article for journal(1)
DESCRIPTION
kklTRANSCRIPT

Improving Stroke Education PerformanceMeasures Scores: The Impact of a StrokeNurse Coordinator
Josephine Malfitano, Barbara S. Turner, Ed Piper, Penney A. Burlingame,Elizabeth D’Angelo
ABSTRACTBackground: Stroke is a leading cause of death and adult disability worldwide. North Carolina isconsidered to be a part of an area of the United States called the ‘‘stroke belt.’’ Education coupled withimplementation of a program that promotes primary and secondary stroke prevention is paramount tosupport the reduction of stroke and improvement of stroke care across the continuum. The groundwork forstroke care at Onslow Memorial Hospital began in 2006 with participation in the North Carolina StrokeCare Collaborative (NCSCC), which allowed for benchmarking of data. Methods: A pretest and posttestdesign was used to evaluate the effectiveness of a dedicated stroke nurse coordinator on stroke educationperformance measure scores. Compliance with stroke education performance measures is met whendocumentation reflects education provided or material given during the hospital stay. Three hundred sixty-sevencharts submitted to the NCSCC from Onslow Memorial Hospital were reviewed. Data collected were enteredinto the NCSCC Registry database during the period of 2008Y2010. Performance measures were compared atthree points: the year before implementation of the stroke nurse coordinator, the implementation year, and,the year after the implementation of the stroke nurse coordinator position. Results: Stroke educationperformance measure scores for the preimplementation year (2008) were 58.1%, which improved to 86.4%for the year that the nurse coordinator position was created and filled, and rose to 96.9% for the 1-yearperiod after the position was filled. Scores from Z tests comparing proportions over time between each of the3 years were statistically significant. Conclusions: Implementation of a stroke nurse coordinator to improvestroke care and education is a coordinated effort that will impact stroke outcomes across the healthcarecontinuum, with efforts geared toward primary and secondary prevention strategies. This role providessupportive resources for the community, individualized care with patients and families as well as supportingstaff in providing stroke education, and awareness. Stroke education has shown improvement in patientsunderstanding the signs and symptoms of stroke as well as improved compliance with treatment plans; the useof a dedicated educator is supported.
Keywords: education, nurse coordinator, performance measures, quality, stroke, stroke education
S troke is a leading cause of death and adult dis-ability worldwide and the fourth leading causeof death in the United States. North Carolina
ranks fifth in the nation in the incidence of strokes(American Heart Association, 2011; Huston, 2010;North Carolina Stroke Care Collaborative [NCSCC],2010) and is a part of the southeastern United Statescalled the ‘‘stroke belt’’Va cluster of 8Y12 stateswith higher stroke mortality than the national average(NCSCC, 2010). In addition to the human sufferingcaused by strokes, the economic impact of strokes inNorth Carolina is estimated at 1.05 billion dollars ayear (Holmes, 2008).
Currently, only 18% of adults in North Carolinacan correctly identify stroke signs and symptoms, andthose at high risk for stroke with (hypertension or aprevious stroke) do not know the symptoms any betterthan those at lower risk (Holmes, 2008). Educatingthe public as well as those who have experiencedstroke, their families, and healthcare professionals onthe signs and symptoms and need for early interven-tion is one strategy for improving stroke preventionand outcomes. A focused resource provider who offers
Journal of Neuroscience Nursing332
Questions or comments about this article may be directed toJosephineMalfitano,DNPMBARNFNPCPHQNE-BC,at [email protected]. She is the Performance Improvement & AccreditationManager, Onslow Memorial Hospital, Jacksonville, NC.
Barbara S. Turner, PhD RN FAAN, is the Elisabeth P. HanesDistinguishedProfessor andDirectorof theDoctorofNursingPracticeProgram at Duke University School of Nursing, Durham NC.
Ed Piper, PhD FACHE, is the President and CEOofOnslowMemorialHospital, Jacksonville, NC.
