atherosclerosis coronary heart disease angina pectoris myocardial infarction
TRANSCRIPT

AtherosclerosisCoronary heart disease
Angina pectorisMyocardial infarction

Causes of death in Europe
• men– coronary heart disease (MI) 21%– trauma and poisoning 12%– stroke 11%– pulmonary carcinoma 6%– carcinomas in GIT 4%
• women– coronary heart disease 21%– stroke 18%– other CVS diseases 15%– trauma and poisoning 5%– breast carcinoma 3%
Atherosclerosis• syndrome affecting large and medium-sized arteries
• artery wall thickenings – lipid infiltration - atheroma creation
• chronic inflammatory response in the walls of arteries
• hardening of the artery wall (loss of elasticity)
• Result - insufficient blood supply
to the heart – myocardial infarction (heart attack)
to the brain – stroke
to the legs – claudicatio

Tunica intima
Endothelial cells
Tunica media
Smooth muscle cells
Tunica adventicia

Atherosclerosis

Atherosclerotic plague
Endothelial cells
Thrombus
Rupture of fibrous cap
Smooth muscles cells
Lipid core
Platellets
Foam cells

Stages of atherosclerotic plaque development
• Type I – isolated foam cells– macrophages with a droplet of fat in intima
• Type II – fatty streaks– foam cells layer
• Type III – higher amount of lipids under the foam cells layer
• Type IV – atheroma– lipid core, fibrous cap
• Type V – more collagen and smooth muscle cells in fibrous cap
• Type VI– atheroma with complications - thrombosis


Coronary heart (artery) disease
• result of the ateromatous plaques within the walls of the coronary arteries
• limitation of blood flow to the heart → ischaemia
• Result
Angina pectoris
Myocardial infarction

Coronary heart disease
physical acitivy (emotional stress)
activation of sympathicus
heart rate and contraction
demand after oxygen supply
coronary artery obstruction due to atherosclerosis
lack of blood (oxygen) supply
PAIN

Risk factors (CHD, IM)• Basic biological
– age, gender, family history (= genes)
• Biochemical, classical– cholesterol, LDL-CH, TAG, HDL-CH, apoproteins, Lp(a), indexes
• Biochemical, new– fibrinogen, homocysteine, ferritin– small dense LDL, oxidized LDL
• Nutrition and life style– too much fat, sugar, antioxidant and fiber deficiency– SMOKING, SEDENTARY LIFE STYLE
• Diseases– obesity, diabetes (IR!), hypertension, kidney failure
• Genetic RF – LDL receptor (FH), apo E variants and many others

Basic biological factors
• age
– men > 45 years
– women after menopause
• gender
– men > women

Obesity
obesity
hyperinsulinaemia
dyslipidaemiacentral typ

Hypertension
• endothelium damage

Smoking• nicotine
– effect on lipid metabolism
– vasoconstriction
• CO
– carboxyhaemoglobin
• increased coagulation cascade activity

Endothel
• Intelligent interface between blood and vessel wall/tissues
• 1500 g, football field (1000 m2)• Endocrine, paracrine and autocrine functions
– vessel tonus, coagulation, adhesion, cell replication
• Organ specificity, differences in arteries, capillaries a venes
• Dysfunction in hypertension, diabetes, dyslipidemia...

Lipoproteins
Cholesterol, free and esters with fatty acids• 275 mmol in the body
– 50 mmol LP, GIT, liver – 25 mmol fat tissue– 90 mmol muscles & vessel wall– 110 mmol nervous system
• 3 mmol/d exchange• Cholesterol
– In: food and synthesis in cells (from CoA)– Breakdown: no– Out: bile (enterohepatal circuit); stool
• LDL cholesterol– The normal level (3,1 – 3,9 mmol/l) is not normal for the endothel– Newborns & atherosclerosis resistant animals only 0,8 mmol/l

Triacylglycerols & fatty acidsTAG & FFA
• 15 kg in nonobese subjects• 570 000 kJ; enough for 3 months• Thermal isolation, fertility, body shape• Intake & synthesis: 80 – 170 mmol/d• Different fatty acids – saturated, unsaturated,
polyunsaturated (eikosanoids), shorter and longer chain• Rapid turnover dependent on diet and alcohol intake,
breakdown through physical activity (FFA – minutes)

• water-soluble particles, that transport water-insoluble lipids
in the blood
Lipoproteins
Phospholipids
Apolipoproteins
TriacylglycerolsCholesterol esters
lipids
proteins
Free cholesterol


