asymmetric flaccid paralysis: a neuromuscular presentation of west nile virus infection
TRANSCRIPT

Asymmetric Flaccid Paralysis:A Neuromuscular Presentation of
West Nile Virus InfectionJun Li, MD, PhD,1 Jeffrey A. Loeb, MD,1,2 Michael E. Shy, MD,1,2 Aashit K. Shah, MD,1
Alex C. Tselis, MD,1 William J. Kupski, MD,3 and Richard A. Lewis, MD1
The neuromuscular aspects of West Nile virus (WNV) infection have not been characterized in detail. We have studieda group of six patients with proven WNV infection. All cases presented with acute, severe, asymmetric, or monolimbweakness, with minimal or no sensory disturbance after a mild flu-like prodrome. Four cases also had facial weakness.Three of our cases had no encephalitic signs or symptoms despite cerebrospinal fluid pleocytosis. Electrophysiologicalstudies showed severe denervation in paralyzed limb muscles, suggesting either motor neuron or multiple ventral nerveroot damage. This localization is supported further by the finding of abnormal signal intensity confined to the anteriorhorns on a lumbar spine magnetic resonance imaging. Muscle biopsies from three patients showed scattered necroticfibers, implicating mild direct or indirect muscle damage from the WNV infection. In summary, we describe a group ofpatients with acute segmental flaccid paralysis with minimal or no encephalitic or sensory signs. We have localized theabnormality to either the spinal motor neurons or their ventral nerve roots. It will be important for physicians toconsider WNV infection in patients with acute asymmetric paralysis with or without encephalitic symptoms.
Ann Neurol 2003;53:703–710
West Nile virus (WNV) is a RNA virus that belongs tothe flavivirus family taxonomically.1 The dramatic out-break of WNV infection in New York City in 1999heralded the virus reaching North America.2 Sincethen, WNV has rapidly spread across the UnitedStates. There were only 142 cases with 18 deaths be-tween 1999 and 2001. However, during the summerof 2002, the incidence of WNV infection drasticallyincreased to a total of 3,052 cases with 153 deaths todate.3 Ten percent of patients with WNV infectionfrom Israel and New York City presented with acute,bilateral flaccid paralysis.2,4 The findings from theirelectromyography and nerve conduction studies werenot described in detail but were interpreted as axonalmotor neuropathy, imitating Guillain–Barre syn-drome.2 There also have been a few case reports de-scribing patients with WNV infection and a “polio-like” syndrome.5–7
During this past summer (2002), Michigan had asignificant number of cases of WNV infection. In thisreport, we describe a group of WNV-infected patientspresenting with a peculiar acute segmental flaccid pa-
ralysis. We provide detailed electrophysiological andneuroimaging evidence that this disorder is localized tothe anterior horn motor neurons and/or ventral rootsof the spinal cord.
Patients and MethodsSix patients, four men and two women, were examined,ranging in age from 27 to 63 years old. Workup includedmagnetic resonance imaging (MRI) of the brain and spine,lumbar puncture, electrophysiology, and muscle /nerve bi-opsy. Four of these patients had positive IgM antibodies toWNV by enzyme-linked immunosorbent assay (ELISA) testof their cerebrospinal fluid (CSF), performed in the Depart-ment of Health of the State of Michigan. The remaining twocases had positive IgM antibodies in the serum with positiveneutralizing antibody test, which is also confirmatory.
ResultsCase ReportsLaboratory and neuroimaging results for all cases arelisted in Table 1.
From the 1Department of Neurology, 2Center for Molecular Med-icine and Genetics, and 3Department of Pathology, Wayne StateUniversity School of Medicine, Detroit, MI.
Received Nov 21, 2002, and in revised form Feb 19, 2003. Ac-cepted for publication Mar 7, 2003.