Penney A. Burlingame, DHA RN FACHE, is the Senior Vice Presidentof Nursing and Clinical Services of Onslow Memorial Hospital,Jacksonville, NC.
Elizabeth D’Angelo, MD, is a Radiologist and Chief of Staff atOnslow Memorial Hospital, Jacksonville, NC.
The authors declare no conflicts of interest.
Copyright B 2013American Association of Neuroscience Nurses
DOI: 10.1097/JNN.0b013e3182a3ce63
Copyright © 2013 American Association of Neuroscience Nurses. Unauthorized reproduction of this article is prohibited.Copyright © 2013 American Association of Neuroscience Nurses. Unauthorized reproduction of this article is prohibited.

stroke education to patients, families, and staff is ameans to support one of the stroke quality indicatorsproposed by the NCSCC and The Joint Commission.
BackgroundA lack of prevention strategies and lack of care co-ordination once stroke patients leave the hospital aremajor problems in stroke care (Lennert, 2009). Giventhe importance of early intervention for stroke, it isimperative that patients and families understand riskfactors for stroke, recognize stroke signs and symp-toms, and act by calling 9-1-1. Research suggests thatdelay in seeking treatment for acute coronary andstroke symptoms limits effective treatment optionsand results in a greater likelihood of permanent dis-ability or death (Huston, 2010). Redfern, Rudd, Wolfe,and McKevitt (2008) have reported on attempts to im-prove secondary prevention of stroke through patientand caregiver education initiatives to improve strokeknowledge. One approach described was the develop-ment of nurse coordinators to transition the patient’scare between healthcare providers, with the goal ofimproving access to care. Lindsay et al. (2008) foundthat stroke education improved patient knowledge ofsigns and symptoms of stroke as well as compliancewith the treatment plans for stroke. Similarly, Greenand Newcommon (2006) have reported that imple-mentation of stroke standards of care along with a ded-icated stroke educator improved the quality of care forstroke patients after discharge and also improved sys-tems and processes.
These studies point to the need for focused educa-tion interventions to improve stroke care and outcomes.Yet, despite awareness among health professionals ofthe importance of risk factor management for sec-ondary stroke prevention, studies show that adherenceto secondary prevention is still poor (Slark, 2010).Strategies are needed to involve patients and familiesin sharing information, setting goals, and assessingneeds, which are a part of discharge planning (Almborg,Ulander, Thulin, & Berg, 2009). Understanding theneeds of stroke patients and their families can providea basis for educational processes to improve outcomes.
Setting and MethodsIn North Carolina, Onslow County is in the south-eastern region of the state, a significant risk area forstroke; it is considered the ‘‘buckle’’ of the stroke belt,an area with even greater stroke mortality, three timeshigher than the national average (NCSCC, 2010). Theregion has high rates of hypertension, cardiovasculardisease, obesity, and diabetesVfactors that put the pop-ulation at significant risk for stoke according to the
NC County Trends report from the NCDepartment ofHealth and Human Services. Onslow County showedan increase in stroke deaths in 2006, despite a declinein overall state deaths from stroke (North Carolina De-partment of Health and Human Services Resources:Division of Public Health, 2006).
Onslow Memorial Hospital (OMH) is a 162-bednot-for-profit acute-care community hospital. OMH isa leader in healthcare to a community that has sig-nificant uninsured and underserved populations. Thesepopulations regularly seek acute disease managementthrough the emergency department because they havelimited access to primary care, and they receive incon-sistent follow-up for prevention of recurrent strokes.
OMH began in 2006 through participation in theNCSCC, benchmarking data. Initial data collected thatyear showed that compliance in providing strokeeducation was only 28%. There was a clear need toimprove stroke care at OMH. Improvements in strokecare were made by implementing standing orders,using evidence-based clinical practice guidelines forinpatients and the emergency department, improvingdysphagia screening, and the process of expeditingradiology diagnostic testing and developing a strokefolder with patient education material. Compliance instroke education improved to 40% in 2007. However,the stroke team believed that more could be accom-plished with the implementation of a full-time strokenurse coordinator (SNC) to provide stroke education/awareness and prevention strategies to frontline staff,patients, and families.
