august cme glaucoma supplement-dl 7-27 - eyeworld cme glaucoma suppl… · university of texas,...
TRANSCRIPT
A CME Supplement from an EyeWorld Educational Symposium held at ASCRS•ASOA 2007 in San Diego
CME EDUCATION
Suggestions for Management ofPatients with Glaucoma and Ocular Surface Disease
by Michael B. Raizman, M.D.
Ocular surface disease is prevalent in patients with glaucoma. Withmany patients using two or three different drops on the ocular sur-face to control glaucoma, it’s unfortunate that conditions such asdry eye complicate glaucoma management. As a result, it is impor-tant to learn to diagnose and manage ocular surface disease, in
addition to properly managing glaucoma.
Spotting Dry EyesDry eye is no longer considered a simple aqueous tear deficiency. While weused to think about dry eye as a simple loss of the aqueous tear layer, it’snow apparent that there are numerous factors involved. It seems that thereis a very strong and dynamic interaction between the tear film and theepithelium and also between the interface and both of these components.Oils from the lids, mucin from the conjunctiva, and tears from the lacrimalglands all interact with the corneal epithelium and the complex milieu atthe epithelial-tear interface. Disrupting any component easily perturbs thisdynamic interaction.
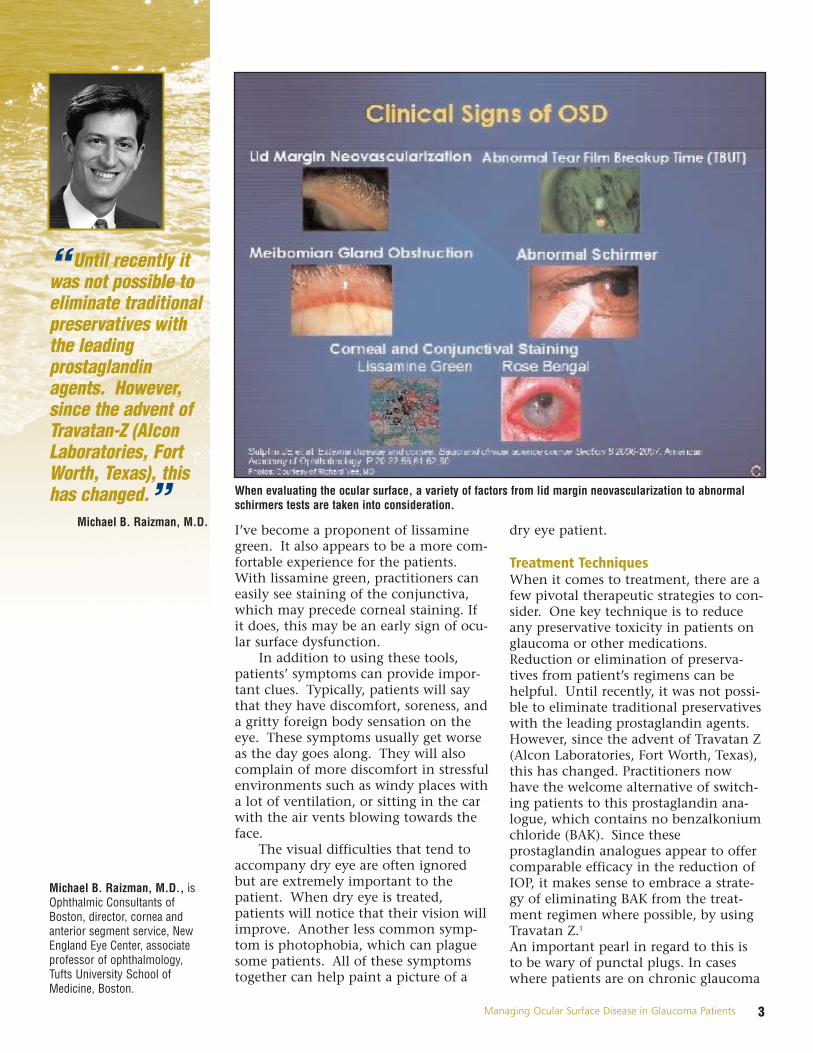
There are a number of ways you can screen for ocular surface diseasewhen examining a dry eye patient. Look closely at the lids and ocular sur-face of your patients with glaucoma. I like to evaluate the lid margins,looking for meibomian gland obstruction and vascularization. How thickare the oils when the lid is gently pressed? How much crusting is present?The tear film should be evaluated before the eye is applanated and beforeanesthetic is applied. What is the volume of the tear film? How large is themeniscus? Schirmer testing is a traditional method to assess the tears butlacks sensitivity and specificity, takes time, and can vary from day to day.
Looking at the tear film breakup time only takes a few seconds. Withjust a few blinks, tear film quality can be assessed with fluorescein in theeye. This can be done by having the patient blink and then stare. Countthe seconds until the fluorescein on the surface begins to break up. Normalbreakup time should exceed seven to eight seconds. If the patient’s tearbreakup time is shorter than the interval between routine blinks, then theyhave some desiccation of the corneal epithelium in every single blink.Those patients will invariably have damage to the ocular surface.
Staining the ocular surface with vital dyes is critical. While many practi-tioners currently use fluorescein to stain the eye, it is my belief that lis-samine green and Rose Bengal staining are actually more sensitive products.However, patients tend to complain that the Rose Bengal dye stings andthat they don’t like the red eyes they often get from the test. As a result,
EyeWorld Supplement — August 2007
Supported by an unrestricted educational grant from Alcon Laboratories Inc.