Address correspondence to Dr Li, Department of Neurology,Wayne State University, 4201 St. Antoine, UHC-8D, Detroit, MI48201. E-mail: [email protected]
ORIGINAL ARTICLES
© 2003 Wiley-Liss, Inc. 703

PATIENT 1. A 36-year-old woman was healthy until 1week before presentation when she developed mild“flu-like” symptoms, including headache, malaise, andgastrointestinal upset. One day before admission, shenoted lower back pain. On the morning that she cameto the hospital, she awoke to find her left leg paralyzed.At no time did she have confusion, neck stiffness, orother meningoencephalitic symptoms or signs. She de-nied bowel and bladder dysfunction or muscle pain.
Examination showed a temperature of 38.2°C and aflaccid left leg without movement except for minimalankle dorsal and plantar flexion. There was minimallyreduced sensation to pinprick in the leg and absent leftknee and ankle deep tendon reflexes. All other reflexeswere well preserved, and the rest of her examinationwas normal.
She received a course of intravenous immunoglobu-lin treatment (1gm/kg/day for 2 days) with no signifi-cant improvement. After 5 months, there had been noimprovement of her motor deficit.
PATIENT 2. Six days before admission, this 45-year-oldman fell on the steps of his front porch and found thathis left leg was weak. He struggled to stand up and wasable to walk only a few blocks. The weakness in thisleg progressed over the next hour to the point that hecould no longer walk or even support himself. He hadsignificant diarrhea 1 day before admission. He hadone incident of bowel incontinence, but it was unclearwhether the incontinence was from diarrhea or second-ary to sphincter dysfunction. He denied muscle pain.There was no fever, headache, or neck stiffness. Theday after admission, he was noted to be confused.
His examination on day 2 showed a temperature of36.6°C, disorientation to time and place, and mildnystagmus on lateral gaze to the right and bilateral fa-cial weakness including frontalis muscles. Muscle ex-amination showed 2/5 strength in the left leg and 4/5strength in the right leg. Sensory examination was nor-mal for vibration and equivocal to pinprick in the leftleg. Deep tendon reflexes were absent in the left kneeand ankle, but normal in other limbs.
His mental status returned to normal over 4 days,but his weakness persisted.
PATIENT 3. A 27-year-old man with a history of alco-hol abuse presented with diarrhea, vomiting, and gen-eralized fatigue approximately 2 weeks before admis-sion. Six days before admission, he fell while climbingstairs. The next morning, he awoke with right arm pa-ralysis. Within 2 to 3 days, the left arm also becamemildly weak. He denied sensory disturbance, musclepain, and bowel and bladder dysfunction. There wasno alteration of mental status. He did not have head-ache, fever, or neck stiffness.
His examination showed a normal temperature andmental status. There was neck flexor and bilateral facialweakness including frontalis muscles, 0/5 strength inthe right arm and 4/5 in the left arm. There was min-imal weakness of both legs. Sensory examination wasnormal. Deep tendon reflexes were normal in the leftarm but were reduced in all other limbs.
He received a course of intravenous immunoglobulin(1gm/kg/day for 2 days), which did not alter his motordeficit. A telephone interview 2 months later suggestedthat his arm weakness persisted.
Table 1. Laboratory and Neuroimaging Results
Test
Patient No.
1 2 3 4 5 6
Brain MRI Normal Normal Not done; head CT:a 1cm mass inpituitary
Not done;head CT:normal
Normal Normal
Spine MRI Normal Normal Not done Not done Stenosis at C3-7,intact cord;T/L/S spineMRI: normal
Abnormal signalintensity atanterior hornof C/L cord
CSF (day) Day 20 Day 1 Day 25 Day 2 Day 9 Day 7Cell and
differentiationRBC 22,
Nuc 61L 84%
RBC 10,Nuc 32L 85%
RBC 1140, Nuc15L 90%
RBC 14,Nuc 425L 24%
RBC 33, Nuc 4L 81%
BC 10, Nuc150 L 24%
protein 171 96 145 83 193 52Glucose 77 84 80 72 67 66CK 220 17,808 — 28 — 141WNV IgM ab � In CSF � In CSF � In CSF � In serum � In serum � In CSF and
serum
aDays after onset of symptoms.