OMH’s focus is on increasing the state’s strokeawareness program using a three-pronged approach:prevention and education in prehospital screening,
Because prevention and early
recognition of stroke are critical in
minimizing the potentially negative
short- and long-term outcomes
related to cerebrovascular disease,
it is imperative that patients and
families receive focused education
that could improve these.
Volume 45 & Number 6 & December 2013 333
Copyright © 2013 American Association of Neuroscience Nurses. Unauthorized reproduction of this article is prohibited.Copyright © 2013 American Association of Neuroscience Nurses. Unauthorized reproduction of this article is prohibited.
individualized acute care education, and posthospitalfollow-up. The dedicated educator/SNC serves as theliaison and resource for community stroke needs andpatient and family education, while also providingeducation and support to hospital staff. The SNC alsofacilitates interdisciplinary care coordination andmon-itors stroke outcomes.
The SNC provides community outreach and edu-cation on inpatient and poststroke care by leveragingNC Stroke Association Programs and by implementingestablished standards of stroke care. A Stroke RiskIdentification Screening Program provides standard-ized protocols for identifying stroke risk factors, coun-seling participants, directing them to resources, andproviding outcome management through partnershipsfor those found to be at high risk for stroke. In thisway, we identify interventions needed or potentialproblems with access. A Beyond the Hospital Programprovides evidence-based practice protocols for post-stroke education to patients in the acute care settingand at discharge. Each person is then contacted within3months with a follow-up call. This approach provides
quantifiable care measures and educational outcomesfor stroke prevention.
The SNC serves as a center for education and faci-litation of stroke care across the continuum. The workbegins with programs to increase community aware-ness and healthcare screenings as well as interactionswith the local health department and emergency man-agement offices to establish collaborations in stroke care.In the hospital, the stroke nurse makes rounds daily toreinforce inpatient stroke care based on evidence-basedguidelines. Patients and families are provided educa-tional materials, video-on-demand stroke resources, andan interdisciplinary plan of care based on individualneeds. The SNC ensures that staff education is ongoingfrom the time of orientation to the organization; the edu-cation includes annual mandatory computerized modulelearning, regular staff meetings, and real-time feedbackwith chart reviews and updated care management dis-cussions. The SNC is readily accessible to staff viapager and also supports families. The coordinator alsoreviews cases, analyzes and shares data for stroke im-provement initiatives, and serves as a resource for other
