Autacoids
“Autacoids” : a varied group of endogenous substances occurring in minute amounts and possessing distinct chemical structure with distinct biologic/ pharmacologic activity
Autos = self; Akos = medicinal agent or remedy (Greek).

AUTACOIDS• Naturally occurring substances• Localized in tissues• Do not normally circulate• Diverse physiological and pharmacological
activities• Differ from hormones and neurotransmitters• Short duration of action• Usually involved in response to injury• Sites of action restricted to the synthesis
area

Examples of autacoids
• Amines: histamine, serotonin (5HT)
• Polypeptides: kinins, oxytocin, angiotensin II, vasopressin, atrial natriuretic factor, endothelins.
• Fatty acids: prostaglandins, leukotrienes, thromboxanes, platelet activating factor (PAF).
• Others: endothelium-derived relaxing factor (NO), cytokines (proteins).

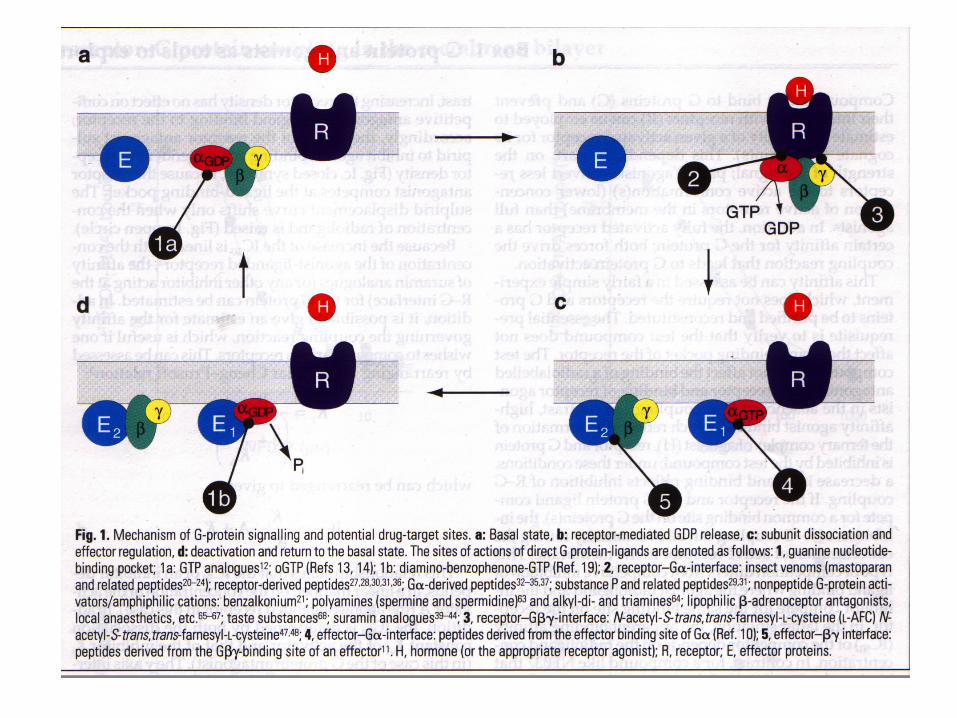
G-protein-coupled receptors (GPCRs)*
• Major target of drug development
• Signalling mechanism & potential target sites for drug action 1. Basal state (“switch off”) 2. Receptor-mediated GDP release 3. Subunit dissociation & effector regulation 4. Deactivation & return to basal state

Histamine (-aminoethylimidazole): a basic amine
COOH
Histamine is formed from histidine by histidine decarboxylase.
Small amounts of histamine formed by bacteria in the gastro-intestinal tract (GIT) is broken down in the gut wall and liver.

Distribution of histamine
• Widely distributed in:
• - bacteria
• - plants
• - animals
• - venoms and stinging fluids (stinging nettle, insect stings, bee venom).

Histamine• Signal involved in local
immune response, also a neurotransmitter
• synthesized by the decarboxylation of histidine
• Either stored or quickly inactivated by histamine-N-methyltransferase and diamine oxidase
• Release of histamine from mast cells is stimulated by IgE antibodies which respond to foreign antigens in the body

Synthesis
• Decarboxylation of amino acid L-histidine catalyzed by pyridoxal PO4-dependent L-histidine decarboxylase.
• Ingested from food or formed by bacteria in the GIT
• Storage sites:– perivascular tissue – mast cell– circulation – basophil (bound to chondroitin SO4)– others – GIT, lungs, skin, heart, liver, neural tissue,
reproductive mucosa, rapidly growing tissues and body fluids

Storage of histamine• ‘Slow-turnover’ histamine is stored as
heparin-histamine complex in cytoplasmic granules in mast cells (lungs, GIT, skin) and basophils.
• ‘Fast-turnover’ histamine is stored in CNS neurons, skin and enterochromaffin-like cells (ECL) of stomach.