Continuing Medical Education
Moderator
Terrence P. O'Brien, M.D.Professor of Ophthalmology, CharlotteBreyer Rodgers Distinguished Chair inOphthalmology, Director of the RefractiveSurgery Service, Bascom Palmer EyeInstitute of the Palm Beaches , West PalmBeach, Florida
Faculty
Michael B. Raizman, M.D. is OphthalmicConsultants of Boston, director, cornea andanterior segment service, New EnglandEye Center, associate professor ofophthalmology, Tufts University Schoolof Medicine, Boston.
Douglas J. Rhee, M.D. is assistant profes-sor, Massachusetts Eye and Ear Institute(MEEI), Harvard Medical School, Boston
Richard W. Yee, M.D. is clinical professor,University of Texas, Houston MedicalSchool, Department of Ophthalmology andVisual Science.
Richard Lewis, M.D. is assistant clinicalprofessor, University of California-Davis,Sacramento
Educational ObjectivesOphthalmologists who take part in thiseducational activity will:
• Review the impact of ocular surface dis-eases on glaucoma patients
• Understand the unique parameters oftreating patients with concurrent glauco-ma and ocular surface disease
• Develop patient-specific strategies toeffectively treat ocular surface disease inthe presence of glaucoma
continued on page 2
Notice About Off-Label Use PresentationsThis EyeWorld Educational Symposium Supplement may include presentationson drugs or devices or uses of drugs or devices that may not have beenapproved by the Food and Drug Administration (FDA) or have been approved bythe FDA for specific uses only. The FDA has stated that it is the responsibility ofthe physician to determine the FDA clearance status of each drug or device hewishes to use in clinical practice.
ASCRS is committed to the free exchange of medical education. Inclusion of anypresentation in this program, including presentations of off-label uses, does notimply an endorsement by ASCRS of the uses, products, or techniques presented.
Continuing Medical Education (CME) The American Society of Cataract and Refractive Surgery is accredited by theAccreditation Council for Continuing Medical Education (ACCME) to provide con-tinuing medical education to physicians. ASCRS takes responsibility for the con-tent, quality, and scientific integrity for these activities.
CME CreditsASCRS designates this educational activity for a maximum of 1 AMA PRACategory 1 Credit™. Each physician should claim credit commensurate with theextent of his participation in the activity. Please note physicians must check in atthe symposium registration desk on-site to be eligible for credit.
Claiming CME CreditQuestions have been developed for this written supplement about material cov-ered in the EyeWorld Educational Symposium, Managing Ocular Surface Diseasein the Glaucoma Patient, presented on Monday, April 30, 2007 in San Diego.
Participants must take the written test once they have completed their review ofall material within this supplement. To receive CME credit, 80% of the questionsmust be answered correctly. The test must be completed individually, andanswers must be based on personal knowledge gained from reviewing the writ-ten material.
The test is available online at www.eyeworld.org. Go to Online Education for test.Once the test has been completed with a score of 80% or higher, a CME certifi-cate will be available to print using the browser's print function.
Participants who score less than 80% will have the opportunity to review thematerial and take the test again.
ASCRS will keep the earned CME information on file for the required time.
Expiration DateCME credit for this educational activity is valid through January 15, 2008. CMEcredit will not be awarded after that date.
CME QuestionsPlease contact Laura Johnson with the American Society of Cataract andRefractive Surgery at 703-591-2220, or e-mail her at [email protected] if youhave any questions regarding CME credit for this educational activity.
Financial Interest DisclosureAs a sponsor accredited by the ACCME, ASCRS•ASOA must ensure balance, independence, objectivity, and scientific rigor in all its individually or jointly sponsored activities.
All individuals participating in an ASCRS-sponsored CME activity must disclose anyfinancial interest or relationship with the manufacturer(s) of any commercial prod-uct(s) and/or provider(s) of commercial services discussed in an educational pres-entation or lack thereof. Persons with financial interests can include employees, con-sultants, major stockholders, members of a speakers bureau, etc. and those whoreceive grants or research support from companies discussed in the presentation.
The intent of this disclosure is not to prevent participants with a significant finan-cial relationship or other relationship from presenting; it is to provide theProgram Committee with information so it can design and implement a balanced,independent, and scientific educational activity. The Financial Interest Index with-in the sponsored activity's Final Program provides information to attendees sothey can make their own judgment regarding the interest or relationship and thematerials presented.
Richard A. Lewis, MDIsta Pharmaceuticals Inc. AiScience ASanten Inc. A
Terrence P. O'Brien, MDAdvanced Medical Optics AAlcon Laboratories AAlimera Sciences AAllergan Inc. ABausch & Lomb AINSPIRE AIsta Pharmaceuticals Inc. ASanten Inc. A
Category Code Specific Financial Interest
Product P I earn royalty or derive other financial gain froman ophthalmic product or service.
Investor R I have a significant investment interest in a company that makes/develops/provides oph-thalmic products or services.
Consultant A I receive a retainer, ad hoc fees, or other con-sulting income from a company that makes/develops/provides ophthalmic products or services.
B I am a member of the speaker's bureau of a company that makes/develops/provides oph-thalmic products or services.
C I provide practice management or marketing consulting services to ophthalmic practices.
Research D My research is fully or partially funded by a company that makes/develops/provides oph-thalmic products or services.
Travel E My travel expenses have been reimbursed, paidin full or subsidized, by a company that makes/develops/provides ophthalmic products or services.
None N I have no financial interest in any company thatmakes/develops/provides ophthalmic products or services.
