athletic activity clearance packet kern high school … · name: uid# athletic activity clearance...
TRANSCRIPT

1/19/18
Nam
e: U
ID #
Name: UID#
Athletic Activity Clearance Packet Kern High School District
The following forms must be filled out neatly and completely. Students will not
be allowed to participate until ALL forms have been completed and turned in to
__________________________________________High School Athletic office,
verified and issued a clearance card.
Check List: Academic Eligibility
2.0. GPA, Passed 4 courses, 20 units, but must be enrolled in 5 courses, 25 units
Physical Examination Form Completed by MD or DO per A.R. 6145.5
Emergency Cards (2 pages) Please fill out each section and list Preferred Hospital. All 3 cards must have parent signatures
Steroid Use Policy Agreement Student and Parent Signatures
Athletic Release/Consent to Participate Form (Risk Acknowledgement) Student and Parent Signatures
Discipline Code Summary Student and Parent Signatures
Concussion Acknowledgment Form Student and Parent Signatures
Ethics in Sport Student and Parent Signatures
Sudden Cardiac Arrest Parent Review Form Student and Parent Signatures
Physician Letter to School/ACE Form Student and Parent Signatures
Parent/Guardian keeps: Ethics in sports description; concussion fact sheet; Physician Letter/ACE evaluation form; SCA parent review Form
Sport GPA/Money Owed Clearance Date
Fall / Fall
Winter / Winter
Spring / Spring

1/19/18
PHYSICAL EXAMINATION FORM FOR STUDENTS
Name: UID#
Grade: School Site: Birth Date: Sex:
Father: Mother:
Address:
Parent Consent: Date:
Medical history to include: rheumatic fever, tuberculosis, epilepsy, allergies, operations, serious illnesses,
congenital defects and menstrual disturbances
Has your son/daughter had a concussion? Yes No
If so, how many? Date of Last concussion:
Immunization Recommendations:
Physical Examination
Check
Additional Remarks
Normal, Abnormal, Not Examined N A NE General Weight & Nutrition General Appearance Skin (Acne, Tinea, Dermatitis) Eyes (Conjunctivae, Cornea, EOM) Ears (Perforations, Deafness) Nose (Allergy, Deformities) Teeth (Cavities, Gingivitis, Occlusion) Tonsils Lymph Nodes Chest (Deformities) Lungs Heart (Size, Murmur, Rhythm) Breast Abdomen Hernias Genitalia Back (Kyphosis, Lordosis, Scoliosis) Skelton (Limited Motion, Deformities) Feet (Flat, Pronated, Tinea)
Blood Pressure: Height: Weight:
This student may participate in:
Competitive Sports Yes No
Regular Physical Education Yes No
Limited P.E. Only Yes Duration
Physician’s Signature Date
Type or print physician’s name License Number
PHYSICALS FROM A CHIROPRACTOR ARE NOT VALID FOR ATHLETIC CLEARANCE

1/19/18
KERN HIGH SCHOOL DISTRICT
PARENT MEDICAL CONSENT/ATHLETIC PARTICIPATION (Allows your student athlete to compete in sports and receive medical attention if needed.)
Previous Sport
Student Name:_ UID # Grade: 9 10 11 12 Sport:
Parent’s Name:_ Address: Home Phone:_
Student’s Date of Birth:_ Male/Female Work Phone:_
Month Day Year (Circle One)
In the events the parents cannot be contacted, please list another person to call:
Name: Relationship: Phone:
Name: Relationship: Phone:
Family Physician: Phone:_
Preferred Hospital: Phone:_
Insurance Company:_ POLICY #
LIST ANY MEDICATIONS/ALLERGIES:_
I HEREBY GIVE MY CONSENT FOR THE ABOVE NAMED STUDENT TO RECEIVE NECESSARY EMERGENCY MEDICAL
TREATMENT IF HE/SHE IS INJURED OR ILL WHILE PARTICIPATING ON A KHSD ATHLETIC TEAM.
PARENT SIGNATURE DATE
KERN HIGH SCHOOL DISTRICT
PARENT MEDICAL CONSENT/ATHLETIC PARTICIPATION (Allows your student athlete to compete in sports and receive medical attention if needed.)