Release of ‘Slow turnover’ histamine
Allergic reaction: Antigen combines with IgE antibodies on the surface of mast cells or basophils.
Mechanical–induced degranulation: e.g., scratch.
Non-exocytotic: displacement of histamine from storage site by a drug, e.g., tubocurarine, morphine.
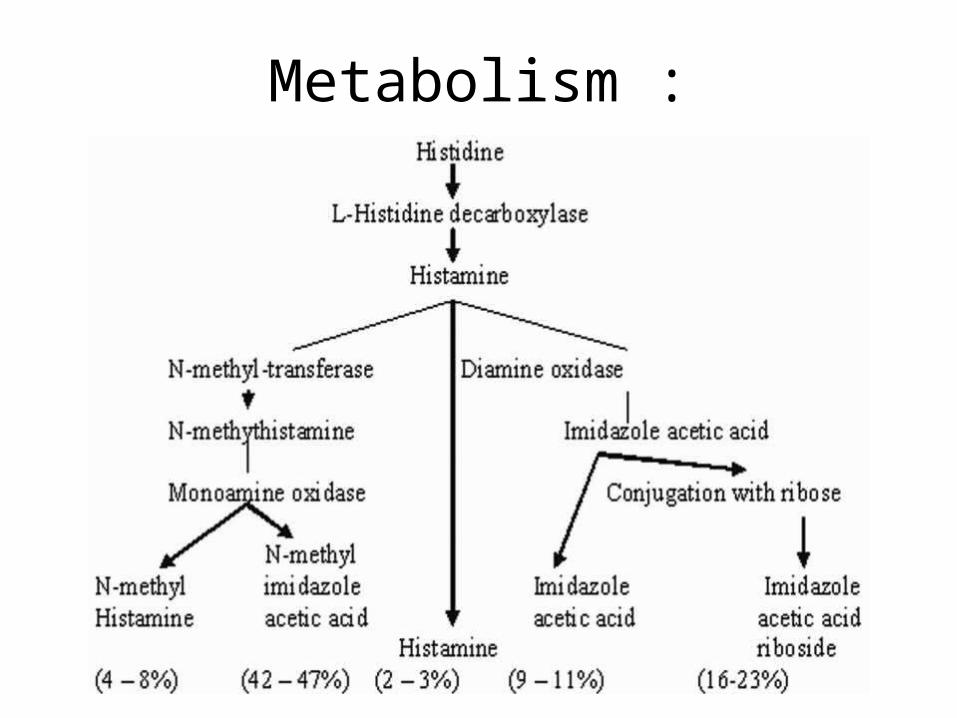
Metabolism :
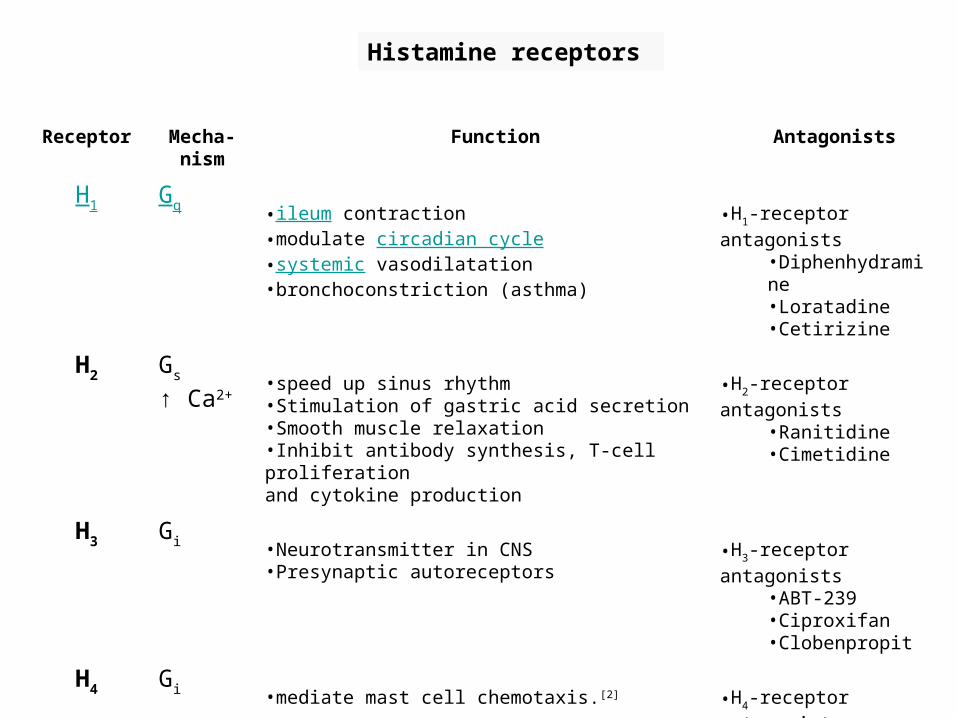
Histamine receptors
Receptor Mecha-nism
Function Antagonists
H1 Gq •ileum contraction •modulate circadian cycle •systemic vasodilatation •bronchoconstriction (asthma)
•H1-receptor antagonists •Diphenhydramine •Loratadine •Cetirizine
H2 Gs
↑ Ca2+•speed up sinus rhythm •Stimulation of gastric acid secretion •Smooth muscle relaxation •Inhibit antibody synthesis, T-cell proliferation and cytokine production
•H2-receptor antagonists •Ranitidine •Cimetidine
H3 Gi •Neurotransmitter in CNS •Presynaptic autoreceptors
•H3-receptor antagonists •ABT-239 •Ciproxifan •Clobenpropit
H4 Gi •mediate mast cell chemotaxis.[2] •H4-receptor antagonists •Thioperamide •JNJ 7777120

Histamine H1-receptors
• Present in endothelium, smooth muscles cells, nerve endings.
• Receptor activation → diacylglycerol and IP3
• Contract smooth muscles: intestine, bronchi
• V/d: direct + NO release → flushing, headache
Vascular permeability : contract endothelial cells in venules)
• Triple response: flush, flare and wheal.
• Stimulate nerve endings: pain, itch; release epinephrine and norepinephrine from adrenal medulla; central excitation.

Triple response (Lewis,1927)
Response Action Effect
1 Loczd red spot “flush”
relaxation of vasc smooth m
vasodilation
2 Swelling or
edema “wheal”
contrxn endoth cells, postcap venl
increased “cap”
perm or leakage
3 Brighter red
halo, “flare”
local axon reflx Indirect vasodi-lation

Pathophysiological action of histamine
• Mediate type 1 hypersensitivity reactions: hives and hay fever.
• Emesis: mediation of motion sickness
• Histamine shock (hypotension): systemic anaphylaxis.
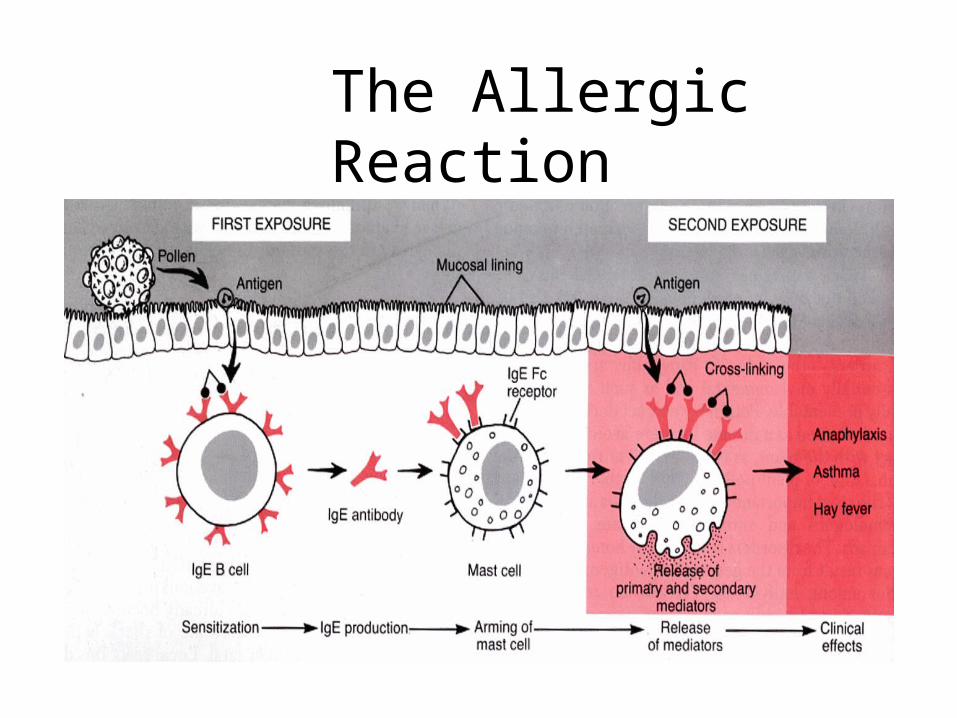
The Allergic Reaction
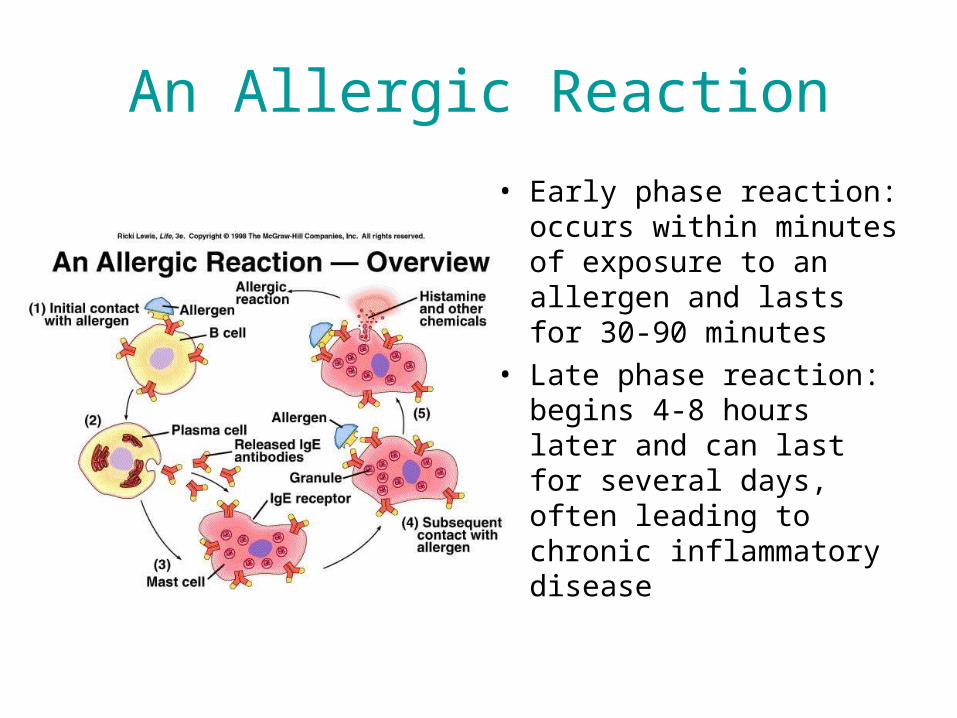
An Allergic Reaction
• Early phase reaction: occurs within minutes of exposure to an allergen and lasts for 30-90 minutes
• Late phase reaction: begins 4-8 hours later and can last for several days, often leading to chronic inflammatory disease