Michael B. Raizman, MDAlcon Laboratories A, B, D, EAllergan Inc. A, B, D, EBausch & Lomb A, DIsta Pharmaceuticals Inc. AVistakon Pharmaceuticals Inc. A, E
Douglas J. Rhee, MDAlcon Laboratories BAllergan, Inc. B, DJohnson & Johnson AMerck BPfizer D
Richard W. Yee, MDAlcon Laboratories A, B
This supplement was produced by EyeWorld under an educational grant from Alcon Laboratories Inc.
Copyright 2007 ASCRS Ophthalmic Corporation. All rights reserved. The views expressed here do not necessarily reflect those of the editor, editorial board, or the publisher and in no way imply endorsement by EyeWorld or ASCRS.
CME – from page 1
3Managing Ocular Surface Disease in Glaucoma Patients
Michael B. Raizman, M.D., isOphthalmic Consultants of Boston, director, cornea andanterior segment service, NewEngland Eye Center, associateprofessor of ophthalmology,Tufts University School ofMedicine, Boston.
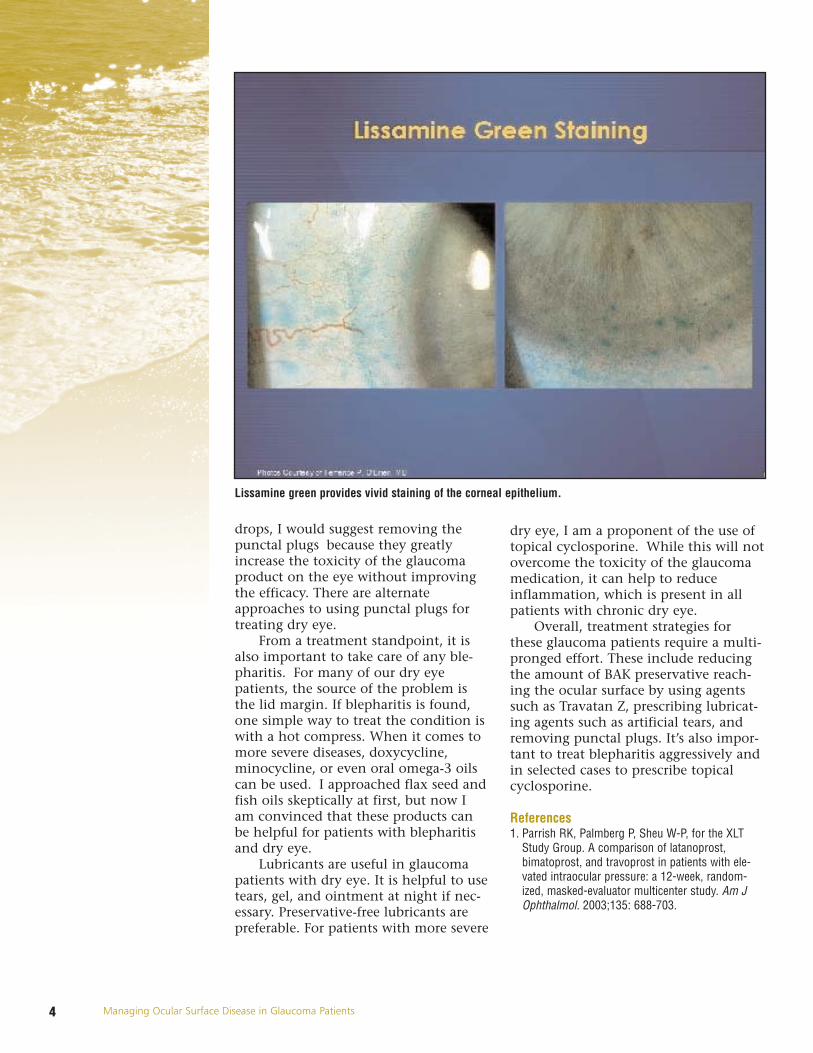
I’ve become a proponent of lissaminegreen. It also appears to be a more com-fortable experience for the patients.With lissamine green, practitioners caneasily see staining of the conjunctiva,which may precede corneal staining. Ifit does, this may be an early sign of ocu-lar surface dysfunction.
In addition to using these tools,patients’ symptoms can provide impor-tant clues. Typically, patients will saythat they have discomfort, soreness, anda gritty foreign body sensation on theeye. These symptoms usually get worseas the day goes along. They will alsocomplain of more discomfort in stressfulenvironments such as windy places witha lot of ventilation, or sitting in the carwith the air vents blowing towards theface.
The visual difficulties that tend toaccompany dry eye are often ignoredbut are extremely important to thepatient. When dry eye is treated,patients will notice that their vision willimprove. Another less common symp-tom is photophobia, which can plaguesome patients. All of these symptomstogether can help paint a picture of a
dry eye patient.
Treatment TechniquesWhen it comes to treatment, there are afew pivotal therapeutic strategies to con-sider. One key technique is to reduceany preservative toxicity in patients onglaucoma or other medications.Reduction or elimination of preserva-tives from patient’s regimens can behelpful. Until recently, it was not possi-ble to eliminate traditional preservativeswith the leading prostaglandin agents.However, since the advent of Travatan Z(Alcon Laboratories, Fort Worth, Texas),this has changed. Practitioners nowhave the welcome alternative of switch-ing patients to this prostaglandin ana-logue, which contains no benzalkoniumchloride (BAK). Since theseprostaglandin analogues appear to offercomparable efficacy in the reduction ofIOP, it makes sense to embrace a strate-gy of eliminating BAK from the treat-ment regimen where possible, by usingTravatan Z.1
An important pearl in regard to this isto be wary of punctal plugs. In caseswhere patients are on chronic glaucoma
“ Until recently itwas not possible toeliminate traditionalpreservatives withthe leadingprostaglandinagents. However,since the advent ofTravatan-Z (AlconLaboratories, FortWorth, Texas), thishas changed.”