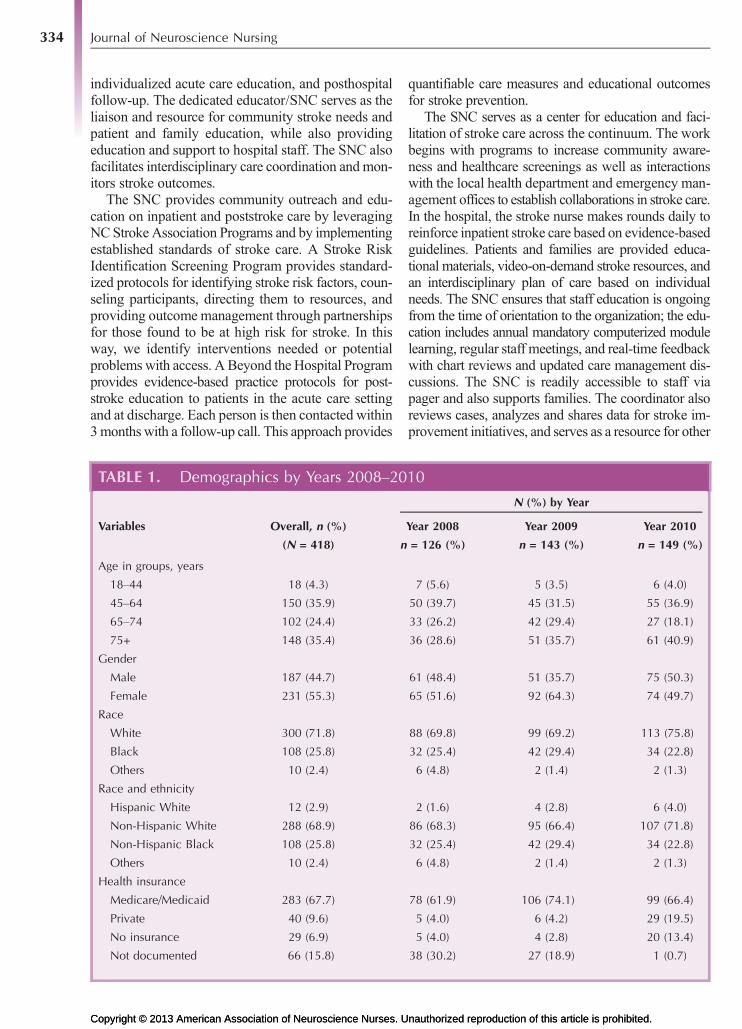
TABLE 1. Demographics by Years 2008Y2010
N (%) by Year
Variables Overall, n (%) Year 2008 Year 2009 Year 2010
(N = 418) n = 126 (%) n = 143 (%) n = 149 (%)
Age in groups, years
18Y44 18 (4.3) 7 (5.6) 5 (3.5) 6 (4.0)
45Y64 150 (35.9) 50 (39.7) 45 (31.5) 55 (36.9)
65Y74 102 (24.4) 33 (26.2) 42 (29.4) 27 (18.1)
75+ 148 (35.4) 36 (28.6) 51 (35.7) 61 (40.9)
Gender
Male 187 (44.7) 61 (48.4) 51 (35.7) 75 (50.3)
Female 231 (55.3) 65 (51.6) 92 (64.3) 74 (49.7)
Race
White 300 (71.8) 88 (69.8) 99 (69.2) 113 (75.8)
Black 108 (25.8) 32 (25.4) 42 (29.4) 34 (22.8)
Others 10 (2.4) 6 (4.8) 2 (1.4) 2 (1.3)
Race and ethnicity
Hispanic White 12 (2.9) 2 (1.6) 4 (2.8) 6 (4.0)
Non-Hispanic White 288 (68.9) 86 (68.3) 95 (66.4) 107 (71.8)
Non-Hispanic Black 108 (25.8) 32 (25.4) 42 (29.4) 34 (22.8)
Others 10 (2.4) 6 (4.8) 2 (1.4) 2 (1.3)
Health insurance
Medicare/Medicaid 283 (67.7) 78 (61.9) 106 (74.1) 99 (66.4)
Private 40 (9.6) 5 (4.0) 6 (4.2) 29 (19.5)
No insurance 29 (6.9) 5 (4.0) 4 (2.8) 20 (13.4)
Not documented 66 (15.8) 38 (30.2) 27 (18.9) 1 (0.7)
Journal of Neuroscience Nursing334
Copyright © 2013 American Association of Neuroscience Nurses. Unauthorized reproduction of this article is prohibited.Copyright © 2013 American Association of Neuroscience Nurses. Unauthorized reproduction of this article is prohibited.
facilities to network, benchmark data, and develop bestpractices measures in stroke care.
Key supporters of the role of the SNC are strokechampions, including those in frontline nursing, reha-bilitation, radiology, pharmacy, dietary, education, localEmergency Medical Services, emergency departmentstaff/providers, and leadership. The SNC facilitatesthe work of interdisciplinary teams so that stroke careand education are consistent across the continuum.Evidence-based practice guideline protocols and policiesas well as tools and checklists for more effective andefficient documentation have been developed. Hard-wiring system improvements and processes includechecklist documentation on the nursing record andinterdisciplinary discharge plans of care. Local newspaperarticles have been developed on stroke awareness, alongwith Web sites and videos. Additional educational re-sources include a stroke awareness packet, stroke riskpamphlet, and stroke publication flyers provided topatients and staff.