MRI � magnetic resonance imaging; C/L � cervical/lumbar; CT � computed tomography; CSF � cerebrospinal fluid; L � lymphocytes;RBC � red blood cell; T/L/S � thoracic/lumbar/sacral; WNV � West Nile virus.
704 Annals of Neurology Vol 53 No 6 June 2003

PATIENT 4. A 48-year-old man with a previous medicalhistory of diabetes and non-Hodgkin’s lymphoma (cy-clophosphamide, hydroxydaunomycin, vincristine, andprednisone chemotherapy completed 2 years earlier) de-veloped diarrhea, vomiting, and abdominal cramps andgeneralized fatigue 4 days before admission. On the dayof admission, he acutely became unable to walk and de-veloped a flaccid left arm. He denied any sensory distur-bance, muscle pain, and bowel and bladder inconti-nence. He became disorientated soon after admissionbut improved the following week. He denied fever,headache, or neck stiffness before admission.
His examination showed a low-grade fever (38.3°C)and disorientation to time and place. There was bilat-eral facial weakness including frontalis muscles, 0/5strength in the left arm, 4/5 in the right arm, and 3/5in both legs. Sensory examination was unremarkable.Deep tendon reflexes were normal in the right arm butotherwise reduced throughout.
By telephone interview 1 month later, the patientreported that his leg strength improved enabling himto walk with a walker; however, his arm weakness re-mained the same.
PATIENT 5. A 63-year-old healthy man awoke 6 daysbefore admission with pain in the middle of his backand found that his left leg was weak and that he wasunable to walk. There were no sensory symptoms,muscle pain, or bowel and bladder dysfunction. He de-nied fever, malaise, gastrointestinal discomfort, head-ache, neck stiffness, and confusion.
His examination showed normal temperature, men-tal status, and cranial nerve function. His left leg wasflaccid except for minimal flexion of the knee and an-kle joints. The strength of the right leg was mildly re-duced (4/5), but strength in upper limbs was normal.Pinprick, light touch, and vibration modalities weresymmetrically reduced in the distal legs and feet, withnoticeable hammertoes and high-arch feet. Deep ten-don reflexes were normal in all joints but were absentin both ankles. The tone of the anal sphincter was nor-mal.
By telephone interview 5 months later, the patientreported that his leg weakness remained the same.
PATIENT 6. A 51-year-old healthy woman developed“flu-like” symptoms 1 week before hospitalization.Two days after admission, her right leg became para-lyzed. Her left arm also became weak. The weaknessquickly spread to the left leg and right arm but was lesssevere. She was bed-bound. She had diffuse back mus-cle aching, but no other sensory disturbance. The pa-tient denied bowel and bladder incontinence. She hada fever of 38.8° C and a stiff neck upon admission.
The patient was not evaluated by us until 5 monthsafter the onset of her symptoms. At this time, she had
normal cranial nerve function, severe weakness (1–2/5)in the right leg, and mild to moderate weakness (3–4/5) in her other limbs. Sensory examination was nor-mal. Deep tendon reflexes were brisk in all joints withdown-going toes.
Her strength has improved over 5 months from be-ing bed-bound to ambulating with a wheeled walker.
Highlights of Laboratory FindingsFour patients had positive IgM antibodies to WNV de-tected by ELISA on the CSF. These patients were con-sidered confirmed cases of WNV. Patients 4 and 5 hadpositive IgM antibodies in the serum with positiveneutralizing antibody test, which was also confirmat-ory.8 No ELISA test was conducted on the CSF ofPatients 4 and 5. Patient 2 had a markedly elevatedcreatine kinase level. Because the patient fell 6 days be-fore presentation, the creatine kinase level could be re-lated to muscle injury, but the creatine kinase level el-evation persisted for more than 12 days, making atraumatic cause less likely. CSF examination showedprotein elevation and pleocytosis with lymphocytic pre-dominance in four patients (see Table 1). Patient 4 had76% neutrophils initially but converted to 93% lym-phocytes in the second CSF examination collected 4days later.
