article - guidelines for flapless surgeryelectrosurgery.com/pdf/publications/dental/guidelines for...
TRANSCRIPT

B
Soaptivdiatiofortooraeratheturisowiadthatainiqprochpla
pu
*SurDeDav
Floant© 2
027
doi
F1
AQ: 1
ASIC AND PATIENT-ORIENTED RESEARCH
J Oral Maxillofac Surgxx:xxx, 2007
Guidelines for Flapless SurgeryAnthony G. Sclar, DMD*
With the introduction o� n-of�ce cone beam computed tomography (CT), improved access to conven-tional CT scanning, and dental implant treatment planning software allowing on-the-spot 3-dimensionalevaluations of potential implant sites, the use of “�apless” implant surgery has gained popularity amongsurgeons. Although the �apless approach was initially suggested for and embraced by novice implantsurgeons, the successful use of this approach often requires advanced clinical experience and surgicaljudgment. This article reviews the advantages and disadvantages of and indications and contraindicationsfor �apless dental implant surgery, with special emphasis on requirements for establishing or maintaininglong-term health and stability of the peri-implant soft tissues. Prerequisites for surgeons wishing to usethe �apless tissue punch approach in dental implant surgery are outlined and put into perspectiverelative to conventional open-�ap surgery techniques and other minimally invasive procedures currentlyused in implant surgery. Procedures for single- and multiple-tooth applications are illustrated.© 2007 American Association of Oral and Maxillofacial Surgeons
ARTICLE IN PRESS
J Oral Maxillofac Surg xx:xxx, 2007
tioplaofforamsuaccabapnoapan
adtisdeanresaftofanforexincplatopcemolatofaro
F2
me of the earliest applications of the “�apless”proach in dental implant surgery involved innova-e site preservation techniques developed for imme-te or delayed implant placement after tooth extrac-n in areas of high esthetic concern. The rationalethe �apless approach in these case scenarios wasisolate the implant and/or grafted socket from thel cavity obtaining an inclusive guided bone regen-tion e�ect while preserving circulation and es-tic soft tissue contours. 1 This was a radical depar-e from the then strongly supported concept oflating implants placed into fresh extraction socketsth a barrier membrane and primary �ap closure. 2 Indition, mounting clinical experience demonstratedt esthetic hard tissue contours were also main-ned by using minimally traumatic extraction tech-ues and substitution bone graft materials. This ap-ach yielded predictable results even in the mostallenging case scenarios with multiple contiguous im-nts placed in areas of high esthetic concern ( Fig 1).With the introduction of-in of�ce cone beam com-ted tomography (CT), improved access to conven-
Director of Clinical Research and Postgraduate Dental Implantgery, Department of Oral and Maxillofacial Surgery, College ofntal Medicine, Nova Southeastern University, Fort Lauderdale-ie, FL.Address correspondence and reprint requests to Dr. Sclar: Southrida OMS, 7600 Red Road, Suite 101, Miami, FL 33143; e-mail:[email protected] American Association of Oral and Maxillofacial Surgeons
8-2391/07/xx0x-0$32.00/0
ge:10.1016/j.joms.2007.03.017
1
nal CT scanning, and new dental implant treatmentnning software allowing 3-dimensional evaluationpotential implant sites, the use of �apless surgeryimplant placement has been gaining popularityong implant surgeons. In its simplest form, �aplessrgery involves using a tissue punch device to gainess to the alveolar ridge for implant placement orutment connection (Fig 2). Although the �aplessproach was initially suggested for and embraced byvice implant surgeons, the successful use of thisproach often requires advanced clinical experienced surgical judgment.Although �apless implant surgery has numerousvantages, including preservation of circulation, softsue architecture, and hard tissue volume at the site;creased surgical time; improved patient comfort;d accelerated recuperation, allowing the patient toume normal oral hygiene procedures immediatelyer, the approach does have some drawbacks. Somethese include the surgeon’s inability to visualizeatomic landmarks and vital structures, the potentialthermal damage secondary to reduced access for
ternal irrigation during osteotomy preparation, thereased risk of malposed angle or depth o� mplantcement, a decreased ability to contour osseousography when needed to facilitate restorative pro-dures and to optimize soft tissue contours, and,st importantly, the surgeon’s inability to manipu-e soft tissues to ensure circumferential adaptationadequate dimensions of keratinized gingival tissuesund emerging implant structures.As such, there are certain prerequisites for sur-
ons wishing to use the �apless approach for im-
FIG sdem dimp alfac
An
2 GUIDELINES FOR FLAPLESS SURGERY
COLOR
ARTICLE IN PRESS
UNCORRECTE
D PROOF
URE 1. Replacement o ailing maxillary incisors with multiple adjacent implants using a s approach.A and B , Preoperative radiographonstrating maxillary incisors with unfavorable root morphology and moderate horizontal bone loss.C , Three adjacent 1-piece nonsubmergelants (Straumann USA, Andover, MA) were placed with the Bio-Col ridge preservation technique immediately after s tooth removilitated by the use of periotomes.D andE, Postoperative radiographs documenting ideal placement of 3 adjacent implants and the lack of
t surgical and restorative dimension to allow placement of a fourth implant. (Figure 1 continued on next page.)
thony G. Sklar. Guidelines for Flapless Surgery. J Oral Maxillofac Surg 2007.
