august 2018- gastroparesis awareness month · an electrogastrogram, another experimental study that...
TRANSCRIPT

August 2018- Gastroparesis Awareness Month
A note from the author— Hello NCP friends! I hope everyone is enjoying the sun, hot weather, and beach days. For this month’s health ministry, I wanted feature a health condition that is not every well known… Gastroparesis. This condition is considered rare (fewer than 200,000 cases per year in the United States), but is chronic and incurable. This month, learn more about this disease by reading more below. Happy August!
What is Gastroparesis Awareness Month? August is Gastroparesis Awareness Month. With sponsorship by the International Foundation for Functional Gastrointestinal Disorders (IFFGD), Gastroparesis Awareness Month was listed on the U.S. National Health Observances Calendar beginning in 2016. Health observances are days, weeks, or months devoted to promoting particular health concerns. Individuals, health professionals, teachers, community groups, and others can use these special times to sponsor health promotion events and stimulate awareness of health issues.

Gastroparesis is a gastrointestinal disorder that can cause mild to severe symptoms. In rare cases, gastroparesis can even become life threatening. However, there is still much to be learned about how to diagnose and treat this condition. The IFFGD works to focus attention on important health messages about gastroparesis diagnosis, treatment, and quality of life issues. The goals include improving understanding of gastroparesis to help patients and families manage the condition, and encouraging preventive strategies. The IFFGD encourages people experiencing the symptoms of gastroparesis to consult their physicians and to browse their web pages or contact them to receive information regarding the condition.
What is Gastroparesis? Gastroparesis is a disorder that occurs when the stomach takes too long to empty food. This disorder, also known as delayed gastric emptying, is a result of weak or abnormal muscles in the stomach. Gastroparesis is a condition that affects the normal spontaneous movement of the muscles (motility) in your stomach, which means there is a weakness of the muscles of the stomach. Ordinarily, strong muscular contractions propel food through your digestive tract. But if you have gastroparesis, your stomach's motility is slowed down or doesn't work at all, preventing your stomach from emptying properly.