Previous Sport
Student Name:_ UID # Grade: 9 10 11 12 Sport:
Parent’s Name:_ Address:_ Home Phone:_
Student’s Date of Birth:_ Male/Female Work Phone:_
Month Day Year (Circle One)
In the events the parents cannot be contacted, please list another person to call:
Name: Relationship: Phone:
Name: Relationship: Phone:
Family Physician: Phone:_
Preferred Hospital: Phone:_
Insurance Company:_ POLICY #
LIST ANY MEDICATIONS/ALLERGIES:_
I HEREBY GIVE MY CONSENT FOR THE ABOVE NAMED STUDENT TO RECEIVE NECESSARY EMERGENCY MEDICAL
TREATMENT IF HE/SHE IS INJURED OR ILL WHILE PARTICIPATING ON A KHSD ATHLETIC TEAM.
PARENT SIGNATURE DATE

1/19/18
KERN HIGH SCHOOL DISTRICT
Previous Sport
PARENT MEDICAL CONSENT/ATHLETIC PARTICIPATION (Allows your student athlete to compete in sports and receive medical attention if needed.)
Student Name:_ UID # Grade: 9 10 11 12 Sport:
Parent’s Name:_ Address:_ Home Phone:_
Student’s Date of Birth:_ Male/Female Work Phone:_
Month Day Year (Circle One)
In the events the parents cannot be contacted, please list another person to call:
Name: Relationship: Phone:
Name: Relationship: Phone:
Family Physician: Phone:_
Preferred Hospital: Phone:_
Insurance Company:_ POLICY #
LIST ANY MEDICATIONS/ALLERGIES:_
I HEREBY GIVE MY CONSENT FOR THE ABOVE NAMED STUDENT TO RECEIVE NECESSARY EMERGENCY MEDICAL
TREATMENT IF HE/SHE IS INJURED OR ILL WHILE PARTICIPATING ON A KHSD ATHLETIC TEAM.
PARENT SIGNATURE DATE
KERN HIGH SCHOOL DISTRICT
PARENT MEDICAL CONSENT/ATHLETIC PARTICIPATION (Allows your student athlete to compete in sports and receive medical attention if needed.)
Previous Sport
Student Name:_ UID # Grade: 9 10 11 12 Sport:
Parent’s Name:_ Address:_ Home Phone:_
Student’s Date of Birth:_ Male/Female Work Phone:_
Month Day Year (Circle One)
In the events the parents cannot be contacted, please list another person to call:
Name: Relationship: Phone:
Name: Relationship: Phone:
Family Physician: Phone:_
Preferred Hospital: Phone:_
Insurance Company:_ POLICY #
LIST ANY MEDICATIONS/ALLERGIES:_
I HEREBY GIVE MY CONSENT FOR THE ABOVE NAMED STUDENT TO RECEIVE NECESSARY EMERGENCY MEDICAL
TREATMENT IF HE/SHE IS INJURED OR ILL WHILE PARTICIPATING ON A KHSD ATHLETIC TEAM.
PARENT SIGNATURE DATE

1/19/2018
Print Name of Student-Athlete:
As a condition of membership in the CIF, all schools shall adopt policies prohibiting the use and
abuse of androgenic/anabolic steroids. All member schools shall have participating students and
their parents, legal guardian/caregiver agree that the athlete will not use steroids without the
written prescription of a fully licensed physician (as recognized by the AMA) to treat a medical
condition (Bylaw 524).
By signing below, both the participating student-athlete and the parents, legal guardian/caregiver
hereby agree that the student shall not use androgenic/anabolic steroids without the written
prescription of a fully licensed physician (as recognized by the AMA) to treat a medical
condition. We also recognize that that under CIF Bylaw 200.D., there could be penalties for
false or fraudulent information. We also understand that the Kern High School District policy
regarding the use of illegal drugs will be enforced for any violations of these rules.
Signature of Student Date
Signature of Parent Date
1/19/2018
ATHLETIC RELEASE AND WAIVER OF LIABILITY AND INDEMNITY AGREEMENT
Student’s Name: __________________________________________Date of Birth: __________________
Sport/Activity: ____________________________________________School Year: ___________________
WARNING: Participation in athletics may result in severe injury which can range from minor to
catastrophic injuries. Both the student and parent/guardian must understand that the dangers and risks of
playing or practicing include but are not limited to: death, complete or partial paralysis, brain damage,
serious injury to virtually all internal organs, bones, joints, ligaments, muscles, tendons and other aspects of
the skeletal system and potential impairment to other aspects of the body, general health and well-being.