Symptoms
• Allergic Rhinitis
• Conjunctivitis
• Bronchoconstriction
• Urticaria
• Atopic Dermatitis
• Anaphylaxis
http://allergy.healthcentersonline.com/nasalsinus/allergicrhinitis.cfm

Symptoms:anaphylaxis, swelling (skin, mucosa); itching, bronchospasm, hypotension, shock, phospholipase C and A2 activation.
Liberators: large molecules (proteins – egg white, serum, venom, toxins); surface active agents, proteolytic enzymes, drugs etc.
Clinical uses: diagnosis of achlorhydria, diagnosis of pheochromocytoma, and to verify integrity of axon reflexes.

Histamine H2-receptors
Receptor activation: stimulation of adenylyl cyclase cAMP.
• Parietal cells: H+ secretion.
• Vascular smooth muscle cells: vasodilatation
• Heart: force of contraction, HR.
Histamine H3-receptors
• Largely presynaptic receptors in brain, myenteric plexus and other neurons.
• Autoreceptors: negative feedback inhibition of histamine synthesis and release.
• Heteroreceptor: release of norepinephrine, dopamine, serotonin and acetylcholine.
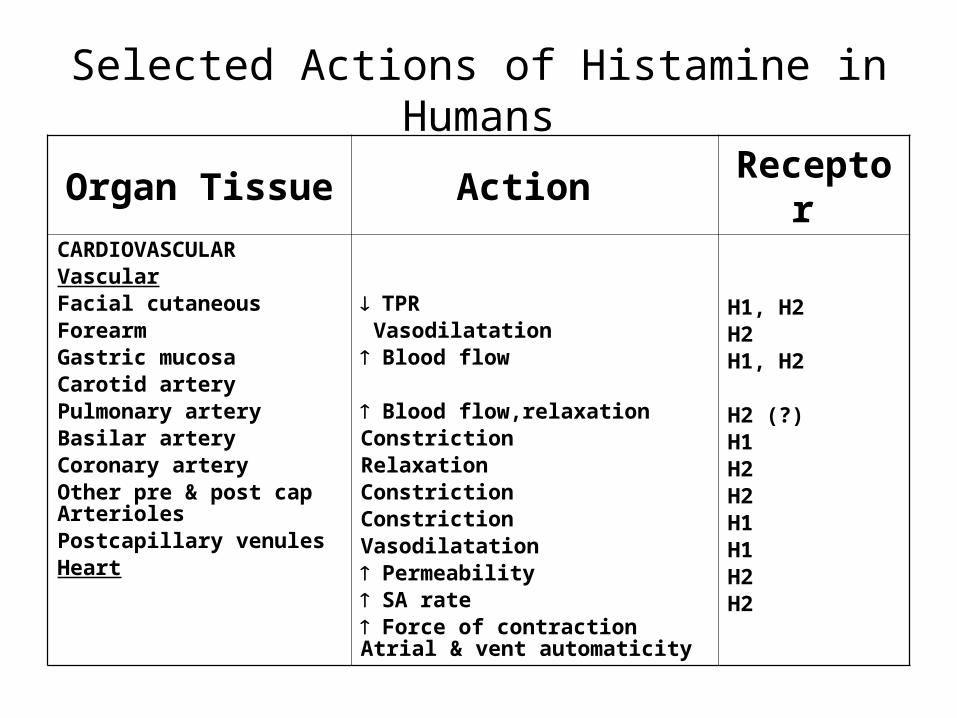
Selected Actions of Histamine in Humans
Organ Tissue Action Receptor CARDIOVASCULARVascularFacial cutaneousForearmGastric mucosaCarotid arteryPulmonary arteryBasilar arteryCoronary arteryOther pre & post cap ArteriolesPostcapillary venulesHeart
TPR Vasodilatation Blood flow
Blood flow,relaxationConstrictionRelaxationConstrictionConstrictionVasodilatation Permeability SA rate Force of contraction Atrial & vent automaticity
H1, H2H2H1, H2
H2 (?)H1H2H2H1H1H2H2

Selected Actions of Histamine in Humans
Organ Tissue Action Receptor
RESPIRATORY
Bronchiolar smooth muscle Contraction (more prominent)
Relaxation
H1
H2
GASTROINTESTINAL
Oxyntic mucosa
GI smooth muscle
Gallbladder smooth muscle
Acid and pepsin secretion, If
Relaxation & Contraction
(more prominent)
Relaxation (?)
H2
H1
H2 (?)
CUTANEOUS NERVE ENDINGS (Sensory)
Pain & itching
(esp to insect bites & needle stings)
H1, H2 (?)
ADRENAL MEDULLA Epinephrine release H1
BASOPHILS Inhibition of IgE – dependent degranulation
H2