Michael B. Raizman, M.D.
When evaluating the ocular surface, a variety of factors from lid margin neovascularization to abnormalschirmers tests are taken into consideration.
4 Managing Ocular Surface Disease in Glaucoma Patients
drops, I would suggest removing thepunctal plugs because they greatlyincrease the toxicity of the glaucomaproduct on the eye without improvingthe efficacy. There are alternateapproaches to using punctal plugs fortreating dry eye.
From a treatment standpoint, it isalso important to take care of any ble-pharitis. For many of our dry eyepatients, the source of the problem isthe lid margin. If blepharitis is found,one simple way to treat the condition iswith a hot compress. When it comes tomore severe diseases, doxycycline,minocycline, or even oral omega-3 oilscan be used. I approached flax seed andfish oils skeptically at first, but now Iam convinced that these products canbe helpful for patients with blepharitisand dry eye.
Lubricants are useful in glaucomapatients with dry eye. It is helpful to usetears, gel, and ointment at night if nec-essary. Preservative-free lubricants arepreferable. For patients with more severe
dry eye, I am a proponent of the use oftopical cyclosporine. While this will notovercome the toxicity of the glaucomamedication, it can help to reduceinflammation, which is present in allpatients with chronic dry eye.
Overall, treatment strategies forthese glaucoma patients require a multi-pronged effort. These include reducingthe amount of BAK preservative reach-ing the ocular surface by using agentssuch as Travatan Z, prescribing lubricat-ing agents such as artificial tears, andremoving punctal plugs. It’s also impor-tant to treat blepharitis aggressively andin selected cases to prescribe topicalcyclosporine.
References 1. Parrish RK, Palmberg P, Sheu W-P, for the XLT
Study Group. A comparison of latanoprost,bimatoprost, and travoprost in patients with ele-vated intraocular pressure: a 12-week, random-ized, masked-evaluator multicenter study. Am JOphthalmol. 2003;135: 688-703.
Lissamine green provides vivid staining of the corneal epithelium.
5Managing Ocular Surface Disease in Glaucoma Patients
Douglas J. Rhee, M.D., isassistant professor,Massachusetts Eye and EarInstitute (MEEI), Harvard MedicalSchool, Boston
by Douglas J. Rhee, M.D.
Problems with dry eye are anunfortunate occurrence arounda glaucoma office. My practiceconsists almost entirely of glau-coma patients and what I have
found is that the chief complaint frommost is related to ocular surface disease.It is uncommon for a patient to come incomplaining that his field is closing in—usually he or she will say, “I’m havingthis itching, and this burning,” or “Itfeels like there is something in my eyesfrom time to time.” Even though I prac-tice glaucoma, I almost inevitably endup having a mini cornea clinic with mypatients for the first few minutes of anexamination.
Many glaucoma patients are plaguedby ocular surface disease, which makesus wonder whether the medicationshave something to do with it. Even withlaser and glaucoma surgery, the majorityof glaucoma patients still rely onnumerous topical medications to con-trol their disease. One common ingredi-ent in many of these medications is thepreservative benzalkonium chloride(BAK).
We worry about anything that mayreact on the ocular surface, but arepreservatives such as BAK bad for theeye? In fact, they do serve a function.They provide an antimicrobial environ-
ment to allow the prolonged use ofmedications. This enables practitionersto have multiuse medications. Whilethis is positive, the downside is thatpatients can have allergic reactions tothe preservative. Glaucoma specialistswho are treating blinding disease areoften tempted to sweep such allergicreactions “under the rug.” The thinkingis that by comparison to glaucoma, anallergic reaction tends to be an episodicsymptomatic issue for patients but isnot something that will likely causethem to lose vision. Patients will oftenchoose to remain on medications ratherthan opt for laser trabeculoplasty orincisional surgery. In addition, there justaren’t too many BAK-free medicationsfrom which to choose.
Chronic EffectThe effect that chronic glaucoma med-ication use has on the conjunctiva isalso worthy of consideration. Thesemedications have been known to induceinflammation in experimental models.Tear samples from glaucoma patientshave greater amounts of inflammatorycytokines compared to their normalcounterparts. Also, conjunctival biopsysamples obtained at the time of tra-beculectomy show a correlation betweengreater numbers of medications andgreater amounts of sub-epithelialinflammation.
The use of glaucoma medicationsalso puts the success of glaucoma filter-ing surgery at risk. A link between med-ications with BAK and trabeculectomyfailures has been noted. Investigatorslaunched a study of 124 patients todetermine the effect of long-term topicalanti-glaucoma therapy on the results ofglaucoma filtration surgery. In the study,112 patients underwent trabeculectomyand 12 underwent a triple procedure oftrabeculectomy, cataract extraction, andintraocular lens implantation.1 A con-junctival biopsy was obtained at the
Clinical Implications of Preservativesin Glaucoma Medications
“ While practicallyspeaking it might bedifficult to takeglaucoma patientsoff their medicationsfor a month prior totrabeculectomy, it isgood to know thatwe can reversedamage to theconjunctiva.”
Douglas J. Rhee, M.D.
Rabbit studies suggest that preservative-freeTimolol helps to spare the conjunctiva frominflammation.
6 Managing Ocular Surface Disease in Glaucoma Patients
time of surgery. At the six-months post-op, investigators found that for patientswho had primary trabeculectomies andwere medication naïve, the success rateswere similar to those in a group treatedwith beta blockers. These results werebetter than those for patients treatedwith both beta blockers and miotics.The group that fared the worst were onseveral drugs: beta blockers, miotics, andsympathomimetics. Results suggestedthat the more medication patients weretaking, the worse they fared.