plainc
thimknniqqutisthmvia
dis
m
binimpeanwiingim
FIG byEst eadyforcirc
An rg 2007
ANTHONY G. SKLAR 3
COLOR
ARTICLE IN PRESS
nt placement and uncovering procedures. Theselude in-depth knowledge of the criteria for optimalp designs used in dental implant surgery, as well ase clinical goals for surgical management of peri-plant soft tissues. The surgeon should also beowledgeable regarding the indications and tech-ues (soft tissue surgical maneuvers) commonly re-ired for successful management of peri-implant softsues during conventional open p surgery. Finally,e surgeon should be familiar with other availableinimally invasive techniques that incorporate abbre-
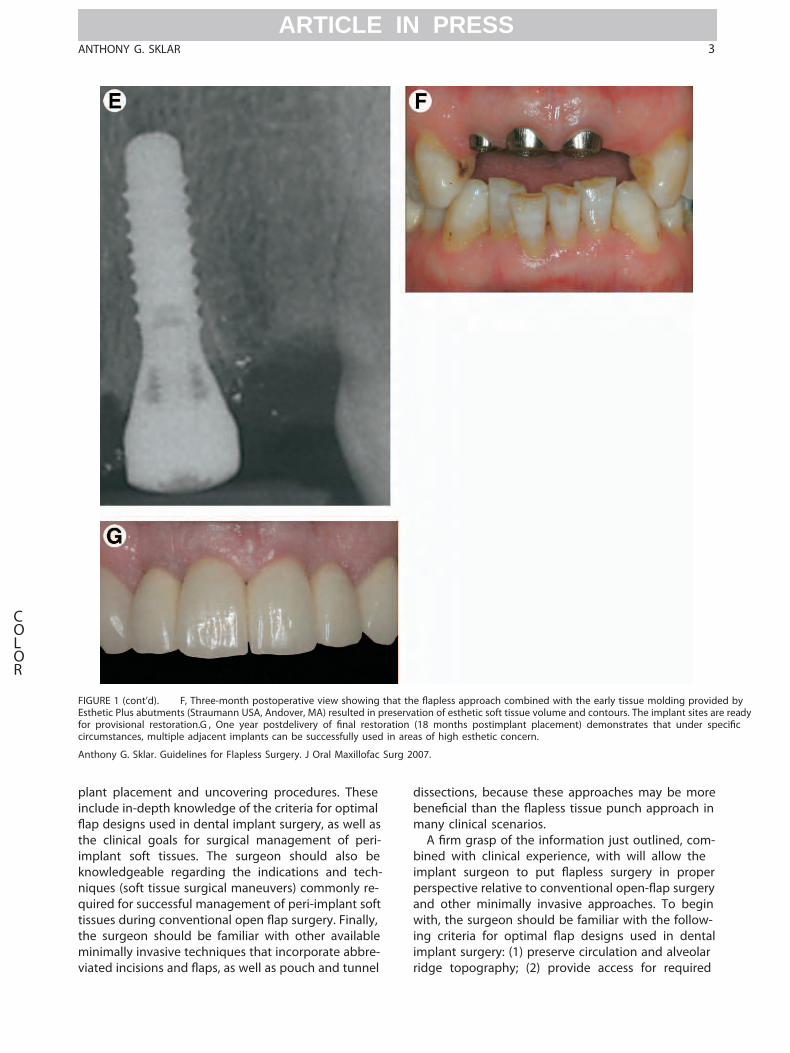
URE 1 (cont’d). F, Three-month postoperative view showing thahetic Plus abutments (Straumann USA, Andover, MA) resulted in preprovisional restoration.G , One year postdelivery of l restoratumstances, multiple adjacent implants can be successfully used in
thony G. Sklar. Guidelines for Flapless Surgery. J Oral Maxillofac Su
ted incisions and , as well as pouch and tunnel rid
sections, because these approaches may be morel than the s tissue punch approach in
any clinical scenarios.A m grasp of the information just outlined, com-ed with clinical experience, with will allow theplant surgeon to put s surgery in properrspective relative to conventional p surgeryd other minimally invasive approaches. To beginth, the surgeon should be familiar with the follow-criteria for optimal p designs used in dental
plant surgery: (1) preserve circulation and alveolar
s approach combined with the early tissue molding providedn of esthetic soft tissue volume and contours. The implant sites are rmonths postimplant placement) demonstrates that under
of high esthetic concern.
.
t theservatioion (18areas
ge topography; (2) provide access for required

imvitseocat�xmitat(8)goturcatbubeproancalmoanadsiomepro
clinofsuap(wizethevidnemeri�Alttherougretisprocogiepreby
recintioingtistiscattwadtheenqusiotorcreunidewiFinthestrenhacesuapsu
tone(sosu
FIGhelrotareabl
Anlofa
4 GUIDELINES FOR FLAPLESS SURGERY
COLOR
ARTICLE IN PRESS
plant instrumentation; (3) allow identi�cation ofal structures; (4) provide access for modifying os-us contours and/or local bone harvest when indi-ed; (5) provide for closure away from submergedture installation or augmentation sites; (6) mini-ze postsurgical bacterial contamination; (7) facili-e �ap elevation, retraction, and wound closure; andaid in achieving circumferential adaptation of
od-quality tissues around emerging implant struc-es.3 Although Brånemark et al4 originally advo-ed using �aps incorporating vestibular incisions,ccal �aps initiated with pericrestal incisions haveen shown to provide a practical and e�ective ap-ach to implant placement, abutment connection,d ancillary grafting procedures. 3 Typically, the buc -�ap is outlined by a pericrestal incision and 1 orre vertical releasing incisions located at the mesiald distal extent of the site. The surgeon simplyjusts the position and bevel of the pericrestal inci-n to accommodate for submerged or nonsub-rged implant placement and abutment connection
URE 2. Tissue punch devices for �apless implant surgery. Hand-d punch (Uni-Punch; Premier Medical, King of Prussia, PA) andary tissue punch (Salvin Dental Specialties, Charlotte, NC) devicesavailable in multiple diameters corresponding to commonly avail-e implant diameters.
thony G. Sklar. Guidelines for Flapless Surgery. J Oral Maxil-c Surg 2007.
