association between paraoxonase-1 (pon-1) polymorphisms and
TRANSCRIPT

Int J Clin Exp Med 2016;9(2):1490-1499www.ijcem.com /ISSN:1940-5901/IJCEM0015013
Original ArticleAssociation between paraoxonase-1 (PON-1) polymorphisms and polycystic ovary syndrome susceptibility: a meta-analysis
Boyang Chen1*, Yafeng Wang2*, Wenwei Lin1*, Heping Jiang3, Chao Liu4, Changqing Dong4, Haiyong Gu5, Mingqiang Kang1, Weifeng Tang1
1Department of Thoracic Surgery, The Union Clinical Medical College of Fujian Medical University, Fuzhou, Fujian Province, China; 2Department of Cardiology, The People’s Hospital of Xishuangbanna Dai Autonomous Prefecture, Jinghong, Yunnan Province, China; 3Department of Emergency, Affiliated Jintan People’s Hospital of Jiangsu University, Jintan, China; 4Department of Cardiothoracic Surgery, Affiliated People’s Hospital of Jiangsu University, Zhenjiang, Jiangsu Province, China; 5Department of Thoracic Surgery, Shanghai Chest Hospital, Shanghai Jiaotong University, Shanghai, China. *Equal contributors.
Received August 24, 2015; Accepted January 30, 2016; Epub February 15, 2016; Published February 29, 2016
Abstract: Several investigations have focused on the relationship between paraoxonase-1 (PON-1) polymorphisms and the risk of polycystic ovary syndrome (PCOS); however, the result remains conflicting. To obtain a more precise estimation of the correlation between PON-1 polymorphisms [rs705379 C>T (-108C/T), rs854560 T>A (55Leu/Met) and rs662 A>G (192Gln/Arg)] and the risk of PCOS, we performed a meta-analysis of 940 PCOS cases and 881 controls concerning rs705379 C>T polymorphism, 1,436 PCOS cases and 1,053 controls concerning rs854560 T>A polymorphism and 1,306 PCOS cases and 983 controls concerning rs662 A>G polymorphism from eight publi-cations. The crude odds ratios (ORs) with 95% confidence intervals (CIs) were harnessed to measure the strength of the association. Our findings suggested that there was an evidence of a correlation between the PON-1 rs705379 C>T polymorphism and increased risk of PCOS in three genetic models: allelic comparison, homozygote comparison and recessive comparison. While the association between PON-1 rs854560 T>A polymorphism and a decreased risk of PCOS was found in dominant model. PON-1 rs662 A>G polymorphism is not correlated with PCOS susceptibil-ity. In summary, this study suggests that PON-1 rs705379 C>T polymorphism may cause an increased risk of PCOS, while PON-1 rs854560 T>A polymorphism may cause a decreased risk of PCOS.
Keywords: Polymorphism, paraoxonase-1, polycystic ovary syndrome, risk
Introduction
Polycystic ovary syndrome (PCOS), a heteroge-neous endocrine metabolic disorder, is charac-terized by oligo- or anovulation, exaggerated production of androgens and the presence of polycystic ovaries [1-3]. PCOS is a leading cause of infertility and affects about 5-10% of reproductive-age women [2, 3]. PCOS is often associated with increased prevalence of meta-bolic syndrome and type 2 diabetes, obesity, elevated oxidative stress, systemic chronic inflammation and increased susceptibilities of atherosclerosis and cardiovascular disease [4-10]. These findings encourage researchers to explore the interaction between predispos-
ing genes and environmental factors to inter-pret this disease. The etiology of PCOS is very elusive, although a variety of investigations have focused on the function of the oxidative stress and chronic inflammation.
The paraoxonase-1 (PON-1) gene lies in chro-mosome 7 and encodes a 43KDa protein. PON-1, a versatile calcium-dependent antioxidant enzyme, is mainly produced in the liver and cir-culates within HDL particles [11]. Prior studies demonstrated that decreased PON1 activity in PCOS cases was associated with the high level of hyperandrogenemia [12, 13]. Treatment with hormonal supplements (cyproterone acetate and ethinyloestradiol) and metformin has been
PON-1 polymorphisms and polycystic ovary syndrome
1491 Int J Clin Exp Med 2016;9(2):1490-1499
shown to elevate PON1 activity, and then de- creases oxidative stress in women with PCOS [14, 15].
Recently, several studies suggested that PON-1 single nucleotide polymorphisms (SNPs) were associated with a number of diseases such as cardiovascular disease and diabetes [16-19]. More studies have demonstrated that the oxi-dative stress plays an important role in the eti-ology of PCOS [20-22]. To date, several studies have explored the relationship of PON-1 poly-morphisms [rs705379 C>T (-108C/T), rs8545- 60 T>A (55Leu/Met)] and rs662 A>G (192Gln/Arg)] with PCOS susceptibility [23-30]; however, the results remain conflicting. Thus, we carried out this meta-analysis by pooling data to iden-tify the function of the PON-1 polymorphisms in the development of PCOS.
Materials and methods
The meta-analysis is reported on the basis of PRISMA checklist guideline (Table S1) [31].
Search strategy
PubMed, EMBASE and China National Know- ledge Internet (CNKI) databases were searched the publications which were published before
study, (c) studies that provided insufficient data and (d) duplicated data.
Data extraction
Three reviewers (B. Chen, Y. Wang and W. Lin) independently screened and extracted infor-mation from the eligible studies that met the inclusion criteria. If there were any discrepan-cies, an agreement was reached by discussion between all reviewers. The following informa-tion was sought and extracted from each publi-cation: (a) first author’s surname, (b) year of publication, (c) country of origin, (d) ethnicity, (e) genotyping method, (f) sample size, and (g) numbers of genotypes and alleles.