Apoproteins
APOPROTEIN, FUNCTION LOCATION OF THE
GENE
MAIN OCCURENCE
A 1 – ACTIVATOR OF LCAT 11q23-qter HDL, CHYA 2 – ACTIVATOR OF LIVER LIPASE,INHIBITOR OF LCAT
11q21-q23 HDL, CHY
A 4 – LCAT ACTIVATION 11q23-qter HDL, CHYB 100 LIGAND OF LDL RECEPTOR 2p23-24 LDL, IDL, VLDLB 48 SHORT FORM OF B 100 ib. CHYC 1 – LCAT COFACTOR 19q12-q13.2 CHY, VLDLC 2 – LPL ACTIVATOR (LIPOPROTEIN LIPASE) 19q12-q13.2 CHY, VLDL, HDLC 3 – LPL & LIVER LIPASE INHIBITOR 11q23-qter CHY, VLDL, IDLD – CHOLESTEROL ESTER TRANSFER REGULATION 3q14.2-qter HDLE – RECEPTOR LIGAND 19q12-q13.2 CHY, VLDL, IDL

3 lipoprotein families (LP)
• spherical or discoid particles synthesised in guts or liver
– Hydrophilic surface (phospholipids, cholesterol esters and apoproteins)
– Hydrophobic inner part (TAG, CH)
– Dynamic interaction with vessel wall and each other
• Chylomicrons chylomicron remnants
• VLDL IDL LDL (heterogenous group)
• HDL nascent HDL3 HDL2

Chylomicrons
• Enterocytes• apoB48, others from HDL• TAG into fat and other tissues, LPL• CH into liver (from bile and food)• Peak 3 – 6 h after meal, t1/2 30 min, after 9 h Ø• Remnants into liver through receptor cytotoxic and atherogenic

VLDL – LDL family
• Liver, endogeneous TAG, CH• B100 and others• functions and metabolism similar to CHY• VLDL t1/2 2 – 4 hod, transformation to IDL, LDL• LDL has a slow turnover, can be modified – oxidation,
glycation• small dense LDL• Receptor and scavenger receptor

LDL classes
LDL class density, g/ml diameter, nm % of LDL
I 1,025 27,5 – 26,0 3
II 1,028 26,0 – 25,5 16
III 1,034 25,5 – 24,2 50
IV 1,048 24,2 – 21,8 22
V > 1,048 < 21,8 9
Small dense LDL• small
– easy transport to intima of vessels• higher density• higher TAG concentration• easy oxidation
Lipoprotein(a)• LDL with apoproteine(a) – glykoprotein very similar to plasminogen• higher risk of thrombosis
Oxidized LDL (oxLDL)• high atherogenity• higher macrophage afinity - 8 - 10x higher than to LDL

Reverse transport of cholesterol by HDL
• Liver, enterocytes and fromCHY as nascent „disc“
• Lot of apoproteins
• LCAT and CEPT– lecitin-cholesterol acyltransferase, esterifies CH
– cholesterol ester transfer protein transprots CH-E from HDL into other LPs
• Takes out cholesterol from tissues, disc is filled to HDL3
• Exchanges CH-E for TAG with other LPs transforms to HDL2
• Binds through AI to specific receptor in liver

