australia elsevier proofs sample...12 integrated care and multidisciplinary teamwork 203 jane l....
TRANSCRIPT
Sample
proo
fs © Else
vier A
ustra
lia
AN INTRODUCTIONSIXTH EDITION
Contexts of Nursing
Sample
proo
fs © Else
vier A
ustra
lia

AN INTRODUCTIONSIXTH EDITION
EDITED BY
JOHN DALY
DEBRA JACKSON
Contexts of Nursing
Sample
proo
fs © Else
vier A
ustra
lia

CONTENTSContributors vii
Preface x
1 Presenting nursing … a career for life 1John Daly and Debra Jackson
2 Visioning the future by knowing the past 15Madonna Grehan
3 Nursing and social media 39Caleb Ferguson
4 Key concepts informing nursing: caring, compassion and emotional competence 57Stacey Wilson
5 Becoming a critical thinker 71Steve Parker
6 Reflective practice: what, why and how 89Kim Usher and Zachary Byfield
7 Research in nursing 105Elizabeth Halcomb
8 Ethics in nursing 119Megan-Jane Johnstone
9 An introduction to legal aspects of nursing and midwifery practice 129Amanda Adrian
10 Power and politics in the practice of nursing 165Stacey Wilson and Katheryn Butters
11 Becoming a nurse leader 183Patricia M. Davidson and Binu Koirala
12 Integrated care and multidisciplinary teamwork 203Jane L. Phillips, Claire Fraser and Louise D. Hickman
13 Technology and professional empowerment in nursing 223Caleb Ferguson
Sample
proo
fs © Else
vier A
ustra
lia
vi CONTENTS
14 Nursing practice and digital health interventions: a focus on improving care 241Deborah Debono, Susan Maree Hanson and Berne Gibbons
15 Healthy communities: the evolving roles of nursing 263Anne McMurray
16 Health disparities: the social determinants of health 285Denise Wilson and Stephen Neville
17 Mental health promotion 301Wendy Cross
18 The challenges and rewards of rural and remote nursing 319Marie Hutchinson and Leah East
19 Cultural safety in nursing and midwifery 335Tamara Power and Kim Usher
20 Connecting clinical and theoretical knowledge for practice 349Jane Conway
21 Global health and nursing 369Michele Rumsey
Glossary 393
Index 403
Sample
proo
fs © Else
vier A
ustra
lia

CONTRIBUTORSAmanda Adrian RN, BA, LLB, FACN
Amanda Adrian and Associates, President, Climate and Health Alliance, NSW, Australia
Katheryn Janine Butters RN, MPhil
Lecturer, School of Nursing, Massey University, Wellington, New Zealand
Zachary Byfield RN, Bphil, BN, GdipN, MN, Mphil
Lecturer of Nursing, School of Health, University of New England, Armidale, NSW, Australia
Jane Conway RN, BHSc, BNurs(Hons1), Ded
Associate Dean, Teaching and Learning, Faculty of Medicine and Health, Discipline Lead, Nursing,
School of Health, University of New England, Armidale, NSW, Australia
Wendy Cross RN, BAppSc, MEd, PhD
Professor and Dean, School of Health, Federation University Australia, Berwick Campus, Vic, Australia
John Daly RN, HonDNurs, PhD, FACN, FAAN, FFNMRCSI
Professor of Nursing, Head of School & Dean, Susan Wakil School of Nursing and Midwifery, Sydney
Nursing School, Faculty of Medicine and Health, The University of Sydney, Sydney, NSW, Australia
Patricia M Davidson RN, MEd, PhD, FAAN, FACN
Dean and Professor, Johns Hopkins University School of Nursing, Baltimore, MD, USA
Deborah Debono RN, PhD, BA(Psych Hons)
Senior Lecturer, Centre for Health Services Management, Faculty of Health, University of Technology
Sydney, Sydney, Australia
Leah East RN, GradCertAP, BN(Hons), PhD
Associate Professor in Nursing (Primary Health Care), Joint appointment with Hunter New England
Health, School of Health, University of New England, Armidale, NSW, Australia
Caleb Ferguson RN, PhD
Senior Research Fellow, Heart Foundation Postdoctoral Fellow, Western Sydney Nursing & Midwifery
Research Centre, Western Sydney University & Western Sydney Local Health District
Claire Fraser RN, BSc(Nur), MPallCare
PhD Candidate, Centre for Improving Palliative, Aged and Chronic Care through Clinical Research and
Translation (IMPACCT), Faculty of Health, University of Technology Sydney, NSW, Australia
Berne Gibbons RN, Diploma in Nursing
Adjunct Professor, Faculty of Health, University of Technology Sydney, NSW, Australia
Madonna Grehan RN, RM, GradDipHlthEth, PhD
Honorary Fellow, Nursing, School of Health Sciences, The University of Melbourne, Vic, Australia
Elizabeth Halcomb RN, BN(Hons), GradCertICNurs, GradCertHE, PhD, FACN
Professor of Primary Health Care Nursing, School of Nursing, University of Wollongong, NSW, Australia
Sample
proo
fs © Else
vier A
ustra
lia