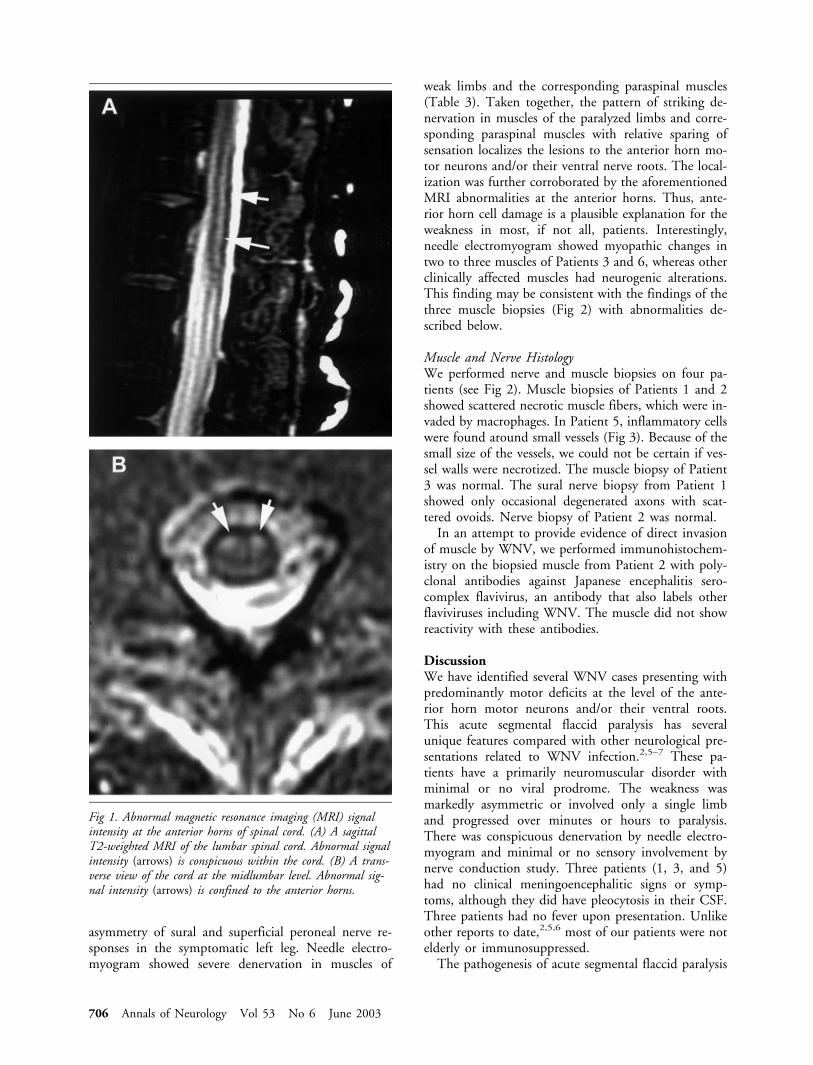
MRI studies in Patients 1 and 2 did not show ab-normalities in the brain or spinal cord. Cervical MRIin Patient 5 showed degenerative changes causing ste-nosis at C3 to C7, but the cord was normal. The spineMRI of Patient 6, performed 3 days after the onset ofweakness, was remarkable for showing focal abnormalsignal intensity within the anterior horns on T2-weighted images (see Fig 1). The level of abnormalMRI findings corresponded to the weakness. No ab-normal signals were found in roots, nor were roots en-hanced after injection of contrast.
Routine blood counts were normal in three patients,but one had increased leukocytes (Patient 3) and twohad reduced platelets (Patients 3 and 4). Sedimentationrates were only performed in Patients 1 and 3 and weremarkedly elevated.