Histamine & Agonists : Chemical Structure

Histamine Antagonists
1. Physiologic antagonism – epinephrine
2. Release inhibitors – cromolyn sodium, Beta 2 adrenoceptor agonists
3. Histamine receptor antagonists

Histamine H1-receptor antagonists
• Competitive; some are antimuscarinic, some block -adrenoceptors, and receptors for bradykinin, serotonin, and some have local anesthetic properties.
• First generation antihistamines: lipid soluble → sedative (children may experience excitation)
• Second generation antihistamines: Non-sedative: loratadine

First Generation Antihistamines• Small, lipophilic molecules that could cross the BBB• Not specific to the H1 receptor• Groups:
– Ethylenediamines– Ethanolamines– Alkylamines– Piperazines– Tricyclics
• Common structural features of classical antihistamine– 2 Aromatic rings– Connected to a central Carbon, Nitrogen or CO– Spacer between the central X and the amine– Usually 2-3 carbons in length– Linear, ring, branched, saturated or unsaturated– Amine is substituted with small alkyl groups eg CH3
•

Histamine Antagonists
A. Ethanolamines1. Carbinoxamine maleate2. Clemastine fumarate3. Diphenhydramine HCl4. Dimenhydrinate B. Ethylenediamines1. Pyrilamine maleate2. Tripelennemine HCL/citrate3. PPA C. Alkylamines1. Chlorpheniramine maleate2. Brompheniramine maleate
D. Piperazines 1. Hydroxyzine HCl/pamoate
(long acting) 2. Cyclizine HCl/lactate 3. Meclizine HCl 4. ChlorcyclizineE. Phenothiazines
1. Promethazine HCl
First Generation Agents
Second Generation Antihistamines
• Modifications of the First Generation Antihistamines to eliminate side effects resulted in the Second Generation Antihistamines
• More selective for peripheral H1 receptors• Examples:
– terfenadine– loratadine – cetirizine – mizolastine – astemizole

Second Generation Agents
A. Alkylamines• Acrivastine
B. Piperazines• Cetirizines HCl
C. Piperidines• Astemizole• Levocabastine• Loratadine• Terfenadine• Fexofenadine

“Next” Generation Antihistamines
• Metabolite derivatives or active enantiomers of existing drugs
• Safer, faster acting or more potent than Second Generation drugs
• Examples:– Fexofenadine– Desloratadine– Levocetirizine
Therapeutic Uses:
1. Dermatosis
2. Allergic rhinitis
3. Motion sickness & emesis
4. Parkinson’s disease
5. EPS
6. Insomnia
7. Adverse reactions

Adverse Reactions and Side Effects
• First Generation Drugs:– Anticholinergic CNS interactions– Gastrointestinal reactions– Common side effects: sedation, dizziness, tinnitus, blurred
vision, euphoria, lack of coordination, anxiety, insomnia, tremor, nausea and vomiting, constipation, diarrhea, dry mouth, and dry cough
• Second Generation Drugs:– Common side effects: drowsiness, fatigue, headache, nausea
and dry mouth
• Side effects are far less common in Second Generation drugs
Adverse Effects:
1. CNS : sedation, agitation, nervousness, delirium, tremors, incoordination, hallucinations, & convulsions - common in first generation antihistamines
2. GIT : vomiting, diarrhea, anorexia, nausea, epigastric distress, constipation- dryness of mouth, throat & airway, urinary retention - first generation
3. Headache, faintness4. Chest tightness, palpitations, hypotension5. Visual disturbances6. Hematological - leukopenia, agranulocytosis, HA

Structural Class Prototype Characteristics
First Gen. Agents:
1. Ethanolamine Diphenhydramine
Significant antimuscarinic activity
Sedation, somnolence
Incidence of GI symptoms
Effective in emesis & motion
sickness
2.Ethylenediamine/
Ethylamine
Pyrilamine
Mepyramine
Pyranesamine
Most specific H1 antagonist
Anticholinergic activity
Feeble CNS effects
Somnolence GI s/s common
3. Alkylamine Chlorpheniramine
Pheniramine
Chlorphenamine
Most potent
Not so prone to develop drowsiness
More suitable for older patients
Sedation/CNS stimulation 4. Piperazine Chlorcyclizine Oldest member
More prolonged action
Incidence of drowsiness

Structural Class Prototype Characteristics
Hydroxyzine
Long acting
Widely used for skin allergies
CNS depressant
More prominent antipruritic action
Cyclizine Counters motion sickness (primarily)
Meclizine/Meclozine Counters motion sickness & emesis

Structural Class Prototype Characteristics
5. Phenothiazine Promethazine Anticholinergic
Prominent sedation
Counters motion sickness primarily antiemetic
Second Gen.Agents
1. Piperidine
Terfenadine Highly selective for H1 receptor
Non-sedating
(-) anticholonergic action
(-) pass BBB
incidence of S/E
2. Alkylamine Acrivastine Rapid onset of action (30 mins)
(-) anticholinergic effects
Reduce both wheal & flare response
Potential to penetrate BBB
Skin allergy
Allergic rhinitis
3. Piperazine Cetirizine Rhinitis, urticaria
(-) pass BBB

Histamine H2-receptor antagonists
• Competitive
• Cimetidine, ranitidine, famotidine.

Uses of histamine H2-receptor antagonists
Secretion of H+ and pepsin: more effective on nocturnal (due to histamine) than food-induced (due to ACh, gastrin and histamine) secretion.
- Gastric ulcer: normal H+, mucosal defense.
- Duodenal ulcer: H+, Helicobacter pylori infection?
- Reflux esophagitis
- Zollinger-Ellison syndrome (gastrin producing tumor)

Side effects of histamine H2-receptor antagonists
• Cimetidine (Tagamet) – antiandrogenic (gynecomastia in man), inhibit several cytochrome P450 drug metabolism pathways - hepatic [O] of many drugs (e.g., propranolol, alcohol).
• Ranitidine (Zantac) – 5x more potent than cimetidine; reversible liver dysfunction.
• Famotidine (Pepcid) – 5x more potent than ranitidine.

BIOGENIC AMINESSEROTONIN
Source: plants (banana, pineapple, plums) & animals (mollusks, arthropods, mammals (platelets, not in mast cells).
Biosynthesis: Hydroxylation of tryptophan, then decarboxylation to serotonin(5-hydroxy tryptamine;5-HT). Rapidly absorbed into secretory granules. Accumulated in platelets, degradation by oxidative deamination.
Uses: No therapeutic use. Antagonists are highly useful.

