asi kovalam
TRANSCRIPT

Feb 22, Kovalam
GIST
Chandramohan K
RCC


TILL THE PAST DECADE
• Treated them as Leiomyomas or Leiomyosarcomas
• Treated them with RT
• Treated them with conventional chemo
FAILED MISERABLY
LAST DECADE
• Molecular genetics
• Epidemiology
• Management

EPIDEMIOLOGY
• 80 % of GI Sarcoma.
• GIST = 1% to 3% of all malignant GI tumors.
• Annual incidence rate across the world = 10 to 15 cases / million people.
Cassier PA et al Br J Cancer 2010;103(2):165–170




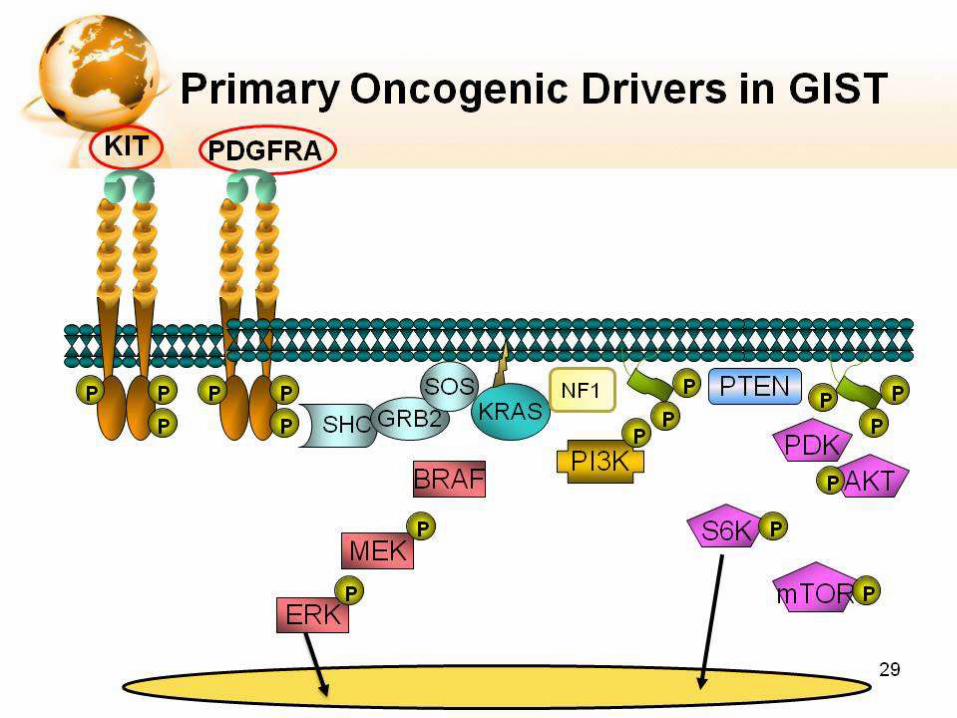