Practitioners have subsequently usedthis as the basis to say that the amountof preservatives affected the success andfailure rates of trabeculectomy.Although this could be the case, thestudy design does not exclude the possi-bility that the pharmacologic agentsthemselves were the cause of the prob-lem. Alternatively, patients on moremedications could have simply hadworse disease, inevitably doing morepoorly in the end.
Also, although these studies werewell designed, some of the glaucoma
medications that were investigated, suchas miotics like pilocarpine and sympath-omimetics like epinephrine, are notcommonly part of the medication arse-nal anymore.
There is some thought that the med-ications themselves may be the cause ofthe surgical failure. All glaucoma med-ications appear to have the ability tocause hyperemia potentially increasingsurface bleeding at the time of surgery.Meanwhile, prostaglandin analogues(PGA) are known to affect matrix metal-loproteinases both inside the eye andsclera and could have an effect on con-junctival wound healing. In addition, allPGAs are vasodilatory. Topical carbonicanhydrase inhibitors, which like mosttopical medications still contain BAK,are delivered in balanced pH solutionsto allow for adequate solubility. Also,several alpha agonists are vasoconstric-tive, but are known to cause a follicularconjunctival reaction. So, all the med-ications have the possibility of interfer-ing with surgical results, or it may bethat BAK is the source of the problem.
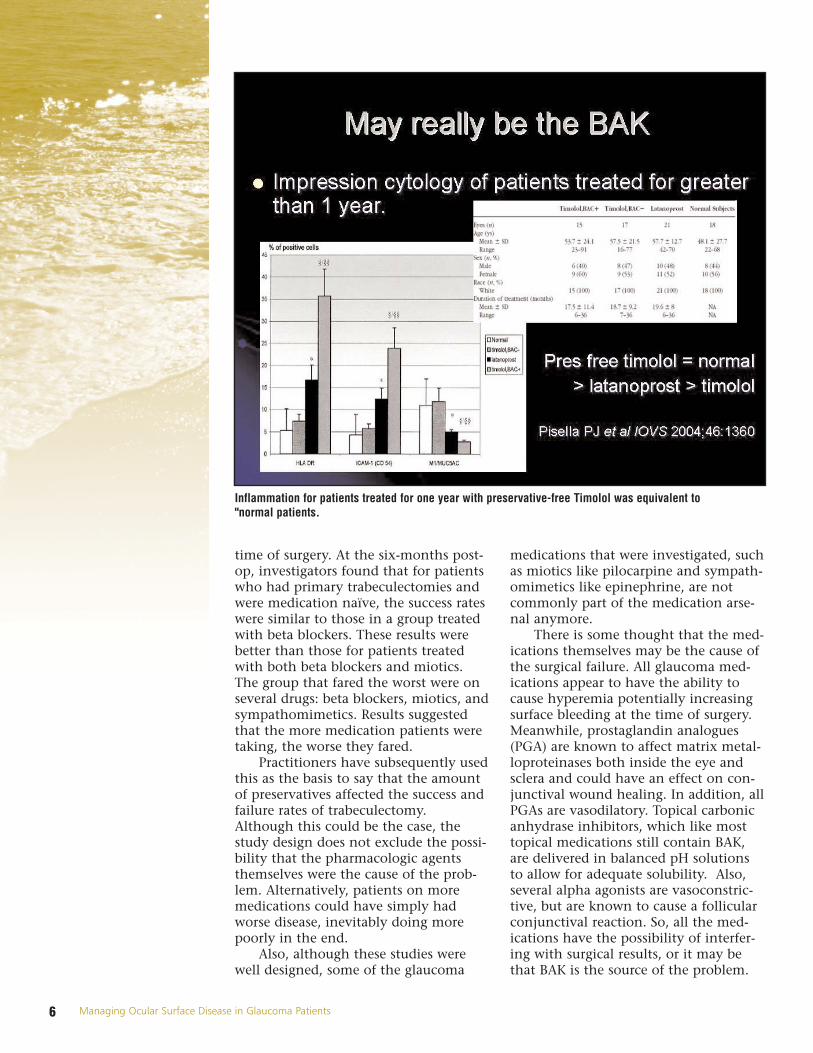
Inflammation for patients treated for one year with preservative-free Timolol was equivalent to"normal patients.

7Managing Ocular Surface Disease in Glaucoma Patients
A more convincing link to BAK wasfound in one study where investigatorsperformed cytology on patients whowere treated for over one year with oneof three agents: preservative-freeTimoptic (Merck, Whitehouse Station,N.J.), preserved timolol, or aprostaglandin analog. Using impressioncytology, they found that the amount ofinflammation for those using the preser-vative-free Timoptic was equivalent tonormals, and better than those on eitherthe prostaglandin analog or preservedtimolol. Those on the preserved timololhad the most inflammation of all thepatients.2
Reversing the DamageWe wonder what happens whenpatients stop taking these medications.Are the effects on the conjunctivareversible? A group of investigators inone study took 30 patients who werereceiving chronic epinephrine off theagent for one month and began treat-ment with the topical corticosteroidFML (1% fluorometholone, Allergan,Irvine, Calif.). They found that theeffects on the conjunctiva were reversed.During a one month period, investiga-tors noted a significant decrease in thenumber of fibroblasts and inflammatorycells throughout the conjunctiva.3
While practically speaking, it mightbe difficult to take glaucoma patients offtheir medications for a month prior totrabeculectomy, it is good to know thatwe may be able to reverse damage to theconjunctiva. The outcomes of the tra-beculecomies were also investigated,with results for 16 trabeculectomypatients compared with 16 matchedpatients whose pre-op regimens had notbeen altered. The investigators foundthat the trabeculectomies were ultimate-ly more successful for those patientswho had received pre-op FML.Investigators suggested that it might bebeneficial for practitioners to try a simi-lar regimen to improve the success ratesof trabeculectomy for patients.2
Indeed, as a result of this study,many glaucoma specialists do pre-treatpatients with corticosteroids for at leasta day before surgery. However, there isno strict consensus on this practicebecause patients in this study were off
their medications for one month andmost glaucoma patients who requiresurgery just can’t be washed out for thatlong.