viii CONTRIBUTORS
Susan Maree Hanson RN, BSc(N), MSc(PHC)
Co-Chair, Palliative Care Network, Agency for Clinical Innovation, Sydney, NSW, Australia; Subject
Coordinator and Adjunct Professor, Faculty of Health, University of Technology Sydney, NSW,
Australia
Louise D Hickman RN, MPH, PhD
Associate Professor, UTS Fellow, Care of Vulnerable Older Populations, Faculty of Health, University of
Technology Sydney, NSW, Australia
Marie Hutchinson RN, BAppSc, GradDipHA, MHSc, PhD
Professor, School of Health and Human Sciences, Southern Cross University, NSW, Australia
Debra Jackson RN, AO, PhD, FACN
Professor, School of Nursing and Midwifery, University of Technology Sydney, NSW, Australia
Megan-Jane Johnstone RN, AO, BA, PhD
Independent Scholar; formerly Professor of Nursing (now retired), Deakin University, Vic, Australia
Binu Koirala RN, MGS, PhD
Assistant Professor, Johns Hopkins School of Nursing, Baltimore, MD, USA
Anne McMurray RN, AM, BA(Psych), MEd, PhD
Emeritus Professor, School of Nursing and Midwifery, Griffith University, Qld; Emeritus Professor, School
of Nursing, Murdoch University, WA; Adjunct Professor, University of the Sunshine Coast, Qld,
Australia
Stephen Neville RN, BA, MA, PhD, FCNA(NZ)
Professor and Head of Department, Nursing, Auckland University of Technology, Auckland, New
Zealand
Steve Parker BEd, PhD
Associate Dean (Teaching & Learning), School of Nursing & Midwifery, Flinders University, Adelaide,
SA, Australia
Jane L Phillips RN, BSc(Nur), PGD-HP, PhD, FACN
Professor, Palliative Nursing; Director, Centre for Improving Palliative, Aged and Chronic Care through
Clinical Research and Translation (IMPACCT), Faculty of Health, University of Technology Sydney,
NSW, Australia
Tamara Power RN, BN(Hons), GradCertDiabEdM, PhD
Senior Research Fellow, Faculty of Health, University of Technology Sydney, NSW, Australia
Michele Rumsey RN, GradDipHlth, FACN
Director, WHO Collaborating Centre for Nursing, Midwifery and Health Development, Faculty of Health,
University of Technology Sydney, NSW, Australia; Global Network of WHO Collaborating Centres for
Nursing and Midwifery, Secretariat, South Pacific Chief Nursing and Midwifery Officers Alliance
Kim Usher RN, AM, BA, DipAppSc, MNSt, PhD, FACN, FACMHN
Professor of Nursing, School of Health, University of New England, Armidale, NSW, Australia
Sample
proo
fs © Else
vier A
ustra
lia

ixCONTRIBUTORS
Denise Wilson BA(SocSc), MA(Hons), PhD
Professor, Māori Health and Associate Dean, Māori Advancement, Faculty of Health & Environmental
Sciences; Co-Director, Taupua Waiora Māori Health, Research Centre, Auckland University of
Technology, Auckland, New Zealand
Stacey Wilson RN, MPhil(Dist.), PhD
Clinical Programmes Lead, Mental Health and Addictions Directorate, MidCentral District Health Board;
Adjunct Senior Lecturer, School of Nursing, Massey University, New Zealand
Sample
proo
fs © Else
vier A
ustra
lia

PREFACEWelcome to the sixth edition of Contexts of Nursing. There has never been a more exciting time to be a nurse! As we write this preface in 2020, the year designated by the Seventy-second World Health Assembly as the International Year of the Nurse and the Midwife; the world is gripped by a deadly pandemic, and nurses everywhere are in active service in
State of the World’s Nursing 2020
editions, this volume introduces students to the theory, language and scholarship of nursing
extend them. This is a good thing, and will hold students in good stead for the future, as the discipline and profession of nursing continues to evolve, mature and develop within
are explored and considered in relation to professional nursing practice and the context of healthcare.
We have explained previously why the notion of ‘contexts’ has appeal for us in concep-
as-fabric’ metaphor provides access to a number of other related ideas, such as weaving
nurses who found previous editions useful in undergraduate and graduate courses and in their educational development and practice.
edition, a number of new strategies have been incorporated to facilitate deeper personal
been learned so far. Stories are used by a number of contributors as case study examples
internalisation of content by the reader.
their ongoing enthusiasm, encouragement, support and assistance in the preparation and
Sample
proo
fs © Else
vier A
ustra
lia
xiPREFACE
again to the challenge of developing engaging, scholarly and learning- and teaching-oriented
John Daly
Debra Jackson
Sydney, June 2020.
References
Daly J, Jackson D, Anders R, Davidson P M 2020 Who speaks for nursing? COVID-19 highlighting gaps in leadership. Journal of Clinical Nursing, April. doi:10.1111/jocn.15305
World Health Organization (WHO) 2020 State of the World’s Nursing Report 2020. Online. Available: https://www.who.int/publications/i/item/nursing-report-2020 8 June 2020
Sample
proo
fs © Else
vier A
ustra
lia
Caleb Ferguson
NURSING AND SOCIAL MEDIA
C H A P T E R 3
LEARNING OBJECTIVES
After reading this chapter, readers should be able to:
define social media and describe a variety of applications for nursing practice;
describe how social media interfaces with nursing across practice, education, research and policy;
apply regulatory policies and guidelines for social media use and discuss their implications for nursing;
describe ethical and professional issues for nurses to consider when using social media in practice;
contemplate the future innovations and horizons for social media and nursing.
KEY WORDSdigital nursing
e-professionalism
ethics
professionalism
social media
social networking
technology
Twitter chat
INTRODUCTIONCommunication is a vital aspect of human interaction. On 10 March 1876 Alexander Graham Bell invented the telephone, sparking the advent of a new telecommunications industry. Within today’s society, the internet is a critical piece of communication infrastructure for many people, and therefore denying or restricting access, while hospitalised for example, is failing to address people’s needs. In today’s world, the internet is a central element of daily life, and has replaced the
Sample
proo
fs © Else
vier A
ustra
lia
40 CONTEXTS OF NURSING: AN INTRODUCTION
telephone as the main source of communication. The face of the internet is constantly evolving, and social media platforms are rapidly changing living landscapes. Web 2.0 describes a change in the way humans interact with information online. Since the inception of Web 2.0 we have witnessed internet users adjust from being passive recipients of web-based content to active creators and curators of digital content (Ferguson 2013). Social media platforms are wide ranging and include Facebook, Twitter, LinkedIn, Google+, YouTube, Instagram, Pinterest and Snapchat to name a few. Users of these platforms can actively create their own content by posting and uploading photos, sharing content, ‘liking’ or blogging information and ideas. Social media is an umbrella term that includes social networking (such as LinkedIn), content sharing (such as Instagram), web publishing (such as blogging and micro-blogging) and wikis (including Wikipedia) (Department of Education and Early Childhood Development 2013). While nursing has been relatively slow to take up these innovative tools and the social media boom, the potential application within nursing practice, policy, education and research is extremely far reaching and should be embraced (Ferguson 2013). However, social media should be approached with risk at front of mind. Nursing remains one of the most risk-averse professions, and rightly so, as we are charged with caring for vulnerable individuals. Therefore, it is important that when applying social media to nursing practice, this is carefully risk managed and assessed for appropriateness in practice.
There is a vast array of novel examples of social media application in nursing. These include online support blogs for individuals living with atrial fibrillation (AF), stroke survivor support groups on Facebook and social media-facilitated journal clubs and Twitter chats for nursing researchers and clinicians to name a few. An extensive and diverse range of platforms continue to emerge. However, it is important that nurses have a basic understanding of social media and its implications for nursing practice within the context of the contemporary healthcare system.
What is social media?
-
Sample
proo
fs © Else
vier A
ustra
lia