Stroke education is one of 10 quality performanceindicators endorsed by the National Quality Forum. Thestroke education performance measures state that meet-ing compliance in stroke education requires that docu-mentation of ischemic stroke patients or their caregivers
were given educationalmaterial during their hospital stayaddressing all of the following five elements: activationof the emergency medical system, follow-up after dis-charge, medications prescribed at discharge, risk fac-tors for stroke, and warning signs and symptoms ofstroke (The Joint Commission and Center of Medicare/Medicaid Services, 2011).
Accurate and consistent documentation of educationmust be recorded in the medical record. When docu-mentation is incomplete, the performance is considereda failure or variance.
To determine whether an SNC improved strokeeducation, we collected data at three measurementpoints to see if there were significant trends in strokeeducation performance scores: 2008, the year beforeintroduction of the SNC; 2009, the year of imple-mentation; and 2010, the year after implementation ofthe SNC position. The first 6 months of 2011 werealso analyzed to determine if improvements were sus-tained. During 2008Y2011, 418 stroke patient chartswere reviewed. To be included in the analysis, patientshad to be 18 years old or older and discharged with anICD-9 for stroke. Patients who had a length of staygreater than 120 days, palliative care patients, and patientsenrolled in clinical trials or patients admitted for elective
TABLE 2. Stroke Education Compliance Scores Z Test Comparison Proportions Over Time
Sample Population:Stroke Only
Sample Population:Stroke and TIA
Comparing ProportionsOver Time:
Probability by YearSample Population:
Stroke Only
Year NPerformanceMeasure Score N
PerformanceMeasure Score Year Z Score p
2008 62 58.1 108 49.1 2008Y2009 3.716 .0001
2009 66 86.4 120 80.0 2009Y2010 2.2003 .0139
2010 65 96.9 104 91.3 2008Y2010 5.8097 G.0001
2011a 21 95.2 35 97.1
Note. Data provided by NCSCC.aStatistically significant at p G .05.
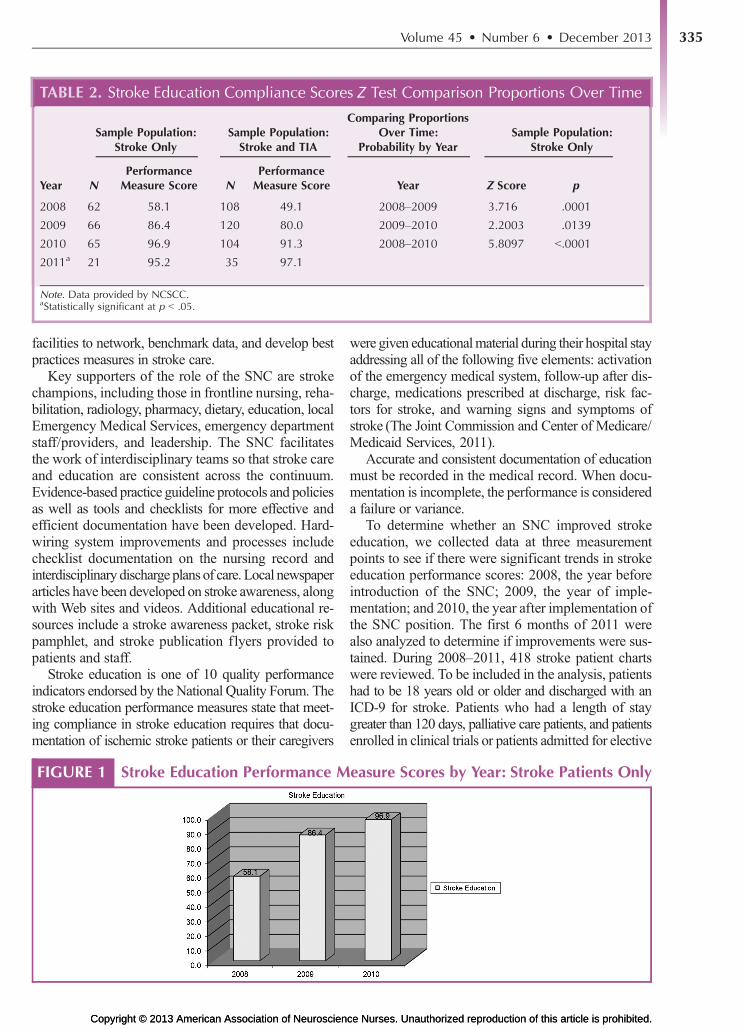
FIGURE 1 Stroke Education Performance Measure Scores by Year: Stroke Patients OnlyFIGURE 1
Volume 45 & Number 6 & December 2013 335
Copyright © 2013 American Association of Neuroscience Nurses. Unauthorized reproduction of this article is prohibited.Copyright © 2013 American Association of Neuroscience Nurses. Unauthorized reproduction of this article is prohibited.