ElectrophysiologyMotor nerve conduction studies showed severely re-duced amplitudes of compound muscle action poten-tials in symptomatic limbs (Table 2). Nerve conduc-tion velocities (CVs) in these limbs were relativelypreserved. All patients whose CVs were mildly reducedalso had very low amplitudes of their compound mus-cle action potential, making it probable that the de-creased CVs were caused by severe axonal loss. Sensorynerve conduction studies were normal except for Pa-tients 4 and 5 who had a history of diabetes andhammertoes/high-arch feet (possibly a pre-existing neu-ropathy), respectively. Patient 1 had a conspicuous
Li et al: Segmental Flaccid Paralysis 705
asymmetry of sural and superficial peroneal nerve re-sponses in the symptomatic left leg. Needle electro-myogram showed severe denervation in muscles of
weak limbs and the corresponding paraspinal muscles(Table 3). Taken together, the pattern of striking de-nervation in muscles of the paralyzed limbs and corre-sponding paraspinal muscles with relative sparing ofsensation localizes the lesions to the anterior horn mo-tor neurons and/or their ventral nerve roots. The local-ization was further corroborated by the aforementionedMRI abnormalities at the anterior horns. Thus, ante-rior horn cell damage is a plausible explanation for theweakness in most, if not all, patients. Interestingly,needle electromyogram showed myopathic changes intwo to three muscles of Patients 3 and 6, whereas otherclinically affected muscles had neurogenic alterations.This finding may be consistent with the findings of thethree muscle biopsies (Fig 2) with abnormalities de-scribed below.
Muscle and Nerve HistologyWe performed nerve and muscle biopsies on four pa-tients (see Fig 2). Muscle biopsies of Patients 1 and 2showed scattered necrotic muscle fibers, which were in-vaded by macrophages. In Patient 5, inflammatory cellswere found around small vessels (Fig 3). Because of thesmall size of the vessels, we could not be certain if ves-sel walls were necrotized. The muscle biopsy of Patient3 was normal. The sural nerve biopsy from Patient 1showed only occasional degenerated axons with scat-tered ovoids. Nerve biopsy of Patient 2 was normal.
In an attempt to provide evidence of direct invasionof muscle by WNV, we performed immunohistochem-istry on the biopsied muscle from Patient 2 with poly-clonal antibodies against Japanese encephalitis sero-complex flavivirus, an antibody that also labels otherflaviviruses including WNV. The muscle did not showreactivity with these antibodies.
DiscussionWe have identified several WNV cases presenting withpredominantly motor deficits at the level of the ante-rior horn motor neurons and/or their ventral roots.This acute segmental flaccid paralysis has severalunique features compared with other neurological pre-sentations related to WNV infection.2,5–7 These pa-tients have a primarily neuromuscular disorder withminimal or no viral prodrome. The weakness wasmarkedly asymmetric or involved only a single limband progressed over minutes or hours to paralysis.There was conspicuous denervation by needle electro-myogram and minimal or no sensory involvement bynerve conduction study. Three patients (1, 3, and 5)had no clinical meningoencephalitic signs or symp-toms, although they did have pleocytosis in their CSF.Three patients had no fever upon presentation. Unlikeother reports to date,2,5,6 most of our patients were notelderly or immunosuppressed.
The pathogenesis of acute segmental flaccid paralysis
Fig 1. Abnormal magnetic resonance imaging (MRI) signalintensity at the anterior horns of spinal cord. (A) A sagittalT2-weighted MRI of the lumbar spinal cord. Abnormal signalintensity (arrows) is conspicuous within the cord. (B) A trans-verse view of the cord at the midlumbar level. Abnormal sig-nal intensity (arrows) is confined to the anterior horns.