Injuries can occur as a result of negligent conduct of the Student, other participants in the sport, coaches,
instructors, trainers and volunteers. Even with protective equipment and safety rules, serious and even fatal
injuries may still occur.
AS A CONDITION OF PARTICIPATION IN ATHLETICS, THE UNDERSIGNED ACKNOWLEDGE
THAT THEY HAVE READ AND UNDERSTAND THIS WARNING STATEMENT AND THAT THEY
VOLUNARILY AGREE TO ASSUME ALL RISKS ASSOCIATED WITH PARTICIPATION IN
ATHLETICS.
IN CONSIDERATION FOR YOUR PARTICIPATION IN ATHLETICS, THE UNDERSIGNED
HEREBY RELEASE, WAIVE, DISCHARGE AND COVENANT NOT TO SUE THE KERN HIGH
SCHOOL DISTRICT, ITS EMPLOYEES, REPRESENTATIVES, BOARD, MEDICAL
PERSONNEL, OFFICERS, COACHES, TRAINERS, STAFF, VOLUNTEERS AND ANY OTHER
AGENTS (HEREINAFTER “RELEASEES”), FROM ANY AND ALL LIABILITY, ACTIONS,
DEBTS, CLAIMS AND DEMANDS FOR ANY LOSS OR DAMAGE TO STUDENT RESULTING
IN INJURY OR DEATH OF THE STUDENT, INCLUDING FOR NEGLIGENCE OR OTHER
WRONGFUL ACTS OF THE RELEASEES AND THIRD PARTIES, WHICH MAY ARISE OUT
OF OR IN CONNECTION WITH THE STUDENT’S PARTICIPATION IN ATHLETICS.
The undersigned further agree to indemnify, defend, save and hold Releasees harmless from any and all
liability, actions, debts, claims and demands of every kind which may arise out of or in connection with the
Student’s participation in athletics.
The undersigned agree that this release, waiver and indemnity agreement is intended to be as broad and
inclusive as is permitted by the laws of the State of California, and that if any portion is held invalid, the
balance shall continue in full legal force and effect. The undersigned further agree that no oral
representations, statements or inducements apart from the foregoing written agreement have been made.
The undersigned agree that this release shall extend to Student’s heirs, personal representatives, assigns, and
next of kin.
I (we) have read and understand the information above and consent to participate in the athletic activity.
____________________________________________ ___________________________
Student Signature Date
____________________________________________ ____________________________
Parent/Guardian Signature Date

1/19/2018
KERN HIGH SCHOOL DISTRICT DISCIPLINE CODE SUMMARY
OFFICE OF ACTIVITIES/ATHLETICS The Board of Trustees of the Kern High School District, in association with the CIF, supports a strong, wholesome interscholastic program as an integral part of the educational process for students attending high schools. Each student athlete is required to adhere to the rules and regulations of the California Interscholastic Federation and to the Kern High School District Athletic Control Code.
Each parent/guardian and student athlete must sign and return this letter to the finance office, indicating that each has read the summarized regulations. A COMPLETE COPY OF THE ATHLETIC AND ACTIVITY CONTROL CODE IS AVAILABLE AT YOUR S ON’ S/DAUGHTER’S HIGH SCHOOL UPON REQUEST.
SCHOLASTIC ELIGIBILITY
1. The student is currently enrolled in at least 25 semester periods of work. 2. The student has maintained during the previous grading period a minimum of 2.0 G.P.A. in all
enrolled courses. a. No more than one (1) service type class with no more than five (5) semester periods of credit
can be included in the classes counted for eligibility in any one grading period.
REGULATIONS GOVERNING STUDENTS ON AND OFF SCHOOL CAMPUSES
1. ALCOHOLIC BEVERAGES Use or possession of alcoholic beverages by a student is prohibited at any time during the school year.
2. TOBACCO Use or possession of tobacco in any form by a student is prohibited at any time during the school year.
3. DRUGS, NARCOTICS Use, possession, sale, or distribution of any illegal drugs (marijuana, cocaine, etc.), drug paraphernalia, or controlled substance (steroids, etc.) (unless prescribed by a licensed physician) is prohibited during the calendar year.
4. CIVIL OR CRIMINAL OFFENSE Involvement in an offense classified as a felony or misdemeanor that threatens the discipline of the team, the welfare of or the educational functions of the school is prohibited during the calendar year.