There is a growing body of evidencethat chronic use of glaucoma medica-tion is associated with conjunctivalinflammation, with many glaucomapatients suffering from ocular surfacedisease.
For those who are looking for alter-natives for their patients, the only pre-servative-free medication that’s availableis timolol, which comes in unit dosevials that need to be specially ordered.For those who want to avoid BAK, thereare three other options that containalternative preservatives: Alphagan P(brimonidine, Allergan, Irvine, Calif.),which has a purite preservative;Travatan Z (travoprost, Alcon, FortWorth, Texas) which uses the alternativepreservative Sofzia; and PhospholineIodide (echothiophate iodide withchlorobutanol, Wyeth-Ayerst, PearlRiver, N.Y.). The latter, however, is nolonger considered a first-line agent.Even though these studies concerningBAK have been going on for the last 15years, many practitioners, includingmyself, have for the large part ignoredthem. The thinking on this has been,“Well, what else am I going to do?”
Now, with the advent of new med-ications using alternative preservativessuch as Alphagan and Travatan Z, we arestarting to enter an era where we andour patients have more flexibility. Withnumerous glaucoma patients sufferingfrom ocular surface disease either as aprimary event or secondary to theirmedications, we whole-heartedly wel-come measures that would improve thequality of life of these sufferers.
References1. Broadway, D. C., Adverse effects of topical
antiglaucoma medication. II. The outcome of filtra-tion surgery, Archives Ophthalmol. November1994:112:1446-1454.
2. Pissella, P.J., Conjunctival proinflammatory andproapoptotic effects of latanoprost and preservedand unpreserved timolol: an ex vivo and in vitrostudy. Investigative Ophthalmology and VisualScience, May 2004: 45:1360-1368.
3. Broadway, D.C., Reversal of topical anti-glaucomamedication effects on the conjunctiva. Archives ofOphthalmology, March 1996:114:262-267.

8
Richard W. Yee, M.D. is clinicalprofessor, University of Texas,Houston Medical School,Department of Ophthalmologyand Visual Science.
by Richard W. Yee, M.D.
For glaucoma patients, ocular sur-face disease is more commonthen most believe. Some surveysput the number of patientsaffected by dry eye around 40%,
but given that most glaucoma doctorsdon’t evaluate for ocular surface and thenumber of medications that thesepatients are taking, the number is likelyhigher—perhaps as high as 60%.
Glaucoma patients tend to be part ofthe elderly population. These patientsare usually on one medication or morethat contain benzalkonium chloride(BAK). While BAK helps protect againstsecondary bacteria contamination andincreases penetration of the medication,it has a downside. It is fairly toxic to thesurface of the eye. When it comes incontact with the eye, it breaks junctionsopen of epithelial cells. In addition, itchanges the ocular surface characteristicsby increasing the breakup time of tears.
This tear breakup time is a measure-ment of how well the ocular surface isprotected between blinks. Patientswhose breakup time is normal have aprotective coating present for about tenseconds or so after they blink. However,the tear film layer breaks down morerapidly if exposed to BAK. As a result,patients develop dry spot cycles such asthe normal blink interval, or staring at acomputer screen. As the cycle repeatsitself, there are problems of desiccation,which in turn incite all of the inflam-matory pathways.
Chronic InflammationAs a result, chronic use of medicationcontaining BAK incites inflammatorycytokines to the ocular surface. Thesecytokines can be upregulated in the con-junctival cells as well as the trabecularmeshwork cells. Also, the amount ofBAK that reaches the surface appears to
Physiologic Impact of Preservativesin Topical Glaucoma and Dry Eye
“ In patientswho have glaucoma,we have found thatwhen they are onmultiple medicationscontaining BAK,they do developlymphocytes andmacrophages, whichcan in turn result inthe upregulationof inflammatorycytokines.”
Richard W. Yee, M.D.
Managing Ocular Surface Disease in Glaucoma Patients
A tear film exposed to BAK breaks down more rapidly than at the usual ten second intervals.

9
be connected to the degree of inflamma-tion that is found in a dose dependentfashion. So, the more drugs containingBAK are used, the more inflammation isseen.
However, over a short period oftime, some use of BAK appears to befine. The eye has enough time to regen-erate and patients often do not haveany problems. However, it is a differentstory when use is prolonged. The heal-ing corneal ocular surface is a greatexample of what toxic medications cando to the corneal epithelium over timeand how this can be problematic insome cases. For example, in cases wherea patient is taking an antibiotic for aweek at a time, usually there is no diffi-culty. However, if a patient is using aglaucoma drop every day for months toyears at a time, the cornea doesn’t havea chance to recover. BAK is continuallybreaking up the ocular surface, chroni-cally causing it to desiccate and dry. Asa result, these patients often complainof symptoms such as dryness and red-ness.