Gastroparesis results in poor grinding of food in the stomach into small particles and slow emptying of food from the stomach into the small intestine. When the contractions of the stomach’s muscles are weakened, food is not thoroughly ground and does not empty into the intestine normally. Since the muscular actions whereby solid food and liquid food are emptied from the stomach are slightly different, the emptying of solids and liquids follows different time courses, and there may be slow emptying of solid food (most common), solid and liquid food (less common), or liquid food alone (least common). Certain medications, such as opioid pain relievers, some antidepressants, and high blood pressure and allergy medications, can lead to slow gastric emptying and cause similar symptoms. For people who already have gastroparesis, these medications may make their condition worse. Gastroparesis can interfere with normal digestion, cause nausea and vomiting, and cause problems with blood sugar levels and nutrition. The cause of gastroparesis is usually unknown. Sometimes it's a complication of diabetes, and some people develop gastroparesis after surgery. Although there's no cure for gastroparesis, changes to your diet, along with medication, can offer some relief.
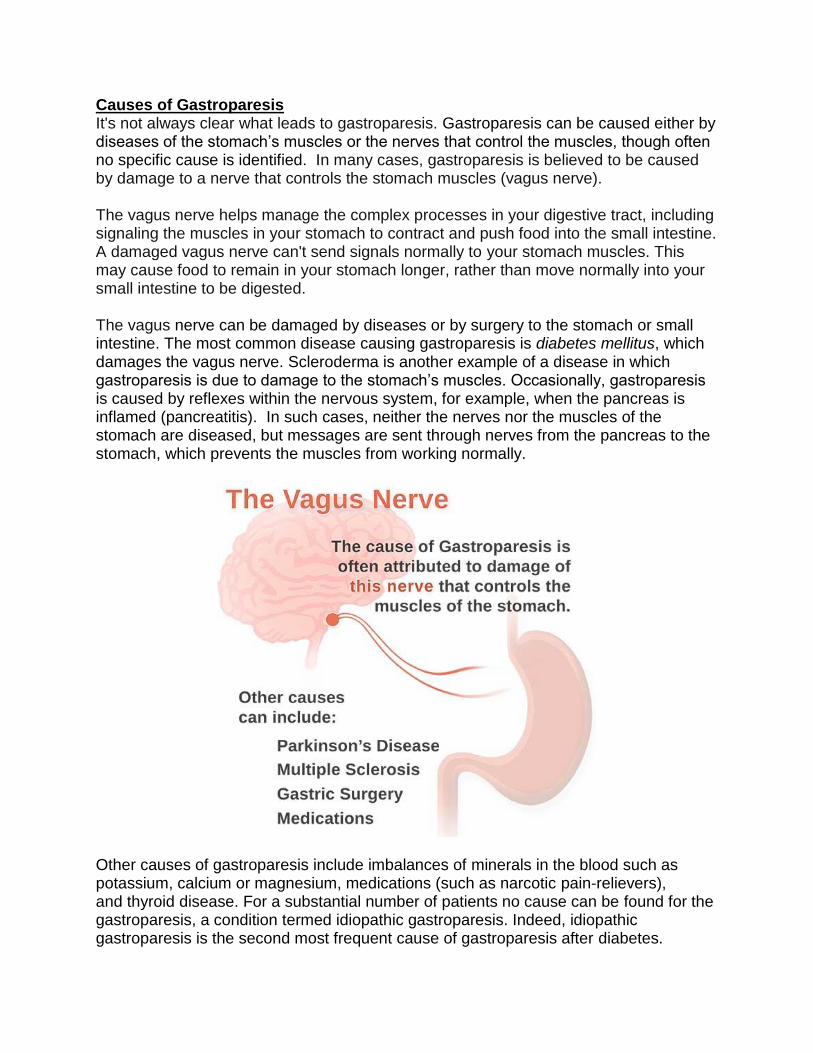
Causes of Gastroparesis It's not always clear what leads to gastroparesis. Gastroparesis can be caused either by diseases of the stomach’s muscles or the nerves that control the muscles, though often no specific cause is identified. In many cases, gastroparesis is believed to be caused by damage to a nerve that controls the stomach muscles (vagus nerve). The vagus nerve helps manage the complex processes in your digestive tract, including signaling the muscles in your stomach to contract and push food into the small intestine. A damaged vagus nerve can't send signals normally to your stomach muscles. This may cause food to remain in your stomach longer, rather than move normally into your small intestine to be digested. The vagus nerve can be damaged by diseases or by surgery to the stomach or small intestine. The most common disease causing gastroparesis is diabetes mellitus, which damages the vagus nerve. Scleroderma is another example of a disease in which gastroparesis is due to damage to the stomach’s muscles. Occasionally, gastroparesis is caused by reflexes within the nervous system, for example, when the pancreas is inflamed (pancreatitis). In such cases, neither the nerves nor the muscles of the stomach are diseased, but messages are sent through nerves from the pancreas to the stomach, which prevents the muscles from working normally.
Other causes of gastroparesis include imbalances of minerals in the blood such as potassium, calcium or magnesium, medications (such as narcotic pain-relievers), and thyroid disease. For a substantial number of patients no cause can be found for the gastroparesis, a condition termed idiopathic gastroparesis. Indeed, idiopathic gastroparesis is the second most frequent cause of gastroparesis after diabetes.