carotid intervention were excluded. Using these inclu-sion criteria, there were 367 charts eligible for review.
The NCSCC conducts a data quality assessmentannually. Reliability of 5% of the data entered into theNCSCC Registry from April 2009 through June 2010was examined to determine if the data submitted tothe NCSCC were in agreement with the medical re-cord documentation. There was 95% congruence indata elements. Additional quality assessment was con-ducted through case ascertainment to determine if thenumber of stroke cases admitted to the hospital duringa designated 60-day period was consistent with thenumber of missing cases entered and to determine ifthe number and type of stroke cases admitted to thehospital during a 1-year period was comparable withthose entered into the NCSCC.
Data abstraction followed consistent and recog-nized national guidelines. Data for obtaining strokeeducation performancemeasures were collected usingretrospective chart audits following the format of theNCSCC stroke care cards, which contain numerousquestions to determine if documentation to supportcompliance with performance indicators is maintained.Charts were selected for review using patients whowere discharged with an ICD-9 stroke code. The sam-ple included 100% of the stroke patients who were
hospitalized in the preimplementation and postim-plementation times. Charts were reviewed monthly,and data abstraction was done by the SNC and threeperformance improvement personnel, who were trainedto abstract data and follow the prescribed definitionsto enter the data into the appropriate databases. Assign-ing consistent staff for data abstractions prevented var-iability in the interpretation of the data. To further supportthe reliability and integrity of the data, queries relatedto stroke performance measures that were identified dur-ing chart abstraction were filtered through the NCSCCRegistry or the Joint Commission for clarification.
Data AnalysisThree hundred sixty-seven patient records from 2008to 2011, including 35 chart audits during JanuaryYJune 2011, were analyzed. All included inpatients witha primary diagnosis of ischemic stroke and/or transientischemic attack who met the inclusion criteria.
Table 1 depicts the demographic of the sample, andTable 2 and Figures 1Y3 document improvement in strokeeducation compliance scores, from 58.1% in the yearbefore the initiation of the SNC role to 86.4% in theyear the role was filled and 96.9% in the year after therole was initiated. Data for 2011 (partial year) showedcontinued sustainability of the improvement, at 95.2%.