Surgical Wound HealingIn addition to impacting patient com-fort, the health of the ocular surface canalso have an impact on ocular surgicaloutcomes. We find that it is importantthat the surface is pristine during thewound healing period. When perform-ing PRK or LASEK, I take special care toensure that we don’t create toxicity onthe surface and that we optimize theenvironment to promote speedy woundhealing. When a wound heals optimallyand in a rapid fashion, there is lesschance of upregulating problematicwound healing elements such as badcytokines, which can result in haze insurface ablation.
We follow a parallel model for casesof trabeculectomy. We want healing totake place in affected areas but not tothe point that the bleb shuts off.Unfortunately, that’s what happens incases of abnormal wound healing. Weneed to be vigilant with ocular surfacedisease because this may actually causeproblems in the healing. As a result,there may be more scarring or abnormalblebs. Although we do not have defini-tive proof on this, we do believe that
healing abnormalities could be relatedto the lack of optimization of the ocularsurface.
We have found that when patientswho have glaucoma are on multiplemedications containing BAK, theydevelop lymphocytes and macrophages,which can in turn result in the upregu-lation of inflammatory cytokines.1
Other work has shown that adverseeffects of topical antiglaucoma medica-tion can be reversed. In one investiga-tion, patients stopped their use of glau-coma medications for one month andwere treated with steroids. Investigatorsfound a notable decrease in the numberof fibroblasts and inflammatory cellsthroughout the conjunctiva. They alsosaw trabeculectomy success rise from50% to 80%,2 which illustrates theimportance of a pristine ocular surface.In this case, a two-pronged approachwas tried. One was the use of FML tosuppress the inflammatory reactions ofthe fibroblasts and inflammatory cellsthat were present and the other was tostop the use of the offending glaucomamedications containing BAK for onemonth.
Keeping all this in mind, we thinkthat it is better to optimize the surfacefor any procedure that needs healing inthe eye—be it surface ablation or glau-coma surgery. This way you can helpavoid abnormal wound healing andscarring scenarios.
We do this with our patients.Everything that we use in the eye weput in our tissue culture systems in ourlaboratory to make sure that they’re notacutely toxic to the cells. That’s why wefelt that it was important to test BAK-free Travatan Z in our tissue culture sys-tem. We then compared this to otherantibiotics such as gentamycin, usingboth the tear substitute, Systane (Alcon,Fort Worth, Texas) and tissue media ascontrols, as well as to another glaucomaagent Xalatan (Pfizer, New York, N.Y.),which contains BAK. We found that theTravatan Z without BAK fared signifi-cantly better with less toxicity than theXalatan.
Clinical UseClinically, I feel that it is important totry to minimize the amount of BAK on
Managing Ocular Surface Disease in Glaucoma Patients

10
the ocular surface even for those on mul-tiple glaucoma medications. Eventhough some of these medications willcontain BAK, we think that the effect onthe ocular surface is dose dependent onthose who are on more medications andare more likely to have more infiltrates.
When it comes to glaucoma medica-tions, I see Travatan Z as a breakthroughbecause it is the first alternative multi-dose prostaglandin analogue that doesnot contain BAK. While there are otherpreservative-free glaucoma drugs avail-able, these are typically expensive andinvolve single-use dosing. Of course,there is also Alphagan P (Allergan,Irvine, Calif.), but this is not aprostaglandin analogue.
Going forward, having BAK-freeoptions can only help our patients. Inthe past, if a glaucoma patient developedsensitivity to BAK there was nothing elseto choose from. It became a matter ofthe lesser of two evils—glaucoma or sur-
face toxicity. Now we are fortunate tohave some choices to remedy the glau-coma and without adding toxicity ormorbidity to the ocular surface.
Ultimately, I believe that this is rev-olutionary for ophthalmology in termsof how we think about the drugs thatwe add to the eye. Perhaps when weprepare new pharmaceuticals in thefuture we will do so knowing that we dohave alternatives and that we can createsafe and effective preservatives that donot interfere with the ocular surface andstill meet United States Pharmacopeia(USP) requirements.
References1. Baudouin C, et al. Ocular surface inflammatory
changes induced by topical antiglaucoma drugs.Ophthalmology. 1999; 106: 556 – 563.
2. Broadway D.C., Reversal of topical antiglaucomamedication effects on the conjunctiva. Archives ofOphthalmology. March 1996; 114: 262 -267.
Managing Ocular Surface Disease in Glaucoma Patients
Chronic use of BAK incites inflammatory cytokines to the ocular surface.

11
Richard Lewis, M.D. is assistantclinical professor, University ofCalifornia-Davis, Sacramento
Safety and Efficacy of Preservative-freeGlaucoma Medications
by Richard A. Lewis, M.D.
Prostaglandin analogues are anintegral part of treatment forglaucoma patients. However,there is a wide body of evi-dence suggesting that the
chronic application of these medicationsis deleterious to the ocular surface.Practitioners have wondered for sometime what is at the root of this problem.The question has arisen whether diffi-culties with the ocular surface are theresult of the active ingredient or a func-tion of the preservatives in the drops.
The preservative most often used inglaucoma drops, such as theprostaglandin analogues, is benzalkoni-um chloride (BAK). This is frequentlyplaced in multi-dose eye drops to pro-tect against microbial contamination.We find that BAK is effective in twoways here. First, it acts like a detergentand is a very effective agent for prevent-ing microbial contamination. Second, itenhances the corneal penetration ofsome drugs by causing epithelial separa-tion. BAK helps to enhance penetration,which explains how it helped back inthe early days of ophthalmology whenpractitioners had to use high concentra-tions of drugs such as pilocarpine topenetrate the eye. With the addition ofBAK, the drug was able to penetrate theeye much more easily and less of thedrug could be used.