Statistical analysis
Hardy-Weinberg equilibrium (HWE) was mea-sured via an internet-based Fisher’s exact test (http://ihg.gsf.de/cgi-bin/hw/hwa1.pl) and P< 0.05 was considered significant. Correlations between PON-1 polymorphisms and PCOS sus-ceptibility were assessed using crude odds ratios (ORs) and their 95% confidence intervals (CIs). The Chi-square-based Q-statistic and I2
statistical tests were harnessed to access the heterogeneity assumption among studies [32]. The value of I2>50% or P<0.10 indicates sub-
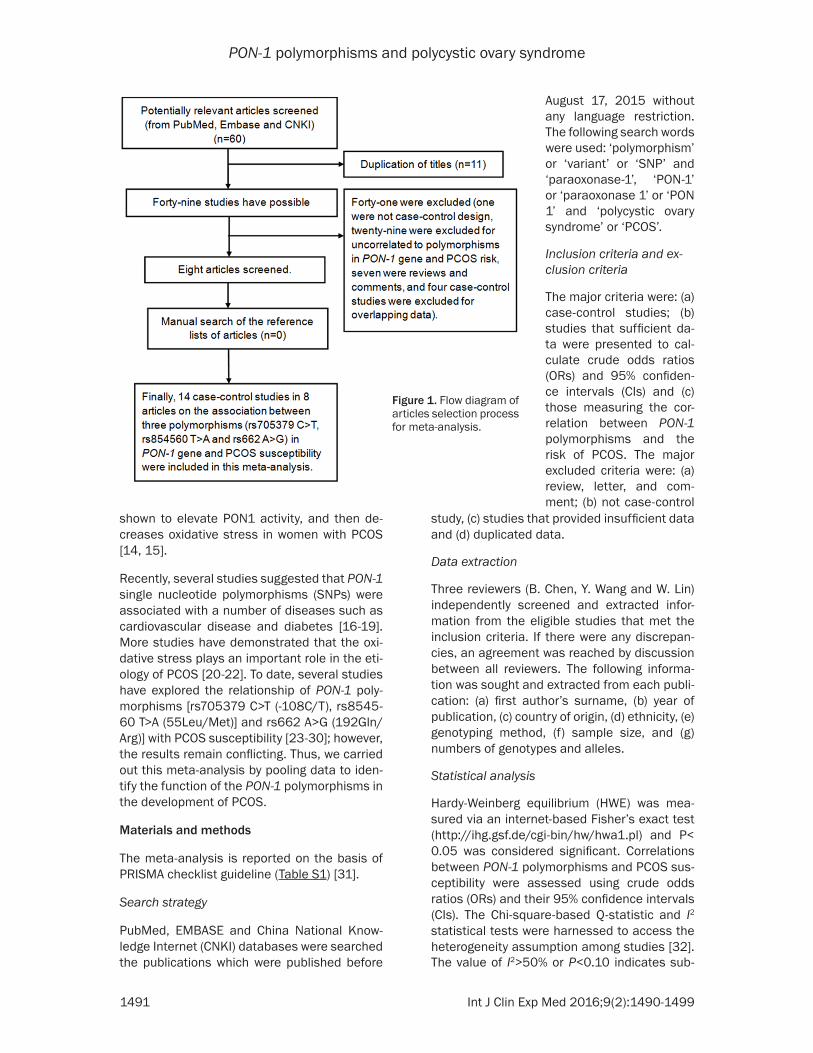
Figure 1. Flow diagram of articles selection process for meta-analysis.
August 17, 2015 without any language restriction. The following search words were used: ‘polymorphism’ or ‘variant’ or ‘SNP’ and ‘paraoxonase-1’, ‘PON-1’ or ‘paraoxonase 1’ or ‘PON 1’ and ‘polycystic ovary syndrome’ or ‘PCOS’.
Inclusion criteria and ex-clusion criteria
The major criteria were: (a) case-control studies; (b) studies that sufficient da- ta were presented to cal-culate crude odds ratios (ORs) and 95% confiden- ce intervals (CIs) and (c) those measuring the cor-relation between PON-1 polymorphisms and the risk of PCOS. The major excluded criteria were: (a) review, letter, and com-ment; (b) not case-control
PON-1 polymorphisms and polycystic ovary syndrome
1492 Int J Clin Exp Med 2016;9(2):1490-1499
stantial heterogeneity among the studies, ran-dom-effects models using DerSimonian-Laird method were used to calculate the pooled ORs and CIs [33], otherwise, fixed-effects models using Mantel-Haenszel methods were har-nessed [34]. The Begg’s funnel plot [35] and Egger’s linear regression [36] were used to measure the potential publication bias among the studies. For publication bias, a P<0.1 was considered significant. If there were any biases, nonparametric “trim-and-fill” method was per-formed to assess the stability of our results. All analyses were conducted with Stata 12.0 sta-tistical software (Stata Corp LP, College Station, TX, USA). A P<0.05 (two-sided) was defined as representative of statistically significant differ- ence.
Results
Study characteristics
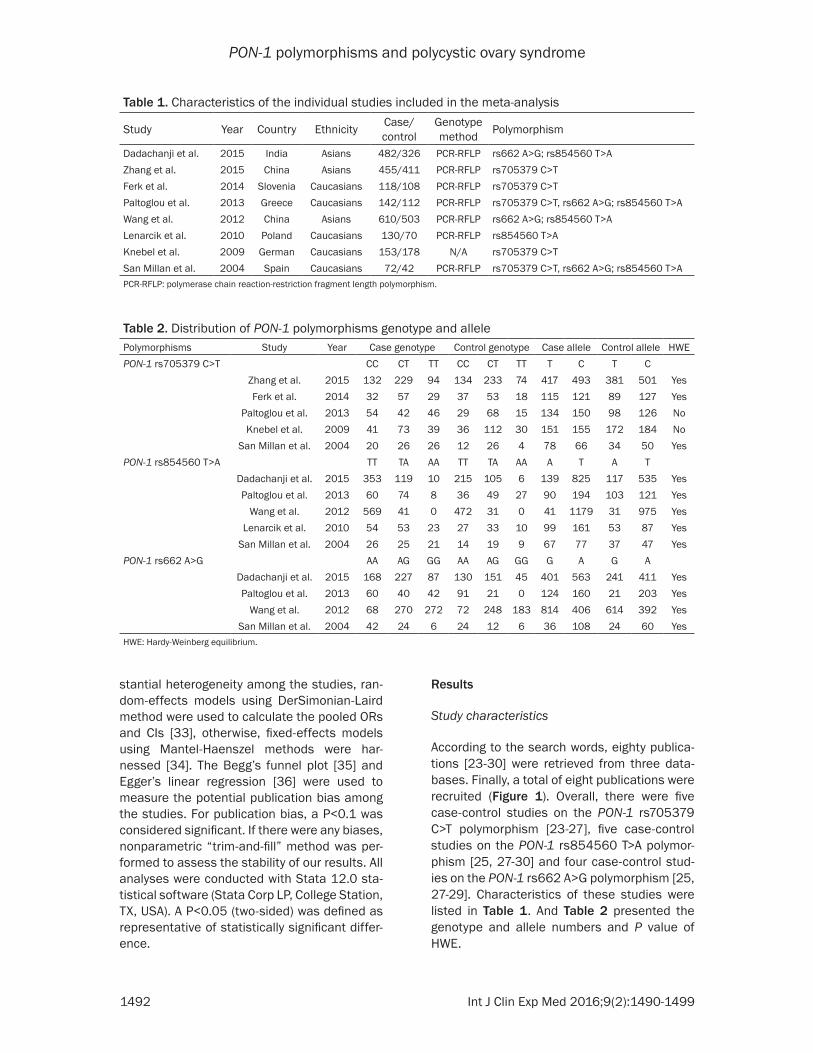
According to the search words, eighty publica-tions [23-30] were retrieved from three data-bases. Finally, a total of eight publications were recruited (Figure 1). Overall, there were five case-control studies on the PON-1 rs705379 C>T polymorphism [23-27], five case-control studies on the PON-1 rs854560 T>A polymor-phism [25, 27-30] and four case-control stud-ies on the PON-1 rs662 A>G polymorphism [25, 27-29]. Characteristics of these studies were listed in Table 1. And Table 2 presented the genotype and allele numbers and P value of HWE.