HDL3 HDL2
nascent HDL
liver
vessel
tissues
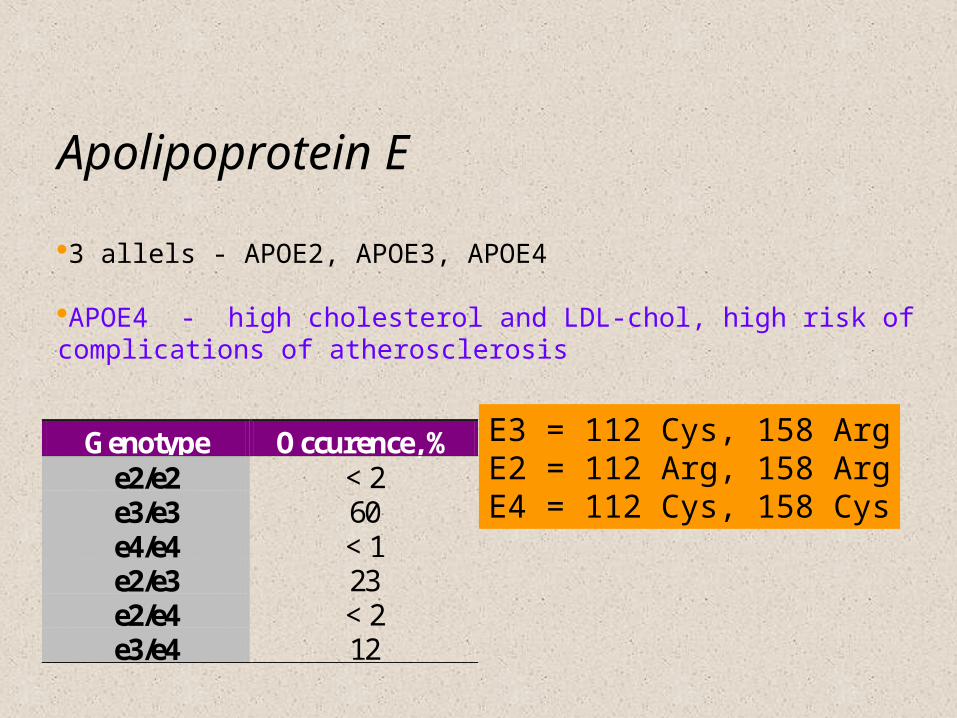
Apolipoprotein E
3 allels - APOE2, APOE3, APOE4
APOE4 - high cholesterol and LDL-chol, high risk of complications of atherosclerosis
Genotype Occurence, % e2/e2 < 2 e3/e3 60 e4/e4 < 1 e2/e3 23 e2/e4 < 2 e3/e4 12
E3 = 112 Cys, 158 ArgE2 = 112 Arg, 158 ArgE4 = 112 Cys, 158 Cys

Normal (desired) values
• T-CH < 5,0 mmol/l 4,55 – 5,45
• HDL-CH > 1,0 mmol/l 0,87 – 1,13
• LDL-CH < 3,0 mmol/l 2,65 – 3,35
• TAG < 2,0 mmol/l 1,70 – 2,30
INDEXES
• T-CH/HDL-CH < 5,0
• NONHDL-CH < 3,8
• LDL-CH/HDL-CH < 3,0
• Klimov (T-CH – HDL-CH)/HDL-CH < 4,2
• APO AI/APO B > 1,3
Other laboratory methods
• Special– Apo B, Apo AI, Lp(a)
– homocysteine, coagulation and fibrinolytic factors.
• Very special– LDL receptors
– Apo C, E, LPL, CETP, LCAT
– classes of LDL, HDL
• Yesterday– total lipids, phospholipids, fatty acid esters
– elektrophoresis
• Tomorrow - genomics
Hyperlipoproteinemias
Classifications
• Fredrickson 1967, WHO 1970– I, IIa, IIb, III, IV, V, VI - partly history
• Therapeutical 1992, European task force– CH, TAG, both
• Etiological – future– primary and secondary DLP is not sufficient! – most primary DLP are not exactly characterized

“Primary DLP”
Familiar hypercholesterolemia (LDL rec.) Familiar defect of ApoB100 (FDB)
? Polygenous hypercholesterolemia
? Polygeneous hypertriglcyceridemia
? Dysbetalipoproteinemia (IDL)
? Familiar type V hyperlipidemia

“Secondary DLP”• Nutrition and lifestyle
– including smoking, alcohol and micronutrient deficiency• Obesity• Diabetes mellitus
– type 2 usually, decompensated type 1 (BG 20 – extreme TAG)• Kidney failure• Liver disease• Endocrine diseases – thyroid function• Drugs• Hormones – anticonception, gravidity, postmenopausal, anabolics
Familial hypercholesterolaemia•AD inherited •defect of LDL receptor (> 300 mutations of LDLR)
Symptoms•increased LDL-chol concentration•atherosclerosis (high risk of MI, homozygouts in 2. -3. decenium)
LDL
LDL receptor

Symptoms and signs
xantomasarcus lipoides corneae
xantelasma palpebrarum
atherosclerosis and CHD

Angina pectoris• severe chest pain due to ischaemia of the heart muscle, due to
obstruction of the coronary arteria
• Symptoms
– after exertion, emotional stress, in the rest
– chest pain (or discomfort)
– lasting several minutes
– referred pain to the arms, shoulders, neck, chin
– exacerbated by full stomach or cold temperature
– breathlessness, sweating, nausea
– pain relieved by nitroglycerin