Gastroparesis can occur as an isolated problem or it can be associated with weakness of the muscles of other parts of the intestine, including the small intestine, colon, and esophagus.
What increases your Risk for Gastroparesis? Factors that can increase your risk of gastroparesis:
Diabetes Abdominal or esophageal surgery Infection, usually a virus Certain medications that slow the rate of stomach emptying, such as narcotic pain
medications Scleroderma (a connective tissue disease) Nervous system diseases, such as Parkinson's disease or multiple sclerosis Hypothyroidism (low thyroid)
Women are more likely to develop gastroparesis than are men.
Symptoms of Gastroparesis Signs and symptoms of gastroparesis include:
Vomiting Nausea A feeling of fullness after eating just a few bites Vomiting undigested food eaten a few hours earlier Acid reflux Abdominal bloating Abdominal pain Changes in blood sugar levels Lack of appetite Weight loss and malnutrition

The primary symptoms of gastroparesis are nausea and vomiting. Other symptoms of gastroparesis include bloating with or without abdominal distension, early satiety (feeling full quickly when eating), and in severe cases, weight loss due to a reduced intake of food because of the symptoms. Abdominal pain also is present frequently though the cause of the pain is unclear. Reduced intake of food and restriction of the types of food that are eaten can lead to nutritional deficiencies.
The vomiting of gastroparesis usually occurs after meals; however, with severe gastroparesis, vomiting may occur without eating due simply to the accumulation of secretions in the stomach. The characteristic vomiting happens several hours after a meal when the stomach is maximally distended by the presence of food and secretions stimulated by the meal. Since the grinding action of the stomach is absent, the vomited food often contains larger pieces of recognizable food. (This can be contrasted with the more common type of vomiting in which the food appears as small, uniform, unidentifiable particles.) Other, less frequent effects of gastroparesis are the promotion of gastroesophageal reflux disease (GERD) and malnutrition. Many people with gastroparesis don't have any noticeable signs and symptoms. Make an appointment with your doctor if you have any signs or symptoms that worry you.

The Negative Impact of Gastroparesis Gastroparesis can cause several complications, such as:
Severe dehydration. Ongoing vomiting can cause dehydration. Malnutrition. Poor appetite can mean you don't take in enough calories, or you
may be unable to absorb enough nutrients due to vomiting. Undigested food that hardens and remains in your stomach. Undigested food
in your stomach can harden into a solid mass called a bezoar. Bezoars can cause nausea and vomiting and may be life-threatening if they prevent food from passing into your small intestine.
Unpredictable blood sugar changes. Although gastroparesis doesn't cause diabetes, frequent changes in the rate and amount of food passing into the small bowel can cause erratic changes in blood sugar levels. These variations in blood sugar make diabetes worse. In turn, poor control of blood sugar levels makes gastroparesis worse.
Decreased quality of life. An acute flare-up of symptoms can make it difficult to work and keep up with other responsibilities.
Diagnosing Gastroparesis The most common method for diagnosing gastroparesis is a nuclear medicine test called a gastric emptying study, which measures the emptying of food from the stomach. For this study, a patient eats a meal in which the solid food, liquid food, or both contain a small amount of radioactive material. A scanner (acting like a Geiger counter) is placed over the stomach for several hours to monitor the amount of radioactivity in the stomach. In patients with gastroparesis, the food takes longer than normal (usually more than several hours) to empty into the intestine.

The antro-duodenal motility study is a study that can be considered experimental and is reserved for selected patients. An antro-duodenal motility study measures the pressure that is generated by the contractions of the muscles of the stomach and intestine. This study is conducted by passing a thin tube through the nose, down the esophagus, through the stomach and into the small intestine. With this tube, the strength of the contractions of the muscles of the stomach and small intestine can be measured at rest and following a meal. In most patients with gastroparesis, food (which normally causes the stomach to contract vigorously) causes either infrequent contractions (if the nerves are diseased) or only very weak contractions (if the muscle is diseased).
An electrogastrogram, another experimental study that sometimes is done in patients with suspected gastroparesis, is similar to an electrocardiogram (EKG) of the heart. The electrogastrogram is a recording of the electrical signals that travel through the stomach muscles and control the muscles' contractions. An electrogastrogram is performed by taping several electrodes onto a patient's abdomen over the stomach area in the same manner as electrodes are placed on the chest for an EKG. The electrical signals coming from the stomach that reach the electrodes on the abdomen are recorded at rest and after a meal. In normal individuals, there is a regular electrical rhythm just as in the heart, and the power (voltage) of the electrical current increases after the meal. In most patients with gastroparesis, the rhythm is not normal or there is no increase in electrical power after the meal. Although the gastric emptying study is the primary test for diagnosing gastroparesis, there are patients with gastroparesis who have a normal gastric emptying study but an abnormal electrogastrogram. Therefore, the electrogastrogram can be useful primarily when the suspicion for gastroparesis is high but the gastric emptying study is normal or borderline abnormal. A physical obstruction to the emptying of the stomach, for example, a tumor that compresses the outlet from the stomach or scarring from an ulcer, may cause symptoms that are similar to gastroparesis. Therefore, an upper gastrointestinal