5. WILLFUL OR RECKLESS CONDUCT Willful or reckless conduct which results in, or is likely to result in bodily injury or damage to person or real property is forbidden during the calendar year insofar as such conduct threatens the discipline and welfare of the school.
A student found guilty of violating regulation 1, as outlined above, will forfeit all athletic privileges for a period of nine (9) regular athletic school weeks. If a student is found in violation of regulation two (2), as outlined above he/she will automatically forfeit the privilege of participating in athletics for a period of four (4) regular athletic school weeks. If a student is found in violation of regulation three (3), as outlined above he/ she will automatically forfeit the privilege of participating in athletics for a period of nine (9) regular athletic school weeks. If a student is found in violation of regulation four or five (4 or 5), as outlined above he/ she will automatically forfeit the privilege of participating in athletics for a period of nine (9) and not more than eighteen (18) regular athletic school weeks. Second and third violations of the regulations will result in a period of ineligibility of up to one year. First time offenders for Alcohol, Tobacco and Drugs have an alternative program available of Brief Intervention. Selection of the Brief Intervention program could shorten the suspension period. See your Athletic Director for information
Warning: Football players are NOT to use helmets to butt, ram or spear an opposing player. This is in violation of the football rules, and such use can result in severe head or neck injuries, paralysis or death to you and possible injury to your opponent. No helmet can prevent all head or neck injuries a player might receive while participating in football.
NAME OF STUDENT (PRINT) STUDENT ID#
PARENT/GUARDIAN SIGNATURE DATE STUDENT’S SIGNATURE DATE
1/19/2018
AB 25 (Concussion Information Form)
What can happen if my child keeps on playing with a concussion or returns to soon?
Athletes with the signs and symptoms of concussion should be removed from play immediately. Continuing to play
with the signs and symptoms of a concussion leaves the young athlete especially vulnerable to greater injury. There
is an increased risk of significant damage from a concussion for a period of time after that concussion occurs,
particularly if the athlete suffers another concussion before completely recovering from the first one. This can lead
to prolonged recovery, or even to severe brain swelling (second impact syndrome) with devastating and even fatal
consequences. It is well known that adolescent or teenage athlete will often under report symptoms of injuries. And
concussions are no different. As a result, education of administrators, coaches, parents and students is the key for
student-athlete’s safety.
If you think your child has suffered a concussion Any athlete even suspected of suffering a concussion should be removed from the game or practice immediately. No
athlete may return to activity after an apparent head injury or concussion, regardless of how mild it seems or how
quickly symptoms clear, without medical clearance. Close observation of the athlete should continue for several
hours. The CIF Bylaw 503H now requires implementation of long and well-established return to play concussion
guidelines that have been recommended for several years:
“A student-athlete who is suspected of sustaining a concussion or head injury in a practice or game shall be
removed from competition at that time and for the remainder of the day.”
and
“A student-athlete who has been removed may not return to play until the athlete is evaluated by a licensed heath care
provider trained in the evaluation and management of concussion and received written clearance to return to play
from that health care provider”.
A student diagnosed with a concussion cannot return to activity for a minimum of seven (7) days as
determined by the doctor. See CIF bylaw 503H.
You should also inform your child’s coach if you think that your child may have a concussion, remember it’s better
to miss one game than miss the whole season. And when in doubt, the athlete sits out.
For current and up-to-date information on concussions you can go to:
http://www.cdc.gov/ConcussionInYouthSports/
Student-Athlete Name Printed Student-Athlete Signature Date
Parent or Legal Guardian Printed Parent or Legal Guardian Signature Date

1/19/2018
California Interscholastic Federation - Central Section Jim Crichlow-Central Section Commissioner

1/19/18
P.O. Box 1567, Porterville, CA 93258
Phone (559) 781-7586 FAX (559) 781-7033
ETHICS IN SPORTS
I. Policy Statement
The Central Section, CIF is committed to the exhibition of sportsmanlike and ethical behaviors in and around all
athletic contests. All contests must be safe, courteous, fair, controlled and orderly for all athletes and fans alike.
It is the intent of the CIF that violence, in any form, not be tolerated. In order to enforce this policy, the Central
Section has established rules and regulations, which set forth the manner of enforcement and of this policy and the
penalties incurred when violation of the policy occurs. The rules and regulations shall focus upon the responsibility
of the coach to teach and demand high standards of conduct and to enforce the rules and regulations set forth by
CIF.