Table 1. Characteristics of the individual studies included in the meta-analysis
Study Year Country Ethnicity Case/control
Genotype method Polymorphism
Dadachanji et al. 2015 India Asians 482/326 PCR-RFLP rs662 A>G; rs854560 T>AZhang et al. 2015 China Asians 455/411 PCR-RFLP rs705379 C>TFerk et al. 2014 Slovenia Caucasians 118/108 PCR-RFLP rs705379 C>TPaltoglou et al. 2013 Greece Caucasians 142/112 PCR-RFLP rs705379 C>T, rs662 A>G; rs854560 T>A Wang et al. 2012 China Asians 610/503 PCR-RFLP rs662 A>G; rs854560 T>ALenarcik et al. 2010 Poland Caucasians 130/70 PCR-RFLP rs854560 T>AKnebel et al. 2009 German Caucasians 153/178 N/A rs705379 C>TSan Millan et al. 2004 Spain Caucasians 72/42 PCR-RFLP rs705379 C>T, rs662 A>G; rs854560 T>A PCR-RFLP: polymerase chain reaction-restriction fragment length polymorphism.
Table 2. Distribution of PON-1 polymorphisms genotype and allelePolymorphisms Study Year Case genotype Control genotype Case allele Control allele HWEPON-1 rs705379 C>T CC CT TT CC CT TT T C T C
Zhang et al. 2015 132 229 94 134 233 74 417 493 381 501 YesFerk et al. 2014 32 57 29 37 53 18 115 121 89 127 Yes
Paltoglou et al. 2013 54 42 46 29 68 15 134 150 98 126 NoKnebel et al. 2009 41 73 39 36 112 30 151 155 172 184 No
San Millan et al. 2004 20 26 26 12 26 4 78 66 34 50 YesPON-1 rs854560 T>A TT TA AA TT TA AA A T A T
Dadachanji et al. 2015 353 119 10 215 105 6 139 825 117 535 YesPaltoglou et al. 2013 60 74 8 36 49 27 90 194 103 121 Yes
Wang et al. 2012 569 41 0 472 31 0 41 1179 31 975 YesLenarcik et al. 2010 54 53 23 27 33 10 99 161 53 87 Yes
San Millan et al. 2004 26 25 21 14 19 9 67 77 37 47 YesPON-1 rs662 A>G AA AG GG AA AG GG G A G A
Dadachanji et al. 2015 168 227 87 130 151 45 401 563 241 411 YesPaltoglou et al. 2013 60 40 42 91 21 0 124 160 21 203 Yes
Wang et al. 2012 68 270 272 72 248 183 814 406 614 392 YesSan Millan et al. 2004 42 24 6 24 12 6 36 108 24 60 Yes
HWE: Hardy-Weinberg equilibrium.
PON-1 polymorphisms and polycystic ovary syndrome
1493 Int J Clin Exp Med 2016;9(2):1490-1499
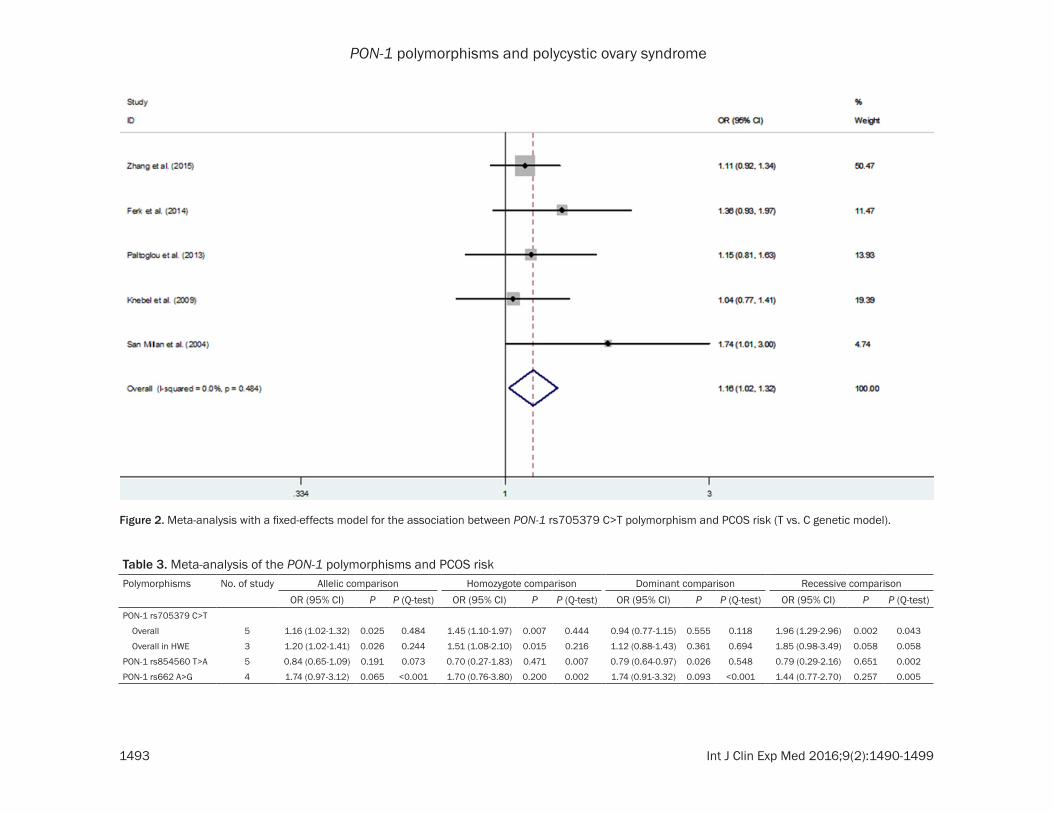
Figure 2. Meta-analysis with a fixed-effects model for the association between PON-1 rs705379 C>T polymorphism and PCOS risk (T vs. C genetic model).