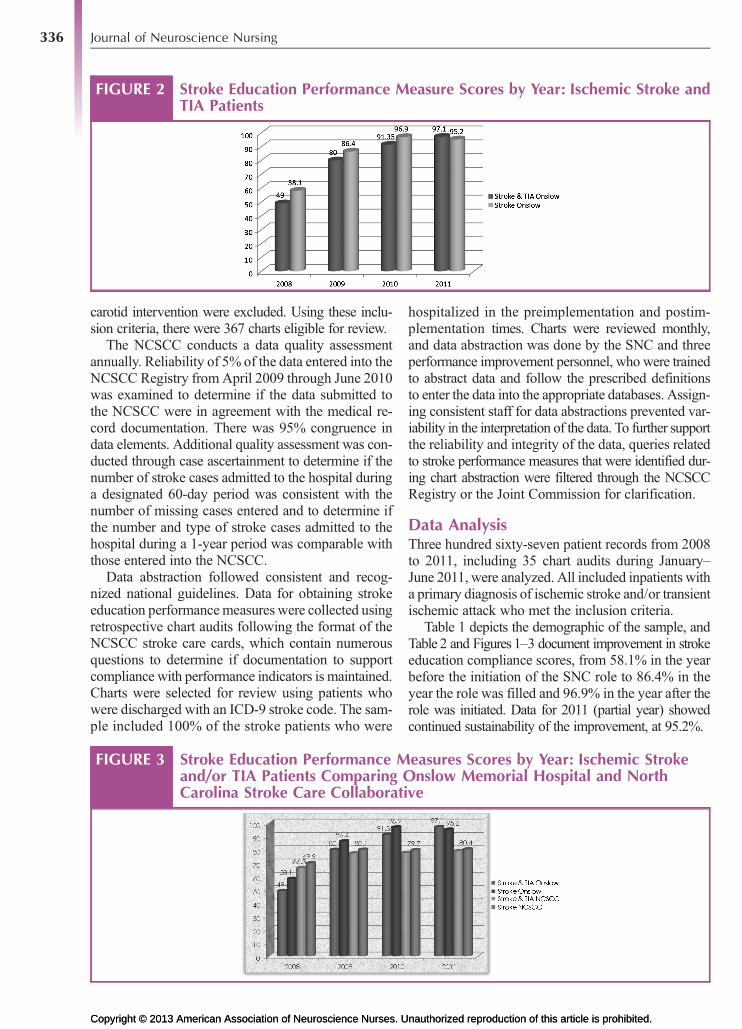
FIGURE 2 Stroke Education Performance Measure Scores by Year: Ischemic Stroke andTIA Patients
FIGURE 2
FIGURE 3 Stroke Education Performance Measures Scores by Year: Ischemic Strokeand/or TIA Patients Comparing Onslow Memorial Hospital and NorthCarolina Stroke Care Collaborative
FIGURE 3
Journal of Neuroscience Nursing336
Copyright © 2013 American Association of Neuroscience Nurses. Unauthorized reproduction of this article is prohibited.Copyright © 2013 American Association of Neuroscience Nurses. Unauthorized reproduction of this article is prohibited.

When the data from patients with stroke and tran-sient ischemic attack were analyzed, the improvementsin stroke education compliance scores were similar tothose for stroke alone.
DiscussionImplementation of the SNC role was associated withimproved stroke education performance measure scores.The coordinator provides supportive resources for thecommunity and individualized care for patients andfamilies, while also supporting staff in providing strokeeducation and awareness. The SNC functions to aligncollaborative stroke care efforts for seamless processimprovement in the acute care setting. Studies of com-pliance in poststroke care management at home haveshown that adherence to secondary prevention is stillpoor, supporting the significance of this role for strokeeducation and awareness among healthcare profes-sionals, patients, and families (Slark, 2010). Strokehealthcare teams need to develop strategies to involverelatives of stroke patients in sharing information,goal setting, and discharge planning (Almborg et al.,2009). Understanding the needs of stroke patientsand their families can assist the care team to provideeducation for improved outcomes. Additional con-siderations include further investigations that willalign the compliance with performance measures andoutcomes notable with strategies currently beingimplemented such as with postdischarge telephonecalls and demonstration of readmission reduction.
Since the implementation of the SNC role at OMH,stroke education compliance has shown sustainedimprovements, from 58% in 2008, the year beforeimplementation of the coordinator, to 86% in 2009(the implementation year) and 96% at the end of2010 (1-year post implementation of the SNC role).In the first 6 months of 2011, the data continue to showsustainability, with stroke education performancescores at 95%.
Of interest is that the data from OMH, when com-pared with North Carolina statewide scores, show higherperformance measures for 2009Y2011Vthe time pe-riod associated with the use of the dedicated SNC.