(GI) endoscopy test usually is performed to exclude the possibility of an obstruction as the cause of a patient's symptoms. (Upper GI endoscopy involves the swallowing of a tube with a camera on the end and can be used to visually examine the stomach and duodenum and take biopsies.) Upper GI endoscopy also may be useful for diagnosing one of the complications of gastroparesis, a bezoar (a clump or wad of swallowed food or hair). Because of the poor emptying of the stomach, hard to digest components of the diet, usually from vegetables, are retained and accumulate in the stomach. A ball of undigested, plant-derived material can accumulate in the stomach and give rise to symptoms of fullness or can further obstruct the emptying of food from the stomach. Removing the bezoar may improve symptoms and emptying. A computerized tomographic (CT) scan of the abdomen and upper gastrointestinal X-ray series also may be necessary to exclude cancer of the pancreas or other conditions that can obstruct the emptying of the stomach. An alternative method of looking at gastric emptying is a large capsule (SmartPill) that is swallowed. The capsule measures pressure, acidity and temperature, and then transmits the measurements wirelessly to a recorder. By analyzing the measurements it can be determined how long it takes the capsule to empty from the stomach, and the amount of time necessary for emptying correlates well with other measures of gastric emptying. Most Common Diagnostic Testing Doctors use several tests to help diagnose gastroparesis and rule out conditions that may cause similar symptoms. Tests may include:
Gastric emptying study. This is the most important test used in making a diagnosis of gastroparesis. It involves eating a light meal, such as eggs and toast, that contains a small amount of radioactive material. A scanner that detects the movement of the radioactive material is placed over your abdomen to monitor the rate at which food leaves your stomach. You'll need to stop taking any medications that could slow gastric emptying. Ask your doctor if any of your medications might slow your digestion.
Upper gastrointestinal (GI) endoscopy. This procedure is used to visually examine your upper digestive system — your esophagus, stomach and beginning of the small intestine (duodenum) — with a tiny camera on the end of a long, flexible tube. This test can also diagnose other conditions, such as peptic ulcer disease or pyloric stenosis, which can have symptoms similar to those of gastroparesis.

Ultrasound. This test uses high-frequency sound waves to produce images of
structures within your body. Ultrasound can help diagnose whether problems with your gallbladder or your kidneys could be causing your symptoms.
Upper gastrointestinal series. This is a series of X-rays in which you drink a white, chalky liquid (barium) that coats the digestive system to help abnormalities show up.
Treatment for Gastroparesis Gastroparesis is a chronic (long-lasting) condition. This means that treatment doesn’t cure the disease. But there are steps you can take to manage and control the condition. Some patients may benefit from medications. One of the best ways to help control the symptoms of gastroparesis is to modify your daily eating habits. People who have diabetes should try to control their blood sugar levels to minimize the problems of gastroparesis. A neuropsychiatric specialist is sometimes called in to address mental health concerns that can accompany this chronic disease. If you wake up sick every day and vomiting all the time, this disease can quickly move from a purely physical one to a psychiatric one, so it is good to treat the possible components of depression, anxiety, pain and so on, too.
Treating gastroparesis begins with identifying and treating the underlying condition. If diabetes is causing your gastroparesis, your doctor can work with you to help you control it. Changes to your diet Maintaining adequate nutrition is the most important goal in the treatment of gastroparesis. Many people can manage gastroparesis with diet changes and dietary changes are the first step in managing this condition. Your doctor may refer you to a dietitian who can work with you to find foods that are easier for you to digest so that