Table 3. Meta-analysis of the PON-1 polymorphisms and PCOS riskPolymorphisms No. of study Allelic comparison Homozygote comparison Dominant comparison Recessive comparison
OR (95% CI) P P (Q-test) OR (95% CI) P P (Q-test) OR (95% CI) P P (Q-test) OR (95% CI) P P (Q-test)PON-1 rs705379 C>T
Overall 5 1.16 (1.02-1.32) 0.025 0.484 1.45 (1.10-1.97) 0.007 0.444 0.94 (0.77-1.15) 0.555 0.118 1.96 (1.29-2.96) 0.002 0.043
Overall in HWE 3 1.20 (1.02-1.41) 0.026 0.244 1.51 (1.08-2.10) 0.015 0.216 1.12 (0.88-1.43) 0.361 0.694 1.85 (0.98-3.49) 0.058 0.058
PON-1 rs854560 T>A 5 0.84 (0.65-1.09) 0.191 0.073 0.70 (0.27-1.83) 0.471 0.007 0.79 (0.64-0.97) 0.026 0.548 0.79 (0.29-2.16) 0.651 0.002
PON-1 rs662 A>G 4 1.74 (0.97-3.12) 0.065 <0.001 1.70 (0.76-3.80) 0.200 0.002 1.74 (0.91-3.32) 0.093 <0.001 1.44 (0.77-2.70) 0.257 0.005

PON-1 polymorphisms and polycystic ovary syndrome
1494 Int J Clin Exp Med 2016;9(2):1490-1499
Figure 3. Meta-analysis with a fixed-effects model for the association between PON-1 rs854560 T>A polymorphism and PCOS risk (AA+TA vs. TT genetic model).
PON-1 polymorphisms and polycystic ovary syndrome
1495 Int J Clin Exp Med 2016;9(2):1490-1499
Quantitative synthesis
PON-1 rs705379 C>T polymorphism: There were five publications [23-27] met the inclusion criteria with 940 PCOS cases and 881 controls concerning rs705379 C>T polymorphism. Four case-control studies were from Caucasians [24-27] and one was from Asians [23]. Overall, PON-1 rs705379 C>T polymorphism was corre-lated with a significantly increased risk of PCOS (OR, 1.16; 95% CI, 1.02-1.32; P = 0.025 for T vs. C; OR, 1.45; 95% CI, 1.10-1.97; P = 0.007 for TT vs. CC and OR, 1.96; 95% CI, 1.29-2.96; P = 0.002 for TT vs. CC+CT; Figure 2 and Table 3). For limited number of studies, a subgroup analysis was not performed.
PON-1 rs854560 T>A polymorphism: A total of 1,436 PCOS cases and 1,053 controls from five case-control studies [25, 27-30] were in- cluded in our analysis on the relationship between PON-1 rs854560 T>A polymorphism and PCOS susceptibility. Two case-control stud-ies were from Asians [28, 29] and three were from Caucasians [25, 27, 30]. The present find-ings suggested an evidence of the correlation between PON-1 rs854560 T>A polymorphism and the decreased risk of PCOS (OR, 0.79; 95% CI, 0.64-0.97; P = 0.026 for AA+TA vs. TT; Figure 3 and Table 3).