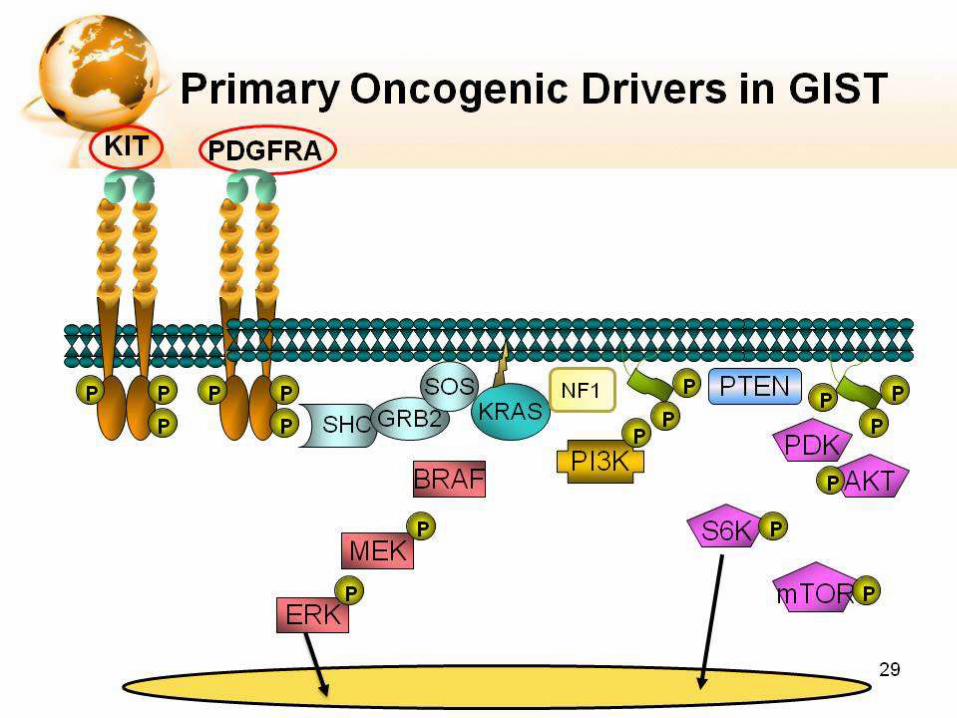
The Development of A Molecular Understanding of GIST
• CD117 antigen a marker for the presence of KIT protein.
• KIT protein is present in nearly 95% of GIST.
• KIT mutations lead to uncontrolled, ligand-independent phosphorylation by the KIT kinase.
Wang L et al. Arch Pathol Lab Med 2000;124:1471.
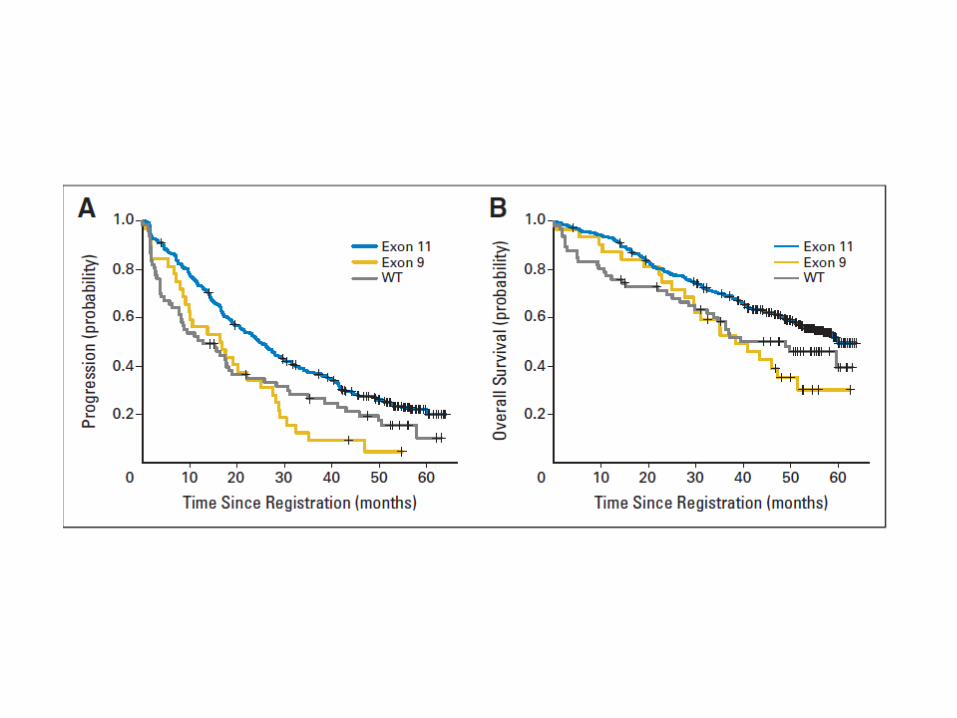
• KIT mutations - 85% of GIST lesions.– 70% of cases in exon 11 of KIT, others are exon 9, 13,
17.
• 10 % have mutation in PDGFR- A.Heinrich MC et al Science 2003;299:708