41CHAPTER 3 NURSING AND SOCIAL MEDIA
Relevance to nursing and modern healthcare
-
TelegraphSample
proo
fs © Else
vier A
ustra
lia

42 CONTEXTS OF NURSING: AN INTRODUCTION
FIGURE 3.1
News reports of nursing misconduct related to social media Sample
proo
fs © Else
vier A
ustra
lia
43CHAPTER 3 NURSING AND SOCIAL MEDIA
Social media ethics and e-professionalism
1
2
3
4
Guidance, policy and regulation
Contemporary application in nursing
PATIENT SUPPORT AND NURSING INTERVENTIONS
Sample
proo
fs © Else
vier A
ustra
lia

44 CONTEXTS OF NURSING: AN INTRODUCTION
Web publishing, blogging and online communities
BOX 3.1
Recommendations for nurses using social media
• Be cognizant and proactive about knowing and understanding the terms and
conditions of each of the social media sites that you use. This can often be
challenging, given the frequency with which these are updated, but it is important to
keep abreast of these updates and review these and their privacy settings on a
regular basis.
• Users of social media should consider all posts as public. It’s very easy for a private
post to become public (such as a ‘friend’ or connection screen grabbing a post and
re-posting it). Therefore, users should adopt a ‘time out’ strategy and develop a
‘think and reflect’-before-you-post attitude. Be careful in crafting posts, as with the
written word; this is easily misconstrued, taken out of context and could have both
damaging and negative consequences for professional relationships and career
prospects.
• Never consider posts to be anonymous.
• It is essential to regularly monitor and evaluate your digital presence. At minimum, a
yearly digital presence personal review is recommended.
• Ensure that you are adhering to your professional standards for practice, employer
code of conduct and that you are up to date with privacy and confidentiality
legislation.
• Do not post content outside your area of expertise, and avoid the use of testimonials
(in adherence with new advertising legislation and guidance) (AHPRA 2014a, 2014b).
Sample
proo
fs © Else
vier A
ustra
lia

45CHAPTER 3 NURSING AND SOCIAL MEDIA
Patient support and nursinginterventions
Patient servicesand workforce
issues
Education andprofessionaldevelopment
Policy, procedureand research
FIGURE 3.2
Key areas for social media innovation in nursing
BOX 3.2
Examples of patient support and nursing interventions delivered via social media
• Raising organ and tissue donation awareness (advocating via Twitter, see Fig. 3.3)
• Providing ad hoc supportive care for patients and family members via a digital forum
• Assisting with diabetes management (such as blood glucose tracking)
• Maintaining a personal health diary (e.g. posting via MyFitnessPal to Facebook)
• Connecting patients with similar conditions (National Stroke Foundation Australia’s
EnableMe—online patient community for stroke http://www.enableme.org)
• Providing smoking cessation assistance (ability for real-time feedback from smoking
cessation counsellors)
• A platform to engage with exercise training and management
• Receiving ‘daily health tips’ from credible sources (e.g. secondary stroke prevention)
PATIENT SUPPORT
• Obtaining weight management support (e.g. ‘Lark’ smartphone application)
• Engaging with epilepsy support groups (such as consumer-driven or NGO-led
Facebook page initiatives)
• Engaging with stroke survivor support groups
• Engaging with brain tumour support groups (such as Nurse Consultant-led Facebook
groups after discharge post-surgery)
Sample
proo
fs © Else
vier A
ustra
lia

46 CONTEXTS OF NURSING: AN INTRODUCTION
Health promotion
-
FIGURE 3.3
An example of social media advocacy for organ and tissue donation through @DonateLifeToday Twitter account
Sample
proo
fs © Else
vier A
ustra
lia
47CHAPTER 3 NURSING AND SOCIAL MEDIA
PATIENT SERVICES AND WORKFORCE
EDUCATION AND PROFESSIONAL DEVELOPMENT
-
Sample
proo
fs © Else
vier A
ustra
lia

48 CONTEXTS OF NURSING: AN INTRODUCTION
Twitter chats
BOX 3.3
Examples of social media-delivered patient services and workforce interventions
EXAMPLES OF SOCIAL MEDIA-DELIVERED PATIENT SERVICES
• Patient care reminders in the clinical setting (automated text messaging SMS services
for clinic appointments)
• Prescription management, including pharmacy refill reminders
• Coordinating preoperative, peri-operative and post-operative care
• Arranging outpatient care
• Coordinating allied healthcare services during patient admissions
• Coordinating patient discharges across clinical services
• Post-discharge patient consultations
• Case management functions
• Checking hospital ratings with other healthcare consumers (e.g. MyHospital)
EXAMPLES OF SOCIAL MEDIA-DELIVERED WORKFORCE INTERVENTIONS
• Transmitting critical laboratory values to nurses and physicians
• Augmenting telemedicine
• Remote wound care assistance
• Shift bidding for nurses and other healthcare professionals (e.g. CASCOM, which is
an online open shift-bidding platform for casual staff that can be accessed via
smartphone and desktop devices)
• Recruitment of healthcare staff (advertising on LinkedIn for job opportunities and
vacancies)
• Communicating with nursing supervisors
Sample
proo
fs © Else
vier A
ustra
lia