cedures. Wh
The implant surgeon also must be familiar with theical goals and guidelines for surgical managementperi-implant soft tissues. The clinical goal of thisrgical management is to establish an adequate zone,proximately 3.0 mm in apicocoronal dimensionidth), of attached nonmobile, preferably keratin-d, soft tissue that is circumferentially adapted totransmucosal implant structures. 3 Doing so pro-
es the epithelial and connective tissue elementseded for soft tissue integration and the develop-nt of circumferential biological width without sac-cing the underlying peri-implant supporting bone. 5
hough long-term success is possible with less thanrecommended 3.0 mm of keratinized tissue sur-nding an implant restoration, predictability is farater with the recommended amount, because thesues are better able to withstand the trauma ofsthetic procedures, abutment connection, and re-nnection; the forces of mastication and oral hy-ne maintenance; and the mechanical challengessented by removable implant prosthesis securedresilient prosthetic attachments.Nevertheless, it is also important for the surgeon toognize that tissue thickness plays a signi�cant rolesurgical decision making with regard to the selec-n of appropriate soft tissue surgical maneuvers dur-implant surgery and determination of when soft
sue augmentation is needed to prevent progressivesue recession. Long-term clinical observations indi-e that ideal tissues thickness is somewhere be-een 2.5 and 3.0 mm, and that the presence ofequate soft tissue thickness greatly contributes tomaintenance of a stable peri-implant soft tissue
vironment. In addition, the combination of ade-ate soft tissue thickness and apicocoronal dimen-n of keratinized tissue surrounding an implant res-ation helps resist recession, protects peri-implantstal bone levels, and provides esthetic masking ofderlying metal components. Furthermore, at theal tissue thickness, a reduction in the apicocoronaldth of keratinized tissue may become acceptable.ally, in areas of high esthetic concern, along withobjectives outlined earlier, preservation or recon-
uction of esthetic soft tissue contours is required tosure that the peri-implant gingival tissues are inrmony with the soft tissues surrounding the adja-nt natural dentition in terms o� orm, color, andrface texture. In many cases, this requires greatericocoronal dimensions of keratinized gingival tis-es than recommended earlier.Another prerequisite for implant surgeons desiringperform �apless implant surgery includes aware-ss of the indications and the surgical techniqueft tissue surgical maneuvers) commonly used forccessful management of peri-implant tissues.3
en placing a nonsubmerged implant or performing

abmasiokeemdimingselpacir
ofpla
whgivimsutoanpeanNeadthesectat
dekeadniqsu
TS
WiGBu
Anlofa
FIGthe ng the�ap tto allyadj din t
An
ANTHONY G. SKLAR 5
COLOR
T1
F3
ARTICLE IN PRESS
utment connection to a submerged implant, opti-l �ap design dictates locating the pericrestal inci-n such that approximately 3.0 mm of good-qualityratinized tissue remains on the oral aspect of theerging implant structures. Then the apicocoronalension (width) of the keratinized gingival remain-on the elevated buccal �ap guides the surgeon in
ecting the appropriate surgical maneuver for thatrticular site, keeping in mind the need to obtain acumferential adaptation of approximately 3.0 mm
able 1. GUIDELINES FOR SELECTING SOFT TISSUEURGICAL MANEUVERS
dth of Keratinizedingiva Present onccal Flap Margin Indicated Surgical Maneuver
5 to 6 mm Resective contouring4 to 5 mm Papilla regeneration (Palacci)3 to 4 mm Lateral �ap advancement
thony G. Sklar. Guidelines for Flapless Surgery. J Oral Maxil-c Surg 2007.
URE 3. Resective contouring.A, When apicocoronal dimension oresective contouring maneuver is used to obtain circumferential ti, tissue is taken from the top of the ridge and moved in a buccal direthe emerging implant neck, after which the tissue is adapted arouacent to each implant site.C, The contoured �ap is then apically rehe interimplant areas. (Reprinted with permission.3)
thony G. Sklar. Guidelines for Flapless Surgery. J Oral Maxillofac Surg 2007
keratinized tissue surrounding the emerging im-nt (Table 1).Resective contouring (gingivectomy) is indicateden the apicocoronal dimension of keratinized gin-al remaining on the buccal �ap adjacent to theplant site is 5 to 6 mm (Fig 3). Typically, thergeon begins by passively aligning the �ap adjacentimplant abutment at one end of the surgical sited uses a low-pro�le scalpel (eg, a 15c blade) torform the resection. The �ap is then secured mesiald distal to that abutment with interrupted sutures.xt the surgeon evaluates the width of tissue at thejacent sites and, i� ndicated, sequentially performsresective contouring maneuver at each site andures the �ap to obtain circumferential tissue adap-ion around the remaining abutments (Figs 3B,C).The papilla regeneration technique, as originallyscribed by Palacci, 6 is indicated when 4 to 5 mm ofratinized tissue remains on the buccal �ap marginjacent to the implant site in question. This tech-ue is very useful for obtaining circumferential clo-re of good-quality tissue around the emerging im-
ized tissue remaining on the buccal �ap is between 5 and 6 mm,sure around the emerging implant neck or abutment. After outlini, A 15c scalpel is used to precisely perform the gingivectomy adjacenabutment and, if appropriate, the resection is repeated sequentied and secured around each emerging implant with sutures place
f keratinssue cloction.Bnd theposition
.