706 Annals of Neurology Vol 53 No 6 June 2003

is unknown currently but probably involves the ante-rior horn motor neurons or their ventral nerve roots.Although the clinical presentation of acute segmentalflaccid paralysis is rather unique, because WNV is aflavivirus, it is not surprising that the anterior horn re-gion is affected.1 All flaviviruses of the Japanese andtick-borne encephalitis complex, including WNV, areknown to affect lower motor neurons.8–18 Of interestis that several the flaviviruses causes prominent facial,neck, and shoulder girdle weakness, best typified byRussian spring summer tick borne encephalitis.19 Ittherefore is reasonable to speculate that the paralysis ofthe patients described from Mississippi5 and Georgia6
as well as our cases are caused by anterior horn celllesions, similar to that seen in acute poliomyelitis. Oneof our patients had an MRI showing abnormal signalintensity confined to the anterior horns, further sup-porting a role for spinal motor neurons in the patho-genesis of the disease. However, a potential involve-ment of ventral nerve roots and distal motor nervefibers, as well, cannot be excluded. The rapidity of theparalysis also raises the possibility that damage to theanterior horn may be of vascular origin secondary tothe meningeal inflammation. This is supported by in-flammatory changes around vessels seen in the musclebiopsy of Patient 5 (see Fig 3). Interestingly, similar
Table 2. Eletrophysiology
Nerves Norms
1a
(day 5)2
(day 10)3
(day 7)4b
(day 11)5b
(day 6)6
(5 mo)
R L R L R L R L R L R L
Lower extremity nerve conduction studiesPeroneal
DML �5.5msec 5.4 6.0 5.4 NR 3.9 — — 8.0 NR 7.0 NR NRCV �41m/sec 47 49 38 43 33 29Amp �3mv 4.3 0.5 2.6 3.2 0.1 0.3F �56msec 55 NR NR 50 — NR NR
TibialDML �6.0msec 5.0 7.0 — — 5.5 — — 5.9 6.5 6.4 6.5CV �41m/sec 46 45 46 36 37 39 38Amp �4mv 5.0 1.0 11 2.0 6.5 3.0 0.6F �58msec 57 NR 53 65 66 54 NR
SuralLat �4.5msec 3.8 4.2 3.9 3.8 4.6 — — NR 3.5 NR 4.1 5.1CV �35m/sec 47 45 44 47 37 40 35 36Amp �6�V 17 11 9.3 12 21 8.5 7 10
Sup perLat �4msec 3.6 4.2 — — — — — NR NR — —CV �35m/sec 54 41Amp �5�V 21 9
Upper extremity nerve conduction studiesMedian motor
DML �4.5msec 3.6 — — — 6.0 4.6 5.0 3.9 5.0 4.0 4.0CV �50m/sec 57 44 47 45 50 52 52 51Amp �4mv 9.3 2.0 4.0 2.0 4.5 5.4 8.0 6.0F �32msec 30 39 32 NR 34 — 31 29
Ulnar motorDML �3.5msec 3.0 — — — 5.2 3.3 3.7 3.3 3.1 2.8CV �50m/sec 57 44 51 45 50 57 56Amp �6mv 10 1.0 3.0 4.0 4.6 7.6 8.0F �32msec 28 36 31 NR 36 31 28
Medi senLat �3.5msec 3.2 — — — 4.3 3.4 4.0 4.1 2.9 3.5 3.8CV �45m/sec 56 42 56 48 44 48 50 47Amp �20�V 35 41 39 11 9.2 23 26 29Ulnar senLat �3.5msec 3.5 — — — 4.4 3.4 3.9 3.8 — 3.3 3.5CV �45m/sec 50 41 50 45 47 54 54Amp �10�V 35 52 50 7.0 11 17 27
aDays after onset of weakness.bPatient 4 received prior cyclophosphamide, hydroxydaunomycin, vincristine, prednisone chemotherapy and has a history of diabetes, whichmay contribute to the conduction abnormalities. Patient had evidence of pes cavus suggesting a possible pre-existing neuropathy.
DML � distal motor latency; CV � conduction velocity; L � left; R � right.
Li et al: Segmental Flaccid Paralysis 707

Fig 2. Muscle and nerve biopsies: (upper left) Left lateral gastrocnemius muscle biopsy from Patient 1 shows scattered acutely ne-crotic myofibers (arrows) in early stage of phagocytosis. Frozen section, hematoxylin and eosin stain, �250 original magnification.(upper right) Muscle biopsy from Patient 1. Detail of a necrotic fiber (arrow). Note absence of inflammation or endomysial fibrosisin surrounding muscle. Frozen section, hematoxylin and eosin stain, �500 original magnification. (lower left) Left vastus lateralismuscle biopsy from Patient 2 shows scattered basophilic regenerating fibers (arrows) in distribution similar to Patient 1. Note ab-sence of inflammation or fibrosis. Frozen section, hematoxylin and eosin stain, �250 original magnification. (lower right) Cross-section of sural nerve biopsy from Patient 1 shows several degenerating fibers (arrows). Overall fiber density appears normal. Noinflammation is noted. Plastic embedded section, toluidine blue stain, �500 original magnification.