Principles of surgery
• Mainstay of therapy for patients with primary
non metastatic GIST
• Initial therapy if the tumor is technically
resectable with minimum morbidity or loss of function.

Goals
Complete gross resection
Intact pseudo capsule
Negative microscopic margins
Minimum morbidity

Stomach Wedge resection
Small intestine Segmental resection
Omentum, mesentery en bloc removal
Rectum, oesophagus W/E

prognosis favourable intermediate unfavourable
histology spindle epithelioid Mixed
Size in cm <5 5-10 >10
gender female male
mitosis <3 3 -15 >15
Kit mutation Exon 11
Mis sense
Exon 11
Del / ins
Exon 9, 13

Disease specific survival and tumor size
Ann Surg 231:51-57, 2000




IMMUNOHISTOCHEMICAL MARKERS IN DIAGNOSIS OF GIST
• KIT MUTATION
• PDGFRA MUTATION
• ADDITIONAL MARKERS
• CD-34
• H-Caldesmon
• SMA
• EMERGING MARKERS:-DOG1(Discovered On GIST).DOG 1 IN D/D of GIST
• PKC-THETA

Emerging Marker: PKCθ
PKCθ, protein kinase C theta.
Images reproduced with permission from Blay P et al. Clin Cancer Res. 2004;10:4089-4095.
1. Blay P et al. Clin Cancer Res. 2004;10:4089-4095.
2. Motegi A et al. Pathol Int. 2005;55:106-112.
3. Duensing A et al. Cancer Res. 2004;64:5127-5131.
GIST
×10
KIT PKCθ
5% of GIST lack detectable KIT expression 85% to 100% of GIST stain positive for PKCθ1,2
Other similar mesenchymal neoplasias do not stain positive for PKCθ3

Emerging Marker: DOG1
*DOG1.1 antibody was used to detect DOG1; DOG1, discovered on GIST-1; Images reproduced with permission from Espinosa I et al. Am J Surg Pathol. 2008;32:210-218.
Espinosa I et al. Am J Surg Pathol. 2008;32:210-218.
87% of GIST stain positive for DOG1 Other similar mesenchymal neoplasms do not stain positive for DOG1
DOG1 and KIT show similar staining patterns consistent with ICC staining in the small bowel
DOG1.1* KIT



PROGNOSTIC FACTORS OF GIST
• TUMOR SIZE
• MITOTIC RATE
• LOCATION OF PRIMARY TUMOR
• COMPLETENESS OF RESECTION
• TUMOR RUPTURE
• CELLULAR PROLLIFERATION INDEX
• DIFFUSE MUCOSAL INVASION
• ANEUPLOIDY
• TELOMERASE EXPRESSION
• EXTENT OF DISEASE

Modality of Rx
Operable = Operate
Non operable = TKI

SURGERY
• R0 resection
• No routine lymphadenectomy
• No tumour rupture or spillage
• Peritoneum & Liver carefully examined
• LAP safe in low risk and localised

Influence of Tumour Rupture on Recurrence Free Survival
No rupture
Rupture
Pro
ba
bil
ity
of
rela
ps
e-f
ree
su
rviv
al p=0.00001
Time [years]
Rutkowski et al. EJSO 2011 Jul 5 [Epub ahead of print].
Are Any GIST Benign?
• Surgery is the principal treatment and only curative therapy for localised, resectable primary disease
• All lesions ≥ 2 cm should be resected
• In the past, lesions < 2 cm have been followed (often by endoscopy) rather than resected
• Rationale for observation now called into question
– All GIST have malignant potential
– tumours < 2 cm and < 5 mitoses / 50 HPF may have low risk of
recurrence, but it is IMPOSSIBLE to assess mitotic rate on small
endoscopic biopsy samples
Casali et al. Ann Oncol 2008;19 (suppl 2):ii35–ii38.
Demetri et al. J Natl Compr Canc Netw. 2007;5 (suppl 2):S1-29.34

GIST Recurrence After Surgery
• Recurrence of moderate to high-risk GIST following surgery is common
– Majority of high-risk patients experience recurrence
– Median time to recurrence for those who recur is 2 years
• Five-year survival rates of primary GIST patients before Imatinib era was approximately 30–60%
• Recurrent disease should be treated as metastatic disease
DeMatteo et al. Hum Pathol. 2002;33:466-477.
Pierie et al. Arch Surg. 2001;136:383-389.
Rossi et al. Int J Cancer. 2003;107:171-176.
DeMatteo et al. Ann Surg. 2000;231:51-58.
Ng et al. Cancer. 1992;69:1334-1341.35
Management of Metastatic, Unresectable, or Recurrent GIST: The Paradigm Changes for Advanced Disease
• Failure of Traditional Systemic and Locoregional CytotoxicChemotherapy.
• Rates of objective antitumor response to a variety of chemotherapy agents for patients with GIST in the range of 0% to, at best, less than 5%. Goss GA et al. Proc Am Soc Clin Oncol 2000;19 .
• RT rarely plays any role in the management of patients with metastatic GIST.
• Multifocal hepatic metastases or multiple sites of intra-abdominal metastatic disease- Role of Sx dismal.

• What to use ?
• Why to use ?
• When to use ?
• Till when to use ?
• What next to use ?