49CHAPTER 3 NURSING AND SOCIAL MEDIA
Development of clinical skills
POLICY, PROCEDURE AND RESEARCH
Sample
proo
fs © Else
vier A
ustra
lia
50 CONTEXTS OF NURSING: AN INTRODUCTION
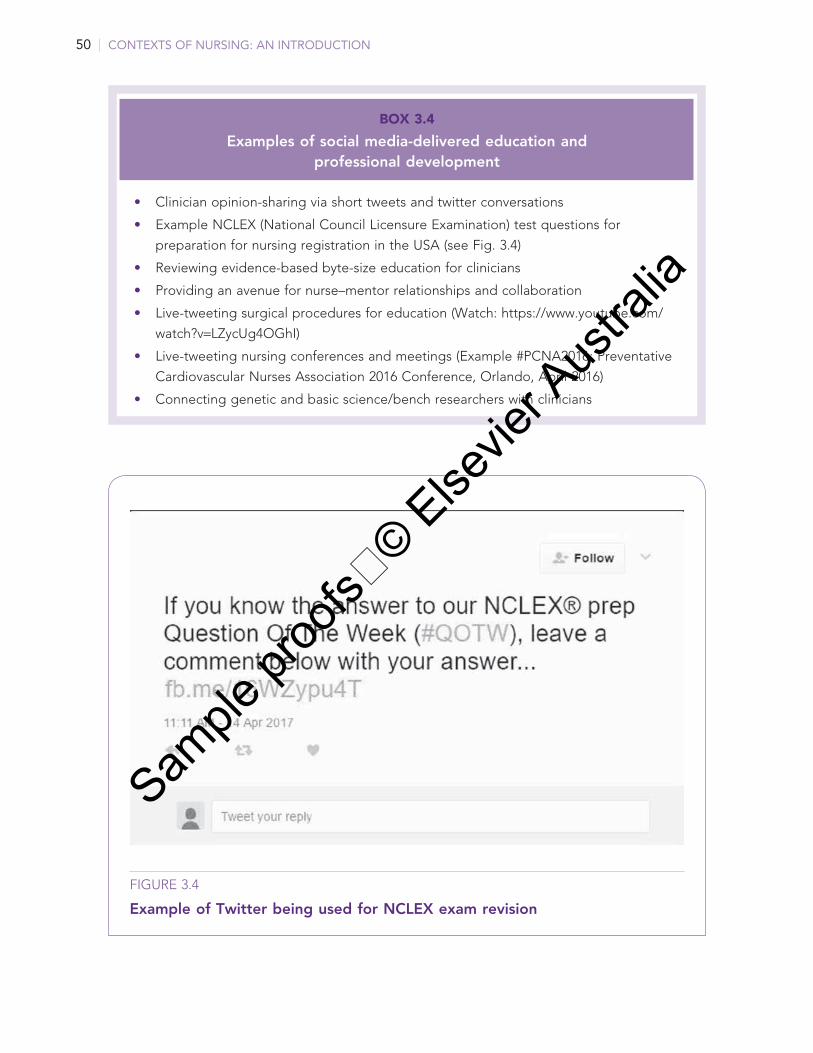
BOX 3.4
Examples of social media-delivered education and professional development
• Clinician opinion-sharing via short tweets and twitter conversations
• Example NCLEX (National Council Licensure Examination) test questions for
preparation for nursing registration in the USA (see Fig. 3.4)
• Reviewing evidence-based byte-size education for clinicians
• Providing an avenue for nurse–mentor relationships and collaboration
• Live-tweeting surgical procedures for education (Watch: https://www.youtube.com/
watch?v=LZycUg4OGhI)
• Live-tweeting nursing conferences and meetings (Example #PCNA2016; Preventative
Cardiovascular Nurses Association 2016 Conference, Orlando, April 2016)
• Connecting genetic and basic science/bench researchers with clinicians
FIGURE 3.4
Example of Twitter being used for NCLEX exam revision
Sample
proo
fs © Else
vier A
ustra
lia
51CHAPTER 3 NURSING AND SOCIAL MEDIA
-
+
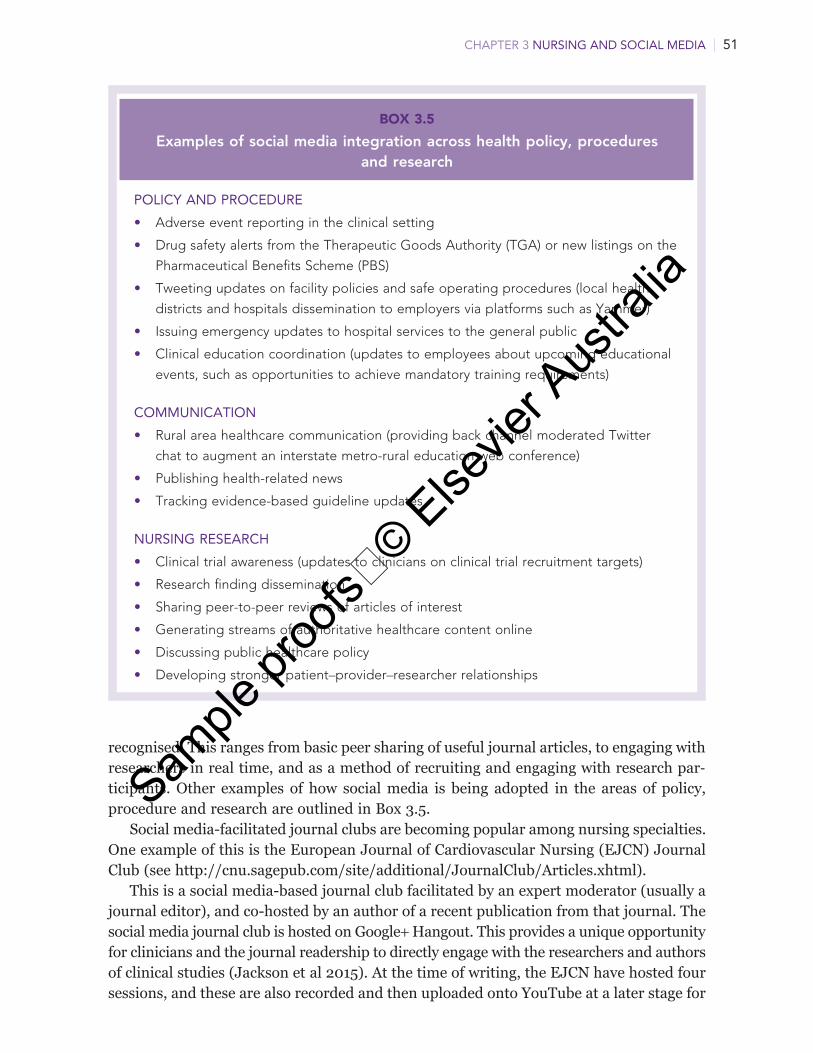
BOX 3.5
Examples of social media integration across health policy, procedures and research
POLICY AND PROCEDURE
• Adverse event reporting in the clinical setting
• Drug safety alerts from the Therapeutic Goods Authority (TGA) or new listings on the
Pharmaceutical Benefits Scheme (PBS)
• Tweeting updates on facility policies and safe operating procedures (local health
districts and hospitals dissemination to employers via platforms such as Yammer)
• Issuing emergency updates to hospital services to the general public
• Clinical education coordination (updates to employees about upcoming educational
events, such as opportunities to achieve mandatory training requirements)
COMMUNICATION
• Rural area healthcare communication (providing back channel moderated Twitter
chat to augment an interstate metro-rural education web conference)
• Publishing health-related news
• Tracking evidence-based guideline updates
NURSING RESEARCH
• Clinical trial awareness (updates to clinicians on clinical trial recruitment targets)
• Research finding dissemination
• Sharing peer-to-peer reviews of articles of interest
• Generating streams of authoritative healthcare content online
• Discussing public healthcare policy
• Developing stronger patient–provider–researcher relationships
Sample
proo
fs © Else
vier A
ustra
lia
52 CONTEXTS OF NURSING: AN INTRODUCTION
You are working as a new graduate registered nurse in a busy acute surgical ward in a major metropolitan teaching hospital. You are caring for Hayley, a 23-year-old female patient who has recently been involved in a road traffic accident and has fractured her
neck of femur. You are administering an injection to her. While obtaining Hayley’s consent for a subcutaneous injection, and checking the five rights of medication administration, Hayley asks you if she can record and live broadcast a short Facebook video of her injection to her friends using her smartphone. Hayley’s mum is also present at the bedside, and thinks this would be pretty ‘cool’ to do too, and is keen to assist in recording this video.
Reflective questions
1 What would your nursing actions be in this scenario?
2 How would this interaction with Hayley affect your therapeutic relationship with her?
3 What could the professional repercussions of your actions be if you allow Hayley to record and broadcast this procedure?
4 What are important factors of consent in this scenario?
STORY
You have been working for three years in the general medical ward of a regional hospital. During this time, you have received many ‘friend requests’ on Facebook from your nursing colleagues in the ward, which you have accepted. You have had a busy morning
shift, and were short of staff and acuity of patients was unexpectedly high. That evening you log onto Facebook at home, and see a post from a colleague that you were working alongside that morning. She is venting about the terrible shift she had experienced, makes note of the intensity of the workload and is insulting and offensive to other colleagues from your unit.
Reflective questions
1 What reaction would you have to your colleague’s post?
2 How would you approach your colleague both online and offline?
3 Would you report this behaviour to your nurse unit manager?
STORY
Sample
proo
fs © Else
vier A
ustra
lia
Deborah Debono, Susan Maree Hanson and Berne Gibbons
NURSING PRACTICE AND DIGITAL HEALTH
INTERVENTIONS: A FOCUS ON IMPROVING CARE
C H A P T E R 1 4
LEARNING OBJECTIVES
After reading this chapter, readers should be able to:
consider the design, development and implementation of digital health interventions using co-design principles and approaches;
understand barriers and opportunities for the use of digital health interventions to improve patient outcomes and care;
understand how digital health innovations underpin intelligence-informed healthcare;
appreciate the role of technology in supporting the use of data to improve patient safety and clinical quality;
discuss the innovative technologies available to nurses that can improve patient safety and clinical quality.
KEY WORDSadaptive change
clinical information
digital health interventions
electronic medical records
improving care
safety concerns
workarounds
Sample
proo
fs © Else
vier A
ustra
lia