plaalswhspfasgeabgin
the4Bintthecau
mawifromutiosu
secinsitthrproKethrmearosittistosioce
tis3
tisterimeq
FIGthe iningthe tedin t iverot ntialtiss
An rg 2007
6 GUIDELINES FOR FLAPLESS SURGERY
F4
F5
COLOR
ARTICLE IN PRESS
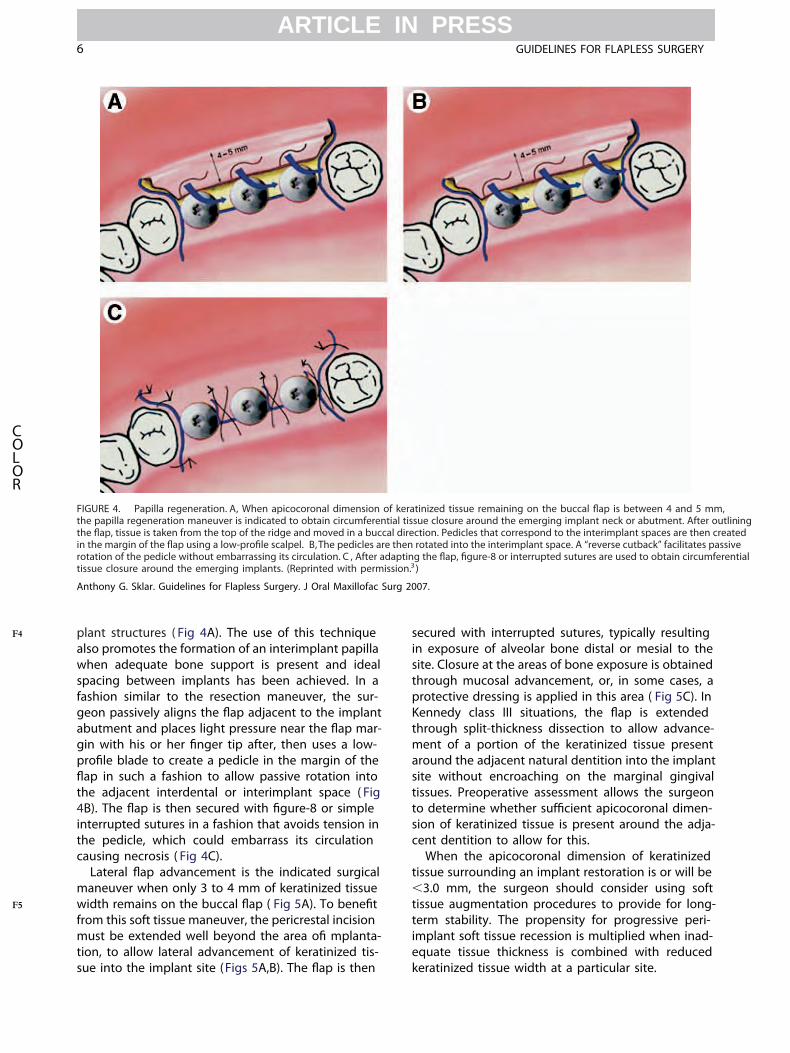
nt structures ( Fig 4A). The use of this techniqueo promotes the formation of an interimplant papillaen adequate bone support is present and idealacing between implants has been achieved. In ahion similar to the resection maneuver, the sur-on passively aligns the p adjacent to the implantutment and places light pressure near the p mar-with his or her r tip after, then uses a low-e blade to create a pedicle in the margin of the
p in such a fashion to allow passive rotation intoadjacent interdental or interimplant space ( Fig
). The p is then secured with 8 or simpleerrupted sutures in a fashion that avoids tension inpedicle, which could embarrass its circulationsing necrosis ( Fig 4C).Lateral p advancement is the indicated surgicalneuver when only 3 to 4 mm of keratinized tissuedth remains on the buccal p ( Fig 5A). Tom this soft tissue maneuver, the pericrestal incisionst be extended well beyond the area o mplanta-n, to allow lateral advancement of keratinized tis-
URE 4. Papilla regeneration. A, When apicocoronal dimension ofpapilla regeneration maneuver is indicated to obtain circumferenti
, tissue is taken from the top of the ridge and moved in a buccalhe margin of the p using a e scalpel. B,The pedicles areation of the pedicle without embarrassing its circulation. C , After adaue closure around the emerging implants. (Reprinted with permiss
thony G. Sklar. Guidelines for Flapless Surgery. J Oral Maxillofac Su
e into the implant site (Figs 5A,B). The p is then ke
ured with interrupted sutures, typically resultingexposure of alveolar bone distal or mesial to thee. Closure at the areas of bone exposure is obtainedough mucosal advancement, or, in some cases, atective dressing is applied in this area ( Fig 5C). Innnedy class III situations, the p is extendedough split-thickness dissection to allow advance-nt of a portion of the keratinized tissue presentund the adjacent natural dentition into the implante without encroaching on the marginal gingivalsues. Preoperative assessment allows the surgeondetermine whether t apicocoronal dimen-n of keratinized tissue is present around the adja-nt dentition to allow for this.When the apicocoronal dimension of keratinizedsue surrounding an implant restoration is or will be.0 mm, the surgeon should consider using softsue augmentation procedures to provide for long-m stability. The propensity for progressive peri-plant soft tissue recession is multiplied when inad-uate tissue thickness is combined with reduced
ized tissue remaining on the buccal p is between 4 and 5 mm,closure around the emerging implant neck or abutment. After outl
on. Pedicles that correspond to the interimplant spaces are then creatated into the interimplant space. A “reverse cutback” facilitates passhe , 8 or interrupted sutures are used to obtain circumfere
.
keratinal tissuedirectithen ropting tion.3)
ratinized tissue width at a particular site.

icasuthemiex
orcoproanusancoinvgemamaeraintge
matiovelatpre
linthe
theoudialusgradetreosofforsh
FIG4 m plantenv lantcom ed ina b s,the izedtiss
An rg 2007
ANTHONY G. SKLAR 7
F6
F7-8
F9
COLOR
ARTICLE IN PRESS
Along with having in-depth knowledge of the clin-l goals, guidelines, and surgical techniques used forccessful management of peri-implant soft tissues,implant surgeon also should be familiar with other
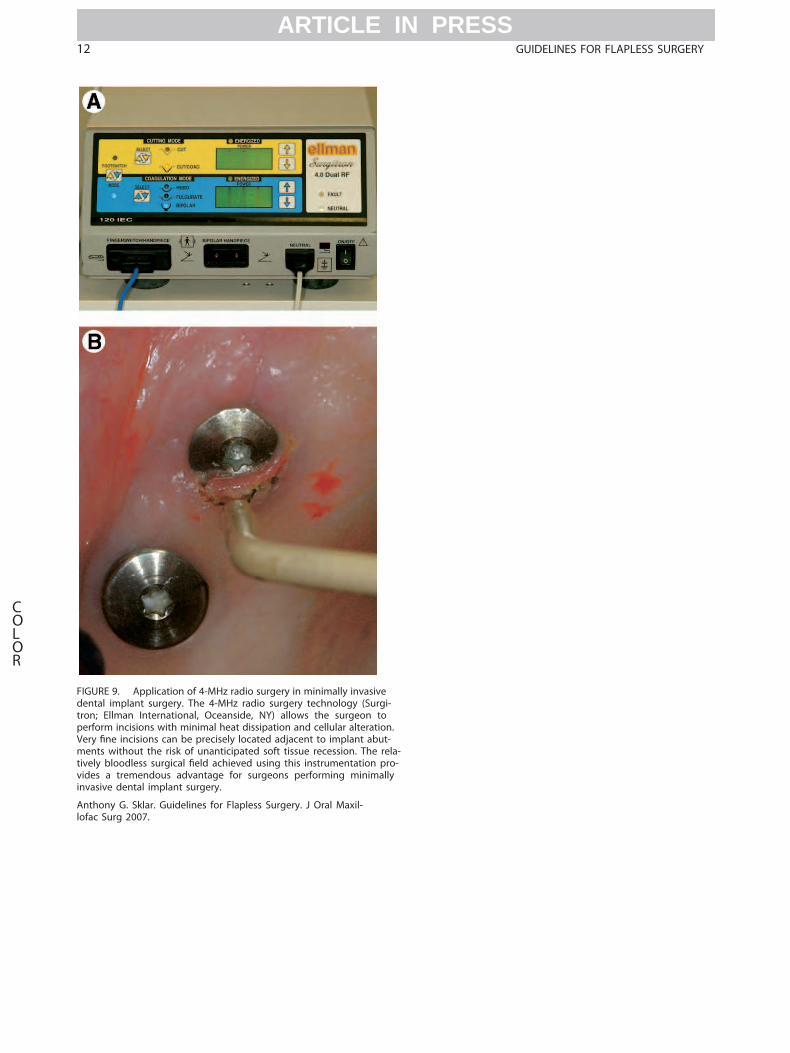
nimally invasive approaches for implant placement,posure, and grafting, such as U-shaped peninsulas (Fig 6), abbreviated trapezoidal , and pouchtunnel dissections, which can have advantagesmparable to those of the s tissue punch ap-ach with improved access and visualization ( Figs 7d 8). 3 Furthermore, the surgeon should considering instrumentation that minimizes tissue traumad helps preserve soft tissue volume, which is inncert with the underlying concept of minimallyasive surgery. High-frequency (4 MHz) radio sur-ry instrumentation allows the implant surgeon tointain a relatively “bloodless” d during mini-lly invasive procedures, thus maximizing intraop-tive visibility ( Fig 9). This provides araoperative for surgeons performing implant sur-