Potential BAK ProblemsDespite all its benefits, BAK has somenegative effects. It compromises theepithelium and impairs healing. It alsoincreases conjunctival inflammatorycells and causes a loss of goblet cells.Ultimately, it affects tear functionincluding the tear film breakup time.Even at extremely low concentrations,BAK can cause cell death. When youexpose human cells to different concen-trations of BAK for 10 minutes, a con-centration as low as .0001% is all that isneeded to induce cell growth arrest anddeath by necrosis or apoptosis.1
BAK can also lead to problems withglaucoma surgeries. In trabeculectomy,bleeding, scarring and other problemscan result from long-term application ofmedications—particularly those withpreservatives. There is a risk of scarringfor patients having trabeculectomy whoare on chronic long-term drops. Tissuebiopsies of the conjunctiva show infil-tration in the subconjunctival tissue offibroblastic cells. This led to the intro-duction of 5FU and mitomycin C(MMC) to control this type of fibroblas-tic response and to try to prevent thescarring that practitioners were facing inglaucoma surgery.
Unfortunately, the effect of BAK iscumulative. Elderly patients on long-term glaucoma treatment with thesemultiple topical medications ultimatelyhave decreased tear secretion. The use ofBAK can also result in glaucoma surgicalcomplications, as well as ocular surfacedisease. Such ocular surface disease maycontribute to poor patient compliancewith some individuals who will skipdoses of their glaucoma medication orfail to take it altogether.
Through the years, many glaucomadrugs have included BAK in varyingconcentrations. However, we have feltthat it would be nice to get away fromthe use of BAK either by using an alter-native preservative or no preservativeat all.
New BAK-free AgentBut what would be the profile of a desir-able alternative for an IOP loweringagent? We would hope that such anagent would be BAK-free, have good IOPlowering efficacy with enduring effects,be well-tolerated, and come in a multi-dose bottle. We would also expect that itwould have the same or at least similarcosts to what we expect from currentagents and have antimicrobial activitymeeting or exceeding the regulatorystandards.
“ What would bethe profile of adesirable alternativefor an IOP loweringagent? We wouldhope that such anagent would beBAK-free, havegood IOP loweringefficacy withenduring effects,be well-tolerated,and come in a multi-dose bottle.”
Richard Lewis, M.D.
Managing Ocular Surface Disease in Glaucoma Patients

12
A clinical glaucoma group recentlyput this challenge to Alcon, askingwhether they could come up with analternative agent for lowering pressurethat didn’t include BAK. In answer tothis, they developed Travatan Z (AlconLaboratories, Fort Worth, Texas). Recentstudy results comparing the safety andefficacy of Travatan (Alcon) with andwithout BAK have been very promisingin that regard.2 The large multicenterstudy included 700 open-angle glaucomaor ocular hypertension patients withpressures between 24 and 36 mm Hg,with at least one eye able to qualify foreach of the six time points. In this dou-ble-masked, randomized, parallel groupstudy, the medication was dosed once aday in the evening and IOP was meas-ured during the course of the day atthree different intervals.
The results showed that BAK is notnecessary for drug penetration, which isjust what practitioners were hoping for.This drug remains effective despite thefact that alternative ways are used to pre-serve the compound. Across all ninestudy visits, the mean IOP reductionrange was between 7.3 and 8.5 mm Hg.Most importantly, there was a statisticalequivalence concerning the mean IOPchanges between Travatan with andwithout BAK. When it came to complica-tions, these were similar for the twogroups. Results indicated that 6.4% ofpatients treated with the BAK-free ver-sion of Travatan experienced problemswith hyperemia compared with 9% ofthose treated with the original formula-tion. Also, none of the patients using theBAK-free version needed to discontinuethe drug as a result of hyperemia.
Both drugs offer very similaramounts of penetration. Therefore, whenyou have a drug that penetrates as wellas Travatan, BAK is unnecessary toenhance penetration.
In addition to its excellent penetra-tion, Travatan has remarkable endurance
in lowering IOP. This was illustrated in adouble-masked, randomized study of106 patients. Those included in this par-allel group, multi-center trial received adose of placebo once in the morningand a dose of Travatan once in theevening. Patients were assessed at twoweeks to see how long it lowered pres-sure.3 Investigators found that the travo-prost molecule provided great pressurelowering for up to 60 hours after thedose was first administered. This is goodnews for patients who have question-able compliance and may miss a dose.This means that we will still see suffi-cient pressure lowering and good main-tenance of their IOP.
Overall, we find that BAK has somesignificant negative effects in terms ofhealing and tear function. It can alsoaffect the outcomes of glaucoma sur-gery. We hope to find a desirable alter-native IOP lowering agent that wouldnot require BAK. Research has shownthat Travatan Z without BAK is equiva-lent to Travatan in both safety and effi-cacy. Both have a low incidence of ocu-lar hyperemia. The IOP loweringendurance of the BAK-free formulationof Travatan Z is equal to the originalTravatan. This BAK-free ocular medica-tion offers a beneficial alternative.Going forward, the hope is that glauco-ma specialists will begin to seek moreand more medications without BAK toin order provide a better ocular surfacefor our glaucoma patients.
References1. De Saint, Jean M., et al. Effects of benzlkonium
chloride on growth and survival of Chang conjunc-tival cells. Invest Ophthalmol Vis Sci, March 1999;40:619-630.
2. Lewis, R.A., Travoprost 0.004% with and withoutbenzalkonium chloride: a comparison of safetyand efficacy. Journal of Glaucoma, January2007;161:98-103
3. Data on file: Alcon Laboratories, Inc.
Managing Ocular Surface Disease in Glaucoma Patients