242 CONTEXTS OF NURSING: AN INTRODUCTION
INTRODUCTIONRecent research suggests that nurses perceive that they are currently inadequately prepared for the digital age, not ready to lead decision making about the adoption of digital technology, facilitate digital literacy or model digital professionalism in healthcare (Mather et al 2019:1). Given the rapid spread of digital health interventions across healthcare and nurses’ pivotal role in leading and delivering healthcare, it is essential to address this gap.
This chapter provides a high-level overview of the intersection between digital health interventions and nursing practice. Digital health is a rapidly growing field with an ever-expanding body of knowledge and evidence supporting its adoption. It would not be feasible to cover all aspects in a single chapter. This chapter establishes a baseline of understanding that can both inform current nursing practice and form the basis of further study or exploration. The chapter provides the reader with a practical definition of digital health technology that can assist with promoting meaningful use, an overview of the current state of play in the UK, the USA and Australia, and an introduction to the opportunities and challenges that are associated with the digitalisation of healthcare. We have focused on the implementation and impact of digital clinical records, as both nationally and internationally these form the backbone of digital health strategies. Importantly, the chapter should assist nurses to become aware of the frontline clinical practice implications that are associated with digital health interventions.
Data driven careThere is no doubt that the introduction of digital technology in health has brought, and
Sample
proo
fs © Else
vier A
ustra
lia
243CHAPTER 14 NURSING PRACTICE AND DIGITAL HEALTH INTERVENTIONS: A FOCUS ON IMPROVING CARE
as it is done as it is imagined to be done
Sample
proo
fs © Else
vier A
ustra
lia
244 CONTEXTS OF NURSING: AN INTRODUCTION
What is a digital health intervention?
Sample
proo
fs © Else
vier A
ustra
lia