PON-1 rs662 A>G polymorphism: In total, 1,306 PCOS cases and 983 controls from four studies were recruited in the current study on the association between PON-1 rs662 A> G polymorphism and PCOS susceptibility. Two
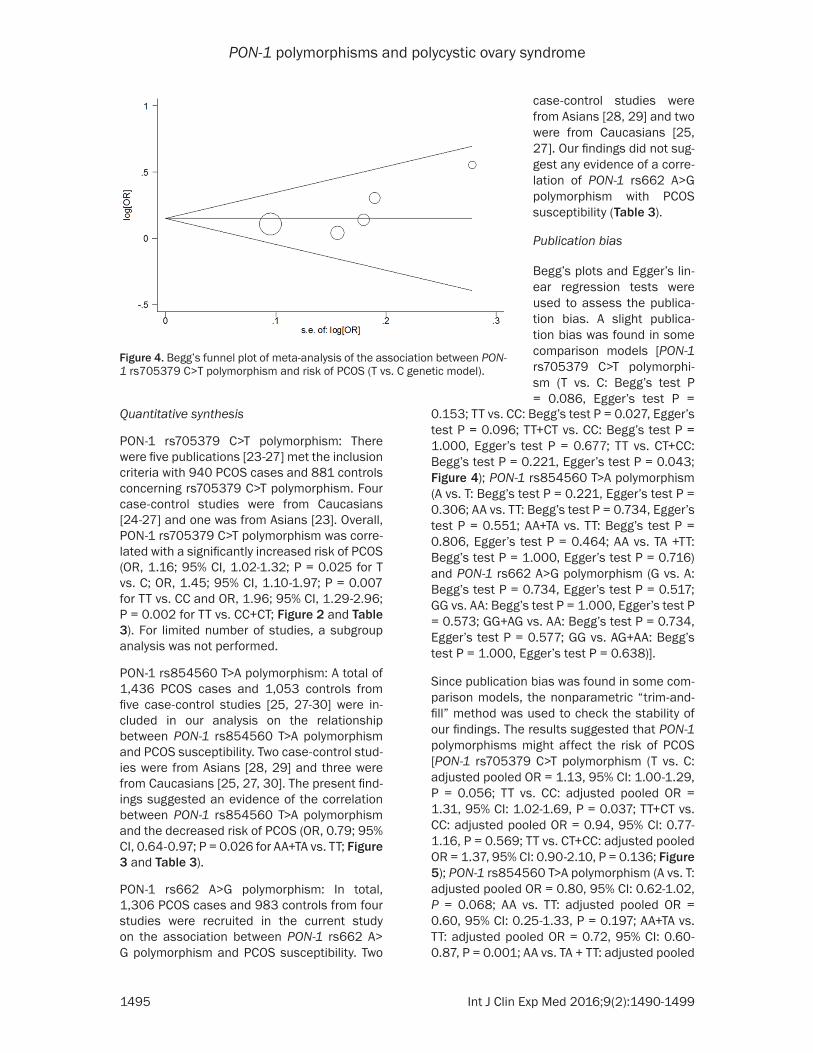
0.153; TT vs. CC: Begg’s test P = 0.027, Egger’s test P = 0.096; TT+CT vs. CC: Begg’s test P = 1.000, Egger’s test P = 0.677; TT vs. CT+CC: Begg’s test P = 0.221, Egger’s test P = 0.043; Figure 4); PON-1 rs854560 T>A polymorphism (A vs. T: Begg’s test P = 0.221, Egger’s test P = 0.306; AA vs. TT: Begg’s test P = 0.734, Egger’s test P = 0.551; AA+TA vs. TT: Begg’s test P = 0.806, Egger’s test P = 0.464; AA vs. TA +TT: Begg’s test P = 1.000, Egger’s test P = 0.716) and PON-1 rs662 A>G polymorphism (G vs. A: Begg’s test P = 0.734, Egger’s test P = 0.517; GG vs. AA: Begg’s test P = 1.000, Egger’s test P = 0.573; GG+AG vs. AA: Begg’s test P = 0.734, Egger’s test P = 0.577; GG vs. AG+AA: Begg’s test P = 1.000, Egger’s test P = 0.638)].
Since publication bias was found in some com-parison models, the nonparametric “trim-and-fill” method was used to check the stability of our findings. The results suggested that PON-1 polymorphisms might affect the risk of PCOS [PON-1 rs705379 C>T polymorphism (T vs. C: adjusted pooled OR = 1.13, 95% CI: 1.00-1.29, P = 0.056; TT vs. CC: adjusted pooled OR = 1.31, 95% CI: 1.02-1.69, P = 0.037; TT+CT vs. CC: adjusted pooled OR = 0.94, 95% CI: 0.77-1.16, P = 0.569; TT vs. CT+CC: adjusted pooled OR = 1.37, 95% CI: 0.90-2.10, P = 0.136; Figure 5); PON-1 rs854560 T>A polymorphism (A vs. T: adjusted pooled OR = 0.80, 95% CI: 0.62-1.02, P = 0.068; AA vs. TT: adjusted pooled OR = 0.60, 95% CI: 0.25-1.33, P = 0.197; AA+TA vs. TT: adjusted pooled OR = 0.72, 95% CI: 0.60-0.87, P = 0.001; AA vs. TA + TT: adjusted pooled
Figure 4. Begg’s funnel plot of meta-analysis of the association between PON-1 rs705379 C>T polymorphism and risk of PCOS (T vs. C genetic model).
case-control studies were from Asians [28, 29] and two were from Caucasians [25, 27]. Our findings did not sug-gest any evidence of a corre-lation of PON-1 rs662 A>G polymorphism with PCOS susceptibility (Table 3).
Publication bias
Begg’s plots and Egger’s lin-ear regression tests were used to assess the publica-tion bias. A slight publica- tion bias was found in some comparison models [PON-1 rs705379 C>T polymorphi- sm (T vs. C: Begg’s test P = 0.086, Egger’s test P =

PON-1 polymorphisms and polycystic ovary syndrome
1496 Int J Clin Exp Med 2016;9(2):1490-1499
OR = 0.63, 95% CI: 0.26-1.53, P = 0.310) and PON-1 rs662 A>G polymorphism (G vs. A: adjusted pooled OR = 1.74, 95% CI: 0.97-3.11, P = 0.064; GG vs. AA: adjusted pooled OR = 1.24, 95% CI: 0.50-3.07, P = 0.639; GG+AG vs. AA: adjusted pooled OR = 1.74, 95% CI: 0.91-3.32, P = 0.093; GG vs. AG+AA: adjusted pooled OR = 1.42, 95% CI: 0.79-2.56, P = 0.238)].
Discussion
A total of eight publications were recruited to explore the relationship between PON-1 poly-morphisms and the risk of PCOS. According to the results, the PON-1 rs705379 C>T variants were suggested to be correlated with an in- creased risk of PCOS, while PON-1 rs854560 T>A variants might be a protective factor for PCOS. We failed to confirm the correlation between PON-1 rs662 A>G polymorphism and PCOS susceptibility.
For PON-1 rs705379 C>T polymorphism, the T allele carriers showed higher PCOS incident risk in comparison with the C allele carriers. The crude ORs and 95% CIs were 1.16 and 1.02-1.32, 1.45 and 1.10-1.97, and 1.96 and 1.29-2.96 for T vs. C, TT vs. CC and TT vs. CC+CT, respectively. There were two case-con-trol studies [25, 26] was deviated from HWE. When we omitted these studies, the results were not substantively changed (Table 3), sug-gesting the stability of our findings. For PON-1 rs854560 T>A polymorphism, the A allele carri-
5379 C>T variants were associated with the risk of PCOS. Our findings were supported by some prior case-controls. In a previous study in Spain conducted by San Millan et al. [27], com-pared with the C allele, the T allele was a risk factor of PCOS. These results were also sup-ported by the other study [25], in which the TT homozygote increased the risk of PCOS significantly. The ORs and 95% CIs were 3.01 and 1.62-5.92 for recessive comparison. The majority of our findings highlighted the T allele of PON-1 rs705379 C>T polymorphism modi-fied the susceptibility of PCOS. In vitro, PON-1 rs705379 C>T variants were associated with the expression level of PON1; the rs705379 TT genotype decreased the expression of the PON1-relative enzyme compared to the rs705- 379 CC genotype [37]. In combination with our findings, PON-1 rs705379 C>T variants might increase the susceptibility of PCOS, probably through reducing the expression of the enzyme, decreasing the PON1 lactonase activities and promoting oxidative stress.