This TKI…. active in Lab
Addition of imatinib to GIST cells in culture rapidly and completely blocked the constitutive activation of KIT, arrested cell proliferation, and induced apoptosis in the tumor cells.
Tuveson DA et al Oncogene 2001;20:5054.



Case report to clinical practice
• single-patient pilot study in Helsinki, Finland, with close intellectual collaboration from U.S.-based investigators.
• Treatment with four 100-mg capsules of STI571 once daily was started in March 2000.


Summary of Clinical Studies of Imatinib Mesylate in Patients with Metastatic or Unresectable Gastrointestinal Stromal Tumors (GISTs)
Study (Ref.) N Imatinib Dosage (mg) Results
Joensuu et al., 2001 (74) 1 400 daily Major response, durable for more than 2 y
van Oosterom et al., 2001 (75) 40 (36 GIST) 400 to 1,000 daily Partial remissions in 19/36 (53%) GIST patients
with additional minor responses in 6/36 (17%)
Total clinical benefit rate = 70%
No responses in non-GIST patients
Demetri et al., 2002 (61) 147 400 or 600 daily Partial remissions in 97/147 (66%) with additional
minor responses and durable stable disease in
25/147 (17%)
Total clinical benefit rate 83%, no differences for
different doses
Verweij et al., 2003 (76) 51 (27 GIST) 800 daily Complete remissions in 4%, partial remissions in
67%, with additional minor responses and durable
stable disease in 18%
Total clinical benefit rate 89%
Verweij et al., 2003 (87) 946 400 or 800 daily Complete remissions in 5%, partial remissions in
45%, with additional minor responses and durable
stable disease in 32%
Total clinical benefit rate 82%, no differences for
different doses
Blanke et al., 2008 (86) 746 400 or 800 daily Complete remissions in 2%, partial remissions in
46%, with additional minor responses and durable
stable disease in 26%
Total clinical benefit rate 74%, no differences for
different doses


Feb 22, Kovalam
Optimal dose….


Median f/u- 4.5yrs.PFS -18MNTH—400mg/dy
20mnth---800mg/dy.OS
55 mnth—400mg/day51 mnth—800mg/dy






Both ESMO and NCCN guidelines recommend that patients with exon 9 mutations should be treated with 800mg/day imatinib

Feb 22, Kovalam
Duration of imatinib……..



® at 1 yr
Randomised at 3 years
Randomised at 1 year(Blay et al, JCO 2007)
Randomised at 3 years(Le Cesne et al, Lancet Oncol 2010)
Discontinue Imatinib?
Randomised at 1 year
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 6 12 18 24 30 36 42 48 54 60 66 72 78 84 90 96
Months
Surv
ival
pro
bab
ility
CONT group
19 evts / 26 patients
1-year PFS: 85%
Median PFS : 29 months ; CI95 = [18 - 41]
STOP group
29 evts / 32 patients
1-year PFS: 28%
Median PFS : 7 months ; CI95 = [3 - 9]
Log-rank P value < 0.0001
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 6 12 18 24 30 36 42 48 54 60 66 72
Months
Surv
ival
pro
bab
ility
CONT group
9 evts / 25 patients
1-year PFS: 92% ; CI95 = [72 - 98]
2-years PFS: 80% ; CI95 = [58 - 91]
STOP group
21 evts / 25 patients
1-year PFS: 32% ; CI95 = [15 - 50]
2-years PFS: 16% ; CI95 = [5 - 33]
Log-rank P value < 0.0001

Randomised at 5 years(Le Cesne et al. ASCO 2011, abstract 10015)
Treatment should be continued indefinitely, since treatment interruption is generally
followed by relatively rapid tumour progression in virtually all cases (Casali et al, ESMO
guidelines, Annals of Oncology 2010)
Randomization at 10 yrs? (ongoing BFR14 amendment)
BFR14: Imatinib Discontinuation Randomization at 5 yrs
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 6 12 18 24 30 36
Months
Surv
ival
pro
bab
ility
CONT group
0 evts / 13 patients
1-year PFS: 100%
STOP group
7 evts / 14 patients
1-year PFS: 65% ; CI95 = [31 - 85]
Log-rank P value = 0.0056

BFR14
(i) Interruption of imatinib after 1, 3, or 5 years of treatment in patients with nonprogressive GIST was associated with a high risk of progression even in patients with a complete response.
(ii) Rechallenge with imatinib restored tumor control in most patients, but the tumor response seldom reached that before treatment interruption.
(iii) Patients receiving continuous imatinib had a high rate of prolonged tumor control, which increased with longer imatinib treatment.