Serotonin Synthesis
PCPA: inhibits TH
5-HT Precursor
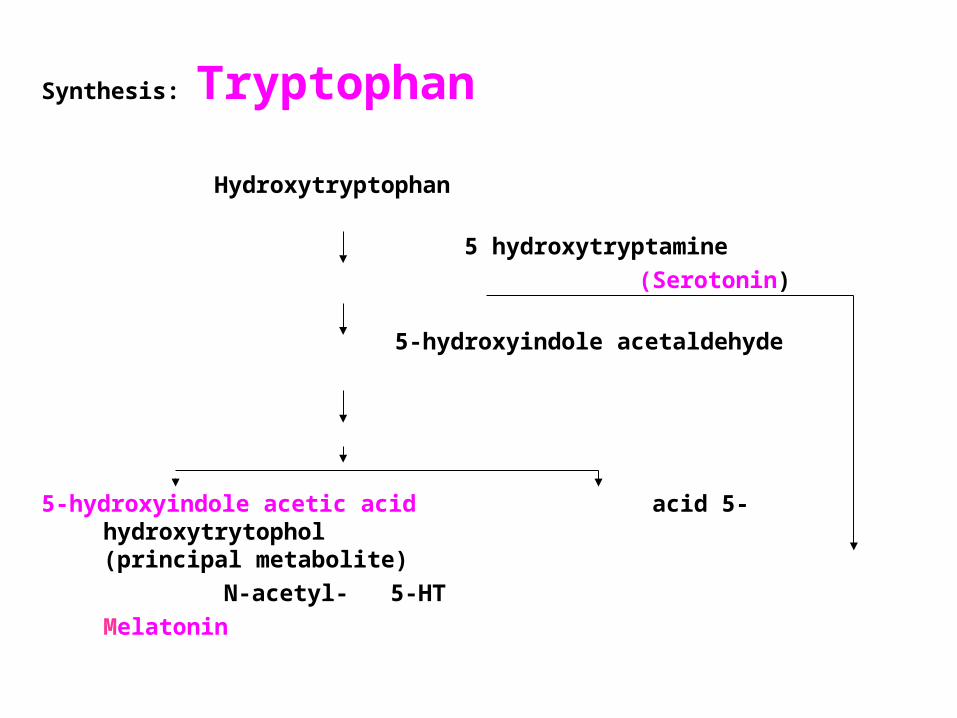
Synthesis: Tryptophan
Hydroxytryptophan
5 hydroxytryptamine
(Serotonin)
5-hydroxyindole acetaldehyde
5-hydroxyindole acetic acid acid 5-hydroxytrytophol(principal metabolite)
N-acetyl- 5-HT
Melatonin

Synthesis and Metabolism
• Competition at the level of brain and neuronal uptake
• Rate limiting enzyme not saturated usually• No end-product negative feedback• 5-OHTr decarboxylase same as DOPA
decarboxylase• 5-OHIAA actively extruded from CNS
(probenecid-sensitive) and excreted in urine.
BIOGENIC AMINESSEROTONIN
Actions • Neurotransmitter in the CNS• Precursor of melatonin• Induces sleep, Intestinal motility• Involved in Temperature regulation• Affects mood and behavior (humans)• Deficiency causes depression• Hemostasis : 5-HT2 receptors → aggregation and
vasoconstriction of platelets• Carcinoid syndrome (tumor of serotonin producing cells)
large amounts released leading to diarrhea, bronchoconstriction and edema
Serotonin Receptors
• At least 15 types and subtypes• Multiple transduction mechanisms• 5HT-1A: role in anxiety/depression• 5HT-1D: role in migraine• 5HT-2: role in CNS various behaviors, and
in cardiovascular system• 5-HT3: role in nausea and vomiting esp.
due to Chemotherapy.
Serotonin Pharmacological Effects
• Respiratory system: bronchoconstriction if asthmatic; stimulation of aortic and carotid chemoreceptors → ↑ RR and minute vol.
• GI tract: small intestine very sensitive to serotonin → intense rhythmic contractions due to direct and indirect (ganglia in wall) effects.
Also stimulates vomiting (5-HT3 receptors on vagal afferents and centrally).

• Cardiovascular system: Multiple direct and indirect effects:
1. Direct vasoconstriction (large arteries) and indirect vasodilation (NO and PGI2 – mediated)
2. Heart: direct inotropic and chronotropic effects3. Reflex mechanisms due to change in BP4. Stimulation of sensory nerve endings in
baroreceptors and in vagal afferents in coronary circulation (Bezold Jarrisch reflex) → bradycardia and hypotension
Serotonin Pharmacological Effects -2

• Pain perception• Sleep/Wakefulness• Various behaviors normal/abnormal:
depression, schizophrenia, obsessive compulsive behavior, etc.
• Neuroendocrine regulation – controls hypothalamic cells involved in release of several anterior pituitary hormones.
Serotonin in the Central Nervous System

Serotonin Agonists• Sumatriptan: 5-HT1D agonist;
contraindicated in patients with angina • Fluoxetine: Selective serotonin uptake
inhibitors for depression and other indications• Buspirone: 5-HT1A agonist for anxiety• Cisapride: 5-HT4 agonist to ↑ GI motility and
decrease G-E reflux (Removed from US market due to fatal arrhythmias)
• LSD: 5HT1A – hallucinogen• Ergot alkaloids: 5-HT1 and 2 and other
receptors

Serotonin Antagonists
• Methysergide and Cyproheptadine. 5HT2 antagonists. In carcinoid, migraine.
• Ketanserin: 5HT2 and Alpha antagonist – used as antihypertensive.
• Ondansetron: 5-HT3 antagonist for chemotherapy induced nausea and vomiting
• Clozapine: 5HT2A/2C antagonist: for schizophrenia.
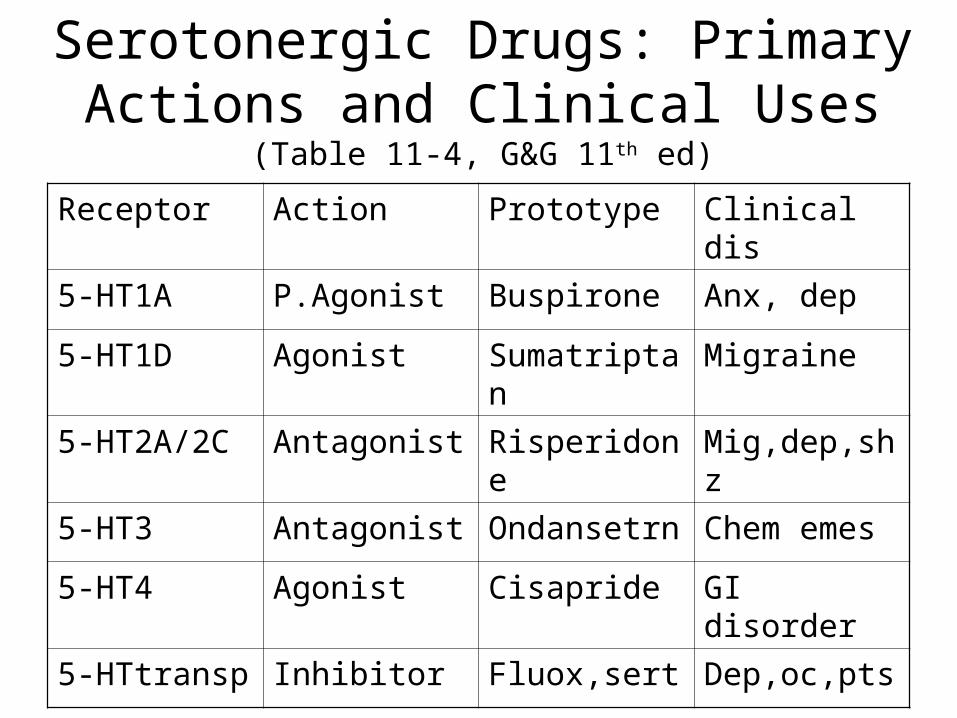
Serotonergic Drugs: Primary Actions and Clinical Uses (Table 11-4, G&G 11th ed)
Receptor Action Prototype Clinical dis
5-HT1A P.Agonist Buspirone Anx, dep
5-HT1D Agonist Sumatriptan Migraine
5-HT2A/2C Antagonist Risperidone Mig,dep,shz
5-HT3 Antagonist Ondansetrn Chem emes
5-HT4 Agonist Cisapride GI disorder
5-HTtransp Inhibitor Fluox,sert Dep,oc,pts