Results of Several previous study [25, 28] dem-onstrated that compared with the PON-1 rs- 854560 T allele, the A allele was a protective factor of PCOS. A polymorphisms, namely PON-1 rs854560 T>A in exon 3 of the PON1, have been known to modulate the stability and active site of the enzyme, and then affecting its levels and catalytic efficiency respectively [38]. Thus, PON-1 rs854560 T>A variants might decrease the risk of PCOS, probably through
Figure 5. Filled funnel plot of meta-analysis of the association between PON-1 rs705379 C>T polymorphism and risk of PCOS (T vs. C genetic model).
ers showed lower PCOS inci-dent susceptibility in com-parison with the T allele car-riers. The crude ORs and 95% CIs were 0.79 and 0.64-0.97 for AA+TA vs. TT genetic model.
For PON-1 rs705379 C>T polymorphism, publication bias was identified in three genetic comparison models (allelic comparison, homozy-gote comparison and reces-sive comparison), the non-parametric “trim-and-fill” me- thod was carried out to mea-sure the stability of our re- sults. The results of adjust- ed pooled ORs and CIs also suggested that PON-1 rs70-

PON-1 polymorphisms and polycystic ovary syndrome
1497 Int J Clin Exp Med 2016;9(2):1490-1499
elevating the expression of the enzyme, in- creasing stability and active site of the enzyme and reducing oxidative stress.
Nevertheless, our findings still have some limi-tations. First, large heterogeneity among in- cluded studies was observed, which might be due to the difference in ethnicity and geograph-ic areas (some environmental factors). Second, the sample sizes of these studies were relative-ly small, which might lead to limited statistical power. Third, lack of sufficient data from the eligible studies imposed restriction on further assessment of potential interactions; however, this was very important because gene-gene and gene-environment interactions might mod-ify various PCOS risks. Fourth, there were only eight studies included in our analysis; there-fore, subgroup analyses were not conducted. Finally, due to the limited number of studies recruited in current study, sensitivity analyses were not carried out.
To summarize, our findings highlight that T allele of the PON-1 rs705379 C>T polymor-phism may increase the risk of PCOS. However, the A allele of PON-1 rs854560 T>A polymor-phism is a protective factor of PCOS. For practi-cal reasons, additional studies across different populations incorporating with further function-al assessments are needed to confirm these findings.
Acknowledgements
This study was supported in part by Jiang- su University Clinical Medicine Science and Technology Development Fund (JLY201400- 12), National Natural Science Foundation of China (81472332, 81341006), Fujian Province Natural Science Foundation (2013J01126, 2013J05116), Fujian Medical University pro-fessor fund (JS12008), The Fund of Union Hospital (2015TC-1-048 and 2015TC-2-004) and Fujian Province science and technology programmed fund (2012Y0030).
Disclosure of conflict of interest
None.
Address correspondence to: Drs. Weifeng Tang and Mingqiang Kang, Department of Thoracic Surgery, The Union Clinical Medical College of Fujian Medical University, Fuzhou 350001, China. E-mail: twf001-
[email protected] (WFT); [email protected] (MQK)
References
[1] Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syn-drome. Fertil Steril 2004; 81: 19-25.
[2] Ehrmann DA. Polycystic ovary syndrome. N Engl J Med 2005; 352: 1223-1236.
[3] Pasquali R and Gambineri A. Polycystic ovary syndrome: a multifaceted disease from adoles-cence to adult age. Ann N Y Acad Sci 2006; 1092: 158-174.
[4] Lerchbaum E, Schwetz V, Giuliani A and Obermayer-Pietsch B. Influence of a positive family history of both type 2 diabetes and PCOS on metabolic and endocrine parameters in a large cohort of PCOS women. Eur J Endocrinol 2014; 170: 727-739.
[5] G S, A B, Kamath A, Shivaprakash P, Adhikari P, Up R, Hn G and Padubidri JR. Acanthosis Nigricansin PCOS Patients and Its Relation with Type 2 Diabetes Mellitus and Body Mass at a Tertiary Care Hospital in Southern India. J Clin Diagn Res 2013; 7: 317-319.
[6] Macut D, Bjekic-Macut J and Savic-Radojevic A. Dyslipidemia and oxidative stress in PCOS. Front Horm Res 2013; 40: 51-63.
[7] Murri M, Luque-Ramirez M, Insenser M, Ojeda-Ojeda M and Escobar-Morreale HF. Circulating markers of oxidative stress and polycystic ova-ry syndrome (PCOS): a systematic review and meta-analysis. Hum Reprod Update 2013; 19: 268-288.
[8] Solano ME, Sander VA, Ho H, Motta AB and Arck PC. Systemic inflammation, cellular influx and up-regulation of ovarian VCAM-1 expres-sion in a mouse model of polycystic ovary syn-drome (PCOS). J Reprod Immunol 2011; 92: 33-44.
[9] Meyer ML, Malek AM, Wild RA, Korytkowski MT and Talbott EO. Carotid artery intima-media thickness in polycystic ovary syndrome: a sys-tematic review and meta-analysis. Hum Reprod Update 2012; 18: 112-126.
[10] de Groot PC, Dekkers OM, Romijn JA, Dieben SW and Helmerhorst FM. PCOS, coronary heart disease, stroke and the influence of obesity: a systematic review and meta-analysis. Hum Reprod Update 2011; 17: 495-500.
[11] Goswami B, Tayal D, Gupta N and Mallika V. Paraoxonase: a multifaceted biomolecule. Clin Chim Acta 2009; 410: 1-12.