Post OP Imatinib
• Complete resection possible in 85% of pts with primary GIST but approx 50% will develop mets or recurrence.
• Even in R0 resection look for Risk scoring.


Very low risk Low risk Intermediate risk High risk
NIH consensus
criteria1
<2 cm and <5 mitotic
index
2−5 cm and <5 mitotic
index
5−10 cm and <5 mitotic
index or
<5 cm and 6−10 mitotic
index
>5 cm and >5 mitotic
index or
>10 cm and any
mitotic index or
any size and >10
mitotic index
Modified NIH
consensus
classification2
Any location: <2 cm
and 5 mitotic index
Any location: 2.1−5 cm
and 5 mitotic index
Gastric: 2.1−5 cm and
>5 mitotic index or
5.1−10 cm and 5
mitotic index
Any location: <5 cm
and 6−10 mitotic index
Any location: Tumor
rupture, or >10 cm, or
>10 mitotic index, or
>5 cm and >5 mitotic
index
Non-gastric: 2.1−5
cm and >5 mitotic
index, or 5.1−10 cm
and 5 mitotic index
Mitotic index, number of mitoses per 50 high-power fields. RFS, recurrence-free survival1. Fletcher CD et al. Hum Pathol 2002;33:459-465. 2. Miettinen M et al. Arch Pathol Lab Med 2006;130:1466-1478. 3. Joensuu H. Hum Pathol 2008;39:1411-1419.
Risk Classification Systems
Mitotic index, number of mitoses per 50 high-power fields. RFS, recurrence-free survival1. Fletcher CD et al. Hum Pathol 2002;33:459-465. 2. Joensuu H. Hum Pathol 2008;39:1411-1419.




3-6 cm
6-10 cm
> 10cm

Duration of post OP imatinib


36 months of imatinib
12 months of imatinib
Number at risk
36 months of imatinib 198 184 173 133 82 39 8 0
12 months of imatinib 199 177 137 88 49 27 10 0
Re
curr
en
ce-f
ree
an
d a
live
(%
)100
60·1%
47·9%
86·6%
65·6%
Hazard ratio 0·46 (95% CI 0·32-0·65)
p<0·0001
Years since randomisation
0 1 2 3 4 5 6 70
20
40
60
80

36 months of imatinib
12 months of imatinibAliv
e (
%)
96·3%
Number at risk
36 months of imatinib 198 192 184 152 100 56 13 0
12 Months of imatinib 199 188 176 140 87 46 20 0
Years since randomisation
Hazard ratio 0·45 (95% CI 0·22-0·89)
p=0·019
92·0%
94·0%
81·7%
0 1 2 3 4 5 6 7
0
20
40
60
80
100

Risk Assessment

Algorithm: Management of Unresectableor Metastatic GIST1–3
CR, complete response; PR, partial response; RFA, radiofrequency ablation; SD, stable disease; TKI, tyrosine kinase inhibitor.
1. Reichardt P. EJC Suppl. 2006;4(suppl 1):19-26.
2. National Comprehensive Cancer Network. Clinical Practice Guidelines. Soft tissue Sarcoma. V.2.2011.
http://www.nccn.org/professionals/physician_gls/f_guidelines.asp.
3. Casali P et al. Ann Oncol 2010: 21:v98-v102.
Progression
Progression
Metastatic
KIT exon 9+
Imatinib 800 mg/d
Dose-escalate
Imatinib 800 mg/d
Metastatic
Imatinib 400 mg/d
Unresectable
Imatinib 400 mg/d
CR, PR, or SD
Secondary surgery
Continue imatinib
CR or SD
Continue imatinib
CR, PR, or SD
Continue imatinib
• Continue imatinib at same dose or
• Increase imatinib dose as tolerated or
• Switch to sunitinib
• Consider surgery, RFA
• Increase imatinib dose as tolerated or
• Change to sunitinib
• Consider clinical trial
Limited/Local Generalized/Systemic
73

Suggested Treatment Algorithm for GIST Patients Who Experience Progression on Imatinib
*May not be available in all countries
Patel S. Cancer Treat Rev 2011.

Feb 22, Kovalam
Imatinib in Neo-adjuvant setting


• After maximal response (usually occurring within 4 to 6 months), definitive surgery could be performed.
• Marginally resectable or resectable with high risk of morbidity.
• Imatinib to be started soon after surgery irrespective of surgical margins.