Types of angina pectoris• Stable AP
– stable atherosclerotic plaque– retrosternal pain precipitaded by activity (walking, running)– no pain in rest– 3 – 5 min– referred pain to the arms, shoulders, back...
• Unstable AP– „crescendo“ angina– unstable atherosclerotic plaque– at rest– > 10 min.– more serious symptoms
• Variant (Prinzmetal´s, vasospastic) AP– caused by vasospasm– unknown mechanism (dysfunction of endothelium?)– atherosclerotic changes – not necessary– at rest (at night, early morning)

Myocardial infarction• Acute myocardial infarction• Heart attack
• Necrosis of the heart cells due to interruption of blood supply to the part of the heart
Causes• rupture of the ustable atherosclerotic plaque → trombosis• coronary artery obstruction by the stable plaque

• Signs and symptoms– sudden chest pain radiating to the left arm, shoulder, neck,
chin...
– pain not relieved by nitroglycerin
– anxiety
– nausea, vomiting, sweating
– dyspnea
– pale, cold skin
– cardiogenic shock symptoms
• arterial pressure decrease
• tachycardia
– sometimes silent ischaemia – without pain (e.g. diabetic neuropathy)

Painleft shoulder
right shoulder
arm
neck
epigastrium
chest

T wave inverion
ST segment elevation
patological Q wave
ECG diagnosis
• Complication of MI– dysrhythmias
– heart failure
– shock and hypotension
– myocardial rupture
– valve defects
– embolisation
– pericarditis
Cardiac markers
• myoglobin (Mb)
• troponin I (TnI), T (TnT)
• creatine kinase (CK)
• heart MB subtype (CK-MB)
• lactate dehydrogenase (LD)
• aspartate aminotranspherase (AST)
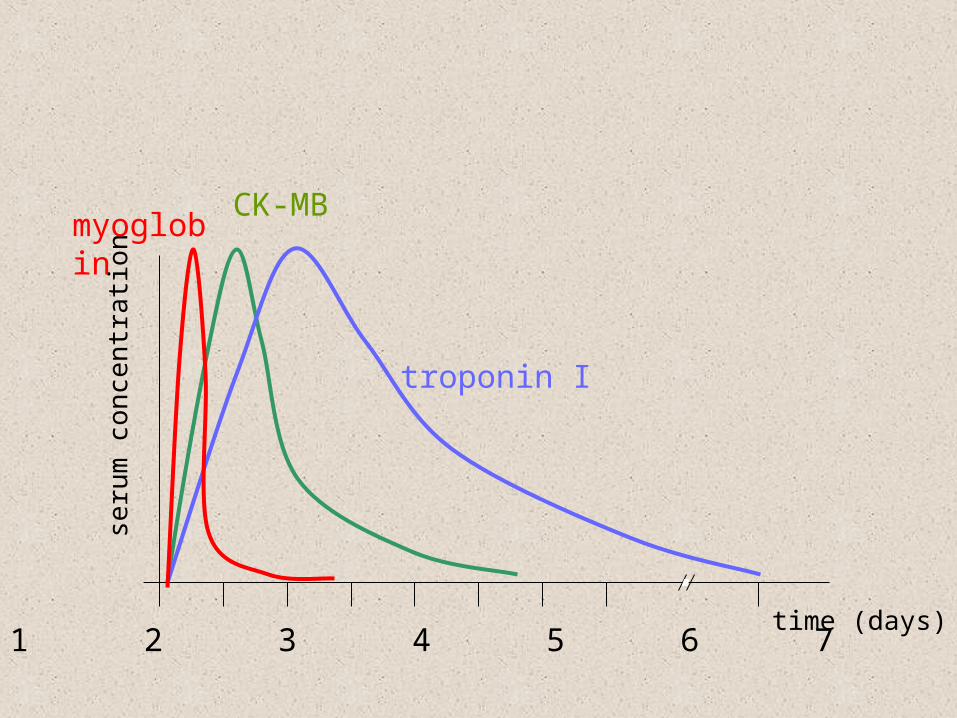
seru
m c
once
ntra
tion
time (days)0 1 2 3 4 5 6 7 14
myoglobinCK-MB
troponin I

activity
time (days)0 1 2 3 4 5 6 7
CK-MB
AST
LD

• Complication of MI– dysrhythmias
– heart failure
– shock and hypotension
– myocardial rupture
– valve defects
– embolisation
– pericarditis