[12] Bayram F, Kocer D, Ozsan M and Muhtaroglu S. Evaluation of endothelial dysfunction, lipid metabolism in women with polycystic ovary
PON-1 polymorphisms and polycystic ovary syndrome
1498 Int J Clin Exp Med 2016;9(2):1490-1499
syndrome: relationship of paraoxonase 1 activ-ity, malondialdehyde levels, low-density lipo-protein subfractions, and endothelial dysfunc-tion. Gynecol Endocrinol 2012; 28: 497-501.
[13] Dursun P, Demirtas E, Bayrak A and Yarali H. Decreased serum paraoxonase 1 (PON1) ac-tivity: an additional risk factor for atheroscle-rotic heart disease in patients with PCOS? Hum Reprod 2006; 21: 104-108.
[14] Kocer D, Bayram F and Diri H. The effects of metformin on endothelial dysfunction, lipid metabolism and oxidative stress in women with polycystic ovary syndrome. Gynecol Endo- crinol 2014; 30: 367-371.
[15] Carlioglu A, Kaygusuz I, Karakurt F, Gumus, II, Uysal A, Kasapoglu B, Armutcu F, Uysal S, Keskin EA and Koca C. The platelet activating factor acetyl hydrolase, oxidized low-density li-poprotein, paraoxonase 1 and arylesterase lev-els in treated and untreated patients with poly-cystic ovary syndrome. Arch Gynecol Obstet 2014; 290: 929-935.
[16] Han Y, Dorajoo R, Ke T, Ayala B, Chang X, Khor CC, van Dam RM, Yuan JM, Koh WP, Liu J, Goh DY, Friedlander Y and Heng CK. Interaction effects between Paraoxonase 1 variants and cigarette smoking on risk of coronary heart disease in a Singaporean Chinese population. Atherosclerosis 2015; 240: 40-45.
[17] Lawlor DA, Day IN, Gaunt TR, Hinks LJ, Briggs PJ, Kiessling M, Timpson N, Smith GD and Ebrahim S. The association of the PON1 Q192R polymorphism with coronary heart dis-ease: findings from the British Women’s Heart and Health cohort study and a meta-analysis. BMC Genet 2004; 5: 17.
[18] Al-Hakeem MM, Abotalib Z, Alharbi KK and Khan IA. Relationship between the paraox-onase 1 gene glutamine 192 to arginine poly-morphism and gestational diabetes mellitus in Saudi women. Clin Biochem 2014; 47: 122-125.
[19] Batool A, Jahan N, Sun Y, Hanif A and Xue H. Genetic association of IDE, POU2F1, PON1, IL1alpha and IL1beta with type 2 diabetes in Pakistani population. Mol Biol Rep 2014; 41: 3063-3069.
[20] Foroozanfard F, Jamilian M, Bahmani F, Talaee R, Talaee N, Hashemi T, Nasri K, Asemi Z and Esmaillzadeh A. Calcium plus vitamin D supplementation influences biomarkers of in-flammation and oxidative stress in overweight and vitamin D-deficient women with polycystic ovary syndrome: a randomized double-blind placebo-controlled clinical trial. Clin Endocrinol (Oxf) 2015; 83: 888-94.
[21] Razavi M, Jamilian M, Kashan ZF, Heidar Z, Mohseni M, Ghandi Y, Bagherian T and Asemi Z. Selenium Supplementation and the Effects
on Reproductive Outcomes, Biomarkers of Inflammation, and Oxidative Stress in Women with Polycystic Ovary Syndrome. Horm Metab Res 2015; [Epub ahead of print].
[22] Selen ES, Bolandnazar Z, Tonelli M, Butz DE, Haviland JA, Porter WP and Assadi-Porter FM. NMR Metabolomics Show Evidence for Mito- chondrial Oxidative Stress in a Mouse Model of Polycystic Ovary Syndrome. J Proteome Res 2015; 14: 3284-3291.
[23] Zhang Y, Liu H, He J, Xu K, Bai H, Wang Y, Zhang F, Zhang J, Cheng L and Fan P. Lacto- nase activity and status of paraoxonase 1 in Chinese women with polycystic ovarian syn-drome. Eur J Endocrinol 2015; 172: 391-402.
[24] Ferk P and Gersak K. Association of -108 C>T polymorphism with polycystic ovary syndrome. Biomed Rep 2014; 2: 255-259.
[25] Paltoglou G, Tavernarakis G, Christopoulos P, Vlassi M, Gazouli M, Deligeoroglou E, Creatsas G and Mastorakos G. PON1-108 TT and PON1-192 RR genotypes are more frequently en-countered in Greek PCOS than non-PCOS women, and are associated with hyperandro-genaemia. Clin Endocrinol (Oxf) 2013; 79: 259-266.
[26] Knebel B, Janssen OE, Hahn S, Nitzgen U, Jacob S, Haas J, Mack S, Muller-Wieland D and Kotzka J. [Combined analyses of paraox-onase-1 and IGF-2 polymorphism in polycystic ovary syndrome]. Dtsch Med Wochenschr 2009; 134: 1040-1046.
[27] San Millan JL, Corton M, Villuendas G, Sancho J, Peral B and Escobar-Morreale HF. Associ- ation of the polycystic ovary syndrome with ge-nomic variants related to insulin resistance, type 2 diabetes mellitus, and obesity. J Clin Endocrinol Metab 2004; 89: 2640-2646.
[28] Dadachanji R, Shaikh N, Khavale S, Patil A, Shah N and Mukherjee S. PON1 polymor-phisms are associated with polycystic ovary syndrome susceptibility, related traits, and PON1 activity in Indian women with the syn-drome. Fertil Steril 2015; 104: 207-216.
[29] Wang Y, Liu H, Fan P, Bai H, Zhang J and Zhang F. Evidence for association between paraox-onase 1 gene polymorphisms and polycystic ovarian syndrome in southwest Chinese wom-en. Eur J Endocrinol 2012; 166: 877-885.
[30] Lenarcik A, Bidzinska-Speichert B and Tworow- ska-Bardzinska U. The role of chronic inflam-mation and Leu55Met PON1 polymorphism in the pathogenesis of polycystic ovary syn-drome. Gynecol Endocrinol 2010; 26: 673-683.