The Central Section requires the following Code of Ethics be issued each year and requires signing by student
athletes, parent/guardian and coaches prior to participation as a guide to govern their behavior.
II. Code of Ethics
a. To emphasize the proper ideas of sportsmanship, ethical conduct and fair play.
b. To eliminate all possibilities which tend to destroy the best values of the game.
c. To stress the values derived from playing the game fairly.
d. To show cordial courtesy to visiting teams and officials.
e. To establish a happy relationship between visitors and hosts.
f. To respect the integrity and judgment of sports officials.
g. To achieve a thorough understanding and acceptance of the rules of the game and the standards of eligibility.
h. To encourage leadership, use of initiative and good judgment by the players on a team.
i. To recognize that the purpose of athletics is to promote the physical, mental, moral, social and emotional well-
being of the individual players.
j. To remember that an athletic contest is only a game, not a matter of life and death for player, coach, school,
official, fan, or nation.
I have read and I understand the Policy Statement, the Code of Ethics and the violations and Minimum Penalties of the
“Ethics in Sports” policy. I agree to abide by the policy and related consequences while participating in interscholastic
athletics, regardless of context, site or jurisdiction.
Student Signature Printed Name Date
Parent Signature High School
_________________________________________ _________________________________________
Coach’s Signature Athletic Directors Signature

1/19/18
III. Violations and Minimum Penalties
ACT PENALTIES
1. First ejection of player or coach from a contest or
SCRIMMAGE for unsportsmanlike conduct. Ineligible for the next CIF contest (league, non-league, tournament,
invitational, playoff, etc. scrimmage excluded). The next contest
could be the second game of a doubleheader or even the next season
of sport. Athletes competing in concurrent sports would be ineligible
for both sports.
2. Second ejection of a player or coach from a
contest during the same season of sport for
unsportsmanlike conduct.
Ineligibility for next two CIF contests as above will carry over the next
season of sport.
3. Third ejection of a player or coach from a contest
during the same season of sport for
unsportsmanlike conduct
Ineligibility for all CIF contests for one calendar year (365 days). Any
appeal must go through the CIF Eligibility Committee.
4. Any players that leave the “bench” area to begin
a confrontation or leave these areas during an
altercation.
Ejection from the contest for those players designated by officials. The
contest may be terminated by the officials. One or both teams may
forfeit the contest.
5. When players leave the bench area to begin a
confrontation or leave the bench area during an
altercation and in the opinion of the officials, the
situation is out of control.
Contest stopped, ejection from the contest for those players designated
by the officials. The team(s) that left the bench area must forfeit
contest, record a loss, and the team(s) and players will be put on
probationary status for the balance of the season. A second similar
infraction during the season of sport will result in cessation of the
sport for the team(s) and/or players. If the act occurs at the end of
the season, the probationary period will extend to the next year’s
season of sport. Any appeal would have to be made to the CIF
Executive Board.
6. Illegal participation in next contest by player
ejected in previous contest. Ineligibility for remainder of season for player. Forfeiture of contest.
7. Illegal placement of ejected player or illegal
participation by coach ejected in previous
contest.
Constitution and sport governing rules and procedures for a coach who
knowingly violates CIF or Section Rules.
8. Any acts of a more serious nature by individuals
or teams or situations not specifically covered by
this policy or the Constitution or Governing
Rules.
Area Commissioner may determine and implement penalties for
individuals and teams not otherwise specified by CIF Central Section
Constitution and Bylaws.
9. If act occurs in CIF Section Finals and both
teams are charged with a forfeit. After deliberation by the CIF and a double forfeit is in order, there will
be no champion.
10. An ejected coach must leave the site of the contest. The coach may have no contact with his/her team from that point on. If
there is no certificated replacement for the coach, the contest is halted and the game is forfeited. The coach must also sit out
the next contest and cannot attend the contest or have any contact with the team during the contest. The coach may be
allowed to participate in practices on days other than the day of the contest.
11. An ejected player may stay on the bench for the remainder of the contest for supervision reasons. Further disruption by
ejected players may force them to be removed from the site. This could lead to a forfeit. Players ejected must sit out the next
contest, but may sit on the bench in street clothes.
APPEALS PROCEDURE – First and Second Ejection
All appeals MUST come from the school Principal or his/her designee. Only misidentification and misapplication of a rule may be appealed. NO
JUDGMENT DECISIONS by officials may be appealed.