The Pharmacology of INFLAMMATION
Cyclooxygenase Enzyme & Other Tales
The inflammatory reaction
• Complex series of integrated phenomena
• Cellular components & chemical mediators
• Events : arteriolar dilatation, increased vascular permeability, leukocyte interaction with endothelium, diapedesis and migration (chemotaxis)
• Symptoms : dolor, rubor, calor, tumor
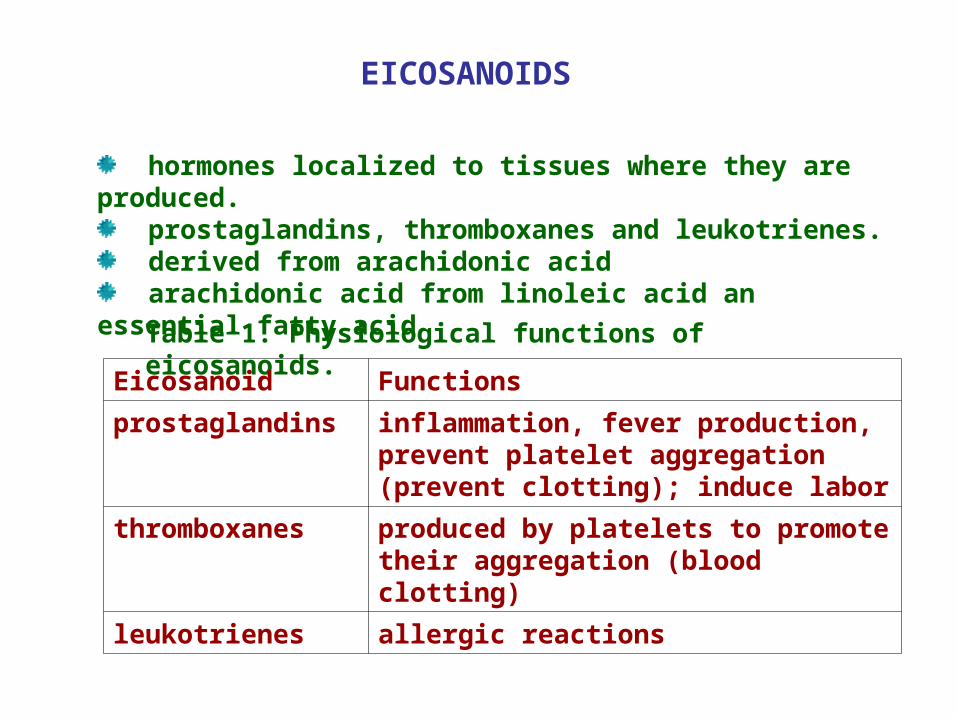
EICOSANOIDS
hormones localized to tissues where they are produced. prostaglandins, thromboxanes and leukotrienes. derived from arachidonic acid arachidonic acid from linoleic acid an essential fatty acid
Table 1. Physiological functions of eicosanoids.
Eicosanoid Functions
prostaglandins inflammation, fever production, prevent platelet aggregation (prevent clotting); induce labor
thromboxanes produced by platelets to promote their aggregation (blood clotting)
leukotrienes allergic reactions

Eicosanoids: The Arachidonic Acid Derivatives
•All C-20 Derivatives of 5,8,11,14 Eicosatetraenoic Acid
•Three classes: Prostaglandins, Thromboxanes, Leukotrienes
•Generated by cleavage of C-2 ester of phosphatidyl inositol in membrane-associated signaling events
•Active at very low concentrations – regulate blood pressure, coagulation, reproduction, pain & fever
•Tissue-specific generation – often opposing actions
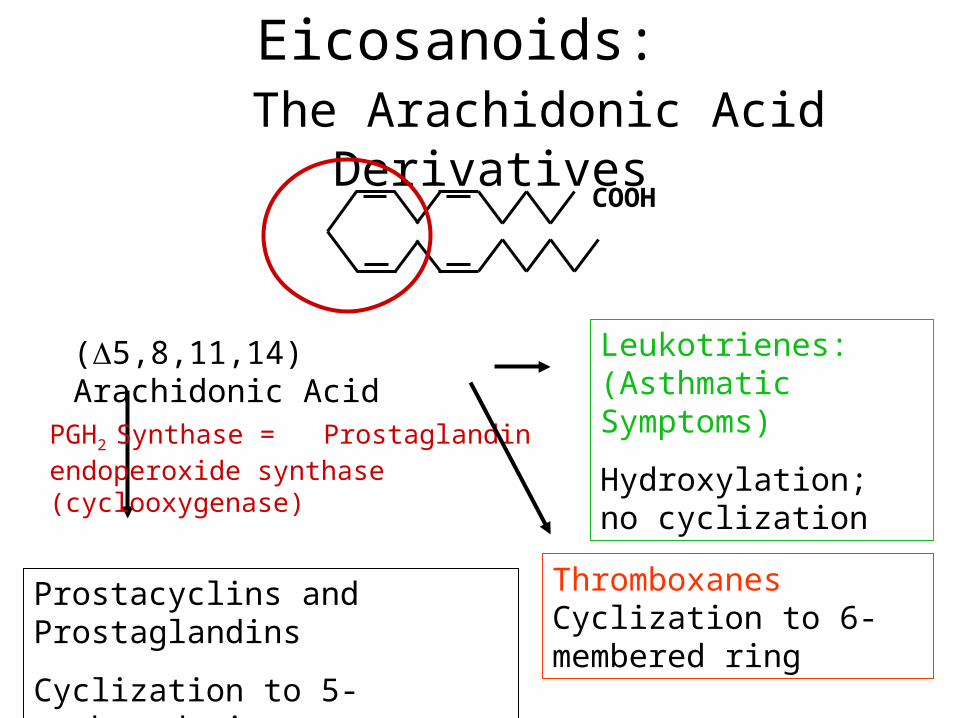
Eicosanoids: The Arachidonic Acid Derivatives
(5,8,11,14) Arachidonic Acid
Leukotrienes: (Asthmatic Symptoms)
Hydroxylation; no cyclization
PGH2 Synthase = Prostaglandin endoperoxide synthase (cyclooxygenase)
COOH
Prostacyclins and Prostaglandins
Cyclization to 5-membered ring
Thromboxanes Cyclization to 6-membered ring