245CHAPTER 14 NURSING PRACTICE AND DIGITAL HEALTH INTERVENTIONS: A FOCUS ON IMPROVING CARE
DIGITAL HEALTH TECHNOLOGIES
Ohashi et al 2014)
2018, Hydari et al 2018)
Sample
proo
fs © Else
vier A
ustra
lia

246 CONTEXTS OF NURSING: AN INTRODUCTION
Lessons from global implementation of digital health technologiesGLOBAL STRATEGIES FOR DIGITAL HEALTH TECHNOLOGY ADOPTION
ELECTRONIC HEALTH OR MEDICAL RECORDS
across within a single care
TABLE 14.1
Health-related social networks
SOCIAL NETWORK FOCUS
MedHelp Online health community that partners with hospital doctors and medical research institutions to deliver online discussion boards on healthcare topics
CureTogether Crowdsourcing initiative that brings patients and researchers together to find cures for chronic conditions
Vitals Online search tool to help consumers search for the best medical care
DailyStrength Online social network centred on support groups, where users provide one another with emotional support by discussing their struggles and successes with each other
PatientsLikeMe Online patient network that connects patients with one another, whereby they can share their experience with disease, share their health data to track their progress, help others and contribute to research that advances medicine, improving their outcomes and enabling research
Inspire Online health community providing a safe and secure place for patients and caregivers to support and connect with one another
FacetoFace Health Online health community that connects one-on-one with others who share similar health experiences
Bichel-Findlay et al 2017.
Sample
proo
fs © Else
vier A
ustra
lia
247CHAPTER 14 NURSING PRACTICE AND DIGITAL HEALTH INTERVENTIONS: A FOCUS ON IMPROVING CARE
Electronic health records in the United Kingdom
1
2
3
4
5
6
7
8
9
10
Sample
proo
fs © Else
vier A
ustra
lia

248 CONTEXTS OF NURSING: AN INTRODUCTION
Electronic health and medical records in the United States
Digital health interventions in Australia
1 Putting users at the centre2
3 Fostering agile collaboration4
5
Sample
proo
fs © Else
vier A
ustra
lia

249CHAPTER 14 NURSING PRACTICE AND DIGITAL HEALTH INTERVENTIONS: A FOCUS ON IMPROVING CARE
6
1
2
3
4
5
6
7
Understanding barriers and opportunities to the implementation of digital health technologiesSUCCESSES AND UNEXPECTED CHALLENGES
Sample
proo
fs © Else
vier A
ustra
lia
250 CONTEXTS OF NURSING: AN INTRODUCTION
1
2 Extended (i.e. > 4 hours) eHR unavailability (either planned or unplanned)
3 Failure to heed a computer-generated warning or alert
4 System-to-system interface errors
5
Sample
proo
fs © Else
vier A
ustra
lia
251CHAPTER 14 NURSING PRACTICE AND DIGITAL HEALTH INTERVENTIONS: A FOCUS ON IMPROVING CARE
6 eHR time measurement translational challenges
7 Incorrect item selection from a drop-down list of items
8 Open or incomplete orders
SOCIO-TECHNICAL MODELS FOR UNDERSTANDING THE INTERSECTION BETWEEN TECHNOLOGY AND NURSING PRACTICE
Workarounds and adaptations
Sample
proo
fs © Else
vier A
ustra
lia
252 CONTEXTS OF NURSING: AN INTRODUCTION
Adaptive change
Sample
proo
fs © Else
vier A
ustra
lia

253CHAPTER 14 NURSING PRACTICE AND DIGITAL HEALTH INTERVENTIONS: A FOCUS ON IMPROVING CARE
Ethical and policy challenges in digital health
Sample
proo
fs © Else
vier A
ustra
lia
254 CONTEXTS OF NURSING: AN INTRODUCTION
Opportunities: Implications for nursing practice
CONCLUSIONSam
ple pr
oofs
© Elsevie
r Aus
tralia