[31] Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med 2009; 151: 264-269, W264.
PON-1 polymorphisms and polycystic ovary syndrome
1499 Int J Clin Exp Med 2016;9(2):1490-1499
[32] Cochran WG. The combination of estimates from different experiments. 1954.
[33] DerSimonian R and Laird N. Meta-analysis in clinical trials. Control Clin Trials 1986; 7: 177-188.
[34] Mantel N, Haenszel W. Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst 1959; 22: 719-748.
[35] Begg CB and Mazumdar M. Operating charac-teristics of a rank correlation test for publica-tion bias. Biometrics 1994; 50: 1088-1101.
[36] Egger M, Davey Smith G, Schneider M and Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997; 315: 629-634.
[37] Brophy VH, Jampsa RL, Clendenning JB, Mc- Kinstry LA, Jarvik GP and Furlong CE. Effects of 5’ regulatory-region polymorphisms on para-oxonase-gene (PON1) expression. Am J Hum Genet 2001; 68: 1428-1436.
[38] Harel M, Aharoni A, Gaidukov L, Brumshtein B, Khersonsky O, Meged R, Dvir H, Ravelli RB, McCarthy A, Toker L, Silman I, Sussman JL and Tawfik DS. Structure and evolution of the se-rum paraoxonase family of detoxifying and an-ti-atherosclerotic enzymes. Nat Struct Mol Biol 2004; 11: 412-419.

PON-1 polymorphisms and polycystic ovary syndrome
1
Table S1. PRISMA checklistSection/topic # Checklist item Reported on page #TITLE
Title 1 Identify the report as a systematic review, meta-analysis, or both. Title page
ABSTRACT
Structured summary 2 Provide a structured summary including, as applicable: background; objectives; data sources; study eligibility criteria, participants, and interventions; study appraisal and synthesis methods; results; limitations; conclu-sions and implications of key findings; systematic review registration number.
Abstract page
INTRODUCTION
Rationale 3 Describe the rationale for the review in the context of what is already known. Introduction section
Objectives 4 Provide an explicit statement of questions being addressed with reference to participants, interventions, comparisons, outcomes, and study design (PICOS).
Introduction section
METHODS
Protocol and registration 5 Indicate if a review protocol exists, if and where it can be accessed (e.g., Web address), and, if available, provide registration information including registration number.
N/A
Eligibility criteria 6 Specify study characteristics (e.g., PICOS, length of follow-up) and report characteristics (e.g., years consid-ered, language, publication status) used as criteria for eligibility, giving rationale.
Materials and methods, 2nd paragraph
Information sources 7 Describe all information sources (e.g., databases with dates of coverage, contact with study authors to identify additional studies) in the search and date last searched.
Materials and methods, 1st paragraph
Search 8 Present full electronic search strategy for at least one database, including any limits used, such that it could be repeated.
Materials and methods, 1st paragraph
Study selection 9 State the process for selecting studies (i.e., screening, eligibility, included in systematic review, and, if ap-plicable, included in the meta-analysis).
Materials and methods, 3th paragraph
Data collection process 10 Describe method of data extraction from reports (e.g., piloted forms, independently, in duplicate) and any processes for obtaining and confirming data from investigators.
Materials and methods, 3th paragraph
Data items 11 List and define all variables for which data were sought (e.g., PICOS, funding sources) and any assumptions and simplifications made.
Materials and methods, 3th paragraph
Risk of bias in individual studies 12 Describe methods used for assessing risk of bias of individual studies (including specification of whether this was done at the study or outcome level), and how this information is to be used in any data synthesis.
Materials and methods, 4th paragraph
Summary measures 13 State the principal summary measures (e.g., risk ratio, difference in means). Materials and methods, 4th paragraph
Synthesis of results 14 Describe the methods of handling data and combining results of studies, if done, including measures of consistency (e.g., I2) for each meta-analysis.
Materials and methods, 4th paragraph
Risk of bias across studies 15 Specify any assessment of risk of bias that may affect the cumulative evidence (e.g., publication bias, selec-tive reporting within studies).
Materials and methods, 4th paragraph
Additional analyses 16 Describe methods of additional analyses (e.g., sensitivity or subgroup analyses, meta-regression), if done, indicating which were pre-specified.
Materials and methods, 4th paragraph
RESULTS
Study selection 17 Give numbers of studies screened, assessed for eligibility, and included in the review, with reasons for exclu-sions at each stage, ideally with a flow diagram.
Figure 1
Study characteristics 18 For each study, present characteristics for which data were extracted (e.g., study size, PICOS, follow-up period) and provide the citations.
Tables 1 and 2
Risk of bias within studies 19 Present data on risk of bias of each study and, if available, any outcome level assessment (see item 12). Results section, Publication Bias; Figures 4 and 5
Results of individual studies 20 For all outcomes considered (benefits or harms), present, for each study: (a) simple summary data for each intervention group (b) effect estimates and confidence intervals, ideally with a forest plot.
Table 3; Figures 2 and 3

PON-1 polymorphisms and polycystic ovary syndrome
2
Synthesis of results 21 Present results of each meta-analysis done, including confidence intervals and measures of consistency. Results section, Quantitative synthesis; Table 3; Figures 2 and 3
Risk of bias across studies 22 Present results of any assessment of risk of bias across studies (see Item 15). Results section, Publication Bias, Figures 4 and 5
Additional analysis 23 Give results of additional analyses, if done (e.g., sensitivity or subgroup analyses, meta-regression [see Item 16]).
N/A
DISCUSSION
Summary of evidence 24 Summarize the main findings including the strength of evidence for each main outcome; consider their relevance to key groups (e.g., healthcare providers, users, and policy makers).
Discussion section, 1st paragraph
Limitations 25 Discuss limitations at study and outcome level (e.g., risk of bias), and at review-level (e.g., incomplete retrieval of identified research, reporting bias).
Discussion section, 5th paragraph
Conclusions 26 Provide a general interpretation of the results in the context of other evidence, and implications for future research.
Discussion section, 6th paragraph
FUNDING
Funding 27 Describe sources of funding for the systematic review and other support (e.g., supply of data); role of funders for the systematic review.
Acknowledgements section