you're more likely to get enough calories and nutrients from the food you eat. A dietitian might suggest that you try to:
Eat smaller meals more frequently Chew food thoroughly Eat well-cooked fruits and vegetables rather than raw fruits and vegetables Avoid fibrous fruits and vegetables, such as oranges and broccoli, which may
cause bezoars Choose mostly low-fat foods, but if you can tolerate them, add small servings of
fatty foods to your diet Try soups and pureed foods if liquids are easier for you to swallow Drink about 34 to 51 ounces (1 to 1.5 liters) of water a day Exercise gently after you eat, such as going for a walk Avoid carbonated drinks, alcohol and smoking Try to avoid lying down for 2 hours after a meal Take a multivitamin daily
Here's a brief list of foods recommended for people with gastroparesis (your dietitian can give you a more comprehensive list): Starches
White bread and rolls and "light" whole-wheat bread without nuts or seeds Plain or egg bagels English muffins Flour or corn tortillas Pancakes Puffed wheat and rice cereals Cream of wheat or rice White crackers Potatoes, white or sweet (no skin) Baked french fries Rice Pasta
Protein
Lean beef, veal and pork (not fried) Chicken or turkey (no skin and not fried) Crab, lobster, shrimp, clams, scallops, oysters Tuna (packed in water) Cottage cheese Eggs Tofu Strained meat baby food
Fruits and vegetables
Baby food vegetables and fruits Tomato sauce, paste, puree, juice Carrots (cooked)

Beets (cooked) Mushrooms (cooked) Vegetable juice Vegetable broth Fruit juices and drinks Applesauce Bananas Peaches and pears (canned)
Dairy
Milk, if tolerated Yogurt (without fruit pieces) Custard and pudding Frozen yogurt
Medications Medications to treat gastroparesis may include:
Medications to stimulate the stomach muscles. These medications include metoclopramide (Reglan) and erythromycin (Eryc, E.E.S.). Metoclopramide has a risk of serious side effects. Erythromycin may lose its effectiveness over time, and can cause side effects, such as diarrhea. A newer medication, domperidone, with fewer side effects, is also available with restricted access.
Medications to control nausea and vomiting. Drugs that help ease nausea and vomiting include prochlorperazine (Compro) and diphenhydramine (Benadryl, Unisom). A class of medications that includes ondansetron (Zofran) is sometimes used to help nausea and vomiting.

Surgical treatment Some people with gastroparesis may be unable to tolerate any food or liquids. In these situations, doctors may recommend a feeding tube (jejunostomy tube) be placed in the small intestine. Or doctors may recommend a gastric venting tube to help relieve pressure from gastric contents. Feeding tubes can be passed through your nose or mouth or directly into your small intestine through your skin. The tube is usually temporary and is only used when gastroparesis is severe or when blood sugar levels can't be controlled by any other method. Some people may require an IV (parenteral) feeding tube that goes directly into a vein in the chest.
Treatments under investigation Researchers are continuing to investigate new medications to treat gastroparesis. One example is a new drug in development called relamorelin. The results of a phase 2 clinical trial found the drug could speed up gastric emptying and reduce vomiting. The drug is not yet approved by the Food and Drug Administration (FDA), but a larger clinical trial is currently underway. A number of new therapies are being tried with the help of endoscopy — a slender tube that's threaded down the esophagus. One procedure used endoscopy to place a small tube (stent) where the stomach connects to the small intestine (duodenum) to keep this connection open.