255CHAPTER 14 NURSING PRACTICE AND DIGITAL HEALTH INTERVENTIONS: A FOCUS ON IMPROVING CARE
James, a nursing student averaging High Distinctions, embraced the call to adopt gold standard practices when delivering patient care. He was excited that the ward he was assigned to for his first placement, as a newly graduated nurse, used an electronic
medication administration system (EMMS). He anticipated this digital health technology would support him to deliver high-quality care.
Three months into this placement, as he prepares to go to work, James reflects on the shifts he has completed since starting on Nightingale medical ward. It was his first ward allocation in the new graduate program. He had felt fortunate to have secured a position in the postgrad program and had been excited to start as a registered nurse. He was, however, rapidly losing his drive to embrace technological innovations for excellent care, and even his passion for nursing.
Each shift James is conscious of the eye rolling, the displeasing looks, the muttering and the obvious judgement and conclusion by the senior nurses that he is too slow. It has been made obvious that his newly graduated peers have been given opportunities that he has not because, based on demonstrated ‘time management’, he has not yet demonstrated that he warrants additional responsibilities. He knows that he is handing on more tasks to the nurses on the next shift than the others, even though he takes much shorter breaks and stays back to write up the patients’ notes. James is also conscious that he takes longer to complete medication rounds than the other nurses, including some of his newly graduated peers. He has noticed that while he is adhering to all the prescribed steps when administering medication using the EMMS, his colleagues do not always do so.
James is acutely aware that he is one of the few nurses on the ward who uses (or tries to use) the technology as it is intended to be used when administering medication. When administering medication James pushes the computer on the dedicated trolley to the bedside so that he is able to conduct the 5Rs when administering medication. Many of his peers have adopted the medication administration practices elected by the more experienced staff. He concludes that this is a major contribution to his time management.
There are some patient rooms in which there are black spots, so the computers do not work at the bedside. In other rooms, it is really difficult to get the computer into the room because of the equipment already in there. James spends time moving equipment and furniture out so that he has the room to take the computer into these crowded rooms so that he can legitimately check the 5Rs at the bedside when administering medication. He then has to move everything back into the room, which is a very time-consuming process.
Some of the computers have a very short battery life, which means the computer has to be plugged in quickly in each room. James recalls several occasions when, because he was talking to a patient and their visitors, he had not plugged the computer in quickly enough and, because of the short battery life, it had shut down, losing the information he had entered (about which medica-tions he had put in the medication cup). In each instance, he had thrown out those medications and had started the process all over again. Rather than taking the dedicated computer trolley (workstation on wheels (WOW)) to the bedside to check the 5Rs when administering medication, some nurses leave it in the corridor outside the patient’s room, sign off the medication before administering it and either memorise the patient’s medical record number and name or write it on a piece of paper to complete the 5Rs.
STORY
Continued
Sample
proo
fs © Else
vier A
ustra
lia
256 CONTEXTS OF NURSING: AN INTRODUCTION
There are some instances that James has observed when, even though they could have used the technology as intended, some nurses did not because they said it took too long and that they wanted to avoid delays for their patients. They prepare the medications for each of their allocated patients in the medication room, write the patient’s bed number or name on the medication cup, sign all the medications off in the computer in the medication room and then take the labelled cups to each patient to administer them.
James feels extremely uncomfortable with these workaround practices. There are times, however, when not taking the WOW to the bedside seems to be best for the patient. For example, when the patient is isolated, taking the computer to the bedside constitutes an infection risk. In those scenarios James takes the WOW to the bedside and thoroughly cleans the trolley and wheels each time he administers medication—again taking him much longer than his colleagues who use a workaround.
James is concerned that his performance review will not be positive. Last night he had been allocated six patients, one of whom, Mrs Jones, had shown signs of confusion and agitation on previous night shifts. According to handover, the nurses had used a range of strategies to help Mrs Jones remain settled overnight. James was reminded of the noise-reducing strategies embraced on this ward, including soft closing bins, soft-soled shoes, call bells diverted to pagers and, where possible, using the sink at the nurses’ station rather than in the patients’ rooms. Mrs Jones had been asleep since the nurses commenced the night shift. Mrs Breen, in the bed opposite Mrs Jones, was due a medication at 02.00. James had pushed the WOW to her bedside so that he could conduct the 5Rs. The noise of the trolley and the lights of the computer woke Mrs Jones who started calling out, waking the other patients in her room and in the room across the hall. One of the nurses looked pointedly at James and suggested that next time he might consider the impact on patients’ sleep of taking the WOW to the bedside in the middle of the night. James felt torn. He knew that not taking the WOW to the bedside made him professionally vulnerable if he had made a medication error.
Reflective questions
1 How does James’ situation reflect the gap between work-as-imagined and work-as-done?
2 How might consideration of the complexity of patients’ responses to hospitalisation, environment, equipment and expectations (e.g. Key Performance Indicators) prior to implementing technology have mitigated James’ dilemma?
Sample
proo
fs © Else
vier A
ustra
lia

Tamara Power and Kim Usher
CULTURAL SAFETY IN NURSING AND MIDWIFERY
C H A P T E R 1 9
LEARNING OBJECTIVES
After reading this chapter, readers should be able to:
explain the concept of culture;
define the terms cultural safety and cultural capability and how these concepts inform nursing care;
discuss culture in the context of nursing and the healthcare system;
examine the role of cultural safety in improving access to healthcare services;
reflect and think critically about own values and beliefs when caring for Aboriginal and Torres Strait Islander peoples, Māori and people from other cultural and ethnic backgrounds;
identify specific considerations for the delivery of culturally safe nursing care for Aboriginal and Torres Strait Islander peoples, Māori and people from other cultural and ethnic backgrounds;
understand how the social determinants of health can impact those who are not part of the dominant culture.
KEY WORDSAustralia
colonisation
cultural capability
cultural safety
culturally safe nursing care
culture
First Peoples
Māori
multiculturalism
New Zealand
social determinants of health
Sample
proo
fs © Else
vier A
ustra
lia
336 CONTEXTS OF NURSING: AN INTRODUCTION
INTRODUCTIONAustralia and New Zealand’s populations are becoming increasingly culturally and socially diverse due to immigration. To provide effective nursing and midwifery care for all people, nurses and midwives need to be adaptable and able to accommodate cultural considerations and differing constructs of health in their work. In recognition of Indigenous Peoples as the original inhabitants, and their unique healthcare needs that stem from a history of colonisation, marginalisation and racism in both Australia and New Zealand, this chapter will differentiate the healthcare needs of Indigenous Peoples from the needs of people from other culturally and linguistically diverse (CALD) backgrounds.
Before reading this chapter
Culture
The concept of culture and its relationship to nursingCULTURE IS DYNAMIC
Sample
proo
fs © Else
vier A
ustra
lia

337CHAPTER 19 CULTURAL SAFETY IN NURSING AND MIDWIFERY
Cultural safety
cultural safety
Sample
proo
fs © Else
vier A
ustra
lia