URE 5. Lateral p advancement.A, When the apicocoronal dimem, resective maneuvers may result in less than the ideal soft tissironment. Instead, the lateral p advancement maneuver is usponents. After outlining a p that extends well beyond the plann
uccal direction. B and C , The resultant p is apically repositioned aclosure begins at the anterior most implant and progresses distally wues are advanced into the implant surgery site from adjacent area
thony G. Sklar. Guidelines for Flapless Surgery. J Oral Maxillofac Su
ry and adjunctive procedures through the mini- of
lly invasive approaches described earlier. In addi-n, this technology allows the surgeon to performry e incisions in precise locations with negligibleeral tissue damage, resulting in maximum tissueservation at the site.7
Finally, armed with the necessary prerequisites out-ed earlier, the surgeon can take full advantage of
s approach in dental implant surgery. Thes (tissue punch) approach is indicated when
surgeon has e that the underlying osse-s anatomy is ideal relative to the planned implantmeter and 3-dimensional placement in the alveo-. Typically, this is determined by clinical and radio-phic evaluation, aided by analysis of articulatedntal study models. Nevertheless, interactive CTatment planning is of great t for evaluatingseous ridge morphology in a t percentagecases. In cases where site preservation is per-med at the time of tooth removal, the surgeonould closely observe and document the dimensions
f keratinized tissue remaining on the buccal p is between 3 andensions required to establish a stable hard and soft tissue peri-imobtain circumferential tissue closure around the permucosal implant surgery site, tissue is taken from the top of the ridge and movpted around the emerging implant structures and, in most instancetures placed in the interimplant areas. As a consequence, the keratininted with permission. 3)
.
nsion oue dimed toed impnd adaith su
s. (Repr
the remaining alveolar housing and the morphol-

ogallpromeis
mu
ofemestjeotiokergeatitemadremstaeamuuseea�awhditpre
Re1.
2.
3.
4.
5.
6.
7.
8.
FIGadvwitofper
Anlofa
8 GUIDELINES FOR FLAPLESS SURGERY
COLOR
F10
F11
F12
AQ: 2
AQ: 3
AQ: 4
ARTICLE IN PRESS
y of any socket wall defects. This information willow the surgeon to decide whether a �apless ap-ach will be feasible for subsequent implant place-nt in most cases when delayed implant placementplanned after the tooth extraction.Most importantly, as outlined earlier, the surgeon also
URE 6. The U-shaped peninsula �ap. This �ap provides theantages of tissue preservation and patient comfort associatedh the �apless tissue punch approach with enhanced visualizationosseous anatomy during implant surgeries. (Reprinted withmission.3)
thony G. Sklar. Guidelines for Flapless Surgery. J Oral Maxil-c Surg 2007.
st be able to determine whether an adequate volume
good-quality soft tissues will remain surrounding theerging implant structures for optimal function andhetics. To minimize soft tissue complications that canpardize the long-term success of an implant restora-n, the quantity, quality, and position of the existingatinized tissues relative to the planned implant emer-nce should be evaluated before surgery.3 This evalu-on is facilitated by a preoperative try-in of the surgicalplate, allowing the surgeon to determine whether
equate apicocoronal width of keratinized tissue willain after a tissue punch procedure to establish able peri-implant soft tissue environment, as discussedrlier. To make this determination, the implant surgeonst be familiar with the criteria for optimal �ap designsd for implant placement and exposure as outlinedrlier ( Fig 10). When these criteria are not met, thepless approach is contraindicated ( Fig 11). Finally,en unexpected intraoperative �ndings necessitate ad-ional access or visualization, the surgeon must bepared for the appropriate course of action ( Fig 12).