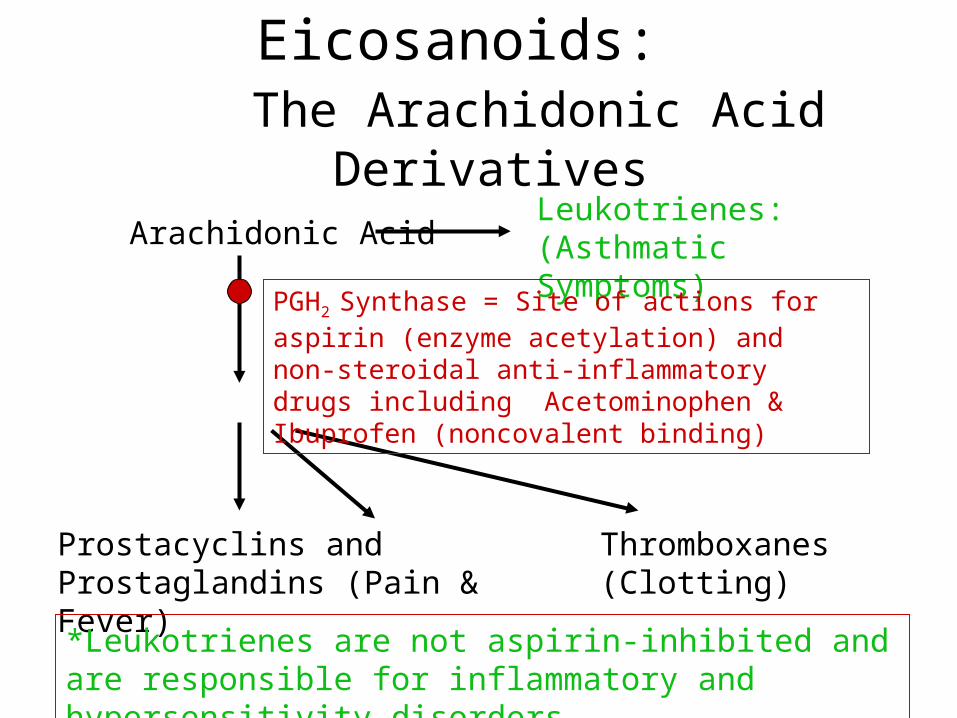
Eicosanoids: The Arachidonic Acid Derivatives
Arachidonic AcidLeukotrienes: (Asthmatic Symptoms)
Prostacyclins and Prostaglandins (Pain & Fever)
Thromboxanes (Clotting)
*Leukotrienes are not aspirin-inhibited and are responsible for inflammatory and hypersensitivity disorders
Cortisteroids- block PLA2 to block the release of Arachidonic Acid
Eicosanoids: The Arachidonic Acid Derivatives
Arachidonic AcidLeukotrienes: (Asthmatic Symptoms)
Prostacyclins and Prostaglandins (Pain & Fever)
Thromboxanes (Clotting)
PGH2 Synthase = Site of actions for aspirin (enzyme acetylation) and non-steroidal anti-inflammatory drugs including Acetominophen & Ibuprofen (noncovalent binding)
*Leukotrienes are not aspirin-inhibited and are responsible for inflammatory and hypersensitivity disorders

Membrane Phospholipid
Phospholipase A2
Arachidonic acid
Lipoxygenase
Leuokotrienes
Cyclooxygenase
PGH2 Thromboxanes in platelets
Prostaglandins in many cells
Conversion of arachidonic acid to eicosanoids.
inhibited by glucocorticoids
inhibited by aspirin, ibuprofen

Inflammatory Conditions : Drug therapy
• Nonsteroidal antiinflammatory drugs (NSAIDs) or aspirin-like drugs
• Corticosteroids
• Drugs modifying acute rheumatic diseases (DMARDs)
• Antigout therapy
ASA : A century hence
• Turn of the century drug
• 1971 : landmark discovery of COX (Vane)
• 1992 : discovery of COX-2, an inducible isoform vs COX-1 which is constitutively expressed

COX-1 and COX 2 : Fraternal Enzymes
• COX-1 : widely distributed throughout the GIT, believed to be gastroprotective (as in kidneys); “housekeeper”
• COX-2 : minimal amts in GIT; detectable in leukocytes, synovium, CNS (site of inflam, fever & pain); inducible, upregulated in response to growth factors & cytokines; “homewrecker”

COX-mediated effects of Aspirin (acetylsalicylic acid)
• Analgesic-antipyretic
• Antiinflammatory
• Antiplatelet
• Adverse Effects : gastric/duodenal ulcers, bleeding, nephropathy

Outline: Bringing concepts together
• Problem : Inflammation (eg, joints)• Pathophysiology : Phases => s/s=>Dx• Cellular Events : Cells, mediators ; enzymes,
receptors =>• Targets for drug action =>• Drugs : Steroids, NSAIDs, DMARDs, & Biologics
(basic pharmacology)• Clinical Pharmacology & Therapeutics :
Evidence of efficacy, safety, suitability

Sick Person(Inflamed Joint: s/s)Pathophysiology: cells,mediators, cytokines etcTargets for drug action
THERAPYGoal: Relief & Restoration, Prevention
Drugs : Symptomatic (Steroids, NSAIDs), Disease-Modifying (Gold, Mtx, Tetracyc), Biologics
Surgery, Rehab/PT, ExerciseAlternative therapies (Acu, Glucosamine, Chondroitin)
Assessment: Proof of Efficacy & Safety
Healthy Person(Normal/Fxnal Joint)
CONCEPT MAP: INFLAMMATION
Antiinflammatory Agents :Nonsteroidal AntiinfIammatory
Drugs (NSAIDs)

NSAIDS: Nonsteroidal Antiinflammatory Drugs
• Prototype: Aspirin (circa 1899)• Mechanism of NSAIDS or aspirin-like
drugs revolves around the enzyme prostaglandin synthase or cyclooxygenase (C0X)
• Shared properties: 1 antiinflammatory, analgesic, antipyretic actions
2 side effects

INFLAMMATION: Friend or Foe?
• Essential for survival versus environmental pathogens and injury (ie, beneficial effect)
• May be exaggerated and sustained for no apparent beneficial reason (ie, problem/ disease)