Several research trials investigated the use of botulinum toxin administered through endoscopy without much success. This treatment is not recommended. Doctors are also studying the use of a minimally invasive surgical technique when someone needs a feeding tube placed directly into the small intestine (jejunostomy tube). Gastric electrical stimulation and pacing Gastric electrical stimulation is a surgically implanted device that provides electrical stimulation to stimulate stomach muscles to move food more efficiently. Study results have been mixed. However, the device seems to be most helpful for people with diabetic gastroparesis. The FDA allows the device to be used under a compassionate use exemption for those who can't control their gastroparesis symptoms with diet changes or medications. However, larger studies are needed. Gastric pacing also involves a surgically implanted device that stimulates the stomach muscles, but this device tries to more closely mimic normal stomach contractions. Currently, the device is too large and causes discomfort. Gastric pacing devices are only available in clinical trials right now.

Lifestyle and home remedies If you're a smoker, stop. Your gastroparesis symptoms are less likely to improve over time if you keep smoking. People with gastroparesis who are overweight are also less likely to get better over time.
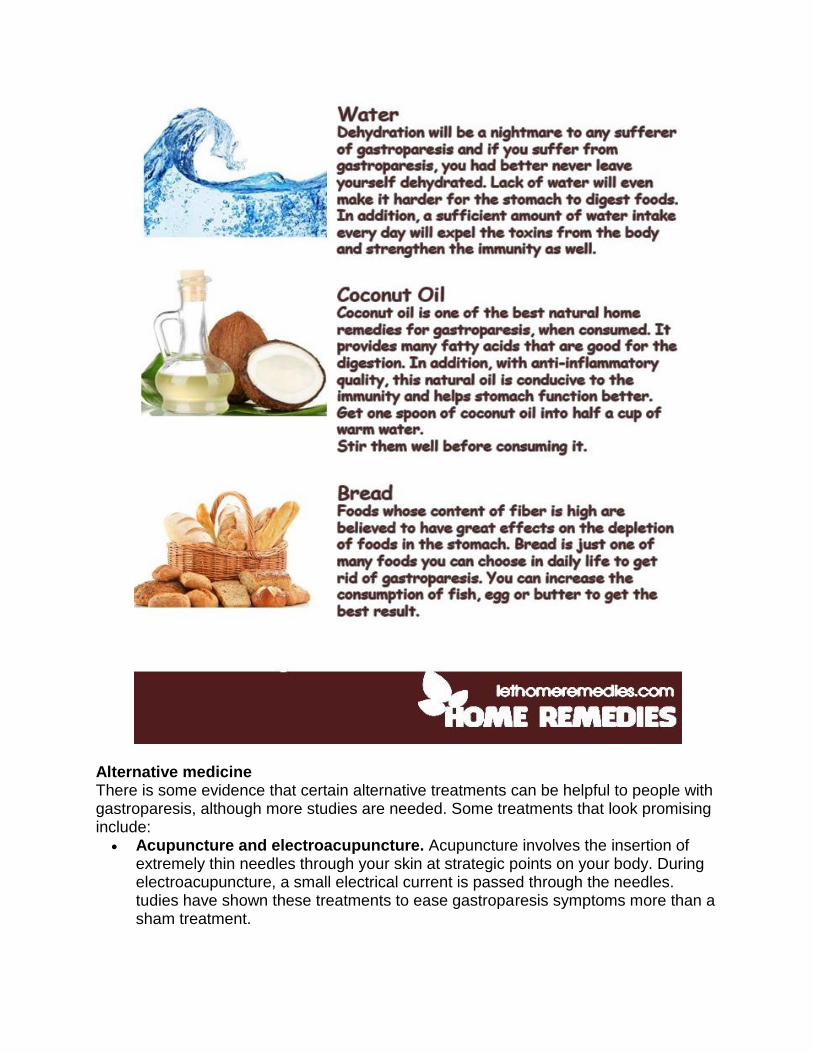
Alternative medicine There is some evidence that certain alternative treatments can be helpful to people with gastroparesis, although more studies are needed. Some treatments that look promising include:
Acupuncture and electroacupuncture. Acupuncture involves the insertion of extremely thin needles through your skin at strategic points on your body. During electroacupuncture, a small electrical current is passed through the needles. tudies have shown these treatments to ease gastroparesis symptoms more than a sham treatment.