338 CONTEXTS OF NURSING: AN INTRODUCTION
Aboriginal and Torres Strait Islander peoples in Australia
Info
Info
Info
Sample
proo
fs © Else
vier A
ustra
lia

339CHAPTER 19 CULTURAL SAFETY IN NURSING AND MIDWIFERY
Māori people in New Zealand
Multicultural Australia
Sample
proo
fs © Else
vier A
ustra
lia
340 CONTEXTS OF NURSING: AN INTRODUCTION
Multicultural New Zealand
BOX 19.1
Key dates in New Zealand’s history
1300 East Polynesian people arrive—now known as Māori
1642 Abel Tasman visits
1769 James Cook arrives and claims New Zealand for Great Britain
1835 Declaration of Independence signed by 34 Māori chiefs
1840 Treaty of Waitangi
1865 Wellington declared capital in place of Auckland
1893 New Zealand becomes the first country to give all women the right to vote
1907 New Zealand becomes a dominion
1908 Population reaches 1 million
1933 Adopts own currency
1947 Adopts the Statute of Westminster (1931) and becomes independent of Great
Britain
1952 Population reaches 2 million
1967 Decimalisation of currency
1973 Population reaches 3 million
1983 Closer Economic Relations (CER) agreement signed with Australia
1985 Waitangi Tribunal given power to hear Māori land grievances going back to
1840
2003 Population reaches 4 million
2020 Population reaches 5 million
Sample
proo
fs © Else
vier A
ustra
lia

341CHAPTER 19 CULTURAL SAFETY IN NURSING AND MIDWIFERY
Refugees and asylum seekers
BOX 19.2
Working with Indigenous people
Things to be aware of when working with Indigenous people include:
• Indigenous people perceive health and illness differently from the Western
biomedical model. Be sensitive to alternative worldviews.
• It may not be appropriate for a nurse to care for an Indigenous consumer of a
different gender. Where possible ask that a nurse of the same gender is assigned to
care for that person or ask if a family member is able to assist in any way. If this is not
possible, explore solutions with the consumer; for example, delaying personal care
till the next shift.
• Indigenous consumers must be consulted and included in all decisions about their
care. Sometimes this may also mean involving family members. Be guided by the
consumer in this matter. Indigenous consumers often have an extended family and
group of carers who all should be consulted.
• Avoid asking questions about ceremonial business, bereavement, sexuality, fertility,
domestic habits and other similar sensitive issues. If you are unsure regarding what is
appropriate to ask, meet with an Aboriginal Liaison Officer for guidance. Engage in
ongoing professional development regarding Indigenous culture.
Adapted from Haswell et al 2009, Westerman 2004.
Sample
proo
fs © Else
vier A
ustra
lia

342 CONTEXTS OF NURSING: AN INTRODUCTION
TABLE 19.1
Periods in Australian immigration policy development
YEARS POLICY FEATURES HEALTH POLICY IMPLICATION
1945–70 Assimilation Predominantly White Australian Anglo-Saxon policies.
Absence of government assistance.
1970–80 Integration White Australia policy relaxed and gradually abandoned.
Relevant services provided.
Some cultural characteristics tolerated. Welfare needs of migrants being addressed.
1980–89 Multiculturalism Pluralistic approach to immigration.Policies to limit discrimination on racial and ethnic grounds.Cultural and ethnic diversity becoming more accepted in Australian society.Cultural identity, social justice and economic efficiency were adopted.
Provision of various health services.Equality of access to culturally appropriate services.
1983 Mainstreaming Redirecting service delivery from marginal to a central base.
Promotion of culturally sensitive health services.
Concern of government institutions based on social equity and access; economic efficiency and cultural identity.
Equality of access to health services by immigrants.
1999 Inclusiveness Diversity.Multicultural policies built upon civic duty, cultural respect, social equity and productive diversity.The term multiculturalism to remain.Inclusiveness.
Promotion of culturally sensitive health services.Equality of access to health services by immigrants.
2000–08 United in diversity
National agenda for a multicultural Australia.Policy framework including: all Australians are expected to have a ‘loyalty to Australia and its people, and to respect the basic structures and principles underpinning our democratic Society. These are: Constitution, Parliamentary democracy, freedom of speech and religion, English as the National language, the rule of law, acceptance and equality’ (Commonwealth of Australia 2008:1–2).
Main components of ‘Multicultural Australia: united in diversity policy 2003–06’: responsibility, respect, fairness and benefits for all.
2008–12 Benefits of cultural diversity
Celebrate and value the benefits of cultural diversity. Emphasis on justice, inclusivity, trade, racism and discrimination.
The People of Australia: Australia’s multicultural policy launched in 2011.
2013–17 Strength in diversity
Recognise the strength inherent in a multicultural society.
Multicultural Australia—united, strong, successful: multicultural statement released 2017
Source: Commonwealth of Australia 1999, 2003, 2008, Department of Home Affairs 2020, Spinks 2009
Sample
proo
fs © Else
vier A
ustra
lia

343CHAPTER 19 CULTURAL SAFETY IN NURSING AND MIDWIFERY
Correlations between disadvantage and the social determinants of health
Providing culturally safe nursing care
CULTURAL AWARENESS
Sample
proo
fs © Else
vier A
ustra
lia

344 CONTEXTS OF NURSING: AN INTRODUCTION
CULTURAL SENSITIVITY
FIGURE 19.1
The process of achieving cultural safety in nursing and midwifery practice
Cultural Awareness
• Is a beginning step towards understanding difference. Many people undergo courses designed to sensitise them to formal ritual and practice rather than the emotional, social, economic and political context in which people exist.
Cultural Sensi�vity
• Alerts students to the legitimacy of difference and begins a process of self-exploration as the powerful bearers of their own realities and the impact this may have on others.
Cultural Safety
• Is an outcome of nursing education that enables safe service to be defined by those who receive the service.
Sample
proo
fs © Else
vier A
ustra
lia