Table 3. Needle EMG
Patient Muscle Fibs/� Waves Motor Unit Recruitment
Case 1 L leg 0/1� N 3�L lumbar paraspinal 2�/1�R leg 0/0 N N
Patient 2 L leg 2�/3� N 3�L lumbar paraspinal 0/1�R leg 0/1� N 2�
Patient 3 L deltoid and biceps 2�/3� 1� amp/dur 2� poly 1�L triceps 2�/1� N 2�L abductor pollicis brevis 2�/1� N 1�L cervical paraspinal 0/1�R arm 2�/3� N 3–4�L leg 1�/0 N NL orbicularis oris 2�/4� 1 � Polyphasic 3�
Patient 4 L arm 2�/2–3� N� 2� polyphasic 2�L leg 0/0–1� N� 1� polyphasic NAL cervical paraspinal 1�R leg 1�/1� Unable to assess NA
Patient 5 L leg 0 1 Polyphasic 2 4�R leg 0 N 2 2–3�
Patient 6 L arm 3� Polyphasic 2�L leg - - -R arm 1� Polyphasic 2–3�R leg 3�/4� Polyphasic 3–4�R lumbar paraspinal 2�
708 Annals of Neurology Vol 53 No 6 June 2003

inflammatory changes have been described in other fla-vivirus infections.20
The histological findings from muscle biopsies areintriguing. Scattered, necrotic muscle fibers are an un-likely explanation for the severe paralysis observed. Thepresence of these necrotic muscle fibers raises the pos-sibility of viral invasion of muscle. However, immuno-histochemistry did not detect WNV on biopsied mus-cle. Because the immunohistochemistry was performedin only one case, the possibility of direct viral invasionto muscles cannot be completely excluded at this time.
We observed prolonged distal motor latencies andF-wave latencies in at least two patients (see Table 2),implying that there may be a demyelinating compo-nent. However, this slowing might be exaggerated bythe low amplitudes of the compound muscle actionpotential and ventral nerve root damage. Moreover, theinflammatory infiltration identified in the terminaltwigs of motor nerves (see Fig 3) may contribute to theprolongation of distal motor latencies. Interestingly,there was a recent case report documenting an acuteinflammatory demyelinating polyneuropathy–like pre-sentation in a WNV infection patient with CVs of ap-proximately 20 to 30 meter/second.21 These are wellbelow the CVs we observed. In addition, monolimb
involvement and conspicuous asymmetry of weaknessmake it unlikely that these cases were variants of Guil-lain–Barre syndrome, such as acute motor axonal neu-ropathy.22
In summary, acute segmental flaccid paralysis maybe a more common presentation of WNV than previ-ously considered and can occur in the presence of, orabsence of, clinical signs of meningoencephalitis or sys-temic viremia. It therefore will require a high index ofsuspicion to consider this diagnosis. The acute onset ofparalysis without significant sensory loss in one or twomotor regions should make one consider WNV infec-tion, especially in an epidemic area.
We thank Dr W.-J. Shieh for immunohistochemistry study on bi-opsied muscles and B. True and Dr J. Garbern for preparation ofphotomicrographs.
References1. Campbell GL, Marfin AA, Lanciotti RS, Gubler DJ. West
Niles Virus. Lancet Infect Dis 2002;2:519–529.2. Nash D, Mostashari F, Fine A, et al. The outbreak of West
Nile Virus infection in the New York City area in 1999.N Engl J Med 2001;344:1807–1814.