The best way to treat a stroke is to prevent it (Albert,2011). Education is the mechanism for delivering thismessageVprimary prevention and, in the case of thepopulation involved in the study, secondary preven-tion. Patients who have had a stroke are at higher riskfor another stroke. Education coupled with imple-mentation of a program that promotes primary and/orsecondary stroke prevention is paramount to supportthe reduction of stroke and improvement of stroke careacross the continuum. Strategies that enhance patientand professional awareness of stroke risk factors are
feasible to produce and deliver and can improve strokecare and disease management (Lennert, 2009). TheSNC role supports stroke care improvement interven-tions and strategies for increasing education and aware-ness of risk factors, medications, signs, and symptomsof stroke and activation of emergency managementsystem calling 9-1-1.
AcknowledgmentsThis project was funded in part through the NorthCarolina Stroke Care Collaborative, North CarolinaStroke Association, and Kate B. Charitable Trust.Data were provided through the North CarolinaStroke Care Collaborative.
ReferencesAlbert, M. (2011). Personal communication. Northwestern Uni-
versity. [email protected]
Almborg, A., Ulander, K., Thulin, A., & Berg, S. (2009).Review: Understanding the needs of families: Dischargeplanning of stroke patients: The relatives’ perceptions ofparticipation. Journal of Clinical Nursing, 18, 857Y865.
American Heart Association. (2011). About stroke. Retrievedhttp://www.strokeassociation.org/STROKEORG/AboutStroke/AboutStroke_UCM_30829_SubHomePage.jsp
Green, T., & Newcommon, N. (2006). Advanced nursing practice:The role of the nurse practitioner in an acute stroke program.Journal of Neuroscience Nursing, 38(4), 328Y330.
Holmes, A. (2008). Stroke in North Carolina: Addressing the burdentogether. Raleigh, NC: NC Stroke Advisory Council Meeting.
Huston, S. (2010). Heart disease and stroke prevention branchchronic disease and injury section: The burden of cardio-vascular disease in North Carolina (annual report). Divisionof Public Health, North Carolina Department of Health &Human Service. Retrieved from http://www.startwithyourheart.com/Default.aspx?pn=CVDBurden
Lennert, B. (2009). Care management for TIA and strokepatients: Riding the quality improvement wave. AmericanHealth and Drug Benefits, 2(6, Suppl. 8), S24YS27.
Lindsay, P., Bayley, M., Hellings, C., Hill, M., Woodbury, E.,& Phillips, S. (2008). Public awareness and patienteducation: Patient and family education. Canadian MedicalAssociation Journal, 179(Suppl. 12), 15Y16.
North Carolina Department of Health and Human Services Re-sources: Division of Public Health. (2006). North CarolinaStatewide and County Trends in key health indicators: OnslowCounty. Raliegh, NC: State Center of Health Statistics.
North Carolina Stroke Care Collaborative. (2010). NorthCarolina in the buckle of the stroke belt. Retrieved http://ncstrokeregistry.com/stroke2010/Overview/Stkbuckle.htm
Redfern, J., Rudd, A., Wolfe, C., & McKevitt, C. (2008). Stopstroke: Development of an innovative intervention toimprove risk factor management after stroke. PatientEducation and Counseling, 72, 201Y209.
Slark, J. (2010). Adherence to secondary prevention strategiesafter stroke: A Review of the literature. British Journal ofNeuroscience Nursing, 6(6), 282Y286.
The Joint Commission and Center of Medicare/MedicaidServices. (2011). Specifications Manual for NationalHospital Inpatient Quality Measures (Version 3.2c) [datafile]. Washington, DC: Author.
Volume 45 & Number 6 & December 2013 337
Copyright © 2013 American Association of Neuroscience Nurses. Unauthorized reproduction of this article is prohibited.Copyright © 2013 American Association of Neuroscience Nurses. Unauthorized reproduction of this article is prohibited.