PHYSICAL ASSAULT CIF State Constitution, Article 5, Section 522. Any student who physically assaults the person of a game or event official shall be banned from interscholastic
athletics for the remainder of the student’s eligibility. A game or event official is defined as a referee, umpire or any other official assigned to interpret or enforce rules competition at an event. A student may, after a lapse of 18 calendar months from the date of the incident, apply for reinstatement of eligibility to the State CIF
Commissioner.
For this document, the Central Section also includes coaches, administrators or other school personnel assigned to the contest or games as a game official.

1/19/18
PARENT KEEPS

DELIVER TO PHYSICIAN
KHSD PRELIMINARY HEAD INJURY REPORT
Name: ________________________________________ Date:____________ Time:_____________
Cause of head injury: __________________________________________________________________
____________________________________________________________
____________________________________________________________
____________________________________________________________
First Aid given:
____________________________________________________________ Signs/Symptoms of injured athlete:
Headache Nausea Pressure in head Confused Change in personality
Unequal pupils Slurred Speech Confused about plays Seizures or has a fit
Can’t recall events before or after the injury Drowsiness Emotional Tired or Low Energy
Loss of memory Loss of conscious Loss of motor skills Difficulty standing-walking
Bothered by light or noise Feeling foggy or groggy Moves clumsily or awkwardly Neck Pain
Reporting Party Contact Information:
Name:__________________________ Phone:_____________________________
Stan Greene
Director
School Support Services
www.kernhighnetwork.com www.kccc.us

1/19/18
Physician Letter to School
To Whom It May Concern:
Student Name: DOB:
INJURY STATUS
Date of Concussion Diagnosis by MD/DO: Date of Injury:
Student has been diagnosed by a MD/DO with a concussion and is currently under our care.
Medical follow-up evaluation is scheduled for (date):
Student was evaluated and did not have a concussion injury. There are no limitations on school and physical activity.
ACADEMIC ACTIVITY STATUS (Please mark all that apply)
This student is not to return to school.
This student may begin to return to school based on successful progression through the CIF Concussion Return to Learn Protocol. This student requires the necessary school accommodations set forth on the Physician (MD/DO) Recommended School Accommodations Following Concussion form.
This student is no longer experiencing any signs or symptoms of concussion and may be released to full academic participation.
Comments:
PHYSICAL ACTIVITY STATUS (Please mark all that apply)
This student is not to participate in physical activity of any kind.
This student is not to participate in recess or other physical activities except for untimed, voluntary walking.
This student may begin a graduated return to play progression (see CIF Concussion RTP Protocol form).
This student has medical clearance for unrestricted athletic participation (Has completed the CIF Concussion RTP Protocol).
Comments:
Physician (MD/DO) Signature: Exam Date:
Physician Stamp and Contact Info:
Parent/Guardian Acknowledgement Signature: Date:
Revised: 10/2017 CIF
1/19/18
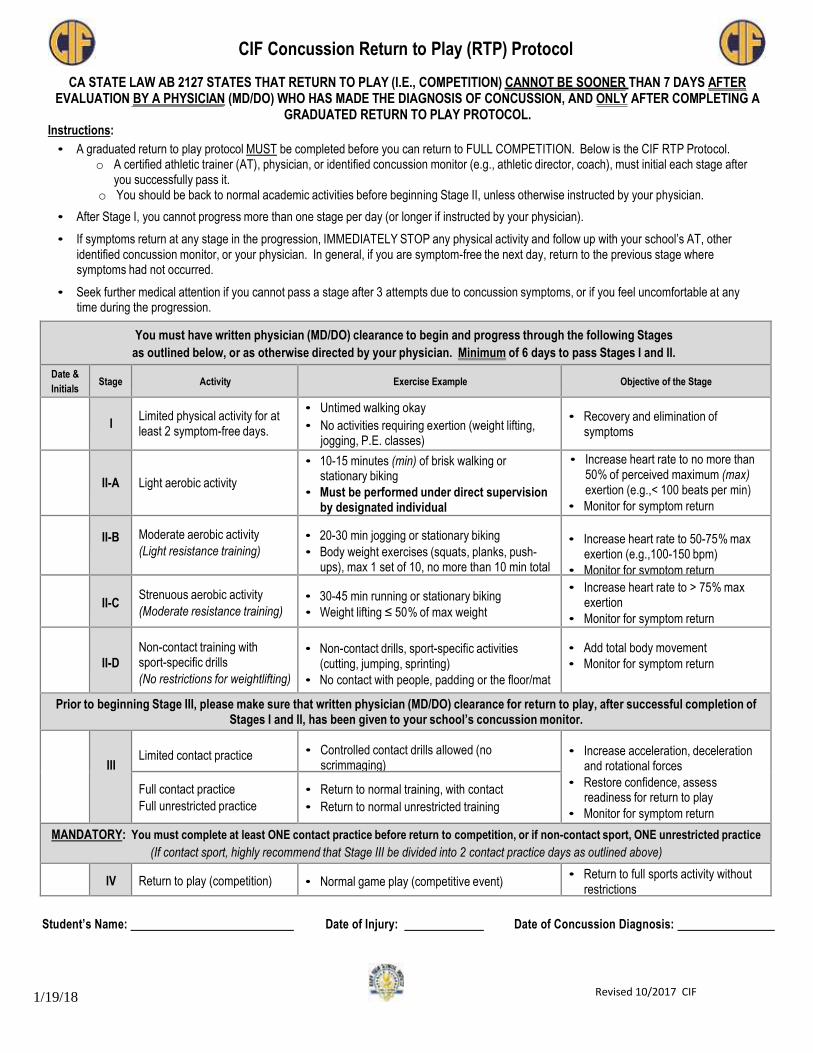
CIF Concussion Return to Play (RTP) Protocol
CA STATE LAW AB 2127 STATES THAT RETURN TO PLAY (I.E., COMPETITION) CANNOT BE SOONER THAN 7 DAYS AFTER EVALUATION BY A PHYSICIAN (MD/DO) WHO HAS MADE THE DIAGNOSIS OF CONCUSSION, AND ONLY AFTER COMPLETING A
GRADUATED RETURN TO PLAY PROTOCOL. Instructions:
• A graduated return to play protocol MUST be completed before you can return to FULL COMPETITION. Below is the CIF RTP Protocol. o A certified athletic trainer (AT), physician, or identified concussion monitor (e.g., athletic director, coach), must initial each stage after
you successfully pass it. o You should be back to normal academic activities before beginning Stage II, unless otherwise instructed by your physician.
• After Stage I, you cannot progress more than one stage per day (or longer if instructed by your physician).
• If symptoms return at any stage in the progression, IMMEDIATELY STOP any physical activity and follow up with your school’s AT, other identified concussion monitor, or your physician. In general, if you are symptom-free the next day, return to the previous stage where symptoms had not occurred.
• Seek further medical attention if you cannot pass a stage after 3 attempts due to concussion symptoms, or if you feel uncomfortable at any time during the progression.
You must have written physician (MD/DO) clearance to begin and progress through the following Stages
as outlined below, or as otherwise directed by your physician. Minimum of 6 days to pass Stages I and II.
Date &
Initials
Stage
Activity
Exercise Example
Objective of the Stage
I
Limited physical activity for at least 2 symptom-free days.
• Untimed walking okay
• No activities requiring exertion (weight lifting, jogging, P.E. classes)
• Recovery and elimination of symptoms
II-A
Light aerobic activity
• 10-15 minutes (min) of brisk walking or stationary biking
• Must be performed under direct supervision by designated individual
• Increase heart rate to no more than 50% of perceived maximum (max) exertion (e.g.,< 100 beats per min)
• Monitor for symptom return
II-B
Moderate aerobic activity
(Light resistance training)
• 20-30 min jogging or stationary biking
• Body weight exercises (squats, planks, push- ups), max 1 set of 10, no more than 10 min total
• Increase heart rate to 50-75% max exertion (e.g.,100-150 bpm)
• Monitor for symptom return
II-C
Strenuous aerobic activity
(Moderate resistance training)
• 30-45 min running or stationary biking
• Weight lifting ≤ 50% of max weight
• Increase heart rate to > 75% max exertion
• Monitor for symptom return
II-D
Non-contact training with sport-specific drills
(No restrictions for weightlifting)
• Non-contact drills, sport-specific activities (cutting, jumping, sprinting)
• No contact with people, padding or the floor/mat
• Add total body movement
• Monitor for symptom return
Prior to beginning Stage III, please make sure that written physician (MD/DO) clearance for return to play, after successful completion of Stages I and II, has been given to your school’s concussion monitor.