INFLAMMATION: Stimuli & S/S (review)
• Series of events elicited by numerous stimuli (infectious agent, ischemia, ag-ab interaction, thermal/other physical injury) leading to a characteristic pattern of response
• Accompanied by clinical signs/symptoms: erythema (rubor), pain (dolor), edema (tumor), fever (calor), tenderness (hyperalgesia)

3 Phases of Inflammatory Response (review)
1 Acute transient phase local vasodilation & increased capillary permeability (floodgates open)
2 Delayed, subacute phase
infiltration of leukocytes & phagocytic cells (chemotaxis & diapedesis)
3 Chronic proliferative phasetissue degeneration & fibrosis (± repair)
Proinflammatory AUTACOIDS
• Histamine (early transient phase)
• Bradykinin & serotonin (5-HT)
• Leukotrienes
• Platelet Activating Factor (PAF)
• Eicosanoids : Prostaglandins
• Nitric oxide (NO)

Pharmacologic Properties : LEUKOTRIENES
SITE ACTION EFFECT
CVS Contraction, coronary & pulm, mesent vasc
Hypotension
Airway
Smooth m ;
Bronchial glands;
Bld vessels
Contraction of smooth m;
Stimulate secretion;
Airway narrowing
Inc mucus
Mucosal edema
Inflam & Immunity (major)
Stim aggreg of pmn, neutr adhesion to endoth wall, transendoth migration; stim synth proinflam cytokines
Chemotaxis

Functions of endogenous
leukotrienes
• Inflammatory & Immune Response: LTs are generally proinflammatory
• CysLTs prob dominate during allergic constriction of the airway
Proinflammatory Cells & Factors (review)
• Endothelial Cell (EC), Leukocytes• Cell Adhesion Molecules (CAMs):
E-, P-, L-selectins• ICAM-1, VCAM-1• Cytokines : IL-1, TNFa, chemokines)• Leukocyte integrins• NO synthase (iNOS vs nNOS,eNOS)• Complement factor (C5a)
Natural Antiinflammatory factors => homeostasis
• IL-1 receptor antagonist (IL-1ra)
• Other cytokines & growth factors : transforming growth factor(TGF-ß1), IL-10, Interferon gamma
• Targets for novel antiinflammatory agents
Lipid-Derived AUTACOIDS
EICOSANOIDS & PAF

Products of COX Pathway: Active Compounds
• PGD2
• PGE1, PGE2
• PGF2a
• PGI2 via prostacyclin synthase
• TXA2 via thromboxane synthase

Prostaglandin Receptor Diversity
• Distinct receptors for specific activity• Subtypes/Agonists/G protein/2nd mssgr
DP PGD2 Gs cAMP EP1 PGE2 Gq (?) Ca2+;IP3/DAG (?)EP2 PGE2 Gs cAMP EP3 PGE2 Gi,Gs,Gq all of aboveEP4 PGE2 Gs cAMP FP PGF2a Gq IP3/DAG/Ca2+
IP PGI2(E2) Gs cAMP TP TXA2,H2 Gq IP3/DAG/Ca2+
Endogenous Eicosanoids: Possible Fxns in Physiol/Pathol Processes
• Platelet-vessel wall interaction, hemostasis• Reproduction & Parturition• Vascular and pulmonary smooth muscle tone
modulation• Renal blood flow modulation, urine regulation,
renin• Inflammatory and Immune Response• Malignancy (eg, colon, breast ca)

Therapeutic Uses of Eicosanoids
• Induction of labor at term : PGE2 or PGF2a• Gastric cytoprotection: PGE1 analog
(misoprostol)• Impotence: PGE1 (alprostadil)• Maintenance of PDA: PGE1 in some neonates
with congenital heart disease• Primary pulmonary hypertension: PGI2
(epoprostenol)

Outline: Bringing concepts together
• Problem : Inflammation (eg, joints)• Pathophysiology : Phases => s/s=>Dx• Cellular Events : Cells, mediators ; enzymes,
receptors =>• Targets for drug action =>• Drugs : Steroids, NSAIDs, DMARDs, & Biologics
(basic pharmacology)• Clinical Pharmacology & Therapeutics :
Evidence of efficacy, safety, suitability

ANALGESIC-ANTIPYRETIC & (NONSTEROIDAL)
ANTIINFLAMMATORY AGENTS
Chemical Classification
• Nonselective COX Inhibitors : aspirin, paracetamol, indomethacin, diclofenac, ibuprofen,mefenamic acid, meloxicam, nabumetone
• Selective COX-2 Inhibitors : rofecoxib, celecoxib, nimesulide, etodolac

Aspirin vs tNSAIDs (How Aspirin-like are they?)
• Aspirin covalently modifies both COX-1 and COX-2 => irreversible inhibition of COX activity. For COX-1 => serine 530; for COX-2 => serine 516
• Platelets are especially susceptible to aspirin; they cannot regenerate COX
• In contrast to aspirin, most NSAIDs act as reversible, competitive inhibitors of COX
NSAIDs: Shared Properties (THERAPEUTIC Effects)
• 1 antipyretic • 2 analgesic, for low-to-mod intensity like dental
pain, postop pain or pain from inflammatory conditions. Not visceral pain.
• 3 antiinflammatory, symptomatic relief in musculoskeletal disorders (eg, rheumatoid arthritis, osteo-arthritis, ankylosing spondylitis)
(except paracetamol, which is effective vs brain COX only, not antiinflam in peripheral tissues)
Other Therapeutic Uses of NSAIDs
• Indomethacin for postnatal closure of PDA (not during pregnancy)
• Relief of cramps in primary dysmenorrhea
• Emerging use: prevention of colon/breast cancer, Alzheimer’s (?) with COX-2 inhibitors
Shared Properties of NSAIDs: SIDE EFFECTS (due to COX inhibition)
1 Gastric or intestinal ulceration due to loss of cytoprotective - PGI2 & PGE2
2 Disturbance in platelet function - TXA23 Prolongation of gestation/spont labor (COX2 inh)4 Premature closure of ductus 5 Renal function changes, critical in CHF,
cirrhosis, chronic renal dis, hypovolemic *(not shared/less risk with highly selective COX-2 inhibitors)

COXibs : Continuing Issues & Food for Thought
• The present coxibs (COX2 Inhibitors) do not appear to be more efficacious than older NSAIDs
• They are the drugs of choice for those with gastric sensitivity;their claimed advantage seems to be in reducing ulcerogenic effect
• Adverse effect profile similar to other NSAIDs (even increased cardiac risk?)
• Emerging use: vs cancer , Alzheimer’s
Summary
• 1. Autacoids are part of a heterogenous group of substances that participate in homeostasis.
• 2. Autacoids have different sources, fates, and biologic activities.
• 3. Autacoids play an important role in health and disease.
• 4. Understanding the pharmacologic properties of these agonists, antagonists & inhibitors using prototype drugs is important to effectively utilize these agents in the clinical setting.