Fig 3. Inflammatory changes in muscle biopsy. Left rectus femoris muscle biopsy from Patient 5 includes intramuscular nerve twigshowing inflammation of small endoneurial and perineurial blood vessels (long arrows) and scattered degenerating myelinated nervefibers (short arrows). There were perivascular cuffs of mononuclear inflammatory cells around the vessels, and some of the inflam-matory cells may have infiltrated the vessel wells. Because the small size of the vessel, we could not be certain whether vessel wallswere necrotized. Frozen section, hematoxylin and eosin stain, �500 original magnification.
Li et al: Segmental Flaccid Paralysis 709

3. No author. West Nile Virus Activity–United States, October10–16, 2002, and Update on West Nile Virus Infections inRecipients of Blood Transfusions. MMWR 2002;51;929–931.
4. Klein C, Kimiagar I, Pollak L, et al. Neurological features ofWest Nile Virus infection during the 2000 outbreak in a re-gional hospital in Israel. J Neurol Sci 2002;200:63–66.
5. Leis AA, Stokic DS, Polk JL, Winkelmann M. A poliomyelitis-like syndrome from West Nile Virus infection. N Engl J Med2002;347:1279–1280.
6. Glass JD, Samuels O, Rich MM. Poliomyelitis due to WestNile Virus. N Engl J Med 2002;347:1280–1281.
7. Leis AA, Stokic DS, Polk JL, et al. Acute flaccid paralysis syn-drome associated with West Nile Virus Infection–Missippi andLouisiana, July–August 2002. MMWR 2002;51:825–828.
8. Tyler KL. West Nile Virus encephalitis in America. N EngJ Med 2001;344:1858–1859.
9. Naidich A, Elliott. St. Louis encephalitis with focal neurologicalsigns. Clin Infect Dis 1999;29:1334–1335.
10. Southern PM Jr, Smith JW, Luby JP, et al. Clinical and labo-ratory features of St Louis encephalitis. Ann Intern Med 1969;71:681–689.
11. Burrow JN, Whelan PI, Kilburn CJ, et al. Australian encepha-litis in the Northern Territory. Clinical and epidemiologicalfeatures 1987–1996. Aust N Z J Med 1998;28:590–596.
12. Misra U, Kalita J. Anterior horn cells are also involved in Jap-anese encephalitis. Acta Neurol Scand 1997;96:114–117.
13. Jackson A. Leg weakness associated with Powassan virus infec-tion. Can Dis Wkly Rep 1989;15:123–124.
14. Haymaker W, Sabin A. Topographic distribution of lesions incentral nervous system in Japanese encephalitis. Nature of thelesions, with report of a case on Okinawa. Arch Neurol Psych1947;57:673–692.
15. Lincoln A, Sivertson S. Acute phase of Japanese B encephalitis.Two hundred and one cases in American soldiers. JAMA 1952;150:268–273.
16. Shieh WJ, Guarner J, Layton M, et al. The role of pathology inan investigation of an outbreak of West Nile Encephalitis inNew York, 1999. Emerg Infect Dis 2000;6:370–372.
17. Ceausu E, Erscoiu S, Calistru P, et al. Clinical manifestations inthe West Nile virus outbreak. Rom J Virol 1997;48:3–11.
18. Gadoth N, Weitzman S, Lehmann EE. Acute anterior myelitiscomplicating West Nile fever. Arch Neurol 1979;36:172–173.
19. Smorodintsev A. Tick-borne Spring-Summer encephalitis. ProgMed Virol 1958;1:210–248.
20. Chu CT, Howell DN, Morgenlander JC, Hulette CM. Elec-tron microscopic diagnosis of human Flavivirus encephalitis.Am J Surg Pathol 1999;23:1217–1226.
21. Ahmed S, Libman R, Wesson K, et al. Guillain-Barresyndrome: an unusual presentation of West Nile virus infection.Neurology 2000;55:144–146.
22. McKhann GM, Cornblath DR, Griffin JW, et al. Acute motoraxonal neuropathy: a frequent cause of acute flaccid paralysis inChina. Ann Neurol 1993;33:333–342.
710 Annals of Neurology Vol 53 No 6 June 2003