Adverse effect of Imatinab
Adverse effects of Imatinib are generally mild (grade 1 or 2).
– Edema - approx 74% ; especially notable in the loose subcutaneous tissues of
the facial periorbital region),
– Diarrhea - 45%,
– Myalgia or musculoskeletal pain - 40%,
– Skin rashes -30%,
– Headache -25%.– Myelotoxicity is markedly less common in GIST patients than in
patients with CML.

Feb 22, Kovalam
What next when Imatinabfails……



• In stratum 1-
– stable disease -36%
– progressive disease -54%
• In stratum 2-
– partial response- 2%,
– stable disease - 43% SD,
– progressive disease - 32%.

Phase III GRID Trial
(GIST – Regorafenib In Progressive Disease)
Phase III Data on Bayer’s Regorafenib Met Primary Endpoint Showing Significant Improvement in Progression-Free Survival in Patients with GIST.
• INCLUSION criteria: Pt whose disease progressed despite prior treatment with imatinib and sunitinib.
• Patients were randomized in a 2:1 ratio to receive either regorafenib (160 mg once daily, three weeks on/ one week off) plus best supportive care (BSC) or placebo plus BSC to evaluate efficacy and safety
• The GRID study met its primary endpoint of improvement in progression-free survival (PFS) (HR=0.27, p<0.0001).
• The median PFS was 4.8 months in the regorafenib arm versus 0.9 months in the placebo arm.

Mutation Type Likely Influences Efficacy of Adjuvant Therapy
• PDGFRA mutation D842V is considered imatinib resistant– Frequency, 8.7% of the tumours in SSGXVIII
• KIT exon 9 mutation may require 800 mg/d dose1
– Frequency, 7.1% of the tumours in SSGXVIII
• Wt GIST (9.0% in SSGXVII) – Many may not be imatinib sensitive (NF1 or Carney/Carney-Stratakis
syndrome-associated GIST); succinate dehydrogenase (SDHA, SDHB, SDHC) mutations2,3 ?
1.GIST Meta-Analysis Group (MetaGIST). J Clin Oncol. 2010;28(7):1247-1253.
2.Janeway KA et al. PNAS 2011;108:314-8.
3.Pantaleo MA et al. JNCI 2011;103:1-5.84

FUTURE
• TAILORED THERAPY ( PDGFRA D842 mutation)
• Blood level testing of imatinib
• Intermediate risk group
• Adjuvant ? 3 yrs
• Other drives and other inhibitors


History , physical examination
Abdominal/pelvic CT
with contrast, and/or MRI
Chest imaging
Endoscopic ultrasound
Endoscopy as indicated
FDG PET in indicated cases

Localized or potentially resectable disease
Resect
Pathologyandriskassessment
Negative microscopic
margins
Positive Microscopic
margins
Gross residual d/s
DocumentedGIST

Negative microscopic margins
Adjuvant Imatinib
At least 12 monthsDeMatteo et al. Adjuvant imatinib mesylate increases recurrence free survival in patients with completely resected localized primary gastrointestinal stromal tumor (GIST): North American Intergroup Phase III trial ACOSOG Z9001. 2007 ASCO
optimal duration has not yet been determined.
Observe

ACOSOG Z9001 (american college of surgeons oncology group)
Follow-up of 1.2 yearsEnd point Recurrence
At 1.2 yrs 21% of the expected events had occurredRFS
Imatinib - 91% Placebo - 83%
OS - Same
Subset analysis ( high risk group )RFS
Imatinib - 96%Placebo - 67-86%

Management not well defined
No evidence for re-excision.
OptionsRe-excision,
Watchful waiting, ? Adjuvant imatinib.
Positive Microscopic Margin

Gross residual d/s
ImatinibConsiderReresection
NED
Persistentgross disease
imatinib

Function sparing
Marginally resectable
Technically resectable, but considerable morbidity
Neo adjuvant Imatinib
BaselineCT ± MRIConsiderPET
neo adjuvant Imatinib

Imatinib
Assess therapeutic effect
No Progression
Continue imatinib
Consider resection
Unresectable or Metastatic disease

Unresectable or Metastatic disease
On Rx with TKI Response, stable d/s
Limited – 1 or more (limited) foci of progression
Generalised – diffuse, multiple foci of progressionsystemic d/s
progression