ferencesSclar AG: Preserving alveolar ridge anatomy following toothremoval in conjunction with immediate implant placement: TheBio-Col technique. Atlas Oral Maxillofac Surg Clin North Am7: , 1999Lazzara RJ: Immediate implant placement into extraction sites:Surgical and restorative advantages. Int J Periodont Rest Dent9:333, 1989Sclar AG: Surgical techniques for management of peri-implantsoft tissues. In : Soft Tissue and Esthetic Considerations in Im-plant Therapy. Chicago, IL, Quintessence, 2003, p 43Branemark P-I, Zarb GA, Albrektsson T: Tissue-Integrated Pros-theses: Osteointegration in Clinical Dentistry. Chicago, IL, Quin-tessence, 1985, p 211Berglundh T, Lindhe J: Dimension of the peri-implant mucosa:Biologic width revisited. J Clin Periodontol 23:971, 1996Palacci P, Ericsson I, Engstrand P, et al: Optimal Implant Posi-tioning and Soft Tissue Management for the Brånemark System.Chicago, IL, Quintessence, 1995, p 59Niamtu J: 4.0-MHz radiowave surgery in cosmetic facial surgery.Australas J Cosmetic Surg 1:52, 2005Sclar AG: The Bio-Col technique. In : Soft Tissue and Esthetic
Considerations in Implant Therapy. Chicago, IL, Quintessence,2003, p 75
FIG tendthe ct.C , Bycom sfor age.The
An
ANTHONY G. SKLAR 9
COLOR
ARTICLE IN PRESS
URE 7. Abbreviated �ap-pouch procedure.A, An abbreviated �ap is outlined by incisions that are beveled toward the center of the site thaat the mucogingival junction.B, After subperiosteal elevation of the abbreviated �ap, surgical access and visualization is enhanced by extendingdissection further apically (pouch dissection), allowing a guided bone regeneration procedure to be performed to repair a fenestration defeThe beveled portions of the �ap are precisely readapted and simple interrupted sutures are used for closure at both lateral incisor sites. D,bining an abbreviated �ap with a subperiosteal pouch, an ideal esthetic result was obtained. This minimally invasive approach provided accesperforming the guided bone regeneration procedure without extensive �ap elevation that can result in �ap retraction and soft tissue shrinkpapillary sparing beveled incisions resulted in inconspicuous incision lines and maintenance of scalloped soft tissue architecture.
thony G. Sklar. Guidelines for Flapless Surgery. J Oral Maxillofac Surg 2007.

10 GUIDELINES FOR FLAPLESS SURGERY
COLOR
ARTICLE IN PRESS
FIGURE 8.
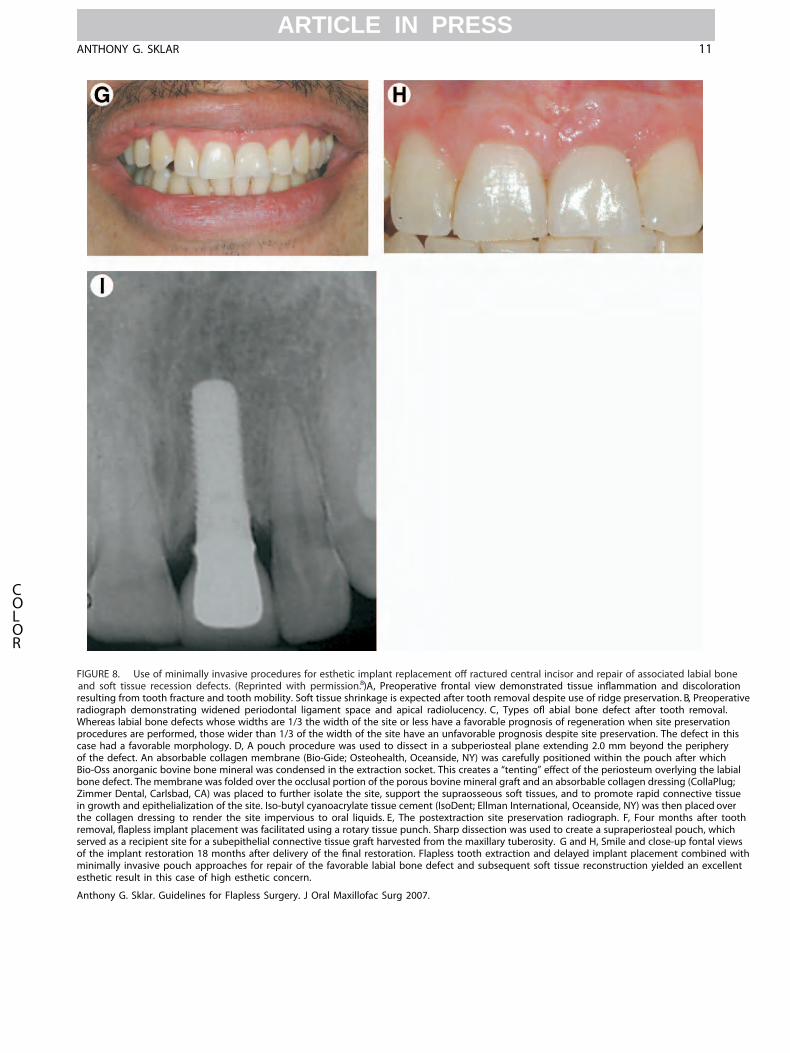
FIG eand onres ativeradWhpro iscasof tBio ialbon ;Zim uein g rthe othrem hser wsof t withmin ntest
An
ANTHONY G. SKLAR 11
COLOR
ARTICLE IN PRESS
URE 8. Use of minimally invasive procedures for esthetic implant replacement o� ractured central incisor and repair of associated labial bonsoft tissue recession defects. (Reprinted with permission.8)A, Preoperative frontal view demonstrated tissue in�ammation and discolorati
ulting from tooth fracture and tooth mobility. Soft tissue shrinkage is expected after tooth removal despite use of ridge preservation. B, Preoperiograph demonstrating widened periodontal ligament space and apical radiolucency. C, Types o� abial bone defect after tooth removal.ereas labial bone defects whose widths are 1/3 the width of the site or less have a favorable prognosis of regeneration when site preservationcedures are performed, those wider than 1/3 of the width of the site have an unfavorable prognosis despite site preservation. The defect in the had a favorable morphology. D, A pouch procedure was used to dissect in a subperiosteal plane extending 2.0 mm beyond the peripheryhe defect. An absorbable collagen membrane (Bio-Gide; Osteohealth, Oceanside, NY) was carefully positioned within the pouch after which-Oss anorganic bovine bone mineral was condensed in the extraction socket. This creates a “tenting” e�ect of the periosteum overlying the labe defect. The membrane was folded over the occlusal portion of the porous bovine mineral graft and an absorbable collagen dressing (CollaPlugmer Dental, Carlsbad, CA) was placed to further isolate the site, support the supraosseous soft tissues, and to promote rapid connective tissrowth and epithelialization of the site. Iso-butyl cyanoacrylate tissue cement (IsoDent; Ellman International, Oceanside, NY) was then placed ovecollagen dressing to render the site impervious to oral liquids. E, The postextraction site preservation radiograph. F, Four months after tooval, �apless implant placement was facilitated using a rotary tissue punch. Sharp dissection was used to create a supraperiosteal pouch, whicved as a recipient site for a subepithelial connective tissue graft harvested from the maxillary tuberosity. G and H, Smile and close-up fontal viehe implant restoration 18 months after delivery of the �nal restoration. Flapless tooth extraction and delayed implant placement combinedimally invasive pouch approaches for repair of the favorable labial bone defect and subsequent soft tissue reconstruction yielded an excellehetic result in this case of high esthetic concern.