STW 5 (Iberogast). This herbal formula from Germany contains nine different herbal extracts. It hasn't been shown to speed up gastric emptying, but was slightly better at easing digestive symptoms than a placebo.
Rikkunshito. This Japanese herbal formula also contains nine herbs. It may help reduce abdominal pain and the feeling of post-meal fullness.
Cannabis. There aren't any published clinical trials on cannabis and gastroparesis. However, cannabis — commonly known as marijuana — is thought to ease nausea and other digestive complaints. Derivatives of cannabis have been used by people who have cancer in the past, but there are better FDA-approved medications available to control nausea now. Because cannabis is often smoked, there's concern about possible addiction and harm, similar to what occurs with tobacco smoke. In addition, daily users of marijuana (cannabis) may develop a condition that mimics the symptoms of gastroparesis called cannabis hyperemesis syndrome. Symptoms can include nausea, vomiting and abdominal pain. Quitting cannabis may help.
Preparing for you Doctor’s Appointment You're likely to first see your primary care doctor if you have signs and symptoms of gastroparesis. If your doctor suspects you may have gastroparesis, you may be referred to a doctor who specializes in digestive diseases (gastroenterologist). You may also be referred to a dietitian who can help you choose foods that are easier to process.
What you can do Because appointments can be brief, it's a good idea to be well-prepared. To prepare, try to:
Be aware of any pre-appointment restrictions. At the time you make the appointment, be sure to ask if there's anything you need to do in advance, such as restrict your diet. Your doctor's office might recommend that you stop using certain pain medications, such as narcotics, prior to coming for an appointment.
Write down any symptoms you're experiencing, including any that may seem unrelated to the reason for which you scheduled the appointment.
Write down key personal information, including any major stresses or recent life changes.
Make a list of all medications, vitamins or supplements that you're taking. Consider taking a family member or friend along. Sometimes it can be difficult
to remember all the information provided during an appointment. Someone who accompanies you may remember something that you missed or forgot.
Write down questions to ask your doctor.
Questions to ask Your time with your doctor is limited, so preparing a list of questions will help you make the most of your time together. List your questions from most important to least important in case time runs out. For gastroparesis, some basic questions to ask your doctor include:
What's the most likely cause of my symptoms? Could any of my medications be causing my signs and symptoms? What kinds of tests do I need? Is this condition temporary or long lasting? Do I need treatment for my gastroparesis? What are my treatment options, and what are the potential side effects? Are there certain foods I can eat that are easier to digest? I have other health conditions. How can I best manage these conditions together? Should I see a dietitian?

Should I see a specialist? What will that cost, and will my insurance cover it? Are there brochures or other printed material that I can take with me? What
websites do you recommend? Do I need a follow-up visit? I have diabetes. How might gastroparesis affect my diabetes management?
In addition to the questions that you've prepared, don't hesitate to ask other questions during your appointment. What to expect from your doctor Your doctor is likely to ask you a number of questions. Being ready to answer them may allow more time later to cover other points you want to address. Your doctor may ask:
When did you first begin experiencing symptoms? Have your symptoms been continuous or occasional? How severe are your symptoms? Does anything seems to improve your symptoms? What, if anything, appears to worsen your symptoms? Did your symptoms start suddenly, such as after an episode of food poisoning? What surgeries have you had?

Resources https://www.mayoclinic.org/diseases-conditions/gastroparesis/symptoms-causes/syc-20355787 https://www.medicinenet.com/gastroparesis/article.htm https://aboutgastroparesis.org/gastroparesis-awareness-month.html https://www.accordclinical.com/news/august-gastroparesis-awareness-month/ https://www.g-pact.org/gastroparesis-awareness-month https://nursingassistantguides.com/2017/gastroparesis-awareness-month/