III
Limited contact practice
• Controlled contact drills allowed (no scrimmaging)
• Increase acceleration, deceleration and rotational forces
• Restore confidence, assess readiness for return to play
• Monitor for symptom return
Full contact practice
Full unrestricted practice
• Return to normal training, with contact
• Return to normal unrestricted training
MANDATORY: You must complete at least ONE contact practice before return to competition, or if non-contact sport, ONE unrestricted practice
(If contact sport, highly recommend that Stage III be divided into 2 contact practice days as outlined above)
IV
Return to play (competition)
• Normal game play (competitive event) • Return to full sports activity without
restrictions
Student’s Name:
Date of Injury:
Date of Concussion Diagnosis:
Revised 10/2017 CIF

1/19/18
Concussion Return to Learn (RTL) Protocol
Instructions:
• Keep brain activity below the level that causes worsening of symptoms (e.g., headache, tiredness, irritability).
• If symptoms worsen at any stage, stop activity and rest.
• Seek further medical attention if your child continues with symptoms beyond 7 days.
• If appropriate time is allowed to ensure adequate brain recovery before progressing mental activity, your child may have a better outcome (do not try to rush through these stages).
• Please give this form to teachers/school administrators to help them understand your child’s recovery.
Stage Home Activity School Activity Physical Activity
Brain Rest
• Rest quietly, nap and sleep as much as needed
• Avoid bright light if bothersome
• Drink plenty of fluids and eat healthy
foods every 3-4 hours
• Avoid "screen time" (text, computer, cell phone, TV, video games)
• No school
• No homework or take-home tests
• Avoid reading and studying
• Walking short distances to get around
is okay
• No strenuous exercise
• No driving
Progress to the next stage when your child starts to improve, but may still have some symptoms
Restful Home Activity
• Set a regular bedtime/wake up schedule
• Allow at least 8-10 hours of sleep and short naps if needed (less than 1 hour)
• Drink lots of fluids and eat healthy foods every 3-4 hours
• Limit "screen time" to less than 30
minutes total a day; use large font
• No school
• May begin easy tasks at home (drawing, baking, cooking)
• Soft music and ‘books on tape’ okay
• Once your child can complete 60-90 minutes of light mental activity without a worsening of symptoms they may go to the next step
• Progress physical activity, like
untimed walking
• No strenuous physical activity or contact sports
• No driving
Progress to the next stage when your child starts to improve and has fewer symptoms
Return to School -
PARTIAL DAY
• Allow 8-10 hours of sleep per night
• Limit napping to allow for full sleep at night
• Drink lots of fluids and eat healthy foods every 3-4 hours
• "Screen time" less than 1 hour a day
• Limit social time outside of school
• Gradually return to school
• Start with a few hours/half-day
• Take breaks in the nurse’s office or a quiet room every 2 hours or as needed
• Avoid loud areas (music, band, choir, shop class, locker
room, cafeteria, loud hallway and gym)
• Use brimmed hat/earplugs as needed. Sit in front of class
• Use preprinted large font (18) class notes
• Complete necessary assignments only
• No tests or quizzes. Limit homework time
• Multiple choice or verbal assignments better than long
writing assignments
• Tutoring or help as needed
• Stop work if symptoms increase
• Progress physical activity and as
instructed by physician
• No strenuous physical activity or contact sports
• No driving
Progress to the next stage when your child can complete the above activities without symptoms
Return to School -
FULL DAY
• Allow 8-10 hours of sleep per night
• Avoid napping
• Drink lots of fluids and eat healthy foods every 3-4 hours
• "Screen time" and social activities outside of school as symptoms tolerate
• Progress to attending core classes for full days of school
• Add in electives when tolerated
• No more than 1 test or quiz per day
• Give extra time or untimed homework/tests
• Tutoring or help as needed
• Stop work if symptoms increase
• Progress physical activity and as
instructed by physician
• No strenuous physical activity or contact sports
• Okay to drive
Progress to the next stage when your child has returned to full school and is able to complete all assignments/tests without symptoms
Full Recovery
• Return to normal home and social
activities
• Return to normal school schedule and course load
• Start CIF Return to Play Protocol
** Guidelines adapted from Cincinnati Children’s Hospital Return to Learn Protocol CIFSTATE.ORG Revised, 10/2017 CIF

1/19/18