thony G. Sklar. Guidelines for Flapless Surgery. J Oral Maxillofac Surg 2007.
FIGdentroperVerme a-tive -vidinv
Anlofa
12 GUIDELINES FOR FLAPLESS SURGERY
COLOR
ARTICLE IN PRESS
URE 9. Application of 4-MHz radio surgery in minimally invasivetal implant surgery. The 4-MHz radio surgery technology (Surgi-n; Ellman International, Oceanside, NY) allows the surgeon toform incisions with minimal heat dissipation and cellular alteration.y �ne incisions can be precisely located adjacent to implant abut-nts without the risk of unanticipated soft tissue recession. The relly bloodless surgical �eld achieved using this instrumentation proes a tremendous advantage for surgeons performing minimallyasive dental implant surgery.
thony G. Sklar. Guidelines for Flapless Surgery. J Oral Maxil-c Surg 2007.

FIGma erad hspos forpla epap etisspos thehar otethe
An
ANTHONY G. SKLAR 13
COLOR
ARTICLE IN PRESS
URE 10. Application of the �apless approach for implant replacement of a failing mandibular molar. A , Preoperative radiograph of a failingndibular molar. The patient had experienced continued sensitivity after completing endodontic therapy over a 2-year period. Note thiolucency in the interradicular area indicating a chronic in�ammatory process most likely associated with bacterial ingress. B, Three monttextraction with site preservation with the Bio-Col technique, the location and apicocoronal dimension of keratinized tissue at the site is idealcement of the implant through a �apless approach.C, One week post-�apless implant placement. Peri-implant tissue health is ideal, and thillary and col anatomy have been preserved. Note that adequate apicocoronal dimension of keratinized tissue surround the implant despite thue punch procedure. Accelerated healing and improved postoperative oral hygiene are evident. D and E, Clinical and radiographic views 1 yeartdelivery of the �nal restoration. The �apless approach for tooth extraction, site preservation, and subsequent implant placement preservedd and soft tissue ridge contours facilitating the delivery of an implant restoration that is functional, self-cleansing, and esthetically pleasing. Ncomplete resolution of preexisting radiolucency and maintenance o� deal crestal bone levels.
thony G. Sklar. Guidelines for Flapless Surgery. J Oral Maxillofac Surg 2007.
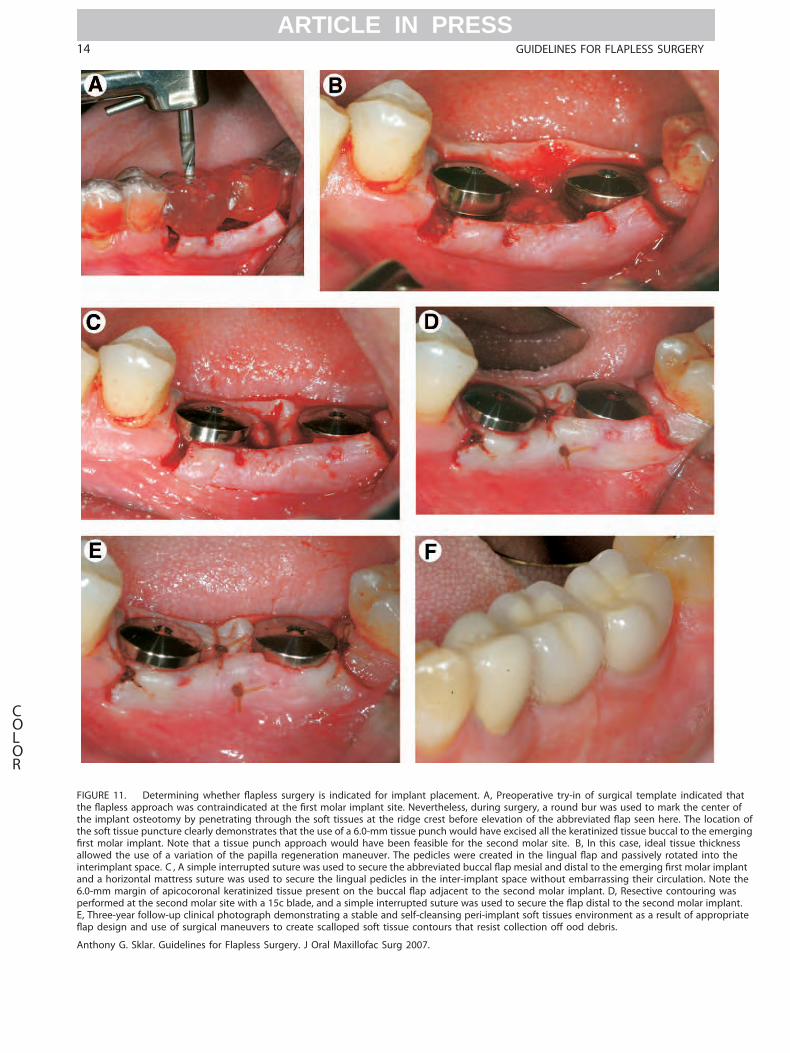
FIG hatthe ofthe on ofthe rging�rs ssallo einte lantand the6.0 sper nt.E, T riate�ap
An
14 GUIDELINES FOR FLAPLESS SURGERY
COLOR
ARTICLE IN PRESS
URE 11. Determining whether �apless surgery is indicated for implant placement. A, Preoperative try-in of surgical template indicated t�apless approach was contraindicated at the �rst molar implant site. Nevertheless, during surgery, a round bur was used to mark the centerimplant osteotomy by penetrating through the soft tissues at the ridge crest before elevation of the abbreviated �ap seen here. The locatisoft tissue puncture clearly demonstrates that the use of a 6.0-mm tissue punch would have excised all the keratinized tissue buccal to the emet molar implant. Note that a tissue punch approach would have been feasible for the second molar site. B, In this case, ideal tissue thicknewed the use of a variation of the papilla regeneration maneuver. The pedicles were created in the lingual �ap and passively rotated into thrimplant space. C , A simple interrupted suture was used to secure the abbreviated buccal �ap mesial and distal to the emerging �rst molar impa horizontal mattress suture was used to secure the lingual pedicles in the inter-implant space without embarrassing their circulation. Note
-mm margin of apicocoronal keratinized tissue present on the buccal �ap adjacent to the second molar implant. D, Resective contouring waformed at the second molar site with a 15c blade, and a simple interrupted suture was used to secure the �ap distal to the second molar implahree-year follow-up clinical photograph demonstrating a stable and self-cleansing peri-implant soft tissues environment as a result of appropdesign and use of surgical maneuvers to create scalloped soft tissue contours that resist collection o� ood debris.
thony G. Sklar. Guidelines for Flapless Surgery. J Oral Maxillofac Surg 2007.
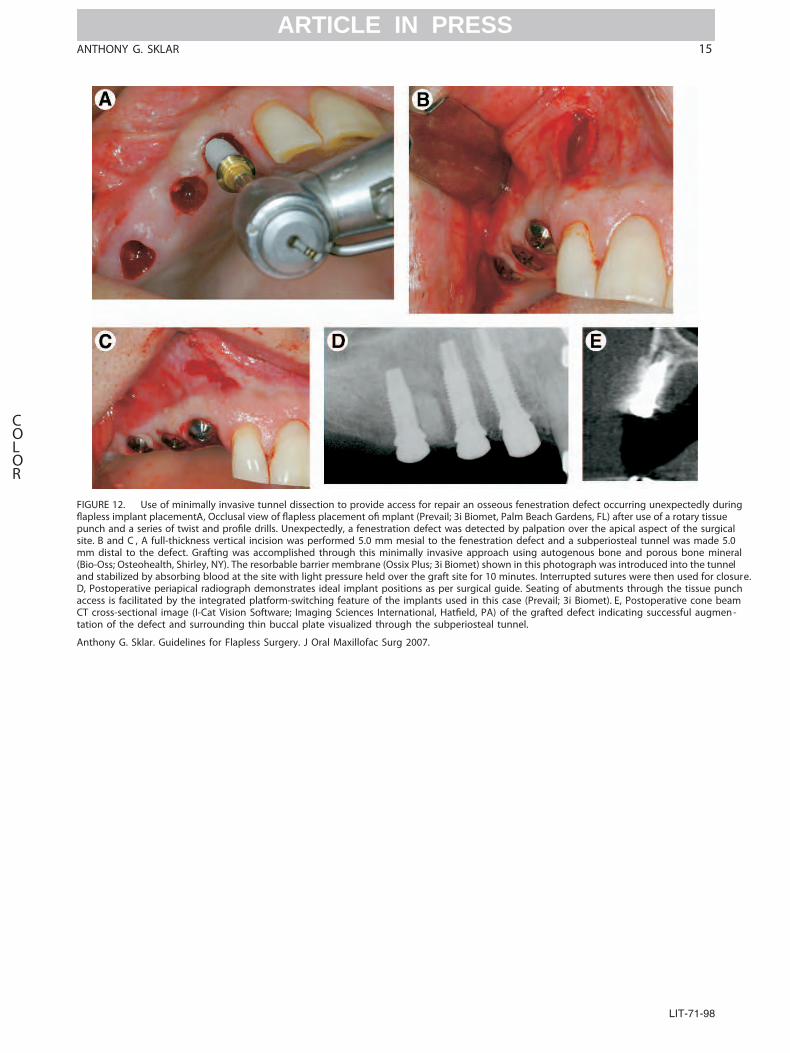
FIG ing
pun alsite .0mm ral(Bio eland sure.D, chacc mCT -tati
An
ANTHONY G. SKLAR 15
COLOR
ARTICLE IN PRESS
URE 12. Use of minimally invasive tunnel dissection to provide access for repair an osseous fenestration defect occurring unexpectedly durs implant placement.A, Occlusal view of s placement o mplant (Prevail; 3i Biomet, Palm Beach Gardens, FL) after use of a rotary tissue
ch and a series of twist and e drills. Unexpectedly, a fenestration defect was detected by palpation over the apical aspect of the surgic. B and C , A full-thickness vertical incision was performed 5.0 mm mesial to the fenestration defect and a subperiosteal tunnel was made 5distal to the defect. Grafting was accomplished through this minimally invasive approach using autogenous bone and porous bone mine-Oss; Osteohealth, Shirley, NY). The resorbable barrier membrane (Ossix Plus; 3i Biomet) shown in this photograph was introduced into the tunnstabilized by absorbing blood at the site with light pressure held over the graft site for 10 minutes. Interrupted sutures were then used for clo
Postoperative periapical radiograph demonstrates ideal implant positions as per surgical guide. Seating of abutments through the tissue puness is facilitated by the integrated platform-switching feature of the implants used in this case (Prevail; 3i Biomet). E, Postoperative cone beacross-sectional image (I-Cat Vision Software; Imaging Sciences International, , PA) of the grafted defect indicating successful augmenon of the defect and surrounding thin buccal plate visualized through the subperiosteal tunnel.
thony G. Sklar. Guidelines for Flapless Surgery. J Oral Maxillofac Surg 2007.
LIT-71-98